#infertility evaluation
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr Inc. is funded by 13 investors.
Text
ive never had the desire to have kids never experiences baby fever or anything like that but idkkkk like im thinking abt it and it kinda sucks that i probably dont even have the opportunity even if i wanted to
#i donttt want kids but i dont like having no choice in the matter ykno?#i say probabbly infertile because ive never actually gone to a doctor to get it evaluated but umm how to put this#i use maybeee like 15 pads in an entire year. which im pretty sure is weird#sorry tmi but i just dont like having no say urgrhghrzrhhhhsh
15 notes
·
View notes
Text
Best Fertility Evaluation Doctor in Delhi - Laimaa

Laimaa Healthcare is renowned as the best fertility evaluation doctor in Delhi, specializing in comprehensive assessments that pave the way for effective infertility treatments. Our expert team employs state-of-the-art technologies and personalized care plans to diagnose and address fertility challenges. As one of the best infertility treatment clinics in Delhi, we are committed to guiding couples through their journey with compassion and expertise. Whether you seek in-depth evaluations or advanced treatment options, Laimaa Healthcare is dedicated to helping you achieve your dream of parenthood
#best ivf clinic in delhi#best ivf centre in delhi#best fertility evaluation doctors in delhi#best infertility treatment clinic in delhi
0 notes
Text

Explore key factors for choosing the best infertility centers in Hyderabad. Learn about essential considerations for successful fertility treatments.
Do Visit: https://www.healixhospitals.com/blogs/choosing-the-best-infertility-centers-in-hyderabad:-factors-to-consider
#Best Infertility Centers in Hyderabad#Top Infertility Centers in Hyderabad#Infertility Centers in Hyderabad#Infertility centers in Hyderabad#Fertility clinics in Hyderabad#Best fertility centers criteria#Hyderabad fertility specialists#Infertility treatment factors#Choosing fertility clinics#Top infertility centers in Hyderabad#Criteria for selecting fertility centers#Infertility clinic services#Evaluating fertility centers#Hyderabad fertility treatment options#Factors in infertility center selection#Assessing infertility clinics#Services offered by fertility centers#Expertise of fertility specialists#Hyderabad infertility treatment criteria#Reputation of infertility centers#Success rates of fertility clinics#Patient reviews of infertility centers#Infertility center accreditation
1 note
·
View note
Text
Understanding Male Infertility and its Management
Introduction Infertility is a common concern affecting couples worldwide. While often associated with females, male infertility is also a significant factor contributing to difficulties in conceiving. In this article, we will explore the incidence, causes, types, pathophysiology, diagnostic evaluations, and management options for male infertility. Incidence In the year 2023, the incidence of male…
View On WordPress
0 notes
Text
I forget why, but I was on the Wikipedia page for polycystic ovarian syndrome, and I started researching hirsutism in women, and I learned the following things in this order:
there's a diagnostic criteria used to evaluate how hairy a woman is
This is important because being too hairy is a diagnostic criteria of most disorders that cause hyperandrogenism
Disorders that cause hyperandrogenism can be diagnosed by...measuring how hairy you are (this is the main and most important diagnostic criterion for PCOS)
Disorders that cause hyperandrogenism are important because they are correlated with obesity, infertility, and...being too hairy?
I think to myself, wait, what is a normal range for testosterone in women? I find this article...which set reference ranges for "normal" testosterone levels in women...EXCLUDING WOMEN WITH PCOS?
Quote: "Polycystic ovary syndrome (PCOS) is another notable condition in genetic (XX) females, which is characterized by excessive ovarian production of androgens. This condition is included for comparison with DSD, as the affected females with PCOS are genetic and phenotypic females. The elevated levels of testosterone in these females can lead to hyperandrogenism, a clinical disorder characterized variably by hirsutism, acne, male-pattern balding, metabolic disturbances, impaired ovulation and infertility. PCOS is a common condition, affecting 7%-10% of premenopausal women."
So: the study claims to demonstrate a clear distinction between the normal range of hormone levels in "Healthy" men and "healthy" women...with "healthy" being defined in the study as...having hormones within the "normal" range.......................
So I researched what the clinically established "normal" range for testosterone in women is
THERE ISN'T ONE????
Quote from the above article: "Several different approaches have been used to define endocrine disorders. The statistical approach establishes the lower and the upper limits of hormone concentrations solely on the basis of the statistical distribution of hormone levels in a healthy reference population. As an illustration, hypo- and hypercalcemia have been defined on the basis of the statistical distribution of serum calcium concentrations. Using this approach, androgen deficiency could be defined as the occurrence of serum testosterone levels that are below the 97.5th percentile of testosterone levels in healthy population of young men. A second approach is to use a threshold hormone concentration below or above which there is high risk of developing adverse health outcomes. This approach has been used to define osteoporosis and hypercholesterolemia. However, we do not know with certainty the thresholds of testosterone levels which are associated with adverse health outcomes."
What the fuck?
What the fuck?
It's batshit crazy to make a diagnostic criteria for medical disorders by placing arbitrary cutoffs within 2-5% of either end of a statistical distribution. What the actual fuck?
"The results came back, you have Statistical Outlier Disease." "What treatments are available?" "Well, first, we recommend dietary change. You should probably stop eating so many spiders."
Another article which attempted to do this
Quote: "Subjects with signs of hirsutism or with a personal history of diabetes or hypertension, or a family history of polycystic ovarian syndrome (PCOS) were excluded."
"We're going to figure out the typical range of testosterone levels that occur in women! First, we're going to exclude all the women that are too hairy from the study. I am very good at science."
Anyway I got off topic but there are apparently race-specific diagnostic tools for "hirsutism." That's kinda weird on its own but when I looked more into this in relation to race I found this article that straight-up uses the term "mongoloid"
19K notes
·
View notes
Text
0 notes
Text
Best Thing I’ll Ever Do - Lio x Savannah (Part 3)

A/N: This chapter really encompasses a lot of what you all wanted to see with Lio and Sav in this part! I am really loving the way Lio is showing up for Savannah in these parts. I just... the way he has grown, both for her and himself... it's beautiful! Courageous! Aspirational! We love you, Lee 🥰
Word Count: 4.7k
Trigger Warnings: infertility, mentions of blood, pregnancy/birth
Part 1 | Part 2| Part 4 |
Inside a bright room atop a Manhattan skyscraper, Savannah delicately arranges the ‘Oh Baby!’ sign hanging down the gorgeous, flower wall filled with roses. The wall is fake flowers, but looks so real, Savannah didn’t believe they were fake until she ran her fingers over them. The flowers are dotted with the theme of the day which is delicate little butterflies, just like the baby they are celebrating today.
Baby Girl Wood #2 is due in 6 short weeks. Or long depending on which one of her parents you’re talking to.
“My ankles are already swelling up.” Lucie complains from where she is sitting at the bar, sipping on a strawberry lemonade. She extends her legs out in front of her, baby pink skirt hitting just below her knees. She evaluates each ankle while sipping consistently from her straw. “Oh! She loves sugar.” Lucie chuckles, rubbing over her rounded belly where the baby presumably moves.
Savannah glances over, throwing a sweet smile as Lexi pats her daughter’s shoulder comfortingly. Behind them, Mack, the hostess of the baby shower, is adjusting the little gift bags on the table by the door, making sure they are all aligned and in place.
“Soph did too. Would practically punch through my skin when I had lemonade.”
“I can’t relate. Lio was always fighting people in my belly, I swear.” Emma adds in her two cents. Savannah smirks, turning to call towards her.
“So his punching people started young?”
“Ha!” Emma points at her future daughter-in-law. “Yes. I’m sorry.” She cringes. “I tried. Too much of his dad in him.” Emma pauses, looking over Savannah’s work. “Wow, that looks so real. I am in love with the butterfly touch. That was a great idea!” Emma walks over, inspecting it up close as Savannah steps back to be in line with her.
“Thank you! I am satisfied.” Savannah confirms, crossing her arms over her chest while continuing to look with critical eyes.
“Perfect.” Emma murmurs, then wraps an arm around Savannah’s upper back. “How are you?” Savannah turns, meeting Emma’s eyes. She can tell Lio and his mother spoke this morning. How much of her recent struggles Lio shared with her, Savannah isn’t sure. But nothing has been easy since Connor and Lucie told them they were expecting a baby.
The heartache and immutable circumstances Savannah thought she had come to terms with no longer felt resolved. It was easy to say this was all okay, but being thrust into a pregnancy journey with someone they are so close with has changed everything. Some days, it takes everything for Savannah to get out of bed. The mere act of existing weighs on her. Lio has been so patient and understanding. Savannah isn’t sure how she is going to get out of this funk. It’s never gripped her this hard before. But she has also never loved anyone as much as she loves Lio, or planned a life with someone to this extent.
Every step closer they take towards forever- the wedding, the honeymoon, discussing if they are going to move- it all seems like a magnifier on this gaping hole Savanna has eating through the ventricles of her heart. She loathes herself for reverting back into old habits- retreating within, staying out of the house longer to avoid Lio, and the negative self-talk when she sees mothers with their children. It’s all so immature. She should be past this by now.
In an act of asserting willpower and taking back control, Savannah offered to help Mack plan the baby shower. Emma had been helping, but stepped aside when Savannah offered her time and creative mind. Getting immersed in the world of Pinterest and all the different options for showers had been surprisingly therapeutic as long as Savannah ignored the reason for the party.
This morning, when she woke up and Lio mentioned it sounded like Connor and Lucie settled in on a name for their baby, everything shattered inside Savannah again. She hit the wood floor, collapsing under the crushing weight of knowing she will never have this moment. She will never be able to understand what it's like to have people celebrate her pregnancy. Though she has faced this thought before today, it reopens the wound every moment she remembers.
“I’m good.” Savannah assures Emma, leaning in to hug her soon to be mother in law. Emma squeezes her back hard, fully like a mama does, and it takes several calming breaths before Savannah is sure she won’t cry from the sweetness. She cannot wait to officially join the Meier family. She is hitting the jackpot with Lio’s family.
Not long after the flower wall is completed, guests begin to arrive. The list consists of mostly family, a few of Lucie’s college friends, and the Rangers WAGS. They all arrive together as a group, descending into the room like gorgeous runway models. Savannah smiles when they see her, offering a wave. The group grabs various drinks, then comes over to where Savannah is standing by the table of quick shower games.
“Hi Savannah!” One of them, Whitney, exclaims. The two women hug, then she is introduced to the other three women: Gianna, Crystal, and Kyra. Whitney and Savannah know each other from a few mutual friends, Lucie included.
“Nice to meet you.”
“Savannah is engaged to Lucie’s cousin, Lio. He plays for the Devils.” Whitney fills in for the group.
“Oh! I know!” Kyra giggles. “ I love your content on TikTok.”
“Oh god. Thanks!” Savannah starts to blush. While she loves creating content, she feels a little awkward when she sees someone in the wild who has seen her stuff. It feels like the other person knows so much about her and she knows nothing about them. Like a one-sided relationship Savannah never knew she entered into.
“Congratulations on your engagement!” Gianna notes Savannah’s ring. “It was recent?”
“Thank you! Yes, not long ago.” Savannah switches her glass to the other hand so she can extend her fingers out to show off her huge, square cut engagement ring. “It’ll do.” The girls laugh.
“So, when is the wedding?”
“Next summer, we are planning on July.”
“Here?” Whitney asks.
“Yes! We finally decided on getting married here in the U.S. We were going back and forth on different places in Europe, but with the unknowns of the hockey season, it felt safer to plan for here. You know cause the cup.”
“One day our lives won’t revolve around a silver cup.” Whitney jokes.
“Keep dreaming. They never stop talking about it, girls. Even after they win it.” Lexi says as she walks past towards Mack by the windows. The girls laugh at the former captain’s wife.
“Well soak it up! It won’t be long before everyone transitions into baby discussions. Unless you already have them?” Crystal comments.
“Oh no, we don’t and won’t have any.” Savannah clears the air. The silence that falls over the wives is awkward immediately. Savannah chews on her bottom lip for a moment, then takes a sip of her mimosa.
“That’s nice. Kids are… so much work.” Gianna says assuringly. “You’ll be able to travel and do so much more without them.”
“Yeah.” Savannah nods, swallowing hard. All these things she gets to do that she would trade in a heartbeat for a baby. “That will be nice.” She smiles weakly.
“And you’ll actually get to sleep at night. No late night feedings or changes or just the non-stop screaming. Unlike this girl.” Crystal murmurs, grabbing at Lucie’s forearm as she walks up to the group.
“What about me?”
“We were just telling Savannah that not having kids is the right choice.” Lucie’s face drops in utter horror. She looks over at Savannah so apologetically.
“Some things aren’t a choice.” Lucie snaps, glaring at her shower guest.
“It’s okay, Luc.” Savannah interjects immediately. The group of girls fall into confused silence. “I actually can’t have kids. I would if I could.” Savannah nods as she speaks, waving her hands awkwardly as she explains.
“Oh my god, I am so sorry.” Crystal closes her eyes and shakes her head immediately. “I should not have assumed.”
“Probably not.” Lucie mumbles, clearly annoyed.
“It’s okay. Seriously, I’m fine.” Savannah plays it off to the group.
But after that, the party isn’t the same. Even after Lucie walks Savannah to a private corner to check in on her.
“This is your party. Stop worrying about me! I am fine. I’m having a great time and I am hating how much of this is feeling like it’s about me. It’s about you and this perfect butterfly who is joining us soon.”
“Sav, I love you and I know you’re struggling, even if Lio keeps trying to shield your pain from the world.” Lucie sighs. “You know you can talk to me?”
“Yes.” Savannah nods. But they both know why she won’t. Lucie is currently pushing it’s little feet out of her ribs.
At the end of the shower, Connor and Stella Wood pop in as the guests are starting to disperse. Stella bolts in, attaching to Mack’s waist immediately.
“I saw Uncle Davey!” She announces.
“You did!? Did you keep him in line?”
“Um, well he tried to eat my pancakes, so I stabbed him with the fork.”
“Oh…” Mack hides her hand to laugh. “How did that go?”
“Not good. I had to go to timeout.”
“They shouldn’t be giving us another baby.” Lucie jokes.
“Who is this they?” Mack asks her sister. “Y’all know what you did.”
“And I enjoyed it. Ready for more of it this weekend.” She grins at her husband who chuckles.
“Plenty of it.” He says into her hair. “You ready? I got the car packed, bags are in there. Got Stella’s here for her adventure.” He holds up her purple duffle bag. Lucie and Connor are heading to the coast for a baby moon while Lio and Savannah take Stella for the next few days.
“Where is my pillow!?” She shrieks, running away from Mack to her dad.
“In here. I put it on top.” He assures her.
“Okay. Where is Uncle Lee?”
“He is at home waiting for us.” Savannah assures her.
“Let’s go then.”
“Stella. Patience.” Connor snips a bit at her, clearly annoyed with her attitude. Him and Lucie share a look. His wife chuckles, then wraps an around around his waist.
“Okay, Stell, we are going to go. You’re in the best of hands this weekend, so please be kind and respectful and listen to the adults, okay?”
“Okay. I love you!” She bounces up on her tip toes, puckering her small lips for a smooch from both her parents.
“I love you.” Lucie responds.
“Love you, bug. Be good. We will see you on Tuesday.”
“Yeah.” Stella nods, then swallows hard. She grips Savannah’s hand tightly which makes Sav’s heart beat stronger in her chest. Stella and her are in a great place now. It was touch and go in the beginning but the little girl has begun to cling to her just like she does to Lio. It’s the ultimate sign of love from a five year old.
Lucie and Connor pass around hugs and appreciation to the remaining family members, then walk hand in hand to the elevator to begin their long awaited baby moon. Savannah looks down at Stella’s hand still resting in hers.
“Should we go see what Uncle Lee is up to?” Savannah asks.
Stella grins up at her, ready to rush across town to see her favorite person in the world.
- - -
(Lio)
The sound of the quiet crowd clapping at the Yankees game filters to Lio’s ears as he lightly dozes on his couch. Savannah is on her way back to their apartment with Stella and he is taking the last few moments of quiet to his full advantage. He pops one eye open when the crowd cheers exceedingly loud. A double. Nice. He scratches at an itch on his nose, then crosses his arms over his chest, wiggling deeper into the couch cushions.
A faint whine is heard from the hallway. It grows increasingly louder until he recognizes Stella’s sobs. Lio bolts up, rushing over to the door to open it. His eyebrows raise in surprise when he sees his fiancé on the other side of the door. Stella is propped on her hip as Savannah is loaded down with various different bags.
“Whoa.” He says as he takes note of the tears streaking the makeup off her cheeks. “What is going on?”
“Help me.” Savannah snaps.
“Okay.” He reaches for Stella, taking her into his chest. The little girl presses her wet cheek into his shoulder, hot puffs of hair hitting his neck with each cry.
“Ow.” She whines to him. “Ow!” She yells harder when he doesn’t react.
“Okay, Stella is hurt. Are you hurt?” He asks Savannah.
“No. Just.. she skinned her knees.”
“Okay.” Lio grabs the bags from her left hand, ushering her into the apartment completely. “What happened?”
“I don’t know what to do with children! That’s what happened!” She throws the remaining bags in her hands to the couch, then rushes from the room. Lio stares at her in confusion. The bedroom door shuts hard and loud, making both Stella and Lio jump.
“Uncle Lee, she’s mad at me! I said I was sorry!”
“Let’s look at you.” Lio says, putting her on the counter. He looks down at her knees, seeing both of them have been skinned down a bit. The left one has dots of blood in it while the other one has red dribbling down her calf. Stella looks down at them with him.
“Look at it.”
“Yeah. That’s not fun. But I think you’ll live.” He assures her. He scoops her back up, carrying her to the bathroom where he can work on cleaning them up. He sets her on the closed toilet, then kneels down at her knees. He wets a washcloth, carefully dabbing at them with the warm cloth.
“No, no, no, no!” Stella says, pushing his hands.
“Stell, I have to clean it. Those streets are nasty.” Lio sighs, trying to reason with her.
“I want daddy to do it!” She says, bouncing anxiously and kicking her feet.
“How about I do this and we pick out a really cool BandAid from the Disney pack Auntie got you?” He suggests. Stella contemplates. “I bet Mulan is in there.” Stella grins.
“Yessss!” She holds her legs out for him, allowing him to clean them off.
“How did this happen?” He asks her, careful of her sensitive skin. He works the soft cloth over her scrapes, pressing through even as he hates her little whimpers.
“Um, well…” She trails off, looking towards the sky. Lio knows a guilty Stella when he sees one.
“You didn’t listen?”
“Yeah.” She sighs, like such circumstances were beyond her control.
“We talked about this.”
“Well, I wanted to go into the M&M store! My mama was supposed to take me this week and she didn’t because of my stupid baby sister that makes her feel icky and then Auntie Sav said we could go in after the shower! But, but, then she walked by and I wanted to go back and she said no.”
“And you did what?” Stella pauses, mashing her little lips together nervously. She doesn’t want to say. “Stella.”
“I ran away.”
“Stella Wood.” Lio gets stern, dropping the washcloth down to his side. “That is not okay.”
“I-”
“No. You need to listen. To your parents, to me, and to your auntie, especially when you’re out in public. She promised your mama and daddy that she would take care of you. She can’t do that if you aren’t behaving or using your listening ears.” A nasty scowl drops Stella’s eyebrows and lower lip. “You hear me?” His blue eyes pin her in place. She nods reluctantly. “When we are done here, you’re going to apologize to Auntie Sav.”
“But she said I could go and then didn’t take me! That’s not fair!”
“You are 4 years old-”
“-I’m almost five!-”
“Okay, you’re proving my point more. You are almost five years old and I know you understand the rules. You do not get to disobey adult decisions. You had no idea what was happening. Maybe she was trying to protect you from something. Maybe she wasn’t feeling well. Maybe she had a better idea planned for you here at home. But it shouldn’t matter. You need to listen and be respectful of your caretakers.” Stella drops her gaze. Lio looks down at her brown curls, sighing heavily. “Stell, do you understand?”
“Yes.”
“Good. Now pick out your bandaids.” He encourages her, holding open the box for her. She picks an Olaf and an Elsa bandaid because there were in fact ZERO Mulan bandaids, which she was sure to point out. Then Lio got her situated on the couch with a movie and an apple juice box before he headed down to Savannah.
“Hey.” He calls as he walks in. She is on her side, curled up on top of their comforter. Her head rests on her arm with the opposite hand palm up under her cheek.
“Hi.”
“I talked to Stell.”
“I overreacted.” Savannah sighs.
“She shouldn't have run off.”
“Yeah. But I did tell her we could go into the M & M store and I was... struggling, so when we got there, I couldn’t stand another second of being out in public. That’s not her fault. Should she have run off? No, but it was an all around fail by me.”
“What’s wrong? Was.. did something happen at the party?”
“You mean did all the Rangers girls look at me like what’s wrong with her when I said we didn’t have kids and weren't going to?” Lio’s eyebrows furrow together angrily.
“What the fuck?”
“It wasn’t intentional, and no it wasn’t all of them, but it felt like it at that moment. Then I just wanted to leave and there was so much of the party left. I kept having to pretend everything was fine and your mom was being so sweet, but also kept coming up and checking in on me and it was all too much.” Lio encourages her to roll onto her back so he can look down in her face. She stares blankly back at him, almost unfeeling and disassociated from the moment. He runs his hand up her thigh to rest on her stomach. Savannah weaves their fingers together there. “Is she okay? I didn’t really get a good look but it looked like minor scrapes.”
“She’ll live. She’s got cool bandaids and apple juice.” Savannah tries for a small smile. She plays with his fingers while he looks her over more.
“Guess Mother Nature knew I would be a shit mom and made it so I couldn’t be.”
“Don’t say that.” Lio responds quietly. “I’m not okay with you talking about yourself like that. I don’t like it. You had an off day, babe. That’s it.”
Savannah doesn’t respond, but she tilts the corners of her mouth up at him in agreement. The worry in Lio’s gut continues to grow. He hasn’t seen her like this in a long time, not since Lucie first said she was pregnant. As the days grow closer to Lucie’s upcoming birth, he gets more and more uneasy. Now, with a sassy and defiant Stella in the house, he isn’t sure this is the best fit for his fiance's mental health. He loves Stella. He was really looking forward to this time together, but he needs to support his other girl too.
“Go back to Stell. I’ll be okay.” She whispers.
Lio doesn’t want to go, but Stella unattended in the living room isn’t a long-term solution. He gives her a kiss, cradling her head in his hands before heading back into the living room. Stella is in the same place he left her, juice box tossed onto the other couch cushion, mouth agape as she watches the scene unfold.
“I’ll be right back.” He assures her with a gently pat on the head,
Lio sighs as he steps onto the balcony. He leans on the railing for a minute, taking a breather from the chaos he just came out of. He contemplates what he should do next.
When he has collected himself, he pulls his phone out to make the call.
“You called me not Lucie.” Mack answers the phone.
“Ah.. yeah I meant to call you.” Lio responds.
“... Oh. I figured it was the wrong button or something.”
“No. I need a favor.” Lio says, shooting straight with her immediately. This is how they are.
“Kay.”
“I need you to take over watching Stella.”
Loud silence comes over the phone line.
“David and I had plans that did not involve children.” A hint of annoyance is in her voice. He supposes he doesn’t blame her. He has bailed on commitments in the past. No one has been slower on accepting the changed version of Lio than Mackenzie Hischier. She’s not a forget and forgive kinda girl. He respects that about her.
“Yeah, I’m sorry about that, but Sav isn’t okay. I need to focus on her right now.”
“Okay. I’ll send David to come get her. She loves his truck.”
Lio smiles at the way Mack doesn’t press further and the annoyance has dropped completely. Lucie would be all “mama” with him and ask a million questions, already on her way over trying to fix everything. Not Mack. As long as you give her enough information to make a decision, she takes over with whatever is needed.
“Thank you.” Lio murmurs, closing his eyes in relief. “Sorry to ruin your plans.”
“No problem.” Mack pauses. “Are… you okay?”
“Ahm, yeah.” Lio clears his throat. “Yeah.” He repeats more firmly.
“Okay. David should be back from his run soon. I’ll send him over after his shower. Are you calling Lucie or am I?”
“I’ll call her. Thank you.”
“Yep. Bye.” Mack clicks off first. Lio chuckles. Now to break the news to Stella.
Stella takes it well, especially when she hears about Uncle Davey coming to pick her up, but Lucie on the other hand is as concerned as he knew she would be.
“What’s wrong with Sav? Should we come home?”
“No. I’m taking care of everything, but your daughter has this idea that I should entertain her at all times. I can’t do that and do what I need to for Sav.” Lio speaks to the phone while packing up Stella’s suitcase that was already strewn all about their guest room.
“Fair.” Lucie agrees then blows out a heavy sigh. “She just loves you.”
“I know. And I love her. But she has other people here who will take care of her.”
“Mack won’t do the bedtime routine though.” Lucie grumbles.
“I guess I should tell you I don’t either.”
“Lio!” Lucie yells.
“Lu, what you do at your house is your business, but that is too many steps for me. She gets into pajamas, brushes her teeth and by the time I'm shutting the book she is out. That’s it.”
“How is Lio Meier of all people better at bedtime than me?”
“Because you have always made things complicated.” Lio says, flipping the suitcase shut again and zipping it up. “Like this conversation.”
“Wow.” Lucie snips. “Okay, well sounds like you all have it figured out. I’ll check in with Mack tonight.”
“Alright. Have a good rest of your trip.” Lio places the small suitcase on its wheels, shoving it towards the door.
“Lee?” Lucie pauses.
“Yeah.”
“I asked Sav if it was okay for her to help with the shower, and for you to watch Stell. I hope I didn’t overstep somehow. I would never want something I did to hurt her.”
“No, Luc, you didn’t do anything wrong. She wanted to help with these things. But she is struggling more than I think she even realizes.”
“Okay.” Lucie responds. Her voice drips with sadness, clearly concerned for her friend. “I feel really bad.”
“It’s okay. You can’t fix this.”
“Neither can you.” She reminds him. He juts his lower jaw out in disagreement.
That’s her opinion. He is still gonna try like hell to.
- - -
Winnie Wood came into the world in a chaotic c-section on a rainy, September morning. Stella had arrived at Lio and Savannah’s the previous night when Lucie’s contractions started picking up. Despite being put to bed in the guest room, Stella ended up in bed with the adults and none of them slept well after that. Lio has no idea how Connor and Lucie can stand to sleep with her and her flailing limbs on a regular basis.
Next to him, Savannah rests her temple on the steel of the elevator. They ride up to their place the same way they rode in the car home from the hospital: silent. Stella has been dropped with all her grandparents for dinner tonight and will be back at their apartment later tonight, then home tomorrow to sleep in her own bed with a new baby sister.
Lio glances over at Savannah as the elevator pauses on their floor.
“Babe?” He calls to her when she doesn’t move to get out. She startles, clearly lost in another world.
“Oh sorry.” She sniffs, then walks out past him. He reaches for her shoulder from behind, wanting to pull her back into him to comfort her. Instead, she shrugs his touch off. That hurts.
He sighs as silently as he can, then waits next to her as she unlocks the door. She walks in, heading immediately towards their bedroom. She abruptly stops before going in, a loud suffering sob coming from her lips.
“Lio, I’m not okay.” Savannah hiccups from the doorway. Lio rushes forward quickly to hold her.
“I know, baby. It’s okay that you’re not.” He grabs her hand, gently encouraging her fully into his chest. She weakly grips his hand back, blinking her tears down her cheeks.
“Oh fuck I’m so sad.” She wails, curling over at the waist. “I’m never gonna have that. I’m never going to know what it feels like to hold my baby in my arms.” She starts to cry so hard that no noise comes out of her. Lio wraps an arm around her waist, holding her up until he can guide her safely to the floor. The bed is less than ten feet away but he knows they won’t make it. He sits down next to her, then encourages her to crawl into his lap. Savannah shoves her face into his shirt, smearing black mascara all over the light blue fabric.
“She already has a baby. Why can’t it be me?” Savannah sobs into Lio’s shoulder.
“Baby it could be you.” Lio murmurs, feeling brave even as she falls apart in his hands.. “There are so many avenues we haven’t tried. We could try surrogacy. Or IVF.” Savannah pulls away, looking at him like he has grown three heads.
“Lee, you don’t want kids.” Her sadness pierces through the room.
“I want whatever you want.” A look of deep sympathy softens over his face.
“No.” Savannah pushes away from his chest, clearly withdrawing from him again. “I’m not doing kids that way. I’m not forcing you into IVF or surrogacy because I want this and you don’t. I’m not going back on our deal. It’s not in our cards.” Her teeth are gritted shut. She wipes her tears away, trying to get her shit back together.
“Babe, I’ll do it for-”
“Please stop.” Savannah whispers, then purses her lips together to stop the sob in her throat. Her eyes close, steady tears flowing down from her closed eyelids. Lio feels his heart crack open again in his chest. For her. For himself. For them and the things they’ll never get to experience together. He would do anything to give this to his wife. He would give up everything they have to give her a baby. But she won’t even let him try.
Heaviness fills the room between them. While she continues to turn inwards, struggling, Lio holds her tighter, gathering up all of her pieces and keeping them together until she can do it again herself.
Read more Lio and Savannah here
32 notes
·
View notes
Photo
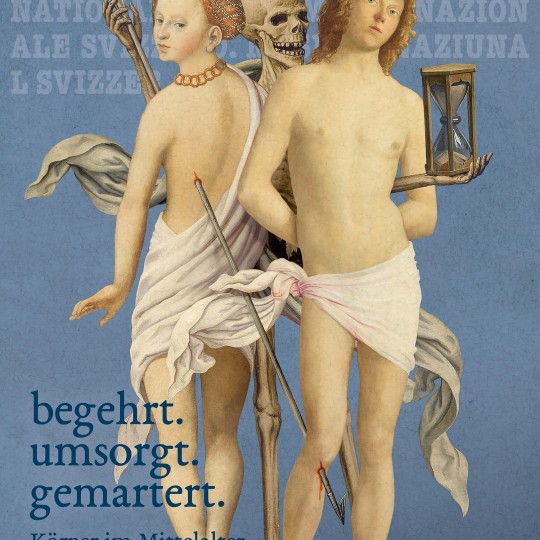
Interview: Bodies in the Middle Ages
In the Middle Ages, attitudes to the human body were rife with contradictions: Glorified, oppressed, cared for, and chastised. A new temporary exhibition at the Swiss National Museum in Zürich – coveted. cared for. martyred. Bodies in the Middle Ages – re-evaluates the ways in which medieval Europeans saw, conceived, and imagined the human body. In this interview, James Blake Wiener questions Curator Christine Keller about the exhibition's finer points.
JBW: Dr. Keller, many thanks for speaking to me on behalf of World History Encyclopedia (WHE).
We tend to think of the Middle Ages as an era dominated by faith. However, we should remember that those living in medieval Europe also participated in secular society and non-religious activities. With that in mind, how did you decide to showcase the rich interplay between physical presence and secular interests and pursuits?
CK: In selecting the themes and exhibits, we have tried to show not only the medieval Church's view but also the secular attitude to the body by means of excerpts from medieval literature – such as erotic novels – profane art, and themes such as sport. We try to show that although the Church propagated certain ideas about physicality (in particular the Christian concept of human sexuality as sin), many testimonies from this period, such as popular erotic literature, reports by secular doctors, and obscene badges in the form of personified genitals, speak a language contrary to church morality.
JBW: While the Catholic Church posited the body as the seat of desire and sin, visual representations of the body of Jesus Christ and the femininity of the Virgin Mary were omnipresent. So too were those body parts that believers worshipped as holy relics, which could heal the sick, bring victory in battle, and cure infertility. What can you tell us about the reliquaries and other objects of devotion on display? What secrets do they reveal about medieval body image?
CK: The exhibition includes a reliquary from Limoges from the late 12th century as well as figurative reliquaries such as busts and arm reliquaries from the 14th and 15th centuries. They bear witness to the great veneration and power of the relics of saints. Figurative reliquaries such as busts, arms, legs or feet bring to life or embody the bones or secondary relics stored in them (such as hair, contact relics, etc.). As so-called 'speaking reliquaries', they thus make the abstract, sacred powers more visible. It is relevant for the medieval image of the body that the relics simultaneously reflect death and life and that the saints venerated in the relics were regarded as mediators between this world and the afterlife. The wooden bust reliquaries from the 14th century (for example the Ursula reliquary) were painted in such a way that the surface appears flesh-like, the eyes animated and alive. In these busts, the saints met the viewer as the 'living dead'.
JBW: Death was an immediate and looming concern to our medieval predecessors. Average lifespans were lower than they are today and disease was rampant. How did the concern of death and the belief in everlasting life – on the day of resurrection – shape conceptions of the body during this era?
CK: Death and mortality were omnipresent and a major topic in the Middle Ages. In view of the resurrection, care was taken during one's lifetime to ensure that one's own life remained as free as possible from sins and vices or that these could be redeemed during one's lifetime. In terms of the body, this meant among other things: no gluttony (gula), no lust (luxuria), no vanity (superbia), no indolence (acedia). The concept of bodily resurrection was characterised by the statements of one of the early Church Fathers, Augustine of Hippo (354-430): according to his interpretation, the physical condition at the time of death was irrelevant for the resurrection. For example, if a dead body was mauled by animals or burned, it still emerged from the grave on the day of resurrection intact and at the age of 30 or 33, the age at which Jesus died. In this sense, depictions of the resurrected show them with their intact, naked bodies.
JBW: It was during the Middle Ages that a number of first steps in public health were undertaken: the practice of quarantine; the establishment of hospitals; and the provisioning of medical care and social assistance. There was, as a consequence, an interest in health, hygiene, and hospice, which is delineated throughout the exhibition. I wondered if you might share with us some details about bathing and cupping during the Middle Ages. I suspect many readers would be surprised to learn how commonplace these and other practices were in actuality.
CK: The medieval theory of health is based on the 'theory of the four humours' and the four elements. If the humours (blood, phlegm, black and yellow bile) are not in balance, the person becomes ill. In order to maintain this balance, an excess of substances must be equalised. Bathing parlours (with sweat baths), cupping, and bloodletting – or the application of leeches – were used for this purpose. Numerous health guides, which were particularly widespread in the late Middle Ages, describe the appropriate time for these methods and use illustrations – the so-called Vein Man – to point out the suitable body parts and the appropriate time for bloodletting. Health care was a major topic throughout the Middle Ages and was widespread.
JBW: Bodies in the Middle Ages underscores that while medieval attitudes to the human form and body were contradictory, much has remained the same across the centuries. Whether through the quest for physical perfection or a preoccupation with health or illness, we are not all that different from our medieval predecessors. What do you hope visitors gain from a visit to the exhibition? Moreover, what would you like the public to learn about the Middle Ages as a result of your work?
CK: A survey in the exhibition revealed that the exhibition on the body in the Middle Ages inspired the majority of our visitors to think about the body in the present day. We hope that with this exhibition we can show a somewhat different view of the Middle Ages and that we can break down the often still prevalent stereotypes of a rigid and anti-body era.
JBW: Dr. Keller, thanks so much for sharing your expertise with our audience. On behalf of World History Encyclopedia, I wish you many happy adventures in research.
coveted. cared for. martyred. Bodies in the Middle Ages runs at the Swiss National Museum in Zürich, Switzerland until July 14, 2024.
Christine Keller is an art historian and curator at the Swiss National Museum.
Continue reading...
30 notes
·
View notes
Note
I'm a little confused about the teaching that it's ok for a couple to use a perforated condom to collect a sperm sample for medical testing (as stated in USCCB's 2020 "Reproductive Technology Evaluation and Treatment of Infertility Guidelines for Catholic Couples"). I assume that even a punctured condom must still reduce the chance of a pregnancy by a little, otherwise it wouldn't collect a sample very well? Isn't reducing the chance of fertilization through the use of a tool like this kinda partially being closed to life? Regular condoms don't have a 100% prevention rate and yet we still condemn them for reducing the chance. I'm also assuming that a couple who does the same behavior but without the intent of keeping a sample for medical testing is doing something faulty. But don't we say that a faulty act cannot be made permissible even with a good intent, like with it still being unacceptable to masturbate to obtain a sperm sample? And I guess I'm confused about the theology handles nitpicks like, how small can the holes be before it's no longer permissible. This isn't like a pressing relevant issue in my life by any means but I'm trying to better understand the logical thinking behind topics in sexual morality! Thanks
The reduced chance of conception in this scenario is so negligible that it is practically non-existent. You honestly need very little sperm to get a woman pregnant; that's why the pull-out method doesn't work as birth control, because even the sperm in the pre-ejaculate is enough to cause conception. To say the amount of sperm a man ejaculates during sex is overkill is an understatement.
Intent doesn't necessarily excuse faulty action, but intent is nonetheless important in determining whether an action was faulty in the first place. Some actions are inherently sinful; others are sinful based on circumstance, means, and intention. Avoidance of conception during sex falls in the latter category. Masturbation falls in the former. (I'm happy to explain why, if you'd like).
I think the problem here is that you assume the issue with condoms are that they reduce conception rates. Which is true, but the moral issue is not the thing itself, but the purpose of its use. The tools themselves are neutral. Using it to collect samples for health evaluations wherein its property for potential barrier to conception has, in all practicality, been rendered harmless, is a licit use of a neutral tool.
FYI, a couple could actually licitly use a condom during sex regularly -- i.e., such a textured one for assisting the wife's pleasure -- if they were to cut the tip off. I don't really see any reason why a couple would regularly use a perforated condom except with the hope of potentially mitigating conception, in which case the intent is clearly sinful (even though it wouldn't work lol).
11 notes
·
View notes
Text


Round 2
Propaganda why Harry Dresden is insufferable:
Sir can you treat women as competent peers and not as damsels you need to protect? Do you have to comment on the attractiveness of every woman you meet?
This man's lower head is doing the thinking far more often the his upper head for at least half of his page time, yet as insufferable as THAT is, Harry also manages to make the situation exponentially worse by annoying the women around him with obnoxiously performative chivalry (that some of them expressly reject, which does not stop him.) It's the white knighting that drives me nuts, it's so condescending.
Basically everything bad that happens to him and those around him is his own fault, but he somehow never learns and just keeps doing things like 'protecting' others by not telling them crucial information. I get that he's CURSED, OH THE HUMANITY, but come on. And he does that annoying male gaze thing where he subconsciously evaluates every female character by attractiveness. Couldn't stand being in his head.
Propaganda why Ted Mosby is insufferable:
He’s so selfish, immature, and annoying. Death!
He's one of those ""nice guys"" who also thinks he's funny and smart when at best he's average at both.
Ted repeatedly chases women who are unattainable. (Stella, etc) and that he is fundamentally incompatible with. (Robin). Especially after Robin finds out she's infertile, it's a big asshole move of him to chase after her knowing that he'll eventully leave for a women that wants to marry and have kids. Ted is pretentions and lacks the moral backbone to go against Barney's bullshit. Ted often chases after women half his age with Barney.
certified Nice Guy syndrome where he's a huge misogynist but acts like he's just a widdle baby....UGH
He tells his kids some really inappropriate things and comes off as annoying even though he is the one narrating the show. Also, he’s only telling the story so his kids will approve of him going after their Aunt Robin
#harry dresden#the dresden files#ted mosby#how i met your mother#insufferable protagonist poll#insufferable protagonist tournament#tournament poll
16 notes
·
View notes
Text
In Quebec, the number of young trans people is increasing, and the lists waiting times for specialized clinics are getting longer. Eight months in Meraki, a year in Sainte-Justine.
"Do you have an appointment with that today?" "With Doctor [Retracted]..." "We'll open your file, if you don't mind. I have a little information, but I'm missing a little."
There is another option: private.
"You see here, there is a sexologist's office, and for $115, we offer a consultation. And at the end of the consultation, we can have a letter of recommendation for hormone therapy. It says it may take a session or two to get the letter. It's private.
We received a message from a mother, who told us that [her] daughter told her about that doctor."
This general practitioner sees the patient and prescribes, without referral from another healthcare professional. The clinic is private. It is the patient who pays.
This is where we took Sasha back, interpreted by a 14 year old actress.
"Sasha would prefer to go alone, is that correct?" "Yes, yes."
She will tell the doctor that she identifies as trans.
"So, I'll give you this. There is a pencil here. You can go through the document, initial it, or you must sign where you need and everything."
She must read and sign as seven-page form which describes the side effects, sometimes permanent, of testosterone before entering the doctor's office.
This is the first time this doctor has seen the patient. She quickly gets to the heart of the matter.
"You can tell me, a little deep down, since when you know you're not in the right body? Is it in childhood, is it more in puberty?"
Sasha reports that she doesn't like her body and that she was getting vomited at age 12.
"At one point, my mother grabbed me. She took me to see a psychologist. That's when they said I had an eating disorder. I told myself that it couldn't be eating disorders, it didn't make sense in my head. But at 13, I came across a video, of a trans person in fact, who talked about having eating disorders, but in fact it was because she was in the wrong body. At that moment, I really recognized myself in this person."
The doctor then asks if she has the support of [her] parents.
"Your family... did they understand a little of what's going on?" "Yes, they understood a little." "Do they know you're here today?" "Yeah."
Five minutes into the consultation, she addresses the question of surgeries.
"Are you considering surgeries in the future?" "Surgeries?" "Yeah." "Gender?" "Mastect. Mastectomy, removing the chest." "Yeah." "There are other surgeries that exist. We have a uterus, at the bottom with ovaries. So basically, it's possible to remove, it's something that can sometimes cause dysphoria."
Testosterone can make a woman infertile. The subject of fertility is the subject of a question.
"Is fertility, I understand that it is perhaps far away for you at 14, but is fertility something you want to maintain before you start?" "No. I always knew I didn't want children."
And finally, less than nine minutes into the consultation:
"Basically, the logic right now, I still prescribe hormones today in theory. Because the logic is that, basically there is nothing in your balance sheet that would stop me from giving you hormones basically. I'll start at one dose, it's not a mini-dose, like an intermediate dose between adults and..." "... non-binary, let's say." "No problem. The best is yet to come."
The consultation lasted less than 17 minutes. The side effects of testosterone do not have been addressed, which may seem surprising.
Confronted with this fact, the doctor told us that: "... a medical consultation cannot be evaluated in terms of duration, but rather in terms of quality of the exchange of information..."
#Canada#Quebec#medical corruption#medical malpractice#medical scandal#testosterone#cross sex hormones#wrong sex hormones#gender ideology#gender identity ideology#queer theory#intersectional feminism#gender affirming care#gender affirming healthcare#gender affirmation#religion is a mental illness
14 notes
·
View notes
Text
Being Trans, Heterosexual and Dating.
Here is some dating advice:
1. Give your love interest time to get to know you. It does not make you a liar to get to know someone before confiding in genital talk. Your safety is the most important so its best to "feel out" (get to know) your love interest before you make your move. When I was actively dating with intent to find a wife, I used to tell the girl after the second date. That way I figured they'd see if they liked me enough to get past my genitals, but I did face rejection. However, rejection is a part of the dating process. Which leads to my next point of advice;
2. Know your worth. You deserve respect, consideration, and love. There will be people who try to play on insecurities like; feeling undateable. I had many interactions where women would use that insecurity of mine to try to pressure me into whatever agenda at the time. If someone who claims to love you is weaponizing you being trans, don't take it lightly and be sure to really evaluate what's happening.
3. Not everyone is the same. I have also met plenty of women who do not care what's in my pants. Women that liked me for me. I found that building a relationship with romantic expectations revealed, can make a great relationship. Some find safety and acceptance in developing relationships with other LGBTQ+ members; my experience is that not all members are accepting. Treat everyone as their own person. My wife is bisexual but that doesn't mean that all bisexual people are the same level of accepting a romantic relationship.
Now let's talk about after surgery. You don't have to tell anyone, I would also say you are infertile as well just as a point if that time were to come (kids). But let's get personal here. If you meet a woman who is everything you want and more, if she ever were to find out from another source but you, it could jeopardize your relationship, especially the longer two have been together, because she may see that as you lied to her and weren't honest and upfront. At some point it is better to be honest with someone it's also nice to have someone in your corner.
If you have that gut feeling you can't tell this person, that might not be the person for you.
There's lot of fish in the sea, I'm sure you'll clean up!
Good luck Anon and anyone else wondering about being trans and dating heterosexually.
- Zestual
If you have any questions or I missed something please feel free to reach out to me again!
P.s I told my wife early into our relationship. She was so nice and kind. She actually forgets I'm trans 99.9999% of the time. It's something that doesn't come up unless I basically bring it up. So you won't have to carry the trans label with you forever if that's your goal. You have this! You have lots of time to figure this all out.
#being ftm and dating heterosexually#being trans and dating straight#ftm and dating heterosexually#ftm and dating women#transgender#trans ftm#ftm transition#transman#ask me things#lgbtq#ftm dating straight women#ftm and heterosexually
8 notes
·
View notes
Text
This is so totally not to do with fallout but I wanted to talk about this personal thing and maybe i dunno? See if anyone can provide advice? Vent??? (under the cut, CW: prescription drug dependency, opiates, ketamine, drug rehab and detox, pregnancy, IVF, infertility, family planning, reproductive health.)
Right so getting personal here but I've hit a point where I cannot afford to put off having kids anymore. I have always, always wanted to be a parent, but I have the triple whammy of PCOS, adenomyosis and endometriosis and my husband and I have been trying to get pregnant since... I've lost track, but it was before we even got married. I'd say we're closing in on around 4 or 5 years now and we've been together for 8 years.
We've been to several fertility specialists and my issue is that I just don't ovulate like I should. Everything else is fine -- thankfully my uterine tissue is fine despite the adeno, and we've surgically got my endo under control, but PCOS means I just don't drop eggs like I'm meant to. (Although, recently, I've like, shed weight thanks to my new ADHD medication which has overcome my insulin resistance and I ovulated last month! So who knows?)
Anyway, all this to say that I'm running out of time now and we're going to start the IVF process next year. Thankfully my odds are extremely good and (touch wood) we're likely to get lucky quickly. IVF is invasive and expensive and I am terrified but I figure I'm gonna go through birth eventually, right? May as well get scared early and get used to it. (When I say IVF is invasive I mean we went through a cycle once before and it was so traumatising to me despite everything going fine that it inspired me to write Embryology, which is a body-horror fic lmao.)
However,
These medical conditions also cause me a lot of pain. Like, a lot, chronically. I have been in pain since I was 12 and started getting periods and I've been on opiates (legally and under medical supervision) for well, well over a decade. They're awesome, they have improved my quality of life drastically. I'm able to walk my dog, go to the grocery store, hold down a job and go to the gym every second day -- which I couldn't without them.
I don't abuse my opiates. I see my doctor once a month and see a pain management specialist annually to evaluate my pain and the best way to treat it and how I'm going, which is required before you can get the kind of prescription I have in my country (this is also overseen by the government, who provide my doctor with a permit after assessments that allow them to prescribe me) I have never had a dose increase and they're totally happy with my use. I am 100% aware that opiates are scary and dangerous and cause a lot of heartache for people but I assure you that in my case it is responsibly managed and safe.
The issue, though, is that I'm getting pregnant (hopefully) next year. This means that before I undergo my first IVF cycle, I have to go off opiates. Psychologically, I'm fine with this. I want a baby more than I want opiates, and thankfully, it's almost guaranteed that pregnancy will actually stop my pain as endo and adeno pain has, as we've seen in studies, always responded well to pregnancy for the duration of it.
But physically? I have an opiate dependency. This is the physical response to withdrawal of a drug, and it happens with any drug. (There's a lot of things that your body with develop a chemical reliance on in some way that aren't drugs, too!) It's nothing to be ashamed of and I'm not ashamed of it at all.
There's no way around it, even if I am not psychologically dependant on opiates and have no history of abuse or misuse, my body is a different story and I am going to have to go through a detox stage. In a lot of parts of the world including the western world, this is done through a weening process or by swapping whatever opiate a person is using to a more controlled substance like Suboxone (which I am avoiding) and then weening off the 'safer,' controlled, replacement opiate instead.
This would suck. If you've never had opiate withdrawls, imagine you have the worst flu ever -- no cough or fever, but you feel like you have a fever. You get a runny nose and sore throat, you get congested, your eyes start to burn, your skin starts to sting, your joints hurt. You sweat through your clothes and sheets at night and during the day you feel like you have a fever even if you don't have one. Oh, and the shitting. You don't stop shitting. It starts as run of the mill diahhoreah and then turns into water. You eat, get debilitating stomach and digestive tract pain as the food works its way through you and then it comes out two hours later as water. It's never ending. You shit oil after a while. If you didn't have TMJ beforehand, withdrawals will give you TMJ. Your teeth will hurt and, to top it off, opiate withdrawals cause insomnia. Even once you pass out from exhaustion from shitting for 8 hours straight, you will wake up every five minutes and go into a cycle of 'wake up,' 'stay awake for give minutes,' 'pass out from exhaustion again,' 'wake up five minutes later.' You cannot sit still. It is pure agony.
This would take months. I would be physically unwell the whole time, being that sick for that long would probably fuck with my mental health, and even once it's out of my system -- a lot of the time, your brain matter never forgets opiates. You can be fine for years and then see something and your neurons will involuntarily fire off and your opioid receptors will start SCREAMING for opiates.
However, I'm really, extremely lucky and ketamine treatment is being offered in my country for detox and rehabilitation from opiates!
This means that instead of the agonizing weening process that can take months and even years in cases worse than mine, I spend a week in hospital under medical supervision with a constant drip of ketamine until I've fully detoxed. Ketamine is actually a really incredible drug when it comes to medical uses (I already have a prescription for something called a troche, which is a microdose that you dissolve in your mouth. I use it for when I have a cyst burst and need immediate pain relief while my other medication kicks in.) It's not just used as an analgesic or anaesthetic anymore and you've probably read about it being used to treat PTSD or treatment resistant depression. (I can definitely attest that my mood as someone with bipolar disorder and PTSD has been the most stable it's ever been since starting to use it, which is a side bonus.)
There's a lot of studies and evidence that ketamine actually re-sets or re-wires your brain's pathways, which is why opioid infusions are used for chronic neuropathic pain a lot. The idea is that a long and low dose of ketamine is delivered with a pump at regular intervals around the clock so you basically spend a full week or so having your brain's pathways re-programmed and your opiate receptors renovated.
This means that I'll both be made comfortable during withdrawal (ketamine is shown to lessen the neuropathic and painful withdrawal symptoms, but as I'm in a hospital with nurses who are specifically trained to handle withdrawal cases, I'll also be given supporting medication for the diarrhea, restlessness etc) but it'll give my brain somewhat of a clean slate, meaning I should (fingers crossed) be able to live the rest of my life without feeling random cravings.
The biggest benefit to this is that it should re-wire my brain's pain pathways (which are worn the fuck out from feeling pain for decades -- think of it like having an ass groove in a couch and picking up the cushion and beating the shit out of it until the groove is gone,) meaning that my body may feel my usual pain as lesser and that regular pain medication like ibuprofen or tylenol (panadol for us Australians) will have a far better chance of working as well on my brain as opiates do, just without the buzz.
So it's a slam dunk win and I'm absolutely taking it, but a week on ketamine is still scary. During infusions, they start you on a microdose and then work your dosage up until they work out what your limit is before you venture into a k-hole and then reduce it to the highest level they can give you without sending you to space, but it's still going to be enough that I will experience some psychedelic effects and hallucinations.
I'll be safe and cared for but given that I do have some trauma I'm a little frightened. My specialist has warned me that it might bring that up in ways I won't expect and I might get a bit distressed at times and even feel a little mentally freaked out -- which is all normal because I'm on fucking ketamine duh -- but that's still a terrifying prospect, to have to do that for an entire week.
My long term plan is that once I have this baby, I'm getting a hysterectomy as we're pretty confident that most of my pain comes from my adenomyosis, which should make it manageable afterwards, even without opiates. I have something of a light at the end of the tunnel and it's, hopefully opiate free, and that sounds nice. Not that I have a problem with opiates -- honestly, if I could stay on them forever I would because they let me live a life and I love that peace of mind knowing it's there if I get hit with debilitating pain again. But the stigma and judgement around it and the way unfamiliar doctors and nurses treat me when they find out I take opiates (even with a prescription and all that supervision and all those safety checks!) is just awful, and the way people choose to see me because of legal medication I take -- I'm refused treatment for unrelated things so often because doctors see that on my medication list and assume I'm drug seeking. HUGE CN HERE for pregnancy loss - I miscarried in a hospital waiting room once after waiting in there for 6 hours without being seen because the triage nurse decided that I was trying to get more opiates and didn't even put my details in the system, meaning that no one was ever going to come see me anyway! I want to get off them and be free of that judgement and be treated like a human being again!
But I dunno. I guess I'm just scared that I'm gonna go through like, a trauma trip for a week and then just wind up back on opiates in two years and have to keep living a life where I'm treated as less deserving of respect or dignity because of something that's just... well, it's wrong to treat people like that, even if they do abuse their medication or use street opiates, anyway. The medical system is just callous and cruel.
Anyway, the reading I've done suggests bringing comforting things to do or watch during your stay, and I know I'm looking 12 months ahead (which is the plan at the moment) but I'm trying to figure out what that is in case I want to save for something like a new laptop or even a steam deck to play comfort games (simple stuff like stardew valley, easy, calm things) and watch easy viewing stuff?? idk. This is weird.
3 notes
·
View notes
Text
Choosing The Best Infertility Centers In Hyderabad: Factors To Consider

Introduction
Infertility can be a challenging journey, but finding the right infertility center can make all the difference. In Hyderabad, several infertility centers offer a range of services to help individuals and couples overcome fertility issues. However, choosing the best center requires careful consideration of various factors. This article explores the key factors to consider when selecting an infertility center in Hyderabad, empowering individuals to make informed decisions about their fertility care.
Reputation and Success Rates
One of the most crucial factors to consider is the reputation and success rates of the infertility center. Research the center's track record, including its success rates for various fertility treatments such as in vitro fertilization (IVF), intrauterine insemination (IUI), and egg freezing. Reading patient testimonials and reviews can also provide insights into the experiences of previous patients and the quality of care provided by the center.
Expertise and Credentials of the Medical Team
The expertise and credentials of the medical team are paramount when choosing an infertility center. Look for centers with board-certified reproductive endocrinologists, fertility specialists, embryologists, and support staff who are highly trained and experienced in treating infertility. Additionally, consider whether the center offers access to other specialists such as urologists, genetic counselors, and mental health professionals to provide comprehensive care.
Top Infertility Specialist at Healix Hospitals
Dr.M.L Avani: MBBS, MS - Obstetrics & Gynaecology
Dr. Avani is an Obstetrician,Gynecologist and Urogynecologist in Madinaguda, Hyderabad and has an experience of 10 years in these fields. Dr. Avani practices at Healix Hospitals in Madinaguda, Hyderabad,Apollo Fertility in Kondapur, Hyderabad and Apollo Fertility in Banjara Hills, Hyderabad. She completed MBBS from Mamata Medical College, Khammam in 2003 and MS - Obstetrics & Gynaecology from Kamineni Institute of Medical Sciences, Narketpally in 2008.
She is a member of Federation of Obstetric and Gynaecological Societies of India (FOGSI). Some of the services provided by the doctor are: Cosmetic labiaplasty,Fertility Treatment,Mini Port Surgeries,Laparoscopic Surgery and Single Port Surgeries etc.
Patient Stories for Dr. Avani
Sai jyothi: I visited Dr. Avani Manam for a fertility consultation and I was very impressed by his professionalism and expertise. He explained the different options and procedures in a clear and respectful way, and answered all my questions patiently. He also gave me realistic expectations and honest advice. I felt comfortable and confident in his care. I would highly recommend him to anyone looking for a fertility specialist.
Rakesh D: Dr. Avani is such a terrific doctor. She is patient and understanding and made us feel like we were heard and not simply another number. She answered all our questions. Dr. Avani is such a great, informed doctor and is well worth it. Our first appointment with her was in 2022, then she was extremely thorough with her diagnosis for us. She provided us with options of what we wanted to continue ahead with. In 2023, my wife is pregnant with 10 weeks now. We are incredibly appreciative and thankful to Dr. Avani. Dr. Avani has been an answer to our prayers. We highly recommend her and if we could give her more than five stars we would definitely.
Source: https://www.practo.com/hyderabad/doctor/avani-1-gynecologist-obstetrician/recommended?specialization=Obstetrician&practice_id=796300
Factors to Consider When Choosing an Infertility Center
1. Expertise of Fertility Specialists
Opting for a center staffed with experienced and board-certified fertility specialists is paramount. Look for professionals with specialized training in reproductive endocrinology and infertility (REI) who demonstrate proficiency in a wide range of fertility treatments and technologies.
2. Range of Services Offered
Evaluate the breadth of services provided by the infertility center, including diagnostic testing, ovulation induction, intrauterine insemination (IUI), IVF, and advanced reproductive techniques such as intracytoplasmic sperm injection (ICSI) and embryo cryopreservation.
3. Success Rates and Patient Outcomes
Review the center's success rates for various fertility treatments, including live birth rates per treatment cycle and pregnancy rates per embryo transfer. Additionally, consider patient testimonials and reviews to gain insights into the overall patient experience and satisfaction.
4. Accreditation and Quality Assurance
Ensure that the infertility center is accredited by reputable organizations such as the Joint Commission International (JCI) or the National Accreditation Board for Hospitals & Healthcare Providers (NABH). Accreditation signifies adherence to stringent quality standards and best practices in patient care.
Do Read: https://www.healixhospitals.com/blogs/choosing-the-best-infertility-centers-in-hyderabad:-factors-to-consider
#Best Infertility Centers in Hyderabad#Top Infertility Centers in Hyderabad#Infertility Centers in Hyderabad#Infertility centers in Hyderabad#Fertility clinics in Hyderabad#Best fertility centers criteria#Hyderabad fertility specialists#Infertility treatment factors#Choosing fertility clinics#Top infertility centers in Hyderabad#Criteria for selecting fertility centers#Infertility clinic services#Evaluating fertility centers#Hyderabad fertility treatment options#Factors in infertility center selection#Assessing infertility clinics#Services offered by fertility centers#Expertise of fertility specialists#Hyderabad infertility treatment criteria#Reputation of infertility centers#Success rates of fertility clinics#Patient reviews of infertility centers#Infertility center accreditation
1 note
·
View note
Text
Hydroxyurea and Sperm Abnormalities in Patients with Sickle Cell Disease by Dr. Salma M. AlDallal in Journal of Clinical Case Reports Medical Images and Health Sciences
ABSTRACT
Hydroxyurea is a key treatment option for patients having sickle cell disease. Although the treatment has been effective in improving the survival rate, new concerns over improving quality of life are forthcoming due to spermatogenesis-related toxicities and teratogenic effects. The available evidence shows that hydroxyurea might exacerbate the existing sperm abnormalities. There is a lack of comprehensive, systemic evidence to demonstrate the precise effects and role of hydroxyurea on sperm abnormalities in patients with sickle cell disease. Patients and healthcare providers require accurate and extensive information on sperm-related toxicities to make informed decisions. Here, I discuss the effects of hydroxyurea (HU) on sperm parameters, clinical study evidence, and treatment options available for fertility preservation in these patients.
Keywords: Sickle cell disease, Hydroxyurea, Sperm abnormalities
INTRODUCTION
Sickle cell disease (SCD) is a group of genetic blood disorders that leads to abnormality in hemoglobin. In patients with SCD, newer medical treatments have improved survival rates and quality of life along with a reduced disease-related morbidity. Consequently, the focus of the treatment is diverging to encompass the reproductive issues associated with these treatments. In adolescents and young patients with SCD, sexual maturation is delayed by 1.5-2 years [1, 2], and approximately 24% of SCD patients may have hypogonadism, infertility, erectile dysfunction, and poor libido [3]. The issues related to fertility and reproductive organs in SCD are either related to disease or to the treatments used to treat SCD-related morbidity.
Reduced SCD-related morbidity has been observed with treatments like hydroxyurea (HU) and hematopoietic stem cell transplantation (HSCT). However, adverse effects and toxicities associated with these therapies are a concern. HU use has been associated with sperm abnormalities and teratogenic effects [4, 5]. However, HU affects rapidly dividing cells, raising concerns about related toxicities. Therefore, it is essential to evaluate if there is an exacerbation of fertility problems in men with SCD. This review summarizes the spermatogenic effects of HU in males with SCD.
Fertility issues in males with SCD
Some of the disease-related fertility issues observed in patients with SCD are hypogonadism, sperm abnormalities, erectile dysfunction, delay in sexual maturation, and abnormal hormone (testosterone, follicle-stimulating hormone (FSH), and luteinizing hormone (LH)) levels.
The sperm abnormality rate is as high as 91% in males with SCD [6]. Although some reports attribute sperm abnormalities to delayed puberty in males with SCD [7], some others attribute it to testicular infarction or hypogonadism. It is also worth noting that sperm abnormalities also exist with normal testosterone, FSH, and LH levels [8].
In addition to sperm abnormalities, the incidence of erectile dysfunction in men with SCD is reported to be 21%–35% [9-11]. Also, a decrease in semen is reported in men with SCD [12]. Laboratory findings show low testosterone levels with variable FSH and LH levels. Moreover, abnormalities in accessory organs like seminal vesicles and prostate glands may be present due to recurrent urinary tract infections. These reproductive issues are exacerbated by therapies like HU, which have therapeutic effects through impairing DNA synthesis.
HU in treatment of SCD
HU is approved for the prevention of vaso-occlusive pain in SCD. HU is a ribonucleotide reductase inhibitor that impairs DNA synthesis due to its S-phase-specific cytotoxic action. It is an antimitotic agent that can impair human spermatogenesis. It is a disease-modifying therapy that decreases episodes of acute pain and acute chest syndrome in SCD patients [13]. The HU therapy increases the fetal haemoglobin, which does not sickle under low oxygen tension. Low-dose HU therapy (10 mg/kg/day) has been effective in improving clinical and hematological parameters, reducing painful crises, and reducing blood transfusion requirements in SCD patients. Although HU has improved the quality of life and survival rate, its use is limited by its toxicities, particularly its effect on fertility parameters.
SCD itself manifests in some abnormalities like spermatogenesis, and seminal fluid, which may be exacerbated with cytotoxic HU therapy. HU is associated with abnormal sperm morphology [14] and a decrease in sperm count [14-16] in patients with SCD. At a therapeutic dose, it has short-lived, irregular cytotoxic effects on dividing cells [4]. Since it is an antimetabolite, it is hypothesized to have a risk of affecting sperm development [4]. These effects are often brief and reversible with discontinuation of the drug administration.
Infertility in Men with SCD
Although HU treatment has improved outcomes in patients with SCD, it has been associated with effects on spermatogenesis and teratogenicity, for example, testicular atrophy, hypogonadism, decreased sperm count, abnormal sperm motility, and abnormal sperm morphology.
Hypogonadism
Male hypogonadism is decreased functional activity of the gonads that results in a testosterone deficiency. Testosterone deficiency can cause infertility, muscle wasting, and the absence of secondary sex characteristics. The mechanism for the cause of hypogonadism may be primary gonadal failure [17-19], repeated testicular infarction [20], zinc deficiency [21, 22], and partial hypothalamic hypogonadism [23].
Abnormal spermatogenesis
Impaired spermatogenesis has been reported in male patients with SCD receiving HU therapy, which leads to testicular atrophy, oligozoospermia (low sperm count), abnormal sperm morphology, and azoospermia (decreased sperm motility) [6, 15, 16, 24-31]. It is yet unclear if the abnormalities directly affect HU therapy. However, some researchers believe that the extent of sperm abnormalities might be associated with the length of HU therapy [29, 30]. Since SCD is a genetic condition manifesting at an early age, the duration of HU therapy remains long.
Abnormal Hormone level
A few studies have reported altered levels of testosterone and dihydrotestosterone, FSH, and LH in patients with SCD [12, 32, 33]. The testosterone levels have a direct effect on fertility [6], reduction in semen volume, sperm count, and motility in sickle cell male patients [10].
Priapism
Priapism is defined as a prolonged and lasting continued penile erection unrelated to sexual interest or stimulation [34]. The prevalence of priapism and erectile dysfunction in patients with SCD is 45% and 30%, respectively [35-37].
Penile erection is regulated by the neurotransmitter nitric oxide (NO). In SCD patients, the bioavailability of NO is decreased, disturbing the relaxation of penile smooth muscle [38, 39]. Also, the adenosine regulation pathway might be contributing to the pathophysiology of priapism in SCD patients.
Studies evaluating the effect of HU therapy on spermatogenesis SCD patients
Several studies have reported the role of HU in the exacerbation of various sperm abnormalities in patients with SCD. A non-interventional study (ESCORT-HU-European Sickle Cell Disease Cohort-Hydroxyurea) evaluated safety, morbidity, and mortality in 422 SCD patients of age 15years and older treated with HU [40, 41]. The study reported 67 pre-treatment and 24 during treatment semen analyses. Before treatment with HU, 49% of sperm analyses were normal, and 25% were abnormal (at least 1 abnormality: sperm mobility, sperm count, appearance). The rate of abnormalities during HU treatment increased to 50%. The abnormalities observed were asthenospermia, hypospermia, oligospermia, azoospermia, and atypical forms. These results confirmed that sperm abnormalities are exacerbated after HU treatment.
A prospective, Phase 4 multicentre study called HYDREP (NCT01609192) assessed the effect of HU treatment in patients with SCD [42]. The study reported a significant and rapid decrease in mean total sperm count from 129.8 million at baseline to 24.1 million at month 6. Furthermore, 86% of patients had an abnormal value of total sperm count at month 6 compared to only 40% at baseline. Researchers also found that 6 months of HU treatment did not affect the semen volume. They reported that the treatment of SCD with HU causes significant abnormality in spermatogenesis. After treatment, the number of men with abnormal total sperm count and cryptozoospermia increased to 30 patients and 5 patients, respectively. Additionally, six patients (17%) became azoospermic, and 19 were oligozoospermic.
An unmatched case-control study in Nigeria compared serum testosterone concentration among 47 patients with hemoglobin phenotype SS and 28 volunteers with hemoglobin phenotype AA [43]. The concentrations of serum testosterone in 44 of 47 hemoglobin phenotype SS patients were significantly lower as compared to 7 of 28 volunteers with hemoglobin phenotype AA.
A group of researchers evaluated the effect of long-term HU treatment from childhood to adult age in four patients [44]. These patients were receiving HU treatment for more than 8 years. They observed that two patients experienced severe oligozoospermia and two azoospermia. The treatment exposure in patients experiencing oligozoospermia was shorter (8 and 9 years) compared to patients experiencing azoospermia (12 and 15 years). There was also an increased percentage of abnormal spermatozoa morphology in these patients.
Furthermore, a study assessed spermatogonial quantity in prepubertal patients who received alkylating agents to compare with patients who received non-alkylating agents. They demonstrated that the quantity of spermatogonia per transverse tubular cross-section was significantly low in patients with SCD receiving hydroxyurea (0.3 ± 0.6, n = 6; P = 0.008) [45].Contrarily, a recent study reported no difference in semen volume, sperm concentration, total sperm count, or spermatozoa motility, morphology, and vitality between patients with SCD who received HU before puberty and who did not receive HU during puberty [46].
Semen analysis
A significant reduction in sperm density, ejaculate volume, sperm motility was reported in the SCD patients compared to the control subjects [43]. Likewise, some former studies that performed semen analysis in men with SCA reported a reduction in sperm motility, sperm density, and sperm morphology [44]. Similarly, Osegbe et al. and Agbaraji et al. analyzed sperm density, motility, morphology, and semen volume in patients with SCD. They reported a decrease in sperm motility, sperm density, and abnormal morphology in patients with SCD. [12, 47] Osegbe et al. observed no difference in semen volume [33]. Additionally, Friedman et al. reported oligospermia in 3 out of 4 patients with SCD [47].
Similar to Osegbe et al., a recent study also reported a normal volume of ejaculate in 75% of the samples of SCD patients. However, all sperm parameters during HU treatment were affected [47]. There were no incidents of azoospermia in five patients, although a marked decrease in sperm density during the HU treatment compared to before the HU treatment was reported. Interrupting HU treatment did not help recuperate the sperm parameters to initial levels.
However, before HU was established as a standard of care to treat SCD, subfertile range sperm parameters had been reported in patients. More recent studies have reported at least one abnormal sperm parameter in about 90% of patients [47].
HU treatment, even in low doses, exacerbates sperm parameters abnormalities in SCD patients. Therefore, routine seminal fluid parameters assessment is recommended to monitor sperm parameter changes during treatment with HU.
Treatments Available
For patients who have abnormal spermatogenesis due to their underlying condition or treatment of the conditions, the option of fertility preservation can be considered. The “optimal” age for fertility preservation is still a discussion. Below are some of the options available [46]-
Erectile dysfunction can be managed with penile implants effectively
Testicular tissue cryopreservation
Gonadal shielding
Sperm cryopreservation
Testicular sperm extraction
Electroejaculation- electrical current to trigger ejaculation.
Symptoms of hypogonadism can be treated with testosterone undecanoate injections12 and clomiphene13
In prepubertal males, patients have very limited experimental options, for example, removal and preservation of part of the testicle [47]. However, there have been no reports of live human births from re-implanted testicular tissue yet.
Counseling about infertility risk associated with the disease and treatments, and options for fertility preservation is important in these situations. Many unresolved ethical dilemmas arise for pediatric patients regarding counseling about fertility issues and preservation. The first dilemma is with whom the responsibility of making the decision should rest. Although some guidelines consider it should be parents, often patients (mostly children in case of SCD) and parents may have different opinions and choices. The American Academy of Pediatrics has published guidelines encouraging healthcare providers to discuss the issues and options with patients and guardians [48].
Since fertility preservation may not be feasible in all cases of SCD, regular monitoring for sperm abnormalities during HU therapy has been suggested.
Conclusions
HU has significantly improved the treatment outcomes in SCD patients. However, some concerns regarding the cytotoxic effects of HU on spermatogenesis emerge. Extensive research is required to evaluate the before and after treatment sperm parameters and the effects of treatment with HU on spermatogenesis.
Newer medical advances have improved survival rates and reduced disease-related morbidity in SCD patients, bringing reproductive issues to the forefront. Prospective, large population-based studies among patients with SCD are required to determine cellular and functional impairment of fertility and evaluate the impact of HU therapy on the impairment.
The clinical practice and future research should be streamlined to focus on improving the quality of life along with the prognosis of the patients. The patient-centric research will help in better management and treatment of patients with SCD with HU therapy.
#Sickle cell disease#Hydroxyurea#Sperm abnormalities#jcrmhs#Journal of Clinical Case Reports Medical Images and Health Sciences quartile#clinical images journal
4 notes
·
View notes
Text
Gynecologist Doctor In Punawale

1. Polycystic Ovary Syndrome (PCOS)
PCOS is a common hormonal disorder among women of reproductive age, causing irregular periods, weight gain, and fertility issues. Dr. Balaji Nalwad Reddy offers a range of treatments, from lifestyle changes to medications, to help manage PCOS symptoms and improve overall health.
2. Heavy Menstrual Bleeding
Heavy menstrual bleeding, also known as menorrhagia, can disrupt daily life and lead to anemia. Dr. Reddy uses advanced techniques like hysteroscopy to identify the cause of heavy bleeding and provide treatments that may include medications or minimally invasive surgeries to control the bleeding.
3. Pelvic Inflammatory Disease (PID)
PID is an infection of the reproductive organs that can cause pain and lead to fertility problems if untreated. Dr. Reddy provides effective antibiotic treatments to control the infection and prevent complications, ensuring women's reproductive health is preserved.
4. Infertility
For couples facing difficulty in conceiving, Dr. Balaji Nalwad Reddy offers infertility evaluations and treatments. He conducts thorough assessments to identify the root cause of infertility, such as ovarian cysts, endometriosis, or hormonal imbalances, and suggests appropriate treatments like fertility medications or assisted reproductive technologies.
5. Contraceptive Counseling and Family Planning
Dr. Reddy provides expert advice on contraceptive methods, helping women and couples choose the best options for their family planning needs. He offers long-term and short-term contraceptive solutions, including IUDs, oral contraceptives, and sterilization procedures, to ensure safe and effective family planning.
Dr. Balaji Nalwad Reddy is dedicated to providing comprehensive gynecological care in Punawale, ensuring that his patients receive the best possible treatment for their reproductive health. If you need expert care for any gynecological concerns, make an appointment with him today.
For More Info-https://gynaeclaproscopicsurgeon.com/blog/2024/10/02/gynecologist-doctor-in-punawale/
#ovarian#ovarian cancer#ovarian cyst#polycystic ovarian syndrome#premature ovarian failure#chronic fatigue#endometriosis treatment#fibroid surgery#ovarianstimulation
2 notes
·
View notes