#covid 19 case
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
There were a total of 171.5 billion posts on Tumblr in 2019.
Text
Hey guys?
What are we gonna do when our kids get homework about COVID in their History classes to interview us about it?
#“our kids” in this case means the kids in our lives#they don’t have to be *your* kids#because you will probably know at least some children#covid#covid 19#thoughts#random thoughts#i have no idea how to tag this#whatever#i don’t actually care#if it becomes a big thing‚ it becomes a big thing#cb writing stuff
55 notes
·
View notes
Text
stranou pozornosti měl dneska narozky tenhle krasavec.
už je mu pět! 🥳


48 notes
·
View notes
Text
In the summer of 2023 I was hiking in the mountains of Scotland and Norway.
In the summer of 2024 I found myself in a wheelchair because I cannot travel without airport assistance.
I no longer work. Or leave the house (except for doctor's appointments). Or watch a movie in one sitting.
I hardly ever see my friends or family, and never for long.
COVID is not just a cold. COVID is not just a flu.
The risk of getting long COVID is cumulative.
#And just... if in doubt do a LFT - for your sake (in case you get LC you want to be able to say you know you had COVID) - and OTHERS#Don't get COVID if you can help it#What I would give to go back to my former self and asked her to be more careful#Long COVID#COVID 19
20 notes
·
View notes
Text

Many such cases :(
#Many such cases :(#cats memes#cat memes#memes#meme#fascism#oppression#repression#dictatorship#covid 19#covid conscious#covid isn't over#long covid#covid#woke mob#wokeness#i just woke up#anti woke#woke#bourgeoisie#ausgov#politas#auspol#tasgov#taspol#australia#fuck neoliberals#neoliberal capitalism#anthony albanese#albanese government
41 notes
·
View notes
Note
??I slept for wayy too long???
It was around 12 am when i slept and i woke up at 3.30 pm
My new record lol
shu- a new record, huh? how... impressive

*proceeds to sleep through a couple of centuries, no biggie*
#diabolik lovers#sakamaki#shu sakamaki#once i slept 19 hrs#after getting the worst case of covid#never doing viruses again thanks
8 notes
·
View notes
Text
I was doing ok and a conversation with my mother left me full of anxiety. She knows I'm worried about covid, and I feel like I am the only one in all of my social circle who is worried about this and trying to do something (and I think it's the bare minimum really, masking when there is a lot of people or in closed spaces).
She told me she is sick, I told her to get a covid test. She said "well, if it's covid, bad luck". I told her that covid is supercontagious for days and that it creates inmunodeficiency for months, so that is the interest of knowing if it's covid. She still didn't care.
We were planning on eating at her place and now I don't want to because I will have to go with a mask just in case she had covid and she doesn't know.
So it's really that people do not give a shit. I understand the trauma of the pandemic and not wanting to think about it but I really can't grasp how you can just tell a person who you know is worried about covid, who has been telling you that there is a pike in covid cases, that you don't fucking care if you have covid and that you don't want to test, not even for their sake.
#right now covid comes with symptoms like diarrhea or vomits on top of all the other ones we know#so basically whatever “feeling kind of sick” symptom you have just get a test just in case#because it might as well be covid#covid 19#I feel so fucking lonely guys. It's incredible
13 notes
·
View notes
Text
Latest COVID-19 Developments: India's JN-1 Variant Insights
Explore insights into COVID-19, rising cases in India, and the JN-1 variant. Stay informed on preventive measures and vaccination for a healthier future.
7 notes
·
View notes
Text
tonsil trouble scene by scene rant (FROM THE VAULT [2020])

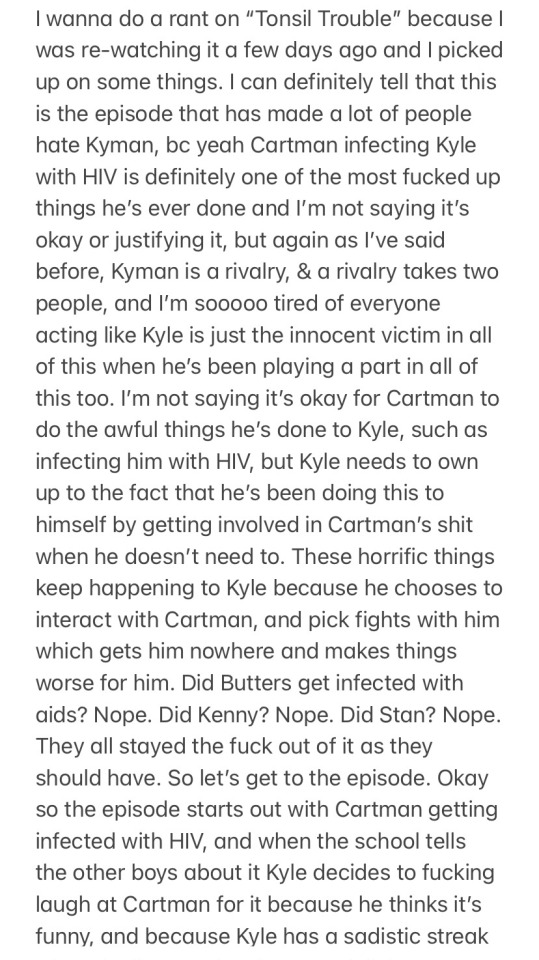
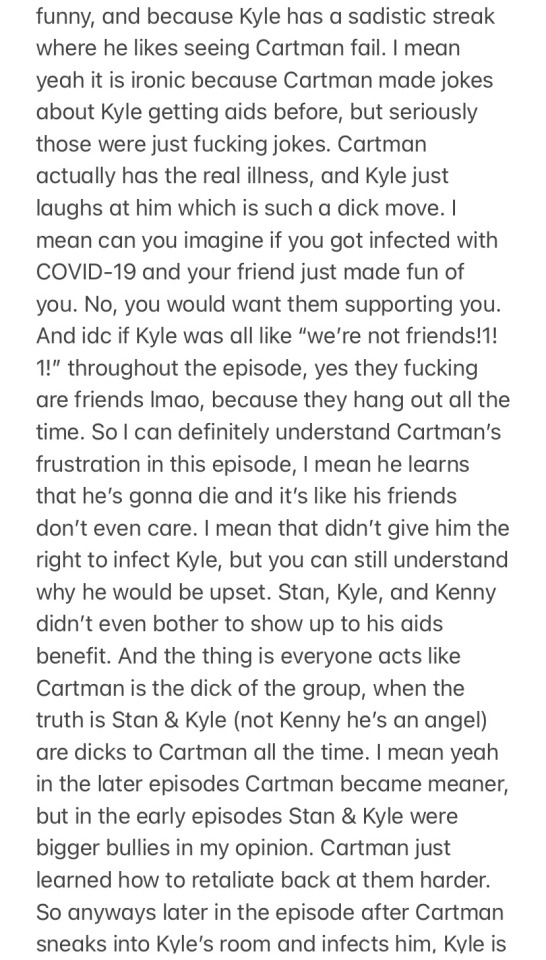
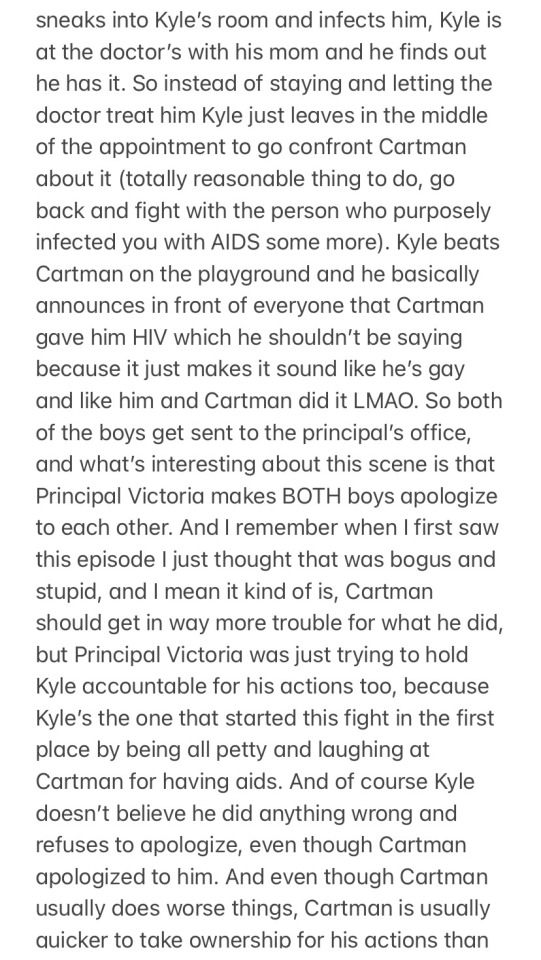
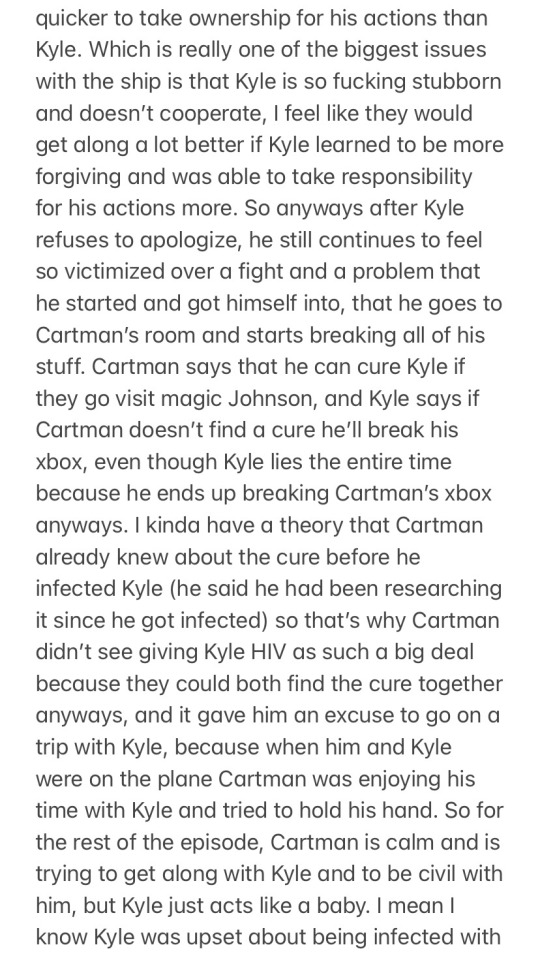

me in 2020: yeah cartman prob shouldn’t have given kyle aids
me now: fuck kyle he deserved to get infected with aids
#that covid-19 comparison aged poorly#now we know covid isnt as horrible as everyone made it out to be#bc it’s just like having a cold in the majority of cases#kyman#south park#KYMANRANTGARBAGE
23 notes
·
View notes
Text
Bad news: I am Diseased.
Good news: The coughing is giving me chiseled abs.

#shitpost#meme#Best case scenario: I get stronger. I grow immune. I have chiseled abs.#Worst case: Showing off my chiseled abs with a sexy hospital selfie.#It's not necessarily Covid-19.#But not necessarily not.#I'm gonna be so muscular. So buff.#So ill...
8 notes
·
View notes
Text
One of five people charged with attempting to bribe a Minnesota juror with a bag of $120,000 in cash in exchange for an acquittal in a fraud case pleaded guilty in federal court Tuesday. Abdimajid Mohamed Nur, 23, pleaded guilty to one count of bribery of a juror, admitting that he recruited a woman to offer the juror money as part of an elaborate scheme that officials said threatened foundational aspects of the judicial system. Four other defendants charged in the bribery scheme have pleaded not guilty. The bribe attempt surrounded the trial of seven defendants in one of the country’s largest COVID-19-related fraud cases. The defendants were accused of coordinating to steal more than $40 million from a federal program that was supposed to feed children during the COVID-19 pandemic. Nur is one of five people who were convicted in the initial fraud case. More than $250 million in federal funds were taken overall in the scheme, and only about $50 million has been recovered, authorities say.
5 notes
·
View notes
Text
2 notes
·
View notes
Text
Successful Jatene procedure for great arteries transposition correction in newborn with SARSCoV-2 infection by Guillermo Careaga-Reyna MD in Journal of Clinical Case Reports Medical Images and Health Sciences
Abstract
Pandemic of COVID-19 represents a challenge for treatment of patients with congenital herat disease. We present a newborn with great vessels transposition and positive SARS-CoV-2 PCR test. The patient was submitted to a successful surgical treatment with corrective Jatene procedure, requiring opened chest wall during 72 h of postoperative period and 43 days of total in-hospital lenght of stay.
KEY-WORDS: COVID-19, SARS-CoV-2, great vessel transposition, Jatene procedure, congenital heart disease.
Introduction
Coronaviruses are single stranded ribonucleic acid viruses with a diameter of 60–140 nm and a high rate of genetic mutations and recombinations, rendering them capable of escaping from the immune system and causing novel infections (1). In less than six months, the coronavirus disease 2019 (COVID-19) pandemic has swiftly spread from one city in China to over 190 countries worldwide (2-4). Neonatal infections with SARS-CoV-2 have been described although robust data on vertical transmission are lacking. In most instances where neonatal infection has been reported, close contact with infected mother or caregiver is postulated to have occurred (4).
In newborns, the case is regarded as positive for infection if any of the following conditions occurs, (1): positive PCR for SARS-CoV-2 in respiratory tract or blood samples, high homology of viral gene sequences of the samples from the respiratory tract or blood to the COVID-19 sequence.
We present a case of a newborn with great vessel transposition and SARS-CoV-2 infection.
Case Report
We present a new born with great arteries transposition associated to aquired SARS-COV-2 infection.
The patient was refrerred to our hospital, with a positive SARS-CoV-2 test, with mechanical ventilatory support in order to confirm a complex congenital heart disease.
The diagnosis was established via echocardiographic evaluation which showed normal venous return, concordance atrio-ventricular and ventriculo-arterial discordance. It was concluded: great arteries transposition, patent ductus arteriosus and permeability of foramen oval.
The patient was recovered from a septic shock with no evidence of systemic inflammatory response requires inotropic support and after stabilization in neonatal intensive care unit, at 10 day in-hospital stay, was submitted to an open heart surgery consisted in anatomic correction with Jatene procedure. The aortic cross-clamping time was 119 min, with cardiopulmonary bypass (CPB) of 181 min. It was decided to maintain in postoperative period opened chest wall, and after 72 the chest wall closure was succesfully realized with favorable posoperative evolution. After 32 days of postoperative, the patient was discharged from hospital. Actually, two years after surgery, the patient is doing well, only with mild pulmonary stenosis without hemodinamic or clinical repercusion.
Discussion
For infants born to COVID positive mothers should be reasonable to separate him from the mother if will need cardiac surgery to try avoid post-natal infection.
In fact, there is minimal evidence of placental vertical transmisión. In this case, the patient has a positive test for SARS-CoV-2 infection and evolved with septic shock in the preoperative period.
It may also be reasonable to do serial testing on the infant, but there is no consensus on the correct timing surgery should be scheduled with advice from a multidisciplinary team of experts including cardiac medical, cardiac surgical, and infectious diseases as indicated. After evaluation of the clinical conditions for a heart team in our hospital, it was decided to realize the surgical procedure in order to avoid progression of heart damage and irreversible heart failure.
However we must remember that, if prudent, surgery should be delayed until the patient’s symptoms have improved and/or testing has been repeated (often after 14 days) and is negative (5).
On the other side, in older patients the inflammatory response due to SARS-CoV-2 infection has been a frequent complication.
In our patient, probably due to the age, it was no presented even with the septic shock o posteriorly associated to the use of CPB during the surgical procedure
It was concluded taht COVID-19 may affect all age patients. However with cautious evaluation and treatment of associated disease as in our case, the patient improves survival, despite severity of viral illness, and during this pandemic period, patients with active COVID-19, at neonatal period we have no treated any other.
#COVID-19#SARS-CoV-2#great vessel transposition#Jatene procedure#congenital heart disease#JCRMHS#Clinical Images journal#Journal of Clinical Case Reports Medical Images and Health Sciences submissions
2 notes
·
View notes
Text
youtube
Fact checking Donald Trump is a full time, even overtime job. He told over 30,000 lies just during his term.
The problem with live news coverage of Trump is that he gets to spew lies and that the factchecking has to wait until he shuts his porcine mouth or producers cut him off.
Low information voters are therefore likely to hear Trump's semi-coherent rants but miss any attempts to call out his lies.
Having said that, MSNBC on Super Tuesday night did a decent attempt at countering a few of Trump's main lies.
Joy Reid is pointing something out that Democrats need to do much more. Trump TOTALLY botched the US pandemic response right from the start. A reminder of what Trump said at CNBC on 22 January 2020 – the day the first COVID-19 case appeared in the US.

Of course it wasn't just fine under Trump.
The Obama administration, which limited the 2014-2016 Ebola pandemic in the US to under a dozen cases, had put together a pandemic playbook. You can read it here. Trump totally ignored it. He spent 50 days after the first US COVID case doing typically idiotic Trump stuff like criticizing 2020 Oscar Best Picture winner Parasites. And afterwards he became preoccupied with quack cures for COVID as it spread throughout the US.
People who claim they had it better under Trump are hoping that the memories of voters are as impaired as Trump's cognition.
We need to be prepared to offer clear fact checks to anybody hearing Trump's lies. Of course convincing MAGA zombies is a waste of time. But when around low information voters who may not be part of the Trump cult we need to be able to offer convincing short refutations. Pointing out that Trump did nothing for the first 50 days of COVID in the US is a good start. So speak up!
Trump's lack of a competent COVID response led to a cascade of acute economic problems which took several years to sort out.
#donald trump#trump lies#factchecking trump#super tuesday#covid-19#pandemic#trump did nothing for 50 days after the first us covid case#economic problems caused by trump#the incompetent trump administration#joy reid#election 2024#vote blue no matter who#Youtube
7 notes
·
View notes
Text
Spouse and I have covid 😭 we had a good run, this is the first time. I am grumpy and congested and feverish but am fine so far. I will continue to be horrible at answering DMs! This concludes my press conference
#personal#covid-19#cw: covid#cw: covid-19#I am on paxlovid and acetemenophen & we are going to get pharmacist-proctored tests in case we need it for insurance later
22 notes
·
View notes
Text
Please be aware, data not being collected does not mean there is no data. Reach out to your local representatives to push HARD for continued funding of waste water monitoring. It is the most reliable, and an incredibly vital resource. Without information about viral trends, it becomes quite uncertain how to proceed for the average person and for communities.

I posted an article awhile back about waste water monitoring finding quite potentially being in a precarious position. Furthermore this would lead to outbreaks and the general public being unawares and run afoul of horrible outcomes.
The work of aggregating and collating of data is being left to individuals, which is not only horrifying, unethical and well out of step with science based methods and guidance, but highly unusual given data is kept and provided for other illnesses, especially ones as severe and concerning as covid-19 (SARs CoV 2).
For the time being, I personally will be assuming transmission is moderate to high in addition to my sources. In the absence or great reduction of data and reports, greater estimations and assessment of made, and when only observations, assumed. Be as safe as you can everyone 💝 - Admin
Please be aware of what may no longer be offered, operating or an out of pocket cost. Masks, tests (all types), vaccines, remote options, COVID-19 tracking apps. Also be mindful of any local or nationwide level policies, proposals, news or trends that cite mask and other NPI removals, bans, stigma or efforts towards criminalization.
For the time being, the following resources remains invaluable:

https://biobot.io
It has come to my attention the person whose account is Laughter In Light has falsely claimed a prominent disability advocate encouraged or engaged in doxxing and slander with no demonstrable proof which has led to great harm. Laughter in light has provided some very helpful information throughout the pandemic. It is also important to be aware, critical and hold people into account for their actions, ideologies, commentary/statements and or stances. There are many other wonderful sources to inform oneself and stay up to date. - Admin
Provides regular updates on infectious diseases news

Sadly they don't have a website or any links I know of. Their Twitter is public however and can be viewed even without an account.
Give incredible analysis and updates on SARS CoV-2! Excellent medical and scientific communicator!
Stella has been amazing since the beginning and continues to be. Definitely worth following! Check out their link tree! They're also on Tiktok!
If anyone has any international resources for updates and tracking, please add it via reblog and I'll definitely share! - Admin
#covid-19#covid 19#sars cov 2#covid#Data tracking#Reports#Waste Water Monitoring#Cases#Deaths#Excess Deaths#Long covid#long haul covid#the pandemic#pandemic#public health#Lucky#Lucky Tran#Peoples CDC#Biobot Analytics#Laughter in Light#Tiffany Najberg#Walgreens Covid-19 Index#Waste Water Scan Dashboard#Our World In Data
20 notes
·
View notes
Text


[Source 1] [Source 2]
#dysautonomia#autonomic neuropathy#pots#orthostatic hypotension#covid-19#cw covid-19#will add my rantings in a reblog in case anybody wants a clean version#vent postings
6 notes
·
View notes