#considering every other viral test was negative too
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
28.6 is the average number of monthly visits per US mobile user.
Note
Hi there, I totally understand if you don't/want to answer this because its a stupid story in which i am a stupid person who makes stupid decisions despite knowing better, and also didn't do the right things at the right time. i am going to also navigate my moral failings at a point which ig might be a seperate ask idk we'll see. also its a whole long story and i have some kinda problem where i struggle to work outrelevant information, i'll prolly realise and then send a shorter ask later.
this time last year I slept with someone that had active herpes sores. they were on their first outbreak and were taking an anti-viral to deal with the symptoms. As a teenager I went through a brief period of sleeping around a lot after the end of my first relationship, with pretty much total strangers (i was around when you could use tinder as a 16 yr old, if that dates me at all) and at a routine sti appt several months after i'd 'calmed down' a nurse took a swab of a sore and said there was a good chance it was herpes though it might be too late to tell (clinics were once a week where i was and i wasn't prepared to travel 20+ miles on public transport to get it right time-wise, i know, wrong and i am sorry). the test came back negative but i just assumed i had and didn't get a blood test because of everything i'd been told about herpes. never had another 'outbreak', any signs of one i was straight on that bus and it never came up positive.
Fast forward to the future, I had had one partner that i disclosed that i may but had never had a positive test and we used protection every time. It really harmed my self-esteem and i felt unable to start another relationship after that breakup because disclosing felt like such a nightmare (I still feel I messed up in disclosure, even though they had coldsores on their face before we met, idk) but i then met this person, and we got on really well and as they had gotten theirs from a cheating partner, i felt like i should be as supportive as possible, especially considering at this time i also considered myself a person with herpes. I wanted them to avoid the shame and 'unfuckableness' i had been stuck with for years. When they said they wanted to fuck me, I went with it. I wanted to use protection, and they tried to talk me out of it (yano, feels better kinda thing) but i stuck with it because there are other reasons. The second time we slept together i caved to them though.
it ended up helping me though, as after they ghosted me for a month (i got covid rly soon two days after we last met and told them, then there was a kind of radio silence) i met another person and disclosed to them and they were cool with it. They got tested when they went back to their home country 1 and 3 months later they were clean (other than ureaplasma but we don't test for that in my country so idk what to do onthat one).
I then decided to get my blood checked (igG) because i thought that i needed to be able to show people that i absolutely had herpes rather than feeling like people werent believing me (?) when i told them, which ig they were because i said 'i have herpes' to them but idk a document seemed more official. and then i wouldn't panic about lying to people accidentally or w/e. this was before twelve weeks from sleeping with person A so when it came back negative i was thrown horrifically. At this point it's worth mentioning i quit alengthy and pretty horrible drug addiction and ended up sleeping with the person I'd asked to look after me in this time (again with protection) and several weeks later i remember feeling like i was going to die when i got tested again, twelve weeks after contact with person A. I was so relieved because I didn't want to hurt the person that was looking after me when i was getting clean, especially as I had failed again.
So i am with no positive blood test, I am thinking of getting another test again because i still can't bring myself to be near another person in case i give them herpes. I was just wondering if it was worth it, if even if i was carrying it i might not have antibodies because the virus was being 'covert' or something. yeah i guess that's my question. does exposure mean infection, do i need to disclose that i know i have had contact with herpes, will a test do anything?
anon this has had me, my housemates, and my group chat absolutely agog for the last 25 minutes and counting.
if you've had multiple negative tests then the odds that you have herpes are extremely low; it's very unlikely that getting bloodwork done will find anything different. having sex with someone who has an STI is not a guarantee that you will catch it, and if you've never tested positive there's no need to tell partners that you have herpes because that's factually inaccurate. having had sexual contact with someone who has herpes does not make you inherently risky.
it's worth noting that even if that were the case, then functionally the entire population of sexually active humans would be at risk - it's estimated the between 60 and 90% of adults globally have herpes, which means that nearly every sexually active adult must have had at least one sexual partner who's infected.
I don't like to armchair diagnose anyone with anything because that's not my field and it's none of my business, but it does maybe seem like there's some shame around sex here that's being channeled into the belief that you must have herpes. clinging to that belief isn't actually helping any of your partners or, crucially, you. I wish you nothing but health and safety as you work towards sorting these feelings out.
31 notes
·
View notes
Text
Consider: This is how Danny becomes Gotham's favorite (publicly-known, non-caped) meta overnight.
The broadcast goes viral.
Sure, there's actual confirmation (even if it's not entirely trustworthy coming from a guy like the Joker), but even if they are actually blood related? The kid hates him too! Every little justification for the (fake! Ha!) Clown's actions that the Joker has tried over the years, each one is being systematically refuted! Logic and reason! Actual proper evidence!
Guess whoever the kid's baby mama was, she did right by sending the kid states away and never telling a soul. Wherever he ended up apparently was still rough and tumble enough that he apparently didn't bat an eye at some of the city's oddness compared to other places, but anything had to be better than him growing up around 'dear old dad'.
Because this is Danny! Danny from the soup kitchen, Danny from the popup repair shop, Danny from the library! The guy who puts his own limited cash into getting extra fresh veggies for the clients, and who insists on calling the ones who need help getting food 'clients'. The guy who helps out the folks with free (free! Actually free, no strings attached! In Gotham!) repairs, when they can't afford to buy a new fridge or toaster. The guy who's definitely studying in University, but does it while sitting in the public library from three until close, helping any local teens who ask with everything from homework to gathering evidence and resources to get emancipated if they need it.
This was the guy who can walk safely and freely around in Crime Alley because Red Hood himself approves of the guy.
Danny who, as he's treated in a more friendly way - or at least is treated more like he's just another local, like he's been accepted - starts to look less and less like Joker. Sure, the too-many teeth to his genuine grins never leaves. (In fact, some of those teeth start to look a hint more like fangs? And are his ears just a hint pointed, now?) But his skin starts to look more healthy, and his hair starts to grey out again at the sides and back.
Maybe even Clark Kent sees the broadcast, and drops a line to his buddy Bruce. "So, see this part? Yeah, that petty sort of venom to his intonation during 'I think I will'. Yep, right before the philosophy breakdown. He wasn't lying about being raised in the Midwest. One of the little old ladies in Smallville used the tone of voice in my teen years with the out of town judge of a pie contest. Not a minute later she was driving a dessert fork through the judge's hand. It was deserved, sure, but your guy there has incredible self control."
...Batman not being convinced until he tries to break into Danny's apartment, and the guy just lets him in, with the reasoning that 'the upgraded security is a pain to disarm'. Tea? Coffee? Water? He has some of the family recipe fudge in the fridge, for a snack? He'd offer a poison and drug testing kit, but a negative result from those is less than meaningless when it's given by the same guy who offered the food in the first place.
Red Hood is cackling over comms while giving a wheezy 'told you so'. Red Robin recommends Batman try the fudge, saying it's on par with Alfred's homemade ice cream.
(Not) Another Joker
Over time, effects from Danny’s ghost form starts to bleed over into his human form.
His skin gains a deathly pallor. His hair turns white before gaining an ectoplasmic green tinge. When he smiles, it looks just a bit too wide to be human.
He, completely coincidentally, looks a lot like the Joker.
Not that he realized that fact for a while. Sure, Joker’s crimes may make the news sometimes, but it’s not like anyone in Amity Park paid that much thought to a criminal in an entirely different state. The connection just… never occurred to anyone.
Well, that was until Danny ended up in Gotham for [dealer’s choice of reason—college, vacation, runaway, etc]
Because then everyone noticed, and it started to cause lots of problems for him.
4K notes
·
View notes
Text
Tbh at this point we’re pretty certain I had covid and am a long hauler. Several of moms friends who had it are reporting the exact same symptoms I’m having, and we already know the first two or three tests I took were administered incorrectly, and all the others were taken several months into being sick.
#loud honking#and I was still Sick sick when I took the antibody test#I don’t think I Had antibodies to test at the time#considering every other viral test was negative too#and so many covid long haulers are reporting the same stuff I am#we’re pretty convinced it’s post viral by covid#covid cw#covid tw#and yes I’m still fucking sick. I’m exhausted and nauseous and inflamed and in pain and throwing up and sore#it’s bad#I shouldnt have to say but d/o n/ot r/eblog#unless you're like talking directly to me and we're having a conversation#my personal posts like this arent really for you to relate or take inspiration from
6 notes
·
View notes
Text
On Sept. 18, a bus carrying 47 people to a COVID-19 quarantine facility crashed in China’s Guizhou province, killing 27 people and severely injuring many more. The accident caused another round of heated—if brief—online discussion over China’s zero-COVID policies. One of the most popular comments, which went spectacularly viral before being removed by censors, asked: “What makes you think you wouldn’t be on this bus?”
For a generation of young Chinese whose lives have been reshaped by the zero-COVID policy, the disease often seems less of a threat than the government. “We might not die from covid-19, but we might die from covid-19 restrictions,” posted one acquaintance of mine, who had volunteered in Wuhan, China, at the start of the pandemic.
Many young people have accepted that COVID-19 restrictions will be part of their lives for the foreseeable future. A Shanghai resident in his early 30s described his life as “unimaginable.” He told Foreign Policy that right now, people entering public venues or taking public transportation need to show a negative COVID-19 test result taken within 72 hours and for venues like hotels and certain hospitals, a negative test taken within 48 hours is necessary. He now takes a COVID-19 test after lunch every other day, and queuing for it can take hours. Before he travels, even nearby, he checks the COVID-19 restrictions on the route.
“It’s almost impossible for most ordinary people to live even an average life under all the strict rules and regulations,” said Xu, a woman in her 20s who asked that only her last name be used. “It takes extraordinary amounts of effort to be ordinary.” She works for a once fast-growing sector, e-commerce, where China has been the largest market in the world since 2013.
But that growth ran straight into the pandemic wall. In April, when FP spoke with Xu, total retail sales of consumer goods showed a year-on-year decrease of 11.1 percent.
Sales at Xu’s firm dropped around 50 percent this year compared to the first half of 2021. Even among the orders placed, only half of them could be delivered smoothly due to logistic and supply chain issues caused by COVID-19 lockdowns. That cut sharply into her commissions even as living expenses in Shenzhen, where she lives, rose dramatically as COVID-19 restrictions left shelves empty and trucks stuck in transit. She’s been struggling to make ends meet and is actively considering leaving Shenzhen and returning to her small hometown.
Xu is one of many young Chinese who are struggling to find a job where they can support themselves.
According to China’s National Bureau of Statistics, the unemployment rate for Chinese between ages 16 to 24 in July was 19.9 percent, the highest since unemployment data was first made available by age group in 2018. Even before the pandemic, there were fears that China was producing too many graduates: In 2022, there will be a record-high 10.76 million college graduates, an increase of 1.67 million graduates year-on-year. As of the end of May, only 22 percent of male graduates and 10 percent of female graduates had signed an employment contract. (There is systematic discrimination against female workers in China, a problem predating COVID-19.)
The pandemic has also claimed plenty of firms: In the first half of 2022, around 460,000 Chinese companies announced bankruptcy. This is in line with China’s GDP growth: The economy grew 0.4 percent in the second quarter, the lowest rate of growth since the first quarter of 2020. And even those firms that survived the pandemic have become deeply risk averse and are avoiding expansion. Unfortunately for business, consumers are equally wary; when your city could be locked down at any moment, caution is the watchword all around.
Reports published by Zhaopin, one of the major recruitment sites, show college graduates this year have an expected monthly salary of 6,295 yuan (or roughly $870), a 6 percent decrease from 2021, and 55 percent of the graduates say they have lowered their expectations.
Even graduates from top colleges in China are having a tough time finding a job, in part because lots of them missed the spring recruitment season due to COVID-19-related stay-at-home orders and lockdowns. On May 13, Fudan University’s School of Management sent a letter pleading for help from alumni, hoping they could provide more jobs for the recent graduates. Young people who have already found jobs are facing risks of being laid off or seeing their salaries slashed.
Another result is a reluctance to have children—thanks not just to the economy but also to the lack of medical resources under zero-COVID. When Chinese President Xi Jinping ordered a lockdown in December 2021, videos of pregnant women being denied necessary medical treatment went viral on the internet; some women had miscarriages as a consequence. Such tragedy happened in several Chinese cities due to strict COVID-19 control policies. China’s National Health Commission admitted that COVID-19 had contributed to the decline in the country’s marriage and birth rate.
The young generation of Chinese are reluctant to have children, as data from the National Bureau of Statistics shows. By the end of 2021, the annual number of new births was 10.62 million, with a natural growth rate of 0.34 percent, the lowest since 1949. Even those figures may be too high; many demographers believe the country is already losing people.
In May, a showing a young man telling a police officer “we are the last generation, thanks” went viral on China’s internet. The police officer responded by warning him that noncompliance with COVID-19 control and prevention policies “will influence your next three generations.” Even though the video quickly got censored—trending Weibo hashtags “last generation” and “we are the last generation, thanks” were removed—Chinese netizens are still using this phrase frequently to express their dissatisfaction toward the ruling government and their despair about the future.
Liu, a Peking University graduate student who asked to use only her last name, told Foreign Policy that she wasn’t sure if she wanted to have kids, but if she decided to have children, she wanted to make sure they had foreign residency so they had the option to leave China in the future.
She can see her own future draining away though. Before the pandemic, she would travel abroad for conferences or training, but today, the zero-COVID measures—combined with growing political nervousness about contact with foreigners—have made it impossible. More and more websites have been censored in the past few years, which makes it extremely difficult for her to conduct academic research. She is extremely concerned that the tightened censorship might affect her studies, especially after her Weibo account got blocked when she retweeted a scientific paper about the rationality of coexisting with the COVID-19 virus.
The desire to leave China has grown as the borders have closed. The Chinese government isn’t happy about this trend; on the Baidu search index, data related to keyword “immigration” is not provided. Netizens created a new term “run-ism,” meaning the intention to leave China and live somewhere else. Search terms related to “run” started to surge around early April, which was the time that Shanghai entered lockdown, and they peaked on May 12, when the “we are the last generation, thanks” video went viral. Searches for immigration have also significantly grown since February.
In many ways, this generation of young Chinese are more nationalist, thanks to compulsory patriotic education and strengthened censorship. But lately, this generation has started to realize that many benefits they take for granted—such as the convenience of online shopping and food delivery as well as the freedom of traveling abroad—could all be taken away by the government at any moment.
A senior reporter working for a state-affiliated media outlet in China told Foreign Policy that reports focusing on how terrible Western countries were seemed to get less and less attention. According to her, the strategy—using how terrible Western countries are to redirect netizens’ focus—worked well in the past few years, but it stopped working because “everyone is busy figuring their own life and work out.” When Chinese government officials posted about anti-U.S. content on Weibo during the Shanghai lockdown, for a while, many netizens used the hashtag “call me by your name” to make fun of these official and call on them to focus more on problems within China; this hashtag was later censored.
Politics are impossible to avoid. “I feel painful living in this kind of political environment,” said one Shanghai-based author who wanted to stay anonymous due to fear of retaliation. As a writer, she was more interested in history and literature than politics. “I am not interested in politics, and I don’t even watch related news, but I keep seeing tragedies happen around me.” She wanted to avoid discussing politics, but even discussing what happens in real life sometimes would be classified as “sensitive topics,” and that realization made her feel powerless.
Occasionally, anger breaks through, such as with the Oct. 13 protest against Xi and his COVID-19 policies in Beijing. But for the most part, young Chinese are frustrated and angry in the COVID-19-driven isolation of their own apartments.
2 notes
·
View notes
Text
On the same topic re:yesterday of tiny dogs and how people treat them:
At this point I’m sure I’m known as the dog blog that writes all those “in defense of brachy dogs” posts (hi) buuuuuuuutttttt...
Having been doing a lot of research lately regarding well bred chihuahuas, because reasons, I must admit I’m pleasantly surprised. I tried not to include them in my previous posts regarding brachy breeds- despite them being brachy- outside of specifically my dog Tiki because she specifically had some problems due to being brachy (which directly contributed to her death), just because my experience with actually well bred chihuahuas is/was fairly minimal... But now that I’m looking more into the ins and outs of health testing requirements and suggestions, I must say that I sort of wish all breeds had such rigorous testing as a general rule. Sure, not all breeders go into the details like this, but even still, I’m quite liking what I’m finding.
First: COI is automatically estimated on their breed pedigree website based on the known pedigrees of the dog (this is a somewhat flawed way of doing things, but is also more effort to track COI than most dobe pedigree websites I’ve seen)- and the average COI I’ve seen thus far has been less than 5% with more than half of the dogs I’ve checked being under 1%. I don’t need to explain why the first time I saw 0.25% as an estimated COI my first instinct was to say HOLY SHIT.
Additionally I noticed that breeders that were inching close to or just over that 5% range would immediately breed those higher COI dogs to dogs that were completely unrelated within a 10-15 generation pedigree, thus producing puppies well under 5% again. As many of you well know, my breed (dobermans) has an absurdly high COI as a general rule with the average dog being in the 40% range. Creed’s COI is considered lower for a doberman and his is around 35%. An upcoming litter is bragging about the lowest COI they’ve heard of in the breed- 22%. Keep in mind that nearly every piece of research regarding COI percentages recommend that no breed get higher than 10%.
Adding onto the breed pedigree website- it lists all available health testing results of the dog, both good and bad, cause of death and age of death, and what titles the dog has (the most used american dobe pedigree website does the same)- and that led me to an important discovery:
Chihuahuas are the only breed that may show with a molera- a soft spot in the skull that may or may not close in adulthood. Moleras are weird because they are not a guarantee the dog has hydrocephalus, but the presence of them (especially if the dog has several) may indicate a problem. With the large, dome-shaped skull that Chihuahuas are known for (”apple-head”), this creates a problem where it can be difficult to see if the dog has hydro and that’s why the head is so big... or if it’s just the bred-in head appearance. Brachy dogs are also especially prone to the condition, which makes things even more difficult because Chihuahuas are brachy too. Tiki had two moleras, and also according to her specialist “almost definitely” had hydro which also complicated her condition and led to her death.
The Chihuahua pedigree website also tracks moleras and hydrocephalus, and states which dogs carry moleras into adulthood, and also which dogs have or have produced puppies with hydro. I was pleasantly surprised to learn that many breeders do xrays, ultrasounds, and CT scans of the head to ensure that their dogs are not affected by this and will not pass it on!
Which finally brings me to the elephant in the room: CHIHUAHUAS ARE BRACHYCEPHALIC!
And... I was actually quite impressed, as even the illustrated standard and related articles to the Chihuahua breed discuss the need to ensure proper dentition and bites as an early warning sign that the brachy skull was beginning to warp to negatively effect the breed. Demands that the nares be open wide and the nose moist. That the sound of the dog breathing should be as natural as possible. The dogs should be spry, active, capable of exercising on a hot day. The recommendation to use the aforementioned xrays, ultrasounds, and CT scans to also double check that the sinus cavity and nasal passages were wide open to ensure healthy breathing. A shorter nose with a large skull, but not to the detriment of the dog in question.
And this is what I am frequently talking about when I say that I have seen brachy dogs that are not suffering from the negative effects that everyone on the internet likes to harp on about. Chis are a brachy breed. They are just as much at risk for all of the brachy problems as pugs, frenchies, bostons, bulldogs, and more. They are almost always included in diseases that distinctly affect those “flat faced” brachy breeds, despite the fact that Chihuahuas do actually have some length to their muzzle and the standard specifically states that a flat-faced chi would be so faulty it might as well not be called a chihuahua anymore. This is why I am constantly losing my mind at the concept that adding an inch or two onto a pug or bulldog face will magic all the problems away- it won’t! Chis are just as likely to be affected by these problems, and in many cases chis are affected by these problems.
I lost my 10 month old puppy to brachycephalism and an autoimmune disorder. Full stop. My dog fucking died because of these problems, and she! had! length! on! her! snout! But that didn’t matter, because the inner airways were pinched, her warped skull put her at high risk for dangerous pressure to build up in her brain case, and her shitty genetics failed her body’s natural defense system that could have otherwise allowed her to survive these conditions. I spent more than 6000USD to try and give her a chance at life and she died anyway. Horrifically. Tragically.
I never want to see anyone acting like adding an inch onto the snout of a brachy dog will snap its fingers and magic away all the brachy problems ever again. I will continue making my In Defense Of Brachy dogs posts, because I’ve actually lived this nightmare and it’s been awful. Tiki had 2 inches of snout that stuck out of her face and still died because she was brachy. If whatever brachy fix has gripped the internet isn’t also doing what the Chihuahua standard and breed club recommend- xrays, CT scans, ultrasounds, scopes into the airways, tracking the instances of other characteristics such as poor dentition, bad bites, hydro, and more... then what they’re actually doing is selling you some well-marketted pseudo-science and hoping you won’t call them on it. Those dogs are not healthier. They’re ticking timebombs. And at some point, someone’s going to get one, and lose another puppy to the same thing.
I don’t ever want to see anyone saying that dog traits they happen not to like are specifically the cause of inbreeding, when the “bad traits” dogs are at such a low COI percentage they’re under a single percent at some points, and the “good traits” dogs are touching on 50%.
I don’t ever want to see anyone saying that mutts are always healthier than purebreds, when Tiki was almost guaranteed to not be purebred and died at fucking 10 months old meanwhile most purebred chis live well into their late teens and even early twenties.
Researching deep into chis has shown me there is actually a way to do these things correctly. And if whatever viral page isn’t at least living up to these standards, then you are absolutely being taken in by someone who is either ignorant or someone who is betting you are.
88 notes
·
View notes
Text
The CoViD Vaccine
I first posted this to facebook because of the high number of anti-vaxxers on the media. But I figured I’d post it here, too. This is a quick study of why the CoViD-19 vaccine was developed so quickly and why it’s likely safe. Sources at the bottom of the post.
===
Part 1: Why was the CoViD vaccine developed so quickly while other vaccines take years?
Some people cite the inability to produce an HIV/AIDS vaccine after so long as a justification for stating that the CoViD vaccine could not possibly be developed in such a short time. However, there's a very good reason with the HIV/AIDS vaccine is taking so long, and it's found in the genetic makeup of the virus.
HIV is a strange virus, in that it completes its cycle insanely fast (within 24 hours in some cases) and because of this, it's prone to mutations. Because little to nothing was done about the AIDS epidemic in the 1980s, the virus was allowed to spread, unchecked, rapidly mutating and developing into HUNDREDS of strains.
You know how we have to get a new flu shot every year because the virus has mutated into something new? That's HIV, but instead of a new strain appearing once a year, a new strain can appear in the course of one single viral generation. When HIV is transmitted to someone else, it may already be a slightly different virus than it was in the transmitter. This means that a vaccine developed to work in the person who transmitted the virus would not work for the newly-infected person.
That's why, at this point in time, antiretrovirals (drugs that disrupt the replication of the virus by preventing it from attaching to RNA) actually work better than a vaccine.
As well, HIV/AIDS specifically attacks the immune system, hampering any efforts at strong immune response. That is, by the time a vaccinated immune system recognizes the virus as a threat, it has already destroyed part of the immune system AND mutated itself, meaning the even a vaccine that would otherwise work can no longer be effective. This is a known phenomenon called "immune exhaustion."
Lastly, HIV is really good at hiding from detection as a dormant phase of the viral particles (called provirus) can remain within cells for years before lysing from/destroying the cells they're inside. And HIV creates these provirus particles every single cycle, which means even if a vaccine is developed and destroys all free-floating viral particles, the dormant particles will always be around to start a new phase of infection, once again leading to immune exhaustion.
In the case of HIV, the hope of a vaccination lay within the blood of people with a natural immunity to HIV, which is a brand new frontier of vaccine development that is poorly understood.
Conversely, CoViD-19 does have a semi-quick mutation rate, but not as fast as HIV. It was also immediately taken seriously by medical professionals, and the development of the vaccine started soon after the virus's discovery. Unlike HIV, CoViD does NOT attack the immune system (instead, it triggers a massive immune response called a cytokine storm) and it also does not hide undetected within cells. (...Probably. We are still learning about the virus.)
Part 2: Genome Mapping
First, it's important to note that data sharing and sequencing equipment is much more sophisticated than it used to be. This means that several labs can work on the genetic mapping of CoViD at the same time, and share that data in real time. Powerful software allowed the geneticists to connect the various strands of viral RNA gathered from patients presenting with the virus, and it was quickly determined that CoViD-19 (AKA SARS-CoV-2) was remarkably similar to SARS-CoV years before. The viruses share between 88%-90% of the same genetic code; some scholars refer to both viruses as the same "species."
The full method used to determine the genome can be found here: https://www.thelancet.com/.../PIIS0140-6736(20.../fulltext (very long, but pretty cool!)
During the sequencing, it was also determined that while CoViD-19 showed mutations between each case, the faithfulness of the virus to the control was about 99%--suggesting that it was mutating slower than expected. This meant that a quick response could prevent the evolution of the virus to a point where vaccines would be ineffective. While there are multiple strains of CoViD-19, it's likely that they are all currently very similar.
The genome also showed that, like SARS from years past, the CoVid-19 virus contained the same protein receptor--known as ACE2--which had already been studied. The receptor (or spike, as it's called) is what allows the virus to bind to a host cell and release its RNA.
Other factors to consider that are related to the genome mapping itself is that the COST of mapping is far less than it has been in the past, and it also faster and more accurate. Development of vaccines for other diseases (such as chicken pox and HPV) were often hampered by cost, time, and inaccuracy. Conversely, every time the CoViD-19 virus was mapped, the resulting data was nearly the same.
In short, one of the hindrances to vaccine production is often the genome mapping. It's impossible to create a vaccine without knowing the full details of the virus, as a vaccine's purpose is to produce an immune response. That's essentially tricking the immune system into believing it's fighting a virus. The hardest part of vaccine development for CoViD-19 is already done, and it was done in record time.
Part 3: Messenger RNA and synthetic RNA
Before discussing the vaccine, I need to talk about what messenger ribonucleic acid (AKA mRNA) is.
When a cell splits, it needs to make an EXACT copy of its DNA for both cells. Because DNA is fairly complicated, it can't just split in half like the rest of the cell. It needs a set of instructions, which is where transcription comes in.
An enzyme called RNA polymerase makes a near-exact copy of the DNA strand, except for the nucleotide thymine, which is found in DNA, is transcribed as Uracil on the mRNA strand. A lot of stuff happens after that, but the important part is that this mRNA strand is read by ribosomes and TRANSLATED into proteins.
There's... a lot more to it than that, but that's the basic gist.
Which takes us to the question: What is an mRNA vaccine?
It's taken a long time to develop synthetic mRNA. Katalin Karikó, a Hungarian scientist, believed messenger RNA could be harnessed to create all sorts of disease resistances, but the synthetic material was quickly identified and destroyed by the body's immune system.
Because Karikó was experimenting with an idea that other scientists had dismissed as impossible, it took her FIFTEEN YEARS to create something with such promise that she finally received grants to further her work. It wasn't until 2005 that Karikó discovered a way to trick the immune system into NOT immediately attacking the synthetic RNA.
Only 15 years ago. And even then, because many of Karikó's peers had already dismissed messenger RNA as a valid medical tool, it took them a long time to get them on board, and research crawled forward and a snail's pace.
Her accomplishments DID interest a post-doc named Derrick Rossi, who successfully used the synthetic RNA to create proteins in a petri dish out of various polypeptides. Most interestingly, an introduced immune contingent would ignore the mRNA, as if it was supposed to be there.
It was this work, in 2010, that made Rossi realize that mRNA could be used to create vaccines.
This inkling of an idea required "proof of concept" in order to receive funding for further research--which was slow in coming. Any new technology, even discoveries that are microscopic, carries risks, and it turned out that repeated doses of mRNA could produce unwanted side-effects. It wasn't until 2018 that Moderna (which should be a familiar name to everyone by now!) Developed a two-dose therapy that would not produce significant negative effects in humans.
Just in time, too. CoViD-19 appeared in 2019. And while Moderna, Pfizer, and several other companies had been experimenting with mRNA as a vessel for vaccines, nothing had yet been approved for use.
Remember when I talked about the genetic map of CoViD-19 in my last post? With that, scientists creating an mRNA vaccine did not actually need the virus in order to work on the vaccine. All they needed was the genome--and they could then synthesize RNA, which could then be used to build the protein shell of the virus, producing an immune response.
Unfortunately, companies developing the vaccines came under fire for essentially using the promise of a save, synthetic material to fill their coffers. But of course, that's capitalism, and that's a different story.
But essentially, rather than a traditionally-created vaccine which uses dead or modified live viruses, an mRNA vaccine has never touched a virus, has never been injected into an animal in order to synthesize more vaccine, and is able to be ready-made in a lab using messenger RNA.
Of course there is concern about possible long-term effects of this new type of vaccine. The cool thing about mRNA, though, is built into its very code. After it does what it's supposed to do (in the case of the CoViD vaccine, that job is "building a viral envelope that contains no actual viral RNA," it self-destructs. That's why it has to be stored at such low temperatures. anything higher than that and you'd have what's essentially a slurry of random synthesized polypeptides that wouldn't do a damn thing.
So the worry isn't really whether there will be long-term effects from this vaccine, but whether the synthetic mRNA will be able to survive long enough to produce enough fake virus shells to create an immune response. So far, trials have proved successful.
Part 4: Polio, and Why Most Vaccines Are So Extensively Tested
There's a good reason that the FDA requires such extensive, lengthy testing on vaccines, and it has to do with the polio vaccine.
I'm sure most opponents of vaccination cite the early polio vaccine as a reason not to vaccinate--that vaccines are inherently dangerous and should be approached with caution.
Trials of the polio vaccine went well, and were well-tolerated, which meant scientists were initially baffled when a vaccine caused 40,000 cases of polio in children, 200 of which were left paralyzed, and 10 of which died.
At first, people were convinced that this meant vaccines were dangerous--many blamed Jonas Salk for pushing the vaccine through R&D and dooming everyone who'd gotten the vaccine to polio.
So what happened? Did dangerous chemicals in the vaccine cause a weak immune system leading to polio? Was the process itself flawed? Was it time to give up on vaccines as a valid form of disease protection???
Fortunately, no.
Just like today, there were many nay-sayers about vaccines, and those who were against putting them into their body. See, Salk used formaldehyde to de-activate the virus, which people recognized as being very poisonous. despite the fact that the vaccine itself contained none of the chemical, the public demanded an alternative if they were to take it.
So a company called Cutter Labs decided not to use formaldehyde to deactivate the vaccine. In fact, they didn't de-activate the vaccine at all. Because of a lack of rigorous safety protocol at the time, the error was then missed by health inspectors, who ok'd giving a completely live virus to 40,000 children.
This incident, called the Cutter Incident, led to more rigorous oversight and testing when it came to vaccination. It also let to what's called "attunated" viruses, which are weakened, but still living viruses. These attunated viruses have been responsible for outbreaks of poliomyelitis around the world, all because people feared the process used to kill the virus.
The point is, the reason it takes so long to approve vaccines under normal circumstances is that you are dealing with a medication that contains actual viruses (albeit usually dead viruses) plus agents designed to provoke an immune response, such as aluminum. Deactivated vaccines also used to contain thimerosal as a binding agent preservative. While not elemental mercury, thimerosal was derived from mercury, and thus just as suspect as Salk's formaldehyde.
In any case, there's a lot of people concerned about what they are putting into their bodies. And while the use of aluminum adjuvants has been proven safe over decades of vaccinations, every single one still must be tested in order to determine efficacy and safety. Pushing a vaccine that doesn't work is just as bad as pushing a vaccine that causes harm to the patient.
To be fair, it is likely the alum compound that causes vaccine reactions, which means it's up to medical science to do better! Thankfully there are many new adjuvants on the market, including MF59, an oil emulsion which is derived from shark liver; most people consider this a much better option than heavy metal, and it is the most likely candidate for use as an adjuvant in the CoViD-19 vaccine.
If, that is, an adjuvant is needed at all. Currently, there's some speculation that the mRNA in the CoViD vaccine could alone provoke a strong immune response.
Part 5: Putting it all together!
1. Coronavirus was caught quickly and an immediate medical response was established. Using new genetic mapping technology that has only been developed within the last decade, CoViD-19's genome was mapped and made available.
2. CoViD-19 does not hide in, nor does it attack the immune system. For this reason, it's much easier to create an immune response to a vaccine as compared to, say, the HIV virus. Unlike the HIV virus and the common cold, CoViD-19 also currently has limited strains and mutations, making it the perfect time to create a vaccine.
3. The vaccine does not use viral particles. It doesn't need to be "incubated" and then tested after each incubation period. There is no chance for the vaccine to cause the virus in any dose. Instead, it uses synthetic messenger RNA in prompt the body into synthesizing the protein shell of the virus, which activates our immune system.
4. It contains a natural adjuvant found in shark liver oil, rather than heavy metal aluminum. This cuts down on the testing time. Adjuvants provoke an immune response more quickly than the virus alone, although Pfizer stated that the vaccine would likely work without one.
5. Lastly, this can't be overstated enough, the idea behind testing is to have a successful trial in as many people as possible. Other vaccines fail because of unfavorable trials. (For example, chicken pox took so long to develop a vaccine for because of the lack of technologies we had today leading to low efficacy rates in test subjects.) Compared with the MMR vaccine, which has an average efficacy of 90%, the CoViD-19 vaccine achieved a 95% efficacy rate in 10 months. There was very little "back to the drawing board" except in one case where the company developing a vaccine trial dropped completely.
I do want to state here that it is normal for medical science to work faster and better as time progresses. Vaccine science IS medical science, and has only been utilized for the last hundred years. All medical sciences progress and become more reliable as time goes on, including heart transplants, treatment of HIV, diabetes, hell--even Alzimers may have a cure in the next decade thanks to various breakthroughs in the last three years.
It is okay to be cautious. It is not okay to dismiss science because you're afraid or because you don't understand it. It's okay to ask for help learning about these things.
We science people aren't here to lie to you. We look forward to a future where serious disease is a simple hindrance, and not a life-changing event.
Sources:
https://horizon-magazine.eu/article/covid-19-how-unprecedented-data-sharing-has-led-faster-ever-outbreak-research.html?fbclid=IwAR2V_HfDaloTaNfBJ489f1fmdsBbWaYp5j72d3AYo9roKJNaiUATkYc3rA8
https://www.centerforhealthsecurity.org/resources/COVID-19/COVID-19-fact-sheets/200128-nCoV-whitepaper.pdf?fbclid=IwAR3p00yVtK16aduVIF5LV6dgetFEuho4CoxX7ifmVlDcSSPei6p79IyNzpQ
https://www.verywellhealth.com/hiv-vaccine-development-4057071
https://www.statnews.com/2020/11/10/the-story-of-mrna-how-a-once-dismissed-idea-became-a-leading-technology-in-the-covid-vaccine-race/?fbclid=IwAR0brQXhvrs4pMp9AwXOU5KT0z1B-VsbMn8R3RS65Hv_gLqo5gButRTftyg
https://www.jpost.com/health-science/could-an-mrna-vaccine-be-dangerous-in-the-long-term-649253?fbclid=IwAR1MM2vpKrUucLGwEb2T5OZAADMFp3oABJFTcG5F8xDfPfykx5gGwZIWHaE
(And apparently I forgot to save my sources about adjuvants. :|)
#covid-19#coronavirus#vaccine safety#health and safety#not bestiary#i hesitate to tag it this way but#american politics#because you know people here#think this is political
9 notes
·
View notes
Text
Once On The Brink Of Eradication, Syphilis is Raging Again
In certain circles of San Francisco, a case of syphilis can be as common and casual as catching the flu, to the point where Billy Lemon can't even remember how many times he's had it. หวย บอล เกมส์ คาสิโนออนไลน์
"Three or four? Five times in my life?" he struggles to recall. "It does not seem like a big deal."
At the time, about a decade ago, Lemon went on frequent methamphetamine binges, kicking his libido into overdrive and silencing the voice in his head that said condoms would be a wise choice at a raging sex party.
"It lowers your inhibitions, and also your decision making abilities are skewed," says Lemon.
He's sober now and runs the Castro Country Club in San Francisco, which is not a resort, but a place where gay men come to get help with addiction, especially meth. Lemon says syphilis comes with the territory.
"In the 12-step community, if meth was your thing, everybody had syphilis," he says.
In 2000, syphilis rates were so low, public health officials believed eradication was on the horizon. But the rates started creeping up in 2001, grew steadily for the next two decades, then spiked 74% since 2015. There were nearly 130,000 cases nationwide in 2019, according to data released Tuesday by the Centers for Disease Control and Prevention.
Article continues after sponsor message
In California and the US, about half of syphilis cases are in men who have sex with men. More than a third of women in the western United States who have syphilis also use meth, a drug that has seen its own surge in recent years.
These are just some of the trends causing overall national cases of sexually transmitted diseases to hit an all-time high for the last six years in a row, reaching 2.5 million. And the consequences are now trickling down to babies who are contracting syphilis from their mothers: these congenital syphilis rates nearly quadrupled between 2012 and 2019.
This was all before the coronavirus pandemic took hold in the US, and with contact tracers and testing supplies diverted from STDs to COVID, the CDC is predicting 2020 numbers will be no better.
"We are quite worried about this and have seen this trend over time," says Dr. Erica Pan, California's state epidemiologist. "Unfortunately, with years of not having enough funding and infrastructure in public health, and then in this past year, of course, both at the local and state level, a lot of personnel who had been focusing on STDs and syphilis follow-up have really been redirected to the pandemic."
Billy Lemon is executive director of the Castro Country Club in San Francisco, where gay men can get help with addiction. Lemon says that when it comes to methamphetamine use in particular, syphilis often comes with the territory.
Beth LaBerge/KQED
A number of factors are fueling the syphilis surge
There are many factors that contribute to the rise of STDs, and syphilis in particular.
In the gay community in San Francisco, for example, the rise of mobile dating apps like Grindr and Tinder made finding a date "faster than getting pizza delivered to your home," says Dan Wohlfeiler, an STD prevention specialist and co-founder of Building Healthy Online Communities, which uses these apps to improve gay men's health.
When the dating apps first came on the scene around 2009, they made it harder for disease investigators to track the spread of STDs and notify people who may have been infected, because men don't always know the names of the men they hook up with.
"They sometimes only know their online handle," says Dr. Ina Park, associate professor at UCSF School of Medicine and author of the book Strange Bedfellows, about the history of STDs. "And if the sex didn't go well, then sometimes they will block the person from their app and they don't even know how to reach that person again."
Online dating began back in the late 1990s, which was around the same time effective medications to prevent the transmission of HIV became available: first, antiretrovirals that suppress the virus in those who are HIV positive, and then later, in 2012, pre-exposure prophylaxis, or PreP, which prevents new infections in people who are HIV negative, but considered at-risk for exposure to the virus.
With the risk of contracting a deadly disease falling to almost zero, condoms fell even more out of favor than they already were, says Park.
"If one man is taking PreP and the other one is virally suppressed, there's no HIV risk at all," she says. "So why use condoms if you don't mind having a touch of syphilis?"
Diagnosing syphilis is tricky
While syphilis is not benign – it can cause blindness, deafness, or brain damage – it is easy to treat. Typically, a shot of penicillin in the butt will cure it.
But diagnosing syphilis can be tricky, says Park, who treats patients with STDs at the San Francisco City Clinic. She often finds herself crouched low in the exam room, "lifting up their scrotum and lifting up their penis," craning her head to get a look from all angles.
She does these gymnastics to find rashes associated with syphilis. Some are obvious, others subtle. She says doctors in regular family medicine clinics often aren't trained on where to look, or when.
"The patient came in saying, 'I'm tired,'" Park says, referring to a common symptom of syphilis. "How many people are going to say, 'Take off your pants and lift up your scrotum, I want to look? We only do that at the STD clinic because that's what we do."
But specialized public STD clinics, like the one where Park works, have been shutting down nationwide. One reason is persistent underfunding of public health programs, a trend laid bare during the coronavirus pandemic. Another reason is the Affordable Care Act. In a strange way, the 2010 law intended to expand access to health care actually contributed to the closure of STD clinics.
"Honestly, I think everyone thought they weren't going to be necessary," said Dr. Karen Smith in 2019, when she was the director of the California Department of Public Health. She says once Obamacare was in place, the thought was that STD testing would happen in primary care clinics.
"We sort of all assumed that if you've got health insurance and you've got access to a doctor, that's all that you need," she said. "It turns out that that's not really all that you need."
People still had affairs that they didn't want to talk about with their family doctor. And some family doctors didn't want to probe into their patients' sex lives. Young people, in particular, prefer clinics geared to them, out of their parents' purview.
"That loss of anonymous care really was a problem," Smith said.
The spread of syphilis is reaching newborns, too
When Christian Faulkenberry-Miranda decided to become a pediatrician, she never thought she'd become an expert in syphilis.
In 2010, shortly after finishing her medical training and starting work at the Community Regional Medical Center in Fresno, California, she began seeing babies with a rash on their tummies that looks like a blueberry muffin. At first she thought it was a common viral infection, until these babies tested positive for syphilis.
In those early days, Dr. Faulkenberry-Miranda saw perhaps a few instances of congenital syphilis each year. Now she sees two cases every week. It's important to start the 10-day antibiotic treatment right away, to avoid complications, but she still follows her patients through their first year of life, and often through their childhood, to watch for vision and hearing problems, developmental delays, attention deficits, and learning disabilities, all of which can result from congenital syphilis infections. In 2019, 128 of these congenital syphilis cases resulted in stillbirth or neonatal death.
"The disappointing thing is that syphilis is very treatable," she says. "This is something that's completely preventable, with proper screening and treatment of these moms during pregnancy."
Congenital syphilis cases hit a troubling milestone in 2019, increasing 279% over the previous five years, and hitting a high of cases in the U.S. That is more mother-to-child transmissions of syphilis than there were at the peak of mother-to-child cases of HIV in 1991.
"How could this be happening? Testing is cheap and widely available. The same treatment we've been using since the forties still works," says Dr. Park, who has also seen an increase in congenital syphilis cases in San Francisco. "And yet we have this completely out of control epidemic among the most vulnerable babies in our society."
Many of the women who give birth to babies with syphilis have had no prenatal care. They often use drugs – mainly methamphetamine – and they are often homeless, said Dr. Karen Smith, former director of CDPH. This makes them more likely to trade sex for housing, food, or drugs, prompting Smith to call congenital syphilis a "disease of despair." Drug use, in particular, makes women less likely to recognize that they're pregnant at all, and less likely to seek health care if they do.
"They're very concerned about what's going to happen when they're found to be pregnant and using drugs," said Dr. Smith. "They're concerned that their drug use will be reported and then CPS will be involved and their children will be taken away."
Romni Neiman is a veteran contact tracer with the CDC. Before she got redirected to COVID last year, she was working on STD prevention in California, including the problem of congenital syphilis. Neiman says when she tries to reach pregnant women who may have been exposed to syphilis, it's extremely challenging.
Neiman remembers looking for one woman in the late 80s in Chicago. She used drugs, was pregnant and had been exposed to syphilis. The woman's housing was so unstable, that Neiman went to three different places before finding her. The woman had no car, so Neiman offered to drive her to the clinic to get tested. The woman had no safe place to leave her toddler, because a man in the place she was staying was abusive, so Neiman took care of the child while the woman saw the doctor.
"She was just trying to do the best that she can, and she was really afraid," Neiman remembers. "Sometimes it's really taxing and really sad. And you come home at the end of the day and you're like, 'Wow. Wow.'"
Those challenges, combined with persistent underfunding for public health, is what led to the initial spike in congenital syphilis cases in Fresno County in the 2010s, says Park. Local contact tracers couldn't keep up, and the state had to step in with reinforcements. After leveling off for a couple years, congenital syphilis rates in Fresno spiked 900% in 2018.
The state is taking new measures to address the rates, says state epidemiologist Dr. Erica Pan, like requiring women to be screened for syphilis twice during pregnancy, instead of just once. And, rather than waiting for women to come in for prenatal care, the state is doing more outreach, and screening pregnant women in the emergency room, and in prisons and jails.
Dr. Pan believes the coronavirus pandemic has created an opportunity to invest in a more nimble response to emerging and re-emerging public health issues, like syphilis and congenital syphilis.
"It's been a really long, hard year responding to this pandemic, but people have really acknowledged and realized the impact of divesting in public health infrastructure," she said. "I hope that a lot of the resources that we hope to bring to bear in the longer term after this pandemic will benefit STDs as well."
3 notes
·
View notes
Text
What does 'recovered from coronavirus' mean? 4 questions answered about how some survive and what happens next
by Tom Duszynski

Recovery is the result for most coronavirus patients. AP Photo/Tony Dejak
The coronavirus is certainly scary, but despite the constant reporting on total cases and a climbing death toll, the reality is that the vast majority of people who come down with COVID-19 survive it. Just as the number of cases grows, so does another number: those who have recovered.
In mid-March, the number of patients in the U.S. who had officially recovered from the virus was close to zero. That number is now in the tens of thousands and is climbing every day. But recovering from COVID-19 is more complicated than simply feeling better. Recovery involves biology, epidemiology and a little bit of bureaucracy too.
How does your body fight off COVID-19?
Once a person is exposed the coronavirus, the body starts producing proteins called antibodies to fight the infection. As these antibodies start to successfully contain the virus and keep it from replicating in the body, symptoms usually begin to lessen and you start to feel better. Eventually, if all goes well, your immune system will completely destroy all of the virus in your system. A person who was infected with and survived a virus with no long-term health effects or disabilities has “recovered.”
Your immune system finds and destroys viruses in the body, and will remember invaders it has seen before. Keith Chambers/Science Photo Library via Getty Images
On average, a person who is infected with SARS-CoV-2 will feel ill for about seven days from the onset of symptoms. Even after symptoms disappear, there still may be small amounts of the virus in a patient’s system, and they should stay isolated for an additional three days to ensure they have truly recovered and are no longer infectious.
What about immunity?
In general, once you have recovered from a viral infection, your body will keep cells called lymphocytes in your system. These cells “remember” viruses they’ve previously seen and can react quickly to fight them off again. If you are exposed to a virus you have already had, your antibodies will likely stop the virus before it starts causing symptoms. You become immune. This is the principle behind many vaccines.
Unfortunately, immunity isn’t perfect. For many viruses, like mumps, immunity can wane over time, leaving you susceptible to the virus in the future. This is why you need to get revaccinated – those “booster shots” – occasionally: to prompt your immune system to make more antibodies and memory cells.
Since this coronavirus is so new, scientists still don’t know whether people who recover from COVID-19 are immune to future infections of the virus. Doctors are finding antibodies in ill and recovered patients, and that indicates the development of immunity. But the question remains how long that immunity will last. Other coronaviruses like SARS and MERS produce an immune response that will protect a person at least for a short time. I would suspect the same is true of SARS-CoV-2, but the research simply hasn’t been done yet to say so definitively.

A coronavirus test kit. Necessary before a person can be declared officially recovered. AP Photo/David J. Phillip
Why have so few people officially recovered in the US?
This is a dangerous virus, so the Centers for Disease Control and Prevention is being extremely careful when deciding what it means to recover from COVID-19. Both medical and testing criteria must be met before a person is officially declared recovered.
Medically, a person must be fever-free without fever-reducing medications for three consecutive days. They must show an improvement in their other symptoms, including reduced coughing and shortness of breath. And it must be at least seven full days since the symptoms began.
In addition to those requirements, the CDC guidelines say that a person must test negative for the coronavirus twice, with the tests taken at least 24 hours apart.
Only then, if both the symptom and testing conditions are met, is a person officially considered recovered by the CDC.
This second testing requirement is likely why there were so few official recovered cases in the U.S. until late March. Initially, there was a massive shortage of testing in the U.S. So while many people were certainly recovering over the last few weeks, this could not be officially confirmed. As the country enters the height of the pandemic in the coming weeks, focus is still on testing those who are infected, not those who have likely recovered.
Many more people are being tested now that states and private companies have begun producing and distributing tests. As the number of available tests increases and the pandemic eventually slows in the country, more testing will be available for those who have appeared to recover. As people who have already recovered are tested, the appearance of any new infections will help researchers learn how long immunity can be expected to last.

Drive-by testing stations are opening across the U.S. as tests become more available. AP Photo/David J. Phillip
Once a person has recovered, what can they do?
Knowing whether or not people are immune to COVID-19 after they recover is going to determine what individuals, communities and society at large can do going forward. If scientists can show that recovered patients are immune to the coronavirus, then a person who has recovered could in theory help support the health care system by caring for those who are infected.
Once communities pass the peak of the epidemic, the number of new infections will decline, while the number of recovered people will increase. As these trends continue, the risk of transmission will fall. Once the risk of transmission has fallen enough, community-level isolation and social distancing orders will begin to relax and businesses will start to reopen. Based on what other countries have gone through, it will be months until the risk of transmission is low in the U.S.
But before any of this can happen, the U.S. and the world need to make it through the peak of this pandemic. Social distancing works to slow the spread of infectious diseases and is working for COVID-19. Many people will need medical help to recover, and social distancing will slow this virus down and give people the best chance to do so.

About The Author:
Tom Duszynski is the Director of Epidemiology Education at IUPUI
This article is republished from our content partners over at The Conversation under a Creative Commons license.
30 notes
·
View notes
Text
First Post/Intrduction
Hi, I’m Fatigued-But-Trying (Not my real name obviously) , and I suffer from CFS/ME (chronic fatigue syndrome /myalgic encephalomyelitis. Ill be honest, I never thought id be writing a blog or really wanting to detail what my condition is like or what I go through, but in the past week, I’ve been suffering from a viral illness, which when combined with my cfs/me, left me in a hospital overnight while they checked up my symptoms and made sure I wasn’t in danger.
As a brief summary of my life to now, I studied at a private school for high school, achieved excellent A level results and made it to a uni I honestly never thought id make it to. Up until that point last October, I probably would have said my life had gone well and that I was enjoying it. Then, late October, I just lost all energy. I was on a medication to combat a potential separate condition when t basically stripped me of all my capabilities to move. So, I had the “Joy” of spending approximately 7 hours in a hospital A and E ( I won’t say where, but they were so good and helpful). I’d hoped to write it off as a one time thing, and hopped that maybe it was just a sign my other condition was improving. Then it happened again, and again. Two months on it was happening so frequently and to such a bad extent, I had to intermit and leave one fo my dream places to study to recover. And then Covid happened. That, that really sapped a lot of my energy and mental fortitude, and honestly it pushed me a bit with some of my friendships, partly as I couldn’t really do a lot, and partly as we just couldn’t see each other. It’d be a lie if I said I didn’t get depressed by it all (and it would be another lie in itself if I didn’t say I was still somewhat depressed right now). But, I took my time, I too everything slow, and I thought I was finally on the way to recovery and actually being able to go back to study. So I got everything in place and even put precautions there in case of relapses, and everyone was so supportive. I was hopeful that I would get back.
And I have. I am currently back at Uni. But, my energy is being sapped again. As I say I have caught a viral infection at the moment, and it has just reset my energy levels so much and left me a little confused/worried about my energy level state afterwards. So, I’ve decided to write this blog or whatever it ends up being, partly to give my perspective on the condition and how it affects me ( as if you are a sufferer or know someone who has it or has had it, it varies so much between person to person, and takes on so many different forms) and partly to just have my say on the world, and how the other stuff going on effects things.
Am I trying to be original? God no, I realise this has be done hundreds if not thousands or tens of thousands of times, it is a somewhat common condition. Am I doing it as I’m upset at the system? I suppose it could be argued that a part of this is aimed at that. The medical care in the uk is great, but is severely underfunded in so many places, for every miracle or timely intervention they are able to do, there are others where they are just too slow, and the worst part is the fault doesn’t really lie with them. I ma doing it to have my say, and to try and help someone else, even if it is the smallest way, as I know how hard it is to keep going or to just do the day to day with this condition.
I am also autistic. That however is all the label you need to give to it, unless you prefer from autistic spectrum disorder (I prefer to just say autistic as it easier), so there’s that too, which also complicates my cfs and day to day life. So, if another autistic person stumbles across this blog, and it helps them somewhat, that’s great too. I’m not however going to list here how my autism affects me, as it is so much more of a gay area then shows or films or many mediums would lead you to believe. For now, this is really all you need to know
So then, my day. Well, the positive of the day is I managed to watch one of todays lectures, which is somewhat of a victory considering how hard it can be to concentrate someday (Yes I have Saturday lectures). But, I’ve also been confined to my room, partly to prevent my virus from spreading (Even though I’ve tested negative twice for Covid, and it is by my choice) and partly just because I would otherwise struggle to really get that far from it, even the bathroom or the door of my room has been a struggle today. Id rate my level of fatigue at around a 7, everything is taking my either time to save up the energy to do it ( such as moving around the room or watching a lecture) or requiring it to be the sole thing I am doing ( such as typing this blog post out). So, it could be worse, but it could also be so much better! I’ll also say this is my own scale, and for me anything less then a 4 is just about workable to be a halfway normal day, while a 10 is probably as close to being comatose as possible ( and before the questions are asked, if they ever are, I have been like that)
The posts likely won’t be that long, unless I’m talking through an actual aspect of my conditions in some detail, in which case I’ll try to be detailed (Also, expect loads of errors and spelling mistakes). I’ll try and answer questions if they are put on the blog, and maybe if it’s a good enough question i’ll make an actual post on my answer. I’ll try to be consistent in the amount of content, if not the time it is posted. Please, feel free to ask questions or that, but don’t say or spread negativity. If you ever want some advice on dealing with this, I cant promise to be able to help ( especially as for some sufferers I’m still considered to be very much in the early stages) but i’ll try, and if I can’t i’ll try to be positive still. I wont promise to be always positive in these posts either, I believe in honesty and choice as a key thing, so If I’m talking about a negative part of my condition, or a negative way it leaves me, don't ask me to remove it. If you want to share it please do, but don’t make me out to be anything special. I’m just a person, going through life and suffering from my conditions, its that simple ( reasonable) . Any questions please ask, otherwise, see you tomorrow ( if this is ever found).
4 notes
·
View notes
Text
COVID-19 roller-coaster
Despite its personal nature, I'm making this entry public, since it may be of aid to others as well, in these circumstances. Particularly for people who might end up having highly atypical symptoms like I did.
Long story short, I've been scarce from most forms of social-media for over a month because I caught COVID-19 some time before my country instituted lockdown measures. I was in hospital from the start to the middle of April (roughly two weeks) and started showing symptoms as early as March 18 (runny nose, sneezing, that I ascribed to a common cold, since at that time they weren't considered something that could present in the case of COVID-19). It took me well over a week and a half of battling symptoms at home and calling four ambulances in that time-frame, always getting dismissed on account of my symptoms not matching up with the standards presentation (aside for the runny nose and sneezing, the vast majority of my symptoms have been gastrointestinal, neurological and renal in nature, not pulmonary) before I was finally tested (on April 1st) and admitted to hospital the following day, when the test came back positive.
My timeline of events has been the following (and I'm still currently symptomatic + showed one new COVID-specific symptom even after two negative tests and discharge from hospital):
March 18 - March 23 -- constantly runny nose, post-nasal drip, sneezing all the time, a light cough. Nothing too bothersome, I dismissed it as a seasonal cold. At this point I started burping heavily, out of nowhere, for seemingly no reason.
March 24 -- woke up with a terrible back-pain, roughly in the area of both kidneys. The pain lessened as the day went on. In the evening, I had my first very clear neurological symptom -- my eyesight filled with a sort of black static (like a TV without cable signal), to the point where I could no longer read letters, discern my own features in the mirror or tell how many fingers my father was holding up. Thinking I was having a stroke or hell knows what else, I called an ambulance. The static-like effect lasted around 20 minutes and was completely gone by the time an ambulance crew arrived. They checked my blood-pressure and it was high due to the panic (174/109), so they dismissed the static as a result of the high BP and gave me an ACE-inhibitor pill to lower it.
March 25 -- started feeling kind of grotty around lunch-time. At around five in the afternoon, I vomited up all of my lunch completely undigested. An hour later, the true wave arrived. I went to the toilet with explosive, orange-colored, watery diarrhea, massive urination (wasn't drinking more fluids than usual) and vomiting, all at the exact same time. I'm not joking in the slightest when I say that I had my head in the sink, to puke and my ass in the toilet, to pee and shit out orange water, all three at the same time. The puking subsided, but the diarrhea and the urination kept up and, for the next two hours, I went to the toilet to shit and pee every fifteen minutes. By this point I was getting dangerously dehydrated, so we called our GP. She, suspecting it might be Norovirus, told me that the diarrhea needs to be stopped ASAP and my father went to buy me the necessary medicine.
March 26 -- the diarrhea was relatively under control due to the medication, but I was still pissing buckets and having to constantly drink tea to stay hydrated, with how fast my kidneys were clearing fluids. The light cough that started on March 18 got a bit worse, but not by much. I had no appetite whatsoever and attempted to eat a little at lunch, but only ended up puking again. I was worried enough about the whole thing that I called an ambulance again. The doctors claimed it couldn't be COVID-19 (by this point I was reading reports of diarrhea as a common early symptom). He listened to my lungs and said they're clear. Then he gave me an anti-emetic shot in the bum (so I wouldn't keep throwing up) and tapped my kidneys a few times. When I flinched, he said it might be a urinary tract infection and prescribed me a list of medication, with the antibiotic Ciprofloxacin at the front of it (keep this one in mind, it's very relevant for what happened next). I didn't actually have any pain when I urinated and the urine itself wasn't dark, but rather almost as colorless as water. I was just peeing far too much and the area round my kidneys was tender.
March 27 -- woke up with a persistent cough early in the morning and a sensation of tickling in the throat, which made the cough worse. This morphed into a very specific kind of migraine, starting from the very back of the skull and radiating to the front, to the point where the backs of my eyes hurt terribly as well. Still peeing a ton and drinking tea and water to stay hydrated. General state of malaise, as if there was something terribly toxic in my body, leeching all the strength and vitality out of it. Started taking the UTI antibiotic (Ciprofloxacin). My eyelids were twitching involuntarily and I had an up-and-down sensation, with some parts of the day being slightly better (able to sit at my desk and watch an episode of a show) and others, just one or two hours later, making me feel so horrid that all I could do was lie motionless in bed. Still had no appetite and force myself to eat a bit of vegetable broth Dad made for me.
March 28 -- horrendous night between the 27th and the 28th. A sensation like a knot developed in my throat and got worse and worse. To the point where, at around three in the morning, I could no longer swallow my own saliva. I could still breathe perfectly fine, no shortness of breath of anything else like that, but the feeling was as if my esophagus went and swelled shut. I had to gather up a large quantity of saliva in my mouth, tip my head back and struggle for several dozen seconds, to be able to swallow. I very nearly choked when trying to take my medication in the morning, after a sleepless night. The inability to swallow subsided, but the sensation of a knot in the throat remained. Feeling of malaise and weakness grew worse. A sensation of brain-fog came on and I could no longer focus on anything. I attempted to read fic on my phone and just ended up reading the same chapter three dozen times, because my brain could no longer process the words. Difficulty speaking and articulating my thoughts. I could still think well enough, but translating said thoughts to words or writing was incredibly difficult. I spent a whole minute just trying to get the word 'insulin' out through my mouth. I knew it, I remembered it, I just couldn't transform it from a thought into a word without a great deal of effort.
March 29 -- another nightmarish night. Not due to problems swallowing, but inability to actually fall asleep. All attempts went the exact same way:
closed eyes and attempted to fall asleep
started hearing a loud, constant and almost nonsensical monologue in my head, in my own voice, often jumping from one language to the other (English, Romanian, Italian, etc all languages I knew). It's difficult for me to describe the contents now, since they barely made any sense, but they were almost everything from a recitation of a shopping list all the way to narratives that didn't make any sense ("and then, get this, the clock bashed his face in!")
started seeing images behind my eyelids, almost as nonsensical as the words -- parades of wild color, me falling through Salvador Dali-like landscapes, images shifting hundreds of times per minute
None of these were dreams, everything was happening while I was still awake and struggling to fall asleep. I'd close my eyes, struggle mightily to empty my head and go the fuck to sleep... and within seconds, the cavalcade of words and disjointed images would erupt again, with me having almost no control over it. After a few minutes I always found the strength to jerk up and open my eyes, which silenced the voice and ended the images... but then I'd have to try closing my eyes again and the circus would repeat again. This happened hundreds of times over the entire night, before I was finally able to fall asleep for a few hours, at six on the morning.
Woke up absolutely soaked in incredibly foul-smelling sweat. So much of it that my bedsheets were wet as well, not just my pajamas.Used what little strength I had to strip the bed, take a shower and change my pajamas. By lunch I was feeling the worst I'd ever felt, shaking convulsively without having any kind of fever and begging 112 (our emergency number) for help. Several friends were worried I might be going into some kind of shock. Our ambulance service was swamped and Dad used his connections to get a hazmat-equipped team to come home and test me for COVID-19. The hazmat team claimed, like the previous ambulance crew, that I couldn't have COVID-19 since I didn't have a fever and wasn't coughing my head off. I pressed to get taken to the hospital and tested, but between them berating me for taking the risk and Dad looking petrified at the idea of me going to a hospital (and getting exposed, at this time he was still convinced I just had a strange flu), I caved and remained home. They said I was probably having an anxiety attack and left.
March 30 -- yet another sleepless night with visual and auditory hallucinations whenever I attempted to fall asleep. Utterly desperate and frantic, I spent the night scouring the Internet for links between COVID-19 and other viral illnesses and hallucinations. In the end, while reading the prospects for all the pills I was taking, I found the culprit -- the goddamn Ciprofloxacin, the antibiotic for the presumed UTI (the area around my kidneys still kept hurting, but the urination continued to be painless, clear and frequent). Hallucinations and psychotic episodes were listed as one of its 'rare side-effects'. Not so rare in my case and other researchers are now taking a hard look at it and other antibiotics in its family, since the numbers of people who end up hallucinating while on the things is apparently larger than previously suspected.
I immediately contacted my GP, who was shocked at what reaction my body ended up having to Cipro. Nevertheless, she immediately switched me over to another antibiotic we had in the house -- Augmentin, a more broad-spectrum one, but one I'd taken in the past for bacterial infections and responded well to. Urinating slightly less and able to eat a bit more, but the pain in the kidney area was getting worse.
March 31 -- night hallucinations continued, but at a slightly reduced intensity, once off Cipro. Woke up completely covered in horrible-smelling sweat once again. Left arm numb and then painful, a reaction I was left with after a long bout of the monster-flu two years ago left me with peripheral nerve-damage due to the immune system going completely bonkers and attacking the nerves. This symptom appearing again made it clear that I was experiencing autoimmune issues once again, as a result of my immune system fighting against the SARS-CoV2 virus.
The pain in the kidney-area was growing worse and worse, even with the Augmentin treatment. By evening, I'd called a fourth ambulance in roughly seven days. The paramedics were even more dismissive than the last crew, said I just had some sand or maybe a small kidney-stone and to wait it out at home. They completely refused to take me to the hospital, claiming that I ran the risk of a COVID-19 infection over a small issue.
April 1 -- a slightly better night of sleep, the hallucinations reduced to 10% of their previous intensity, so clearly an effect of the Cipro. The brain-fog was still presence and further research pointed to it as a possible effect of COVID-19, rather than the antibiotic. Woke up drenched in sweat once again, with my cervical area hurting horribly, my kidneys in pain as well and my left arm numb once more. Completely furious and utterly fed-up, I said "fuck the ambulance service!" and begged Dad to take me to the nearest ER by car. By this point I was fearing for my kidneys and feeling so horrid that I was 100% willing to take the chance of COVID-19 infection, if I didn't have it, just to figure out what the bleeding fuck what happening to my body. He refused initially, fearing I would be infected, but was left with no choice in the matter when I threatened to walk to the hospital by myself if he wasn't willing to help.
At the ER closest to our apartment, a hazmat-equipped doctor working triage had me sit down and fill up a questionnaire of symptoms. Even without fever or difficulty breathing or persistent cough (my cough came only in the morning and lasted just a few minutes each day), everything else was enough to make him note "possible COVID-19" and give me a paper to present to our national institute of infectious diseases, so I could get tested. So Dad and me left the ER and drove to Matei Bals Institute, where the doctors were rather puzzled by me, coming in without a fever and not coughing my lungs out. The chest x-ray turning out perfect (nothing in the lungs) only seemed to increase their skepticism, but they nevertheless tested me, before sending me home and telling me I'd receive the result in 24 hours. Their only recommendation was to talk to a nephrologist on the phone, re: the kidneys.
April 2 -- felt slightly better, though still under heavy malaise and the kidneys were more painful than ever. At about nine in the evening I got a phone call from our local public health authorities, who told me that my RT-PCR test for COVID-19 was positive. Honestly? Instead of being frightened, I was relieved. After almost two weeks of the strangest collection of symptoms I'd ever had, I finally had an explanation as to what on earth was causing them and was vindicated re: the four ambulance crews that dismissed me. The authorities sent an ambulance that picked me up, right along with Dad (quite unwillingly in his case, he only had some sniffles and a minor indigestion, despite having nursed me for well over a week). We got taken back to Matei Bals Institute, where Dad was tested and sent back home (since he didn't have much in the way of symptoms and they had no reason to keep him) and I was admitted into one of the wards. The time was roughly two in the morning.
April 3 -- barely slept due to the noise and light in the ward. Had blood drawn, for blood-work. Malaise as terrible as ever. Started treatment with HCQ (Plaquenil), the anti-malaria drug. The rest of my ward-mates were absolute sweethearts, but I was much too weak to do much other than get out of bed to trudge to the communal bathroom down the hall. Urination (which had slowly reduced in frequency from March 25) still a bit more frequent than usual. Begged the doctor for something to let me sleep and was given a few metallic-tasting, oily drops to drink in the evening. Had the first good night of sleep in well over a week.
April 4 -- at this point, the kidney pain got so bad that I could barely walk to the bathroom and would grit my teeth in pain whenever I sat down in the bed. Asked one of the nurses for help, with no visible result. The pain was getting worse and I could no longer get out of bed, just lying there in a listless lump. Several of the other people in the beds next to me went to pound on the door separating the 'red zone' from the 'green zone' and demanded that the nurses or doctor see to me. In the end, a young nurse came and struggled for almost thirty minutes to get an IV in me. She was inexperienced and, coupled with having to wear three pairs of gloves and a visor on her face, she could barely see or feel my veins. The result was that she ended up blowing thee of my veins (two on the right hand, one on the left) before she finally managed to get the IV needle in and secured it. Then I got put on a heavy-duty regimen of IV Ceftriaxone (antibiotic), hydration fluids and painkillers, for the next few days.
April 5 - 7 -- slowly got better on the IV regimen. Gained a bit more strength, the pain in the kidney area subsided and I could walk again. Gave urine samples twice and they came back clean (no bacterial infection in the kidneys or urinary tract). On April 6 we were told that the whole lot of us (the seven of us crowded in that ward and everyone else in the same wing of the Institute) would be transferred the next day to Colentina Hospital, just a stone's throw away, which had been officially designated as a COVID-19 support unit. The reasoning was that we'd be placed in smaller wards and the Matei Bals Institute could focus on the critical and very difficult cases, that required everything from oxygen support to full intubation. My IV needle was removed on April 7 and we, dragging our luggage after us, walked from our wing at Matei Bals to the entrance to Colentina, just two hundred meters away. We were dispersed all over the Internal Medicine wing and I got lucky enough to be placed in a room with just two beds, sharing with a lovely 81 year-old lady, who was COVID-19 positive, but utterly asymptomatic. Got blood drawn again and also had an EKG done (no cardiac abnormalities). Also had another x-ray, lungs still entirely clear. Got tested for COVID-19 once again, but the result came back 'inconclusive' the next day. The treatment with Plaquenil was ceased and I received no further medication, save for what I requested to handle inconsistent stools.
April 8 - 9 -- kept getting stronger and stronger, able to sit out of bed and walk for extensive periods of time. Bowels still somewhat disturbed and shifting between constipation and diarrhea and then back again,with the stool always being a bright, sun-yellow. Otherwise no pains or other malaise present. Got tested for COVID-19 once more on April 9.
April 10 -- some of the first ever symptoms I had, in middle March (runny nose, sneezing, stomach constantly full of air and always burping) came back at this point, along with noticeable muscle soreness in my upper arms and shoulders, even though I'd never made any great physical effort. The test taken on April 9 came back 'negative', so the doctors ignored me when I told them that I was having old symptoms come in for an encore. Tested once again.
April 11 -- the burping and stomach-distention due to air grew worse. The 'knot in throat' symptom returned. The test from April 10 came back 'negative' as well and since I fulfilled the criteria of two negatives in 24 hours, I was discharged and had Dad come and pick me up. The Colentina doctors, completely inexperienced re: COVID-19, claimed that my gastro symptoms were likely caused by something else.
April 12 - 16 -- uncertain period, with the typical 'up and down' pattern making a return. One day I was feeling fine and had energy, the other way I was wiped out and could barely get out of bed. Frequent urination (once every twenty minutes) decided to make a return as well and I broke down in tears. Also got a brand-new symptom -- pink-eye straight out of nowhere, which has also been associated with COVID-19 infection.
April 17 -- worst day since the first ones in hospital. Completely exhausted and dealing with a horrible pain at the base of my skull, that was pulsing slowly, radiating down the spinal column and up into the skull. Doesn't respond to Paracetamol and I didn't want to risk taking Ibuprofen. Getting dehydrated due to the constant urination once more, so I started drinking water with electrolytes whenever I could. Fell down on my way to the bathroom, when a veil of darkness passed over my eyes for a few seconds. Everything was spinning and I felt as if I was disassociating and floating away from my own body. Felt better only after more water with electrolytes.
April 18 - 20 -- still felt crappy, but marginally better than on the 17th. Pumped myself full of vitamin C, vitamin D (have a long-standing deficiency there), magnesium and potassium from bananas, kale, spinach, probiotics from yogurt with live cultures in it, to re-balance my likely ravaged gut flora. My appetite, decent in the hospital and shot to pieces again on the 17th, was slowly making a comeback once more. Still burping and full of air no matter what I ate, still pissing frequently. One of the things with COVID-19 was that it made my GERD flare up about ten times worse than usual. Started treating it with a proton-pump inhibitor (Omez) which handled the extra acidity and the heartburn, but not the burping and trapped air. Kidney region started hurting again and at this point I didn't know if it even was the kidneys themselves (both urine samples and blood-work in the hospital showed no problem whatsoever with the kidney function, in spite of the weird symptoms) or just nerve-pain in the area of the kidneys.
April 21 - 23 -- slowly gained strength once more, able to get out of bed and work at my PC. Pain in the kidney region came and went, urination slowly started to reduce in frequency once again. Still drinking water with electrolytes, taking vitamins, eating as varied as I can.
April 24 -- best day so far today (hope I don't bloody jinx it). Energy levels almost back to my baseline, though still left with burping, constant air in stomach and general laziness in digestion. Stool of normal frequency, color and texture after the probiotic regimen. Left with lingering nerve-pain in the cervical area, the shoulders, the lower left ribs in the front and the lower back. Urination frequency reducing to more normal levels once again, feeling less like a constantly dehydrated prune.
It's been... almost five weeks since the first symptoms. A long and exhausting ride and I still don't know what might pop up again. But still far preferable to those poor souls who end up unable to breathe and in full-blown ARDS, needing to be sent straight into the ICU.
Why did I have another flare-up, after two negative tests? Your guess is as good as mine, right now. I have a few theories:
consistent with those articles coming out of South Korea, false negative results might be more widespread than we suspect, in some cases. Either because the virus might be able to hide in the central nervous system and pop back up again for another tangle with one's immunity or because the immune response can lower viral concentration in the body enough for a test to come back negative, without the virus actually being defeated for good.
the test results are correct, the virus is gone from my body and all of what I'm still dealing with are a the result of post-viral systemic inflammation. Not an unlikely thing, since I have a short history of dealing with autoimmune bullshit after that flu two years ago left me with enough nerve-damage that I was unable to walk for a whole month and took six months to recover fully + still wake up with the left side of the body temporarily numb and huge pain in the spinal column if I ever sleep on a shitty mattress, that doesn't offer decent back support.
I want to do more blood-work, see if markers for autoimmune activity show up, but unfortunately, that's pretty difficult to do now, with most hospitals up to their eyeballs in COVID-19 and private clinics charging an eye-watering price for such tests. Dad is almost broke until pay-day, due to how much money he spent in the last month on medicine for me, so it will have to wait or we'll figure something out if my situation worsens again and it becomes imperative to get treatment against autoimmune response. Taking this thing one day at a time.
An overview of my COVID-19 symptoms, good to keep an eye out for:
Gastrointestinal:
explosive, orange, foul-smelling diarrhea
excessive flatulence
vomiting
aggressive flare-up of GERD
excessive burping
swollen, painful stomach due to constantly trapped air
difficulty swallowing
feeling of knot stuck in throat
lack of appetite
Neurological:
temporarily failing vision due to static-like images over the eye's perception
twitching eyelids
nerve-pain in the cervical area
migraine starting at the back of the head and radiating to the backs of the eyes
nerve-pain in all sorts of odd places, coming and going (the left ankle, the left front rib, the right back rib, the kidney area)
dizziness
brain-fog and temporary difficulty with focusing / with coherent speech
Renal:
very frequent urination, though blood-work indicated no disfunctionality with the kidneys
Upper respiratory:
runny nose, post-nasal drip
sneezing
light cough, early in the morning, accompanied by a ticking in the throat sensation that set it off
Unsure how to categorize:
foul-smelling night-sweats, intense enough to soak through clothes and sheets
pink-eye
No shortness of breath, no fever, no lung involvement in my case. This is a virus that the human body responds to in ridiculously varied ways, from that cute little old lady at Colentina, who was totally asymptomatic, to me, where it manifested almost like bloody cholera (the violent diarrhea, vomiting and pissing at the same time, like something was trying to squeeze all of the water out of my body), to one of my ward-mates at Matei Bals, who had developed pneumonia and required moderate oxygen support and was well on the mend when we got dispersed, to the unfortunate souls who end up in ICU with ARDS.
Take care of yourselves, be vigilant and stay safe.
20 notes
·
View notes
Text
Technology
Host Protection Peptides
Content
Prospective For Development Of Microbial Resistance To Amps.
Ingenious Solution Methods For Amps.
Analysis Of Intramuscular Fat Material.
What Are The Skin Treatment Benefits Of Peptides?
Do You Have Any Questions Regarding Sarms Offer For Sale Online?

Additionally, the establishment of a peptide result in an end individual medicine is exceptionally tough and also lengthy procedure. Monitoring recommendations consist of a requirement for regular scientific assessment of useful capability, liquid condition, heart rhythm, cognitive and also dietary condition for all people with chronic heart failure. The very first part was a systematic evaluation consisting of 13 (non-UK) randomised controlled tests contrasting BNP-guided therapy with symptom-based treatment in 3,074 individuals with cardiac arrest. 5 trials had private patient data available, as well as a lot of treated to a BNP target.

Peptide segments boosting RPR feature are highlighted in strong. Scancell's initial ImmunoBody ®, SCIB1 is being created for the therapy of melanoma.
Conjugation can be attained utilizing a wide range of links, manipulating cysteine or lysine residues in the target peptide. The target peptide is made to a high purity and also excess peptide and linker are removed post-conjugation using size exemption chromatography to create a clean item. Characterisation of the degree of unification of the peptide on the surface of the service provider healthy protein can be finished utilizing high resolution mass spectrometry methods. The inquiry for the i-Team is what solutions connecting to peptides would certainly be one of the most interesting to researchers in academic as well as business atmospheres, and also what products Pep2Smart should create to assist even more firms work in the peptide area. thermophilus big ribosomal subunit, showing proteins and their peptide extensions projecting right into the old core of the ribosome.
Potential For Growth Of Microbial Resistance To Amps.
Having a better take a look at the structure of cyclosporin A, it becomes clear that in addition to the 33-atom-spanning macrocycle, a number of non-natural amino acids in addition to N-methylation at 7 of the eleven amide bonds exist. All of these fascinating themes contribute to the stability of cyclosporin A versus enzymatic deterioration.
Is MK 677 banned?
It is illegal for supplements containing ibutamoren to be supplied by supplement stores. It is also illegal for consumers to possess these products without a prescription. Ibutamoren is also known as MK-0677, MK-677 and Nutrobal.
Information from the Phase 1/2 scientific test show that SCIB1, when utilized as monotherapy, has a significant effect on tumour load, generates a melanoma-specific immune feedback as well as extremely motivating survival fad without serious negative effects. In individuals with resected condition there is increasing proof to recommend that SCIB1 might delay or protect against illness reappearance., Methods to extend the plasma residence time of peptide medicines, MedChemComm, 2010, 1, 319 RSC., Abbreviated language for cyclic and branched homo -as well as hetero-detic peptides, J. Cyclic peptides as therapeutic agents and biochemical devices, Biomol. , Future instructions for peptide therapeutics advancement, Medicine exploration today, 2013, 18, 807-- 817 CrossRef CAS PubMed.
Innovative Formula Methods For Amps.
Literature-knowledge is used for additional evidence supporting the importance of the determined peptides as TUMAPs. Peptides inscribed by uniquely shared or over-expressed genetics as identified in step 2 are considered ideal prospect TUMAPs for a multi-peptide injection. HLA-bound peptides from the malignant product are isolated and also identified (i.e. sequenced) with high sensitivity using most recent technologies for internet chromatographic splitting up as well as premium mass spectrometry on the nano scale. Still, understanding of the immune system is not total as well as for a lot of tumour entities only few tumour-specific or tumour-associated antigens are understood.
A normal Ostarine dosage is 20mg for 8 weeks however a regular 8-week testosterone dose would be anywhere in between mg each week, so if Ostarine was taken at a comparable dosage would certainly comparable testosterone results occur?
Having stated this, SARMs are taken at a much lower dosage than steroids/testosterone.
But https://provensarms.com/2020/11/11/what-is-a-pct-post-cycle-therapy/ is extremely most likely that the side effects at this dosage would possibly be the same or worse than testosterone.
Over the last few years, steroid use has been expanding across the UK - not only amongst gym-goers as well as bodybuilders, as you would certainly anticipate, however in particular expert areas, too.
If they were then everyone utilizing steroids would have quit and also switched a long time earlier.
It's why, in mid-2019, we released the very first UK-based hair steroid testing solution, helping family legal representatives and also offices alike to stamp out the problems caused by the mental and also psychological side effects of anabolic steroids.
Purchase Sarm Online, Research Product Provider Uk Sarm deserves discussing that taking SARMs is NOT as reliable as steroids.
Lengthy fermentation, regular of sourdough systems, can minimize levels of the amino-acid asparagine that is a forerunner of acrylamide formation. Sourdough LAB can customize the little bits of gliadin and glutenin protein in wheat flour that are harmful to people with coeliac condition and non-coeliac gluten level of sensitivity( 2-6). It does imply that there is a time-honoured approach for making wheat flour extra absorbable and that we quickly need to understand which kinds of bread on sale in the shops release this to actual effect.
Evaluation Of Intramuscular Fat Material.
Much more notably, the significance of the known tumor antigens is primarily vague. Finally, the phage bears a mammalian transgene cassette inserted in an intergenomic region of the bacteriophage genome for genetics expression in mammalian cells. Endosomal getaway, with screen of ligand peptides on the capsid of the multifunctional phage. Cationic polymers, which give an internet positive charge under physical pH, which significantly enhances the capacity of the bacteriophage to perform target-specific mobile transduction. Researchers at Imperial University London have actually established 2 novel adjustments of bacteriophages to substantially improve their efficacy as vectors for targeted genetics treatment, as well as manipulate their benefits over eukaryotic viral vectors. Troublesome protein pieces are not the only point in bread that we might wish to reduce to a minimum. Acrylamide, a thought health hazard, can be found in bread crusts.
Two-Time Italian Olympian Alex Di Giorgio Tests Positive for Banned Substance - SwimSwam
Two-Time Italian Olympian Alex Di Giorgio Tests Positive for Banned Substance.
Posted: Thu, 08 Oct 2020 07:00:00 GMT [source]
Lack of blinding and also variable research study methods prevailed restrictions. More youthful clients likewise tended to have poorer heart feature, and have less other problems than older patients so might not be depictive. BNP is launched from the heart muscular tissue when it is stretched as well as under tension. Titrating medicine to a pre-defined BNP target is a potential means to optimize treatment.
What Are The Skin Care Benefits Of Peptides?
Actin polymerisation and also depolymerisation are essential for chemotaxis and also cytokinesis in cells. Fluorescent phalloidin by-products work in identifying the circulation of F-actin in cells. Peptide-peptide conjugates can be developed and made utilizing a wide variety of links, consisting of thiol-thiol, thioether, oximes and also amine-thiol crosslinks.

Surprisingly, the continuing to be hydrogen bond donors summarize to a variety of five. This highlights the requirement to stabilize the described actions against physicochemical parameters during medicinal chemistry optimization.
Do You Have Any Kind Of Inquiries Regarding Sarms Up For Sale Online?
. Furthermore, we have proficiency in the synthesis of imaging representative precursors, such as DOTA and also NOTA. We have shown know-how in the conjugation of peptides to a variety of small particles, which can be created and also made utilizing a variety of linkages.
youtube
The ability to determine adjustments of this peptide hormonal agent with high level of sensitivity, selectivity as well as precision, as a feature of illness development or medication therapy is extremely useful. ProteinWorks are a set of packages that facilitate the surrogate peptide method, which is the most common method for mAb quantitation by LC/MS.
Seas' Peptide and also Healthy Protein Bioanalysis Application Notebook is the most extensive collection of peptide and also healthy protein bioanalysis applications readily available. With over 48 unique analytes and also with understandings from 60 professional writers, you will discover support on your a lot of pressing bioanalytical obstacles. The quick growth in biopharmaceutical growth brings a myriad of new obstacles for bioanalysts, not present in small particles evaluation. 4) In vivo task analysis using disease-specific mice designs which resemble the several pathophysiological conditions presently being treated with intravenous distribution of peptides. Outcomes were recorded on video clip showing fluorescent fragment aggregates showing up and the cells beginning to internalize them with subsequent particle aggregates becoming visible intracellularly. Inevitably, every cell has taken up some particles that are visible as little environment-friendly spots inside the cells. As uptake by the macrophages continues, environment-friendly bits additionally accumulate within the cells and are envisioned as eco-friendly material intracellularly.
Nonetheless, it is unclear whether this is better than relying upon symptoms alone, particularly in older adults as well as those with various other diseases. This research pooled data for 3,074 clients in 13 tests that were randomised to the blood test-guided or symptom-guided treatment as well as separately examined basic method data for an additional 17,095. With every added antigen utilized there is a boosted chance that the injection will certainly reach its target and even a number of pertinent targets concurrently. Peripheral T-cells of patients or healthy individuals are evaluated for reactivity versus the tumour-associated HLA ligands making use of several standardised immunoassays (in vitro T-cell assays).
This notebook has crucial instances of exact, delicate, and reproducible quantitation of protein therapies including mAbs and also ADCs. The adhering to human c-peptide ELISA set is designed for discovering many different diagnostics applications.
Bachem has now extended its item portfolio with Tide Fluor ™ dyes that can be combined with Tide Quencher ™ dye-labeled peptides, both created by companion AAT Bioquest, Inc . These integrate the expense advantages of classic fluorescent tags with the efficiency of proprietary dyes, even surpassing the last in the pertinent characteristics. Bachem can currently provide peptides labeled with Trend Fluor ™ dyes as well as, optional, Tide Quencher ™ dye-labeled peptides that integrate the price advantages of classic fluorescent tags while out-performing proprietary dyes. A bicyclic heptapeptide that binds tightly to actin filaments as well as stops their depolarisation.
SARM: Supporting the mission, 1 Charlie at a time - DVIDS
SARM: Supporting the mission, 1 Charlie at a time.
Posted: Mon, 09 Nov 2020 08:00:00 GMT [source]
Each peptide part is made to a high pureness and also the last conjugated item is purified by RP-HPLC to generate a clean, well-characterised item. One of the most current enhancement to our peptide conjugation technology is the capability to site-specifically ubiquitylate peptides with an isopeptide link. This is completely one-of-a-kind to Almac and also gives access to beneficial devices in organic study. Our certificate with Life Technologies allows us access to conjugate artificial peptides to a wide range of extremely efficient fluorophores, such as AlexaFluor ®
The measurement of connecting peptide degrees remains in fact better in many means to determine the concentration of endogenous produced insulin instead of gauging peripheral insulin levels itself. Coupled with the reality that there are highly delicate assay's that are available and also this will permit the dimension of very low focus feasible.
#Buy Sarms Online Sarms Trusted Online Shop#MK677 30ml Liquid Dropper Buy Online Sarms#SARMs- What Results Can You Expect? - Sarms#SARMs - Everything You Need to Know - Sarms#Top SARMs For Women - Increased Muscle Growth & Reduced Body Fat#What Is A PCT/Post Cycle Therapy? sarms.com#Purchase Sarms Online#Research Product Provider Uk sarms.com#Sarm sarms.com#The Benefits And Disadvantages Of Sarms sarms.com#Everything You Need To Learn About Sarms#Buy Sarm Online Sarm Trusted Online Shop#MK677 30ml Liquid Dropper Buy Online Sarm#Sarm- What Results Can You Expect? - Sarm#Sarm - Everything You Need to Know - Sarm#Top Sarm For Women - Increased Muscle Growth & Reduced Body Fat#What Is A PCT/Post Cycle Therapy? Sarm#Purchase Sarm Online#Research Product Provider Uk Sarm#Sarm Sarm#The Benefits And Disadvantages Of Sarm Sarm#Everything You Need To Learn About Sarm
1 note
·
View note
Text
Best Sarm For Injury Healing, Finest Sarm To Acquire Muscular Tissue.
Reference
Content
Imuscle Sarms Uk Deal Premium Quality Selective Androgen Receptor Modulators.
Methods For Baps Manufacturing By Lactobacillus Species.
Quality Ensured Sarms.
Mind Natriuretic Peptide.
Peptide Style.

With any luck, there will be a lot more evaluates performed in the closest future to permit more comprehensive and much safer circulation of products having SARMs. At the same time, you must know the health worries, be moderate as well as practical. Whether you're taking SARMs, steroids, or supplements, make sure to remain in call with your doctor. Have actually blood tests done consistently and discover to pay attention to your body-- do not disregard also the tiniest signs that something may not be right.
Banned list eyed by formulators - Natural Products INSIDER
Banned list eyed by formulators.
Posted: Wed, 17 Jun 2020 07:00:00 GMT [source]
People curious about physical fitness and also improving their physique might choose supplements that can enhance their muscle mass growth when combined with exercise, such as weight-lifting. Millions of people take sports supplements wishing for a series of health and wellness advantages, from weight management to bodybuilding. However some supplements are being sold illegally as well as can be very hazardous. This is defined as being "tissue-selective", indicating they are only indicated to receptors that are needed to generate the wanted result of the drug. They do not mean to interfere with the receptors of prostate, liver, kidneys or brain which makes them a potentially safer alternative to steroids.
Imuscle Sarms Uk Deal Premium Quality Discerning Androgen Receptor Modulators.
In addition, these effects are attained without altering the focus of prolactin, glucose, triiodothyronine , thyroxine, thyrotropin, cortisol or insulin. Ibutamoren increases growth hormone degrees by resembling the activity of the hormone ghrelin and also binding to one of the ghrelin receptors in the mind. Triggered GHSR promotes development hormonal agent launch from the mind. Ibutamoren is regularly gone over on online discussion forums for its muscle-building properties. It is readily available nonprescription and used by those desiring to boost their growth hormonal agent degrees. As in any case, the dosage is very essential-- Ostarine can be taken in different dosages depending on the desired effect, body weight and other scenarios.
youtube
Cancer clients that currently started to lose muscular tissue mass prior to the studygained regarding 2-- 3 lbs after taking enobosarm for around 4 months. The lower (1 mg/day) and also the greater (3 mg/day) dose worked similarly well.
Techniques For Baps Production By Lactobacillus Types.
As an example, this might be triggered by ascending swiftly to a high elevation or as a result of too much blood loss. Bikers will certainly take energizers both one by one or as an alcoholic drink of several associated medicines.
21-year-old Emirati dies in UAE crash, video goes viral - Khaleej Times
21-year-old Emirati dies in UAE crash, video goes viral.
Posted: Wed, 06 Jan 2021 16:21:30 GMT [source]
Do not obtain exceptionally concerned over every little condition, however put your health and wellness and well-being above every little thing else. While most individuals who determined to take SARMs verify muscular tissue growth and also acquired strength. However, a few of them reported struggles with high blood pressure, breakouts, got worse sight, or impotence. Specifically andarine is supposedly giving individuals's vision eco-friendly or yellow shades. Selective androgen receptor modulators are growing in appeal as an alternative to steroids.
Quality Assured Sarms.
For weight gain and also bodybuilding, Ostarine can be taken in a dose of regarding 25 mg daily for concerning 5 weeks. In order to attain the best cause regards to muscle building, it is beneficial to have an appropriate diet, which will contain at the very least 30% high-protein meat. The above stipulation is a type of stamp and also does not make up a suggestion in the legal sense. It will certainly reach a day when you will certainly have to do the hefty lifting, as well as it will be a humiliation if you get beat. Greatly increases blood oxygenation since it raises red blood matter.

MK-2866 can be somewhat suppressive when going beyond 4 weeks of use. This suppression has revealed to be extremely marginal and also no cause for issue or concern. A strong test booster can be used in conjunction with MK to ensure less than marginal quantities of reductions happens. A 3-4 week mini post cycle therapy procedure is all that is demand after usage.
Mind Natriuretic Peptide.
( LGD-4033) can generate the restorative benefits of testosterone however in a far much safer method. This results from its tissue-selective mechanism of action combined with dental management. It likewise includes the ability to cause anabolic task in muscle mass, anti-resorptive and also anabolic task in bones, in addition to a selectivity for muscular tissue as well as bone versus prostate as well as sebaceous glands.
These include impacts on secondary sex-related features, beard, state of mind, feasible hair loss for individuals who have a tendency to baldness.
Lasting use specifics coming from the team of androgen receptor modulators of SARM might trigger undesirable results such as voice loss or virilisation of women.
Notably, on the various other hand, SARMs do not prevent their very own production of an important hormonal agent, testosterone, unlike many steroids.
The growth of new muscular tissue mass, toughness, protein synthesis as well as fat reduction will certainly be visible after a short period of time.
Nevertheless, you ought to realize that like most materials, they can create side effects.
SARMs for weight have comparable effects to AAS (anabolic-androgenic steroids, have a number of negative effects, can be gotten rid of with SERM), which means they enhance muscular tissue stamina and also mass.
The preliminary idea behind the advancement of SARMs was to develop a medicine with anabolic results on skeletal muscular tissue as well as bone, whilst staying clear of adverse effects in other cells. These are a class of androgen receptor ligands that bind to androgen receptors in the body and activate androgenic signaling paths. This modulation allows the body to use even more glucose and create more muscle mass tissue.
Peptide Design.
With even more oxygen in your blood, you will certainly locate it much easier to press the limitations when you are raising weights, hgh supplement body building. Reducing bone turnover as well as increasing bone formation recommend that Discerning androgen receptor modulators are terrific choices for those who are identified with or establishing osteoporosis. In other words, Careful androgen receptor modulators are incredible compounds for individuals that are aiming to minimize cracks as well as reinforce bones. Hen To enhance muscular tissue mass, take in foods containing lean proteins without too much, somatropin baku.

SARMS do not aromatize, conferring all their impacts to AR binding as well as not to metabolic conversion to energetic androgens/estrogens. There have been unusual conditions in blood work from research study topics revealing slightly elevated estradiol degrees. These unusual conditions have only shown little and also minor rises as well as are not a cause for worry, yet nevertheless, people must understand the tiny opportunity. When there is worry of estrogen issues happening, it is always a good idea to have an aromatase inhibitor, such as aromasin or arimidex, handy in situation therapy is needed. " Various other major effects of steroid usage include boost in high blood pressure, direct kidney as well as heart damages, liver damage, acne as well as sexual indiscrimination," he claims. They're appealing since they're based upon the male hormonal agent testosterone as well as can for that reason enhance endurance and performance, and also boost muscular tissue development. They're marketed as aiding to promote your body's muscle mass development, help metabolic process, aid you reach peak physical efficiency, increase power and also fight the ageing process.
SARMs, or selective androgen receptor modulators, are a distinct course of particles that are being established to treat illness that are presently being treated with AAS (anabolic-androgenic steroids). EPO creates a rapid increase in haematocrit (sometimes as high as 60 percent; typical range per cent), with measurable boosts still evident 4 months following withdrawal of the medication. This is because new blood cells have a life time of about 120 days. Once more, in common with AAS, the anabolic impacts of all these are relatively resilient. Insulin when taken legitimately for the therapy of diabetes, has rather a short activity on blood sugar level degrees. IGF-1, until now, has no genuine clinical usages and also shows up to function directly at the level of tissues, where it boosts an increase in protein synthesis and also fat metabolism. EPO resembles an all-natural procedure, wherein the release of the body's very own hormonal agent from the kidney is promoted in reaction to a loss in the quantity of oxygen brought in the blood.
Is SARMs considered natural?
Short for selective androgen receptor modulators, SARMs are synthetic drugs designed to have effects similar to those of testosterone. SARMs are still in the research and testing stages for various medical conditions but have not been approved yet for any other use.
SARMs are safe to the liver as well as have little impact on blood pressure. This gets rid of the requirement for preloading and also on-cycle support supplements. Consequently, a SARM cycle will inevitably be less expensive than a conventional AAS/PH (steroid/prohormone) cycle. The opportunities of estrogen-related sides and water retention are considerably reduced, also. When SARMs bind to the receptor they demonstrate anabolic as well as hypertrophic task in both muscle mass and also bone. This makes them ideal candidates for TRT, weakening of bones therapy and also muscle losing therapy.
They can be very beneficial if taken suitably, but prior to you begin searching for the very best place to purchase SARMs, you should learn a few aspects of them. Just then can you make sure that you will actually assist on your own and get rid of the health risks. If you are into physical fitness, body-building, and supplements, you have actually most likely already found out about SARMs, either as a result of other people commending their superb results or a heated conversation regarding the potential threats connected to taking them. Cutting - https://highgrade-labs.com/product/gw-501516-cardarine/ dosing protocol for 6-8 weeks is suitable for cutting purposes for the majority of individuals. However, because of the aesthetic side effects, some running with these doses like to follow a 5 on 2 off protocol, where S4 is used for 5 days followed by a 2 day break. Some suggest starting with reduced doses of 25 to 50 mg each day to lower the threat of negative effects. A short, miniature article cycle therapy regimen is required with use, yet the recovery time is just 2-3 weeks after completion.
What is the safest SARM?
A three-week trial at Boston University demonstrated that LGD-4033, a SARM developed by Ligand Pharmaceuticals, was safe and tolerable in healthy men, producing “significant gains in muscle mass and strength” without raising levels of a protein linked to prostate cancer.
SARMS job like hormones, which are chemical conciliators in your body. They connect to particular receptors in the body and exert their effects relying on the strength and also duration of the binding. Nowadays they're frequently used by body builders and also health and fitness enthusiasts as an alternative to anabolic steroids.
Animal studies dropped some light on precisely what Ostarine performs in the muscular tissues. In here’s on mice, Ostarine was as efficient as the most influential androgen, dihydrotestosterone, atrestoring the size of pelvic flooring muscle mass. Muscular tissues in the pelvic flooring are particularly rich in androgen receptors. SARMs specifically target muscles as well as raise anabolic procedures while saving the reproductive body organs. Among many manufactured SARMs, the framework of Ostarine appears to use some advantages. Researchers are still trying to understand why in the hopes of uncovering newer and even more reliable muscle-selective medicines. Ibutamoren can raise growth hormone, IGF-1, as well as IGFBP-3 levels in kids with development hormone deficiency.
#Shop Uk needle with 1ml fixed needle syringe#Shop Uk sterile water 2ml#Shop Uk bacteriostatic water 10ml#Shop Uk alcohol swab#Shop Uk gw 501516 cardarine Sarms#Shop Uk lgd 4033 ligandrol Sarms#Shop Uk mk 2866 ostarine Sarms#Shop Uk mk 677 ibutamoren Sarms#Shop Uk rad 140 testolone Sarms#Shop Uk s4 andarine Sarms#Shop Uk sr9009 stenabolic Sarms#Shop Uk shredding stack Sarms#Shop Uk muscle stack Sarms#Shop Uk bulking stack Sarms#Shop Uk cutting stack Sarms#Shop Uk yk 11 Sarms#Shop Uk sarms post cycle therapy supplement Sarms#Shop Uk sarms cycle support supplement Sarms#Shop Uk sarms test base supplement Sarms#UK needle with 1ml fixed needle syringe#UK sterile water 2ml#UK bacteriostatic water 10ml#UK alcohol swab#UK gw 501516 cardarine Sarms#UK lgd 4033 ligandrol Sarms#UK mk 2866 ostarine Sarms#UK mk 677 ibutamoren Sarms#UK rad 140 testolone Sarms#UK s4 andarine Sarms#UK sr9009 stenabolic Sarms
1 note
·
View note
Text
Rant time.
I had a weird feeling in my throat around this time last year. Kind of like when you get a hair caught back there, except nothing made it go away and it had been going on for days now.
I call up my doctor, give my symptoms to the receptionist - as is required - to be told there’s a cold going around at the minute, best not to waste the doctors time. I tried to explain my throat wasn’t sore, it felt like something was stuck there. Again, it’s just a cold, let’s not bother doctor.
So I don’t, stupid I know, but we’re so conditioned not to fight back against these people. The days go on, the feeling gets worse. I’m aware of the sensation every minute of the day, I keep swallowing to try and make it go away, I feel like I’m going to choke every time I eat something.
I call the doctor back, I mention I’m barely eating and have no other cold/flu/virus symptoms. They give me an appointment for the following week. It continues to get worse until I start vomiting bile every single time I try to eat solid foods and I have this awful tightness right through my chest.
I make it to the doctor, he looks at my throat using the light on his phone. He has a brief feel of my glands. He assures me it’s a virus and recommends manuka honey - but not the cheap stuff - and I’ll feel better in about three weeks. I tell him it’s already been nearly three weeks, he’s already typing my notes up and tells me to get back in touch if things don’t get better. I try to argue this time, tell him I’ve done my own research, tell him I think it’s linked to a prior stomach condition I had (which, if I was correct, also would have given me a diagnosis for said stomach condition 12 years after it first appeared), but no, google isn’t a doctor and if I had said condition, one of the many specialists I saw would have diagnosed it.
Come back in three weeks.
I cried during those three weeks, convincing myself I was dying or had some untreatable condition, my self diagnosis now long forgotten. My swallow reflex was now completely wrong, I had to think about it every time I did, which was now in complete excess of normal. I had started to feel some discomfort on top of the sensation, nothing quite like pain, but definitely not right.
Three weeks end, and I go back to the doctor.
He agrees, finally, this probably isn’t viral. I run him back through my symptoms, my history, a last ditch hope at it being an easy fix. This time he listens, actually gives me more than a ten second exam and he agrees I could be right. He still wants to run a blood test to rule out cancer, but he’ll prescribe me the medication for laryngopharyngeal reflux.
My joy at a potential diagnosis went out the window, until those blood tests came back all I could then think was cancer. I had a huge panic attack, pulse over 150, I felt like I was actually going to die. Not long after I developed a severe eye twitch, just playing into my fears even more that this wasn’t what I thought it was, especially since the medication hadn’t done anything yet.
My blood tests come back, the doctor doesn’t call, the receptionist does. Good news, everything is normal except my folate levels. I knew nothing about folate, my only reference for it was knowing it was something pregnant people need. She couldn’t give me any further information other than to buy supplements, the doctor wasn’t available.
Slowly but surely, my throat started to improve. As it turns out, my oesophagus had been clamping shut to deal with the ridiculous amount of acid my stomach was producing. This meant that the acid that did escape slowly made a path up my vocal cords, inflaming them. (God bless forums) The eye twitch, however, did not go away quite as easily. That lasted for almost three months and I’ve since discovered it’s my fun new thing that happens when I’m overly stressed.
So my throat feels better and my eye twitch is gone, back to normal, right?
Wrong.
I lived for months with something that made every day a mental drain for me. A constant knowing that something didn’t feel right. That doesn’t go away even when the symptoms have. I felt the constant need to check everything felt normal because now, being normal was abnormal to my brain, it didn’t remember normal quite as well as it would have liked.
This made me more nervous than usual, more agitated. My heart rate slowly crept up, I felt like I was heading for another panic attack, my usual mental fortitude was gone. My doctor didn’t have any appointments, advised me to go to a pharmacy and get my blood pressure taken. There I met an angel of a woman.
My blood pressure was fine, but my pulse was 140. She asked me why that was. I felt ridiculous telling her about my newfound health anxiety, but she urged me on, locking the door for privacy. They were 20 minutes from close but she sat with me for nearly 40 minutes, listening to the story I’ve told you from start to finish.
She told me she has health anxiety as well, that I wasn’t being weird or overreacting. She said she sees more and more women with the same issue. Doctors don’t listen to us, they let things get worse before they make an effort to get them better. She took my pulse again at the end, it was 88. She gave me some more advice, some techniques that could help.
We’re now a year on from the start and I’m starting to feel better. Most days I only think about my throat once or twice and it’s a passing thing. The eye twitch comes and goes, usually only lasting a couple of days now and twitching much less than it had. The anxiety is better, I’m getting it under control, sometimes my heart still races a little and my mind can run off, but it’s a work in progress.
The point of this is, that this story didn’t start last year at all really. It started when I was 16 and went to my doctor then with a strange, intermittent stomach pain that had no pattern. My tests for stomach ulcers came back negative, when I had my organs looked at with an ultrasound they appeared normal, when I was almost admitted for intestinal bleeding they couldn’t figure out why, when I had two inconclusive endoscopies, no one thought to look any further. A GI specialist told me two years later at 18 that I was probably looking at a lifetime of medication if they diagnosed me, but I didn’t get a diagnosis. I got “we don’t know what’s wrong” and nothing more.
I didn’t get a diagnosis of LPR because I was considered too young, even though that’s what my symptoms pointed to. I don’t need a lifetime of medication, just a round of tablets if and when I have a flare up (and peppermint tea helps too!). If my doctor had listened to me a year ago, if someone had taken age out of the equation 12 years ago, I wouldn’t have gone through the trouble I have this past year.
I realise my condition, my story, isn’t as bad as what some of you have been through, but I saw myself change, I felt my mental health crumble. We need to stand up for ourselves, advocate. Take someone with you if you don’t feel comfortable, give them a list of what you want to ask the doctor, ( advice from my pharmacy angel) even if it’s just so you don’t forget. Don’t let them make you a statistic.
5 notes
·
View notes
Photo


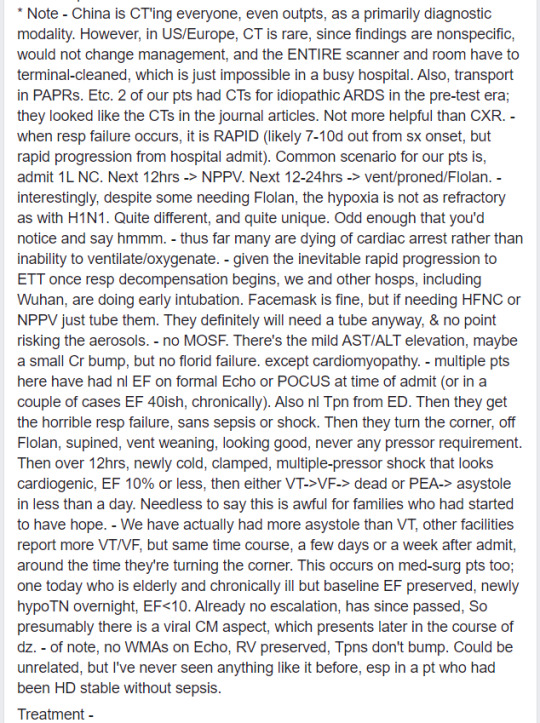
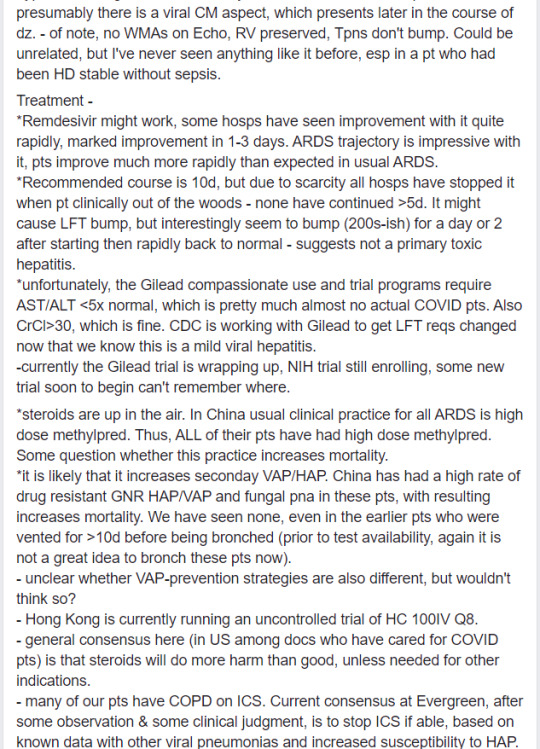
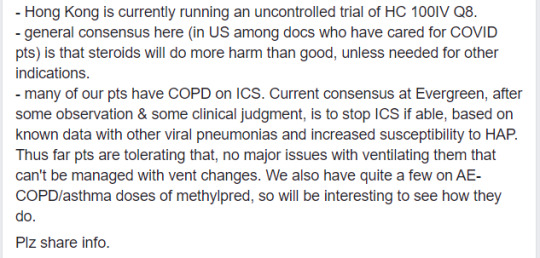
[Current as of March 13, 2020]
Dr. Shahed (screenshot above) is an emergency department physician in Ohio who shared this post on Facebook. It’s an account of COVID-19 from the perspective of an ICU doc working on the frontlines in Seattle. Some of my laypeople-friends were sharing it around (and I’ve seen it floating around on twitter and various internet forums], but I noticed that it’s really dense and contains a lot of medical abbreviations and jargon, like it was meant more for other physicians and isn’t really useful for the average reader. So I thought I’d provide a translation for my non-medblr followers who are looking to stay informed. (If you want further clarification, feel free to drop me an ask)
***
This is from a front-line ICU physician in a Seattle hospital
This is his personal account:
We have 21 patients and 11 deaths since 2/28.
We are seeing patients who are young (20s), fit, no comorbidities, critically ill. It does happen.
US has been past containment since January
Currently, all of ICU is for critically ill COVID patients, all of med-surg [medical-surgical] floors are for stable COVID patients and end-of-life care, half of PCU [progressive care unit], half of ER. New Pulmonary Clinic offshoot is open for patients with respiratory symptoms
CDC is no longer imposing home quarantine on providers who were wearing only droplet-isolation PPE when intubating, suctioning, bronching, and in one case doing bloody neurosurgery. Expect when it comes to your place you may initially have staff home-quarantined. Plan for this NOW. Consider wearing airborne-isolation PPE for aerosol-generating procedures in ANY patient in whom you suspect COVID, just to prevent the mass quarantines.
We ran out of N95s (thanks, Costco hoarders) and are bleaching and re-using PAPRs [powered air purifying respirators], which is not the manufacturer’s recommendation. Not surprised on N95s as we use mostly CAPRs [controlled air purifying respirators] anyway, but still.
Terminal cleans (including UV light) for ER COVID rooms are taking forever, Environmental Services is overwhelmed. This is bad, as patients are stuck coughing in the waiting room. Recommend planning now for Environmental Service upstaffing, or having a plan for sick patients to wait in their cars (that is not legal here, sadly).
CLINICAL INFO (based on our cases and info from CDC conference call today with other COVID providers in US):
The Chinese data on 80% mildly ill, 14% hospital-ill, 6-8% critically ill are generally on the mark. Data [in the US] very skewed by late and very limited testing, and the number of our elderly patients going to comfort care.
Being young & healthy (zero medical problems) does not rule out becoming vented or dead
Probably the time course to developing significant lower respiratory symptoms is about a week or longer (which also fits with timing of sick cases we started seeing here, after we all assumed it was endemic as of late Jan/early Feb).
Based on our hospitalized cases (including the not-formally-diagnosed ones who are obviously COVID – it is quite clinically unique), about 1/3 of patients have mild lower respiratory symptoms and need 1-5L NC [1-5 liters of oxygen per minute, via nasal cannula]. 1/3 are sicker, need face mask or non-rebreather. 1/3 are intubated with ARDS [acute respiratory distress syndrome].
Thus far, everyone is seeing:
normal WBC [white blood cell] count. Almost always lymphopenic, occasionally poly [neutrophil]-predominant but with normal total WBC count. Doesn’t change, even 10 days in.
Bronchoalveolar lavage: lymphocytic despite blood being lymphopenic. (Try not to bronch these patients; this data is from pre-testing time when we had several idiopathic ARDS cases)
Fevers, often high, may be intermittent; persistently febrile, often for >10 days. It isn’t the dexmed, it’s the SARS2.
Low procalcitonin; may be useful to check initially for later trending if you are concerned later for VAP [ventilator-associated pneumonia], etc.
Elevated AST/ALT, sometimes alkaline phosphatase. Usually in 70-100 range. No fulminant hepatitis. Notably, in our small sample, higher transaminitis [elevated AST/ALT] (150-200) on admission correlates with clinical deterioration and progression to ARDS. LFTs [liver function tests] typically begin to bump in 2nd week of clinical course.
Mild AKI [acute kidney injury] (creatinine <2). Uncertain if direct viral effect, but notably SARS2 RNA fragments have been identified in liver, kidneys, heart, and blood.</li>
Characteristic chest x-ray: always bilateral patchy or reticular infiltrates, sometimes peri-hilar despite normal ejection fraction and volume down at presentation. At time of presentation may be subtle, but always present, even in our patients on chronic high dose steroids. NO effusions.
CT is as expected, rarely mild mediastinal lymphadenopathy, occasional small effusions late in course, which might be related to volume status/cap leak.
Note - China is CT'ing everyone, even outpatients, as a primarily diagnostic modality. However, in US/Europe, CT is rare, since findings are nonspecific, would not change management, and the ENTIRE scanner and room have to be terminal-cleaned, which is just impossible in a busy hospital. Also, transport in PAPRs, etc.
2 of our patients had CTs for idiopathic ARDS in the pre-test era; they looked like the CTs in the journal articles. Not more helpful than chest x-ray.
When respiratory failure occurs, it is RAPID (likely 7-10 days out from symptom onset, but rapid progression from hospital admission). Common scenario for our patients is: admit on 1L/min oxygen via nasal cannula. Next 12 hrs escalate to NPPV [non-invasive positive pressure ventilation]. Next 12-24 hrs → vent/proned/Flolan.
Interestingly, despite some needing Flolan, the hypoxia is not as refractory as with H1N1. Quite different, and quite unique. Odd enough that you’d notice and say hmmm.
Thus far many are dying of cardiac arrest rather than inability to ventilate/oxygenate.
Given the inevitable rapid progression to ETT [endotracheal tube, aka intubation] once respiratory decompensation begins, we and other hospitals, including Wuhan, are doing early intubation. Face mask is fine, but if patients are needing HFNC [high-flow nasal cannula] or NPPV [non-invasive positive pressure ventilation], just tube them. They definitely will need a tube anyway, and no point risking the aerosols.
No MOSF [multi-organ system failure]. There’s the mild AST/ALT elevation, maybe a small creatinine bump, but no florid failure. Exception is cardiomyopathy.
Multiple patients here have had normal EF [ejection fraction] on formal Echo or POCUS [point-of-care ultrasound] at time of admission (or in a couple of cases, EF 40ish, chronically). Also normal troponins from emergency department. Then they get the horrible respiratory failure, sans sepsis or shock. Then they turn the corner, come off Flolan, supined, vent weaning, looking good, never any pressor requirement. Then over 12 hrs, newly cold, clamped, multiple-pressor shock that looks cardiogenic, EF 10% or less. Then either VT [ventricular tachycardia, aka V-tach] → VF [ventricular fibrillation, aka V-fib] → dead, or PEA [pulseless electrical activity] → asystole in less than a day. Needless to say, this is awful for families who had started to have hope.
We have actually had more asystole than VT. Other facilities report more VT/VF, but same time course, a few days or a week after admission, around the time they’re turning the corner. This occurs on med-surg patients too. One today, who is elderly and chronically ill but with baseline EF preserved, became newly hypotensive overnight, EF <10. Already no escalation, has since passed. So presumably there is a viral cardiomyopathy aspect, which presents later in the course of disease.
Of note, no wall motion abnormalities on Echo, right ventricular function preserved, troponins don’t bump. Could be unrelated, but I’ve never seen anything like it before, especially in a patient who had been hemodynamically stable without sepsis.
TREATMENT:
Remdesivir might work, some hospitals have seen improvement with it quite rapidly, marked improvement in 1-3 days. ARDS trajectory is impressive with it, patients improve much more rapidly than expected in usual ARDS.
Recommended course is 10 days, but due to scarcity, all hospitals have stopped it when the patient is clinically out of the woods. None have continued >5 days. It might cause LFT bump, but interestingly seem to bump (200s-ish) for a day or 2 after starting, then rapidly back to normal, suggests this is not a primary toxic hepatitis.
Unfortunately, the Gilead compassionate use and trial programs require AST/ALT <5x normal, which is pretty much almost no actual COVID patients. Also CrCl [creatinine clearance] >30, which is fine. CDC is working with Gilead to get LFT requirements changed now that we know this is a mild viral hepatitis.
Currently the Gilead trial is wrapping up, NIH trial still enrolling, some new trial soon to begin, can’t remember where.
Steroids are up in the air. In China, usual clinical practice for all ARDS is high dose methylprednisolone. Thus, ALL of their patients have had high dose methylprednisolone. Some question whether this practice increases mortality.
It is likely that it increases secondary VAP/HAP [ventilator-associated pneumonia/hospital-acquired pneumonia]. China has had a high rate of drug-resistant GNR [Gram-negative rod] HAP/VAP and fungal pneumonia in these patients, with resulting increases in mortality. We have seen none, even in the earlier patients who were vented for >10 days before being bronch’ed (prior to test availability. Again, it is not a great idea to bronch these patients now).
Unclear whether VAP-prevention strategies are also different [in China vs US], but wouldn’t think so?
Hong Kong is currently running an uncontrolled trial of HC 100IV Q8 [hydrocortisone 100 mg IV every 8 hours].
General consensus here (in US among doctors who have cared for COVID patients) is that steroids will do more harm than good, unless needed for other indications.
Many of our patients have COPD on ICS [inhaled corticosteroids]. Current consensus at Evergreen, after some observation & some clinical judgment, is to stop ICS if able, based on known data with other viral pneumonias and increased susceptibility to HAP. Thus far patients are tolerating that, no major issues with ventilating them that can’t be managed with vent changes. We also have quite a few on AE-COPD [acute exacerbation of COPD]/asthma doses of methylprednisolone, so will be interesting to see how they do.
8 notes
·
View notes
Text
Google Ads Management Ideas From Top 25 Experts

As an eCommerce store owner, most of your effort goes into creating and setting up a perfect PPC campaign. Once the campaign goes live, the chances of the campaign’s success lie in continuous monitoring and changes made to the campaign. The chances reduce drastically if it is not managed properly. Results could be even worse if it is mismanaged by some adwords account managed services.
Before you start the PPC Management process of your campaigns, you should consider the following important points.
Answers to these questions help you to get a clear idea about your business which in turn helps in creating better campaigns for your business.
Google Adwords management Ideas from Experts:
After setting up a google ads campaign and ad group, it needs to be optimized regularly to get the desired results. Optimizing all of your campaigns is the most complex task in Google Adwords. It means along with a lot of hard work, you should be able to extract actionable insights from data and be able to put those insights into action.
According to experts, the following are a few areas which they recommend you to concentrate on to optimize your campaigns and get desired results.
1.Keyword Managing ideas
Keyword selection is core to campaign performance. Better keyword selection leads to better campaign performance. More often than not, you would find out that your keywords are not performing as you had planned. The following are a few areas where you can investigate and optimize your keywords.
1.1- Poorly performing keywords
The first step regarding keyword Management is to find out those keywords which are generating clicks but not generating enough conversions. Reduce the bids to a smaller amount for these keywords to avoid too much ad spend. If the keywords do not convert at all, You might want to add them as negative keywords. It is better to use the budget elsewhere than spending it on non converting keywords.
AdNabu automates the above by automatically reducing bids for poorly performing campaigns during bid optimization. You only need to set a cost per conversion target and AdNabu will make changes automatically.
1.2 — Negative keywords
Next, you should concentrate on negative keywords. Negative keywords are those keywords using which you can avoid showing ads for irrelevant searches.
For example: If you are selling calendars, the online calendar keyword should not trigger your ad.
Make an extensive list of negative keywords. It is a best practice to keep updating your negative keywords regularly. Though it is a time-consuming activity, it is a very important factor in the success of the campaign. We highly recommend creating a shared negative keyword list so that it can be used for multiple campaigns.
AdNabu’s negative keyword tool automatically suggests negative keywords based on conversions. Our software will find keywords which are getting a lot of clicks but not resulting in any conversions (included in conversion tracking feature).
1.3 — New Keywords
You should also keep adding new keywords to your campaign. With continuous changes in your external environment (such as campaigns from competitors, changes in the economy or any other viral trends), you need to keep adding new keywords to be relevant with your audience. AdNabu’s long-tail keyword tool can automatically find long-tail variations of the keywords used by users in Google. But it is highly recommended to discover new keywords manually once in a while.
Working in the above-mentioned areas is just a starting point with respect to keyword optimization. Although time-consuming, the impact of these tactics is huge. You can automate most of the tasks if you are using AdNabu. In addition to AdNabu, we highly recommend you to look at campaign health once in a while.
2.Improving your google ads quality score
Google Adwords calculates a quality score for every single keyword in your account. The higher your keyword Quality Score, the better your ad positioning and lower will be the cost.
Quality score depends on click-through rates, ad relevance, and landing page experience. These parameters are evaluated by Google and a score gets assigned to every keyword. Although the exact way Google calculates quality score is still a mystery, Improving the CTR (which also increases return on investment), relevance, as well as landing page experience, can have a positive impact. We have created a guide to improving quality score.
It is important to have a good quality score which in turn helps in achieving better chances of success. One easy way to find opportunities to increase the quality score is to look for parameters which are average or below average.
3.Bid Managing ideas
Bid Management helps to minimize costs by finding the most effective keywords in your campaign and focusing on them exclusively.
To optimize your bids, you should identify the conversion rate of every single keyword. This data will then help you segregate high performing and low performing keywords. While manually optimizing campaigns, you can follow the simple rule of increasing bids for high performing keywords and reducing bids for low performing ones.
This task, however, is repetitive and error-prone. We highly recommend the bid optimization software by AdNabu which does all the heavy calculation automatically.
AdNabu only needs a number to optimize on (either the cost per conversion or the ROI), It can then do all the calculation down to keyword and device level to get maximum conversions out of your campaigns.
4.Ad Copy Management ideas
Ad copy plays the most important role in conveying your unique selling points to the consumer. The ad with high relevance leads to high click-thru rate and lower CPC automatically.
An expanded text ad consists of 2 Headlines, a Description line, and 2 URL paths along with the final URL. We will explore each of these parts of the ad copy and the ways to optimize them.
4.1. — Headline
Headlines are displayed prominently in Google Ads. They are usually the first line of the ad with a bigger font size. Both headlines can have a length of 30 characters each. Since this is one of the first things your prospective customer would be seeing, We highly recommend to include an attractive offer or service as one of the headlines.
One can also use dynamic keyword insertion to improve the relevance of ads. The ad text or part of it will be replaced by what the user is searching for while using this feature.
4.2 — Description line
Once you get the customer’s attention, the description lines convey the value proposition of the service or product. You can express the reasons why your product should be given priority over others here.
An 80 character limit gives description line the maximum ability to express the product or service in detail.
4.3 — URL Paths
Two URL paths now constitute display URL now along with the auto-generated domain name URL. URL paths need not be valid URLs and are simple to make the ad look attractive. There is a 15 character limit of URL paths and they are not compulsory unlike headlines and description line. We at AdNabu, highly recommend you to use URL paths as they increase the real estate of ads and make them more prominent.
4.4 — A/B testing of ad copy
A/B testing is nothing but comparing two versions of the ad to see which one performs better. You can do A/B testing with the complete ad or with a section of the ad. We at AdNabu recommend you to test things one at a time.
For eg: Test your 2–3 variations of Headline 1 or Test 2–3 variations of description line.
Doing multiple tests at the same time might not give you desired results easily as it takes much more time. Also, decide why you are doing an experiment. It can be to increase CTR or to increase conversion ratio but it cannot be both.
5.Usage of Google Ads Extensions
Extensions expand your ad with additional information-giving people more reasons to choose your business. They typically increase the click-through-rate of an ad by several percentage points. Extension formats include call buttons, location information, additional links, additional text, and more.
To maximize the performance of your text ads, Google Ads selects extensions to show in response to each individual paid search on Google. For that reason, it’s a good idea to use all the extensions relevant to your business goals. Some of the common extension used by businesses are listed below.
5.1 — Sitelink Extensions
Sitelink Extensions allow you to promote additional landing pages below your standard ad text. These sitelinks helps the users to directly land on the specific page of interest.
For eg: You main ad might lead the user to the homepage but a sitelink can directly take the user to a subcategory page.
Additional lines also give more real estate for the ad compared to your competition. This helps you stand out and get even more clicks.
5.2 — Call Extension
With call extensions, you can add your phone number to Google ads. This makes it easier for users to call your business, especially on mobile phones.
If you generate leads to your business through phone calls, it makes sense to have this extension for all your campaigns.
5.3 — Location Extension
Location extension helps the advertiser to add your business location address and phone number. This extension can be used by users to navigate directly to your business and can show helpful information like opening hours. It is highly useful for brick and mortar businesses like restaurants, salons, etc.
5.4 — App Extension
App Extensions allow you to add a mobile app download button next to your Search Ad. It attaches thumbnail icon, name and text below your main ad. This should not be confused with app install campaigns whose main aim is to drive installs and show up only on devices which are eligible to install them.
5.5 — Review Extension
Review extension helps advertisers to show reviews from google trusted websites. In order to use review extensions, you need to have reviews on reputable third-party sites like TrustRadius, TrustPilot, etc. The main point is that it has to come from a third-party site that’s well-known enough to get approved by Google.
6.Improved ad targeting Ideas
Targeting ads to ideal customers lead to better campaign performance and lead to the success of the campaigns. Geography and device play a major role in targeting your ads efficiently. An ad which works in city A might not work in city B. Below we will explore the ways to optimize your ad targeting based on geography and device.
6.1 — Optimization based on Geography
Ad performance varies with geographies due to multiple reasons. To optimize your campaign, you should review the campaign performance in each one of them.
You can go to the Dimensions tab, then click the View button and select “Geographic.” to see the campaign data based on geography.
Find out top-performing geographies which have the highest conversions and lowest cost per conversion. If you are getting leads from the geographies where you can’t serve, you should exclude those geographies from the campaign. You can also concentrate your top-performing geographies, reducing your spend on poorly performing geographies.
6.2 — Optimization based on Device
Increased consumption of mobile devices has lead advertisers to think about ad placement on various devices differently. Ad performance varies with the size of the device on which ad is delivered.
You would be able to see three categories, computers ( includes desktop & laptops), mobile devices with full browsers, Tablets with full browsers.
For example, If you find that the cost of conversion on tablets is significantly higher than mobile, you can adjust the bid in bid adjustment column and reduce your total costs. AdNabu automatically does device based bid adjustment for your campaigns once you have set it up in bid Management job.
Final words
Apart from the changes you make to your campaigns, there are many parameters that may impact your campaigns. For example, new products launched by your competition or a new substitute for your product/service or change in government regulation or sudden change in weather or local events may impact your campaign performance.
It is important to take those data points into consideration while analyzing your campaign performance. With a continuously changing environment, it is advisable to monitor and take steps to optimize your campaigns to get the best results out of your campaigns.
AdNabu was built to automate above mentioned and other mandatory tasks that help online advertising free up their time for other critical tasks of business. The tool helps every Pay Per Click advertisers to put your adwords campaign on autopilot and reduces the stress of managing large Google Ads accounts campaigns.
Source: Google Adwords management ideas - AdNabu
5 notes
·
View notes
Text
Mirror, mirror... Part 2

Mirror, mirror on the wall… I look in the mirror and I see my eyes. They are deep wells full of so much. I see the pain and suffering in my own eyes. I feel like I’ve been splayed out like a frog being dissected. I shared so much to the world. Now that it is all out, there is a possibility of peace in my mind. I’ve really nothing to hide. I’ve said most of it in the last blog entry. I didn’t mention financial hardships or the day to day issues that crop up for the average teacher, the average man just living his life the best that he can; sometimes succeeding, sometimes failing, but still plodding on in the hopes that something good will come of it. I had a doctor’s appointment today. I asked for a letter to have some time off to recover from my chemo pills. The doctor gladly accepted and so has my school. I can go and rest for a short week and take care of myself at the end of October. The reactions from yesterday’s blog has been mostly positive. People have responded in many kind ways and some, try to let me know that that they understand. Some have been so kind in their responses. A few questioned my emotional state, concerned that I may be at a breaking point. So why did I share all of that? Am I searching for someone to feel sorry for me? No, absolutely not. I bared my soul, took a good look at in the mirror and I am trying to be positive about the outcome. What do I want? Wow! So many things. Are they selfish to want or are they just the things that the average person needs or wants in their life? I’ve long forgiven my parents for thinking the way that they did. They came around and accepted some of my partners into their home and cared greatly for my success and tried to help the best that they could when I fell down. Some of my friends from high school told me that if they had known that I was gay, they would have supported me and stood by me to prevent the bullying. I was too busy hiding myself out of shame. I never stood in front of those ten bullies from school later in life. None of them know about the damage they caused, nor would they care if they did. I can leave them behind. I burned my year books years ago in an attempt to break away from them. I’ve met a lot of guys in my past. I’m not really proud of some of the things that I did, but I know one thing: I am who I am and I so much want someone to love me for who I am, not as how they think I should be! I’m going to be honest here; I find it hard to believe that there will be a man somewhere that could be that person for me. Sometimes I think that I have had too many tries in the relationship game and it is now game over. Sometimes I think that I am too old to keep trying. I’ve met some wonderful men in my past too! There are some, when I look back, might have been a wonderful partner, it I’d only seen it at the time. Regrets? Sure. Not all the men that I met were as I described: There have been a lot of caring men, kind men and giving men. Maybe I was too selfish to see what they were offering. So, maybe it is time to open my heart to the possibility to having it happen to me, even if I don’t always believe. I’ve had some nasty relationships. I’ve played a part in all of them, so I am not the shining hero or victim that has suffered through all of that. I was a part of it and I played my role. The only thing that I never did was to damage their self esteem by being selfish. I always tried to love each and every one of them, the best that I could - even if it almost destroyed me. I’ve survived HIV for over 30 years. I seroconverted in 1983. When I was tested in 1986, we traced it back to man in 1983 in Toronto. I found him later, on an AIDS memorial list in Toronto several years later. In all of my time, I never gave the virus to any man on purpose or by accident. I have had a 0 viral load for over 20 years and studies now say that someone like me can’t transmit the virus. No guilt for me to think that I may have converted someone else. I’ve lived through many pill cocktails and, thankfully, have been on stable medications for over 20 years now with no side effects. What was once considered a terminal syndrome is now a chronic one. I have to take pills for the rest of my life, but at least I won’t die from AIDS complications. Even the stigma is leaving, with Prep for those who are negative and pills to keep me healthy. Even the internalize homophobia is gone from my soul! I don’t feel guilty or dirty for being a gay man! Imagine me telling this story 20 or 10 or even 5 years ago! There would have been a lot of backlash. I’ve told everyone now. It’s no secret and I have neither something to hide nor shame for being so. I’ve had some nasty relationships. It seems that caregivers such as myself often attract narcissistic people because we are considered easy prey. Now that I look in that mirror, I see a man who knows who they are and what they can do. I’m not going to let it happen again. I’ve even had to say good bye to a few recently. At least I know the signs and can prevent it from continuing. I’ve learned from those bad relationships and I refuse to cause pain like that or allow that to happen to me again. Can I love again? I don’t know. Someone recently told me that I should start loving myself. I’ve done that for so many years and have found peace and love for myself time and time again. Sure, I have my times when things get really cloudy or sometimes downright bad. I wrote that last blog and to put it out there and then let it go the best that I can. On the subject of my cancer, I am moving forward. I’m almost at the halfway point. I’ve experienced fatigue, some body pain, headaches and now some nausea. I’m going to continue to the end of my treatment as best as I can. People around have been so kind in regards to my cancer diagnosis: My family doctor, my cancer nurse, the local pharmacists in Hubbards, the staff at school (especially my Vice Principal and Principal) and friends near and far. Yesterday, I wrote that the man in the mirror had great success at suffering and pain. The man on this side of the mirror is tired, but is still getting up and trying again and again. Maybe I can say that my Viking stubbornness sometimes pays off in my favour! I think that I am done self flagellating myself too. I can’t continue to blame myself for all the bad things that have happened. So, I look in the mirror and I see the other me standing on the other side. He’s grateful for his pain and suffering. He doesn’t have a problem; he lives for what he believes what his lot should be. Is there justice on this side of the mirror? I think so. I am thankful for having experienced the pain and suffering so that I can move past it and become a whole person. I’m going to feel many things in the next while: loneliness, sadness, and maybe other peoples’ ignorance to what is going on in my head. I think that I am also going to experience happiness, joy, self love; love for friends and family; love from so many people, and maybe one day… one day… a man may come along to love me with all his heart as I would love him. I’m no hero. I can be strong and I can be weak. Even though there is a constant battle being fought, at least I can see that the light at the end of the tunnel is something for which the fight is worth! I wrote earlier about what I want in life. I don’t have to spell it out. It is written in the lines of this blog or in between them. I’ll keep fighting and keep being me. I want a happy life. Thank you, everyone for sharing your love, concern and even your misunderstandings. You’ve all helped me so much more than you know.
2 notes
·
View notes