#benzylpenicillin
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Average visit duration of Tumblr.com is 10 mins and 25 secs.
Text

Etest
“Etest being used to determine the susceptibility of Neisseria gonorrhoeae to benzylpenicillin.” - via Wikipedia
#the commons page didn’t have a description so i pulled this one from the article itself. seemed best to put a caption on this one.#wikipedia#wikipedia pictures#wikimedia commons#medicine#medicalcore#medcore#medicore#medical aesthetic#labcore#stemcore#laboratory aesthetic#science#antibiotic resistance#antimicrobial resistance#bacteria#microbiology#Neisseria gonorrhoeae#N. gonorrhoeae#neisseria#infectious diseases#etest#Epsilometer test#antibiotic sensitivity test#antimicrobial sensitivity#benzylpenicillin#penicillin g#peng#benpen#antibiotics
21 notes
·
View notes
Text
Oropharyngeal primary syphilis by Dr Louis Noël in Journal of Clinical Case Reports Medical Images and Health Sciences
A 48-years-old healthy male was referred to our tertiary care center from an otorhinolaryngologist. The patient complained of odynophagia for the last 4 months, without any history of smoking nor chronic alcohol intake. A biopsy was performed and diagnosed chronic inflammation with fungal mycelia. Oral fluconazole did not bring any improvement.
Upon arrival, the examination shows some granular and erythematous pharyngeal lesions (Figure 1). A diagnostic work-up with local biopsies and serologies was done.
The PCR came back positive for Treponema pallidum (negative for herpes virus, chlamydia, and gonorrhea). Syphilis serologies were also positives (VDRL titer, 1:8; TPHA titer 20’480). The patient received one intra-muscular benzathine benzylpenicillin injection (2.4 million I.U.). The odynophagia and the lesions disappeared within 48 hours (Figure 2), without relapse for over two years.
Syphilis should be considered in every acute and chronic pharyngeal lesion, as oral sex may not be disclosed upon first medical consultation.
We declare no conflict of interest nor funding source. We obtained the patient’s written consent for the publication of this case report.
#Oropharyngeal primary syphilis#odynophagia#Oral fluconazole#jcrmhs#Journal of Clinical Case Reports Medical Images and Health Sciences submissions#Clinical decision making#Clinical Images journal
3 notes
·
View notes
Text
Listeria
For whatever reason it reminds me of Desperate Housewives and Wisteria lane. Or just Wisteria in general.

It's unfortunately it's anything but wistful or romantic.
This is inspired by the netflix series Poisoned. I hate that title but it's a great watch. I learned a lot from it. I highly recommend it particularly for medical students and residents etc.
So, listeria are gram positive rods (most bacilli are negative) making this relatively easier to remember (purple rods). Also catalase positive. IT's also a facultative anaerobe - so both cultures may be positive (aerobic and anaerobic bottles).

the species that is the culprit for major human pathogens is Listeria monocytogenes.
At increased risk groups (more likely to die of Listeriosis) - the immunocompromised and extremes of life, including the elderly, pregnant women and neonates. Immunocompromised: HIV, anyone on long term highish doses of steroids, leukaemia/oncology patients etc. Worryingly, incubation time is 3-90 days in these groups, so it's difficult to really trace or keep track of. Pregnant women are at 20x higher risk of acquiring the severe form.
Source: CDC

Hence why during pregnancy you're advised not to consume raw salads, fruits, cold cuts, soft cheeses, sprouts and smoked salmon or sushi, no mayo and no raw egg (definitely no raw milk) etc. Similarly, common recommendation is you serve none of these to children under the age of 1. It naturally lives in soil (hence avoidance of raw sprouts) and can live in animals. So it can frequently contaminate food.
Image Source: SA Health

As with COVID (I can't believe I'm using COVID as a measure of things), it can cause mild food borne illness (nausea, vomiting diarrhoea, myalgias, even fevers) to invasive disease causing sepsis and even meningitis or encephalitis. Incubation time is a few days in the mild form.
IMage source:
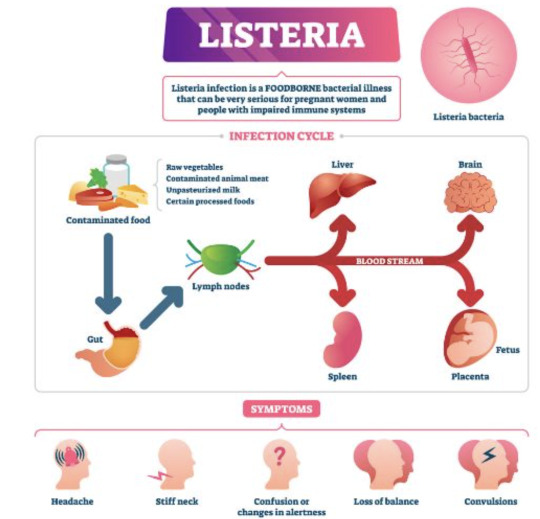
Death by Listeria when you have the severe form (Listeriosis) is 20%, astonishingly high given you have a 1% chance of dying from Salmonella.
It's a small risk but the issue is that complications and fatality if you do acquire is high. It's also highly preventable, but the challenge is food safety and avoiding certain foods as a consumer.
i.e. in pregnancy, most will have diarrhoeal illness that's mild. But in the subset that get invasive disease and really unwell, there's a 20% risk of miscarriage, risk of premature labour and risk of still birth at 3% in the US. In the states, pregnant women are also 10x more likely to get Listeria infection. That is, illness after exposure.
On the final note of prevention, also always properly refridgerate food to 4 degrees celsius and cook meat to 165 fahrenheit or 73 degrees celsius. As I've learned from the Poisoned documentary, you can ask restaurants to do this, ask them to use an internal thermometer to measure - as rare/medium rare etc have no meaning as it pertains to food safety. If they can't, order something else.

With meningoencephalitis, we just presume that Listeria is a possibility and treat empirically while awaiting investigations.
Investigations: - CSF (lumbar puncture) in event of signs of meningism or encephalitis (classic headache/fever/stiff neck/rash and/or acute confusion or seizure AND fevers) --> expect the classic features of bacterial meningiits and gram stain positive for purple rods - PCR - stool cultures have no value - blood cultures--> look for gram positive rods in the preliminary findings, expect a call from the lab Empirical therapy: - none in asymptomatic or mild disease. just monitoring until symptoms resolve and supportive care (fluids etc.) - Listeria is a notifiable disease to the health department in most Western countries that keep track of outbreaks. - in the US, standard treatment is ampicillin. - in Australia at least, standard therapy is IV benzylpenicillin, 2.4 g 4 hrly in meningitis or encephalitis and everyone is just started on this until bug identification/gram staining and sensitivities return. - in hypersensitivity, bactrim is used. - cephalosporins have no activity against them (or "inherently resistant), hence you can see IV ceftriaxone and benzylpen in the drug regimen for empirical therapy of meningitis - cef covers gram negatives, strep pneumo (most common cause of meningitis) and neisseria meningitidis - duration of therapy in severe disease: 3 weeks, 6 weeks if immunosuppressed
Really great summary here.
Random historical trivia
listeria is named for Dr. Joseph Lister, a British surgeon who introduced sterilisation of equipment and antiseptics to surgery, improve post op care and observed that microbes are the cause of cases of poor wound healing or post op infections. he also began to look at them under the microscope as an early pioneer of bacteriology.

Lister's father by the way, made compound microscopes for a living, so lister became proficient at using this and started publishing articles during medical school
this also led to a lot more research on inflammation and coagulation
weirder trivia: in his med school days, surgeons commonly did not wash hands between patients and some didn't even change gowns, glorifying how busy they where by how many stains were on it by the end of the day
so unsurprisingly his early battles to pioneer antiseptics and aseptic techqniues to prevent the transmission of infection in surgical patients were pretty uphill
Resources CDC guidelines WHO guidelines FDA Statpearls --> great at covering basic physiology and pathology etc. in a short form. Australian therapeutic guidelines - unfortunately not free.. so won't bother to link. If you work at any large-ish Australian hospital you'll have 'free' access. Wikipaedia US list of outbreaks CDC recommendations on foods to avoid vs okay to eat to avoid Listeria
7 notes
·
View notes
Text
Alexander Fleming was born on August 6, 1881. A Scottish physician and microbiologist, best known for discovering the world's first broadly effective antibiotic substance, which he named penicillin. His discovery in 1928 of what was later named benzylpenicillin (or penicillin G) from the mold Penicillium rubens is described as the "single greatest victory ever achieved over disease". For this discovery, he shared the Nobel Prize in Physiology or Medicine in 1945 with Howard Florey and Ernst Boris Chain. Fleming was knighted for his scientific achievements in 1944. In 1999, he was named in Time magazine's list of the 100 Most Important People of the 20th century.
#alexander fleming#antibiotics#penicilln#medicine#nobel prize#nobel prize winners#science#science history#science birthdays#on this day#on this day in science history
14 notes
·
View notes
Text
Funguary 2024 Day 7
☁️ Week 1: Celestial 🧽 Penicillin

He/him
This guy is a future doctor, and he is currently investigating the cause of mold and green spots on his body. Maybe he can use it in medicine.
I indicated benzylpenicillin by mistake, but I think it's no big deal.
Previous day 🍄 Next day 🍄 All days
5 notes
·
View notes
Text
Antibiotika


Bakterizide Wirkung
= Töten Bakterien ab über Hemmung d. Zellwandsythese
Betalaktame
Penicilline
Penicillin G (=Benzylpenicillin-Procain) - Schmalspektrum
Ampicillin (Aminopenicillin) - Breitspektrum
Amoxicillin (Aminopenicillin) - Breitspektrum
Caphalosporine
Ceftiofur (3. Generation) Reserveantibiotikum
Cefquinom (4. Generation) Reserveantibiotikum
Betalaktaminhibitoren
Clavulansäure
Polypeptidantibiotikum
Polymyxin E (=Colistinsulfat) Reserveantibiotikum
Bakteriostatische Wirkung
= hemmt Wachstum u. Vermehrung von Bakterien
Aminoglykoside
hemmen die Proteinsynthese
Gentamicin
Dihydro-Streptomycin
Neomycin
Paromycin
Apramycin
Spectinomycin
Tetrazykline
hemmen die Proteinsynthese
Doxycyclin
Oxytetrazyklin
Chlortetrazyklin
Makrolide
hemmen die Proteinsynthese Reserveantibiotika
Tylosin
Tulathromycin
Tildipirosin
Tilmicosin
Phenicole
hemmen die Proteinsynthese
Florfenicol
Pleuromutiline
hemmen die Proteinsynthese
Tiamulin
Valnemulin
Lincosamide
hemmen die Proteinsynthese
Lincomycin
Flourquinolone
= Gyrasehemmer Reserveantibiotika
Enrofloxacin
Marbofloxacin
Danofloxacin
Sulfonamide
= Hemmen die Folsäuresynthese
Sulfamenthoxazol
Sulfamidin
Sulfadoxin
Sulfadiazin
Trimethoprim
= hemmt die Folsäuresynthese

0 notes
Text

Pharmacology MCQ Question 227:- Question Link- https://examobjective.com/pharmacological-nursing-mcq-set-29/ The drug used by health workers in the management of acute respiratory illness is
(a) Cotrimoxazole (b) Chloramphenicol (c) benzylpenicillin (d) gentamycin
0 notes
Link
1 note
·
View note
Text
What Is Antibiotic Resistance and Why Is It Important?

Antibiotic resistance is also known as antimicrobial resistance (AMR) and represents one of the biggest threats to public health and development in the world. Bacterial AMR was responsible for an estimated 1.27 million deaths globally in 2019 and contributed to a further 4.95 million deaths.
The main drivers behind the development of drug-resistant pathogens are the overuse and misuse of antimicrobials in plants, animals, and humans.
What Are Antimicrobial Resistant Bacteria?
Antimicrobial resistant bacteria are bacteria that aren’t killed or controlled by antibiotics. They can both survive and multiply even when an antibiotic is present. While many types of bacteria that cause infections can gain resistance to some antibiotics, bacteria that’s resistant to many antibiotics are termed multi-resistant organisms (MROs). Furthermore, some types of bacteria have a natural resistance to antibiotics; for example, benzylpenicillin has little effect on most bacteria present in the human gut.

The Devastating Effects of AMR
AMR is responsible for a huge global death toll, and one that is likely to increase unless action is taken. While inequality and poverty exacerbate its consequences and effects, AMR impacts all countries, although middle and low-income nations are most affected. As well as making it harder to treat infections, it makes undertaking many other treatments significantly riskier.
As well as the devastation of disability and death, AMR comes with a huge economic cost, with the World Bank estimating that it could result in around $1 trillion to $3.4 trillion worth of GDP losses per year by 2030 and $1 trillion in additional healthcare costs by 2050.
youtube
How Can the AMR Challenge be Tackled?
Those with experience in this field – such as Alec Simonson, who was involved in bioinformatics and neuropharmacological research during his studies – know that one of the most important ways to prevent AMR is to use antibiotics properly. This means reducing the overprescribing of antibiotics and preventing unnecessary use. It’s also important that patients complete the entire course of any antibiotics they are prescribed so the medication will be fully effective and not promote resistance. Good hygiene (such as handwashing) and the deployment of appropriate infection control procedures will also play a key role in tackling AMR.
The Global Action Plan (GAP) on AMR was adopted by countries during the 2015 World Health Assembly. Adoptees committed to developing and implementing multisectoral national action plans to tackle AMR, using a One Health approach.
For information about World AMR Awareness Week, take a look at the embedded PDF.

#Alec Simonson#AMR#Antibiotic Resistance#world health organization#who#healthcare#health and medicine#bacteria#effects of amr#Antimicrobial Resistant Bacteria#Youtube
1 note
·
View note
Text

Isaac took the time to read her questions carefully. Once he was done, he opened her file, offering her a polite smile. He was not planning on lying to her, not about that at least. "It might not make a lot of sense to you, but I can tell you what we found in your blood. We found traces of Ciprofloxacin, Benzylpenicillin and Tetracycline. Those are antibiotics, and can actually make you ill when taken that way."

"We also found traces of alprazolam and diazepam, strong anxiolytics that were meant to keep you sedated. Now, If there is something you don't understand, you can tell me."
⋆ ˚。⋆୨୧˚ she follows him back to the desk , taking a seat across from him like she had done the first day she got here. it had the same chill to it as she felt then , but that could be the whole of the hospital , and it could also be from how tired she was that she could not get warm. she didn’t pay it much mind , she just let it be. when he assures her she can ask about his own well being , she smiles. “ o —- okay , t —thank y — you. “ she is aware he has to be more invested in her well being since this is a hospital , but she could not help but ask. she clasps her hands , settling them in her lap , waiting his response. ⋆ ˚。⋆୨୧˚
#he's not sugar coating it lol#&(valerie)#isaac (oh now you want to talk to god?)#read at your own discretion#drugging tw#dcmur3
61 notes
·
View notes
Text
Discovery Of Penicillin
penicillin, perhaps the earliest despite everything quite possibly of the most generally utilized anti-toxin specialist, got from the Penicillium form. In 1928 Scottish bacteriologist Alexander Fleming originally saw that states of the bacterium Staphylococcus aureus neglected to fill in those region of a culture that had been coincidentally tainted by the green form Penicillium notatum. He secluded the form, developed it in a liquid medium, and found that it created a substance fit for killing a large number of the normal microbes that taint people. Australian pathologist Howard Florey and English natural chemist Ernst Boris Chain separated and cleansed penicillin in the last part of the 1930s, and by 1941 an injectable type of the medication was accessible for helpful use.
Discovery Of Penicillin
Have some familiarity with penicillin's revelation by Alexander Fleming and advancement by Ernst Chain and Howard Florey and its outcome in treating the injured in The Second Great War Have some familiarity with penicillin's revelation by Alexander Fleming and advancement by Ernst Chain and Howard Florey and its outcome in treating the injured in Universal Conflict IISee all recordings for this article The few sorts of penicillin blended by different types of the shape Penicillium might be separated into two classes: the normally happening penicillins (those framed during the course of form maturation) and the semisynthetic penicillins (those wherein the construction of a compound substance — 6-aminopenicillanic corrosive — found in all penicillins is changed in different ways). Since it is feasible to change the qualities of the anti-microbial, various kinds of penicillin are delivered for various helpful purposes.
The normally happening penicillins, penicillin G (benzylpenicillin) and penicillin V (phenoxymethylpenicillin), are as yet utilized clinically. In light of its unfortunate security in corrosive, quite a bit of penicillin G is separated as it goes through the stomach; because of this trademark, it should be given by intramuscular infusion, which restricts its value. Penicillin V, then again, commonly is given orally; it is more impervious to stomach related acids than penicillin G. A portion of the semisynthetic penicillins are likewise more corrosive stable and consequently might be given as oral prescription.
All penicillins work similarly — specifically, by restraining the bacterial catalysts answerable for cell wall amalgamation in recreating microorganisms and by enacting different proteins to separate the defensive mass of the microorganism. Thus, they are viable just against microorganisms that are effectively imitating and delivering cell walls; they likewise hence don't hurt human cells (which essentially need cell walls).
A few kinds of beforehand defenseless microbes, like Staphylococcus, have fostered a particular protection from the normally happening penicillins; these microorganisms either produce β-lactamase (penicillinase), a chemical that upsets the inner construction of penicillin and in this manner obliterates the antimicrobial activity of the medication, or they need cell wall receptors for penicillin, extraordinarily lessening the capacity of the medication to enter bacterial cells. This has prompted the development of the penicillinase-safe penicillins (second-age penicillins). While ready to oppose the action of β-lactamase, be that as it may, these specialists are not as successful against Staphylococcus as the regular penicillins, and they are related with an expanded gamble for liver harmfulness. Besides, a few types of Staphylococcus have become impervious to penicillinase-safe penicillins; a model is methicillin-safe Staphylococcus aureus (MRSA).
extreme touchiness to penicillin extreme touchiness to penicillin Penicillins are utilized in the treatment of throat contaminations, meningitis, syphilis, and different diseases. The central symptoms of penicillin are touchiness responses, including skin rash, hives, enlarging, and hypersensitivity, or unfavorably susceptible shock. The more serious responses are phenomenal. Milder side effects might be treated with corticosteroids yet typically are forestalled by changing to elective anti-toxins. Anaphylactic shock, which can happen in recently sharpened people inside the space of seconds or minutes, may require quick organization of epinephrine.
0 notes
Text
makes me laugh every time i hear a doctor call benzylpenicillin benpen
0 notes
Photo




#BENZYLPENICILLIN = #PENICILLIN G injectable
Powder for injection in vials of:
1 MIU (600 mg), to be dissolved in 2 ml of water for injection or 0.9% sodium chloride
.
.
5 MIU (3 g), to be dissolved in 5 ml of water for injection or 0.9% sodium chloride
For IM injection or slow IV injection through an infusion tube (3 to 5 minutes) or infusion (60 minutes) in 0.9% sodium chloride or 5% glucose.
.
.
Dosage: Severe leptospirosis
Child: 50 000 IU (30 mg)/kg (max. 2 MIU or 1200 mg) by IV injection every 6 hours
Adult: 1 to 2 MIU (600 to 1200 mg) by IV injection every 6 hours
Neurosyphilis
Adult: 2 to 4 MIU (1200 to 2400 mg) by IV injection every 4 hours
Congenital syphilis
50 000 IU (30 mg)/kg by IV injection every 12 hours from D1 to D7, then
50 000 IU (30 mg)/kg by IV injection every 8 hours from D8 to D10
Duration: Severe leptospirosis: 7 days
Neurosyphilis: 14 days
Congenital syphilis: 10 days
.
.
Remarks: Do not confuse short-acting benzylpenicillin, administered several times a day by IV route, with long-acting #penicillins (#benzathine benzylpenicillin and #procaine benzylpenicillin) administered by IM route only.
Do not mix with other drugs in the same syringe or infusion.
Storage:– – Below 25 °C
Once reconstituted, suspension must be used immediately.
0 notes
Link
0 notes
Text
Kokzidiose (Huhn)
= Eimeriose
Erreger: 7 verschiedene Eimerienarten kommen beim Huhn vor E. acervulina E. burnetti E. maxima E. mitis E. necatrix (sehr pathogen) E. praecox E. tenella (sehr pathogen): Erreger rote Kükenruhr
ubiquitäres Vorkommen, streng wirtsspezifisch Oozysten sehr widerstandsfähig, Elimination mittels geeigneter Desinfektionsmittel (zB Kresole) u. korrekter (langer) Einwirkzeit !Wichtige Wegbereiter f. bakterielle Sekundärinfektionen va. Clostridium perfringens (Verursacher nekrotisierende Enteritis), e.Coli!
Übertragung u. Lebenszyklus
Ausscheidung unreifer Oozysten mit dem Kot
Sporulation in Außenwelt -> infektiös und sehr widerstandfähig
Orale Aufnahme (Futter/ Wasser)
Präpatenz: 4-7 Tage (variiert je nach konkreter Art) Ausscheidung stoppt nach wenigen Tagen von selbst Es kommt zu einer Immunität nach mehrmaliger Reinfektion mit geringen Mengen (meist in 3.-4. LW)!
Symptome: va. Jungtiere sehr anfällig Erstinfektion meist symptomlos -> erste Anzeichen zw. 3.-6. LW meist Mischinfektionen: vorherrschende Art bestimmt Krankheitsbild
vermindertes Allgemeinverhalten (tw. bis Somnolenz), ungepflegtes Gefieder, hängende Flügel, eingezogener Kopf
erhöhtes Wärmebedürfnis -> Gruppenbildung
verminderte/ vollkommen fehlende Futter-/Wasseraufnahme -> Exsikkose
aufgekrümmter Rücken
Auseinanderwachsen, schlechte Futterverwertung, Leistungsdepression
erhöhte Mortalität
E. tenella: braunroter Kot, verschmutze Kloake
E. burnetti: massiver Durchfall, Exsikkose
ev. Anämie (va E. tenella u. necatrix)
Diagnose
Sektion:
leichte bis hgr. Darmentzündung charakteristische Läsionen je nach Art:

Mikroskopischer Erregernachweis:
Entwicklungsstadien in oberflächlichen/ tiefen Darmschichten nachweisbar mittels Schleimhautabstrich
Kot- od. Einstreuproben
Bestimmung d. konkreten Eimerienart mittels Lokalisation im Körper, Art d. Läsionen ev. computerunterstützt (zB mit COCCIMORPH online)
Prophylaxe
Ziel: Aufbau einer Immunität
Lebendimpfstoff -> verdrängt pathogene Feldstämme Auch attenuierte Impfstoffe erhältlich Übers Trinkwasser od. als Spray bereits in der Brüterei !Puten: KEIN attenuierter Impfstoff verfügbar!
Kokzidiostatisch wirksame Futterzusatzstoffe (va. in Junghuhn- u. Putenmast)= Metaphylaxe (Achtung: Resistenzen! -> regelmäßiger Wechsel v. Präparaten) zB Sulfonamide, Ionophoren !NICHT in Kombination geben! !Sulfonamide nicht bei Legehennen! !Ionophore können Myopathien u. Lähmungen verursachen!
Senken d. Infektionsdrucks: Reinigung u. Desinfektion, häufiges Nachstreuen u. Misten, Umtreiben !Oozysten werden SEHR leicht verschleppt -> komplette Eimerienfreiheit eig unmöglich!
Therapie
!Für Legehennen sind KEINE Therapeutika zugelassen! Kokzidiose= selbstlimitierende Krankheit, adulte Tiere weniger anfällig -> Anstreben einer natürlichen Durchseuchung mit Immunitätsausbildung
wasserlösliche Antikokzidia (zB Toltrazuril) + Benzylpenicillin bei Puten -> Vorbeugung nekrotisierender Enteritis
Unterstützende Gabe v. Vit. A/E und appetitfördernden pflanzlichen Präparaten
Nachbehandlung gegen bakterielle Sekundärinfektionen bei Bedarf
0 notes
Text
Syphilis!
Syphilis is caused by Treponema pallidum. This is a spirochaete, with a low reflective index, and it is motile using its spiral shape to propel itself (it has internal flagella attached to the cytoplasmic membrane). It is too thin to visualise with gram staining, but it can be viewed using dark-field, electron, Steiner silver stain and fase-contrast methods.
Treponema palladium can also cause Yaws (burrows under the skin), Pinta (hyperkeratosis) and Bejel (much more like syphilis, but not an STI; spread using same cooking utensils).
There are 3 stages of syphilis:
Primary: Chancre: immune response causes tissue degradation without pain, which eventually disappears.
Secondary: 6-8 weeks after infection, patients present with generalised malaise and rashes, even palmar rashes. This is systemic.
Tertiary: after 3-30 years of a latent period, symptoms can reappear, including gummas across body/tongue (do not contain many bacteria cells, mainly an immune response), cardiovascular/meningovascular lesions (leading to aneurisms/strokes), and ‘general paresis of the insane’, aka neurosyphilis (hypersensitivity in the brain).
Lesions from syphilis often allow secondary infections to occur, such as S. aureus.
Spread:
Syphilis spreads HORIZONTALLY as an STI or via contaminated blood. It spreads VERTICALLY as congenital syphilis.
Congenital syphilis is typified with Hutchinson’s teeth, Sabre teeth, bone lesions and neurosyphilis; however it can present anywhere between 5-25 years old. The mother should be treated prophylactically if there is a risk.
Diagnosis:
Using exudate/biopsy from chancre.
Using serology to identify reagin, an antibody produced during body damage, using VDRL/RPR testing. FTA serology finds antibodies specific to T. pallidum. These tests rely on antigen and antibody complexes binding to an anti-human antibody which is conjugated to a fluorophor at the FAB region for visualisation.
It is found highest between the ages of 20-40, and is higher in men: 9:1. It mostly affects men who have sex with men. Education around HIV and AIDS also decreased the incidence.
Treatment:
Benzylpenicillin or a macrolide (bacteriostatic, such as the new azithromycin) are used to block the peptide exit tunnel of T. pallidum’s 50S ribosomal subunit.
Old treatments: Mercury, salvarsan, malaria (increases temperature beyond limits of the bacteria), and penicillin.
1 note
·
View note