#anterior jugular veins
Text
Louis’ Anterior Jugular Veins appreciation post










I think I’ll update this post every once in awhile
#Louis’ AJV#you dont understand how much im obsessed with them#i wanna kiss gently 🫠#respectfully staring at the first pic#the tattoo picking out makes my knee weak#anterior jugular veins#do not confuse with external jugular which is more common to see#his veins are very superficial#ltwt#all pictures from#dailytomlinson
160 notes
·
View notes
Text
Ivan’s neck scar
(Cw: mentions of decapitation, mentions of attempted s*icide, violent historical events and mental health issues)
So in case this is new information, Ivan Braginsky does in fact have a scar around his neck

(not the best image but it’s there under the neck bandages, I promise)
It’s not yet been revealed when or how he got that scar but it’s there and Ivan seems to not what people to see it, much less talk about it. That leads me to believe that whatever happened was a very traumatic incident for him which leads me to a few theories.
Mongolia or Tatarstan attacked Ivan when he was a child.
When a very young Ivan first meets a very young Tolis, he explains to him that living under Tatar is very difficult and that he wants to become a crazy strong country soon so he is no longer under their control. There’s even a brief moment where you can see blood on Ivan’s hands, and maybe even on his clothes, implying he has to fight everyday just to survive till the next day. It’s very possible that Ivan tried to rebel a few times. Given that at the time he was a very small child, neither of the aforementioned older nations probably punished him too severely but I can see a situation where they got fed up with Ivan’s rebellious attitude and either completely or partially decapitated him as a way to show him who was stronger and that if he kept rebelling, they’d do worse.
Either Feliks or Tolis tried to decapitate him.
Both Lithuania and Poland we’re having wars with Russia/the Soviet Union starting in the early 1900s and some of the battles got really intense so there might have been an intense fight between 2, or even all 3, parties involved and one of them struck a deadly blow to Ivan. Tolis in particular is stated to be a very disciplined and competent combatant so I’m definitely leaning more towards the idea that in the heat of the battle, Tolis either particular or completely decapitated Ivan.
A human attacked Ivan during one of the many revolutions that occurred in Russia’s history.
I specifically think Ivan was attacked during the attack knows as “Bloody Sunday”(St. Petersburg January 22, 1905). We see time and time again in the anime and Manga, especially with Russia, that nations have to follow their bosses orders to the letter even if they personally don’t agree with what they’re bosses are doing. He was most likely ordered to join the imperial forces and shoot his citizens, some of whom did try to fight back before dying. I don’t think they fought back enough to go too deep, but I do think the human who attacked him most likely picked up some scrap metal and at the very least cut through his exterior and anterior jugular veins.
He’s done it to himself…multiple times
You don’t live through some dark times and come out unscathed. His history has canonically caused psychological damage to Ivan’s psyche that persists into modern day. It’s very likely that living through so much traumatic history would leave him with depression and PTSD at minimum. He has more than likely tried, on multiple occasions, to end his suffering by attempting to take his own life but has never succeeded because of his immortality.
Whatever the cause, I definitely think it’s caused physical issues such as his voice being as high pitched and airy as it is. He sounds very young and childish, as if his vocal cords didn’t develop properly once he hit puberty. He’s capable of deepening his voice but he has to actively force it, such as when he’s mad and wants to sound intimidating/threatening or during character songs when his voice slips into a deeper tone when he’s actively forcing his voice. When he laughs it’s a very airy “ufufuf” sound. That might also be due to vocal damage and if he’s ever in a situation where he’s laughing so hard, he’s holding his sides, he’ll most likely have an eerily silent laugh where he only makes noise when his trying to take air into his lungs. I also imagine neck is very sensitive and he doesn’t allow people to touch him there unless he absolutely trusts them with his entire being. Swallowing might also be a problem for Ivan, especially if he’s eating very hot food.
Of course he also has some self esteem issues because of his neck scar. Looking at it makes him feel ashamed because it’s a reminder that he was weak enough to let someone hurt him. It’s also a reminder that people didn’t like or trust him in the past so he thinks that’s still true. It’s a scar that reminds him of all that he has suffered and of all the people who have hurt him, it’s a reminder that he’s survived over 1,000 years of hell on earth.
#hetalia#aph Russia#hws Russia#Ivan Braginsky#aph lithuania#hws lithuania#tolys laurinaitis#aph poland#hws poland#feliks łukasiewicz#aph mongolia#hws mongolia#cw: decapitation#cw: attempted suicide#cw: war#cw: historical violence#Ivan’s really gone through some shit
25 notes
·
View notes
Text
Veins of the Upper Extremity: Part Two
Divided into two parts: Deep (running next to arteries) and Superficial (right beneath the skin). The deep veins have more valves than the superficial veins.
Deep Veins
Interosseous veins
next to interosseous arteries
anterior interosseous veins start in front of the wrist
connect to deep radial and ulnar veins
anterior interosseus veins join to posterior interosseous veins at top of forearm
Deep palmar veins
connect to deep ulnar veins on inside of hand
end in radial artery on outside of hand
join to deep radial veins by thumb
Brachial veins
one vein on each side of brachial artery
join axillary vein at bottom of subscapularis
Axillary vein
large vein
is the continuation of the basilic vein
starts at border of teres major and latissimus dorsi tendons
gets bigger as it continues upwards
ends just below clavicle, becoming subclavian vein
covered in front by pectoral muscles
partially overlaps axillary artery
connects to cephalic vein near its end
Subclavian vein
continuation of axillary vein
runs from outer end of first rib to inner end of clavicle
joins internal jugular to make innominate vein
sits on pleura
sometimes comes level to subclavian artery in neck
usually has valves an inch from its end near external jugular vein
Innominate/Brachio-cephalic veins
one on each side of neck
are joining of internal jugular veins and subclavian veins
no valves
Internal mammary veins
two for each artery
follow where artery goes
connect and end in innominate vein
Inferior thyroid veins
often three or four
start in venous plexus of thyroid body
create plexus in front of trachea behind sterno-thyroid muscles
left vein joins left innominate
right vein opens where right innominate meets superior vena cava
have valves where they connect to innominate veins
Superior intercostal veins
drain blood from intercostal spaces
right vein joins vena azygos major
left vein joins left innominate vein
Superior vena cava
gives blood to heart from upper part of body
starts below cartilage of first rib near sternum
ends in upper part of right auricle
curves slightly to right
Azygos veins
connect superior vena cava and inferior vena cava together
vena azygos major sits on right side and starts in branch of right lumbar veins
vena azygos minor sits on left side and starts in branch of lumbar veins or left renal vein
[Gray, H. 2010, Gray's Anatomy, 15th Edition, Barns & Noble, Inc., New York. pp 587-590.]
#raz anatomy#anatomy#veins#circulatory system#upper veins#medblr#studyblr#not med student just interested#blood-vascular system#study#studying#medicine#medical#biology#gray's anatomy book
4 notes
·
View notes
Text
Explained - Secondary assessment: Trauma
Secondary assessment: Trauma
During a full-body trauma assessment, you are looking for
Deformities, Contusions, Abrasions, Punctures/Penetrations, Burns, Tenderness, Lacerations, Swelling (DCAP-BTLS)
HEAD
Scalp: Examine for any bleeding or DCAP-BTLS by palpating the skull
Ears: Look inside the ear for any blood or CSF, behind the ears for Battle’s signs, palpate the mastoid process
Eyes: Palpate the orbital bones, look for raccoon eyes, determine pupil size and reaction with pen light
Facial areas: Palpate the mandible and maxilla
Oral: Look inside the mouth for any fluids or foreign objects
Nasal: Palpate the bridge of the nose and look inside for any fluid or foreign objects
NECK
Posterior: Palpate cervical spine for step-off
Anterior: Look for tracheal deviation
Lateral: Look for jugular vein distention
*Make sure to palpate the cervical spine prior to applying a c-collar *
CHEST
Inspect: Look for flail chest, sucking chest wounds, unequal respirations, etc.
Palpate: Clavicles, shoulders, sternum, ribs
Auscultate: Lung sounds
ABDOMEN
Palpate: All four quadrants separately with flat palms in a rolling motion
Inspect: Do you note any pulsating masses/rebound tenderness/swelling?
PELVIS
Palpate: Push inwards then downwards, noting any instability
*If you feel any instability when you push inwards, DO NOT PUSH DOWN*
GENITALS
Verbalize: Checking genitalia with palm facing upward
EXTREMITIES
Palpate: Palpate the entire extremity from most proximal joints downwards. Use a cup-like motion with your hands to feel both the anterior and posterior sides.
Pulse: Radial/dorsalis pedis/posterior tibial
Motion: Test your patient’s ability to squeeze, push, pull, or wiggle fingers/toes
Sensation: Can the patient feel and differentiate between which hand/foot is being touched
POSTERIOR:
Palpate: The posterior spine looking for step-off, instabilities, or deformities
*Make sure to palpate the spine prior to rolling a patient onto a backboard*
Management of secondary injuries: Bleeding control, splinting, full spinal immobilization, etc.
3 notes
·
View notes
Text
Structures in the Anterior Median Region of the Neck
Structures in the Anterior Median Region of the Neck
Skin
Superficial fascia
Decussating fibres of platysma
Anterior jugular Vein
Jugular venous Arch
Submental Lymph Nodes
Terminal part of transverse Nerve
Deep fascia
Investing layer
Above hyoid bone — splits to enclose submandibular gland
Below splits to enclose suprasternal space
Deep structure above hyoid bone
Mylohyoid muscle
Anterior belly of digastric
Superficial part of…

View On WordPress
0 notes
Photo

bone chip
100 notes
·
View notes
Text
TENSION PNEUMOTHORAX MULTI-ASK
Hey there lovelies! Thanks so much for your asks!
First off, basics: check the ( thoracic trauma ) tag and the ( pneumothorax ) tag. This is ground we've covered before!
There's also a chapter in Blood on the Page: a Writer's Compendium of Injuries (amazon link; yes, I am the author) on pneumothoraces. I believe it's in section 2.2: Penetrating Trauma > Chest.
I genuinely thought this chapter had already posted, but it hasn't.
So have a free chapter on me! (Below the cut)
Tension Pneumothorax
Lethality Index
5 / 5
What Is It?
Tension pneumothorax is a life-threatening injury that occurs when air gets into the chest but is outside the lungs. The buildup of air begins to put pressure on the lung, the heart, and the great veins. The condition is rapidly lethal.
Breathing is a pressure system. To inhale, the body pushes the diaphragm down and expands the ribs, which creates negative pressure in the lungs; that negative pressure draws air into the lungs from the outside world. To exhale, the diaphragm comes up and the chest relaxes — it gets smaller — pushing the air out. Easy peasy.
Tension pneumothorax changes this closed system to an open one, where air leaks from the lung into the sac around the lungs (the pleura) and gets trapped there. Positive pressure then builds up in the pleura, compressing the lung.
The fact that there's air in the lung is known as simple pneumothorax. (Pneumomeans air, and thorax means chest.)
What makes a tension pneumothorax such a big problem is that the air pocket in the pleura becomes large enough that it collapses the lung.
In addition to collapsing the lung, having that much pressure on one side of the chest is a big problem. It actually causes the organs of the chest to shift, to skooch over to the other side. In that shifting, the heart and other lung wind up pinching off blood flow through the heart, reducing blood flow everywhere.
Clinical Signs
· Severe, worsening shortness of breath, with rapid breaths.
· Diaphoresis (sweating).
· Elevated heart rate.
· Narrow pulse pressure (the “distance” between the systolic (top number) pressure and the diastolic (bottom number) pressure; e.g. 90/80 instead of 120/80).
· Engorged veins in the neck (jugular venous distention, JVD).
· Cyanosis (bluing of the skin of the lips and nail beds). (Late)
· Cold, clammy skin. (Late)
· Tracheal shift — the trachea is no longer midline in the neck, and instead is pushed away from the affected lung. (Late)
· Loss of consciousness. (Late)
· Death. (Late)
Symptoms
· Pain at the injury site and possible pain in the rest of the chest.
· Trouble breathing and panic.
· Feeling of impending doom.
· Dizziness, disorientation.
How Does It Happen?
Tension pneumothorax develops when a character suffers penetrating trauma to the chest that allows air to move between the outside and inside of the chest. This can be the result of a stabbing, shooting, impalement, or other penetrating trauma. It's especially common when the lung itself has been lacerated.
Immediate Treatment
Keep the character upright.
Provide oxygen, if available.
If the character is in respiratory failure — if they're dying — someone might give them mouth-to-mouth resuscitation or use a bag-valve-mask (BVM) to ventilate them. This actually makes the pneumothorax worse, but it may be beneficial in the short term because of increased gas exchange.
Needle Decompression
Needle decompression is the act of taking a big fat IV catheter and sticking it into the chest on the affected side. (There are two landmarks in common use: between the 2nd and 3rd ribs, on a line drawn straight down from the middle of the clavicle, or between the 5th and 6th ribs, in line with the front border of the armpit. These are technically called the 2nd intercostal space (ICS) at the midclavicular line, and the 5th ICS at the anterior axillary line.
Needle decompression works by giving the air trapped in the pleura an effective way out.
The problem with needle decompression is that, especially with larger characters, it isn't necessarily effective. Oftentimes the needle is simply too short to reach the pleura, especially in larger characters with strong pectoralis muscles or fat deposits, including breasts. Other times the catheter may kink or get backed up with blood.
Definitive Treatment
Needle decompression has the potential to be a definitive treatment for the injury, but only if it's effective in the first place, and only if the needle is hooked up to some form of drain system to make sure that air can escape.
Surgery / Hospitalization
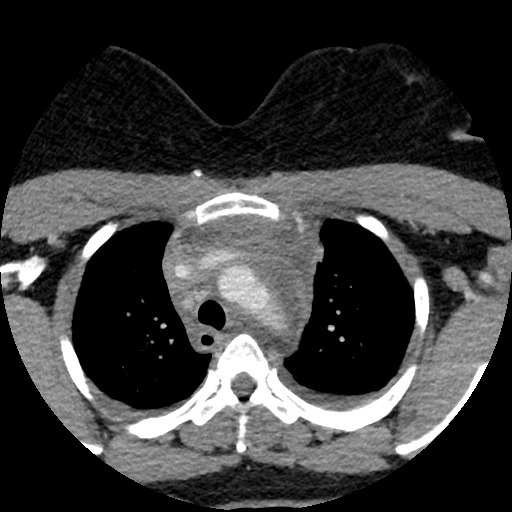
Diagnostics will include a chest X-ray and likely a chest CT, though if the character is in mortal danger, these will always take a back seat to a clinical diagnosis – i.e. by signs, symptoms, and history – and providers will treat first and image later.
The definitive treatment for tension pneumothorax is placement of a chest tube or pigtail catheter in the chest. A chest tube is a large, straight tube, while a pigtail catheter is of a smaller diameter and is curled, like a pig’s tail.
Both are simple, quick procedures in the ER. They both involve putting a tube into the chest at the 4th or 5th intercostal space (between the 4th–5th or 5th–6th ribs) vertically aligned with the armpit (axillary line).
The end of the tube will have something called a Heimlich valve, which is a one-way valve (air can go out but not in).
Another option is a procedure called a finger thoracostomy. The surgical landmark is the same as for all other procedures, but the act is simpler and more brutal. The site is identified and the doctor — who is likely an ER physician — simply cuts down through the chest wall until they're touching lung. This is done in extreme circumstances, where the character is about to die. Otherwise, a chest tube or pigtail catheter is preferred.
In the Austere Environment
Characters who suffer a tension pneumothorax in extreme conditions are likely to die, unless a knowledgeable character with the correct equipment is around.
In settings before about 1950, the character is also likely to die, and they'll die gasping. Treatment of the tension pneumothorax requires understanding pressures inside the chest, which weren't readily measurable till then. Trauma surgery simply hadn't advanced to the point of understanding this rapidly lethal wound until that point.
The Rocky Road to Recovery
Capabilities Retained
Characters will retain the use of all four limbs and will be cognitively unaffected (barring brain damage from an extended period of low oxygen levels).
Disabilities: Temporary
Your character is likely to have a sensation of pressure at the catheter insertion site. Once the lung is reinflated, they can walk and perform most normal activities while the wound heals.
They will be instructed not to fly for six months after the pneumothorax. This is because altitude affects pressure and can cause reexpansion of the pneumothorax.
Disabilities: Permanent
Tension pneumothorax shouldn't cause any permanent disabilities, unless there are other complicating features of the injury.
Features of Recovery: Hospital Stay
Characters with no other complications, who respond well to the pigtail, can actually be sent home with the catheter in place. Characters with other injuries or who got bigger tubes will likely be admitted.
Features of Recovery: Aftercare
Characters will be instructed to walk up to their capacity, and increase their walking daily. They may want to use a pillow or other object to hold when they cough, because that can be painful.
If a character is sent home, they must come back for follow-up X-ray within 48 hours, to make sure the pneumothorax hasn't reexpanded.
The catheter should be removed after 3–5 days if no other issues arise.
Complications
Pigtail catheters are good for patients because they're smaller than chest tubes, which means they hurt less and can often be sent home in the patient.
Pigtail catheters are bad for patients because they're smaller tubes, which means that they might kink and then fail to vent out the air they need to get rid of.
Flying before the recommended date can cause another pneumothorax, though this is unlikely to be severe enough to collapse the lung again. However, the character might experience significant shortness of breath and exhaustion.
The New Normal
If the lung tissue itself wasn't damaged by the object, your character will return to their full function within 2–4 weeks. (No Disability)
If the lung was damaged by the injury, they may have other complications with the lung.
Future Risks
Even when they think they're healed, significant, rapid changes in altitude within the first 6 months could cause your character's pneumothorax to recur. No long-term risks are known.
Total Recovery Time (Typical)
Uncomplicated: 2–4 weeks
Complicated: Minimum 4 weeks but typically longer, depending on the damage
Sensory
Sights
The hole in the chest might be small, or it might be fairly large. Through a large enough hole, characters can see the injured's lung expanding and collapsing with each breath.
Sounds:
The wound may make a sucking noise as the character breathes. (This is known, appropriately, as a sucking chest wound.)
Medspeak
Tension pneumothorax is abbreviated in a chart as TPTx or TPx, and is colloquially known as a "tension pneumo."
Chest tubes are listed in various sizes; pigtails tend to be 12 French or 14 French, whereas chest tubes are larger: 24 Fr to 36 Fr. Pigtails are inserted over a guide wire, which is called the "Seldinger technique." They are held in place with a kind of stitching called "purse string" suture.
A TPTx that also has significant pooling of blood in the pleural space is a hemopneumothorax, or a "hemopneumo."
The landmarks are almost never said as "intercostal space," but referred to as the "ICS."
Key Points
· Tension pneumothorax is a rapidly lethal condition, developing from slight trouble breathing to deadly within minutes to an hour.
· TPTx collapses the lung and puts enormous pressure on the heart. It also kinks the great vessels.
· TPTx is treated by allowing the built-up air to escape. This is done with a needle, insertion of a tube, or cutting down until the lung can “communicate” directly with the outside world.
#this post is not medical advice#this post is writing advice#blood on the page#tension pneumothorax#pneumothorax#asks#recursive tagging
122 notes
·
View notes
Text
Blood on the Beach (Adam+ Dave)

Characters: David Herring (Selkie- Immo), Adam Walker (Hunter - Tapir)
Summary: Adam encounters a hongrey seal. Dave is fighting for keeps but Adam disobeys protocol.
Content Warning: Head Trauma, Vomit
The spellcaster’s blood was still thick and heavy in his mouth, but no matter how rich a delicacy it was, there was an even better prize on the table. Where before Dave had barely had the tiniest threads of self control, strained to the edge after so many days of resisting a hunger he still refused to seek help for, with the smell of selkie in the air, all bets were off. His focus was pinpoint thin, as he cut through the water, following the scent without realising it was so close to the docks he’d been trying to avoid for the past several days. Reaching shore, Dave strode out in soaking wet clothes that were stained in varying ages in blood.
A man in his early thirties was chilling on the shore, in shorts despite the chilly wind whipping around them as he read a well worn. Ollie George was skinny and sinewy, inclined to spending his time on the beach regardless of which skin he was wearing. As Dave approached, he sat up, squinted at Dave through the bright sunlight and smiled toothily as he waved. “Hey Dave! You look rough, have you- woah!” He yelped as Dave grabbed him to the throat, and dragged him backward. Scratching at Dave’s bloody arms, Ollie managed to get onto his feet, only to have the air knocked out of him as Dave slammed him against the seawall. Dave panted heavily, his teeth bared. But a tiny voice kept him from lunging just yet.
“Yo Dave I talked to Sebastian and…”
Adam strode down the ramp at the far edge of a nearby pier, jogging into the low tide zone toward where he’d caught sight of his noodling partner. The crunch of Adam’s shoes on the sand and shells paused as the Hunter took in Dave pressing another guy up against the cement sea wall. From the way the lean dude was struggling and Dave’s teeth were barred, Adam doubted he’d walked in on a mlm remake of the Shape of Water.
Hesitation costs lives. Adam sprinted across the remaining stretch of beach to barrel into Dave with a footballer’s full-bodied tackle.
Dave was aware of Adam in the way a horse might be aware of a gnat, some hind brain motor processing that he could smell the hunter nearby and opting not to care. A vein bulged in his forehead, pressing his forearm against Ollie’s throat as he opened his maw ever wider. Inch by treacherous inch. A lifetime of protecting selkies was slowly overridden with a hunger Dave did not know how to explain.
The hair was knocked out of him as Adam sent them both careening into the sand and rocky dirt. Ollie slumped against the seawall, clutching at his chest as he gasped for air. Dave swung his head round to look at him as Ollie began staggering towards the water and his escape. Normally, Dave would have kept his eye on Adam, the skilled youthful hunter who appeared the obvious threat. Dave barely even acknowledged him other than to slam a fistful of rocks and sand into his face. He rolled onto his knees and sprinted after Ollie, towards the waterfront.
Adam drew both legs anterior to his chest and kicked himself back to his feet and with an economy of motion born from a lifetime of drills. The Hunter had already drawn two tactical knives from their sheathes before he was even fully standing.
The next step was simple, practiced countless times, and Adam was already using the momentum from the kick-up to bring his arm forward and pitch a knife straight into Dave’s back. The impalement would stagger the Selkie for a moment, and that’d be all the Hunter would need to end this.
Yet, the knife never left Adam’s hand. A flicker of indecision turned lethal grace into a baseball newbie’s first stumping on the pitcher’s mound, blinking sand from his eyes.
Could he really do this all over again? …What about this other guy running from Dave? Was it right to jeopardize his life for the sake of sentiment? ...Dave would never do this in his right mind...But Adam had already needed to put down plenty of people who couldn’t control themselves to save other lives...He no more right to spare Dave’s life then he had the right to take it.
Adam’s head was filled with contradictions, but silver and iron blades dropped to the sand as he sprinted headlong after Dave.
Sprinting under the pier, Ollie vaulted abandoned netting rigs, ripped up tarps, and something that might later be identified as a mummified hand, yelling as he tried to gain distance from Dave through the obstacles, but Dave ran with the same precision that he swam with, a predator nearly in his element even with saliva slobbering down his mouth. Making a last ditch effort, Ollie veered right toward the see, but the tide barely lapped at the soles of his feet before Dave tackled him, slamming both bodies into the floor. Veins bulging, Dave pinned Ollie’s arms under him, grappling with himself too, and the hunger that felt as wrong as it felt demanding.
Ollie bared his own seal teeth, eyes filled with terror as he tried to snap at Dave’s face, but he was pinned down by Dave’s forearm. He begged, voice creeping up in pitch with every frantic word.
“Dave, Dave, stop stop stop! Is this about the lobsters? Because I swear I didn’t know they were Karkinoids, I would never- please, Dave c’mon it was only one finger it was a- hey help! HELP!”
Dave’s head whipped to where Ollie was looking, and he growled deep in the back of his throat. “Stay back, hunter.”
“No, Dave man this isn’t you,” insisted Adam.
Looking at Dave now, teeth barred and feral in the eyes, Adam experienced an unwelcome memory of himself at the Hunter’s Moon. A twinge of self-loathing nausea came with recollections of the intoxicating power that’d bled into him from the red moonlight. Had he seemed just like this to poor Rio and Nell, hopped up to the crazy eyeballs on some paranormal bullshit till one barely resembled the original person?
A small pain in the Hunter wondered whether the true Adam underneath was really so different the then moon-drugged killer his friends had confronted on the glass lake, but Adam pushed such thoughts aside.
All that mattered was that whatever had gotten into Dave, literally, he shouldn’t have to wake with a stomach full of fellow selkie.
“Sorry dude, gonna have to eat me to get rid me. Noodler-bro unity.”
Adam sprinted towards where the two paranormals were grappling and shifted his center of gravity and thrust forward his right leg while keeping the left leg slightly behind it. The Hunter hit the last stretch of sand into a rough slide tackle that’d have earned an immediate red card on any soccer field. Adam’s low hooking kick slammed into Ollie as if he were the soccer ball, directly hitting him a combination with mutant strength and accelerated leverage, wrenching him from the other Selkie’s grasp by blunt impact. The rest of Adam’s momentum carried him bodily into Dave in a unguarded full-on collision, a price to pay for getting the hostage outta there.
Dave lunged for Ollie as he was knocked out of Dave’s grip, but Ollie grunted, rolling out of Dave’s reach, clutching his side. He didn’t even get to his feet, scrabbling into the water without a second glance at his assailant or his rescuer. He slipped into the waves as easily as if it was his second skin, gone, while Adam slammed into Dave. With a growl of bared teeth, Dave salivated over the fresh meat trapped underneath him, even though he was furious at the loss of the tastier prize. “No.”
When it came to killing hunters, the easiest thing was to ambush them, pull them out of their element and into the water. Even the weakest of them was stronger than he was on any day of the week, with the training and energy to go along with it. Take out the limbs, get the throat, don’t let them find their balance. Kill before they could land a single blow, because if a hunter wanted you dead, that was all the hope chance you had. Dave couldn’t separate his training from Adam any more than he could separate the hunger from his rationality. He took as little note of his own desire not to kill and eat Adam as he did Adam’s desire not to kill him.
With a quick shift of his weight, he trapped on of Adam’s arms under his body weight, and opened his mouth wide, but it wasn’t Adam’s throat or head that he aimed for, but the meat of Adam’s shoulder on his other side.
For a moment Adam’s whole world was just flares of veined red in a black tunnel as pain lanced though his shoulder into the bone. His body begged to pass out. Adam’s back arched as he spasmed with in agony. Dave’s teeth closed like an aspiration straight into the marrow. Warm blood broke like a wave down over Adam’s back to stain the sunbright sand. Shock threatened at the threshold of his guts like an approaching wave of cold.
The Hunter willed himself to stop spasming as training ran his mind through the next steps of getting out of this hold. If Dave wrestled him to the water and got his neck exposed, Adam’d be arguing about today’s Black Bears game with Dad in under a minute.
But although his reflexes were primed to end this now, Adam fought back against that lifetime of muscle memory as a higher purpose than just survival gave his mind clarity through pain.
Adam let out a ragged rap of pain as he twisted in Dave’s grasp, tearing his own flesh further with the movement. He swung up his free arm toward the side of Dave’s head. While survival instincts screamed to cave Dave’s head in, enough of Adam’s reason remained to hold back.
Instead Adam used the flat of his palm to try to daze the Selkie enough to break his hold, even though ever bit of training dictated that a puncturing blow to the jugular with mutated strength would be the “correct” move.
There was a moment when Dave’s teeth met the resistance of bone, that only lasted the length of two heartbeats, where he could have bitten right through the socket and leave Adam without an arm he could ever use again. Or he could twist his head and tear away the flesh already between his teeth, so that Adam’s blood would spurt over the sand rather than in his mouth while Dave could finally, finally eat.
He did neither, frozen in an internal battle as ferocious as the external, slowly increasing the pressure on the bones between his teeth as muscle and sinew popped to get the bone out of his way. Coppery blood coated his tongue, lips and chin, tantalisingly close to what he wanted and so far from what he wanted it might have been on another planet.
Stars exploded from Dave’s temple, the force of Adam’s blow knocking his jaw loose and body off balance, giving Adam all the time to get out from under him, leaving a bloody mess in the sand and granite. It wasn’t the first time Adam had bled on a beach in front of Dave, leaving a mess in his wake as he’d bargained with a monster for his and Dave’s life. Dave blinked away the stars and sentimentality as he bounced to his feet.
Like the bloody mess of his arms and the deep gash in his face, Dave shook his head to shake off the growing headache, bared his bloodied teeth, and slammed Adam into one of the pier’s wooden pillars.
Everything flared white. The high pitched ringing in Adam’s ears made the foamy surf sound like it was screaming onto the beach.
Adam had never been trained to merely subdue or fend someone in a fight. Adam wasn’t a police officer, bouncer, or street tough who roughed up squishy humans to assert authority. Adam had been conditioned as a soldier to fight ravenous immortals, giant beasts, and eldritch things from beyond this universe. These adversaries were so preternaturally lethal anything less then the most brutally efficient kill meant you were dead a second later. Even a lowly Spawn could tear a human in half. The common forest Carach could wade straight through small arms fire and pop open your ribcage like a candy orange. The mission had always been simple: kill this thing before it kills you and everyone else.
Except today apparently, where Adam’s mission was to put a cease and desist on roid-rage Captain Ahab here.
Shit shit shit
Pain splintered into Adam’s back as the pier barnacles sliced his back open. Dark red stained the white clusters clinging to the pier as their razor edges tore into Adam’s flesh. The Hunter felt the bitter salt sting of the barnacle cysts grinding deep into the wound as Dave slammed him against the sodden wood pillar, probably looking for an opening to sink those teeth into Adam’s throat.
The muscle memory of training immediately pulled Adam towards the lethal solution. A glance at Dave told the mutant where he could aim blows that’d punch through ribs with enough momentum to rupture organs.
Adam let out a shuddering breath, gagging on the bloody bile and trying to fight past the concussed fog in his brain. With another rasping exhale, Adam pushed away the deadly conditioning that’d served him so well for so long. That wasn’t why he was here.
Adam reached his arms up and behind his head to grab the opposite side of the pier pillar. The tired muscles of the Hunter’s biceps knotted as Adam hoisted himself into a dead hang up through leverage and brought his knees up to slam a quick two-legged kick into Dave’s gut. Adam pulled his weight off from the kick a bit just before impact, not wanting to break anything internal.
----
Crashing backwards into the sand, Dave grimaced as his distended, overful stomach pushed acid up his throat. Days and days of overeating while still famished were taking a toll, but he couldn’t afford to let the pain breath. Dave pushed himself back onto his feet, eyes fixed on the bloodied mess of Adam’s shoulder.
He should have torn that arm right out of its socket. The thought turned his stomach too. There were a couple dozen humans in the surrounding hundred feet. All Dave would have to do would be climb on the docks. No one up there would fight back, not enough to be a problem. A stranger wouldn’t create such a strong internal struggle. Dave glanced up at the pier, then back down at Adam, hands curled into fists so tight the skin of his knuckles might split.
“Get out of here.” Dave warned through grit teeth. Or begged.
Adam’s eyes followed Dave’s gaze up past the rock seawall towards where passerby in the harbor were blissfully going about their business. Understanding passed from killer to killer.
Adam shook his head. “Don’t do it.”
The effort of the deadlift moments before has taken its toll. One arm hung limp at Adam’s side as the exacerbated injury in his shoulder sent ripples of cold numbness that made it hard to even his finger. Adam’s clothes were a mess, torn by lacerations, barnacles, and sodden with spreading scarlet from one shoulder, all across his shredded back and the blunt-impact head wound now bleeding down his neck.
But Adam lifted his remaining functional arm in a boxing guard. He squared up to face Dave, feet angled parallel with the right slightly ahead of the left, chin up, eyes forward.
Dave blurred in out of focus in Adam’s vision, seeming to merely be a distortion of light from the crystalline blue surf and pale sand. The athlete knew more than enough about bloodloss and concussions to realize the danger he was in, but running was a non-option.
“I’m not gunna kill you man,” Adam assured, moving slowly to the side and around as he looked for an opening in Dave’s guard. “Come back with me, we’ll find an antidote. I’ll keep you from hurting anybody while we figure out to get this out of you.”
Adam’s words only barely made it through Dave’s skull as he stared at Adam, mouth open and closing like it was longing for something to chew. An antidote? Dave didn’t need one of those. The only fix to starvation was consumption. But he’d known something had been wrong for a while, since that day on the beach with Griffin, since before.
Dave forced himself to look at Adam as more than meal and enemy. His eyes didn’t quite focus on Dave’s, his guard was one handed, and his expression resolute. His stance was as sturdy as could be, but on shifting sands that were quickly getting wet with his blood, Dave didn’t see much strength in him.
Maybe the hunter would be an easy meal after all. If Adam took half a step forward, he’d step on a seaweed coated net, that if Dave pulled on just right could knock the boy off his feet, maybe even hauled into the water. It was tempting. One more bite and even a hunter’s healing likely wouldn’t be enough to pull Adam back from the brink. Or, the steps up onto the pier weren’t that far either, a dozen satiating meals chatting idly about the May sun, just waiting for his bite.
“No.” Dave trembled, taking a slow, uncertain step back.
The hunger inside him wasn’t just poisonous, but monstrous too. The kind people like Adam were needed for. Dave swallowed, Adam’s blood still mixed in with the saliva dripping out of the corner of his mouth. This sliver of control, paid for in Adam’s injuries, wasn’t going to last. The hunger was clawing its way up his throat, down his gullet, like it might consume him from the inside out.
“No.”
Like if he didn’t eat someone else, his hunger might eat him. Dave took another step back, grimacing at the ache of a bruise forming under his ribs. A wave rushed water up to his ankles. The only advantage of Adam bleeding so profusely is that Dave could no longer smell the enticing scent of selkie. He opened his mouth to speak again, but couldn’t find any words.
Dave plunged into the waves, speeding away from shore, putting as much distance between him and Adam as he could before his hunger eclipsed his conscience once more.
Adam tried to sprint at the departing Selkie but his steps became sluggish in the sand. Dave was a black spot vanishing into foam as refractions from the surf were burning lances across his vision. Everything spun, the sky and sea switched places in a rush of blue. Light went out.
9 notes
·
View notes
Text
Symptoms Leading to Diagnosis
Middle of January 2019
I woke up with a sore/kinked neck, mainly on my left side, which I assumed was from sleeping on the couch or working out too hard and not stretching afterwards. Around the same time I also noticed swelling around my throat. The swelling was minimal and only noticeable to me. I remember asking others and they couldn't see or feel a difference, while I could feel that it was a lot more tender and firm than usual. Immediately I assumed it was a swollen lymph node and I might be sick or having an infection my body is fighting. (Previously in 2015 I also had an encounter with a swollen lymph node on the right side of my neck, which followed with a case of minor shingles on my neck. I did get an ultrasound for it and it came back as nothing serious; it eventually went away as well so I assumed this was similar case).
Tuesday, January 29th, 2019
11.30 AM: Massage at Leela Eco Spa
After the soreness and achy feeling on the left side of my neck and upper back didn't go away after a week I decided to get a massage to see if that would help the pain.
February 2019
The massage only helped deal with the pain temporarily but the achy feeling was still there. At this point it had been a few weeks now since I noticed my initial symptoms and the swelling was still present as well. After being reluctant to take medicine, I finally tried to take some and had difficulty swallowing the medication. I could feel the pill slowly go down my throat and it took bottles of water to help it go down, which isn't normal. I also noticed difficulty swallowing certain foods, especially if I didn't chew it several times.
Wednesday, February 6th, 2019
5.00 PM: Attended Aspen Medical Clinic (walk-in)
I decided to attend a walk-in clinic because I didn't want to wait to book an appointment with my doctor. The doctor at Aspen Medical Clinic was very nice and attentive. She took the swelling and my difficulty swallowing very seriously, and provided me with a requisition for blood test and scheduled an ultrasound appointment for me.
Thursday, February 7th, 2019
10.00 AM: 1st Blood test
2.30 PM: Ultra Sound at Mayfair Diagnostic in Aspen - for my neck area
Saturday, February 9th, 2019
10.50 AM: Follow-up appointment with Dr. Houbi at Aspen Medical Clinic
Dr. Houbi is not the initial doctor I met with at Aspen Medical Clinic but from this point forward, he took care of me as a patient and he was just as attentive with my symptoms. After receiving the results of my blood test and ultrasound, he prescribed me antibiotics for 10 days to see if that would help and scheduled me for a CT scan of my neck, as recommended from my ultrasound results. (*In 2015 when I got the ultrasound of my neck they saw immediately that it was a swollen lymph node and didn't refer me to get a CT scan).
Blood Test Results = High white blood cell count
Ultrasound Results = “Cervical neck ultrasound showing left-sided pathological lymphadenopathy adjacent to the thyroid gland causing extrinsic mass effect upon the internal jugular vein. CT neck recommended for further assessment."
Wednesday, February 20th, 2019
Last day of antibiotics (Teva-Cephalexin 500mg TAB). The antibiotics didn't have any effect and the swelling and difficulty swallowing still persisted.
Tuesday, March 5th, 2019
9.30 PM: CT Scan at South Health Campus - for neck area
Saturday, March 9th, 2019
8.00 AM: 2nd Blood test
Second blood test was ordered so the doctor could see if my blood count leveled out, and compare it to my initial blood test done in February.
Tuesday, March 12th, 2019
12.30 PM: Follow-up appointment with Dr. Houbi at Aspen Medical Clinic - to discuss my results
Due to the results of my CT scan, my doctor put an immediate rush request for X-Ray, Ultrasound, CT Scan of my chest and abdomen area and additional blood test.
CT Scan Results = “There is abnormal soft tissue density involving the anterior and superior mediastinum which measures approximately 4.9 cm mediolateral by 5 cm anteroposterior by 5.7 cm vertical with mild patchy irregular enhancement. This tumor is displacing the trachea and thyroid gland rightward. Evaluation of the adjacent great vessels reveals a bovine arch anatomical variant which is splayed with the left common carotid artery displaced laterally towards the left in the brachiocephalic trunk demonstrate a horizontal course displaced inferiorly by the presence of the tumor. The tumor appears to encase the left common carotid artery along its proximal course.
No internal calcification or cystic components are noted within the tumor. The tumor mass is predominately within the anterosuperior mediastinum. Tumor compression results in complete effacement of the left brachiocephalic vein and contrast reflux in the left jugular vein. Venous collateral branches Carries contrast through the dorsal paraspinal neck and drainage into the azygos vein….
The imaging features and appearance are concerning for Hodgkin’s lymphoma, with alternative neoplastic etiologies also possible.
A dedicated thoracic CT examination is recommended for further assessment. Given the venous compression of the left innominate vein, please request a right-sided contrast injection for the thoracic CT.”
1.30 PM: X-Ray at Mayfair Diagnostic in Aspen - for chest/abdomen
2.30 PM: 3rd Blood test
Thursday, March 14th, 2019
5.00 PM: 4th Blood test
Tuesday, March 19th, 2019
5.30 PM: Check-in for CT Scan at South Health Campus - for chest, abdomen, and pelvis
For this CT scan, instead of getting an injection, I had to drink a cup of a mixture of water and some liquid every half hour for 2 hours.
7.30 PM: Actual CT Scan
Friday, March 22nd, 2019
8.00 AM: Ultra Sound at Mayfair Diagnostic in Aspen - for chest, abdomen, and pelvis
For this ultrasound I was required to have a full bladder so I was instructed to either not go to the washroom in the morning or drink lots of water prior to my appointment.
Tuesday, March 26th, 2019
10.40 AM: Follow-up appointment with Dr. Houbi at Aspen Medical Clinic - to get results
Due to the results of my second CT Scan and the likelihood of lymphoma, Dr. Houbi put a referral for me to meet with a general surgeon. At this point, I was now being referred to specialist and this was my last appointment with Dr. Houbi.
CT Scan Results = “1. As on recent CT imaging study of the soft tissues of the neck, today’s evaluation confirms a superior mediastinal mass.. The homogenous attenuation of the mass and its displacement of surrounding structures without encasement or vascular thrombosis suggests a soft tissue tumor such as lymphoma. No other mediastinal nodal deposits are seen.
2. No pathological nodal deposits in the abdomen or pelvis. No evidence of splenomegaly or other organomegaly.
3. Questionable mucosal thickening at the level of the pylorus. Although uncommon, lymphomatous infiltration is a diagnostic possibility. Endoscopy may be appropriate.”
Monday, April 1st, 2019
10.10 AM: Consult with General Surgeon, Dr. Rothwell
Though I was a little dissatisfied after this appointment because, again, I felt like I had no definite answers as to what the mass was or what steps would be taken next; Dr. Rothwell was a very pleasant doctor. He noted my CT scan results and took a look at the swelling/mass in my neck area. Based on this, he advised me that due to the location of the mass he, as a general surgeon, wouldn't be able to operate on me and would need to refer me to a Thoracic Surgeon.
#symptoms#diagnosis#hodgkin's lymphoma#lymphoma#stage 4#cancer#fuck cancer#cancer survivor#survivor#cancer journey#my journey#lymphoma survivor#vianny
4 notes
·
View notes
Text
Case 35
History: neck and check pain. Swelling


Answer: Thrombophlebitis of the Left bracheocephalic vein with mediastinitis
Check out the new X-ray. We definitely see widening of the upper mediastinum. But can we be more specific? Where is the “mass”

We can see from our current exam that the contour of the aortic silhouette (red arrow) is maintained so it should not be adjacent to the aorta. If fact it actually obscures the left subclavianartery silhouette (yellow arrows) so it has to be in that region of the anterior mediastinum.
So what’s next? How about the CT?

Now we clearly see the extensive stranding throughout the anterior mediastinal fat, with severe narrowing of the left bracheocephalic vein and left jugular vein.
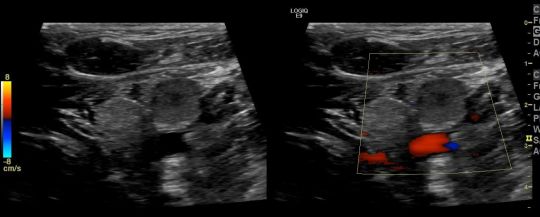
Finally we have the Doppler Ultrasound of the left jugular vein showing occlusion. In fact the left jugular and subclavian veins were thrombosed as centrally as able to be visualized.
What’s the source? Here’s a higher slice from the neck CT showing retropharengeal fluid likely relating to pharengeal infection.

In summary, we have thrombosis of the left jugular, subclavian and bracheocephalic veins with associated thrombophlebitis and mediastinitis preumably secondary to a pharyngeal infection. This is similar to a Lemierre’s Syndrome however classically that involved the internal jugular vein but here we have common jugular and distal thrombophlebitis.
Lemierre’s Syndrome:
Presentation:
Neck pain and swelling with ongoing/recent oropharengeal inection
Male predominance
generally 16-25 years old
Pathology:
80% caused by Gram (-) Fusobacterium necrophorum but can get polymicrobial even including MRSA
Radiology:
shows jugular vein thrombosis. US generally easiest and most straight forward but can be limited in the chest
CT/MR can be helpful for more central venous evaluation and to identify source/site of primary infection
Complications: Pulmonary Septic emboli and systemic dissemination
Treatment: Anticoagulation and IV Abx. Mortality rates can be as high at 18%.
3 notes
·
View notes
Text

Today I'm going to see a tracheostomy and percutaneous endoscopic gastrostomy. This is from Grant's Atlas.
A. Surface anatomy. B.Tracheostomy. The U-shaped hyoid bone lies superior to the thyroid cartilage at the level of the C4 and C5 vertebrae. The laryngeal prominence is produced by the fused laminae of the thyroid cartilage, which meet in the median plane. The cricoid cartilage can be felt inferior to the laryngeal prominence. It lies at the level of the C6 vertebra. The cartilaginous tracheal rings are palpable in the inferior part of the neck. The 2nd to 4th rings cannot be felt because the isthmus of the thyroid, connecting its right and left lobes, covers them. The 1st tracheal ring is just superior to the isthmus.
Tracheostomy. A transverse incision through the skin of the neck and anterior wall of the trachea (tracheostomy) establishes an airway in patients with upper airway obstruction or respiratory failure. The infrahyoid muscles are retracted laterally, and the isthmus of the thyroid gland is either divided or retracted superiorly. An opening is made in the trachea between the 1st and 2nd tracheal rings or through the 2nd through 4th rings. A tracheostomy tube is then inserted into the trachea and secured. To avoid complications during a tracheostomy, the following anatomical relationships are important:
The inferior thyroid veins arise from a venous plexus on the thyroid gland and descend anterior to the trachea (see Fig. 8.10).
A small thyroid ima artery is present in approximately 10% of people; it ascends from the brachiocephalic trunk or the arch of the aorta to the isthmus of the thyroid gland (see Fig. 8.21).
The left brachiocephalic vein, jugular venous arch, and pleurae may be encountered, particularly in infants and children.
The thymus covers the inferior part of the trachea in infants and children.
The trachea is small, mobile, and soft in infants, making it easy to cut through its posterior wall and damage the esophagus.
Cricothyrotomy. The incision is made through the cricothyroid membrane, and the tube inserted between the thyroid and cricoid cartilages.

Infrahyoid Region, Superficial Muscular Layer
The pretracheal fascia, right anterior jugular vein, and jugular venous arch have been removed.
A persistent thymus projects superiorly from the thorax.
The two superficial depressors of the larynx (“strap muscles”) are the omohyoid (only the superior belly of which is seen here) and sternohyoid.
Fracture of the hyoid. This results in depression of the body of the hyoid onto the thyroid cartilage. Inability to elevate the hyoid and move it anteriorly beneath the tongue makes swallowing and maintenance of the separation of the alimentary and respiratory tracts difficult and may result in aspiration pneumonia.

A. Dissection of the left side of the root of the neck. The three structures contained in the carotid sheath (internal jugular vein, common carotid artery, and vagus nerve) are retracted. The left recurrent laryngeal nerve ascends on the lateral aspect of the trachea, just anterior to the recess between the trachea and esophagus. B. Arterial supply of thyroid gland. The thyroid ima artery is infrequent (10%) and variable in its origin.
During a total thyroidectomy (e.g., excision of a malignant thyroid gland), the parathyroid glands are in danger of being inadvertently damaged or removed. These glands are safe during subtotal thyroidectomy because the most posterior part of the thyroid gland usually is preserved. Variability in the position of the parathyroid glands, especially the inferior ones, puts them in danger of being removed during surgery on the thyroid gland. If the parathyroid glands are inadvertently removed during surgery, the patient suffers from tetany, a severe convulsive disorder. The generalized convulsive muscle spasms result from a fall in blood calcium levels.
6 notes
·
View notes
Note
I just wanted to say that if god gave me a chance, I would like to bite the back of Louis' neck, with all respect and obvious consent!
Is that you, Lestat de Lioncourt?







You are in the right place because I’m obsessed with his neck.
#this is about the video where we see Louis from behind isnt it?#but listen I have a tag for this Ive been dying to update it#anterior jugular neck veins#anterior jugular veins on Louis’ neck
12 notes
·
View notes
Photo

CERVICAL FASCIA VS. FORWARD HEAD POSTURE ⠀ [OSTEOPATHIC LINKS & PATHOLOGY] ⠀ From my previous post you know the anterior cervical region houses the carotid artery, jugular vein, thyroid, trachea, esophagus and vagus nerve to name a few. All of these important structures are “housed” within the cervical fascia and it’s compartments. ⠀ The investing layer (external layer) of deep cervical fascia envelopes the upper trapezius muscle and SCM while continuous with the platysma (Pic 2). The third illustration (inspired by Poirier) demonstrates the next deepest layer, the pretracheal layer of deep cervical fascia (SCM removed). This layer attaches to the hyoid bone and forms pockets for the sternohyoid and omohyoid (more lateral) muscles (Pic 4). This layer has many intersecting and crossing collagen fibers, making a “weave-like” appearance. This tissue is also the envelope for the thyroid, thyroid cartilage and trachea and called middle layer of deep cervical fascia (deep to the infrahyoid strap muscles). ⠀ The fifth illustration shows a 3D coronal view of the fascial compartments in geographical relationship to the trachea, esophagus and cervical vertebrae. ⠀ Tension on the pretracheal layer of deep cervical fascia, which is very common in “Forward Head Posture”, can affect the hyoid bone, thyroid, esophagus, trachea and even the pericardium resulting in visceral complaints as well as typical mechanical neck pains (Pic 6/7). ⠀ Fascia is responsible for the links between the musculoskeletal systems and visceral systems. Don’t forget to observe this important organ when you treat patients and not only focus on single structures! ⠀ Credit: @AnatomyLinks ⠀ #anatomy #anatomie #fascia #biomechanics #neck #tensegrity #neck #neckpain #textneck #fascial #chiropractic #osteopathy #physicaltherapy #yoga #physio #massage #manualtherapy #acupuncture #dryneedling #thyroid #softtissue #muscle #pilates #osteopathie #rolfing #crossfit #manualtherapy #dr #medicine #student #medstudent #fascialanatomy (hier: Shanghai, China) https://www.instagram.com/p/B3gd3e_CaI5/?igshid=iomvgbwnn2yo
#anatomy#anatomie#fascia#biomechanics#neck#tensegrity#neckpain#textneck#fascial#chiropractic#osteopathy#physicaltherapy#yoga#physio#massage#manualtherapy#acupuncture#dryneedling#thyroid#softtissue#muscle#pilates#osteopathie#rolfing#crossfit#dr#medicine#student#medstudent#fascialanatomy
3 notes
·
View notes
Text
Veins of the Upper Extremity: Part One
Divided into two parts: Deep (running next to arteries) and Superficial (right beneath the skin). The deep veins have more valves than the superficial veins.
Superficial Veins
Superficial veins of the hand and fingers
mostly placed on top
have inner and outer collection on back of hand
inner -> pinkie, ring finger and half middle finger
outer -> thumb, index finger and half middle finger
arch of veins created where inner and outer collections meet
Anterior ulnar vein
starts on the bottom part of the pinkie side of hand
continues to elbow and joins to posterior ulnar vein to make the common ulnar
in front, connects to branches of median vein
in back, connects to branches of posterior ulnar vein
Posterior ulnar vein
starts on the pinkie side of the wrist
continues to the elbow and joins to anterior ulnar vein to make the common ulnar
can join to the median basilic to create the basilic
connected to deep veins in palm under pinkie
Common ulnar
formed by connecting anterior and posterior ulnar veins
joins median basilic to create basilic vein
when it doesn't exist, anterior and posterior ulnar veins separate into median basilic vein
Radial vein
starts at back hand side of wrist
connects to deep veins with branch through wrist bones
continues up thumb side of forearm
connects at elbow to median cephalic to create cephalic vein
Median vein
starts on front of forearm
connected to anterior ulnar and radial veins
divides into median cephalic and median basilic veins at elbow
Median cephalic
passes between biceps and supinator longus muscles
joins radial to create cephalic vein
Median basilic vein
passes between biceps and pronator radii teres
joins common ulnar to create basilic vein
sits in front of parts of internal cutaneous nerve
Basilic vein
large vein
created by joining common ulnar with median basilic
passes along inner part of biceps muscle
passes latissimus dorsi and teres major muscles and becomes axillary vein
Cephalic vein
passes along outside of biceps in same place as musculo-spinal nerve
passes between pectoralis major and deltoid muscles in same place as acromial-thoracic artery
ends in axillary vein just below collarbone
sometimes connects to external jugular or subclavian vein
[Gray, H. 2010, Gray's Anatomy, 15th Edition, Barns & Noble, Inc., New York. pp 584-586.]
#raz anatomy#anatomy#circulatory system#veins#studyblr#medblr#superficial veins#not a med student just interested
1 note
·
View note
Text
Day 1 of preparing for University exams
21st September 2022
Biochemistry
Read and made sticky notes for heme synthesis. couldn't achieve my target but I'm proud that I broke the vicious cycle and I finally started.
Anatomy
Started anterior triangle and it's contents.
4 triangles
1.submental
2.submandibular
3.carotid
4.muscular
Note: common carotid's terminal branches are ext and int carotid.
External has branches. Internal no branches
Lateral to cc internal jugular vein.
Physiology
Ear spl senses started
1 note
·
View note
Text
The Success Rate of Spinal Surgery & Potential Complications

The Success Rate of Spinal Surgery & Potential Complications
Spine Surgery has emerged as very safe now because of the considerable availability and opportunities for training like spine fellowships, observer ships, cadaveric workshops, conferences, etc. Spine surgical treatment has also emerged as safer than before, because of the supply of advanced imaging which helps in better planning and execution of surgical procedures, and because of advances in anesthesia and neuromonitoring facilities that are widely available at a cheaper rate now. Nevertheless, all surgeries have a few inherent risks. ( There is no surgery with 0 risks). It is essential to discuss with your medical doctor what he/she feels the overall chances of a specific complication are in your condition.
The spinal cord and spinal nerves are more sensitive compared to other tissues. Delay in diagnosis with endured stress can add to the probabilities of complications, specifically in conditions like Cancer, infections( like TB), high-pace collision accidents, etc. Earlier surgical treatment is carried out during the disease process to reduce the possibilities of complications. It is best to go to a spine specialist and get the necessary assessment in advance than later.
All surgery has inherent threats. Certainly, spinal surgery has its own set of risks which may also consist of infection, pain on the incision site, lack of fusion, as well as neurologic complications. However, with well-trained hands, the occurrence of complications differs very little from other surgical conditions. It is essential to discuss with your neurosurgeon what he feels the overall probabilities of a particular complication are in your given setting.
Potential Complications of Surgery
You should discuss the complications related to surgical operation with your Spine specialist earlier than surgery. The list of complications provided here is not meant to be complete and is not an alternative choice to discussing the risks of surgery with your Spine expert. Only your Spine Specialist can evaluate your condition and tell you of the risks of any treatment that can be recommended.
Anesthesia — Any surgical operation that requires anesthesia can be potentially harmful. Surgery at the cervical spine generally requires that you be placed under standard anesthesia. General anesthesia means that you are put to sleep. Anesthesia contains a risk of allergies to the medications. There also are different life-threatening conditions that may occur during anesthesia. It is extremely not likely that these complications will occur, however, you should be aware that they are possible.
Infection — Any surgical treatment involving an incision in the skin can become infected. In addition, the bone graft and area around the spine may come to be infected. An infection will generally require some kind of antibiotic medicine to treat the infection. If the infection includes the bone, it may require one or extra additional surgeries to drain the infection. The danger of infection is generally much less than one percent.
Blood Vessel Damage — There are large arteries and veins that travel via the neck into the brain. The carotid artery and the jugular vein are nearby. It is possible to harm those blood vessels during the surgery. Again, it is extremely unlikely that this could occur, possibly much less than one in a thousand.
Nerve Damage — There are nerves in the neck that travel alongside the area in which the incision is made to perform an anterior cervical discectomy and fusion. These nerves go to the vocal cords. There is the possibility that those nerves can be harmed at some point during surgery. This can result in hoarseness. If this occurs, the nerves will usually get better unless they are completely damaged or cut. Again, that is unlikely.
Spinal Cord Damage — Surgeries can be performed in the cervical spine region of the spinal cord at risk for injury. Spinal cord damage might be more likely in the larger, extra severe operations such as the corpectomy and strut grafting procedures. These are complex, hard operations and are done for extremely critical issues which can be not likely to respond to any other kind of treatment. Routine anterior discectomy and fusion are common surgeries that can be extremely safe. While harm to the spinal cord is possible, it is quite unlikely.
Graft Displacement — One of the more common issues which can occur after an anterior cervical discectomy and fusion is that the bone graft may also flow out of position. If it moves too much, it could require a 2nd surgery to place a new bone graft in its place.
Non-Union — In spite of a successful surgery and proper bone graft, a fusion may not occur among the vertebrae. This is called a non-union or pseudarthrosis. Usually, your surgeon may be able to inform whether a fusion has come about by looking at X-rays taken over a three- to the six-month period after the surgical procedure. If a fusion does not occur and you have no pain, a 2nd surgical procedure will not be necessary. If you still have pain, and a non-union is diagnosed after a surgical procedure, your surgeon may also suggest a 2nd attempt at fusion. When attempting for the second time after a failed fusion, most surgeons will generally include some sort of internal fixation, such as a plate and screws.
What is minimally invasive spine surgery and way is it different from traditional spine surgical operation ?
Traditional spine surgery usually requires lengthy incisions in the lower back. Muscles are cut and separated from the spine to allow access to the spinal anatomy. Minimally invasive spine surgical treatment is executed through small incisions in the lower back. Surgeons use specialized instruments and navigational equipment which includes interoperative x-ray, Pedi-guard, microscopes, and tubular retractors. Like traditional spine surgery, the aim of minimally invasive surgery is to relieve your lower back and/or leg pain. But it adheres to a distinctive philosophy—that as little muscle tissue as possible should be damaged.
What are the complications of spine surgery ?
Like any surgical operation, there are some complications associated with spine surgery. There are sure dangers of general anesthesia which are extremely rare and consist of death and different life-threatening reactions to anesthesia. With inexperienced and well-trained hands, the threat of paralysis or permanent nerve damage is extremely rare however can unfortunately still arise even in the best of hands. People with greater severe preexisting spinal cord or nerve compression are at more risk of this. There are certain measures that I take preoperatively and intraoperatively to monitor the spinal cord and nerves carefully so that I am aware of the status of the spinal cord and nerves always during complicated spine surgical operation cases while working across the spinal cord and placing instrumentation. Dr. Sachin Mahajan is an experienced Spine Surgeon in Pune with many years of expertise. Dr. Sachin Mahajan has helped various patients in his tremendous long span of experience as a Spine specialist.
1 note
·
View note
Last Seen Blogs




