#What is the recovery time for the coronavirus disease?
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
The most popular pages on Tumblr are about Minecraft, GIFs, and David J. Peterson.
Text
Long COVID symptom severity varies widely by age, gender, and socioeconomic status - Published Sept 2, 2024
By Dr. Sushama R. Chaphalkar, PhD.
In a recent study published in the journal JRSM Open, researchers analyze self-reported symptoms of long coronavirus disease 2019 (LC) from individuals using a healthcare app to examine the potential impact of demographic factors on the severity of symptoms. The researchers found that LC symptom severity varied significantly by age, gender, race, education, and socioeconomic status.
Research highlights the urgent need for targeted interventions as age, gender, and social factors play a crucial role in the intensity of long COVID symptoms. What factors increase the risk of long COVID? Several months after recovering from coronavirus disease 2019 (COVID-19), patients with LC may continue to suffer from numerous symptoms, some of which include fatigue, brain fog, and chest pain. The prevalence of LC varies, with estimates ranging from 10-30% in non-hospitalized cases to 50-70% in hospitalized patients.
Although several digital health interventions (DHIs) and applications have been developed to monitor acute symptoms of COVID-19, few have been designed to track long-term symptoms of the disease. One DHI called "Living With COVID Recovery" (LWCR) was initiated to help individuals manage LC by self-reporting symptoms and tracking their intensity. However, there remains a lack of evidence on the risk factors, characteristics, and predictors of LC, thereby limiting the accurate identification of high-risk patients to target preventive strategies.
About the study In the present study, researchers investigate the prevalence and intensity of self-reported LC symptoms to analyze their potential relationship with demographic factors to inform targeted interventions and management strategies. To this end, LWCR was used to monitor and analyze self-reported LC symptoms from individuals in 31 LC clinics throughout England and Wales.
The study included 1,008 participants who reported 1,604 unique symptoms. All patients provided informed consent for the use of their anonymized data for research.
Multiple linear regression analysis was used to explore the relationship between symptom intensity and factors such as time since registration, age, ethnicity, education, gender, and socioeconomic status through indices of multiple deprivation (IMD) on a scale of one to 10.
Education was classified into four levels denoted as NVQ 1-2, NVQ 3, NVQ 4, and NVQ 5, which reflected those who were least educated at A level, degree level, and postgraduate level, respectively. The intensity of symptoms was measured on a scale from zero to 10, with zero being the lowest and 10 the highest intensity. Descriptive statistics identified variations in symptom intensity across different demographic groups.
Study findings Although 23% of patients experienced symptoms only once, 77% experienced symptoms multiple times. Corroborating with existing literature, the most prevalent symptoms included pain, neuropsychological issues, fatigue, and dyspnea, which affected 26.5%, 18.4%, 14.3%, and 7.4% of the cohort, respectively. Symptoms such as palpitations, light-headedness, insomnia, cough, diarrhea, and tinnitus were less prevalent.

Fifteen most prevalent LC symptoms. Multiple linear regression analysis revealed that symptom intensity was significantly associated with age, gender, ethnicity, education, and IMD decile. More specifically, individuals 68 years of age and older reported higher symptom intensity by 32.5% and 86%, respectively. These findings align with existing literature that highlights the increased risk of LC symptoms with age, which may be due to weakened immunity or the presence of comorbidities. Thus, they emphasize the need for targeted interventions for this population.
Females also reported higher symptom intensity than males, by 9.2%. Non-White individuals experienced higher symptom intensity by 23.5% as compared to White individuals.
Individuals with higher education levels reported up to 47% reduced symptom intensity as compared to those with lower education levels. Higher IMD deciles, which reflect less deprived areas, were associated with lower symptom intensity; however, no significant association was observed between the number of symptoms reported and the IMD decile.

Regression results with 95% confidence interval. Note: For age, the base group is people in the age category 18–27. For IMD, the base group is people from IMD decile 1. For education, the base group is people who left school before A-level (NVQ 1–2). A significant positive association was observed between symptom intensity and the duration between registration on the app and initial symptom reporting. This finding suggests individuals may become more aware of their symptoms or that worsening symptoms prompt reporting.
Some limitations of the current study include the lack of data on comorbidities, hospitalization, and vaccine status. There is also a potential for bias against individuals lacking technological proficiency or access, which may affect the sample's representativeness, particularly for older, socioeconomically disadvantaged, or non-English-speaking individuals. Excluding patients with severe symptoms or those who were ineligible for the app may also skew the findings.
Conclusions There remains an urgent need to develop targeted interventions to address the severity of LC in relation to age, ethnicity, and socioeconomic factors. LC treatment should prioritize prevalent symptoms like pain, neuropsychological issues, fatigue, and dyspnea while also considering other possible symptoms. Furthermore, sustained support for LC clinics is essential to effectively manage the wide range of symptoms and complexities associated with LC and improve public health outcomes in the post-pandemic era.
Journal reference:
Sunkersing, D., Goodfellow, H., Mu, Y., et al. (2024). Long COVID symptoms and demographic associations: A retrospective case series study using healthcare application data. JRSM Open 15(7). doi:10.1177/20542704241274292.
journals.sagepub.com/doi/10.1177/20542704241274292
#covid#mask up#pandemic#covid 19#wear a mask#coronavirus#sars cov 2#public health#still coviding#wear a respirator#long covid
38 notes
·
View notes
Text
What Is Long COVID? Understanding the Pandemic’s Mysterious Fallout > News > Yale Medicine
Originally published: April 15, 2024. Updated: June 4, 2024
Just weeks after the first cases of COVID-19 hit U.S. shores, an op-ed appeared in The New York Times titled “We Need to Talk About What Coronavirus Recoveries Look Like: They're a lot more complicated than most people realize.”
...
Unlike most diseases, Long COVID was first described not by doctors, but by the patients themselves. Even the term “Long COVID” was coined by a patient. Dr. Elisa Perego, an honorary research fellow at University College in London, came up with the hashtag #LongCOVID when tweeting about her own experience with the post-COVID syndrome. The term went viral and suddenly social media, and then the media itself, was full of these stories.
Complaints like "I can't seem to concentrate anymore" or "I'm constantly fatigued throughout the day" became increasingly common, seemingly appearing out of nowhere. With nothing abnormal turning up from their many thorough lab tests, patients and their physicians were left feeling helpless and frustrated.
The World Health Organization (WHO) has defined Long COVID as the "continuation or development of new symptoms three months after the initial SARS-CoV-2 infection, with these symptoms lasting for at least two months with no other explanation." This deliberately broad definition reflects the complex nature of this syndrome. We now understand that these symptoms are wide-ranging, including heart palpitations, cough, nausea, fatigue, cognitive impairment (commonly referred to as "brain fog"), and more. Also, many who experience Long COVID following an acute infection face an elevated risk of such medical complications as blood clots and (type 2) diabetes.
In April 2024, an estimated 5.3% of all adults in the United States reported having Long COVID, according to the Centers for Disease Control and Prevention (CDC). Data from the CDC suggest that Long COVID disproportionately affects women, and individuals between the ages of 40 and 59 have the highest reported rates of developing this post-acute infection syndrome.
...
Inderjit Singh, MBChB, a YSM assistant professor specializing in pulmonary, critical care, and sleep medicine, and director of the Pulmonary Vascular Program, is actively engaged in clinical trials aimed at uncovering the fundamental underpinnings of Long COVID.
...
Through this work, a significant revelation emerged. They observed that patients grappling with Long COVID and facing exercise difficulties were unable to efficiently extract oxygen from their bloodstream during physical exertion. This discovery identifies a specific cause underlying the biological underpinnings of Long COVID.
... Dr. Singh, along with other researchers, is focused on the identification of blood-based markers to assess the severity of Long COVID. For example, a research group, led by Akiko Iwasaki, PhD, Sterling Professor of Immunobiology and Molecular, Cellular, and Developmental Biology, and director of the Center for Infection & Immunity at YSM, most recently created a new method to classify Long COVID severity with circulating immune markers.
Further investigations conducted by Dr. Singh's team identified distinctive protein signatures in the blood of Long COVID patients, which correlated with the degree of Long COVID severity. Researchers identified two major and distinct blood profiles among the patients. Some of them exhibited blood profiles indicating that excessive inflammation played a prominent role in their condition, while others displayed profiles indicative of impaired metabolism.
...
Researchers currently believe that the impairment of a spectrum of key bodily functions may contribute to these diverse symptoms. These potential mechanisms include compromised immune system function, damage to blood vessels, and direct harm to the brain and nervous system. Importantly, it's likely that most patients experience symptoms arising from multiple underlying causes, which complicates both the diagnosis and treatment of Long COVID.
...
The last word from Lisa Sanders, MD:
I’m the internist who sees patients at Yale New Haven Health’s Multidisciplinary Long COVID Care Center. In our clinic, patients are examined by a variety of specialists to determine the best next steps for these complex patients. Sometimes that entails more testing. Often patients have had extensive testing even before they arrive, and far too often—when all the tests are normal—both doctors and patients worry that their symptoms are “all in their head.”
One of our first tasks is to reassure patients that many parts of Long COVID don’t show up on tests. We don’t know enough about the cause of many of these symptoms to create a test for them. The problem is not with the patient with the symptoms, but of the science surrounding them. If any good can be said to come out of this pandemic, it will be a better understanding of Long COVID and many of the other post-acute infection syndromes that have existed as long as the infections themselves.
#covid#long covid#article#research#study#akiko iwasaki#lisa sanders#yale medicine#2024#june 2024#summer 2024#long covid research#inderjit singh
46 notes
·
View notes
Text
Known COVID-19 Health Complications
Last Updated September 8, 2023
Repeat Infections
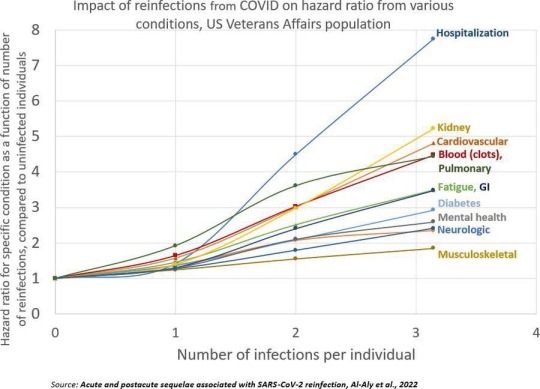
Summary: Repeat infections, even if mild during the acute phase, cause cumulative damage to the body and increase your risk of developing health complications or Long COVID. You should aim to limit the number of times you are infected as much as possible, even if you are not currently high risk (Note: Health complications post-COVID-19 infection can make you high risk) and have been vaccinated.
Published Research
Acute and postacute sequelae associated with SARS-CoV-2 reinfection | Nature Medicine Bowe, B., Xie, Y, & Al-Aly, Z. (2022).
Articles & Reports
Repeat COVID-19 infections increase risk of organ failure, death – Washington University School of Medicine in St. Louis (wustl.edu) Sauerwein, K. (2022).
Why Getting COVID-19 Multiple Times Is Risky For Your Health | Time Park, A. (2022).
Heart & Cardiovascular Damage
Summary: COVID-19 increases your risk of heart failure, heart attacks, strokes, pulmonary embolism, palpitations, arrhythmia, myocarditis, blood clots (thrombosis), etc. post-infection. Inflammation during the acute phase of a COVID-19 infection can damage the heart and blood vessels.
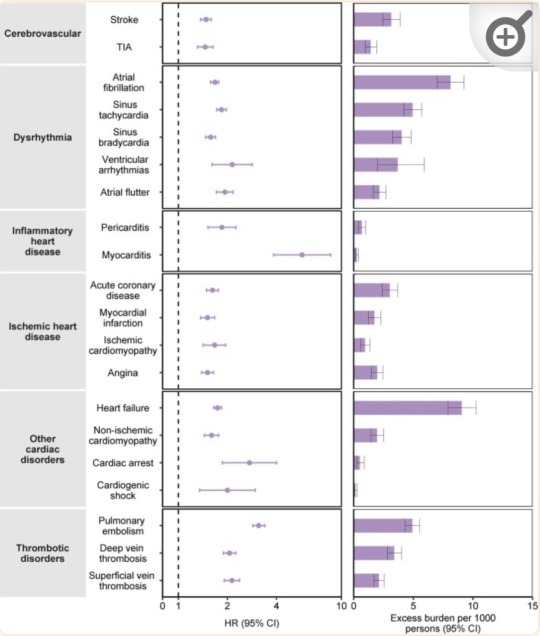
“Risks and 12-month burdens of incident post-acute COVID-19 cardiovascular outcomes in participants without any history of cardiovascular outcomes prior to COVID-19 exposure compared to the contemporary control cohort.” (Xie et al., 2022)
Published Research
Core mitochondrial genes are down-regulated during SARS-CoV-2 infection of rodent and human hosts | Science Translational Medicine Guarnieri, J. W., Dybas, J. M., ... Wallace, D. C. (2023).
Long-term cardiovascular outcomes of COVID-19 - PMC (nih.gov) Xie, Y., Xu, E., Bowe, B., & Al-Aly, Z. (2022).
Articles & Reports
Blood Clotting Proteins Might Help Predict Long COVID Brain Fog - Scientific American Reardon, S. (2023, September 1).
SARS-CoV-2 can damage mitochondrion in heart, other organs, study finds | CIDRAP (umn.edu) Van Beusekom, M. (2023, August 9).
Your vascular system and COVID | Heart and Stroke Foundation Heart and Stroke Foundation. (2023).
COVID, heart disease and stroke | Heart and Stroke Foundation Heart and Stroke Foundation. (2023, April 17).
How does coronavirus affect your heart? - BHF British Heart Foundation. (2023, March 21).
COVID-19 and Heart Damage: What You Should Know (clevelandclinic.org) Cleveland Clinic. (2022, May 10).
Heart Problems after COVID-19 | Johns Hopkins Medicine Post, W. S., & Gilotra, N. A. (2022).
COVID and the Heart: It Spares No One | Johns Hopkins | Bloomberg School of Public Health (jhu.edu) Desmon, S., & Al-Aly, Z. (2022, March 14).
COVID-19 takes serious toll on heart health—a full year after recovery | Science | AAAS Wadman, M. (2022, February 9).
Brain & Neurological Damage
Summary: COVID-19 infection increases your risk of developing cognitive impairments, mental health issues, poor memory, early onset dementia, and permanent loss of smell due to brain damage and the atrophy of brain matter. "Brain fog" and problems concentrating are common complaints post-infection that have also been linked to brain damage. Damage to blood vessels due to inflammation during the infection may be responsible for this by restricting oxygen flow to the brain. COVID-19 may also directly infect the brain.
Published Research
Biology | Free Full-Text | Vascular Dysfunctions Contribute to the Long-Term Cognitive Deficits Following COVID-19 (mdpi.com) Shabani, Z., Liu, J., & Su, H. (2023).
Frontiers | COVCOG 2: Cognitive and Memory Deficits in Long COVID: A Second Publication From the COVID and Cognition Study (frontiersin.org) Guo, P., Ballesteros, B. A., Yeung, S. P., Liu, R., Saha, A., Curtis, L., Kaser, M., Haggard, M. P., & Cheke, L. G. (2022).
COVID-19 and cognitive impairment: neuroinvasive and blood‒brain barrier dysfunction - PMC (nih.gov) Chen, Y., Yang, W., Chen, F., & Cui, L. (2022).
Comparison of post-COVID depression and major depressive disorder | medRxiv Perlis, R. H., Santillana, M., Ognyanova, K., Green, J., Druckman, J., Lazer, D., & Baum, M. A. (2021).
Articles & Reports
Long COVID May Impair Memory, Cognition for Months (healthline.com) Rossiaky, D. (2022).
COVID Variants Can Affect the Brain in Different Ways - Neuroscience News (2023).
The hidden long-term cognitive effects of COVID-19 - Harvard Health Budson, A. E. (2021). Harvard Medical School.
Long Covid: Even mild Covid is linked to damage to the brain months after infection (nbcnews.com) Ryan, B. (2022). NBC News.
COVID-19 Can Affect the Brain Even Long After an Infection | Time Ducharme, J. (2023). Time.
Lung Damage
Summary: COVID-19 infections can cause lung damage or scarring, and can trigger pneumonia, bronchitis, ARDS, and sepsis. Additionally, some people experience shortness of breath (dyspnea) and difficulty exercising as a post-acute sequela after infection, or multiple infections.
Published Research
At a crossroads: COVID-19 recovery and the risk of pulmonary vascular disease - PMC (nih.gov) Cascino, T. M., Desai, A. A., & Kanthi, Y. (2021).
[Pulmonary manifestations in long COVID] - PubMed (nih.gov) Sommer, N., & Schmeck, B. (2022).
Residual Lung Abnormalities after COVID-19 Hospitalization: Interim Analysis of the UKILD Post-COVID-19 Study - PubMed (nih.gov) Stewart, I., Jacob, J., George, P. M., Molyneaux, P. L., Porter, J. C., Allen, R. J., Aslani, S., Baillie, J. K., Barratt, S. L., Beirne, P., Bianchi, S. M., Blaikley, J. F., ...Jenkins, G. R. (2023).
Articles & Reports
Even mild cases of COVID-19 may cause long-term lung damage - UPI.com HealthDay News. (2022). United Press International.
COVID-19 Lung Damage | Johns Hopkins Medicine Galiatsatos, P. (2022).
Immune System & Autoimmune Diseases
Summary: COVID-19 infection can impair the functioning of your immune system. This means that those who have previously been infected are potentially immunocompromised (higher risk). For some people, the way COVID-19 impairs their immune system results in the onset of autoimmune diseases.
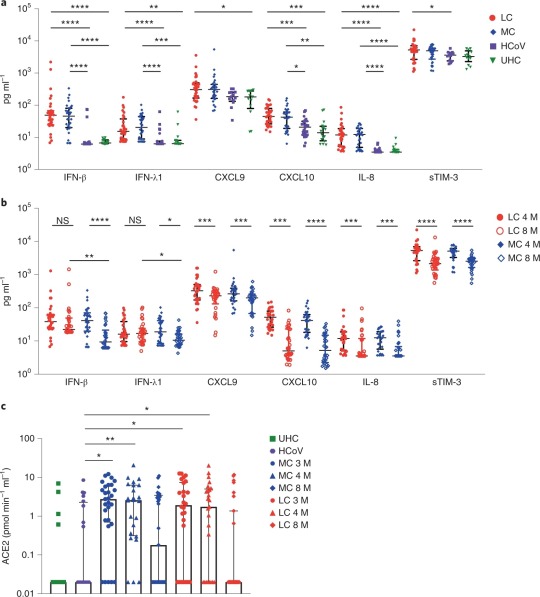
“Elevated levels of proinflammatory cytokines that persist more than 8 months following convalescence.” (Phetsouphanh et al., 2022)
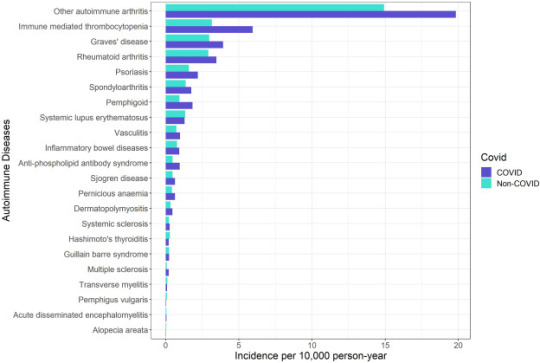
“Crude incidence of each autoimmune disease by COVID-19 and non-COVID groups.” (Peng et al., 2023)
Published Research
Immunological dysfunction persists for 8 months following initial mild-to-moderate SARS-CoV-2 infection | Nature Immunology Phetsouphanh, C., Darley, D. R., Wilson, D. B., Howe, A., Munier, M. L., Patel, S. K., Juno, J. A., Burrell, L. M., Kent, S. J., Dore, G. J., ... & Matthews, G. V. (2022).
Long-term perturbation of the peripheral immune system months after SARS-CoV-2 infection | BMC Medicine | Full Text (biomedcentral.com) Ryan, F. J., Hope, C. M., Masavuli, M. G., Lynn, M. A., Mekonnen, Z. A., Yeow, A. E. L., Garcia-Valtanen, P., Al-Delfi, Z., Gummow, J., Furguson, C., ... Lynn, D. J. (2022).
Risk of autoimmune diseases following COVID-19 and the potential protective effect from vaccination: a population-based cohort study - eClinicalMedicine (thelancet.com) Peng, K., Li, X., Yang, D., Chan, S. C. W., Zhou, J., & Wan, E. Y. F. (2023).
Long-term perturbation of the peripheral immune system months after SARS-CoV-2 infection | BMC Medicine | Full Text (biomedcentral.com) Winheim, E., Rinke, L., Lutz, K., Reischer, A., Leutbecher, A., Wolfram, L., Rausch, L., Kranich, J., Wratil, P. R., Huber, J. E., Baumjohann, D., ... Krug, A. B. (2021).
Articles & Reports
How COVID-19 Changes the Immune System | Time Park, A. (2023, August 18).
How COVID-19 alters the immune system -- ScienceDaily ScienceDaily. (2021, October 28).
Impacts of COVID on the immune system (medicalxpress.com) Herrero, L. (2022, September 19).
COVID-19's impact on the immune system, and how this may affect subsequent infections - ABC News Smith, B. (2022, December 1).
COVID-19 can derange immune system; survivors have autoimmune diseases (usatoday.com) Szabo, L. (2021, March 2).
Long COVID & PASC
Summary: Long COVID is an umbrella term that refers to the onset of disabling symptoms/conditions resulting from any of the previously mentioned organ, immune system, and vascular damage sustained during infection. These conditions are also referred to as "post-acute sequelae of COVID-19" (PASC). Vaccination can reduce the damage experienced by decreasing inflammation during an infection, but Long COVID/PASC can affect anyone. This is especially true in the case of multiple infections. Your risk of developing Long COVID, or worse/new symptoms, increases with each additional infection.
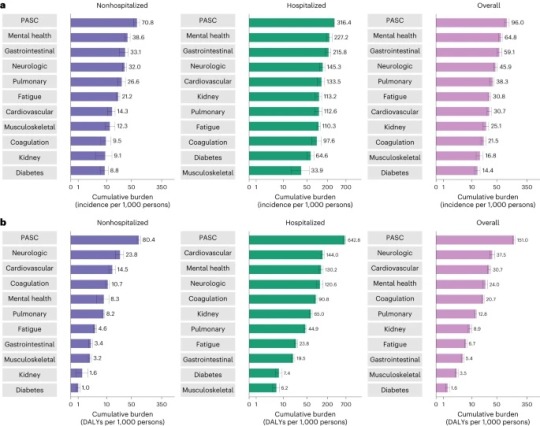
“Cumulative incidence and DALYs of postacute sequelae overall and by organ system at 2 years after infection.” (Bowe et al., 2023)
Published Research
T cell apoptosis characterizes severe Covid-19 disease - PubMed (nih.gov) André, S., Picard, M., Cezar, R., Roux-Dalvai, F., Alleaume-Butaux, A., Soundaramourty, C., Cruz, A. S., Mendes-Frias, A., Gotti, C., … Estaquier, J. (2022).
SARS-CoV-2 reservoir in post-acute sequelae of COVID-19 (PASC) | Nature Immunology Proal, A. D., VanElzakker, M. B., Aleman, S., Bach, K., Boribong, B. P., Buggert, M., Cherry, S., Chertow, D. S., Davies, H. E., Dupont, C. L., ... Wherry, E. J. (2023).
The immunology of long COVID | Nature Reviews Immunology Altmann, D. M., Whettlock, E. M., Liu, S., Arachchillage, D. J., & Boyton, R. J. (2023).
Long COVID: major findings, mechanisms and recommendations | Nature Reviews Microbiology Davis, H. E., McCorkell, L., Vogel, J. M., & Topol, E. J. (2023).
Long COVID prevalence and impact on quality of life 2 years after acute COVID-19 | Scientific Reports (nature.com) Kim, Y., Bae, S., Chang, H., & Kim, S. (2023).
Postacute sequelae of COVID-19 at 2 years | Nature Medicine Bowe, B., Xie, Y., & Al-Aly, Z. (2023).
Articles & Reports
Long COVID | NIH COVID-19 Research National Institutes of Health. (2023, June 8).
Long COVID or Post-COVID Conditions | CDC Centers for Disease Control and Prevention. (2023, July 20).
The Most Important Question About Long COVID | Harvard Medical School Pesheva, K. (2023, August 9).
Nearly One in Five American Adults Who Have Had COVID-19 Still Have "Long COVID" (cdc.gov) Centers for Disease Control and Prevention. (2022, June 22).
2 notes
·
View notes
Text
The Weight of 2020
When did it start? The first time you put on a mask, fabric trapping your breath? The first day of quarantine, when you gazed out the window at streets so barren, it was like everyone was already dead? The first time you heard the phrase ‘novel coronavirus’, before ‘novel’ became ‘new normal’? Or was it when you realized the pandemic was a string of firsts with no lasts? If the story of sickness has no beginning, how can you expect it to end?
Sometimes, it starts with a whisper– start small, skip breakfast. I hear it many times before I listen. You know you’re sick when a fever spikes, but the virus was waiting within you for days, even weeks. You were carrying the disease all along.
High temperature. Shortness of breath. Lunches emptied into the trash, untouched. I can get away with it; I eat alone. I was quarantined before it was cool. I sit in silence as my body burns, wishing the flames would devour me faster. Loss of appetite, loss of taste. It’s not so different, after all.
Nausea, vomiting– the same nights hunched over, heave and splatter. Is it the sickness, or is it me? Did I choose this? I didn’t catch it. I guess that makes it my fault. As I empty myself of all that I am– you are what you do not eat– I feel her watching from the mirror.
An issue of self-image– the self and the image refuse to be joined. They are much more than a hyphen apart, lacking the quickness of Covid-19, uttered in a single hushed breath. Self. Image. Illness isolates; you become well-acquainted with the separate self.
Rising numbers. Flatten the curve. Fear is a line graph angling steeply toward an unseen zenith, stolen moments of normalcy shattered by too much, too much, too much! It haunts me, like the silence that falls after a cough in the supermarket, the cessation of safety, sanity. The resuming clatter of carts cannot lighten air left leaden, laden.
When you’re sick, you want to get well. I don’t want to be well; I want to be nothing. I don’t want to rest, drink water, breathe. What I really want is to erase myself, but there’s no escape from the grotesqueness of flesh, the ghoul in the mirror.
It’s not my body—all the forgiveness I do not have weighs on me. If there was ever a time to forget compassion, it would be now. You expect, somewhere between the hoarding and hysteria, for the mask of humanity to slip. I expected it, in my animal brain of hurts and hungers, but I was proven wrong.
A week after the graduation I never had, I tried to carry a box. It was light, but I was weak, and getting to the post office, half a mile from my shell of a dorm room, was more than I could bear.
It wasn’t just the box. It was the gaping windows, lifeless eyes in the ruins of buildings still standing; Van Hise, where the elevators skipped floors 2-5; the humanities building, a concrete maze; the English building, where I should have gone to the award ceremony senior year, but the one year I won, the whole world lost. It was all the detritus of my former life suspended around me that made my task unbearable.
I was painfully aware of my tight breath, aching back, trembling hands. Trembling– what I was doing felt more violent, like tearing myself apart. My hands shook for hours afterward, but when I found myself collapsing under the weight of 2020, I dropped my box, and two girls picked it up. We were in a pandemic, but they saw my suffering body and rushed to its aid when I only ever saw myself as an adversary, an illness. To them, I was human.
So, I went to the hospital. My disease was not the one on anyone's lips, least of all mine. Even then, I was alone in the deepest way, too sick to be contagious. I wished I could have coughed to spread my pain. I laid there, staring at white ceilings, quarantined in my own head.
Recovery. For some, illness spends itself in days. In others, it lingers for months, years. Healing never happens all at once, in a moment of truth, the second we choose to get better. How do you know when you’re finally well? How do you know when the pandemic’s over?
How do you vaccinate for anorexia?
#original fiction#flash fiction#covid#tw ed#recovery#I wrote this back when I was going to a local writer's workshop last fall but I don't think I ever posted it
1 note
·
View note
Text
Covid-19 : 2 Big Legal Tips!
Two Big Covid-19 Legal Tips
When Wilma (all names changed) went to the hospital for Covid-19, they had to put her on a ventilator.
But years ago, Wilma had signed something called a living will which said that she did not want to be hooked up to any machines. What should the doctors do?
In Louisiana, a living will is a legal document that tells your doctors and your family whether or not you want to be hooked up to machines in order to keep you alive. Of course, if you are conscious and competent, then you can tell the doctors what to do about the machines regardless of what your living will says. But in Wilma’s case, she was unconscious. In a situation like that, the doctors are going to be interest in whether she has a living will.
But living wills only apply in certain situations. Here’s what Louisiana law says: the doctor must follow your living will if you have “a terminal and irreversible condition” and you are “comatose, incompetent, or otherwise physically or mentally incapable of communication.” When it comes to determining whether you have “a terminal and irreversible condition,” two doctors must agree that you are in “a continual profound comatose state with no reasonable chance of recovery” or you have “a condition caused by injury , disease, or illness which, within reasonable medical judgment, would produce death and for which the application of life-sustaining procedures would serve only to postpone the moment of death.”
In other words, if there’s a chance that you can recover, then the doctors are going to hook you up to the machines. A living will only applies if two doctors have determined that you’re not going to get better and hooking you up to the machines would keep you alive but only “postpone the moment of death.”
So, Wilma’s got Covid-19. Contrary to what you may have heard, that isn’t necessarily a death sentence. Intubation and placement on a ventilator might actually save Wilma’s life. She could get better and be just fine. Her condition isn’t “terminal and irreversible.” In “reasonable medical judgment,” there is a “reasonable chance of recovery.” That means that Wilma’s living will doesn’t apply to her situation.
Tip #1: Some living wills say that under no circumstances is the patient to be intubated. Is that really what you want?
But let’s get back to Wilma. The doctors have decided that there’s a “reasonable chance” that she could recover. But she’s still unconscious and can’t tell the doctors what to do. What happens then?
If Wilma has a health care power of attorney, then the doctors are going to ask the power of attorney what to do. In Wilma’s case, she had given her health care power of attorney to Fred, her husband. Which means that Fred will have to decide whether to have his wife put on a ventilator.
The difference between a living will and a health care power of attorney is whether or not the patient has a “terminal and irreversible condition.” If so, then the doctors are going to do what the living will says. But if it’s not a “terminal and irreversible condition,” then the doctors will go ask your power of attorney what to do. And in usual circumstances, the doctors would ask Fred in person. But with the Coronavirus, that may be impossible.
Tip #2: Which brings me to tip #2: make sure that your health care power of attorney specifically says that your agent (the person you give health care power of attorney to) has authority to communicate with your medical professionals by phone and electronic means.
That shouldn’t be necessary. There is nothing in Louisiana law that says that powers of attorney can only act in person. But does your health care agent know that? Do all health care providers in the state of Louisiana know that? The point of a good estate plan is to prevent problems before they happen. Especially in our Coronavirus times.
https://www.gilsoul-law.com/covid-19-2-big-legal-tips/
#power of attorney#family law attorney#living will#living trust#attorneys in shreveport#elder lawyer
0 notes
Text
☽ Crystal Magic / Part Three ☾
I explored and discovered a myriad of concepts all stemming from powerful anecdotes. Jeannie Di Bon offers much information. Nikki has become a personal inspiration to me, especially with how she discusses more social elements of fitness and how they discourage hypermobile individuals and hinder our success. Dr. Jen Crane expresses a lived reality that juxtaposes the very treatment guidelines I was initially given regarding Ehlers Danlos and hypermobility.
Holy shit. My dead mother left me to inherit her disease without a single cue of guidance, nearly a thousand miles away from the genetic blood that looked and lived like she and I alone did. Suddenly, every time I unlocked my phone, I was faced with images of people who looked like me and who hurt like me and who, like me were discovering and sharing about the relief that exercise can bring to individuals with hypermobile conditions. My mom had, in her best mindset, at times in my childhood, told me stories about how when she lifted weights, she was the healthiest she’d ever been—folly, dreaming up a fantasy of doing it all over again, and imagining, maybe hopelessly, but maybe almost in genius, that weights were the real cure all along.
I took off. I’d already known a bit about fitness thanks to childhood interests and pursuits. A more psychologically sound understanding of how to appropriately maintain my intake and body image allowed me to properly nourish myself. I gained strength rapidly. Occasional classes, many work-books and an exercise mat, resistance bands, free-weights and even sometimes going to a real-life -gym—it all became just another part of my routine.
I became stronger than I could ever remember being. I became profoundly more able-bodied than I’d been in years. I walked at a theme park—and rode roller coasters—and felt good.
And then, something sinister started cooking. Finally, the last piece of the equation shuffled out from behind a curtain, and I was faced with the finale of my psycho-spiritual-medical-crisis.
In late 2022 I caught coronavirus despite being fully vaccinated. I’ve read that those of us who had an allergic reaction to the vaccines might be more prone to actual infection should the vaccines efficacy be reduced. Either way, I caught it. Miraculously, my usually-life-threatening asthma didn’t seem to flare up nearly as much as another part of my body—a part I had long thought I was quite literally divinely intimate with: my nerves.
It started with intense cold flashes and sweats. I don’t remember much besides the misery of those sensations. I recovered from Covid relatively quickly, so I thought I’d gotten away without incident. As the months past my recovery began to add up, however, I found myself facing a whole new set of symptoms. When the holidays rolled around, my partner helped me piece together that these symptoms were not, in fact, new, but instead were just now very pronounced.
Irritiability, severe insomnia, sleep disturbances, visual hallucinations and convulsions began dominating a week out of every month of my life. It quickly became so disorganizing that I found myself unable to keep up with my diet or exercising as neatly as my health generally required—which I’m certain only worsened things. I didn’t understand it—not at all—and moaned to my therapist about how my rising symptoms simply didn’t make sense.
I’m not ready to address most of what happened next because as it continues to unfold, I still struggle to process it all. What I will say, however, was that my small family was hit with a sobering realization. For a lifetime, I’d been excused away with “mental illness” as many women and people assigned female at birth are. “It’s just anxiety,” they’d say. We discovered something I never could have imagined, thanks to my background; Anxiety isn’t always the cause of something—sometimes, anxiety is a symptom.
And sometimes, meditation isn’t the most reliable treatment, despite its accessibility.
My new understanding might be new, in fact, but I’m told that everything about me has been present from the start, and instead, it’s merely the environment I interacted with that has both emboldened and extinguished various aspects of my DNA. Perhaps, with a stronger, less wobbly neck, I would have a condition with a different name, or have no condition at all. Perhaps if I’d grown up never meditating or playing videogames or sitting much too close to the tv screen or listening to binaural beats very loudly in the attempt to depersonalize from my period cramps, perhaps things would be different. Instead, this is my reality.
Something big awoke in me. It coincided with meeting a friend who herself was so fully invested in the realm of spirituality that she seemed to pull it out of whatever metaphysical box-in-the-closet I’d yet again returned it all to within myself. My crystal garden made it’s way out into the living room. White candles appeared. A pendulum gently rests on a glass end table, reflecting the image of its own crystalline structure, looking four-dimensional.
If this entire time the very labels of my conditions were little more than unmedicated symptoms, then what else do I have to trust but that intuition that I have found for myself, by myself, and within myself, which I can carry with me everywhere?
I always knew it was real. It wasn’t the presence of ghosts, nor a sensation generated by my psychology—though certainly worsened by its illness.
My own anxiety is a symptom, an aura. My suicidality is nothing more than a temporary, illegitimate side effect. That’s why no amount of cognitive reasoning has ever touched it. It’s not a thing that exists in the realm of reason, but an impulse that exists in the same way of my need for vestibular stimulation during a temper tantrum.
These feelings are not the problem—they’re a cue that the problem is acting up again. Just like the kaleidoscope headaches. Just like the shaking in bed at night.
“Catamenial,” they go on, charting in their little documents. Treatment-resistant. More cancer-causing-hormone-pills, less kundalini-breathing.
No. No, to put it simply. No longer are my experiences merely a collection of human behaviors meant to be labeled and categorized so that I might slip through every possible crack in the system for decades like my mother had. When I learned that my anxiety itself was merely a symptom of something else that was happening inside of my brain—something that apparently, is mostly influenced by the level of estrogen circulating in my body—I felt like the world as I knew it had ended. I know, PMDD, etc., all of these other catch-all labels exist to describe what I suppose one could call hormone-related-mood-changes—but to describe this phenomenon as PMDD, an arm-chair descriptor that people are nearly encouraged to self-diagnose with, would be like describing the alphabet without phonetics. Why PMDD?
Why are the symptoms happening—not “what are they”, and “how can we put a band aid over them and ignore them until whatever underlying condition initially caused them spirals out of control, spills all over the floor and makes a big mess everywhere?”
What mechanisms in the brain are genuinely responsible for the experiences of a patient? Through the lens of psychology, despite the field vocally recommending away from Freudian roots, one human being can quite literally observe—as in, using only their core senses, and making only direct notations—the deeply rooted, totally invisible, mysterious, largely inexplicable interpersonal workings of another human’s brain. Sure, the anecdotal, self-reported status of patients improve alongside the treatment of these “immaterial” symptoms. I told myself I had PMDD, and my childhood counselor agreed with me, and my “treatment” of sticky-notes telling me I’m pretty on the mirror seemed to help. Yet it hadn’t, but to fulfill the social role of psychiatric illness, I told myself, my doctor and everyone else that it did. Meanwhile, the twisted neurological and endocrinological concoction that was actually behind my conditions, one that influenced every single fathomable aspect of my perception, decision-making, executive function and socialization continued to devolve.
It's so easy for this timeline to occur with any condition where physical proof of its very existence is lacking. I don’t mean to discredit the studies of “depressed brains” and such, which of course really do convey meaningful data, but to simply call into question the expediated pace at which someone with profound medical abnormalities might somehow find themselves rapidly re-focused on coping with their deterioration rather than taking accountability to prevent it. Why was my condition labeled as “PMDD” before a single EEG was ever done on me? I’ll answer that—because the psychologist who told me I had PMDD didn’t need to run an EEG for the insurance to pay her for my continued sessions. I don’t blame her, or any psychologist who are part of the many that I believe to be overly diagnosing mental illnesses that might be side effects of untreated physical illnesses—especially in areas where healthcare access is strained. We all just want to feel better and help each other feel better… But at some point, we must take responsibility for the enterprises we subscribe to without protest. Those enterprises may be of science or of religiosity—but in this specific example, in this chapter of my personal story—the scientific truth was delivered to me through a god-fearing scientist. How ironic.
Oh, the book of shadows—the pretty little labeled jars of quartz and things that are just quartz but with pigment, and other, actually precious stones—and the white candles laced with jasmine oil—they all found their ways right back, front-and-center in my home. Feeling unsafe inside of one’s own mind is quite the experience. Pascal and his wager had nothing to do with it, this time, however. Instead, I was searching for a comfort that I realized no form of science could ever award me with.
At first, my neurology was all over the place, and everything felt spontaneous and pattern-less. With the practice of my long-locked-away spiritual mindfulness, however, slowly, I have been becoming more able to recognize the semi-conscious patterns in my neurology that I’ve been mislabeling as anxiety for decades. When I meditate, I can feel my brain. I can pay attention to how it feels. I can notice little things. For most of my life, those little things were labeled as evil. Then, they were labeled as some kind of Munchausen or psychosis. Then, thanks to one single doctor, I came to learn that they were in fact my brain experiencing itself and trying to explain those experiences back to me. They are clues indeed, and those very clues will go on to help expert doctors find a long-term treatment for me that isn’t nearly as risky as some of the blanket-treatments for my conditions. Yes, to the experts, these phenomena are measurable and relatively simple to study. Perhaps not with Freudian psychotherapy—but with simple labs and imaging.
Alas, I am finally liberated to begin to take ownership of these experiences. Not a “mental illness” that I must constantly battle against to retain my artificial “I’m a good and normal person” token—not the spiritualist woo that I grew up on, balancing good versus evil—but simply put, biology. On the glass table where I’ve fabricated my little would-be alter, if I were a conventional, non-secular type, a slice of citrine glitters underneath my ceiling fan. It helps me relax during the meditative practices that have found their way back into my daily routine. Only because I, for myself, because of myself, and entirely by myself decided so—I uphold my practice. It makes me feel good, and I now know how integral and critical the sensation of “feeling good” is to my measurable neurological wellbeing. The “feel good” is the absence of severity in many of the neurological challenges I live with. It is not victim to the advice, wisdom, influence or even suggestion of others—not grifting diviners or established churches or stemming from even a single branch of modern medicine.
Instead, I am focused on the philosophy behind the creations of medicine and psychology themselves. 5,000 years ago, when humans were initially preserving information about mental and physical health, the concepts of medicine and psychology were often, if not always unified. A deviation point from this unified perspective, at least in Western thinking, might be, for example, Cartesian dualism. Contrastingly, however, certain concepts associated with early human medicine, often questioned as archaic or outdated, permeate into the everyday lives of many peoples.
Aspects of archaic medicinal cultures continue to suggest the applicability of such concepts through the day, such as in the still-popular techniques described in Ayurvedic medicine. In Ayurvedic medicine, the various more consumable treatments simultaneously affect physical and mental health. Some physical ailments are suggested to co-occur with mental ailments, or there is such a pattern where any one kind of patient complaint would immediately warrant investigation into the corresponding psychological or physiological complaints to those ascribed sorts of issues. I think this juxtaposes well against the western use of medicine that isolates and treats one specific problem, while describing the other, undesirable results of the treatment on other bodily systems, or on the mind, or on the body itself, depending on the treatments context, as simple, predictable side effects. Medicine has long had roots in a more epistemological, relational background, which many people find anecdotally superior to this day.
I, however, have realized, from this sort-of-bird’s-eye-view forcibly provided to me by chronic illness, that subscribing to any single body of thought, particularly any that is absolutist in its declaration, might be provably un-helpful. Once any concept, even a medical concept, becomes well-known enough, I believe it all becomes a bitter game of “telephone” between speakers and leaders and their audience. One can either go to heaven or to hell—one can choose to live the ultimate healthy lifestyle, or a savagely short one—one might be infinitely ethical or practically evil—black and white thinking frames the conversation. As the history, research and data is transcribed over and over across not only thousands of years but thousands of miles, too, observers can become empathetic toward the situation that has resulted in multigenerational agony in my family. Other people will find means to justify the acceptance or growth of the concept they defend. Yet it doesn’t take long for something with a tremendous capacity for healing to be turned into a way to blame an individual for their lack of medical treatment success, or the lack of success in other areas of their lives. Once a tool is being used to shame, limit or restrict other individuals, its capacity for harm has become apparent.
Am I a bad witch for being secular?
Am I bad depression-patient for turning to witchcraft?
A bad patient for not wanting pills?
Am I a bad person because I can’t eat only plants anymore?
Yes, and that is why all of those everyday-extremes warrant talking about. All of these communities might defame, exclude and otherwise seek to quiet my perspective because it breaks their systems of moral justification. Should I, even for a moment, humor any of these ethical extremes, I’ll find my fragile human brain thrown back into the make-believe cycle of spiritually condemning my sin-ridden, selfish-for-wanting-peace self to pain. Similarly, if I throw all of it away and rely on “conventions” to “make me feel better,” then I am simply crazy—as in, the only explanation for my ongoing dissatisfaction with either my state of being or the overt decay of our world—is that I must just be crazy… Until another genius comes around the corner with another test that nobody else had thought to run yet.
Now, this is where this article (err.. novelette) will become challenging as I attempt to convey my conclusion. I have personally concluded nothing besides liberty from this situation. I have come to the realization that the greatest source of “how I’m doing” quite really is myself. I can determine if a treatment, philosophy, or even a particular incident of practice is appropriate and dignifying for me. I don’t have to be vegan to eat fruit salad. I don’t have to believe in Aphrodite to practice witchcraft. I don’t have to take AEDs to control my seizures (at least yet). The liberty of removing myself from the constraints of hierarchical, social labels is unbridled.
So, my experiences have hopefully landed me enough perspective to guide other seekers into a path of their own conviction. I would recommend beginning to simply challenge or question some of the categories we have itemized our personhood into. Analyze the surrounding community of people in the group you’re reflecting on. Do those people live lives that you would like to have for yourself? Do they behave with traits that you want for yourself? Are they as authentic and genuine as you want to be? Rather than targeting an individual, identify more general sources of communication for these organizations or groups. It can be easy to fool ourselves with the help of a singular good-enough-looking role model.
I find it helpful to meditate on the color purple, the rock called amethyst, and other such subjects that express the bridging between what’s perceivable and what might be divine. If a placebo works, then it’s just as good as a drug. If a drug doesn’t work and makes you feel horrible, then regardless of what your blood tests say, is it really any better than just pretending you feel better? Humor my centering of dignity.
At the same time, one must be their own prescriber of placebos to avoid being conned into statistically supporting another capitalized ideology, which is certainly not easy. In a time where advertisements have slowly but surely replaced nearly all of the media we consume, it can be difficult to weave out what part of a persona is authentic—even within our own everyday friendships. Thus, like good little researchers, witches and scientists, we must explore, practice and test the concepts around us. Like in the way that we communicate with one another using words, pictures, gestures and metaphors—the physical world around us communicates back to us, not always in ways that appear quantified in lab work, and not always in ways that we might assume to be experiencing with our souls. Instead, we are left alone with our mindfulness and memories as our only real guides.
Faint words fall onto deaf ears in an audience of people I know are so much akin to me that I might as well be talking into a mirror. Perhaps I am, and I am okay with that. I am not rejecting either wellness or science, but rejecting the full-throttled trust and commitment to any pre-defined system, with or without checks and balances, because all of the logos and data and legends mean nothing next to ones active personhood. Do what feels genuinely, truly, authentically, and completely good.
Spend time with yourself. Check in with your body. Check in with your soul. Have a dialogue with your ethics. Acknowledge and engage with the thoughts in your head because, though it may feel otherwise, they are not happening to you—you are creating them. Justification is a psychological process that means nothing to much of the rest of the animal kingdom, who, thanks to a lack of Big Stupid Words like those I’m typing now, communicate with their natural world using only their most instinctive biology.
Your body is talking to you. Unlike you’ve been told, you might not have ever needed a translator.
References:
Palsson, O. S., & Whitehead, W. E. (2017). HORMONES AND IBS. IBS-and-Hormones. Retrieve d January 21, 2023, from https://www.med.unc.edu/ibs/wp-content/uploads/sites/450/2017/10/IBS-and-Hormones.pdf
0 notes
Text
How corona virus takes our life || Symptoms of COVID-19 || Preventive measures || Latest COVID-19
Watch The Video
Dosto aaj aap dekhenge ki coronavirus kaise kisi jan leta hai ,kaise wo hamare under aakar hame nuksan pahuchata hai.iske sath hi ham ye v janenge ki ham corona virus kaise bach sakte hai or coronavirus yaani COVID-19 Ke lakshan kya kya hai sabke ke bare me detail me janege. #amleshmahato
View On WordPress
#Amlesh#cdc coronavirus#coronavirus cases#coronavirus cases in india#coronavirus in india#coronavirus india#coronavirus map#coronavirus sneezing#coronavirus stats#coronavirus update#coronavirus worldometer#COVID-19#Is the coronavirus disease new?#Is the coronavirus disease the same as SARS?#Mahato#What is the official name of the coronavirus disease?#What is the recovery time for the coronavirus disease?#Who is most at risk for the coronavirus disease?
1 note
·
View note
Note
Dear Mr Badge, as a Brit I can't comment comfortably on the pandemic in the US - I'm just glad that you're staying as safe as you can. I'm having a bit of a contre-temps with the brother in law, however. He says Steve Rogers wouldn't wear a mask due to the serum. I disagree. Steve would wear a mask - if even just a handful of people do the same it's reducing the transmission risk. What I want to know, though, is what is on his masks? Has he been sewing scrubs and masks and donating them?
LOL, I bet he wears blue mask with a white star, he kinda has a brand.
I do think Steve would wear a mask for the same reason I think if he got sick he would be under 100% quarantine in a medical facility. The serum isn’t fully understood in almost any canon. Given we don’t know how his immune system works, it’s possible he could be a carrier, and it’s possible for disease to mutate; imagine he caught coronavirus, maybe even several times, and his immune system killed all but the very strongest strain, which he then asymptomatically spread to others.
I imagine, given he’s likely immune, he might volunteer to care for people who have covid and/or need recovery care.
166 notes
·
View notes
Link
LETTERS FROM AN AMERICAN
September 9, 2021
Heather Cox Richardson
After weeks of pleading with Americans to get vaccinated as Republican governors opposed mask mandates, ICUs filled up, and people died, today President Joe Biden went on the offensive.
Saying, “My job as President is to protect all Americans,” he announced that he was imposing new vaccination or testing requirements on the unvaccinated. The U.S. government will require all federal employees, as well as any federal contractors, to be vaccinated. The government already requires that all nursing home workers who treat patients on Medicare and Medicaid have to be vaccinated; Biden is expanding that to cover hospital workers, home healthcare aides, and those who work in other medical facilities. “If you’re seeking care at a health facility, you should be able to know that the people treating you are vaccinated.”
Using the Department of Labor’s Occupational Safety and Health Administration (OSHA), Biden will also make employers with 100 or more employees require that their employees either be vaccinated or show a negative coronavirus test at least once a week. He pointed out that big companies already are doing this, including United Airlines, Disney… and the Fox News Channel.
Together, the new vaccine requirements will affect about 100 million Americans, making up two thirds of all U.S. workers.
Biden also urged those who run large entertainment venues to require vaccines or show a recent negative test for entry. He has already required teachers at the schools run by the Defense Department to get vaccinated, and today he announced that the government will require teachers in the Head Start program, which is federally funded, to be vaccinated. He called on governors to require that all teachers and staff be vaccinated for coronavirus, as their states already require a wide range of vaccinations for other diseases.
Calling out those like Florida governor Ron DeSantis, who has taken a stand against mask mandates and is threatening to withhold the salaries of school officials who defy him, Biden said that “if these governors won’t help us beat the pandemic, I’ll use my power as President to get them out of the way.”
He is using the Defense Production Act to increase production of rapid tests and has worked with major retailers to sell those tests at cost for the next three months. The government has also expanded free testing at 10,000 pharmacies and will spend $2 billion to distribute nearly 300 million rapid tests to community health centers, food banks, and schools. He has ordered the Transportation Safety Administration to double the fines on travelers that refuse to mask.
After deploying nearly 1000 healthcare workers to address this summer’s surges in 18 states, the president is now sending in military health teams from the Defense Department. Meanwhile, he said, the U.S. continues to donate vaccines to the rest of the world, “nearly 140 million vaccines over 90 countries so far, more than all other countries combined, including Europe, China, and Russia.... That’s American leadership on a global stage, and that’s just the beginning.” The U.S. is now shipping 500 million more Pfizer vaccines to 100 lower-income countries.
“Many of us are frustrated with the nearly 80 million Americans who are still not vaccinated, even though the vaccine is safe, effective, and free,” Biden said. More than 175 million Americans are fully vaccinated, and for the past three months we have created 700,000 new jobs a month. But while nearly three quarters of those eligible have gotten at least one shot, the highly contagious Delta variant has ripped through the unvaccinated, who are overcrowding our hospitals, threatening the health of our children, and weakening our economic recovery.
“[D]espite America having an unprecedented and successful vaccination program, despite the fact that for almost five months free vaccines have been available in 80,000 different locations, we still have nearly 80 million Americans who have failed to get the shot…. And to make matters worse, there are elected officials actively working to undermine the fight against COVID-19,” Biden said. “Instead of encouraging people to get vaccinated and mask up, they’re ordering mobile morgues for the unvaccinated dying from COVID in their communities. This is totally unacceptable.”
“[W]e have the tools to combat COVID-19, and a distinct minority of Americans—supported by a distinct minority of elected officials—are keeping us from turning the corner…. We cannot allow these actions to stand in the way of protecting the large majority of Americans who have done their part and want to get back to life as normal.”
“We’ve been patient, but our patience is wearing thin. And your refusal has cost all of us,” he said. “So, please, do the right thing.”
The Biden administration is pushing back, too, on Texas’s Senate Bill 8, which prohibits abortion after 6 weeks and thus outlaws 85% of abortions in the state. Today, the United States of America sued the state of Texas for acting “in open defiance of the Constitution” when it passed S. B. 8 and deprived “individuals of their constitutional rights.” The United States has a “profound sovereign interest” in making sure that individuals’ constitutional rights can be protected by the federal government, the lawsuit declares. "The act is clearly unconstitutional under longstanding Supreme Court precedent,” Attorney General Merrick Garland said.
What is at stake in this case is the ability of the federal government to defend Americans’ constitutional rights against local vigilantes, a power Americans gave to the federal government in 1868 by ratifying the Fourteenth Amendment to the Constitution after white former Confederates in southern states refused to accept the idea that their Black neighbors should have rights.
Since the 1950s, the Supreme Court has used federal power to protect the rights of minorities and women when state laws discriminated against them. S. B. 8 would strip the government of that power, leaving individuals at the mercy of their neighbors’ prejudices. The government has asked the U.S. district court for the western district of Texas to declare the law “invalid, null, and void,” and to stop the state from enforcing it.
This issue of federal supremacy is not limited to Texas. Glenn Thrush of the New York Times today called out that in June, Missouri governor Mike Parson signed the Second Amendment Preservation Act, which declares federal laws—including taxes—that govern the use of firearms “invalid in this state.” Like the Texas abortion law, the Second Amendment Preservation Act allows individuals to sue state officials who work with federal officials to deprive Missourians of what they consider to be their Second Amendment rights. “Obviously, it’s about far more than simply gun rights,” one of the chief proponents of the bill, far-right activist Aaron Dorr, said to Thrush about his involvement.
There were other wins today for the Biden administration. Today was the deadline for federal agencies to produce a wide range of records surrounding the events of January 6 to the House Select Committee to Investigate the January 6th Attack on the United States Capitol, and according to the committee’s Twitter feed, those records have, in fact, been forthcoming.
And Taliban officials did allow a plane carrying about 115 Americans and other nationals to leave Afghanistan.
Biden’s new approach to the pandemic is, as Josh Marshall of Talking Points Memo points out, good politics as well as good for public health. About 65% of the voting age population is already vaccinated, and older people are both more likely to be vaccinated and more likely to vote. With most Americans vaccinated and increasingly frustrated with those who refuse, there is little political risk to requiring vaccines, while Republicans standing in the way of public health measures are increasingly unpopular. Florida, where deaths from coronavirus soared to more than 300 a day in late August, has begun to limit the information about deaths it releases.
If Biden’s new vaccine requirements slow or halt the spread of the coronavirus, the economic recovery that had been taking off before the Delta variant hit will resume its speed, strengthening his popularity. Those Republican lawmakers furious at the new vaccine requirements are possibly less worried that they won’t work than that they will.
Notes:
https://www.justsecurity.org/wp-content/uploads/2021/09/lawsuit-doj.pdf
https://www.whitehouse.gov/briefing-room/speeches-remarks/2021/09/09/remarks-by-president-biden-on-fighting-the-covid-19-pandemic-3/
https://www.cnn.com/2021/09/09/politics/biden-administration-texas-abortion-law/index.html
https://january6th.house.gov/news/press-releases/select-committee-issues-sweeping-demand-executive-branch-records
https://www.nytimes.com/live/2021/09/09/business/economy-stock-market-news
https://docs.google.com/document/d/1b3CD2rFn105IQ7ziTfcTT5m8bzv1gBXE5-RXEV0phMM/edit
https://www.nytimes.com/2021/09/09/us/politics/missouri-gun-law.html
https://www.cbsnews.com/news/afghanistan-news-taliban-to-let-americans-evacuate-flights-from-kabul-airport/
https://www.nbcmiami.com/news/local/as-covid-deaths-soar-florida-curtails-public-records-on-which-counties-hit-hardest/2547538/
Josh Marshall @joshtpmThe vax mandate is good public health. It’s also good politics. A big majority of the voting age population is already vaxed. About 65%. Propensity to vote and likelihood of being vaxed both rise with age. The vaxed are losing patience w the voluntarily unvaxed who …
288 Retweets1,742 Likes
September 10th 2021
LETTERS FROM AN AMERICAN
HEATHER COX RICHARDSON
#vaccine mandate#COVID-19#public health#vaccination#Federal Government#The US Constitution#political#Heather Cox Richardson#Letters From An American
4 notes
·
View notes
Text
also preserved at the archive
By: Jessica Wildfire
You don't need me to tell you how bad it's getting.
I'll tell you anyway, though.
As we drown in endless waves of Covid that generate millions of infections and thousands of deaths per week, our leaders have effectively stripped away every tool we have. They prefer a society that sacrifices themselves for short-term economic and political gains and then becomes ripe clientele for the pharmaceutical industry. They collude with the media to push out a daily barrage of misinformation aimed exclusively at ensuring we continue to work, shop, and vacation, because that's what they care about. Meanwhile, they do absolutely nothing about pandemics on the way as dozens of diseases spread out of control, at levels 10 times worse than normal. As the World Health Organization sounds alarms, telling us "we have arrived in the post-antibiotic era," and that we faced a future pandemic up to 20 times worse than Covid, our leaders focus on vibes. That last part should get our attention. Yes, we are here. We have arrived in the time when superbugs aren't responding to antibiotics. If that weren't bad enough, they're preying on our weakened immune systems.
And bird flu has likely gone human to human.
But it's not hopeless.
Four years ago, we looked to plants to protect us from pathogens because vaccines and treatments weren't coming anytime soon. The minute those vaccines and antivirals came out, most people forgot all about plants. They reverted to their old assumptions that plants were for hippies.
Well, here we are again.
Our vaccines and treatments are failing, and when they work they're often in short supply, or we can't even get access to them. Moms and dads are rolling out the NyQuil in little cutesie Facebook posts, along with all the pills that treat the symptoms but leave the disease itself to roam free all over your body.
We can do better.
As we mask while demanding clean air and better medicine, it's time to revisit those plants and see what they can do.
Do they even work?
Yeah, they do.
A 2024 review of studies in Viruses identified 10 different plant compounds with broad antiviral properties and effectiveness specific to Covid (and in many cases several other viruses). As they write, "plat-derived molecules can tackle viruses by acting on different aspects of their infection process" and "inhibit coronavirus/host protein pathways" by blocking them. The authors initially identified 45 different compounds and then narrowed them to the 10 most effective.
Plants work because they contain terpenoids, flavonoids, phenols, and alkaloids that all demonstrate "high anti-viral potential against SARS-CoV-2 particles" as well as other viruses. They do this in a variety of ways that work across variants because they block virus entry while also tamping down replication and essentially "stopping its life cycle."
Sounds good to me...
Let's get into it.
First, ginkgo biloba contains two bioflavonoids called quercetin and rutin that can block Covid's 3CLPro BS PL-pro enzymes, as demonstrated in two different studies that looked at how they bind to parts of the spike protein. According to an article in Nature, 3CLPro plays a central role in virus replication, specifically for Covid. Ginkgo also contains kaempfero that inhibits Covid's envelope protein E, "consequently suppressing virus activity and proliferation." G. Biloba also brings an anti-inflammatory effect that can help with recovery as well.
Second, turmeric and curcumin "can either bind directly to the receptor binding domain of the viral S-proteins or secure ACE2 receptors of the hosted cell." Basically, they stop viral entry into your cells. As the authors write, a curcumin derivative called bi-demethoxycurcumin "displayed the best binding affinity" to spike proteins.
It also works on the original SARS virus.
Third, a common spice called artemesia annua demonstrated antiviral activity in clinical trials. The group who took an artemisia compound called artemisinin-piperaquine "took significantly less time to reach undetectable levels of SARS-CoV-2 than the controls." In fact, artemisinins "are known for their extended-spectrum antiviral activity." An artemisia derivative called artesunate has shown effectiveness against both DNA and RNA viruses including hepatitis and HIV.
Artemesia compounds work similar to ginkgo by latching on to five different parts of the spike protein "which might explain its remarkable binding affinity." In addition to flavonoids like quercetin, researchers have identified di-caffeoylquinic acid as doing a lot of the heavy lifting here. Like curcumin, these flavonoids also bind to ACE2 receptors on your cells and protect them. Medical researchers are working on refining these compounds into artenimol, a single high-potency compound for giving to patients.
Fourth, nigella sativa (black cumin seeds) have shown antiviral activity by disrupting viral RNA transcription. Carvacrol and nigellidine extracted from these seeds "can block ACE2 receptors, thus inhibiting the SARS-CoV-2 entry into the host cells."
Fifth, ginger (6-gingerol, 8-gingerol, 10-gingerol) can inhibit parts of the Covid spike protein. Specifically, it's the bioactive compounds geraniol, shogaol, zingiberene, and zingiberenol that do the blocking.
Sixth, garlic (allium sativum) shows antiviral activity. It contains compounds called allicin, ajoene, and garlicin that work against several viruses in the same ways as the other compounds, by targeting spike proteins, disrupting transcription, and protecting your cells' entry channels.
Next:
Cinnamon at 50 ug/ml operates the same way as the other compounds, by blocking host cell entry and viral replication. Rosemary (rosmarinus officinale) shows effectiveness in blocking viral activity, even in a study that compared it to the antivirals remdesivir and favipiravir.
Want an unusual suspect?
It's dandelion.
Dandelion extract has shown to be "effective against influenza virus infection" and in higher concentrations "showed efficacy against spike proteins... and its different mutants" in human lung and kidney cells, while also helping to prevent the cytokine storm that's often so deadly in the acute stage. Here in particular, studies have shown that dandelion extract works regardless of the variant.
Finally, oregano (origanum vulgare) extract demonstrates antiviral activity against many DNA and RNA viruses, including Covid and HIV. As the authors write, extracts "showed remarkable efficacy against equine influenza virus, canine coronavirus, RS, and H1N1. In fact, it can inhibit up to 74 percent of viral activity at certain sites.
Again, carvacrol does the heavy lifting.
I've looked at other supplements and extracts with antiviral properties. They include grapeseed extract, grapefruit seed extract, olive leaf extract, echinacea, St. John's-Wort, and elderberry.
A 2024 study found that oleuropein, found in olive leaf extract, demonstrates high antibacterial activity at 130 mg/ml and high antifungal activity at 65 mg/ml. Another 2022 study found that oleuropein showed significant effectiveness against Covid in hospitalized patients when they were given 250-500 mg every 12 hours for five days. (No real difference between 250 and 500 mg.) The study also reviews previous research that oleuropein has shown effectiveness against other viruses, including HIV and influenza. It works the same way as other flavonoids, lectins, secoiridoids, and polyphenols, by blocking ACE2 receptors.
A 2022 study reviews available research on elderberry (sambucus nigra), confirming antiviral activity against HIV, flu, and coronaviruses. As the researchers write, adults in clinical trials "showed a significant reduction in symptoms, averaging 50 percent." Elderberry has also shown the ability to stimulate the production of immune cells. A 2019 study confirms that elderberry works against flu via "multiple modes of therapeutic action," including the inhibition of replication and host cell entry. An extensive 2021 study looking at prior research found that high-quality elderberry extracts enriched with anthocyanin work especially well.
A 2022 study in Nature found that a mixture of St. John's Wort (hypericum perforatum) and Echinacea showed significant antiviral activity against Covid. Specifically capsules with .9 mg of St. John's "can significantly reduce SARS-CoV-2 viral load," peaking at 36 hours after the start of treatment.
St. John's Wort works just fine on its own. The authors stress the importance of maintaining its concentration if you add other compounds like echinacea.
That said, a 2022 study in Frontiers in Pharmacology found that echinacea at 4,000 mg for 10 days led to a substantial reduction in viral load and fewer hospitalizations when used to treat Covid patients.
Here's a chart docs.google.com/spreadsheets/d/1cTJ3lXHPUW7AyrZPXQb63IjmhVbahRm_7Y5IMxKcqO8/edit?usp=sharing&ref=okdoomer.io
You can also look up most of these supplements and extracts on Mount Sinai's health library. They'll give you a good breakdown. It's a good idea to talk with a doctor if you're skeptical or not sure about interactions with other drugs, or look at the studies on your own. The studies linked in the sheet provide the most detailed dose information I can find, usually presented in a table. Duration runs around two weeks for an acute illness and 3-4 months for chronic infections like HIV.
Do I think it's sustainable to take high amounts of supplements all year long to ward off all kinds of airborne diseases, for the rest of our lives? Not really. That's why we absolutely need clean indoor air, masks, better vaccines, and better treatments. Until then, at least we have this information.
List of studies raindrop.io/JW_Lists/alternative-treatments-47681852
So there you have it.
If you've been wondering whether this stuff really works, the answer appears to be a loud yes. We need more research on dose amounts, but the studies all point in the direction of taking as much as you can while staying within the safe limits, for the duration of any time you feel at risk of getting sick.
Most of these extracts work against multiple viruses. They also help regulate your immune system and push it toward a less inflammatory response.
That's good to know.
My family has been using some of these supplements for several years, and it might explain why we've managed to steer clear of Long Covid. We still wear N95 masks everywhere. We advocate for clean air and better vaccines, along with better treatments. In the meantime, it looks like we can up our supplement game and that it's actually going to bring some benefit.
This isn't magic.
These plant compounds work the same way as many of the antivirals on the market. Medical researchers have been researching the antiviral properties of plants for decades, and cultures have used them for thousands of years. Given our current outlook, they're worth taking seriously.
Use what you can.
#mask up#covid#pandemic#covid 19#wear a mask#public health#coronavirus#still coviding#sars cov 2#wear a respirator
24 notes
·
View notes
Text
Week 7: Relationship between social media and Covid-19 in Malaysia
Covid-19
The Coronavirus disease 2019 (COVID-19) is an illness caused by the SARS-CoV-2 virus, which causes mild to severe respiratory illness including death. In December 2019, COVID-19 was first identified in Wuhan City, Hubei Province, China. By January 2020, the COVID-19 outbreak was declared a global health emergency by WHO. (Medscape, 2021)

Social Media
Since the COVID-19 pandemic, social media has been a big part of everyone's day more than usual of social distancing and home lockdowns. They rely on news sources and social media platforms to seek health information for themselves and their loved ones. (de Calheiros Velozo J, 2018).
Social media platforms have provided easy access to health information which empowered people to evaluate their health-related concerns. (Tengku Mohd TAM, Yunus RM, Hairi F, 2018) As social media users typically produce and share health information available through local and international sources to the public world regarding the global COVID-19 pandemic. As everyone is eager to seek information and stay connected with other people during tough times where everyone is stuck at home.

It has been over a year since COVID-19 emerged from the world. Countries all over the world are at various stages of disease mitigation, As of October 29, 2020, Malaysia has recorded 29,441 total COVID-19 cases, with 18,499 recoveries and 246 total deaths. (Southeast Asia Covid-19 Tracker, 2020) Malaysia is perceived as one of the most successful countries in disease management thanks to Movement Control Order (MCO) on March 18, 2020. (Omar ARC, Ishak S, Jusoh MA, 2020) Since the implementation of the MCO, the Malaysian public has heavily relied on both local and international media for information relating to COVID-19. MOH Malaysia and the Malaysian National Security Council (NSC) are the official source responsible for communicating information regarding COVID-19. (Mohamad E, Azlan AA, 2020) After official sites have broadcasted important news, usually social media platforms like Facebook, Twitter and Instagram will rebroadcast in a simpler and shorter format to cater to a wider and younger audience, keeping everyone in the loop.

Social media may be handy in raising awareness and health information about COVID-19, but it may also raise potential fake news as well. For example, in August 2020, a message circulated on social media claiming the infrared thermometers being widely used to scan people when entering premises were causing brain damages. (Diyana Pfordten, 2021) However, the rumour quickly got shut down by the Health Ministry. Health director-general Datuk Dr Noor Hiisham Abdullah said "It is designed to detect and absorb heat in the form of infrared rays emitted from the human body and converts it into electricity. The electronic circuit within the thermometer processes the electrical signal to determine the temperature and display the reading on the screen. Since infrared thermometers do not emit harmful radiation, it is safe to use." (New Straits Times, 2020)

Conclusion
The internet and social media is a great tool to seek health information and get news about what is going on within Malaysia and all over the world. However read with caution, make sure they have citations, references and proof that they are not fake news.

References
David J Cennimo, 22 October 2021, Medscape, 26 October 2021, <https://emedicine.medscape.com/article/2500114-overview#a1>.
Abbas J, Wang D, Su Z, Ziapour A, 2 October 2020, Dovepress, 26 October 2021,
<https://www.dovepress.com/the-role-of-social-media-in-the-advent-of-covid-19-pandemic-crisis-man-peer-reviewed-fulltext-article-RMHP#cit0069>.
J Med Internet Res, 12 November 2020, JMIR Publications, 26 October 2021, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7674144/>.
New Straits Times, 3 August 2020, New Straits Times, 26 October 2021, <https://www.nst.com.my/news/nation/2020/08/613661/health-dg-no-infrared-thermometers-dont-cause-brain-damage>.cheers
2 notes
·
View notes
Text
Did you know, the government's planned response to Coronavirus goes entirely against WHO advice for countries? The best advice is Self-isolation and social distancing aka the advice from the World Health Organisation. The UK Government, instead, has dithered and dallied and refused to ban mass gatherings, close schools and universities (or at least make learning an online thing for the time being), and so on. That's because Sir Patrick Wallace, who is the chief scientific advisor to the government argues herd immunity is what is needed.
Now, he's not wrong. With diseases, herd immunity really helps. That's why we get told to get the vaccines for so many diseases like measles, mumps, rubella, the common cold, tetanus, etc. Because those vaccines give us immunity to the live version of the disease. This, in the long-run, protects those who can't have vaccines or who vaccines don't work on because they're immunocompromised.
Immunocomprised is, essentially, your immune system being crap at fighting off illness.
People with Asthma are immunocompromised.
People with Diabetes are immunocompromised.
People with Chronic Fatigue are immunocompromised.
People with Cancer are immunocompromised.
People who are Elderly are immunocompromised.
Herd immunity for most diseases is possible because of mass vaccinations (this is why you see so many "vaccinate yo kids!" memes on the internet, it's important and saves lives). Coronavirus is different to the diseases we have herd immunity for.
Corona has no vaccine as of yet.
The only way herd immunity will happen without a vaccine is through infection and recovery of the majority whilst a minority die due to the disease.
Approximately 42 million Brits would need to be infected for herd immunity to be effective against corona. With an approximate 2% fatality rate, 1.2 million people in the United Kingdom would die during this phase of obtaining herd immunity. These would be primarily disabled, elderly, and immunocompromised. But there would be those with undiagnosed health conditions who will die. You may think yourself healthy, family, or friends, but you could be blindsided by corona revealing a condition you didn't know you had and it could be the death of you.
This is why vaccination-based herd immunity is so important.
Corona is, in comparison to other diseases, not as deadly as you'd think, but it spreads fast and that is the risk of it. That's why the WHO advice for infected countries, and communities at risk of infection, is to self-isolate for two weeks (not just 7 days like the government has stated) and to engage in social distancing.
Avoid publicly crowded areas.
Cough into your elbow not the air.
Wash your hands for 20 seconds (the chorus of Mr Brightside works for timing).
Use a tissue if you sneeze.
Don't shake hands, wave in greeting.
If you feel sick, isolate yourself.
These are just a few, simple things you can do to both reduce the risk of infection and of spreading corona.
I know this post sounds very doom-and-gloom, but corona isn't the end of the world. It's a huge pandemic that the world wasn't ready for. That, with austerity and reductions to health services, is a huge strain on a strained system. But it's still something survivable.
You can recover from corona. It generally is just like a bad case of the flu. But even the flu can kill.
We need to be responsible and commit to rational, responsible behaviour. Don't ignore the threat just because you don't think you're at risk. We never think something bad will happen to us until it does.
#Important#UK#Coronavirus#Corona#Herd immunity#News#Kat talks#It's important to take it seriously yes#But also to not not take it seriously#We need to need to be responsible#And herd immunity without a vaccine is irresponsible
245 notes
·
View notes
Text
"Most states are reopening to some degree this week, even as public-health experts warn that it’s too soon. Proponents of early reopening use some variation of six arguments. Here is what’s wrong with each of them:
"Instead of preventing covid-19, we should let people infect each other to achieve herd immunity. 'Herd immunity' occurs when enough people in a community — generally 60 percent to 80 percent — develop antibodies to an illness, either through vaccination or recovery. Banking on herd immunity without a vaccine is a dangerous proposition: It’s unclear whether people acquire immunity after contracting covid-19. Even if those who recover become immune, an infection rate of 60 percent would mean nearly 200 million infected Americans. Millions could die.
Most cases of covid-19 are mild. "We can keep older people at home and allow young, healthy people to go back to school and work. This is wrong for multiple reasons. Older people aren’t the only ones contracting covid-19. One in 5 patients requiring hospitalization in the United States are ages 20 to 44, the Centers for Disease Control and Prevention found in March. Infected people in their 30s and 40s are dying of strokes.
"Even if young people are not as likely as older individuals to become severely ill, they can be asymptomatic carriers who spread the virus. Growing evidence suggests that children with mild or no symptoms can be highly contagious carriers. In New York, 66 percent of hospitalized covid-19 patients appear to have been sheltering at home. This suggests they probably contracted the virus from someone close who had exposure to others.
"People are getting sick and dying from other illnesses in greater numbers than covid-19. It’s true that emergency department visits for other illnesses are decreasing and that patients are eschewing medical treatment because they fear risking infection. Chronic medical conditions require care. Mental health is also affected by social isolation. Allowing the coronavirus to spread without restrictions would lead to hospital overcrowding, further inhibiting patients from obtaining necessary care.
"Controlling the pandemic, by contrast, would create confidence and increase people’s willingness to seek care for other conditions. Meanwhile, mental health needs to be a priority not only to help people experiencing isolation but also to treat the trauma and grief of those who have lost loved ones.
"It’s worth the sacrifice if some people die so that the country has a functioning economy. This is a false choice; there are ways to safely reopen, and consumer confidence depends on the reassurance of public health protections.
"Another flaw with this argument is that those making it are committing others to a sacrifice they did not choose. Covid-19 has disproportionately affected people of color, who are more likely to be essential workers, as well as to have chronic health conditions that make them more susceptible to severe illness.
..."We’ve been in lockdown for more than a month and cases aren’t declining; social distancing doesn’t work. Actually, social distancing has worked in places where measures were applied early and consistently. The two states with earliest known community transmission, California and Washington, avoided surges. New York was able to 'flatten' its curve, and the number of cases at this epicenter is declining.
"U.S. case numbers have not declined as much as case numbers in other countries because we have not applied the aggressive measures that some Asian and European countries have. At best, the United States has had a piecemeal approach. Some states never issued stay-at-home orders. Social distancing was intended to buy time to prepare hospitals and scale up capacity to test, trace and isolate coronavirus infections. Hospitals are better prepared than they were two months ago, but the country still lacks the resources for mass testing and contact tracing/isolation on the scale needed to tamp down infections. New Zealand and other countries have been successful when they combined social distancing with public health measures. U.S. inaction has limited the benefits we could have realized.
"We can’t keep the country in lockdown until a vaccine is developed, which could take years. No one is arguing to extend stay-at-home orders for years. But reopening criteria set out by the White House’s own coronavirus task force have not been met. Removing restrictions too soon would have predictably grim results.
"In reopening against public-health guidance, officials and others across the country have effectively decided to give up on trying to contain the coronavirus. This is a dangerous decision that is certain to lead to many preventable deaths. Let’s stop using misleading arguments to justify it."
132 notes
·
View notes
Link
Early results from a new international COVID-19 trial in people “has proven that a drug can block this virus.” Anthony Fauci made the announcement April 29 at a White House news briefing. Fauci heads the National Institute of Allergy and Infectious Diseases in Bethesda, Md., which sponsored the trial.
The drug is called remdesivir (Rem-DESS-ih-veer). And it seems to speed recovery from the new coronavirus by 31 percent. What that means: Patients on the drug tended to be released from a hospital or were well enough to resume normal activity four days earlier than people who got a placebo. A placebo is pill or liquid that resembles a drug but contains no active ingredients. Sometimes people call placebos “sugar pills.”
Explainer: What is a coronavirus?
“A 31 percent improvement doesn’t seem like a knockout 100 percent,” admitted Anthony Fauci. Still, he noted, “it is a very important proof of concept.”
The trial compared this drug to a placebo. Patients were randomly assigned to get either the drug or the placebo by an intravenous infusion. Neither the patients nor their doctors knew who was getting the real drug or the fake. Such randomized, double-blind, placebo-controlled trials are the gold standard for testing new drugs.
The trial began February 21 and involved 1,063 people hospitalized with COVID-19. The median time to recovery was 11 days for the remdesivir group. For those getting the placebo, it was 15 days.
Normally, researchers would not have announced the findings until the results had been reviewed by other scientists. But here the team chose to make the announcement early, Fauci said. “Whenever you have clear-cut evidence that a drug works, you have an ethical obligation to immediately let the people who are in the placebo group know so that they can have access [to the drug].”
Remdesivir will now be the standard of care against which all other drugs are judged, Fauci said.
Going forward, he noted, the initial trial will change. It will now compare this drug alone to its use with an antibody — one that aims to limit inflammation. Other drugs or antibodies may also tested to see if they do a better job than remdesivir.
Gilead Sciences of Foster City, Calif., developed remdesivir. The drug mimics a building block of RNA. That’s the coronavirus’s genetic material. When an infected cell attempts to copy the virus, the drug gets used instead of the usual RNA components. This cuts down how much virus is made.
126 notes
·
View notes
Text
Perception Of The Viruses & The Importance of COVID-19 Tests
Coronavirus is a virus family that affects both humans and animals. SARS, MERS, and NCoV are the three varieties of coronavirus. While these three diseases are similar in some aspects, they also have distinct characteristics that necessitate separate diagnostic and treatment approaches. This article examines the three types of coronavirus and how they are different from one another.
What Are The Three COVID-19 Test Types?
-First: A sort of coronavirus illness test is an RT-PCR test, which detects the virus directly. This test is performed on a person suspected of having the coronavirus's blood or respiratory secretions. -Second: Antibodies produced by the immune system to fight the disease are looked for in this test. This is referred to as a serology test. -Third: It recognizes the virus based on amino acid patterns in virus particles. The outcome of these tests is determined by who is being tested, the period between testing and reporting the results, and the patient's health and age.
Fever, headache, confusion, shortness of breath, vomiting, and internal and external bleeding are among the symptoms of Covid. Symptoms appear anywhere from an hour to a day following exposure. As the disease progresses, however, the symptoms grow more common rather than more acute, and they can stay considerably longer.
How Is SARS Different From MERS & NCoV?
-The acronym SARS stands for Severe Acute Respiratory Syndrome. SARS-CoV is a virus that causes respiratory disease. The virus that causes SARS is known as SARS-CoV (Severe Acute Respiratory Syndrome Coronavirus). It's commonly spread via close physical contacts, such as coughing or sneezing into the nose or eyes. Coughing or sneezing into a damaged or enlarged lung is how most individuals become sick. People become ill in two to nine days, with short-term recovery or no symptoms at all. Infected patients with SARS generally show no signs or symptoms. SARS can infect anyone at any time.
-Middle Eastern Respiratory Syndrome (MERS) is an acronym for Middle Eastern Respiratory Syndrome. In many aspects, it resembles SARS. For example, one out of every five people who contract MERS will also contract SARS. MERS, on the other hand, differs in a few key areas, such as whether it causes pneumonia and how serious the sickness is. Approximately 90% of persons infected with MERS show no signs or symptoms. As their lungs and other body organs swell with fluid, the remaining 10–15 percent of infected persons suffer severe pneumonia.
What Are SARS, MERS, and NCoV Symptoms?
-Fever, cough, headache, and muscle aches are all symptoms of SARS.
-Fever, cough, shortness of breath, and diarrhea are all signs of MERS.
-Fever, muscle aches, and headache are all signs of the NCoV virus.
If you're experiencing any of these symptoms, consult a doctor as soon as possible. As long as you don't have any other underlying difficulties, you should be fine.
What Is the Treatment for SARS?
SARS is a new coronavirus that causes an acute respiratory illness (the virus family that includes the common cold). Droplets are used to transfer the infection from one person to another. For better survival, a breathing tube may be required. Pneumonia and increased liver enzymes are two of the most common SARS symptoms (ALT). Toxins produced by liver enzymes harm and kill liver cells. Septicemia, or lung inflammation, emerged as soon as two weeks after infection.
In a medical setting, MERS cases are more or less a coin flip among healthcare professionals. A person has a 1 in 2,000 risks of acquiring pneumonia after 90 days of illness, or roughly 10 days after infection. According to The New York Times, 60 percent of MERS patients get pneumonia, compared to 30 percent of SARS cases.
NCoV is a coronavirus that is passed down via families and primarily affects humans. NCoV symptoms appear rapidly, similar to SARS, and gradually improve over time. NCoV is communicable inside a human or animal home, just like SARS.
Visit the Centers for Disease Control and Prevention (CDC) website or The Official website of Covid Clinic for further information.
#covid test for travel#rapid covid test#covidrapidtestnearme#covid 19 free testing#free covid 19 testing#bestCOVID19antibodytest
1 note
·
View note
Text
Getting Off Life Support
Getting Off Life Support
Monetary authorities both here and abroad feel more confident in future economic growth as we are finally getting our arms around the Delta variant. Openings can accelerate once again.
They are on the brink of slowly removing extraordinary measures such as buying $120 billion of bonds here and nearly $100 billion abroad per month. This is excellent news as it is a vote of confidence that better days are ahead, so it’s time to get off life support and return to standard monetary policies. Tapering is not tightening, and even when they begin to hike rates, it probably won’t be until 2023, and the “real” funds rates will likely remain negative, which won’t put the brakes on growth.
Monetary authorities realize that their policies cannot impact shortages and supply line issues which penalize economic growth while boosting inflation. Investors have not appropriately factored into their forecasts what the other side will look like after these problems abate. We see much higher production rates as pent-up demand is filled and inventory levels are normalized. We see higher operating margins, profits, and cash flow as extraordinary costs normalize next year, for example, transportation expense. S&P operating margins are forecasted to hit close to 14% by the end of 2023, up from 12.1% in 2019, and earnings could exceed $235/share up from $162/share in 2019.
While we remain positively inclined to equities over the next 12 to 24 months, uncertainties persist, keeping a lid on markets for now. While monetary policy is more in focus, fiscal policies here and abroad are still in the air. And we still need to vaccinate the unvaccinated! Our government is dysfunctional, and China needs to take a more proactive role over Evergrande, a problem caused by their own monetary and fiscal policies. It will take many months for shortages and supply line issues to diminish. Still, the other side looks better by the day as global liquidity continues to build; we expect a surge in capital spending supported by governments everywhere, and inflationary pressures subside.
Let’s look at the key issues facing investors.
News on the Delta outbreak continues to improve by the week. The number of new cases has declined by 12% here and abroad over the last 14 days, while deaths, which lag, continue to increase here but are still falling abroad. More than 6.03 billion doses have been administered worldwide across 184 countries at a daily rate of 31.5 million doses per day. In the U.S., 387 million doses have been given so far at an average rate of 750,942 doses per day. Infectious disease experts that vaccinating 70-85% of the population would enable a return to normalcy which should be reached globally within six months. Fortunately, Pfizer, Moderna, and J&J will have enough doses available to handle globally even booster shots next year. We learned last week that the FDA panel recommended booster shots for ages 65 and up as well as those in need and that J&J’s booster shot provides 94% protection two months after the first dose. All good news. Hopefully, drug companies come up with a combination flu/coronavirus shot within a year.
The Fed took a more hawkish view gaining control over the narrative in their meeting last week, commenting that tapering is ready to begin now, although raising rates is well down the road. The financial markets took it in stride as the Fed will continue buying hundreds of billions in debt over the foreseeable future. The “real” funds' rate will remain negative for many years, which is anything but restrictive. Fed Chairman Powell said all the criteria to begin tapering were “all but met,” implying that it would be announced and start in November and be finished by mid-2022. We still do not see a rate hike until 2023 and we question the Fed’s trajectory of hikes into 2024. While no one knows when shortages and supply issues diminish, we are confident that inflation, on the other side, will be a positive surprise as productivity gains will be solid, benefitting from the surge in technology spending and operational changes made during the pandemic. Flows from abroad arbitraging rates continue to limit the steepening in our yield curve, which supports our markets.
What can be said about our political system other than it is dysfunctional? Everyone agrees that we need a sizeable traditional infrastructure bill, so why tie it to a social agenda and a debt ceiling? Passing the debt ceiling should be a non-event, too, but here again, the Dems are holding it hostage to their huge social spending bill. Our domestic and foreign policies are in disarray, as shown by Biden’s falling poll numbers. It may be so bad that he needs a victory, so he forces his party to separate the bills and move forward asap with the traditional infrastructure bill needed to rebuild our aging base to enhance our global competitive position. That’s our bet.
The domestic economy is a tale of two cities as services are suffering due to the Delta variant. At the same time, the production end is strong, producing everything that it can limited only by shortages and supply line issues. Key data points reported last week include: index of the consumer in September rose slightly to 71.0, current economic conditions fell to 77.1, and consumer expectations increased to 67.1; August leading indicators rose 0.8% to 117.1, coincident rose 0.2% to 105.9 and lagging increased to 106.3; composite output index fell to 54.5 in September due to shortages and supply line issues, services index fell to a 14 month low at 54.4, manufacturing PMI was a still strong 60.5, and manufacturing output was 55.2; building permits rose 6% in August and housing starts increased 3,9%, but builder confidence fell to a 13 month low, and jobless claims unexpectedly increased to 351,000. It is important to note that consumers see the worst buying conditions in decades due to high prices. And finally, the U.S opened air travel to vaccinated foreigners which should boost growth. The economy is set to reaccelerate as the Delta variant ebbs. Still, shortages and supply line issues will limit growth for the foreseeable future, setting up a very strong and profitable mid-2022 onward as these problems diminish, especially if an infrastructure bill is passed.
The OECD lowered its forecast slightly for global growth in 2021 to 5.7%, keeping China’s growth unchanged at 8.5% (we are lower); Japan at 2.5%; U.S. growth down to 6.0%; India at 9.7% for FY 2022; 4.3% in the Eurozone; Southeast Asia at 3.1% and 4.0% in Australia. The recovery pattern remains uneven due to the coronavirus, shortages, and supply line issues, with increasing inflationary pressures everywhere. The outlook for 2022 growth was lifted to 4.7% as these problems abate.
Investors are focused on China. Not only has growth slowed quickly due to covid, but their largest developer, Evergrande, is on the brink of bankruptcy. It has been here before. While we expect the financial fallout to remain limited to China, it clearly will penalize near-term growth, which had already been under pressure due to the Delta variant. The People’s Bank of China has already injected around $71.0 billion into the banking system and stands ready to do more. We fully expect the PBOC to lower reserve requirements shortly and pump a lot more money into their system. Plans are also being made to step up fiscal support, as jobs are the government's number one priority. Don’t bet against China?
While global growth for 2021 was revised slightly lower due to the spread of the Delta variant, the outlook for growth in 2022 has improved, permitting monetary authorities to look at removing life support tools soon.
Investment Outlook
It is good news that monetary authorities no longer believe that extraordinary measures are needed to support their economies. Tapering does not mean that tightening is on the horizon. 2021 will go down as an extraordinary year as we have had to deal with the pandemic, shortages, supply line issues, geopolitical risks and more. Nevertheless, economies recovered substantially only to slow down over the summer due to the outbreak of the Delta variant. But that is changing as the world gets vaccinated. Better days are ahead.
Investors have not factored into their 2022 projections the positive impacts of ending shortage and supply line issues which ratcheted costs up dramatically in 2021 while also curtailing production/sales. Inventories are at all-time lows everywhere and need to be rebuilt. Infrastructure plans are on the horizon globally on top of significant increases in capital spending and research. All good for growth.
We continue to favor investing in value stocks tied to global economic growth and technology companies riding the wave of digitalization. Companies hurt by shortages and supply-side issues will be the winners next year, too, as these problems abate. Inflation will subside too. We continue to see a steepening yield curve, but it will be held down by large inflows from abroad arbitraging the yield differential.
Getting off life support is a good thing.
1 note
·
View note