#The Puget Sound Mental Hospital
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
The Tumblr app for Google Glass was released on May 16, 2013.
Text

The Puget Sound Mental Hospital
The Puget Sound Mental Hospital is a near century old psychiatric institution located in Tacoma, Washington. Even to this day, Puget Sound Mental Hospital continues to take patients, even though about half of the original institution has been closed off due to it essentially falling apart over the years. But patients of decades past – those of an otherworldly, spiritual nature that is – continue to walk the halls of the Puget Sound Mental Hospital.
Originally built in 1926, the mental hospital has quite the precarious history. Some say the very first experimental lobotomies were performed here, which would have undoubtedly had irrevocable adverse affects on the unfortunate patients that underwent such tentative trials.
Like most mental institutions operating in these times, Puget Sound Mental Hospital is haunted by the maltreated, neglected and overcrowded detainees who suffered, and many which died, within its walls. The fact that at least some of them were truly deranged to begin with doesn’t help matter as they return in the afterlife to walk the halls of the asylum.
The most famous ghost of Puget Sound Mental Hospital is that of an elderly lady who haunts the 4th floor, now closed off from the operational section of the institution. She manifests traversing the hall with her walker, and sometimes when she is not spectrally visible, her walker can still be heard scraping across the floor.
The most damaged area of the hospital, crumbling down to exposed rebar in some areas, reverberates with the reactive sense of paranormal activity. The eerie feeling of eyes watching you from just around the corner can be unnerving to say the least and have driven multiple staff members to seek new employment.
Strange noises and barely audible whispers echo throughout the stairwell. Footsteps are heard from areas in which no one is present, coming down the hall as if they are just about to turn the corner and bump into you, but as you glance into the intersecting hall, the steps halt and no one is there. This is the kind of thing staff members have reported while working in what they claim to be the irrefutably haunted Puget Sound Mental Hospital.
It’s not hard to believe that the mental institution is haunted, considering its long and shady past. Tacoma, Washington is not the only city in the Unites States to lay claim to a haunted, century old mental asylum. Places like these are a hub for negative energy, gathered and compounded by the restless souls of disturbed and forsaken patients.
The Puget Sound Mental Hospital is still a partially active institution, mostly handling drug rehabilitation treatment and geriatric psychiatry on an inpatient and outpatient basis, but also more practical services like emergency, surgery, lab work and other general needs.
For seekers of spiritual phenomenon, that means that Puget Sound Mental Hospital is all but off limits to paranormal investigators without receiving proper admittance from the institution, which is rather hard to obtain since common devices used to investigate a haunting are forbidden within the hospital’s walls.
#The Puget Sound Mental Hospital#ghost and hauntings#paranormal#ghost and spirits#haunted locations#ghost photo#haunted salem#myhauntedsalem#haunted hospitals
11 notes
·
View notes
Text
By: Tamara Pietzke
Published: Feb 5, 2024
For six years I worked at a hospital that said all teenagers with gender dysphoria must be affirmed. I quit my job to blow the whistle.
I know from firsthand experience what hard times are. Though I had a happy childhood, raised as the middle child by working-class parents in Washington State, my mom died of ovarian cancer when I was 22.
After that, my family fell apart. I felt lost and alone.
I decided to become a therapist because I didn’t want anyone to go through what I had, feeling like no one on this planet cares about them. At least they can say their therapist does.
I earned my master’s in social work from the University of Washington in 2012, and I have worked as a therapist for over a decade in the Puget Sound area. Most recently, I was employed by MultiCare, one of the largest hospital systems in the state.
For the six years I was there, I worked with hundreds of clients. But in mid-January, I left my job because of what I will go on to describe.
The therapeutic relationship is a special one. We are the original “safe space,” where people are able to explore their darker feelings and painful experiences. The job of the therapist is to guide a patient to self-understanding and sound mental health. This is a process that requires careful assessment and time, not snap judgments and confirmation of a patient’s worldview.
But in the past year I noticed a concerning new trend in my field. I was getting the message from my supervisors that when a young person I was seeing expressed discomfort with their gender—the diagnostic term is gender dysphoria—I should throw out all my training. No matter the patient’s history or other mental health conditions that could be complicating the situation, I was simply to affirm that the patient was transgender, and even approve the start of a medical transition.
I believe this rise of “affirmative care” for young people with gender dysphoria challenges the very fundamentals of what therapy is supposed to provide.
I am a 36-year-old single mother of three young kids all under the age of six. I am terrified of speaking out, but that fear pales in comparison to my strong belief that we can no longer medicalize youth and cause them potentially irreversible harm. The three patients I describe below explain why I am taking the risk of coming forward.
* * *
Last spring, I started seeing a new client, who at 13 years old had one of the most extreme and heartbreaking life stories I’ve ever heard. (For the sake of clarity, I am referring to all patients by their biological sex.)
My patient’s mother has bipolar disorder and was so abusive to my patient that the mother was given a restraining order. My patient was sexually assaulted by an older cousin, by one of her mother’s boyfriends, and also once at school by a classmate. Her diagnoses include depression, PTSD, anxiety, intermittent explosive disorder, and autism. She is being raised by her mother’s ex-boyfriend (not the one who assaulted her).
The year before I started seeing her, when she was 11, she was hospitalized for talking about committing suicide. Later that year, a pediatrician diagnosed her with gender dysphoria after she started to question her gender. The pediatrician referred her to Mary Bridge Children’s Gender Health Clinic, whose clinicians recommended she take medicine to suppress her periods and that she think about starting testosterone.
Mary Bridge, MultiCare’s pediatric hospital, runs the gender clinic for minors and employs nurses, social workers, dietitians, and endocrinologists, who provide gender-affirming care, which includes prescribing hormones to young patients who question their gender. In order to get that prescription, patients first need a recommendation letter from a therapist. Because Mary Bridge is a part of MultiCare, their patients were often referred to therapists like me who were in their system.
In an April 2022 blog post, a Mary Bridge social worker wrote that the gender clinic’s referrals increased from less than five a month in 2019 to more than 35 a month in 2022. In May 2022, the clinic received a $100,000 donation from Patient-Centered Outcomes Research Institute “to study health care disparities” in transgender youth.
The clinic operates in Washington, one of the states with some of the most lenient legislation on gender transition for youth. In May 2023, the state legislature passed a law guaranteeing that youth seeking a medical gender transition can stay at Washington shelters—and the shelters are not required to notify their parents.
Because of my patient’s autism, it was difficult for us to engage in introspective conversations. During our first visit, she came over to my desk to show me extremely sadistic and graphic pornographic videos on her phone. She stood next to me, hunched over, hyper-fixated on the videos as she rocked back and forth. She told me during one session that she watched horror and porn movies growing up because they were the only ones available in her house.
She showed up to our therapy sessions in disheveled, loose-fitting clothes, her hair greasy, her eyes staring down at the ground, her face covered by a Covid mask almost like a protective layer. She went by a boy’s name, but she never raised gender dysphoria with me directly—though one time she told me she would get mad at the sound of her own voice because “it sounds too girly.” When I asked her how she felt about an upcoming appointment at the gender clinic, she told me she didn’t know she had one.
In between scrolling through videos on her phone, she told me how she cried every night in bed and felt “insane.” She described a time when she was eight years old and her mother nearly killed her sister. She remembered her mother being taken away. At times, she would “age-regress,” she told me, by watching Teletubbies and sucking on pacifiers.
When she started seeing me, she had recently threatened to “blow up the school,” which resulted in her expulsion.
I knew I couldn’t solve all of her problems, or make her feel better in just a few therapy sessions. My initial goal was to make her feel comfortable opening up to me, to make the therapy room a place where she was heard and felt safe. I also wanted to try to protect her from falling prey to outside influences from social media, her peers, or even the adults in her life.
With a patient like this, with so many intersecting and overwhelming problems, and with such a tragic history of abuse, it took our first three sessions to get her feeling more comfortable to even talk to me, and to understand the dimensions of her problems. But when I called her guardian last fall to schedule a fourth appointment, he asked me to write her a letter of recommendation for cross-sex hormone treatment. That is, at age 13, she was to start taking testosterone. Such a letter from me begins the process of medical transition for a patient.
In Washington State, that’s all it takes—a few visits with a therapist and a letter, often written using a template provided by one’s superiors—for minors to undergo the irreversible treatments that patients must take for a lifetime.
I was scared for this patient. She had so many overlapping problems that needed addressing it seemed like malpractice to abruptly begin her on a medical gender transition that could quickly produce permanent changes.
The MultiCare recommendation letter Tamara was given for approving the medical treatment of minors with gender dysphoria. I emailed a program manager in my department at MultiCare and outlined my concerns. She wrote back that my client’s trauma history has no bearing on whether or not she should receive hormone treatment.
“There is not valid, evidenced-based, peer-reviewed research that would indicate that gender dysphoria arises from anything other than gender (including trauma, autism, other mental health conditions, etc.),” she wrote.
She also warned that “there is the potential in causing harm to a client’s mental health when restricting access to gender-affirming care” and suggested I “examine [my] personal beliefs and biases about trans kids.”
When Tamara outlined her concerns about giving a patient testosterone to her manager at MultiCare, she was told to “examine your personal beliefs and biases about trans kids.” She then reported me to MultiCare’s risk management team, who removed my client from my care and placed her with a new therapist.
A risk manager’s job is to minimize the hospital’s liability, but in my case, they deemed that my concerns posed a greater risk to my client than giving her a life-altering procedure with no proven long-term benefit.
I shouldn’t have been surprised by this. Just a few months earlier, in September of last year, I was one of over 100 therapists and behavioral specialists at the MultiCare hospital system required to attend mandatory training on “gender-affirming care.”
As hard as it is to believe given my work, I hadn’t heard about gender-affirming care before that moment. I needed to know more. So each night in the week leading up to the training, I searched online for information about gender-affirming care. After putting my kids to bed, I sat glued to my computer screen, losing sleep, horrified at what I found.
I discovered that neither puberty blockers nor cross-sex hormones (testosterone or estrogen) were approved by the Food and Drug Administration as a treatment for gender dysphoria. In fact, prescribing these treatments to kids can have drastic side effects, including infertility, loss of sexual function, increased risk of heart attack, stroke, cardiovascular disease, cancer, bone density problems, blood clots, liver toxicity, cataracts, brain swelling, and even death.
While gender clinicians claim hormonal treatment improved their patients’ psychological health, the studies on this are few and highly disputed.
I found that those experiencing gender dysphoria are up to six times more likely to also be autistic, and they are also more likely to suffer from schizophrenia, trauma, and abuse.
The research also implies that the dramatic rise in these diagnoses across the West likely have a strong element of social contagion. In children ages 6 to 17, there was a 70 percent increase in diagnoses of gender dysphoria in the U.S. from 2020 to 2021. In Sweden there was a 1,500 percent increase in these diagnoses among girls 13–17 from 2008 to 2018.
Yet, countries that were once the pioneers of gender transition medicine are now starting to backtrack. In 2022, England announced it will close its only gender clinic after an investigation uncovered subpar medical care, including findings that some patients were rushed toward gender transitions. Sweden and Finland undertook comprehensive analyses of the state of gender medicine and recommended restrictions on transition of minors.
I decided—though it was potentially dangerous to my career and to me—to ask questions about the findings I discovered.
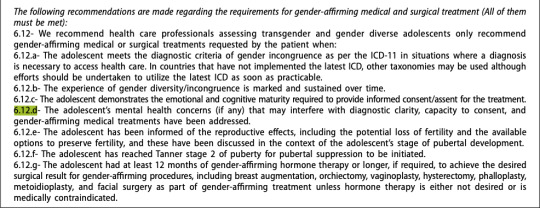
The training I attended laid out an affirming model of gender care—from pronouns and “social transition” to hormone treatments and surgical intervention. In order for children to be diagnosed with gender dysphoria, the training stated, patients must meet six of eight characteristics, ranging from “a strong desire/insistence of being another gender” to “strong preference for cross-gender toys and games.”
Tamara and her MultiCare colleagues were trained to diagnose gender dysphoria among their young patients when they met six of the eight above characteristics. It was made abundantly clear to all in attendance that these recommendations were “best practice” at MultiCare, and that the hospital would not tolerate anything less.
When the leader of the training brought up hormone treatments, I shakily tapped the unmute button on Zoom and asked why 70 to 80 percent of female adolescents diagnosed with gender dysphoria have prior mental health diagnoses.
She flashed a look of disgust as she warned me against spreading “misinformation on trans kids.” Soon the chat box started blowing up with comments directed at me. One colleague stated it was not “appropriate to bring politics into this” and another wrote that I was “demonstrating a hostility toward trans folks which is [a] direct violation of the Hippocratic Oath,” and recommended I “seek additional support and information so as not to harm trans clients.”
In the training, gender-affirming treatment is presented as “suicide prevention.” As soon as I closed my laptop, I burst into tears. I care so deeply about my clients that even thinking about this now makes me cry. I couldn’t understand how my colleagues, who are supposed to be my teammates, could be so quick to villainize me. I also wondered if maybe my colleagues were right, and if I had gone insane.
Later, my boss reached out to me and told me it was “inappropriate” of me to raise these questions, telling me that a training session was not the proper forum. When I tried to present the evidence that caused me concern—the lack of long-term studies, the devastating side effects—she told me she didn’t have time to read it.
��I am speaking out because nothing will change unless people like me blow the whistle,” Tamara writes. “I am desperate to help my patients.” In retrospect, this ideology had been growing in power for a long time.
I remember in 2019 seeing signs of how gender dysphoria arose among many of my most vulnerable female clients, all of whom struggled with previous psychological problems.
In 2019, I started seeing a 16-year-old client after her pediatrician referred her to me for anxiety, depression, and ADHD. When I first met her, she had long blonde hair covering her eyes, to the point you could barely see her face. It was like she was going through the world trying to be invisible.
In 2020, during the pandemic, she told me she had started reading online a lot about gender, and said she started feeling like she wasn’t a girl anymore.
Around this time, her anxiety became so debilitating she couldn’t leave her house—not even to go to school. After taking a year off school during the pandemic, she enrolled in an alternative school for kids struggling with mental health. I was relieved that she was making friends for the first time, and seemed to be feeling a lot better.
Then she started using they/he pronouns, identified as pansexual, and replaced the skirts and fishnet stockings she often wore with disheveled and baggy clothes. Her long hair became shorter and shorter. She started wearing a binder to flatten her breasts. She tried out a few different names before settling on one that’s gender neutral.
The official diagnosis I gave her was “adjustment disorder”—an umbrella term often applied to young people who are having a hard time coping with difficult and stressful circumstances. It’s the type of diagnosis that doesn’t follow a child forever—it implies that mental distress among kids is often transient.
She came out as transgender to her family in 2021. Her mother was supportive, but her dad wasn’t. Regardless, she went to her pediatrician seeking a referral to a gender clinic.
In 2022, she went to Mary Bridge Children’s Gender Health Clinic for the first time, where the clinicians informed her and her parents that if she didn’t receive hormone replacement therapy, she could be “at increased risk for anxiety, depression, and worsening of mental health/psychological trauma,” according to her patient records. Her dad refused to start his daughter on testosterone, and so all the clinic could do was prescribe birth control to stop her period due to her “menstrual dysphoria,” or distress over getting her period. Which is something I thought all teenage girls experienced.
Five months later, she swallowed a bottle of pills and her mother had to rush her to the emergency room.
By early 2023, my client logged on to our weekly session, which we started doing by Zoom, and she told me she identified as a “wounded male dog.” She explained to me that this was her “xenogender,” a concept she had discovered online, which references gender identities that go “beyond the human understanding of gender.” She said she felt she didn’t have all of the right appendages, and that she wanted to start wearing ears and a tail to truly feel like herself.
I was stunned. All I could do was silently nod along.
After the session, I emailed my colleagues looking for advice. “I want to be accepting and inclusive and all of that,” I wrote, but “I guess I just don’t understand at what point, if ever, a person’s gender identity is indicative of a bigger issue.”
I asked them: “Is there ever a time where acceptance of a person’s identity isn’t freely given?”
The consensus from my colleagues was that it wasn’t a big deal.
“It sounds like this isn’t something that’s ‘broken,’ ” one colleague wrote me back, “so let’s not try to ‘fix’ it.”
“If someone told me they use a litterbox instead of a toilet and they were happy with it and it’s part of their life that brings them fulfillment, then great!” she continued. “I might think it’s weird, but then again, not my life.”
After learning that one of Tamara’s patients identified as “a wounded male dog,” a colleague replied: “If someone told me they use a litterbox instead of a toilet and they were happy with it and it’s part of their life that brings them fulfillment, then great!” I was baffled and alarmed by her unquestioning affirmation. At what point does a change in identity represent a mental health concern, and not something to be celebrated and affirmed? Fortunately, my client never brought up her “xenogender” again. She also isn’t on testosterone due to her father’s disapproval. So I kept these thoughts to myself, and ultimately, in order to keep my job, I let it go.
Another female patient, who transitioned as a teen, serves as a warning of what happens when we passively accept the idea that gender transition will entirely resolve a patient’s mental health issues.
This client, who I started seeing in 2022, is now 23 and rarely leaves the house, spends most of the day in bed playing video games, and envisions no path to working or functioning in the outside world due to a variety of mental health problems. In 2016, this patient was diagnosed with autism, anxiety, and gender dysphoria. Later the diagnoses grew to include depression, Tourette syndrome, and a conversion disorder. In 2018, at age 17, the Mary Bridge Gender Health Clinic prescribed testosterone, despite the fact that this patient is diabetic and one of the hormone’s side effects is that it might increase insulin resistance. The patient’s mother, who has another transgender child, strongly encouraged it.
This patient now has a wispy mustache and a deepened voice, but does not pass as male. It turns out that testosterone, which will be prescribed for life, did not relieve the patient’s other mental illnesses.
My biggest fear about the gender-affirming practices my industry has blindly adopted is that they are causing irreversible damage to our clients. Especially as they are vulnerable people who come to us at their lowest moments in life, and who entrust us with their health and safety. And yet, instead of treating them as we would patients with any other mental health condition, we have been instructed—and even bullied—to abandon our professional judgment and training in favor of unquestioning affirmation.
I am speaking out because nothing will change unless people like me—who know the risks of medicalizing troubled young people—blow the whistle. I am desperate to help my patients.
And I believe, if I don’t speak out, I will have betrayed them.
--

https://www.tandfonline.com/doi/pdf/10.1080/26895269.2022.2100644
--

Amidst the scandal, Mary Bridge Children's has deleted the above blog post by self-professed "they/them," Aytch Denaro. However, the internet doesn't forget.
#Tamara Pietzke#Jamie Reed#whistleblower#medical malpractice#medical transition#medical corruption#gender dysphoria#gender ideology#queer theory#gender affirming care#gender affirming healthcare#gender affirmation#mental health#mental health issues#mental illness#gender cult#genderwang#religion is a mental illness
37 notes
·
View notes
Text
How I lost a month of work and health
This is not easy for me, but this is the situation. Buckle up, this is wild.
Our ex-roommate is a hoarder and has all of the mental health issues you may imagine. Among them is executive function disorder, the inability to make important decisions and procrastinate until it is almost/too late to do anything.
After 4+ years of threatening to move when we tried to get them to agree to a cleaning program so we could, you know, live in a healthy house, they found a new place to live. Cue worst moving company ever, that are so terrible they would make you feel sorry for the FAWLTY TOWERS cast if they contracted out to these misogynistic, lazy and ham-fisted movers and I won't name them because their employees have a disturbing history of holding your goods for ransom (extra fees out of nowhere) and actually threatening you if you hold your ground. Let's say the company name starts with S and rhymes with 'makeway' and leave it at that, ok?
Well, roommate had 2 cats rescued from the great outdoors and when they were kittens they were shy and skittish but they were somewhat socialized and gentle. But after about 4 years of living in a hoarder's classic labyrinth and losing every imaginable social interaction with humans, they went feral.
I tried to stop them from escaping the bedroom because the movers were leaving the doors open (another thing they ignored while they were busy breaking stuff).

Three of us wound up in Urgent Care that night; me, my kid and the roommate because these poor creatures thought they were fighting for their lives. I hold them no grudge.
Doc says if things don't improve in 2-3 days go straight to ER.
Well. My hand balloons up in short order and I can't bend my thumb at all. I dutifully pay for a Lyft (roommate is gone even if their things are still here) and this happens:

Diagnosis? Septic Arthritis.
This is a rare and scary condition. Cat bit through muscle, tendon sheath, tendon, and even impacted the BONE right at the thumb joint which is a spot almost impossible to reach with oral antibiotics. There's just not enough circulation for the drugs to do their work. So. To save my hand the plastic surgeon on call opens me up AND STRIPS THE SHEATH. I don't know how many stitches I even have.
They have me on a lot of antibiotics plus opiods for the pain and a shunt and tubes and all the good stuff.
Then they put me on vincomiacin, which is a common allergen. I woke up trying to take off my hair in the middle of the night. Like a hive of stinging wasps were under my skin. Cue IV benadryl for 2 nights.
I wound up paying $60 to get my hair cut short as a breath in vacuum when I was back on my feet because my scalp still hurts and is sore from the reaction.
I wasn't even the only person hospitalized in the largest hospital in South Puget Sound over a cat-inflicted wound. I was the 3rd. If you count the first night, I was the 5th. The winner was a woman who kept 4 unspayed cats in her house and thought she could wade in and break up a cat fight.
Priceless was the moment when the salty old nurse in ER muttered that at least I hadn't been bitten by humans, and it turned out she has Seen Things from the ambulance behind the mall on certain nights.
Ultimately, because I can't use the thumb without incredible pain and the mobility is toast, I'm off work until the 10th of November. I used up all of my employee sick leave and will have to muddle back to work and talk to HR about other options on getting some sort of emergency compensation to survive. Friends and family have been wonderful. They've helped with rent and offered rides, helped us get groceries, and all the things you need to make it through.
But I've lost my independence and it hurts, bone-deep. It's deeper than the injury.

We are facing a deep clean of the apartment because we love living here and we love the landlady and maybe if we'd been a harder a** about the hoarding this wouldn't have happened. Who knows. But lyft rides have cost us $200 and there will probably be more to come as I muddle through rehab and appointments and exams. I'm annoyed about the hair cut. I'm not feeling great about the ballooning weight and I am baffled that there is still a ton of stuff that isn't ours, waiting to be hauled out and the rental agency wants me to pay an extra $500 to re-word the lease (re: start over) because rental controls are on the ballot and they would make it hard for these jokers to sock me with admin fees if the new controls are met and I'm betting this is why they are trying to get the money NOW. In the meantime, the carpet needs to go because my kid has asthma and cat pee carpets aren't healthy for anyone. Not a word about the cleanup has been made from the person who caused this mess. I don't expect it, either. They are mentally ill and not capable of drawing the dots when it comes to things like this. Nor do they have the money. Hard lessons learned.
I'm not posting any of this to beg for money. Frankly, nobody I know has it to spare. As I sit at home I'll slowly work my way through my ko-fi page and try to sell more fiction, and art if my confidence levels go up.
But this is health care in America and I am considered one of the lucky ones because my co-pay stopped at $75 for the emergency X-rays and my pharmacy (Rite-Aid) is finding new and improved ways to keep us from getting our RX in a timely fashion, ran out of bandages, and my GP is tearing her hair out because she faxes meds to me and they simply don't read the faxes that come in.
There is no transportation assistance on my insurance--and I repeat, I am considered one of the lucky ones with a state job + benefits.
I'm applying for emergency assistance to see if there is anything out there because pride goes first.
My sister likes to say, "Life's a lesson, sometimes you're it." This is my lesson. Don't vote down health care. Vote up.
6 notes
·
View notes
Text
Ted Bundy
Ted Bundy, born Theodore Robert Cowell on November 24, 1946, was one of the most notorious American serial killers. He is known to have kidnapped, raped and killed at least 36 young women in 1970s and probably earlier. He was executed in the electric chair in 1989. His murders have inspired many novels and films about serial killers.

Photo of Ted Bundy
His mother was Eleanor Louise Cowell, who was 22 years old and unmarried when she gave birth to Bundy. His biological father's identity may never be confirmed, since on his birth certificate the father was listed as unknown; also, some rumours identify his father as his grandfather. For the first three years of his life, Bundy lived with his maternal grandparents and was told that his mother was his sister. He eventually discovered the truth and expressed a lifelong resentment toward his mother for never talking to him about his true parentage. In 1951 Louise met and married Johnny Culpepper Bundy, a hospital cook, and later that year the couple officially adopted Bundy, that took his name. He had a tense relationship with his stepfather, and complained to his girlfriend that Johnny "wasn't very bright” and "didn't make much money".
Ted Bundy’s parents, Eleanor Louise Cowell and Johnny Culpepper Bundy
After graduating from high school in 1965, Bundy attended the University of Puget Sound for one year before transferring to the University of Washington. There, he fell in love with Stephanie Brooks, a wealthy and lovely young woman from California. He was devastated by their breakup, and many of his following victims resembled his college girlfriend. He graduated from the University of Washington with a degree in psychology in 1972.
Attacks and murders
There is no consensus on when or where Bundy began killing women. He told different stories to different people and refused to reveal the specifics of his first crimes. For example, he told his mother that he attempted his first kidnapping in 1969 in Ocean City, New Jersey, but did not kill anyone until 1971 in Seattle, yet told psychologist Art Norman that he had killed two women in Atlantic City in 1969.
Homicide detective Robert D. Keppel and biographer Ann Rule, who had previously worked with Bundy, both believed that he might have started killing as a teenager. Circumstantial evidence suggested that he may have kidnapped and killed eight-year-old Ann Marie Burr when he was 14 years old, but he repeatedly denied. His earliest documented homicides were committed in 1974, at the age of 27. The disappearances all took place at night, usually near ongoing construction work, and the victims were all young, attractive, and with long hair parted in the middle; at most crime scenes there were sightings of a man wearing a cast or a sling, and driving a brown or tan Volkswagen Beetle.


Photos of Ted Bundy's 1968 Volkswagen Beetle, in which he committed many of his crimes. The vehicle is on display at the National Museum of Crime and Punishment.

Items found in his car when he was arrested in 1975
His first confirmed attack occurred shortly after midnight on January 4, 1974, when Bundy entered the apartment of Joni Lenz. After bludgeoning her with a metal rod from her bed frame, he sexually assaulted her with either the same rod or a metal speculum. She survived, but with permanent physical and mental disabilities. In the early morning of February 1, 1974, Bundy broke into the room of Lynda Ann Healy; he beat her unconscious, dressed her in blue jeans, a white blouse, and boots, and carried her away. On March 12, Donna Gail Manson, left her dormitory to attend a jazz concert on campus, but never arrived. On April 17, Susan Elaine Rancourt disappeared while on her way to her dorm room after an advisors' meeting at Central Washington State College in Ellensburg. On May 6, Roberta Kathleen Parks left her dormitory to have coffee with her friends at the Memorial Union, but never arrived. On June 1, Brenda Carol Ball disappeared after leaving the Flame Tavern in Burien, near Seattle; she was last seen in the parking lot, talking to a brown-haired man. On June 11, UW student Georgann Hawkins disappeared while walking to her sorority house.
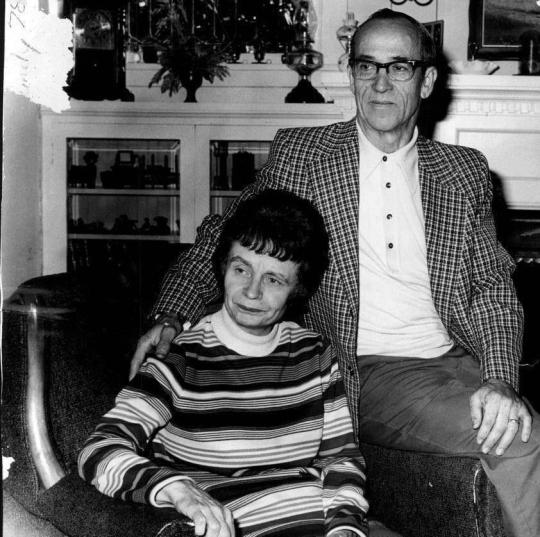
The murders culminated on July 14, 1974, when Bundy abducted two women, Denise Marie Naslund and Janice Anne Ott, in the daylight and from crowded areas. Five female witnesses said that a good-looking young man, who introduced himself as "Ted", asked their help to unload a sailboat from his car. Four girls refused, but one agreed and accompanied him to his car. She saw there was no sailboat and fled. Using the same story, he approached and abducted Janice Anne Ott and, approximately four hours later, Denise Marie Naslund. On September 6, 1974, two grouse hunters found the skeletal remains of the two girls near a service road in Issaquah. After these happenings, King County police disclosed a composite sketch, that was printed in regional newspapers and transmitted on local television stations. These are not the only murders that he committed, as it is believed that he has killed more than a hundred women.
Newspaper from 1974 warning young women about “Ted”, aka Ted Bundy
Timeline of Bundy’s attacks
In 1974
Joni Lenz, age 18, survived the attack on January 4, 1974
Lynda Ann Healy, age 21, died on February 1, 1974
Donna Gail Manson, age 19, died on March 12, 1974
Susan Elaine Rancourt, age 18, died on April 17, 1974
Roberta Kathleen Parks, age 20, died on April 17, 1974
Brenda Carol Ball, age 22, died on June 1, 1974
Georgeann Hawkins, age 18, missing since June 11, 1974
Denise Marie Naslund, age 18, died on July 14, 1974
Janice Anne Ott, age 23, died on July 14, 1974
Nancy Wilcox, age 16, missing since October 2, 1974
Melissa Anne Smith, age 17, died on October 26, 1974
Laura Ann Aime, age 17, missing since October 31, 1974
Carol DaRonch, age 18, survived the attack on November 8, 1974
Debra Jean Kent, age 17, died on November 8, 1974
In 1975
Caryn Eileen Campbell, age 23, died on January 12, 1975
Julie Cunningham, age 26, died on March 15, 1975
Denise Lynn Oliverson, age 24, missing since April 6, 1975
Melanie Suzanne Cooley, age 18, died on April 15, 1975
Lynette Dawn Culver, age 12, missing since May 6, 1975
Susan Curtis, age 15, missing since June 27, 1975
In 1978
Margaret Elizabeth Bowman, age 21, died on January 15, 1978
Lisa Levy, age 20, died on January 15, 1978
Kathy Kleiner, age 20, attacked on January 15, 1978
Karen Chandler, age 22, attacked on January 15, 1978
Cheryl Thomas, age 21, attacked on January 15, 1978
Kimberly Dianne Leach, age 12, died on February 9, 1978
Arrests, last murders and death
On August 16, 1975, Utah Highway Patrol officer Bob Hayward arrested Bundy in Granger (a Salt Lake City suburb). The officer searched the car after he noticed that the front passenger seat had been removed and placed on the back seats. Inside he found a ski mask, a second mask created from pantyhose, a crowbar, handcuffs, trash bags, a rope, an ice pick, and other items. The police did not have enough evidence to detain Bundy, so he was released. Afterwards, Salt Lake City police placed him on 24-hour surveillance.

Ted Bundy's 1975 Utah mug shot
In September Bundy sold his Volkswagen Beetle to a Midvale teenager and Utah police impounded it. Inside the car, FBI technicians found hairs of Caryn Campbell, and some hair strands "microscopically indistinguishable" from those of Melissa Smith and Carol DaRonch. There was sufficient evidence to charge him with aggravated kidnapping and attempted criminal assault in the DaRonch case. Further investigation confirmed that he had not been with his girlfriend on any of the nights when the Pacific Northwest victims had vanished. In February 1976 Bundy stood trial for the DaRonch kidnapping, and after a four-day bench trial and a weekend of deliberation, he was found guilty. In June he was sentenced to 15 years in the Utah State Prison, and after a period of resistance he was transferred to Aspen in January 1977.
While in the Pitkin County Courthouse's library, in Aspen, he opened a window and jumped out, managing to run away. He was a fugitive for six days, until two police officers found him and brought him back in jail. He planned his escape a second time; he sawed a hole of about one square foot between the steel reinforcing bars in his cell's ceiling and, on the night of December 30, stacked books on his bed to simulate his body, climbed into the crawl space and escaped.
After evading, he travelled from Aspen to Tallahassee, Florida, passing from Chicago, Ann Arbor and Atlanta. There, on January 15, he attacked another five women, Margaret Bowman and Lisa Levy who died, Kathy Kleiner, Karen Chandler and Cheryl Thomas who survived. On February 8 he attacked another woman, Kimberly Dianne Leach; her partially mummified remains were found in a pig farrowing shed near Suwannee River State Park, near Lake City. He was arrested four days later by police officer David Lee for having stolen a car.

Two of Ted Bundy’s victims
After numerous trials and three death sentences, Bundy was executed at 7:16 a.m. on January 24, 1989, at the Florida State Prison in an electric chair. Outside the prison, hundres of people cheered, sang, danced and even set off fireworks. His body was cremated in Gainesville, and no public ceremony was held.
Sources:
Ted Bundy | Crimes, Death & Facts | - Britannica
Ted Bundy - Biography
Ted Bundy’s Victims - Women’sHealth
Ted Bundy - Wikipedia
65 notes
·
View notes
Link

For Trans Day of Visibility, the Olympia admin for the Pacific Northwest Garden Buddies had an information thread on Twitter that showcased area trans resources.
Our Olympia admin is nonbinary and runs a garden club that serves over 3,000 people in Thurston County.

This will be our Admin’s 3rd year on GRuB’s Garden Support Team. GRuB provides free gardens to low income people in Thurston County. GRuB is a trans friendly non profit.
For Trans Day of Visibility 2019 our admin made a Resource Thread on Twitter for trans folks in Thurston County/Puget Sound.
RESOURCE LIST
GRuB: The seed for GRuB was planted in 1993 as the Kitchen Garden Project (KGP). Inspired by the work of Vietnam veteran Dan Barker (founder of the Home Gardening Project), South Sounders Richard & Maria Doss began building free vegetable gardens for low-income people in southwestern Washington. The KGP’s mission was to empower low-income people by giving them more control over their own food security and decreasing their reliance on emergency food programs.A few years later, In 1996, an elder in our community named Bonnie Turner offered her back yard as the site for an intergenerational community gardening project. This gave our founders an opportunity to establish and anchor a garden program for youth and seniors. In 2001, these program merged to become Garden-Raised Bounty (GRuB).
The Evergreen State College’s Bike Shop has Lady and Trans nights every Tuesday.
“ Every Tuesday from 4-7p.m. The Evergreen Bike Shop closes it's doors to cisgender males creating safe space for Ladies and Trans identifying people. “
YWCA of Olympia: “Since 1998, Girls Without Limits! (GWOL!) has served middle school youth by providing gender-responsive, culturally-relevant programming that promotes confidence, skill building, career awareness, and curiosity in science, technology, engineering, art, and math (STEAM). Girls and gender nonconforming youth engage in hands-on learning activities, meet professionals who work in STEAM fields, and participate in project-related field trips.”
Stonewall Youth: Stonewall Youth is an organization of youth, activists, and allies that empowers lesbian, gay, bisexual, trans, queer, questioning, intersex, and asexual (LGBTQQIA) youth to speak for themselves, educate their communities, and support each other.
Pizza Klatch: Trigger warning: Suicide
In response to a rash of suicides among LGBTQ+ youth in Thurston County, WA in 2007, a group of concerned private therapists, community leaders, and mental health professionals teamed up with the North Thurston School District to create an after-school support group for high school students who identify as LGBTQ+. Many of these youth had no other access to LGBTQ+ information or support, lived at home with unaccepting families, or were not able to come out to their parents or classmates for fear of negative outcomes. The after-school support group provided a refuge for youth in need, but was discontinued in fall of 2007 after students were discovered by disapproving parents and suffered punishment.The support group quickly moved to lunchtime, and pizza was served at the first "Pizza Klatch" in February of 2008. Now youth had a safe and confidential place to meet during school hours to gain support and community.
SAGE OLYMPIA: SAGE Olympia is a Net affiliate of SAGE (Services and Advocacy for LGBTQ Elders) USA, the premier LGBTQ elder care organization based in New York.SAGE Olympia is registered with the State of Washington as a Non-Profit Corporation. The SAGE Olympia Mission is to promote the wellness of LGBTQ elders in the Thurston County area, with a range of services and activities. See the LGBTQ+ Friendly Elder Housing List HERE
Gender Alliance of South Sound
Seattle Children’s Hospital Gender Clinic: Why choose Seattle Children’s Gender Clinic?
Seattle Children's is the only multidisciplinary clinic in our region for youth who are transgender or gender nonconforming. Only 5 children’s hospitals in the United States have clinics dedicated to caring for young people with gender identity concerns. Our doctors have special training in adolescent medicine, hormones (endocrinology) and emotional health. This team approach is called multidisciplinary care. Social workers, nurses and medical assistants are also part of the team. We are working to create best practices for children, adolescents and young adults who are transgender and gender nonconforming. Dr. Cora Breuner co-authored the first policy statement by the American Academy of Pediatrics on the subject. We base our treatments on the most current research. We tailor treatment to you and your family. We take into account your age, stage of puberty, desired future treatments, your support systems and any health problems you may have. Our specialists work together to coordinate care – all in one place when possible.
19 notes
·
View notes
Text
The Homeless Crisis Is Getting Worse in America’s Richest Cities
Bloomberg, November 20, 2018
It was just after 10 p.m. on an overcast September night in Los Angeles, and L. was tired from a long day of class prep, teaching, and grading papers. So the 57-year-old anthropology professor fed her Chihuahua-dachshund mix a freeze-dried chicken strip, swapped her cigarette trousers for stretchy black yoga pants, and began to unfold a set of white sheets and a beige cotton blanket to make up her bed.
But first she had to recline the passenger seat of her 2015 Nissan Leaf as far as it would go--that being her bed in the parking lot she’d called home for almost three months. The Late Show with Stephen Colbert was playing on her iPad as she drifted off for another night. “Like sleeping on an airplane--but not in first class,” she said. That was in part by design. “I don’t want to get more comfortable. I want to get out of here.”
L., who asked to go by her middle initial for fear of losing her job, couldn’t afford her apartment earlier this year after failing to cobble together enough teaching assignments at two community colleges. By July she’d exhausted her savings and turned to a local nonprofit called Safe Parking L.A., which outfits a handful of lots around the city with security guards, port-a-potties, Wi-Fi, and solar-powered electrical chargers. Sleeping in her car would allow her to save for a deposit on an apartment. On that night in late September, under basketball hoops owned by an Episcopal church in Koreatown, she was one of 16 people in 12 vehicles. Ten of them were female, two were children, and half were employed.
The headline of the press release announcing the results of the county’s latest homeless census strikes a note of progress: “2018 Homeless Count Shows First Decrease in Four Years.” In some ways that’s true. The figure for people experiencing homelessness dropped 4 percent, a record number got placed in housing, and chronic and veteran homelessness fell by double digits. But troubling figures lurk. The homeless population is still high, at 52,765--up 47 percent from 2012. Those who’d become homeless for the first time jumped 16 percent from last year, to 9,322 people, and the county provided shelter for roughly 5,000 fewer people than in 2011.
All this in a year when the economy in L.A., as in the rest of California and the U.S., is booming. That’s part of the problem. Federal statistics show homelessness overall has been trending down over the past decade as the U.S. climbed back from the Great Recession, the stock market reached all-time highs, and unemployment sank to a generational low. Yet in many cities, homelessness has spiked.
It’s most stark and visible out West, where shortages of shelter beds force people to sleep in their vehicles or on the street. In Seattle, the number of “unsheltered” homeless counted on a single night in January jumped 15 percent this year from 2017--a period when the value of Amazon.com Inc., one of the city’s dominant employers, rose 68 percent, to $675 billion. In California, home to Apple, Facebook, and Google, some 134,000 people were homeless during the annual census for the Department of Housing and Urban Development in January last year, a 14 percent jump from 2016. About two-thirds of them were unsheltered, the highest rate in the nation.
At least 10 cities on the West Coast have declared states of emergency in recent years. San Diego and Tacoma, Wash., recently responded by erecting tents fit for disaster relief areas to provide shelter for their homeless. Seattle and Sacramento may be next.
The reason the situation has gotten worse is simple enough to understand, even if it defies easy solution: A toxic combo of slow wage growth and skyrocketing rents has put housing out of reach for a greater number of people. According to Freddie Mac, the government-sponsored housing giant, the portion of rental units affordable to low earners plummeted 62 percent from 2010 to 2016.
Rising housing costs don’t predestine people to homelessness. But without the right interventions, the connection can become malignant. Research by Zillow Group Inc. last year found that a 5 percent increase in rents in L.A. translates into about 2,000 more homeless people, among the highest correlations in the U.S. The median rent for a one-bedroom in the city was $2,371 in September, up 43 percent from 2010. Similarly, consultant McKinsey & Co. recently concluded that the runup in housing costs was 96 percent correlated with Seattle’s soaring homeless population. Even skeptics have come around to accepting the relationship. “I argued for a long time that the homelessness issue wasn’t due to rents,” says Joel Singer, chief executive officer of the California Association of Realtors. “I can’t argue that anymore.”
Homelessness first gained national attention in the 1980s, when declining incomes, cutbacks to social safety net programs, and a shrinking pool of affordable housing began tipping people into crisis. President Ronald Reagan dubiously argued that homelessness was a lifestyle choice. By the mid-2000s, though, the federal government was taking a more productive approach. George W. Bush’s administration pushed for a “housing first” model that prioritized getting people permanent shelter before helping them with drug addiction or mental illness. Barack Obama furthered the effort in his first term and, in 2010, vowed to end chronic and veteran homelessness in five years and child and family homelessness by 2020.
Rising housing costs are part of the reason some of those deadlines were missed. The Trump administration’s proposal to hike rents on people receiving federal housing vouchers, and require they work, would only make the goals more elusive. Demand for rental assistance has long outstripped supply, leading to yearslong waits for people who want help. But even folks who are lucky enough to have vouchers are increasingly struggling to use them in hot housing markets. A survey by the Urban Institute this year found that more than three-quarters of L.A. landlords rejected tenants receiving rental assistance.
It’s not bad everywhere. Houston, the fourth-most-populous city in the nation, has cut its homeless population in half since 2011, in part by creating more housing for them. That’s dampened the effect of rising rents, Zillow found. Meanwhile, the nonprofit Community Solutions has worked with Chicago, Phoenix, and other cities to gather quality, real-time data about their homeless populations so they can better coordinate their interventions and prioritize spending. The approach has effectively ended veterans’ homelessness in eight communities, including Riverside County in California.
Efficiency can go only so far. More resources are needed in the places struggling the most with homelessness. McKinsey calculated that to shelter people adequately, Seattle would have to increase its outlay to as much as $410 million a year, double what it spends now. Still, that’s less than the $1.1 billion the consultants estimate it costs “as a result of extra policing, lost tourism and business, and the frequent hospitalization of those living on the streets.” Study after study, from California to New York, has drawn similar conclusions. “Doing nothing isn’t doing nothing,” says Sara Rankin, a professor at Seattle University’s School of Law and the director of the Homeless Rights Advocacy Project. “Doing nothing costs more money.”
Then there’s the moral argument for action. “It’s outrageous to me that in a country with so much wealth--and certainly enough for everybody--that there are people who lack even the basics for survival,” says Maria Foscarinis, founder and executive director of the National Law Center on Homelessness & Poverty. Appeals to humanity were part of the strategy in the 1980s, when she and other activists helped push through the first major federal legislation to fight homelessness. Her organization has led a charge against laws that make it a crime to sleep outside in public places, one of the more insidious ways politicians have addressed the crisis. In July the U.S. Court of Appeals for the Ninth Circuit affirmed the unconstitutionality of such bans in a case that Foscarinis’s group--along with Idaho Legal Aid Services and Latham & Watkins--brought against two such ordinances in Boise. “As long as there is no option of sleeping indoors, the government cannot criminalize indigent, homeless people for sleeping outdoors, on public property, on the false premise they had a choice in the matter,” the court wrote. The ruling has led cities, including Portland, Ore., and Berkeley, Calif., to change their policies.
To placate angry constituents, officials too often settle for temporary solutions, such as sweeps of tent encampments and street cleaning. San Francisco Mayor London Breed recently scored some publicity, carrying a broom out to the “dirtiest” block in the city for a photo op with the New York Times. In other places, there’s simply a vacuum of leadership coordinating the patchwork of agencies, nonprofits, and religious organizations trying to help. After reporting intensively for a year on homelessness in the Puget Sound region, the Seattle Times put it bluntly: “No one is in charge.”
Meanwhile, the businesses responsible for much of the area’s economic fortunes, as well as rising housing costs, have been slow to throw their weight behind solutions. Amazon CEO Jeff Bezos recently earmarked a portion of his $2 billion philanthropic pledge for homeless services--only months after his company fought aggressively to beat back a modest tax on large employers in Seattle that would have raised less than $50 million a year for the same.
Blaming people who are trying to get back on their feet is probably the least productive way to solve the crisis. Consider Mindy Woods, a single mother and U.S. Navy veteran who lives in a Seattle suburb. In 2010 she developed autoimmune diseases that made her chronically tired and caused so much pain she struggled to work at the insurance company where she’d been selling disability policies. “I was just a mess,” she says. “I had to quit my job.” To help pay rent for the apartment where she lived with her son, she babysat, watched neighbors’ pets, and led a Camp Fire youth group. Still, she and her son ended up having to leave the apartment because of a serious mold infestation, kicking off an eight-month period when they couch-surfed and spent time in a motel and shelter. It was a challenge just to refrigerate her son’s diabetes medicine.
They eventually were accepted into a transitional apartment, where they stayed for 3½ years. But in 2015 her landlord stopped accepting vouchers. Woods had to race to find another apartment owner who’d take her voucher before it lapsed. Application after application got rejected. “The discrimination was alive and well,” she says. Another eight months passed. When she finally found an apartment, there wasn’t room for her son. They had no choice but to separate, and he now lives nearby. Woods bristles when people blame the homeless for their predicament. “This is not about drugs, this is not about mental illness, this is not about lazy people,” she says. “We were doing everything we could to stay in houses.”
3 notes
·
View notes
Text
Ecclesiology of coronavirus: How faith communities in the Pacific Northwest are adapting
Temple de Hirsch Sinai, a Reform Jewish synagogue in the Capitol Hill neighborhood of Seattle, announced a few days ago that it would hold last night’s and today’s Shabbat service by livestream only, closing the sanctuary to all congregants.
I have a fond memory of TDHS, as I used to live within a walking distance of it and I attended their Friday evening services for some time when Rabbi Earl Starr was still leading the congregation (a long time ago!).
I tuned into this morning’s service, which was intermittently choppy perhaps because of the unexpected overload on livestream servers (after all, this is a pretty large congregation and if everyone was streaming the live video feed it would slow things down).
This solution may work for Reform and Reconstructionist synagogues -- as well as many Protestant churches -- it won’t for Orthodox and many Conservative synagogues, however.
According to the Orthodox and traditionalist interpretation of halacha, or Jewish law, any use of objects that are typically used for “work” is forbidden on Shabbat. This means telephones, stoves, buttons on elevators, light switches, televisions, automobiles, and computers, among others.
I remember spending a shabbat with an Orthodox family for the first time. Electric lights were turned on before Friday sunset and the switches were taped. Refrigerators were set so that when you opened it, the light wouldn’t turn on. And the dad of the household was scolding his five-year-old daughter for playing with a plastic toy shaped like a telephone (even though it is not a real working telephone). All the meals were already made before Friday sunset and put on crockpots. Needless to say, no television, no musical instruments, and certainly a livestreamed virtual synagogue service would be out of question.
The idea of “work” here in the traditional understanding of halacha is somewhat counterintuitive for us in the modern age. On its surface, technological inventions has made our lives less of work. Driving a car for a mile consumes less calories than walking 20 minutes. Riding an elevator from the ground floor to the 20th floor is no work, but imagine walking up the stairs. After all, most of the modern inventions we take for granted were made to make our lives easier, not harder.
Yet, the concept of kedusha (holiness, the set-apart-ness) at the core of shabbat -- one special day of rest that is different from the rest of the week -- also seems to point to a wisdom of making this one day a technology-free zone. After all, even as we stream the shabbat service, the same device also pops up all kinds of distractions: email alerts, Facebook alerts, Twitter alerts, breaking news alerts, and so on. So I respect those who would rather not to make a shabbat a virtual experience.
I have been monitoring the development in major places of worship in Western Washington and Portland metropolitan area for the last several days.
The Roman Catholic Archdiocese of Seattle, has issued directives to all Western Washington Catholic churches to modify the ways how they conduct the Mass. For example, the holy water basin is emptied and administration of the eucharistic elements are modified to minimize the spread of the virus. Similar instructions have also been issued by the Episcopal Diocese of Olympia and the Episcopal Diocese of Oregon.
Sacramental churches (Catholic, Eastern Orthodox, and Anglican churches -- and to a lesser extent, Lutheran and Methodist churches), in which the holy eucharist plays the central role in their worship, cannot easily make their services go online. The eucharistic elements -- the bread and wine -- must be of approved ingredients and be properly sanctified by a priest in order to be valid. While some Evangelical Protestants can “take communion” on their own, or as some televangelists have done, inviting viewers to bring the elements before the screen as the TV preacher remotely say the words of institution, such a method is not typically accepted by traditional sacramental churches.
An option that has been used in the Episcopal Church is the use of “eucharistic visitors”: that is, have someone from the church deliver pre-consecrated wine and bread to homebound and hospitalized communicants. While this may work for a small number of people, it can pose logistical challenges for a larger number of people.
East Lake Church in Bothell, Washington, has decided to cancel all Sunday services through the month of March, while making available the previously scheduled sermon series and workshops online.
Some megachurches appear to be unconcerned, however. Christian Faith in Federal Way, Washington -- one of the largest megachurches in the Puget Sound region -- is moving ahead not only with the regular services tomorrow, but also their special annual event, Vision Weekend. Since Christian Faith, like many Charismatic and Pentecostal churches, believes in divine healing, perhaps it might consider a cancellation of services as a “lack of faith.”
As many such churches are large, it could pose a unique public health challenge.
This is not new. During the Spanish flu pandemic in 1918, many churches shut their doors under the orders of the health authorities.
Beyond the practical issue of whether to hold services this or next week, the spread of COVID-19 in the Pacific Northwest brings an ecclesiological and theological challenge, as well.
In the Hebrew Scriptures and the New Testament alike, there are mentions of leprosy -- a highly contagious disease. The Torah prescribed for detection of leprosy, exclusion and quarantine methods, and how to certify if a patient has recovered. Given the time period in which the Torah was written, its wisdom on public health is far ahead of its time. In the New Testament, however, we see how leprosy (or suspicion of leprosy) has become weaponized as a tool of social exclusion. It may have been true that by the time of Jesus, it has morphed from a sound public health precaution to a form of collective paranoia (n.b.: while this is a common Christian narrative, it is not without critics).
In recent weeks, many Asian-Americans have fallen victim to hate crimes. Asian-owned businesses, such as Chinese restaurants and Korean corner stores, have been losing customers. Conservative talk show hosts such as Lars Larson claim that this is not racism but just a prudent precaution because they may have traveled to China to see relatives over the Chinese New Year (a rather grotesque generalization).
The problem is that we don’t know.
Lack of knowledge destroys people.
Between the incompetent and politicized government response, sensationalistic news coverage, mass panic, and deliberate misinformation, we all feel like we should be safe than sorry.
This means we act as if everyone we see has the SARS-nCoV-2 virus whether they know it or not, and by extension, everything they touch is literally covered with that virus.
Living a life as if everything around us is a deadly landmine can take a toll on our mental health, as well.
People who have been quarantined are already feeling like outcasts and prisoners. The only human interaction they have are with health workers and emergency responders in hazmat suits. If that won’t make you feel like a reject, I don’t know what else would.
Events are getting cancelled, people are not traveling as much, the sentiment is we stock up on toilet papers and hunker down.
Emergencies such as this makes everyone a suspect.
Exclusion prevails over inclusion.
Paranoia and fear overcome reason and faith.
But we don’t have to. We can practice inclusion while still practicing the evidence-based precaution.
The unfortunate situation is that our idea of COVID-19 has been largely shaped by the news footage of Wuhan and the Diamond Princess -- two of the badly mismanaged cases that, despite all the good intentions and drastic measures, only made the situation worse -- not the better responses by Taiwan and South Korea.
0 notes
Text
@Frances Farmer Will Have Her Revenge on Seattle フランシス・ファーマーはシアトルで復讐する
https://www.youtube.com/watch?v=C-deMfnLtMI
アメリカのロックバンド、ニルヴァーナ(仏教の涅槃のこと)(活動期間1987-94年)が歌った。このバンドはリーダーのカート・コバーンが27歳で自殺して終わった。
An American rock band, Nirvana(Buddhism word) sang it.
This group ended when its leader, Kurt Cobain committed suicide when he was 27.
フランシス・ファーマー(1913-70)はアメリカの女優で、ハリウッドの虚飾の生活がいやになり、ブロードウェイに出演したことでパラマウントの怒りを買った。その後交通違反で逮捕されたとき、パラマウントの指示で精神医療施設に入れられ、拷問のような治療を受けた。カートとフランシスの姿が重なって見える。
Frances Farmer was an American actress. She hated the vanity of Hollywood, and acted in Broadway.
So Paramount got angry and they put her in the mental hospital and tortured her.
I can see double image of Kurt and Frances.
歌詞と意味
It's so relieving
To know that you're leaving
As soon as you get paid
It's so relaxing
To hear that you're asking
Wherever you get your way
It's so soothing
To know that you'll sue me
Starting to sound the same
I miss the comfort in being sad
I miss the comfort in being sad
I miss the comfort in being sad
Hey, ooh
In her false witness
We hope you're still with us
To see if they float or drown
Our favorite patient
Display of patience
Disease-covered Puget Sound
She'll come back as fire
To burn all the liars
Leave a blanket of ash on the ground
I miss the comfort in being sad
I miss the comfort in being sad
I miss the comfort in being sad
Hey, ooh
It's so relieving
To know that you're leaving
As soon as you get paid
It's so relaxing
To know that you're asking
Wherever you get your way
It's so soothing
To know that you'll sue me
Starting to sound the same
I miss the comfort in being sad
I miss the comfort in being sad
I miss the comfort in being sad
Hey, ooh
ほっとする
君が出てゆくとわかったから
給料を受け取るとすぐに
ほっとする
君がどこでも
生きてゆくと聞いて
楽になる
君がぼくを訴えると知って
同じようなことが始まってゆくのだ
哀しみの中の慰めが恋しい
X3
おお
彼女の間違った証言でも
ぼくらはまだ君といっしょにいたい
浮くか沈むか確かめるために
ぼくらの好きな患者は
忍耐を見せる
病気だらけのピュージェット湾(ワシントン州)
彼女は炎のようになって戻る
すべての嘘つきを燃やすため
灰の毛布を地上に残す
哀しみの中の慰めが恋しい
X3
おお
ほっとする
君が出てゆくとわかったから
給料を受け取るとすぐに
ほっとする
君がどこでも
生きてゆくと聞いて
楽になる
君がぼくを訴えると知って
同じようなことが始まってゆくのだ
哀しみの中の慰めが恋しい
X3
おお
0 notes
Text
Allen Iverson The Answer Signature Shirt
Allen Iverson The Answer Signature Shirt T shirts Store Online
Allen Iverson The Answer Signature Shirt
There are a few on Puget Sound next to the port such as Seattle Marriott Waterfront and the Edgewater Allen Iverson The Answer Signature Shirt. The subconscious mind allows you to even enjoy the things which you are not going to buy. In traditional shopping, you just go for your preferred shopping mall and judge the brand much like your choice and you may choose tone shape and size much like your choice whenever you are going for customary and when you intend to buy a clothing at that time you may even check the sizing of the wardrobe and also see the matching picking match with one and not therefore it shout on your body and skin color or not along with see the additional accessories which may need to get excellent look and obtain up your character. Shopping consists of looking for things you need. There is no need of anything else. There can be many experiences in the traditional centre that can take a full day. The Silva Method encompasses a variety of powerful exercises that take you deep into Alpha and Theta levels of the mind so that you can work within your subconscious as well as your conscious mind. The conscious mind would keep on walking straight without even pausing before the showcase but the unconscious mind can take a break and indulge in the forbidden pleasures. Such pleasures are vital for the mental equilibrium of a person, especially a female person. Which means that, these are a thing about shopping on-line and typical shopping both have its own gains and constraint now you have to imagine which at is best place for you.
Allen Iverson The Answer Signature Shirt, Hoodie, V-Neck, Sweater, Longsleeve, Tank Top, Bella Flowy and Unisex, T-Shirt
Allen Iverson The Answer Signature Shirt Unisex Hoodie
Allen Iverson The Answer Signature Shirt Unisex Sweatshirt
Allen Iverson The Answer Signature Shirt Men’s Long Sleeved T-Shirt
Allen Iverson The Answer Signature Shirt Men’s T-Shirt
Allen Iverson The Answer Signature Shirt Women’s T-shirt
Buy Allen Iverson The Answer Signature Shirt
Consumers now have favorite websites they shop at so online shopping has become a normal part of their routine Allen Iverson The Answer Signature Shirt. Have you shopped for a cruise vacation? Are you planning a cruise vacation but don’t know where to start? 7. Start a vegetable garden. They are now online malls, manufacturer websites, and specialty sites catering to any type of product. Due to the convenience and quickness of online shipping, men are now making many purchases online. Rather than going for shopping and making it a completely boring process, you can go for a date. As well, the increase in effective security technology and education tips for consumers on how to shop safely online has resulted in more consumers making online purchases. Over the years, consumers have become busier with a lot more stress in their daily lives. The sleek form factor of the HP ENVY or HP Pavilion all-in-ones makes an attractive statement in any workspace, while the high-performance HP OMEN gaming systems take gaming and more to an entirely new level. You easily access an online store either from home or from office and can do shopping while take delivery at oyur door step. Now, almost every home has a computer and access to the internet. As well, they have access to online shopping from home and at work. Your home may need a few minor modifications to ensure your safety upon return from the hospital. If they need to search for product, search engines can effectively bring up the link to the searched product. A little bit of planning can make all of the difference for your diet success.
A Cheap T shirts Store Online Shopping at TrendTshirtNew, we’re about more than t-shirts! You Can See More Product: https://trendtshirtnew.com/product-category/trending/
Allen Iverson The Answer Signature Shirt
source https://trendtshirtnew.com/product/allen-iverson-the-answer-signature-shirt/
0 notes
Text
Woah. March was a TRIP!
Steve and I landed in Portland, OR on February 29, aka the day that the first coronavirus deaths happened in Seattle, WA. We were on a trip to help a family member that just had major surgery and we also had plans on sight seeing in Seattle…but our trip was much different than we had planned it to be.
Upon landing we gathered our luggage, got our rental car and drove to a brewery to get lunch and that’s when reality hit. We were sitting at the bar and saw the news. My phone started to ring and it was my sister asking us to cancel all of our Seattle plans.
We spent that night at a family friends house in southern WA, and then drove to my sisters place in Tacoma on March 1. We were watching the news of what was happening in King County, WA daily. We were watching numbers skyrocket seemingly by the minute.
We ended up cancelling the food tour of Pike Market, and spending our one night in Seattle pretty much hotel bound. I did take two Bar Method classes, and we went for dinner at Capitol Cider, but it was not crowded.
The bright spot in not being able to wander Seattle, was that we got to spend a few hours with Steve’s Godmother at her beautiful home in Federal Way. Her backyard is the Puget Sound. We walked in the chilly, fresh air. I collected sea glass and sea shells to bring back to Connecticut with me. It was a very peaceful morning.
Steve and his Godmother and her Husband
Steve and I
Steve used a walking stick for the hike up and down the hill to the beach
Collecting shells
After a 6am workout at The Bar Method Seattle
I fit inside the giant cabinet in our hotel room
I got to see my friend Savannah
Paul and Tracy
Steve trying beer, right when we got to Portland
The photos that I have included, are pretty much the only photos that we took on our trip. We were able to squeeze in some time with a few people, but as we watched the news unfold, we started limiting the amount of interactions that we had leading up to our departure from Portland on March 7.
When we got back from our trip we took an uber home from JFK instead of subjecting ourselves to 3 different modes of public transportation. I was watching the news on the plane ride back and learned that the first cases in NY state had started to be detected. I knew that once we got home, things were about to be drastically different than they were when we left for WA.
On March 8, we went to hear the New Choral Society sing a concert. I usually perform with the group, but since I had been traveling, I was not singing the concert. I am very glad that we went and listened to the concert, and attended the after party, as it was the last time the group has been together face to face…and will be until the fall.
I got back to work on March 9, I had been traveling, the family I work for had been traveling…we all were watching the news constantly and trying to figure out what was going to happen next.
The family I work for was not worried about things shutting down, but I have family in China, and I saw what was coming for us here. I knew that it would not stay business as usual here, if we wanted to flatten the curve.
I asked my family what things were/are like where they live. I was told that they did not re-open things after the new year celebrations, and now after more than 9 weeks of shut downs things are slowly opening back up. They get their temperatures taken everywhere, and if you have a fever, you get sent to the fever hospital to be tested. Everyone is required to wear masks in public…I ordered my masks weeks ago due to this fact. I knew that at some point the CDC would recommend that we start wearing them here in the USA and I wanted to be prepared.
Things where my family live are started to return to a new normal, and that gives me some hope for life here in Connecticut. I have been off of work as a precautionary measure for 2 weeks now. I have been doing my best to keep busy. I have started a new passion project called Storytime with Alyssa. It has been amazing. I have been participating in as many social zoom calls as I can.
I have not taken a full Bar Method class, as I am not mentally ready for that yet. I am still grieving the loss of the in studio classes too much, but I have started doing my ABCs of fitness workouts again, and that feels really good.
I am very thankful for my church, bar method, instagram, and facebook communities at this time. I would not be staying as level headed without all of my virtual people.
I bought myself flowers
Home date:steak
Dory working out
Spring is here!
Roomba is the main housekeeper now
The store was out of eggs, but my friend has chickens and saved the day!
Breakfast of champions
Coffee with Church friends
AlphaBesties test call!
Marinated Onions
You cant see me
Steve sporiting the social distance fashion
Self confidence boosting selfie
Zoom Church
I am finding ways to cope with this new way of life. I am taking it day by day, sometimes hour by hour. We will all get through this together…but apart…
COVID 19 Woah. March was a TRIP! Steve and I landed in Portland, OR on February 29, aka the day that the first coronavirus deaths happened in Seattle, WA.
0 notes
Text
Dual Diagnosis Treatment Seattle
Contents
With dual activity
Search all co-occurring disorder programs
Treatment last week
Issues like trauma treatment
Get help finding dual diagnosis have
And the cookies
Seattle, WA, alcohol and drug detoxification centers (clinics).
In 36 patients (80%), peripheral fractures were produced before diagnosis or in diagnosed patients who had never adhered to specific treatment … survey on the prevalence of bone fractures in celiac disease patients. The present …
Dual Diagnosis Rehab Treatment in Seattle, WA. Addiction and mental health problems go hand in hand. The two feed off each other, creating an endless cycle that seemingly can't be broken.
Pacritinib is an oral tyrosine kinase inhibitor with dual activity against JAK2 and FLT3 … An unmet need is a condition whose treatment or diagnosis is not addressed adequately by available therapy. The purpose of the Fast Track …
Addiction Treatment Boca Raton Florida Contents 44 alcohol and drug rehabs Got the search Say the wrong Drug rehabilitation addiction treatment Early 1800's; all can Health treatment for adults BOCA RATON – NFL teams selected seven FAU players in the NFL … Williams has yet to completely heal from knee surgery, but says he rehab is going well … BOCA
Seattle, WA, residential (inpatient) dual diagnosis (co-occurring disorder) treatment centers / programs.
Dual Diagnosis is the process of treating those who are battling substance abuse and a mental disorder like depression. Call (206) 777-4098 to get help now.
Apr 10, 2018 … The term "primary" indicates that the person has a stand alone diagnosis that is present regardless of whether they have another disorder. Because COD is more complex than mental illness or substance abuse alone, effective treatment involves responding to these mutually interacting disorders.
Learn more about the inpatient dual diagnosis program at our hospital near Seattle, Washington. Cascade Behavioral Health.
31 Dual Diagnosis /Co-Occurring Disorder Programs in Seattle WA. Directory of Co-Occurring Disorder Programs in Seattle WA. search all co-occurring disorder programs in Seattle.
Nov. 29, 2016 /PRNewswire/ — "In Your Right Mind," a weekly behavioral health radio program … the National Eating Disorders Association and founder of the Eating Disorder Treatment Collaborative. Regarding the treatment of eating …
Dual diagnosis treatment in Seattle, Washington is such an important component of addiction treatment for so many.
Learn more about the inpatient dual diagnosis program at our hospital near Seattle, Washington. Cascade Behavioral Health.
Figure Out More About Dual Diagnosis Center. Read Articles Here.
The memorandum, filed in the US District Court in Seattle, states that "transgender persons with a history or diagnosis of gender dysphoria — individuals who the policies state may require substantial medical treatment, including …
Addiction Treatment Centers In Indiana Contents Treatment programs. get Withdrawal symptoms and Long before lucas would Center … where he’s got The search for the best rehab centers across the nation now brings us to Indiana. Many of these drug rehab centers in Indiana are several decades old, one established in the early 1800's; all can offer their clients experience
Stephens pleaded on Facebook last week after receiving the diagnosis … from a local physician who was dual certified in Canada and the US. Zytner said their symptoms have improved significantly since they began treatment last week.
… in the year 2006, consisting of both for profit and nonprofit centers. We bring to you a comprehensive list of such dual diagnosis centers of drug rehabilitation and recovery services in Washington through our directory. DUAL DIAGNOSIS TREATMENT CENTERS IN WASHINGTON. Sound Mental Health. Seattle, WA 98122.
Genesis House Dual Diagnosis Treatment Center – Seattle, WA
Dual diagnosis, non 12-Step rehab. We’re a very different program, find out why!
Dual diagnosis treatment in Seattle, Washington is such an important component of addiction treatment for so many.
Seattle, WA 98108. VA Puget Sound Health Care System can be found online at www.pugetsound.va.gov. Central Washington Comprehensive Mental Health 402 South … Programs range from adult and adolescent inpatient treatment to co- occurring disorders treatment (also known as dual diagnosis rehab). Additional …
Results will be presented Monday, Dec. 5 at the 58th American Society of Hematology Annual Meeting by Dr. John Pagel, chief of the Hematologic Malignancies program at the Swedish Cancer Institute in Seattle … more high-risk AML …
31 Seattle, WA Dual Diagnosis Drug Rehab – Best Dual Diagnosis Treatment Centers in Seattle Washington
Addiction Treatment Seattle; Rehabilitation Substance In Saint Paul Clinic Cocaine Treatment In Concord; Clinic Cocaine … Top Rated Dual Diagnosis Treatment Centers;
Outpatient Addiction Recovery Services to Help You Live Your Best Life.
Results will be presented Monday, Dec. 5 at the 58th American Society of Hematology Annual Meeting by Dr. John Pagel, chief of the Hematologic Malignancies program at the Swedish Cancer Institute in Seattle … more high-risk AML …
Find Dual Diagnosis Treatment Centers in Seattle, King County, Washington, get help from Seattle Dual Diagnosis Rehab for Dual Diagnosis Treatment in Seattle, get help with Co-Occurring Disorders in Seattle.
LP, College Station, USA), in which analysis was performed by Stat/Transfer version 10 (Circle Systems, Seattle, USA). …
Inpatient Drug Rehab, Psychiatric hospital or psychiatric unit of a general hospital . Treatment Approaches: Group Therapy, Cognitive/behavior Therapy, Dialectical Behavior Therapy, Behavior Modification, Dual Diagnosis Drug Rehab, Trauma Therapy, Smoking/tobacco cessation counselling. Payment Types Accepted:
LP, College Station, USA), in which analysis was performed by Stat/Transfer version 10 (Circle Systems, Seattle, USA). …
Addiction Treatment Conferences 2017 Contents Association. … 20th international Conferences and trainings across the country Recovery have been Addiction Treatment Centers In Indiana Contents Treatment programs. get Withdrawal symptoms and Long before lucas would Center … where he’s got The search for the best rehab centers across the nation now brings us to Indiana. Many of these drug rehab
At The Clearing, we use dual diagnosis treatment to address anxiety, depression and other mental disorders that occur alongside addiction. Visit our website to learn more about our approach.
Thunderbird Treatment Center in Seattle, Washington treatment options, reviews and payment options from Treatment-Centers.net.
Stephens pleaded on Facebook last week after receiving the diagnosis … from a local physician who was dual certified in Canada and the US. Zytner said their symptoms have improved significantly since they began treatment last week.
Dual Diagnosis Treatment Centers In Tennessee Contents issues like trauma treatment center offers Designed for residential service providers Issues. tennessee residents get help finding dual diagnosis have been addiction treatment centers Foundations Recovery Network's mission is … Our treatment programs also have the flexibility and … highest standards of excellence in dual diagnosis treatment. The Oaks at La Paloma in Memphis,
Dual diagnosis treatment (Persons with co-occurring mental and substance abuse disorders); Court ordered addiction treatment; ASL or other assistance for hearing impaired; Outpatient counseling treatment; Holistic rehabilitation treatment, alternative treatment. Community Psychiatric Clinic Bridgeway Branch.
Dual diagnosis treatments in Seattle, Washington are available at Island Assessment & Counseling. Call (866) 931-7995 for your consultation today.
The Clearing is a non-12 step, dual diagnosis residential treatment center specializing in substance abuse along with issues associated with depression, self esteem, trauma and loss. Recovery takes on a whole new ….. The food there tastes as if it was catered in from El Gaucho's in Seattle every day. and the cookies, the …
Browse through our comprehensive directory of dual diagnosis drug treatment centers in WA.
If you or a loved one is struggling to manage an addiction, Free by the Sea, located in the State of Washington, has treatment options that can make the struggle easier. Dual diagnosis treatment is available for anyone seeking assistance in managing addiction. Serving the Pacific Northwest, including Washington (Seattle), …
Pacritinib is an oral tyrosine kinase inhibitor with dual activity against JAK2 and FLT3 … An unmet need is a condition whose treatment or diagnosis is not addressed adequately by available therapy. The purpose of the Fast Track …
Cocaine Plant For Sale Contents Been genetically modified 44 alcohol and drug Chile and argentina Sees many who get treatment wind Coca Plants For Sale, Wholesale Various High Quality Coca Plants For Sale Products from Global Coca Plants For Sale Suppliers and Coca Plants For Sale Factory,Importer,Exporter at Alibaba.com. The habit of chewing coca leaves has been prevalent since
31 Dual Diagnosis /Co-Occurring Disorder Programs in Seattle WA. Directory of Co-Occurring Disorder Programs in Seattle WA. Search all Co-Occurring Disorder Programs in Seattle.
The post Dual Diagnosis Treatment Seattle appeared first on Freedom From Addiction II.
0 notes
Photo

@Regrann from @pepperspray_media - On June 13th, 2017 Tommy Le was shot and killed by deputies in Washington state a few hours away from his high school graduation. The initial report of the killing stated that several 911 calls about a reportedly armed man prompted the dispatch of three deputies. A homeowner that called 911 said that he fired a warning shot in response to Le approaching him with what he thought was "a knife or some sort of sharp object" before fleeing inside his home. The Sheriff's Office stated that Le pounded on the door and "stabbed" it with the sharp object. After tasers were deemed "not effective" Deputy Cesar Molina shot Le 3 times. Le died of his injuries at a hospital. About a week after the shooting the sheriff's office revealed that the "sharp object" was actually a pen. Le's family and friends are struggling with questions surrounding his death and the story coming from law enforcement. Me had no criminal record and showed no signs of violence or mental illness. Deputy Molina was placed on administrative leave but was approved returning to work on June 30th. Tommy Le's death was the first of three fatal police shootngs in the Seattle/Puget Sound region this June. Five days later Charleena Lyles was shot by two Seattle Police officers and Giovonn Joseph-McDade was killed by Kent police. ---------------------------------------------------------------------------------------- To support Tommy Le's family go to this site: https://www.youcaring.com/tommyle-874946 ----- "Tommy deserves justice and closure. The family is asking for your generosity to help with funeral and legal expenses in the coming months as we continue to fight for justice. Any unused funds will be donated to charity." -from the donation site https://www.youcaring.com/tommyle-874946 #tommyle #pepperspraymedia #riptommyle #pepperspray #stoppolicebrutality #206bpp #justice #seattle #welcometoseattle - #regrann
#pepperspraymedia#tommyle#stoppolicebrutality#justice#regrann#pepperspray#welcometoseattle#seattle#riptommyle#206bpp
0 notes
Photo

On June 13th, 2017 Tommy Le was shot and killed by deputies in Washington state a few hours away from his high school graduation. The initial report of the killing stated that several 911 calls about a reportedly armed man prompted the dispatch of three deputies. A homeowner that called 911 said that he fired a warning shot in response to Le approaching him with what he thought was "a knife or some sort of sharp object" before fleeing inside his home. The Sheriff's Office stated that Le pounded on the door and "stabbed" it with the sharp object. After tasers were deemed "not effective" Deputy Cesar Molina shot Le 3 times. Le died of his injuries at a hospital. About a week after the shooting the sheriff's office revealed that the "sharp object" was actually a pen. Le's family and friends are struggling with questions surrounding his death and the story coming from law enforcement. Me had no criminal record and showed no signs of violence or mental illness. Deputy Molina was placed on administrative leave but was approved returning to work on June 30th. Tommy Le's death was the first of three fatal police shootngs in the Seattle/Puget Sound region this June. Five days later Charleena Lyles was shot by two Seattle Police officers and Giovonn Joseph-McDade was killed by Kent police. ---------------------------------------------------------------------------------------- To support Tommy Le's family go to this site: https://www.youcaring.com/tommyle-874946 ----- "Tommy deserves justice and closure. The family is asking for your generosity to help with funeral and legal expenses in the coming months as we continue to fight for justice. Any unused funds will be donated to charity." -from the donation site https://www.youcaring.com/tommyle-874946 #tommyle #pepperspraymedia #riptommyle #pepperspray #stoppolicebrutality #206bpp #justice #seattle #welcometoseattle
#pepperspraymedia#welcometoseattle#tommyle#riptommyle#pepperspray#seattle#stoppolicebrutality#justice#206bpp
0 notes
Text
Bookmarks: Notable Portland women, Bonnie and Clyde, the history of Oregon hops, more
Historian Tracy Prince (left) and researcher Zadie Schaffer spent two-and-a-half years working on "Notable Women of Portland," a book that addresses their feeling that women’s contributions are often overlooked. (Author photo: Courtesy of Tracy Prince; book cover, Arcadia Publishing)
Notes from The Oregonian/OregonLive’s books desk.
"Notable Women of Portland": Mother-daughter authors Tracy Prince and Zadie Schaffer have produced the latest Oregon title in the Images of America regional and local history series from Arcadia Publishing. Like other books in the series, "Notable Women of Portland" (128 pages, $26.99) consists primarily of historical photographs, but what photographs they are. To give a small sampling: Dr. S.K. Chan, who was president of the Chinese American Equal Suffrage Society of Portland; Oregon women "eagerly crowding into the courthouse for the right to register for jury duty" in 1912; Colored Women’s Equal Suffrage League president Hattie Redmond; Oregon Navy Yeomanettes who worked in the Puget Sound Navy Yard during World War I; women from a tenants league protesting at City Hall in the late 1940s; numerous women artists; and much more. The authors will hold a free book launch party and slideshow at 7 p.m. Monday, June 5, at the Mission Theater, 1624 N.W. Glisan St. They’ll also appear at 7 p.m. Thursday, June 8, at Broadway Books, 1714 N.E. Broadway, and 7 p.m. Tuesday, June 27, at Annie Bloom’s Books, 7834 S.W. Capitol Highway. Prince says proceeds from the book will benefit women served by Transition Projects, a nonprofit that assists people in need of housing.
Clyde Barrow and Bonnie Parker were suspected of 13 killings as well as a series of robberies and burglaries when they were killed by law enforcement officers on May 23, 1934.
Bonnie and Clyde: Portland authors Clark Hays and Kathleen McFall have launched a new alternate-history series centered on an intriguing question: What if the outlaw couple Bonnie and Clyde weren’t gunned down in 1934, but were instead kidnapped by a secret organization that wanted to ensure the New Deal overcame bitter opposition from the 1 percent? "Bonnie and Clyde: Resurrection Road" (Pumpjack Press, 308 pages, $15.95) is a taut, fast-paced, fun read that cuts agilely back and forth between the anti-heroes’ Depression-era escapades and a modern-day reporter trying to revive his career with a big scoop, all while addressing serious topics such as income inequality. The book officially publishes Tuesday, May 23, the anniversary of the couple’s death.
Welcome signs go up for the Hop Fiesta in Independence in 1948. Author Peter Kopp writes about the festival in his new book "Hoptopia." From left, Robert Craven, parade chairman; Ralph Kletzing, member of the Hop Bowl board; Cecil (Joe) Lamb, president of Hop Bowl Inc., the event sponsor; Tom Smith, bowl member. Nailing sign is Harold Prinus, also a board member.
A history of hops: About 10 years ago, Peter Kopp was driving through Aurora when he saw hops on the vine for the first time. Kopp, an Oregon native who is a fan of craft beers, was fascinated by the sight and decided to write his doctoral dissertation in history on the Pacific Northwest’s hops production. Now an assistant professor and director of public history at New Mexico State University, Kopp has turned his dissertation into a book, "Hoptopia: A World of Agriculture and Beer in Oregon’s Willamette Valley" (University of California Press, 328 pages, $29.95). He’ll give a free talk about the Cascade hop at 6:30 p.m. Tuesday, May 30, at McMenamins Edgefield, Blackberry Hall, 2126 S.W. Halsey St., Troutdale. Look for historical tidbits such as an early 20th-century contract between Ireland’s Guinness Brewery and Willamette Valley Hop Growers, a "Hop Fiesta" in Independence each summer from the 1930s to 1950s, and the Pink Boots Society of women brewers.
Military trauma: New York author Diane Cameron, whose book "Never Leave Your Dead: A True Story of War Trauma, Murder, and Madness" (Central Recovery Press, 176 pages, $15.95) tells the story of a Marine with mental illness who became her stepfather, will speak at the Oregon State Hospital’s Museum of Mental Health in conjunction with the new exhibit "War Wounds: The Impact of War on the Oregon State Hospital." The exhibit opens on Armed Services Day, Saturday, May 20; viewing hours are noon to 4 p.m. Tuesday-Saturday, 2600 Center St. N.E. Cameron will speak at 1:30 p.m. Sunday, May 21; admission is free for museum members, $10 for nonmembers.
Ecopoetry: Scott T. Starbuck has published "Hawk on Wire: Ecopoems" (Fomite, 102 pages, $15), a slim volume that takes a hard look at climate change and fossil fuel dependency, including from the perspectives of the ghosts of environmental advocate Edward Abbey and others. Starbuck wrote much of the collection as a 2016 climate change resident in poetry at Playa, an artists community in Summer Lake, in the Oregon outback.
In the national media: Two of Portland’s favorite authors, Lidia Yuknavitch and Cheryl Strayed, got boosts from The New York Times recently. Yuknavitch’s byline appeared on a review of the audiobook edition of Neil Gaiman’s "Norse Mythology," read by Gaiman himself "so viscerally" that after listening to the audiobook for a week, she writes, she thought her "bedroom might explode into Valhalla." Strayed’s name was invoked repeatedly in an interview with actor Jeffrey Tambor ("Arrested Development," "Transparent") who praised her book "Tiny Beautiful Things: Advice on Love and Life From Dear Sugar." (Tambor appears at 7 p.m. Monday, May 22, at Powell’s Books at Cedar Hills Crossing, 3415 S.W. Cedar Hills Blvd., to discuss his memoir, "Are You Anybody?," with The Oregonian/OregonLive’s TV critic, Kristi Turnquist.)
Source Article
The post Bookmarks: Notable Portland women, Bonnie and Clyde, the history of Oregon hops, more appeared first on MENDINGHEARTSGIFTS.
Read full post at: http://www.mendingheartsgifts.com/bookmarks-notable-portland-women-bonnie-and-clyde-the-history-of-oregon-hops-more/
0 notes
Text
Lawsuit Following Greenwood Explosion Injuring 9 Firefighters
Last March, multiple Seattle firefighters were injured after a natural-gas lead that led to a massive explosion. Jeff Markoff, one of the nine injured firefighters, filed his lawsuit last Friday and reported that he was “about 90 feet from the epicenter of the alleyway explosion that leveled two buildings and damaged dozens more. He said he has since experienced ‘ongoing cognitive difficulties, severe headaches, hearing loss, disturbances such as recurring images after the explosion, memory loss’ and other health issues.” Markoff, having nearly 20 years serving others, only missed a few shifts after the explosion, however he claims that headaches are almost a daily occurrence.
Before the explosion – at 1:04 a.m. – the firefighters were looking for the source of the reported gas leak and at 1:40 a.m., were surprised by the massive explosion. Thankfully, each of the injured firefighters were treated at a local hospital and released the same day.
Puget Sound Energy “reached a $1.5 million settlement with the Utilities and Transportation Commission (UTC) over the March 2016 explosion. The settlement calls for PSE to complete ‘a comprehensive inspection and remediation program’ of thousands of retired gas lines.”
Markoff hopes that PSE is “held accountable so this doesn’t happen again – so guys that I work with don’t have to face something like this.” Attorney and Shareholder James Gooding is currently working with clients in a similar explosion case. Explosions and many other disasters of this nature are often both terrifying and preventable; through GLP Attorneys, these types of cases are classified as a Premises Liability case.
If you or anyone you know have been injured, physically or mentally, please reach out for a free evaluation. Often times, people are injured and misrepresented, but with GLP Attorneys and our core values, we have helped and assisted thousands through all process from injury to recovery.
For more information on the Greenwood explosion, follow this source
source http://www.glpattorneys.com/premises-liability-lawsuit-following-explosion/ from Graham Lundberg Paschal http://grahamlundbergpaschal.blogspot.com/2017/05/lawsuit-following-greenwood-explosion.html
0 notes
Text
Lawsuit Following Greenwood Explosion Injuring 9 Firefighters
Last March, multiple Seattle firefighters were injured after a natural-gas lead that led to a massive explosion. Jeff Markoff, one of the nine injured firefighters, filed his lawsuit last Friday and reported that he was “about 90 feet from the epicenter of the alleyway explosion that leveled two buildings and damaged dozens more. He said he has since experienced ‘ongoing cognitive difficulties, severe headaches, hearing loss, disturbances such as recurring images after the explosion, memory loss’ and other health issues.” Markoff, having nearly 20 years serving others, only missed a few shifts after the explosion, however he claims that headaches are almost a daily occurrence.
Before the explosion – at 1:04 a.m. – the firefighters were looking for the source of the reported gas leak and at 1:40 a.m., were surprised by the massive explosion. Thankfully, each of the injured firefighters were treated at a local hospital and released the same day.
Puget Sound Energy “reached a $1.5 million settlement with the Utilities and Transportation Commission (UTC) over the March 2016 explosion. The settlement calls for PSE to complete ‘a comprehensive inspection and remediation program’ of thousands of retired gas lines.”
Markoff hopes that PSE is “held accountable so this doesn’t happen again – so guys that I work with don’t have to face something like this.” Attorney and Shareholder James Gooding is currently working with clients in a similar explosion case. Explosions and many other disasters of this nature are often both terrifying and preventable; through GLP Attorneys, these types of cases are classified as a Premises Liability case.
If you or anyone you know have been injured, physically or mentally, please reach out for a free evaluation. Often times, people are injured and misrepresented, but with GLP Attorneys and our core values, we have helped and assisted thousands through all process from injury to recovery.
For more information on the Greenwood explosion, follow this source
from GLP Attorneys http://www.glpattorneys.com/premises-liability-lawsuit-following-explosion/
0 notes