#Sheila cohen
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr was the first site to host the blog for President Barack Obama in 2011.
Photo
🇬🇧

Sheila Cohen and Nigel Waymouth - founders of King’s Road boutique Granny Takes a Trip circa 1967
(Courtesy of Roger Klein)
#nigel waymouth#Sheila cohen#granny takes a trip#swinging london#king's road#swinging sixties fashion#1967#british psychedelia
83 notes
·
View notes
Text


Colin and Sheila, What We Do In The Shadows S3 E8 'The Siren'
(Click for better quality)
#digital art#art#my art#fanart#krita#what we do in the shadows#what we do in the shadows fanart#wwdits#colin robinson#sheila#the siren#vampires#mark proksch#catherine cohen#i've been meaning to draw from this series for so long#and i really liked this episode. and sheila - she's very cute#this conversation was really good too#one of the times i felt for colin robinson hehe
19 notes
·
View notes
Text



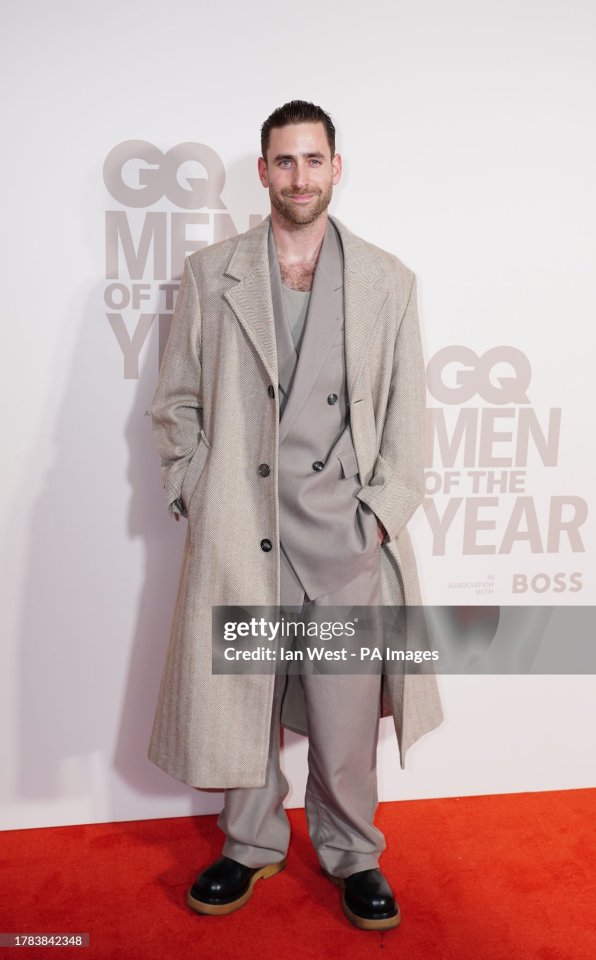




oliver jackson-cohen featuring actress/singer sheila atim at the gq men of the year awards at the royal opera house on 15 november 2023
#oliver jackson-cohen#oliver jackson cohen#sheila atim#jackdaw#jackdaw film#2023#NOT!!!!! in all black!
46 notes
·
View notes
Video
youtube
Carlos Santana has a career that moves within a variety of idioms, though he remains a rock musician at heart. Sure, he appears on many jazz fusion records, yet he always puts some of his rock stylings in these proceedings. That makes his collaboration with Herbie Hancock on Monster weird, since you can't really locate much of the rock idiom there. To be honest, you can't find jazz there either. Actually, I am quite happy to hear Herbie Hancock did some LPs, where he discarded his genre and which probably pissed off most of his audience. Nonetheless, there's something admirable about someone like him doing something like this, more musicians should do this more often. And the fact that he convinced Santana for this? Even better.
#herbie hancock#monster#saturday night#carlos santana#wah wah watson#freddie washington#alphonse mouzon#sheila escovedo#greg walker#bill champlin#julia tillman waters#luther waters#oren waters#maxine willard waters#jeffrey cohen#david rubinson#80's music#disco
0 notes
Text
@elonmusk
These awful people all need to be voted out, either in the primaries or the general election. They sully the Capitol Building with their presence.
THESE ARE THE 158 DEMOCRATS WHO VOTED AGAINST DEPORTING SEX OFFENDERS Alabama: -Terri Sewell California: -Pete Aguilar -Ami Bera -Julia Brownley -Salud Carbajal -Tony Cárdenas -Judy Chu -Jim Costa -Mark DeSaulnier -John Garamendi -Robert Garcia -Sylvia Garcia -Jimmy Gomez -Jared Huffman -Ro Khanna -Sydney Kamlager-Dove -Barbara Lee -Ted Lieu -Zoe Lofgren -Doris Matsui -Kevin Mullin -Grace Napolitano -Nancy Pelosi -Katie Porter -Linda Sánchez -Adam Schiff -Brad Sherman -Norma Torres -Mike Thompson -Maxine Waters Colorado: -Jason Crow -Diana DeGette -Brittany Pettersen -Joe Neguse Connecticut: -Rosa DeLauro -John Larson -James Himes Delaware: -Lisa Blunt Rochester Florida: -Kathy Castor -Sheila Cherfilus-McCormick -Lois Frankel -Maxwell Frost -Darren Soto -Frederica Wilson -Debbie Wasserman Schultz Georgia: -Sanford D. Bishop Jr. -Lucy McBath -Henry “Hank” Johnson -Nikema Williams -David Scott Hawaii: -Ed Case -Jill Tokuda Illinois: -Sean Casten -Danny Davis -Jesús “Chuy” Garcia -Jonathan Jackson -Raja Krishnamoorthi -Robin Kelly -Delia Ramirez -Janice Schakowsky -Mike Quigley -Bill Foster -Brad Schneider -Lauren Underwood Indiana: -André Carson Kentucky: -Morgan McGarvey Louisiana: -Troy Carter Maine: -Chellie Pingree Maryland: -Steny Hoyer -Glenn Ivey -Kweisi Mfume -Jamie Raskin C.A. Dutch Ruppersberger -John Sarbanes -David Trone Massachusetts: -Jake Auchincloss -Katherine Clark -Bill Keating -Seth Moulton -Ayanna Pressley -Richard Neal -Lori Trahan -James McGovern Michigan: -Dan Kildee -Debbie Dingell -Rashida Tlaib -Shri Thanedar -Haley Stevens Minnesota: -Betty McCollum -Ilhan Omar -Dean Phillips Mississippi: -Bennie Thompson Missouri: -Cori Bush -Emanuel Cleaver New Hampshire: -Ann Kuster New Jersey: -Andy Kim -Rob Menendez -Donald Norcross -Bonnie Watson Coleman -Frank Pallone New Mexico: -Melanie Stansbury -Teresa Leger Fernandez New York: -Jamaal Bowman -Adriano Espaillat -Hakeem Jeffries -Yvette Clarke -Gregory Meeks -Alexandria Ocasio-Cortez -Jerrold Nadler -Nydia Velázquez -Paul Tonko -Dan Goldman -Ritchie Torres -Grace Meng -Joseph Morelle North Carolina: -Alma Adams -Valerie Foushee -Deborah Ross Ohio: -Shontel Brown -Joyce Beatty -Greg Landsman Oregon: -Earl Blumenauer -Suzanne Bonamici -Valerie Hoyle Pennsylvania: -Madeleine Dean -Mary Scanlon -Summer Lee Rhode Island: -Gabe Amo South Carolina: -James Clyburn Tennessee: -Steve Cohen Texas: -Greg Casar -Veronica Escobar -Joaquin Castro -Sylvia Garcia -Lloyd Doggett -Lizzie Fletcher -Al Green -Jasmine Crockett -Marc Veasey Vermont: -Becca Balint Virginia: -Donald Beyer -Gerald Connolly -Jennifer McClellan -Bobby Scott Washington: -Suzan DelBene -Derek Kilmer -Rick Larsen -Marilyn Strickland -Pramila Jayapal Wisconsin: -Gwen Moore -Mark Pocan Source: Newsweek
54 notes
·
View notes
Text

𝗧𝗵𝗲 𝟯𝟵 𝗟𝗮𝘄𝗺𝗮𝗸𝗲𝗿𝘀 𝗟𝗲𝗮𝘃𝗶𝗻𝗴 𝗖𝗼𝗻𝗴𝗿𝗲𝘀𝘀 𝗜𝗻 𝟮𝟬𝟮𝟰 (𝗧𝘄𝗶𝗰𝗲 𝗔𝘀 𝗠𝗮𝗻𝘆 𝗗𝗲𝗺𝗼𝗰𝗿𝗮𝘁𝘀 𝗔𝘀 𝗥𝗲𝗽𝘂𝗯𝗹𝗶𝗰𝗮𝗻𝘀)
1. Ruben Gallego
2. Debbie Lesko
3. Tony Cardenas
4. Anna Eshoo
5. Barbara Lee
6. Grace F. Napolitano
7. Katie Porter
8. Adam Schiff
9. Ken Buck
10. Lisa Blunt Rochester
11. Jim Banks
12. Victoria Spartz
13. John Sarbanes
14. David Trone
15. Dan Kildee
16. Elissa Slotkin
17. Dean Phillips
18. Andy Kim
19. Brian Higgins
20. George Santos
21. Dan Bishop
22. Jeff Jackson
23. Bill Johnson
24. Brad Wenstrup
25. Earl Blumenauer
26. Colin Allred
27. Michael C. Burgess
28. Kay Granger
29. Sheila Jackson Lee
30. Abigail Spanberger
31. Jennifer Wexton
32. Derek Kilmer
33. Alex Mooney
34. Joe Manchin
35. Tom Carper
36. Mike Braun
37. Ben Cardin
38. Mitt Romney
39. Debbie Stabenow
- Ezra A. Cohen
#pay attention#educate yourselves#educate yourself#knowledge is power#reeducate yourself#reeducate yourselves#think about it#think for yourselves#think for yourself#do your homework#do some research#do your own research#ask yourself questions#question everything#news
51 notes
·
View notes
Text




Fiction Recommendations: Cozy Holiday Romances
Cozy up with one of these heartwarming romance picks this holiday season!
Make the Season Bright by Ashley Herring Blake
It's been five years since Charlotte was ditched at the altar by her ex-fiancée, and she’s doing more than okay. Sure, her single mother never checks in, but she has her strings ensemble and her life in New York is a dream come true. As the holidays draw near, her ensemble mate Sloane persuades Charlotte and the rest of the quartet to spend Christmas with her family in Colorado, but when Charlotte arrives, she discovers that Sloane’s sister Adele also brought a friend home - none other than her ex, Brighton. Nothing can melt the ice in their hearts, though... right?
Love You a Latke by Amanda Elliot
Snow is falling, holiday lights are twinkling, and Abby Cohen is pissed. For one thing, her most annoying customer, Seth, has been coming into her café every morning with his sunshiny attitude, determined to break down her emotional walls. And, as the only Jew on the tourism board of her Vermont town, Abby's been charged with planning their Hanukkah festival. Desperate for support, Abby puts out a call for help and discovers she was wrong about being the only Jew in town...so is Seth. Over latkes, doughnuts, and winter adventures, Abby begins to realize that Seth might just be igniting a flame in her own guarded heart.
Christmas Eve Love Story by Ginny Baird
Annie Jones works hard designing windows for iconic New York City department store Lawson's Finest. So when her Christmas window display gets upended by some rambunctious kids on Christmas Eve, the all-too-realistic store Santa gives Annie a little decorating tip on how to start over. With help from friendly security guard Braden Tate, Annie repairs the damage and heads home. But when she wakes the next morning, she's bewildered to find that it's Christmas Eve all over again. As little everyday choices bring her closer to Braden and to Christmas Day, Annie starts to picture what her new life could look like.
The Merry Matchmaker by Sheila Roberts
Frankie Lane knows what’s best for just about everyone but herself. From her divorced sister to her shy employee, her daughter to her best friend, Frankie knows she could help all of them, if they’d just let her - and if all of her help didn’t end in utter disaster. Then there’s Mitch Howard, the owner of the local hardware store. He got her through the nightmare of losing her husband. He’s kindhearted, been divorced for years, and is the fittest, finest man Frankie knows. Mitch needs someone. And Frankie is determined to help him find that someone - whether he likes it or not.
#holiday romance#cozy reads#romance#fiction#reading recommendations#reading recs#book recommendations#book recs#library books#tbr#tbr list#to read#booklr#book tumblr#book blog#library blog#readers advisory
3 notes
·
View notes
Text
WASHINGTON (Reuters) - President Joe Biden supports a study on whether descendants of enslaved people in the United States should receive reparations, White House spokeswoman Jen Psaki said on Wednesday, as the issue was being debated on Capitol Hill.
Psaki told reporters that Biden “continues to demonstrate his commitment to take comprehensive action to address the systemic racism that persists today.”
Reparations have been used in other circumstances to offset large moral and economic debts - paid to Japanese Americans interned during World War Two, to families of Holocaust survivors and to Blacks in post-apartheid South Africa.
But the United States has never made much headway in discussions of whether or how to compensate African Americans for more than 200 years of slavery and help make up for racial inequality.
HR-40, a bill to fund the study of “slavery and discrimination in the colonies and the United States from 1619 to the present and recommend appropriate remedies” has been floated in Congress for more than 30 years, but never taken up for a full vote.
Democratic Representative Sheila Jackson Lee reintroduced it in January.
Fellow Democratic Representative Steve Cohen, who chairs the House Subcommittee on the Constitution, Civil Rights and Civil Liberties, told a hearing on Wednesday it was fitting to consider HR-40 at a time when the country is reckoning with police violence against Blacks and a pandemic that has disproportionately affected African Americans.
Biden told the Washington Post last year that “we must acknowledge that there can be no realization of the American dream without grappling with the original sin of slavery, and the centuries-long campaign of violence, fear, and trauma wrought upon Black people in this country.”
But like nearly all of the Democratic presidential candidates at the time, he did not embrace the idea of specific payments to enslaved people’s descendants, instead promising “major actions to address systemic racism” and further study.
A Reuters/Ipsos poll conducted last June following the death in police custody in Minneapolis of George Floyd, an African-American man, found clear divisions along partisan and racial lines, with only one in 10 white respondents supporting the idea and half of Black respondents endorsing it.
Calls have been growing from some politicians, academics and economists for such payments to be made to an estimated 40 million African Americans. Any federal reparations program could cost trillions of dollars, they estimate.
Supporters say such payments would act as acknowledgement of the value of the forced, unpaid labor that supported the economy of Southern U.S. states until the Civil War ended slavery in 1865, the broken promise of land grants after the war and the burden of the century and a half of legal and de facto segregation that followed.
#White House says Biden supports study of slavery reparations#biden#Reparations#Reparations Study#Freedmen#Black Freedmen#Reparations NOW
6 notes
·
View notes
Text
books i've read this year (2023)
reading goal: 30 books
total read so far: 29 (last updated: 10/31/23)
MARCH 2023
1. And I Do Not Forgive You by Amber Sparks
APRIL 2023
2. Nine Liars by Maureen Johnson 3. Vladimir by Julia May Jonas 4. Convenience Store Woman by Sayaka Murata 5. Local Woman Missing by Mary Kubica
MAY 2023
6. Brutes by Dizz Tate 7. Pretty Girls by Karen Slaughter
JUNE 2023
8. The Drowning Kind by Jennifer McMahon 9. Blackmail and Bibingka by Mia P. Manansala 10. Natural Beauty by Ling Ling Huang
JULY 2023
11. All’s Well by Mona Awad 12. Dykette by Jenny Fran Davis 13. A Touch of Jen by Beth Morgan 14. The Grownup by Gillian Flynn 15. The Guest by Emma Cline 16. Sarahland by Sam Cohen
AUGUST 2023
17. Monstrilio by Gerardo Sámano Córdova 18. Pure Colour by Sheila Heti 19. Ripe by Sarah Rose Etter 20. Nightbitch by Rachel Yoder 21. All-Night Pharmacy by Ruth Madievsky
SEPTEMBER 2023
22. The Writing Retreat by Julia Bartz 23. My Husband by Maud Ventura 24. I Hold a Wolf by the Ears: Stories by Laura van den Berg 25. I Who Have Never Known Men by Jacqueline Harpman
OCTOBER 2023
26. The Centre by Ayesha Manazir Siddiqi 27. Slewfoot by Brom 28. Tender is the Flesh by Agustina Bazterrica 29. Carmilla by J. Sheridan Le Fanu
6 notes
·
View notes
Text
Supporters of #NoHostageLeftBehind Open Letter to Joe Biden - Part 2/2
Gabe Turner
Gail Berman
Gary Barber
Genevieve Angelson
Gideon Raff
Grant Singer
Greg Berlanti
Guy Nattiv
Hannah Fidell
Hannah Graf
Harlan Coben
Harold Brown
Henrietta Conrad
Howard Gordon
Iain Morris
Imran Ahmed
Inbar Lavi
Jackie Sandler
Jake Graf
Jake Kasdan
Jamie Ray Newman
Jaron Varsano
Jason Fuchs
Jason Biggs & Jenny Mollen Biggs
Jason Segel
JD Lifshitz
Jeff Rake
Jen Joel
Jeremy Piven
Jesse Itzler
Jesse Sisgold
Jill Littman
Jody Gerson
Joe Hipps
Joe Quinn
Joe Russo
Joe Tippett
Joel Fields
John Landgraf
Jon Bernthal
Jon Glickman
Jon Liebman
Jonathan Baruch
Jonathan Groff
Jonathan Tropper
Jonathan Marc Sherman
Jonathan Steinberg
Jonathan Tisch
Josh Goldstine
Josh Greenstein
Josh Grode
Julia Lester
Julie Greenwald
Karen Pollock
Kelley Lynch
Kevin Kane
Kevin Zegers
Kitao Sakurai
KJ Steinberg
Laura Pradelska
Lauren Schuker Blum
Laurence Mark
Laurie David
Lee Eisenberg
Leslie Siebert
Leo Pearlman
Limor Gott
Lina Esco
Liz Garbus
Lizanne Rosenstein
Lizzie Tisch
Lorraine Schwartz
Lynn Harris
Lyor Cohen
Mandana Dayani
Maria Dizzia
Mara Buxbaum
Marc Webb
Marco Perego
Mark Feuerstein
Mark Shedletsky
Mark Scheinberg
Mathew Rosengart
Matt Lucas
Matt Miller
Matthew Bronfman
Matthew Hiltzik
Matti Leshem
Dame Maureen Lipman
Max Mutchnik
Maya Lasry
Meaghan Oppenheimer
Melissa Zukerman
Michael Ellenberg
Michael Aloni
Michael Green
Michael Rapino
Michael Weber
Mike Medavoy
Mimi Leder
Modi Wiczyk
Nancy Josephson
Natasha Leggero
Neil Blair
Neil Druckmann
Nicole Avant
Nina Jacobson
Noa Kirel
Noah Oppenheim
Noreena Hertz
Odeya Rush
Oran Zegman
Pasha Kovalev
Paul Haas
Paul Pflug
Peter Traugott
Rachel Riley
Rafi Marmor
Ram Bergman
Raphael Margulies
Rebecca Angelo
Rebecca Mall
Reinaldo Marcus Green
Rich Statter
Richard Kind
Rick Hoffman
Rick Rosen
Robert Newman
Rob Rinder
Roger Birnbaum
Roger Green
Rosie O'Donnell
Ryan Feldman
Sam Trammell
Sarah Baker
Sarah Bremner
Sarah Treem
Scott Tenley
Seth Oster
Scott Braun
Scott Neustadter
Shannon Watts
Shari Redstone
Sharon Jackson
Shauna Perlman
Shawn Levy
Sheila Nevins
Simon Sebag Montefiore
Simon Tikhman
Skylar Astin
Stacey Snider
Stephen Fry
Steve Agee
Steve Rifkind
Susanna Felleman
Susie Arons
Todd Lieberman
Todd Moscowitz
Todd Waldman
Tom Freston
Tom Werner
Tomer Capone
Tracy Ann Oberman
Trudie Styler
Tyler James Williams
Vanessa Bayer
Veronica Grazer
Veronica Smiley
Whitney Wolfe Herd
Will Graham
Yamanieka Saunders
Yariv Milchan
Ynon Kreiz
5 notes
·
View notes
Text
my record collection 2023 :)
Vinyl
Scary Monsters & Super Creeps - David Bowie The Dreaming - Kate Bush Never For Ever - Kate Bush The Songs of Leonard Cohen - Leonard Cohen Wind on the Water - Crosby & Nash Crosby, Stills & Nash - CSN Songs of the Sea - Pete Dawson Ultraviolence - Lana del Rey Lust for Life - Lana del Rey Norman Fucking Rockwell - Lana del Rey Romance in 1600 - Sheila E. Liege & Lief - Fairport Convention Tusk - Fleetwood Mac Close up the Honky-Tonks - The Flying Burrito Bros Transangelic Exodus - Ezra Furman A Trick of the Tail - Genesis Godspell (original cast recording) Dookie - Green Day Hair (original cast recording) Live Through This - Hole Celebrity Skin - Hole Living In the Past - Jethro Tull Jesus Christ Superstar (1973 motion picture soundtrack) Greatest Hits (1974) - Elton John Joanne - Lady Gaga Court & Spark - Joni Mitchell On The Threshold Of A Dream - The Moody Blues The Black Parade/Living with Ghosts - My Chemical Romance Bella Donna - Stevie Nicks Songs for our Times - John O'Connor GP - Gram Parsons Raising Sand - Robert Plant & Alison Krauss Queen - Queen Queen II - Queen Sheer Heart Attack - Queen A Night at the Opera - Queen A Day at the Races - Queen News of the World - Queen Jazz - Queen The Works - Queen Live at the Rainbow 1973 - Queen New Again - Taking Back Sunday Man on Fire - Roger Taylor Goats Head Soup - The Rolling Stones Through the Past, Darkly - The Rolling Stones Metamorphosis - The Rolling Stones Get Yer Ya-Yas Out! - The Rolling Stones Linda Rondstadt - Linda Rondstadt It’s My Way! - Buffy Sainte-Marie Parsley, Sage, Rosemary & Thyme - Simon & Garfunkel The Sound of Music (motion picture soundtrack) Nebraska - Bruce Springsteen The River - Bruce Springsteen Below the Salt - Steeleye Span Stephen Stills - Stephen Stills Under Soil & Dirt - The Story So Far Grave New World - Strawbs Crime of the Century - Supertramp GLA - Twin Atlantic Hesitant Alien - Gerard Way Blunderbuss - Jack White _
CD
Almost Famous (motion picture soundtrack) Little Earthquakes - Tori Amos Odelay - Beck Daisy - Brand New Grace - Jeff Buckley Hounds of Love - Kate Bush Let Love In - Nick Cave & the Bad Seeds Push The Sky Away - Nick Cave & the Bad Seeds Everybody Else Is Doing It… - The Cranberries Blue Bannisters - Lana del Rey Flowers of Flesh & Blood - Nicole Dollanganger Observatory Mansions - Nicole Dollanganger Ode to Dawn Weiner - Nicole Dollanganger I Told You I Was Freaky - Flight of the Conchords Ceremonials - Florence + the Machine High As Hope - Florence + the Machine Born This Way - Lady Gaga Wolfways - Michael Hurley A Creature I Don’t Know - Laura Marling The Mask & Mirror - Loreena McKennitt Elemental - Loreena McKennitt The Book Of Secrets - Loreena McKennitt The Visit - Loreena McKennitt Blue - Joni Mitchell Clouds - Joni Mitchell Jagged Little Pill - Alanis Morissette Three Cheers For Sweet Revenge - My Chemical Romance Danger Days - My Chemical Romance GP/Grievous Angel - Gram Parsons Trio - Dolly Parton, Linda Ronstadt & Emmylou Harris Meds - Placebo Band of Joy - Robert Plant The Bends - Radiohead OK Computer - Radiohead The King of Limbs - Radiohead Transformer - Lou Reed Darkness on the Edge of Town - Bruce Springsteen The Promise - Bruce Springsteen Western Stars - Bruce Springsteen Carrie & Lowell - Sufjan Stevens Suede - Suede Dog Man Star - Suede Dead & Born & Grown - The Staves Velvet Goldmine (motion picture soundtrack) Want Two - Rufus Wainwright Harvest - Neil Young
12 notes
·
View notes
Text
📺 8 SHOWS TO GET TO KNOW ME
(thanks for tagging me, @savebytheodoresnonjosestuff 💐)
In alphabetical order:
1. The 10th Kingdom (2000)
Fantasy / Dramedy | 1 Season
Kimberley Williams-Paisley | John Larroquette | Scott Cohen | Dianne Wiest
Virginia Lewis and her father, Tony, get trapped in a fairytale dimension. They must travel across the 9 kingdoms, avoiding trolls, wicked witches, and the huntsman, to find the magic mirror that can take them home.
Favourite Episode: n/a (my DVD has it as one long film)
Favourite Character: Wolf

2. Being Erica (2009 - 2011)
Dramedy / Time Travel | 4 Seasons
Erin Karpluk | Michael Riley | Reagan Pasternak
After a near-death experience, Erica Strange meets the mysterious Dr. Tom, a therapist with the ability to send his patients back to relive and ‘correct’ their deepest regrets.
Favourite Episode: 3x12 Erica, Interrupted
Favourite Character: Dr. Tom
3. Justified (2010 - 2015) (2023)
Neo-Western / Crime / Drama | 6 Seasons + City Primeval
Timothy Olyphant | Walton Goggins | Joelle Carter
Enforcing his own brand of justice, Deputy US Marshal Raylan Givens is reassigned from Miami to his childhood home in the rural coal mining towns of eastern Kentucky.
Favourite Episode: 2x01 The Moonshine War
Favourite Character: Raylan Givens
4. Merlin (2008 - 2012)
Fantasy / Drama | 5 Seasons
Colin Morgan | Bradley James | Katie McGrath | Richard Wilson
A young warlock named Merlin has come to Camelot, where those who study magic are killed under the King’s command, to fulfil his destiny of protecting the future King, Arthur Pendragon.
Favourite Episode: 3x03 Goblin’s Gold
Favourite Character: Gaius

5. One Foot in the Grave (1990 - 2000)
Comedy / Sitcom | 6 Seasons
Richard Wilson | Annette Crosbie | Doreen Mantle
When Victor Meldrew is forced into early retirement, he has a lot more time on his hands to observe the world around him, and he finds it insufferable.
Favourite Episode: 4x05 The Trial
Favourite Character: Victor Meldrew

6. Sabrina the Teenage Witch (1996 - 2003)
Fantasy / Teen Sitcom | 7 Seasons + 2 Films
Melissa Joan Hart | Caroline Rhea | Beth Broderick
When Sabrina Spellman turns 16, she discovers that she is a witch, and she must now learn how to control her powers.
Favourite Episode: 2x18 The Band Episode
Favourite Character: Salem Saberhagen

7. Santa Clarita Diet (2017 - 2019)
Comedy / ZomCom | (criminally only) 3 Seasons
Timothy Olyphant | Drew Barrymore | Liv Hewson | Skyler Gisondo
Real-a-tor couple Joel & Sheila Hammond lived a perfectly normal quiet life in Santa Clarita with their teenage daughter Abby. Until one day Sheila suddenly died and came back to life. Now, her new diet is putting a tremendous strain on the family.
Favourite Episode: 1x07 Strange or Just Inconsiderate?
Favourite Character: Joel Hammond

8. Stranger Things (2016 - 2024)
Horror / Supernatural / Drama | 5 Seasons (4 Released)
Winona Ryder | Millie Bobby Brown | et al.
The vanishing of schoolboy Will Byers leads his group of friends to uncover a terrifying secret about their hometown.
Favourite Episode: 4x04 Chapter Four: Dear Billy
Favourite Character: Steve Harrington

This was fun! I know everyone else was just doing a list, but I’m nothing if not over-the-top 🙈
Tagging: literally anyone who reads this & wants to do it 🫶🏻
3 notes
·
View notes
Text
tagged by @thesunsethour to list my top 10 songs with a name in them. took me a while lol (mainly bc i also had to maintain my mysterious vibe)
Alrighty Aphrodite - Peach Pit
Sheila Take a Bow - The Smiths (was also going to do William, It Was Really Nothing, but I thought that would be too easy)
Saint Bernard - Lincoln
Ana Ng - They Might Be Giants
Madame George - Van Morrison
Isombard - Declan McKenna
Enola Gay - Orchestral Manoeuvres in the Dark
John, I’m Only Dancing - David Bowie
Cassandra - ABBA
So Long, Marianne - Leonard Cohen (i was going to do Chelsea Hotel #2 instead bc i love that song but I felt bad bc that’s not referring to a first name)
tbh idrk who to tag so I’m not going to tag anyone lol
1 note
·
View note
Text
🇺🇸THESE ARE THE 158 DEMOCRATS WHO VOTED AGAINST DEPORTING SEX OFFENDERS
Alabama:
-Terri Sewell
California:
-Pete Aguilar
-Ami Bera
-Julia Brownley
-Salud Carbajal
-Tony Cárdenas
-Judy Chu
-Jim Costa
-Mark DeSaulnier
-John Garamendi
-Robert Garcia
-Sylvia Garcia
-Jimmy Gomez
-Jared Huffman
-Ro Khanna
-Sydney Kamlager-Dove
-Barbara Lee
-Ted Lieu
-Zoe Lofgren
-Doris Matsui
-Kevin Mullin
-Grace Napolitano
-Nancy Pelosi
-Katie Porter
-Linda Sánchez
-Adam Schiff
-Brad Sherman
-Norma Torres
-Mike Thompson
-Maxine Waters
Colorado:
-Jason Crow
-Diana DeGette
-Brittany Pettersen
-Joe Neguse
Connecticut:
-Rosa DeLauro
-John Larson
-James Himes
Delaware:
-Lisa Blunt Rochester
Florida:
-Kathy Castor
-Sheila Cherfilus-McCormick
-Lois Frankel
-Maxwell Frost
-Darren Soto
-Frederica Wilson
-Debbie Wasserman Schultz
Georgia:
-Sanford D. Bishop Jr.
-Lucy McBath
-Henry “Hank” Johnson
-Nikema Williams
-David Scott
Hawaii:
-Ed Case
-Jill Tokuda
Illinois:
-Sean Casten
-Danny Davis
-Jesús “Chuy” Garcia
-Jonathan Jackson
-Raja Krishnamoorthi
-Robin Kelly
-Delia Ramirez
-Janice Schakowsky
-Mike Quigley
-Bill Foster
-Brad Schneider
-Lauren Underwood
Indiana:
-André Carson
Kentucky:
-Morgan McGarvey
Louisiana:
-Troy Carter
Maine:
-Chellie Pingree
Maryland:
-Steny Hoyer
-Glenn Ivey
-Kweisi Mfume
-Jamie Raskin
C.A. Dutch Ruppersberger
-John Sarbanes
-David Trone
Massachusetts:
-Jake Auchincloss
-Katherine Clark
-Bill Keating
-Seth Moulton
-Ayanna Pressley
-Richard Neal
-Lori Trahan
-James McGovern
Michigan:
-Dan Kildee
-Debbie Dingell
-Rashida Tlaib
-Shri Thanedar
-Haley Stevens
Minnesota:
-Betty McCollum
-Ilhan Omar
-Dean Phillips
Mississippi:
-Bennie Thompson
Missouri:
-Cori Bush
-Emanuel Cleaver
New Hampshire:
-Ann Kuster
New Jersey:
-Andy Kim
-Rob Menendez
-Donald Norcross
-Bonnie Watson Coleman
-Frank Pallone
New Mexico:
-Melanie Stansbury
-Teresa Leger Fernandez
New York:
-Jamaal Bowman
-Adriano Espaillat
-Hakeem Jeffries
-Yvette Clarke
-Gregory Meeks
-Alexandria Ocasio-Cortez
-Jerrold Nadler
-Nydia Velázquez
-Paul Tonko
-Dan Goldman
-Ritchie Torres
-Grace Meng
-Joseph Morelle
North Carolina:
-Alma Adams
-Valerie Foushee
-Deborah Ross
Ohio:
-Shontel Brown
-Joyce Beatty
-Greg Landsman
Oregon:
-Earl Blumenauer
-Suzanne Bonamici
-Valerie Hoyle
Pennsylvania:
-Madeleine Dean
-Mary Scanlon
-Summer Lee
Rhode Island:
-Gabe Amo
South Carolina:
-James Clyburn
Tennessee:
-Steve Cohen
Texas:
-Greg Casar
-Veronica Escobar
-Joaquin Castro
-Sylvia Garcia
-Lloyd Doggett
-Lizzie Fletcher
-Al Green
-Jasmine Crockett
-Marc Veasey
Vermont:
-Becca Balint
Virginia:
-Donald Beyer
-Gerald Connolly
-Jennifer McClellan
-Bobby Scott
Washington:
-Suzan DelBene
-Derek Kilmer
-Rick Larsen
-Marilyn Strickland
-Pramila Jayapal
Wisconsin:
-Gwen Moore
-Mark Pocan
Source: Newsweek
0 notes
Text
@elonmusk
These awful people all need to be voted out, either in the primaries or the general election. They sully the Capitol Building with their presence.
THESE ARE THE 158 DEMOCRATS WHO VOTED AGAINST DEPORTING SEX OFFENDERS Alabama: -Terri Sewell California: -Pete Aguilar -Ami Bera -Julia Brownley -Salud Carbajal -Tony Cárdenas -Judy Chu -Jim Costa -Mark DeSaulnier -John Garamendi -Robert Garcia -Sylvia Garcia -Jimmy Gomez -Jared Huffman -Ro Khanna -Sydney Kamlager-Dove -Barbara Lee -Ted Lieu -Zoe Lofgren -Doris Matsui -Kevin Mullin -Grace Napolitano -Nancy Pelosi -Katie Porter -Linda Sánchez -Adam Schiff -Brad Sherman -Norma Torres -Mike Thompson -Maxine Waters Colorado: -Jason Crow -Diana DeGette -Brittany Pettersen -Joe Neguse Connecticut: -Rosa DeLauro -John Larson -James Himes Delaware: -Lisa Blunt Rochester Florida: -Kathy Castor -Sheila Cherfilus-McCormick -Lois Frankel -Maxwell Frost -Darren Soto -Frederica Wilson -Debbie Wasserman Schultz Georgia: -Sanford D. Bishop Jr. -Lucy McBath -Henry “Hank” Johnson -Nikema Williams -David Scott Hawaii: -Ed Case -Jill Tokuda Illinois: -Sean Casten -Danny Davis -Jesús “Chuy” Garcia -Jonathan Jackson -Raja Krishnamoorthi -Robin Kelly -Delia Ramirez -Janice Schakowsky -Mike Quigley -Bill Foster -Brad Schneider -Lauren Underwood Indiana: -André Carson Kentucky: -Morgan McGarvey Louisiana: -Troy Carter Maine: -Chellie Pingree Maryland: -Steny Hoyer -Glenn Ivey -Kweisi Mfume -Jamie Raskin C.A. Dutch Ruppersberger -John Sarbanes -David Trone Massachusetts: -Jake Auchincloss -Katherine Clark -Bill Keating -Seth Moulton -Ayanna Pressley -Richard Neal -Lori Trahan -James McGovern Michigan: -Dan Kildee -Debbie Dingell -Rashida Tlaib -Shri Thanedar -Haley Stevens Minnesota: -Betty McCollum -Ilhan Omar -Dean Phillips Mississippi: -Bennie Thompson Missouri: -Cori Bush -Emanuel Cleaver New Hampshire: -Ann Kuster New Jersey: -Andy Kim -Rob Menendez -Donald Norcross -Bonnie Watson Coleman -Frank Pallone New Mexico: -Melanie Stansbury -Teresa Leger Fernandez New York: -Jamaal Bowman -Adriano Espaillat -Hakeem Jeffries -Yvette Clarke -Gregory Meeks -Alexandria Ocasio-Cortez -Jerrold Nadler -Nydia Velázquez -Paul Tonko -Dan Goldman -Ritchie Torres -Grace Meng -Joseph Morelle North Carolina: -Alma Adams -Valerie Foushee -Deborah Ross Ohio: -Shontel Brown -Joyce Beatty -Greg Landsman Oregon: -Earl Blumenauer -Suzanne Bonamici -Valerie Hoyle Pennsylvania: -Madeleine Dean -Mary Scanlon -Summer Lee Rhode Island: -Gabe Amo South Carolina: -James Clyburn Tennessee: -Steve Cohen Texas: -Greg Casar -Veronica Escobar -Joaquin Castro -Sylvia Garcia -Lloyd Doggett -Lizzie Fletcher -Al Green -Jasmine Crockett -Marc Veasey Vermont: -Becca Balint Virginia: -Donald Beyer -Gerald Connolly -Jennifer McClellan -Bobby Scott Washington: -Suzan DelBene -Derek Kilmer -Rick Larsen -Marilyn Strickland -Pramila Jayapal Wisconsin: -Gwen Moore -Mark Pocan Source: Newsweek




20 notes
·
View notes
Text
Muses

Canon Muses

name: Barry age: 24-28 sexuality: bi occupation: pawn shop owner, mechanic, drug dealer, and every other shit job on the Outer Banks tribe: kook associate face claim: Nicholas Cirillo
name: JJ Maybank age: 18-24 sexuality: (closeted) gay (very selective romantic shipping) occupation: will take any shitty job to scrape by, mild kleptomaniac tribe: pogue 4 life face claim: Rudy Pankow

name: Rafe Cameron age: 19-26 sexuality: verse dependent (selective with new romantic ships) occupation: son and psychopath tribe: kook king face claim: Drew Starkey
name: Louisa “Wheezie” Cameron age: 18-22 occupation: the least favorite daughter, student with a new major every other week, tiktok influencer in the making tribe: kook face claim: Victoria Justice
Canon Muses from Other Media & Original Characters

name: Trevor Anderson originally from: Hellraiser (2020) age: 21-28 sexuality: no label background: eldest son of Ward Cameron and his late wife, grew up in Boston with the man he until recently believed to be his father, on the island to claim what rightfully belongs to him occupation: not disclosed tribe: kook by birthright face claim: Drew Starkey
name: Peter Rumancek originally from: Hemlock Grove age: 19-24 sexuality: pan background: Romani, ends up on the island by chance, human in this verse occupation: thief and con artist, occasionally taking low paid jobs tribe: free spirit, pogue associate face claim: Aaron Taylor-Johnson

name: Daniel Carter original character age: 36-40 sexuality: straight background: comes to the island when he learns that he has a daughter from his high school sweetheart character: caring and calm occupation: former college professor for ancient societies, now high school history teacher tribe: new kook face claim: Joshua Jackson
name: Autumn Winter original character age: 18-22 sexuality: demi background: moved to the island with her mother (Sheila Winter, fc. Katie Holmes) when she was a toddler, grew up in a hippie community, now lives on Figure Eight with her father (Daniel Carter) character: ambitious and aloof occupation: waitress and writer tribe: pogue turned kook face claim: Emilia Jones

name: Lincoln Alexander original character age: 30-35 sexuality: bi background: made a fortune in finance, building a luxury resort on the island, potential links to drug trade character: powerful and passionate occupation: investor tribe: kook face claim: Oliver Jackson-Cohen
name: Gunner originally from: Bates Motel age: 20-26 sexuality: pan background: kicked out by his stepfather the day he turned 18, just trying to chill character: kind and kinda pathetic occupation: whatever pays the rent tribe: pogue face claim: Keenan Tracey

name: Luciana Aguilar original character age: 24-32 sexuality: bi background: older sister of Killian, aware of her privileged background she wants to use her influence to make a difference character: willful and wary occupation: law student/lawyer tribe: kook face claim: Eiza González
name: Killian Aguilar original character age: 18-24 sexuality: straight (he says) background: youngest Underwood, an overprivileged kook with some secrets character: arrogant and assertive occupation: business student tribe: kook face claim: Gabriel Guevara

name: Natalie Scartoccio originally from: Yellowjackets age: 18-23 sexuality: pan background: just another trailer park girl occupation: shop assistant, waitress, babysitter tribe: pogue face claim: Sophie Thatcher
Please note: All my muses are works in progress.
Outer Banks verse only on this blog
5 notes
·
View notes