#Oncology journals
Text
Economic Loss from U.S. Cigarette Smoking Topped Almost $900 Billion in 2020, New Study Shows
Economic Loss from U.S. Cigarette Smoking Topped Almost $900 Billion in 2020, New Study Shows
EMBARGOED FOR RELEASE – 6:30 p.m., EDT – September 28, 2022
Newswise — ATLANTA, September 28, 2022 — New findings by the American Cancer Society (ACS) found cumulative economic losses from cigarette smoking topped $891 billion in 2020, or 4.3% of the United States Gross Domestic Product. The economic loss significantly outpaced the cigarette industry’s $92 billion revenue by nearly a ten-to-one…
View On WordPress
#All Journal News#American Cancer Society (ACS)#Cancer#Dr. Nigar Nargis;American Cancer Society;ACS;Cancer;Tobacco;Oncology;Smoking;Smoking Cessation#Economics#Embargoed Feed - hidden#Government/Law#Newswise#Smoking
0 notes
Text
COVID-19's long-term effects on the body: an incomplete list
COVID’s effect on the immune system, specifically on lymphocytes:
NYT article from 2020 (Studies cited: https://www.biorxiv.org/content/10.1101/2020.05.18.101717v1, https://www.biorxiv.org/content/10.1101/2020.05.20.106401v1, https://www.unboundmedicine.com/medline/citation/32405080/Decreased_T_cell_populations_contribute_to_the_increased_severity_of_COVID_19_, https://www.medrxiv.org/content/10.1101/2020.06.08.20125112v1)
https://www.biorxiv.org/content/10.1101/2022.01.10.475725v1
https://www.science.org/doi/10.1126/science.abc8511 (Published in Science)
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9057012/
https://www.forbes.com/sites/williamhaseltine/2022/04/14/sars-cov-2-actively-infects-and-kills-lymphoid-cells/
https://www.cleveland.com/news/2022/10/in-cleveland-and-beyond-researchers-begin-to-unravel-the-mystery-of-long-covid-19.html
SARS-CoV-2 infection weakens immune-cell response to vaccination: NIH-funded study suggests need to boost CD8+ T cell response after infection
https://www.merckmanuals.com/professional/hematology-and-oncology/leukopenias/lymphocytopenia
https://thetyee.ca/Analysis/2022/11/07/COVID-Reinfections-And-Immunity/
Dendritic cell deficiencies persist seven months after SARS-CoV-2 infection
https://www.frontiersin.org/articles/10.3389/fimmu.2022.1034159/full
https://www.n-tv.de/politik/Lauterbach-warnt-vor-unheilbarer-Immunschwaeche-durch-Corona-article23860527.html (German Minister of Health)
Anecdotal evidence of COVID’s effects on white blood cells:
https://twitter.com/DrJohnHhess/status/1661837956875956224
https://x.com/TristanVeness/status/1661565201345564673
https://twitter.com/TristanVeness/status/1689996298408312832
Much more if you speak to Long Covid patients directly!
Related information of interest:
China approves Genuine Biotech's HIV drug for COVID patients
COVID as a “mass disabling event” and impact on the economy:
https://www.ctvnews.ca/health/report-says-long-covid-could-impact-economy-and-be-mass-disabling-event-in-canada-1.6306608
https://x.com/inkblue01/status/1742183209809453456?s=20
COVID’s impact on the heart:
https://www.dailystar.co.uk/news/world-news/deadly-virus-could-lead-heart-31751263 (Research from: Japan's Riken research institute)
https://www.brisbanetimes.com.au/national/queensland/unlike-flu-covid-19-attacks-dna-in-the-heart-new-research-20220929-p5bm10.html
https://www.mdpi.com/2077-0383/12/1/186
https://medicalxpress.com/news/2023-04-mild-covid-effects-cardiovascular-health.html
https://publichealth.jhu.edu/2022/covid-and-the-heart-it-spares-no-one
https://www.bhf.org.uk/informationsupport/heart-matters-magazine/news/coronavirus-and-your-health/is-coronavirus-a-disease-of-the-blood-vessels (British Heart Foundation)
COVID’s effect on the brain and cognitive function:
https://www.openaccessgovernment.org/article/brain-infection-by-sars-cov-2-lifelong-consequences/171391/
https://www.cidrap.umn.edu/covid-19/study-shows-covid-leaves-brain-injury-markers-blood
https://www.theguardian.com/world/2020/jul/08/warning-of-serious-brain-disorders-in-people-with-mild-covid-symptoms
Cognitive post-acute sequelae of SARS-CoV-2 (PASC) can occur after mild COVID-19
Neurologic Effects of SARS-CoV-2 Transmitted among Dogs
https://journals.lww.com/nsan/fulltext/2022/39030/neurological_manifestations_and_mortality_in.4.aspx
https://www.salon.com/2023/06/17/new-evidence-suggests-alters-the-brain--but-the-extent-of-changes-is-unclear/
https://www.scientificamerican.com/article/covid-virus-may-tunnel-through-nanotubes-from-nose-to-brain/
https://neurosciencenews.com/post-covid-brain-21904/
https://www.thelancet.com/journals/lanpsy/article/PIIS2215-0366(22)00260-7/fulltext
https://medicalxpress.com/news/2022-08-covid-infection-crucial-brain-regions.html
https://news.ecu.edu/2022/08/04/covid-parkinsons-link/
Covid as a vascular/blood vessel disease:
https://www.salon.com/2020/06/01/coronavirus-is-a-blood-vessel-disease-study-says-and-its-mysteries-finally-make-sense/
https://www.salon.com/2023/12/27/brain-damage-caused-by-19-may-not-show-up-on-routine-tests-study-finds/
https://www.nih.gov/news-events/news-releases/sars-cov-2-infects-coronary-arteries-increases-plaque-inflammation
https://www.mdpi.com/2077-0383/12/6/2123
https://www.sciencedaily.com/releases/2021/10/211004104134.htm (microclots)
Long Covid:
Post-COVID-19 Condition in Canada: What we know, what we don’t know, and a framework for action
https://www.ctvnews.ca/health/coronavirus/more-than-two-years-of-long-covid-research-hasn-t-yielded-many-answers-scientific-review-1.6235227
https://www.cbc.ca/news/canada/london/cause-of-long-covid-symptoms-revealed-by-lung-imaging-research-at-western-university-1.6504318
https://www.cbc.ca/news/canada/montreal/long-covid-study-montreal-1.6521131
https://news.yale.edu/2023/12/19/study-helps-explain-post-covid-exercise-intolerance
Other:
- Viruses and mutation: https://typingmonkeys.substack.com/p/monkeys-on-typewriters
Measures taken by the rich and world leaders
Heightened risk of diabetes
https://jamanetwork.com/journals/jama/fullarticle/2805461
https://www.nature.com/articles/d41586-022-00912-y
Liver damage:
https://timesofindia.indiatimes.com/city/mumbai/46-of-covid-patients-have-liver-damage-study/articleshow/97809200.cms?from=mdr
tl;dr: covid is a vascular disease, not a respiratory illness. it can affect your blood and every organ in your body. every time you're reinfected, your chances of getting long covid increase.
avoid being infected. reduce the amount of viral load you're exposed to.
the gap between what the scientific community knows and ordinary people know is massive. collective action is needed.
#putting this somewhere at least as reference for... somebody hopefully#covid#disability#y'all. it is bleak out there but some very good people are doing their best to help#we need as many people aware and helping as possible
464 notes
·
View notes
Photo

Over seven million women suffer from breast cancer, making it one of the deadliest cancers across the globe.
A team of researchers at the University of Washington School of Medicine (UWSM) has been working on a breast cancer vaccine for over the last 20 years. In their recently published study, they finally revealed the results of the phase one human trials of their breast cancer vaccine.
The study is published in the journal JAMA Oncology. During the phase one trials, the experimental breast cancer vaccine has proved to be safe and highly effective in preventing the growth of human epidermal growth receptor 2 (HER2) cancer tumor cells. High levels of HER2 protein in the body are responsible for causing the most complex, aggressive, and rapidly spreading type of breast cancer in women. Therefore, the new vaccine might turn out to be a groundbreaking discovery in the field of modern medicine.
The researchers are now conducting phase two trials of their vaccine. If successful, it’d be one of the greatest miracles of medical science – fingers crossed! Source: Interesting Engineering (link in bio) #science #cancer #innovation https://www.instagram.com/p/CnCQgiVO_xi/?igshid=NGJjMDIxMWI=
1K notes
·
View notes
Text
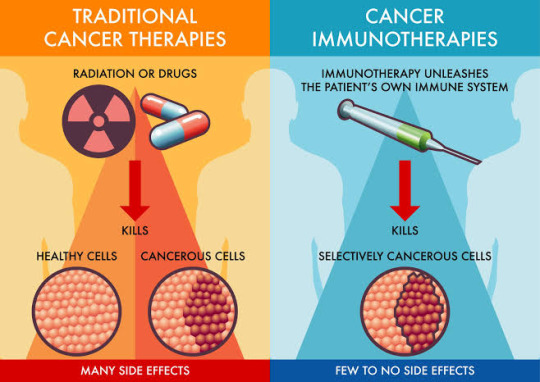
The Power of Immunotherapy: A Deep Dive into Cancer Treatment
Immunotherapy, a groundbreaking approach in cancer treatment, has been making waves in the medical world. 🌟 But what exactly is it, and how does it work? Let's delve into the intricacies of this cutting-edge therapy. 💉
Immunotherapy at a Glance: 🔬 Immunotherapy, or immuno-oncology, is a therapeutic strategy that harnesses the body's immune system to combat cancer cells. Unlike traditional treatments like chemotherapy, which target both healthy and cancerous cells, immunotherapy is highly targeted, making it a game-changer in the fight against cancer.
Key Players in Immunotherapy: 🦠
Tumor Antigens are molecules found on cancer cells that act as red flags, signaling the immune system to attack. 👥
T Cells: The immune system's soldiers. They are trained to recognize and destroy threats, including cancer cells.
💡 Checkpoint Inhibitors: Proteins that, when blocked, enhance the immune response against cancer. 🧬
CAR-T Cell Therapy: Genetic engineering to supercharge T cells for precision attacks on tumors.
How Does Immunotherapy Work? Immunotherapy comes in various forms, but they all aim to accomplish one goal: boost the immune system's ability to recognize and eradicate cancer cells. Whether through checkpoint inhibitors, vaccines, or CAR-T cell therapy, the goal remains: empower the immune system's fighters!
Immunotherapy is a testament to the power of science and innovation, offering new hope to cancer patients worldwide. 🌍
Let's continue to explore, research, and advance this remarkable field to improve the lives of those affected by cancer.
References:
Postow, M. A., Callahan, M. K., & Wolchok, J. D. (2015). Immune Checkpoint Blockade in Cancer Therapy. Journal of Clinical Oncology, 33(17), 1974–1982. doi:10.1200/jco.2014.59.4358
Rosenberg, S. A., Yang, J. C., & Restifo, N. P. (2004). Cancer immunotherapy: moving beyond current vaccines. Nature Medicine, 10(9), 909–915. doi:10.1038/nm1100
June, C. H., & Sadelain, M. (2018). Chimeric Antigen Receptor Therapy. New England Journal of Medicine, 379(1), 64–73. doi:10.1056/nejmra1706164
#immunotherapy#science#biology#college#education#school#student#medicine#doctors#health#healthcare#immune system#cancer#disease#immune health#immune response
58 notes
·
View notes
Text
Researchers experimenting with artificial intelligence have found that these tools seem to reliably detect breast cancer, while also reducing a demanding workload for radiologists.
Breast cancer is the most common cancer among adults, with more than 2.3 million cases diagnosed each year, according to the
World Health Organization. In most countries, the illness is one of the top two leading causes of cancer deaths in women.
But research shows that early detection and treatment can save lives.
To increase screening capacity and better identify high and low risk breast cancer, two recent studies show that specific applications of artificial intelligence (AI) performed similarly to highly trained radiologists.
"I think that breast imaging, especially mammography, [is] one of the front runners when it comes to the maturity of these AI tools," said Kristina Lång, lead author on one of the studies.
Lång's research, which was published in the Lancet Oncology journal last month, is the first of its kind to use AI to detect breast cancer from mammograms in a randomized control trial.
Preliminary results of the Swedish trial show that AI detected more cancer, while keeping false positives to a minimum.
Continue Reading
69 notes
·
View notes
Text
mRNA vaccines have gained widespread attention for their crucial role in fighting the COVID-19 pandemic. Yet, even before the pandemic, researchers at Memorial Sloan Kettering Cancer Center were investigating the potential of mRNA vaccine technology in the fight against cancer.
Leading this innovative research is Dr. Vinod Balachandran, a physician-scientist associated with the David M. Rubenstein Center for Pancreatic Cancer Research, the Human Oncology and Pathogenesis Program, and the Parker Institute for Cancer Immunotherapy.
Dr. Balachandran's groundbreaking efforts have paved the way for a clinical trial focused on using mRNA vaccines to treat pancreatic cancer, offering new hope to patients confronting this challenging disease.
Neoantigens in Pancreatic Tumors
At the heart of this innovative approach lies the concept of neoantigens, proteins found within pancreatic tumors that serve as alarm bells, alerting the immune system to the presence of cancer cells. These neoantigens play a pivotal role in rallying the immune response to keep pancreatic cancer at bay.
Unlike traditional vaccines, which are one-size-fits-all, these mRNA vaccines are tailored to each individual, with the aim of stimulating the production of specific immune cells known as T cells. These T cells are trained to recognize and target pancreatic cancer cells, reducing the risk of cancer recurrence following surgical removal of the primary tumor.
Intriguingly, the results of this groundbreaking research have shown remarkable promise. Among the 16 patients studied, eight experienced activation of T cells that recognized their own pancreatic cancers.
Importantly, these patients demonstrated delayed recurrence of their pancreatic cancers, providing tantalizing evidence that the T cells activated by the vaccines may be effectively holding the cancer at bay.
Dr. Balachandran's work in pioneering mRNA vaccines for pancreatic cancer received a significant boost through collaboration with BioNTech, the company responsible for developing the Pfizer-BioNTech COVID-19 vaccine.
When asked about the inspiration behind using a vaccine to combat pancreatic cancer, Dr. Balachandran explained, "There has been great interest in using immunotherapy for pancreatic cancer because nothing else has worked very well. We thought immunotherapy held promise because of research we began about seven years ago."
This research, spanning seven years, revealed that a select group of pancreatic cancer patients managed to defy the odds and survive after tumor removal surgery. Upon close examination, it was observed that these tumors harbored an unusually high number of immune cells, particularly T cells.
These immune cells were drawn to the tumors by signals emitted from within. These signals, as it turned out, were neoantigens—proteins that T cells recognize as foreign invaders, prompting an immune system assault on the cancer.
Even more intriguing was the discovery that T cells recognizing these neoantigens persisted in the bloodstream of these fortunate patients for up to 12 years after tumor removal.
This sustained immune response resembled an autovaccination, with T cells retaining a memory of the neoantigens as a threat, akin to the way vaccines confer long-term protection against pathogens. This finding sparked the idea of artificially inducing a similar effect in other pancreatic cancer patients.
Unlocking the Potential of mRNA Vaccines
To understand how mRNA vaccines can combat pancreatic cancer, one must delve into their intricate mechanisms. Dr. Balachandran and his team published their findings on immune protection in long-term pancreatic cancer survivors in the prestigious journal Nature in November 2017. During this time, they were also exploring methods to deliver neoantigens to patients in the form of vaccines, with a particular focus on mRNA vaccines.
Unlike traditional vaccines, which introduce weakened or inactivated pathogens into the body, mRNA vaccines leverage a piece of genetic code known as messenger RNA (mRNA).
This genetic code instructs cells in the body to produce a specific protein, thus triggering an immune response. Coincidentally, BioNTech's co-founder and CEO, Uğur Şahin, expressed interest in the research conducted by Dr. Balachandran's team, initiating a collaboration that would prove pivotal.
In late 2017, Dr. Balachandran and his team journeyed to Mainz, Germany, where BioNTech is headquartered. Over dinner, they discussed the potential of mRNA vaccines in the context of pancreatic cancer treatment. This marked the beginning of a journey that held immense promise for cancer patients worldwide.Scientist, CEO and co-founder of BioNTech Ugur Sahin. (CREDIT: BERND VON JUTRCZENKA/POOL/AFP via Getty Images)
The intricacies of designing an effective cancer vaccine are manifold. Given that cancer arises from the body's own cells, distinguishing proteins in cancer cells as foreign entities is a formidable challenge for the immune system. Nevertheless, advances in cancer biology and genomic sequencing have paved the way for the design of vaccines capable of discerning the difference.
Dr. Balachandran's team, in conjunction with BioNTech and Genentech, capitalized on these advances, recognizing the critical role played by tumor mutations in triggering immune responses. Their optimism in the potential of mRNA vaccines for pancreatic cancer was well-founded, setting the stage for their groundbreaking research.
Personalized mRNA Vaccines: A Tailored Approach
The personalized nature of mRNA vaccines for pancreatic cancer is a testament to their efficacy. After a patient undergoes surgical removal of a pancreatic tumor, the tumor is genetically sequenced to identify mutations that generate optimal neoantigen proteins—those that appear most foreign to the immune system.
Subsequently, an mRNA vaccine is meticulously crafted, containing the genetic code specific to these neoantigens present in the individual's tumor.
During the vaccine production process, patients receive a single dose of a checkpoint inhibitor drug. This combination is intended to enhance the immune response to tumors. Once the mRNA vaccine is administered into the bloodstream, it prompts dendritic cells—an essential component of the immune system—to produce the neoantigen proteins.
These dendritic cells simultaneously educate other immune system components, including T cells, to recognize and attack tumor cells bearing the same neoantigen proteins. With T cells primed to seek out and destroy cells displaying these proteins, the chances of cancer recurrence are diminished.
Overcoming Challenges: The Road to Success
The road to realizing personalized mRNA vaccines for pancreatic cancer was fraught with challenges, not least of which was the complexity of the manufacturing process. Unlike mass-produced vaccines like those for COVID-19, the mRNA cancer vaccine had to be custom-made for each patient based on the unique characteristics of their tumor.Neoantigens are an important feature of cancer cells and help to stimulate anti-cancer immune responses. (CREDIT: Technology Networks)
This necessitated an intricate series of steps, including the surgical removal of the tumor, shipping the tumor sample to Germany for sequencing, manufacturing the vaccine, and returning it to New York—all within a tight timeframe.
Thankfully, Dr. Balachandran's team and their collaborators rose to the occasion, successfully enrolling the target total of 20 patients nearly a year ahead of schedule. Their unwavering dedication and meticulous planning ensured that the personalized mRNA vaccines could be provided to those in dire need.
As if the hurdles of personalized vaccine production weren't enough, the emergence of the COVID-19 pandemic added an unprecedented layer of complexity to the clinical trial. Dr. Balachandran and his team recognized the urgency of adapting swiftly to ensure that patients were not adversely affected.
Under the leadership of Cristina Olcese and with the unwavering support of individuals such as Department of Surgery Chair Jeffrey Drebin and Hepatopancreatobiliary Service Chief William Jarnagin, the team orchestrated the logistics required to maintain the trial's momentum.
Remarkably, what was initially estimated as a two-and-a-half-year trial was completed in a mere 18 months. The tireless efforts of Dr. Drebin, Medical Oncologist Eileen O'Reilly, Physician-Scientist Jedd Wolchok, Biologist Taha Merghoub, Computational Biologist Ben Greenbaum, and the support from Stand Up 2 Cancer/Lustgarten Foundation were instrumental in making this trial a reality amidst the challenges posed by the pandemic.
A Bright Future for mRNA Vaccines in Pancreatic Cancer Treatment
The recent findings from this pioneering research offer a beacon of hope for patients grappling with pancreatic cancer. Dr. Balachandran affirms that "an mRNA vaccine can trigger the production of T cells that recognize pancreatic cancer cells."
The prospect of personalized vaccines enlisting the immune system in the fight against pancreatic cancer—a disease in dire need of improved treatments—holds tremendous promise. Moreover, these developments may extend their impact to other forms of cancer as well.
Looking ahead, Dr. Balachandran and his team are committed to further analyzing the data obtained from the clinical trial. This analysis will provide valuable insights into the factors that facilitate the vaccine's efficacy in patients. Armed with this knowledge, they aim to refine the vaccines to make them more effective and applicable to a broader spectrum of pancreatic cancer patients.
In a testament to the forward-thinking vision of the Memorial Sloan Kettering Cancer Center, this pioneering work exemplifies their commitment to bringing cutting-edge treatments to cancer patients.
Through their partnership with BioNTech and Genentech, and with the support of Stand Up 2 Cancer/Lustgarten Foundation, a larger study is already in the pipeline, aiming to test personalized mRNA vaccines in a more extensive cohort of pancreatic cancer patients.
As Dr. Balachandran notes, they were at the forefront of mRNA vaccines before their popularity surged, leveraging scientific discoveries to make a tangible impact on patients' lives. The future indeed looks brighter for those facing the formidable challenge of pancreatic cancer, thanks to the relentless pursuit of innovation in the field of mRNA vaccines.
Key Takeaways
Some people with pancreatic cancer survive many years after diagnosis.
In these patients, the immune system keeps the cancer from returning.
A messenger RNA vaccine based on this concept is being tested in combination with another type of immunotherapy.
Early results suggest the vaccine is having the desired effect on the immune system.
12 notes
·
View notes
Photo

I know Love Actually is a Christmas romcom but my fics are never ready on time (the Easter chocolate hunt fic is staring at me in my WIP files).
Now, the real question is, should I write this 👇? I did spend way too long writing that plot that was supposed to be short.
Vincent is a stage actor. The company he’s in will be playing God of Carnage, from the French playwright Yasmina Reza. This play presents two couples seemingly politely discussing the fact that one of the sons hit the other. Vincent is one of the fathers and Adriel plays the other one. Unlike Vincent, Adriel has made his career in Hollywood, he is well-known and well-loved by the public. Adriel’s ego makes him insufferable for everyone in the company but that’s not why Vincent is having such a hard time working with him. No. They have history together, and Vincent hasn’t forgotten that.
Beatrice, the play director ー said to be one of the most promising directors of her generation ー is trying her best to ease the tensions between her two male leads because the words have gotten out that movie-star Adriel and his co-star could not stand each other. She doesn’t want that kind of press for her play. Ava, working at the opening, lets her know whenever journalists are trying to get information.
Ava dreams of being a movie star. Waiting for an opportunity to present itself, she shares an apartment with her older sister, Shannon, and Shannon’s friend, Lilith.
Shannon has graduated with a journalism degree and is now struggling with her debuts. As for Lilith, she works in a small flower shop.
SEPTEMBER, 29th. That’s where she meets Camila, a student in computer science who likes to do random good things for people and who has decided, that day, to pick flowers for people in the nearest hospital. Shannon, passing by the shop to drop Lilith’s keys she forgot in the morning, sees Camila struggling with the many bouquets she has ー she offers to help her.
Mary works in this hospital as a nurse in oncology. Her patients find Camila’s initiative lovely. As a public hospital underfunded, nurses and doctors are overworked, there aren’t enough beds, patients must sometimes be left waiting in the hallways and wait for hours before someone can come check on them. It’s a shock for Shannon, because she can tell it’s not a lack of care from the staff, it’s a fault in the system.
Shannon wants to do something. She asks Mary what she thinks of the possibility of Shannon writing an article about the current situation in collaboration with nurses and clinicians. She doesn’t want sensationalism, she wants to raise awareness and point fingers where the fault lies. Mary is reluctant at first but eventually notices Shannon only means well. She suggests she talks to upper directions.
Mary’s best friend is Suzanne, a teacher, who’s Vincent’s little sister. Between her clumsy enthusiastic assistant, Yasmine, who means well but requires a lot of her time, her kind yet exhausting pupils and her brother’s awful mood because of Adriel, Suzanne has been begging Mary for a weekend away, just the two of them, to flee the stress of her everyday life. This little getaway would also be a great opportunity for Suzanne to set Mary on a date with a perfect stranger, since Mary has rejected anyone Suzanne knows.
OCTOBER, 15th. Tonight is the opening night and it couldn’t possibly be worse. Vincent and Adriel aren’t talking to each other, they refuse to get out of their respective lodge for the finale rehearsal and Beatrice has no other choice than to call their respective agents. She regrets her decision the moment she realises Francesco Duretti, Vincent’s agent from O.C.S, and Jillian Salvius, Adriel’s agent from F.B.C, are sworn enemies in their own business, constantly trying to steal each other’s actors. Despite their mutual contempt, they need to get the two actors back on stage before tonight, which won’t be easy considering Adriel won’t talk to Jillian and Vincent is ignoring Francesco’s calls.
Ava is the one who suggests to Jillian that she tries talking to Vincent’s sister because she’s the only one who scares him enough to get him to do anything. Ava has overheard Suzanne mention her students once, but she’s not sure which school it is, just that it’s nearby. Jillian visits three schools before finding the right one. Suzanne finds it weird, yet not completely not funny, to know that this stranger has been looking for the most part of her afternoon so she agrees to talk to her brother. Vincent eventually agrees to come out of his lodge and if Adriel doesn’t want any bad press, he has to play along.
The opening night goes smoothly, as opposed to the entire day. Everyone is in the room. Yasmine came with her roommate Camila who came with Lilith who herself came with Ava and Shannon. Mary came with Suzanne. Jillian and Francesco are there to make sure their actors won’t try running away during intermission. Everyone gets to stay for the After Party, Beatrice lets Ava know her friends are more than welcome.
Suzanne gets to meet Shannon and she quickly notices her interest in Mary that has grown while the two of them were working together for the article. And Suzanne has heard a lot about Shannon from her friend. She just needs to get Mary to be brave enough to ask Shannon on a date.
Yasmine, Camila and Lilith hang out together, they like staying near the buffet and try to guess people’s most embarrassing secrets.
Ava gets the courage to tell Beatrice that she inspires her. Beatrice could faint but eventually confesses to her that she kept her distance because she was scared Ava’s attempt at getting closer only was to get a first role somewhere. It hurts Ava that Beatrice would think something like that but she understands it must have happened before for it to be such a strong fear. She promises she has no secret interests behind her willingness to get to know Beatrice better.
Jillian manages to steal Suzanne from her brother, Francesco and their friends for a few minutes. She thanks her again for allowing the situation to go back to normal. Suzanne is reluctant to talk to the agent, Francesco has warned her about Jillian Salvius’ questionable methods. Jillian ensures her that her brother is not the one she’s interested in. She tells Suzanne that if she ever gets bored of the five men she seems to be destined to spend her evening with, she can come find her later. Later that night, Suzanne gets a text from an unknown number:
“You didn’t come.”
“How did you get my number?”
“Questionable methods ;)”
“You had already left.”
Jillian actually asked Ava if she could ask Suzanne’s number to Vincent. Ava instead asked her sister to ask Mary. Jillian had left the party in a hurry after a call from her babysitter informing her that her son, Michael, was running a fever. Her 8 years old only recently recovered from leukaemia. His first nurse when he was 4 was Mary.
NOVEMBER, 2nd. Taking a walk in the city with Suzanne, Mary recognises Jillian and Michael in a park. She tells Suzanne she needs to say hi. That’s how Suzanne meets Michael for the first time and how Mary understands Jillian is the woman Suzanne has been talking to since the opening night without ever agreeing to meet her on a proper date. Michael tells Mary that, for Halloween, he was dressed as Dr Noru, the scary chief of oncology. Mary laughs, because Dr Noru was indeed terrifying. Later that day, Mary offers Suzanne a deal: if she goes on a date with Jillian, she’ll ask Shannon out. It’s a deal.
NOVEMBER, 10th. Ava knows it’s Beatrice’s birthday. She asks Lilith and Shannon to disappear for the night so she can have their place. She cooks, bakes, and decorates the room for Beatrice. She buys her flowers, the English tea that Ava has noticed Beatrice had run out of, and she has collected all positive reviews about the play and specifically Beatrice as a director in a journal that she’ll give to her. She knows Beatrice doesn’t have plans so she calls her and asks her to come over because she has some very important news to share with her. Beatrice is grumpy when she shows up, thinking Ava is going to tell her she was offered her first role and would soon have to leave. She bursts into tears when she realises what Ava has done for her. It turns out Ava is a great baker but a terrible cook. They end up ordering food and spend the entire evening talking. Ava asks if Beatrice wants to stay over. They fall asleep in Ava’s room, watching a movie together.
In the meantime, Lilith is enjoying board game night at Yasmine and Camila’s. They have invited their friends Hans, Todd and Chanel to join them and Lilith really enjoys Chanel’s company.
Shannon has asked Mary if she was free tonight because her sister was kicking her out of home. Mary’s shift supposedly ended at 8pm. It’s 10 when she finally gets out. She’s too tired to go anywhere and Shannon offers to just make them both dinner and then let Mary sleep. Mary tells her she can stay. Shannon is shy and doesn’t want to cross any boundaries so when Mary is asleep, she leaves a note on the kitchen counter and goes back home where she finds burnt cannelloni in the shrink.
DECEMBER, 14th. Suzanne’s class goes to visit the Science Museum with another class that turns out to be Michael’s class. He’s happy to see her, she’s been at his home a few times lately but has never stayed long. He spends the whole visit holding her hand. When it’s time for parents to come pick their children, Michael’s teacher complains that Jillian is late again. Suzanne tells her to go, she’ll bring Michael home, she knows his mother. When Jillian opens the door, she’s paler than usual and she’s slightly shaking. Food poisoning, she explains to Suzanne. There’s no risk for Michael to catch it so they should be fine. She thanks Suzanne for bringing him home. Suzanne doesn’t leave her a choice and walks in. She helps Michael with her homework, makes Jillian rest on the couch with a bucket on the ground for emergencies and busies herself with making something for dinner that Jillian’s stomach might not immediately reject.
DECEMBER, 20th. Love actually is a Christmas movie so it’s Christmas!
It’s the last day the theatre is open for the season and the last representation of Gods of carnage tonight. They’re having a little Christmas party after. It’s just them, it’s nothing much but Ava insisted they did a Secret Santa this year with the possibility of only giving something homemade. After the party, Ava asks Beatrice what she’s going to do for Christmas. Beatrice won’t fly home. There’s nothing stopping her from accepting Ava’s invitation to come celebrate Christmas Eve and Christmas and Post Christmas with her, her sister and their friends. Neither Ava or Beatrice are very certain of what they are to each other. Both hope.
Lilith invited Camila and Yasmine and told them to bring Hans, Todd and Chanel if they had nothing better to do. Todd will spend the holidays with his family but Hans won’t go back to Switzerland and Chanel has lost contact with her family, they’re delighted to have this Christmas time with their friends. Shannon and Ava can’t stop teasing Lilith at how delighted she is to learn that Chanel will be here.
Shannon knows Mary will be working on Christmas and asks if it’s okay if she comes to the hospital to spend time with her during her breaks. She could bake Christmas cookies for the patients and the staff. Mary tells her that will make a lot of Christmas cookies. Shannon spends the whole day baking to make sure there are enough for everyone.
It’s the last day of school and when Suzanne hands the last kid to his parents and tells them to enjoy the holidays, she notices Yasmine coming back with Michael’s hand glued to hers. “He was looking for you.” Michael wants Suzanne to spend Christmas with them. Disclosed reason: she needs to save them from Jillian’s cooking. Secret reason: he saw mistletoe at the flower shop near their house and is planning to buy some for his mum and her friend who should really be her girlfriend instead. Suzanne calls Jillian to make sure she doesn’t go into cardiac arrest when Michael’s teacher tells her he’s already left. Suzanne drops him home and before she leaves, Jillian shyly asks what her plans for the holidays are.
CHRISTMAS filled with Christmas activities (hot chocolate, gingerbread houses, decorating a tree, Christmas cooking, Christmas movies, board games, ice skiing, snowball fight, building a snowman, cuddling by the fireplace, kissing under the mistletoe, last minute Christmas shopping…)
SO, should I write this?
#warrior nun#should i write this?#avatrice#doctorsuperion#mary x shannon#Adriel and Vincent are once again exes#Duretti and Jillian have a thing going on à la Call my agent#warrior nun au#ava silva#Sister Beatrice#jillian salvius#Mother Superion#sister camila#sister shannon#sister lilith#sister yasmine#and yes I want Lilith to meet Chanel and to fall in love with her#Father Vincent#adriel#Michael Salvius is a cute little boy trying to get his mum a girlfriend
97 notes
·
View notes
Text
He knows who she is the moment she steps through the door. And it isn’t just his doctor.
Dana Katherine Scully, age thirty-three. Short, slim, with short red hair — though he only knows the last part from the file — she is the youngest doctor in the oncology ward of the Holy Cross Memorial Hospital.
What the file doesn’t describe, what her black and white photo does not credit her with is elegant features, as if she were carved in marble by an ancient Greek master, or wide blue eyes that swim with the right balance of heavy respect and sympathy to make it genuine, personal. What the file doesn’t prepare him for is the aura of professionalism and kindness that makes Mulder want to trust this woman with his life.
And, to his credit, it isn’t that she is breathtakingly stunning — there is too much at stake in this small room, with its bright LED wall and sterile equipment, and not just his life. No. It isn’t even all the competence that radiates out of her exemplary scientific journal entries displayed on his shelf at home. Though those two facts do make him think of staking more than his life on this impossible, predestined, chance meeting.
It is simply the way she narrows in on his face with humanity and says his name like she already knows him, knows the burden he is carrying.
“Fox Mulder?” He nods and receives her hand. “I’m Dana Scully, one of your oncologists. I’m sorry we have to meet under these circumstances. It must seem disorienting to come face to face with a new doctor in the middle of the process.”
He finds a smile so easily in the face of her. “Not all that disorienting,” he assures her. “Nor surprising. As you may have noted from the file I’m very eager to fight this thing, so inviting in new doctors has been a recurrent decision.”
And he has the means to do so, he doesn’t add.
She’s difficult to read, Doctor Scully. When she presses her plumb lips together, he can’t tell if it’s to keep back condolences that he has come to the end of his rope and is now being treated by someone young and comparatively inexperienced, or a note on the funds he’s using, looking for a cure.
But the fire he sees in her blue eyes gives him hope that the young and comparatively inexperienced may be more willing to risk and be reckless.
“Well,” she says, “let’s see if we can’t meet your expectations somewhat today.”
Scully flips open the file she has on him and produces several x rays, newly minded and fresh off the press.
Even in her white lab coat, she is a foreboding black silhouette against the white LED wall surrounded by a series of sculls, and even without her translation it is clear that the cancer has yet to leave him alone.
She distracts herself momentarily, looking around for a chair, and Mulder is struck by the consistency in her kindness. He has been invited to sit enough times to know from the gesture that this will not be an optimistic delivery on her part, but a cursory look around the room should have made her note the lack of chairs, and Scully taking her time to doublecheck tells her all he needs.
With nothing tangible to offer him, Scully gestures instead for him to take a step closer.
“Don’t worry,” he assures her, taking advantage anyway to fall into her field of gravity. “I won’t faint at bad news.”
She finds his eyes then, attention drawn, and Mulder is pleased to see a smile crinkle at there corner of hers.
“I don’t think you should try to catch me anyway,” he adds, keeping his voice low.
Another spark, defiance, crackles in her impossible eyes. “That’s my job, Mr Mulder,” she admonishes him. “So I will.”
He grins, a flash of teeth.
Oh, Doctor Scully is interesting.
She doesn’t like being reminded of her short stature or the expected strength difference inherent in their bodies, but it doesn’t matter. Because right this moment, Scully seems the most formidable, most powerful defender of his life that he could ever entrust his fragile body to.
“So,” he says, with real cheer. “Cancer.”
Closer now, he can see the red circle she’s marked a white growth with. Right between his brows.
“Yes,” Scully confirms, her voice shifting to one of complete medical professionalism. “It’s a Nasopharyngeal mass,” she says. “It’s a small growth on the wall between the superior concha and the sphenoidal sinus. A tumor, in other words. But you already knew that.”
“I did,” he admits, rubbing the soft skin between his brows carefully.
Seeing it confirmed right in front of him like this once again sends a burning sensation through his body, his grief like a phantom pain his brain cannot yet express in any other way.
It’s been his constant companion for five years now.
“It doesn’t look like it’s grown since last time,” he observes, keeping his eyes glued to the profile x ray.
If it pushes into his brain, he knows, he will have no chance of survival.
And no matter his hatred towards himself, the odd sensation that the planet has found a way to punish him appropriately for his betrayal, he cannot die. It is simply not a possibility he is willing to entertain or humor.
Beside him,, Scully shifts silently. A distraction that draws him.
“I hate to have to correct you, Mr Mulder,” she says. “But, while it hasn’t grown towards your brain, it has widened its reach horizontally and vertically.”
She produces another frontal x ray from his file, the one from a couple of months ago. Silently she places the two x rays beside each other, and shows him with a specialised electronic ruler how it has grown. Almost nothing to the naked eye, but there it is in clear digits, black-on-green.
Mulder keeps very still right at her side.
“What can you do?” He murmurs, when he can no longer simply stare at the evidence of his body having taken up his habit of self-destruction.
He doesn’t ask if surgery will solve it. He already knows what the answer will be.
When she turns the full front of her body to him, it’s like she’s dragged him out of a trance, freeing him from having to face himself. And Mulder mirrors her, the easiest thing in the world.
“The truth is that the type and placement of the tumor makes it difficult to the extreme to treat and impossible to operate.”
Mulder stares down at her, and is reminded of another set of wide blue eyes, another bob of hair, the colour of which he can’t accurately discern. Vertigo hits him so powerfully, his hand flies out to steady himself.
The LED war buzzes under his hand like a thousand bees, unsteadying him further.
It’s a slow thing when he falls apart. The crumbling of his limbs like an ancient building that loses its foundation across history. The strength goes, and he glides down the electronic wall like a man sitting himself in the chair.
His sigh falls between his fingers, warming his palms.
“I have to refuse to believe that.”
There’s a tiny rustle, as his tiny doctor kneels at his side. A warmth on his shoulder as she connects their bodies, touches him for the first time since their introduction.
“Of course, you have to fight this,” she says. “And I’ll do everything I can to help you live—“
“No,” he corrects her, looking up from the darkness of his own hands. “This isn’t about me.”
Lit by the LED wall behind him, Scully is a flame of light that gives life to his shadows.
“I have a daughter,” Mulder tells her. “A tiny, four year old sprout of a girl. I have to live for her.”
That is it. That is all. Everything that defines Fox Mulder is the child entrusted to his protection and care, gifted to him to keep him in line. And he will do anything, sacrifice anyone, to keep her healthy and smiling.
If that means keeping his sorry ass alive, then so be it.
“Okay.”
Mulder doesn’t know what he looks like, but he sees the moment that he becomes less of a hollow of a man and much more a fire alike to hers in Scully’s eyes. He sees the shift in the blue when he becomes more human than patient, when she understands what gives him a reason to live.
“Okay,” she says again, nodding, as if his quest has become hers. “Of course. Let’s start with that.”
Find full chapter here!
#the x files#txf#msr#fox mulder#dana scully#fic#fanfic#fanfiction#AU#Emily sim#writing#louie writes#Vandalize the stars fic
10 notes
·
View notes
Text
Power Play
Book: Open Heart, Book 2
Pairing: Dr. Ethan Ramsey x F!MC (Dr. Sawyer Brooks)
Rating: Explicit
Warning: 🔥NSFW, 18+ Only, contains sexual content
Category: Fluff, Smut
Word count: 2.9K
Prompt/Summary: Fed up with some of Ethan’s catty and manipulative admirers, Sawyer tries to beat them at their own game.
A/N: Inspired by this ask and the follow up request from @annfg8 for a jealous Sawyer fic. This takes place shortly after the softball game kiss.

Even Ethan was on board when June suggested they present at the conference and bring some much needed attention to Edenbrook. The event coordinators were excited to promote the renowned diagnostics team as the headliners. As such, the team was asked to be part of a moderated panel discussion that morning, followed by Q&A breakout sessions throughout the afternoon.
In between sessions, Sawyer began to notice just how many admirers sought the attention of the famed Dr. Ethan Ramsey. Most of them women, with an air of sophistication about them in both appearance and accomplishment. They stood before him in their classy sheath dresses and power pantsuits, accessorized with expensive jewelry, designer shoes, and handbags that cost more than her rent. She heard snippets of their conversations with mentions of groundbreaking research, articles published in prestigious medical journals, keynote presentations, and AMA awards. Sawyer also observed the flirtatious posturing. How they leaned in, tilted their heads, subtly touched his arms and shoulders, and on occasion even flashed their eyebrows.
No longer able to stomach the view, Sawyer escaped to the restroom for a moment to herself. Locking herself into a stall, she heard the click-clack of high heels as two women entered.
“I would let that man do absolutely anything to me. An-y-thing. And from what I’ve heard, he’s currently available,” the woman sang, fixing her hair in the mirror.
Applying a fresh coat of lipstick, the other laughed, “Ha, good luck. He’s been eye fucking that protégé of his all day.”
“Please. Ethan Ramsey is a man of refined taste. He dated Harper Emery for fucks sake.”
“Let’s go find Hirata and get the scoop.”
Red hot anger crept up her neck as Sawyer waited for the coast to clear. As she moved to wash her hands, a poised red-head joined her at the sinks.
“Ignore them.”
“Pardon?” Sawyer asked, making eye contact through the mirror.
“You’re Dr. Brooks from Edenbrook. Sawyer is it?” she pumped soap from a dispenser. “I’m Kellie. Kellie Wicker. I’m in Oncology over at Brigham. I’m a friend of Ethan and Harper’s.”
“It’s nice to meet you,” Sawyer greeted cautiously.
Repeating the advice, “Just ignore them. Sadly, a good majority of the women in attendance only come to these conferences to meet men. And those bitches are notorious for coming in and marking their territory.” Drying her hands she added, “As if they have any chance with Ethan Ramsey either.” Her snicker echoed in the tiled room.
Unclear whether it was meant to be a dig, the word “either” didn’t get past Sawyer, who shook the excess water from her hands and reached for a paper towel.
Tucking her copper strands behind an ear, Kellie continued, “If it’s any consolation, I can tell Ethan respects you. He’s a very proud mentor, and as he put it when we spoke earlier, he thinks you have tremendous potential.”
“Thank you. Dr. Ramsey’s been a great teacher. I’m incredibly lucky to have the opportunity to work with him, as well as Dr. Hirata and Dr. Mirani.”
“Lucky indeed,” Dr. Wicker concurred. “Well, it was nice to meet you, Sawyer. I look forward to seeing you at the reception later,” she offered, turning on her heel to leave.
“Sorry, can I ask you a quick question? How fancy is this event tonight? I packed a couple different dresses but–”
“Oh…oh, it’s not fancy at all,” Kellie paused with one foot out the door, “Business professional, dear.”
“Glad I asked. Thanks.”
Sawyer returned to the lobby where she found Baz obnoxiously flagging her down. “Sawyer, you’ve got a fan seeking an autograph,” he pointed to the mystery man.
As she rolled her eyes, the man turned around and Sawyer squealed with excitement. “Ben! What are you doing here?”
“Brooksie! Wow, Boston looks good on you, honey. Aside from the fact that you are in desperate need of a spray tan,” he teased.
She playfully swatted at him as he pulled her off to the side to chat.
Having missed the initial exchange, Ethan entered the lobby, his eyes immediately drawn to the man hovering over what he wished he could publicly claim as his own.
From what he could ascertain, the flamboyant doctor was someone she knew from Los Angeles. Ben personified the Beverly Hills doctor stereotype right down to his sleek Armani suit and shiny Prada shoes. If Ethan had to guess, he was most likely a plastic surgeon.
As Ben rubbed his hand up and down Sawyer’s arm, Ethan’s muscles tensed. And when Ben pulled her into a hug and placed a chaste kiss on her cheek, Ethan gritted his teeth. Swiftly gathering his belongings, he announced to Baz that he was heading back to his hotel room. With urgent steps he exited the conference center, ignoring those who still wished to win him over with favors and flattery.
Agreeing to share a drink with Ben later at the reception, Sawyer tried to catch up to Ethan.
He was already several steps down the hall of their floor, when the second elevator chimed behind him.
Not wanting to disturb any hotel guests by shouting, Sawyer jogged to his side placing her hand on his lower back to get his attention. “Hey.” The thrill of her touch reduced his blood pressure just slightly.
Catching her breath, “I feel like I haven’t talked to you all day. How are you?”
“Fine,” his tone curt.
“That was quite an impressive following I witnessed down there today. I mean, I saw a bit of it in Miami, but those were mostly pharma execs,” she tried gauging his mood, “I bet you’re glad to finally have some time to yourself.”
“Yes, I am,” he fished for the keycard in his pocket.
“Ah, the downside of fame,” she teased.
A hint of irritation in his voice, “It looked as though you had plenty of your own admirers.”
With a breathy chuckle, “The only people who approached me wanted to know what you were like,” she stated honestly.
“Hmph. Well, this is me. If you’ll excuse me, I have a couple calls to return.”
Disappointed there was no suggestion of going to the reception together, Sawyer dug into her purse in search of her own room key. “Okay. Well, I guess I’ll see you downstairs later,” she said as Ethan entered his room and closed the door. The interaction, or lack thereof, only fueled the festering feelings of insecurity.
A couple hours later, Sawyer approached the entrance to the hotel lounge. Stopping short, she noticed how the other men and women entering the room wore formal cocktail attire. Then sashaying across the hallway in a sequined minidress, Kellie glanced to her right. She scanned Sawyer from head to toe and with a quiet but villainous laugh she walked on triumphantly. As the two-faced ginger crossed over the threshold, Sawyer heard her phony voice ring out. “Ethan. Hello handsome. Come, have a drink with me.”
Turning one hundred and eighty degrees, Sawyer retraced the steps back to her room, all the way debating whether to even return. And if she decided to return to that hyena’s den, she wondered which of the dresses in her suitcase she should change into.
Standing in front of the full-length mirror in her nicest black pantsuit, Sawyer made the decision to fight fire with fire. She thought to herself, she may not be as polished and accomplished as the Harper Emery types who paraded around downstairs, but she did have certain assets that would set her apart from the pack. And she wasn’t afraid to use them.
Shrugging her suit jacket off, Sawyer lifted the ivory silk tank top over her head and removed her bra. She carefully smoothed her wavy hair into a sleek bun and wiped the neutral colored lipstick away, replacing it with a bold shade of red. Her modest jewelry was traded for a sparkly necklace, one that would be sure to draw attention to the aforementioned assets. Tugging her jacket back on, she fastened the only two buttons located at her waist. Sawyer turned from side to side making sure she wasn’t giving too much away, and when she was satisfied, she grabbed her clutch and made her way back down to the reception.
Meanwhile downstairs, Ethan stood at a high table sipping his whiskey neat as Kellie droned on about her recent hormone replacement study. He swept the room often, shifting his eyes to the doorway every time someone entered.
Sawyer was a fairly punctual person. With the reception well underway, Ethan’s concern for her grew. His mind raced with all sorts of theories. The worst was that she might be off with Dr. 90210, who was also nowhere in sight.
Finally revealing her true intentions, Kellie changed the subject. “I ran into Harper a while back. She mentioned that you two were no longer together.”
“We are not. It was time to move on.”
“Are you seeing anyone new?”
Ethan didn’t answer. Instead he shook his head, not in reply but in annoyance, and took a swig of his drink.
“Come on, Ethan. We’ve been dancing around each other for years now. Let’s have some fun tonight,” she pawed at his arm.
As soon as the words left her mouth, Sawyer stepped into the cocktail bar, stealing the attention from many conversations. After briefly surveying the room, her confident form glided in his direction. Ethan chewed the inside of his bottom lip to keep his mouth from falling open. But there was little to be done to stop his eyes from roaming her exposed chest. Her bare breasts taunted him, only the lapels of her suit jacket hiding the most sensitive parts. Sawyer looked from him, to his company, and back again. “Dr. Ramsey,” she acknowledged with a nod as she sauntered past.
“There she is!” Baz shouted as Sawyer approached the bar table where he and June shared drinks. “Whoa, step aside, Beyonce. Sawyer Brooks is the one slaying now.”
After rolling her eyes at his ridiculousness, Sawyer looked around taking in the overall atmosphere, but June easily saw through the farce. Psychoanalyzing, she could tell Sawyer searched for reaction from Ethan and his current companion.
“That is quite the statement you are making, Sawyer. Who exactly is the intended audience?”
Sawyer snapped her head to June, finding a smug expression on her face.
A few tables away, Kellie followed Ethan’s eyes as they tracked Sawyer across the room. Trying to regain his attention, she ran the lapel of his jacket through her fingers, “So, what do you say?”
He looked to the table where his colleagues stood. “Please excuse me. I need to touch base with my team,” he said, grabbing his drink and backing away.
“Good evening,” Ethan met the table, coming to stand at Sawyer’s side.
“Hey, Boss!” Baz greeted in return. “So, how’d you all think it went today?”
June spoke, “I’d say ‘mission accomplished.’ I was approached by an editor from the NEJM who wants to write a feature about the team. And speaking of…” spotting the man, she followed him to the bar.
So that only she could hear, Ethan leaned close to Sawyer’s ear. "You seem to be missing something.”
“If you mean a stiff drink, then yes, I was hoping to fix that.”
His eyes flashed quickly to the fleshy mound peeking out from underneath her suit coat. “Not what I was referring to,” he straightened, “but allow me to remedy the drink issue. I could use another myself. Be right back.”
Baz picked up the conversation asking Sawyer what she had thought about the conference, but was suddenly distracted with a passerby. “Scotty?! Scott Briscoe, is that you? Excuse me, Sawyer,” he apologized, leaving to reunite with his old college pal.
As Ethan waited at the bar for their drinks, he looked back to Sawyer who now stood alone at the table. While it pleased him to find her staring back, he was not thrilled to see men at nearby tables eyeing her as well.
A moment later, Ethan placed a drink in front of her and Sawyer initiated a familiar game of people-watching. As they searched for their next targets, Ethan spotted Ben schmoozing at a table in the far corner of the room. At the same time, Kellie stood nearby glaring at Sawyer.
Ethan jutted his chin toward an exit that led outdoors. “Care to join me for some fresh air?”
“God, yes,” she sighed with relief.
They threw back the rest of their drinks and made their way outside, finding a long and windy path that curved around to an overlook of the ocean.
“So, what’s with the bold look tonight?”
She shook her head. “It’s actually quite embarrassing and pathetic really.”
“What is?”
Taking a deep breath, Sawyer proceeded to tell him about the gossiping women and Kellie’s “kindness.”
“So, anyway…I…I guess I was just feeling a bit insecure and jealous watching these women hang on you all day. And after getting hoodwinked by that Kellie woman, I decided I could either hide in my room all night or play the game using my advantages.”
“Which are?” he was curious.
“That I’m younger and hotter,” she stated proudly, earning a laugh from Ethan.
As they continued down the path, Ethan frequently glanced over at Sawyer trying to understand the root of her jealousy. How could she have any doubt that he only had eyes for her? But he already knew the answer to that question. The uncertainty of their situation was of his own making.
“You know there’s no reason to be jealous, right?”
When she barely acknowledged him, he reached for her hand, stopping them in their tracks. “Hey. I know I’ve spent the last several months confusing you. And I’m genuinely sorry, Sawyer. But whether it’s a crowded room or a busy hallway at work, my eyes are always and only searching for you,” he affirmed. “You stole my attention in that waiting room last year and have had it ever since,” pulling her into his arms, “I’m all yours.”
Sawyer squeezed her arms tight around Ethan’s torso, thankful for the confirmation.
After a comforting moment, Ethan pulled back to admire, “I wish I could tell you that jealousy looks terrible on you…but fuck, Sawyer…this sexy power play of yours is a major turn on.” His fiery blue eyes burned right through her, causing Sawyer to shiver.
“Cold?”
“It is a bit drafty,” she giggled.
“Let me try and warm you up.”
Ethan turned her away from him, wrapping an arm around her waist to hold her snug to his chest. Grazing his lips past her ear, she felt the warmth of his breath before he began placing heated open mouth kisses down the column of her neck. With his free hand, he caressed her goose-pimpled skin from neck to navel, his fingers slipping through the open door of her jacket. He traced around her breast before cupping it with his large palm, kneading tenderly. Not wanting to be neglectful, Ethan gave equal attention to her other side.
Sawyer reached behind, hands holding his hips close, needing to feel more of his hardened length against her ass. “Kiss me,” she urged, tilting her head back.
Obeying, he captured her lips in a hungry kiss, savoring the taste that he had craved every day since Miami. He worked to unbutton her jacket as Sawyer nipped along his jawline. Twisting in his arms, she framed his face and traced her tongue across his lips enticing him to open to her again.
Ethan drove himself into her until she bumped into the wooden railing. Lifting her onto the top rail, he grasped Sawyer’s backside, anchoring his hands firmly to her ass cheeks to prevent a backward fall. A convenient gust of ocean breeze pushed a flap of her unfastened jacket open. And taking advantage, Ethan buried his head into her chest licking and sucking her peaked nipple.
Sawyer’s gasps and moans were visible in the cool night air.
“Mmm…Sawyer,” he mumbled against her silky flesh, “...tell me you’re mine too.”
Dragging him up to eye level, she locked her legs around his waist and slipped her hand between their bodies, eliciting a gratifying groan. Lips barely brushing his, she massaged his erection and purred, “I’m yours, Ethan. Only yours.” Punctuating her declaration, she deepened the kiss.
Pulling back for air, Ethan tilted his head upward and closed his eyes, enjoying the increased pressure and speed of her ministrations. When suddenly he felt a drop of moisture smack his face. Sawyer felt it too on her naked chest. They both looked to the sky, then to each other, bringing their foreheads together as they accepted their defeat against mother nature.
“C’mon, we should get you covered up and back inside before hypothermia sets in,” Ethan helped guide her feet back to the ground.
After adjusting their clothing and making sure the twins were safely tucked back in, Ethan took her hand in his.
As they walked back to the hotel entrance, Sawyer leaned into him. “Ethan, has there ever been a time when you were jealous over me?”
Without hesitation, he answered truthfully. “Yes. Many times.”
“Really?”
“Rookie, I asked you to come out here with me because I saw Doc Hollywood walk into the lounge…and I didn’t want to share.”
“Doc Hollywood?” she looked up in question.
“The handsy blonde guy you were hugging earlier at the conference center.”
With an amused laugh, “Ben? You were jealous of Ben?”
“Why’s that funny? How do you know him?”
“His husband is my good friend from Caltech. I was in their wedding party.”
“Oh,” he said, cheeks flushing red. “Well, either way…I still wanted you all to myself.”
Tag List: @choicesficwriterscreations @openheartfanfics @potionsprefect @jamespotterthefirst @annfg8 @peonierose @socalwriterbee @tessa-liam @jerzwriter @quixoticdreamer16 @mysticalgalaxysstuff @inlocusmads @txemrn @trappedinfanfiction @mvalentine @takemyopenheart @ofmischiefandmedicine @openheartforeverinmyheart @doriopenheart @coffeeheartaddict2 @genevievemd @starrystarrytrouble @hopelessromantic1352 @kyra75 @lsvdw-blog @rookiemartin
#open heart#open heart choices#open heart fanfic#ethan ramsey#ethan ramsey x mc#ethan x mc#ethan x sawyer#choices stories you play#choices open heart#playchoices#choices fic writers creations#cfwc fics of the week
62 notes
·
View notes
Text
Lower drug pricing does not follow from an expansion of innovative medicine indications, according to Dutch researchers. They claim pharma companies often fail to pass on their financial gain to patients and health services.
If more patients are prescribed a certain medicine, the price could be reduced because pharmaceutical companies can recoup the research costs incurred more quickly, researchers from Erasmus University Rotterdam and the Erasmus Medical Centre Rotterdam claim.
This finding emerges from their study published in the peer-reviewed PLoS ONE journal last February.
The study considers the possible financial effects of a broader use of two cancer drugs, pembrolizumab (Keytruda) and daratumumab (Darzalex), which have already been approved by the European Medicines Agency (EMA) and the Food and Drug Administration (FDA) in the US.
“Pharmaceutical companies are responsible for their own pricing strategy; it is not up to academics to dictate what exact price reduction to accept,” study first author Renaud Heine told Euractiv.
However, when asked about the potential of this new pricing method, the Dutch Association for Innovative Medicines (VIG), which is a member of EFPIA, cited arguments raised by economics professor Lieven Annemans that the proposed model change does not value true innovation and that value-based pricing remains more appropriate.
Indication broadening and pricing
Heine explained they aimed to study the effect of indication broadening on price when applying cost-based pricing (CBP).
“Our results indicate that cost-based prices drop consistently after indication broadening and are below known list prices,” he said.
Building on the CBP model developed by two researchers, Uyl-de Groot and Löwenberg, in 2018, the research group explored price changes of these medicines if there was a continuous indication expansion.
Both drugs are immuno-oncology drugs. Pembrolizumab was first used for only one type of tumour, but now it is prescribed for approximately 35 different indications for various types of tumours. Daratumumab was initially used for one type of cancer, multiple myeloma. It is now prescribed for eight other indications within multiple myeloma.
While development costs for new drugs can be significantly high for the first indication, they become lower with each expansion of use in new indications.
However, this financial gain for pharmaceutical companies is often not passed on to society despite the lower costs, the researchers say.
continue reading

#netherlands#big pharma#drug pricing#cost of research#expanded use of drugs#financial gain#not past on#capitalism
5 notes
·
View notes
Text
Thess vs Why We Fight
Another one from the bowels of Reddit, mostly because it's interesting.
There's a subreddit - r/antijob - that I follow mostly to keep track of real people's experiences in the workplace other than my own. And there was a post where the question was asked, "Why do you do more than the bare minimum?" That was the title, anyway. While the question was genuine, it was also at least half a lead-in to "If you're not stealing time back from the company that abuses you for too little pay, you're doing it wrong".
Thing is ... I had an answer. And that answer is: "I do it for the patients".
Yes, I complain a lot about how much I'm being taken advantage of by my colleagues. How management is allowing and in fact encouraging me to torture myself by taking on overtime that Occupational Health has told me I should not be doing. But the thing is ... I could technically just ... not do it. I could say, "Fuck it; you're on your own". And I probably would, except for the fucking patients.
See, I type histology reports for a living. And while some of those are absolutely routine, bog-standard stuff that shouldn't be an issue ... a lot of them aren't. They don't take out your tonsils or appendix or gallbladder unless there's something wrong. They certainly don't take off your breasts or cut out your kidneys or segments of your fucking intestines unless there's something wrong. They don't stick needles in you to take pieces of your liver or your prostate or your lungs or that weird lump on your breast, or cut off bits of skin because that mole just doesn't look right ... unless there's something potentially wrong. Nine times out of ten, they're looking for cancer.
Now, I know a lot about cancer. I've worked a few oncology departments in my time. And the main thing I know is that you have to catch it early. The sooner you catch it, the sooner it can be treated, and the sooner it's treated, the better the odds that you'll get full remission. More to the point, if you delay any of that, it might spread to another part of the body and then the odds of the patient's survival just drop into the sub-basement. The first step to catching it? Getting histology results to the right people. And even though I only do the macroscopic reports and not the microscopic ones that let you know whether a thing's malignant or not, they can't authorise a report without that information on the damn form. So, in my own small way, I am helping to save lives. That is why I do what I do. That's why I couldn't really hack anything that wasn't directly medical. Arranging the diary of the head of the Royal College of General Practitioners or handling submissions to a medical journal? Eh, I could do it, but it wasn't satisfying. I want to be helping. I want my job to mean something. And mine does.
So I answered the Reddit post with that very fact. And I got, "Well, it wouldn't be your fault if things got delayed; it'd be the boss' fault for not hiring more staff". And thankfully someone else got in before me with the reply of, "Yeah, and Thess is going to feel so much better about a patient potentially dying, potentially painfully, just because it's not technically their fault, even though they could have done something? Have some fucking empathy!" From what I can tell, half the people who read that remark of mine think I'm a hero, and the other half think I'm a doormat. I dunno; maybe both, maybe neither. I just know that reports need doing ASAP because sometimes, even a few days makes a difference.
I don't think my colleagues understand that. I don't think my colleagues let themselves understand that. They just look at it as, "They dictate, I type". I never forget that the tissue those doctors were cutting up and poking at while dictating this stuff was fairly recently attached to and/or inside of a human being, and the fact that they're getting bits cut off or out means, as I said above, that there is something potentially wrong. Best case scenario? Everything's fine, and the patient gets relief from the stress of potentially being sick a little sooner. Worst case scenario? There is a problem and the report gets to the right people quicker, and the patient stands a better chance of surviving it. Either way, it's important. What we do is important.
So I guess it's not even just work ethic, although that's a good-sized part of it. Most of all, it's making a difference, in a small way that might become something huge. And that's why I work three hours of overtime when we're this swamped.
...I just hate that my empathy and general humanity is being taken advantage of by lazy bints who only see it as "it's just a job; do the bare minimum".
7 notes
·
View notes
Text
Medical Misinformation Rating System:
1) Source(s):
A) Does the creator claim to have the credibility/knowledge to accurately disseminate the information in the post/article/reblog? (YES = 1)
Non-doctors are obviously allowed to give medical advice (and some of it can be well-informed, useful, and good)
It is fradulent to pass oneself off as a medical doctor without a practicing license. Always consider that an individual may not be a certified doctor in easy-to-manipulate and anonymous online spaces (e.g., tumblr, facebook, twitter, etc.).
If the OP has stated somewhere that they have expertise/background/experience with a field relevant to the post, then this point is given.
CRITERIA for who is judged on this point:
If the OP makes an argument and has citations, they are assessed for 1A, 2C-D, 3A-D.
If the OP makes an argument but does not have citations, they are assessed for 1A, 2C-D, 3A-D.
If the OP does not make an argument, and has citations, the primary author of the citation is assessed for 1A, 2C-D, 3A-D.
B) Does the post/article/reblog link to primary/secondary information sources (e.g., scholarly journal articles (research based), theses, dissertations, symposia and conference proceedings, interviews, and autobiographies)? (YES = 0.5) Is the information source relevant? (YES = 0.5)
Secondary information sources (e.g., textbooks, books, biographies) can also be highly authentic. It is still important to follow the same skepticism as with primary sources.
Tertiary information sources (e.g., Wikipedia, encyclopedias/dictionaries, manuals/handbooks) should really only be used as a launch-pad for further primary research.
All three sources should be properly citing primary sources in-text and on a references/bibliography/citations page (or be properly linked).
Relevancy to the topic at hand is key. A cited article could itself be authentic, but (1) be misinterpreted either on purpose or on accident, (2) irrelevant to the arguments/statements/topic, (3) be cited by mistake, or cited (4) as a means to appear more authentic.
CRITERIA for completion of 1C and 1D:
If citations are primary/secondary sources and relevant, they are assessed in 1C and 1D.
If citations are primary/secondary sources but not relevant, they are not assessed in 1C and 1D.
If citations are not primary/secondary sources and not relevant, they are not assessed in 1C and 1D.
If citations are not primary/secondary sources but are relevant, citations within the linked article/video are substitutionally assessed if the following are additionally met:
-- If the substituted citations are primary/secondary sources and relevant, they are assessed in 1C and 1D.
-- If the substituted citations are primary/secondary sources but not relevant, they are not assessed in 1C and 1D.
-- If the substituted citations are not primary/secondary sources but relevant, they are not assessed in 1C and 1D.
-- If the substituted citations are not primary/secondary sources and not relevant, they are not assessed in 1C and 1D.
If there are no further citations within the linked article/video, sections 1C and 1D are not completed.
Note that citations which are "talked about" but not cited are not assessed in 1C and 1D.
C) If the article links an information source, for one randomly selected link, does the citation come from an accredited journal (i.e., high-quality and peer-reviewed) and publisher? (YES = 0.2) Is the full-text public and available? (YES = 0.2) Does the primary author represent an accredited university/college/organization? (YES = 0.2) Does the article itself cite primary research? (YES = 0.2) Are the vibes of the article good? (YES = 0.2)
Highest ranked medical journals: The Lancet, New England Journal of Medicine, Journal of Clinical Oncology, Nature Medicine, Journal of the American Medical Association
Largest academic journal publishers: Springer, Taylor & Francis, Elsevier, Wiley, SAGE
D) If the article links an information source, for the same randomly selected link, is the citation objective and thorough? (YES = 0.25) Do the results match the conclusions drawn? (YES = 0.25) Is the research design highest standard/best practice? (YES = 0.25) Do the authors cite themselves more than expected in the body of the work? (NO = 0.25)
An overabundance of author citations is considered bad form and can often lead to bias.
Research designs can be ranked in terms of the strength of their conclusions (lowest to highest: editorials/expert opinion, case studies (with control is better), cohort studies, quasi-experiments, randomized control trials, systematic review/meta analyses).
2) Authenticity/timeliness:
A) Is the post recent (i.e., created within the last year) AND the information matches current literature? (YES = 1)
Search Google Scholar, scientific journals/publishers, and other primary sources to see if the information provided appears to match current views and beliefs.
Current posts/articles/reblogs that spread misinformation or disinformation fail this question if authentic information contradicting the post appears to be available at the time of posting.
B) Is the randomly selected citation recent (i.e., published within the last two decades) AND the information matches current literature? (YES = 1)
Ideas change over time. Sometimes what was believed to be true is no longer true.
C) Does the OP gain from the information dissemination (i.e., financially or shock value)? (NO = 1)
If the information appears to benefit the OP in some way, then red flags should be raised about its authenticity, as their interest may be more selfish than helpful.
D) Is there a statement of further inquiry? (YES = 1)
Credible sources of information often acknowledge that there is more that is not known. They will suggest questions for further research and/or to speak to a doctor/professional if you are unsure.
That being said, sometimes these statements are used as a means to avoid responsibility.
3) Emotionality:
A) Is the tone of the post/article/reblog objective? (YES = 1)
Anger indicates the reblogger/poster may have been hurt by something relevant to the content of the post. Enthusiasm could be excitement or a statement of "how could you not know this!?". Paranoia (e.g., X person/organization is trying to hide this from you) could be a sign of disinformation.
Sensational headlines or "stop scrolling and read this!" posts are intended to grab attention, the purpose being to get the information to as many readers as possible. Dig further into the information provided.
Information should be provided as objectively as possible.
B) Is there direct slander, discrimination, or hateful speech against a single individual or group of people? (NO = 1)
Generalizations, insults, and/or statements diminishing the integrity of someone(s) are inherently subjective and often indicative of poorer quality and authenticity of the information provided.
Discrimination is "unfair or prejudicial treatment of people and groups based on characteristics such as race, gender, age, or sexual orientation."
Hate can be described as abusive language, aggression (or threats), cyberbullying, personal attacks, provocation, discrimination, and/or toxic speech.
Slander can be described as statements that are false, malicious, or defamatory.
C) Are the conclusions/interpretations of the post and/or citation malicious towards a group of people? (NO = 1)
If the information serves to hurt a population, group, and/or minority (and nothing else) then it is likely to be mis- or dis-informaiton. Similarly to subjectivity and hateful speech, the information is likely intended to fuel further hurt rather than be factual.
Other problematic conclusions include claims about massive (or near-magical) changes to lifestyle (e.g., diet, sleep, exercise) to improve health or cure diseases/disorders. Trust your gut if the information feels outlandish.
D) Does the information appear to confirm an OPs preconceived bias? (NO = 1)
Ask yourself whether the information being provided aligns with how a poster might expect the world to be. Investigate the rest of their blog to see if their other posts are similar in nature.
This question is failed if the OP has posted something similar within the last 20 posts (reblogs don't count).
Confirmation bias often colours the information the OP chooses to disseminate.
You too are not immune to propaganda. Perhaps surprisingly, we are almost always biased in the information we choose to interact with (i.e., always investigate).
4) Other:
A) Is the post/article/reblog a joke? (YES = J+)
Along with tonality, it is important to recognize if a piece is a satirical or humorous work. Assess if the content is outlandish or absurd on purpose--usually for laughs.
---
Descriptive Rank Definition:
Poor: 1-3
Mediocre: 4-6
Adequate: 7-9
Excellent: 10-12
2 notes
·
View notes
Text
"This is mind-blowing.
Big Pharma is secretly “ghostwriting” articles in top medical and oncology journals to trick doctors into buying their drugs.
Here’s how the scam works:
First, pharma pays companies big money to ghostwrite studies that look legit.
Then, they approach doctors, offering them prestige in exchange for slapping their names on these ghostwritten studies.
Once published in top medical journals, these articles deceive other doctors into prescribing their drugs, believing the results are authentic.
This scheme tricks doctors into promoting treatments based on false research, driving up drug sales while putting patients at risk.
Watch Dr. Russell Blaylock explain. The “conspiracy theorists” were right again.
The pharmaceutical industry doesn’t want you healthy; it wants you sick and dependent.
Click here to watch this free docuseries (http://www.thetruthaboutcancer.tv/FOX) and discover the best ways to prevent and beat cancer in ways you’ve never been told.
Follow @VigilantFox 🦊"
1 note
·
View note
Text
Back to Life Is Really Hard (Residency Edition)
Things I've learned: I do like obstetrics. Mainly, I like that routine obstetric clinic visits are fast and easy, I like that I know how to do basic labor and triage tasks quickly and efficiently, and I like that I get to do cesarean deliveries. That being said, I think I can live without it. There's lots of confounding hours (like who's on my team, the better hours, etc), but gyne is where I'm much, much happier. And that's where I am now!! At the same time I'm trying to buckle up for MIGS applications which happen next year, and basically the advice given to me was to make peace with the numbers because it's possibly one of the most competitive fellowships across all specialties with a 50/50 chance. I'm motivated: I'm about to submit an IRB for my research project, I'm working on manuscript revisions for my med school paper, I'm involved with ACOG on a state level, I have another research project that might come to fruition, and I'm hoping to design a surgical skills curriculum for medical students. I've also started looking in-depth at away rotations for MIGS, and I'm making a spreadsheet of every program I want to apply to (so, probably 50-60 programs). But I also need to be realistic and have a Plan B, because it's a coin flip whether I match.
But to level with ya'll, despite this sliver of ambition I've regained, I'm SO depressed. Like, VERY FREAKING DEPRESSED. I'd say my mood is largely fine, but man, it is incredibly difficult to get out of bed, to be on time, want to be around my co-residents. I'm finally on weekly Prozac again, but my dose most likely needs increased. I'm also starting therapy (again) tomorrow. But it's just... hard. My life got pretty bad at the start of the year. My cat getting really sick, going into a lot of debt from vet bills and conference costs, my car getting vandalized. My oncology rotation was probably the worst I have ever performed in all of residency. I got some really, really tough feedback. It really knocked me on my ass. Things are slowly getting better, but again, I'm working against this baseline depression. The best I can describe it is just... heavy, or blurred. I lost my zest for life. It's like my life is muted.
I drew a tarot card yesterday to describe where I'm at in my life right now. I drew the 10 of Swords.
Yep. That's residency.
My tarot draws are always like this. I gravitate towards swords and cards like The Tower. It's not all bad, though. I like the concept of death, decay, and endings. I like that it creates fertile soil with which life can rise anew. Consider the artwork from the Light Seer's tarot:


We face the loss, the betrayal, the stress... whatever it is that is causing us so much pain. It will always be a part of us, but what rises up from the ashes is much brighter and stronger, "vulnerable, whole, and totally and powerfully alive."
I drew the Tower card before I drew the 10 of Swords. I like the chronology of it, too. It makes sense with the sequence of events in my life, first undergoing its major upheaval (my break-up with my fiance, moving to a new city alone, being dumped by the rebound I fell in love with, living independently for the first time in over a decade, all with the background of my chronic depression)... and then when the fire finally goes out and the dust settles... it's this empty, desiccated landscape, full of hurt and pain and loneliness. But despite all this, the sun still shines, the rain falls, and slowly life springs forth from the rot. I really resonate with cards like these, like Death, The Tower, The Fool, any card that represents endings and beginnings.
(Lol I lost my actual journal and my thoughts had to go somewhere so here we are.)
Anyway back to medicine (ugh), I'm again trying to focus on the ME outside of residency. The YA romantasy books, training for a Tough Mudder, resuming my interest in obscure non-fiction, tennis.
I'm also researching creatine??? IDK my brain is in a million places right now. My boxing class got cancelled so I biked for 40 minutes while watching 1000-lb sisters. Before I was obsessively looking up MIGS fellowship programs and I needed to get my mind OFF residency and medicine.
And since I find my mind drifting back to something that already occupies WAY TOO MUCH SPACE in my life, I'm gonna peace and work on Kingdom of Ash until I fall asleep
2 notes
·
View notes
Text

FLP BOOK OF THE DAY: The Wrong Place by Tawn Parent
On SALE now! Pre-order Price Guarantee: https://www.finishinglinepress.com/product/the-wrong-place-by-tawn-parent/
The Wrong Place attempts to answer the question: How does a #mother cope when her worst nightmare comes true? This collection of #poems and #essays chronicles the author’s journey alongside her young son as he is diagnosed and treated for a rare #cancer. Readers follow the #family as they learn the vocabulary of cancer, develop a new way of #parenting, and grieve the loss of their son’s innocence. The #family navigates endless medical procedures and hospital stays while seeking to maintain a sense of themselves outside of “cancer world.” Throughout, the author relies on humor and hope to pull her through.
A native and resident of Indianapolis, Tawn Parent has been a professional writer and editor for 30 years. Her poetry and essays have appeared in Tipton Poetry Journal, Home Planet News Online, Anti-Heroin Chic, Last Stanza Poetry Journal, and Nzuri. She has worked for various business publications, and also served as proofreader for two books.
PRAISE FOR The Wrong Place by Tawn Parent
Tawn Parent’s powerful new collection of poetry, The Wrong Place, takes us on a terrifying journey no one ever wants to take. Yet her language of careful understatement and humility and her final insights that lead to a certain wisdom, make us all the better for having done so. This is an important book that needs to be read.
–Matthew Graham, author of The Geography of Homeand 2020-23 Indiana State Poet Laureate
In The Wrong Place, Tawn Parent does what she must do: Tell the compelling story of her teen son’s treacherous cancer journey and hers as a mother by his side. “Is this my son…” she asks, “this teen…/cruising toward adulthood/suddenly entered freefall/ and landed back in my arms.” From the moment he wakes with pain to numerous treatments later, she immerses you in their lives, teetering on tears (“What’s oncology?” he asked) to welcoming relief and joy: “Here is the bell,” the nurse says, “Come ring it!” In Parent’s book, you are in the right place for insightful poems of courage and hope.
–Bonnie Maurer, author of The Reconfigured Goddess, Poems of a Breast Cancer Survivor
Tawn Parent’s The Wrong Place is required reading for anyone who has been touched by cancer. Parent’s heartfelt poems follow her journey through her young son’s diagnosis and how it affects her and her family, like when she discovers the side effects of “the five drugs/with their unpronounceable names” that may produce “red urine, red sweat … red tears” and she tries to “picture my son with red tears/coursing down his cheeks/It sounds like a horror movie.” She also learns “Parenting a child with cancer/has meant throwing out/so many rules…,” and shares with us about the first difficult Christmas. But through it all, Parent never loses her defiant humor or her unyielding hope in writing about such a difficult subject and in turn gives others a glimpse of how to cope with something so unthinkable as a child with cancer.
–Lylanne Musselman, author of It’s Not Love, Unfortunately and Staring Dementia in the Face
Please share/please repost #flpauthor #preorder #AwesomeCoverArt #poetrybook #read #poems #essays #childcancer #cancer #parenting #family
#poetry#flp authors#preorder#flp#poets on tumblr#american poets#finishing line press#small press#essays#cancer#childhood cancer
1 note
·
View note
Quote
残念です。チバユウスケさんに深く哀悼の意を表します。
食道がんも初期は症状がないことがほとんどです。進行すると食べた時のつかえ感や飲み込んだ時の胸の違和感等の症状が出て来ます。
診断は内視鏡検査により為され、特殊な色素や波長の光等を用いて食道がんを発見する技術も進歩しています。
問題なのは診断の遅れです。コロナ禍の影響をうけ食道がん等の診断が遅れていることが研究でわかっており【Journal of Clinical Oncology 41, no. 4_suppl 302-302】さらには日本の調査でも食道がんの診断が少なくなっていると明らかになり【Eur J Cancer. 2022 Apr; 165: 113–115】これは見通しが悪化する要因です。
「食道がんの主な要因は喫煙と飲酒」(国立がん研究センター)とわかっておりこれらを多く嗜む方に症状が出た場合は、早めの受診が大切でしょう。
チバユウスケさんが死去 55歳、4月に食道がん公表 元「ミッシェル・ガン・エレファント」ボーカル(スポーツ報知) - Yahoo!ニュース
2 notes
·
View notes
Last Seen Blogs


andrejkerner-blog
здравствуй, это я!

ofpackandpride
I write stuff

jagodziankamix
Bez tytułu

steveharrirngton
you weren't mine to lose