#National Institute of Allergy and Infectious Diseases (NIAID)
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Premium Tumblr themes are available from anywhere between $9 to $49.
Text
Lee Moran at HuffPost:
Then-President Donald Trump unloaded about Joe Biden and bombastically predicted he would beat his 2020 rival in a landslide in his expletive-laden last conversation with Dr. Anthony Fauci, the former longtime director of the National Institute of Allergy and Infectious Diseases revealed in his memoir.
Trump called Fauci from Air Force One on Nov. 1, 2020 — just two days before the election — in “what turned out to be” their final exchange, Fauci wrote in “On Call: A Doctor’s Journey in Public Service,” which debuted Tuesday. The Daily Beast and The New York Times shared excerpts from the book. Trump reportedly boasted to Fauci: “I am going to win this election by a fucking landslide. Just wait and see. I always did things my way. And I always win, no matter what all these other fucking people think. And that fucker Biden. He is so fucking stupid. I am going to kick his fucking ass in this election.” Trump lost the election, but continues to falsely claim it was stolen from him. Fauci served as chief medical adviser to the Biden White House until his retirement in 2022.
[...] Fauci also recalled his “first experience” of bearing the brunt of Trump’s rage during a call on June 3, 2020, when the then-president “started screaming at me” for correctly predicting immunity to coronavirus from vaccines would probably last six months to a year. Trump was furious by the implication that booster shots would likely be required after the administration of initial vaccines, which had yet to be rolled out.
Former NIAID head Dr. Anthony Fauci recounts in his newest memoir On Call: A Doctor’s Journey In Public Service that Donald Trump called Joe Biden “that fucker Biden” 2 days before the 2020 general elections and boasted about he was “going to win this election”.
From the 06.17.2024 edition of MSNBC's The Rachel Maddow Show:
youtube
#Dr. Anthony Fauci#Donald Trump#Joe Biden#On Call: A Doctor’s Journey In Public Service#Coronavirus#Pandemics#2020 Presidential Election#2020 Elections#National Institute of Allergy and Infectious Diseases#NIAID#MSNBC#The Rachel Maddow Show#Coronavirus Vaccines
4 notes
·
View notes
Text
We're Having A COVID Summer Surge. Should You Get The Updated Vaccines Now?
The FDA Just Approved an Updated Vaccines, and Officials Say Paxlovid is Still Effective in Preventing Severe Cases.
— By Sanjay Mishra | August 22, 2024

A Colorized Ccanning Electron Micrograph of a Cell (Blue) Infected with the Omicron Strain of the SARS-CoV-2 virus (Yellow). Micrograph By National Institute of Allergy and Infectious Diseases (NIAID)/National Institutes Of Health/Science Photo Library
The summer of 2024—the fifth since the COVID-19 pandemic began—is projected to be the biggest summer wave of COVID infections to date.
Since early May, COVID infections have steadily increased in the United States, Europe, Singapore, New Zealand, and Australia. The U.S. Centers for Disease Control and Prevention estimates that COVID-19 infections are currently increasing in 25 states based on data from emergency department visits. However, hospitalizations and deaths from COVID remain at their lowest levels.
Now, the U.S. Food and Drug Administration has approved updated vaccines to protect against current variants of the virus.
This recent surge has been driven mainly by a new group of closely related Covid subvariants, known collectively as "FLiRT."
As the summer winds down, students across the U.S. will return to school. Traditionally, this also coincides with the season of respiratory viruses, such as flu, RSV, and increasingly COVID.
"Not sure what will happen this fall and winter," says Kei Sato, a virologist at the University of Tokyo. While the FLiRT variants are likely to keep evolving after summer, entirely new subvariants cannot be ruled out. "An Omicron-like event” seems to have occurred every year in the fall since 2021, says Sato.
Here's what you need to know about the new variants and the new vaccines.
What Are FLiRT Variants?
The "FLiRT" variant family includes the majority of currently circulating variants, identified with the letters KP, JN, and the variant LB.1.
The unofficial name "FLiRT" is an acronym for a set of mutations on the spike protein of SARS-CoV-2, the virus that causes COVID-19. The virus uses spike protein to bind with ACE2 receptors in our nose and lung cells to cause infection.
All proteins are made up of amino acids that string together like beads. Mutations can change one amino acid to another, thereby altering the behavior of the protein and making the virus more or less infectious, or able to dodge immunity.
The FLiRT subvariant family members are descended from the JN.1 variant that was dominant in the U.S. in early 2024. JN.1 itself was highly unusual because it acquired 41 mutations that differentiated it from Omicron XBB.1.5, which is the variant upon which the current bivalent COVID booster is based.
Should You Get The New Vaccines?
The two updated mRNA vaccines, manufactured by Pfizer-BioNTech and Moderna, target a FLiRT variant called KP.2. Anyone over the age of 12 can get the new shots, as long as they haven't received a booster in the last two months.
“Vaccination continues to be the cornerstone of COVID-19 prevention,” Peter Marks, director of the FDA’s Center for Biologics Evaluation and Research said in a statement.
Another vaccine targeting the variant JN.1 and manufactured by Novovax is also under review and could be approved soon.
Previous research also showed that older vaccines based on XBB.1.5, an earlier subvariant of Omicron, were still effective in preventing severe COVID-19. While this vaccine produces antibodies that still target the FLiRT variants, the efficiency is notably reduced. A recent infection from the JN.1 variant also seems to provide strong protection against all the FLiRT variants.
That said, the CDC recommends that everyone six months and older get a COVID vaccine. Those at high risk for serious COVID-19 should get vaccinated with the most recent versions available.
How Alarming Are FLiRT Variants?
Coronaviruses, such as SARS-CoV-2, frequently mutate to avoid recognition by antibodies. The two FLiRT mutations remove the sites on the virus where antibodies bind the SARS-CoV-2 virus.
Additional mutations on the FLiRT variants can either help the virus bind more efficiently to ACE2 receptors making it more infectious, help it evade previous immunity, or both, says Adrian Esterman, an epidemiologist at the University of South Australia, Allied Health & Human Performance in Adelaide, Australia
Early studies show that all existing FLiRT subvariants are very good at dodging previous immunity acquired through multiple COVID vaccinations—including the most recent COVID bivalent booster—or a breakthrough infection from a previous strain of Omicron.
But the good news is that by escaping the antibodies, the FLiRT variants have also seem to lost some ability to infect their target because the virus needed the original antibody-binding sites to bind the ACE2 receptor and enter cells.
"These variants are not yet particularly concerning, even with the new mutations that affect certain aspects of the virus's biology," says Shan-Lu Liu, a virologist at the Ohio State University.
It is common for viruses to acquire mutations that help them dodge immunity, which can affect their ability to infect cells, says Liu. "The viruses can quickly evolve new mutations to restore their infectivity."
But in the meantime, Sato thinks that waning immunity from previous vaccinations and infections, coupled with the FLiRT variant's ability to dodge remaining immunity, are probably the main reason for the recent surge in infections.
Liu also agrees that the currently rising numbers of COVID infections are mostly due to low booster uptake and increased summer travel.
Are COVID Medicines Still Effective?
Emergency department visits, hospitalizations, and deaths have all spiked during this summer but are still much lower compared to earlier waves of the pandemic.
There is no indication that these new FLiRT variants are more dangerous than other Omicron strains.
A study shows that Paxlovid is still effective against FLiRT variants. Other antiviral drugs such as molnupiravir and remdesivir are also expected to work since their mechanism of action is not affected by mutations in the spike protein.
#COVID#Summer Surge#Updated Vaccines#Paxlovid | Very Affective#Food and Drug Administration (FDA)#Corona Virus 🦠#Respiratory System#Immune System#Vaccination#Medicine 💊#National Institute of Allergy and Infectious Diseases (NIAID)
2 notes
·
View notes
Text
CHOP Researchers Identify Molecules that Optimize Immune Presentation of Antigens across the Human Population
Newswise — Philadelphia, February 24, 2023—Researchers at Children’s Hospital of Philadelphia (CHOP) have identified variants of a chaperone molecule that optimizes the binding and presentation of foreign antigens across the human population, which could open the door to numerous applications where robust presentation to the immune system is important, including cell therapy and immunization. The…
View On WordPress
#All Journal News#Cell Biology#chaperone molecules;chaperone proteins;major histocompatibility complex;MHC class I;immunogenecity;Antigen Presenting;Cell Therapy;Immunizat#children#Embargoed Feed - hidden#Immunology#National Institute of Allergy and Infectious Diseases (NIAID)#National Institute of General Medical Sciences (NIGMS)#Newswise
0 notes
Text
Also preserved in our archive
by JANA ZAHLAN
In the early days of the COVID-19 pandemic, the phrase “herd immunity” spread rapidly and highlighted America’s hope for a quick end to the emerging event.
According to the World Health Organization (WHO), herd immunity is “the indirect protection from an infectious disease that happens when a population is immune either through vaccination or immunity developed through previous infection.”
While many people have been either infected, vaccinated, or both, this does not provide the same protection from COVID-19 that it might from other infectious diseases. Experts recommend taking additional steps, rather than depending on herd immunity, to stay safe from the harmful effects of COVID-19.
Dr. Luca Giurgea, a physician scientist at the National Institutes of Health (NIH) and National Institute of Allergy and Infectious Diseases (NIAID), discussed the concept of herd immunity with the AmNews: “With COVID, there’s a few assumptions that need to hold true for this herd immunity concept to work out …. I don’t really like applying the herd immunity concept to COVID … because I think, particularly in the general population, [it] comes with certain expectations that will disappointingly not be met.”
While herd immunity has successfully protected populations from other infectious diseases, such as measles and smallpox, all efforts to stop the SARS-CoV-2 virus — the virus behind COVID-19 — from spreading have fallen short. According to Giurgea, immune responses against this virus, whether achieved through vaccination or a previous infection, subside with time. Additionally, the ability of the virus to mutate allows it to evade these immune responses and continue to spread in the population.
(At the full link is an embedded list of long covid symptoms if you'd like to browse them)
Despite the efforts of public health officials to relay this information to the public, myths and misconceptions about COVID-19 herd immunity continue to influence opinions and decisions about protective measures, such as social distancing, masking, and vaccinations. To better understand the reason behind these misconceptions, the AmNews spoke with Dr. Lauren Ancel Meyers, an epidemic computational epidemiologist and professor at the University of Texas at Austin.
Asked about belief in herd immunity as a reason to abandon COVID-19 protective measures, Ancel Myers said there is a “misunderstanding of what herd immunity is … The technical meaning of herd immunity means … a large fraction [of the population] have gotten it. [That there is] a lot of immunity in the population, so it’s going to stop spreading [until] we’re done with it, and clearly, we are not in that universe at all.”
Ancel Myers said there may be a need for a new term that captures the change in perceived COVID-19 risk over the course of the pandemic and reduces confusion about the concept of herd immunity.
“We do have more immunity in the population because people have gotten infected, because people have gotten vaccinated now multiple times … and that has, indeed, made the virus less severe … but it’s not stopping it from spreading, so we don’t have herd immunity,” Ancel Myers said. “… the threat is different than it was early on, and that is in part because of immunity.”
Echoing this notion, Giurgea emphasized the benefits of keeping up with yearly vaccine boosters. Research has demonstrated the role of vaccines in reducing the number of hospitalizations, deaths, and Intensive Care Unit admissions after COVID-19 infection in vulnerable patient populations. COVID-19 vaccines also have been shown to protect infected individuals from long-term health problems, generally referred to as Long Covid.
Immunity does not have to be perfect to be beneficial. “Even though we might not get to the point of eradicating COVID altogether … the more immunity we have in the population … the slower the virus is going to spread and the less likely any one of us is to get infected or end up in the hospital,” Ancel Myers said. “Even if we can’t achieve … this aspirational target of reaching herd immunity, there is still a huge amount of public health benefit to increasing immunity in the population through vaccination.”
For additional resources about COVID-19, visit www1.nyc.gov/site/coronavirus/index.page or call 311. COVID-19 testing, masks, and vaccination resources can also be accessed on the AmNews COVID-19 page: www.amsterdamnews.com/covid/. To get free COVID tests, visit the City of New York’s webpage and the NY Health and Hospitals webpage.
#mask up#covid#pandemic#wear a mask#public health#wear a respirator#covid 19#still coviding#coronavirus#sars cov 2
64 notes
·
View notes
Text
Think Fauci torturing and killing dogs is bad? Wait till you learn what he did to orphaned kids in NYC for HIV "research".
In New York’s Washington Heights is a 4-story brick building called Incarnation Children’s Center (ICC). This former convent houses a revolving stable of children who’ve been removed from their own homes by the Agency for Child Services. These children are black, Hispanic and poor. Many of their mothers had a history of drug abuse and have died. Once taken into ICC, the children become subjects of drug trials sponsored by NIAID (National Institute of Allergies and Infectious Disease, a division of the NIH), NICHD (the National Institute of Child Health and Human Development) in conjunction with some of the world’s largest pharmaceutical companies – GlaxoSmithKline, Pfizer, Genentech, Chiron/Biocine and others.
I have seen and saved a couple of photos, but I can't post them here. It would be grounds for me to be instantly deactivated. What these soulless entities have done to children is beyond evil‼️ And that's putting it mildly 🤔
#pay attention#educate yourselves#educate yourself#knowledge is power#reeducate yourself#reeducate yourselves#think about it#think for yourselves#think for yourself#do your homework#do your own research#do some research#ask yourself questions#question everything#save the children#save our children#save humanity#crimes against humanity#crimes against children#evil#news
54 notes
·
View notes
Text
by Maryanne Demasi, PhD
An explosive new study conducted within the U.S. Food and Drug Administration’s (FDA) own laboratory has revealed excessively high levels of DNA contamination in Pfizer’s mRNA COVID-19 vaccine.
Tests conducted at the FDA’s White Oak Campus in Maryland found that residual DNA levels exceeded regulatory safety limits by 6 to 470 times.
The study was undertaken by student researchers under the supervision of FDA scientists. The vaccine vials were sourced from BEI Resources, a trusted supplier affiliated with the National Institute of Allergy and Infectious Diseases (NIAID), previously headed by Anthony Fauci.
Recently published in the Journal of High School Science, the peer-reviewed study challenges years of dismissals by regulatory authorities, who had previously labelled concerns about excessive DNA contamination as baseless.
The FDA is expected to comment on the findings this week. However, the agency has yet to issue a public alert, recall the affected batches, or explain how vials exceeding safety standards were allowed to reach the market.
8 notes
·
View notes
Text
Fwd: Research Technician Job: UConnecticut.ResTechAnimalCare
Begin forwarded message: > From: [email protected] > Subject: Research Technician Job: UConnecticut.ResTechAnimalCare > Date: 6 September 2024 at 06:47:34 BST > To: [email protected] > > > The University of Connecticut is searching for a full-time lab research > technician, to work in Dr. Daniel Bolnick’s lab group in the Department > of Ecology and Evolutionary Biology, on the evolutionary genetics of > fish immunity to tapeworm parasites. > > The primary responsibility of the technician will be to run the lab’s > fish colony of threespine stickleback. Secondary responsibilities include > assisting with laboratory experiments, and lab management tasks. This > position is funded by a National Institute of Allergy and Infectious > Disease (NIAID) grant to map the genetic basis of differences in immunity > between natural populations of fish, and differences in immune suppression > between populations of tapeworm parasites. > > Tasks: Animal colony management includes feeding fish, aquarium system > maintenance, monitoring fish health, record keeping, and breeding lab > animals. The technician will also supervise and coordinate other lab > members who contribute fish care help. Secondary responsibilities > related to the fish colony will be to collaborate with lab members > doing laboratory experiments (e.g., vaccination assays) and associated > laboratory work. In addition the technician will help with general lab > management including purchasing lab supplies for lab members, ensuring > safety compliance, and helping to keep the lab organized. > > Minimum Qualifications: Applicants must be have an undergraduate degree > (BSc or BA) in biology or a related field. They must be organized and > reliable and have the ability to carry out independent laboratory research > and fish care protocols after initial training. Previous educational > experience and work records should demonstrate a good work ethic, > organizational ability, and interest in scientific research. > > Preferred Qualifications: Experience with animal care is strongly > preferred. Prior experience with care of fish or other aquatic organisms > is especially valuable. Some prior experience with laboratory research > such as (but not limited to) molecular genetics, immunology, or cell > biology, is helpful but not required. > > Start date and duration: The position is available to begin as early > as September 16, and we would prefer candidates who could begin before > October 1. The position will begin with a one year appointment subject > to renewal for up to four years. The position might be extended for > additional years beyond four, if additional grants are funded. > > Salary is expected to be between $38,000-$45,000 per year depending > on qualifications. > > Applicants should electronically submit a single pdf file containing the > following in order: > > 1. Cover letter (1 – 2 pages), including summary of relevant > job experience, research experience, career goals, and how > this position fits your career plans. > > 2. CV > > 3. List of two (or three?) references, with contact information > (email, telephone and mailing address) > > We will request letters directly from these references, after identifying > top candidates. > > The application pdf file should be emailed to Dr. Daniel Bolnick > ([email protected]). Include the subject line “Fish Care > Technician Application:
2 notes
·
View notes
Text
richard henry creel is really such a character. Such a character.
so, quick summary, in one of the newspaper articles there’s a mention of someone names richard brenner

found by @aemiron-main
richard brenner is listed as the head of the Narcotic Enforcement Division from 1954-1971
richard henry creel is the son of virginia fackle creel and henry clay creel. im sure the connection is obvious
anyway, when we look into who this richard henry creel guy was, we learn that he was the assistant surgeon general of the U.S. public health service, and to become this head he’d have to have had specialized training or significant experience in public health. so, this guy was heavily involved in this stuff, though his exact service starts in 1921 but the end is never specified
under the PHS, the, “The Division of Venereal Diseases was established in 1918, and the Narcotics Division in 1929 (it eventually became the National Institute of Mental Health).”
now, richard henry creel was born in 1878 — he would’ve been in his 50’s by the time the narcotics division was actually created
1955 - “The National Microbiological Institute became the National Institute of Allergy and Infectious Diseases (NIAID) by order of the Surgeon General on December 29. The Biologics Control Laboratory was detached from the institute and expanded to division status within NIH.”
1957 - “The Center for Aging Research was established November 27 as the focal center for NIH extramural activities in gerontology.”
1958 - “On July 16 the Division of General Medical Sciences was established by order of the Surgeon General, extending research into noncategorical areas covered until that time by the Division of Research Grants. The Center for Aging Research was transferred from the National Heart Institute to the Division of General Medical Sciences on November 4.”
1962 - “Five acres of land for a Gerontology Research Center were donated by the City of Baltimore in December.”
1963 - “The National Institute of Child Health and Human Development and the National Institute of General Medical Sciences were established on January 30. The Center for Research in Child Health and the Center for Research in Aging (established in 1956) were transferred from NIGMS to NICHD.”
1967 - “The National Institute of Mental Health [narcotics division] was separated from NIH and raised to bureau status in PHS by a reorganization that became effective January 1.“
1971 - “The White House Conference on Aging recommended creating a separate National Institute on Aging on December 2.”
source
now that’s a lot of words and moving and bullshit, so here’s the most important stuff to know.
richard henry creel was appointed assistant general surgeon in 1921, and 8 years later the Narcotics Division was formed. the surgeon general he was serving served from 1920 to 1936 — it isn’t much of a reach to say he was probably involved in the creation of this division
now, richard brenner was supposedly the head of the Narcotics Enforcement Division from 1954 to 1971. during that time, the narcotics division was brought up to bureau status, putting it at rank with programs like the FBI and an entire institute dedicated to researching the effects of aging were created, merging aging research with child health research
all of this stuff has roots in the PHS, and the PHS’ biggest start up was chemical research. all of this gets rooted back to chemical research
so, when we look at it, we can see that the same year the institute on aging was created, richard brenner was resigned and richard creel died. this was the year that all the main kids were born, most importantly el and will
i’d also like to point out the center of aging stuff began about two years before henry was taken by brenner. that would be when henry was 10, and i believe that that was the year henry moved to hawkins (trust in @laozuspo) and it was only a year after richard brenner had gotten involved with the narcotics division
what could this all be pointing to? well, both em and james have been feeding me stuff about henry’s regeneration abilities. more importantly, how they resemble cancer. what i didn’t include in the info from 1955 is that the first ever cancer chemotherapy center was established — the same year the Biologics Control Laboratory was given its own division. the BCL explored viral diseases and produced vaccines. the word ‘sick’ in the show has prominent value on a deeper level, as stav has explained, but if we take it more surface level…
ALL i’m saying is that a ton of this stuff lines up. i don’t have a clear answer as to what exactly it means or how we got from A to B for sure, but it seems a lot like this richard character was interested in henry’s cancer-like regeneration abilities. possibly even in an attempt to prevent the process of aging. maybe, just maybe, richard brenner, richard henry creel, and martin brenner aren’t all that different *wink wink*
#at least this is what i’ve found so far#i’m still digging but i need to get this out of my head so i can focus on the other stuff i’m supposed to be working on#like. i shouldn’t be focusing on this or virginia fackle creel’s garden i have 3 different posts im supposed to be making and a fic#but . But this is so#richard brenner#martin brenner#richard henry creel
49 notes
·
View notes
Text
Incredibile: Fauci ha nascosto i piani per potenziare il virus del vaiolo delle scimmie, rendendolo molto più mortale
Secondo la Commissione energia e commercio della Camera dei rappresentanti USA Fauci aveva piani segreti per uno studio di guadagno funzionale del Vaiolo delle Scimmie, con il rischio di causare una vera epidemia ad alta mortalità.
Per quasi nove anni, l’Istituto di Anthony Fauci ha nascosto i piani per progettare un virus mpox, cioè il vaiolo delle scimmie, in grado di provocare una pandemia, con un tasso di mortalità fino al 15 percento, come hanno rivelato i membri di una commissione inquirente del Congresso degli Stati Uniti in un nuovo rapporto martedì 11 giugno.
Nel giugno 2015, uno scienziato del National Institute of Allergy and Infectious Diseases (NIAID) ha ricevuto l’approvazione formale da parte del National Institutes of Health’s Institutional Review Board per gli esperimenti che avrebbero dovuto progettare un virus mpox con alta trasmissibilità e moderata mortalità.
Ecco perchè i virologi marchettari continuano ad allarmare: "Vedrete il prossimo virus! Sarà una teraggeddia". Perchè LO SANNO che è in preparazione da anni.
L'articolo completo su Scenari Economici
4 notes
·
View notes
Photo
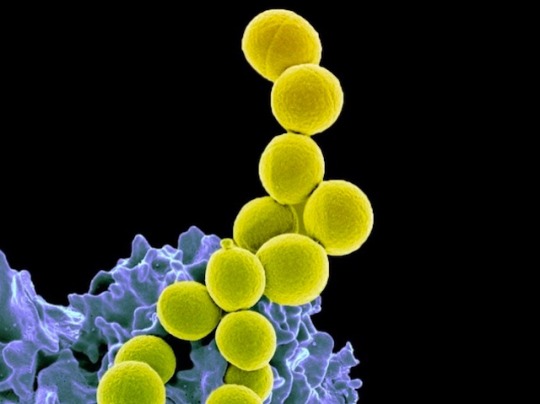
Potential Pathogen
These yellow spheres are Staphylococcus aureus bacteria on the surface of a human immune cell (blue). They are found in, and on, about a third of the human population and are generally harmless except, that is, for when they’re not. S. aureus can cause severe and potentially fatal infections of the skin, soft tissues, bone and blood, and especially dangerous are the drug-resistant strains – so called, methicillin-resistant S. aureus (MRSA). The bacteria were thought to mainly inhabit the skin and nose, but recent research shows they are most abundant in the gut. This discovery led researchers to test whether probiotics – oral doses of friendly bacteria – could suppress S. aureus colonisation. And they could – by around ninety-five percent. Probiotics work more slowly than traditional antibiotics for tackling infections, but they can be taken for much longer without harm, and will likely be able to tackle MRSA strains when regular drugs cannot.
Written by Ruth Williams
Image from the NIH, National Institute of Allergy and Infectious Diseases (NIAID), Bethesda MD, USA
Research by Pipat Piewngam & Sunisa Khongthong, et al, NIAID and Rajamangala University of Technology Srivijaya, Thailand
Image in the Public Domain
Research published in Lancet Microbe, January 2023
You can also follow BPoD on Instagram, Twitter and Facebook
#science#biomedicine#staphlococcus aureus#staph aureus#bacterial infections#mrsa#antibiotic resistance#probiotics#electron microscopy
34 notes
·
View notes
Text
Judicial Watch announced recently it received 5 pages of records from the Federal Bureau of Investigation (FBI) in a Freedom of Information Act (FOIA) request that show an April 2020 email exchange with several officials in the bureau’s Newark Field Office referring to Dr. Anthony Fauci’s National Institute of Allergies and Infectious Diseases (NIAID) grant to the Wuhan Institute of Virology (WIV) in China as including “gain-of-function research” which “would leave no signature of purposeful human manipulation.”
2 notes
·
View notes
Text
Dr. McCullough nomme les quatre principales personnes coupables de crimes contre l'humanité
1.) Dr. Anthony Fauci, Former Director of the National Institute of Allergy and Infectious Diseases (NIAID).
2.) Dr. Ralph Baric, Prof à la University of North Carolina at Chapel Hill
3.) Peter Daszak, President du EcoHealth Alliance.
4.) Dr. Shi Zhengli, virologue en chef du Wuhan Institute of Virology de Wuhan, Chine.
Autres nouvelles sur @Vigilant_News:
Suivez @VigilantFox 🦊
#big pharma est toujours en bonne santé#big pharmla#covid&corruption#covid de sens#covid au cerveau#mon ministre est sinistre
3 notes
·
View notes
Text
A Promising Vaccine Candidate Against Lassa Virus
Researchers from the Texas Biomedical Research Institute (Texas Biomed), The Scripps Research Institute, and the National Institute of Allergy and Infectious Diseases (NIAID) have developed a vaccine candidate for Lassa virus that successfully protected guinea pigs from an otherwise lethal dose of the virus. Their findings were recently published in npj Vaccines.
Lassa virus, which currently has no approved vaccine or cure, causes tens to hundreds of thousands of cases of Lassa fever each year. The virus is transmitted to humans through contact with food or surfaces contaminated by infected rodents. While many individuals experience no symptoms, the virus can lead to severe illness, including fever, heavy bleeding, and organ failure, often within two weeks of infection. Fatality rates are estimated to range between 15% and 20%.
0 notes
Text
Also preserved on our archive
By Julia Doubleday
This week, the head of the National Institute of Allergy and Infectious Diseases (NIAID), Jeanne Marrazzo, sat down with Stat News to discuss succeeding Anthony Fauci amid public concerns over ongoing H5N1 and mpox outbreaks.
The conversation yielded a staggering admission from Dr. Marrazzo as she downplayed risks of a bird flu pandemic:
"Can I make a quick digression? We recently had a long Covid [research] meeting where we had about 200 people, in person. And we can’t mandate mask-wearing, because it’s federal property. But there was a fair amount of disturbance that we couldn’t, and people weren’t wearing masks, and one person accused us of committing a microaggression by not wearing masks. And I take that very seriously. But I thought to myself, it’s more that people just want to live a normal life. We really don’t want to go back. It was so painful. We’re still all traumatized. Let’s be honest about that. None of us are over it."
This jaw-dropping justification is perhaps more jaw-dropping given that Dr. Marrazzo was not asked to comment on the meeting but broached the topic herself. Her statement clarifies that she and other public health officials don’t wear masks because they find basic disease control to be psychologically triggering. Let’s unpack the layers of anti-science, anti-patient, anti-public health and anti-reality rhetoric - not to mention rancid ableism- in this statement.
First let’s consider the context. Dr. Marrazzo is not referring to masking generally, although any public health official who is informed about the cumulative risks of COVID infections like long-term disability and brain damage should be. She is specifically justifying a refusal to mask at a Long COVID research meeting.
The RECOVER-TLC meeting in Bethesda at the end of September gathered hundreds of scientists, medical professionals and patients to discuss Long COVID. What is Long COVID? Let’s use the definition offered in a recent review article published in Nature Medicine:
"Long COVID represents the constellation of post-acute and long-term health effects caused by SARS-CoV-2 infection; it is a complex, multisystem disorder that can affect nearly every organ system and can be severely disabling. The cumulative global incidence of long COVID is around 400 million individuals, which is estimated to have an annual economic impact of approximately $1 trillion—equivalent to about 1% of the global economy. Several mechanistic pathways are implicated in long COVID, including viral persistence, immune dysregulation, mitochondrial dysfunction, complement dysregulation, endothelial inflammation and microbiome dysbiosis."
In other words, a quite serious, quite common outcome of SARS-COV-2 infection with a multitude of physical markers, poised to drastically disrupt world economies. Even after vaccination, Long COVID risk remained around 3-4% in a recent study. Long COVID can follow any COVID infection and affect anyone, and risks are known to be cumulative. That means reinfections continue to raise your risk of developing Long COVID. COVID is an airborne virus, transmitted by sharing air with infected individuals.
To debunk several misapprehensions, there is no special kind of person who gets Long COVID. There is, conversely, no special, “healthy” kind of person who cannot develop Long COVID. A person who has had COVID three times and feels okay is not now “immune” to Long COVID. No one has long-term immunity to COVID, and vaccinations can reduce the risk of, but not entirely prevent, COVID infections. COVID spreads in our communities at high rates year-round, with late-September wastewater data showing about half a million cases per day, or one in 57 Americans infected.
But experts gathering at a meeting about Long COVID should be well aware of all of the above.
In year five of the ongoing COVID pandemic, we have plenty of tools to ensure that a meeting- even an indoor, in-person meeting- remains safe for all attendees. Mitigation measures that would have reduced the risk of COVID transmission include adequate ventilation, CO2 monitoring, HEPA filtration, on site testing, Far UVC technology, and- of course- the use of high-quality, respirator style masks. While patients were easy to identify in respirators, many of the government officials and scientists who spoke plainly chose to make the space more dangerous for people with Long COVID.
The Sick Times noted that the lack of accessibility, the risk of reinfection for patient attendees paired with a poor-quality livestream, undercut the meeting’s message of urgency and care around the treatment of Long COVID.
Meetings among experts could easily serve as a gold standard for airborne disease mitigation, modeling how to prevent infections and therefore, inevitably, more Long COVID cases. Airborne disease mitigation could and should be the first line of defense against Long COVID; it is the one and only tool we have that is proven to be effective vs the little-understood disease. This is especially important at this early stage, when treatments are so limited, with no proven path to recovery and certainly no “cure”.
But Dr. Marrazzo and her colleagues, instead of focusing on how to halt the spread of COVID at their Long COVID research meeting, are focused on how to preserve their psychological denial that they, personally, are special people who are not at risk of developing Long COVID.
There is no scientific basis for this idea; it is the fantasy of the crowd, the collective delusion of people much less informed than they are, who are desperate to resume pre-pandemic life and have been fed years of propaganda about COVID’s supposed harmlessness. To participate in this public delusion rather than attempt to pop it is a social decision, not a scientific one. Marrazzo’s statement admits as much.
Marrazzo notes that there was a “fair amount of disturbance” that researchers continue to refuse to mitigate COVID while claiming to want to address the Long COVID crisis. She goes on to state that “one person” accused the group of “committing a microaggression” by not wearing masks, obliquely referring to longtime HIV/AIDS and COVID activist JD Davids. But Davids was far from the only activist angry with the lack of mitigations.
Long COVID patients have been exceedingly clear, for months and years, about their ongoing anger that even doctors explicitly engaged in COVID work refuse to practice mitigations. This failure to mitigate is violence that very literally harms, disables and kills people.
Long COVID patients participating in medical studies like this one at Stanford have been forced to drop out of critical research projects due to staff’s refusal to mask, take airborne precautions, and provide protection from reinfection in dangerous healthcare facilities.
Twitter user Michael Coyle stated in February 2023 that, “my partner and I have both dropped out of a multi-decade (longitudinal) health study, and I dropped out of a COVID transplant study because they weren't taking airborne precautions.”
In July of this year, Jordan Crane wrote, “I have had to withdraw from the Stronger study run by @georgeinstitute in collaboration with @monashuni, 11 months in. LC patients should not be exposed to reinfection during trials aimed at helping those with LC, but that's exactly what @monashuni are doing.”
This is not only immoral, it is bad science; if research teams reinfect Long COVID patients, as well as potentially infecting control subjects, any purported results of said studies would be corrupted and invalid.
If the public at large can claim ignorance- they have, after all, been repeatedly told that risks of COVID infection are minimal and comparable to other common viruses- public health officials have no such excuse.
And why is it, by the way, that the public is so certain that repeated, continual infection with COVID-19 will not harm them? Could it have something to do with the fact that researchers, doctors and public health officials continue to appear in public unmasked, clearly communicating that continual reinfections are safe and nothing to fear?
NIAID officials and other health professionals masking at a large, indoor meeting serves multiple critical public health purposes: one, it avoids spreading the virus, which would create new Long COVID cases. Two, it conveys to the public that SARS-COV-2 infections are not harmless, that Long COVID is serious and can develop from any case of COVID. And three, it expresses that prevention is the most vital- and really, the only- tool we currently have to effectively fight Long COVID.
Marrazzo states that she took public criticism of the lack of masks “seriously”. She then goes on to provide an entirely unserious response, dismissing said criticism by whining, “people just want to live a normal life.”
What, exactly, is meant by this? What population is seen as “people”, who is excluded, and what is “normal” in the construction of this odd sentence?
Quite clearly, Marrazzo and her colleagues do not want to live the life Long COVID patients and other disabled people are now forced to live- a life of continual infection avoidance. They do not want to wear masks, be associated with those who wear masks, be seen as “disabled,” as “other,” as “sick,” “vulnerable” or “abnormal”. They want to be normal- in other words, abled and ableist.
They do not want to be stigmatized, like the abnormal patients they claim to serve.
They do not want to stand out from the crowd of abled people who are healthy enough to tolerate another COVID infection- the “normal” people who aren’t annoying or weird or old or sick or dying.
Like normal (abled) people, they want to spread COVID in peace, while pretending they do not know the damage it inflicts. Like normal people, they want to use conferences as an opportunity to have their photos taken and network over cocktails. Like all the normal people who continue to exclude Long COVID patients from public spaces, these officials, too, will not be making it any easier for sick people to be safe outside their homes. Like normal people, they are going to operate under the assumption that Long COVID and disability cannot happen to them.
Because no study, no statistic, no patient, and no research can educate a medical professional out of ableism, the unmasked people who attended this meeting have all the information in front of them, and yet cannot understand that they, too, are at risk of disability.
Marrazzo goes on to say that she and her colleagues “don’t want to go back” because “it was so painful.” What was? Disease control? The thing public health literally exists to do? Because COVID is still very much with us - 1 in 57 Americans currently positive, you recall? Long COVID patients, disabled people, and people who are avoiding infection do not have any choice but to practice mitigations, and to do so with extreme strictness, given the lack of any coordinated disease control coming from the top. Every day, this task is made harder by the abdication of public health leaders who prioritize the comfort of the most privileged over the safety of the most vulnerable.
Patients are not merely harmed by the superspreader events Marrazzo and her colleagues continue to hold- although they and surrounding communities certainly are harmed by the spread of the virus itself- they are also harmed by the blasé attitude of officials which leads the families and friends of Long COVID patients to doubt the seriousness of their condition, or the need for precautions. Long COVID patients are unsafe in their own homes because masking has been so stigmatized that their own spouses, parents, and children will not stop reinfecting them.
If the head of the NIAID declares that she cannot wear a mask because she wants to be “normal,” what hope does an ill patient have to convince her husband to buck the social, political and professional pressure he faces in public life to consistently mask? When the very public health leaders who should be stressing the importance of tools that prevent reinfections are stigmatizing them, framing them as weird, abnormal and scary?
Lastly Marrazzo insists that researchers cannot wear masks because “we’re still all traumatized,” and “none of us are over it.”
A moment for the absurdity of the statement that you cannot use a safety tool that very literally saved lives during a traumatic event because you’re psychologically triggered by it. It is akin to saying you can’t wear a seatbelt because you were in a bad car accident and people died. Go to therapy. Wear the seatbelt. Definitely do not project your personal psychological problem with seatbelts onto the people fighting for auto safety.
Watching people get infected and die during a pandemic is certainly traumatizing. But…masks didn’t do that. SARS-COV-2 did. The same virus you’re spreading when you refuse to acknowledge and mitigate it, despite being well-aware of the long-term and cumulative harms of continual reinfections. By claiming the mask is triggering your trauma by reminding you of COVID, you are essentially saying that you exist in a state of utter denial that COVID currently surrounds you.
It’s doubly astounding to dare use the word “trauma” to describe the relationship of health officials toward masks while dismissing the trauma of patients being gaslit, ignored, further disabled, and forcibly reinfected by society at large- all while those who claim to want to heal them participate in stigmatizing the best prevention tool available.
Long COVID patients are traumatized by their illness, their abandonment, their social stigmatization, the relationships they continue to lose, in many cases the loss of careers and homes, and their utter exclusion from public life. Public health officials are not “traumatized” by having to mitigate the disease that inflicted and continues to inflict all of those actual traumas.
There is a social and cultural problem within public health institutions regarding airborne disease control. Broader social norms of ignorance and denial of the virus’s harms- which were themselves seeded by mainstream politicians and media, whose rhetoric was in turn cribbed from far-right libertarian thinktanks- have been absorbed into medical and public health settings.
The stigmatization of masking certainly began on the far right, but as Biden’s administration sought to normalize recurrent COVID reinfections and push people “back to normal,” Democrats joined in on the political project to socially destroy the tool humans would have killed for in centuries past. To be able to make use of respirators is not a burden or traumatic- it is a gift, not to mention a privilege that many around the world cannot access. People gathering for a Long COVID meeting should be all the more grateful, knowing full well the outsize outcomes such a small device can prevent.
It is a shame, a failure, and a shock to hear a public health official with so much power contribute to anti-mask sentiment amidst spreading mask bans which will kill disabled people. At a time when public health should be educating the public about the importance of mitigation, stressing the value of these tools, people in power are declaring masks weird and abnormal, contributing to further stigmatization of those who need these devices to even enter public spaces.
It is shockingly anti-science to hear a public health official disparage disease control technology at the altar of fascist social norms that seek to disappear disabled people from public entirely.
Dr. Marrazzo’s words reveal that she does not identify with Long COVID patients, nor does she see them as “people” who deserve to be a part of “normal” life. Only the able-bodied- those who have not yet been disabled by COVID- have a right to “normal,” which is defined by the disappearance of accessibility, disease mitigation, and medical devices. Trauma is not what has been and continues to be inflicted on those most harmed by COVID, it is what is experienced when a doctor sees a mask and, for just a second, remembers what it felt like to be scared, to feel vulnerable, to feel like maybe illness and death weren’t things that come only for the weak, the lesser, and the old.
But those days are over.
#long covid#covid conscious#mask up#covid#pandemic#covid 19#wear a mask#public health#coronavirus#sars cov 2#still coviding#wear a respirator#covid is airborne#covid isn't over
66 notes
·
View notes
Text

Happy birthday to Anthony Fauci, who was born on this day in 1940.
known as an American physician-scientist and immunologist who served as the director of the National Institute of Allergy and Infectious Diseases (NIAID) from 1984 to 2022, and the chief medical advisor to the president from 2021 to 2022.Fauci was one of the world's most frequently cited scientists across all scientific journals from 1983 to 2002. In 2008, President George W. Bush awarded him the Presidential Medal of Freedom, the highest civilian award in the United States, for his work on the AIDSrelief program PEPFAR.
Fauci received his undergraduate education at the College of the Holy Cross and his Doctor of Medicine from Cornell University. As a physician with the National Institutes of Health(NIH), Fauci served the American public health sector for more than fifty years and has acted as an advisor to every U.S. president since Ronald Reagan. During his time as director of the NIAID, he made contributions to HIV/AIDS research and other immunodeficiency diseases, both as a research scientist and as the head of the NIAID.
During the COVID-19 pandemic, Fauci served under President Donald Trump as one of the lead members of the White House Coronavirus Task Force. His advice was frequently contradicted by Trump, and Trump's supporters alleged that Fauci was trying to politically undermine Trump's run for reelection. After Joe Biden took office, Fauci began serving as one of the lead members of the White House COVID-19 Response Teamand as Biden's chief medical advisor.Fauci stepped down at the end of 2022.

#Anthony fauci#science#environment#ecology#scientists#geology#science education#science facts#science side of tumblr#biology#science fantasy#science fiction#doctors#hospital#medicine#vaccines#infectious diseases#vaccination
0 notes
Text
H5N1: Dangerous reassortment growing more likely
H5N1 is widespread in the animal world, infecting cows and poultry, killing cougars and cats, decimating terns and seals. It's human flu season. Reassortment is beginning to look less and less unavoidable.
Image: A colorized electron microscope image released by the National Institute of Allergy and Infectious Diseases shows avian influenza A(H5N1) virus particles (yellow), grown in Madin-Darby Canine Kidney epithelial cells (blue). (CDC / NIAID via The Associated Press) Three bits of news from this week: The CDC confirmed the first severe human case of bird flu—the D1.1 genotype found in wild…
#avian-influenza#bird flu#cats#cougars#epidemic#H5N1#health#news#olympic neninsula#pandemic#reassortment#seals#terns#Washington State
1 note
·
View note