#Hemiparesis
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr has been providing a Korean-language service since 2013.
Text
Very often people say that ambidextrous people are actually just lefties who were forced to use their right hand.
Meanwhile my hemiparetic (right side) ass is sitting here like "Am I a joke to you?" 😂
My right side may be weak, which is why I often use my left hand/arm for things that need muscle strength, but I automatically started writing with my right hand when I learned how to write 😅
33 notes
·
View notes
Text
I saw a woman with hemiparesis win gold at the Paralympics for Colombia.
On one hand, as someone who just became hemiparetic, she’s an inspiration to me. On the other, the fact that there is a category at the Paralympics for the same condition I just got hammers home to me the fact that I’m now disabled disabled.
I’ve had fibromyalgia for about ten years, and that’s a disability, but it’s an invisible one, and something I could ignore more or less. This is not just painful, but visible and functionally limiting, not to mention scary.
9 notes
·
View notes
Text
#Stroke recovery#Physical disability#Motor impairments#Hemiparesis#Hemiplegia#Paralysis#Muscle weakness#Balance issues#Coordination problems#Spasticity#Contractures#Sensory loss#Speech difficulties#Dysphagia (swallowing difficulties)#Chronic pain#Fatigue#Cognitive impairments#Stroke rehabilitation#Neuroplasticity#Functional recovery#Stroke-related fatigue#Post-stroke depression#Stroke complications#Walking difficulties#Vision problems#Bladder and bowel dysfunction#Post-stroke care#health & fitness
3 notes
·
View notes
Text
And muscle
I’m here, I’m queer, and my joint pain is moderate to severe
84K notes
·
View notes
Text
Mengenal Hemiparesis
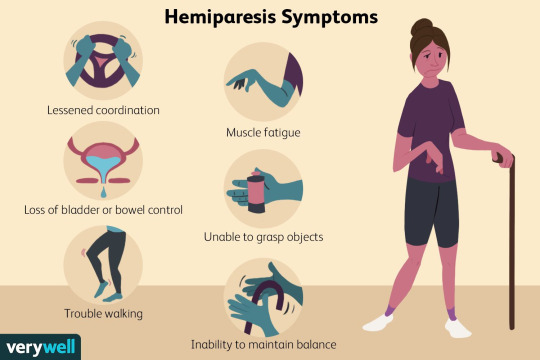
Hemiparesis adalah kondisi yang ditandai dengan kelemahan pada satu sisi tubuh, atau yang masyarakat sering kenal sebagai lumpuh sebelah. Kondisi ini sering terjadi akibat stroke atau cedera otak dan dapat mempengaruhi kemampuan seseorang untuk melakukan aktivitas sehari-hari. Pentingnya mengenali gejala hemiparesis dan memahami kedaruratannya tidak bisa diabaikan. Gejala hemiparesis dapat…
View On WordPress
1 note
·
View note
Text
Delayed onset of intracerebral tension pneumocephalus 2 years after an anterior skull base fracture: Case report by Sokchan Sim in Journal of Clinical Case Reports Medical Images and Health Sciences
ABSTRACT
Pneumocephalus, the presence of air within the cranial cavity, is most commonly caused by trauma, tumor, infection and fistulation into the intracranial cavity or secondary to neurosurgery. We describe an unusually delayed neurological deficit from intracerebral tension pneumocephalus, 2 years following a head trauma with anterior skull base fracture. A 22-year-old man presented to our neurosurgical consultation with recurrent seizures and progressive right hemiparesis. The brain CT scan without iv contrast revealed an intracerebral tension pneumocephalus in the left frontal lobe, and a persistent hole in the left anterior frontal skull base connecting to pneumocephalus. We performed a left frontal craniotomy, and dura-plasty using galea flap to cover the skull-base bone defect. The patient has recovered gradually from his motor deficit after this surgery, finally to the level that he could play his favorite guitar. This is a rare case of a delayed development neurological deficit due to pneumocephalus from a “ball-valve” effect secondary to an old anterior skull base fracture.
Key words: Pneumocephalus, hemiparesis, craniotomy, dura-plasty
INTRODUCTION
Pneumocephalus is an air entrapment in the cranial cavity. It is commonly seen after head and facial trauma, ear infections, and tumors of the skull base or neurosurgical interventions. In some extremely rare cases, it happens spontaneously. Pneumocephalus is a complication of head injury in 3.9–9.7% of the cases. The accumulation of intracranial air can be acute (<72 h) or delayed (≥72 h). In tension pneumocephalus, the continuous accumulation of intracranial air is thought to be caused by a “ball-valve” mechanism. In turn, this may lead to a mass effect on the brain, with subsequent neurological deterioration and signs of herniation. Delayed tension pneumocephalus is extremely rare and requires proper neurosurgical attention. Surgical treatment involves aspiration of air into a syringe and closure of the dura defect through a cranial surgery.
CASE REPORT
A 22-year-old male presented to our neurosurgical consultation with chronic headaches, progressive right-sided weakness and occasional seizures. Two years prior to this visit, he suffered a severe traumatic brain injury by motorcycle accident. He had lost his consciousness for three days, and hospitalized in a provincial hospital for two weeks without any surgical intervention. He was then discharged home with persistent rhinorrhea for 10 months before it ceased spontaneously. 18 months after his injury, this patient began having progressive weakness on his right side of the body, and some episodes of seizures. He also reported occasional headaches. He was otherwise healthy before this accident. On examination, the young man had full consciousness, was alert and oriented. He had grade 3 out of 5 hemiparesis on his right side. A brain CT scan without iv contrast was obtained revealing a large pneumocephalus in the left frontal lobe. We noted a continuity of the air and the anterior skull base defect. (Figure.1)
CSF examination and culture were negative for infection, as well as the nasal swab.
Figure 1: A. Axial view of the CT scan showing hypodensity area in the left frontal lobe, pneumocephalus. B. Sagittal view presenting the large air space with its connection to the frontal skull base. C. Coronal view showing the bony defect of the anterior skull base.
We decided to perform the surgery by doing bi-coronal approach for a left frontal craniotomy and repair of the dura defect on the frontal skull base using the pedunculated galea flap. (Figure.2)
Figure 2 :A. Bi-coronal incision with preservation of large frontal galea. B. Galea still attached to the frontal base is lifted up.
The surgery went well without any complication. The post-operative course was without any significant event. No sign of infection was noticed. The patient recovered gradually from his motor deficit on his right side. The post-operative CT scan showed complete resorption of the intracerebral pneumocephalus. (Figure.3). Intravenous prophylactic antibiotics were used to prevent meningitis.
Figure 3: Post-operative CT scan showing no hypodensity area in the left frontal lobe, complete disappearance of the pneumocephalus A. Axial view B. Sagittal view C. Coronal view. Noted the small bone defect from craniotomy site.
At one-month follow-up, his motor function on the right body became normal that he could play his favorite guitar again. At three-month follow up, he had an episode of new seizures, we controlled his seizures with anti-epileptic drugs for two years afterward.
DISCUSSION
The term “pneumocephalus” was first coined more than one century ago by Luckett and Wolff independently. The term “tension pneumocephalus” was proposed by Ectors, Kessler, and Stern in 1962. Pneumocephalus or also known as pneumatocele or intracranial aerocele is defined as the presence of air in the epidural, subdural, or subarachnoid space, within the brain parenchyma or ventricular cavities. It is a complication of head injury in 3.9 – 9.7% cases. It also appears after supratentorial craniotomy surgery. The accumulation of intracranial air can be acute, less than 72 hours, or delayed, more than 72 hours.
Two mechanisms have been proposed to explain pneumocephalus. In the first mechanism, the pathophysiologic process starts with Cerebro-Spinal Fluid (CSF) leak in the presence of associated discontinuity of the cranium and leptomeningeal disruption. Subsequent development of relative negative Intra-cranial Pressure (ICP) results in a sufficient “vacuum effect” to cause additional accumulation of air within the cranial cavity. This air is generally distributed in the subarachnoid space. The second mechanism is based on the presence of a “one-way valve” at the site of the leptomeningeal tear. In this case, we found on the CT scan images a bone and dura defect in the left anterior skull base, in connection with intracerebral air collection. The air went in, and was trapped inside the frontal cerebral parenchyma. Slowly it became larger and more significant, putting mass effect into the brain tissue of the patient’s frontal lobe. The patient had experienced rhinorrhea (CSF leak through the nose) after the head trauma but disappeared spontaneously after 10 months. He then developed right hemiparesis and experienced episodes of seizures. Recurrent headaches were also a main complaint. These signs and symptoms were described in previous reports about tension pneumocephalus.
The diagnostic imaging for pneumocephalus is CT scan. “Mount Fuji sign” is described when there are bilateral hypoattenuation collections, causing compression and separation of the frontal lobes on CT scan. In our case, an intraparenchymal air-filled long cavity was seen in the left frontal lobe, with its tip connecting to the frontal skull base.
Most cases of pneumocephalus tend to resolve spontaneously with conservative management. Nonoperative management involves oxygen therapy, maintaining the patient supine or in Trendelenburg position, prophylactic antimicrobial therapy (especially in posttraumatic cases), adequate analgesia, frequent neurologic checks, and repeated CT scans. The use of continuous high concentration inspired oxygen as a treatment modality for traumatic pneumocephalus may have certain theoretical benefits. Prompt decompression of intracranial air is the initial treatment of symptomatic pneumocephalus. The principles of subsequent treatment parallel those for a CSF leak. It is important to identify the site where the communication between the air cavity and the external environment occurs. If the site can be identified, the passage should be sealed off, thereby decreasing the possibility of worsening or recurrent pneumocephalus. Effective therapy of tension pneumocephalus through a controlled decompression using a closed water-seal drainage system has also been described. In our case, we performed a full scale left frontal craniotomy to evacuate air from the intraparenchymal cavity, closure of the skull base defect by using pedunculated galea flap, re-enforced by bio-glue as a sealing material.
CONCLUSION
Tension pneumocephalus is a life-threatening neurosurgical case. Although the development of this massive intracerebral air trap was delayed in this case, it caused significant neurological deficit. The patients who suffer from head trauma, with CSF leak should be subject for long term follow up.
Disclosure: Nothing to disclose, and there was no conflict of interest among the authors.
Research ethics: Informed consent has been obtained from the patient.
For more information: https://jmedcasereportsimages.org/about-us/
For more submission : https://jmedcasereportsimages.org/
#Pneumocephalus#hemiparesis#craniotomy#dura-plasty#CT#neurosurgical#headaches#Cerebro-Spinal Fluid#ICP#Intra-cranial Pressure#CSF#Sokchan Sim#jcrmhs
1 note
·
View note
Text
Being away has made me realize that I’m far from creating a CC hair that I can feel proud of sharing with you all. And yes, I am treating myself within entry-level here. I see so many beautiful creations, new and ongoing, and then think of what I’ve done so far with mine, and yeah… Yeah. I’m happy but not happy with some of the strands in the hair. I look at it, and see noodles. Soup noodles. Hopefully I can overcome this disheartening feeling that I feel inside.

#thoughtful miss pepeshi#miss pepeshi’s heart aches a bit#everything will be alright#things happen#kudos to those who can create wonderful things#sometimes i feel like i need step by step guidance#fuck hemiparesis#delete later
14 notes
·
View notes
Text
Yeah it's almost like a lot of what makes having an illness awful is the SYMPTOMS.
which, when the test comes back clear, are STILL THERE
A doctor saying "Good news! Your labs look great" is like if you were watching a cop show and the chief walked in like "Great news, everybody! The best news! The killer is still at large and we have no leads."
#yeah my neuro told me i should be grateful i didnt have ms... just. enough severe symptoms of ms that i was being regularly hospitalised#with no hope of treatment or mitigating it#like. mate. im so glad ive got hemiparesis down one side for NO REASON WE CAN FIND
46K notes
·
View notes
Text
How Long Does It Take To Recover From Hemiplegia?
Hemiplegia, a neurological situation characterized through paralysis on one aspect of the body, is usually a end result of a stroke, annoying mind damage, or unique essential apprehensive device issues.
Can You Live A Normal Life With Hemiplegia? Recovery from hemiplegia varies drastically, stimulated via the cause, severity, individual health factors, and the quality of rehabilitation.
If you or a cherished one is navigating this hard journey, Big Apollo Spectra Hospital in Patna is an super preference for Neurologist Doctor In Patna, and ultra-present day centers.
Can Hemiplegia Be Cured Completely?
Right Side Hemiplegia Recovery Time arises while the mind or spinal wire is damaged, disrupting conversation between the anxious tool and the muscles.
Common motives encompass:
Stroke: The most commonplace motive of hemiplegia because of interrupted blood deliver to the brain.
Traumatic Brain Injury (TBI): Physical effect on the mind principal to localized paralysis.
Brain Infections: Conditions like meningitis can have an effect on mind characteristic.
Congenital Conditions: Such as cerebral palsy, that could cause lifelong hemiplegia.
Recovery Timeline: Factors That Influence Progress the healing duration from hemiplegia isn't always regularly occurring and is predicated upon on numerous factors:
Severity of the Condition: Individuals with moderate hemiplegia often recover faster than people with more intense paralysis.
Prompt Medical Intervention: Timely remedy, mainly in stroke-brought on hemiplegia, can extensively beautify recuperation effects.
Rehabilitation Therapy: Access to physiotherapy, occupational remedy, and speech remedy speeds up recuperation.
Age and Overall Health: Younger individuals and those with fewer pre-modern fitness conditions commonly heal quicker.
While some human beings begin to see enhancements inside weeks, others may additionally take months or maybe years.
In some instances, full healing might not be viable, however large development may be finished with everyday Left Side Hemiplegia Treatment.
Phases of Hemiplegia Recovery
#1. Acute Phase (First three Months)
The first three months put up-evaluation are essential for recovery. During this segment, the mind reveals the nice plasticity, allowing new neural connections to form.
Patients regularly experience visible upgrades in mobility and feature with the help of physiotherapy.
At Big Apollo Spectra Hospital, advanced therapeutic techniques are applied to enhance healing at some point of this section.
#2. Sub-Acute Phase (three to six Months)
This section keeps to expose improvement, although at a slower tempo.
Rehabilitation stays critical, focusing on strengthening muscle mass, regaining balance, and improving coordination.
Treatments like electric stimulation and robotic-assisted remedy are often hired to maximise recuperation.
#3. Chronic Phase (6 Months and Beyond)
Recovery after six months has a tendency to plateau; however persevered remedy can yield incremental enhancements.
Patients who maintain a consistent remedy ordinary regularly regain extra independence through the years.
Treatment Modalities That Aid Recovery
Physical Therapy: Focuses on restoring electricity and mobility via guided bodily activities.
Occupational Therapy: Helps sufferers relearn each day sports like dressing and eating.
Speech Therapy: Essential for those experiencing issue with speech or swallowing.
Psychological Support: Emotional properly-being is critical for motivation and prolonged-term restoration.
Medications: May encompass capsules to lessen spasticity or enhance blood float to the mind.
Advanced options like virtual fact remedy and neurostimulation, to be had at Big Apollo Spectra Hospital, have proven promising outcomes.
What Is The Recovery Rate For Hemiplegia?
How Long Does It Take To Cure Hemiparesis? Seek immediate hospital therapy at a reputed hospital inclusive of Big Apollo Spectra Hospital in Patna, for well-timed analysis and remedy.
Consistency in Therapy: Regular therapy instructions make certain regular progress.
Home Exercises: Practicing prescribed physical activities at domestic can accelerate restoration.
Healthy Lifestyle: A balanced weight loss plan, hydration, and correct sufficient sleep help the recuperation method.
Family Involvement: Encouragement and help from loved ones offer emotional energy.
Why Choose Big Apollo Spectra Hospital in Patna?
Big Apollo Spectra Hospital can be the first-rate neurology hospital in Patna for several motives:
Expert Neurology Team: Led through skilled neurologists and supported with the useful resource of professional therapists.
Advanced Facilities: Equipped with modern era to offer modern-day remedies.
Comprehensive Rehabilitation Services: Includes physical, occupational, and speech remedies tailor-made to man or woman desires.
Patient-Centric Care: A compassionate approach ensures that patients and families sense supported at each step.
Proven Track Record: Numerous fulfillment testimonies of sufferers getting higher from complicated neurological situations.
Can You Fully Recover From Hemiplegia?
Recovery from hemiplegia is a slow process that wishes staying strength, perseverance, and get right of entry to brilliant hospital therapy.
While the timeline varies, many patients gain massive improvement with early intervention and constant remedy.
If you're looking for the pleasant care for Left Side Hemiplegia Recovery Time, Big Apollo Spectra best Neurologist in Patna offers know-how and advanced remedy options.
Trust their committed team to manual you or your loved one on the course to recuperation and regain independence.
#Can You Fully Recover From Hemiplegia#Can Hemiplegia Be Cured Completely#What Is The Recovery Rate For Hemiplegia#Can You Live A Normal Life With Hemiplegia#How Long Does It Take To Cure Hemiparesis#Right Side Hemiplegia Recovery Time#Left Side Hemiplegia Recovery Time#Right Side Paralysis Treatment#Left Side Hemiplegia Treatment
0 notes
Text
Guys watching Sanremo altered my brain chemistry and now I want to learn how to sing (and to play the keytar since it seems one only has to use the right hand for the keys - I don't have much control on my left hand's fingers so I think it's ideal - and I also think it's an hella cool instrument)
1 note
·
View note
Text

Sadly I cannot cut paper well enough to make this work ):
Where do other furry artists order custom stickers and keychains and stuff without it being one million dollars or you have to order one billion copies of it…
#fun sqrkyclean lore#I have hemiparesis! and a brain tumor#and have incredibly dogshit spacial reasoning and hand eye coordination
43 notes
·
View notes
Note
I’m making a backstory / writing fic about a minor character from a show. In her promo images, she had what looked like a lower leg / ankle brace, as well as a walking stick. In her few appearances, it turned out these were just decorative (not a brace, just an odd shoe). I was thinking of writing her as disabled in a fic, however there are 2 problems. One, I don’t know how she was disabled. What sort of problems require a brace? Two, I’m not disabled. Is it okay to make this change?
Hey!
I think it's fine to make an already existing character disabled. Especially if you're doing it for the reason you said and not for the way too common "angst because disability is so sad and tragic" reasons.
The type of ankle/calf brace you're describing would probably be what we call an ankle-foot-orthosis (AFO for short), but I can't tell you 100% without knowing how exactly it looks like. This is the most common type of orthosis. A lot of people use it.
For younger people; cerebral palsy will be the most common reason they are used, and by a wide margin. A stroke or a brain injury (traumatic, or infectious like encephalitis) could also cause it. Someone with late onset spinal muscular atrophy could also use AFOs or KAFOs (K for knee, they go above it), same for people who have low level spinal cord damage (e.g. multiple sclerosis, lumbar SCI, polio etc.). A tumor in either brain or spine could also require braces long-term.
If you specifically want her to have one orthosis and not two, you should probably look into hemiplegia/hemiparesis. All three of the first suggestions above could cause it, as well as conditions like Brown-Séquard syndrome.
All of the above would make sense for using a cane as well. I hope this helps,
mod Sasza
52 notes
·
View notes
Note
What was it like when you learned how to read and write? How old were you?
I don't really remember, I'm hyperlexic and was 2 when I learned how to read... But learning to write was hard because I'm right-handed and have hemiparesis on my right side 😅 They thought that I'd naturally use my left hand, but I started writing with my right hand from the beginning. Writing was when I entered school in 1st grade.
15 notes
·
View notes
Text
Speech & Language Pathology Stroke Terms
Disorganised list of terms used in slt for stroke- for study/quick reference.
AAC- Alternative augmentative communication.
ABI- Acquired brain injury (anytime after birth).
Agnosia- Inability to process sensory information (in Greek gnosis- "not knowing").
Aphasia- Impairment of language, affecting the production or comprehension of speech and the ability to read or write, depending on the affected area of the brain. (Greek a/without + phásis/speech").
Apraxia- Inability to execute purposeful, previously learned motor tasks, despite physical ability and willingness. (Greek a/without + praxis/action).
Aspiration- Food or fluid accidentally enters the lungs through the windpipe, often as a result of dysphagia.
Bilateral- Involving or affecting both sides, usually referencing both sides of the body.
Capacity- Ability to reason, make decisions and consider choices, express views and receive and understand information (AWI= Adult With Incapacity).
Cerebro-Vascular Accident (CVA)- Stroke.
Cognitive function- Anything involving thinking.
Deep Vein Thrombosis (DVT)- Blood clot forms in a deep vein.
Deglutition- The act of swallowing.
Dementia- Decline of function in the brain causes cognitive problems such as difficulty with memory, understanding and mood.
Dysfluency- Any type of speech which is marked with repetitions, prolongations and hesitations; an interruption in the flow of speech sounds. Commonly known as stuttering or stammering.
Dysarthria- Collection of motor speech disorders.
Dysphagia- Swallowing difficulties.
Embolism- Blockage of a blood vessel by a blood clot or piece of fatty material or other debris in the blood stream. An embolism is a type of stroke.
Enteral feeding- Feeding through a tube connected to the person's stomach.
FAST test- 'Facial drooping, Arm weakness, Speech problems, Time to call 999'
Fluency- Smoothness with which sounds, syllables, words and phrases are joined together during oral language.
Hemorrhagic stroke- Caused when a blood vessel in the brain bleeds into the brain tissues or the space around the brain.
Hemianopia- Loss of one half of your visual field.
Hemiparesis- Weakness on one side of the body.
Hemiplegia- Complete paralysis on one side of the body.
Hypotonia- Abnormal decrease of muscle tone.
Ischemic stroke/ Infarct- Damage to the brain caused by lack of blood flow, usually from a clot. An area of tissue that is dead because of a loss of blood supply. This is the most common type of stroke.
Infarction- A sudden loss of a tissue’s blood supply causing the tissue to die.
Ischemia- Blood flow (and thus oxygen) is restricted or reduced in a part of the body.
Ischemic penumbra- Areas of damaged but still living brain cells arranged in a patchwork pattern around areas of dead brain cells.
Lacunar stroke/infarct- When a small artery deep in the brain becomes blocked, causing a small area of damaged brain tissue.
Left hemisphere- Controls speech, comprehension, arithmetic, and writing.
Muscle tone- The degree of natural tension in a person's muscles. Abnormally high muscle tone can lead to muscle tightness and stiffness (spasticity). Very low muscle tone can cause floppiness (hypotonia).
Muscle tension- When muscles of the body remain semi-contracted for a period of time in the resting state.
Naso-gastric (NG) tube- Medical catheter that's inserted through your nose into your stomach. Used both to deliver substances to your stomach and to draw substances out.
Neglect- Not being aware of one side of the body and/or environment.
Neuron- Nerve cell.
Neuroplasticity- The ability of undamaged parts of the brain to take over the jobs of damaged areas.
Nystagmus- Continuous uncontrolled movement of the eyes.
Paralysis- Partly or entirely unable to move the affected parts of the body.
Percutaneous endoscopic gastrostomy (PEG)- Feeding tube placed through the abdominal wall and into the stomach.
Right hemisphere- Controls creativity, spatial ability, artistic, and musical skills
Stroke- Occurs when something blocks blood supply to part of the brain or when a blood vessel in the brain bursts.
Spasticity- Abnormal increase in muscle tone or stiffness of muscle
Thrombolysis- An early treatment for some types of strokes caused by a blood clot.
Thrombosis- A blood clot that forms in an artery.
Transient Ischaemic Attack (TIA)- sometimes called a “mini-stroke”. Blood flow to the brain is blocked for a short time, usually no more than 5 minutes.
Vertebral artery dissection (VAD)- A tear in the walls of an artery at the back of the neck, blood can then get between the layers of artery walls and can lead to a clot forming, causing a blockage (a stroke).
Visual field loss- The loss of sight in a particular area of visual field.
31 notes
·
View notes
Text
What he needs (15528 words) by HecticDemon, 42donotpanic Chapters: 1/1 Fandom: The Avengers (Marvel Movies), Hawkeye (Comics) Rating: Mature Warnings: No Archive Warnings Apply Relationships: James "Bucky" Barnes/Clint Barton, Clint Barton & Kate Bishop, James "Bucky" Barnes & Kate Bishop, Clint Barton & Lucky (Hawkeye), James "Bucky" Barnes & Lucky (Hawkeye) Characters: James "Bucky" Barnes, Clint Barton, Steve Rogers, Tony Stark, Lucky (Hawkeye), (he's called Arrow here), Kate Bishop Additional Tags: Paralysis, Brain Damage, Stuttering, Bucky Barnes Recovering, Hurt Bucky Barnes, Bucky Barnes Has Issues, Deaf Clint Barton, Trans Clint Barton, Protective Clint Barton, Tony Stark Has Issues, Tony Stark Is Not Helping, Not Steve Rogers Friendly, lucky is still called Arrow, why the hell would Clint Barton rename a Dog named Arrow, Digital Art, story and art inside, Marvel Bang 2024, Non-Sexual Intimacy, Cuddling & Snuggling, Napping, Coffee, Tacos Summary: After a Failed Attempt to get the Programming Out of Bucky's Head, he is left to deal with the Consequences of a Traumatic Brain Injury, including Hemiparesis, Aphasia, Apraxia, Fatigue and many more. Clint does his best to support him while also keeping their life at the Tower as normal as possible for both their sake. Even if that sometimes means following stupid impulses.
Art imbedded in the work.
#marvel bang#marvel fanart#marvel fanfction#winterhawk#clintbucky#2024 marvel bang submission#marvelbang#marvel_bang
2 notes
·
View notes
Text
Postictal State
-- occurs after a seizure has stopped
-- muscles relax to become flaccid
-- breathing becomes labored -> fast -> deep
-- acids have built up in the bloodstream
-- acids clear away in a few minutes
-- patient will be able to breathe normally in a few minutes
-- the longer the seizure lasts, the longer it will take for breathing to return to normal
-- longer seizures result in longer postictal states
-- a normal level of consciousness signals the end of the postictal state
-- may be characterized by hemiparesis -> one-sided weakness -> resembles a stroke -> soon resolves
-- common characteristics -> lethargy -> confusion -> possible combativeness
-- do not leave a patient alone until they have a normal level of consciousness and are awake, alert, and oriented
.
Patreon
#studyblr#notes#medblr#medical notes#med notes#my notes#ems#ems notes#emergency medical technician#emergency medical technician notes#prehospital care#pre-hospital care#emergency medical services#emergency medicine#emergency medicine notes#paramedic notes#paramedic#paramedic care#emt care#biology#bio#health science#life science#first responders#first responder training#emt training#paramedic training
3 notes
·
View notes