#Dysphagia (swallowing difficulties)
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Kazakhstan’s Minister of Communications and Informatics has blocked the Tumblr site because it contained 60 sites of terrorism, extremism, and pornography in 2015.
Text
as someone with more mild dysphagia (difficulty swallowing) that hasn't required thickened liquids (as of it)
Hearing the people are using thickened water to make.... fucking slime, of all things. Is so entirely disrespectful.
It's already in limited supply in places that do stock it. If you don't have a need for it, Don't grab it! Please!
your sensory needs are not worth starving someone over..
35 notes
·
View notes
Text
#Stroke recovery#Physical disability#Motor impairments#Hemiparesis#Hemiplegia#Paralysis#Muscle weakness#Balance issues#Coordination problems#Spasticity#Contractures#Sensory loss#Speech difficulties#Dysphagia (swallowing difficulties)#Chronic pain#Fatigue#Cognitive impairments#Stroke rehabilitation#Neuroplasticity#Functional recovery#Stroke-related fatigue#Post-stroke depression#Stroke complications#Walking difficulties#Vision problems#Bladder and bowel dysfunction#Post-stroke care#health & fitness
5 notes
·
View notes
Text
a pretty recent conversation that I had with my mom that really pissed me off was my mom basically telling me "I know that you have difficulty swallowing but can't you just pretend that you don't, that you are 100% fine while visiting our family?" and it angered me so much and i'm still SO ANGRY remembering this. Idk why i'm writing this but I just don't have anyone else to tell and tumblr is my public journal.
#scribble.txt#I told her that it literally does not work that way.#or well I think I might have yelled#im stil so pissed off. she still doesnt believe me#medical cw#and she wants me to go on some family vacation without our family members finding out#that me her kid has fucking difficulty swallowing(im trying to get an appointment as soon as possible to figure out why. i guess what i hav#could be called dysphagia? i am not sure of anything yet)#and like. does she expect me to suddenly become capable of eating normally around our extended family?#i hate this stupid family and vacation and life.
2 notes
·
View notes
Text
Yes!!!
And furthermore, Dysphagia is often just a symptom or sign—the first one, even—of other conditions of the throat/esophagus.
It can also have a very slow progression (like months or years slow) that can seem to feel the same for a while before suddenly getting just a bit worse… again… and again… and again… over and over. So if you’re like me from a few years ago, and feel at this time like you’re “managing it” whenever your food sticks by, say:
Drinking water
Tilting your head back
Stretching
Getting up to walk around
…well, you might be managing it right now, but…
…managing is not the same as treatment, and untreated problems tend to get worse.
Since this problem is happening to a VERY IMPORTANT part of your body, it’s a very important problem to address. So PLEASE talk to your doctor about treating it.
Take it from someone who just got diagnosed with Achalasia this week, after years of dealing with swallowing problems which kept gradually worsening despite every attempted “management strategy”, diet change, and acid reflux treatment—you DON’T want to be like me and keep waiting around to get better treatment for an essential part of your body. It took me until the point of becoming underweight and stuck eating a miserably restrictive puréed-food diet to recognize how much I needed better treatment. It SUCKS to be at this point, so PLEASE take care of yourself so you don’t potentially end up in an equally sucky situation.
TLDR: If you can’t swallow food or drink normally, TALK TO YOUR DOCTOR ABOUT TREATING THAT. Swallowing is an important function of your body, essential to your health and survival—if you aren’t able to eat/drink properly, your whole body can suffer.
hello world!!!
I want to talk to you about swallowing (not in a sexual light)
swallowing is supposed to be:
efortless
automatic
painless
and should happen without conscious thought
choking is supposed to be infrequent
if that does not sound like your swallowing experience you are probably part of the 5-15% of the population that has dysphagia. if your swallowing is bothering you then you can (and should) bring up your concerns to a doctor
swallowing is not supposed to be difficult!
#physical disability#physically disabled#cripple punk#cripplepunk#chronic illness#chronically ill#dysphagia#disability#disabled#achalasia#Achalasia cardia#swallowing problems#swallowing issues#acid reflux#gastroesophageal reflux disease#gerd#stomach problems#stomach issues#esophagus issues#esophagus problems#heartburn#difficulty swallowing#difficulty eating#painful swallowing#trouble eating#trouble swallowing#trouble drinking#difficulty drinking#psa#health psa
881 notes
·
View notes
Text
Yall, I think I'm just dehydrated actually.
#ariambles#its just so weird how my throat is like this despite there being No Pain. it cant be sore throat. it cant also be dysphagia or wtv the hell#google is giving me. like the biggest thing bout this is Zero Pain and it isnt the esophagus. cuz it legit is difficult to Swallow#as in. the throat. its the throat. it hasnt even reached the esophagus. its That kind of difficulty in swallowing#so then i yawned and was like-- nowd i think bout it. my tongue has a Strange feeling to it nowadays. so then i thought--#what happens if theres too little saliva? WELL! would you look at that. my symptoms. its still the quencies... gah
0 notes
Text
Causes Difficulty In Swallowing - ENT Specialist Near Me

Swallowing, a herbal and regularly neglected function, is critical for eating food, drinks, or perhaps saliva.
Is Difficulty Swallowing A Sign Of Cancer? However, for some human beings, this reputedly simple act can turn out to be a giant challenge, medically known as dysphagia.
I Feel Like I Can't Swallow My Saliva? Difficulty in swallowing can have an impact on anybody and is often indicative of underlying health situations.
At Big Apollo Spectra Hospital in Patna, we deal with diagnosing and treating swallowing problems.
Recognized as the best ENT Hospital in Patna, our group of ENT doctors and advanced diagnostic device offer complete care to repair normal swallowing characteristic and decorate exquisite of life.
Common Causes of Difficulty in Swallowing
Trouble Swallowing Saliva But Not Food! Understanding the reasons of dysphagia can beneficial useful resource in nicely timed evaluation and remedy, making sure the exceptional consequences for sufferers.
1. Neurological Disorders
Neurological conditions frequently disrupt the coordination and electricity of the muscle tissues worried in swallowing. Common troubles consist of:
Stroke: A foremost reason of dysphagia, strokes can harm the mind’s functionality to control swallowing.
Parkinson’s Disease: This present day ailment affects motor capabilities, together with the muscle tissue used for swallowing.
Multiple Sclerosis (MS): MS can impair nerve signs, affecting the throat and esophagus muscles.
Amyotrophic Lateral Sclerosis (ALS): ALS weakens the muscle tissues chargeable for swallowing, primary to massive problem.
2. Esophageal Disorders
The esophagus is a critical shape for transporting food to the belly. Several conditions can impair its function, together with:
Gastroesophageal Reflux Disease (GERD): A long-term acid reflux condition can damage the lining of the esophagus, leading to scarring and constriction.
Esophageal Stricture: A constricted esophagus can lead to difficulties and pain while swallowing.
Achalasia: A rare condition in which the lower esophageal sphincter does not relax, preventing food from entering the stomach.
3. Muscle Disorders
Certain muscle issues can interfere with the swallowing device:
Scleroderma: This autoimmune condition causes the tissues of the esophagus to harden and tighten.
Myasthenia Gravis: This condition reduces the strength of voluntary muscle functions, including those necessary for swallowing.
4. Obstructions within the Throat
Physical blockages in the throat or esophagus can lead to difficulties in swallowing:
Foreign Objects: Swallowed items, particularly in children, can obstruct the airway or esophagus.
Throat Infections: Serious infections such as tonsillitis or abscesses may cause inflammation and discomfort, making it difficult to swallow.
Tumors: Both noncancerous and cancerous masses in the throat can disrupt swallowing.
5. Aging-Related Changes
Swallowing troubles are extra commonplace in older adults due to:
Loss of muscle strength and coordination.
Conditions such as dementia or Alzheimer’s disease that impact cognitive and physical abilities.
6. Other Contributing Factors
Dry Mouth (Xerostomia): Inadequate saliva production complicates the act of swallowing.
Allergies: Intense hypersensitive responses (anaphylaxis) may lead to throat swelling.
Injuries: Damage to the throat or esophagus, whether from surgical procedures or accidents, can hinder swallowing.
When Should I Be Worried About Trouble Swallowing?
If you or a loved one studies the subsequent Dysphagia Symptoms, it may suggest a swallowing disease:
Pain or pain at the same time as swallowing.
Feeling like food is caught within the throat or chest.
Frequent choking or coughing at the same time as consuming or eating.
Hoarseness or adjustments in voice.
Regurgitation of food or liquids.
Unintended weight reduction due to hassle eating.
Diagnosis and Dysphagia Treatment in Patna
At Big Apollo Spectra Hospital, our ENT specialist in Patna have cutting-edge techniques to identify issues with swallowing. Typical diagnostic approaches include:
Endoscopy: A slender, adaptable tube equipped with a virtual camera is utilized to examine the throat and esophagus.
Barium Swallow Test: This X-ray examines the movement of food or liquid as it passes through the esophagus.
Manometry: Measures the strain and movement in the esophagus.
Once the reason is diagnosed, treatment alternatives are customized to the affected man or woman’s desires. Common treatments encompass:
Medications for GERD or infections.
Swallowing remedy with a speech-language pathologist.
Endoscopic or surgical techniques to cast off obstructions or widen the esophagus.
Advanced treatments like botox injections for achalasia.
Why Choose Big Apollo Spectra Hospital?
Big Apollo Spectra Hospital in Patna would be the most inexperienced vacation spot for ENT care, way to our:
Expert Team: Our quite professional ENT specialists in Bihar provide correct diagnoses and powerful treatment plans.
Advanced Technology: Cutting-problem gadget guarantees specific and minimally invasive strategies.
Patient-Centered Care: We prioritize affected character comfort and recovery, presenting customized remedy tailor-made to each individual.
Comprehensive Facilities: From evaluation to treatment and rehabilitation, our facilities cater to all factors of swallowing issues.
What Causes Difficulty In Swallowing?
Why Is It Hard To Swallow All Of A Sudden? Difficulty in swallowing is not first-class a minor inconvenience; it may significantly effect one’s brilliant of existence and health.
Early assessment and appropriate treatment are crucial for managing this case efficiently. If you or a cherished one is experiencing swallowing issues, don’t hesitate in reaching out for ENT Doctor in Patna.
Visit Big Apollo Spectra Hospital in Patna, Top ENT Hospital for complete assessment and remedy.
Our devoted ENT Specialist Near me help you regain everyday swallowing function and experience a healthier, happier existence.
#Is Difficulty Swallowing A Sign Of Cancer#I Feel Like I Can't Swallow My Saliva#When Should I Be Worried About Trouble Swallowing#Dysphagia Symptoms#Why Is It Hard To Swallow All Of A Sudden#Trouble Swallowing Saliva But Not Food#Dysphagia Treatment
1 note
·
View note
Text
Swallowing difficulties, or dysphagia, can be a challenging condition affecting individuals of all ages. At home health care in Orange, California, we understand the importance of managing these difficulties to ensure safe and comfortable eating experiences. Here are some effective strategies to help manage swallowing difficulties.
0 notes
Text

Trouble swallowing? Is food getting stuck? Please don't ignore it! It could be Achalasia-Cardia, a rare esophageal disorder. Discover more about this condition and consult with our specialists for expert guidance. Don't let Achalasia-Cardia go unnoticed – take action now!
#Swallowing Difficulties Treatment#Swallowing Difficulties Specialist#dysphagia treatment#gastroenterologist
0 notes
Text
Working with but not being a soeech pathologist is fun. Today I forgot the word 'commercial', as in commercial kitchen. I could depend on them to get it with the clues I gave them....I just wish it didn't involve feeling like I have aphasia. I also really like soft, saucy food because I have a crooked jaw (I think). So yay dysphagic too.
#speech pathology#communication#communication difficulties#dysphagia#swallowing difficulties#feeling tired#and kinda down
0 notes
Text
BEN CLARK HEADCANONS. Finally!!
I've been sitting on these for awhile theyre finally here!!
//mentions of strangulation, fighting, etc.
-ben is the type of person to have a million different playlists. he's so me fr
-he has one playlist that's a couple of others combined. its like 6 hours long
-he listens to EVERYTHING. all the genres. (even a few country songs cause im sick of seeing "i listen to everything except country!" THAT ISNT EVERYTHING???)
-whenever i see chatfics he always types grammatically correct and that is WRONG. he's the fastest typer ever trust
-after they decided he was the medic of the group, i like to think he did like tons of reading and research on how to treat injuries . like there was no way he went from helping aiden with a scraped knee to a branch through tyler's stomach
-he knows EVERYTHING about EVERYONE. he's literally gretchen wieners. most people forget he's there so he hears the juiciest tea ever
-at the end of every week the group has a "gossip session" and its literally just them all calling (or hanging out) and ben telling them the stuff he's heard through the week
-ash and taylor too cause they seem like the kind of people to find the craziest tea
-ben and ash quiet kid solidarity
-i like to think ben gave a lot of clothes to lily :)
-i also think he'd be SUPER worried about her in school, esp when she gets to the older grades
-him and aiden once made mug cakes at four in the morning during one of the group's sleepovers cause they couldn't sleep (i did that once)
-aiden and ben are literally brothers atp and they know like everything about each other
-when they woke up after aiden hurt his ankle ben lectured him with a very angry and very loud text to speech voice
-I also like to think aiden has heard ben's voice at least once
-he's somehow the heaviest and lightest sleeper ever. he could sleep through an earthquake but also at the same time if you breathe wrong he'll wake up. he's me
-he used to sleep talk, kinda scared he still does
-he's a cat person and that's the end of it. me again
-he'd be very naturally warm but his hands are always freezing. idk it feels right
-ALEX G ENTHUSIEST
-he has once punched a phantom in the face. it didn't go very well
-i think he'd protect his neck a lot when fighting phantoms
-he has ptsd probably (they all do lets be real)
-I like to think he has dysphagia (difficulty swallowing) so he doesn't like to eat in public that much
-i think it took him a bit to warm up to the group about that :)
-he has lots of scars, like from fighting, nail scars on his neck, etc
-i like to think the reason why he wears grey all the time is bcs he doesn't want to stand out. he's working on that
-he still actively goes to therapy
60 notes
·
View notes
Text
Today's whumpy pondering: dysphagia.
Dysphagia being the medical term for swallowing difficulties.
Like, I deal with it on the daily, and it just has such potential! Consider a whumpee who needs to use a straw, because otherwise they more often than not choke on their liquids. Or maybe a straw makes it worse.
And how specific one's dietary needs can get! A whumpee who can't eat bread based products or dense foods because it's physically painful and immensely difficult to manage. Who has to keep an eye on the temperature of certain things because even that can affect matters.
And then there's the possibilities. Maybe a caretaker who doesn't fully get it, and keeps bringing whumpee toast or sandwiches as a "simple meal". Maybe a whumper who does know, and who deliberately only gives whumpee foods they can't swallow without their whole face scrunching up in pain, or water in a cup, knowing it'll probably mean a few minutes of drowning that probably won't be fatal.
And hey, there's more to think about than just that. I mean, this is based off my own experiences. But think about it.
30 notes
·
View notes
Note
can you elaborate on some of your Ricky headcanons?😁
Hi! I'm assuming you're referring to my tags on this post that I reblogged earlier today referring to the more medical side of expanding on Ricky in canon?
I think maybe hc was kind of the wrong way for me to describe my Ricky ideas in this area. It's more like, I have the background knowledge to speculate some of what Ricky might have going on outside of what we see in canon. Keep in mind I'm drawing from what I learned back in school and on the job, not my own lived experiences, and obviously not everyone with disabilities like Ricky's have the same universal experience so I make no claim that my word is gospel here ofc!!
For one I think he actually Does have a feeding tube. I've seen him drawn a few times with an ng/nj tube but seeing as a. His condition is, as the post I linked to outlines, most likely neuromuscular and b. This affects him systemically and affects his speech, he most likely also has difficulty swallowing as the same groups of nerves and muscles are involved with both and so speech and swallowing sorta go hand in hand. There are no 100% absolutes and I can't speak for every single scenario that might necessitate a feeding tube. However I do find from working in my field that generally, people who have one due to dysphagia because of a permanent condition (such as his, which is understood to be progressive) have gastrostomy tubes, which go directly into the stomach through the abdominal wall. I've drawn him with this type of tube a couple of times, but obviously it's generally less visible than one inserted nasally and the only way for it to be very visible in a drawing is, ya know, if Ricky pops his top off, lol, or at least pulls it up some.
That being said, not everyone with a feeding tube gets nutrition by this route exclusively. Some people with g tubes eat orally to varying degrees with certain preparations and supplement with tube feedings, and other people can't take anything at all by mouth. I feel like Ricky is somewhere in the middle and that he'd eat soft stuff with textures and consistencies that make it easy to chew and swallow, and drink thickened liquids. (I think Ricky actually quite likes to eat and uses a lotta sauce c:) Any meds he takes are in liquid form or crushed pills mixed with water that go into the g tube. I think he knows the ins and outs of taking care of the g tube on his own, however sometimes it seems to have a mind of its own (stuff happens sometimes with any kind of equipment ofc) and also sometimes it'd be an uphill battle keeping the cats away from it
I'm a little tuckered out from work right now and it would take me a while to call to mind all of my speculations but yeah that's basically just a little bit I imagine about Ricky based on observations I've made working with real people
Outside of the more medical side of Ricky I'm always drawing fun content of him as I run @enter-the-rickyverse and sometimes I incorporate my own hcs into the drawings (ie. He has a great sense of humor, he plays piano, he likes to wear short sleeves shirts over long sleeved shirts, fun stuff like that) I mean he's really just an awesome character to delve into exploring in all sorts of aspects
18 notes
·
View notes
Text
Wtf do you mean dysphagia is a symptom of dysautonomia?
And wtf do you mean saying dysphagia is difficulty swallowing?
Wtf do you mean it presents as a tendency to cough or choke when you try to swallow water, food or even your own saliva?
You mean to tell me my super power, being able to choke swallowing air, is a fucking symptom of the chronic condition i fucking have?
#dysautonomia#dysautonomia/pots#chronic illness#chronic disability#chronically ill#disabilties#physical disability#disability#disabled#jay and... jay what are you doing?
10 notes
·
View notes
Text
In a normal esophagus, contraction waves are progressive, and the lower esophageal sphincter (LES) relaxes properly to allow food to pass. However, disorders like achalasia, diffuse esophageal spasm, and hypercontractile esophagus disrupt this process.
In general, all patients with suspected achalasia should initially undergo upper endoscopy and/or esophageal barium swallow; findings may support the diagnosis.
Esophageal manometry is indicated to establish the diagnosis (confirmatory test of choice), irrespective of the initial imaging findings.
Achalasia is marked by the failure of the LES to relax, leading to difficulty swallowing, regurgitation, and weight loss. A key diagnostic feature is the bird-beak sign on a barium swallow, with high LES resting pressure observed on manometry.
Diffuse esophageal spasm presents with retrosternal chest pain and simultaneous, repetitive contractions. Patients often experience dysphagia and pain, particularly during eating. The hallmark finding is corkscrew esophagus on imaging.
Lastly, hypercontractile esophagus, also known as jackhammer esophagus, shows extremely strong contractions and often retrosternal pain. Manometry reveals a high distal contractile integral (DCI), indicating very forceful contractions.
Management includes lifestyle changes, medications like calcium channel blockers or nitrates, and in severe cases, endoscopic therapy or surgery to improve esophageal function and patient quality of life.
15 notes
·
View notes
Text
Explaining dysphagia
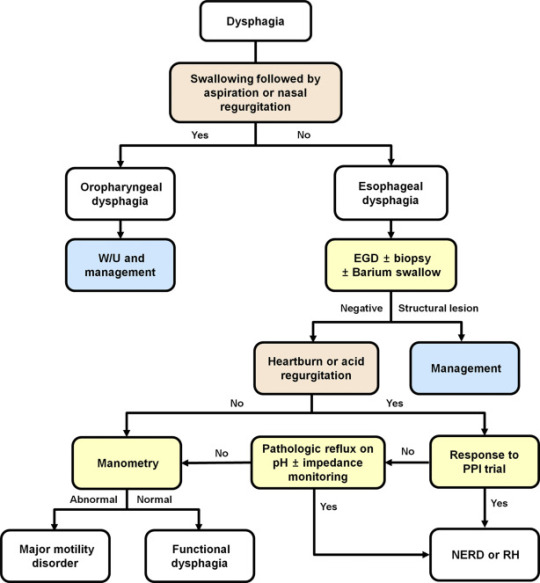
Dysphagia is simultaneously a symptom and a diagnosable condition. Most people think of it (if they think of it at all) as the choking on food disease but in reality it's much more complicated than that.
There are four categories of dysphagia: oropharyngeal, esophageal, esophagogastric, and paraesophageal
only two of those categories (oropharyngeal and esophageal) are commonly used and diagnosed so those are the main two I'll be talking about.
The diagnosis of dysphagia is a fairly complicated process involving a lot of radiological testing and things stuck up your nose and down your throat.
lost the source :(
source
the ICD 10 further divides dysphagia into unspecified, oral phase, oropharyngeal phase, pharyngeal phase, pharyngoesophageal phase, and other dysphagia which includes cervical dysphagia and neurogenic dysphagia
Oropharyngeal dysphagia
Oropharyngeal dysphagia occurs when someone has difficulty initiating a swallow. It's often accompanied by coughing, choking, feeling food stick in the throat, and nasal regurgitation. Other symptoms include frequent repetitive swallows, frequent throat clearing, a gargly voice after meals, hoarse voice, nasal speech and dysarthria, drooling, and recurrent pneumonia.
Oropharyngeal dysphagia is diagnosed with a modified barium swallow and/or a transnasal video endoscopy.
Some of the consequences of oropharyngeal dysphagia include aspiration pneumonia, upper respiratory infections, and weight loss. Common treatment includes rehabilitative swallowing exercises, botox, surgery, and/or a feeding tube.
Esophageal Dysphagia
Esophageal dysphagia is dysphagia where there is a problem with the passage of food or liquids through the esophagus between the upper and lower esophageal sphincter. Esophageal dysphagia is usually a result of abnormal motility in the esophagus or a physical obstruction to the esophagus. Symptoms of esophageal dysphagia vary depending on cause.
Motility: People with esophageal motility disorders will experience problems with swallowing both liquids and solids. Motility disorders consist of abnormal numbers of contractions in the esophagus, abnormal velocity of contractions, abnormal force of contractions, abnormal coordinated timing of contractions, or several of these simultaneously. People with esophageal motility disorders may also experience spasms or chest pain.
Obstruction: People with an esophageal obstruction will have more difficulty swallowing solids than liquids.
Some symptoms of both include pain when swallowing, the inability to swallow, sensation of food being stuck in your throat or chest, drooling, and regurgitation.
Esophageal dysphagia can be diagnosed with a barium swallow, upper endoscopy, esophageal manometry, and an endoFLIP.
Some common treatments for esophageal dysphagia include medication, esophageal dilation, surgery, stent placement, and/or a feeding tube.
Esophagogastric Dysphagia
Esophagogastric dysphagia occurs when there is a problem with material passing from the lower esophageal sphincter into the gastric fundus.
Paraesophageal Dysphagia
Paraesophageal dysphagia occurs when the esophagus is narrowed due to extrinsic compression.
The ICD 10 Classifications
Oral phase - difficulty moving food or liquid to the back of the throat
Oropharyngeal phase - difficulty initiating swallowing
Pharyngeal phase - difficulty swallowing when food or liquid is at the top of the throat
Pharyngoesophageal phase - unable to find information
Other dysphagia- cervical dysphagia (caused by problems with the cervical spine) or neurogenic dysphagia (caused by problems with the central or peripheral nervous system)
Sources
x x x
+ some others I definitely (/sarcasm) didn't lose the link to
94 notes
·
View notes
Text
To go into more detail regarding the last ask in case
Last year I was diagnosed with Barrett’s esophagus (GERD) dysphagia (difficulty swallowing) and esophageal motility issues (two out of the three muscles in my esophagus don’t function as they should thank you Ehlers danlos very cool)
I have a very hard time swallowing without taking medication daily as a result of a lot of different medical crap combined which as a result has led me to have a very limited list of things I can eat because my body is ✨sensitive✨
Among the many many things I had to cut out was sugar (except white chocolate every once in a while as a treat) soda, fried anything, most sauces, basically almost every fast food place etc etc etc…
That being said since last February I’ve just been losing because I can’t really eat too much to begin with nor do I have much variety or options at all

#disability tag#unintentional weight loss#weight loss#gerd#barretts esophagus#dysphagia#esophageal motility issues#I’m normal about it#🙂#sometimes not but whatever fuck it wii bowl
5 notes
·
View notes