#Flowmetry
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
China blocked Tumblr because of pornography and censorship problems in 2013.
Text
México en LRC París, Francia 🇫🇷 2024
Copa Mundial Electro Dance En este mítico festival de Electro considerado para muchos la Copa mundial, México hizo presencia para defender el título Campeones de Equipo contra Equipos y representarnos por medio de distintos bailarines experimentados en las categorías 1vs1. Fue del 13 al 15 de diciembre del 2024 que se llevó a cabo el LRC(Life’s Round Contest) World Festival en el Teatro…
0 notes
Note
aha! more quoting the internet! (https://www.sciencedirect.com/science/article/abs/pii/S1748681512005505) Methods
24 male Wistar rats were randomly assigned to either no treatment (control) or application of cold (17 °C) or warm (37 °C) water applied for 20 min. Evolution of burn depth, interspace necrosis, and microcirculatory perfusion were assessed with histology, planimetry, respectively with Laser Doppler flowmetry after 1 h, as well as 1, 4, and 7 days.
Results
Consistent conversion from a superficial to a deep dermal burn within 24 h was obtained in control animals. Warm and cold water significantly delayed burn depth progression, however after 4 days the burn depth was similar in all groups. Interspace necrosis was significantly reduced by warm water treatment (62 ± 4% vs. 69 ± 5% (cold water) and 82 ± 3% (control); p < 0.05). This was attributed to the significantly improved perfusion after warming, which was present 1 h after burn induction and was maintained thereafter (103 ± 4% of baseline vs. 91 ± 3% for cold water and 80 ± 2% for control, p < 0.05).
Conclusion
In order to limit damage after burn injury, burn progression has to be prevented. Besides delaying burn progression, the application of warm water provided an additional benefit by improving the microcirculatory perfusion, which translated into increased tissue survival.
"Huh..."
2 notes
·
View notes
Text
Revolutionary Brain Monitoring Technology: You Won't Believe the Sensitivity and Usability of This New Method to Track Blood Flow
Revolutionary Brain Monitoring Technology: You Won't Believe the Sensitivity and Usability of This New Method to Track Blood Flow Revolutionary Brain Monitoring Technology: You Won't Believe the Sensitivity and Usability of This New Method to Track Blood Flow Introduction The ability to monitor blood flow in the brain is a crucial function in the medical field. It has become increasingly important for researchers and doctors to track blood flow in the brain in order to better understand how it works, and to develop treatments for various brain disorders. Revolutionary brain monitoring technology has recently made its way into the market, offering a new and improved method to track blood flow in the brain. This technology is highly sensitive and user-friendly, making it the go-to method for tracking blood flow in the brain for researchers, doctors, and patients alike. In this article, we will discuss this new technology and how it is changing the way we monitor blood flow in the brain. Understanding Brain Blood Flow Before diving into the technology, it is important to understand the significance of monitoring blood flow in the brain. Blood flow in the brain is what provides the brain with the necessary oxygen and nutrients, which enables it to function properly. Blood flow to the brain is also crucial in diagnosing and treating various brain disorders, such as strokes and Alzheimer's disease. Traditional methods of monitoring blood flow in the brain have been limited in their sensitivity and accuracy. For example, methods like MRIs and CT scans can provide some information about blood flow, but they are often not sensitive enough to provide detailed information. How the New Technology Works The new brain monitoring technology uses a laser doppler flowmetry (LDF) technique to track blood flow in the brain. This technique measures the speed and volume of blood flow in the brain by measuring the scattering of light through the skin. This technique is highly sensitive and allows for precise measurements of blood flow in the brain. It is also non-invasive, meaning it does not require any incisions or probes to be inserted into the brain. Additionally, the technology is highly user-friendly. It is portable and can be used in a variety of settings, including hospitals and research labs. It is also non-toxic, making it safe for use on patients of all ages. Benefits of the New Technology The new brain monitoring technology is changing the way we monitor blood flow in the brain. Its high sensitivity and accuracy make it a more reliable method for tracking blood flow than traditional methods. Additionally, its non-invasive nature makes it more comfortable for patients, as it does not require any incisions or probes to be inserted into the brain. This makes it an ideal method for monitoring blood flow in patients with sensitive skin or those who are resistant to traditional methods. Finally, the technology is highly portable and user-friendly. This makes it easier for researchers and doctors to use the technology in a variety of settings, from research labs to hospitals. Conclusion The new brain monitoring technology is a game-changer in the field of neuroscience. Its high sensitivity, accuracy, and ease-of-use are revolutionizing the way we monitor blood flow in the brain. As technology continues to advance, we can expect even more advancements in the field of neuroscience. But for now, this new brain monitoring technology is leading the way in providing reliable and non-invasive methods for monitoring blood flow in the brain. #HEALTH Read the full article
0 notes
Link
While the pathogenesis of ME/CFS and post-COVID-19 syndrome remain poorly understood, it seems that the underlying pathology involves the CNS; the autonomic nervous system; and a persistent, dysregulated immune and metabolic response to the infectious agents [10]. Previous studies have shown a high propensity of patients with ME/CFS to be misdiagnosed with a psychiatric condition.
We hypothesized that ME/CFS and post-COVID syndrome are not primary mental health conditions but share some clinical features and common pathophysiological mechanisms related to autonomic dysfunction and microcirculation disorder.
We assessed microcirculation by amplitude–frequency wavelet analysis of blood flow oscillations with laser Doppler flowmetry (LDF) [24]. Because of the proven parallelism between microcirculatory changes in the skin and inner organs, we investigated forearm blood flow in the participants with «LASMA MC-1» peripheral blood and lymph flow laser diagnostic complex.
…the belonging of four symptoms to the domain of “sleep disturbance” and one symptom to the domain of “pain syndromes” confirms the validity of the treatment approach to ME/CFS, described in the recent guidelines from the European Network on Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (EUROMENE). According to this approach, to reduce the severity of fatigue, patients are provided first of all with symptomatic help to normalize sleep and combat pain.
…the belonging of four symptoms to the domains associated with disorders of the nervous system (autonomic, sensory, and motor functions) confirms the classification of ME/CFS in ICD-10, where it belongs to the chapter G—“Diseases of the nervous system”.
Our data, therefore, not only agree with the concept of ME/CFS as a disease with neuroimmune pathogenesis but also allow us to make assumptions about approaches to diagnosis and treatment of this disease, as well as the most effective organization the patient care in ME/CFS, which optimally should be provided by neurologists.
In the past, ME/CFS has often been misdiagnosed as a psychiatric disorder of the affective spectrum, leading to mismanagement and deterioration of the patient’s health [31]. Today, it is believed that anxiety and depressive symptoms, which are common in ME/CFS [32,33], should not always be considered as a sign of an alternative diagnosis.
it should be remembered that recent research data on this topic suggests that depression and anxiety in ME/CFS are associated with the neuroinflammation process, pain syndromes, psychological distress due to the inability to return to work, and reduced physical functioning, social isolation, as well as insufficient knowledge of medical specialists about the disease. Consequently, they are deontologically vulnerable and have skeptical attitudes toward the patient’s problems.
POTS itself often develops following infectious diseases and, at least in some cases, may be associated with the production of autoantibodies against adrenergic and cholinergic receptors.
…in ME/CFS that developed after COVID-19, there is a more pronounced increase in heart rate starting from the 6th minute of the test compared to the control group. This allowed us to assume that POTS is one of the key characteristics of ME/CFS of post-COVID genesis. It is important to note that in 4/13 people who met POTS criteria in our study, the required increase in heart rate was achieved only at the 8–10th minute of the active orthostatic test. This confirms the practice of carrying out the test in its complete (within 10 min) and not abridged (5 min) version.
The rhythmic characteristics of oscillatory processes in the microcirculation system are useful for the diagnosis of many diseases related to the changes in the microcirculation [36]. The LDF method allows a non-invasive assessment of human blood microcirculation system disturbances. In this work, LDF was applied to assess the dynamic characteristics of microcirculation in ME/CFS, including post-COVID genesis (in the latter subgroup—it was done for the first time, to the best of our knowledge). A change in the microcirculation index (increase or decrease) characterizes, respectively, an increase or decrease in perfusion. Its increase can be associated with a lower tonus of the arterioles, which leads to an arterial hyperemia, or with the congestion of blood in the venules and venous hyperemia. Regarding the regulation of microcirculation, there are “active” and “passive” mechanisms. The “passive” mechanisms include external factors that act outside the microcirculatory bed: a pulse wave and the suction action of the “respiratory pump” from the veins. “Active” factors directly affect the vessels of the microvasculature by periodically changing the resistance of blood vessels to blood flow through vasomotions and creating transverse fluctuations in blood flow. These active factors are sympathetic nerve fibers, smooth muscle cells of the vascular wall, and endothelium-derived regulatory molecules. When carrying out spectral analysis, the active factors correspond to low-frequency oscillations [37]. There are several forms of microcirculation disorders: arterial hyperemia, venous hyperemia, combined hyperemia, ischemia, and stasis [38]. The changes identified in this study in ME/CFS, including ME/CFS of post-COVID-19 nature, correspond to the hyperemic form of microcirculation disorders, which is characterized by increased blood flow into the microcirculatory bed. It is distinguished by a significant increase in the number of functioning capillaries, an increase in tortuosity, vasodilation, and an increase in the permeability of the vascular wall. This form of microcirculation disorder is usually observed in acute inflammatory response or other conditions of decreased systemic vasoconstriction.
Bond et al. showed that chronic oxidative stress could contribute significantly to the development of ME/CFS symptoms due to the development of endothelial dysfunction [39]. The relationship between chronic inflammatory processes and increased arterial stiffness is well-known [40]. An increase in vascular resistance in cohort 1 compared to cohort 2 may reflect the contribution of the chronic inflammatory process of a long course to microcirculation disorders and suggests the existence of long-term consequences of ME/CFS, in particular, an increased risk of cardiovascular diseases.
Changes in microcirculation in ME/CFS (including ME/CFS of the post-COVID-19 nature) identified with the LDF method correspond to the hyperemic form of microcirculation disorders which is generally observed in acute inflammatory response or in case of the systemic vasoconstriction failure. It seems that increased vascular resistance may occur later in the disease course due to the chronic inflammatory process.
#long covid#microclots#teamclots#covid effects#science journal#me/cfs#chronic fatigue syndrome#microcirculation#Laser Doppler Flowmetry
0 notes
Text
my rheumatologist has done more for me towards getting a POTS diagnosis than my cardiologist thats kinda sad bro
i came in to the cardiologist the other day (finally after waiting MONTHS) hoping for a tilt table test to see how my heart rate and blood pressure react to orthostasis in a controlled setting. the doctor didnt actually do a thing to test me for it in-office, i was just told to schedule an echo (which is fine), holster (alright) and stress test (why). but i was also prescribed eastern medicine as a treatment....“superbrain yoga”? like i dont want to seem closeminded because she is an indian doctor and there are some things that western medicine hasn’t caught on to but i realy wish i was told why it is supposed to work. like i want to know physiologically how and why it supposedly works. get technical and mechanical with me bro i have le autism, thats my language if you wanna really convince me. if it’s about toning up the muscles in my legs to squeeze the blood into my core upon standing why dont i just do squats? why do i have to do all this really specific stuff like hold my tongue at the roof of my mouth and face east, crossing my arms (right arm must go over left) and maneuver my hands in a certain way to grab my earlobes while doing those squats? is that merely a concentration sort of thing to make your brain focus? if so, why not just let me know what the purpose to these specific movements are (and what does focusing my brain have to do with treating POTS symptoms anyway)?? i’m not a spiritual person so the spiritual aspects of it do nothing for me. but at least i wasn’t given intensive aerobic exercise because i cant do that lol. i was just prescribed core strength training with planks and crunches (fine with me) and “superbrain yoga” (the specifics still confuse me but i’m doing it anyway)
but i didnt even get a tilt table test while i was there, i asked about it and she said “we stopped doing tilt table tests a while ago” and i was like ????????? thats like the gold standard to test for POTS my guy. based on just my symptoms she said i had dysautonomia and i asked “what about POTS?” and she said “it could be” and i was like ? could be? bro you didnt even test for it?
the whole visit just felt really vague and dismissive to my issues (yet again). fucking even my rheumatologist said before this visit to the cardiologist that i “probably have POTS”
so when i left the cardiologist the other day i wrote this up because i was very upset, felt dismissed, and took matters into my own hands to show what kind of medical concepts i’m capable of comprehending and the kind of language i want doctors to talk to me about my conditions in. and today i read it to my rheumatologist during today’s appointment:
the cardiologist says i have dysautonomia, “caused by dysfunction of the small blood vessels”. in the clinic, the nurse measured my laying vs standing blood pressure (which increased rather than decreased) but they didn’t do my heart rate there for some reason. but on my own i’ve measured my heart rate to jump above 30 bpm within 10 minutes of standing, so with all the symptoms lining up exactly with what’s expected of POTS (heart rate increase greater than 30 bpm within 10 minutes of standing, no drop in blood pressure, lightheadedness, brain fog, palpitations, prolonged fatigue, heat intolerance, excessive sweating etc), i’m convinced that the type of dysautonomia i specifically have is POTS, not just the umbrella term “dysautonomia”, and the specific brand of POTS i have is the neuropathic POTS subtype which is thought to be caused by sympathetic denervation (partial autonomic neuropathy) in the lower extremities. this causes the blood vessels in my legs not to constrict as they should when standing, which in turn causes blood to pool in the legs and not return to the heart, causing the heart to have to source its blood supply from elsewhere in the meantime to compensate (with an overall lower venous return), driving up the heart rate and causing lightheadedness. my blood tests also showed i am also very slightly anemic by 0.1 point below the normal range (11.6 g/dL) the resulting denervation hypersensitivity from the sympathetic denervation what is thought to cause erythromelalgia—which i express all the hallmark symptoms of as well in my feet (redness, increased skin temperature, burning sensation (feels like walking on a hot pool deck), cold to touch and bluish purple when not actively flaring, flaring occurs at night, symptoms worsen with exposure to heat and exercise (including walking on feet while flaring) and are relieved with cooling and elevation). i have no response to the cold unlike with what is seen in raynauds. i actually consider cold exposure my savior; the heat is my worst enemy, it makes me feel faint and lightheaded dysautonomia-wise and it makes my feet flare up rheumatologically.
“Several previous investigations have provided clues that patients with the postural tachycardia syndrome have peripheral autonomic dysfunction. Streeten et al. found that patients with orthostatic tachycardia had excessive venous pooling in the legs while standing and suggested that denervation of the legs was a mechanism of the syndrome. This hypothesis was supported by the finding of hypersensitivity to infusion of norepinephrine into the veins of the foot, despite high plasma catecholamine concentrations. [...] These stimuli increased norepinephrine spillover in the arms of both the patients with the postural tachycardia syndrome and the normal subjects, with similar increases in the two groups, but failed to increase norepinephrine spillover in the legs of the patients. [...] The reduced clearance of norepinephrine in the legs, without a similar reduction in the arms, may result from impairment of norepinephrine-reuptake mechanisms due to isolated damage to nerve terminals in the legs. [...] CONCLUSIONS: The neuropathic postural tachycardia syndrome results from partial sympathetic denervation, especially in the legs.” — (https://www.nejm.org/doi/full/10.1056/NEJM200010053431404)
“The laser Doppler flowmetry signal after sympathetic stimulation of reflexes mediated through the central nervous system, was significantly diminished in patients with erythromelalgia as compared with healthy controls. [...] Vasoconstrictor responses involving central sympathetic reflexes were attenuated in erythromelalgia. Local neurogenic vasoconstrictor regulation, vasodilator response to local heating and hyperemic response to ischemia were maintained. [...] The finding of reduced skin perfusion before provocation is in accordance with the clinical observations that many erythromelalgia patients exhibit cold acral skin between attacks. [...] These results indicate that postganglionic sympathetic dysfunction and denervation hypersensitivity may play a pathogenetic role in primary erythromelalgia.” — (https://linkinghub.elsevier.com/retrieve/pii/S0022-202X(15)41629-X)
“Denervation hypersensitivity is a phenomenon peculiar to smooth muscle innervated by the general visceral efferent system. Following denervation there is increased sensitivity of the muscle to neurotransmitters. This is evident in smooth muscle innervated by sympathetic neurons when the postganglionic axon is affected. Such denervated muscle shows hypersensitivity to the application of epinephrine or to circulating epinephrine released during excitement.” — (https://www.sciencedirect.com/science/article/pii/B9780721605616500198)
although my rheumatologist is in no position to give me a POTS diagnosis she very much agreed with the connections i made and said she thinks i am right on the mark with my conditions. she told me im a real academic patient and even that i’d be well suited for going into medicine lol. not only is it refreshing to have a doctor that doesn’t disregard their patient’s knowledge, but it’s good to see what i’ve learned about nerves from my biopsych classes (and in my own time for funsies) paying off in ways concerning my health. my mom who is a nurse also agrees that neuropathic POTS and erythromelalgia are what i have.
anyway the POTS symptoms have been a massive thing for me since puberty and the erythromelalgia developed a year or so after my POTS symptoms started. but i’ve always had freezing cold clammy hands and feet since i was a young child, they just hadn’t started changing colors and flaring until after i hit puberty. i’m not sure what destroyed the sympathetic nerve fibers in my legs (as most POTS happens in teenagers due to some viral illness but i’ve never had that?), i was also just tested for a bunch of autoimmune factors and disorders and my results came back negative. maybe it’s just a genetic factor, who knows, probably something caused by a hormone’s cascading effect gone awry at some point. it seems a lot of autistic afab people have POTS or some other type of dysautonomia for some reason and i’m curious as to why.
anyway i’m really stuck in a liminal space because i have no official diagnosis beyond “dysautonomia” but i’ve been sure of what it is for like over a year and it keeps getting clearer and clearer that i was right all along
51 notes
·
View notes
Text
When should you visit the Urologist?

Having problems when urinating, such as pain or itching, and noticing blood in the urine can be signs that something is not quite right in your urinary system. Who should you go to solve a possible urine problem? Although not everyone thinks about it from the first moment, the most important thing, especially if your age is over 40, is to see a specialist in the urinary system, that is, a urologist in Noida.
In the case of men, going to the best urologist in Noida is even more important since the urologist not only treats urinary tract problems but is also in charge of preserving male sexual health.
The first visit to the urologist step by step
The first step of the urological consultation is the doctor’s interview with the patient. This part of the first visit to the urologist is divided into two steps. The first is the patient’s medical history, knowing why he goes to the urologist in Ghaziabad and what pathologies he suffers or has suffered, as well as knowing if he is currently taking any relevant medication. Among the data that the doctor will ask you for are your age, the surgeries you have had, if any, your lifestyle, especially in terms of tobacco and alcohol consumption, etc.
The second part of the interview with the best urologist in Ghaziabad is to find out the patient’s family history. This is important because there is a direct relationship between genetics and the appearance of certain pathologies. Obviously, what the specialist will be most interested in is whether there is a urological history in your family, that is, problems related to prostate cancer, hematuria (blood in the urine), urinary lithiasis, incontinence or erectile dysfunction. In the case of women, the urologist will also ask about the history related to the muscles of their pelvic floor such as childbirth, postpartum, abortions, etc.
What is the next step after the interview with the urologist?
The next step in the first visit to the urologist in Greater Noida is the physical examination. When the specialist already knows all the necessary details of the patient’s health and the causes that led him to come to the consultation, it is time to assess him physically.
In the urology consultation, the general examination is mainly based on detecting if there is any urinary infection or renal involvement. However, the urologist also observes and studies the abdomen to rule out masses as well as a bladder balloon. After that, the specialist will also observe how the perineum area is located, the vaginal area in women, especially in search of pelvic organ prolapse, and the scrotal area in men to verify that its size, consistency, and sensitivity are correct.
Finally, the best urologist in Greater Noida will carry out a rectal examination in men focused on assessing the size of the prostate as well as its volume, consistency and sensitivity. This digital rectal examination is especially indicated to rule out the existence of prostate cancer.
Finally, during the first visit to the urologist in Rohini and after the history and examination, some basic tests may be necessary. Among them, the urologist usually requests a flowmetry or urine sediment test where the pH of the urine is analyzed and the presence, if any, of hematuria, bacteria, or leukocytes.
In addition, it is also common to perform a blood test to check the PSA levels in men and creatine (kidney function) of the patient. In addition to these tests, if the doctor considers it necessary, sometimes a urological ultrasound is also performed.
What happens at the end of the urological consultation?
After completing the urological consultation and the tests that have to be carried out, the urologist in Delhi will be in charge of explaining to the patient whether or not a treatment is necessary. There are many treatments and all of them depend on each particular case. For this reason, a personalized and individualized assessment is essential to ensure the most appropriate solution for each patient.
#Urologist in Noida#Best Urologist in Noida#Urologist in Greater Noida#Best Urologist in Greater Noida#Urologist in Ghaziabad#Best Urologist in Ghaziabad
0 notes
Photo

Flowmetry Plumbing Services and Solutions is the Best Mains Waterworks in Southall. They are a technical plumbing engineering company with over 25 years experience. Types of jobs are Water Tanks, Taps, Leaks, Toilet Flushes Etc.
0 notes
Text
Saw Palmetto
Scientific Names: Serenoa repens (synonyms: S. serrulata, Sabul serrata) Other Common Names: American dwarf or cabbage palm, palmier Nain, sabal fructus Overall Safety: 😊
Therapeutic Efficacy and Considerations:
BPH: 😊 Saw palmetto has been frequently compared to placebo and to finasteride for the treatment of BPH. Several meta-analyses of these studies have been performed and conclusions have all been similar: saw palmetto decreases symptoms and improves urine flowmetry to a mild-to-moderate extent with fewer side effects than finasteride. Prostate volume and PSA levels are not affected. Two trials against α-blockers found that the α-blockers had more effects on obstructive symptoms, with saw palmetto having similar or more effects on irritative symptoms. A recent high-quality trial found no difference between saw palmetto and placebo. Overall, current evidence does support a recommendation for treatment of mild-moderate BPH, especially irritative symptoms. Patients with primarily obstructive symptoms or greatly enlarged prostates will probably not benefit as much from therapy. Dose: 320 mg/day of extract standardized to 80-95% fatty acids and sterols given in one or two doses. Note: because of the possibility of masking the symptoms of prostate cancer and delaying diagnosis and treatment, patients must be screened and diagnosed by a physician prior to treating BPH with saw palmetto or any other dietary supplement. Saw palmetto is first line therapy for BPH in several European countries.
Chronic Prostatitis: 🙁 One trial has compared finasteride and saw palmetto for the treatment of chronic prostatitis. Symptoms in the saw palmetto group were improved to a similar extent as finasteride at 3 months but worsened over the rest of the treatment year. The current evidence does not support a recommendation for use for this indication.
Hair Growth Stimulant: 🙁 Only one small trial has examined efficacy for stimulation of hair growth. Although some improvement was seen, the change was not statistically significant. More research is warranted but saw palmetto cannot currently be recommended for this indication.
Prostate Cancer Prevention: 🙁 One large epidemiological study found no relationship between use and the risk of prostate cancer. Saw palmetto is not recommended for this indication.
Chemistry/Pharmacology: Saw palmetto has benefit for BPH through several mechanisms. It is a non-competitive inhibitor of both subtypes of 5-α-reductase (finasteride only inhibits type 2), the enzyme that converts testosterone into the more active dihydrotestosterone (DHT). Effects seem to be more localized; systemic levels of DHT are not generally lowered with saw palmetto therapy. Competitive inhibition of DHT receptor binding seems to occur. Apparent anti-inflammatory effects are via inhibition of cyclooxygenase and lipoxygenase, as well as mast cell inhibition. Epithelial proliferation induced by growth factor is inhibited and involution of prostate epithelium occurs. In vitro studies have demonstrated some α1 blocker activity, but this does not seem to occur in vivo. Prostate size and PSA levels are not affected with saw palmetto therapy.
Drug Interactions: Hormonal or anti-hormonal therapies (due to possible opposing or additive effects); anticoagulants (due to possible increased bleeding risk, monitor closely). Although in vitro studies noted inhibition of α1 blocker binding, clinical significance is unknown. A pharmacokinetic study determined that saw palmetto has no effect on CYP450 2D6, 1A2, 2E1, or 3A4.
Contraindications/Precautions: Pregnancy/lactation (absolute contraindication due to hormonal effects); therapeutic androgens (due to antiandrogenic activity). This medication should be used with caution in patients already receiving an alpha-blocking agent for the treatment of BPH.
Adverse Effects: Generally, well tolerated. Mild GI distress (nausea, constipation, diarrhea; take with food to minimize), headache, dizziness, possible increased blood pressure, and increased bleeding time. Reports of sexual side effects have included both improvement and worsening of libido and erectile/ejaculatory function. One case report implicated saw palmetto in acute hepatitis and pancreatitis that was clinically improved by withdrawal of the saw palmetto.
#sigler dietary supplement drug cards#2nd edition#saw palmetto#serenoa repens#serenoa serrulata#sabul serrata#american dwarf palm#cabbage palm#palmier nain#sabal fructus#drug facts
0 notes
Photo

☕ Why Is Coffee so Healthy? 21) Coffee improves blood circulation A study found that caffeine stimulates the heart in a way that makes it pump more blood than usual. Employing non-invasive laser Doppler flowmetry, the researchers discovered that after drinking some regular coffee, the participants experienced a 30 percent increase in blood circulation to their fingers for 75 minutes. Blood carries oxygen, which muscles need to function. The more oxygen your muscles receive, the better these body parts of yours can function. The better your muscles function, the better you can perform physically. #coffee #europajoe #bloodcirculation #heart
0 notes
Text
Examination of Nailfold Capillaries Can Unmask Systemic Nature of Exfoliation Glaucoma

MedicalResearch.com Interview with:

Dr. Ritch Robert Ritch, MD, FACS, FARVO Shelley and Steven Einhorn Distinguished Chair Professor of Ophthalmology, Surgeon Director Emeritus Chief, Glaucoma Services Emeritus The New York Eye and Ear Infirmary of Mount Sinai New York, NY 10003 Founder, Medical Director and Chairman, Scientific Advisory Board The Glaucoma Foundation MedicalResearch.com: What is the background for this study? Response: Nailfold capillaroscopy (NFC), long used in rheumatology is a new approach to investigation of glaucoma. Posterior to the nailbed and just anterior to the proximal nailfold is the cuticle, which has no structural elements visible to the naked eye. NFC is a non-invasive imaging modality that provides a highly magnified view of the capillaries at the nailfold of digits. It has also been used in ophthalmology to show morphological changes at the nailfold capillaries of POAG and XFG/XFS patients, helping to confirm the systemic nature of these diseases.
Nailfold Capillaroscopy / Dr. Ritch With nailfold capillaroscopy, an extensive array of capillaries can be seen greatly enlarged on a monitor screen. Capillary loops can be imaged, stored, recorded with videoscopy, and blood flow actively imaged and measured.. The first series of papers on glaucoma were written by Prof Josef Flammer’s group at the turn of the 21st century, looking at vasospasm, blood flow in normal-tension and high-tension glaucoma, and relating ocular blood flow alterations to systemic vascular regulation and relating laser Doppler flowmetry to NFC. Studies from Korea later associated nailbed hemorrhages and loss of nailbed capillaries to the presence of optic disc hemorrhages and investigated correlation of of heart rate variability with visual field defects and nailfold capillaroscopy. Studies by our group began with the publication in 2015 of a paper by Pasquale et al (Nailfold Capillary Abnormalities in Primary Open-Angle Glaucoma: A Multisite Study. IOVS;56:7021) using NFC video microscopy, associating dilated capillaries, avascular zones, and hemorrhages with primary open-angle glaucoma. Successive manuscripts and presentations at conferences have indicated differences between capillary loop patterns in high-tension and normal-tension POAG and exfoliation syndrome/exfoliation glaucoma. Our goal in this paper was to compare nailfold peripheral blood flow in XFG, which had not previously been compared to control subjects using NFC. We explored the peripheral blood flow at the nailfold of patients with high-tension glaucoma, normal-tension glaucoma, exfoliation glaucoma (XFG) and compared it to control subjects further evaluate the possible differences between these glaucoma entities. We examined the morphology and extent of nailfold capillary loops, vascular tortuosity, blood flow, and nailfold hemorrhages. MedicalResearch.com: What are the main findings? Response: Both primary open-angle glaucoma (POAC) and XFs/XFG involve abnormal blood flow, but XFS/XFG is increasingly known to be associated with cardiovascular and cerebrovascular disorders and more recently, disease of elastic tissue. XFS is a distinct disease with specific genetic, biochemical, cell biological, and pathophysiologic mechanisms leading to trabecular dysfunction. It is the most common recognizable cause of open angle glaucoma worldwide and is not a “type” or form” of glaucoma, but rather glaucoma is the most common manifestation of this systemic disease. We hypothesized that XFS/XFG would reveal more pronounced differences from primary open-angle glaucoma. We found a significantly lower and limited range of resting peripheral blood flow in XFG. This may represent stiffened vasculature or impaired maximal flow in the peripheral vasculature of XFG patients compared to control subjects. It may also be related to increased tortuosity in XFS patients. XFS has also been reported to show decreased optic nerve head blood flow to the optic nerve head. Our study is the first to show decreased non-ocular resting peripheral capillary blood flow as measured by nailfold capillaroscopy in XFG compared to control subjects even after correction for multiple co-variables. The vascular hemodynamic alteration at the peripheral nailfold circulation in XFG may represent the systemic nature and etiology of exfoliation glaucoma, which necessitates further studies. MedicalResearch.com: What should readers take away from your report? Response: What use can we conceive of to carry this work further? First, assuming that differences in nailfold capillaroscopy morphology and blood flow in different glaucomas reflect the vasculature both systemically and in the eye, this could be the beginning of a new approach to the disease. It might serve as a diagnostic tool to differentiate or substantiate findings in different glaucomas. Studies measuring blood flow might be indicative or predictive of glaucoma severity. MedicalResearch.com: What recommendations do you have for future research as a result of this work? Response: Correlations between NFC and ocular blood flow are an additional area of investigation and if these were to bear out, the results of NFC might be predictive of a predisposition to the rate of progression. The effect of drugs given topically or systemically might be reflected in nailfold capillaroscopy and counterintuitively, the effect of drugs on NFC might be reflected in measurement of ocular blood flow, providing an alternative means of assessing or verifying alterations in the ocular circulation. Future studies will hopefully provide the information to gather this information and to determine the value of NFC in glaucoma. Citation: Philip S, Najafi A, Tantraworasin A, Pasquale LR, Ritch R. Nailfold Capillaroscopy of Resting Peripheral Blood Flow in Exfoliation Glaucoma and Primary Open-Angle Glaucoma. JAMA Ophthalmol. 2019;137(6):618–625. doi:https://doi.org/10.1001/jamaophthalmol.2019.0434 Last Modified: The information on MedicalResearch.com is provided for educational purposes only, and is in no way intended to diagnose, cure, or treat any medical or other condition. Always seek the advice of your physician or other qualified health and ask your doctor any questions you may have regarding a medical condition. In addition to all other limitations and disclaimers in this agreement, service provider and its third party providers disclaim any liability or loss in connection with the content provided on this website. Read the full article
0 notes
Photo
Assessment of cutaneous microcirculation by laser Doppler flowmetry in type 1 diabetes. A new interesting article has been published in Microvasc Res. 2019 Jul;124:91-96. doi: 10.1016/j.mvr.2019.04.002. Epub 2019 Apr 6.
0 notes
Text
Symptoms that may indicate that the prostate is inflamed
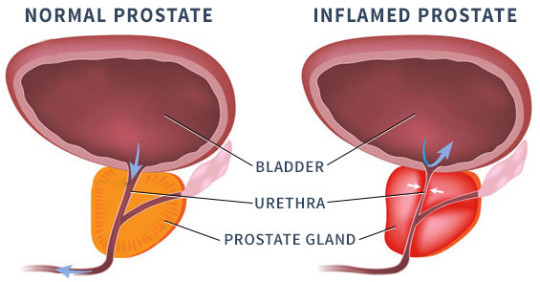
Prostatitis is characterized by an inflammation of the prostate that causes an increase in its size, which can cause symptoms such as pain, burning during urination, fever, among others, says urologist in West Delhi.
Generally, prostatitis is caused by a bacterial infection and, in general, the treatment consists in the administration of antibiotics, analgesics and anti-inflammatories indicated by the urologist.
What are the symptoms of prostatitis
The most common symptoms that may indicate the presence of a prostatitis, which is inflammation of the prostate, are mainly the decrease in the strength of the urine stream and painful urination.
In addition to the symptoms indicated, prostatitis can also cause fever and chills, especially if the prostatitis is caused by an infection. However, the only way to confirm the diagnosis is to consult a urologist in Janakpuri to indicate laboratory tests such as a blood test, urine or even an ultrasound.
When urinary frequency increases, there may be blood in the urine, which is common cause impotence due to constant pain. However, these symptoms can also be related to a urinary infection in man.
Most common causes of prostatitis
Although there are different causes that can result in inflammation of the prostate, most prostatitis is caused by an infection, especially bacteria. For this reason, it is relatively common for prostatitis to be treated with the use of antibiotics, which must be prescribed by the urologist in Palam.
In some cases, prostatitis can be caused by surgeries or injuries in the region and in some situations, it is not possible to determine what the cause is.
Classification of prostatitis
Prostatitis is classified as:
Type I – Acute bacterial prostatitis;
Type II – Chronic bacterial prostatitis;
Type III A – Pelvic pain syndrome, also known as chronic inflammatory prostatitis;
Type III B – Chronic non-inflammatory prostatitis, pelvic pain syndrome or prostatodynia;
Type IV – Asymptomatic inflammatory prostatitis.
In general, acute and chronic prostatitis present the same symptoms, only the acute one becomes chronic when the symptoms last for more than 3 months.
How the diagnosis of prostatitis is made
The diagnosis of prostatitis is made considering the symptoms referred by the patient and, which are usually related to difficulty urinating.
Also, the urologist in Dwarka can indicate the collection of urine, prostatic fluid and recommend the performance of tests such as flowmetry, digital rectal examination, PSA blood test or even biopsy to confirm the cause of the prostate enlargement.
Treatment for prostatitis
The treatment of prostatitis is indicated by the urologist in Uttam Nagar, who in most cases, identifies an infection and prescribes the use of antibiotics in tablets or, in more severe cases, medications that are applied directly intravenously at the kidney hospital in Uttam Nagar.
In addition, the doctor may also prescribe painkillers and anti-inflammatories to relieve symptoms or alpha blockers such as tamsulosin, which helps relax the neck of the bladder and muscle fibres where the prostate attaches to the bladder.
In chronic bacterial prostatitis, treatment with antibiotics lasts for approximately 3 months. However, when antibiotics do not help reduce inflammation, surgery may be necessary to remove the prostatic abscess that is causing the symptoms, says urologist in Hari Nagar.
#urologist in west delhi#urologist in janakpuri#urologist in hari nagar#urologist in dwarka#urologist in uttam nagar#kidney hospital in Uttam Nagar
0 notes
Text
Benign Prostatic Hyperplasia (BPH)
What is BPH disease?
The benign prostatic hyperplasia or BPH is the enlargement of the prostate gland. It is more common in men as their age progresses. You can then check information described by urologist in East Delhi about its causes, symptoms and treatment.
Causes and symptoms of benign prostatic hyperplasia
What is Benign Prostatic Hyperplasia (BPH)?
BPH is the non-cancerous growth of the prostate gland due to an increase in the number of cells in the gland. The large prostate is exceptional before age 40, however the enlargement increases with age and between 50 and 60 years, 50% of men present it. Many men raise their concern infront of the best urologist in East Delhi that is it cancer. But, It is not cancer, nor does it increase the risk of suffering it and its development is associated with the natural aging of the cells.
What are the symptoms of inflamed prostate?
The prostatic hyperplasia is clinically manifested called lower urinary tract symptoms (LUTS). These symptoms are divided into three groups.
Emptying symptoms
Weak, weak jetwith little torrent.
Slow urination. Some patients begin to be aware of this when they urinate in public places. They notice that the bathroom light goes out when they have not finished urinating, or when they notice that other people enter, urinate and leave, they are still urinating there.
Watering in the shower, the jet is not thin, it opens and inevitably stains the toilet lid.
Distressed urination. The patient begins urination and stops, starting again and cutting once or several times.
Delayed onset of urination. It takes to start urinating. Some patients describe it as if the urine came from far away.
Voiding effort. The patient instinctively makes some force to shorten the time of urination but sometimes does not, paradoxically, make it slower.
Increased terminal drip. The end of urination becomes a continuous drip, like a poorly closed tap.
Irritative filling symptoms
Urgency. It goes from not wanting to urinate, to have a pressing desire in a short space of time (in the path of an elevator, in a garage or in the car, forcing to stop to evacuate).
Increased urinary frequency. It starts to urinate often. There may come a time when the patient urinates before any action he is going to commit, however short it may be, a waiting line, a short drive, when entering a cinema, etc. so as not to be in a compromised situation later.
Urinary incontinence. Sometimes because it does not arrive on time, sometimes due to overflow.
Nocturia. He begins to get up at night to urinate, more and more times, losing quality of sleep and therefore of life.
Postmictional symptoms
Feeling of incomplete emptying.
Dripping postmiccional. Despite waiting a few seconds after finishing urinating and the patient has already dressed, there is a small and traitorous escape, which causes his underwear to get stained.
Urologist in Noida reminds that apart from benign prostatic hyperplasia, there are also other pathologies that give voiding symptoms and that can be confused with BPH such as the following:
Potomania
Ureteral lithiasis
Bladder tumor
Urethral stricture
Prostatitis
Foreign bodies in urethra and bladder
Urinary tract infections
Bladder neurogenic dysfunction
Detrusor muscle hypoactivity
Nocturnal polyuria
Detrusor hyperactivity, etc.
Screening and testing in patients with BPH
There is a degree of recommendation in all guides by the best urologist in Noidaregarding what diagnostic tests should be performed to diagnose inflammation of the prostate.
Recommended tests
A detailed medical history, with a physical examination that also includes a rectal examination, as well as an ultrasound and blood tests with PSA termination and finally a urinary sediment
Optional tests
Flowmetry, daily voiding, sexual function.
Treatment of benign prostatic hyperplasia
Frequently, the increase in prostate volume causes some problems or discomforts. Depending on the size of the prostate of the symptoms it generates and also on the characteristics of the person suffering from it, one or the other treatment will be established by urologist in Ghaziabad.
The treatment of benign prostatic hyperplasia less invasive is to prescribe oral medication, medications known as alpha blockers are used.
On the other hand, sometimes it is recommended by the best urologist in Ghaziabad to perform a surgical treatment. The surgical technique varies according to the prostate size, the age of the patient, the concomitant diseases, although it must also be taken into account, if the growth is of the whole prostate or only of the middle lobe, in addition to the mastery of each of the techniques by part of the urologist is an important factor. In general, in very large prostates open surgery is very effective and effective. On the contrary, in the small ones, there are different forms of transurethral resection (bipolar, laser, etc.) that also offer very good results.
When benign prostatic hyperplasia should be operated?
If the patient perceives that the symptoms produced by prostate growth, whether it is the difficulty in urinating, the frequency with which he urinates etc., worsen his quality of life.
When signs appear on the bladder -prostate ultrasound such as the significant increase in bladder thickness, the appearance of diverticula in the bladder or stones.
If recurrent urine infections arise despite treatment with correct oral medication.
Acute urinary retention is more frequent in patients with BPH. If these occur in an accidental way for example, triggered by an anesthesia a surgical intervention, It is not considered a criterion to perform the surgical operation of BPH. However, when the patient has already presented a couple of episodes of urinary retention if a criterion to be intervened will be considered.
Affects the intervention of benign prostate hypertrophy to sexual life
The interventions of benign prostate hypertrophy do not affect the erection, since they do not touch the nerves and vessels that participate in the erection mechanism. It is the same as the surgical technique is performed through the urethra or through open surgery.
The intervention of benign prostatic hypertrophy does affect ejaculation and although the patient has an orgasm of intense note, however, semen does not come out of his urethra. The semen in the prostate surgery is then mixed with the urine.
Finally, according to sexologist in Vaishali, the intervention also affects fertility, since no semen in sexual intercourse does not produce a pregnancy. However, sperm can be obtained by centrifugation of postcoital urine.
#urologist in East Delhi#best urologist in East Delhi#urologist in Noida#best urologist in Noida#urologist in Ghaziabad#best urologist in Ghaziabad#sexologist in Vaishali
0 notes
Text
52
Massachusetts Institute of Technology
Responsibility for PATENT RIGHTS. COMPANY shall assume responsibility for preparation, filing, prosecution and maintenance of all of the PATENT RIGHTS in M.I.T.'s name using attorneys acceptable to M.I.T. Such activities shall be conducted in M.I.T.'s best interest and COMPANY shall not abandon any substantive claim of the PATENT RIGHTS without permission from M.I.T. M.I.T. shall be copied on all correspondence regarding patent filing, prosecution and maintenance and shall have reasonable opportunities to advise COMPANY and shall cooperate with COMPANY in such filing, prosecution and maintenance.
Payment of all fees and costs, including attorneys fees, relating to the filing, prosecution and maintenance of the PATENT RIGHTS shall be the responsibility of COMPANY, whether such amounts were incurred before or after the EFFECTIVE DATE. COMPANY shall reimburse all amounts incurred by M.I.T. within [**] days of invoicing; late payments shall accrue interest pursuant to Section 4.2.
Tolerance is the responsibility that upholds human rights, pluralism (including cultural pluralism), democracy and the rule of law. It involves the rejection of dogmatism and absolutism and affirms the standards set out in international human rights instruments. Consistent with respect for human rights, the practice of tolerance does not mean toleration of social injustice or the abandonment or weakening of one's convictions. It means that one is free to adhere to one's own convictions and accepts that others adhere to theirs. It means accepting the fact that human beings, naturally diverse in their appearance, situation, speech, behaviour and values, have the right to live in peace and to be as they are. It also means that one’s views are not to be imposed on others.
Existing techniques may be categorized according to their underlying measurement physics principles including mechanical (plethysmography), optical [photoplethysmography, laser Doppler flowmetry (LDF), and laser speckle contrast imaging (LSCI)], acoustic (ultrasound), and thermal (various forms of thermal clearance). Plethysmography relies on the measurement of bulk changes in limb dimensions caused by changes in blood volume, thereby only providing an estimate of flow to the entire limb. Measurements typically involve strain gauges wrapped around the limb to quantify dimensional changes or, in the case of photoplethysmography, optical illumination to identify changes in optical absorption, both of which follow from changes in blood volume. Ultrasound techniques rely on acoustic Doppler shifts. Similar Doppler shifts in optical signals form the basis for laser LDF measurements.
Массачусетский технологический институт
Ответственность за патентные права. Компания принимает на себя ответственность за подготовку, подачу, судебное преследование и поддержание всех патентных прав на имя М.Т.И. с использованием адвокатов, приемлемых для М.Т.И. Такие действия должны проводиться в интересах М.Т.И., и компания не должна отказываться от каких-либо существенных претензий на ПАТЕНТНЫЕ ПРАВА без разрешения М.Т.И.. M.Т.И. копирует всю корреспонденцию, касающуюся подачи патента, судебного преследования и технического обслуживания, а так же имеет обоснованные возможности консультировать компанию и сотрудничать с компанией, что касается регистрации, судебного преследования и технического обслуживания.
Компания оплачивает все пошлины и издержки, включая гонорары адвокатов, связанные с подачей, судебным преследованием и поддержанием патентных прав, независимо от того, были ли такие суммы произведены до или после даты вступления в силу договора. Компания возмещает все суммы, понесенные М.Т.И. в течение [**] дней с момента выставления счета; за просроченные платежи начисляются проценты в соответствии с разделом 4.2.
Толерантность - это ответственность, которая защищает права человека, плюрализм (включая культурный плюрализм), демократию и верховенство права. Она предполагает отказ от догматизма и абсолютизма и подтверждает стандарты, изложенные в международных документах по правам человека. В соответствии с уважением прав человека, практика толерантности не означает терпимость к социальной несправедливости или отказ от своих убеждений или их ослабление. Это означает, что человек свободен придерживаться своих собственных убеждений и признает, что другие придерживаются своих. Это означает признание того факта, что люди, естественно различающиеся по своей внешности, должности, речи, поведению и ценностям, имеют право жить в мире и быть такими, какие они есть. Это также означает, что взгляды не должны навязываться другим.
Существующие методы могут быть классифицированы в соответствии с их принципами базовой физики измерений, включая механическое (плетизмография), оптическое [фотоплетизмография, лазерная допплеровская флоуметрия (LDF) и лазерная спекл-контрастная визуализация (LSCI)], акустическое (ультразвук) и тепловое (различные формы теплового очищения). Плетизмография основывается на измерении объемных изменений размеров конечностей, вызванных изменениями объема крови, что позволяет оценить только приток крови ко всей конечности. Измерения обычно включают в себя тензометрические датчики, обернутые вокруг конечности, для количественного определения изменений размеров или, в случае фотоплетизмографии, оптического освещения для выявления изменений в оптическом поглощении, оба из которых следуют за изменениями объема крови. Ультразвуковые методы основаны на акустических допплеровских сдвигах. Подобные допплеровские сдвиги в оптических сигналах составляют основу лазерных измерений LDF.
0 notes
Text
The diagnostic accuracy of laser Doppler flowmetry in assessing pulp blood flow in permanent teeth: A systematic review.
http://dlvr.it/QyYcQB
0 notes
Text
The diagnostic accuracy of laser Doppler flowmetry in assessing pulp blood flow in permanent teeth: A systematic review.
http://dlvr.it/QyYMKS
0 notes