#European Medicine Agency
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
The Tumblr office adopted Tommy, an 11-year-old Pomeranian.
Link
Space Nuts Episode 471: HERA's Journey and the Light of Healing Join Andrew Dunkley and Professor Fred Watson in this enlightening episode of Space Nuts, where they explore the latest developments in Space exploration and the fascinating role of light in both astronomy and human healing. Episode Highlights: - HERA Mission Milestones: Discover the latest updates on the HERA mission, including critical trajectory corrections and its upcoming Mars gravity assist. Learn about its objectives, including a close encounter with Mars' moon Deimos, and its ultimate goal of orbiting the asteroid Didymos. - Black Hole Light Echoes: Delve into the intriguing concept of black hole light echoes and how light can be bent by gravity to create multiple observations of the same event. Understand the potential of using Very Long Baseline Interferometry to study these phenomena and what it could reveal about accretion discs. - Healing with Light: Explore the historical and modern uses of light in medicine, from ancient sun worship to contemporary phototherapy treatments. Hear Andrew's personal experience with radiation therapy and the importance of regular health checks. For more Space Nuts, including our continually updating newsfeed and to listen to all our episodes, visit our website. Follow us on social media at SpaceNutsPod on facebook, X, YouTube, Tumblr, Instagram, and TikTok. We love engaging with our community, so be sure to drop us a message or comment on your favourite platform. For more Space and Astronomy News Podcasts, visit our HQ at www.bitesz.com. Become a supporter of this podcast: https://www.spreaker.com/podcast/space-nuts/support. Stay curious, keep looking up, and join us next time for more stellar insights and cosmic wonders. Until then, clear skies and happy stargazing. 00:00 - Andrew Dunkley: Coming up on Space Nuts is the HERA mission 02:11 - I'm interested in two different stories about light about the hero mission 02:59 - ESA's HERA mission will make a close approach to Mars next year 11:07 - Andrew Dunkley and Fred Watson discuss light echoes in Space Nuts 13:17 - Measuring Black Hole Light Echoes with Very Long Baseline Interferometry 21:42 - Measuring black hole light echoes with very long baseline interferometry 22:39 - Even since ancient times, we've used light for medical purposes 27:55 - Fred has been receiving radiation therapy for prostate cancer for five weeks now 34:16 - Professor Fred Watson: Believe me, I'll be around for next episode ✍️ Episode References European Space Agency https://www.esa.int Phys.org https://www.phys.org Universe Today https://www.universetoday.com Astrophysical Journal Letters https://iopscience.iop.org/journal/ 8205 5--- The Conversation https://theconversation.com Cancer Council New South Wales https://www.cancercouncil.com.au
#accretion-disc#assist#black#black-holes#dart-mission#deimos#didymos#dimorphos#echoes#european-space-agency#gravity#hera-mission#hole#light#light-therapy#mars#medicine#phobos-grunt#prostate-cancer#space-exploration
1 note
·
View note
Text
Cell And Gene Therapy For Rare Diseases
Rare diseases, defined by their low prevalence and often complex genetic origins, have long posed significant challenges for healthcare providers. Traditional treatment options have frequently been limited or ineffective, leaving many patients with few avenues for relief. However, the emergence of cell and gene therapies has marked a turning point in the field, offering transformative potential for treating previously considered untreatable conditions.

READ MORE:https://www.lifesciencesreview.com/news/cell-and-gene-therapy-for-rare-diseases-nwid-2208.html
0 notes
Text
Investigate Europe has found that the European Medicines Agency is beset by several conflicts of interest concerns over professional and financial ties to industry. It is also facing growing criticism for fast-tracking drugs that could pose serious risks to patients. At the end of 2019, two pharmaceutical consultants check-in to an Amsterdam hotel. It is one of hundreds of options in the city. It is also where experts from the European Medicines Agency (EMA) are staying for their monthly meeting. Many are their former colleagues. Senior figures from the agency’s Committee for Medicinal Products for Human Use (CHMP), its most influential body, were gathering at its headquarters in the Dutch capital. They were there to discuss applications from pharmaceutical firms wanting to market their drugs in Europe. It is these experts, plucked from their day jobs at national agencies or health authorities, that the EMA relies on to assess the merits of drugs that could be used by millions. Discussions are highly confidential. Guido Rasi, the EMA’s director until 2020, says drones were even once sent to spy on proceedings by unknown actors. The consultants, Tomas Salmonson, a Swede, and Briton Robert Hemmings, previously had a seat at the table. For years they were part of the EMA’s inner circle, in the CHMP and on expert panels. Now, through their joint enterprise Consilium Salmonson & Hemmings, they advise big pharma on how to get the coveted authorisations they once approved. After setting up Consilium, according to Rasi, the pair would corner experts in the corridors of the hotels. Their presence at hotels did raise eyebrows but the pair deny any wrongdoing. Salmonson said they “repeatedly tried to avoid” staying at the same venue, but it was not always possible. “We tried to avoid meeting CHMP members by, for example, having breakfast after the meeting started.” But it was not “100 per cent successful as on occasions we have accidentally met CHMP members in the lobby.” However, there are bigger questions that exist for the regulator. Tomas Salmonson was chairman of the CHMP for six years until September 2018. Three months later he launched his consultancy firm (Consilium Sweden AB). His friend Robert Hemmings, who was a CHMP member for 11 years, incorporated at the same time, Consilium Hemmings (UK) Ltd. “Our best work has been in partnership,” reads the website of their new venture, Consilium Salmonson & Hemmings. Significantly, as they were not EMA employees, but instead are hired by their national agencies, neither were covered by the EU’s conflict of interest framework. “EMA's committee members… are not employed by EMA and therefore the EU staff regulations do not apply to them,” a spokesperson said. This is a “significant loophole”, campaigners argue. “It is incredible that no rules are in place to prevent revolving door cases involving scientific experts,” says Shari Hinds, policy officer at Transparency International. “We urge the EMA to implement effective and comprehensive rules to prevent such cases in the future.”
continue reading
#netherlands#european medicines agency (EMA)#Committee for Medicinal Products for Human Use (CHMP)#big pharma#conflicts of interest#capitalism#long read
0 notes
Text
So apparently some Swiss company found out that Brazilian blood has more immunoglobulin (which is used in some medications made by pharma companies) than European blood, and now international pharma companies are lobbying to change Brazilian law to allow them to use our blood as a resource
There is no current evidence that those things are related, but it just so happens that at the same time there is also another law being discussed that would get rid of "bureaucracy" when it comes to ethics analyses of trials on humans. It would also remove the right, which all brazilians currently have, to access to the medication resulting from the trials they participated in
Both sources are in Portuguese because both news have been recently broke by a Brazilian investigative news agency, but if you don't speak it, you can always use automatic translation
I know there's a lot of fucked up shit happening in the world right now, but please pay attention to medical rights in Brasil right now. Especially if you're European, because virtually every company related to this is from your continent and plans to benefit you above all
ETA: using blood as a resource for these medications is not new; however, current law in brasil only allows that use to come from donated blood (because it comes from the plasma and apparently not all of it is used in blood transfusion; I'm not a doctor so I'm not clear on the details but that's the gist of it) and to be processed and used by Hemobr��s, the State-owned company that handles this type of medical technology. The new law would allow for private companies to buy our blood from blood banks for their use. It is worth noting that at least one company has already explicitly stated that they won't be making the resulting medication available in the Brazilian market, so, essentially, they will be taking blood Brazilians donated to help other Brazilians and using it to treat immunocompromised Europeans, to the detriment of immunocompromised Brazilians that need the medicine. In the process, they will be making it harder for our State-owned company to use that same blood, forcing us to import from them and therefore making the medication more expensive. They also want to make it possible for Brazilians to sell their own blood - a deeply ethically questionable practice that is discouraged by the WHO and that has led to HIV outbreaks in Brasil in the past
#i hate it here i hate it here i HATE IT HERE im sick of this shit#social justice#geopolitics#latin america#brasil#brazil#social issues#latine shit
20K notes
·
View notes
Text
The Erez border crossing, which connects Israel with northern Gaza, remains closed and no humanitarian aid has been allowed to enter the Strip through it, according to Juliette Touma, director of communications for the United Nations agency for Palestinian refugees (UNRWA), speaking to EL PAÍS from Jordan. Touma stresses that the announcement last Thursday by the Israeli authorities that they would reopen the crossing remains only “a promise.” The Israeli government implicitly confirmed the information to this newspaper. Supplies to alleviate the plight of Gaza’s population have also not yet begun arrive via the nearby port of Ashdod, 30 kilometers (18 miles) north of the enclave. These two concessions were the main commitments made by the Israeli War Cabinet following a telephone call between Prime Minister Benjamin Netanyahu and U.S. President Joe Biden.
This Indian Express article goes into detail about the volume of humanitarian aid entering Gaza
Israel says aid is moving into Gaza more quickly after international pressure to increase access, but the amount is disputed and the United Nations says it is still much less than the bare minimum to meet humanitarian needs. Israel said 419 trucks – the highest since the conflict began – entered on Monday, though the Red Crescent and United Nations gave much lower figures, with the UN saying many were only half full because of Israeli inspection rules.
Aid agencies have complained that Israel is not ensuring enough access for food, medicine and other needed humanitarian supplies and the European Union foreign policy chief Josep Borrell has accused it of using starvation as a weapon of war. UN humanitarian agency (OCHA) spokesperson Jens Laerke also pointed to severe restrictions on delivery of aid inside Gaza itself last month, saying Israel had denied permission for half the convoys it tried sending to the north in March, with UN aid convoys three times more likely to be refused than any other.
An increase in aid flows into Gaza over recent days has also been noted by Red Crescent officials in Egypt, who said more than 350 trucks had crossed from there into Gaza on Monday and 258 on Sunday. That was much more than in recent weeks, when the number was usually fewer than 200, they said. However UNRWA, the main United Nations agency in Gaza, said 223 trucks had entered on Monday, fewer than half the 500 trucks it says are required daily.In its daily situation report on Tuesday, UNRWA said “there has been no significant change in the volume of humanitarian supplies entering Gaza or improved access to the north”.
#yemen#jerusalem#tel aviv#current events#palestine#free palestine#gaza#free gaza#news on gaza#palestine news#news update#war news#war on gaza#famine#gaza genocide#genocide#genocide joe#joe biden
398 notes
·
View notes
Text
In 1975, civilian nuclear technology was part of a worldwide strategy to bring the Organization of Petroleum-Exporting Countries (OPEC) to heel. That body’s power seemed unprecedented, given that most of its countries were historically impoverished or “backward” peoples. [...]
Many developing countries did adopt nuclear technologies, often with crucial parts of their national infrastructures relying on American and European expertise, equipment, and fuel. Rather than seeing liberation from nature, such countries faced renewed forms of dependence. Iran certainly never gained reliable access to uranium and did not become the economic miracle envisioned by Ansari back in 1975. Instead of lifting up the poorer nations of the world, the global nuclear order seemed structured in ways reminiscent of the colonial era. The most heated debates within the IAEA pitted the nuclear weapons states against the so-called LDCs—less developed countries. The agency never became a storehouse for fission products. Instead, one of its primary functions was to monitor an arms control treaty—the Treaty 4 on the Non-Proliferation of Nuclear Weapons. By the end of the century, the IAEA was referred to as a “watchdog,” known for its cadre of inspectors. In 2003, IAEA inspections were crucial talking points in public debates about the invasion of Iraq by the United States [...] evidence gathered over the years by the agency created for the peaceful atom was being interpreted by the United States government as justification for military intervention. [...]
Focusing only on arms control glosses over the domestic politics of nuclear programs, particularly the role of high technology as symbols of state power and legitimacy. But it also does not square with what scholars of the Cold War have been pointing out for decades—that governments, especially the United States, deployed science and technology as diplomatic tools, to achieve feats of prestige, to shape business arrangements, to conduct clandestine surveillance, or to bind countries together with technical assistance programs. Poorer countries’ dreams of modernization, of using advanced technology to escape hunger, poverty, and the constraints of nature—these were the stock-in-trade of US diplomacy. Why, then, should we imagine that the promises connected to peaceful uses of atomic energy were any less saturated with geopolitical maneuvers and manipulation? [...]
American officials in the late 1940s and early 1950s were very worried that commercial nuclear power would siphon off supplies of uranium and monazite needed for the weapons arsenal. So they explicitly played down the possibility of electricity generation from atomic energy and instead played up the importance of radioisotopes for medicine and agriculture—because such radioisotopes were byproducts of the US weapons arsenal and did not compete with it. The kinds of technologies promoted in the developing world by the United States, the USSR, and Europeans thus seemed neocolonial, keeping the former colonies as sites of resource extraction—a fact noticed, and resented, by government officials in India, Brazil, and elsewhere. Mutation plant breeding, irradiation for insect control or food sterilization, and radioisotope studies in fertilizer—these were oriented toward food and export commodities and public health, problems indistinguishable from those of the colonial era. These were not the same kinds of technologies embraced by the global North, which focused on electricity generation through nuclear reactors, often as a hedge against the rising political power of petroleum-producing states in the Middle East. By the mid-1960s and 1970s, the United States and Europe did offer nuclear reactors even to some of the most politically volatile nations, as part of an effort to ensure access to oil. Convincing petroleum suppliers of their dire future need for nuclear reactors was part of a strategy to regain geopolitical leverage. Despite the moniker “peaceful atom,” these technologies were often bundled in trade deals with fighter jets, tanks, and other military hardware [...]
By the close of the century, two competing environmental narratives were plainly in use. One was critical of atomic energy, drawing on scientific disputes about the public health effects of radiation, the experience of nuclear accidents such as Three Mile Island (1979) and Chernobyl (1986), or the egregious stories of public health injustice—including negligence in protecting uranium miners or the wanton destruction and contamination of indigenous peoples’ homelands. In contrast was the narrative favored by most governments, depicting nuclear technology in a messianic role, promising not only abundant food, water, and electricity, but also an end to atmospheric pollution and climate change. [...]
As other scholars have noted, the IAEA tried to maintain a reputation of being primarily a technical body, devoid of politics. But it had numerous political uses. For example, it was a forum for intelligence gathering, as routinely noted by American Central Intelligence Agency (CIA) documents. It also outmaneuvered the World Health Organization and Food and Agriculture Organization in the early 1960s and was able to assert an authoritative voice playing down public health dangers from atomic energy. Further, it provided a vehicle for countries to stay engaged in atomic energy affairs even if they did not sign on to the non-proliferation treaty—India, Pakistan, and Israel most notably. It provided apartheid-era South Africa with a means of participating in international affairs when other bodies ousted it because of its blatantly racist policies. By the same token, it gave the Americans and Europeans political cover for continuing to engage with South Africa, an important uranium supplier.
Introduction to The Wretched Atom, Jacob Hamlin
55 notes
·
View notes
Note
hi! SUPER interesting excerpt on ants and empire; adding it to my reading list. have you ever read "mosquito empires," by john mcneill?
Yea, I've read it. (Mosquito Empires: Ecology and War in the Greater Caribbean, 1620-1914, basically about influence of environment and specifically insect-borne disease on colonial/imperial projects. Kinda brings to mind Centering Animals in Latin American History [Few and Tortorici, 2013] and the exploration of the centrality of ecology/plants to colonialism in Plants and Empire: Colonial Bioprospecting in the Atlantic World [Schiebinger, 2007].)
If you're interested: So, in the article we're discussing, Rohan Deb Roy shows how Victorian/Edwardian British scientists, naturalists, academics, administrators, etc., used language/rhetoric to reinforce colonialism while characterizing insects, especially termites in India and elsewhere in the tropics, as "Goths"; "arch scourge of humanity"; "blight of learning"; "destroying hordes"; and "the foe of civilization". [Rohan Deb Roy. “White ants, empire, and entomo-politics in South Asia.” The Historical Journal. October 2019.] He explores how academic and pop-sci literature in the US and Britain participated in racist dehumanization of non-European people by characterizing them as "uncivilized", as insects/animals. (This sort of stuff is summarized by Neel Ahuja, describing interplay of race, gender, class, imperialism, disease/health, anthropomorphism. See Ahuja's “Postcolonial Critique in a Multispecies World.”)
In a different 2018 article on "decolonizing science," Deb Roy also moves closer to the issue of mosquitoes, disease, hygiene, etc. explored in Mosquito Empires. Deb Roy writes: 'Sir Ronald Ross had just returned from an expedition to Sierra Leone. The British doctor had been leading efforts to tackle the malaria that so often killed English colonists in the country, and in December 1899 he gave a lecture to the Liverpool Chamber of Commerce [...]. [H]e argued that "in the coming century, the success of imperialism will depend largely upon success with the microscope."''
Deb Roy also writes elsewhere about "nonhuman empire" and how Empire/colonialism brutalizes, conscripts, employs, narrates other-than-human creatures. See his book Malarial Subjects: Empire, Medicine and Nonhumans in British India, 1820-1909 (published 2017).
---
Like Rohan Deb Roy, Jonathan Saha is another scholar with a similar focus (relationship of other-than-human creatures with British Empire's projects in Asia). Among his articles: "Accumulations and Cascades: Burmese Elephants and the Ecological Impact of British Imperialism." Transactions of the Royal Historical Society. 2022. /// “Colonizing elephants: animal agency, undead capital and imperial science in British Burma.” BJHS Themes. British Society for the History of Science. 2017. /// "Among the Beasts of Burma: Animals and the Politics of Colonial Sensibilities, c. 1840-1940." Journal of Social History. 2015. /// And his book Colonizing Animals: Interspecies Empire in Myanmar (published 2021).
---
Related spirit/focus. If you liked the termite/India excerpt, you might enjoy checking out this similar exploration of political/imperial imagery of bugs a bit later in the twentieth century: Fahim Amir. “Cloudy Swords” e-flux Journal Issue #115. February 2021.
Amir explores not only insect imagery, specifically caricatures of termites in discourse about civilization (like the Deb Roy article about termites in India), but Amir also explores the mosquito/disease aspect invoked by your message (Mosquito Empires) by discussing racially segregated city planning and anti-mosquito architecture in British West Africa and Belgian Congo, as well as anti-mosquito campaigns of fascist Italy and the ascendant US empire. German cities began experiencing a non-native termite infestation problem shortly after German forces participated in violent suppression of resistance in colonial Africa. Meanwhile, during anti-mosquito campaigns in the Panama Canal zone, US authorities imposed forced medical testing of women suspected of carrying disease. Article features interesting statements like: 'The history of the struggle against the [...] mosquito reads like the history of capitalism in the twentieth century: after imperial, colonial, and nationalistic periods of combatting mosquitoes, we are now in the NGO phase, characterized by shrinking [...] health care budgets, privatization [...].' I've shared/posted excerpts before, which I introduce with my added summary of some of the insect-related imagery: “Thousands of tiny Bakunins”. Insects "colonize the colonizers". The German Empire fights bugs. Fascist ants, communist termites, and the “collectivism of shit-eating”. Insects speak, scream, and “go on rampage”.
---
In that Deb Roy article, there is a section where we see that some Victorian writers pontificated on how "ants have colonies and they're quite hard workers, just like us!" or "bugs have their own imperium/domain, like us!" So that bugs can be both reviled and also admired. On a similar note, in the popular imagination, about anthropomorphism of Victorian bugs, and the "celebrated" "industriousness" and "cleverness" of spiders, there is: Claire Charlotte McKechnie. “Spiders, Horror, and Animal Others in Late Victorian Empire Fiction.” Journal of Victorian Culture. December 2012. She also addresses how Victorian literature uses natural science and science fiction to process anxiety about imperialism. This British/Victorian excitement at encountering "exotic" creatures of Empire, and popular discourse which engaged in anthropormorphism, is explored by Eileen Crist's Images of Animals: Anthropomorphism and Animal Mind and O'Connor's The Earth on Show: Fossils and the Poetics of Popular Science, 1802-1856.
Related anthologies include a look at other-than-humans in literature and popular discourse: Gothic Animals: Uncanny Otherness and the Animal With-Out (Heholt and Edmunson, 2020). There are a few studies/scholars which look specifically at "monstrous plants" in the Victorian imagination. Anxiety about gender and imperialism produced caricatures of woman as exotic anthropomorphic plants, as in: “Murderous plants: Victorian Gothic, Darwin and modern insights into vegetable carnivory" (Chase et al., Botanical Journal of the Linnean Society, 2009). Special mention for the work of Anna Boswell, which explores the British anxiety about imperialism reflected in their relationships with and perceptions of "strange" creatures and "alien" ecosystems, especially in Aotearoa. (Check out her “Anamorphic Ecology, or the Return of the Possum.” Transformations. 2018.)
And then bridging the Victorian anthropomorphism of bugs with twentieth-century hygiene campaigns, exploring "domestic sanitation" there is: David Hollingshead. “Women, insects, modernity: American domestic ecologies in the late nineteenth century.” Feminist Modernist Studies. August 2020. (About the cultural/social pressure to protect "the home" from bugs, disease, and "invasion".)
---
In fields like geography, history of science, etc., much has been said/written about how botany was the key imperial science/field, and there is the classic quintessential tale of the British pursuit of cinchona from Latin America, to treat mosquito-borne disease among its colonial administrators in Africa, India, and Southeast Asia. In other words: Colonialism, insects, plants in the West Indies shaped and influenced Empire and ecosystems in the East Indies, and vice versa. One overview of this issue from Early Modern era through the Edwardian era, focused on Britain and cinchona: Zaheer Baber. "The Plants of Empire: Botanic Gardens, Colonial Power and Botanical Knowledge." May 2016. Elizabeth DeLoughrey and other scholars of the Caribbean, "the postcolonial," revolutionary Black Atlantic, etc. have written about how plantation slavery in the Caribbean provided a sort of bounded laboratory space. (See Britt Rusert's "Plantation Ecologies: The Experiential Plantation [...].") The argument is that plantations were already of course a sort of botanical laboratory for naturalizing and cultivating valuable commodity plants, but they were also laboratories to observe disease spread and to practice containment/surveillance of slaves and laborers. See also Chakrabarti's Bacteriology in British India: laboratory medicine and the tropics (2012). Sharae Deckard looks at natural history in imperial/colonial imagination and discourse (especially involving the Caribbean, plantations, the sea, and the tropics) looking at "the ecogothic/eco-Gothic", Edenic "nature", monstrous creatures, exoticism, etc. Kinda like Grove's discussion of "tropical Edens" in the colonial imagination of Green Imperialism.
Dante Furioso's article "Sanitary Imperialism" (from e-flux's Sick Architecture series) provides a summary of US entomology and anti-mosquito campaigns in the Caribbean, and how "US imperial concepts about the tropics" and racist pathologization helped influence anti-mosquito campaigns that imposed racial segregation in the midst of hard labor, gendered violence, and surveillance in the Panama Canal zone. A similar look at manipulation of mosquito-borne disease in building empire: Gregg Mitman. “Forgotten Paths of Empire: Ecology, Disease, and Commerce in the Making of Liberia’s Plantation Economy.” Environmental History. 2017. (Basically, some prominent medical schools/departments evolved directly out of US military occupation and industrial plantations of fruit/rubber/sugar corporations; faculty were employed sometimes simultaneously by fruit companies, the military, and academic institutions.) This issue is also addressed by Pratik Chakrabarti in Medicine and Empire, 1600-1960 (2014).
---
Meanwhile, there are some other studies that use non-human creatures (like a mosquito) to frame imperialism. Some other stuff that comes to mind about multispecies relationships to empire:
Lawrence H. Kessler. “Entomology and Empire: Settler Colonial Science and the Campaign for Hawaiian Annexation.” Arcadia (Spring 2017)
No Wood, No Kingdom: Political Ecology in the English Atlantic (Keith Pluymers)
Archie Davies. "The racial division of nature: Making land in Recife". Transactions of the Institute of British Geographers Volume 46, Issue 2, pp. 270-283. November 2020.
Yellow Fever, Race, and Ecology in Nineteenth-Century New Orleans (Urmi Engineer Willoughby, 2017)
Pasteur’s Empire: Bacteriology and Politics in France, Its Colonies, and the World (Aro Velmet, 2022)
Tom Brooking and Eric Pawson. “Silences of Grass: Retrieving the Role of Pasture Plants in the Development of New Zealand and the British Empire.” The Journal of Imperial and Commonwealth History. August 2007.
Under Osman's Tree: The Ottoman Empire, Egypt, and Environmental History (Alan Mikhail)
The Herds Shot Round the World: Native Breeds and the British Empire, 1800-1900 (Rebecca J.H. Woods, 2017)
Imperial Bodies in London: Empire, Mobility, and the Making of British Medicine, 1880-1914 (Kristen Hussey, 2021)
Red Coats and Wild Birds: How Military Ornithologists and Migrant Birds Shaped Empire (Kirsten Greer, 2020)
Animality and Colonial Subjecthood in Africa: The Human and Nonhuman Creatures of Nigeria (Saheed Aderinto, 2022)
Imperial Creatures: Humans and Other Animals in Colonial Singapore, 1819-1942 (Timothy P. Barnard, 2019)
Biotic Borders: Transpacific Plant and Insect Migration and the Rise of Anti-Asian Racism in America, 1890-1950 (Jeannie N. Shinozuka)
#ecology#bugs#multispecies#landscape#indigenous#haunted#temporal#colonial#imperial#british entomology in india#mosquitoes#carceral#tidalectics#intimacies of four continents#carceral geography#pathologization
87 notes
·
View notes
Text







[ 📹📸 Major destruction is evident everywhere one looks after Israeli Occupation Forces withdrew its soldiers and vehicles from the Karama, Intelligence towers, Sudaniya, al-Saftawi and al-Tawam neighborhoods in Gaza City.]
🇮🇱⚔️🇵🇸 🚨
💥ISRAELI TANKS WITHDRAW FROM PARTS OF NORTHERN GAZA AS BOMBARDMENT CONTINUES FOR 119TH DAY💥
119 days into Israel's ongoing war of genocide in the Gaza Strip, the Israeli Occupation Forces (IOF) withdrew tanks and armored personnel carriers from the Karam neighborhood, as well as the intelligence towers and the al-Sidaniya neighborhood, even as the occupation's bombardment across various parts of the Gaza Strip continues unabated.
Belgium has announced it has called upon the Israeli ambassador to the central European country to explain Israel's bombing of the Belgian Agency for Development and Cooperation in Gaza after IOF warplanes bombarded and flattened the building.
Interestingly, Belgium's Foreign Minister, Hadjab Lahbib, declared on the social media platform X, "targeting civilian buildings is unacceptable." However, silence as Israel has flattened more than 2/3rds of all buildings in the Gaza Strip belies Belgium's unwillingness to confront the Israeli occupation.
Meanwhile, scores of civilians were killed, and dozens more wounded after Israeli aircraft targeted a residential home in the eastern outskirts of Rafah City, in the southern Gaza Strip.
In addition, six Palestinians were killed after occupation aircraft targeted the Al-Diri Family home in the al-Nasr neighborhood of Rafah City.
At the same time, an occupation airstrike targeting the Deeri family home in the Nasr neighborhood left four dead and wounded several others.
The decomposing corpses of six individuals were transported from the north of Deir al-Balah to Al-Aqsa Martyrs Hospital after the withdrawal of IOF soldiers and vehicles from the area.
In southern Gaza, one civilian was killed and multiple others wounded in Khan Yunis as a result of an occupation airstrike on the al-Amal School where the displaced were seeking shelter from Israel's ongoing bombardment, while 13 additional casualties were recorded after occupation warplanes targeted a civilian home in the vicinity of the Palestinian Red Crescent Society (PRCS) headquarters in the west of Khan Yunis City.
As Israel's bombardment goes on, more than 30'000 civilians sheltering near the Nasser Medical Complex in Khan Yunis face severe water shortages, as well as shortages of food and critical medicines.
A multitude of civilians were also martyred, and several others injured after Israeli forces bombarded a civilian gathering in the vicinity of a stadium in Gaza City while attempting to repair communications and Internet services in the neighborhood.
Several dozen corpses were also discovered northwest of Gaza City after occupation forces and vehicles withdrew from several neighborhoods in the area, revealing the scenes of major destruction and carnage left behind by the Israeli entity.
In the central Gaza Strip, occupation artillery and airstrikes targeted various areas in the al-Bureij Refugee Camp, while occupation jets bombed buildings in the Sheikh Zayed area, as well as in Beit Lahia in northern Gaza.
Israeli jets also launched several firebelts on the Tal Elhwa and Daraj neighborhoods in northern Gaza, while occupation forces destroyed the police headquarters in Gaza City.
Occupation tanks and armored vehicles withdrew from the vicinity of Al-Aqsa University before relocating to the Nasser Hospital area west of Khan Yunis to terrorize civilians near the local medical complex. Additionally, occupation aircraft also bombarded the Taliba Towers neighborhood in Khan Yunis.
Meanwhile, Gaza's Medical authorities are reporting that the IOF has committed a total of 95 massacres resulting in 936 deaths and 1'652 casualties in the period since the International Court of Justice at The Hague ruled that Israel must take steps to reduce civilian harm in its all-out war on Gaza.
Medical sources with PRCS are reporting the continued siege and bombardment of the Al-Amal Hospital area for the 11th consecutive day, with occupation artillery shelling and gunfire targeting the area, while occupation soldiers repeatedly raid the hospital premises, firing towards civilians and medical staff while terrorizing the displaced and the hospital's patients.
Al-Amal's medical staff also reported burying five Palestinian civilians in the courtyard of the hospital complex, bringing the number of buried on the premises to 15.
PRCS is also reporting seven patients severely wounded who face life threatening injuries as a result of occupation shelling and gunfire, warning of their deaths if the wounded cannot be relocated to a better equipped hospital.
As a result of Israel's ongoing genocide, more than 27'000+ Palestinians have been martyred, while another 66'000+ have been wounded by occupation bombing and shelling across the Gaza Strip since October 7th, 2023.
#source1
#source2
#source3
#source4
#source5
#photosource
#videosource
@WorkerSolidarityNews
#gaza#gaza strip#gaza news#gaza war#gaza genocide#genocide in gaza#genocide of palestinians#israeli genocide#israeli war crimes#war crimes#crimes against humanity#israeli occupation forces#iof#israeli occupation#israel#palestine#palestinians#palestine news#war#middle east#israel palestine conflict#politics#news#geopolitics#israeli military#world news#global news#international news#breaking news#current events
34 notes
·
View notes
Text
By: Azeen Ghorayshi
Published: May 13, 2024
After 30 years as one of England’s top pediatricians, Dr. Hilary Cass was hoping to begin her retirement by learning to play the saxophone.
Instead, she took on a project that would throw her into an international fire: reviewing England’s treatment guidelines for the rapidly rising number of children with gender distress, known as dysphoria.
At the time, in 2020, England’s sole youth gender clinic was in disarray. The waiting list had swelled, leaving many young patients waiting years for an appointment. Staff members who said they felt pressure to approve children for puberty-blocking drugs had filed whistle-blower complaints that had spilled into public view. And a former patient had sued the clinic, claiming that she had transitioned as a teenager “after a series of superficial conversations with social workers.”
The National Health Service asked Dr. Cass, who had never treated children with gender dysphoria but had served as the president of the Royal College of Pediatrics and Child Health, to independently evaluate how the agency should proceed.
Over the next four years, Dr. Cass commissioned systematic reviews of scientific studies on youth gender treatments and international guidelines of care. She also met with young patients and their families, transgender adults, people who had detransitioned, advocacy groups and clinicians.
Her final report, published last month, concluded that the evidence supporting the use of puberty-blocking drugs and other hormonal medications in adolescents was “remarkably weak.” On her recommendation, the N.H.S. will no longer prescribe puberty blockers outside of clinical trials. Dr. Cass also recommended that testosterone and estrogen, which allow young people to develop the physical characteristics of the opposite sex, be prescribed with “extreme caution.”
Dr. Cass’s findings are in line with several European countries that have limited the treatments after scientific reviews. But in America, where nearly two dozen states have banned the care outright, medical groups have endorsed the treatments as evidence-based and necessary.
The American Academy of Pediatrics declined to comment on Dr. Cass’s specific findings, and condemned the state bans. “Politicians have inserted themselves into the exam room, which is dangerous for both physicians and for families,” Dr. Ben Hoffman, the organization’s president, said.
The Endocrine Society told The New York Times that Dr. Cass’s review “does not contain any new research” that would contradict its guidelines. The federal health department did not respond to requests for comment.
Dr. Cass spoke to The Times about her report and the response from the United States. This conversation has been edited and condensed for clarity.
What are your top takeaways from the report?
The most important concern for me is just how poor the evidence base is in this area. Some people have questioned, “Did we set a higher bar for this group of young people?” We absolutely didn’t. The real problem is that the evidence is very weak compared to many other areas of pediatric practice.
The second big takeaway for me is that we have to stop just seeing these young people through the lens of their gender and see them as whole people, and address the much broader range of challenges that they have, sometimes with their mental health, sometimes with undiagnosed neurodiversity. It’s really about helping them to thrive, not just saying “How do we address the gender?” in isolation.
You found that the quality of evidence in this space is “remarkably weak.” Can you explain what that means?
The assessment of studies looks at things like, do they follow up for long enough? Do they lose a lot of patients during the follow-up period? Do they have good comparison groups? All of those assessments are really objective. The reason the studies are weak is because they failed on one or more of those areas.
The most common criticism directed at your review is that it was in some way rigged because of the lack of randomized controlled trials, which compare two treatments or a treatment and a placebo, in this field. That, from the get-go, you knew you would find that there was low-quality evidence.
People were worried that we threw out anything that wasn’t a randomized controlled trial, which is the gold standard for study design. We didn’t, actually.
There weren’t any randomized controlled trials, but we still included about 58 percent of the studies that were identified, the ones that were high quality or moderate quality. The kinds of studies that aren’t R.C.T.s can give us some really good information, but they have to be well-conducted. The weakness was many were very poorly conducted.
There’s something I would like to say about the perception that this was rigged, as you say. We were really clear that this review was not about defining what trans means, negating anybody’s experiences or rolling back health care.
There are young people who absolutely benefit from a medical pathway, and we need to make sure that those young people have access — under a research protocol, because we need to improve the research — but not assume that that’s the right pathway for everyone.

[ The Tavistock Gender Identity Development Service in London, which until recently was the National Health Service’s sole youth gender clinic in England. ]
Another criticism is that this field is being held to a higher standard than others, or being exceptionalized in some way. There are other areas of medicine, particularly in pediatrics, where doctors practice without high-quality evidence.
The University of York, which is kind of the home of systematic reviews, one of the key organizations that does them in this country, found that evidence in this field was strikingly lower than other areas — even in pediatrics.
I can’t think of any other situation where we give life-altering treatments and don’t have enough understanding about what’s happening to those young people in adulthood. I’ve spoken to young adults who are clearly thriving — a medical pathway has been the right thing for them. I’ve also spoken to young adults where it was the wrong decision, where they have regret, where they’ve detransitioned. The critical issue is trying to work out how we can best predict who’s going to thrive and who’s not going to do well.
In your report, you are also concerned about the rapid increase in numbers of teens who have sought out gender care over the last 10 years, most of whom were female at birth. I often hear two different explanations. On the one hand, there’s a positive story about social acceptance: that there have always been this many trans people, and kids today just feel freer to express who they are. The other story is a more fearful one: that this is a ‘contagion’ driven in large part by social media. How do you think about it?
There’s always two views because it’s never a simple answer. And probably elements of both of those things apply.
It doesn’t really make sense to have such a dramatic increase in numbers that has been exponential. This has happened in a really narrow time frame across the world. Social acceptance just doesn’t happen that way, so dramatically. So that doesn’t make sense as the full answer.
But equally, those who say this is just social contagion are also not taking account of how complex and nuanced this is.
Young people growing up now have a much more flexible view about gender — they’re not locked into gender stereotypes in the way my generation was. And that flexibility and fluidity are potentially beneficial because they break down barriers, combat misogyny, and so on. It only becomes a challenge if we’re medicalizing it, giving an irreversible treatment, for what might be just a normal range of gender expression.
What has the response to your report been like in Britain?
Both of our main parties have been supportive of the report, which has been great.
We have had a longstanding relationship with support and advocacy groups in the U.K. That’s not to say that they necessarily agree with all that we say. There’s much that they are less happy about. But we have had an open dialogue with them and have tried to address their questions throughout.
I think there is an appreciation that we are not about closing down health care for children. But there is fearfulness — about health care being shut down, and also about the report being weaponized to suggest that trans people don’t exist. And that’s really disappointing to me that that happens, because that’s absolutely not what we’re saying.
I’ve reached out to major medical groups in the United States about your findings. The American Academy of Pediatrics declined to comment on your report, citing its own research review that is underway. It said that its guidance, which it reaffirmed last year, was “grounded in evidence and science.”
The Endocrine Society said “we stand firm in our support of gender-affirming care,” which is “needed and often lifesaving.”
I think for a lot of people, this is kind of dizzying. We have medical groups in the United States and Britain looking at the same facts, the same scientific literature, and coming to very different conclusions. What do you make of those responses?
When I was president of the Royal College of Pediatrics and Child Health, we did some great work with the A.A.P. They are an organization that I have enormous respect for. But I respectfully disagree with them on holding on to a position that is now demonstrated to be out of date by multiple systematic reviews.
It wouldn’t be too much of a problem if people were saying “This is clinical consensus and we’re not sure.” But what some organizations are doing is doubling down on saying the evidence is good. And I think that’s where you’re misleading the public. You need to be honest about the strength of the evidence and say what you’re going to do to improve it.
I suspect that the A.A.P., which is an organization that does massive good for children worldwide, and I see as a fairly left-leaning organization, is fearful of making any moves that might jeopardize trans health care right now. And I wonder whether, if they weren’t feeling under such political duress, they would be able to be more nuanced, to say that multiple truths exist in this space — that there are children who are going to need medical treatment, and that there are other children who are going to resolve their distress in different ways.
Have you heard from the A.A.P. since your report was published?
They haven’t contacted us directly — no.
Have you heard from any other U.S. health bodies, like the Department of Health and Human Services, for example?
No.
Have you heard from any U.S. lawmakers?
No. Not at all.
Pediatricians in the United States are in an incredibly tough position because of the political situation here. It affects what doctors feel comfortable saying publicly. Your report is now part of that evidence that they may fear will be weaponized. What would you say to American pediatricians about how to move forward?
Do what you’ve been trained to do. So that means that you approach any one of these young people as you would any other adolescent, taking a proper history, doing a proper assessment and maintaining a curiosity about what’s driving their distress. It may be about diagnosing autism, it may be about treating depression, it might be about treating an eating disorder.
What really worries me is that people just think: This is somebody who is trans, and the medical pathway is the right thing for them. They get put on a medical pathway, and then the problems that they think were going to be solved just don’t go away. And it’s because there’s this overshadowing of all the other problems.
So, yes, you can put someone on a medical pathway, but if at the end of it they can’t get out of their bedroom, they don’t have relationships, they’re not in school or ultimately in work, you haven’t done the right thing by them. So it really is about treating them as a whole person, taking a holistic approach, managing all of those things and not assuming they’ve all come about as a result of the gender distress.
I think some people get frustrated about the conclusion being, well, what these kids need is more holistic care and mental health support, when that system doesn’t exist. What do you say to that?
We’re failing these kids and we’re failing other kids in terms of the amount of mental health support we have available. That is a huge problem — not just for gender-questioning young people. And I think that’s partly a reflection of the fact that the system’s been caught out by a growth of demand that is completely outstripping the ability to provide it.
We don’t have a nationalized health care system here in the United States. We have a sprawling and fragmented system. Some people have reached the conclusion that, because of the realities of the American health care system, the only way forward is through political bans. What do you make of that argument?
Medicine should never be politically driven. It should be driven by evidence and ethics and shared decision-making with patients and listening to patients’ voices. Once it becomes politicized, then that’s seriously concerning, as you know well from the abortion situation in the United States.
So, what can I say, except that I’m glad that the U.K. system doesn’t work in the same way.
-
When asked after this interview about Dr. Cass’s comments, Dr. Hoffman, the A.A.P.’s president, said that the group had carefully reviewed her report and “added it to the evidence base undergoing a systematic review.” He also said that “Any suggestion the American Academy of Pediatrics is misleading families is false.”
--



#Azeen Ghorayshi#Dr. Hilary Cass#Hilary Cass#Cass review#Cass report#medical scandal#medical malpractice#medical corruption#gender affirming care#gender affirming healthcare#gender affirmation#sex trait modification#religion is a mental illness
14 notes
·
View notes
Text
The synthetic opioid fentanyl was first synthesized in Belgium around 1960. With effects similar to those of morphine but a potency 100 times higher, it became widely used in surgeries and the treatment of chronic painful diseases. Meanwhile in the United States, unregulated and unprescribed fentanyl became a highly addictive and dangerous illegal drug—one that is 50 times stronger than heroin, with even a 2 milligram dose proving to be lethal to most people. But drug policy experts and government officials agree that there has not been a fentanyl crisis in Europe, its place of origin—at least, not until now.
In 2022, more than 70,000 people died in the U.S. of synthetic drug overdose, according to estimates made by the country’s Centers for Disease Control and Prevention. By contrast, in Europe, the latest data from the European Union’s drug monitoring agency shows that 137 people died of drugs of fentanyl’s ilk in 2021, with most of those deaths coming from diverted fentanyl medicines rather than illicitly manufactured substances. Last year, the U.S. Drug Enforcement Agency reported that it seized more than 79.5 million fentanyl-laced fake pills and nearly 12,000 pounds of fentanyl powder. Such confiscations in Europe, although rising recently, have been sporadic.
But European governments are increasingly fretting that fentanyl and similar synthetic opioids may grip the continent and plunge it into a U.S.-style crisis. Late last year, U.S. Secretary of State Antony Blinken told his European counterparts that they either have an undiscovered problem with fentanyl or may have one soon. And scattered signs that the lethal drugs may be starting to spread into the continent are now prompting governments to act.
There are several reasons for the rising fears about fentanyl in Europe. The European Union estimates that most of the roughly 1 million European consumers of illicit opioids use heroin. So far, almost all of that supply has come from Afghanistan. But beginning in April 2022, the Taliban banned “poppy cultivation and all types of narcotics,” and as a result, the area where poppy flowers—from which opium is produced—are grown in the country shrank by 95 percent last year, according to a November 2023 report by the United Nations Office on Drugs and Crime. This has drastically reduced the supply of quality heroin coming out of last year’s harvest.
Facing the shortage, criminal groups are expected to either start supplying heroin mixed with other synthetic opioids such as fentanyl to increase its strength, or to replace it altogether with fentanyl.
“The experience in North America with fentanyl overtaking heroin in major drug markets is illustrative of how a cheaper and readily available synthetic opioid can easily displace heroin,” wrote researchers in the United Nations Office on Drugs and Crime report.
European authorities are already seeing signs that organized crime groups are eyeing the trade of these opioids in Europe. The Italian secret services found that the powerful Calabrian ‘Ndrangheta mafia, which has been flooding Europe with cocaine over the past decades, is testing the fentanyl market in the continent, senior Italian government official Alfredo Mantovano said in March.
Another major concern is that Europe has an existing lab capacity to produce synthetic drugs on its soil. Europol, the European Union’s police agency, said this month that synthetic drug production and trafficking has expanded from mainly Belgium and the Netherlands to Eastern Europe, including Ukraine. In 2021, European authorities dismantled 434 laboratories producing illicit synthetic drugs, according to the latest data published by the European Monitoring Centre for Drugs and Drug Addiction (EMCDDA). Officials conclude that if criminals wanted to produce fentanyl in Europe, they would have the capacity to do it—and, consequently, to trigger a crisis very quickly.
“To be frank, I don’t see how we can avoid it in Europe. I don’t see why criminal networks would avoid selling fentanyl in Europe. The question for me is not if it’s going to touch Europe; it’s when and how big the wave or the hurricane will be. European governments are fully aware of it,” said Pierre Lapaque, a board member of the International Narcotics Control Board, in an interview with Foreign Policy.
The European effort to prevent a potential outbreak of addiction to these drugs has happened on two levels. On the one hand, the continent is reinforcing and adapting its fight against producers and traffickers, including precursors (the substances used as ingredients in drugs). On the other, it is preparing on the health care front to prevent overdose deaths.
One key measure has been the creation of a new drug agency for the bloc, turning the EMCDDA into a full-fledged agency called the European Union Drugs Agency. This new EU-wide body, which becomes operational in July, will carry out health and security assessments on synthetic drugs, closely monitoring any developments across the bloc and helping with the adoption of countermeasures. The new agency will also monitor drug precursors and set up a network of laboratories to identify new substances and define possible trends in the synthetic drug market.
The European Commission, the EU’s executive arm, also plans to speed up and broaden the way that drug precursors are scheduled in order to prevent criminal networks from finding new ways to get the chemical substances needed to produce illicit drugs. It is also seeking to improve checks at European ports. To this end, it has earmarked more than 200 million euros (about $214 million) to fund modern kits for scanning containers for hidden drugs or precursors.
“We are seeing what is happening in the U.S., and we are monitoring any development in the EU to make sure we can anticipate and disrupt any production or trafficking activities of these drugs,” said Claire Georges, Europol’s deputy spokeswoman. The EU police agency is working with the United States to get a better intelligence picture of which criminal groups may be involved.
“Those are the right responses,” said Vanda Felbab-Brown, a senior fellow at the Brookings Institution. “This is in striking contrast with what, until several months ago, was the attitude of many European drug policy experts, who would often say ‘Look, we are not going to have a fentanyl problem because we didn’t have the same initiation through pharmaceutical opioids.’ I was always very uncomfortable with that answer.”
The EU is also seeking to boost cooperation with China, a major producer of fentanyl and its precursors. Chinese representatives held talks in Brussels on April 23 on illegal drug production as well as the diversion and trafficking of precursors and other chemical substances needed to manufacture synthetic drugs.
Collaboration with China is crucial for both the United States and Europe. A 64-page report issued in mid-April by the U.S. House of Representatives’ select committee on China defined the country as “the ultimate geographic source of the fentanyl crisis.” The committee has further argued that China encourages the manufacturing and export of illicit fentanyl chemicals and other narcotics through tax rebates and holds ownership interest in local companies tied to drug trafficking. Additionally, its security services have failed to cooperate with the United States when law enforcement officials requested assistance, according to the report.
European countries are also taking measures at the national level. For instance, Italy has started to monitor the import and export flows of medicines containing fentanyl and the chemical precursors of synthetic drugs, as well as the retail market—including on the web—as part of a national plan against the deadly drug that Rome unveiled last month. At the same time, it plans to equip police officers with portable mass spectrometers to spot synthetic drugs and precursors, both during custom checks and while patrolling the streets.
The Italian Ministry of Health has instructed hospitals and pharmacies to strengthen the protection measures against the theft of fentanyl and similar opioids. It also instructed doctors assisting patients displaying a range of specific symptoms—such as respiratory depression, nausea, vomiting, and vertigo—to consider that they could be intoxicated by fentanyl and could be treated with naloxone, which is an opioid antagonist, or other medicines that can rapidly reverse an opioid overdose. Naloxone will also be provided to the police, who may need it as first responders facing an overdose or after inadvertently inhaling fentanyl during investigations. All ambulances will also be required to carry the medication.
In Spain, where there have been a few instances of drug dealers found with small amounts of fentanyl, some regional authorities are training drug users and emergency personnel on overdose reversal. The national government is also working to speed up the existing warning system on drugs by expanding free drug-checking programs across the country and the testing of wastewater to detect anomalies related to opioids, Joan Villabí, the official in charge of drugs and addiction at the Spanish Health Ministry, told Foreign Policy.
“We are monitoring in a very systematic way. When heroin hit Spain in the late 1970s, we were completely unprepared. It was a disaster,” Villabí said.
Universal medical care may have also protected Europe from a U.S.-style fentanyl crisis. In the United States, many people addicted to fentanyl began with prescription opioids, got hooked, and then when their prescriptions ran out, turned to the illegal market, where criminal rings provided them with the drug.
In the European Union, however, regulated and publicly funded health care systems have maintained a more limited access to prescription opioids, says Esther Gramage, a lecturer at the CEU San Pablo University in Madrid. The access to other procedures to alleviate pain also may have helped keep European patients away from painkillers. But there are growing reasons to fear that public health care won’t be sufficient to shield Europe.
6 notes
·
View notes
Text
APPROVATO IL FARMACO PER IL TRATTAMENTO PRECOCE DELL’ALZHEIMER

Il Comitato per i Medicinali per Uso Umano dell’Agenzia Europea per i Medicinali ha approvato l’uso del lecanemab, un anticorpo monoclonale diretto contro la proteina amiloide, per il trattamento della malattia di Alzheimer in fase precoce.
Questo farmaco ha dimostrato la sua efficacia in seguito ai risultati dello studio effettuato su 1795 pazienti che ne hanno provato la capacità di rallentare il declino cognitivo causato dalla malattia, superando i rischi associati agli effetti collaterali. L’ospedale San Raffaele di Milano è primo centro italiano a somministrare il farmaco. “L’approvazione di lecanemab da parte dell’EMA segna un momento storico nel trattamento della malattia di Alzheimer. Questo farmaco offre una nuova speranza per tutte le persone affette da Alzheimer in fase iniziale, permettendo un intervento che potrebbe modificare l’evoluzione della malattia. È un passo avanti che, come neurologi e ricercatori, accogliamo con profonda soddisfazione”, afferma il professor Massimo Filippi, primario dell’Unità di Neurologia, del servizio di Neurofisiologia e dell’Unità di Neuroriabilitazione dell’IRCCS Ospedale San Raffaele.
La malattia di Alzheimer è una condizione neurologica progressiva e irreversibile che colpisce le funzioni cerebrali, in particolare quelle cognitive inclusa la memoria, il pensiero e il comportamento, che interessa in Italia circa 1 milione di persone. Il principio attivo lecanemab può essere somministrato tramite infusione in vena una volta ogni due settimane.
___________________
Fonte: European Medicines Agency; Ospedale San Raffaele; immagine di Andrea Picquadio

VERIFICATO ALLA FONTE Guarda il protocollo di Fact checking delle notizie di Mezzopieno
BUONE NOTIZIE CAMBIANO IL MONDO Firma la petizione per avere più informazione positiva in giornali e telegiornali

Se trovi utile il nostro lavoro e credi nel principio del giornalismo costruttivo non-profit | sostieni Mezzopieno
4 notes
·
View notes
Text
Forensic report due at an opportune moment!
Peter Halligan
Nov 05, 2024
Unable to cross-post this, so here is the link:
Data Crimes: Deleting Covid Vaccine Deaths
My “cliff notes” - Dutch first doses reduced by 878,000 to reflect only remaining Dutch people who had received just one FIRST dose - deleting emigrants and the deceased - problem is, only 40,000 Dutch people emigrate every year and deaths are around 170,000 a year - official government data is corrupt.
2017: 150,214 deaths, 2020: 168,678, 2022: 170,112 and 169,000 died in 2023.
Emigration 2017: 43,441, 2020: 40,198 - lockdowns thereafter for 2021 and 2022???
This cannot be reconciled to the 878,000 removed records of those who have received first doses.
Here is a taste from Sonia’s SubStack article:
“My second interview with Wouter Aukema, senior data patterns & forensics analyst, who has over 30 years of experience working with governments and corporations- is the most explosive yet. The first interview can be watched below.”
“For the past few years, Wouter Aukema and his team have been downloading voluminous amounts of weekly data on the case safety reports on drugs and vaccines submitted to the European Medicines Agency’s EudraVigilance database and Dutch government institutions, such as the Dutch Health Institute. His painstaking work has led to the discovery of what can easily be described as massive data fraud, which he has written about here.”
“However, the data crimes do not end there and are not exclusive to the Netherlands- at around 37 minutes into the interview, Wouter dropped the biggest bombshell of all! He exclusively informed me that according to his systematic downloading of the data from EudraVigilance (which includes case safety reports from around the world not just the EU)- 40% of worldwide serious case safety reports (including hospitalizations and death) in relation to Covid vaccines (only) have been REMOVED from the European Medicines Agency’s database from October 2021-November 2022. In addition, case safety reports have also been retroactively modified, after their data lockpoint (DLP).”
2 notes
·
View notes
Text
Lower drug pricing does not follow from an expansion of innovative medicine indications, according to Dutch researchers. They claim pharma companies often fail to pass on their financial gain to patients and health services. If more patients are prescribed a certain medicine, the price could be reduced because pharmaceutical companies can recoup the research costs incurred more quickly, researchers from Erasmus University Rotterdam and the Erasmus Medical Centre Rotterdam claim. This finding emerges from their study published in the peer-reviewed PLoS ONE journal last February. The study considers the possible financial effects of a broader use of two cancer drugs, pembrolizumab (Keytruda) and daratumumab (Darzalex), which have already been approved by the European Medicines Agency (EMA) and the Food and Drug Administration (FDA) in the US. “Pharmaceutical companies are responsible for their own pricing strategy; it is not up to academics to dictate what exact price reduction to accept,” study first author Renaud Heine told Euractiv. However, when asked about the potential of this new pricing method, the Dutch Association for Innovative Medicines (VIG), which is a member of EFPIA, cited arguments raised by economics professor Lieven Annemans that the proposed model change does not value true innovation and that value-based pricing remains more appropriate. Indication broadening and pricing Heine explained they aimed to study the effect of indication broadening on price when applying cost-based pricing (CBP). “Our results indicate that cost-based prices drop consistently after indication broadening and are below known list prices,” he said. Building on the CBP model developed by two researchers, Uyl-de Groot and Löwenberg, in 2018, the research group explored price changes of these medicines if there was a continuous indication expansion. Both drugs are immuno-oncology drugs. Pembrolizumab was first used for only one type of tumour, but now it is prescribed for approximately 35 different indications for various types of tumours. Daratumumab was initially used for one type of cancer, multiple myeloma. It is now prescribed for eight other indications within multiple myeloma. While development costs for new drugs can be significantly high for the first indication, they become lower with each expansion of use in new indications. However, this financial gain for pharmaceutical companies is often not passed on to society despite the lower costs, the researchers say.
continue reading

#netherlands#big pharma#drug pricing#cost of research#expanded use of drugs#financial gain#not past on#capitalism
5 notes
·
View notes
Text
How to Choose the Right Propofol Injection Supplier in India
When it comes to choosing the right pharmaceutical products for healthcare needs, ensuring quality and reliability is critical. One such important product is propofol, a widely used anesthetic in surgeries and intensive care units. As hospitals, healthcare facilities, and medical professionals look for dependable suppliers, finding the right propofol injection manufacturers in India becomes essential to guarantee patient safety and the success of medical procedures.

India has emerged as a key player in the global pharmaceutical industry, with many companies producing and exporting high-quality medications, including propofol injections. However, given the variety of options available, selecting the right propofol injection supplier in India can be a challenging task. This blog provides a comprehensive guide on how to choose the best supplier, ensuring that you partner with a company that meets your needs in terms of quality, pricing, regulatory compliance, and service.
1. Evaluate the Manufacturer’s Reputation and Experience
The first factor to consider when selecting a propofol injection supplier in India is the manufacturer’s reputation and experience. Look for companies with a long-standing history in the pharmaceutical industry, as this demonstrates stability, expertise, and trustworthiness.
The best pharma companies in India are known for their commitment to producing high-quality products and adhering to international standards. A manufacturer with a strong track record will have an established reputation for delivering safe and effective medications. Customer reviews, certifications, and feedback from healthcare professionals can provide insights into the company’s reliability.
A key point is to check if the manufacturer is a recognized propofol injection distributor in India. Distribution experience ensures that the company has established supply chains and logistics systems, which are critical for timely and consistent delivery of pharmaceutical products.
2. Ensure Compliance with Regulatory Standards
Compliance with national and international regulatory standards is a non-negotiable aspect when choosing a propofol injection manufacturer in India. Indian pharmaceutical companies are required to adhere to stringent guidelines set by the Central Drugs Standard Control Organization (CDSCO), ensuring that their products meet safety and efficacy standards.
In addition to domestic regulations, if you are seeking a supplier for international needs, it is important to verify that the propofol injection exporter in India complies with the regulatory requirements of your country. For instance, propofol injections intended for export to the United States must meet FDA (Food and Drug Administration) guidelines, while those going to Europe must comply with EMA (European Medicines Agency) standards.
Check if the manufacturer has the necessary certifications, such as:
GMP (Good Manufacturing Practice): Ensures that products are consistently produced and controlled according to quality standards.
WHO-GMP: Recognized by the World Health Organization, ensuring that the pharmaceutical company meets global standards.
ISO Certifications: Indicate the company’s commitment to quality management systems.
By selecting a supplier with these certifications, you can be confident that the propofol injections you receive are of the highest quality and safety.
3. Assess the Quality of Propofol Injections
Quality is one of the most critical aspects when it comes to selecting propofol injection suppliers in India. Propofol is an intravenous anesthetic agent that must be manufactured under strictly controlled conditions to ensure its purity and safety. Poorly manufactured propofol can lead to adverse reactions, infections, or even fatal outcomes.
When evaluating the quality of propofol injections, consider the following:
Sterility: Ensure that the manufacturer adheres to sterile production techniques to prevent contamination.
Purity: The product should meet all pharmacopoeial standards for purity to avoid side effects or complications during anesthesia.
Stability: The product must remain stable and effective throughout its shelf life.
Packaging: The packaging should protect the injection from contamination and degradation. Ampoules or vials should be well-sealed and easy to handle for healthcare professionals.
Some propofol injection distributors in India may offer samples, which allow healthcare providers to evaluate the product’s quality before making large orders. Taking advantage of this option can help ensure you are selecting a reliable supplier.
4. Consider the Supplier’s Distribution Network
The availability of pharmaceutical products is crucial, especially when they are used in critical care settings. A good propofol injection distributor in India will have an extensive distribution network to ensure timely delivery, no matter where your healthcare facility is located.
When assessing a supplier’s distribution capabilities, consider:
Geographical Reach: Does the supplier have a presence across India or in the specific regions where you need the product? Can they also handle international shipments if necessary?
Logistics Efficiency: How quickly can they deliver propofol injections to your facility? Are they equipped to handle emergencies and provide fast delivery when needed?
Cold Chain Management: Propofol injections must be stored at specific temperatures to maintain their efficacy. Ensure that the supplier has proper cold chain management in place to prevent the product from degrading during transportation.
Choosing a supplier with a reliable distribution network ensures that you will have consistent access to propofol injections, reducing the risk of supply shortages or delays in patient care.
5. Compare Pricing and Cost-Effectiveness
Pricing is a significant consideration when selecting propofol injection manufacturers in India. While the cost should never compromise quality, finding a supplier that offers competitive pricing can make a big difference, especially for healthcare facilities managing tight budgets.
It is essential to compare the pricing of different propofol injection suppliers in India to determine which one offers the best value for money. However, keep in mind that the cheapest option is not always the best. The focus should be on the cost-effectiveness of the product—are you getting a high-quality, reliable product at a reasonable price?
Some suppliers may offer discounts or bulk purchasing options, which can further help reduce costs. Be sure to inquire about these options when negotiating with suppliers.
6. Evaluate Customer Service and Support
A strong relationship with your propofol injection supplier in India is essential for ensuring smooth operations and access to critical products when you need them. Customer service plays a vital role in this relationship, so it is important to select a supplier that prioritizes customer satisfaction.
Consider the following when evaluating customer service:
Responsiveness: How quickly does the supplier respond to inquiries or issues? Are they available to address urgent concerns?
Support: Does the supplier offer technical support or assistance with product-related questions? Can they provide guidance on proper storage and usage?
Problem Resolution: How does the supplier handle issues like product defects or delivery delays? Do they offer a clear process for resolving problems?
The best pharma company in India will prioritize customer service and work to build long-term partnerships with healthcare providers. They should be willing to collaborate with you to ensure your needs are met and that you have access to reliable, high-quality propofol injections.
7. Consider Export Capabilities for International Needs
If you are sourcing propofol injections for international purposes, it is important to select a propofol injection exporter in India with experience in global markets. Exporting pharmaceuticals comes with additional complexities, including regulatory compliance, customs clearance, and international shipping logistics.
The best exporters will have a clear understanding of these processes and be able to navigate them smoothly. They should be able to provide documentation, such as certificates of analysis, that meet the regulatory requirements of the destination country. Additionally, they should have a track record of successfully shipping propofol injections to other countries without issues related to product quality or delays.
Conclusion
Choosing the right propofol injection supplier in India is a decision that requires careful consideration of various factors, including the manufacturer’s reputation, regulatory compliance, product quality, distribution network, pricing, and customer service. By taking the time to evaluate potential suppliers against these criteria, healthcare providers can ensure that they are partnering with a company that will meet their needs and provide reliable, high-quality propofol injections.
India is home to some of the best pharma companies in India, known for producing and exporting safe, effective medications, including propofol injections. Whether you are sourcing for domestic or international needs, selecting the right supplier will ensure that your healthcare facility has access to the critical medications needed to deliver excellent patient care.
2 notes
·
View notes
Text

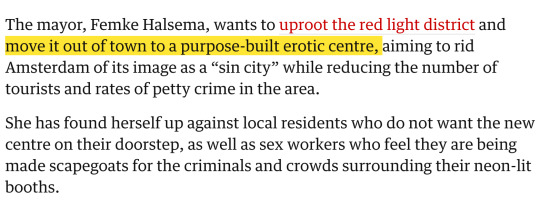
Amsterdam sex workers protest against plan to move red light district (The Guardian, Oct 19 2023)
"Halsema has long opposed the centuries-old red light district, known as De Wallen, where sex workers stand in windows waiting for customers.
The city council has earmarked three possible sites for the erotic centre, which would have 100 rooms for sex workers.
One sex worker, who identified herself as Lucie, dismissed the idea as “one big gentrification project”.
She said: “It’s mainly about combating the crowds in De Wallen, but that is not the sex workers’ fault so I don’t see why we should be punished for it.”
The European Medicines Agency has been caught up in the controversy after it emerged that one possible site for the erotic centre was near its headquarters.
The EMA voiced outrage, saying it could affect the safety of people working late at the office. (…)
Moving the red light district is Amsterdam’s latest effort to transform its image as a party capital.
It has also launched a “stay away” campaign to discourage stag nights and boozy tourists, which caused a stir in Britain after the council said it would start by targeting British men aged 18 to 35."
6 notes
·
View notes
Text
Crafting Clear Skin: The Precision of Salicylic Acid Manufacturing
Salicylic acid has long been a cornerstone in skincare and pharmaceutical formulations, celebrated for its remarkable efficacy in treating acne, exfoliating the skin, and managing various dermatological conditions. As a leading ingredient in numerous products, the demand for high-quality salicylic acid is unwavering. Salicylic acid manufacturers play a crucial role in meeting this demand, employing advanced technologies, stringent quality control measures, and innovative processes to produce this essential compound. In this blog, we explore the world of salicylic acid manufacturing, highlighting its significance, processes, benefits, and why it’s a cornerstone of modern skincare and pharmaceutical solutions.

The Importance of Salicylic Acid
Salicylic acid is a beta-hydroxy acid (BHA) derived from natural sources like willow bark and wintergreen leaves or synthesized in laboratories. It is renowned for its ability to penetrate pores, exfoliate dead skin cells, and reduce inflammation, making it a powerful ingredient in acne treatments, chemical peels, and dandruff shampoos. Its keratolytic properties help to soften and shed the outer layer of skin, promoting cell turnover and revealing a smoother, clearer complexion.
For more information salicylic acid manufacturer
Advanced Manufacturing Processes
Manufacturing salicylic acid involves sophisticated chemical processes to ensure purity, potency, and safety. The most common method is the Kolbe-Schmitt reaction, which synthesizes salicylic acid from sodium phenoxide and carbon dioxide under high pressure and temperature. This method yields high-purity salicylic acid, suitable for both pharmaceutical and cosmetic applications. Manufacturers utilize advanced equipment and precise control systems to maintain optimal reaction conditions, ensuring consistent quality and yield.
Quality Control and Assurance
Quality control is paramount in salicylic acid manufacturing. Rigorous testing protocols are implemented at every stage of production, from raw material selection to final product packaging. Analytical techniques such as high-performance liquid chromatography (HPLC), gas chromatography (GC), and mass spectrometry (MS) are used to verify the purity, potency, and stability of salicylic acid. These tests ensure that the final product meets stringent industry standards and regulatory requirements, guaranteeing safety and efficacy for consumers.
Customization and Innovation
Salicylic acid manufacturers often work closely with cosmetic and pharmaceutical companies to develop customized formulations tailored to specific product needs. Whether creating a potent acne treatment, a gentle exfoliating cleanser, or an effective dandruff shampoo, manufacturers provide expertise in optimizing salicylic acid concentrations and formulations for maximum benefit. This collaborative approach fosters innovation, resulting in new and improved products that address evolving consumer demands and dermatological advancements.
Sustainability and Ethical Practices
In response to growing environmental concerns, many salicylic acid manufacturers are adopting sustainable and ethical practices. This includes sourcing raw materials from renewable resources, minimizing waste and emissions, and implementing energy-efficient technologies. Some manufacturers are also exploring greener synthesis methods that reduce environmental impact while maintaining high-quality production standards. These efforts align with the broader industry trend toward sustainability and responsible manufacturing.
Meeting Regulatory Standards
Compliance with regulatory standards is a critical aspect of salicylic acid manufacturing. Regulatory bodies such as the FDA (Food and Drug Administration) and EMA (European Medicines Agency) set stringent guidelines for the production and use of salicylic acid in cosmetic and pharmaceutical products. Manufacturers must adhere to Good Manufacturing Practices (GMP) and ensure their products are free from contaminants, properly labeled, and safe for consumer use. Regular audits and inspections by regulatory authorities help maintain compliance and uphold product integrity.
Future Trends and Innovations
The future of salicylic acid manufacturing is marked by continuous innovation and adaptation to emerging trends. Advances in green chemistry, biotechnology, and nanotechnology are poised to revolutionize production methods, enhancing efficiency and sustainability. Additionally, research into new applications and formulations of salicylic acid promises to expand its role in skincare and healthcare, offering consumers even more effective and versatile solutions.

Conclusion
Salicylic acid manufacturers are at the forefront of producing one of the most versatile and effective ingredients in skincare and pharmaceuticals. Through advanced manufacturing processes, stringent quality control, and a commitment to innovation and sustainability, these manufacturers ensure the consistent supply of high-quality salicylic acid. As consumer demand for effective skincare solutions continues to grow, the role of salicylic acid manufacturers remains vital, driving the development of products that promote healthier, clearer skin and improved well-being. Embrace the power of precision and discover the transformative benefits of expertly crafted salicylic acid.
2 notes
·
View notes