#Clinical Evaluation Tool
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
In 2020, 27% of US Tumblr users had an annual household income of over $100,000.
Text
UTKU ERDEM OZER (3)

Welcome to our comprehensive guide on the latest advancements in orthopedic services available at Utku Erdem Ozer's clinic. At the forefront of innovative treatment options, we specialize in addressing common yet complex musculoskeletal issues, including injuries related to the anterior cruciate ligament (ACL) and hip labrum tears. Our expert team is dedicated to providing personalized care tailored to meet your unique needs, whether you're facing a sports injury or considering hip replacement surgery.
Anterior Cruciate Ligament (ACL)
The Anterior Cruciate Ligament (ACL) is a critical structure in the knee that helps stabilize the joint during movements, particularly in sports. Injuries to the ACL can be debilitating, often requiring thorough evaluation and treatment to restore function and reduce pain.
Understanding the symptoms and treatment options for an ACL injury is paramount. Common signs include:
Sudden pain and swelling in the knee
A popping sound at the time of injury
Instability during activities, especially when pivoting or cutting
When it comes to treatment, options may vary based on the severity of the injury. For minor injuries, physical therapy and rehabilitation exercises can lead to recovery. However, more severe cases may require surgical intervention to reconstruct the ACL. This procedure often involves using grafts from the patient or a donor to replace the damaged ligament.
With advancements in surgical techniques and rehabilitation protocols, many patients experience a successful return to their pre-injury activities, including sports. It is essential to consult with a specialist to develop a personalized treatment plan that best suits your needs.
Don't let an Anterior Cruciate Ligament (ACL) injury hold you back. Seek professional advice and explore your options today to get back on track!
Hip Labrum Tear
A hip labrum tear is a common injury that can result from repetitive motions or traumatic incidents. This focused damage affects the fibrocartilage structure that surrounds the hip joint, leading to pain and reduced range of motion. If you are experiencing discomfort in your hip, particularly during activities such as walking, running, or twisting, it may be a sign of a hip labrum tear.
Symptoms often include a persistent ache in the hip or groin area, stiffness, and a sensation of catching or locking in the joint. These can significantly hinder daily activities and overall quality of life. Early diagnosis and treatment are crucial to preventing further joint damage. Specialists recommend various treatment options ranging from physical therapy to hip replacement surgery, depending on the severity of the tear.
At our facility, we prioritize a comprehensive approach to your recovery. Our experienced team utilizes cutting-edge diagnostic tools to accurately identify the injury and tailor a treatment plan specific to your needs. We understand that every patient is unique, and we are dedicated to providing individualized care.
If you're seeking relief from hip labrum tear or exploring how anterior cruciate ligament (ACL) issues may impact your recovery, don’t hesitate to contact us. Our commitment to your health ensures you receive the best possible outcome. Take the first step toward improved mobility and comfort today.
Hip Replacement Surgery
When it comes to addressing chronic hip pain or serious injuries, hip replacement surgery stands out as a transformative option. This procedure is designed to eliminate pain and restore mobility, significantly enhancing the quality of life for patients suffering from conditions such as osteoarthritis or severe hip labrum tears.
With advancements in medical technology, hip replacement surgeries have evolved, providing patients with options such as minimally invasive techniques. These approaches not only reduce recovery times but also lead to less scarring and a quicker return to daily activities, ensuring that you can get back on your feet sooner.
Furthermore, the materials used in hip prosthetics have seen remarkable improvements, offering superior durability and compatibility with the human body. This means that patients can expect longer-lasting results and a significantly reduced risk of complications, allowing for a more active lifestyle post-surgery.
Choosing to undergo hip replacement surgery is a significant decision, but when performed by experienced professionals, the results can be life-changing. If you’re considering this procedure, don’t hesitate to seek more information and discuss your options with a qualified healthcare provider.
341 notes
·
View notes
Text
The Autism Diagnosis Deep Dive: Navigating Assessments & Next Steps
Part 1: The "Why Bother?" - Reasons for Seeking a Formal Diagnosis
Before we even talk about how to get diagnosed, let's address the elephant in the room: why would someone go through this often lengthy, sometimes expensive, and emotionally taxing process? The reasons are as diverse as autistic people themselves, but here are some big ones:
Self-Understanding & Validation: This is HUGE, especially for late-diagnosed adults. Suddenly, a lifetime of feeling "different," struggling with social cues, or having intense sensory experiences has a name. It’s not that you’re "broken" or "weird"; your brain is just wired differently. That validation can be incredibly powerful and healing. It’s like finally getting the instruction manual to a device you’ve been fumbling with for years.
Access to Support & Services: A formal diagnosis is often the key to unlocking supports.
For kids: This can mean Individualized Education Programs (IEPs) or 504 plans in school, access to therapies (speech, occupational, developmental), and other early intervention services.
For adults: This might mean workplace accommodations, access to specific mental health professionals who understand autism, disability benefits (in some cases), or specialized support groups.
Community & Connection: Finding out you're autistic can open the door to a vibrant, supportive community of other autistic people. Sharing experiences, finding solidarity, and learning from others who get it is invaluable. The online autistic community, especially on platforms like Tumblr, is a force to be reckoned with!
Informing Others & Self-Advocacy: A diagnosis can give you the language and confidence to explain your needs and differences to family, friends, educators, and employers. It’s a tool for self-advocacy.
Understanding Co-occurring Conditions: Autism often travels with friends like ADHD, anxiety, depression, OCD, Ehlers-Danlos Syndrome (EDS), and gastrointestinal issues. A diagnostic process can help identify these, leading to more comprehensive support.
Tumblr Truth Bomb: Self-diagnosis is widely accepted and validated within the autistic community, especially given the barriers (cost, accessibility, clinician bias) to formal diagnosis. This article focuses on the formal process, but that doesn't invalidate anyone's self-discovery journey. Many seek formal diagnosis for the reasons above, even after self-identifying.
Part 2: The "Who You Gonna Call?" - Professionals Involved in Diagnosis
Navigating the medical and psychological world can feel like trying to read a map written in ancient hieroglyphics. Here’s a breakdown of the types of professionals who might be involved:
For Children:
Pediatrician/Developmental Pediatrician: Often the first port of call. They can do initial developmental screenings (like the M-CHAT-R/F for toddlers) and refer you to specialists. Developmental pediatricians specialize in developmental differences and delays.
Child Psychologist/Neuropsychologist: These professionals are often the ones conducting the comprehensive diagnostic evaluations. They use standardized tests, observation, and interviews.
Child Psychiatrist: Can diagnose and also prescribe medication if co-occurring conditions like ADHD or anxiety need pharmacological support.
Speech-Language Pathologist (SLP) & Occupational Therapist (OT): While they don't typically give the primary autism diagnosis, their assessments of communication, sensory processing, and motor skills are vital parts of the overall picture and often contribute to the diagnostic team's decision.
For Adults:
Clinical Psychologist/Neuropsychologist: Similar to working with children, these professionals are often the primary diagnosticians for adults. They'll use adapted tools and place more emphasis on developmental history and self-report.
Psychiatrist: Can diagnose, especially if you're already seeing one for other mental health concerns. They can also help manage co-occurring conditions.
Neurologist: Less common for primary diagnosis unless there are other neurological concerns, but they can sometimes be involved.
General Practitioner (GP)/Primary Care Physician (PCP): Like pediatricians for kids, they can be a starting point for a referral, though their direct experience with adult autism diagnosis can vary wildly.
Value Add Tip: Look for professionals who specialize in autism, particularly adult autism if that's relevant. Ask about their experience, their approach (is it neurodiversity-affirming?), and what the assessment process entails. Don't be afraid to "interview" them!
Part 3: The "Assessment Arsenal" - What Actually Happens?
Okay, this is where it gets dense, but stay with me! The diagnostic process isn't just a quick quiz. It's a comprehensive evaluation designed to gather information from multiple sources.
Key Components (can vary by age and clinician):
Developmental History & Interviews:
For kids: Parents/caregivers will be interviewed extensively about the child's development from birth, social interactions, communication patterns, repetitive behaviors, interests, and sensory sensitivities. School reports and teacher input are also crucial.
For adults: You'll be asked about your childhood (as much as you can remember or gather from family), your social experiences, communication style, interests, sensory profile, and current challenges. Input from a partner or close family member can sometimes be helpful, but the focus is on your experience.
Direct Observation & Interaction:
This is where tools like the ADOS-2 (Autism Diagnostic Observation Schedule, Second Edition) come in. It's a semi-structured, play-based (for kids) or conversation-based (for adults) assessment where the clinician observes social communication, interaction, and imaginative use of materials. It’s designed to create social situations where autistic traits might become apparent.
Tumblr Real Talk: The ADOS isn't foolproof. Masking (consciously or unconsciously suppressing autistic traits) can affect results, especially in girls, women, and AFAB individuals, or those who've learned to "perform" neurotypically. A good clinician understands this.
Standardized Questionnaires & Rating Scales:
ADI-R (Autism Diagnostic Interview-Revised): A structured interview often used with parents/caregivers, focusing on developmental history related to autism traits.
SRS-2 (Social Responsiveness Scale): Measures social awareness, social cognition, social communication, social motivation, and autistic mannerisms. Can be completed by parents, teachers, or self (for older individuals).
CARS-2 (Childhood Autism Rating Scale): Used to identify children with autism and determine symptom severity.
AQ (Autism Spectrum Quotient): A self-report questionnaire for adults.
RAADS-R (Ritvo Autism Asperger Diagnostic Scale-Revised): Another self-report for adults.
Many, many others! Clinicians pick tools based on age, suspected presentation, and their own expertise.
Cognitive & Language Assessments:
IQ/Cognitive Testing (e.g., WISC, WAIS, Stanford-Binet): To understand cognitive strengths and weaknesses. Autism can co-occur with any level of intellectual ability. Important Note: Autistic individuals can have "spiky profiles" – very high abilities in some areas and significant challenges in others. This doesn't always translate well on standardized IQ tests.
Speech and Language Evaluation: Assesses receptive (understanding) and expressive (using) language, pragmatics (social use of language), and nonverbal communication.
Adaptive Behavior Assessments (e.g., Vineland Adaptive Behavior Scales):
Evaluates daily living skills, communication, social skills, and motor skills compared to age-matched peers. This helps understand the level of support an individual might need.
Sensory Profile: Questionnaires or discussions about sensitivities to light, sound, touch, taste, smell, and movement.
Medical & Neurological Examination (Sometimes): To rule out other medical conditions that might explain symptoms.
The Goal: To build a comprehensive picture. No single test "diagnoses" autism. It's about patterns of behavior, developmental history, and how these impact daily life, all considered against established diagnostic criteria (usually from the DSM-5-TR or ICD-11).
Tumblr Pro-Tip for Assessment Day:
Be Yourself: Easier said than done, especially if you mask. But try to be as authentic as possible.
Write Things Down: Beforehand, jot down examples of your experiences, challenges, and traits. It's easy to forget in the moment.
Bring a Support Person (if allowed/helpful): For moral support or to help recall information (especially for adult diagnosis if a parent or long-term partner is involved).
Ask Questions: If you don't understand something, ask!
It's Okay to Be Nervous/Overwhelmed: This is a big deal. Allow yourself to feel whatever you're feeling.
Part 4: The "Big Reveal" - Receiving the Report & Diagnosis
After all the assessments, there's usually a feedback session where the clinician discusses their findings and provides a written report. This report can be LONG and full of clinical jargon.
If Diagnosed Autistic:
The Emotional Cocktail: Get ready for a potential mix of:
Relief/Validation: "I'm not broken! There's a reason!"
Grief: For the life you might have imagined, for past struggles, for not knowing sooner.
Confusion/Overwhelm: "What does this mean? What now?"
Anger: At past misdiagnoses, at people who didn't understand.
Joy/Excitement: About connecting with a new community and understanding yourself better.
The Report: It will outline the tests done, your (or your child's) scores, observations, and how these meet (or don't meet) diagnostic criteria. It should also include recommendations. Ask the clinician to walk you through it in plain language.
If Not Diagnosed Autistic (but you strongly suspect it):
This can be incredibly invalidating and confusing.
Ask Why: Understand the clinician's reasoning. Did they consider masking? Are they experienced with subtle presentations or adult diagnosis?
Seek a Second Opinion: If you feel the assessment wasn't thorough or the clinician wasn't a good fit, you have the right to get another opinion, especially from someone specializing in the autistic presentation you identify with (e.g., autism in women/AFAB individuals, PDA profile).
Remember Self-Identification: Even without a formal "yes," if the autistic experience resonates deeply, your self-understanding is valid. The autistic community largely embraces this.
Part 5: The "Okay, So Now What?" - Navigating Next Steps
A diagnosis isn't an endpoint; it's a signpost. Here's where the journey really begins.
Breathe. Process. Feel.
Give yourself time. There's no "right" way to react. Talk to trusted friends, family, or a therapist. Journal. Engage in your special interests. Whatever helps you process.
Tumblr Hug: You are not alone in this. Many have walked this path.
Connect with the Autistic Community:
This is arguably one of the MOST important steps. Find autistic-led groups online (Tumblr, Facebook, Twitter/X, Reddit, Discord) or in person.
Listen to #ActuallyAutistic voices. Read blogs, watch videos, follow creators. They offer insights, support, and a sense of belonging that non-autistic professionals often can't.
Value Add: This community can help you decipher what "autism" actually means in lived experience, beyond clinical definitions.
Learn (and Unlearn):
Read books by autistic authors. Learn about neurodiversity as a paradigm.
Unlearn harmful stereotypes about autism (e.g., that all autistics are like Rain Man, lack empathy, or are non-verbal).
Explore concepts like masking, burnout, autistic inertia, monotropism, and special interests (or "spIns").
Consider Therapies & Supports (if needed/wanted):
Crucial Caveat: The goal of support should be to help the autistic person thrive as an autistic person, not to make them "less autistic" or "more neurotypical." Avoid any therapy aiming to "cure" or "normalize" autism.
Occupational Therapy (OT): Can help with sensory processing issues, motor skills, daily living skills, emotional regulation. Look for OTs with a neurodiversity-affirming approach.
Speech-Language Therapy (SLP): Can help with social communication (pragmatics), understanding non-literal language, alternative communication methods (AAC), and feeding issues. Again, ensure they respect autistic communication styles.
Mental Health Support (Therapy/Counseling): Many autistic people benefit from therapy to deal with anxiety, depression, trauma (often from navigating a neurotypical world), or to process their diagnosis. Seek therapists who are autism-knowledgeable AND affirming.
ABA (Applied Behavior Analysis): This is a highly controversial topic.
Traditional ABA has been criticized by many autistic adults for being compliance-based, traumatic, and aiming to suppress autistic behaviors (like stimming) rather than supporting underlying needs.
Some newer/modified forms claim to be more child-led and focus on functional skills.
Tumblr PSA: DO YOUR RESEARCH. Listen to autistic adults about their experiences with ABA. If considering it, scrutinize the provider's methods, goals, and respect for autistic identity. Many autistic advocates advise against it entirely or urge extreme caution.
Social Skills Groups: Can be helpful IF they focus on understanding social dynamics and providing tools, rather than forcing neurotypical masking. Autistic-led groups are often best.
Parent Training/Support (for parents of autistic kids): Focus on understanding your child's needs, adapting the environment, and advocating for them, not changing who they are.
Accommodations & Environmental Adjustments:
School: IEPs/504 plans can provide classroom accommodations (e.g., noise-canceling headphones, visual schedules, movement breaks, modified assignments).
Work: Reasonable accommodations might include a quieter workspace, flexible hours, written instructions, permission to use stim toys.
Home: Create sensory-friendly spaces. Reduce clutter. Establish routines if helpful. Honor sensory needs (e.g., specific food textures, clothing fabrics).
Embrace Strengths & Special Interests:
Autism isn't just a list of deficits! Autistic people often have incredible strengths: intense focus, attention to detail, loyalty, strong sense of justice, unique perspectives, deep knowledge in areas of interest.
Special interests are not "obsessions" to be discouraged; they are sources of joy, learning, regulation, and expertise! Lean into them!
Self-Advocacy & Setting Boundaries:
Learn to communicate your needs. It’s okay to say no, to ask for clarification, to leave overwhelming situations.
This is a skill that develops over time, especially if you've spent years masking.
Patience & Self-Compassion:
This is a marathon, not a sprint. There will be good days and hard days. Be kind to yourself. You're learning a new way of understanding yourself and navigating the world.
Part 6: The "Don't Forget This Stuff!" - Final Thoughts & Value Nuggets
Autism is a Spectrum, Not a Line: It's a diverse constellation of traits. "If you've met one autistic person, you've met one autistic person." Support needs vary wildly.
Masking is Real & Exhausting: Many autistics (especially women, AFAB individuals, and people of color) learn to camouflage their traits to fit in. This can delay diagnosis and lead to burnout.
Late Diagnosis is Valid: Discovering you're autistic as an adult is increasingly common and incredibly validating. It's never "too late."
Internalized Ableism is a Thing: You might have absorbed negative messages about autism or disability. Unpacking this is part of the journey.
Celebrate Neurodiversity: The idea that neurological differences like autism are natural variations in the human genome, not disorders to be cured. Embrace it!
Phew! We made it through the deep dive! Getting an autism diagnosis can feel like the end of one chapter and the very overwhelming beginning of another. But armed with knowledge, community, and self-compassion, it can also be the start of a more authentic, understood, and supported life.
What are your experiences with the diagnostic process? Any tips for folks just starting out? Spill the tea in the comments/reblogs! Let's support each other!
#Autism #Autism Diagnosis #ActuallyAutistic #Neurodiversity #Autistic Adults #Autistic Children #ASD #Sensory Processing #Special Interests #ADOS #Mental Health #Support #Self Advocacy #Tumblr Explains #Long Post #Worth The Read #Neurodivergent #Autism Acceptance
118 notes
·
View notes
Text
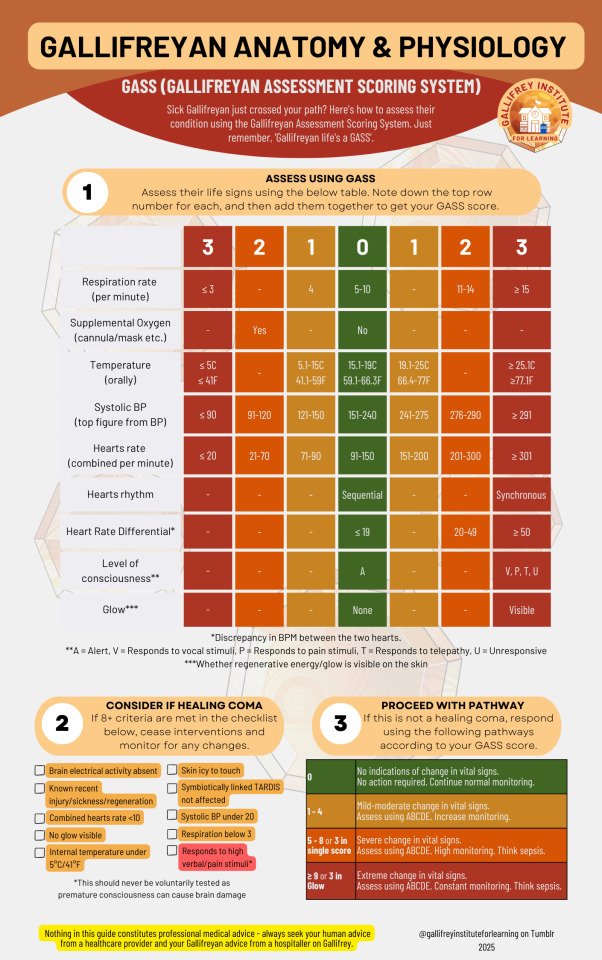
⚕️GASS (Gallifreyan Assessment Scoring System)
Sick Gallifreyan just crossed your path? Here's how to assess their condition using the Gallifreyan Assessment Scoring System. Just remember, 'Gallifreyan life's a GASS'.
BIGGER - Google Drive: PDF / Image JPG / Image PNG
This guide is for use on Gallifreyans and Time Lords only. Always seek your human advice from human health providers.
✨ What is GASS?
The Gallifreyan Assessment Scoring System (GASS) is a tool designed to rapidly evaluate a Gallifreyan's condition. By monitoring vital signs and unique Gallifreyan indicators, it prioritises emergency responses while accounting for their distinct physiology, such as dual hearts and regenerative abilities.
Just remember, Gallifreyan life's a GASS.
📈 What's New in GASS?
This updated version of GASS includes critical refinements for more precise assessments. New categories have been added, such as Heart Rate Differential (HRD) to flag discrepancies between the two hearts and T = Responds to Telepathy in the level of consciousness scale. Adjustments to thresholds for vital signs and regenerative glow visibility also improve detection of emergencies like fibrillation or post-regenerative trauma.
📝 How to Use GASS
1️⃣Initial Observations
Ensure the environment is safe (e.g., no stray Daleks).
Observe for immediate signs of distress: skin colour, breathing effort, or lack of responsiveness.
2️⃣Evaluate Vital Signs and Assign Scores
Refer to the GASS table to assess each category:
🌬️ Respiration Rate: Count breaths per minute. Adjust for respiratory bypass if present.
🫧 Supplemental Oxygen: Note if oxygen support is in use.
🌡️ Temperature: Measure orally.
💓 Systolic BP: Record using a normal sphygmomanometer.
💖 Hearts Rate (Combined): Count the total bpm across both hearts.
🔄 Hearts Rhythm: Sequential beats (thud-thud, thud-thud) are normal; synchronous beats (thud-thud together) indicate fibrillation.
⚖️ Heart Rate Differential (HRD): Calculate the bpm difference between hearts; large discrepancies suggest possible singular heart failure.
🧠 Level of Consciousness (AVPTU): A = Alert, V = Responds to verbal stimuli, P = Responds to pain, T = Responds to telepathy, U = Unresponsive
✨ Regenerative Glow: Check for visible energy on the skin.
3️⃣Check for Healing Coma
If 8+ healing coma criteria are met:
Cease active interventions.
Monitor closely for changes.
Avoid premature waking to prevent neurological damage.
4️⃣Calculate Total GASS Score
Add up the scores from all categories:
0: No concerning changes. Continue routine monitoring.
1–4: Mild to moderate changes. Perform an ABCDE assessment and increase monitoring.
5–8 or 3 in single score: Severe changes. Perform ABCDE, escalate care, and consider sepsis.
≥9 or Glow = 3: Extreme changes. Initiate emergency intervention, constant monitoring, and prepare for sepsis protocols.
5️⃣Reassess After Interventions
Following each intervention, reassess the GASS score to adapt care and ensure stability.
🚨 When to Escalate
Critical signs: Synchronous heartbeats, extreme HRD, or GASS score ≥9.
Sepsis or Specific Emergencies: Use respective protocols for management.
📌 Key Points to Remember
Combine GASS results with clinical judgement.
Healing comas are protective states—let them run their course.
Escalate care if in doubt.
Medical Guides
These are all practical guides to assessing and treating a Gallifreyan in an emergency.
⚕️💕Gallifreyan CPR
⚕️👽Gallifreyan Assessment Scoring System (GASS)
⚕️👽ABCDE Assessment
⚕️⚠️Sepsis Emergency Response (SER)
⚕️⚠️Severe Trauma Protocol
⚕️🌡️Gallifreyan Thermoregulation and Emergency Response
⚕️🔮Psionic Emergency Pathways
⚕️✨Post-Regeneration Management
⚕️💤Gallifreyan Healing Coma Management
⚕️🩸Interpreting Gallifreyan Bloodwork
⚕️👶Gallifreyan Paediatric Emergencies
⚕️🧠Managing Gallifreyan Neurological Trauma
Any orange text is educated guesswork or theoretical. More content ... →📫Got a question? | 📚Complete list of Q+A and factoids →📢Announcements |🩻Biology |🗨️Language |🕰️Throwbacks |🤓Facts → Features:⭐Guest Posts | 🍜Chomp Chomp with Myishu →🫀Gallifreyan Anatomy and Physiology Guide (pending) →⚕️Gallifreyan Emergency Medicine Guides →📝Source list (WIP) →📜Masterpost If you're finding your happy place in this part of the internet, feel free to buy a coffee to help keep our exhausted human conscious. She works full-time in medicine and is so very tired 😴
#doctor who#dr who#dw eu#gallifreyans#gallifrey institute for learning#Time Lord biology#GAP Quick Guides#whoniverse#GIL: Biology#gallifreyan biology#GIL: Species/Gallifreyans#GIL#GIL: Biology/Medical
68 notes
·
View notes
Text
Correlation of patient symptoms with SARS-CoV-2 Omicron variant viral loads in nasopharyngeal and saliva samples and their influence on the performance of rapid antigen testing - Published Oct 9, 2024
Study showing 1. The one-and-done method of rapid testing used by many is not good enough to prove covid negativity because rapid test were desined for serial testing 2. saliva swabs increase the accuracy of Rapid Antigen Tests.
ABSTRACT Evaluating SARS-CoV-2 viral loads in nasopharyngeal (NP) and saliva samples, factors affecting viral loads, and the performance of rapid antigen testing (RAT) have not been comprehensively conducted during SARS-CoV-2 Omicron epidemic. This prospective study included outpatients enrolled during Omicron variant period in Japan. Paired NP swab and saliva samples were collected to measure viral loads by reverse transcription-quantitative polymerase chain reaction (RT-qPCR). The correlation between viral loads and clinical symptoms was examined. The performance of an immunochromatography-based RAT kit was also assessed. A total of 153 patients tested within 3 days of symptom onset were included. The mean viral load was 5.60 log10 copies/test and 3.65 log10 copies/test in NP and saliva samples, respectively, resulting in a significant difference (P < 0.0001). Fever over 37°C (axillary temperature) and total number of symptoms other than fever were identified as independent factors positively correlated with the viral loads in both NP and saliva samples. RAT sensitivity using NP and saliva samples was 92% and 68%, respectively, using positive RT-qPCR results as the reference. The sensitivity of RAT using NP and saliva samples was significantly higher in patients with fever ≥37°C and/or at least one symptom than in those with fever <37°C and/or no symptoms (97% vs 83% in NP swabs; 80% vs 50% in saliva). Distinct symptoms, including fever ≥37°C, may reflect high Omicron variant viral loads. Rapid antigen testing, not only using nasopharyngeal swabs but also using saliva, would be useful for COVID-19 diagnosis as point-of-care testing, particularly for symptomatic patients.
IMPORTANCE We examined nasopharyngeal and salivary viral loads using samples collected from outpatients with SARS-CoV-2 infection during the Omicron epidemic in Japan and explored the outpatient factors correlated with viral loads. In addition, we evaluated the performance of an authorized rapid antigen testing (RAT) kit using nasopharyngeal and saliva samples with RT-PCR testing as the reference. Intriguingly, a correlation between fever and other symptoms and SARS-CoV-2 viral loads in nasopharyngeal and saliva samples was observed based on one COVID-19 outpatient visit. RAT sensitivity was influenced by viral loads. Nevertheless, nasopharyngeal RAT is considered useful for SARS-CoV-2 point-of-care diagnosis. In patients with distinct symptoms, including high-grade fever, salivary RAT could be a practical diagnostic tool because of the higher estimated viral loads. After the Omicron epidemic, outpatients with mild COVID-19 have become the main focus of diagnosis and treatment. Our study provides valuable information regarding the point-of-care diagnosis of these patients.
#mask up#covid#pandemic#public health#wear a mask#covid 19#wear a respirator#still coviding#coronavirus#sars cov 2#rapid antagen test#covid test#covid testing
68 notes
·
View notes
Note
Hi. May I ask you about something that is very common to a majority of people. I don't know if you have it but it is about MALADAPTIVE DAYDREAMING!!!
I spend the majority of time daily, and cannot be productive. Is it useful, is it a tool, a blessing but feels more like e curse which direct you way in massive self-deception and depression rather than directing you towards what you need to do, your goals ect.
I'd love to know your opinion about it.
💋
brain matters: maladaptive daydreaming
as previously mentioned, i was a forensic psych major before i was an english major and before graduating with my b.a. of literature. for 3 years i studied psychology. i do not have a psychology degree, so that does not make me qualified to diagnose anyone or anything... but i do know a bit about psychology and i continue to read research and articles regarding psychology.
so gladly i will give my opinion though i am not a professional.
what is maladaptive daydreaming?
maladaptive daydreaming is often found in those seeking an escape or who seek coping mechanism from trauma, abuse, anxiety, depression, adhd, etc. its a form of daydreaming that may involve long periods of structured fantasy that can interfere with work, school, and/or other life functions/tasks.
is it common?
it is not an officially recognized diagnosis but has comorbidity as i listed above. the few studies/articles i have read, state that it is not common in the general population - only about 2-6% of individuals experience it. depending on the scope of the study group it varies. out of the 7.9 billion individuals on earth only about 158 million experience maladaptive daydreaming. the study i found on pubmed (could only get the preview see below) states 2.2 million in america alone including those with a formal diagnosis that i listed above.
what are the symptoms?
highly vivid/immersive daydreams: these are abnormally long daydreams that are hard to escape / shake. making it hard for you to focus on any given task.
inability to complete daily tasks.
sleep disruption / insomnia: your mind is on but not at the same time throughout the day making it hard to maintain a healthy circadian rhythm.
being triggering into daydreams by external forces such as tv shows, movies, books, etc.
repetitive motion/activity while daydreaming
potential benefits
creativity and problem-solving skills: it can foster creativity, as it allows the mind to explore ideas and scenarios freely. writers, artists, and inventors use their imagination in this way to develop new concepts (but it is safe to say that not all creatives experience maladaptive daydreaming nor is it a requirement for all creatives / skilled problem solvers).
emotional regulation: provides a form of escapism, helping individuals cope with stress or emotional difficulties by temporarily shifting their focus away from real-life challenges.
goal visualization: a strong way to visualize their future or rehearse real-life scenarios, which can improve their ability to achieve goals or prepare for social interactions (lots of therapist teach clients with anxiety "visualization" as a coping mechanism so they can mentally prepare for what could be experienced; they generally guide the visualization to the best possible outcome).
drawbacks
time loss and disconnection from family/friends: the time spent lost in a fantasy often takes away from real-life activities, relationships, and responsibilities. which can lead to procrastination or missed opportunities.
emotional detachment: becominh emotionally invested in their fantasy worlds, making real-life experiences seem dull or less satisfying by comparison. this could cause worsen feelings of loneliness or depression.
interference with mental health: can exacerbate or mask underlying mental health issues like anxiety, depression, trauma, etc., as people use it as a form of avoidance rather than addressing their challenges head-on.
like what you read? leave a tip and state what post it is for! please use my “suggest a post topic” button if you want to see a specific post or mythical asteroid next!
click here for the masterlist
want a personal reading? click here to check out my reading options and prices!
© a-d-nox 2024 all rights reserved
41 notes
·
View notes
Text

Following publication of the final report there have been a number of questions and points for clarification about the findings and recommendations. We have collated those questions, along with our answers, on this page.
-
Did the Review set a higher bar for evidence than would normally be expected?
No, the approach to the assessment of study quality was the same as would be applied to other areas of clinical practice – the bar was not set higher for this Review.
Clarification:
The same level of rigour should be expected when looking at the best treatment approaches for this population as for any other population so as not to perpetuate the disadvantaged position this group have been placed in when looking for information on treatment options.
The systematic reviews undertaken by the University of York as part of the Review’s independent research programme are the largest and most comprehensive to date. They looked at 237 papers from 18 countries, providing information on a total of 113,269 children and adolescents.
All of the University of York’s systematic review research papers were subject to peer review, a cornerstone of academic rigour and integrity to ensure that the methods, findings, and interpretation of the findings met the highest standards of quality, validity and impartiality.
-
Did the Review reject studies that were not double blind randomised control trials in its systematic review of evidence for puberty blockers and masculinising / feminising hormones?
No. There were no randomised control studies identified in the systematic reviews, but other types of studies were included if they were well designed and conducted.
Clarification:
The Review commissioned the University of York to undertake an independent research programme to ensure the work of the Review and its recommendations were informed by the most robust existing evidence. This included a series of systematic reviews which brought together, analysed and evaluated existing evidence on a range of issues relating to the care of gender-questioning children and young people, including epidemiology, treatment approaches and international models of current practice.
Randomised control trials are considered the gold standard in relation to research, but there are many other study designs that can give valuable information. Explanatory Box 1 (pages 49-51 of the final report) discusses in more detail the different kinds of studies that can be used, and how to decide if a study is poorly designed or biased.
Blinding is a separate issue. It means that either the patient or the researcher does not know if the patient is getting an active treatment or a ‘control’ (which might be another treatment or a placebo). Patients cannot be blinded as to whether or not they are receiving puberty blockers or masculinising / feminising hormones, because the effects would rapidly become obvious. Good RCTs can be conducted without blinding.
The University of York’s systematic review search did not identify any RCTs, blinded or otherwise, but many other studies were included. Most of the studies included were called ‘cohort studies’. Well-designed and executed high quality cohort studies are used in other areas of medicine, and the bar was not set higher for this review; even so the quality of the studies was mostly only assessed as moderate.
-
Did the Review reject 98% of papers demonstrating the benefits of affirmative care?
No. Studies were identified for inclusion in the synthesis (conclusions) of the systematic reviews on puberty blockers and masculinising/feminising hormones on the basis of their quality. This was assessed using a standard quality assessment tool appropriate to the types of study identified. All high quality and moderate quality reviews were included in the synthesis of results. This totalled 58% of the 103 papers.
Clarification:
The Newcastle-Ottawa scale (a standard appraisal tool) was used to compare the studies. This scores items such as participant selection, comparability of groups (how alike they are), the outcomes of the studies and how these were assessed (data provided and whether it is representative of those studied). High quality studies (scoring >75%) would score well on most of these items; moderate quality studies (scoring >50% – 75%) would miss some elements (which could affect outcomes); and low-quality studies would score 50% or less on the items the scale looked at. A major weakness of the studies was that they did not have adequate follow-up – in many cases they did not follow young people for long enough for the long-term outcomes to be understood.
Because the ranking was based on how the studies were undertaken (their quality and execution), low quality research was removed before the results were analysed as the findings could not be completely trusted. Had an RCT been available it would also have been excluded from the systematic review if it was deemed to be of poor quality.
The puberty blocker systematic review included 50 studies. One was high quality, 25 were moderate quality and 24 were low quality. The systematic review of masculinising/feminising hormones included 53 studies. One was high quality, 33 were moderate quality and 19 were low quality.
All high quality and moderate quality reviews were included, however as only two of the studies across these two systematic reviews were identified as being of high quality, this has been misinterpreted by some to mean that only two studies were considered and the rest were discarded. In reality, conclusions were based on the high quality and moderate quality studies (i.e. 58% of the total studies based on the quality assessment). More information about this process in included in Box 2 (pages 54-56 of the final report)
-
Has the Review recommended that no one should transition before the age of 25 and that Gillick competence should be overturned.
No. The Review has not commented on the use of masculinising/feminising hormones on people over the age of 18. This is outside of the scope of the Review. The Review has not stated that Gillick competence should be overturned.
The Review has recommended that:
“NHS England should ensure that each Regional Centre has a follow through service for 17-25-year-olds; either by extending the range of the regional children and young people’s service or through linked services, to ensure continuity of care and support at a potentially vulnerable stage in their journey. This will also allow clinical, and research follow-up data to be collected.”
This recommendation only relates to people referred into the children and young people’s service before the age of 17 to enable their care to be continued within the follow-through service up to the age of 25.
Clarification:
Currently, young people are discharged from the young people’s service at the age of 17, often to an adult gender clinic. Some of these young people have been receiving direct care from the NHS gender service (GIDS as was) and others have not yet reached the top of the waiting list and have “aged out” of the young people’s service before being seen.
The Review understands that this is a particularly vulnerable time for young people. A follow-through service continuing up to age 25, would remove the need for transition (that is, transfer) to adult services and support continuity of care and continued access to a broader multi-disciplinary team. This would be consistent with other service areas supporting young people that are selectively moving to a ‘0-25 years’ service to improve continuity of care.
The follow-through service would also benefit those seeking support from adult gender services, as these young people would not be added to the waiting list for adult services and, in the longer-term, as more gender services are established, capacity of adult provision across the country would be increased.
People aged 18 and over, who had not been referred to the NHS children and young people’s gender service, would still be referred directly to adult clinics.
-
Is the Review recommending that puberty blockers should be banned?
No. Puberty blocker medications are used to address a number of different conditions. The Review has considered the evidence in relation to safety and efficacy (clinical benefit) of the medications for use in young people with gender incongruence/gender dysphoria.
The Review found that not enough is known about the longer-term impacts of puberty blockers for children and young people with gender incongruence to know whether they are safe or not, nor which children might benefit from their use.
Ahead of publication of the final report NHS England took the decision to stop the routine use of puberty blockers for gender incongruence / gender dysphoria in children. NHS England and National Institute for Health and Care Research (NIHR) are establishing a clinical trial to ensure the effects of puberty blockers can be safely monitored. Within this trial, puberty blockers will be available for children with gender incongruence/ dysphoria where there is clinical agreement that the individual may benefit from taking them.
Clarification:
Puberty blockers have been used to suppress puberty in children and young people who start puberty much too early (precocious puberty). They have undergone extensive testing for use in precocious puberty (a very different indication from use in gender dysphoria) and have met strict safety requirements to be approved for this condition. This is because the puberty blockers are suppressing hormone levels that are abnormally high for the age of the child.
This is different to stopping the normal surge of hormones that occur in puberty. Pubertal hormones are needed for psychological, psychosexual and brain development, and there is not yet enough information on the risks of stopping the influence of pubertal hormones at this critical life stage.
When deciding if certain treatments should be routinely available through the NHS it is not enough to demonstrate that a medication doesn’t cause harm, it needs to be demonstrated that it will deliver clinical benefit in a defined group of patients.
Over the past few years, the most common age that young people have been receiving puberty blockers in England has been 15 when most young people are already well advanced in their puberty. The new services will be looking at the best approaches to support young people through this period when they are still making decisions about longer-term options.
-
Has the Review recommended that social transition should only be undertaken under medical guidance?
The Review has advised that a more cautious approach around social transition needs to be taken for pre-pubertal children than for adolescents and has recommended that:
“When families/carers are making decisions about social transition of pre-pubertal children, services should ensure that they can be seen as early as possible by a clinical professional with relevant experience.”
Parents are encouraged to seek clinical help and advice in deciding how to support a child with gender incongruence and should be prioritised on the waiting list for early consultation on this issue. This should include discussion of the risks and benefits and the voice of the child should be heard. It will be important that flexibility is maintained, and options remain open.
Clarification:
Although the University of York’s systematic review found that there is no clear evidence that social transition in childhood has positive or negative mental health outcomes, there are studies demonstrating that for a majority of young children presenting with gender incongruence, this resolves through puberty. There is also evidence from studies of young people with differences of sex development (DSD) that sex of rearing seems to have some influence on eventual gender outcome, and it is possible that social transition in childhood may change the trajectory of gender identity development for children with early gender incongruence. Living in stealth from early childhood may also lead to stress, particularly as puberty approaches.
There is relatively weak evidence for any effect of social transition in adolescence. The Review recognises that for adolescents, exploration is a normal process, and rigid binary gender stereotypes can be unhelpful. Many adolescents will go through a period of gender non-conformity in terms of outward expressions (e.g. hairstyle, make-up, clothing and behaviours). They also have greater agency in how they present themselves and in their decision-making.
Young people and young adults have spoken positively about how social transition helped to reduce their gender dysphoria and feel more comfortable in themselves. They identified that space to talk about socially transitioning and how to handle conversations with parents/carers and others would be helpful. The Review has therefore advised that it is important to try and ensure that those already actively involved in the young person’s welfare provide support in decision making and that plans are in place to ensure that the young person is protected from bullying and has a trusted source of support.
Further detail can be found in Chapter 12 of the Final Report.
-
Did the Review speak to any gender-questioning and trans people when developing its recommendations?
Yes, the Review has been underpinned by an extensive programme of proactive engagement, which is described in Chapter 1 of the report. The Review has met with over 1000 individuals and organisations across the breadth of opinion on this subject but prioritised two categories of stakeholders:
People with relevant lived experience (direct or as a parent/carer) and organisations working with LGBTQ+ children and young people generally.
Clinicians and other relevant professionals with experience of and/ or responsibility for providing care and support to children and young people within specialist gender services and beyond.
A mixed-methods approach was taken, which included weekly listening sessions with people with lived experience, 6-weekly meetings with support and advocacy groups throughout the course of the Review, and focus groups with young people and young adults.
Reports from the focus groups with young people with lived experience are published on the Review’s website and the learning from these sessions and the listening sessions are represented in the final report.
The Review also commissioned qualitative research from the University of York, who conducted interviews with young people, young adults, parents and clinicians. A summary of the findings from this research is included as appendix 3 of the final report.
-
What is the Review’s position on conversion therapy?
Whilst the Review’s terms of reference do not include consideration of the proposed legislation to ban conversion practices, it believes that no LGBTQ+ group should be subjected to conversion practice. It also maintains the position that children and young people with gender dysphoria may have a range of complex psychosocial challenges and/or mental health problems impacting on their gender-related distress. Exploration of these issues is essential to provide diagnosis, clinical support and appropriate intervention.
The intent of psychological intervention is not to change the person’s perception of who they are but to work with them to explore their concerns and experiences and help alleviate their distress, regardless of whether they pursue a medical pathway or not. It is harmful to equate this approach to conversion therapy as it may prevent young people from getting the emotional support they deserve and make clinicians fearful of providing this group of children and young people the same care as is afforded to other children and young people.
No formal science-based training in psychotherapy, psychology or psychiatry teaches or advocates conversion therapy. If an individual were to carry out such practices they would be acting outside of professional guidance, and this would be a matter for the relevant regulator.
==
Like any religious fanatics, pathological liars like "Erin" Reed and "Alejandra" Carballo still won't stop lying, since it's all they have. But their disciples should really be noticing how they've been directly refuted.
#Cass review#Cass report#Hilary Cass#Dr. Hilary Cass#disinformation#misinformation#pathological liars#Erin Reed#Alejandra Carabello#Michael Hobbes#medical scandal#medical corruption#medical malpractice#gender affirming care#gender affirming healthcare#gender affirmation#compulsive liars#gender fanatics#gender cult#gender ideology#gender identity ideology#queer theory#intersectional feminism#puberty blockers#cross sex hormones#wrong sex hormones#religion is a mental illness
58 notes
·
View notes
Text
Survey recruitment; I gave feedback as a later consultant & Tuttle is another Autistic AAC user who was involved in the project from the start. Shares are Definitely Helpful :)
Are you an autistic adult who uses speech and other tools (such as augmentative and alternative communication [AAC]) to communicate?
If you answered yes, please consider participating in this survey at this link:
We are interested in learning about the speech, AAC, and assessment experiences of autistic people who use speech and AAC. We are curious if a modified version of the Communicative Participation Item Bank (CPIB) can be a reliable tool for clinicians to utilize in measuring the internal experiences of speaking autistic people. Regarding assessment, we are interested in understanding how their speech efficacy, or the extent to which one can use speech to completely communicate their intended meaning, was measured and considered in the evaluation process and if the evaluation resulted in a recommendation of an AAC tool.
The survey includes a mix of multiple choice, slider, and written response questions and is estimated to take between 10-20 minutes.
No identifying information will be collected in this survey.
Please reach out with any questions or concerns via email.
We thank you in advance for contributing your insight on this important topic!
Karina Rayl, B.S. (Lead Investigator)
Graduate Student
Speech and Hearing Sciences
Portland State University
Email: [email protected]
Pang Lee Herr, B.S. (Lead Investigator)
Graduate Student
Speech and Hearing Sciences
Portland State University
Email: [email protected]
Brandon Eddy, M.A., CCC-SLP (Co-investigator and Faculty Advisor)
Associate Clinical Professor
Speech and Hearing Sciences
Email: [email protected]
Amy Donaldson, Ph.D. CCC-SLP (Co-investigator and Faculty Advisor)
Associate Professor
Speech and Hearing Sciences
Email: [email protected]
Tuttle (External Collaborator)
Email: [email protected]
Alyssa Zisk, Ph.D. (External Collaborator)
Email: [email protected]
#aac#actuallyautistic#disabilty#autism#aac user#actuallydisabled#disabled researchers#autistic researchers#yes it's a research post and yes the two 'external collaborators' are both autistic aac users#please only use our emails for things related to the research but that is what they're for
54 notes
·
View notes
Text
Six Cycles Later -- Part VII
Summary: The other side of the conversation in Part VI. Channel's dealing with her own horrible revelations half a planet away.
Word Count: 3759
Trigger warning: robogore, PTSD
Prior chapter can be found here, start can be found here. Next chapter can be found here.
Fic under cut!
The rain had already begun to pour by the time she laid the tiny Autobot on her work slab. Just moments ago, when he'd crashed outside and staggered to her door, it had been a drizzle at most, a quiet, tapping suggestion of presence. Now it was a downpour. Her optics automatically adjusted when the natural light from the windows darkened.
He wasn’t even able to properly speak. The damage to his helm was so severe she thought he must have stuck it in a press. Usually Channel would have degraded him for being so stupid; she'd quickly realized there was no time for a scolding when he'd collapsed at the door.
Her patient was tiny, less than half her size. She focused on supporting his head, energon pouring over her servos as she carried him across the clinic. It really wasn't much of one: the structure she called an abode was a glorified garage with two rooms attached to it. The "entrance" was a shabby, nondescript door which opened straight into her storage closet, which was so cluttered that only the suggestion of a floor could be garnered from a glance.
Despite the obstacles she'd been cautious to avoid jarring her patient (or exposing him to the chittering cage of sparklets) as she'd brought him into the garage area—her "operating room". It was a wide open space with an operating slab, a single surgical aid machine, and assembly tables scattered about, all covered in tools.Energon stains dotted the bare stone floor like stars in the sky, mixing into fat blobs around the slab as she laid him down.
His optics were darting around the room constantly, trying to evaluate where he was, how to escape, if he was safe or not. Poor thing. The scared animal look never quite left the eyes of the dying, even after they recovered. Brushing against the beast that was mortality left every victim traumatized, and the one on her slab was no exception. But just what had happened to bring him there?
She didn't linger on it and sedated him with a quick injection of spiked energon. The moment his optics quit fluttering about, she picked away what pieces were left of his helm and pressed the modified pads of her fingers to his paneling. A few communications from her own systems to his granted her immediate access into him, permitting her to order a temporary offline. Before leaving, she collected a few memory files, then snapped back into her own body. blinking as she onlined again.
From there she went to work. His helm was almost completely crushed, though his brain was intact. Repairs wouldn't be as simple as hammering out a few dents; he would need an entirely new helm and faceplate. It was a job for someone with parts at their disposal, not her tiny "clinic" in the middle of the Pacific Ocean. Idly, she wondered if this was a job she could even handle with her current tools.
The gray light pouring in suddenly lighting up with a flash. She winced at the sudden boom that followed, her servos clenching instinctively at the sound. The war was over, there was no reason to panic. Earth's weather just did that every now and then.
Even so, a dozen notifications opened in her HUD, warning her to take cover and scan for survivors. She closed them all.
There was no choice. She’d have to repair him as best she could with what she had here, then wipe his memory. If she failed with either, she risked his life and her safety.
First, she checked his sparkbeat--stable--and cleaned his wounds.
I ain’t a doctor. I didn't learn in no system. I didn't attend no classes or read no datapads.
Then, she worked on the warping in his plating.
I got all my experience fixin' everyone I found in the field. We ain't had time for studyin' an' readin' an' practicin'.
After that, she welded what breaks she could and carefully molded his head back together. His visor was a lost cause.
Everythin’ was hands on, in the moment, right there, an' either you got it right, or they died beneath you.
Only once she was sure she'd properly fixed all of his helm did she check his Energon levels, finding them to be lower, but still at a safe level. Her medical Energon stores were shoved right against the always closed garage door, in case she needed to quickly dispose of them. Retrieving a cube from the small pile, she brought it to his dermas and, with only a bit of effort, convinced his unconscious form to drink.
When the cube depleted she placed its empty shell next to the others and returned to online him. It was a careful process to open his helm again and connect. As she turned his head she took in the full sight of his faceplate, with all its mended seams.
The bleeding corpse still looked up at her, his face contorted in agony.
Her fans clicked on instinctively to cool her down. Her hands shook as notifications began to crop up in her HUD again. She disabled them both and pulled her hands away, choosing to let him sleep for a bit longer. No use trying to wake him up if she wasn't fit for it.
Outside the storm raged. She hadn't seen such strong weather in a while--not for at least two earth months. It was lucky the little Autobot had found her before the winds had turned. There was no way in The Pit that he would have been able to fly in such conditions.
Then again, with the damage to his helm, there was no way he should have been able to transform safely either. Luck seemed to be on the little one’s side.
How cruel that the fickle creature decided only now to make its presence known amongst the Autobots.
Crossing the garage, she leaned against one of the window frames and watched the rain fall. It was the perfect distraction for letting her mind wander: the files she'd retrieved would need to be reviewed so she could learn about her patient. That would determine whether she'd contact someone to pick him up for travel to a proper medic, or if she'd give him a knock on the helm and tell him to fly there himself. Opening the files in her HUD, she let the white noise of rainfall train her focus into her own processor.
Starburst was his name. He turned into a rocket—made sense. Speedster build, forged during the war. Had pride issues, liked to flirt. Good thing his vox box was probably broken, then. Visiting Earth to catch up with the Aerialbots; it seemed competitiveness ran in his wires. Before he'd been injured, he'd been responding to...
A distress call. She raised an optical ridge at that. A distress call from humans. On the island of Bali, there had been a call claiming a winged robot had walked out of the sea and crushed several buildings on a tourist beach. Supposedly it had then made for the Demon Swamp. Eager to prove himself, Starburst had rocketed off first, leaving the Aerialbots he'd been intending to challenge behind.
Once at the swamp, he'd found--
Two of them. One enormous, one average. A common build, that of a Seeker, and a custom, hulking monster. The Seeker was lime green--a familiar lime green. Flaking pink paint covered her chassis and ran up her wings, but the rest of her was eye-bleeding green. The larger one was almost entirely black, accented with gold and yellow. Her armor was spiked and segmented, resembling an earth organism in its make-up. Hiding her face was a steely mask and a red visor, over which a helm resembling an insect's head almost seemed to bite down, like it was never meant to be there in the first place.
An Insecticon and a Seeker. Though the memories playing before her vision barely noticed the purple sigils on their wings and chasses, her own systems blared with panic at the sight.
There were no cons left on Earth. They'd abandoned the planet after Megatron had died during the assault on Autobot City. Following the Unicron incident the remaining forces had retreated somewhere unknown in the galaxy. A search over the entire planet Earth had concluded there were no cons left. The planet had been declared a safe haven, with the official announcement that the war, at least here, was over.
And playing right before her vision was proof it was not.
She opened her comms immediately, closing the memory files she'd been viewing. Before she could even open his channel, however, Uptick was pinging her. How convenient. Accepting his request, their communications line opened.
"Ticker's, I got news for y--"
"I need you to hijack a signal for me. There's a sparkeater in Autobot City and it's captured Luster. I need you to find him."
She paused for just a moment, surprised at his interruption before it truly hit her.
'Well, I'll be. Sparkeater's a bit worse 'an this I s'ppose. Aight, gimme the signal."
She followed along with his requests, channeling into his mind through their connection, then into the city’s own signal. It was intimidating, connecting to a Titan–she was no Cityspeaker, and passing through a Titan’s personal frequency made her feel like a bug beneath the eye of Primus.
Metroplex, luckily, did not crush her. Or perhaps it was not luck, for Autobots were notoriously unlucky. Rather, he chose to pay her little mind to avoid overwhelming her, watching her right back, waiting to see what she would do.
Using the radio waves from his own satellite, she mapped his entire body, searching for a specific life signal. He gave her a small boost, aiding her in filtering through the thousands currently populating him. In milliseconds she was zipping through his corridors and over his streets, honing in on the Autobot Metroplex had dubbed “the waning one”.
Uptick could feel most of the information she sent to him, but not that of her momentary connection with Metroplex. It spared him from the sudden pain she felt when the signals were located and one winked out. It spared him from the sudden desire forced into her mind:
Save them.
"Found your kid,” she announced, and pulled out, breaking from Metroplex’s signal to retreat back into Uptick’s.
Environmentally speaking it was like night and day: one was comfortable, familiar, and enclosed. It had been damaged and the cracks showed, but it held together despite them. The other was vast, open, and unknowable. Metroplex’s feelings were wild and enormous, each one a punch to her helm. She could not understand his words or thoughts, only the immensity of his feelings.
If she was in her frame she would have purged. But as a signal in Uptick’s helm, she had no ability to do so. Orienting herself, she promptly sent him the information and retreated back to her own form, crossing thousands of miles instantly.
It took only milliseconds in a literal sense, but to her, it felt like hours. By the time she was back in her own frame her systems were indicating immense stress. Two transfers over such a long distance in so short a time was threatening to overload her.
"Thanks Channel. I'll update you when I've found him."
His tone reminded her of their war days. She couldn’t see him, but the intensity of his voice put the image of that day back in her helm like it had just passed:
He stands over the bleeding corpse, both blasters raised, missile launchers hissing despite their depleted barrels. The fuel boom extended from his side, bleeding out brilliant pink against his black war paint. As another laser bolt blasts into his wing, the corpse lurches, life giving Energon splattering from his mouth as he coughs.
There was no darker day than that. The danger in his tone was equal to himself.
"Right, Tickers, but you should--" She began, and their connection severed. He was off to hunt a sparkeater, and she was not invited.
She blinked, then huffed. Of course she wasn’t invited. Of course he had to do everything himself. Of course he was hellbent on sacrificing his safety and well-being in the name of protecting someone else. The memory was fresh in her mind, and though so much of it had been pulled from his, its pain was still undoubtedly fresh.
She’d have to contact this Redactor fellow when it was all said and done, probably when he was back on Cybertron. Another round of mnemosurgery might be necessary for keeping Uptick safe from himself. But in the meantime…
She took to cleaning her tools and workspace, gathering up the trash and raising the garage door to toss it outside.
A sparkeater. A sparkeater in Autobot City. How was that even possible? Sparkeaters were rumors at best. There didn’t even exist any real photos of them, only artistic depictions. She’d long theorized that they were made up to scare sparklings into behaving, and when the war had started, soldiers into keeping their ranks.
Of course there had been talk that Shockwave was working on creating real ones, but no one really believed him capable of it. Whatever strange spark experiments he’d been performing, if any at all, they’d died with him when Cybertron had been attacked. She’d listened in on what they’d found in his lab. It was gruesome, but nothing as extreme as a real sparkeater.
Still…the Decepticons rearing their ugly heads in Bali and a sparkeater's arrival in Autobot City.
Could the two be connected?
She closed the garage door and headed for her quarters. The door to them was at the very back, and unlike the rest of her poorly constructed, cinderblock clinic, actually mechanical. She tapped a code into her keypad and the metallic door slid open.
Her quarters were small and extremely cramped. Technology was crammed into every square inch of the place. Her computers and signal jackers covered the walls, their wires engaging in a delicate dance for dominance as they crept downwards towards a generator. The energon powered human tech kept the entire place functional, even if it constantly belched fumes and threatened to explode.
Today was not a day where its threats were felt. She climbed over a gathering of human radios, all tuned into different frequencies, and seated herself on said generator, reaching out to tap one of her many touchscreens. It activated, and she pulled up a map of Earth, zooming in on Bali, then Autobot City.
They’d said Shockwave had failed to create a sparkeater, but what if he’d kept something underground? No body had ever been found, and he was currently listed as MIA. She wouldn’t put it past him to create some kind of atrocity in secret.
A real sparkeater, though? It seemed a stretch. And Bali was far from Autobot City. A dual attack on both places at once was idiocy.
Zooming in on the Demon Swamp, she pulled up her informatics on the place and read it over. The Demon Swamp was the home of the Insecticons. Earth-adapted and skilled at hiding themselves, the Insecticons were notorious for their ability to produce clones. Not even one could be spared, otherwise they’d come back with an army.
During the attack on Autobot City, they’d seen many, many Insecticon clones bite the dust. And more than a few had bit the dust. She furrowed her optical ridges, pulling up an image of Shrapnel.
If the cons wanted to start invading Earth again, it would make sense to start with the Insecticons. They could silently create an army from their home location, using the massive distraction of a sparkeater (real or not) to keep eyes off their efforts. And once enough had been reformed, they’d launch a full scale invasion.
She knew for a fact there were still Decepticon bases under the oceans. They were, supposedly, abandoned. But with how lax Earth’s security was, how easily could a Decepticon sneak in and reactivate one, utilizing its cloaking to transport soldiers with an onboard space bridge?
But why a Seeker? A Seeker coming out of the ocean no less. That was about as expected as a tank falling out of the sky.
Replaying Starburst's memory, she tried to check if she could recognize either of the cons in it. Seekers were a dime a dozen, but she swore that the one she witnessed, blurry as it was, resembled Acid Storm. The Insecticon...she drew a blank.
Acid Storm. As far as Seekers went he was one of the more notorious; as a Rainmaker, she’d seen him melt more than a few dozen of her allies. If he was on Earth, it was awful news. Seekers always moved in trines, they were forged for it. Two at the sides, one at the lead. It was how they fought, how they flew. Knowing their movements made them predictable but no less deadly.
“There’ll be three, one behind, two at the sides. You’ll need’a fly low. They’ll outmaneuver ya no matter what height, but if ya stay low, the environment becomes yer friend. They’re delicate. You’ ain’t.”
He looks at her with determined optics and nods.
“All you hafta do is get us close to camp. Aerial support takes it from there.”
She supports his head on her knee, elevating him so the energon stops leaking from his intake.
“We’ll be wit’ ya the whole way. Hey, when we make it outta this, we’ll have a wicked story ta tell, right?”
There were three Rainmakers. Together they could level entire cities. If they had been present at the attack on Autobot City it wouldn’t have been declared a victory.
She tapped her servos together, considering her information. A Rainmaker, an Insecticon, and a sparkeater. None of it felt right. She couldn’t confidently say what the cons were up to, but she could say it needed to be reported. Glancing out at Starburst’s inert form, she grimaced.
She wanted to alert Ultra Magnus to all she'd learned, there was just one issue:
everything she'd just done was illegal.
Not only was she not supposed to be practicing, she hadn't been approved for the 'clinic' she'd built, hadn't received informed consent to probe Starburst's mind, and certainly hadn't acquired the comms of anyone she'd be contacting legally. In theory she could contact Ultra Magnus or Rodimus Prime at any given time. In theory, she could pretend that it was an incorrectly made call.
But considering how much they knew about her now, she highly doubted that anyone would believe anything from her to be accidental. Whatever information she learned, she kept, especially the pieces she wasn't supposed to have.
How much she would love to contact the Ark or the officials in Autobot City—and how much she would love to lose all her freedom because she'd broken their contract the moment she’d stepped foot on Earth. No, there was really only one 'bot she could entrust this information to, and it certainly wasn't Starburst.
She groaned, already dreading the helmache she was sure to develop after pinging Uptick. This would have to be quick, otherwise she risked temporary offlining at best.
He picked up on the first ring. When he spoke his voice almost sounded distant, like he was yelling into the wind. She recognized why immediately: it was the way he sounded when transformed.
"Channel, I need a favor."
Three in one day. He was getting bold. She cocked an optical ridge and frowned.
"Now's a bad time for it, 'Tickers. There’s–”
"It can't wait. I'm sorry. I'm heading to you now."
"Wait, wh'?” She furrowed her optical ridges. “'Tickers, I'm callin' you because I needa’ tell ya somethin'!
"It can wait."
"It really can’t--"
"It has to wait. This isn't negotiable.”
"No, it ain't!" She snapped, slamming a fist down on a radio. It shrieked static, igniting her rage. "'Tickers, I done you two favors today, you're gonna sit your aft down and listen t’ me! A sparkeater's bad, but it ain't alone! The cons are back!"
Silence.
“Ain’t you heard me?! The ‘Cons are–”
“Where are they?” The dangerous calm in his voice went over her head.
“Where? The Demon Swamp! You needa contact Mags--"
"No."
Of all responses he could've given, she never thought he would have said that. It shocked her so much she sputtered.
"Y-you what?!"
"How many of them are back?"
"You--what!? WHAT?!"
"How many?"
Her dermas curled down angrily. "Listen here, you, don't you think for a moment that--"
“How. Many.”
It was her turn to be quiet for a moment, the shrieking of the radio joining with the white noise of the rain outside. She almost wanted to join them, her spark threatening to burn through its chamber walls.
“Two,” she finally said, so much venom dripping from the word that it could melt plating.
"Perfect. Don't tell anyone. I'll deal with them."
There it was. His stupid, self-sacrificing tendencies, rearing their ugly head. If someone didn’t set him straight he’d bleed himself dry trying to fill a broken cup.
And she was the only voice of reason he’d listen to.
"'What the hell are you on about!” She bellowed. “I've a right mind to knock you over the helm!"
He vented. "I know, Channel. I'm...you're going to call me an idiot. And a glitchhead. And a complete and utter fool."
"I can think'a way worse than that, Tickers.” Her helmache was growing, and now the buzzing was starting. She pinched her enstril and vented sharply. “The hell're you up to?"
"It's...bad. It's really bad. But you can fix almost anything, right? You even fixed him, and they said he was a lost cause."
A bolt of pain shot through her processor as her voice dropped dangerously low. "Don't you go bringin' him up. That ain't no way to get on my good side."
“Sorry. But the bot I'm bringing to you is also a bit of a lost cause. The entire city wants him dead at this point. He's got nowhere to go, and I--"
"Tell me you aren't doin' what I think you're doin', 'Tickers. Tell me he ain't..."
She didn't need to say it. There was silence between them for too long. The rain beat heavily, as if howling its disapproval.
"It's Luster," Uptick said at last, voice hesitant. "He's the sparkeater."
#six cycles later#tf ocs#my writing#my ocs#maccadam#oc: uptick#oc: luster#OH BOY WE'RE REALLY STARTING TO GET TO IT NOW#ITS ALL COMING TOGETHER#YEET
6 notes
·
View notes
Link
#Ego#embracingthespiritualtransformationprocess#enneagram#enneagrampersonality#EnneagramPersonalityProfile#enneagrampersonalitytransformation#enneagrampersonalitytransformationjourney#enneagramself-discoveryprocess#enneagramworkshopsforself-discovery#instinct#originsoftheenneagram#personality#processoftheenneagram#self-discoveryprocess#spiritualtransformation#spiritualtransformationprocess#transformationprocessoftheenneagram#typesofpsychometrictools
2 notes
·
View notes
Text
How to Spot the Signs and Symptoms of Breast Cancer
Table of Contents
Introduction
Why Early Detection Matters
Common Signs and Symptoms of Breast Cancer
Less Obvious Symptoms to Watch For
How to Perform a Breast Self-Exam
When to See a Doctor
Diagnostic Tools and What to Expect
Reducing Your Risk
Conclusion
1. Introduction
Breast cancer is the most commonly diagnosed cancer in women worldwide. While advances in medicine have significantly improved outcomes, early detection remains the most powerful tool in fighting breast cancer. Understanding the signs and symptoms can lead to earlier diagnoses, better treatment options, and higher survival rates.
2. Why Early Detection Matters
Catching breast cancer in its early stages:
Improves treatment success rates
Reduces the need for aggressive treatments
Increases the chance of full recovery
Saves lives
That’s why it's vital for individuals—especially women—to stay informed and proactive about breast health.
3. Common Signs and Symptoms of Breast Cancer
The most recognizable signs of breast cancer include:
A new lump in the breast or underarm: Not all lumps are cancerous, but any new or changing lump should be checked.
Swelling or thickening in part of the breast
Dimpling or puckering of the skin on the breast
Change in breast size or shape
Pain in the breast or nipple that doesn’t go away
Nipple discharge (especially if bloody or occurring without squeezing)
Nipple turning inward (inversion)
Redness, flakiness, or irritation of the breast skin or nipple
4. Less Obvious Symptoms to Watch For
Breast cancer symptoms are not always obvious. Some may experience:
Itching or warmth in the breast
Changes in texture, such as the skin appearing like an orange peel (peau d’orange)
Enlarged lymph nodes near the collarbone or underarm
Unexplained weight loss or fatigue, especially in advanced cases
5. How to Perform a Breast Self-Exam
A monthly self-exam helps you become familiar with how your breasts normally look and feel, so you can detect changes early.
Steps for Self-Exam:
Look in the mirror: With shoulders straight and arms on your hips, check for changes in size, shape, or color.
Raise your arms: Look again for any changes.
Check for discharge: Gently squeeze each nipple.
Feel your breasts while lying down: Use your right hand for your left breast and vice versa, using a circular motion.
Repeat standing up: Many women find this easiest in the shower.
6. When to See a Doctor
Make an appointment immediately if you notice:
A new lump or thickening
Persistent pain or irritation
Any nipple changes or discharge
Skin dimpling or unusual redness
Even if you’re unsure, it’s better to have a professional evaluation. Most breast changes are not cancerous, but only a medical assessment can confirm that.
7. Diagnostic Tools and What to Expect
If symptoms are present, your doctor may recommend:
Clinical breast exam
Mammogram
Breast ultrasound
MRI scan
Biopsy (removing tissue for testing)
These tools help identify whether changes are benign or cancerous.
8. Reducing Your Risk
While some risk factors (like age and genetics) can’t be changed, you can reduce your risk by:
Maintaining a healthy weight
Limiting alcohol intake
Exercising regularly
Avoiding tobacco
Breastfeeding, if possible
Attending regular screenings and mammograms
9. Conclusion
Knowing the signs and symptoms of breast cancer can be lifesaving. Regular self-checks, awareness of your body, and routine screenings are key in catching cancer early—when it’s most treatable. If something feels off, trust your instincts and speak to your healthcare provider.
Remember: Awareness is the first step toward protection and prevention.
#breast cancer
2 notes
·
View notes
Text
Best Cardiologist in KPHB
Introduction :
When it comes to trusted and advanced cardiac care, Prathima Hospitals in KPHB is undeniably among the best. Renowned as a premier cardiology hospital in Hyderabad, it has earned national recognition for its world-class infrastructure, patient-centric care, and the presence of internationally trained cardiologists with over 20 years of experience. The Cardiac Sciences department at Prathima Hospitals is committed to offering evidence-based, research-driven care tailored to every patient. Their blend of compassion, technology, and medical excellence makes them the top destination for cardiac treatments in Telangana and India.
Whether it's early detection of heart disease, managing chronic cardiac conditions, or handling emergencies like heart attacks, the hospital is equipped with state-of-the-art technology and a multidisciplinary team. With its track record of successful interventions and a holistic approach to cardiovascular health, Prathima Hospitals continues to stand out as the Best Cardiology Hospital in KPHB, Hyderabad.
An Experienced Team Dedicated to Cardiac Wellness : At the core of Prathima Hospitals’ success in cardiology is its exceptional team of doctors, nurses, technicians, and paramedical staff. The team consists of some of the best cardiologists in KPHB, who are recognized for their clinical acumen, ethical practice, and dedication to patient education. With experience in handling high-risk and complex cardiac conditions, these experts follow international protocols and constantly upgrade their knowledge through global collaborations and research.
In addition to top-tier treatments, the hospital emphasizes the importance of preventive cardiology, conducting awareness programs and routine screenings to identify risks early. The staff is committed to guiding patients and their families through every step — from diagnosis to rehabilitation. Whether you're facing a serious heart problem or just need a consultation, you’ll receive undivided attention and advanced care from the region’s finest cardiac specialists.
Advanced Facilities & Comprehensive Cardiology Services : The Department of Cardiology at Prathima Hospitals KPHB includes a dedicated coronary care unit (CCU), step-down ICU, diagnostic cardiology services, and a fully functional cath lab. The facilities are designed for seamless care and continuous monitoring, especially for patients undergoing cardiac procedures. The team is trained to manage both emergency and elective cardiac interventions, ensuring 24x7 availability for urgent heart care.
Services provided include:
Coronary angiography and angioplasty
Device implantations (pacemaker, ICD)
Electrophysiology studies and ablation procedures
Non-invasive diagnostics like ECG, 2D Echo, TMT, and Holter monitoring
Cardiac rehab and lifestyle counseling
Patients with suspected heart disease, as well as those with diagnosed conditions, receive prompt and thorough evaluation. From admission to discharge, the care process is streamlined, transparent, and centered on restoring optimal heart function.
Specialized Care for Complex Heart Conditions : Prathima Hospitals is well-equipped to manage a wide range of cardiac diseases, including rare and life-threatening conditions. One of the key areas of expertise is the treatment of heart arrhythmias — disorders where the heart beats too fast, too slow, or irregularly. These conditions stem from disruptions in the heart’s electrical signals and are particularly common in older adults, though they can affect younger individuals as well.
Some commonly treated arrhythmias at the hospital include:
Atrial Fibrillation (AFib)
Ventricular Tachycardia
Bradycardia
Symptoms like chest pain, palpitations, dizziness, and breathlessness are carefully assessed using diagnostic tools. Depending on the severity, treatment options range from lifestyle modifications and medications to implantation of pacemakers or defibrillators. The goal is not just to treat the condition, but also to improve the patient’s quality of life.
Why Prathima Hospitals is the Top Choice for Heart Care in KPHB : The excellence of Prathima Hospitals KPHB lies in its consistency, credibility, and commitment to ethical medical care. With a legacy of successful cardiac treatments and thousands of happy patients, it is no surprise that Prathima is recognized as the best cardiology hospital in Hyderabad. The round-the-clock availability of expert cardiologists, quick emergency response, and a full-fledged infrastructure position the hospital as the best choice for heart care in both Telangana and across India.
Whether you're dealing with heart failure, coronary artery disease, hypertension, arrhythmias, or require preventive advice, Prathima Hospitals ensures that you receive nothing short of world-class care. The combination of clinical excellence, compassionate treatment, and technological superiority makes it the ideal destination for anyone seeking the best cardiologist in KPHB.
Read more
2 notes
·
View notes
Text
⚕️ Gallifreyan Paediatric Emergencies
Little Gallifreyans are a bit different from their adult counterparts. Here's how to assess them in an emergency using G-PEAS, if you please.

BIGGER - Google Drive: PDF / Image JPG / Image PNG
This guide is for use on Gallifreyans only. Always seek your human advice from human health providers.
📖 Introduction: Why G-PEAS?
Gallifreyan children differ significantly from adults in metabolism, cardiac function, telepathic control, and physical resilience. Their bodies are still developing key biological functions, making standard emergency assessment tools unsuitable. G-PEAS (Gallifreyan Paediatric Emergency Assessment System) provides a structured approach to identifying life-threatening conditions in paediatric Gallifreyans (ages 0-100).
Unlike adults, young Gallifreyans:
✔️ May only have one heart (Oldbloods develop their second heart upon first regeneration).
✔️ Have higher metabolic activity, resulting in higher normal body temperatures.
✔️ Exhibit psionic instability, leading to false positives in standard consciousness tests.
G-PEAS allows quick identification of critical conditions without the need for secondary tests like artron or Z-cell counts.
📊 How to Perform a G-PEAS Assessment
A Gallifreyan paediatric emergency is scored across five categories, each rated from 0-3, with higher scores indicating increased severity. The total score determines clinical urgency and escalation requirements.
1️⃣ Airway & Breathing (RR & Effort)
Assess the child's respiratory status without assuming respiratory bypass ability (which only develops in adulthood).
Normal respiratory rates: 0-16 years: 14-40 breaths per minute 17-100 years: 12-30 breaths per minute
Signs of respiratory distress: Nasal flaring, retractions, abnormal breath sounds, cyanosis.
Key concern: Young Gallifreyans cannot voluntarily regulate oxygen usage—watch for signs of impending failure.
2️⃣ Circulation (HR & BP)
Determine if the child has one or two hearts and evaluate heart rate accordingly.
Normal heart rates & BP: 0-16 years: HR 50-150 bpm, BP 80/40 – 110/60 mmHg 17-100 years: HR 40-120 bpm, BP 90/50 – 120/80 mmHg
Signs of circulatory failure: Cold extremities, weak or absent pulses, severe tachycardia (>200 bpm), hypotension.
Key concern: Children with one heart are naturally tachycardic compared to dual-hearted children.
3️⃣ Temperature & Metabolism
Metabolic instability is a common paediatric emergency due to higher energy demands.
Normal temperatures: 0-16 years: 16.5-20.5°C 17-100 years: 15.8-20.0°C
Signs of distress: Hypothermia <15.5°C or hyperthermia >21.0°C.
Key concern: Hypothermia in Gallifreyan children impairs psionic and neurological function faster than in adults.
4️⃣ Level of Consciousness (AVPTU & Psionics)
Assess using physical response first—psionic misinterpretation is common in young Gallifreyans.
Signs of concern: Psionic leakage, uncontrolled emotional outbursts, delayed response to verbal or pain stimuli.
Key concern: Unresponsive children may be suffering from telepathic overload rather than neurological failure.
5️⃣ Visual & Physical Examination
Look for signs of injury, vascular instability, or metabolic distress.
Signs of concern: Bruising, petechiae, cyanosis, poor muscle tone.
Key concern: Skin integrity is higher in younger Gallifreyans—visible injury suggests significant trauma.
🔢 G-PEAS Scoring & Interpretation
0-4 (🟢 Stable): Monitor, reassess every 30 minutes. No immediate intervention needed. 5-8 (🟠 Concern): Increased monitoring and assessments, prepare for escalation. Consider sepsis. 9+ (🔴 Critical): Immediate intervention required, activate emergency protocols.
🚨 When to Escalate
HR >150 bpm (0-16 years) or >120 bpm (17-100 years)
Temperature <15.5°C or >21.0°C
Severe hypotension (BP <70/30 mmHg)
Unresponsiveness despite physical stimuli
Psionic seizures or uncontrolled telepathic feedback
📌 Key Points to Remember
✔️ G-PEAS is an adapted assessment system for Gallifreyan children.
✔️ Do NOT assume respiratory bypass is present—children lack the control needed.
✔️ One vs. Two Hearts Matters—heart rate and BP should be assessed accordingly.
✔️ Young Gallifreyans have higher metabolic activity—their normal temperature is higher than adults.
✔️ Psionic responses can be unreliable—false positives may occur in younger children.
Medical Guides
These are all practical guides to assessing and treating a Gallifreyan in an emergency.
⚕️💕Gallifreyan CPR
⚕️👽Gallifreyan Assessment Scoring System (GASS)
⚕️👽ABCDE Assessment
⚕️⚠️Sepsis Emergency Response (SER)
⚕️⚠️Severe Trauma Protocol
⚕️🌡️Gallifreyan Thermoregulation and Emergency Response
⚕️🔮Psionic Emergency Pathways
⚕️✨Post-Regeneration Management
⚕️💤Gallifreyan Healing Coma Management
⚕️🩸Interpreting Gallifreyan Bloodwork
⚕️👶Gallifreyan Paediatric Emergencies
⚕️🧠Managing Gallifreyan Neurological Trauma
Any orange text is educated guesswork or theoretical. More content ... →📫Got a question? | 📚Complete list of Q+A and factoids →📢Announcements |🩻Biology |🗨️Language |🕰️Throwbacks |🤓Facts → Features:⭐Guest Posts | 🍜Chomp Chomp with Myishu →🫀Gallifreyan Anatomy and Physiology Guide (pending) →⚕️Gallifreyan Emergency Medicine Guides →📝Source list (WIP) →📜Masterpost If you're finding your happy place in this part of the internet, feel free to buy a coffee to help keep our exhausted human conscious. She works full-time in medicine and is so very tired 😴
#doctor who#dr who#dw eu#gallifreyans#gallifrey institute for learning#Time Lord biology#GAP Quick Guides#whoniverse#GIL: Biology#gallifreyan biology#GIL: Species/Gallifreyans#GIL#GIL: Biology/Medical
23 notes
·
View notes
Text
Also preserved in our archive
Contributors: Andrea Foulkes, ScD, and Tanayott Thaweethai, PhD
Researchers are investigating why some people experience lasting symptoms after recovering from COVID-19 – a condition called long COVID. It’s estimated that 65 million people in the world have long COVID, with more being diagnosed each day.
But most of this research has only studied adults. Do children and teenagers also get long COVID?
Unfortunately, the answer is yes — even young children can have lasting effects from COVID-19. A new study co-led by Mass General Brigham investigators found common patterns of lasting symptoms in school-age children and adolescents who previously were infected by SARS-CoV-2, the virus that causes COVID-19.
In JAMA, they report children and teens had prolonged long COVID symptoms in almost every organ system, and most had multiple symptoms affecting more than one system. The researchers also designed an index to identify children and adolescents who are most likely to have long COVID, finding that common symptoms were similar, yet slightly different between the two age groups. This index is intended for use in research studies, not clinical diagnosis.
“The symptom patterns we observed tell us we should study and evaluate long COVID differently depending on the child’s age,” says Andrea Foulkes, ScD, a Mass General Brigham biostatistician and co-senior author on the study. “The index used for this study is the first step toward a clinical tool that will help us diagnose, and eventually treat, long COVID in children and teenagers.”
Dr. Foulkes and Tanayott Thaweethai, PhD, a Mass General Brigham biostatistician and co-first author on the study, explain the index and their findings.
What is long COVID? Long COVID, also known as postacute sequelae of SARS-CoV-2 infection (PASC), are signs, symptoms, and conditions that can occur over time in people who were infected by COVID-19. Those symptoms can develop after someone recovers from the initial infection. Or they may be symptoms that occurred during the infection that have since relapsed, or have continued to persist for weeks, months, or years afterward.
The effects of long COVID can be mild, but they can also severely impact a person’s daily life and ability to complete normal tasks. Long COVID symptoms in adults often include worsening of symptoms after physical or mental exertion (called post-exertional malaise), brain fog, intense fatigue, persistent coughing, and loss of smell or taste.
A research initiative funded by the National Institutes of Health (NIH), called RECOVER (Researching COVID to Enhance Recovery), seeks to understand the long-term effects of COVID-19 and identify strategies to prevent and treat long COVID. The RECOVER initiative has also identified a cohort of children aged 0 to 25 years old, called RECOVER-Pediatrics, to study the condition in children.
Studying long COVID in children and adolescents Most long COVID research has only studied adults, so Dr. Foulkes, Dr. Thaweethai, and colleagues set out to understand if the condition affects young children and teenagers differently.
They analyzed data from the RECOVER-Pediatrics cohort, which included symptoms in children aged 6 to 17 that were reported by their caregivers. The researchers note that this was the first data-driven study of the differences in long COVID symptoms among school-age children (6-11 years old) and adolescents (12-17 years old).
Their study identified patients from across the United States, including 751 school-age children who had been infected by SARS-CoV-2 previously and 147 who were not, as well as 3,109 infected and 1,369 uninfected adolescents.
The researchers recorded prolonged symptoms that were present across all patients and narrowed the list down to only include those that were found in at least 5% of patients who had been infected with COVID-19. They then used statistical techniques to identify which of those symptoms were the most predictive of long COVID.
Common long COVID symptoms in children and teenagers The researchers created a PASC index, or measurement tool, that included the symptoms most likely to predict long COVID in children and adolescents. They identified 10 symptoms in school-age children and 8 symptoms in teenagers, with some overlap between the two age groups.
These were the most predictive symptoms of long COVID found in both school-age children and adolescents:
Trouble with memory or focusing Back pain or neck pain Headache Feeling lightheaded or dizzy For children aged 6-11, other unique predictive symptoms included:
Stomach pain Phobias, or fear of specific things Refusing to go to school Itchy skin or rash Trouble sleeping Nausea or vomiting For adolescents aged 12-17, other unique predictive symptoms were:
Change in or loss of smell and/or taste Body, muscle, or joint pain Daytime tiredness, sleepiness, or low energy Tired after walking While most patients in the analysis had multiple symptoms occurring at the same time, the authors acknowledge that even just one symptom could be enough to indicate long COVID.
The effects of long COVID in children Using their PASC index, the researchers estimate that in the RECOVER-Pediatrics cohort, 20% of the school-age children who previously had COVID-19 and 14% of the previously infected teenagers most likely had long COVID. These results, along with similar findings from another study published in Pediatrics, indicate that more children may have long COVID than the Centers for Disease Control and Prevention (CDC) reported as of 2022.
Even more troubling, Dr. Thaweethai adds that, “The children and teenagers with the most symptoms and the most organ systems affected were associated with poorer overall health and quality of life. This attests to the significant impact long COVID can have on children’s lives.”
What should I do if my child or teenager might have long COVID? If you think your child might have long COVID, talk to their pediatrician or primary care provider (PCP). While there isn’t a way for doctors to test for long COVID, they can help you and your child better understand what’s going on and help them cope with their symptoms.
The PASC index from this study can’t be used in clinical settings at this time, but it’s helpful for doctors to know that long COVID symptoms can be different between younger children and adolescents.
“A significant finding from this study was that common symptoms could be different between the two age groups,” says Dr. Thaweethai. “That tells us we should look at long COVID differently in school-age children versus adolescents.”
How can my family avoid long COVID? If you reduce your chances of getting COVID-19, you reduce your chances of getting long COVID.
There are steps you can take to help reduce your chances of getting or spreading COVID-19 and other respiratory viruses, like the flu and respiratory syncytial virus (RSV). Here’s what you can do:
Stay up to date with your vaccines, including the COVID vaccine and annual flu shot. Practice good hand hygiene. When you have a respiratory virus, take precautions to prevent spread. The CDC is a great resource for the latest guidance on respiratory viruses. “Studies like this one show how important it is to study this complex condition across multiple age groups,” say Dr. Foulkes. “The PASC index can help us track long COVID persistence and recovery in children, so we can begin to treat it more effectively.”
Study link: https://jamanetwork.com/journals/jama/article-abstract/2822770 (PAYWALLED)
#mask up#public health#wear a mask#wear a respirator#pandemic#covid#still coviding#covid 19#coronavirus#sars cov 2#long covid#covid conscious#covid19#covid is not over#covid in children
18 notes
·
View notes
Text
Achieve a Brighter, Healthier Smile with Expert Care at Compassion Dental Care, Pomona

Schedule an appointment at Compassion Dental Care Today!!!
Contact Us Today!!!
The Power of a Confident Smile Starts in Pomona, NY
Your smile is one of the first things people notice—and keeping it healthy goes far beyond appearances. At Compassion Dental Care in Pomona, NY, patients of all ages receive expert dental treatment that not only enhances aesthetics but also strengthens overall oral health. If you're looking to achieve a brighter, healthier smile, this trusted local clinic combines the latest technology with a truly compassionate approach.
From preventive cleanings to transformative cosmetic procedures, Compassion Dental Care makes oral wellness both attainable and enjoyable.
Why Compassion Dental Care Is the Preferred Choice in Pomona
Choosing a dental clinic isn’t just about location—it’s about comfort, credibility, and care. Compassion Dental Care has earned the loyalty of Pomona residents by providing reliable, gentle, and modern dental solutions in a warm, family-oriented setting.
A Name That Reflects Its Philosophy
“Compassion” isn’t just in the name—it’s in every interaction. The team prioritizes listening, understanding, and customizing treatment plans to ensure each patient feels safe, heard, and respected. Whether you're nervous about a procedure or simply due for a routine check-up, the staff’s calm and welcoming demeanor makes all the difference.
Personalized Dentistry for Every Smile
Every patient is unique—and so is their dental care. The clinic creates individualized treatment plans based on oral health needs, lifestyle, and long-term goals. This custom approach ensures optimal results with minimal discomfort.
Services That Strengthen, Brighten, and Transform Your Smile
At Compassion Dental Care, achieving a brighter, healthier smile is easier than ever thanks to a comprehensive range of services—all available in one convenient Pomona location.
Preventive Dental Care
A healthy smile starts with a solid foundation. Preventive care helps stop issues before they start:
Professional cleanings & exams
Low-radiation digital X-rays
Fluoride treatments
Dental sealants
Gum health evaluation
Oral cancer screenings
Regular visits help maintain your smile and reduce the need for costly future treatments.
Cosmetic Dentistry to Light Up Your Smile
Looking to brighten or reshape your smile? The clinic offers modern cosmetic treatments tailored to each patient's vision:
Teeth whitening for safe, long-lasting brilliance
Porcelain veneers for a flawless finish
Tooth-colored fillings that blend naturally
Smile makeovers combining art and science
Each procedure is carried out with precision and attention to aesthetic detail, ensuring your smile looks as good as it feels.
Restorative and Emergency Dentistry
To repair, replace, or restore damaged teeth, Compassion Dental Care provides:
Fillings, crowns, and bridges
Root canal therapy
Tooth extractions
Dental implants and dentures
Same-day emergency appointments for urgent care
The practice uses minimally invasive techniques and advanced materials for fast healing and superior durability.
Advanced Technology. Gentle Touch.
Compassion Dental Care pairs cutting-edge dental tools with a soft, human-centered approach. Patients benefit from:
Intraoral cameras for better visibility and diagnostics
Digital impressions for comfort and accuracy
Paperless forms and digital charting
TV-equipped rooms and sedation options for a relaxed visit
This technology not only improves treatment outcomes but also shortens chair time—so you can get back to smiling sooner.
FAQ
Is Compassion Dental Care accepting new patients? Yes. New patients are welcome, and the clinic offers introductory packages for exams, cleanings, and X-rays.
Do they treat both kids and adults? Absolutely. Compassion Dental Care offers full-family care, from toddlers to seniors.
What types of cosmetic treatments are available? They provide whitening, veneers, bonding, and comprehensive smile makeovers.
Does the clinic accept insurance? Yes. Most major dental insurance plans are accepted, and financing options are available for uninsured patients.
What safety measures are in place? The clinic follows ADA and CDC guidelines, with sterilization protocols, air filtration, and contactless check-in to ensure a safe visit.
Conclusion
Whether you want to protect your smile, enhance its brightness, or restore its strength, Compassion Dental Care in Pomona, NY offers the expertise, care, and technology to make it happen. With a compassionate team, tailored treatments, and a genuine dedication to your oral health, there’s no better place to start your journey toward a brighter, healthier smile.
Book your appointment today and experience the difference of dental care delivered with heart.
#dental office in pomona#dental office near me#dentist in pomona#dentist near me#100 days of productivity#911 abc#academia#agatha all along#agatha harkness#anya mouthwashing
2 notes
·
View notes
Text
The Importance of Veterinary Imaging in Modern Animal Healthcare

Understanding Veterinary Imaging
Veterinary imaging encompasses various diagnostic techniques that help veterinarians visualize internal structures of animals without invasive procedures. These imaging techniques include:
Veterinary MRI Services: Ideal for diagnosing neurological disorders, musculoskeletal injuries, and soft tissue conditions.
Veterinary CT Scan Services: Used for detailed cross-sectional imaging of bones, lungs, and complex anatomical structures.
Veterinary Ultrasound: Essential for evaluating soft tissues, abdominal organs, and reproductive health in animals.
Veterinary Radiology Service: Traditional X-rays remain a fundamental tool for detecting fractures, tumors, and internal anomalies.
With the increasing need for precision in veterinary diagnostics, finding a veterinary radiologist near me is becoming a priority for pet owners and veterinary professionals alike.
Why Choose a Veterinary Radiologist?

Benefits of Consulting a Veterinary Radiologist:
Accurate Diagnoses: Specialized training ensures precise interpretation of imaging results.
Advanced Imaging Techniques: Access to cutting-edge imaging technologies for comprehensive evaluations.
Collaborative Approach: Works closely with veterinarians to develop effective treatment plans.
Minimally Invasive Diagnostics: Reduces the need for exploratory surgeries, ensuring animal comfort.
Veterinary MRI: A Game Changer in Animal Healthcare
MRI (Magnetic Resonance Imaging) has revolutionized veterinary imaging by offering high-resolution images of soft tissues, the brain, and the spinal cord. Veterinary MRI services are particularly beneficial for diagnosing conditions such as:
Brain tumors and neurological disorders
Spinal injuries and disc herniations
Joint and ligament injuries
Soft tissue abnormalities
The Role of Veterinary CT Scan Services
Veterinary CT scan services provide detailed three-dimensional imaging, making them invaluable for assessing complex conditions. This imaging technique is commonly used for:
Diagnosing fractures and bone disorders
Evaluating lung diseases and chest abnormalities
Detecting internal tumors and metastases
Planning for complex surgical procedures
For pet owners and veterinarians looking for high-quality diagnostic imaging, veterinary CT scan services are an essential tool in modern veterinary medicine.
The Significance of Veterinary Ultrasound
Veterinary ultrasound is a non-invasive and painless diagnostic tool that helps in real-time visualization of internal organs. It is widely used for:
Monitoring pregnancy and reproductive health
Examining abdominal organs such as the liver, kidneys, and intestines
Detecting fluid accumulation or cysts
Guiding biopsies for accurate sampling
Finding the Right Veterinary Radiology Service
When searching for a vet radiology service, it’s essential to consider factors such as:
Expertise of the Radiologist: Ensure they are board-certified and experienced in interpreting animal imaging.
Turnaround Time: Quick and efficient reporting is crucial for timely treatment.
Availability of Advanced Technology: Clinics with state-of-the-art equipment provide more accurate diagnostics.
Collaboration with Veterinary Clinics: A reliable veterinary radiology service should work closely with general veterinarians to ensure seamless patient care.
Conclusion
Advancements in veterinary imaging have transformed the way veterinarians diagnose and treat animal diseases. Whether you need veterinary MRI services, veterinary CT scan services, or veterinary ultrasound, choosing a qualified veterinary radiologist near me ensures accurate and efficient diagnoses for your pet. With the growing demand for specialized diagnostic services, finding a trusted vet radiology service can make all the difference in ensuring the best possible healthcare for animals.
FAQ
1. What is the difference between veterinary MRI and veterinary CT scan services?
Answer:- Veterinary MRI services are best for imaging soft tissues, the brain, and the spinal cord, making them ideal for neurological and musculoskeletal conditions. Veterinary CT scan services, on the other hand, provide detailed cross-sectional images of bones, lungs, and complex anatomical structures, making them useful for diagnosing fractures, tumors, and lung diseases.
2. How do I find the best veterinary radiologist near me?
Answer:- To find the best veterinary radiologist near me, look for board-certified specialists with experience in interpreting various imaging modalities. Ensure they use advanced technology and provide quick, accurate reports. Collaborating with a reputable vet radiology service can also help ensure high-quality diagnostics.
4 notes
·
View notes
Text
i cant find the original study i read a couple years ago but this quote from this article summarizes it:
According to Dr Samah Jabr, chair of the Palestinian ministry of health’s mental health unit, experiencing such horrors does not easily translate into the clinical definition of, or treatment for, post-traumatic stress disorder (PTSD). Tools for evaluating depression, such as the Beck inventory, do not account for circumstances in which anguish is a reasonable response.
“If western society considers a car accident traumatic, can we use the same word for the level of atrocity happening in Gaza?” she said in an interview with the Observer. “The clinical description of PTSD captures the experience of, for example, a soldier who goes back home … Trauma in Palestine is collective and continuous. PTSD is when your mind is stuck in a traumatic loop. In Palestine, the loop is reality. The threat is still there. Hypervigilance, avoidance – these symptoms of PTSD are unhelpful to the soldier who went home, but for Palestinians, they can save your life. We see this more as ‘chronic’ traumatic stress disorder.”
#ppl in the us care more about the hypothetical poor widdle manipulated 18 year old who didnt know they were signing up to go murder people#than the thousands if not millions in the global south who have no 'post' trauma due to the ongoing violence of western imperialism#i will never feel empathy for us soldiers
3 notes
·
View notes