#C. diff. infection
Text
my dinner tonight was six donuts and milk
yes i regret my decisions but i will say that they were tasty
#shut up lily#shut up sage#me eating as if i dont have some undiagnosed digestive problems#which i definitely do because i have had reoccurring diarrhea for the past THREE YEARS and NO ONE KNOWS WHY#okay first it was a c. diff infection but NOW we dont know#ive had a goddamn colonoscopy and i can say the prep for that sucks#stupid liquid made me throw up in my mouth i could not drink it without gagging#anyways im rambling about health issues#that clearly part of the fault falls on my shitty diet and i am Aware#but I have terrible self control
1 note
·
View note
Text
My How Time Flies, When You're Having Fun?
Life has rather kicked me in the ass the last few months. The fun all started when I decided out of sheer boredom I should go to work in a daycare. I like infants, so that’s where I worked.
Well, we had one come in that I was very suspicious of the child having a condition referred to as C-Diff. Thirty plus years in nursing I had avoided this plague disease. As luck would have it, this very…

View On WordPress
#antibiotics c-diff#c-diff daycare#C-Diff Diabetes#cc-diff diarrhea#doctors nurses#dog snow#dog squat snow#fight infections#gamma globulin#gamma globulin immune compromised#gammagard#Immune compromised#influenza A#iv gammagard#Mayo Clinic#mayo rochester mn#over 65 diabetes#pickup v-plow#pneumonia#snow removal v-plow#snow v-plow#ulcerative colitis c-diff
0 notes
Text
Monopolizing turds

Update 31 May 2023: an earlier edition of this article identified the price of Rebyota as $20,000; this was the rumored price prior to Rebyota’s release in December 2022, when Stephen Skolnick wrote the article I referenced. When Rebyota was actually released in 2023, the average wholesale price (AWP) was $10,800. Thanks to Benjamin Jolley for catching this error, and to Stephen Skolnick for getting to the bottom of it.
It’s been ten years — to the day! — since I first started writing about the bizarre, amazing world of turd transplants, in which a sick person receives a microbiotic infusion in the form of some processed poop from a healthy person:
https://web.archive.org/web/20130608030455/http://blogs.plos.org/publichealth/2013/05/29/why-diy-fecal-transplants-are-a-thing-and-the-fda-is-only-part-of-the-reason/
Gut biomes are one of those understudied, poorly understood medical areas that are both very promising and also full of sketchy medical claims from “supplement” companies, influencers, quacks and grifters. But in the decade since I first started tracking turd transplants (formally called “Fecal Microbiota Transplants” or FMTs), a growing body of sound science has emerged on the subject.
One thing that’s increasingly undeniable is that the composition of your microbial nation is related in significant ways to both your physical and mental health. What’s more, as antibiotic resistant “super bugs” proliferate, FMTs are becoming increasingly central to treating dangerous gut infections that otherwise stand a high chance of killing you.
“Eat Shit and Prosper” is Stephen Skolnick’s delightfully named newsletter about poop and health science. Skolnick is a physicist by training, but has a long history of collaboration with Openbiome, a nonprofit that coordinates between doctors, patients and donors to provide safe FMTs:
https://stephenskolnick.substack.com/
In an edition of Eat Shit from last December, Skolnick recounts the amazing history and dismaying future of FMTs. In 2013, the FDA announced it would regulate FMTs as “Investigational New Drugs,” which could only be administered as part of a registered clinical trial:
https://stephenskolnick.substack.com/p/a-monopoly-on-poop
At that point, FMTs were already in widespread use by docs to treat otherwise untreatable cases of Clostridioides difficile (C. diff), an antibiotic resistant bacterial infection that literally makes you shit yourself to death. These doctors were in no position to run registered clinical trials, which meant that they would have to stop using the most effective therapy they had for a potentially lethal infection.
Doctors and patients kicked up a fuss, and the FDA walked back its guidance, announcing that it would exercise “discretion” in enforcing its Investigational New Drug rule, giving a pass to docs who were treating C. diff with FMTs:
https://www.federalregister.gov/documents/2013/07/18/2013-17223/guidance-for-industry-enforcement-policy-regarding-investigational-new-drug-requirements-for-use-of
That’s where things have stood for the past decade or so. The “discretion” rule means that patients could still get FMTs, but their insurance wouldn’t cover it. But even if you had cash to pay for an FMT, your doc probably wouldn’t administer it for anything except a C. diff infection, despite the promising signs that FMT can help treat other conditions, and despite the generally safe nature of FMTs.
If your doc did give you an FMT, chances are good that they sourced their poop from Openbiome. Openbiome recruits very healthy people, gets them to poop in a bag, then processes the poop — removing nonbacterial solids, testing it for pathogens, freezing it, portioning it, and sending it to docs. All this is done at cost, and it’s not cheap: $1–2k/treatment, mostly due to cold-chain logistics (the poop is shipped at -80C).
Despite the cost, and despite the limitations on treatment, the Openbiome method has proved very reliable. Indeed, FMTs as a whole are pretty darned safe, with the most common side-effects being transient gas and bloating. In the past decade, there’ve been a total of six “adverse effects” associated with Openbiome’s 5,000+ procedures, all in severely immunocompromised people, and none conclusively linked to the treatment:
https://www.sciencedirect.com/science/article/pii/S0016508522003511/pdf
A decade into this system, the FDA has taken the next step forward — only it’s actually a step backwards.
During this intervening decade, a pharma company called Ferring has conducted clinical trials on FMTs and received approval for an FMT product called Rebyota. The process for making Rebyota is effectively identical to the process used by Openbiome: collect poop, remove solids, test for pathogens, add glycerol, freeze and ship.
The main difference between Rebyota and Openbiome’s poop is price. While Openbiome charges $1–2k per treatment, Rebyota charges $10,800
That’s some expensive shit!
Fine. Getting Rebyota through clinical trials means that insurers might start covering it, and perhaps some patients will prefer brand-name poop to open-source poop. But as part of the FDA’s approval of Rebyota, the agency also rescinded its “discretionary enforcement” guidance, making it illegal for docs to source their poop from Openbiome:
https://www.fda.gov/regulatory-information/search-fda-guidance-documents/enforcement-policy-regarding-investigational-new-drug-requirements-use-fecal-microbiota
For Ferring, this is a monopoly on shit, one that lets them charge patients $10.8k for poop that costs $1–2k to process. The FDA does not claim that this is being done in the name of safety. Instead, an FDA official told Skonick that the goal was to “incentivize innovation without creating an access crisis.”
That is, the FDA changed its guidance and put nonprofit stool banks out of business because it wants to incentivize pharma companies to perform expensive clinical trials, and it believes that these companies won’t pay for trials if they have to compete with the likes of Openbiome, which would make it impossible to charge 900% markups on poop.
Trials are important! Evidence-based medicine is important! But Ferring’s clinical trials didn’t tell us anything we didn’t already know. FMTs were already the best therapy we had for C. diff. Testing Rebyota against a placebo didn’t tell us anything new — unlike testing Rebyota against the existing therapies, e.g. product from open stool banks.
Such a trial might have given rise to a very different regulatory outcome, because the cure rate reported by Rebyota is much lower than the cure rate from Openbiome’s own interventions:
https://link.springer.com/article/10.1007/s40265-022-01797-x
That is, using the $1k poop from Openbiome seems to be much more effective than using the $10.8k poop from Ferring. But Openbiome, a nonprofit, hasn’t been able to perform the kind of rigorous — and expensive — clinical trial that Ferring funded.
This points to a significant problem with the FDA’s model. The agency wants good clinical data for the medicines it regulates, as it should, It presumes that the only way to get that data is through granting commercial exclusivity to a for-profit, which ends up costing patients vast sums, and locking many patients out altogether.
This creates all kinds of new dangers. 150,000 people/year in the US contract Recurrent Clostridium difficile Infection (RCdI). FMT increases the cure rate by 20% relative to antibiotics alone. That means that if everyone with RCdI gets a poop transplant, 30,000 extra people will get better. That’s a big number!
For well insured people, Rebyota probably represents a cash-savings — if your insurance covers the $10,800 procedure, you might pay $500 out of pocket, which is far less than the $1–2K you’d pay to get an Openbiome poop transplant. But if you’re uninsured or underinsured, the FDA’s new enforcement rules mean that you’re now on the hook for $10,800.
The FDA did carve out a loophole: if your doc or their hospital are willing to prepare the poop transplant themselves, they can administer that. On the one hand, preparing a poop transplant isn’t that hard — some people do them at home, on their own:
https://web.archive.org/web/20211015060558/https://thepowerofpoop.com/epatients/fecal-transplant-instructions/
But on the other hand, there’s been exactly one death conclusively linked to FMT, and it was from one of these hospital-prepared transplants (the patient had just had a marrow transplant for cancer that wiped out their immune system, and the donor had a novel pathogen that the hospital failed to test for).
So the FDA has created a situation where, if you can’t afford a $10,800 proprietary formulation, your only option is to convince your doc or hospital to prepare their own poop transplant, which will cost less than the $10.8k for Rebyota, but more than the $1–2k from Openbiome, which has all kinds of economies of scale. And if you do manage it, you’ll be getting a procedure that has a much worse safety track-record than the Openbiome process that the FDA just killed.
The FDA has an important role to play here, but as with so many policy questions, how the FDA plays that role depends on things that are far upstream from the agency and its decisions. The choice to fund medical trials through the promise of exclusivity — and with it, extremely high margins — puts the FDA in the position of choosing winners in the marketplace: Ferring wins, Openbiome loses.
Ironically, this is the thing that exclusivity is supposed to prevent. By using profit to incentivize medical research, the FDA is supposed to be recruiting the Invisible Hand as its partner in regulation. But exclusivity is incompatible with the idea of medicine as a public good. The tens (hundreds) of millions that Americans will pay for $10.8k poop transplants from Ferring will add up to far more than it would cost to underwrite clinical trials for an open process like Openbiome’s.
The result: both Americans’ wallets and Americans’ guts suffer.
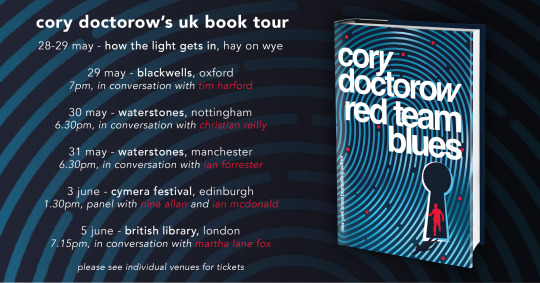
Catch me on tour with Red Team Blues in Hay-on-Wye, Oxford, Manchester, Nottingham, London, and Berlin!

If you’d like an essay-formatted version of this post to read or share, here’s a link to it on pluralistic.net, my surveillance-free, ad-free, tracker-free blog:
https://pluralistic.net/2023/05/29/oh-shit/#rebyota
[Image ID: A poop emoji wearing a top hat and a monocle, posed against a backdrop of e coli bacteria seen through a high-resolution microscope.]
#pluralistic#stool bank#eat shit and live#pharma#fda#regulatory capture#fecal transplants#microbiomes#rebyota#openbiome#c diff#fmt#fecal microbiota transplant
272 notes
·
View notes
Text

Tiaki Vixen you will always be famous!!! 💫🩷
something I was working on while in and out of the hospital…I haven’t made any updates on tumblr, but I recently got diagnosed with IBS and C. Diff so I’ve been fighting that for like 3 months now 😭 finally finished my 1st round of antibiotics so hopefully that keeps the infection away for good, however i’ve heard sometimes C. Diff takes multiple rounds :( so here’s to hoping it’s gone for good
Tiaki belongs to my boyfriend @trenchcoatsss !!! 🩷💋
Kofi | Print Shop
#swaghetti art#swaghetti rambles#fanart#dnd#dungeons and dragons#oc#not my oc#half elf#bard#jester#dnd oc#dnd ocs#dnd oc art#dungeons and dragons oc
19 notes
·
View notes
Text
Parasites take an enormous toll on human and veterinary health. But researchers may have found a way for patients with brain disorders and a common brain parasite to become frenemies.
A new study published in Nature Microbiology has pioneered the use of a single-cell parasite, Toxoplasma gondii, to inject therapeutic proteins into brain cells. The brain is very picky about what it lets in, including many drugs, which limits treatment options for neurological conditions.
As a professor of microbiology, I’ve dedicated my career to finding ways to kill dangerous parasites such as Toxoplasma. I’m fascinated by the prospect that we may be able to use their weaponry to instead treat other maladies.
Microbes as Medicine
Ever since scientists realized that microscopic organisms can cause illness—what’s called the 19th-century germ theory of disease—humanity has been on a quest to keep infectious agents out of our bodies. Many people’s understandable aversion to germs may make the idea of adapting these microbial adversaries for therapeutic purposes seem counterintuitive.
But preventing and treating disease by co-opting the very microbes that threaten us has a history that long predates germ theory. As early as the 1500s, people in the Middle East and Asia noted that those lucky enough to survive smallpox never got infected again. These observations led to the practice of purposefully exposing an uninfected person to the material from an infected person’s pus-filled sores—which unbeknownst to them contained weakened smallpox virus—to protect them from severe disease.
This concept of inoculation has yielded a plethora of vaccines that have saved countless lives.
Viruses, bacteria, and parasites have also evolved many tricks to penetrate organs such as the brain and could be retooled to deliver drugs into the body. Such uses could include viruses for gene therapy and intestinal bacteria to treat a gut infection known as C. diff.
Why Can’t We Just Take a Pill for Brain Diseases?
Pills offer a convenient and effective way to get medicine into the body. Chemical drugs such as aspirin or penicillin are small and easily absorbed from the gut into the bloodstream.
Biologic drugs such as insulin or semaglutide, on the other hand, are large and complex molecules that are vulnerable to breaking down in the stomach before they can be absorbed. They are also too big to pass through the intestinal wall into the bloodstream.
All drugs, especially biologics, have great difficulty penetrating the brain due to the blood-brain barrier. The blood-brain barrier is a layer of cells lining the brain’s blood vessels that acts like a gatekeeper to block germs and other unwanted substances from gaining access to neurons.
Toxoplasma Offers Delivery Service to Brain Cells
Toxoplasma parasites infect all animals, including humans. Infection can occur in multiple ways, including ingesting spores released in the stool of infected cats or consuming contaminated meat or water. Toxoplasmosis in otherwise healthy people produces only mild symptoms but can be serious in immunocompromised people and to gestating fetuses.
Unlike most pathogens, Toxoplasma can cross the blood-brain barrier and invade brain cells. Once inside neurons, the parasite releases a suite of proteins that alter gene expression in its host, which may be a factor in the behavioral changes it causes in infected animals and people.
In a new study, a global team of researchers hijacked the system Toxoplasma uses to secrete proteins into its host cell. The team genetically engineered Toxoplasma to make a hybrid protein, fusing one of its secreted proteins to a protein called MECP2, which regulates gene activity in the brain—in effect, giving the MECP2 a piggyback ride into neurons. Researchers found that the parasites secreted the MECP2 protein hybrid into neurons grown in a petri dish as well as in the brains of infected mice.
A genetic deficiency in MECP2 causes a rare brain development disorder called Rett syndrome. Gene therapy trials using viruses to deliver the MECP2 protein to treat Rett syndrome are underway. If Toxoplasma can deliver a form of MECP2 protein into brain cells, it may provide another option to treat this currently incurable condition. It also may offer another treatment option for other neurological problems that arise from errant proteins, such as Alzheimer’s and Parkinson’s disease.
The Long Road Ahead
The road from laboratory bench to bedside is long and filled with obstacles, so don’t expect to see engineered Toxoplasma in the clinic anytime soon.
The obvious complication in using Toxoplasma for medical purposes is that it can produce a serious, lifelong infection that is currently incurable. Infecting someone with Toxoplasma can damage critical organ systems, including the brain, eyes, and heart.
However, up to one-third of people worldwide currently carry Toxoplasma in their brain, apparently without incident. Emerging studies have correlated infection with increased risk of schizophrenia, rage disorder, and recklessness, hinting that this quiet infection may be predisposing some people to serious neurological problems.
The widespread prevalence of Toxoplasma infections may also be another complication, as it disqualifies many people from using it for treatment. Since the billions of people who already carry the parasite have developed immunity against future infection, therapeutic forms of Toxoplasma would be rapidly destroyed by their immune systems once injected.
In some cases, the benefits of using Toxoplasma as a drug delivery system may outweigh the risks. Engineering benign forms of this parasite could produce the proteins patients need without harming the organ—the brain—that defines who we are.
17 notes
·
View notes
Text
we have an ongoing microbiology project this semester where we pick out a handful of pathogens from a list the professor gave us and then fill out charts about them with info like how they function and what treatments are available or whatever concept we've been learning about recently
and one of the questions was "is it a common hospital-acquired infection?" aka things like pneumonia or c. diff or whatever. which is very useful information to know if you're going into medicine, but also kind of hilarious when the pathogen you're writing about is, like, rabies.
like imagine you bump into an acquaintance who was in the hospital and you go "oh my god i heard you had appendicitis, are you okay???" and they're like "yeah the surgery went great! barely even left a scar. i got rabies while i was there though :("
11 notes
·
View notes
Text
I am home in quarantine, doing a lot better! A lot of stressful & painful things happened, but I have to quarantine for at least 2 weeks thanks to c. diff. I will be able to make more art soon, & I apologize for the delay.
I'd like to shout out the medication Dificid for being run by evil people who want to charge hundreds, if not thousands of dollars, for a cure to a highly contagious & dangerous infection. You are dirty, evil bastards.
If you ever get c.diff in USA, request something called "vancomycin hydrochloride" if you don't want to go broke.

(enjoy my dog!)
#itsme.txt#hospital arc part 4#hopefully final arc#thank you especially specialshinytrinkets for keeping up with my posts ;_;#i big time appreciate you
9 notes
·
View notes
Note
was diagnosed with a uti earlier thought of you❤️❤️
LMFAO as someone who is still on bactrim i feel for you (and praying for you too if you got put on this shit)
remember to drink water, take azo if you're able (do NOT take this shit if you're wearing contacts tho. will turn that shit orange), and take probiotics!!! (not at the same time as you take your antibiotics. like 4 hours after or 4 hours before. you wanna avoid that c diff or yeast infection lmao)
wishing you a fast recovery and bloodless piss 👍
#core responds#i love that i'm just the uti girl now#i get them so often i really gotta see a specialist honestly but who has the time or money for that
10 notes
·
View notes
Text
I am jinxing all of my patients to be positive for all the infections this week. I had 3 people I checked for Hep C and all were positive. I had a lady with a chronic cough who I checked for TB, and she had TB. I had a guy with a minor toe wound that I didn’t like the look of and checked him for osteomyelitis, and he had osteomyelitis. I saw a lady with stomach pain, checked her for H pylori, and she had H pylori. I saw a lady who had severe diarrhea after a hospital stay and checked her for C diff, and she had C diff. I saw a lady with a rash on her palms and soles and tongue and I checked her for syphilis. She had syphilis. Every infection I have checked anyone for this week has come back positive.
I am apparently an infectious disease doctor now instead of a family doctor.
49 notes
·
View notes
Text
Q. What are the more serious potential adverse effects of short-term use of proton-pump inhibitors (PPIs)?

A. Be aware of the rare but serious potential for acute interstitial nephritis or Clostridioides difficile infection. Since PPIs are often started in the ICU for stress, we'll include aspiration pneumonia, instead of aspiration pneumonitis, since higher gastric pH allows more bacteria to live in the stomach and potentially wash into the lungs.
Pro-tip: The risk for C. diff increases significantly after 2 weeks on a PPI.
Image: J.S. Choi, MD
6 notes
·
View notes
Text
So my doctor prescribed me a double course of Dificid (which will cost my insurance around $8,000) for my recurrent c. diff. He also mentioned starting me on a course of Vowst, which is an oral fmt pill that's useful for unlucky gals like me who just can't shake the infection. I was looking up the pricing information for Vowst and-

I'm literally crying rn. I think I might actually cost my insurance half a million before the end of the year, and considering they almost killed me due to not approving my prior authorization until I was admitted to the hospital (which resulted in me having multiple surgeries this year) idgaf, they can fuck right off and pony up every single penny for my medication. 😈
#disability tumblr#chronic illness#clostridioides difficile#c. diff#crohn's disease#don't mind me i'm just finding some morose humor in any way i can#it's the way i cope with all of the medical trauma i've faced#tw: medical#personal#max muses
16 notes
·
View notes
Text
I gotta wonder how this happens
(incase you do not know, C. Diff is a gastrointestinal bacterial infection and it basically just makes you shit yourself really badly, ouch)
5 notes
·
View notes
Note
i might have already asked, but, opinions on nixos if you've tried it?
i haven't actually tried it but i think it's based and i want to try it really bad. the general premise is that you can fix all of your dependency management and reproducibility problems and replace them with new, more exciting problems that have to do with the nix language
i would very much like to trade to have those problems, because my builds would be so much faster than docker builds. docker builds are also a nightmare because they require a bunch of privileges to even run the docker daemon
so like, a brief list of things you get with nix
verifiable, reproducible builds: you could rerun your build pipeline from scratch and get the same SHA for the final artifact. all of your dependencies are also built with this property. so you basically have transitively pinned dependencies for everything managed by nix. that's huge for security and assurance
great build caching: a side effect of the above, this means you can cache intermediate build results instead of starting the whole build over. and you can be very confident that your cache isn't bringing in stale/incorrect gunk. compare to docker, where caching happens at the layer level, has a bunch of confusing caching rules, and can't account for side effects that make cached layers undesirable. plus the layers build on top of one another, so you can't really pick and choose which layers to cache; if you invalidate a lower layer, everything above it has to be rebuilt, even if the diff would be the same
hermiticity: since you know up front the full list of dependency files you need for your build, you can download those ahead of time and then do the build without talking to the internet! this is another huge win for security, because the internet is where all the fucked up and evil shit comes from, so you want to avoid it wherever possible. reduces your attack surface. this is especially important because infecting the build chain is an increasingly popular attack (supply chain attacks) and extremely effective at owning a ton of computers at once--that package you're building will be trusted by the rest of your machines, so it better be built in a secure environment
avoid a large swath of dependency issues that happen with other package managers: nix lets you have multiple versions of the same package, which removes a lot of pain that happens with other package managers. say you have package A, and package B requires A>=1.3 but package C requires A<=1.0. what do you do? well... you suffer. you also can't install A==5.0 for fun because you live on the bleeding edge. not so with nix
there's probably more goodies im forgetting but yeah. nix is based and solves a lot of cool problems in dependency management, build correctness and speed, and supply chain security. the flip side is that you have to learn a new configuration language just for this one thing, and in addition to being a functional language (which most programmers aren't used to), it has its own quirks and sharp edges because it's somewhat niche. also you have to hope the packages you want are already supported, otherwise you'll have to figure out how to build them yourself.
9 notes
·
View notes
Text
Nothing in my day-to-day job shows me the limits of modern medicine like vancomycin does. And it makes me insane.
(extremely long, somewhat incoherent nerd rant below the cut)
See, vanc is really good at, like, three things: treating MRSA (when given IV), treating ampicillin-resistant enterococcus (when given IV), and treating c diff (when administered orally ONLY). Most every use outside of that, like when it’s used to treat methicillin-susceptible staph aureus for “penicillin allergic patients” (don’t get me started on PCN allergies), actually has data that it increases risk of morbidity and mortality (i.e. harm and DEATH).
Unfortunately, due to the prevalence of multi-drug resistant organisms, vancomycin is empiric therapy for a lot of presumed infections. And it's a lot more difficult to actually tell if someone has an infection than you'd think. A lot of medical conditions imitate each other and when time is of the essence to identify what's going on, the most ethical thing is to start an antibiotic and rule out infection as the hospitalization continues. Lab techniques have gotten a lot quicker: I can remember 8 years ago, it would take 3 days just to identify what microbe the patient had in their presumed infection. These days, anno domini 2023, PCR comes back in a matter of hours, identifying gram positive/gram negative staph/strep/bacilli/etc, and it's the sensitivities that take 2-3 days. (Don't get me started on contaminated cultures.) But even with improvements in lab technique, we might not culture any microbe at all or the provider might keep vancomycin on "just in case" because we don't know IF the patient is infected, WHAT they're infected with, or if the infection will get better with a different drug.
And vancomycin is terrible on kidneys. Extremely nephrotoxic. It isn’t as bad as the 80s when the drug first came out and was called Mississippi Mud colloquially, but it will fuck the patient up if not monitored closely.
But finding the correct dose for each patient in a timely manner is nigh impossible. This is because vancomycin is renally eliminated. We have to mathematically estimate how well the kidneys are working. Unfortunately, our mathematic equation is next to useless if you are:
-Less than 50 kg
-Shorter than 5 foot tall
-Have a BMI of more than 40
-Are an adult younger than 45 (twenty-year-olds get astronomical doses that would be destructive in an older patient)
-Are older than 65 (the official definition of 'geriatric', i'm relatively sure)
-Are female (this is really only applicable if the patient is less than 50 kg or older than 65 - think: little old frail lady - we have absolutely no fucking idea how their kidneys are doing until we order the serum drug level. It is next to impossible to accurately dose vancomycin in little old ladies on the first try.)
-Are missing limbs (lots of leg amputations in the older and impoverished diabetic population!!)
-Have a lot of muscle mass (think bodybuilder or really tall guys)
Fun fact: we estimate renal function by looking at height, weight, age, birth gender (few, if any, studies on trans patients taking HRT), and a lab value called serum creatinine. Creatinine is a byproduct of muscle metabolism, I don't know the fine details, but we can generally estimate how well kidneys are working by seeing how much creatinine is in the blood: low creatinine usually means kidneys are excreting it as they 'should' be. High creatinine means there's something wrong, the kidneys aren't able to excrete it as efficiently as they 'should' be. But the effect of low muscle mass and high muscle mass haven't been studied enough to be able to adjust our mathematical equation to compensate for them. And with high BMI: we often overestimate their renal function because we don't know how to estimate their muscle mass vs their body fat.
(I work out in the boonies. ~70% of our patients have diabetes. ~80% of our patients have a BMI of greater than 35. So what I'm trying to say here is: we are shooting in the fucking dark when we're estimating the renal function of the vast majority of our patients.)
Complicating this: vancomycin is useless until it reaches steady-state concentration in therapeutic range. On one side of this problem: a lot, if not most, medical providers assume that vancomycin starts working its magic from the first dose. So we sometimes get orders for "vancomycin 1 gram now and see how the patient is doing in the morning". That isn't going to solve jack shit! That's just going to increase the incidence of microbial resistance!!
OR, like in the multiple situations I dealt with this afternoon, you make an educated guess on what regimen is going to work for the patient. You get a level 48 hours after the dose starts. And you find out that you fucking guessed wrong and the patient is subtherapeutic. It has been two fucking days and the patient hasn't started being treated for their (presumed) infection yet!! And we've increased the possibility of microbial resistance! *muffled screaming in frustration*
So what I'm trying to say here is: on almost every presumed infection that comes into the hospital (which we're guessing like 30%? 50%? of the time), we're starting an extremely toxic drug, oftentimes 100% guessing what regimen will be therapeutic, only finding out in 2 days that it is not therapeutic, and it can sometimes take days and days to titrate the dose sufficiently to find a therapeutic regimen. And sometimes we're really fucking unlucky and we destroy the patient's kidneys temporarily (or permanently! but kidneys can be very resilient so that's thankfully rare) because we guessed a regimen that's too high!! This is a fucking nightmare!!!!!!!!
And if all of this wasn't bad enough, we don't really have any drugs that do what vancomycin does therapeutically. We have things that can be used to cover some of what vancomycin does, but nothing that's equivalent AND less toxic.
Like, to fix this situation, we need:
-Better education to providers on what drugs are appropriate empiric therapy for different presumed infections (we're working on it, we are working on it)
-Better ways to estimate kidney function (there needs to be more research on kidney function in patients with BMI greater than 35!! And little old ladies!! And patients with low body weight and high body weight and amputations and...)
-Better prognostic tools to tell 1. when the patient is infected (looking at you, sepsis!!!) 2. what they're infected with
-Less-toxic antibiotics AND/OR better ways to treat infection (this would be the evolution of medicine as we know it)
And I want to be clear: vancomycin isn't bad. It's an extremely effective tool when used correctly but we often either don't have enough data to use it correctly or the provider doesn't understand that this tool is fucking useless for the job they're trying to perform.
#some days i'm just smacked in the face by the limits of modern medicine#there is so much we don't know!!!#we're doing the best we can!!!#negativity#personal#us healthcare#i understand other hospitals will have a different experience than this#but my corporation is extremely stingy and we get all the new grads#so educating providers and nurses is a never-ending wheel at my facility#and we don't treat anything complicated except orthopedic surgeries#some days I just get overwhelmed by how little we know#if you can guess my profession on the first try please keep it to yourself i'm trying to maintain a low profile here okay#also if you ask me medical questions don't expect an answer#i was a Cs Get Degrees student all I know i've learned on the job and I don't know shit
6 notes
·
View notes
Text
my disclaimer for this is that i have no idea if i'm actually disabled/could be considered disabled etc. but ever since having mono for three terrible months and then getting covid and then hitting autistic burnout and then going abroad and having terrible asthma and fatigue and then getting an ear infection and developing bell's palsy and then getting c diff ... i just KNOW that i would benefit so strongly from a mobility aid. and a shower stool. and probably a million other things that i don't know about. i'm just so fatigued constantly and walking across campus is often too much. thinking abt the "weird girl" in high school who wore a knee brace and had a cane and how much we all (yes myself included) judged her and questioned the "truthfulness" of it. thinking abt how the only thing preventing me from getting a mobility aid rn (besides $$) is fear of my mom's judgement and ridicule. thinking about how the place and people i grew up with contributed to my internalized ableism. anyway ,
18 notes
·
View notes
Text
spider ramble... particularly about false widows
in a Mood™ abt spiders currently, ESPECIALLY false widows. been going back over my arachnid section of the invertebrate module bc i have exams soon and its late and im frustrated abt how false widows get portrayed by the media and percieved by the british public... this is gonna be long and rambly and probably not make much sense and go off in a million and one diff directions sorry i just feel like talking abt spiders. this also came about bc of the big fuckoff house spider that was in my room last night on the top of my door frame but since it was late (like. midnight) and also out of my reach i went eh. ill deal with it in the morning. and then i woke up in the morning and no more spider to deal with! which i should be more stressed about i feel but im so exhausted from the run up to exams and other life stuff that im just like ok cool thats Around somewhere now ig. im guessing it was a female from the size but i cant be sure... anyway without further ado onto the main show.
so here in the uk we arent exactly known for our venomous animals. we have some but they're nothing really that dangerous (to us as humans at least. im not going into venom-prey specificity rn ive had ENOUGH of that recently). we have the european adder (which is also percieved as terrifying bc its a venomous snake but it poses very little risk to us as humans bc they are very shy and i have a lot to say abt adders but thats for another day), wasps, bees, some venomous fish (didnt know this until i found one rockpooling they r pretty neat), even some stinging jellyfish and siphonophores like the portuguese man o war. and then we have the spiders. all species of spider are venomous (minus the uloboridae family, aka the cribellate orb weavers which im not too sure off the top of my head if we have those in the uk... we might have one or two species?? idk but they arent venomous and i think theres another family that has some non venomous spiders BUT THE POINT IM MAKING IS PRETTY MUCH ALL SPIDERS ARE VENOMOUS). there are 650ish spp of spider in the uk and of those VERY FEW are at all medically significant. of these few are the rabbit hutch spider, the cupboard spider, and... the noble false widow. these 3 spiders are all known as false widow spiders. we also occasionally get the meditterreanean false widow, but to my knowledge these only arrive on imports and dont have a population within the uk.
belonging to the genus steatoda, false widows are usually seen as these terrifying death spiders that will kill you just for looking at them when really... they arent actually that dangerous. most cases of bites being severe are either a) a result of an allergy or b) it was actually caused by something other than the bite itself (such as a bacterial infection in the bite, or the "bite" not actually being a bite) or even c) greatly exaggerated by the tabloids (shocker)... like ok we dont have many scary animals in the uk but. we dont need to overexaggerate the ones that really arent as bad as people think! badgers probably pose more of a threat to you than a false widow does. have you seen a badger?! they look so cute but they are VICIOUS those things will FUCK YOU UP and give you TB on top of getting absolutely mauled. a false widow will, at most, just make you feel a bit ill for a couple of days. me personally i would take a falsie over the badger. false widows also only bite in defense! most of the time they bite because you didn't see them and happened to be a very big thing up in their personal space! tbh i would bite too
false widow bites are, to most people, no more harmful than a wasp sting. so its not exactly a fun time but its not exactly the limb destroying death bite that the british media loves to make it out to be. most bites are probably dry bites or have near neglible amounts of venom, so won't cause anything more than a bit of pain. when venom does get involved it gets a bit more complicated bc it depends on how ur body reacts to it. as i said before, most ppl its not much worse than a wasp sting but it can cause things like muscle spasms, sweating, and a raised temperature. it rarely gets worse than that. of course you can be allergic to it which will cause anaphylaxis which is a medical emergency, but this is an exceptional circumstance. most ppl bitten by a false widow will not experience that. the panic over false widows in the uk is a mixture of media-driven mass hysteria and arachnophobia.
anyway in conclusion shoutout brandon collier who did an amazing talk abt false widows during the bhs venom day both at the 2022 and 2023 events both of which i was lucky enough to attend. if i cant go to venom day this year you will see me on the news.
#spiders#false widow#ramble#nixxy's animal talk#making that a tag because this will happen again soon probably#all this being said#i did use their reputation to my benefit last summer#there was one on the outside kitchen door at the cafe i worked in#so in order to not have to go in there#and also to prevent anyone accidentally getting bitten#bc remember i said they bite in defense#being grabbed as someone opens the door would cause them to bite in defense#i told the owner#who told me to not be dramatic#anyway guess who she then asked to deal with the spider on the door handle not 10 minutes later?#me#if im dealing with spiders#im not dealing with the vile customers or horrible owner#as for the beast in my room#i heard it before i saw it#at first i thought oh!#im going crazy again!#and then i looked for the source of the weird tappy scratchy rustly sound and saw one of the biggest spiders i have ever seen#in the uk at least#and that isnt like. a tarantula#tho saying that it was bigger than my friend's new tarantula tho so#new pet ig!#idk where that thing is#ill find it when im packing probably#christ thats a lot of tags
3 notes
·
View notes
Last Seen Blogs

sugar-miilk
Sugar

stephenstroble
tumblr. Haiku

strykercss
Untitled

pvtidiot
Untitled

ei-mae
Unicorns and shizz