#Anaemia Prevention
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Mobile Tumblr US users spend an average of 4.04 minutes per session on the app.
Text
Demystifying Anaemia: 10 Fact You Should Know
Understanding these facts can help debunk myths and encourage people to take anaemia seriously Anaemia is a condition where the body lacks enough healthy red blood cells or haemoglobin to carry adequate oxygen to the tissues, leading to symptoms like fatigue, weakness, and shortness of breath. While commonly attributed to iron deficiency, anaemia can result from various causes, including vitamin…

View On WordPress
#Anaemia#anaemia blood test#anaemia common facts#Anaemia disease#anaemia home remedies#Anaemia in adolescents#anaemia in children#anaemia natural remedies#Anaemia Prevention#anaemia prevention food#Anaemia risk in youth#Anaemia risk reduction#Anaemia Symptoms#anaemia treatment
0 notes
Text
My lovely friends, this is a friendly evidence-based post pertaining to the risk reduction of a few well-known health effects of 4n4 and mia. Including: Amenorrhea (loss of regular menstrual period), anaemia, digestive upset, dehydration, electrolyte imbalance, general well-being, and osteoporosis. It is quite a long post, but please let me know if there’s any other information you would like me to cover. 💕
🪐 Vitamins and Supplements:
• A-Z Multivitamin. Is beneficial for supplementation. For example, Vitamin C is a vitally important vitamin for the body’s connective tissues, including the maintenance of healthy bones and teeth, cellular formation and maturation, resistance to infection, and an increased ability to heal. Additionally, B12 contributes to an adequately functioning nervous system, bone marrow, and intestinal tract. It also acts to increase metabolism of protein, carbohydrates, and fats. Finally vitamin B2 when combined with Vitamin A promotes good vision and healthy skin, as well as assists in metabolising proteins and fats at a cellular level.
• Calcium and Vitamin D. Seek a preparation which offers 1000mg of calcium and 10-20mcg (400-800 iu) of vitamin D. Vitamin D increases the bodies efficacy during the absorption, retention, and metabolising of calcium. Calcium of course being vital for bone integrity and imperative for the prevention of osteopenia/osteoporosis.
• Iron. An appropriate iron intake will restore the functionality of red blood cells, allowing the proper oxygen transportation around the body, increase focus, energy, athletic performance, and sleep. Having a sufficient iron store will alleviate some commonly experienced symptoms of low iron including fatigue, dizziness, pallor, and shortness of breath. It may also reduce the sensation of cold hands and feet.
• Potassium and Zinc. A lack of zinc impairs the ability to smell and taste. Connecting this impairment to nose blindness. For example, a lack of a sense of smell and taste may impair one’s own ability to detect their own bad breath, BO, and other unpleasant smells that others may be able to detect.
• Omega 3’s - Fish oil, Krill oil, Hemp oil, or Flaxseed oil. Improper dietary intake, or supplementation of omega 3 fatty acids will result in areas of epidermal (skin) dryness, hyperkeratosis, and hyperpigmentation. As well as the formation large scales expose underlying tissue, which are easily infected. The hair becomes sparse, dry, lusterless, and brittle, with a reddish tinge. Furthermore, nails become brittle and dull, tear production reduces, the tears are also significantly less oily leading to increased evaporation contributing to chronically dry, red, and itchy eyes.
If oil supplements are scary for you to intake due to calorie fears (there is only approx 25 calories in 2 average fish oil capsules). There are dietary sources of omega 3 that are relatively low calorie including chia seeds, edamame, and seaweed. However they provide little amounts in comparison to supplementation or traditional dietary sources such as fish, avocado, oils etc.
However this should also be considered when deciding whether to supplement omega 3’s - they stimulate the secretion of leptin, a hormone that decreases appetite and promotes the burning of fat. Through the enabling of conversion of dietary fats into body cells for burning as fuel.
🍄 Dietary Intake
•Bone broth (or vegetable broth if meat is not apart of your diet ☺️) I cannot stress how great bone broth is! Extremely low calorie, but incredibly nutrient-dense. It also acts to decrease the inflammation within the gut that many of us will experience due to our dietary habits. Including conditions such as constipation, gastroparesis, liver disease, bloating, abdominal pain, and stomach ulceration.
Bone broth also contains large amounts of protein, collagen, iron, vitamins A and K, fatty acids, selenium, zinc, and manganese. Protein being the most satiating macronutrient can decrease hunger and associated discomfort. Collagen and the variety of micronutrients within the bone broth contributes to joint and bone health. Bone broth will also contribute to hydration.
•Nutrient-dense foods including blueberries l are among the best sources of anthocyanins (antioxidants) that promote brain health and reduce the risk of cognitive decline. Additionally, red tomatoes and red capsicum (Peppers). Tomatoes are the richest source of lycopene, which is a type of carotenoid found in red fruits that has powerful antioxidant effect that may help protect against heart disease and certain types of cancer.
•Fibre is imperative for smooth gastrointestinal function, including regular bowel movements. Fibre is of course typically found in whole fruits and vegetables, beans/lentils, and whole grains. Low calorie fibre sources include: red kidney beans, carrot, and chickpeas. Psyllium, chia seeds are also good sources of fibre. Fibre supplants such as Metamucil may also aid to increase fibre intake. An adequate intake of fibre may reduce the dependence of laxative for bowel movements. Prolonged use of laxatives may create a dependency on them to even have a bowel movement.
🥥 Adequate Hydration
• The best way to ensure adequate hydration is simply by consuming enough water during the day. However, if plain water consumption is difficult, fluid intake will also suffice. Including fluid such as teas, flavoured/enhanced water, diet soft drinks, juices, etc. The optimal fluids to consume in addition to, or instead of simple water to ensure adequate hydration is mineral water, coconut water, or diet electrolyte replacements (Powerade/Gatorade, Pedialyte, Hydralyte). Correct hydration and electrolyte intake will reduce headaches, constipation, and muscle cramps/weakness.
❤️ Reproductive Health
•Amenorrhea is a common experience for those of us with a uterus. However it is imperative to understand that you are more than likely still ovulating despite the lack of a regular menstrual period. Therefore, contraception must still be used. Amenorrhea may be alleviated through dietary supplementation and small changes to the diet to include more micronutrients, but it may not be completely fixed unless there is an increase to body fat percentages.
#fitblr#ed not ed sheeran#ed#edblr#edtwt#ed tmblr#ed bullshit#anorex14#tw ana shit#ana and mia#tw mia#ana e mia#tw ed diet#meanspø#grossp0#fitspiration#notprojustusingthetags#4norexi4#4n4#4n4blr#4norexia
252 notes
·
View notes
Text
Since fools are hand-wringing about (cis) women (and afab trans people) "mutilating" themselves by getting hysterectomies because it """harms""" their bodies and shows an alienation with the body:
The uterus has no hormonal or sexual function (according to my drs). It is a bag to grow a baby in. If you get rid of it, and not the ovaries, you can expect such horrrors as:
A mild and temporary mood drop from hormone fluctuation, especially if you had an IUD that was removed with the uterus.
Some minor temporary intestinal problems as your organs readjust to the gap.
A few months of sexual dysfunction while the body readjusts itself. It went away entirely on its own within 6 months of surgery.
Some mild confusion once a month when you feel like killing or crying about everything but because you no longer menstruate you get no advanced warning or bloody reminder that this is only the standard hormonal fluctuation and not a new type of insanity hitherto unbeknownst to science.
That's it.
Insisting that there are other treatment methods for things like endometriosis and PCOS is actively harmful. I promise you we have tried them all, whether we wanted them or not, whether they worked or not, whether they made things worse or not. It is pretty much impossible to get a doctor to agree to a surgical solution until you are 30 and have tried everything else for at least a year per alternative treatment. Some of these alternative treatments, like lupron, can have awful, permanent consequences for your body, like irreparable loss of bone density, while only working in about 1/3 of patients, and then only temporarily. You can't be on it long term because it will destroy your bones. Most of these treatments involve preventing menstruation, since that's when the symptoms are the worst. For context, I've recovered from surgery without painkillers, I've broken bones, and neither one of those was anywhere near as bad as peak endometriosis symptoms. Heavy bleeding and hemorrhaging, which also occur in these disorders, cause other issues for you body, including but not limited to chronic anaemia.
I get wanting to rehab the uterus' image. I get concerns, given the history of medicine, over a misogynistic society just cutting women up to their detriment rather than treating them holistically and effectively. I get wanting to keep your own uterus. But panic doesn't help here, and neither does insisting this organ is special and necessary and it's function is special and necessary.
If you want to freak out about women being pushed to harmful, unnecessary surgery, gastric bypass and other weight loss surgery is right there y'all.
#menstruation#endometriosis#also you only ~need~ a period if you have a uterus#and even then you dont ~need~ it every month
297 notes
·
View notes
Text
The Blood Runs Thicker (part 6) ~vampire!William Afton x F! Reader~
~100% totally not using this darker fic to vent my frustrations over a paper....totally not...~
Tag-List; @ruh--roh-raggy @randymeeksisafinalgirl @sleepy---head @robin-the-enby @hungrhay @likoplays @slxsher-whxre @nicolezghostz @spiderlilytengu
✧・゚: *✧・゚:* Want more or something different? *:・゚✧*:・゚✧
CW:Minors DNI, (18+ ONLY), Female Reader, legal age gap (Reader- 20's, William - 50's), graphic acts of violence, biting, knife-play, blood, blood-drinking/licking, mention of dead children, anaemia. Graphic description of injuries. The suit stays ON

The car ride back was predominantly silent, and you were glad that there was nobody on the roads as you tried your best to navigate using William's car. He'd simply chucked the keys at you and grunted shortly after the incident at the pizzeria, assuming you knew how to drive. It was lucky that you knew some of basics, but you tried to avoid moving or adjusting things like the seats in case it angered him that you were messing this with stuff. Michael had also climbed into the back-seat, clearly intending to come with the pair of you.
William had clearly gotten off lighter, somewhat thanks to the suit you suspected, you could already make out where the skin had turned pink and started to knit back together painfully slowly. Whereas Michael had clearly taken William's wrath full throttle, shuddering as he poked his tongue through a hole that had been torn into his cheek, exposing his molars in the glow of the streetlamps as you passed them. You weren't even sure both of his eyes were intact, his face too bloody and distorted from being hit by the older man to tell. Something told you that you didn't want to know.
"Left here." Afton growled, his tongue moving to where the tooth had been ripped from his gum as you quietly complied, turning down the long gravel drive and through the trees towards his home. You heard shuffling in the back, making you glance quickly through the seats before focusing on the road again.
"All this time, and you come crawling back here." Michael chuckled, if you could call the gurgling, wet sound emerging from his distorted mouth a laugh. You could almost hear the eye roll from William in return.
"I could say the same about you. After what you did."
"You're one to talk, dad." Michael flipped off William, who responded in kind, a sickly grin on his face as the car pulled up to a stop and you climbed out. Opening the door for William and feeling him roughly bumping into your shoulder as he headed for the house, allowing you to move around to Michael's side and open the door for him. He gave you a bloodied smile before he reached into his pocket, pulling out a black cloth mask and pulling it on over his ears, hiding the gruesome sight from you. He grunted as he tried to stand, his legs giving out slightly and you reached out to catch him, slinging one of his arms over your shoulder.
"Leave him, he's only gone and done it to himself." William called to you, standing impatiently in the doorway, arms folded across his chest as he observed you trying to shoulder some of Michael's weight and help him walk towards the house.
"Do you want him bleeding all over your gravel or do you want him inside?" You snapped back, earning a huff of annoyance and watching as William disappeared inside, slamming the door loud enough to make you flinch, even from across the drive.
"Thanks....You don't have to help me if you don't...don't want." Michael panted, groaning as he shifted against you and tried to keep his weight off of you whilst allowing you to help him.
"He's a prick, and you're in bad shape."
Michael gave another wet sounding laugh at that, finally making it to the porch and letting his weight slump down against the wood. Making you yelp as you were dragged with him, his arm shot out to catch you and prevent your body slamming down however. You were surprised at how strong he seemed to be, even as his body shook gently, clearly in pain and struggling to function as normal. Turning his body in a few slow careful movements, looking out into the emerging dawn and sighing as he tried to run his fingers through his matted hair.
"So why are you with him, if he's such a prick?." He asked, glancing at you from the side with his one good eye. You noticed in the light how they were a more greenish grey compared to William's blue-grey, but you could see some of the resemblance in the face he had left.
"You think I put myself through this all voluntarily?" You scoffed, pointing to the red mark on your neck, the bruising on your jaw and pulling down the shoulder of your top to reveal the bandages there, as well as lifting the leg of your shorts to show the other one there. Michael's eyes flickered to each, but didn't remain long, as if he was afraid of what he would see if he did.
"I did wonder why you were wearing those clothes despite the fact it's freezing out here." He chuckled, sighing again and leaning forwards on his elbows, looking at his knuckles and studying the damage done to his hands. Brow furrowing as he noticed a few of his fingers bending at an unnatural angle, reaching for them and grunting as he grabbed them and pulled. The faint sound of bones grinding against each other hitting your ears and making you grit your teeth as they moved into a more normal position, watching as he wiggled his fingers to test how they moved afterwards.
Carefully, Michael took off his jacket and placed it around your shoulders, the size swallowing you up and your cheeks heating up as he did it, revealing a now extremely bloody white t-shirt beneath it. You opened your mouth to protest, feeling how wet and sticky some parts of the fabric were against you, but Michael waved his hand dismissively as if sensing your protests.
"I don't need it at the moment, but you definitely need the heat." He nodded to you, his eyes crinkling slightly as you assumed he smiled beneath the mask.
"He really....I knew he was cruel but..." You couldn't find the words to express it, and Michael laughed bitterly. His shoulders shaking slightly as he turned his head towards you, tilting it slightly.
"Do I look that bad?"
"I mean... Surely you saw in the rear-view o-or the mirrors on the car." Trying to be polite with him, but raising an eyebrow as he shook his head, chuckling again before it devolved into a small coughing fit. Seeming to take a few deep breaths to recover from the effort before he spoke again.
"Can't see myself in mirrors. He can't either if that's some solace about the narcissist. I'm guessing you've not been here long."
"About a week. Wait, you guys can't see yourselves in mirrors?" Taken by surprise at the thought that they couldn't, but thinking about it, you had never seen William in a reflective surface, or a mirror during the time you had been at his house. And you never bothered to look in the rear-view during the drive back.
"A week and you've not noticed? Guess he's just been avoiding them. Yeah, we can't see ourselves in mirrors, which sucks sometimes when you need to try and make sure you look human and presentable. I was surprised you didn't use the rear-view and check on us."
"I'm too short for how he has his seat set."
There was a pause and another laugh, Michael slapped his knee and began to cough as he took it in. Your cheeks heating up more as you fought back the urge to smile at it. You felt somewhat relaxed around him, although there was still a lingering sense of unease from the pizzeria and the back-room as well as your mind constantly whispering that he was a predator still.
"Head on inside kiddo. I'm going to stay out here for a bit, and you should get warm. Would you mind chucking my jacket in the wash when you have a chance? I think it may need it." You nodded in response and your hand rested on his shoulder lightly as you stood up, smiling at him as he looked up at you. The faint morning light illuminating just the amount of damage that William had done to him. His own son.
"Goodnight Michael."
"Good morning kiddo." He joked back, turning his attention back to the woods as you opened the door and slipped inside. The house eerily quiet and no sign of William immediately, though you placed Michael's jacket on the counter and headed upstairs, watching the shadows carefully for any sign of Afton lurking for you to wander past.
~~
The day was bright outside once you woke up. No Afton licking at you like a barely contained dog at a steak. No more aches and pains than you had become accustomed to in the past few days. You were almost suspicious of how peaceful the day had started out.
Padding down the stairs, you could smell something delicious cooking. William was a good cook, but he seemed to ignore a majority of seasonings for a reason you couldn't define, putting it down to enjoying your misery a little more each day. But coming into the kitchen, you found an unfamiliar back to you at the stove.
"Michael?" You called softly, watching as he spun around. Reaching for the mask he had clearly washed and placed at the side for when you came down. Your eyes widening as you took a look at him in the light from the window.
Whereas you would have put William into older and handsome, despite being a cruel, vindictive bastard. Michael had clearly inherited the sharp features and strong jaw of his father, but with a youthful roundness still in his face. Thinner brows and lighter brown hair that had a slight wave to it framed his face, and you could see how tall he was too. Not as tall as William, but certainly he would have met or exceeded it one day, although unlike Afton's broad, muscular frame; Michael was lithe and slender.
"Good morning sleepyhead!" He said, struggling to put the mask on over his ears. The hole in his cheek still present, although judging from the dampness in his hair, he'd at least had a shower. The eye had had been damaged still red and puffy, bloodshot, but you could see it moving around and looking now rather than just a bloody mess.
"You've....improved?" You said tentatively, making him pause and blink as he looked at you for a second. Laughing, you felt your own smile coming through at the sound, it wasn't dark and foreboding like William's laugh, but it sounded like what you imagined a big brother would laugh at his kid brother falling over or doing something adorable.
"Well, thank you. I mean, I can feel my face is a little less ground-meat this morning, but it's always nice to have the confirmation." Winking at you, he turned back to the stove and put something on the plate, walking it over to the island and putting it down.
"You can cook?"
"Call it the one thing my dad did right."
You headed for the cupboards, intending to find cereal but Michael's hands settled onto your shoulders, directing you to sit infront of the massive stack of pancakes he'd cooked up, watching as he easily opened cupboards and found out syrup and butter for you.
"T-These are for me?" You ask incredulously, thinking back to the cereal and peanutbutter jelly sandwiches you'd had for breakfast for the past week. Your stomach growling in anticipation.
"Well, I didn't make them to look pretty now!" He laughed again, taking a seat opposite you and watching your expression as you picked up a fork. Digging in and your eyes widening at the taste. You weren't sure how William had made sandwiches and cereal taste bland, but the sugar was an overwhelmingly welcome taste.
"Can you even eat?" You ask between bites, letting your curiosity come through as Michael raised an eyebrow, picking up a spare fork from the counter, taking a stab at the edge of the pancake and popping the piece into his mouth. Covering his open cheek with one hand consciously. Chewing and then opening his mouth, sticking out his tongue to show he'd swallowed it.
"Yep. Well....It's a kinda complex answer. Long and short? Yeah, we can eat, but it doesn't taste like anything unless it's super salty, or heavy in certain things like iron. I can just about taste a blue steak, but it's more like you've just swallowed it and are getting the aftertaste?" He tried to explain, putting one elbow on the counter and resting his chin on his hand.
"So...People?"
"Yeah, that's the fucking awful part. Blood has taste to it, it varies from donor to donor, but it all factors into that person's lifestyle, diet ect." Scrunching his nose and then looking at you curiously. Humming in consideration. "Guessing you're anaemic?"
"How'd you know?" You almost choked on your food, deciding to eat more slowly whilst you talked so you didn't end up choking to death from the syrupy goodness. Michael carefully pushed over a water with his free hand, thanks falling from your lips as you took a sip.
"My father is....a preferential hunter. I would say picky bastard, but at least they have standards. I'm sure you got the same four page long health questionnaire that I did when you applied to Freddy's."
"I always thought that was for the insurance." Michael scoffed at your explanation, rolling his eyes and clicking his tongue. Shaking his head slightly and looking down at the counter, brow furrowed as he lost himself in thought for a few moments. "So...weird question then."
"We're talking about vampirism, and how people have taste whilst my face is half open. I don't think weird quite covers it."
"If blood has taste then it must have a smell too right? So...what do I smell like?"
Michael blinked as you asked the question, scanning your face for any signs that you were joking. You tried to keep it serious as he looked at you, sucking on his teeth for a second before his larger hand gently took yours, pulling it towards him, frowning as he saw the bite marks on your skin before he wiped his hand over them. Wincing as one of the scabs came off and a single dot of red appeared against you, watching as he leaned in close and the way his nose crinkled. Shuddering as his cool breath moved against your skin as he exhaled. His turn crumpling further as he let go of your wrist and allowed you to pull it back.
"Honestly, I can't make out you at the moment. You just smell like my dad. Have you gotten any of your own stuff since you arrived?" Sighing as you shake your head and he stands up, throwing the dishes in the sink with a slight clatter as he grabs a hoodie you hadn't noticed on the chair and pulls it on.
"Come on, we'll get you something better than his ratty shit to wear, and when you get back, you're having a shower."
~~
The bright lights of the supermarket had clearly bothered Michael throughout the trip out, wearing thick sunglasses and the face-mask to hide his still slightly gruesome appearance from the public. Watching as he rubbed his temples and his eyes from time to time, like he was trying to dispel a growing migraine. Pushing the cart infront of you, you had tried to pick some clothes that were comfortable and easy to put on. T-shirts, some jeans, a couple of skirts. Underwear. You still weren't sure what had happened to the set that you'd taken off for your first bath in the house, but something told you that William would deny anything had happened if you asked him.
"Where is he today?" You ask as you looked at body wash, trying to find your usual scent and opening the caps carefully to sniff before placing them back. Michael shuffled behind you quietly, the loud environment and lights taking a toll on him physically and mentally as it took him a moment to respond.
"Probably cleaning the place up. Oh, and 'food' run." He air-quoted food, giving you an idea of what he might be up to. Swallowing dryly before you picked out your necessary toiletries, feeling conscious of how much it was all going to cost, and you weren't even sure where your card was to pay for it all. Michael had already leant you a pair of his jeans from when he was a teenager, and they had been a tight fit. Realising that he's always been a lanky man was somewhat comforting, but you did wonder how long ago that had been for him.
Finishing up quickly, Michael gently bumped you out of the way to pay, much to your protests and especially to your protests as he grabbed the heavy bags filled with various snacks, drinks, clothes and toiletries. Carrying them as if they were nothing to him, although his shoulders visibly relaxed as you both stepped outside into the cooler air, the light much more soft and natural.
"Thank you Michael."
"For the love of god woman, you can call me Mike. But, I do have a question for you." He asked, and even though he was wearing sunglasses, you could tell he was looking at you.
"Alright, that seems a little unfair on you, but ask away."
"Back in the pizzeria, how did you know my name?"
You froze up as he asked, thinking back to the darkness. The bear staring at you from around the shelf with hollowed out eyes, the soft whispering, cold air moving against you like some living, breathing thing.
"Can you please help my brother?"
"There was...I don't know how to say it without sounding utterly crazy." You laughed, swallowing and furrowing your brows as you both walked along the side of the road, Mike standing next to the road and keeping you away from it. Looking at your borrowed shoes before you took a deep breath and talked slowly. "There was..a bear.."
"Freddy, yeah he's kinda the face of the whole thing."
"No, like a yellow one." You watched as Mike paused, stopped dead in his tracks as he tilted his head to look at you, studying your features before nudging you down a slightly worn path towards the woods. He clearly wanted to be away from the road.
"Go on..."
"And there were like...these whispers. I thought I was going crazy, but one of them.. they told me your name, they asked me to help you." You explained, watching the woods draw closer as you heard the bags rustling and suddenly Michael took your hand, squeezing it tightly as he didn't look at you. His head keeping up despite the fact you could feel his hand shaking, your brow furrowing as he kept walking, not saying anything for a few moments before he spoke in a shaking voice.
"Can you do me a favour? If you go back...can you ask them if they can forgive me?" He asked, swallowing softly as he slowed his walking as you approached the wooded area. You gave his hand a squeeze back, confused as to what he would need to be forgiven for, but noticing how whatever it was affected him in ways he wasn't willing to talk about.
"Of course."
"And please don't mention it to my dad."
The rest of the walk was silent, but the coolness of Mike's hand against yours as he clung desperately to you like a scared child was enough to speak to you both.
You were both going home to your own monsters.
#steve raglan#william afton#springtrap#william afton x reader#fnaf movie#springtrap x reader#steve raglan x reader#william afton smut#william afton x you#fnaf x reader#vampire william afton
76 notes
·
View notes
Note
Can time lords / Gallifreyan have iron anemia?
Can Time Lords / Gallifreyans get iron anemia?
🩸Gallifreyan Blood and Iron Usage
Unlike humans, who rely on red blood cells to transport oxygen via haemoglobin, Gallifreyans have an entirely independent respiratory system that doesn't use oxygen transport through the bloodstream. Instead, their blood (a metaphorical equivalent made up of Blood X1-cells and Blood X2-cells) circulates nutrients, heat, and chemical messengers.
Blood X1-cells, which contain iron, are vital for cellular respiration and various metabolic processes. Although the respiratory system is independent, iron still plays a key role in Gallifreyan cellular respiration, ensuring that cells can function efficiently and process energy.
😴How Iron Deficiency Might Affect Gallifreyans
Since Gallifreyans don't have haemoglobin or red blood cells, iron deficiency in them wouldn't appear like in humans. In humans, iron deficiency leads to anaemia because there's not enough haemoglobin to carry oxygen to tissues. For Gallifreyans, however, the impact would be different:
Energy and Metabolism: Iron is still essential for cellular respiration, even if the process doesn't involve haemoglobin. Without enough iron, a Gallifreyan's ability to process energy efficiently might be compromised, leading to fatigue or sluggishness.
Healing and Regeneration: Because Blood X2-cells contain artron and lindos (the key substances involved in Time Lord physiology), a lack of iron could slow down or impair these processes. The body's ability to recover from injuries or complete regenerative cycles might weaken.
Cravings and Body Response: A Gallifreyan low on iron would likely experience strong cravings for iron-rich food, such as red meat, as their body attempts to replenish this vital nutrient. The digestive system would work hard to absorb and recycle whatever iron it can find.
🪫Iron Regulation and Deficiency
Gallifreyans have a more advanced regulatory system for iron, allowing them to adapt quickly when levels get too high or too low:
Too Little Iron: When iron levels drop, signals are sent to the circulatory, digestive, and respiratory systems to recycle iron, absorbing as much as possible from food intake and even redistributing internal stores to critical areas. This would likely stave off full-blown iron deficiency for longer than in humans but wouldn't make them immune to it.
Too Much Iron: Conversely, when there's an excess of iron, Gallifreyan kidneys produce artron, which helps neutralise and expel the excess iron, preventing toxicity. This system keeps their iron levels in check, but an iron deficiency might weaken their ability to regulate properly.
🏫So ...
Yes they can, but in a very different way from humans. A Gallifreyan wouldn't develop iron-deficiency anaemia as we understand it in humans, but they could suffer from iron deficiency, leading to issues with energy metabolism, regeneration, and possibly immune response. Their symptoms would likely include:
Fatigue or sluggishness due to compromised cellular respiration
Weakened healing and regeneration abilities
Cravings for iron-rich foods, signalling their body's need to replenish vital nutrients
However, thanks to their advanced biology and ability to recycle and regulate iron levels, it would take a REALLY long time of iron deprivation for these symptoms to become severe.
Related:
💬|🫀🩸Does a Gallifreyan have the same blood type across regenerations?: If a Gallifreyan retains the same blood type across their bodies.
💬|🫀🩸Could a human receive a blood transfusion from a Gallifreyan?: If a human could receive blood from a Gallifreyan, and its benefits.
💬|🥗🍲What does a Gallifreyan diet look like?: Normal eating habits of Gallifreyans
Hope that helped! 😃
Any purple text is educated guesswork or theoretical. More content ... →📫Got a question? | 📚Complete list of Q+A and factoids →😆Jokes |🩻Biology |🗨️Language |🕰️Throwbacks |🤓Facts →🫀Gallifreyan Anatomy and Physiology Guide (pending) →⚕️Gallifreyan Emergency Medicine Guides →📝Source list (WIP) →📜Masterpost If you're finding your happy place in this part of the internet, feel free to buy a coffee to help keep our exhausted human conscious. She works full-time in medicine and is so very tired😴
#gil#gallifrey institute for learning#dr who#dw eu#ask answered#whoniverse#doctor who#gallifreyan biology#time lord biology#gil biology
11 notes
·
View notes
Text

Of all nutrients oxygen is the most essential.
💫Oxygen has more fundamental nutritional roles than vitamins and minerals or any other nutrient.
💫Oxygen is considered a Yang force; without it, fuel in the body cannot be burnt for energy and heat.
💫Anaemia is sometimes a result of insufficient oxygen.
💫Lacking in oxygen, one feels heavy, depressed and without vitality.
💫Oxygen is also needed for vitamin C utilisation, to slow down collagen breakdown and to prevent premature aging.
💫Once sufficient oxygen is in the body, one feels charged with life and is usually no longer attracted to intoxicants.
💫Oxygen is a purifier, helps eliminate waste in the body.
💫Oxygen destroys germs and viruses and resolves pathogenic moisture.
10 notes
·
View notes
Text
End-stage renal disease patients developed left ventricular hypertrophy, Gezira State- Sudan by Dr. Nahla Ahmed Mohammed Abdurrahman in Journal of Clinical Case Reports Medical Images and Health Sciences
Abstract
Background: Left ventricular hypertrophy is the strongest independent predictor of cardiovascular death, and it is worsening in association with SCD. According to studies from the main international registers, cardiac disease is the leading cause of unexpected mortality in dialysis patients. Several studies have found that the prevalence of LVH is high among patients on maintenance haemodialysis, and that numerous risk factors linked with it, such as anaemia, hypertension, and volume overload, are common in these patients. Many clinical and nephrologist researchers are focusing their attention on the processes and factors that are present in these patients in order to prevent and regress the development of LVH.
Aim: The purpose of this study is to investigate the prevalence of left ventricular hypertrophy and associated risk factors among patients receiving routine haemodialysis at Gezira Hospital for Renal Disease and Surgery.
Method: This was a cross-sectional research with 70 patients receiving routine haemodialysis. Personal and clinical information was collected. The measurements included blood pressure, ECG, and echocardiogram. The concentration of haemoglobin was determined.
Result: Patients in the study ranged in age from 20 to 80 years old. Male made up 57 % (n=40). 75% of the individuals had LVH, with 68% undergoing echocardiography and just 7% receiving an ECG diagnosis. LVH affected 30 of the 40 male patients and 15 of the 30 female patients. Anaemia was detected in 44 (88%) of the 48 LVH patients with Hb12 gm/dl. In 74 % of the patients, systemic hypertension (BP>140/90mmHg) was present, and it was identified in 42 of the 48 patients with LVH. According to the evaluation, volume overload was evident in 63 % of the patients (32 out of 48 patients with LVH). The Chi-squire test was performed to determine the frequency and distribution of study participants based on several characteristics (age, gender, anaemia, volume overload, HTN, and dialysis duration) and LVH; the link between age and LVH, HTN and LVH, and DOD and LVH was statistically significant. P-values of 0.001, 0.013, and 0.005 were all significant.
Conclusion: We concluded that LVH is common among haemodialysis patients, and that there is a link between age, HTN, and DOD and LVH in this study.
KEY WORDS: Left Ventricular Hypertrophy, End Stage Renal Disease, Gezira State, Sudan
ABBREVIATION: CKD= Chronic kidney disease, ECG= Electrocardiograph, ESRD=End stage renal disease, Hb=Haemoglobin, HD=Haemodialysis, IVS=Interventricular septum, LVEDD=left ventricular end diastolic diameter, LVH=Left ventricular hypertrophy, LVM=Left ventricular mass, MRI=Magnetic resonance imaging, PW=Posterior wall.
Introduction
When kidney function declines and renal replacement therapy is required, the heart and vascular tree undergo major structural and functional changes, and the prevalence of cardiovascular disease is higher than in the general population (Usrds, 2017), with 40 % of all deaths in patients with end-stage renal disease (ESRD) due to cardiac causes ( Steddon, S, 2014). Left ventricular hypertrophy (LVH) is a typical indication of cardiac structural disease in ESRD patients, defined as an increase in left ventricular mass (LVM) due to increased wall thickness. Anaemia, hypertension, hypervolemia, and mineral metabolism problems are all linked to a loss in renal function, which increases the risk of LVH (McCullough et al., 2016). The researchers discovered that the strongest independent predictor of cardiovascular mortality in patients with chronic kidney disease is LVH (Shlipak et al., 2005), and that worsening of it is associated with SCD in haemodialysis patients (Kim H et al., 2015), which is a major cause of mortality in these patients (Paoletti et al., 2004). In individuals with chronic kidney disease (CKD), the prevalence of LVH is around 40%, and it increases with CKD progression until it reaches 75% in ESRD patients (McCullough et al., 2016).
Chronic kidney disease CKD is defined as kidney damage or a GFR of less than 60 mL/min/1.73 m2 for at least 3 months and is divided into five stages ('K/DOQI clinical practice recommendations for chronic kidney disease: evaluation, classification, and stratification, 2002). Left ventricular hypertrophy LVH, reduced LV function, regional wall motion abnormality, pericardial effusion, and valvular calcification are among the anatomical and functional cardiac abnormalities seen in ESRD patients. LVH is a common complication in ESRD patients and is a preventable risk factor (Charytan, 2014). HTN, vascular calcification (Nitta et al., 2004), anaemia, and volume overload (Vaiinien et al., 2017) are all risk factors for LVH in ESRD patients. The prevention or regression of LVH was achieved with early and effective management of these risk factors (Kim et al., 2015; Erdan et al., 2018).
LVH was caused by a variety of pathophysiologic variables in CKD and ESRD patients, who were categorized into three groups (Ritz and Wanner, 2008):
Afterload: an increase in systemic arterial resistance, raised arterial blood pressure, and impaired large-vessel compliance, which necessitates a rise in intra cavity pressure during ventricular contraction (Mominadam et al., 2008).
Preload: a condition caused by intravascular volume expansion (salt and fluid loading), anaemia, and an AV fistula (Di Lullo, et al., 2011; Cuadrado et al., 2004).
Not related to afterload or preload.
Arterial hypertension and poor control of blood pressure is the most common cause of chronic pressure overload of the left ventricle and cardiac adaptation in response to chronic pressure overload is LVH (Sweety et al., 2014).
Renal dysfunction and poor cardiovascular prognosis are linked to the coexistence of anaemia and LVH (Chang et al., 2014). Non-hemodynamic and hemodynamic adaptations are used in anaemic persons to maintain adequate tissue oxygenation. Increases in erythropoietin synthesis and intra-erythrocytic concentrations of 2,3-diphosphoglycerate (2,3-DPG) lower the affinity between oxygen and haemoglobin, resulting in a shift to the right of the oxygen haemoglobin dissociation curve (Oski et al., 1971).
When compared to conventional haemodialysis, short haemodialysis reduces LVH due to proper fluid control (Ayus et al., 2005), and intensive HD (McCullough et al., 2016). While frequent haemodialysis resulted in LVH regression (Trinh and Chan, 2016;Chan et al., 2018). In comparison to traditional haemodialysis, the improved clinical outcomes resulted in a higher frequency of vascular access procedures complications (Slinin et al., 2015).
Despite the numerous research that have been conducted to improve the quality of haemodialysis, it remains a complex procedure that necessitates a coordinated effort from your entire health-care team, including your nephrologist, dialysis nurse, dialysis technician, nutritionist, and social worker.
Diagnosis of LVH is by
ECG: This is the first non-invasive test, although it is less sensitive in diagnosing LVH (Vanezis and Bhopal, 2008), and there are various criteria for diagnosing LVH:
Limb lead voltage criteria: R in a VL > 11 mm, R in a VL > 13 mm if left axis deviation is present, and S in L III > 15 mm if left axis deviation is present. >25 mm R in LI + S in LIIII
Sokolow-Lyon criteria for chest lead: S in V1 + R in V5 or V6 >35 mm (Sokolow and Lyon, 1949).
Romhilt-Estes criteria: deep S in V1/V2 and tall R in V5/V6, with the aggregate of both exceeding 7 large squares or one of them exceeding 5 large squares (Romhilt and Estes, 1968).
Echocardiography: is a more sensitive and specific method of diagnosing LVH than an ECG. ECG criteria must account for ethnicity in people of African descent (Vanezis and Bhopal, 2008), and they must be correct in patients with HTN to rule out LVH (Pewsner et al., 2007). Left ventricular mass (using the Troy formula according to the American Society of Echocardiography ASE recommendation):= 1.05 (LVEDD+IVS +PW)3 LVEDD3.
The LVMI is calculated by dividing the LVH mass by the body surface area. LVH was characterized as an LVMI of greater than 150 g per m2. (from the Framingham Heart Study) (Armstrong and colleagues, 2014).
MRI: is the gold standard for assessing left ventricular mass, cavity volume, and pattern of LVH, whereas M-mode echocardiography (ECHO) overestimates LV mass in haemodialysis patients when compared to CMRI (Ebeid et al., 2017)
ESRD: but they are not commonly utilized due to cost and lack of availability. In practice, echocardiography is a good all-around instrument that is well-suited to long-term research studies.
Sudden cardiac death is the most prevalent cause of mortality in dialysis, accounting for 40% of deaths, most of which occur in the first three months of dialysis due to difficulty adapting to the cardiovascular stress that is characteristic of dialysis. And it could be due to LVH after a period of acclimatization. LVH is becoming more common among ESRD patients, particularly those on haemodialysis. It is also one of the most common causes of mortality among such patients. Many risk factors for LVH in such people could be treated to reduce the prevalence or regress LVH, and thus the risk of death. As it stands, diagnosis is not difficult and can be accomplished using less invasive techniques such as echocardiography and ECG.
MATERIALS AND METHODS
Study area: The study was conducted in Gezira hospital for renal disease and surgery- Gezira State- Wad Madani Central Sudan, which service the Gezira and whole nearby areas.
Study design: In Gezira hospital for renal disease and surgery, a descriptive, cross-sectional study was done among haemodialysis patients.
Study population: The study comprised 70 patients on daily haemodialysis, both male and female, ranging in age from 20 to 80 years. Each of the patients in this study dialyzed twice a week at the Gezira hospital for renal disease and surgery. Time and duration of dialysis, symptoms of volume overload, blood pressure, and lower limb oedema were among the personal, demographic, and clinical data obtained. The concentration of haemoglobin was determined. In patients with patent arterio-venous fistulae, blood pressure was monitored in the contralateral arm with a mercury sphygmomanometer. Standard limb and chest leads were used, with a paper speed of 25mm/s and a gain of 10mm/mV (or 5mm/mV). Sum of S wave in lead V1 and R wave in lead V5 or V6 35mm and/or R wave in lead aVL 11mm was classified as Sokolow-Lyon LVH. A physician performed the ECG interpretations. IVS, LVPW, LVEDD, and LVESD were measured using M-mode echocardiography and 2-dimensional ultrasonography.
Haemodialysis: The blood is filtered and cleaned out of the body, then reintroduced to the body in this operation, three times a week, for 4-5 hours. which has been used to treat advanced and permanent kidney failure.
Inclusion criteria: All patients who receive regular haemodialysis are eligible.
Exclusion criteria: Patients with established congenital heart disease or a history of heart disease, diabetics, and hypertensive patients prior to dialysis are also excluded.
Data analysis: The data were analysed using statistical package of social science (SPSS) version 24 .
Ethical consideration: All participants in this study were fully told about the study's goal and were promised that any personal information regarding their health status would be kept private.
Ethical clearance: Ethical clearance was acquired from the Gezira university faculty of medicine's ethical committee. Permission to conduct research in the Gezira hospital for renal disease and surgery from the director.
RESULTS
This study included 70 patients on regular haemodialysis in Gezira hospital for renal disease and surgery, including 40 males and 30 females ranging in age from 20 to 80 years. The Chi-square test was performed to determine the frequency and distribution of research participants based on various characteristics. At 0.05, the P-value is considered significant.
There is a significant relationship between duration of hemodialysis and LVH P value (0.005 )
DISCUSSION
Many risk factors contribute to the prevalence of left ventricular hypertrophy in CKD and ESRD patients, which has encouraged clinical nephrologists and researchers to focus their attention on processes and factors that are present in these patients for many years. LVH, which worsens with SCD in haemodialysis patients, is the strongest independent predictor of cardiovascular death in patients with chronic renal disease (Shlipak et al., 2005). The goal of this cross-sectional study was to find out how common LVH is and what the risk variables are among haemodialysis patients.
The main conclusion is that, 68 % of patients had LVH, accords with Foley et al, 2010 who found that LVH was present in 62 % of the study group, implying that the prevalence of LVH is dependent on the degree of renal impairment (Amoako et al., 2017). The current study found no statistically significant link between gender and LVH (p= 0.141), in contrast to the study of Amoako et al. and Paoletti et al., 2016. The link between age and LVH was confirmed in this investigation, with a substantial rise in patient age (P-value 0.001), which was constant with previous findings of (Paoletti et al., 2016).
The drop in haemoglobin concentration begins at levels of creatinine clearance of around 70 ml/min in men and 50 ml/min in women (Hsu, et al., 2002). As a result, the majority of ESRD patients suffer anaemia. In the current study, 88 % of patients have anaemia, defined as Hb 12 mg/dl, with a P-value of 0.512. Many studies have found that a haemoglobin level of 12-13 mg/dl in ESRD patients is related with a better outcome (Regidor, 2006), while a higher haemoglobin level is associated with a higher risk of mortality and arteriovenous access thrombosis (Phrommintikul et al., 2007). The goal haemoglobin level was not reached in the majority of patients due to poor management, blood loss in the dialyzer, and repeated blood sampling, however the basic underlying issue is erythropoietin insufficiency. Sweety et al. (2014) found an association between anaemia and LVH. Anaemic patients have insufficient tissue oxygenation, which is compensated for by increasing blood volume, resulting in an increase in left ventricular mass and assuming an eccentric geometry LVH (Metivier et al., 2000). This finding was consistent with our finding of blood volume in 42 of LVH patients, which was confirmed also by Nasri and Baradaran, 2005. Moreover, their study was confirmed our findings that 40 participants with hypertension had a significant connection between HTN and LVH with P-value of 0.013. Because volume overload is the most common cause of hypertension in ESRD patients (Bellizzi et al., 2006), insufficient clearance of this excess fluid leads to resistant hypertension (Fishbane, et al.,1996). The target blood pressure for adults with CKD is 130/80 mmHg, and for hypertensive individuals without target organ damage is 140/90 mmHg (Chobanian et al., 2003). However, this aim is not met in most patients, resulting in chronic pressure overload of the left ventricle and LVH.
When it comes to volume overload, 15% extracellular volume overload equates to around 2.5 litres of extra fluid in an HD patient (Wabel and colleagues, 2008). As a result, total fluid evacuation during dialysis may not be completed, and normal fluid status may not be achieved even immediately after dialysis. We discovered that 62% of patients were overloaded based on clinical assessment and the presence of lower limb oedema, and that 32 out of 48 patients had LVH (presence of lower limb oedema and shortness of breath does not indicate haemodialysis patients have LVH), but there was no significant relationship between volume overload and LVH P-value 0.238. While Unver et al. found a substantial positive link between hypervolemia and LVH in a study of 97 patients on regular haemodialysis (Unver et al., 2015), and that the presence of lower limb odema and shortness of breath does not mean that haemodialysis patients had LVH. Observational studies have shown that more frequent or longer haemodialysis sessions are associated with proper fluid management and a lower prevalence of LVH (Ly and Chan, 2006). However, another study found that more frequency and longer dialysis did not improve clinical outcome (Slinin et al., 2015).
Significant connection between haemodialysis duration and LVH was found in this study, with P-value of 0.005. Because all patients in this trial have just two- four hrs. sessions per week, they will not achieve their dry weight and will stay hypovolemic even after dialysis, as their Intera-dialytic weight gain will be more than 3 kg between sessions. Foley et al. (2010) investigated whether the incidence of LVH correlates with the length of dialysis in 596 incident haemodialysis patients with no prior history of heart disease. According to the study, 62% of the patients had an elevated LV mass volume index, and 49% of them developed overt LV failure.
Conclusion
We concluded that LVH is common among haemodialysis patients, and that there is a link between age, HTN, and DOD and LVH in this study.
RECOMMENDATION: • Follow up with a nephrologist and a nutritionist on a regular basis to ensure adequate anaemia management during the pre-dialysis phase and after the start of haemodialysis, as well as blood pressure control and prober volume management.
Before starting haemodialysis, all ESRD patients must have an echocardiogram to see if they have LVH and be treated as high-risk patients.
ACKNOWLEDGMENTS: Our best regards and thanks to the staff member of Gezira Hospital for Renal Disease and Surgery , and our appreciate is extend to the patients who participate in this study.
#cardiovascular death#cross-sectional research#Gezira State#Sudan#Left Ventricular Hypertrophy#End Stage Renal Disease#jcrmhs#Clinical Images submissions#Clinical decision making
3 notes
·
View notes
Text
(d) Imposing measures intended to prevent births within the group;
Two thirds of the 57,910 gazans dead are women and children. "Every day, 180 women are giving birth without water, painkillers, anaesthesia for Caesarean sections, electricity for incubators or medical supplies" (Sima Sami Bahous with the UN)*
*This paper was published November 22nd, 2023
And due to these attacks, many women, mainly mothers and pregnant women are suffering. "The almost complete breakdown of the healthcare system, coupled with the lack of food and clean water, means that some 45,000 pregnant women and 68,000 breastfeeding mothers in Gaza are facing the risk of anaemia, bleeding, and death." (Maryam Aldossari with Al Jazeera).
Nearly 1 million women and girls have been displaced, and more than 12,000 women and children have been killed.


Many civilian men have been killed, but alot of them are being detained by the IDF because they are "Hamas" this is not true, family members of these men and boys have pointed them out in IDF footage saying "that's my dad, granfather, brother. They are not with Hamas"
"Last week, images and videos emerged showing Israeli troops detaining dozens of Palestinian men, stripping them of their clothes and forcing them to sit lined up on the ground with their hands tied behind their backs. Israeli media suggested that the men were Palestinian fighters, but provided no evidence." "MEE obtained a list of full names, ages, and professions of 25 people among those arrested by Israel last week. That list, as well as eyewitness accounts, indicate that those detained are academics, journalists, teachers at UN-run schools, school students, blue-collar workers, and employees with the Palestinian Authority."

(from Middle East Eye)
It is clear that Israel is controlling who makes it out of these attacks alive, who won't, and how that will affect the Palestinian population.
8 notes
·
View notes
Text
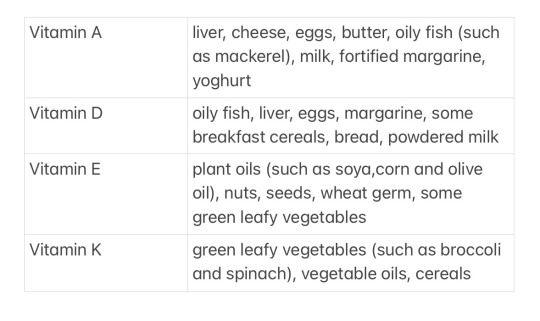
Facts about vitamins A, D, E and K
Vitamins A, D, E and K are fat-soluble.
Vitamin A
Vitamin A, which is actually a group of interrelated substances (retinol, retinal and retinoic acid), can be synthesised in the body from β-carotene, found in dark-green leafy vegetables such as cabbage, sprouts, broccoli and spinach, and in carrots. Cooking the vegetables does not damage the β-carotene molecules and in fact β-carotene is more easily absorbed into the body from cooked carrots.
The speed at which the human eye adapts to seeing in the dark depends on the amount of vitamin A available in the body, known as the vitamin A status. Xerophthalmia or dry-eye is a classic sign of vitamin A deficiency.
Vitamin A is involved in normal growth and bone formation and it plays a part in the production of red blood cells and therefore the prevention of anaemia.
Vitamin D
The main role of vitamin D is to facilitate the uptake of calcium from food, through the lining of the small intestine into the blood. It also controls the deposition of calcium in the bones during growth and maintains adult bone structure.
In fact, the beneficial effect of sunlight, in playing a part in vitamin D synthesis, has to be balanced with the detrimental effect, its role in causing skin cancers. It appears that an exposure to sunlight of about 30 minutes per day (avoiding the part of the day when sunlight is strongest) is an appropriate balance between the harmful and beneficial effects.
Vitamin E
Some chemical reactions in the body produce harmful substances called free radicals that contain single electrons and become involved in chain reactions in the cells, which can be damaging to the body. Antioxidants like vitamins A and E neutralise the harmful substances and prevent further damage.
Vitamin K
Vitamin K is widely distributed in the diet and it is absorbed from the small intestine with the assistance of bile acids.
The main role of vitamin K is in blood clotting. This process requires the presence of a number of different chemicals, called clotting factors, in the blood. A number of these (including prothrombin and Factors VII, IX and X) require vitamin K in their synthesis.
#stay healthy#nutrtion#nutrtion facts#healthy#healthy lifestyle#healthy life tips#stayhealthyinside#medicine inside#studyblr
9 notes
·
View notes
Photo
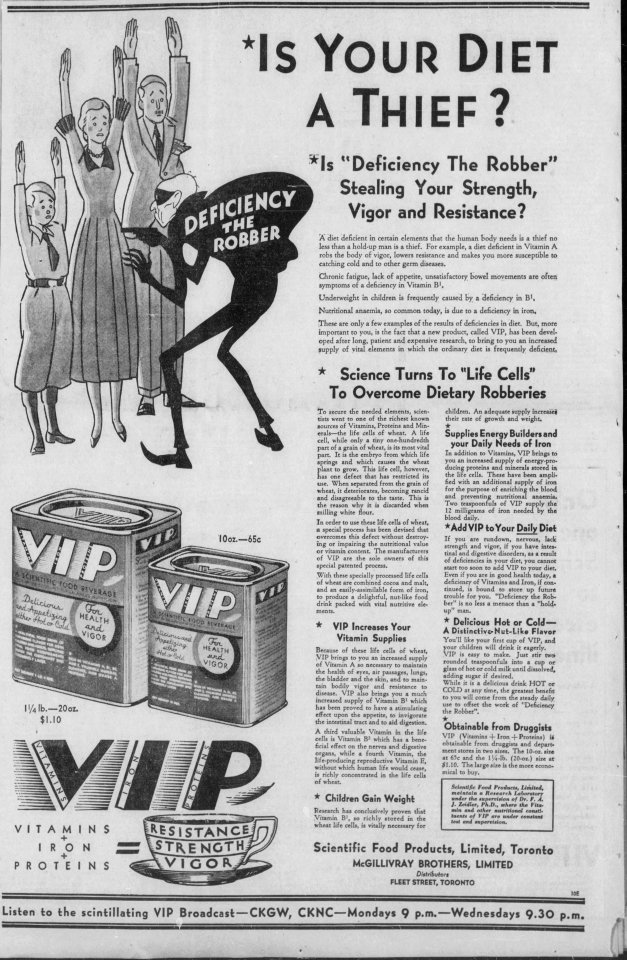
“Is Your Diet A Thief?” Kingston Whig-Standard. February 15, 1933. Page 10, --- Is Deficiency The Robber Stealing Your Strength Vigor and Resistance? --- A diet deficient in certain elements that the human body needs is a thief no less than a hold-up man is a thief For example a diet deficient in Vitamin A robs the body of vigor lowers resistance and makes you more susceptible to catching cold and to other germ diseases.
Chronic fatigue, lack of appetite, unsatisfactory bowel movements, are often symptoms of a deficiency in Vitamin B1.
Underweight in children is frequently caused by a deficiency in B1.
Nutritional anaemia, so common today, is due to a deficiency in iron.
These are only a few examples of the results of deficiencies in diet. But more important to you is the fact that a new product called VIP has been developed after long patient and expensive research to bring to you an increased supply of vital elements in which the ordinary diet is frequently deficient.
Science Turns To "Life Cells” To Overcome Dietary Robberies To secure the needed elements scientists went to one of the richest known source of Vitamins, Proteins, and Minerals— the life cells of wheat. A life cell, while only a tiny one-hundredth part of a grain of wheat, is its most vital part. It is the embryo from which life springs and which causes the wheat plant to grow. This life cell however has one defect that has restricted its use. When separated from the grain of wheat, it deteriorates, becoming rancid and disagreeable to the taste. This is the reason why it is discarded when milling white flour.
In order to use these life cells of wheat, a special process has been devised that overcomes this defect without destroying or impairing the nutritional value or vitamin content. The manufacturers of VIP are the sole owners of this special patented process.
With these specially processed life cells of wheat are combined cocoa and malt, and an easily-assimilable form of iron, to produce a delightful nut-like food drink packed with vital nutritive elements.
VIP Increases Your Vitamin Supplies Because of these life cells of wheat, VIP brings to you an increased supply of Vitamin A so necessary to maintain the health of eyes, air passages, lungs, the bladder, and the skin and to maintain bodily vigor and resistance to disease. VIP also brings you a much increased supply of Vitamin B1 which has been proved to have a stimulating effect upon the appetite to invigorate the intestinal tract and to aid digestion.
A third valuable Vitamin in the life cells is Vitamin B which has a beneficial effect on the nerves and digestive organs, while a fourth Vitamin, the life-producing reproductive Vitamin E, without which human life would cease, is richly concentrated in the life cells of wheat.
Children Gain Weight Research has conclusively proven that Vitamin B1 so richly stored in the wheat life cells, is vitally necessary for children. An adequate supply increase! their rate of growth and weight.
Supplies Energy Builders and your Daily Needs of Iron In addition to Vitamins VIP brings to you an increased supply of energy-pro-during proteins and minerals stored in the life cells. These have bean amplified with an additional supply of iron for the purpose of enriching the blood and preventing nutritional anaemia. Two teaspoonfuls and preventing nutrition teaspoonfuls of VIP supply 12 milligrams of iron needed by the blood daily.
Add VIP to Your Dally Diet If you are rundown, nervous, lack of strength and vigor if you have intestinal and digestive disorders as a result of deficiencies in your diet, you cannot start too soon to add VIP to your diet. Even if you are in good health today a deficiency of Vitamins and Iron if continued is bound to store up future trouble for you "Deficiency the Robber” is no less a menace than a "hold up” man.
Delicious Hot or Cold— A Distinctive-Nut-Like Flavor You'll like your first cup of VIP and your children will drink it eagerly VIP is easy to make Just stir two rounded teaspoonfuls into a glass of hot or cold milk until adding sugar if desired.
While it is a delirious drink HOT or COLD at any time the greatest benefit to you will come from die steady daily use to offset the work of "Deficiency the Robber.”
Obtainable from Druggists VIP (Vitamins + Iron + Proteins) is obtainable from druggists and department stores in two sizes...
Scientific Feed Products Limited Toronto McGILLIVRAY BROTHERS LIMITED Distributors FLEET STREET TORONTO
#toronto#health drink#vitamin drink#crime and society#crime wave#history of crime and punishment in canada#patent medicine#wheat germ#health cure#iron deficient anemia#iron deficiency#vitamin deficiency#vintage ads#vintage advertising
5 notes
·
View notes
Quote
The predominantly cereal based ‘vegetarian’ diet that is currently being imposed on India, is contributory to the crisis of non-communicable disease in the country. 8.7% (50 million) Indians in the age group 20 – 70 year age live with Type 2 diabetes, an attributable risk factor for several complications affecting the eyes, heart, kidney, nervous system and circulatory system. Cutting down on sugars, reducing traditional cereals, and increasing the consumption of animal source foods has the ability to drastically prevent or reduce the large-scale prevalence of Type 2 diabetes and its complications. However, in India, politics, culture, religion, caste and economics around cereals, vegetables, fruits, pulses, oils, eggs, meat etc., constantly dictate what people eat. Even a suspicion of transporting beef or a mention of its nutritional/cultural/religious value can trigger a series of events ranging from abuse, arrest, harassment and lynching. This has been used with a great degree of expertise by politicians seeking to fragment India along caste and religious lines. Anaemia in children less than 5 years is 60 per cent in India. This, with chronic hunger and other nutritional deficiencies that invariably co-exist, can lead to less than expected performance of the child in school.
Dr Sylvia Karpagam, ‘A critical look at Indian healthcare‘, Aura
#Aura#Sylvia Karpagam#India#cereals#vegetarian diet#food imposition#non-communicable diseases#Type 2 diabetes#politics#culture#religion#casteism#economics#abuse#arrest#harassment#lynching#social fragmentation#Pediatric Anemia#chronic hunger#nutritional deficiencies#academic performance
5 notes
·
View notes
Text
My mum has done more than 100 donations and moved on to doing plasma at the age of 66!
I have done 25 blood donations. Started at 17, but piercings/tattoos, international travel, and bouts of anaemia have prevented me from donating as regularly as I could.
It really is not an unpleasant experience, so if you qualify to give, please do. We have not cracked the code on synthesising blood yet.
36K notes
·
View notes
Text
The Benefits of a Genetic Health Check: How It Can Transform Your Health Journey

In today's era of precision medicine and personalized care, understanding your genetic makeup has become a powerful tool in managing and optimizing health. A Genetic Health Check in Kerala offers individuals the opportunity to explore their DNA and uncover insights that could transform their health journey. From identifying hereditary risks to tailoring lifestyle and medical decisions, genetic testing holds immense promise.
Kerala, known for its advanced healthcare systems and skilled professionals, has emerged as a hub for genetic health services. Let’s delve into the benefits of a genetic health check and why considering this option in Kerala could be a life-changing decision.
What Is a Genetic Health Check?
A genetic health check is a diagnostic tool that analyzes an individual’s DNA to identify variations and mutations in their genes. These variations can reveal susceptibility to specific health conditions, inherited disorders, and even traits that influence lifestyle factors like diet and fitness.
By interpreting the genetic code, this process offers valuable insights that can help individuals and healthcare providers make informed decisions about preventive measures, treatments, and overall wellness strategies.
The Growing Importance of Genetic Health Checks
Personalized Health Insights Unlike traditional diagnostic methods, genetic testing focuses on the unique biological blueprint of each individual. It allows for a more personalized approach to healthcare, ensuring treatments and preventive strategies are tailored to your specific needs.
Prevention Over Cure A Genetic Health Check in Kerala can help you identify potential health risks before symptoms appear. Early detection of predispositions to conditions like cancer, heart disease, or diabetes can guide lifestyle changes and regular monitoring to prevent complications.
Family Health Management Genetics play a crucial role in inherited conditions. Understanding your genetic risks can help in making informed decisions about family planning and managing health risks for future generations.
Diet and Fitness Optimization Genetic health checks often include insights into how your body metabolises nutrients or responds to certain types of exercise. This information can be used to design a personalised diet and fitness plan for optimal results.
Mental Health Your genetic makeup can also influence your susceptibility to mental health conditions like depression or anxiety. Knowing these risks can prompt proactive mental health management and early interventions.
Why Choose Kerala for Genetic Health Checks?
Kerala is renowned for its high-quality healthcare facilities and skilled medical professionals. Here’s why opting for a Genetic Health Check in Kerala is a wise choice:
Advanced Technology: Many healthcare centres in Kerala have state-of-the-art genetic testing labs, ensuring accurate and reliable results.
Affordable Services: Compared to other regions, Kerala offers cost-effective healthcare without compromising quality.
Expert Guidance: The state boasts a pool of genetic counsellors and specialists who can help interpret the results and guide you in making informed decisions.
Holistic Care Environment: Kerala’s healthcare philosophy often integrates modern medicine with holistic practices, ensuring a comprehensive approach to health management.
What Can a Genetic Health Check Tell You?
Here are some of the key insights you can gain from a genetic health check:
Disease Risk Assessment
Identify the likelihood of developing conditions such as cardiovascular diseases, cancers, or autoimmune disorders.
Learn about hereditary conditions that could affect your health or that of your children.
Carrier Screening
Determine if you are a carrier for genetic disorders like cystic fibrosis or sickle cell anaemia.
Use this information for family planning and early intervention.
Pharmacogenomics
Understand how your body reacts to specific medications.
Tailor treatments are based on your genetic response to drugs.
Lifestyle Recommendations
Discover genetic factors influencing weight management, sleep patterns, and stress response.
Use this knowledge to adapt your habits for better health.
Steps to Take After Your Genetic Health Check
After receiving the results of your Genetic Health Check in Kerala, it’s important to act on the insights gained.
Consult a Genetic Counselor A counsellor can help you understand complex genetic information and its implications for your health.
Collaborate with Healthcare Providers Share your genetic report with your doctor to integrate the findings into your health management plan.
Adopt Preventive Measures If your results indicate risks for certain conditions, make necessary lifestyle changes such as modifying your diet, increasing physical activity, or scheduling regular screenings.
Involve Your Family Share relevant findings with family members, especially if hereditary risks are involved. This can help them take proactive steps to manage their health.
Ethical Considerations and Privacy
While genetic health checks provide valuable insights, it’s essential to ensure that your data remains private and secure. Opt for reputable services in Kerala that follow strict confidentiality protocols. Additionally, genetic testing should always be a voluntary decision, conducted with informed consent.
Final Thoughts
A Genetic Health Check in Kerala is more than just a diagnostic tool; it’s a window into your unique biological identity. By understanding your genetic blueprint, you can take control of your health, reduce risks, and lead a more informed and empowered life.
With Kerala’s advanced healthcare infrastructure and skilled professionals, undergoing a genetic health check here is an excellent investment in your well-being. Embrace the future of personalized medicine and embark on a transformative health journey today.
#Genetic Health Check in Kerala#Genetic Health Check in India#Genetic DNA Testing Kits India#Govt-Approved DNA Testing Service India#Genetic DNA Testing Kits in Kerala#Govt-Approved DNA Testing Service Kerala#DNA Testing Centres in India#DNA Testing Service India#Buy DNA Testing Kits Online#Home DNA Testing Kits#India#Kerala#Kochi
0 notes
Text
Treatment for White Spot on Skin: A Homeopathic Remedy
Vitiligo is a persistent skin condition that results in the loss of pigmentation on the skin and causes white patches and patches to appear on different parts of the body, as well as throughout the body. There are currently a variety of medical treatments that are available to slow the process and trigger redistribution. These treatments, whether alone or together, have been proven to produce varying levels of pigmentation. Most are reliable and safe. All vitiligo disease treatment are limited, with many having severe side effects and few being completely safe. These include homeopathic treatment for white spots.
How can we stop vitiligo from getting worse?
Vitiligo can manifest at any point in the body, at any age. Preventing its spread is a primary problem for those suffering. But, there are a variety of treatments that can assist in managing and limiting its progression. One treatment is a homeopathic treatment for vitiligo, which can aid in stopping the progression of vitiligo.
Early intervention: Intervention before the age of 18: The earlier you begin treatment for symptoms of vitiligo, the less likely to get worse. The homeopathic vitiligo treatment naturally can aid in reducing the progress of vitiligo as well as the spreading of pigmentation. If you notice the first signs of the disease, it is recommended to seek medical attention to begin the correct treatment.
Topical treatments: A lot of creams are available, especially in the beginning stages. They can help to decrease inflammation and could stop or slow the progression of pigmentation. However, they can only provide temporary relief, which could also have adverse consequences. If you are considering using creams, you should pick a herbal one to ensure that you don't suffer any adverse consequences.
Treatments: These are offered to slow the growth of Vitiligo's rapid spread. By taking them regularly, you can stop the spots from forming, and when they stop, these white spots become more.
Supplements and diet: A few studies suggest that deficiency in certain minerals and vitamins such as B12, vitamin D and folic acid might be a major factor in the development of vitiligo. Healthy food and a balanced diet, as well as maybe taking a homeopathic vitiligo medication may help in managing the condition.
Stress: stress has been recognised as a potential trigger for the development or worsening of Vitiligo. Engaging in activities that reduce stress, such as exercise, meditation, yoga, and consultation with a doctor, may aid in controlling flares or even slow down the development of problems with white spots.
Skin protection: Exposure to sunlight may increase the intensity of normal darkened areas of skin that suffer from vitiligo, such as the hands, elbows, or vitiligo on lips. This can cause vitiligo, face, etc. Applying sunscreen regularly will help protect your skin and slow the occurrence of depigmentation that is caused by UV damage.
Preventing :the triggered conditions or physical injuries like burns, cuts, or abrasions can cause vitiligo. It is crucial to be cautious and avoid causing injury to the skin in order to stop new patches from developing.
How Is Vitiligo Dangerous?
The presence of white spots is not physically hazardous since it doesn't cause any harm or pain to organs internally. But, if you do not receive timely vitiligo disease treatment, it increases the chance that in the event of not being treated, this serious condition could cause an extended period of pain. This condition can be correlated with health issues and complications. The risks are as follows.
Autoimmune diseases: Vitiligo is often linked to autoimmune conditions, where the immune system misinterprets your body's cells. People suffering from vitiligo have a higher risk of developing autoimmune conditions like thyroid diseases (Hashimoto's thyroiditis), pernicious anaemia, type 1 diabetes and Lupus. The link between these disorders is that people who are diagnosed with vitiligo need to be closely monitored for the emergence of other autoimmune conditions.
Psychosocial impacts: The effects of vitiligo on the psychological and emotional consequences may be significant, particularly for those who have spots on their hands or faces. It can cause anxiety about self-esteem, social isolation, depression, and anxiety. Many people find that the stigma of the condition can be among the most difficult issues to deal with, particularly in societies where the focus is given to appearance. The best treatment for vitiligo will help you avoid the problem.
Risk of skin cancer: While the condition doesn't significantly increase the likelihood of developing skin cancer, the lack of melanin in the affected areas implies that the affected areas are more prone to UV rays. Because melanin is an inherent barrier to protect against sun-induced damage, those who suffer from vitiligo should be especially cautious when it comes to exposure to sun. This dangerous disease must be managed through the careful application of sunscreens and natural homeopathic vitiligo treatment naturally to shield the areas of depigmentation from possible damage, which includes skin cancer.
Eye and Hearing Problems: Certain people suffering from vitiligo might suffer from eye issues like inflammation in the eyes (iritis) as well as hearing issues. Melanocytes, cells that produce pigment, are found not just on the skin but also in the eyes and ear. Thus, vitiligo can cause damage to these organs in very rare instances.
Koebner phenomenon: This happens when new patches of vitiligo form on the site of a skin wound, such as burns, cuts, or pressure exerted by tight clothing. It's particularly dangerous for those who are not aware of the dangers and are engaged in activities that can accidentally cause skin damage and increase the risk of pigmentation. If you suffer from this condition, it is advised to seek immediate treatment for white spot on skin to manage the condition and stop vitiligo from advancing.
Homeopathic Vitiligo Hospital to treat white patches
Vitiligo is a persistent condition that, though not physically hazardous on its own, can cause numerous complications. The long-term use of medication can cause dangers, and the disease could be linked to other auto-immune illnesses. The prevention of this spread demands the best treatment for vitiligo. This includes changes in lifestyle, as well as psychological aid to help patients overcome the physical and psychological challenges that the disease can bring. Making the right precautions and remaining vigilant will help reduce the effects of vitiligo as well as enhance your overall living quality.
#treatment for white spot on skin#vitiligo disease treatment#Vitiligo Medication#best treatment for vitiligo
0 notes
Text
Best Gynaecology Hospital in Hyderabad
PACE Hospitals is one of the Best Gynaecology Hospital in Hyderabad, India, providing comprehensive patient-centric treatment for all gynaecological diseases and disorders. The team of experienced and skilled gynaecologist, obstetrician and gynaecology surgeons have wide expertise in managing all types of common and critical women's health conditions, including:
Polycystic Ovary Syndrome (PCOS), Polycystic Ovarian Disease (PCOD), Pelvic Inflammatory Disease (PID)
Vaginosis, Candidiasis, Vulvovaginitis, HPV
Menstrual Disorders, Menopause-related Issues
Endometriosis, Uterine Fibroids, Ovarian Cysts,
Breast Lump, Breast Cyst
Pelvic Organ Prolapse, Pelvic Pain, Preeclampsia
Anaemia in Pregnancy, Ectopic pregnancy
Placenta Previa, Placenta Accreta
Sexually transmitted infections (STI)
Advanced Centre for Gynecological Disease Treatment in Hyderabad, Telangana
The Gynaecology Department at PACE Hospitals is one of the Top gynaecology doctors in Hyderabad. The department is led by a team of experienced gynaecology doctors, obstetricians and gynaecology surgeons, who are highly skilled and have expertise in addressing all types of women's health issues, from regular gynaecological examinations to minimally invasive surgical procedures for complex gynaecological conditions, ensuring the highest standards of gynaecological care. The Gynaecological treatment care at PACE Hospitals is aimed at providing comprehensive, personalized, evidence-based treatments for conditions such as menstrual disorders, fertility issues, pregnancy care, and complex surgeries with a focus on patients receiving the highest quality care with a comfortable, compassionate and supportive environment.
The Department of Gynaecology is equipped with state-of-the-art and cutting-edge facilities that offer a wide range of gynaecological treatments, ranging from preventative care to specialized treatments. The latest and advanced diagnostic facilities enable our gynaecology specialists to perform diagnostic or minimally invasive procedures for complex disorders with utmost precision, reducing recovery times, minimal scarring, and less post-operative pain.
Team of the multi-speciality hospitals in Hyderabad, India, specializes in managing all kinds of Gynaecological Diseases and Treatment. They are skilled in examining and treating a wide array of regular and critical women's health conditions, including menstrual irregularities, hormonal imbalance, polycystic ovary syndrome (PCOS), high-risk pregnancies, menopausal complications, uterine fibroids, ovarian cysts, endometriosis, cervical abnormalities, infertility, breast-related issues and more. The specialized team of obstetrician gynecologist and gynaecology surgeons are highly skilled and apt with the latest and advanced treatment modalities, and minimally invasive procedures to cater for the utmost treatment care with precision, minimal complications and a high success rate.
What we treat?
We have expertise in the treatment and management of a wide array of gynaecological diseases and disorders affecting women's reproductive health conditions. From everyday women's health conditions like menstrual disorders, Polycystic Ovary Syndrome (PCOS), pelvic pain, Breast Pain, Nipple Discharge, Breast lumps and gynaecological infections to complex and critical conditions like uterine fibroids, ovarian cysts, endometriosis, ectopic pregnancy, Uterine Prolapse, Ovarian Hyperstimulation Syndrome (OHSS), Breast Cyst, our team of gynaecologist, obstetrician and gynaecology surgeons is committed to providing the compassionate, patient-centric comprehensive solutions for women's reproductive health.
Gynaecological Diagnostic Test & Procedures
We provide comprehensive and cutting-edge diagnostic and procedural treatment tailored to women's healthcare needs. Our advanced and latest screening approach and diagnostic procedures like pelvic ultrasound, colposcopy, hysteroscopy and endometrial biopsy examine critical conditions like uterine fibroids, ovarian cysts, endometriosis and reproductive health disorders, resulting in the early detection and precise evaluation, enabling our gynaecologist and obstetrician to make an informed decision to proceed with the appropriate treatment approach.
1. Pelvic Examination: Pelvic examination is the process performed to collect information about the pelvic area, which includes vulva, vagina, cervix, uterus, ovaries and fallopian tubes; it is done to look for signs of diseases or infections. Gynaecologists commonly perform this test to detect sexually transmitted infections (STI’s), yeast infections, and bacterial vaginosis. It includes visual external examination, manual examination, speculum exam, pap test and rectal exam.
2. Blood Tests: Women can undergo various blood tests that provide valuable insights into their health. These tests measure specific hormones in a woman's body associated with pregnancy, such as human chorionic gonadotropin (HCG). Blood tests can identify the pregnancy and measure hormone levels (FSH, LH, oestrogen, progesterone, TSH, prolactin), providing valuable information about a woman's overall reproductive health and well-being. These tests can also diagnose specific types of sexually transmitted diseases (chlamydia, HIV, herpes, gonorrhoea, syphilis), often combined with urine tests to confirm, which can be critical in identifying and treating these infections.
3. Urine Examinations: A urinalysis is the most common diagnostic test conducted to examine the urine to detect and measure various compounds through physical, chemical, and microscopic tests and to assess many different aspects of health with a urine sample. It is performed to check protein and sugars.it is performed to confirm kidney problems, diabetes and preeclampsia, urinary tract infections and liver problems.
4. Pelvic Laparoscopy: Pelvic laparoscopy a minor invasive procedure is performed to examine and treat the abnormalities of the uterus, ovaries, cervix, and fallopian tubes in the pelvic area. Conditions treated include endometriosis, chronic pelvic pain, pelvic inflammatory disease and cancers. It includes inserting the instrument into the abdomen by making small incisions. That instrument is called a laparoscope, which contains a thin device with an attached camera and light to visualize the organs.
5. Pelvic Ultrasound: A pelvic ultrasound is a diagnostic test that utilizes sound waves to make images of the organs inside the pelvis that are used to examine the organs and structures within the pelvis, such as the uterus, cervix, fallopian tubes, vagina and ovaries of the female. It allows the visuals of the pelvic organs. Ultrasound uses a transducer which places on the pelvic skin using the conductive gel.
6. Transvaginal Ultrasound: An ultrasound test identifies abnormalities using high-frequency sound waves to create (provide) pictures of internal organs. A transvaginal ultrasound, or endovaginal ultrasound, is used to examine the pelvis organs such as the uterus, ovaries, fallopian tubes, cervix and vagina.
It differs from a regular pelvic ultrasound where it involves the insertion of an ultrasound probe that measures approximately 2–3 inches into the vaginal canal. With this probe, the internal organs can be examined in detail, allowing healthcare professionals to diagnose and treat various medical conditions.
7. Pap Test: It is also called a pap smear test, a screening procedure to assess cervical cancer. It identifies the presence of precancerous or cancerous cells. It can determine the changes in the cells on the opening of the uterus, called the cervix. This test is usually performed by inserting a metal or plastic tool named a speculum into the vagina to open and widen the vagina walls. Gynaecologist uses a swab to take cell samples from the cervix and send it for laboratory evaluation.
8. Human papillomavirus (HPV) Test: The procedures involved in HPV and PAP tests share some similarities. HPV, capable of causing alterations in cervical cells, can be detected through an HPV test. This test can be conducted solely or in combination with a pap test in an approach known as co-testing.
10. Hysteroscopy: Hysteroscopy is a diagnostic procedure used to inspect the inside of the uterus (womb). This procedure involves using a hysteroscope, a thin instrument with a camera and light located at the end. It can be passed into the patient's uterus through the vagina and cervix. The camera can send images (inside the uterus) to the monitor, which is observed by the gynaecologist.
In conclusion, PACE Hospitals stands out as one of the best choices for gynecological care in Hyderabad. With a team of experienced and compassionate specialists, state-of-the-art facilities, and a commitment to patient-centered care, PACE Hospitals ensures that every woman receives the highest standard of treatment and support. Whether it's routine check-ups, high-risk pregnancies, or complex gynecological surgeries, Super specialty hospital in Hyderabad provides expert care tailored to each patient's unique needs. For those seeking trusted and comprehensive gynecological services.
0 notes
Text




Of all nutrients oxygen is the most essential.
💫Oxygen has more fundamental nutritional roles than vitamins and minerals or any other nutrient.
💫Oxygen is considered a Yang force; without it, fuel in the body cannot be burnt for energy and heat.
💫Anaemia is sometimes a result of insufficient oxygen.
💫Lacking in oxygen, one feels heavy, depressed and without vitality.
💫Oxygen is also needed for vitamin C utilisation, to slow down collagen breakdown and to prevent premature aging.
💫Once sufficient oxygen is in the body, one feels charged with life and is usually no longer attracted to intoxicants.
💫Oxygen is a purifier, helps eliminate waste in the body.
💫Oxygen destroys germs and viruses and resolves pathogenic moisture.
5 notes
·
View notes