#suspensory ligaments of the lens
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs




Fun Fact
Tumblr.com is the 103rd most visited website in the world.
Text

The Research Notebooks of S. Sunkavally, page 337.
#aqueous humour#flowing stream#intraocular pressure#suspensory ligaments of the lens#pancreatic hormones#glucagon#leucine#control of transcription#omnivore#sister chromatid exchanges#hypoglycemia#epinephrine secretion#vagus nerve#acetylcholine#parathyroid hormone#osteoporosis#blood calcium level#blood magnesium level#satyendra sunkavally#theoretical biology#manuscript
0 notes
Text
Chapter 5
(part 1)
p. 41: Not a real note but R. K. Narayan is my friend’s name and I’m aware it’s not exactly uncommon but still very unsettling to run into when not expecting it
p. 41: “Tears her to pisces”, not “pieces”. I checked and it’s in the index, so on some level an intentional typo, but whose?
p. 42: I found 4-5 different translations of the Latin, all a little bit more literal than the one given in the text but overall not too different. Here’s an example:
Spurned, she hides in the woods and covers her shamed face with leaves. From that time on she lives alone in caves. But still love grips her and grows stronger with the pain of rejection. Sleepless cares waste away her poor body. Leanness attacks her skin and the lifeblood of her body evaporates into the air. Only her bones and her voice remain. Her voice stays with us; they say that her bones became transformed into the shape of a stone.
From then on she stays hidden in the woods and is no longer seen on any mountain. All hear her, though: the sound that lives in her.
(Translation from Rachel Carter via the Classics Library)
p. 42: The Spanish translation is correct I think. “émula” generally means emulate or follow, but the online translations consistently say “rival” so it’s probably just an additional definition I’m not aware of.
p. 43: Zonule of Zinn is the ring of fibers around the lens of the eye that hold it in place and flatten it when focusing on something far away.

“Suspensory ligaments” is a much clearer name but does not have the benefit of sounding like a character in Wizard of Oz.
p. 44: talaria - winged sandals, like Hermes
#weasel reads house of leaves#the navidson record#medical for ts#flashbacks to sheep eye dissection in high school#how I became a vegetarian#well actually it was the pigs that did it but anyways
0 notes
Text
your mum so lens looking at a distant object she is long and thin. your dad so suspensory ligaments looking at close object he is relaxed
4 notes
·
View notes
Photo

Dry eye is a tear secretion eye disease with dry eyes as the main symptom. It is accompanied by a variety of symptoms. I have almost all the symptoms of dry eye.
I often feel itchy or tingling eyes, foreign body sensation (as if there are always eyelashes falling inside). Sometimes I use the computer a lot during the day, and in the evening I will have symptoms of sore eyes and blurred vision. I used to walk in a venue under ordinary light. There will be no discomfort, but after the occurrence of dry eye, there will be symptoms of photophobia and inability to adapt to strong light. The eyeballs are congested and there are many secretions. Colleagues always think that I stayed up all night and did not sleep well. In fact, it is also one of the symptoms of dry eye.
I have these bad habits:
1. The computer has a slightly brighter light, or use a large-screen display to assist the office (for example, see the details of MRI, CT);
2. Sitting in front of the computer for a long time, working without stopping, and not giving eyes time to rest;
3. Sometimes I wear contact lenses all day, and I wash my hands all the way around at work and take off the glasses directly without paying attention to hygiene;
4. Sometimes you look at the screen with your naked eyes without wearing glasses, and squint to look at the screen;
5. The angle of the computer or monitor is tilted, and sometimes the eyes have to hang down or look up at the screen;
6. Sometimes the room is dim and the computer screen is brighter, I still stick to work;
7. Watching a tablet or mobile phone while walking, and sometimes the screen will be automatically brightened;
8. Just grab the eye drops and eye care solution and use it, but didn't choose the right product according to your needs.
After suffering from dry eye and being tortured repeatedly for half a year, I started to cooperate with the treatment and correct my eye habits at the same time.
1. Be sure to give your eyes plenty of rest time: After working for a period of time, you must close your eyes, look into the distance or gently rub your eyes. These actions can rest your lens, lens suspensory ligament, and ciliary body.
2. Adjust the light intensity of the computer, monitor, and tablet. It is best not to be too different from the surrounding environment. Let your eyes work in a comfortable light intensity environment. You can use CareUEyes (https://care-eyes.com) This eye protection software adjusts the brightness of the computer
3. Adjust the angle of the computer and monitor so that your line of sight is perpendicular to the screen, avoid upward or downward rotation of the eyeball, and reduce the load on the superior and inferior rectus muscles;
4. Avoid working in front of a screen with strong light in a dim room;
5. Operations that touch the eyeballs, such as removing contact lenses and eyelashes that have entered the eyes by mistake, require hands (especially nails) to be cleaned to avoid conjunctival infection;
6. For people with dry eyes and astringent eyes, you can drink water or use artificial tears to relieve symptoms;
7. Some eye drops on the market contain antibiotics, specific drugs and other additives. They are for some infections, glaucoma and immune-related eye diseases. You must choose your own eye drops. Do not mix eye drops with others, let alone choose randomly;
8. When going out to play, especially in the sunny outdoors, you can wear sunglasses to protect your eyes and avoid the irritation of bright light.
To add, more and more myopia patients are now wearing contact lenses. However, the wearing of contact lenses requires special care, otherwise it will cause eye infections and bring undesirable consequences.
1 note
·
View note
Text
Are you familiar with Iridodonesis?
Iridodonesis is a condition in which the iris (coloured part of the eye) vibrates during eye movements. Upon moving the eye rapidly, the iris can appear to ‘dance’, or ‘tremble’ (tremulousness). This occurs when the lens becomes partially detached (lens subluxation) from its suspensory ligaments.
The primary cause of iridodonesis is the subluxation of the lens. This may occur as a result of glaucoma, cataract formation, post-surgical complications, or trauma to the eye. The subluxation of the lens rarely occurs naturally; however, there are reported cases of iridodonesis occurring due to genetic mutations that affect the strength of connective tissues.
Definition by News Medical Life Sciences
Video OP doctormedicine_
#medical video#medical school#medical#medicine#ocular#eyes#hazel eyes#nurses#surgical nurse#nurse#nursestudlife#nursestudent#medstudlife#medstudent#medsurg#medschool#optometrist#optometry#optometrists#weird#this is weird#so weird
154 notes
·
View notes
Text
How to working of eye in the see of a object in simple distance, distance object and near obect of the eye by the working of eye
How to see a object our eye
Working of eye
Eye is work for see a object.
WhenThe light rays reflected from an object it pass through the conjunctiva, then cornea and pupil.
In this pupil before falling on the biconvex lens.
In this time pupil is enlarge or diminished.
Beacause size of the pupil determine the amount of light that will enter into the eye ball.
Pupil is enlarge when intensity of light is low.
Pupil is diminished when the intensity of light is high. Nest work working of eye.
After reflected rays from pupil then light rays are focused on the retina by the biconvex lence.
In this time sharp inverted image is formed on the retina.
This inverted retinal image is carried by the optic norve to the brain where it is being interpreted.
After that eye can see the image by changing the curvature of lens.it is called power of accommodation of eye.
Working of eye to a distance object and near object
When distance object are viewed, in this condition the lence is kept flattened by the suspensory ligaments.
Then inverted image is formed on the retina.
When near object are viewed, the lens becomes more complex by the activities of the ciliary muscles, the curvature of the lens is reduced, pupil contracts.
Then inverted image of the object is formed on the retina.
Thanks for sharing your valuable time. If are you gain knowledge in this article, please comment bellow the post and share article your friends and subscribe our post. Thanks for spending your time.....
2 notes
·
View notes
Text
AQA BIOLOGY PAPER 2 - KEY POINTS FOR GCSE 2018
(ashjhfsdhgfkgjjs sorry this is so late! i will reblog it in the morning! also, i do not own the photos used for the cycles)
Homeostasis and the reflex arc
Homeostasis: maintaining/controlling your internal environment (e.g. body temperature, blood glucose levels, glucose content)
Stimulus is detected by receptor cells, information is sent as an electrical impulse, impulse travels to brain and spinal cord, brain coordinates a response, impulse goes to motor neurones, which sends information to the effector (gland or muscle)
In reflexes, the impulse bypasses the conscious part of the brain (involves chemical diffusion between the synapses of two neurones) so they are rapid and automatic
The brain
Cerebral cortex: consciousness, intelligence, memory and language
Hypothalamus: involved in controlling body temperature
Pituitary gland: produces hormones and chemicals
Medulla: concerned with unconscious activities (heartbeat, breathing etc)
Cerebellum: controls muscles activity and balance
Brain is protected by skull and encased in meninges
Can be studied by matching changes in memory/behaviour to areas of trauma, electrical stimulation, or MRI scans
The eye
Made up of cornea (lets light in), sclera (protects eye, outer layer), retina (light sensitive cells send impulses via optic nerve), suspensory ligaments/ciliary muscles (holds lens), lens (fine-tunes light), iris (controls pupil size), and pupil (changes light entry)
Bright light causes pupils to constrict – circular muscles contract, radial muscles relax
Dim light causes pupils to dilate – circular muscles relax, radial muscles contract
Near objects are refracted strong as the lens thickens – ciliary muscles contract, suspensory ligaments loosen
Far objects are refracted only slightly as lens thins – ciliary muscles loosen, suspensory ligaments contract
Hormones
Hormones are chemical messengers released by a gland in response to an internal change and carried in the blood
Negative feedback is doing the opposite of something to return it to normal
Example: thyroxine (thyroid gland in the throat) – uses iodine in your diet to control metabolic changes (remains stable in adulthood)
Adrenaline is not caused by negative feedback – triggers ‘fight or flight’ response (heart rate increase, glycogen converted to glucose, pupils dilate, mental awareness increase, blood diverted from digestive system to big muscles)
Insulin is released when blood glucose is high, glucose taken in by cells or converted to glycogen in the liver
Glucagon is released if too low, and glycogen is broken down into fats/amino acids, fat broken down for energy
Diabetes symptoms include thirst, glucose in urine, fatigue, weight loss, and overactive bladder
Treated by injecting insulin, pancreas/pancreatic cells implant, embryonic stem cells, diet, exercise and weight loss
Male reproductive hormone is testosterone – causes puberty (growth spurt, pubic and facial hair, larynx grows, testes grow/become active, shoulders and chest broaden)
Female puberty is caused by oestrogen (growth spurt, pubic hair, breast enlargement, external genitals grow, fat deposits on hips/buttocks/thighs, brain changes and matures, menstruation begins)
The menstrual cycle: egg matures, uterus lining thickens to prepare for pregnancy, at 14 ays a mature egg is released (ovulation), if egg is not fertilise by day 28, the uterus lining sheds along with egg
Controlled by 4 hormones – FSH (matures eggs in follicle, stimulates ovaries to create oestrogen), oestrogen (secreted with rising FSH levels, stimulates build of uterus lining, high levels inhibit FSH and stimulate LH), LH (stimulates release of egg, drops after ovulation), and progesterone (inhibits FSH and LH, secreted by empty egg follicle, maintains uterus lining/pregnancy)
Fertility
In IVF, mother is given LH and FSH to stimulate oestrogen, eggs are collected and fertilised with father’s sperm in the lab, fertilised eggs are kept in a special solution until they become embryos, and are then implanted back into the uterus
Contraception is a method of preventing the sperm cells and egg cell meeting fertilised
Includes hormonal methods (pill, implants, injections, patches), chemical methods (spermicides), barrier methods (condoms, diaphragms, IUD), and surgical methods (vasectomy, cutting oviducts)
Thermoregulation
Too cold = vasoconstriction (shunt vessel opens), blood vessels keep blood way from skin surface, less heat loss, muscles contract to raise hair to trap heat, shivering
Too hot = vasodilation (shunt vessel narrows), blood travels near surface of skin, sweat glands produce sweat, takes heat away from skin with radiation as it evaporates
A change in a few degrees can affect enzyme activity and how energy is transferred (i.e. CO2 diffusing out of cells down conc. gradient, body must maintain this steep conc. gradient)
Kidneys
Urea made when amino acids are broken down by deamination (removes amide group), makes ammonia which is converted to urea for safe excretion
Nephrons filter blood
Glucose, mineral ions, water and urea move out of blood
RBC/WBC/proteins are too large to be filtered so bypass kidneys
All glucose is reabsorbed
Water and mineral ions reabsorbed by selective reabsorption
Urine trickles to the bladder
Receptor cells in the brain detect conc. of solutes in plasma
If the blood is too concentrated, lots of ADH is produces, and a small volume of concentrated urine is produced
If blood is too dilute, less ADH is produced, and a large volume of dilute urine is produced
Doing lots of exercise/sweating/drinking little means less urine as more water/mineral ions are absorbed to make sweat
Doing little activity/drinking a lot produces lots of urine
Dialysis involves blood passing between partially permeable membrane surrounded by dialysis fluid with the same conc. of dissolved ions and glucose as a healthy person
Fluid contains urea, meaning a steep concentration gradient means only urea and excess mineral ions diffuse across
No active transport unlike in the kidneys because, contrary to what AQA believe, inanimate objects cannot respire
A transplant can be given but the risk of cell rejection means a patient must be on immune-suppressant drugs for life
Plant hormones
Roots grow down due to gravity (positive gravitropism)
Shoots grow up towards the light (phototropism)
Auxin distribute to bend due to gravity/the shaded side respectively to elongate plant cells and curve growth
Gibberellins stimulate breakdown of food stores in seeds at germination – used to speed up germination
Ethene controls cell division and ripens fruit
To make clones of the same plant (i.e. it has good properties/can be grown quickly), cuttings are taken and mixed with rooting powders
Auxin can be used as a weed killer
Reproduction
Asexual reproduction: one parent, genetically identical offspring, mitosis
Sexual reproduction: two parents, variation in offspring, gametes created by meiosis
In meiosis, genetic information is copied so there are 4 sets of each chromosome, each chromosome forms a pair of chromatids, and the cell divides twice in quick succession to form 4 gametes, each with a single set of chromosomes (23)
Fungi are made of hyphae, in which spores reproduce asexually but undergo meiosis to make the spores
Genetics
DNA: long polymer chain of repeating units, twists and folds into a double helix structure, paired up homologous chromosomes
Genes code for specific sequence of amino acids to make specific proteins by protein synthesis (transcription – DNA unzips, mRNA complements strand, carried out by ribosomes, and translation – tRNA complements mRNA codon and brings amino acid to ribosome, mRNA is entirely decoded until a chain of amino acids forms polypeptides)
The genome is the entire genetic material of an organism
A nucleotide is the combination of a sugar, phosphate backbone, and base
Nucleotides are grouped into 3 (codons)
The complementing base pairs are adenine & thymine, and cytosine & guanine
Non-coding parts of DNA are used for switching certain genes on/off (controls gene expression)
Mutation: change in sequence of bases in DNA, forming a different protein
Mutations in non-coding DNA won’t affect the phenotype, but how certain genes are expressed
Alleles are different versions of the same gene – each code for different protein
Inheritance was first developed as an idea by Gregor Mendel
If only one gene is involved, it is monohybrid inheritance
Polydactyl – dominant, cystic fibrosis (in the paper it’s meant to be in) – recessive, sickle cell anaemia – recessive, Huntington’s disease – dominant
Genetic screening can be done by amino centesis (fluid taken from foetal fluid via needle), chorionic villus sampling (sample of tissue from placenta), or by screening embryos (DNA isolated from embryo cell and tested with fluorescent dye which binds to specific alleles)
Variation and evolution
Discontinuous variation: characteristics can only result in certain values
Continuous variation: characteristics can take any value within a certain range (shown by normal distribution curve)
Speciation is natural selection due to a change in location
Darwin proposed the theory of natural selection (good mutation leads to higher survival rate and therefore is inherited more and more over time)
Lamarck said that animals change to suit their environment, but this was disproven as animals cannot change their genotype
Classification
Animalia, plantae, fungi, protoctista, prokaryote – kingdoms
Archaea, bacteria, eukaryotes – domains (Carl Woese)
Mammals, reptiles, fish, amphibians, birds – class
Kingdom, phylum, class, order, family, genus, species
Named by binomial system (two components) in Latin from the genus and species
Ecology
Ecosystem: all the organism living in a habitat with all the non-living parts
Individual organisms -> populations -> communities
Interdependence is when species rely on each other
When all the species and environmental factors are in balance, it is a stable community
Abiotic factors – light, temperature, moisture, soil pH, minerals, wind, CO2, and Oxygen levels
Biotic factors – food, predators, pathogens, competition between species
Adaptations may be structural, behavioural or functional
Extremophiles live in extreme environments
Population: group of one species living in a habitat
Biodiversity: the variety of different species on earth – allows interdependence
Threats include pollution, over-exploitation, decay/burning of peat, deforestation and global warming (rising sea levels, changes migration, disrupt species distribution etc)
Solutions include breeding programs, protecting rare species, encouraging farmers to leave hedgerows (stop monoculture), reducing deforestation/CO2 emissions, fishing quotas, and adapting net sizes
Decomposition occurs by detrivores beginning the breakdown and then decomposers secreting enzymes to partially digest waste and leave small, soluble food molecules which are absorbed by soil
Producers -> primary consumers -> secondary consumers -> tertiary consumers (apex predators have no predators above them)
In a stable community, predators and prey rise/fall in cycles
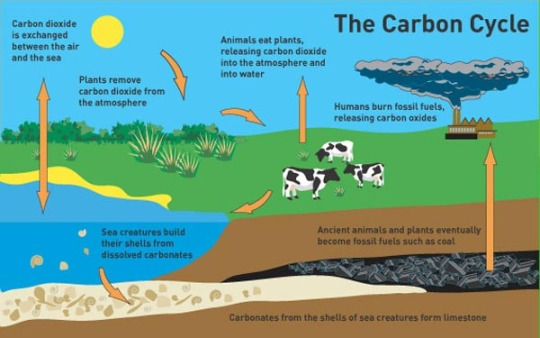
Carbon cycle:
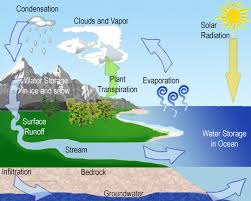
Water cycle:
Pyramids of biomass show trophic levels
Energy is lost due to faeces, excretion, urine, respiration etc so there are less organisms in higher trophic levels
Feeding animals high-protein food increases energy transfer, along with lowering temperatures and movement (although this is unethical)
Biotechnology uses Fusarium in large vats called fermenters with glucose syrup to make mycoprotein, which is then harvested and purified
Mycoprotein is low in fat, high in fibre/protein
Genetically modified crops can provide nutritional value (i.e. golden rice in Asia)
Good luck tomorrow!
#biology#gcse#gcse biology#key points#exam notes#aqa science#aqa biology#studyblr#gcse studyblr#gcse class 2018
215 notes
·
View notes
Text
External Ophthalmomyiasis, Case Report in Campania-Juniper Publishers
Abstract
Objective: To describe a clinical case of external ophthalmomyiasis in a 55 year old man from Umbria, Italy. We are also taking into consideration a differential diagnosis of Onchocerciasis and Cisticercosis.
Design: Case Report Interventional
Participants:1 patient, 2 eyes in an interventional case report
Methods:biomicroscopic examination, surgical removal of the larve, medical treatment, laboratory examination of the specimen and blood screening
Main Outcome Measures:It was not possible to obtain microscopic evidence of the larvae. Blood screening and examination of the specimen was negative but the biomicroscopic evidence of the parasites, together with documented information, made the diagnosis relatively easy
Conclusions:The difference in clinical signs and negative laboratory tests allowed us to exclude all the diseases mentioned above. With case study, we hope to be able to aid in simplifying the diagnosis of this pathology for our colleagues.
Keywords: Ocular Pain; Melanoma; Ciliary Body; Cataract
Abbreviations: BCVA: Best-Corrected Visual Acuity; NMR: Nuclear Magnetic Resonance
Introduction
Ophthalmomyiasis is an infection of the eye by Diptera larvae. Oestrus Ovis is the most frequent cause of ocular myiasis especially in countries with tropical or mild climates [1]. The presence of this pathogen is widely seen in Central and Southern Italy and the islands where sheep farming is common [2]. Ophthalmomyiasis, based on its location, is classified as external, internal and/ or orbital. In its external form the larvae are found on the conjunctiva or on the edge of the eyelid [3]. With accidental contact this can give rise to inflammation of the conjunctiva. The patient may also experience lacrimation, photophobia and foreign body sensation in the eye.
Case History
55 year old male patient, telephoned from Umbria where he was attending an open air public manifestation. He stated that, whilst sitting under a tree the previous evening, he had the sensation that something had “hit” his left eye. He complained of foreign body sensation, pain and photophobia throughout the night. He was advised to come to our private practice. At 14.00 h he arrived. His general condition was good. His left eye was red, painful and intensely photophobic. A biomicroscopic examination revealed numerous tiny worms in rapid movement (Figure 1). The worms were removed by using forceps, cotton buds and continuous irrigation of the inferior and superior conjunctival sac with a iodopovidone 5% solution and netilmycin sulphate 0.455g eye drops equal to 0300g. The patient was then treated with netilmycin sulphate ointment every two hours. At 22.00 h after a second biomicroscopic examination more larvae were removed. Some larvae were preserved in test tubes containing tears and others were placed on slides to be microscopically examined in the laboratory.
The specimens (slides and lacrimal liquid collected in tubes) were examined immediately. One drop of physiological solution at 0, 9% was added to the lacrimal fluid and placed on dry glass slides and observed microscopically (first at 10x field and then 40x). No Diptera larvae were found, because they had dissolved. Giemsa slides at 3% were prepared next. This stain is used to highlight the visibility of other forms of parasites, particularly nematodes and larvae of platelminta cestodes. Thin films of lacrimal liquid were fixed with methanol and then stained with Giemsa at 3% Microscopic examination, at 1000x with an oil immersion lens revealed no parasites.
The following day a blood sample was drawn and biomicroscopic examination revealed the presence of a few slow moving larvae. These were removed with forceps. A complete and thorough examination (vision, IOP, anterior chamber, vitreous and fundus) was normal aside from conjunctival injection. An examination two days later showed the presence of cysts situated in the conjunctiva (Figure 2). The base of the cysts was pearl in color but the upper part was transparent. Haemato chemical tests were negative and a diagnosis of ophthalmomyiasis was made based on physical evidence. An examination six days later revealed a slight reduction in the size of the cysts and an absence of larvae. After eight days the cysts were in a phase of regression and the conjunctiva was no longer inflamed.
Discussions
The term myiasis means the invasion of human tissue by parasites of the type Diptera. The first case of ocular myiasis was described by Keyt in the 1900s [1]. The ocular form can be external, internal or orbital and is commonly associated with Oestrus Ovis [4]. Infestation occurs when the female lays her eggs on the skin or mucous membrane. Stimulated by the warmth these eggs evolve into larvae that are about 1.5 mm in size. The larvae then penetrate the skin or mucous membrane in a few minutes. Penetration inside the eye occurs from perforation of the sclera which allows the larvae to move below the retina. This may leave a hypopigmented trail. Entry into vitreous chamber may occur due to a break in the retina. The larvae can be trapped in the vitreous and gain entry into the anterior or posterior chambers. The risk is partial dislocation or dislocation of the lens and damage to suspensory ligaments (zonulules) [5]. The signs and symptoms of internal ophthalmomyiasis vary accordingly to anterior or posterior positioning of the larvae. The signs of anterior positioning are recurring iritis associated with partial displacement or total displacement of the lens. In posterior positioning one can see vitreous turbidity and possible detachment of the retina [6].
External opthalmomyasis presents symptoms similar to acute catarrhal conjunctivitis as in the case presented. However it is necessary to pay much attention to the treatment, because it could have serious complications such as conjunctival ulceration, endophtalmitis and invasion into other regions of the eye and orbit [4]. Diagnosis is based on anamestetic and clinical data. Identification of the parasite if it is microscopically present. The typical parasitological aspects are, length a little over 1 mm, offwhite color and two hooks in the cephalic segment. Examined under a light the fissures appear tiny and fusiform with cylindrical translucid elements and a black mark at one end. This allows the parasite to be highly mobile and capable of penetrating the conjunctiva [2]. Note, it is extremely difficult to remove and preserve these larvae due to their fragility. Even though some were rapidly placed on slides and others saved in lacrimal liquid in the test tubes, it was not possible for the laboratory to examine them as they dissolved. Treatment requires continual removal of the larvae and antibiotics to prevent further bacterial infection.
We found that irrigation of the conjunctiva with a solution of iodopovidone 5% and nethilmycina, did reduced the number of larvae which helped lower the risk of further infection. It is also necessary to be on the lookout for other conditions that could occur due to larvae having entered the eye. We refer in particular,to cysticercosis and onchocercosis, which , initially, had been considered as possible differential diagnosis.
Cysticercosis is a parasitic disease caused by larvae of platelminta cestode of taenia type A. This cestode has man as its final host and pigs are the intermediary hosts [7]. Clinical symptoms depend on the site of infection and migration. One can see conjunctivitis, iridocyclitis, displacement of the lens, retinal detachment, vitritis, etc. Decreased vision, pain and foreign body sensation are symptoms that the patient may experience [8]. Diagnosis is made by looking for anti cysticercus serum antibodies; enzyme linked immunoelectro transfer blot (EITB).
Onchocercosis is an infectious disease caused by infestation of nematode filariform onchocerca volvulus. The incubation period of 3-12 months shows no clinical signs [9]. The first sign is usually the appearance of subcutaneous nodes. Lesions to the eye, starting at the cornea, begin with opaque white infiltrates and keratitis, followed by corneal opacities. Microfilarie found in the anterior chamber can cause iridocyclitis and glaucoma, whereas, regardless of microfilarie in the posterior chamber, it is possible to find atrophied areas of the retina and choroid. Involvement of the retina can lead to damage of the optic nerve causing reduced vision or eventually blindness [10-11]. Diagnosis is made through anamnestic and laboratory data: an increase in eosinophil, immunoenzymatic tests and the presence of microfilarie. Sample is taken during the night when reproduction of filarie is at its highest.
Conclusion
Although it was not possible to obtain microscopic evidence of larvae, the symptoms, the biomicroscopic aspect of the parasites, together with documented information, made the diagnosis relatively easy. The difference in clinical signs and negative laboratory tests allowed us to exclude any of the diseases mentioned above. With case study, we hope to be able to contribute and aid in simplifying the diagnosis of this pathology for our colleagues.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.com
For more articles in JOJ Ophthalmology please click on: https://juniperpublishers.com/jojo/index.php
For more Open Access Journals please click on: https://juniperpublishers.com
0 notes
Text
An Introduction to Astigmatism
Do you experience symptoms such as blurry or fluctuating vision, headaches and eye strain, which usually manifest after reading a book, staring at a computer screen or looking at far-off distances?1,2 It’s possible that you have astigmatism, a type of refractive error.
Don’t be frightened, however; astigmatism is fairly common and is not a dangerous disorder. But to truly understand why astigmatism occurs, you must first learn how the human eye works.
Here’s How Your Vision Works
When you look at a particular object, light rays from the object need to pass through the eyes so that it can reach the retina. This then triggers nerve messages to be sent from the retina cells down to the optic nerve and then to the brain’s vision centers. The information received is then processed by the brain, which then allows us to see.
Light rays can reflect from an object in all directions. This is because they come from many light sources around us, such as sunlight, moonlight and artificial light (from light bulbs and lamps), which then bounce back from that specific object. However, the part of this bounced light that enters the eye from an object must be focused on a small part of the retina. If this fails to happen, then the object you’re staring at will be blurred.
The task of focusing light falls on your cornea and lens. The cornea is mainly responsible for this, as it refracts or bends the rays of light, which then pass through the lens. The lens then finely adjusts the focusing, by changing its thickness. This is known as “accommodation,”3 as the lens is actually elastic, and can shift from being rounded or flatter. If the lens is more rounded, the light rays can be better bent inward.
The lens’ shape varies depending on the small muscles in the ciliary body. Suspensory ligaments, which are small string-like structures, are attached at one end to the lens, connecting it to the ciliary body. Think of its structure as a trampoline: The lens acts as the bouncy center, the suspensory ligaments are the springs and the ciliary muscles act as the rim around the edge of the bouncy center.
When the muscles in the ciliary body tighten, it causes the ligaments to slacken, making the lens fatter. This is what happens when you’re looking at objects that are near. For objects that are far away, the ciliary muscle becomes relaxed, causing the ligaments to tighten. The lens then thins out. For nearby objects, more refraction of the light rays is necessary to allow better focus. However, less bending is needed if the object is far away.4
So How Does Astigmatism Occur?
Again, refraction is the method by which the eye — specifically the cornea — bends light.5 If you have a refractive error, though, it means that your eyes are not able to properly bend or focus light on the retina, leading to blurry vision.6 This may occur because of two reasons: Either there are abnormalities in the shape of the eyeball or aging has affected the focusing mechanisms of the eye.
Astigmatism is one of these refractive errors, along with hypermetropia, myopia and presbyopia. It happens when the cornea found at the front of the eye is curved instead of being perfectly rounded.
Think of it as a mini rugby ball. If curved in the wrong direction or if the curve is too great, astigmatism happens. This is because the light rays that enter the cornea and lens are not focused on a particular spot on the retina, and instead are spread. Because there’s a lack of point focus, the images transmitted to the brain are blurred.7
Discover More About Astigmatism by Reading These Pages
Astigmatism is fairly common, but don’t fret: It’s not an eye disease, and it can be easily addressed. Read these pages to learn everything you need to know about astigmatism and how you can prevent it from interfering with your daily activities.
MORE ABOUT ASTIGMATISM
• Astigmatism: Introduction
• What Is Astigmatism?
• Astigmatism Symptoms
• Astigmatism Causes
• Astigmatism Test
• Types of Astigmatism
• Astigmatism Treatment
• Contact Lenses For Astigmatism
• Astigmatism Prevention
• Astigmatism FAQ
Next >
What Is Astigmatism?
Next What Is Astigmatism?
from HealthyLife via Jake Glover on Inoreader http://articles.mercola.com/sites/articles/archive/2018/09/29/astigmatism-introduction.aspx
0 notes
Text
Background Knowledge
This is a post on the Bates Method for curing errors of refraction and various other eye problems naturally.
Before I go into the actual Bates Method, let's discuss the structure and workings of the normal eye, accommodation, and a few basic, widely accepted facts on the errors of refraction. This is just to give you some background knowledge to help you understand the theory behind and the techniques of the Bates Method later on. I'm not going to talk about anything bizarre in this post - in fact, you'll find the exact same information on Wikipedia, the ultimate source of truth, and I'll be giving links to various Wikipedia articles and Youtube videos throught this post. Besides, you must have heard most of it anyway. In this post I'm either talking about things both Bates and the mainsteam agree on, or traditional widely accepted views that only Bates differs from.
Let's start with the eye anatomy [x]. For more details on the structure of the human eye, I particularly recommend Chapters 2, 6 and 17 in “Relearning to See” by Thomas Quakenbush. It is a book specifically on the Bates Method, but again, it's something that doesn’t spur controversy.

internal structure of the normal eye; the picture is taken from Wikipedia [x]
The human eye has a spherical shape. Its thick, protective outer layer is called the sclera and it transforms into the transparent cornea at the front, which enables light to enter into the eye. There's the choroid lying in between the sclera and the retina – a system of tiny blood vessels that provide oxygen and nutrients to the whole eye. The eyeball mostly consists of the vitreous humor contained in the vitreous chamber. As for the structures at the front, we have the aqueous chamber filled with the aqueous humor and then the iris and lens. The pupil is just a “hole” in the iris allowing light to pass through into the eye. The pupil narrows in bright light and during accommodation; it constricts when the circular muscle (also called the iris sphincter muscle) surrounding the iris contracts. Pupil dilation is triggered by the contraction of another muscle located within the iris, the radial, or iris dilator muscle. It occurs in dim light or during stress response. Unfortunately, it isn’t marked on the above diagram, but next to the suspensory ligaments is the cilliary body containing the cilliary muscle. Traditionally, it is believed that the cilliary muscle is responsible for adjusting the curvature of the lens in order to enable accommodation. Bates views accommodation entirely differently than mainstream science both in his times and ours.
When light enters our eyes, it passes through the cornea, aqueous chamber, pupil, lens and the vitreous humor, before finally reaching its desination, the retina. The cornea and the lens “refract”, or bend, the light rays in order to correctly focus them onto the retina. The retina cells called rods and cones transform light energy into electrical impulses and send them to the brain through the optic nerve, where they are interpreted and a picture finally formed.
The retina [x] is a highly varied structure. It consists of nine layers and only one of them, the deepest one, is capable of transferring light energy into electical energy. So, cones and rods are “buried” under eight other layers. There is only one spot in the retina where the first eight layers are compressed and reduced so that light doesn't have to travel such great a distance – the fovea centralis. The two types of photoreceptive cells, cones and rods, vary greatly. Cones are able to pick up sharp detail and color, but they need high levels of light to become “activated”. Rodes, on the other hand, can't perceive detail and color but exhibit the highest sensitivity at low levels of light and enable us to see in relative darkness. Additionally, rods are much more effective in detecting movement. The cones and rods are spread together throughtout the retina, but their distribution is far from equal or random. The center of the retina is a structure called “macula lutea” and at the center of the macula lies the aforementioned fovea centralis. The macula is extremely small, and yet it contains the vast majority of our cones and enjoys the highest density of those cells. The fovea consists almost exclusively of cones and at its very core there are virtually no rods. The further away from the fovea, the less cones and more rods there are. Since cones are the only cells providing sharp colorful vision, the area that the human eye can see best, well, the area that the human eye can see anywhere near “good”, is extremely small. Remember that fovea is also the only part of the retina where light doesn't need to trudge through eight other layers, again making the fovea the region of highest visual acuity. This runs contrary to the popular belief, the common illusion being that we can see “everything” equally well at the same time, at least if we enjoy normal vision. But I ensure you, this is no lie: Wikipedia concurs [x].
Because the area seen best is very small, the eye must move constantly between tiny points in order to “gather” enough information. Those continuous, minute, subconscious eye movements (as well as the larger ones we make voluntarily) is what caters to us the illusion that we see a large area all alike simultaneously. Every tiny, incredibly rapid movement provides us with a new bit of information and when the brain receives hunderds of such microscopic bits in a second, it puts them together to create a coherent, extensive image. Eye movements is something Bates puts a lot of emphasis on; he calls them “shifts”, “shifting”, and very often stresses the importance of moving the gaze around and avoiding staring for healthy eyes and acute vision. But I'll write more on this later. Again, mainstream science also recognizes that the human eye is moving all the time; it has distinguished several types of eye movements – here's an overview [x]. To be honest, I haven't yet done much research on the modern discoveries and terminology mentioned in this article, but I know more than enough on what Bates has to say about “shifting”, and that's what's truly important. By the way, Youtube offers quite a lot of eye-tracking videos, such as [x], which show just how much the eyes move and again reiterate that the area seen best is, at any rate, surprisingly small.
Now we need to take a look at accommodation.
All the authorities – both mainstream scientists and Bates – agree that the normal eye at rest is adjusted for distant vision. The light rays being sent off from distant objects are parallel and they fall directly onto the retina (more specifically, the fovea centralis). However, light rays coming off close-up objects are divergent and would focus behind the retina if the eye didn't take any action to re-adjust itself for these kind of rays. Therefore, the eye needs some sort of mechanism to adapt to looking at the near-point. This process is called accommodation.
But how exactly does the eye accommodate? This has been a matter of dispute over the centuries, but the theory which has become widely accepted in Bates' times and remains unchallenged in ours is the one put forward by Hermann von Helmholtz. According to this theory, accommodation occurs when the curvature of the lens is changed by the cilliary muscle. When the eye looks in the distance, the cilliary muscle is relaxed, the lens remains thin, and the eye is adjusted for parallel rays. When the eye looks at the near-point, however, the cilliary muscle contracts in order to make the lens more “convex”, more bulgy. This enhances refraction of the light rays and makes them focus directly on the retina rather than behind it. According to Holmholtz, the primary agent of accommodation is the lens, and the cilliary muscle. You can watch a succint explaination of this theory – presented, of course, as a fact – for example here [x]. As already stated, Bates has a very different opinion on accommodation and we'll get to it in time.

light from a distant object and light from a near object being brought to a focus by the agency of a convex lens as proposed by the theory of accommodation put forward by Helmholtz; the picture is taken from Wikipedia [x]
Now, let's discuss the errors of refraction – that is, near- and far-sightedness, astigmatism, and presbyopia. The eye possessing normal vision is called emmetropic; the focal point, or the point where the light entering the eye converges, is located exactly on the retina.

the normal, or emmetropic eye; the picture is taken from the National Eye Institute website [x]
Errors of refraction occur when the light entering the eye does not focus correctly on the retina (in other words, fails to reach, and converge at, the fovea centralis). Both traditional science and Bates agree that in myopia the axial length of the eye – the distance from the anterior surface of the eye all the way through to the fovea – is too long because the eyeball is too long. As a result, the focal point of the light rays lies before the retina. Glasses prescribed for near-sightedness are concave lenses which diverge the light and therefore move the focal point farther away, bringing it onto the retina.

compensating for myopia using a divergent corrective lens; the picture is taken from Wikipedia [x]
Hypermetropia occurs when the eye is too short; the light rays focus behind the retina. A convex lens is used to converge the light and move the focal point to the front, thereby bringing the light rays into focus at the retina. Astigmatism is usually attributed to the irregular shape of the cornea which prevents light from focusing evenly on the retina and creates more than one focal point. Presbyopia may have the same symptoms as hypermetropia, but according to orthodox science the underlying cause of this condition is not a change in the shape of the eyeball but the hardening of the lens and weakening of the cilliary muscle supposed to control the lens' shape. It is thought an unavoidable consequence of growing old. In presbyopia the ability to accommodate is lost, the light rays focus behind the retina, and therefore one becomes unable to see clearly at the near-point. Just as in far-sightedness, a convex lens is prescribed to correct this state.

compensating for hypermetropia using a convergent corrective lens; the picture is taken from Wikipedia [x]
According to conventional eye doctors, as I am sure you are well aware, all these conditions are organic (that is, a consequence of tissue changes) and uncurable. No solutions are offered to prevent or slow down the progression of these illnesses, and once they develop they are held by both doctors and the public absolutely untreatable. Needless to say, that's a very depressing prognosis.
Before Bates found out how to treat refractive errors and other problems, he was just a regular ophthalmologist; he prescribed glasses and performed operations just as any other eye doctor. However, as he amassed clinical experience he noted that many orthodox teachings on the nature of vision disorders and their irreversibility did not stand ground against multiple cases he and other oculists have observed – and the findings he made in trying to find a sufficient explanation for certain discrepancies enabled him to devise methods for curing various vision problems. What exactly prompted him to do his own research and what he discovered – I will explain in the next post.
xxx Emily
#visionblr#the bates method#bates#natural vision improvement#bates method 101#vision#vision problems#eye problems#blurry vision#myopia#nearsightedness#hypermetropia#farsightedness#astigmatism#presbyopia#blindness#glasses#eye#my post#physical illness#chronic illness#eyes#accommodation#dr. bates
0 notes
Text
How The Human Eye Works Function Of Lens Human Eye
How The Human Eye Works Function Of Lens Human Eye
Function Of Lens In Human Eye How Eyes Lens work The tiny rings of muscle that make your vision sharp
How The Human Eye Works
cameras and human eyes both focus light using a lens. This structure bends the incoming wavelengths so that they hit the right spot on a photographic plate, or on the back of the eye. A camera lens is made from solid glass, and focuses on near and distant objects by…
View On WordPress
#A ring of muscle surrounding the lens can pull it tight#A round#Accommodation explained#allowing the brain to perceive depth#Beneath the iris#By holding your hand in front of your face and closing one eye at a time#cameras and human eyes both focus light using a lens#Combined image#Eye lens#eye lenses function#Eye Works Focusing Cornea Iris and Lens#Eyes lenses#fat lens is good for looking at nearby objects.#Function Of eye Lens#Function Of eyes Lens#Function of Lens in Human Eye how eyes Lens#how eyes lens work#how eyes work diagram#how human eyes lenses focus#How The Human Eye Works Function Of Lens Human Eye#human eye#Human Eyes lenses#individual image#it is easy to see the different 2D views perceived by each eye#lens is responsible for focusing the light on the back of the eye.#muscles are working hard to adjust the lens#nature Human Eyes lenses#Near#or let it relax.#Seeing in three dimensions
0 notes
Video
youtube
What is ACCOMMODATION REFLEX? What does ACCOMMODATION REFLEX mean? ACCOMMODATION REFLEX meaning - ACCOMMODATION REFLEX definition - ACCOMMODATION REFLEX explanation. Source: Wikipedia.org article, adapted under http://ift.tt/yjiNZw license. The accommodation reflex (or accommodation-convergence reflex) is a reflex action of the eye, in response to focusing on a near object, then looking at distant object (and vice versa), comprising coordinated changes in vergence, lens shape and pupil size (accommodation). It is dependent on cranial nerve II (afferent limb of reflex), superior centers (interneuron) and cranial nerve III (efferent limb of reflex). The change in the shape of the lens is controlled by the ciliary muscles inside the eye. Changes in contraction of the ciliary muscles alter the focal distance of the eye, causing nearer or farther images to come into focus on the retina; this process is known as accommodation. The reflex, controlled by the parasympathetic nervous system, involves three responses; pupil accommodation, lens accommodation, and convergence. A near object (for example, a computer screen) appears large in the field of vision, and the eye receives light from wide angles. When moving focus from a distant to a near object, the eyes converge. The ciliary muscle contracts making the lens more convex, shortening its focal length. The pupil constricts in order to prevent diverging light rays from hitting the periphery of the retina and resulting in a blurred image. Information from the light on each retina is taken to the occipital lobe via the optic nerve and optic radiation (after a synapse in the lateral geniculate body of the posterior thalamus), where it is interpreted as vision. The peristriate area 19 interprets accommodation, and sends signals via the Edinger-Westphal nucleus and the 3rd cranial nerve to the ciliary muscle, the medial rectus muscle and (via parasympathetic fibres) the sphincter pupillae muscle. During accommodation, the pupil constricts to increase the depth of focus of the eye by blocking the light scattered by the periphery of the cornea. The lens then increases its curvature to become more biconvex, thus increasing refractive power. The ciliary muscles are responsible for the lens accommodation response Convergence is the ability of the eye to simultaneously demonstrate inward movement of both eyes toward each other. This is helpful in effort to make focus on near objects clearer. Three reactions occur simultaneously; the eyes adduct, the ciliary muscles contract, and the pupils become smaller. This action involves the contraction of the medial rectus muscles of the two eyes and relaxation of the lateral rectus muscles. The medial rectus attaches to the medial aspect of the eye and its contraction adducts the eye. The medial rectus is innervated by motor neurons in the oculomotor nucleus and nerve. The refractive index of the eye’s lens system allows the eye to produce sharply focused images. For example, geometrical optics show that as a distant object is brought closer to the eye, the focus of the object becomes blurrier in the plane behind the retina; however, as a result of the increase in the refractive power of the eye, this image becomes clear. The refractive power mainly resides in the cornea, but the overall refractive power is achieved by the actual lens changing its shape. In order to fixate on a near object, the ciliary muscle contracts around the lens to decrease its size. The suspensory ligaments relax and the radial tension around the lens is released. This causes the lens to form a more spherical shape achieving a higher level of refractive power. When the eye focuses on distant objects, the lens holds itself in a flattened shape due to traction from the suspensory ligaments. Ligaments pull the edges of the elastic lens capsule towards the surrounding ciliary body and by opposing the internal pressure within the elastic lens, keep it relatively flattened.
0 notes
Text
The Human Eye, Retina, and Retinal Laser
The human eye is definitely fascinating, not only because it provides us with the vision of the world, but because its complexity is awesomely beautiful. If you are going to compare it with the digital camera, you would definitely say that it is an awesome technology that is ingeniously created for the human body to enjoy. The human eye is obviously a product of the evolutionary process of humans, and if you are going to carefully consider the evolution of the human eye from lower form of visual organ to a higher form of visual organ, then you would surely conclude that the evolution of the human eye seems to be arbitrarily guided by some higher intelligence. It is hard to imagine that the human eye, in its present form, had evolved blindly, because there seems to be an ingenious designer that had designed its evolution.
The Wonderful Parts of the Human Eye
The human eye, like an ingenious work of invention, has different parts that all function to make the visual experience of every person possible. There are main parts of the human eye that have important functions for the actualization of the human vision. There are also some parts of the human eye that serve and play support roles to the main parts of the human eye. The main parts of the eye is the cornea, the pupil, the iris, the lens, the retina, and the optic nerve. The other parts of the human eye include the posterior and anterior chamber, the sclera, the choroid, the fovea, the macula, the conjunctiva, the ciliary body, the suspensory ligament zonules, the medial, rectus muscle, and the vitreous body.
The eye has various coatings to protect it. The third inner coat of the human eye is the retina, which is a light-sensitive coating consisting of light-sensitive tissues. It is in the retina where the optics of the eye create an image of the outside world. The retina functions like the camera film, and once the light reaches the retina, it initiates various electrical and chemical events. These changes in the retina eventually trigger nerve impulses that are carried to the brain by the optic nerve. The entire retina is usually composed of photo receptor cells, ganglion cells, bipolar cells, plus the pigmented epithelial cells. The growth of retina during the embryonic development of a person came from the outgrowths of the brain that was in the process of development during the early stage of the life of a person. Hence, retina is considered to be part of the nervous system, specifically that of the central nervous system.
Various Diseases that Afflict the Retina
There are various diseases that afflict the retina, and some of these diseases include the retinal retinopathy, retinal degeneration, retinal detachment, retinal vascular occlusions, retinopathy, and retinitinis pigmentosa. Some diseases that afflict the retina necessitate surgeries. Retina surgery using laser such as that of laser photocoagulation is usually performed on those with diabetic retinopathy. This retina laser surgery makes use of heat emitted by a laser equipment. This heat destroys and seals the abnormally leaking blood vessels of the retina due to diabetic retinopathy.
0 notes