#signs and symptom of coronavirus
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs




Fun Fact
Tumblr is used by 21% of adults online aged 18-29 years.
Text
COVID at 3 Years: Where Are We Headed?
March 15, 2023 – Three years after COVID-19 rocked the world, the pandemic has evolved into a steady state of commonplace infections, less frequent hospitalization and death, and continued anxiety and isolation for older people and those with weakened immune systems. After about 2½ years of requiring masks in health care settings, the CDC lifted its recommendation for universal, mandatory…
View On WordPress
#3 year covid anniversary#coronavirus#coronavrius webmd#covid#covid about#covid now#covid statistics#covid then vs now#covid treatments#covid vaccine#covid webmd#Covid-19#long covid#pandemic#pandemic 3rd year#pandemic anniversary#signs of covid#symptoms of covid
1 note
·
View note
Text
Vaccines ensure bouts of COVID are far less deadly than they were at the pandemic's start, yet multiple studies now suggest even seemingly mild cases of the coronavirus have a cost. With every single infection, our risk of long COVID increases. While this risk starts (relatively) low for most of us, particularly those vaccinated and in younger people or children, there are concerning signs it may not stay low. If each new invasion of our bodies allows this insidious virus a greater chance to cause damage, such small risks will eventually add up to a big one. Even if you only experience the symptom of the initial infection mildly.
Continue Reading.
576 notes
·
View notes
Text
COVID patients breathe large amounts of virus early on - Northwestern Now
It is the first longitudinal, direct measure of the number of SARS-CoV-2 viral copies exhaled per minute over the course of the infection — from the first sign of symptoms until 20 days after. On day eight, exhaled levels of virus drop steeply, down to near the limit of detection — an average of two copies exhaled per minute. Northwestern investigators tested breath samples — collected multiple times daily from 44 individuals — over the entire course of infection to determine when a person is most infectious.
...
“The vast majority of research on viral loads over the course of a COVID-19 infection has been based on nasal or oral swabs, which measure virus in the nose or throat,” said lead study author Gregory Lane, senior research project manager in Zelano’s lab. “However, SARS-CoV-2 is spread through breath, and virus on the breath may not match virus in the nose. The dynamics of viral shedding on breath over the course of infection are poorly understood, despite the fact that this is how the virus spreads.”
See also:
#covid#article#research#study#data#covid is airborne#viral load#transmission#viral shedding#aerosols
129 notes
·
View notes
Text
Old news, but something people should remember
Never let them tell you "We didn't know covid was so bad" or "It's mild for kids." We knew.
Also preserved on our archive
By John Anderer
PHILADELPHIA, Pa. — The news about coronavirus and children just got a lot worse. A troubling study by researchers at the Children’s Hospital of Philadelphia reports a “high proportion” of children infected with SARS-CoV-2 show elevated levels of a biomarker tied to blood vessel damage. Making matters worse, this sign of cardiovascular damage is being seen in asymptomatic children as well as kids experiencing COVID-19 symptoms.
Additionally, many examined children testing positive for SARS-CoV-2 are being diagnosed with thrombotic microangiopathy (TMA). TMA leads to clots in small blood vessels and has been linked to severe COVID symptoms among adult patients.
“We do not yet know the clinical implications of this elevated biomarker in children with COVID-19 and no symptoms or minimal symptoms,” says co-senior author David T. Teachey, MD, Director of Clinical Research at the Center for Childhood Cancer Research at CHOP, in a media release. “We should continue testing for and monitoring children with SARS-CoV-2 so that we can better understand how the virus affects them in both the short and long term.”
The complex connection between kids and COVID It’s fairly well established at this point that most children who contract coronavirus experience little to no symptoms. However, a small portion of young patients develop major symptoms or a post-viral inflammatory response to COVID-19 called Multisystem Inflammatory Syndrome in Children (MIS-C).
TMA in adults has a connection to more severe cases of COVID-19. Scientists believe the component of the immune system called “complement cascade” helps to mediate TMA in adults. The complement cascade is supposed to enhance and strengthen immune responses when a threat is present, but it can also backfire and lead to more inflammation. Up until now, the role of complement cascade during childhood TMA hadn’t been investigated.
To research the topic of “complement activation” in kids with SARS-CoV-2, researchers analyzed a group of 50 pediatric COVID-19 patients between April and July 2020. Among the group, 21 showed minimal to no symptoms, 11 experienced severe symptoms, and 18 developed MIS-C.
To search for complement activation and TMA among each patient, researchers used soluble C5b9 (sC5b9) as a biomarker. Scientists have used this substance for quite some time to assess the severity of TMA after stem cell procedures. In brief terms, the higher the level of sC5b9 in a transplant patient, the greater their mortality risk.
No symptoms doesn’t mean there’s no problem Study authors discovered elevated levels of C5b9 in both patients with severe COVID-19 and MIS-C. While this didn’t surprise researchers, they did get a shock from seeing high levels of C5b9 among even asymptomatic youngsters.
Some of the lab data regarding TMA had to be obtained after the fact. This meant researchers didn’t have a complete dataset to work with for all 50 studied patients. Among 22 patients researchers did have complete data for, 86 percent (19 children) were diagnosed with TMA. Every child had elevated levels of sC5b9, even those without TMA.
“Although most children with COVID-19 do not have severe disease, our study shows that there may be other effects of SARS-CoV-2 that are worthy of investigation,” Dr. Teachey concludes. “Future studies are needed to determine if hospitalized children with SARS-CoV-2 should be screened for TMA, if TMA-directed management is helpful, and if there are any short- or long-term clinical consequences of complement activation and endothelial damage in children with COVID-19 or MIS-C. The most important takeaway from this study is we have more to learn about SARS-CoV-2. We should not make guesses about the short and long-term impact of infection.”
The study is published in Blood Advances.
Study Link: ashpublications.org/bloodadvances/article/4/23/6051/474421/Evidence-of-thrombotic-microangiopathy-in-children
#mask up#covid#pandemic#covid 19#wear a mask#public health#coronavirus#sars cov 2#still coviding#wear a respirator
45 notes
·
View notes
Text
Hufvudstadsbladet writes that Alexander Stubb took Åland by storm during his first visit there as president on Tuesday.
Describing it as a "charm visit" the paper features a photo of a seemingly endless queue in the main square in the capital, Mariehamn, of people lined up to take selfies with the president.
Hufvudstadsbladet also points to a more serious side to the visit, writing that Stubb said exactly what the Ålanders wanted to hear — the demilitarised status of the autonomous region is not a problem, and that having reviewed Finland's defence plans for Åland, he sleeps well at night.
Iltalehti reports that the president's press conference in Mariehamn on Tuesday was mainly focused on current foreign and security policy issues.
Asked about his statements to the French newspaper Le Monde regarding possible peace talks between Ukraine and Russia, he stood by his position, stressing that any decision on whether or not to start a negotiation process is in Ukraine's hands.
In reference to the counter-attack by Ukraine in Kursk, Stubb said that Finland would not impose restrictions on the use of the arms it supplies to Ukraine.
"Ukraine has every right to defend itself within the framework of international law," said President Stubb.
Potential for sabotage
Several papers picked up on a report first published online on Tuesday afternoon by Helsingin Sanomat saying that the Finnish Security Intelligence Service (Supo) sees Finnish arms aid to Ukraine as a target of potential Russian sabotage.
This summer, Finland sent its 24th shipment of arms aid to Ukraine. Officials have not revealed any details about their content or, for example, the mode of shipment.
The total value of all defence materials sent from Finland to Ukraine now stands at 2.2 billion euros.
Helsingin Sanomat quotes Supo researcher Lotta Hakala as saying that there are no signs of anything unusual concerning the logistics, storage and transport of Finland's arms aid. However, Supo has now publicly said they are potential targets for sabotage.
Supo has also found no evidence of Russian involvement in recent break-ins and vandalism at some water processing facilities in Finland.
The Security Intelligence Service adds, though, that Russia is trying to influence public opinion in countries that support Ukraine in order to create a climate of fear and uncertainty aimed at eroding popular support for Ukraine.
Covid up, but most cases mild
The number of cases of coronavirus infection is on the rise in Finland, but according to the National Institute for Health and Welfare (THL) symptoms seem to be less severe than in the past, and people are less likely to seek hospital treatment.
Ilta-Sanomat looks at the situation after asking readers to tell the paper about their experiences with covid over the summer, and receiving more than 600 responses by early this week.
The vast majority of respondents said they had mild symptoms after being infected. The most common symptoms included fever, headache, fatigue, cough, runny nose and muscle aches.
This is all very similar to the effects of a common cold.
Around 30 covid deaths were recorded in Finland between June and July this year, compared with over 120 in the same period last year.
Ilta-Sanomat notes that THL specialists have said that for the elderly or others in poor health Covid, like other infections, can still pose a serious and require hospitalisation.
Urban legend debunked
Have you heard of the old lady who feeds bread crumbs to birds from a large bag in Helsinki's central park? The story goes that she wears a black coat and a black scarf in summer and winter and doesn't say a word. If anyone approaches her, she vanishes.
Or how about the treasure hidden under what is now the Laajasalo bridge, stashed away by Carl Olof Cronstedt, a Vice-Admiral in the Swedish Navy? Cronstedt surrendered what is now the Suomenlinna fortress to Russian besiegers in 1808, and the story goes that first, he hid a huge bribe that he received for raising a white flag.
These are a few of the urban legends Helsingin Uutiset mentions before delving into its own investigation of one more — a longstanding rumour that the Helsinki House of Culture is home to an infestation of venomous spiders.
It is a fact that sometime during the 1970s a few Chilean recluse spiders apparently hitched a ride in a crate from South America to Helsinki's Museum of Natural History and established a small colony in the building.
HU set out to find investigate whether there is any truth to claims that something similar happened at the House of Culture.
The facilities production manager, Antti Sarmanne, claims to have seen the spiders several times in well over 20 years on the job.
"I think they came long before me. The story goes that the spiders came to the House of Culture in the equipment of a foreign artist, or from an exhibition," he said.
A thorough search by HU of the cellar's nooks and crannies found spiders, and spiders of more than one species, but none of them exotic or venomous.
Chilean recluse spiders have not been seen outside the Natural History Museum, its curator Timo Pajunen assured HU. During the 1990s, a spider was sent from the House of Culture to the museum for identification and it turned out to be a common house spider.
Helsingin Uutiset's conclusion is that whispers of deadly creepy-crawlers in the House of Culture can safely be ignored.
4 notes
·
View notes
Text
Extracts of the the Judge’s reasoning and analysis:
On November 4, 2020, Plaintiff Brianne Dressen received AstraZeneca’s experimental COVID vaccine as part of a clinical trial in Salt Lake County. 4 Velocity Clinical Research, Inc. (Velocity) administered the trial on AstraZeneca’s behalf. 5 Before receiving the inoculation, Dressen signed an informed consent form (ICF) that outlined her rights and responsibilities as a trial participant and disclosed possible side effects of the vaccine.6 Under the terms of the ICF, the parties agreed AstraZeneca would “reimburse[] for time and travel in the amounts of $125.00 per each completed study visit and $30.00 for each completed phone call.”7 The parties also agreed that a “study doctor” would “provide medical treatment or refer [Dressen] for treatment” if Dressen became ill or injured while participating in the study.8 Additionally, AstraZeneca disclosed that it had an insurance policy to “cover the costs of research injuries as long as [Dressen] followed [the] study doctor’s instructions.”9 AstraZeneca confirmed it would “pay the costs of medical treatment for research injuries, provided that the costs are reasonable, and [Dressen] did not cause the injury [her]self.”10 At the same time, the parties agreed federal law may limit Dressen’s right to sue for injuries caused by the vaccine: Due to the coronavirus public health crisis, the federal government has issued an order that may limit your right to sue if you are injured or harmed while participating in this COVID-19-related clinical study. If the order applies, it limits your right to sue the researchers, healthcare providers, any Sponsor or manufacturer or distributor involved with the Study. You may be prevented from making claims for injuries that have a causal relationship with the use of the investigational product in this Study, including, but not limited to, claims for death; physical, mental, or emotional injury, illness, disability, or condition; fear of physical, mental, or emotional injury, illness, disability, or condition, including any need for medical monitoring; and loss of or damage to property, including business interruption loss. However, the federal government has a program that may provide compensation to you or your family if you experience serious physical injuries or death. If funds are appropriated by Congress, compensation for injuries may be available to you under this Countermeasures Injury Compensation Program.11 Within an hour of receiving the vaccine, Dressen’s right arm began tingling.12 The sensation, a condition called paresthesia, soon spread to her right shoulder and left arm.13 Later the same day, Dressen began experiencing a host of other symptoms, including blurred vison, tinnitus, nausea, and sound sensitivity.14 Dressen first visited an emergency room three days after receiving the vaccine.15 The doctor who treated her diagnosed her with a “vaccine reaction.”16 She returned to the emergency room four days later, and the next day she visited a nurse practitioner at Utah Valley Neurological who diagnosed her with an “immunization reaction.”17 Thirteen days after receiving the vaccine, Dressen visited an otolaryngologist to seek care for “acute sensitivities to light and sound.”18 The doctor noted Dressen was suffering from “a likely side effect due to an increased immune response to the vaccine.”19
2 notes
·
View notes
Text
First-Year Puppy Vaccinations

When you bring that fuzzy ball of puppy energy into your home, you know right away that your new puppy depends on you for, well, everything. It’s up to you to give your new puppy all the care they need every day. It can be a little intimidating — your puppy needs the best puppy food, plenty of attention, puppy training, puppy-safe toys, puppy socialization, a comfortable place to sleep, and proper veterinary care. And that includes making sure to schedule puppy shots throughout your puppy’s first year.
Which Shots Do Puppies Need?
Going to the vet over several months for a series of puppy vaccinations—and then for boosters or titers throughout your dog’s life—may seem inconvenient, but the diseases that vaccinations will shield our puppies and dogs from are dangerous, potentially deadly, and, thankfully, mostly preventable.
We read about so many different dog vaccinations, for so many different illnesses, that it can sometimes be confusing to know which vaccinations puppies need and which puppy shots are important but optional. Here is an overview of the diseases that puppy vaccinations will help your pet avoid.
Bordetella Bronchiseptica
This highly infectious bacterium causes severe fits of coughing, whooping, vomiting, and, in rare cases, seizures and death. It is the primary cause of kennel cough. There are injectable and nasal spray vaccines available.
If you plan on boarding your puppy in the future, attending group training classes, or using dog daycare services, often proof of this vaccination will usually be required.
Canine Distemper
A severe and contagious disease caused by a virus that attacks the respiratory, gastrointestinal (GI), and nervous systems of dogs, raccoons, skunks, and other animals, distemper spreads through airborne exposure (through sneezing or coughing) from an infected animal. The virus can also be transmitted by shared food and water bowls and equipment. It causes discharges from the eyes and nose, fever, coughing, vomiting, diarrhea, seizures, twitching, paralysis, and, often, death. This disease used to be known as “hard pad” because it causes the footpad to thicken and harden.
There is no cure for distemper. Treatment consists of supportive care and efforts to prevent secondary infections, control symptoms of vomiting, seizures and more. If the animal survives the symptoms, it is hoped that the dog’s immune system will have a chance to fight it off. Infected dogs can shed the virus for months.
Canine Hepatitis
Infectious canine hepatitis is a highly contagious viral infection that affects the liver, kidneys, spleen, lungs, and the eyes of the affected dog. This disease of the liver is caused by a virus that is unrelated to the human form of hepatitis. Symptoms range from a slight fever and congestion of the mucous membranes to vomiting, jaundice, stomach enlargement, and pain around the liver. Many dogs can overcome the mild form of the disease, but the severe form can kill. There is no cure, but doctors can treat the symptoms.
Canine Parainfluenza
This is one of several viruses that can contribute to kennel cough.
Coronavirus
The canine coronavirus is not the same virus that causes COVID-19 in people. COVID-19 is not thought to be a health threat to dogs, and there is no evidence it makes dogs sick. Canine coronavirus usually affects dogs’ gastrointestinal systems, though it can also cause respiratory infections. Signs include most GI symptoms, including loss of appetite, vomiting, and diarrhea. Doctors can keep a dog hydrated, warm, and comfortable, and help alleviate nausea, but no drug kills coronaviruses.
Heartworm
When your puppy is around 12-to-16 weeks, talk to your vet about starting a heartworm preventive medication. Though there is no vaccine for heartworm in dogs, it is preventable with regularly administered heartworm medication that your veterinarian will prescribe.
The name is descriptive — these worms lodge in the right side of the heart and the pulmonary arteries (that send blood to the lungs), though they can travel through the rest of the body and sometimes invade the liver and kidneys. The worms can grow to 14 inches long and, if clumped together, block and injure organs.
A new heartworm infection often causes no symptoms, though dogs in later stages of the disease may cough, become lethargic, lose their appetite or have difficulty breathing. Infected dogs may tire after mild exercise. Unlike most of the conditions listed here, which are passed by urine, feces, and other body fluids, heartworms are transmitted by mosquitoes. Therefore, diagnosis is made via a blood test and not a fecal exam.
Kennel Cough
Also known as infectious tracheobronchitis, kennel cough results from inflammation of the upper airways. It can be caused by bacterial, viral, or other infections, such as Bordetella and canine parainfluenza, and often involves multiple infections simultaneously. Usually, the disease is mild, causing bouts of harsh, dry coughing; sometimes it’s severe enough to spur retching and gagging, along with a loss of appetite. In rare cases, it can be deadly. It is easily spread between dogs kept close together, which is why it passes quickly through kennels. Antibiotics are usually not necessary, except in severe, chronic cases. Your vet may prescribe a dog-safe cough suppressant to help your dog (and you) get some rest, and some dog-safe throat soothers can help make a dog more comfortable.
Leptospirosis
Unlike most diseases on this list, Leptospirosis is caused by bacteria, and some dogs may show no symptoms at all. Leptospirosis can be found worldwide in soil and water. It is a zoonotic disease, meaning that it can be spread from animals to people. When symptoms do appear, they can include fever, vomiting, abdominal pain, diarrhea, loss of appetite, severe weakness and lethargy, stiffness, jaundice, muscle pain, infertility, kidney failure (with or without liver failure). Antibiotics are effective, and the sooner they are given, the better.
Lyme Disease
Unlike the famous “bull’s-eye” rash that people exposed to Lyme disease often spot, no such telltale symptom occurs in dogs. Lyme disease (or borreliosis) is an infectious, tick-borne disease caused by a type of bacteria called a spirochete. Transmitted via ticks, an infected dog often starts limping, his lymph nodes swell, his temperature rises, and he stops eating. The disease can affect his heart, kidney, and joints, among other things, or lead to neurological disorders if left untreated. If diagnosed quickly, a course of antibiotics is extremely helpful, though relapses can occur months or even years later.
Talk to your vet about when your puppy will be old enough for tick preventatives. Once your puppy is old enough, keep your dog on tick preventative medication, topicals, or wearables to help stop ticks from biting in the first place.
Parvovirus
Parvo is a highly contagious virus that affects all dogs, but unvaccinated dogs and puppies less than four months of age are at the most risk to contract it. The virus attacks the gastrointestinal system and creates a loss of appetite, vomiting, fever, and often severe, bloody diarrhea. Extreme dehydration can come on rapidly and kill a dog within 48-to-72 hours, so prompt veterinary attention is crucial. There is no cure, so keeping the dog hydrated and controlling the secondary symptoms can keep him going until his immune system beats the illness.
Rabies
Rabies is a viral disease of mammals that invades the central nervous system, causing headache, anxiety, hallucinations, excessive drooling, fear of water, paralysis, and death. It is most often transmitted through the bite of a rabid animal. Treatment within hours of infection is essential, otherwise, death is highly likely. Most states require regular rabies vaccinations. Check with your vet about rabies vaccination laws and requirements in your area.
Talk with your veterinarian about more information and guidance on necessary and optional vaccinations.
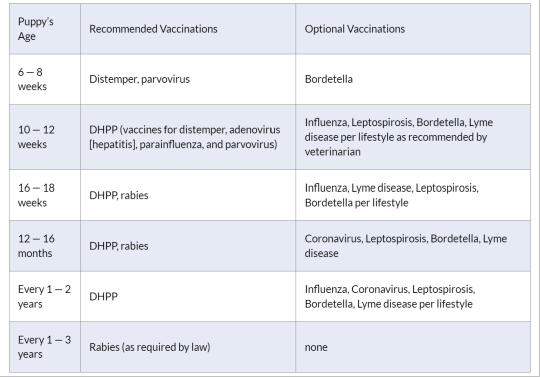
Puppy Vaccination Schedule
The first thing to know is that there is not just one puppy vaccination schedule for all dogs. Factors such as which part of the country you live in, and your dog’s individual risk factors will come into play. Some dogs do not need every vaccine. This decision is between you and your veterinarian. Always discuss puppy vaccinations at your regularly scheduled appointments.
That said, here is a generally accepted guideline of the puppy vaccination schedule for the first year.
How Much Do Puppy Vaccinations Cost?
How much puppy vaccinations will cost depends on several factors. Where you live is a big one: Veterinarians in crowded and expensive urban areas will generally charge more than a rural vet in a small town. You may be able to find low-cost clinics providing rabies vaccinations sponsored by your local municipal government. But no matter what the range in costs, some vaccines, such as the “core vaccines” and rabies, are necessary.
The average cost can average around $75—100. These will include the core vaccines, which are administered in a series of three: at 6-, 12-, and 16 weeks old.
The core vaccines include the DHLPP (distemper, hepatitis, leptospirosis, parvo, and parainfluenza). Your pup will also need a rabies vaccination, which is usually around $15—20. (Some clinics include the cost of the rabies vaccination.)
Often animal shelters charge less for vaccines — approximately $20 — or are even free. If you acquired your dog from a shelter, he would most likely have been vaccinated, up until the age when you got him.
The initial puppy vaccination costs during the first year are higher than during adulthood.
Vaccinations for Adult Dogs: Boosters and Titers
There is a difference of opinion about having your adult dog vaccinated every year. Some vets believe too many vaccinations in adult dogs pose health risks. But others disagree, saying that yearly vaccinations will prevent dangerous diseases such as distemper. Talk with your vet to determine what kind of vaccination protocol works for you and your dog.
Many dog owners opt for titer tests before they administer annual vaccinations. Titer tests measure a dog’s immunity levels, and this can determine which, if any, vaccinations are necessary. One key exception to this is rabies: a titer test is not an option when it comes to the rabies vaccine. This vaccination is required by law across the United States. Your vet can tell you the schedule for your particular state, with boosters often lasting three years.
And it’s all worth it. For your effort and care your puppy will lavish you with lifelong love in return. This critical first year of her life is a fun and exciting time for both of you. As she grows physically, the wonderful bond between you will grow, too.
#puppy vacinations#puppy vaccines#puppy shots#puppy shots schedule#dog vaccinations#dog health#puppy health
5 notes
·
View notes
Text
(Times) This May Be Our Last Chance to Halt Bird Flu in Humans, and We Are Blowing It

The outbreak of H5N1 avian influenza among U.S. dairy cows, first reported on March 25, has now spread to at least 33 herds in eight states. On Wednesday, genetic evidence of the virus turned up in commercially available milk. Federal authorities say the milk supply is safe, but this latest development raises troubling questions about how widespread the outbreak really is.
So far, there is only one confirmed human case. Rick Bright, an expert on the H5N1 virus who served on President Biden’s coronavirus advisory board, told me this is the crucial moment. “There’s a fine line between one person and 10 people with H5N1,” he said. “By the time we’ve detected 10, it’s probably too late” to contain.
That’s when I told him what I’d heard from Sid Miller, the Texas commissioner for agriculture. He said he strongly suspected that the outbreak dated back to at least February. The commissioner speculated that then as many as 40 percent of the herds in the Texas Panhandle might have been infected.
Dr. Bright fell silent, then asked a very reasonable question: “Doesn’t anyone keep tabs on this?”
The H5N1 outbreak, already a devastating crisis for cattle farmers and their herds, has the potential to turn into an enormous tragedy for the rest of us. But having spent the past two weeks trying to get answers from our nation’s public health authorities, I’m shocked by how little they seem to know about what’s going on and how little of what they do know is being shared in a timely manner.
How exactly is the infection transmitted between herds? The United States Department of Agriculture, the Food and Drug Administration and the Centers for Disease Control and Prevention all say they are working to figure it out.
Sign up for the Opinion Today newsletter Get expert analysis of the news and a guide to the big ideas shaping the world every weekday morning.
According to many public health officials, the virus load in the infected cows’ milk is especially high, raising the possibility that the disease is being spread through milking machines or from aerosolized spray when the milking room floors are power washed. Another possible route is the cows’ feed, owing to the fairly revolting fact that the U.S. allows farmers to feed leftover poultry bedding material — feathers, excrement, spilled seeds — to dairy and beef cattle as a cheap source of additional protein.
Alarmingly, the U.S.D.A. told me that it has evidence that the virus has also spread from dairy farms back to poultry farms “through an unknown route.” Well, one thing that travels back and forth between cattle farms and chicken farms is human beings. They can also travel from cattle farms to pig farms, and pigs are the doomsday animals for human influenza pandemics. Because they are especially susceptible to both avian and human flu, they make for good petri dishes in which avian influenza can become an effective human virus. The damage could be vast.
The U.S.D.A. also told me it doesn’t know how many farmers have tested their cattle and doesn’t know how many of those tests came up positive; whatever testing is being done takes place at the state level or in private labs. Just Wednesday, the agency made it mandatory to report all positive results, a long overdue step that is still — without the negative results alongside them — insufficient to give us a full picture. Also on Wednesday, the U.S.D.A. made testing mandatory for dairy cattle that are being moved from one state to another. It says mandatory testing of other herds wouldn’t be “practical, feasible or necessarily informative” because of “several reasons, ranging from laboratory capacity to testing turnaround times.” The furthest the agency will go is to recommend voluntary testing for cattle that show symptoms of the illness — which not all that are infected do. Dr. Bright compares this to the Trump administration’s approach to Covid-19: If you don’t test, it doesn’t exist.
As for the F.D.A., it tells me it hasn’t completed specific tests to confirm that pasteurization would make milk from infected cows safe, though the agency considers it “very likely” based on extensive testing for other pathogens. (It is not yet clear whether the elements of the H5N1 virus that recently turned up in milk had been fully neutralized.) That testing should have been completed by now. In any case, unpasteurized milk remains legal in many states. Dr. Bright told me that “this is a major concern, especially given recent infections and deaths in cats that have consumed infected milk.”
Making matters worse, the U.S.D.A. failed to share the genomes from infected animals in a timely manner, and then when it shared the genomes did so in an unwieldy format and without any geographic information, causing scientists to tear their hair out in frustration.
All this makes catching potential human cases so urgent. Dr. Bright says that given a situation like this, and the fact that undocumented farmworkers may not have access to health care, the government should be using every sophisticated surveillance technique, including wastewater testing, and reporting the results publicly. That is not happening. The C.D.C. says it is monitoring data from emergency rooms for any signs of an outbreak. By the time enough people are sick enough to be noticed in emergency rooms, it is almost certainly too late to prevent one.
So far, the agency told me, it is aware of only 23 people who have been tested. That tiny number is deeply troubling. (Others may be getting tested through private providers, but if negative, the results do not have to be reported.)
On the ground, people are doing the best they can. Adeline Hambley, a public health officer in Ottawa, Mich., told me of a farm whose herd had tested positive. The farm owner voluntarily handed over the workers’ cellphone numbers, and the workers got texts asking them to report all potential symptoms. Lynn Sutfin, a public information officer in the Michigan Department of Health and Human Services, told me that response rates to those texts and other forms of outreach can be as high as 90 percent. That’s heartening, but it’s too much to expect that a poor farmworker — afraid of stigma, legal troubles and economic loss — will always report even mild symptoms and stay home from work as instructed.
It’s entirely possible that we’ll get lucky with H5N1 and it will never manage to spread among humans. Spillovers from animals to humans are common, yet pandemics are rare because they require a chain of unlucky events to happen one after the other. But pandemics are a numbers game, and a widespread animal outbreak like this raises the risks. When dangerous novel pathogens emerge among humans, there is only a small window of time in which to stop them before they spiral out of control. Neither our animal farming practices nor our public health tools seem up to the task.
There is some good news: David Boucher, at the federal government’s Administration for Strategic Preparedness and Response, told me that this virus strain is a close match for some vaccines that have already been formulated and that America has the capacity to manufacture and potentially distribute many millions of doses, and fairly quickly, if it takes off in humans. That ability is a little like fire insurance — I’m glad it exists, but by the time it comes into play your house has already burned down.
I’m sure the employees of these agencies are working hard, but the message they are sending is, “Trust us — we are on this.” One troubling legacy of the coronavirus pandemic is that there was too much attention on telling the public how to feel — to panic or not panic — rather than sharing facts and inspiring confidence through transparency and competence. And four years later we have an added layer of polarization and distrust to work around.
In April 2020, the Trump administration ousted Dr. Bright from his position as the director of the Biomedical Advanced Research and Development Authority, the agency responsible for fighting emerging pandemics. In a whistle-blower complaint, he alleged this happened after his early warnings against the coronavirus pandemic were ignored and as retaliation for his caution against unproven treatments favored by Donald Trump.
Dr. Bright told me that he would have expected things to be much different during the current administration, but “this is a live fire test,” he said, “and right now we are failing it.”
Zeynep Tufekci (@zeynep) is a professor of sociology and public affairs at Princeton University, the author of “Twitter and Tear Gas: The Power and Fragility of Networked Protest” and a New York Times Opinion columnist. @zeynep • Facebook
A version of this article appears in print on April 28, 2024, Section SR, Page 9 of the New York edition with the headline: The U.S. Is Blowing Its Chance to Halt Bird Flu in Humans. Order Reprints | Today’s Paper | Subscribe
3 notes
·
View notes
Text
Study undercuts premise for excluding women from medical research
Women’s body temperatures are no more variable than men’s, despite menstrual cycles and hormonal variability, a recent monitoring study suggests. The analysis, published in the journal Biology of Sex Differences, casts doubt on an idea that has long colored biomedical research — that ovarian cycles make females unsuited for drug trials and other clinical experiments.
That claim — along with gender discrimination and other factors — is thought to fuel women’s ongoing underrepresentation in such trials, which continues despite a concerted effort by the federal government and researchers to bolster sex-specific research.
When researchers looked at six months’ worth of continuous body temperature data from a group of males and females, they found that despite sex differences in body temperature, neither group was more variable than the other.
The researchers looked at temperature data from a pool of age-matched 20-to-79-year-olds: 300 females and 300 males. The participants were part of a broader University of California study, TemPredict, designed to track vital signs and help predict the onset of coronavirus symptoms.
Over the course of six months, patients wore an Oura ring, a wearable “smart ring” that monitors heart rate, respiration, body temperature and movement. (Oura Health Oy, the Finnish technology company that produces the ring, was one of the study’s funders.)
When the scientists delved into the body temperature data, comparing it across sex and over time and looking for excessive variability or measurement errors among females, they did find sex differences. Women with menstrual cycles showed temperature fluctuations across a roughly 28-day cycle, confirming that ovarian rhythms do affect body temperature.
But those differences did not confound or sully the data, and the researchers note that the predictability of the women’s temperature variability actually made their temperatures easier to predict than men’s.
“In this study, the difference between two men is bigger than the difference between the average man and the average woman,” Lauryn Keeler Bruce, the paper’s first author and a PhD student in the Bioinformatics and Systems Biology program at UC San Diego, said in a news release. “In addition, the variability between men and women is not statistically significant.”
2 notes
·
View notes
Text
The federal government has burned through more than $1 billion to study long Covid, an effort to help the millions of Americans who experience brain fog, fatigue, and other symptoms after recovering from a coronavirus infection.
There’s basically nothing to show for it.
The National Institutes of Health hasn’t signed up a single patient to test any potential treatments — despite a clear mandate from Congress to study them. And the few trials it is planning have already drawn a firestorm of criticism, especially one intervention that experts and advocates say may actually make some patients’ long Covid symptoms worse.
Instead, the NIH spent the majority of its money on broader, observational research that won’t directly bring relief to patients. But it still hasn’t published any findings from the patients who joined that study, almost two years after it started.
There’s no sense of urgency to do more or to speed things up, either. The agency isn’t asking Congress for any more funding for long Covid research, and STAT and MuckRock obtained documents showing the NIH refuses to use its own money to change course.
“So far, I don’t think we’ve gotten anything for a billion dollars,” said Ezekiel Emanuel, a physician, vice provost for global initiatives, and co-director of the Healthcare Transformation Institute at the University of Pennsylvania. “That is just unacceptable, and it’s a serious dysfunction.”
Eric Topol, the founder and director of the Scripps Research Translational Institute, said he expected the NIH would have launched many large-scale trials by now, and that testing treatments should have been an urgent priority when Congress first gave the agency money in late 2020.
“I don’t know that they’ve contributed anything except more confusion,” Topol said.
11 notes
·
View notes
Text
Future COVID Vaccines Must Be Better; Science Races to Respond
SOURCES David L. Hoey, president and CEO of Vaxxas, Cambridge, MA, and Brisbane, Australia. Pablo Penaloza-MacMaster, PhD, assistant professor of microbiology and immunology, Feinberg School of Medicine, Northwestern University, Chicago. Jasdave Chahal, PhD, co-founder and chief scientist, Tiba Biotech, Cambridge, MA, and Brisbane, Australia. Vaxart news release: “Vaxart Announced Positive…
View On WordPress
#3 year covid anniversary#coronavirus#coronavirus webmd#covid#covid about#covid now#covid statistics#covid then vs now#covid treatments#covid vaccine#covid webmd#Covid-19#long covid#pandemic#pandemic 3rd year#pandemic anniversary#signs of covid#symptoms of covid
0 notes
Text
By Lambert Strether of Corrente.
On May 25 of this year, JAMA published Development of a Definition of Postacute Sequelae of SARS-CoV-2 Infection (“Definition”), an “original investigation” whose authors were drawn from the RECOVER Consortium, an initiative of the National Institutes of Health (NIH)[1]. This was an initially welcome development for Long Covid sufferers and activists, since questions had arisen about what exactly patients were getting for the billion dollars RECOVER was appropriated. From STAT:
The federal government has burned through more than $1 billion to study long Covid, an effort to help the millions of Americans who experience brain fog, fatigue, and other symptoms after recovering from a coronavirus infection.
There’s basically nothing to show for it.
The National Institutes of Health hasn’t signed up a single patient to test any potential treatments — despite a clear mandate from Congress to study them.
Instead, the NIH spent the majority of its money on broader, observational research that won’t directly bring relief to patients. But it still hasn’t published any findings from the patients who joined that study, almost two years after it started.
(The STAT article, NC hot take here on April 20, is worth reading in full.) Perhaps unfairly to NIH — one is tempted to say that the mountain has labored, and brought forth a coprolite — a CERN-level headcount may explain both RECOVER’s glacial pace, and its high cost:

That’s a lot of violin lessons for a lot of little Madisons!
“Definition” falls resoundingly into the research (and not treatment) bucket. In this post, I will first look at the public relations debacle (if debacle it was) that immediately followed its release; then I will look at its problematic methodology, and briefly conclude. (Please note that I feel qualified to speak on public relations and institutional issues; very much less so on research methodology, which actually involves (dread word) statistics. So I hope readers will bear with me and correct where necessary.)
The Public Relations Debacle
Our famously free press instantly framed “Definition” as a checklist of Long Covid (LC) symptoms. Here are the headlines. For the common reader:
12 key symptoms define long Covid, new study shows, bringing treatments closer CNN Long COVID is defined by these 12 symptoms, new study finds CBS Scientists Identify 12 Major Symptoms of Long Covid Smithsonian These 12 symptoms may define long COVID, new study finds PBS News Hour These Are the 12 Major Symptoms of Long COVID Daily Beast
(We will get to the actual so-called “12[2] Symptoms” when we look at methodology.) And for readers in the health industry:
For the first time, researchers identify 12 symptoms of long covid Chief Healthcare Executive 12 symptoms of long COVID, FDA Paxlovid approval & mpox vaccines with Andrea Garcia, JD, MPH AMA Update Finally! These 12 symptoms define long COVID, say researchers ALM Benefits Pro
With these last three, we can easily see the CEO handing a copy of their “12 symptoms” article to a doctor, the doctor double-checking that headline against the AMA Update’s headline, and incorporating the NIH-branded 12-point checklist into their case notes going forward, and the medical coders at the insurance company (I love that word, “benefits”) nodding approvingly. At last, the clinicians have a checklist! They know what to do!
We’ll see why the whole notion of a checklist with twelve items is wrong and off-point for what “Definition” was actually, or at least putatively, trying to do, but for now it’s easy to see why the press went down this path (or over this cliff). Here is the press release from NIH that accompanied “Definition”‘s publication in JAMA:
Researchers examined data from 9,764 adults, including 8,646 who had COVID-19 and 1,118 who did not have COVID-19. They assessed more than 30 symptoms across multiple body areas and organs and applied statistical analyses that identified 12 symptoms that most set apart those with and without long COVID: post-exertional malaise, fatigue, brain fog, dizziness, gastrointestinal symptoms, heart palpitations, issues with sexual desire or capacity, loss of smell or taste, thirst, chronic cough, chest pain, and abnormal movements.
They then established a scoring system based on patient-reported symptoms. By assigning points to each of the 12 symptoms, the team gave each patient a score based on symptom combinations. With these scores in hand, researchers identified a meaningful threshold for identifying participants with long COVID. They also found that certain symptoms occurred together and defined four subgroups or “clusters” with a range of impacts on health
So there are 12 symptoms, right? Just like the headline says? Certainly, that’s what a normal reader would take away. And if a temporally pressed reporter goes to the JAMA original and searches on “12”, they find this:
Using the full cohort, LASSO identified 12 symptoms with corresponding scores ranging from 1 to 8 (Table 2). The optimal PASC score threshold used was 12 or greater
And if the reporter goes further and finds Table 2 (we’ll get there when we look at methodology), they will see, yes, 12 symptoms (in rank order identified by something called LASSO).
So it’s easy to see how the headlines were written as they were written, and how the newsroom wrote the stories as they did. The wee problem: The twelve symptoms are not meant to be used clinically, for diagnosis.[3], Lisa McCorkell was the patient representative[4] for the paper, and has this to say:
Nevertheless, the “12 symptoms” are out of the barn and in the next county, and as a result, you get search results like this:
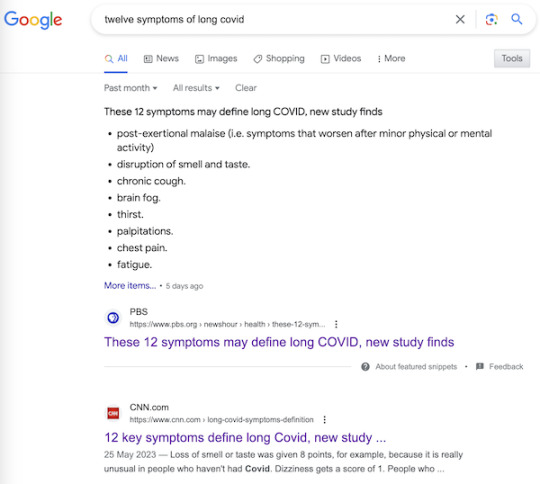
It’s very easy to imagine a harried ER room nurse hearing “12 Symptoms” on the TV news[5], doublechecking with a Google search, and then making clinical decisions based on a checklist not fit for purpose. Or, for that matter, a doctor.
Now, to be fair to the authors, once one grasps the idea that symptoms, even clusters of symptoms, can exist, and still not be suitable for diagnosis by a clinician, the careful language of “Definition” is clear, starting with the title: “Development of a Definition.” And in the Meaning section of the Abstract:
A framework for identifying PASC cases based on symptoms is a first step to defining PASC as a new condition. These findings require iterative refinement that further incorporates clinical features to arrive at actionable definitions of PASC.
Well and good, but do you see “framework” in the headlines? “Iterative”? “First step”? No? Now, I’d like to exonerate the authors of “Definitions” — “They’re just scientists!” — for that debacle, but I cannot, completely. The authors are well-compensated, sophisticated, and aware professionals; PMC, in fact. I cannot believe that the Cochrane “fools gold” antimask study debacle went unobserved at NIH, especially in the press office. How was it possible that “Definitions” was simply… printed as it was, and no strategic consideration given to shaping the likely coverage?[6] One obvious precautionary measure would have been a preprint, but for reasons unknown to me, NIH did not do that. A second obvious precautionary measure would have been to have the patient representative approve the press release. Ditto. Now let us turn to methodology.
The Problematic Methodology
First, I will look at issues with Table 2, which presents the key twelve-point checklist, and names the algorithm (although without explaining it). After that, I will branch out to a few larger issues. Again I issue a caveat that I’m not a Long Covid maven or a statistics maven, and I hope readers will correct and clarify where needed.
Here is Table 2:
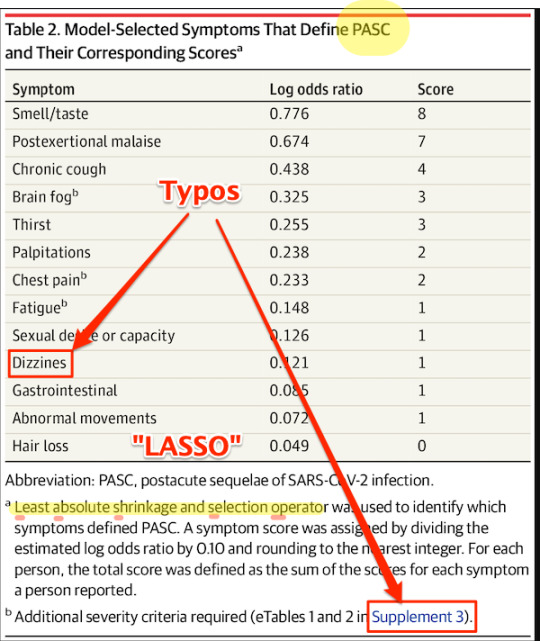
First, some copy editing trifles (highlighted). On “PASC”: As WebMD says: “You might know this as ‘long COVID.’ Experts have coined a new term for it: post-acute sequelae SARS-CoV-2 infection (PASC).” Those lovable scamps, always inventing impenetrable jargon! (Bourdieu would chuckle at this.) On “Dizzines”: Come on. A serious journal doesn’t let a typo like that slip through (maybe they’re accustomed to fixing the preprints?). On “Supplement 3”: The text is highlighted as a link, but clicking it brings up the image, and doesn’t take you to the Supplement. These small errors are important[7], because they indicate that no editor took more than a cursory look at the most important table in the paper. On “LASSO,” hold that thought.
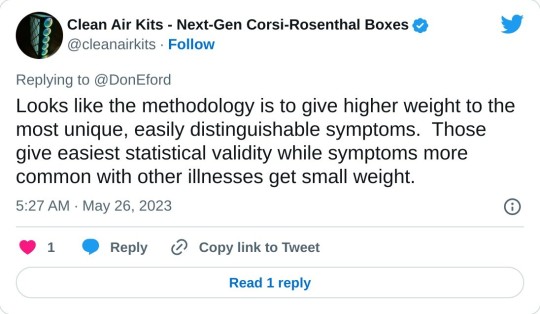
Second, the Covid Action Network points out that some obvious, and serious, symptoms are missing from the list:
[T]he next attempts at diagnostic criteria should take into account existing literature that shows more specifically defined symptoms for Long Covid, from objective findings. (E.g. PoTS, Vestibular issues, migraine, vs more vague symptoms like “headache” or “dizziness.) [The Long Covid Action Project (LCAP)] noticed that while [Post-Extertional Malaise (PEM)] was used as a specific symptom with a high score to produce PASC-positive results, other suites of symptoms, like those in the neurologic category, could have produced an equal or higher score than PEM if questionnaires had not separated neuro-symptoms into multiple subtypes and reduced their total scores. This alone could have created a more scientifically accurate picture of the Long Covid population.
Third, these symptoms — missing, from the patient perspective; to be iterated from the researcher’s perspective, at least one would hope — are the result of “Definition”‘s methodology:
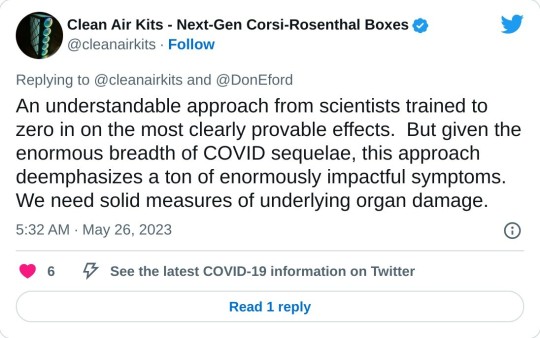
Fourth, I would argue focus on the “most clearly provable effects” — as opposed to organ damage — is a result of the “LASSO” algorithm named in Table 2. I did a good deal of searching on LASSO, and discovered that most of the examples I could find, even the “real world” ones, were examples of how to run LASSO programs, as opposed to selecting the LASSO algorithm as opposed to others. So that was discouraging. I believe — reinforcing the caveats, plural, given above — that I literally searched on “LASSO” “child of five” (“Explain it to me like I’m five”) to finally come up with this:
Lasso Regression is an essential variable selection technique for eliminating unnecessary variables from your model.
This method can be highly advantageous when some variables do not contribute any variance (predictability) to the model. Lasso Regression will automatically set their coefficients to zero in situations like this, excluding them from the analysis. For example, let’s say you have a skiing dataset and are building a model to see how fast someone goes down the mountain. This dataset has a variable referencing the user’s ability to make basketball shots. This obviously does not contribute any variance to the model – Lasso Regression will quickly identify this and eliminate these variables.
Since variables are being eliminated with Lasso Regression, the model becomes more interpretable and less complex.
Even more important than the model’s complexity is the shrinking of the subspace of your dataset. Since we eliminate these variables, our dataset shrinks in size (dimensionality). This is insanely advantageous for most machine learning models and has been shown to increase model accuracy in things like linear regression and least squares.
Since LC is said to have over 200 candidates for symptoms, you can see why a scientist trying to get their arms around the problem would be very happy to shrink those candidates to 12. But is that true to the disease?
Because LASSO (caveats, caveats) has one problem. From the same source:
One crucial aspect to consider is that Lasso Regression does not handle multicollinearity well. Multicollinearity occurs when two or more highly correlated predictor variables make it difficult to determine their individual contributions to the model.
Amplifying:
Lasso can be sensitive to multicollinearity, which is when two or more predictors are highly correlated. In this case, Lasso may select one of the correlated predictors and exclude the other [“set their coefficients to zero”], even if both are important for predicting the target variable.
As Ted Nelson wrote, “Everything is deeply intertwingled” (i.e., multicollinear), and if there’s one thing we know about LC, it’s that it’s a disease of the whole body taken as a system, and not of a single organ:
There are some who seek to downplay Long Covid by saying the list of 200 possible symptoms makes it impossible to accurately diagnose and that it could be encompassing illnesses people might have gone on to develop anyway, but there are sound biological reasons for this condition to affect the body in so many different ways.
Angiotensin-converting enzyme receptor 2 (ACE2) is the socket SARS-CoV-2 plugs into to infect human cells. The virus can use other mechanisms to enter cells=, but ACE2 is the most common method. ACE2 is widely expressed in the human body, with highest levels of expression in small intestine, testis, kidneys, heart, thyroid, and adipose (fat) tissue, but it is found almost everywhere, including the blood, spleen, bone marrow, brain, blood vessels, muscle, lungs, colon, liver, bladder, and adrenal gland
Given how common the ACE2 receptor is, it is unsurprising SARS-CoV-2 can cause a very wide range of symptoms.
In other words, multicollinearity everywhere. Not basketball players vs. skiiers at all.
So is LASSO even the right algorithm to handle entwinglement, like ACE2 receptors in every organ? Are there statistics mavens in the readership who can clarify? With that, I will leave the shaky ground of statistics and Table II, and raise two other issues.
First, it’s clear that the population selected for “Definitions” is unrepresentative of the LC population as a whole:
If the patients in “Definition” are not so ill, that might also account for Table 2’s missing symptoms.
Second, “Definition”‘s questionnaires should include measures of severity, and don’t:

Conclusion
The Long Covid Action Project (materials here) is running a letter writing campaign: “Request for NIH to Retract RECOVER Study Regarding 12 Symptom PASC Score For Long Covid.” As of this writing, “only 3,082 more until our goal of 25,600.” You might consider dropping them a line.
Back to the checklist for one moment. One way to look at the checklist is — we’re talking [drumroll] the PMC here — as a set of complex eligibility requirements, whose function is, as usual, gatekeeping and denial:
what they did is create basically a means test to figure out a dx but for smthg that is still not fully understood. it's premature and rly limited, & this will only further aid ppl already dismissive of lc — Wendi Muse (@MuseWendi) June 3, 2023
If you score 12, HappyVille! If you score 11, Pain City! And no consideration given to the actual organ damage in your body. And after the last three years following CDC, I find it really, really difficult to give NIH the benefit of the doubt. If one believed that NIH was acting in bad faith, one would see “Definition” as a way to keep the funding gravy train rolling, and the “12 Symptoms” headlines as having the immediate and happy outcome of denying care to the unfit. Stay safe out there, and let’s save some lives!
NOTES
[1] Oddly, the JAMA paper is not yet listed on RECOVER’s publications page.
[2] “12” is such a clickbait-worthy brainworm. “12 Days of Christmas,” “12 apostles,” “12 steps,” “12 months,” “12 signs of the zodiac,” etc. One might wonder where if the number had been “9” or “14” the uptake would have been so instant.
[3] To be fair to the sources, most of them mention this: Not CBS, Chief Health Care Executive, or the Daily Beast, but CNN in paragraph 51, Smithsonian (9), PBS (20), AMA Update (10), and Benefits Pro (17).
[4] There was only one patient representative for the paper:
One seems low, especially given the headcount for the project.
[5] I was not able to find a nursing journal that covered the story.
[6] Unless it was, of course.
[7] Samuel Johnson: “When I take up the end of a web, and find it packthread, I do not expect, by looking further, to find embroidery.”
#long covid#naked capitalism#lambert strether#national institutes of health#covid pandemic#covid 19#long covid action project#long covid awareness day
5 notes
·
View notes
Text
Why Organic Elderberry Syrup is a Must-Have for Immune Support
Why Organic Elderberry Syrup is a Must-Have for Immune Support
Why Organic Elderberry Syrup is a Must-Have for Immune Support
Let’s get right to the point. Shall we? Elderberry has been scientifically proven to support the activation of the immune system and prevent the replication of viruses, as well as being active against bacteria. Full stop. Do you need to read that again? Elderberries have some pretty amazing benefits. It’s no wonder I always have a bottle of our organic Elderberry Syrup in the fridge for the first sign of sniffles or scratchy throat. In addition to all the modern research, Elderberry has been used for centuries to treat upper respiratory infections and support health in the wintertime when we seem more susceptible to these bugs. Here are the major takeaways about Elderberry (a plant in the sambucus family with multiple genuses, including nigra) from study results published in scholarly journals on PubMed. Proven to inhibit the infectious activity of viruses (PMID: 26645032) In a study with influenza A & B symptoms were relieved on average 4 days earlier with Elderberry Syrup (PMID: 15080016) Significant reduction of cold duration and severity (PMID: 27023596) Shown to inhibit the viral replication and block the virus attachment of human coronavirus NL63 (HCoV-NL63) (PMID: 31560964) Water-derived elderberry extracts induce potent immune-modulatory effects, which represents the basis for a strong immune-mediated response to viruses including influenza compared to alcohol extracts that do not do this. (PMID: 35409309) Stimulates immune response and prevents viral infection (PMID: 22972323) Inhibits replication of influenza A, B, swine flu and turkey flu, significant improvement of the symptoms within 2 days, complete cure in 2-3 days in 90% compared to up to 6 days in the placebo (PMID: 9395631) Most of the research focuses on viruses (influenza A, B, swine flu, common cold, and recently coronavirus), but there’s also examples of elderberry protecting against bacterial infections. Active against human pathogenic bacteria (Gram-positive bacteria of Streptococcus pyogenes and group C and G Streptococci, and the Gram-negative bacterium Branhamella catarrhalisas) well as influenza viruses (PMID: 21352539) Ok, so if you want to go down the scientific study of elderberry rabbit hole, click any of the links above and read on to your heart's content. Want to know more about the plant itself and some of its more magical qualities? Stay with me. Black Elder (Sambucus nigra) is a shrub that can easily grow into a tree. It grows in Europe and North America, tolerating many environments and enjoying full sun. Each spring it produces clusters of tiny cream colored flowers called elderflowers. These flowers can connect us to the realm of above and fairies, and they have a strong connection to children, representing purity and innocence. Elderflowers tend to be gentle, yet profound. Then as the heat of summer arrives, the flowers wither and the berries ripen. Depending on the genus of the plant they range in color from a dusty light blue to a deep, dark purple. The berries are typically dried and then extracted in water (sometimes glycerine or alcohol), though as referenced above, water extraction is the superior method. Anthocyanins in the elderberries turn the water a deep purple and these are the compounds that stimulate and support our immune, respiratory systems and more. Elderberries are not sweet on their own. They have an affinity for the root and heart chakras, promoting a sense of being centered and open simultaneously. Which makes sense to me because when I am feeling vibrant and healthy I also feel centered and open, and elderberry helps bring us back to vibrant health. I hope you learned something new reading this. Let me know if you have any questions about Elder.
#black elder#cure colds#elderberry syrup#fight bacteria#immune support#influenza A#influenza B#stimulates immune response#water derived elderberry extracts
4 notes
·
View notes
Text
Also preserved on our archive
They are also at higher risk of depression, anxiety and insomnia
COVID-19 survivors show signs of significant cognitive deficits which could become dementia even a year after having the virus 1 . They also have an increased risk of depression, anxiety and disrupted sleep.
People who have had COVID-19 should be subjected to close monitoring and regular check-ups to ensure early detection of cognitive impairment and timely therapeutic interventions, says a team of researchers at the Bangur Institute of Neurosciences in Kolkata.
Previous research has suggested that the coronavirus may enter the brain through the olfactory system but little is known about how the virus affects the brain.
To find out, the scientists, led by Atanu Biswas and Madhushree Chakrabarty, did brain scans and assessed the mental health of COVID survivors using phone and in-person interviews. They then matched these with a control group of people who had not contracted COVID.
The team, which included researchers at the Indian Statistical Institute in Kolkata and the Burdwan Medical College in Purba Bardhaman, found that more than 80% of people tested reported at least one of four symptoms – depression, anxiety, stress and insomnia – ranging from mild to severe.
Patients with higher socioeconomic status experienced less anxiety. At least 6.1% of the patients were diagnosed with mild cognitive impairment and 4% developed dementia.
More than 60% of the patients experienced a loss of taste and smell during the active phase of the infection. This could alter the function of brain areas linked to cognitive ability and emotional well-being, the researchers say.
doi: doi.org/10.1038/d44151-024-00168-7 www.frontiersin.org/journals/psychiatry/articles/10.3389/fpsyt.2024.1370085/full
#long covid#covid conscious#mask up#covid#pandemic#wear a mask#public health#covid 19#wear a respirator#still coviding#coronavirus#sars cov 2#covid is airborne#covid is not over
28 notes
·
View notes
Text
So I just recently returned from vacation, and have been doing some meal prep before I return to work tomorrow. I wore an N95 mask on the plane in both directions, keeping it on continuously from before the start of boarding until after disembarking, making sure to do any eating and drinking in the airport with an appropriate amount of personal space. And I've been self-monitoring for any potential signs and symptoms of influenza, coronavirus, strep, etc.
So here I am cutting some fruit I just got at the grocery store yesterday, and I'm like "hm... this doesn't seem especially fragrant" and promptly zip off to find something else to sniff (my cat's favorite treats smell exactly as fishy as they are supposed to, and my current scented candle smells correct, which is good). And then all I can think is "Bitch, you bought a pineapple... In Ohio... In April... On sale for two fucking dollars... How fragrant were you expecting it to be, dumbass? You're lucky it's even remotely ripe!" (Verdict: I'm a moron, but not ill.)
(In case you were wondering, I had a lovely trip.)
4 notes
·
View notes
Note
Top 5 episodes of mythic quest? Or moments?
I'm going with moments!
5. in "dinner party," brad trolling david into wasting an entire day on, essentially, an oppression olympics bracket ❤️ brad was so hot in his saboteur era and i need that energy to come back.
4. i really love the conflict between poppy and dana in s2 -- their relationship is so sharp and incisive when the show writes it with all the specificity it deserves. dana toeing the line all through s2 is so tense and frustrating. so when she finally snaps in "please sign here" and refuses to take any more any more bullshit from poppy about the stupid personality test, that is just sooo satisfying
3. anytime jo is telling a 12-year-old child to kill himself. enough said
2. basically all of "everlight," but especially the little montage when "we drink light" is playing. (btw, that is charlotte nicdao's husband's band. and what a perfect song for that episode!) i love watching all the nerds rejoice in being a part of a fantasy world. jo's rise to dominating the bracket is amazing, but the best little story to watch during that montage is, surprisingly, rachel and dana's. they're at this very enchanting moment in their will-they-or-won't-they in that episode and it shines during that montage. it's the very last episode before they acknowledge their feelings for each other and start to date. you can see in both their eyes how much they love acting out adventures together. it's really lovely!
1. the climactic rube goldberg sequence at the end of "quarantine." i don't think i will ever forget how good it felt to watch that sequence at the height of lockdown or how feverishly (literally, as i was still dealing with lingering covid symptoms in may 2020) i devoured every article about its production. everyone's faces of pure triumph at the end of the episode and cw's emphatic "fuck you, coronavirus" still make me cry every single time.
6 notes
·
View notes