#seropositive
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr posted its first advertisements in May 2012 and subsequently earned $13M in revenue.
Text
Just like me fr
*crouches to go into stealth*
the cracking of my knees alerts the guards, I am immediately killed
90K notes
·
View notes
Text
Vulnerable
A poem by Ridley Zarate
© sleepyghostface (© Sleepysadwriter on IG & Threads)
Vul•ner•a•ble
Adjective: to open myself up, to tell you what I need. To tell you how I'm feeling.
-------
You asked me to be vulnerable,
but I've never known what that's like.
My mother taught me to hide,
my father to close myself off.
To build walls, to shut down.
because if no one sees it, it's not happening.
There are cracks in the foundation,
and I can't let it show.
So no, I can't be vulnerable.
I can't bring those walls down,
the foundation, my emotions, they'll slip through the cracks and
I can't let you in.
Vulnerability is weakness, and
you don't want to see what lies beneath.
"Tell me what you need."
I want to be good, I want to be what you deserve. But I can't be something I've never understood.
"You're allowed to be vulnerable with me,
have I ever made you feel otherwise?"
I don't know, I only know to
bury it inside.
This way is easy, I don't think I can
let my walls down again.
I can't let you see what
lies beneath, I can't
go through this again.
"Tell me what you need."
I want to be good, I want to be what you deserve. But I can't be something I've never understood.
I want to be what you need,
I want to open myself up again.
You deserve so much better than me.
Vulnerability is a weakness
and I can't let it show.
because if no one sees it, it's not happening.
There are cracks in the foundation,
and I can't let it show.
I want to be more than what you need.
I want to be vulnerable
but I'm so afraid.
I don't know what I want, I
just need you to stay.
#poetry#bpd#poets corner#writeblr#poetry writing#bpd blog#chronic illness#chronically ill#fibromyalgia#seropositive rheumatoid arthritis#just rambling#mental health#mental illness#vulnerable#poems on tumblr#my poem
0 notes
Text
#seropositive erosive rheumatoid arthritis#rheumatoid arthritis#ANCA-associated vasculitis#overlapping conditions#systemic lupus erythematosus#autoimmune
0 notes
Text
Absolutely, yes. I was diagnosed in 2021 with Rheumatoid arthritis and fibromyalgia and that same year started working order pickup in retail, and while it was a bit of a process picking up speed, the idea of moving at half the pace I was back then bums me out bc idk if I'll ever get there.
This last year I started having a lot of issues with my lungs and ribcage, and I know that means I need to get scans, but I'm worried about the autoimmune part of my RA now bc I know it's not just attacking my joints anymore. I get stupid sick at random times, like a few months ago I threw up all over the passenger side of the car when I wasn't feeling too bad when my fiance picked me up from work
I spend my days off basically bed/couch/gaming chair rotting now and feeling terrible, but I don't have much I can do these days. I actually almost started crying the other day bc of the nerves and shit in my arm when I was playing dead by daylight. Doc did diagnose me with bulging discs in my neck and said that they're definitely impacting my arm but they somehow "aren't worried about it rn."
Writing is excruciating for me now bc of said bad arm, and sometimes gaming hurts. Writing has been my passion for 14 years and I'm having to learn to use dictation. The only hobby that actually doesn't hurt me is reading and I don't have many friends who read who I can talk to about it
I'm just a rotting bag of bones, and it's really exhausting. I can't do the things I used to.
The RA has changed me so much in 4 years.
Do any other chronically ill or disabled people feel like they're watching themselves rot away due to how little they can do as a result of their conditions
#seropositive rheumatoid arthritis#fibromyalgia#disc degeneration#chronically ill#chronic pain#chronic illness
2K notes
·
View notes
Text
Also preserved on our archive
By Rob Wallace
From summer into fall, SARS-CoV-2, the COVID-19 virus, ran up another epidemiological spike just as the feds sunset their pandemic control program.
While the virus continues along a loop of boom and bust repeatedly reset by its capacity for evolutionary escape, putting people in the hospital and out of work at a steady clip, U.S. officials and well-connected epidemiologists have abandoned public health in both practice and concept.
Alongside entrapping millions of Americans in a Long COVID vortex, such dereliction of duty places the U.S. in danger should other diseases arise, including, but not limited to, an avian influenza strain that even now is moving beyond cow herds and poultry flocks and beginning to spread in humans.
The COVID-19 pandemic that some of our most august epidemiologists pretend is over portends a broader decline in the very notion of the public commons upon which any functional society depends.
The State of the COVID Nation What’s the present state of the U.S.’s COVID-19 outbreak?
The National Wastewater Surveillance System (NWSS) reports a large majority of its data set of viral load in sewage plants tracked from September 9 to 23 to be in the orange and red zone of 60 percent or more of all the samples taken nationally since December 2021. That is, all those hot points on the NWSS map tell us the viral load in populations across the U.S. is now as high (and widespread) as any previous COVID peak.
On the other hand, the more acute NWSS measure of changes in SARS-2 sewage loads over the 15 days leading up to September 23 shows a mosaic of declines and increases, indicating differences at the sewershed level we still don’t understand.
NWSS tracks only 1,479 of the 16,000 publicly owned wastewater plants, which together serve at best 80 percent of the U.S. population. So, consider the NWSS map of SARS-CoV-2 loads just a snapshot.
The Walgreens COVID-19 Index of national test positivity covers both rapid tests and the more gold-standard polymerase chain reaction tests little available at this point. As of September 29, we see a decline to 21.8 percent of all tests Walgreens processes nationally from 40 percent earlier in the summer, but still as high as most points in the pandemic. The number of tests remains comparatively high, which at this late date in the pandemic may in itself serve as a measure of incidence. People are getting tested because they’re feeling sick.
There’s a geography to this. For late September, we see increases in test positivity in order of sizes of increase, in New Hampshire, Idaho, Oklahoma, Michigan, Pennsylvania and Connecticut, among other states, with New York presently hovering at 35.9 percent positive. These numbers were once available down to the county level until the Centers for Disease Control and Prevention (CDC) abandoned such mapping.
Syndromic surveillance offers another view of the pandemic. We see from Epic Research hospital reports of ICD-10 codes mapped between August 25 and September 7 for COVID infections per 100,000 hospital tests, states in the South and Appalachia are getting hit relatively hard, with the national hospital positivity rate at 16 percent. Hospitals across the U.S. were once required to report in such incidences on a weekly basis. Now only a few voluntarily report.
With such reporting now blacked out, infectious disease modeler J.P. Weiland is using wastewater data from Biobot Analytics and available CDC seropositivities to project COVID cases per day in the U.S. He reports we were at over 589,000 new COVID infections for the single day of September 19.
This summer’s peak isn’t the 5 million infections a day of the first Omicron wave that Weiland estimated in late 2021, but nearly a million infections a day in early August is well within the range of nearly every other COVID peak so far. COVID isn’t tailing off one peak to the next.
Weiland hasn’t released a detailed methodology, which makes the projection’s validity unconfirmed, although the general gestalt of his time series is probably on point. If these estimates are anywhere close to reality, much more forgiving global and U.S. data should now be rated “junk” and the pandemic considered still at strength — especially, as we previously described, as the virus has been given the public health green light to continue to explore its evolutionary possibilities.
Indeed, we see the outbreak stateside continuing to evolve, with a broad mix of 22 sublineages in play, and, as projected September 28, varieties of global variant of concern KP.3 and LB.1 leading the way.
Molecular biologist Raj Rajnarayanan’s 30-day mosaic shows all the genetic sequences of detected sublineages in the U.S. as of September 27, including their geographic origins. We see the near entirety of the country hosting variant JN and its infectious FLiRT offspring, the LBs and KPs 1, 2 and 3. We see the arrival of yet another new lineage, the highly transmissible XEC.
The Real Damage of Long COVID Remains A pandemic’s outcome is a matter of pathogen and host alike. So, while we see the SARS-CoV-2 virus still chugging along, the host population it infects has largely chosen to drop out of the pandemic fight.
While COVID death rates aren’t approaching those of 2020, we are nowhere near a 2019 world as the near entirety of the U.S. establishment pretends. The Swiss Re Institute reports U.S. and U.K. excess mortality rates still at 3 percent and 2.5 percent above pre-pandemic levels.
But here we have both U.S. political parties — and both presidential candidates — placing the ongoing pandemic behind us for good, save for scoring electoral points. The feds are sunsetting bridge funding for COVID antivirals and vaccines, the latter suddenly costing $200 for the uninsured. No wonder, as Science Communications Director Lucky Tran posts, half the Americans in a recent Ipsos poll incredibly expect never to get infected again.
The mass leap away from the reality of a still deadly infection is more from a push from a government that ostensibly holds the monopoly on national health intervention. The U.S. population would likely respond otherwise if signaled so from its elected leadership. Tran reminds us that a 2022 CDC report showed people are more likely to mask when alerted about local outbreaks by public health authorities. Without alerts, on the other hand, Americans are erring on the side of little to no masking.
The resulting health toll continues to beat up the population. Health analyst Mike Hoerger of the Pandemic Mitigation Collaborative — whose models for daily COVID incidences typically run hotter than Weiland’s at 669,000 as of September 30 — projects 1 million to 4 million new Long COVID cases coming out of infections this past month alone.
Previous work showed and estimated that between 5 percent and 30 percent of people infected enter the whirlpool of a Long COVID syndrome for which few tests are available for diagnosis, and there are few prophylaxes available or in development to treat current patients.
A Patient-Led Collaborative Group preprint reporting the results of a survey of 3,300 participants found that increasing the number of SARS-CoV-2 infections a person gets increases the risks of Long COVID, worse Long COVID symptoms and greater overall impairment. Reinfections also appear to diminish the protective effects that vaccination may offer against Long COVID. Few of the surveyed reported Long COVID remission.
The damage extends beyond bodily health. The Wall Street Journal, focusing on the professional-managerial class, ran a story headlined “Long Covid Knocked a Million Americans Off Their Career Paths.”
Understandably, the article was widely retweeted by professionals who lamented their previous 60-hour work weeks and personal bests and marked how far they had fallen. Their work ethic proved no prevention against Long COVID’s siege of microclots, brain damage, cognitive collapse and post-exertional malaise that made some unable to get out of bed for weeks.
Long COVID also impacts many on the other end of the socioeconomic spectrum. A new survey of 7,000-plus adults found low-income Long COVID patients suffered greater food insecurity, especially those who didn’t participate in public food assistance programs.
It isn’t just adults suffering. New research out of the National Institutes of Health’s (NIH) RECOVER program found similar but distinguishable differences in symptoms between children and adolescents among the 5,300 youth it studied, leading RECOVER to declare Long COVID “a public health crisis” for a population some epidemiologists expediently presented as little affected by the infection.
Acknowledging Failures to Keep Them Going Noting that recent COVID deaths in the U.S. were double those of last spring, this New York Times piece from August took a meta view of the failure to see, observing that we no longer observe: “We Have Largely Moved on From Covid, but Covid Isn’t Done With Us” reads the print edition.
But such a gesture at the gap in reality that the newspaper itself helped condition offers the ruling class that effectively ended the COVID campaign permission to continue to ignore the duly noted failure.
The Times interviewed epidemiologists at the highest professional levels about the gap:
"Michael Osterholm, the director of the Center for Infectious Disease Research and Policy at the University of Minnesota, said the newfound complacency can as much be attributed to confusion as to fatigue. The virus remains remarkably unpredictable: Covid variants are still evolving much faster than influenza variants, and officials who want to “pigeonhole” Covid into having a well-defined seasonality will be unnerved to discover that the 10 surges in the United States so far have been evenly distributed throughout all four seasons, he said. Those factors, combined with waning immunity, point to a virus that still evades our collective understanding — in the context of a collective psychology that is ready to move on. Even at a meeting of 200 infectious disease experts in Washington earlier this month — a number of whom were over 65 and had not been vaccinated in four to six months — hardly anybody donned a mask."
And how did officials and the public arrive at such a confusion? After all, other scientists and practitioners standing outside the establishment’s umbrella of respectability debunked the notion that all was well and repeatedly alerted the world to the broader system’s complicit silence.
I wrote in August 2022 that Osterholm himself helped inculcate the confusion:
"Mike Osterholm, who the Times failed to identify as part of the administration’s COVID Advisory Board, converged on this courageous line: “I think [the CDC] are attempting to meet up with the reality that everyone in the public is pretty much done with this pandemic.” A reality the administration worked hard to help manufacture by deft incompetence."
The Times also interviewed epidemiologist Bill Hanage to the effect scientists were themselves confused and that allowed him the freedom of an argument by ex falso quodlibet, a principle from which any proposition can be derived from a contradiction:
"Epidemiologists have long predicted that Covid would eventually become an endemic disease, rather than a pandemic. “If you ask six epidemiologists what ‘endemic’ means, exactly, you’ll probably get about 12 answers,” said Bill Hanage, associate director of the Center for Communicable Disease Dynamics at Harvard T. H. Chan School of Public Health. “But it certainly has a sort of social definition – a virus that’s around us all the time – and if you want to take that one, then we’re definitely there.”"
Ugly sophistry. In actuality, the time series of COVID outbreaks stateside in no way represent the kind of evolutionarily predictable seasonal variants we find in endemic influenza.
And the “socially defined” endemicity to which Hanage alludes was in part of his own making. In one CNN report, we find Hanage alongside Osterholm providing Biden’s CDC cover for dropping recommendations for quarantining at home and testing people without symptoms, brandishing another fallacy:
"Bill Hanage, an epidemiologist at the Harvard T.H. Chan School of Public Health, agrees that the new guidance shows that the CDC is trying to meet people where they are. “I think that this is a point where you actually have to sort of get real and start giving people tools they can use to do something or not. Because otherwise, people will just not take you seriously,” Hanage said."
An appeal to popularity is no epidemiological principle on which to base a response to a pandemic that’s killed anywhere from 1.2 to 1.5 million Americans.
Public Health Rebellion From Below In other words, Osterholm and Hanage and others aren’t the neutral observers they pretend to be, along with the Times.
Rather, they track disease only up to the point the political class can bear, helping bury the problem when it’s inconvenient. Liberals who are upset that science is met with public distrust might ask whether anyone concerned about outbreaks would listen to these brilliant scientists without suspicions they’re catering to other (well-funded) objectives.
How many times will these “men who stare at vaccines” ask us to run into our epidemiological walls — to reference the George Clooney movie about the Pentagon’s First Earth Battalion — as if our reductionist atoms can just pass through those of SARS-CoV-2, avian influenza, mpox, and the queue of other pathogens emerging out of an alienated nature and expropriated circuits of global production?
Vaccines are always only a part of any public health campaign, and their successful deployment depends on the very nonpharmaceutical interventions and structural changes the feds have insisted we abandon.
Figures of authority across local jurisdictions have similarly blanched. Political leaders — turning now to punishing people who continue to mask — are feeding their own health into the COVID maw held agape by establishment epidemiologists.
The best way to contact the dead in the data, these scientist “seancists” signal, is to help usher a public of biased optimists they’ve cultivated to their graves. The CDC continue to invite Americans “just this way, please,” once again adjusting down its color code scheme for its maps to imply we’re in less danger than we are.
Bipartisan rounds of strategic obfuscation follow each new COVID wave as if set as an algorithm. At this end of the U.S. cycle of accumulation, when capital cashes out and disinvests from the public commons, it’s only such manipulation that’s now endemic.
As the Pandemic ThinkTank described early in the pandemic, abandoned by the feds, we need to pursue a revolt from below. Community groups and local public health departments need to work together to reconstruct our public commons to handle the diseases and other disasters already here or on their way.
This article is licensed under Creative Commons (CC BY-NC-ND 4.0), and you are free to share and republish under the terms of the license.
#mask up#covid#pandemic#covid 19#wear a mask#public health#coronavirus#sars cov 2#still coviding#wear a respirator#covidー19#covid conscious#covid is airborne#covid isn't over#covid pandemic#covid19
23 notes
·
View notes
Text
When you type in “inflammation and weight gain” on scholarly search engines, almost every study that comes up swaps “weight gain” to “ob*sity” as a disease. This is because medical research currently operates under the dogma that ob*sity is an illness and therefore must be the chicken. And inflammation, by default, is the egg. Any of my fat patients struggling with an inflammatory illness can tell you: it’s probably the opposite. And as their physician, I stand with them in this suspicion (and in general).
In 2014, researchers from UCLA and Vanderbilt set out to prove us right. (Tip of the hat to them!) They manipulated the genes of mice to make their blood vessels produce more reactive oxygen species, which trigger inflammation. These mice not only had moderate weight gain, but with high-fat feeding, their body mass increased out of proportion. Additionally, they had reduced activity level and energy expenditure, which was believed to be from skeletal muscle dysfunction caused by oxidative stress. Compared to the mice that had the opposite genetic manipulation, high-fat diet did not make them gain weight, and their AT had reduced inflammatory cells. They concluded, logically, that oxidative stress (which happened first) induced weight gain (which happened subsequently).26
In addition to proving that “ob*sity” can be a result of stress/inflammation, the study also elegantly showed two other important points: 1) what the mice ate wouldn’t have caused weight gain if no genetic predisposition to gaining weight was present in the first place, and 2) the ability to exercise and actually spend stored energy were also heavily influenced by genetic makeups. So, were these fat mice “overeaters” or “lazy,” or are those just rodent-blaming terms we used to pathologize fatness?
Ok, I might be getting ahead of myself here because this was a mouse study, not a human experiment. The problem with duplicating such data in humans is that we cannot sufficiently control inflammation or oxidative stress in a study environment. Genetically manipulating humans for medical experimentation is unethical; so is purposely inducing inflammation or stress in human subjects for the sake of measuring weight.
What do we do? Well, it turns out, there is plenty of data readily available to show that inflammation induces weight gain already. We just refuse to believe them.
In 2023, researchers from China used national survey data of over 20,000 patients to study the relationship between weight and arthritis over a 20-year period. Because for those who gained weight over time, their arthritis overlapped with their weight gain in life, the researchers concluded that ob*sity and weight gain increased the risks of arthritis. Even though the study itself admitted that time overlap didn’t mean causality, it still went on to suggest that “weight management throughout adulthood” can be a strategy for preventing arthritis.27 Notably, the study looked at both osteoarthritis – the wear and tear type – and rheumatoid arthritis (RA) – an autoimmune inflammatory disease. The etiology of osteoarthritis might be debatable. But RA has a well-established genetic basis in its cause. And up to 65% of seropositive RA is inherited.28 Therefore, unless “weight management” can alter genetics, it’s entirely plausible that the patients who had RA had RA-related inflammation first (because of their genetics), and the weight gain followed second.
Additionally, if you really investigate the data of this study, you will see that it actually found a “U” shaped association between absolute weight change and the risks of developing arthritis: the arthritic risks went up for both people who gained weight and lost weight over time. Plus, among those who went from “ob*se” to “non-ob*se” over 20 years, their arthritic risk did not change, at all. To me, these two results contradicted each other. The first said that losing weight can increase the risks of arthritis. Yet the second said when the weight loss is significant enough for a person to drop BMI categories, their arthritic risk didn’t change. That’s interesting: because either weight loss induces arthritis, or it doesn’t have anything to do with arthritis. But they can’t both be true! Unless…arthritis happens regardless of weight change, or BMI is a bad measure of weight. Or both.
9 notes
·
View notes
Text
This tbh.
“Nothing lasts forever” holds two very different meanings when you’re in a flare vs in remission.
#chronically ill#disabled#chronic illness#fibromyalgia#seropositive rheumatoid arthritis#rheumatoid arthritis
81 notes
·
View notes
Note
"waa waa snape outed remus as a werewolf"
ok i think the reason the fandom reacts to this the way they do is that they think werewolfism is an allegory for being gay (this is why so many hate remus/tonks, and ship remus/sirius) rather than an allegory for hiv - a devastating virus that will kill the patient but which is only spread under very specific conditions. the aids epidemic didn't reach its peak until 2004, and there wasn't even any treatment for slow the progression of hiv to aids until 1997, but it was well known before that time that you couldn't catch hiv just be being around seropositive people - even if bigots acted like you could. THAT is what remus is meant to represent (this was a very important lesson for children to learn at the time the books were being written, i remember having countless assemblies and lessons about hiv in the 90s). the majority of people with hiv are heterosexual, and most are women. only white anti-gay bigots think hiv is a ~gay disease~ and that therefore remus must be gay and any anti-remus character must be homophobic.
it's not "remus is gay and needs to lose his job", it's "remus has hiv and it was fine up until he negligently exposed children to his bodily fluids, so now he needs to lose his job".
(the way this fandom assigns incorrect meanings to very obvious allegories drives me insane. like people thinking house elves are meant to represent slavery when it's very obvious they're meant to represent battered housewives doing constant unthanked and unpaid domestic labour, with everyone ignoring their bruises and injuries, and when someone does try to help they get told off for being a busybody and not minding their own business. like, their liberation movement is the same acronym as the feminist movement! it's so on the nose a child is supposed to be able to pick up on it. and yet this fandom is like "hurr durr it's slavery and you're meant to think hermione is wrong for trying to end it!!!".)
!!!!! this !!!! all this !!!!
16 notes
·
View notes
Text
Important study published today investigating why some people develop #LongCovid
The most striking finding is a massive disconnect between the humoral (B-cell) and cellular immune (T-cell) response in Long COVID patients.
In summary, these two systems should work together to take care of the virus: the B-cells attach themselves to viral particles to block the virus from entering the cell, while the T-cells kill cells that get infected.
These two systems are coordinated in the recovered COVID patients but not in the Long COVID patients.
Half of the Long COVID patients who produced coronavirus-specific T-cells produced no antibodies to the virus.
Putting all the pieces together, Long Covid patients present a highly inflammatory state, probably driven by immune dysregulation.
With 3 ongoing big NIH-funded T-cell studies underway (Mark Davis at Stanford, Selin-Gill Harvard, Derya Unutmaz at Jackson labs), T-cells are potentially a big deal in ME/CFS. We need to remain optimistic about it!
17 notes
·
View notes
Text
When I was growing up, Thanksgiving was never a time for family. We never went to relatives houses and we never hosted my grandparents or cousins or aunts and uncles.
My parents were the only married couple with kids in their friend group. A big part of this was that they both worked in theater, and so many of their friends were queer and in the early 2000s it was difficult for queer people to make their own family, and common that they would be shunned from the one they were already a part of.
So my mom always had our doors open on Thanksgiving to what she called “the strays.” There were a couple of pillars at every Thanksgiving, people who would come every year. But they were always encouraged to bring their friends as well, anyone who didn’t have a place to go to spend the Holiday. We had so many characters across the years. One year we had the designer of a Malibu Barbie come and he and I were both delighted to learn that I had that same Barbie, and we played together after dinner. Another time we had a man who had immigrated from Sri Lanka only a couple months before, and was bewildered but excited to be experiencing an American Holiday.
But maybe the most impactful guest we ever had was a man named Timothy. He was a professionally trained French chef, and he made us a beautiful roast duck that I did not eat because I was four and thought turkey was an ok bird to eat but duck was not. Everyone else loved it of course. Timothy was with us that year because most of his family had disowned him after he came out, and the rest did after he learned he was HIV+.
Before and after dinner I asked him if he would play with me, and he was hesitant to say yes. My family knew of his seropositive status, he felt it was important to disclose it to people before they welcomed him into their homes. He knew that many people would be uncomfortable with an HIV+ man playing with their young child, so he asked my mom’s permission.
She of course said yes, there was nothing about playing with dolls that would transmit the disease, and him having it did not make him an immoral person that could not be trusted around children. This was the first time anyone had expressed that sentiment to him in years, and he broke down into tears. He told my mom that he had always been excited to be in the children of his family’s life and it was so hard to be told he couldn’t. And then we played for the whole evening.
That Christmas when we sent out cards, my mom asked me to make one for him, since he’d played with me and kept me occupied so she could cook.
Early the next year, my parents received this poem/letter in the mail. [Transcript in alt text]
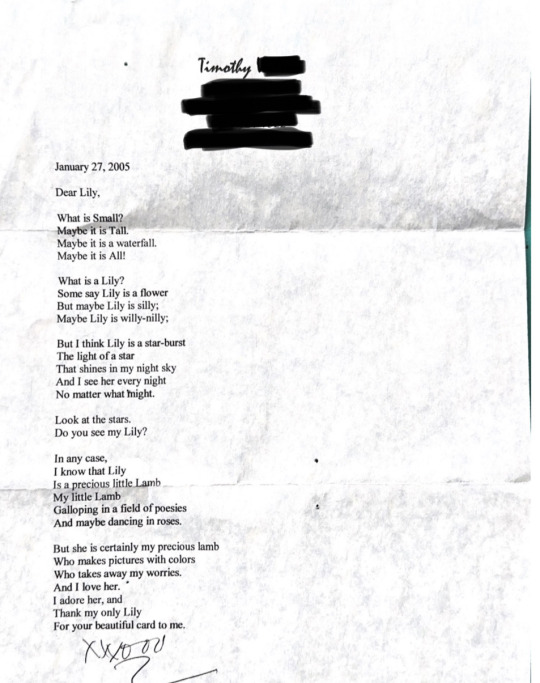
I did not remember much of this story or this day or this man. But my mom told me about him years later, and gave me the poem she had kept for me. Timothy died a couple years ago from complications due to AIDS. I regret that we did not keep in closer contact with him throughout my childhood and I wish I could tell you more about him than this story.
Ever since I learned of his life, and his death, the meaning of Thanksgiving has changed for me. Thanksgiving is not about family, it is about community. It is about providing for those in our vicinity who need it. It’s about mourning those who were not given it. I ask everyone who reads this today to not only grieve our indigenous brothers and sisters, for they certainly deserve the thoughts and attention, but also all of the people left behind by our neoliberal society. Those people abandoned by the nuclear family and the non-existent social safety net. Those who lost their lives as victims to state-sanctioned violence. Please remember your unhoused siblings, your disabled siblings, your undocumented siblings, your refugee siblings. And please open your homes to anyone you know who needs a warm meal in their bellies and a small act of kindness in their hearts.
27 notes
·
View notes
Text
Last pinned was out of date! Hello!
I don't feel like using dictation so I'm summarizing myself with bullet points.
Name: Rid
Age: 26
Nonbinary
Bisexual
Engaged
Cane user (RA, fibro, general chronic pain)
Mentally ill
I have 3 cats.
420 friendly, learning about cannabis cultivation
Read more below
Music taste
Motionless in white
Alpha wolf
Silent planet
Bad omens
Sleep token
My chemical romance
Lil Aaron
Lil peep
Grandson
Bloodveil
Dangerkids
Escape the fate
Dayseeker
Hobbies
Gaming
Writing
Reading
D&D
Games I like
Pokemon (most of them, fave gen is 2 & I shiny hunt a lot)
Dead by daylight
Silent hill 2
Skyrim
Elder scrolls online
Dragon age
Resident evil
I'm still figuring out what I want to do with my career at the moment bc current state of the USA is not looking so good for my career path and I'm low-key annoyed with the field and how things are handled within it. I still wanna write though and am working on a poetry book draft.
#poetry#bpd#writeblr#fibromyalgia#seropositive rheumatoid arthritis#chronic illness#poetry writing#poets corner#bpd blog#chronically ill
3 notes
·
View notes
Text
When a government turns its back on its people is it civil war?
No pride month is complete without remembrance of all those who died of AIDS under governmental neglect. Between the 21st and 24th of June 1990, the Amsterdam cultural center Paradiso hosted the Seropositive Ball, which lasted 69 hours and took place at the same time as the San Francisco International AIDS Conference. The following are a number of quotes from the Gran Fury collective presented at the Seropositive Ball.



Source: Paradiso Archive at the International Institute of Social History
2 notes
·
View notes
Text

For Disability Pride Month, here's another disabled OC: Gabriel!
As a teen, Gabriel had conduct disorder which later developed into ASPD (antisocial personality disorder). He's quite the troublemaker because of this, but ultimately his behavior issues come from trauma. Mainly, abandonment and neglect from his parents who left him with a physically abusive uncle.
Their ASPD also makes them very rebellious and risk-taking, once leading them into a drunk car crash (Gabriel wasn't the driver though) where they broke their collarbone and jaw. It causes minor chronic pain as an adult too.
Gabriel also struggles with alcohol addiction (related to his ASPD and trauma) and is promiscuous. His risk-taking combination of both of these leads him to contract HIV, so his story is also one of living as a chronically ill and immunocompromised person. Not to mention, it's way to rare to see seropositive OCs!
#gabriel#original characters#ocs#oc art#aspd#trauma disorder#disability#mental illness#mentally ill character#characters#character design#watercolor#watercolor artist
10 notes
·
View notes
Text
MMWR Booster #21: SARS-CoV-2 Serology and Self-Reported Infection Among Adults — National Health and Nutrition Examination Survey, United States, August 2021–May 2022
Top 5 Takeaways
1. 41.6% of adults had antibodies indicating past SARS-CoV-2 infection during August 2021–May 2022, with 43.7% potentially asymptomatic. 2. Seropositivity without vaccination was more common among younger adults, Hispanic and non-Hispanic Black adults, and those with less education. 3. The NHANES data suggests disparities in COVID-19 infection rates and vaccination, especially among minority groups. 4. Preliminary NHANES data indicates disparities in seropositivity patterns, with higher infection rates and lower vaccination rates among specific demographic groups. 5. The findings emphasize the need for equity in COVID-19 vaccination efforts, as NHANES data offers more representative insights into asymptomatic infections and vaccination status.
Full summary link: BroadlyEpi.com
Enjoying these summaries? Check back every day at 8am and 4pm Pacific Time (UTC - 8) for a new MMWR Booster. A reblog would also be greatly appreciated, and thanks to everyone who already has! BroadlyEpi hopes to make Epidemiology and Public Health more approachable to anyone who's interested.
2 notes
·
View notes
Text
The River in Winter - Matt Dean
I am completely bewildered by the book I just finished. It was presented as a sort of "learning to love again" literary romance where a man is torn between two very opposite love interests (trite, I know).
However, it turned out that one of them is barely present at all and the other is actually the self-proclaimed counselor of an extra sketchy ex-gay group based out of his home? The main character somewhat inexplicably falls in with the latter almost immediately and spends the majority of the book seriously engaging with an attempt to renounce his homosexuality???
I kept waiting for him to critically assess his situation (or else have someone snap him out of it) but he literally did not come to his senses until the very last page of the very last chapter after the most over-the-top scene possible with the counselor.
Meanwhile, the barely-present opposite interest was setup to exist in the background as some leering, caricaturesque avatar of "degenerate" sexuality. In the penultimate chapter, he finally visits again (after disappearing for 50% of the story), seduces the MC all over again, and then announces that he is seropositive in the middle of unprotected sex with him.
This was all dizzyingly absurd in so many ways. The author includes enough detail to point readers toward where he really stands but I almost couldn't believe it wasn't a kind of Log Cabin Republican fanfiction of a Chick tract at times.
At the very least, it concludes with an epilogue showing that MC has successfully anchored himself to the positive actors in the story again and is back on a good path in life...
4 notes
·
View notes