#rifampin
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
After the announcement of the deal with Yahoo!, there were 170K signatures of unhappy Tumblr users petitioning to prevent the sale in 2013.
Note
Rifampicin (and the class of rifamycins as a whole) were named after a French noir film, Rififi (1955). Rifampicin itself stands for Rif-AMP-(m)icin, with AMP referring to its N-amino-N′-methylpiperazine substitution.
Who says we can't have the pharmaceutical equivalent the sonic the hedgehog protein.
That’s hilarious and when I design this med I will absolutely base it on said movie as well. Bros gonna have a fedora or something.
Also Rifa over here is another member of the “biblically accurate angel looking skeletal structure” club along with Vitamin B12


0 notes
Text
i need to restart my probiotics im doing irreparable damage to my guts
#dont get on rifampin for prolonged periods of time#i was taking it so consistsntly for like 6 months and then everything got screwed up#at least ive been taking my nystatin so that helps#the horrors of longterm antibotics is creeping up on me#.txt
2 notes
·
View notes
Text
incredibly proud of myself for the other day at work when i had to write down a medical word someone said and got it right. like i DID spell it wrong but it was phonetically 100% correct and that’s a win
#rifampin which i wrote down as ryphampin…#i’m used to someone being like ‘glucose’ and me being like ‘did u say blublose?’
4 notes
·
View notes
Text
Hey, I felt like I might be wrong about something here, so I double checked and yep! I was 100% wrong about it being antivirals: its actually antibiotics. The two antibiotics are rifampin (turns things orange) and isoniazid (damages your liver). And thats just for what's called "latent TB" which is essentially the asymptomatic version of TB where you're not infectious or contagious, but the TB is in you and could reactivate.
For ACTIVE infections, you actually have to take BOTH of those meds, PLUS pyrazinimide and ethambutol, but only for the first few months, and then you take just the rifampin and isoniazid together for the rest of the time.
So sorry for the error, but I hope anyone interested in the correction sees this update. Stay safe out there
the anti-quarantine (a method of disease spread management known to be effective for several thousand years atp) hysteria is so bad that I’ve seen people push back on quarantining mandates for people with active TB infections. I really think we’re heading towards extinction atp.
#again: the liver damage IS FIXABLE but boy howdy will you have a bit of a bad time in the interim#if you have the choice: choose the rifampin
96 notes
·
View notes
Text
MDNI tw: baby trapping and manipulation. GazxReader fluffy-dark one-shot.
Kyle is ready for a baby, so when he sees his chance he just can’t resist. And he knows how he’s going to make you an enthusiastic, albeit unknowing, participant.
He was ready.
It’d been a long time coming; you and he had had your ups and downs and always came out stronger on the other side, together. Always together. It was you and him until the end.
You were such a perfect partner for him, practically handmade to fill in all his rough edges and he never let you forget how much he adored you. He bragged about you any time you came up in conversation and wasn’t shy about crowing your achievements from the rooftop.
Your friends were over the moon at your relationship. Every time you met up for brunch or movie nights you would field at least 3 comments about where they could find their own head-over-heels partner.
You had been sick for a few weeks before you finally went to the doctor.
“Tuberculosis.” you rasp to Kyle on the other end of the phone. “They prescribed me some heavy duty antibiotics called rifampin that are the size of horse pills!” you hold the prescription bottle up towards the light and shake the tablets around in disbelief.
Kyle just laughs into your ear, well aware of how much you disliked needing to take large pills. It had been brought up every time one of you got sick throughout your relationship. You insisted that they got stuck in your throat and stayed there for hours before finally dissolving, no matter what Kyle tried to say. He used it as an excuse to brew your favorite tea and pamper you more than usual whenever you had to take them, so he never tried to argue too hard.
“I miss you . . . wish you were here,” you croak, making your way to the couch to relax and try to catch your breath. Your lungs felt physically tired as you tried to breathe. It was a unsettling feeling. Panting lightly, you pulled the blanket off the back of the couch and cocooned yourself, relaxing back into the cushions.
“I know sweetheart. I wish I was there too. I would make you that soup you like and rub your feet while we watched a movie. You wouldn’t have to get up for anything.” The line crackles and breaks for a few moments before clearing up again. “Just a little bit longer, love, and I’ll be able to come home. It’ll be before you know it.”
“I miss you Kyle.”
“I miss you, sweetheart.”
. . .
When the call ends Gaz immediately looks up the medication you said you were prescribed. Rifampin. He’s never had tuberculosis and he wants to verify that this is the standard treatment and if there are any side effects to watch out for. While he isn’t in the country right now he’d figure something out if you needed him back quickly.
Fingers which had been swiping steadily, reading warnings and side effects with the same attention to detail as to mission reports providing intel before an operation, slowed and then stopped as he continued to read. After a moment his screen goes dark and your future shifts and locks into place on the other side of the world.
. . .
It was edging into evening just over a week later when the front door swings open and in steps Kyle. You immediately throw yourself into his arms and begin fussing, hugging him and checking for any new injuries at the same time. He just laughs and squeezes you back tightly. “I’m fine love, just happy to be able to hold you again.”
After sorting out the immediate concerns you tumble into bed, cuddling face to face and sharing a pillow, sharing breath. You’re not sure who kissed who first but you’re both tied for ardor. Your tongues tangled together as hands slide under clothes and down pants. Before things got too involved you pulled back to look at him. “You’re going to have to pull out. This medicine can affect my birth control so you can’t come inside me okay?”
He nodded eagerly as he began to pull your shirt up your torso, fingertips dragging along skin in their own version of a kiss. “Pull out, got it.” He said distractedly, glancing down at the skin and softness he was uncovering. Before you knew it you were both naked and he moved his way down your body, taking his time to slowly work you up. Spending time nibbling along your coller bones, sucking a bruise into the hollow of your throat, tonguing around your neck to the other side to continue.
What follows is hours of pleasure and torture in equal measure. Kyle has never been a stingy lover but tonight it’s like he has something to prove. He brings you to your peak again and again and again . . . and then he holds you there.
While the two of you had dabbled in edging before this, it had never been to this extreme. Tonight had been hours of cruel pleasure, the sheets under you were damp with sweat and you were sobbing with your hands buried in his hair.
“Pl-please,” you hiccup on a sob “I need to come. Please let me-let me come.” you beg him, trying to maintain eye contact through your tears. He currently had three fingers buried deep in your cunt and his lips suctioned to your clit.
His lips pop off with a slurp and you yelp.“Do you need it, baby?” He grins with a feverish gleam in his eyes. “You ready to come?” You nod eagerly, blinking and causing the tears to spill over your lash line.
“Please, please I’ve been good. I’ve been so good, please let me come.”
“God you beg so pretty baby. Okay, but I want to come together.” He climbs to the head of the bed and lays on his back. He grabs you by the hips and helps you climb on top, slotting himself back at you entrance. “Come on, up on top love, thats it.” he babbles as you sink to the base and gasp at the feeling of being stuffed full. “Yes, Just like that, just like that.” is wrung from his throat as you squeeze him tightly.
You begin to pump your hips, pulling away from him before bringing yourself back down but you quickly lose steam. It had been hours at this point and you were on your last legs.
“I know.” Kyle coos condescendingly, brushing the back of his knuckles over your cheek, wiping away tears, sweat and drool. “I know sweet thing, you’re so tired. It’s gonna be okay. Look, I’ll help you.”
He reaches both hands down to your hips, digging his fingers into soft skin and plush rolls. His fingertips causing divots where they press into the fat of your hips. He pulls you into a grinding motion, “Doesn’t that feel good baby? Me holding your hips just right, helping you grind back and forth?”
You nod dumbly, brain fried and only able to think of how good he feels inside you. He drops one of his thumbs down to find your clit, giving it steady, smooth circles to help you finish.
“Yeah? Right there? I can tell it’s good just by your face. I love that fucking face that you’re making.” His mouth begins to run, words dropping out with no prior planning. “If I could tattoo it behind my eyes and carry it around with me for the rest of my life I would die a happy man. You make me so damn happy baby.” He grunts as he begins to move your hips faster, grinding you down firmly against him. “I want you forever, do you hear me? Forever. It’s you and me okay? Yeah, you’re getting close? I am too, love. Mmmm fuck. Just like that, keep rocking your hips baby and you’re gonna make me come. God you’re taking me so well. Tucked up, deep inside you.” His jaw clenches and he pulls you as tightly against him as he can.
“Fuck. I’m gonna come love. You’re gonna make me come.” His words stutter to a close as you continue to grind, chasing the final edge. You could feel it tingling up your legs, across the backs of your thighs.
“Im so close,” you pant, head tilted back, eyes closed, unable to think of anything accept the feel of his cock bumping into your soft walls, creating sparks of pleasure. “Don’t stop baby. I’m so close. I can’t stop. Please”
A groan punches out of Kyle and his grip turn tight enough to leave fingerprint bruises to find in the morning. “If you don’t want me filling you up, you gotta get off baby. I know you’re close but you’re gonna make me come. You told me to pull out just to, just to be safe. I can’t-i cant hold it baby. You’ve gotta get - get off or it’ll all be inside.”
He starts to stutter and lose rhythm still pulling you into him, rubbing your clit with his thumb.
You don’t hear him. A roar is building in your ears, a white noise type of hum that is blocking out everything else. You can feel your release digging its claws into you down to your bones as it gets ready to wrench you from your body.
Your knees begin to shake from their place beside Kyle’s hips as you finally get what you’ve been working towards for the past however many hours. Your vision whites out and your mind blanks.
You clench around Kyle’s cock. warm gummy walls pulsing around him, drawing him inside. You’re grinding down on him as hard as possible, his tip pressed against the back of your channel.
His eyes hold an unusual gleam right before he closes his eyes and tilts his head back, groaning his release as he pumps everything inside of you.
Later when you’re spooned together, his arms wrapped around your waist and legs tangled together, you don’t notice him cupping his hand around your lower stomach. He falls asleep with a smile on his face as he imagines his future together, with all three of you.
Next || Story Repository
#nobody look at me#jk I actually love this#we need more gaz fics in the world#this handsome man can make all the babies he’d like 🥵#you just know they’d be cute#fanfic#cod#kyle gaz x reader#kyle gaz garrick#kyle garrick#simon riley x reader
177 notes
·
View notes
Text
Medblr, I think we ought to have an antibiotics bracket. Just for fun. Everyone can submit their favorite antibiotic regimens and write propaganda for them (or anti-propaganda for the ones you hate) before we crown the one true antibiotic (regimen). Doesn’t have to be a single medication, it can be a combo. Here’s some of what I’m thinking of including:
vanc/zosyn
Azithromycin
Amp/gent
Rifampin/isoniazid/pyrazinamide/ethambutol
Augmentin
Cephalexin
Vanc/ceftriaxone
Amphotericin
Nitrofurantoin
Vote however you want—what you prescribe most, best side effect profile, most interesting mechanism, vibes, whatever. Let me know what other antibiotics you think I should include!
#just for a lark#antibiotic bracket#medicine#medblr#pharmacy#pharmblr#antibiotics#medication#medical school#med school#med student
71 notes
·
View notes
Text






Volume 1: Isolation
First - Previous - Next - Last
Quick Mod Note: The rifampin turning body fluids side effect is normally noticed when the urine turns that color. I decided not to go that route because, while it's medical in nature, I'd rather not risk having the Tumblr mods/admins/whoever flag the related entry. Also, some people on this hellsite would ask way too many questions about it in the wrong way. Anyway, the body fluid color change side effect is pretty interesting because it actually means the drug is working! More to come about all the "fun" side effects that can occur from multidrug TB treatment.
#mlp ask blog#nurse redheart#quarantined redheart#earth pony#mlp g4#pony ask blog#mlp fim#volume 1: isolation#my little pony friendship is magic#my little pony#dr. stable#unicorn
43 notes
·
View notes
Note
Has this been killed and subsumed by Ask Quarantined Redheart?
Okay, I do feel like this does need to be addressed. The short answer is not quite but Ask Poke Eosin specific posts continuing forward are going to require a major change in the blog. Keep reading for the very long, probably rambling answer.
When I started the blog, I was on my holiday break after my first semester of my first year of medical school. My mental health wasn't quite in the toilet but it was getting pretty close. I think a lot of it had to do with the fact that I was struggling to get my studying flow down while still maintaining my hobbies, especially drawing. Couple that with getting depressed/burned out right at the end of that semester while binging Firestarter Spitfire/The Sunjackers and the decision to make this ask blog came about mid-ish December 2022. So I have this blog to thank a lot for helping to make my drawing hobby more consistent.
Now comes the part where I have to take an honest look at what I meant for it to be and where I'm at now. The original intent of the blog was to be this sort of educational blog about the current state of evidence based medicine and stuff that happens/happened to me during medical school, training, and onwards. That second part is the biggest problem. Poke is essentially me, the mod. The "Clinical Quiz" arc from a year or so back is something that happened to me and the way I (mostly) present it is how I tell the story to people in real life. While I doubt any of my colleagues care enough to dig deep for this blog, I still am dancing a little too close to doxing myself with the way the blog is currently.
Perhaps most importantly, I started my third year rotations back in the beginning of August. Pretty much the culmination of all the basic science lectures from the first two years, finally seeing actual patients! I soon realized, though, that I can't present these patients to the masses of the internet, even if they've been redrawn as cute technicolored magical ponies. Not just because of HIPAA issues but just because of the fact that just by going to the doctor and having a medical student like me asking them questions that they'd never answer in any other context. They are vulnerable and I feel like it would be unethical to present them as entertainment. I wouldn't necessarily be against drawing patient presentations but I would seriously need to figure out how to do it without revealing too much.
And finally, perhaps a more selfish reason: I feel like folks like Quarantined Redheart more. The project got its inspiration from a pharmacology lecture about tuberculosis medications during my second year. The fact that TB patients are required to quarantine for at least two months, Rifampin's red/orange body fluid quirk and it causing certain drugs to be metabolized faster, and a third plot point that I won't reveal just yet all came from that lecture. Originally, Quarantined Redheart was supposed to be a side project. The more I worked on it and the more that I fleshed out the plot and its characters, the more I came to love working on it to the point that I'd hesitate to call it a side project anymore. It also gave me the opportunity to say some stuff about the current state of healthcare that I feel like I couldn't do with what is essentially a self insert OC. Seeing that people really do seem to like the story that's being told made turning Quarantined Redheart into the main project a little easier. Is that a great reason to focus one's attentions on a project? Probably not. But it's also the curse of the artist: I draw what I want but the Notes notifications on my dash also lets serotonin stay in the synaptic cleft a little bit longer.
So is Ask Poke Eosin dead? I'm hesitant to say "yes" on that. I think there'll be more shitposts and random educational stuff than any of the full blown patient care stories that I originally thought I'd be doing. But I need to figure that stuff out for sure. Is Ask Poke Eosin dead? Nah. It's just hibernating right now.
5 notes
·
View notes
Note
Sirius black or if you want to practice a pedi ? - how about James Sirius?
Good luck - 🍀
Sirius - TB is a common disease that incarcerated patients obtain. Oh man there is so much to say about TB. Sputum stains acid-fast. There are two tests, the blood test, Quantiferon Gold Assay and the PPD skin test. If a patient has HIV, then an induration <5 then it is positive, At risk (health care workers), are positive <10mm, general population <15 mm. PPD tests are positive in latent, active, and those who have been vaccinated with the BCG vaccine, so a confirmation for an active infection needs to be done with a chest xray. Inactive TB is treated with 7 months of isoniazid and pyrazinamide. Active TB is treated with RIPE - Rifampin Isoniazid, Pyrazinamide, and Ethambutol. Side effects include red piss (rifampin), elevated Liver enzymes, sideroblastic anemia (isoniazid), B6 deficiency, red green colorblindness, and others.
James Sirius has ADHD. Diagnosis needs to be made at 2 different settings for >6 months. So most kids get diagnosed from input from their teacher at school and their parents at home. Hyperactive activity and distractibility. Treatment (which I needed to review!): First line is CBT and stimulants, methylphenidate and amphetamines. Those are considered controlled substances, so if the parent does not want them to have a controlled substance, can treat with nonstimulants like atomoxetine and alpha 2 blockers.
9 notes
·
View notes
Text
The medicine was dismal this time around. House is convinced Anica has Cushing’s — and the symptoms did support it — but never checked a cortisol or ACTH level: the tests that prove the condition, no matter the size of the tumor. Rifampin was a poor choice of drug for Cameron to fool the patient with as it has some nasty side effects. There are safer drugs to use to turn someone’s urine orange. Even more damning was the fact that Anica was started on radiation without a bone marrow biopsy to prove that she had aplastic anemia in the first place.
Just another day at the medical malpractice factory
5 notes
·
View notes
Text
The antiviral drug Rifampin causes orange urine, as well as orange bodily fluids in general! Not to drag them into this for no reason but @moggat had to do a course of rifampin a few years ago and would text me pictures of, like, the toilet after they'd peed and tissues after they'd blown their nose, and it was always this bright-ass almost fluorescent orange. Peak comedy, tbh.
Also if you eat a shit-ton of asparagus or broccoli, your urine sometimes gets a green tint to it.
79K notes
·
View notes
Text
Silent Liver Damage: How Common Medications Can Affect Your Liver Health

Your liver works tirelessly to filter toxins, process nutrients, and metabolize medications. However, certain medications, when overused or misused, can silently damage your liver over time. This often goes unnoticed until serious complications arise. Many people assume only alcohol or viral infections harm the liver, but even everyday medicines can have a lasting impact.
How Medications Can Harm Your Liver
Most medications are processed through the liver. Some may cause drug-induced liver injury (DILI), leading to inflammation, scarring, or even liver failure. While some damage is reversible, prolonged exposure to harmful drugs can lead to chronic liver conditions.
Unexpected Culprits Behind Liver Damage
Pain Relievers (Acetaminophen/Paracetamol) – One of the most common causes of acute liver failure worldwide, especially when taken in excessive doses or combined with alcohol.
Antibiotics (Amoxicillin-Clavulanate, Rifampin, Tetracyclines) – While treating infections, some antibiotics may also trigger liver inflammation.
Statins (Cholesterol-Lowering Drugs) – Though effective for heart health, these drugs can sometimes elevate liver enzymes, leading to potential liver stress.
NSAIDs (Ibuprofen, Aspirin, Naproxen) – Overuse can lead to liver inflammation, especially in individuals with existing liver conditions.
Antidepressants and Antifungal Medications – Certain drugs used for mental health or fungal infections may interfere with liver enzyme function.
Herbal Supplements & Ayurvedic Medicines – Many people assume herbal remedies are safe, but some contain toxins that can severely affect the liver.
How to Recognize Liver Damage Early
Unlike digestive issues that show immediate discomfort, liver damage progresses silently. Watch out for these warning signs:
Persistent fatigue and weakness
Loss of appetite and unexplained weight loss
Yellowing of the skin and eyes (Jaundice)
Abdominal pain or swelling
Dark-colored urine and pale stools
Nausea and vomiting without an apparent cause
How to Protect Your Liver from Medication-Induced Damage
Follow dosage guidelines – Never exceed recommended doses, even for OTC medications.
Limit alcohol intake – Alcohol worsens medication-induced liver stress.
Stay hydrated and eat a balanced diet – Proper nutrition supports liver regeneration.
Get regular liver function tests – If you’re on long-term medication, periodic testing helps detect early damage.
Consult the Best Gastroenterologist in Vadodara for expert guidance.
Seeking the Best Liver Care in Vadodara
If you suspect medication-induced liver damage, timely medical intervention is crucial. At Desai Surgical Hospital, the Best Gastroenterologist Hospital in Vadodara, our expert team provides advanced care, including Jaundice Treatment in Vadodara, Best Acidity Treatment in Vadodara, and Best Gastric Disorder Treatment in Vadodara.
Contact Us for Expert Liver Care
Location: Desai Surgical & Eye Hospital, Near G.P.O, Kharivav Road, Dandia Bazaar Rd, Raopura, Vadodara, Gujarat 390001 Phone: 0265 2435153 Email: care@desaisurgical.com Social Media: Facebook | Instagram | YouTube
OPD Timings: Monday - Friday: 12:30 PM - 02:30 PM | 06:00 PM - 07:00 PM Saturday: 12:00 PM - 02:30 PM Sunday: Closed
24/7 Emergency Services Available
Your liver’s health is in your hands. Take precautions and consult the Top Gastroenterologist in Vadodara at Desai Surgical Hospital today.
#LiverHealthMatters#MedicationAwareness#SilentLiverDamage#DesaiSurgicalHospital#VadodaraGastroCare#ProtectYourLiver
0 notes
Text
Drug Monograph FOR SERIOUS INFECTIONS ONLY Drug Monograph: Vancomycin Drug Name -- Vancocin (brand), Vancomycin HCL -- oral (generic) This is a time-dependent bactericidal antibiotic, which inhibits cell wall synthesis (Levinson, 2009). Glycopeptides VA Class - AM900 CAS Number 1404-93-9 Therapeutic Category -- a tricyclic glycopeptide antibiotic Pharmacology Vancomycin is not too well-absorbed from the GI tract after oral administration (Levinson 2009). When given parenterally, it penetrates the bile, pleural, pericardial, synovial and ascitic fluids. It is excreted unchanged by glomerular filtration (Levison). When taken orally, Vancomycin is not absorbed in the intestines so that it can stop the growth of a severe intestinal condition known as Clostridium difficile-associated diarrhea (Medicine Net, 2012). When vancomycin is given by mouth, it is not absorbed by the body but remains in the intestines. This is to allow it to stop the growth of the Clostridium difficile bacteria. Vancomycin is intended as treatment only for bacterial infections of the intestines. It is not effective for other bacterial infections or infections caused by viruses. Its overuse can decrease its effectiveness (Medicine Net). Indications Vancomycin is intended for the treatment of serious or severe bacterial infections caused by susceptible strains of methicillin-resistant staphylococci (PDR, 2012, Drug.com, 2012). It is indicated for use by patients who are allergic to penicillin and cannot or fail to respond to other drugs. It is for infections caused by Vancomycin-susceptible organisms resistant to other anti-microbials. It is indicated as initial therapy when methicillin-resistant staphylococci infection is suspected. It is also effective in the treatment of staphylococcal endocarditis. It has been successfully used in combination with either rifampin or an aminoglycoside or both for early-onset prosthetic valve endocarditis, caused by S. epidermidis or diphtheroid. Its parenteral form may be administered orally in treating antibiotic-associated pseudomembranous colitis caused by C. difficile and for staphylococcal enterocolitis (PDR, Drug.com). Vancomycin is the drug of choice against serious infection and endocarditis caused by Methicillin-resistant S. aureaus, Methicillin-resistant coagulase-negative Staphylococci, Streptococcus pneumoniae, B-Hemolytic streptococci, Corynebacterium group JK, Viridans streptococci and enterococci (Levinson, 2009). It has been used as an alternative drug for pneumococcal meningitis caused by strains with reduced penicillin sensitivity. But its erratic penetration into the CSF and reported clinical failures make it not advisable for use alone to treat pneumococcal meningitis. Dosages For Adults The usual is 500 mg by IV every 6 hours or 1 g by IV every 12 hours (PDR, 2012). It should be administered no more than at 10 mg per minute or at least 60 minutes, whichever is longer. For those with renal impairment, the initial dose is not less than 15 mg per kg. The daily dosage is about 15 times the GFR in ML per minute. For elderly patients, the dose should be reduced. The initial dose for anephric patients is 15 mg/kg then 1.9 mg/kg/24 hours. The dose for those with marked renal impairment is 250-1,000 mg once every several days and for those with anuria, 1,000 mg every 7-10 days. For PO administration, divided doses of 500-2,000 mg/day should be given for 7-10 days or a maximum dose of 2,000 mg/day. The doses may be diluted in 1 oz of water or administered through an NG tube (PDR). Vancomycin is taken orally usually 4 times a day for 7-10 days according to the doctor's instructions (Medicine Net, 2012). He determines the dosage according to the medical condition and the patient's response to treatment. Cholestyramine and colestipol can lessen the effects of Vancomycin when they are taken at the same time. If they have to be taken, they should be given at least 3-4 hours from Vancomycin. Vancomycin works best when kept at a constant level at the intestines. Medication should be continued until the prescribed amount is completed even if symptoms have disappeared. Re-infection can occur if the medication is stopped before completion. If the condition persists after 7 days or gets worse, the doctor should be informed (Medicine Net). For Pediatric Patients The usual does for all pediatric patients is 10 mg/kg by IV every six hours (PDR, 2012). The initial for newborns is 15 mg/kg, followed by 10 mg/kg every 12 hours for the first week of life. This is continued every 8 hours until their first month of age. Vancomycin should be given for at least 60 minutes. The initial dosage for pediatrics with renal impairment is not less than 15 mg/kg per day or 15 times the GFR in mL/min. Premature infants should have longer dosing intervals. PO administration should be 40 mg/kg/day in 3-4 divided doses for 7-10 days. The maximum is 2,000 mg/day, which may be diluted in 1 oz of water or administered through an NG tube (PDR). Contraindications Vancomycin is contraindicated to patients with hypersensitivity to vancomycin (Drug.com, 2012). Commercially prepared frozen Vancomycyn Hydrochloride injections in 5% dextrose may also be contraindicated to those with known allergic reaction to corn or corn products (Drug.com). Drug-Drug Interactions The patient should inform the doctor or pharmacist of all prescription and non-prescription or herbal products currently used (Medicine Net, 2012; Levinson, 2012). Aminoglycosides, amphotericin B, other antibiotics, and live bacterial vaccines are special mentions. If treatment requires anesthesia, the doctor or dentist should be told if the patient has been using Vancomycin. Although most antibiotics do not significantly affect hormonal birth control medications, they may decrease the effectiveness of these hormone medications and cause pregnancy (Medicine Net). Current or sequential systemic or topical use of neurotoxic or nephrotoxic drugs should be carefully monitored (PDR, 2012). Periodic leukocyte count monitoring with drugs, which may cause neutropenia, should be performed. Serial monitoring of renal function and particular care after dosing should also be done to minimize the risk of nephrotoxicity with concomitant aminoglycoside (PDR). Other Precautions and Potential Adverse Effects A patient's medical history should be revealed before Vancomycin is administed (Medicine Net, 2012). Elderly patients should be able to eliminate the drug from their bodies when needed. Otherwise, it should be administered to them with caution for possible sensitivity to its effects. It should be used on pregnant women only when clearly needed. Risks and benefits should be discussed with the doctor. Vancomycin does not pass on to breast milk and is thus not harmful to nursing infants. But the doctor must still be consulted on its effect on breastfeeding (Medicine Net). Vancomycin may cause hypotension and cardiac arrest, though rarely, by rapid bolus administration (PDR, 2012). Ototoxicity has been reported and calls for caution for those with underlying hearing loss. Prolonged use can lead to an overgrowth of non-susceptible organisms. Safety and efficacy of administration through the intraperitoneal and intrathecal routes have not been confirmed. Use via the intraperitoneal route during dialysis has been reported to lead to a syndrome of chemical peritonitis (PDR). Look-alike/Sound-alike Drugs and Prescription Refill Requirements Vancomycin is 6th in the list of top 10 medications involved in drug errors (Medscape Pharmacists, 2007). These medications are the most commonly mis-used or mishandled some way by healthcare professionals, based on the database of the U.S. Pharmacopoeia. Liquid dose concentrations increase the risk of medication errors. There has been confusion over mL and tsp errors, which leads to overdose or under-dose of up to 5 times if undetected. Reconstituting antibiotics can also be risky as when the antibiotic powder is mixed with alcohol instead of distilled water (Medscape Pharmacists). Vancomycin was also one of the 10 most frequently reported drugs with the highest adverse drug reactions by the Adverse Drug Reaction Reporting Program for 2003-2004 (Bebout, 2004). Half of all the 360 drugs were anti-infective (Bebout). # BIBLIOGRAPHY Bebout, K. (2004). Adverse drug reporting program update and recent drug safety warnings. P & T. News: the University of Iowa Carver College of Medicine. Retrieved on April 20, 2012 from http://www.healthcare.uiowa.edu/pharmacy/PTNews/2004/december.html Drug.com (2010). Vancomycin Hydrochlorde. Drugs.com. Retrieved on April 20, 2012 from http://www.drugs.com/monograph/vancomycin-hydrochloride.html Harrison's Practice (2012). Vancomycin. The McGraw-Hill Companies, Inc. Retrieved on April 20, 2012 from http://www.harrisonspractice.com/practice/ub/view/DrugMonographs/156696/all/Vancomycin Levison, M.E. (2009). Vancomycin. The Merck Manual: Merck Sharp & Dohme. Retrieved on April 20, 2012 from http://www.merckmanuals.com/professionals/infections_diseases/bacteria_and_antibackterial_drugs/vancomycin.html Medicine Net (2011). Vancomycin. Medicine Net. Retrieved on April 20, 2012 from http://www.medicinenet.com/vancomycin-oral/article.htm Medscape Pharmacists (2007). The top 10 drug errors and how to prevent them. Medscape Education: Medscape LLC. Retrieved on April 20, 2012 from http://www.medscape.com/viewarticle/556487 PDR (2012). Vancomycin HCL. Physician's Desk Reference: PDR Network LLC. Retrieved on April 20, 2012 from http://www.pdr.net/drugpages/concisemonograph.aspx?concise=688 Read the full article
0 notes
Text
Help please
I can’t handle heat well at all (Neurological Lyme Disease makes regulating my body in heat impossible and my nervous system and brain see it as a threat)
Plus I am currently on Rifampin which make my body sunburn extra easy and then I get this whole body breakout/rash /swelling thing that creates havoc.
I have serval things I want to do this summer that means I will be outside in sun and heat
Best tips for staying cool and protected from the sun!?
I want to look cute because it’s the The Rose concert and then a Ren Faire but I need any and all suggestions
Me in the Sun And Heat:

#if your understand#why I used this gif#I salute you 🤣🤣#she’s the man#sun sensitivity#heat sensitivity#I have to be a shirt#the rose#ren faire#rennaissance#renaissance fair#renaissance faire#my rambles#chronic illness#chronic illness things#neurological Lyme disease#ocd#bartonella#lyme disease#help please#question#questions#ask
1 note
·
View note
Text
Welcome to the Antibiotic Tournament!
It's about time we had a showdown between our favorite antibiotic regimens. First round start tomorrow (3/8): I'll post two polls a day, and they'll be open for a week. You can find the list of antibiotics below, but it's not too late to submit more--just reply to this post! You can also write propaganda for why your antibiotic should win, and I'll include it in the poll.
Vote however you want: best coverage, coolest mechanism of action, easiest dosing, best side effect profile, etc. You can find all the polls under the tag antibiotic tournament.
Let the games begin!
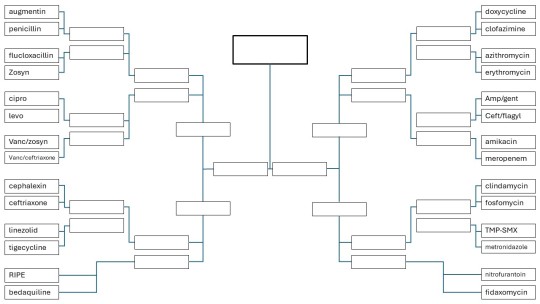
Current list of competitors:
Amikacin
Rifampin/isoniazid/pyrazinamide/ethambutol
Bedaquiline
Meropenem
Cephalexin
Ceftriaxone
Vanc/zosyn (pip-tazo)
Amp/gent
Vanc/ceftriaxone
TMP-SMX
Ceftriaxone/flagyl (metronidazole)
Fosfomycin
Ciprofloxacin
Levofloxacin
Tigecycline
Clindamycin
Azithromycin
Fidaxomycin
Erythromycin
Nitrofurantoin
Metronidazole
Linezolid
Augmentin
Penicillin
Flucloxacillin
Zosyn (Pip/tazo)
Doxycycline
Clofazimine
#medblr#medicine#antibiotics#antibiotic bracket#med student#med school#pharmblr#pharmacy#poll bracket#antibiotic tournament
23 notes
·
View notes
Text
Complications of Tuberculosis in Pregnancy

Tuberculosis (TB) remains a significant public health concern, especially for pregnant women. As a leading gynecologist in PCMC at Hiremath Hospital, Dr. Bharati Hiremath emphasizes the importance of early detection and treatment to ensure the well-being of both mother and baby.
Understanding Tuberculosis in Pregnancy
TB is an infectious disease caused by Mycobacterium tuberculosis, primarily affecting the lungs but also capable of spreading to other organs. Pregnancy can weaken the immune system, making women more susceptible to infections like TB.
How TB Affects Pregnancy
When a pregnant woman is infected with TB, the disease can pose risks to both maternal and fetal health. Common complications include:
1. Maternal Complications
Increased risk of miscarriage: TB infections, especially untreated ones, can lead to pregnancy loss.
Preterm labor: TB has been linked to premature delivery due to systemic inflammation.
Nutritional deficiencies: The disease can cause severe weight loss and anemia, impacting maternal health.
Extrapulmonary TB: TB can spread to the uterus, kidneys, or brain, making management more complex.
2. Fetal Complications
Low birth weight: Babies born to mothers with TB are often underweight due to poor maternal health and placental insufficiency.
Congenital TB: Although rare, TB can be transmitted to the baby in utero or during delivery.
Neonatal respiratory issues: Babies may experience breathing difficulties and increased risk of infections.
Diagnosis and Treatment During Pregnancy
Diagnosing TB during pregnancy requires careful evaluation. Tests such as the Mantoux test, chest X-ray (with abdominal shielding), and sputum analysis are commonly used. Dr. Bharati Hiremath stresses that TB treatment should begin as early as possible to prevent complications.
Treatment includes:
First-line anti-TB drugs (Isoniazid, Rifampin, Ethambutol, and Pyrazinamide): These medications are generally safe in pregnancy and help control the infection.
Regular monitoring: Pregnant women on TB treatment require frequent check-ups to monitor drug effects and fetal growth.
Nutritional support: A healthy diet is essential to improve immunity and prevent deficiencies.
Preventing TB During Pregnancy
To minimize the risk of TB during pregnancy:
Avoid close contact with TB-infected individuals.
Maintain proper hygiene and ventilation at home.
Ensure a nutritious diet and regular prenatal check-ups.
Get screened if exposed to TB or experiencing symptoms like persistent cough, fever, or weight loss.
Conclusion
TB during pregnancy is a serious condition, but with timely intervention and expert care, complications can be minimized. Dr. Bharati Hiremath at Hiremath Hospital in PCMC provides comprehensive prenatal care and TB management to ensure a safe pregnancy and healthy baby.
If you are pregnant and suspect TB or need expert gynecological care, schedule a consultation with Dr. Bharati Hiremath today.
#caesarean section specialist in pcmc#gynecologist in pcmc#normal delivery in pcmc#painless devlivery in pcmc#pcos treatment in pcmc
0 notes