#respiratory exam
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr was named as a finalist in Lead411’s New York City Hot 125 in Aug 2010.
Text




oxBk_PglA84
#doctor and patient#head to toe assessment#physical exam#stethoscope#doctor roleplay#male body#cardio exam#health assessment#heart auscultation#auscultation#male beauty#male aesthetic#pecs#big pecs#respiratory examination#respiratory exam
75 notes
·
View notes
Text
someone get me off this damn site i have an exam tomorrow at 1030am i gotta study 😭😭😭😭😭
#its health assessment w focus on respiratory and cardiovascular and supposedly the hardest of the exams in this class#there’s so much shit and i feel p good on the anatomy and normal vs abnormal signs in patients and stuff#but theres so many risk factors and symptoms we gotta know for cardiovascular diseases#and for respiratory we gotta know shit like what diseases make exactly what sounds and how people cough lmfao. so specific#but im gonna ball anyway IM NOT SETTING MY EXPECTATIONS HIGH THO IM PREPARING FOR DISAPPOINTMENT JUST INCASE U KNOW#send me good luck pleas im begging guys 🙏
9 notes
·
View notes
Text
I know you all are likely sick of these kinds of posts, but my Neuro final is today 🙏
#this is going to be a weekly thing at this point#save me from these weekly exams 🗿#because I literally have my respiratory exam next week#oh and also a respiratory quiz today#despite just starting the class THIS tuesday#i need the good luck i can get#...also a geriatrics exam the week after next week#ahaha...#◈ ░ out of order ⌜ooc⌟
8 notes
·
View notes
Text
I’m just so tired of studying cardio
#I’m only like a third of the way through and the exam is Friday#and I just don’t wanna study anymore today#my respiratory exam is tomorrow and I feel okay about it#idk#I’m just tired
2 notes
·
View notes
Text
100 Questions and Answers about Anatomy of the Chest #anatomyquestions #AnatomyQBank #anatomystudy
#AnatomyQuestions #AnatomyQBank #AnatomyStudyGuide#ThoracicAnatomy #ChestAnatomy #AnatomyQuestions #AnatomyQBank #AnatomyStudyGuide #AnatomyExamPrep #RespiratoryAnatomy #CardiovascularAnatomy #PulmonaryAnatomy #CardiacAnatomy #LungAnatomy #HeartAnatomy #ThoracicWallAnatomy #DiaphragmAnatomy #MediastinumAnatomy #PleuralCavityAnatomy #ChestWallAnatomy #ThoracicCavityAnatomy #ThoraxAnatomy…

View On WordPress
#Anatomy Exam Prep#Anatomy of the Chest Question Bank#Anatomy Practice Questions#Anatomy Question Bank#Anatomy Study Guide#Cardiovascular Anatomy#Chest Anatomy#Chest Anatomy Exam Preparatio#Chest Anatomy Quiz Book#Chest Anatomy Study Guide#pulmonary#Respiratory Anatomy#Thoracic Anatomy#Thoracic Anatomy Practice Questions#Thoracic Anatomy Q&A#Thoracic Region Anatomy Review
0 notes
Text
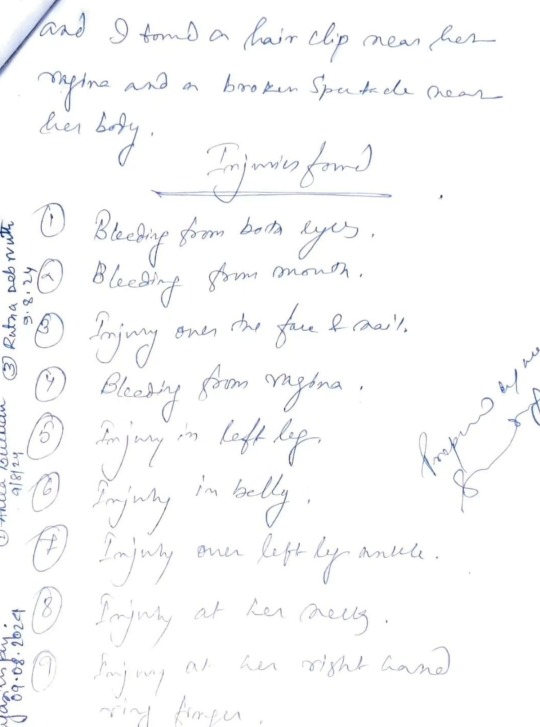
She has not just been raped and murdered, she was very much tortured and brutalized like Nirbhaya. It is all over the Bengali news. I don't understand why no one is talking about this.
A 2nd year Respiratory Medicine in a well known government medical college in Kolkata, West Bengal, India is found in a semi-naked state and the college/ hospital called it a suicide.
I'm a MBBS student in second year. After reading about her, what crossed my mind is the amount of times she would have felt this fear, before this worst fear of hers eventually materialized.
"A young resident doctor was found dead in the seminar room of her medical college in Kolkata. Initial autopsy report suggests possible rape and murder."
As all are saying,
She wasn't walking the street at odd hours. She wasn't wearing clothes that were provocative. She wasn't loitering in dangerous neighbourhoods.
She was a resident doctor, looking for a place to rest in her own hospital.
She had been on duty and had gone to rest in the early hours of Friday.
The one place which was supposed to guarantee her safety failed her, miserably.
Someone comes, rapes a female pg who is merely resting in a seminar hall because there is no proper place for her to rest, brutalized her and kills her. How did NO one know? The college and police initially call it a suicide. Excuse me? It is also being said that under pressure from local politicians, the Principal and Dean attempted to alter the post-mortem report. Autopsy confirms sexual assault.
What are the actions taken? One man arrested because his behavior seemed "shady". This is clearly not an act of one man. And this was a very well aware of and a well executed criminal act.
Also, all this happening in WB right when the situation of bangladesh is in turmoil and news of Bangladeshi Hindus being killed and tortured, seems wrong, VERY WRONG. Happening right before NEET-PG, as 24 lakh doctors prepare to write an exam on Sunday to be resident doctors, this news has wrapped us all in agony and rage,
What are they working so hard for? Why should they aspire to be in a system that ignores their basic needs? The minimum requirement of a workplace is safety. That should be non-negotiable.
This profession demands extereme hardwork, a lot of mental strength and Physical Assaults, harassment, low paying jobs with odd working hours with intense humiliation. Now its the worst of all seeing a bright mind losing her life in the most disrespectful state of all. This should never happen to any woman.
I'd also like to question why isn't any big media house covering this news, where are all the international news channels all this time.
What are the students in other medical colleges doing? This talks about their own safety and lives. What are the medical students across the world doing? It's time for us to stand for the most basic Human right, safety.
Yesterday when my roommate, an MBBS final year intern was heading for her night posting, I feared and prayed for her to come back safely. Thinking about it, in a few years I will also have night posting, I'll also return from my hospital duties late at night. I'll also have to go through the same fear, and I'll also have to keep praying that my worst fears don't turn into reality. So many female doctors, nursing staffs, other Healthcare workers, other working women, non-working women go through the same fear, probably multiple times a day.
It is a shame to be born in such a disgusting world and society, it is shame to witness such a brutal crime, and it is a shame to live in this fear daily.
Those RAPISTS need to be hunged infront of the whole natio...if needed burned alive. People should fear the idea of raping, more than getting raped.
#medicine#desi teen#desi tumblr#desi dark academia#desi things#desi girl#desi academia#desi#kolkata#west bengal#bengali#bangla news#bangla#indian#india#indian students#indian aesthetic#desi memes#desi culture#desi life#justice#justiceformoumitadebnath#nirbhaya#rape/noncon#not incorrect quotes#junko furuta#crimes against humanity#crime against humanity#crime against women#doctor
1K notes
·
View notes
Text


IT STARTED RAINING !!!!
also I have a cardio/respiratory exam in 6 days and I cannot for the life of me get motivated. This will be fine 🙃
#I’m actually gonna die#books#light academia#studyblr#coffee#college#dark academia#study#academia#stem studyblr#pre med#care of line#cottage academia#cottagecore#coffee shop
527 notes
·
View notes
Text
Writing Notes: Coma
Coma - (from the Greek word ‘‘koma,’’ meaning deep sleep)
A state of extreme unresponsiveness, in which an individual exhibits no voluntary movement or behavior.
In a deep coma, even painful stimuli (actions which, when performed on a healthy individual, result in reactions) are unable to affect any response, and normal reflexes may be lost.
Coma is the result of something that interferes with the functioning of the cerebral cortex and/or the functioning of the structures that make up the RAS. In fact, a huge and varied number of conditions can result in coma. A good way of categorizing these conditions is to consider the anatomic and the metabolic causes of coma:
Anatomic causes of coma are those conditions that disrupt the normal physical architecture of the brain structures responsible for consciousness, either at the level of the cerebal cortex or the brainstem.
Metabolic causes of coma consist of those conditions that change the chemical environment of the brain, thereby adversely affecting function.
As in any neurologic condition, history and examination form the cornerstone of diagnosis when the patient is in a coma; however, history must be obtained from family, friends, or EMS.
The Glasgow Coma Scale is a system of examining a comatose patient.
It is helpful for evaluating the depth of the coma, tracking the patient’s progress, and predicting (somewhat) the ultimate outcome of the coma.
It assigns a different number of points for exam results in three different categories:
opening the eyes,
verbal response (using words or voice to respond), and
motor response (moving a part of the body).
Fifteen is the largest possible number of total points, indicating the highest level of functioning.
The highest level of functioning would be demonstrated by an individual who spontaneously opens his/her eyes, gives appropriate answers to questions about his/her situation, and can carry out a command (such as ‘‘move your leg’’ or ‘‘nod your head’’).
Three is the least possible number of total points and would be given to a patient for whom not even a painful stimulus is sufficient to provoke a response.
In the middle are those patients who may be able to respond, but who require an intense or painful stimulus, and whose response may demonstrate some degree of brain malfunctioning (such as a person whose only response to pain in a limb is to bend that limb in toward the body).
When performed as part of the admission examination, a Glasgow score of three to five points often suggests that the patient has likely suffered fatal brain damage, while eight or more points indicates that the patient’s chances for recovery are good.
Expansion of the pupils and respiratory pattern are also important.
Metabolic causes of coma are diagnosed from blood work and urinalysis to evaluate blood chemistry, drug screen, and blood cell abnormalities that may indicate infection.
Anatomic causes of coma are diagnosed from CT (computed tomography) or MRI (magnetic resonance imaging) scans.
Coma is a medical emergency, and attention must first be directed to maintaining the patient’s respiration and circulation, using intubation and ventilation, administration of intravenous fluids or blood as needed, and other supportive care.
If head trama has not been excluded, the neck should be stabilized in the event of fracture.
It is obviously extremely important for a physician to determine quickly the cause of a coma, so that potentially reversible conditions are treated immediately. For example, an infection may be treated with antibiotics; a brain tumor may be removed; and brain swelling from an injury can be reduced with certain medications.
Various metabolic disorders can be addressed by supplying the individual with the correct amount of oxygen, glucose, or sodium; by treating the underlying disease in liver disease, asthma, or diabetes; and by halting seizures with medication.
Because of their low incidence of side effects and potential for prompt reversal of coma in certain conditions, glucose, the Bvitamin thiamine, and Narcan (to counteract any narcotic-type drugs) are routinely given.
Source ⚜ More: Notes & References ⚜ Writing Realistic Injuries
#writing reference#writeblr#dark academia#spilled ink#writers on tumblr#literature#writing inspiration#writing notes#writing prompt#poets on tumblr#writing ideas#creative writing#fiction#medicine#coma#writing resources
90 notes
·
View notes
Text
Yet another new study published by Cambridge reaffirming the same patterns in conformation association with heightened risk of BOAS. The study showed that Bostons had a lower prevalence of BOAS in comparison to previous studies with bulldogs, frenchies, and pugs (I'm guessing this may be tied to the Boston having more moderate, less meaty desired postcranial conformation) but the dogs which tested positive for BOAS had the same phenotypes correlated to BOAS risk as in previous studies with other brachycephalic breeds:

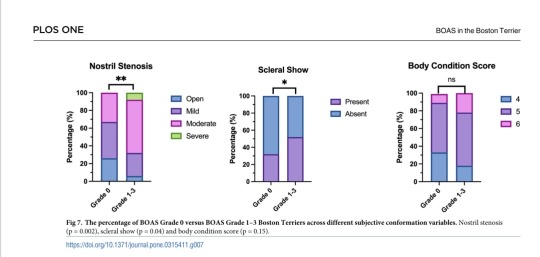
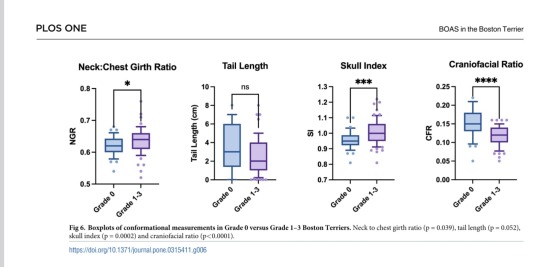
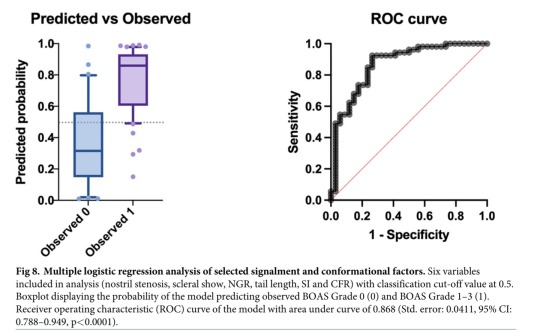
The study does acknowledge that while there are statistically significant links between these traits, there was also frequent overlap between affected and unaffected dogs meaning that a BOAS diagnosis cannot be done by purely visual exam and that dogs must be screened with respiratory testing for accurate results.
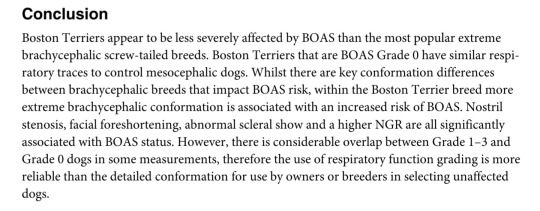
I do want to draw attention to the stenotic nare graph though, zero dogs with severe stenosis had grade 0 BOAS scores in this sampling..
61 notes
·
View notes
Text


8GP5Jf0lcpE
#doctor and patient#head to toe assessment#physical exam#stethoscope#doctor roleplay#male body#cardio exam#health assessment#heart auscultation#auscultation#respiratory exam#cardiac examination#cardiovascular examination#cardio
105 notes
·
View notes
Text
ᴺᴼᵂ ᴾᴸᴬᵞᴵᴺᴳ : Can I ~Kehlani
ᴠᴏʟᴜᴍᴇ : ▮▮▮▮▮▮▯▯▯ ↻ ◁ II ▷ ↺

“This shit so good like it should be illegal” you said to yourself after discretely taking a puff out of the pre-rolls connie left for you, feet over the arm of the huge chair that held you inside of the common rooms of your college. Notebooks of all colors displayed messily along the table in front of you, filled with doodles of the brain, and respiratory system. You were trying to prepare yourself for your pre-med exam in two days, but you couldn’t help think about him.. How he made you touch the back-board of his bed like you was a free throw, how he spent so much time with you that you found yourself…“Little Miss Scholar” using all his lingo,how his ex-girlfriend claimed he lied when he told u he was single. The way his hands slid in between your thighs, fitting like a puzzle piece that you never knew was missing. How he always said “a sweet girl like you shouldn’t know how to fuck like this cus you fuck me like a porn star.. u sure that I’m ya only one?” How he intertwined his longer tattooed fingers with your own freshly polished ones, and squeezed tighter as he heard the mumbles of your “friends” asking “how the fuck he know her home-body ass?” How he left you in shambles everytime his tongue grazed against your clit, shutting your mouth with his hand when you got too loud in the dorms.
You felt as if your pen went dry because of your day dreaming, you scribbled on the paper attempting to gain some ink flow, but managed to get lost in your thoughts again..
The thoughts about him making you squirt, leaving the juices on his pretty white tee shirt, the same night he convinced you to make a sex tape cus he strokes himself to the bloopers..How your velvety walls clenched around his pink tip as a reward, almost as if they were saying “you lasted long babe you’re a trooper.” Gripping him, forcing him to cum inside you.. “Don’t pull out my love, make me proud n thug it out” you would whisper in his ear, running butterfly kisses along his temple. How he then massaged your clit, squeezing the fat of your thighs, while pussy drunk, muttering about how you’re a keeper..But not just because of how you fucked him senseless considering you didn’t partake in those activities, but because it was never hard to read him, to understand him. He wasn’t like everyone else, and you realized this when you didn’t automatically dislike him, it makes you feel even more confident in your relationship knowing how he always says “Baby i need ya” and not in sexual ways. He made it known that he cared about you because he changed his ways so you can mold into him, gave you room to grow and de-cluttered himself so you could use him as extra space when you needed it, when you were stressed and the burden was too much. How he always thought of you and made it obvious in everything that he did even when he didn’t realize it.
“Damn…” you thought wrapping up your daydream realizing that an hour more than passed. The suns rays danced through the huge windows, slightly blinding you almost as if it was a punishment for getting yourself distracted. Eyes peering at the still notebooks below you, waiting to be used, basically taking up dust because of your negligence. The red water bottle resting in your lap was snatched up as you took sips, ignoring the obnoxious sound of the doors opening in the comms, but off of instinct, you still looked up and made eye contact with the tall man who stood in front of the sun..As if he became your sun for a second, and as he came closer, you noticed the buzz-cut and relaxed, resting the water bottle on the table, trying to stop the smile that crept onto your face…
“Hey, can I come over? Is it okay if I stop by n see u later?”……….
↺ ᴿᴱᴾᴱᴬᵀ ‖ ᴾᴬᵁˢᴱ ≫ ᴺᴱˣᵀ ˢᴼᴺᴳ
this one if for you pook! i highlighted my fav lyrics🥸 @soulaanshere ~𝓁ℯ𝓁ℯ
#connie x black y/n#connie smut#black coded reader#black reader#attack on titan#iwanty0uu#fem reader#aot x y/n#aot fanfiction#aot x black reader#connie x black reader#aot connie#connie springer#aot x you#aot x reader#aot smut#aot#black y/n#black tumblr#black girl magic
309 notes
·
View notes
Text
Also preserved on our archive (Daily updates!)
By Stephani Sutherland
Gentle nasal spray vaccines against COVID, the flu and RSV are coming. They may work better than shots in the arm
Alyson Velasquez hates needles. She never liked getting shots as a kid, and her anxiety only grew as she got older. “It really ballooned in my teens and early 20s,” she says. “It became a full-blown phobia.” She would panic at the sight of a needle being brought into an exam room; more than once she passed out. Velasquez says that she took an antianxiety medication before one appointment yet still ran around the room screaming inconsolably “like I was a small child; I was 22.” After that episode Velasquez, now a 34-year-old financial planner in southern California, quit needles completely. “No vaccinations, no bloodwork. For all of my 20s it was a no-go for me,” she says.
Then COVID showed up. “It finally hit a point where it wasn’t just about me,” Velasquez says. “It felt so selfish not to do this for the greater public health and the safety of our global community.” So she got vaccinated against the SARS-CoV-2 virus in 2021, although she had to sit on her husband’s lap while he held her arms. “It was a spectacle. The poor guy at CVS ... he did ask me, ‘Are you sure you want to do this?’” She very much did. “I’m very pro-vaccine. I am a rational human. I understand the necessity of [getting] them,” she insists. But today she still struggles with each injection.
Those struggles would end, however, if all her future vaccinations could be delivered by a nasal spray. “Oh, my God, amazing!” Velasquez says.
The amazing appears to be well on its way. Vaccines delivered through the nose are now being tested for several diseases. In the U.S., early clinical trials are showing success. Two of these vaccines have generated multiple immune system responses against the COVID-causing virus in people who received them through a puff up the nose; earlier this year their makers received nearly $20 million from Project NextGen, the Biden-Harris administration’s COVID medical initiative. Researchers are optimistic that a nasal spray delivering a COVID vaccine could be ready for the U.S. as soon as 2027. Although recent efforts have focused on inoculations against SARS-CoV-2, nasal vaccines could also protect us against the flu, respiratory syncytial virus (RSV), and more.
A few nasal vaccines have been introduced in the past, but they’ve been beset by problems. The flu inoculation FluMist has not gained popularity because of debates about its effectiveness, and a different vaccine was pulled from the market decades ago because some people had serious side effects. In China and India, nasal vaccines for COVID have been approved because those countries prioritized their development during the pandemic, whereas the U.S. and other wealthy nations opted to stick with arm injections. But this new crop of vaccines takes advantage of technology that produces stronger immune responses and is safer than preparations used in the past.
In fact, immunologists say these spritzes up the nose—or inhaled puffs through the mouth—can provide faster, stronger protection against respiratory viruses than a shot in the arm. That is because the new vaccines activate a branch of the immune system that has evolved for robust, rapid responses against airborne germs. “It may be more likely to really prevent infection from getting established,” says Fiona Smaill, an infectious disease researcher at McMaster University in Ontario. Such inoculations may also help reduce the enormous inequities in vaccine access revealed by the pandemic. These formulations should be cheaper and easier to transport to poor regions than current shots.
But nasal vaccines still face technical hurdles, such as how best to deliver them into the body. And unlike injected vaccines, which scientists can measure immune responses to with blood tests alone, testing for immunity that starts in nose cells is more challenging. But researchers working in this field agree that despite the hurdles, nasal formulations are the next step in vaccine evolution.
Traditional vaccines injected through the skin and into an arm muscle provide excellent protection against viruses. They coax immune cells into making widely circulated antibodies—special proteins that recognize specific structural features on viruses or other invading pathogens, glom on to them and mark them for destruction. Other immune cells retain a “memory” of that pathogen for future encounters.
Intramuscular injection vaccines are good at preventing a disease from spreading, but they do not stop the initial infection. A nasal spray does a much better job. That’s because sprays are aimed directly at the spot where many viruses first enter the body: the nose and the tissue that lines it, called the mucosa.
Mucosa makes up much of our bodies’ internal surfaces, stretching from the nose, mouth and throat down the respiratory tract to the lungs, through the gastrointestinal tract to the anus, and into the urogenital tract. Mucosa is where our bodies encounter the vast majority of pathogenic threats, Smaill says, be it flu, COVID, or bacterial infections that attack the gut. This tough, triple-layered tissue is specialized to fight off invaders with its thick coating of secretory goo—mucus—and with a cadre of resident immune cells waiting to attack. “Mucosa is really the first line of defense against any infection we’re exposed to,” Smaill says.
Mucosal immunity not only prepares the immune system for the fight where it occurs but also offers three different types of protection—at least one more than a shot does. Nasal vaccines and shots both mobilize immune messenger cells, which gather the interlopers’ proteins and display them on their surfaces. These cells head to the lymph nodes, where they show off their captured prize to B and T cells, which are members of another part of the immune system called the adaptive arm. B cells, in turn, produce antibodies, molecules that home in on the foreign proteins and flag their owners—the invading microbes—for destruction. Killer T cells directly attack infected cells, eliminating them and the microbes inside. This provides broad protection, but it takes time, during which the virus continues to replicate and spread.
That’s why a second type of protection, offered only by the mucosal tissue, is so important. The mucosa holds cells of the innate immune system, which are the body’s “first responders.” Some of these cells, called macrophages, recognize invasive microbes as foreign and swallow them up. They also trigger inflammation—an alarm sounded to recruit more immune cells.
Another part of this localized response is called tissue-resident immunity. These cells don’t have to detect telltale signs of a pathogen and make a long journey to the infected tissue. They are more like a Special Forces unit dropped behind enemy lines where a skirmish is occurring rather than waiting for the proverbial cavalry to arrive. This localized reaction can be quite potent. Its activation is notoriously difficult to demonstrate, however, so historically it’s been hard for vaccine makers to show they’ve hit the mark. But it turns out that one type of antibody, called IgA, is a good indicator of mucosal immunity because IgAs tend to predominate in the mucosa rather than other parts of the body. In an early trial of CoviLiv, a nasal COVID vaccine produced by Codagenix, about half of participants had detectable IgA responses within several weeks after receiving two doses. That trial also showed the vaccine was safe and led to NextGen funding for a larger trial of the vaccine’s efficacy.
It’s possible an inhaled vaccine may provide yet one more layer of protection, called trained innate immunity. This reaction is a bit of a mystery: although immunologists know it exists and appears also to be produced by intramuscular injections, they can’t quite explain how it works. Immune cells associated with trained innate immunity seem to have memorylike responses, reacting quickly against subsequent infections. They also have been found to respond against pathogens entirely unrelated to the intended vaccine target. Smaill and her colleagues found that when they immunized mice with an inhaled tuberculosis vaccine and then challenged them with pneumococcal bacteria, the mice were protected. In children, there is some evidence that a tuberculosis vaccine, in the arm, generates this type of broad response against other diseases.
Akiko Iwasaki, an immunologist at Yale University who is working to develop a nasal vaccination for COVID, sees two major potential benefits to nasal immunity in addition to better, faster, more localized protection. First, attacking the virus in the nose could prevent the disease from being transmitted to others by reducing the amount of virus that people breathe out. And second, Iwasaki says, the spray may limit how deeply the infection moves into the body, so “we believe that it will also prevent long COVID.” That debilitating postinfection condition, sometimes marked by signs of entrenched viral particles, disables people with extreme fatigue, chronic pain, a variety of cognitive difficulties, and other symptoms.
Making a new vaccine is hard, regardless of how you administer it. It needs to raise an immune response that’s strong enough to protect against future invasions but not so strong that the components of that response—such as inflammation and fever—harm the host.
The lining of the nose puts up its own barriers—literal, physical ones. Because the nasal mucosa is exposed to so many irritants from the air, ranging from pet hair to pollen, the nose has multiple lines of defense against invading pathogens. Nostril hair, mucus, and features called cilia that sweep the nasal surface all aim to trap small foreign objects before they can get deeper into the body—and that includes tiny droplets of vaccine.
And lots of small foreign particles—often harmless—still make it through those defenses. So the nose has developed a way to become less reactive to harmless objects. This dampened reactivity is called immunological tolerance, and it may be the biggest hurdle to successful development of a nasal vaccine. When foreign particles show up in the bloodstream, a space that is ostensibly sterile, immune cells immediately recognize them as invaders. But mucosal surfaces are constantly bombarded by both pathogens and harmless materials. The immune system uses tolerance—a complex series of decisions carried out by specialized cells—to determine whether a substance is harmful. “This is very important because we can’t have our lungs or gastrointestinal tract always responding to nonharmful foreign entities that they encounter,” says Yale infectious disease researcher Benjamin Goldman-Israelow. For example, inflammation in the lungs would make it hard to breathe; in the gut, it would prevent the absorption of water and nutrients.

These barriers may hamper the effectiveness of a nasal flu vaccine that’s been around for a while, called FluMist in the U.S. and Fluenz in Europe. The inoculation is safe, says infectious disease scientist Michael Diamond of Washington University in St. Louis, but it faces a similar problem as do injected flu vaccines: it isn’t very effective at warding off new seasonal flu strains. This might be because flu strains are so common, and people are frequently infected by the time they are adults. Their immune systems are already primed to recognize and destroy familiar flu particles. FluMist is built from a live flu virus, so immune cells probably treat the vaccine as an invader and demolish it as soon as it shows up in the nose, before it has a chance to do any good. This preexisting immunity isn’t such an issue in children, who are less likely to have had multiple flu infections. Nasal flu vaccines are routinely used to inoculate kids in Europe.
In other vaccines, researchers often use adjuvants, special agents that attract the attention of immune cells, to boost a response. Some nasal vaccines use adjuvants to overcome tolerance, but in the nose, adjuvants can pose unique dangers. In at least one case, a nasal adjuvant led to disastrous consequences. An intranasal vaccine for influenza, licensed in Switzerland for the 2000–2001 season, used a toxin isolated from Escherichia coli bacteria as an adjuvant to provoke a reaction to the inactivated virus. No serious side effects were reported during the trial period, but once the vaccine was released, Swiss officials saw a concerning uptick in cases of Bell’s palsy, a disease that causes weakness or paralysis of the facial muscles, often leading to a drooping or disfigured face. Researchers at the University of Zurich estimated that the adjuvanted flu vaccine had increased the risk of contracting Bell’s palsy by about 20 times, and the vaccine was discontinued. “We need to be cautious about using adjuvants like that from known pathogens,” says pharmaceutical formulations scientist Vicky Kett of Queen’s University Belfast in Northern Ireland.
To get around the challenges posed by the nose, some researchers are exploring vaccines inhaled through the mouth. Smaill is working on one of them. She and her McMaster colleagues aerosolized their vaccine for COVID into a fine mist delivered by a nebulizer, from which it rapidly reaches the lungs. Experiments in mice have shown promising results, with mucosal immunity established after administration of the vaccine.
Another vaccine strategy is to use a harmless virus to carry viral genes or proteins. Researchers at the Icahn School of Medicine at Mount Sinai in New York City selected a bird pathogen, Newcastle disease virus (NDV). “It’s naturally a respiratory pathogen,” so it infects nasal cells, says Michael Egan, CEO and chief scientific officer of CastleVax, a company that formed to develop the NDV vaccine for COVID. A small early clinical trial showed the CastleVax vaccine was safe and caused robust immune responses in people. “Those results were very promising,” Egan says. People who received the vaccine also produced antibodies that indicated multitiered mucosal immunity, not simply the adaptive immunity from a shot in the arm.
Following that trial, the CastleVax project received NextGen funding, and results from a trial of 10,000 people are expected in 2026. Half of those people will receive a messenger RNA (mRNA) injection, and half will get the new NDV nasal spray. The data should show whether the new nasal vaccine can do a better job of preventing infection than the mRNA injections. Egan has high hopes. “We’re expecting to see a lot fewer breakthrough infections in people who got the vaccine up the nose by virtue of having those mucosal immune responses,” he says.
Florian Krammer, one of the Mount Sinai researchers behind the vaccine, engineered NDV particles to display a stabilized version of the spike protein that’s so prominent in SARS-CoV-2. “You end up with a particle that’s covered with spike,” he says. Spike protein in the bloodstream can raise an immune response. But the NDV vaccine works in another way, too. The virus particle can also get into cells, where it can replicate enough times to cause virus particles to emerge from the cells, provoking another immune reaction. Before moving into human trials, however, researchers had to complete clinical trials to establish that the Newcastle virus is truly harmless because the nose is close to the central nervous system—it has neurons that connect to the olfactory bulb, which is part of the brain. Those trials confirmed that it is safe for this use.
Nasal sprays aim directly at the spot where most viruses first enter the body: the nose. This type of caution is one reason a COVID nasal vaccine approved in India hasn’t been adopted by the U.S. or other countries. The inoculation, called iNCOVACC, uses a harmless simian adenovirus to carry the spike protein into the airway. The research originated in the laboratories of Diamond and some of his colleagues at Washington University at the start of the pandemic, when they tested the formulation on rodents and nonhuman primates. “The preclinical data were outstanding,” Diamond says. Around the time he and his colleagues published initial animal results in Cell in 2020, Bharat Biotech in India licensed the idea from the university. In a 2023 phase 3 clinical trial in India, the nasal vaccine produced superior systemic immunity compared with a shot.
Diamond says American drug companies didn’t pursue this approach, because “they wanted to use known quantities,” such as the mRNA vaccines, which were already proving themselves in clinical trials in 2020. As the pandemic took hold, there was little appetite to develop nasal vaccine technology to stimulate mucosal immunity while the tried-and-true route of shots in the arm was available and working. But now, four years later, an inhaled vaccine using technology similar to iNCOVACC’s is being developed for approval in the U.S. by biotech company Ocugen. Both inhaled and nasal forms of the vaccine are set to undergo clinical trials as part of Project NextGen. These new vaccines are using classical vaccine methods based on the virus rather than using new, mRNA-based technology. The mRNA preparations were developed specifically for intramuscular injections and would have to be significantly modified.
Codagenix, which is developing CoviLiv, sidestepped the need for a new viral vector or an adjuvant by disabling a live SARS-CoV-2 virus. To make it safe, scientists engineered a version of the virus with 283 mutations, alterations to its genetic code that make it hard for the virus to replicate and harm the body. Without all these genetic changes, there would be a chance the virus could revert to a dangerous, pathogenic form. But with hundreds of key mutations, “statistically, it’s basically impossible that this will revert back to a live virus in the population,” says Johanna Kaufmann, who helped to develop the vaccine before leaving Codagenix for another company earlier this year.
Because most people on the planet have now been exposed to SARS-CoV-2—in the same way they’re regularly exposed to the flu—some nasal vaccines are being designed as boosters for a preexisting immune response that is starting to wane. For example, Yale researchers Iwasaki and Goldman-Israelow are pursuing a strategy in animals deemed “prime and spike.”
The idea is to start with a vaccine injection—the “prime” that stimulates adaptive immunity—then follow it a few weeks later with a nasal puff that “spikes” the system with more viral protein, leading to mucosal immunity. In a study published in 2022 in Science, Iwasaki and her colleagues reported that they primed rodents with the mRNA vaccine developed by Pfizer and BioNTech, the same shot so many of us have received. Two weeks later some of the mice received an intranasal puff of saline containing a fragment of the SARS-CoV-2 spike protein. Because the animals had some preexisting immunity from the shot, the researchers didn’t add any adjuvants to heighten the effects of the nasal puff. Two weeks later researchers detected stronger signs of mucosal immunity in mice that had received this treatment compared with mice that got only the shot.
“Not only can we establish tissue-resident memory T cells” to fight off the virus in the nose, Iwasaki says, but the prime-and-spike method also produces those vigorous IgA antibodies in the mucosal layer. “And that’s much more advantageous because we can prevent the virus from ever infecting the host,” she notes. The study suggests that this approach might also lessen the chances of transmitting the disease to others because of the lower overall viral load. Experiments in hamsters demonstrated that vaccinated animals shed less virus, and they were less likely to contract COVID from infected cage mates that had not been vaccinated themselves.
Although most of the new vaccine strategies are aimed at COVID, nasal vaccines for other diseases are already being planned. Kaufmann, formerly of Codagenix, says the company currently has clinical trials underway for nasal vaccines against flu and RSV. CastleVax’s Egan says “we have plans to address other pathogens” such as RSV and human metapneumovirus, another leading cause of respiratory disease in kids.
Vaccines that don’t need to be injected could clear many barriers to vaccine access worldwide. “We saw with COVID there was no vaccine equity,” Smaill says. Many people in low-income countries never received a shot; they are still going without one four years after the vaccines debuted.
In part, this inequity is a consequence of the high cost of delivering a vaccine that needs to stay frozen on a long journey from manufacturing facilities in wealthy countries. Some of the nasal sprays in development don’t need deep-cold storage, so they might be easier to store and transport. And a nasal spray or an inhaled puff would be much easier to administer than a shot. No health professional is required, so people could spray it into their noses or mouths at home.
For these reasons, needle-free delivery matters to the World Health Organization. The WHO is using the Codagenix nasal spray in its Solidarity Trial Vaccines program to improve vaccine equity. The CoviLiv spray is now in phase 3 clinical trials around the world as part of this effort. “The fact that the WHO was still interested in a primary vaccination trial in the geographies it’s passionate about—that’s indicative that there is still a gap,” Kaufmann says. CoviLiv was co-developed with the Serum Institute of India, the world’s largest maker of vaccines by dose. The partnership enabled production at the high volume required for Solidarity.
The CastleVax vaccine with the NDV vector provides another layer of equity because the facilities required to make it already exist in many low- and middle-income countries. “The cool thing is that NDV is a chicken virus, so it grows very well in embryonated eggs—that’s exactly the system used for making flu vaccines,” Krammer says. For example, for a clinical trial in Thailand, “we just shipped them the seed virus, and then they produced the vaccine and ran the clinical trials,” he says. Many countries around the world have similar facilities, so they will not need to depend on pharma companies based in richer places.
Even high-income countries face barriers to vaccination, although they may be more personal than systemic. For very many people, the needle itself is the problem. Extreme phobia such as Velasquez’s is uncommon, but many people have a general fear of needles that makes vaccinations stressful or even impossible for them. For about one in 10 people needle-related fear or pain is a barrier to vaccinations, says C. Meghan McMurtry, a psychologist at the University of Guelph in Ontario. Needle fear “is present in most young kids and in about half of adolescents. And 20 to 30 percent of adults have some level of fear.” A review of studies of children showed that “concern around pain and needle fear are barriers to vaccination in about 8 percent of the general population and about 18 percent in the vaccine-hesitant population,” McMurtry adds.
Some people are wary of injected vaccines even if they’re not afraid of needles, Kett says; they see injections as too invasive even if the needle doesn’t bother them. “We’re hopeful that something administered by the nasal route would be less likely to come across some of those issues,” Kett says.
In the U.S., however, sprays and puffs won’t be available until they are approved by the Food and Drug Administration, which requires clear evidence of disease protection. As Diamond points out, standards for such evidence are well established for injections, and vaccine makers can follow the rule book: regulations point to particular antibodies and specific ways to measure them with a simple blood test. But for nasal vaccines, Iwasaki says, “we don’t have a standard way to collect nasal mucus or measure antibody titers. All these practical issues have not been worked out.”
Iwasaki is also frustrated with a restriction by the U.S. Centers for Disease Control and Prevention that stops researchers from using existing COVID vaccines in basic research to develop new nasal sprays. The rule is a holdover from 2020, when COVID injections had just been developed and were in short supply; people had to wait to get vaccinated until they were eligible based on factors such as age and preexisting conditions. “That made sense back then, but those concerns are years old; things are different now,” Iwasaki says. “Now we have excess vaccine being thrown out, and we cannot even get access to the waste, the expired vaccine.”
Today scientists want to contrast the effectiveness of nasal formulations with injections already in use. “Those comparisons are really important for convincing the FDA that this is a worthy vaccine to pursue,” Iwasaki says. But the restriction has held up studies by her company, Xanadu, slowing down work. (The CDC did not respond to a request for comment.)
Despite the bureaucratic and scientific hurdles, the sheer number of nasal vaccines now in clinical trials encourages Iwasaki and other scientists pursuing the needle-free route. They say it seems like only a matter of time before getting vaccinated will be as simple as a spritz up the nose.
Velasquez, for one, can’t wait for that day to arrive. The circumstances that finally forced her to reckon with her fear of needles (a global pandemic, the prospect of parenthood and the numerous blood tests that accompanied her pregnancy) were so much bigger than her. If not for them, she might still be avoiding shots. “So having vaccines without needles—I would get every vaccine any doctor wanted me to get, ever. It would be a complete game changer for me.”
#vaccination#mask up#covid#pandemic#public health#wear a mask#covid 19#wear a respirator#still coviding#coronavirus#sars cov 2#get vaccinated#vaccinate your kids
43 notes
·
View notes
Text


Foster rat Cheesecake (lighter colored rat with the white dot) has a URI so he and his buddies got to go to the vet today for cuddles an exam and get some meds. Luckily his buddies don’t have any respiratory concerns and it will hopefully stay that way.
53 notes
·
View notes
Note
If you come back soon could I pretty please request an Amelia (greys) one shot where the reader is her girlfriend and is brought to the ER in critical condition as Jane Doe but as soon as Amelia sees her she’s hysterical and all she wants to is reasure and hold the readers hand! YOU WOULD MAKE MY QUARANTINE SO MUCH BETTER I LOVE YOUR WORKS SM

Authors note: So... um... I know I waited so long to post this request but... I HAVE MISSED IT IN MY INBOX FOR SO LONG AND WHEN I FOUND IT TWO DAYS AGO, I WROTE IT IMMEDIATELY! I am so sorry. I hope you're still out there somewhere recognizing your request and reading it ♥
ᕚ---ᕘ
The hustle and bustle of the emergency room echoed through the cold hallways as the double doors were pushed apart to make way for the ambulance crew and their critical patient. The vehicle's red and blue lights cast flickering shadows on the walls, while the howling sound of the approaching accident conveyed to hospital staff the urgency of the situation.
The paramedics, with serious faces and rustling uniforms, wheeled the gurney into the emergency room. An unknown woman lay on the stretcher, pale and motionless, only the shallow rise and fall of her chest showed any life. A white sheet covered her completely, and her blood-stained hair stuck damply to her forehead. The slow, monotonous beep of the portable monitor accompanied every breath.
Dr. Hunt, the emergency physician in charge, immediately rushed to the bed. His expression was professional, but the depth of his gaze betrayed some concern. The nurses and also Dr. Keppner rushed to help the team take over.
"What do we have?" Owen asked as he looked over the medical file one of the paramedics handed him. "Unknown female person, middle-aged, found unconscious in a park, presumably after an attack. Stabbed in the chest and abdomen. We cannot say any more. No identification and no indication of possible previous illnesses."
The paramedics quickly explained the course of events, how they found the patient and what first aid measures they had taken. The information was relayed with the precision of a well-trained team, but uncertainty about who the woman was and what had happened to her hung in the air.
While Hunt and Keppner began checking vital signs, the unknown woman was wheeled into an examination room. The nurses exchanged hand signals and quietly instructed each other on the next steps. The background noise is a chaotic orchestra of clanging instruments, murmuring conversations and the beeping of medical equipment.
April Keppner leaned over the patient and began a thorough examination. She checked the pupillary reaction, palpated the pulse and analyzed the respiratory rate. The monitors showed unstable readings and the two doctors' facial expressions hardened. A quick look between the two revealed that they were worried.
"We need a CT scan immediately," Owen said, turning to the nurses present. "I also want blood samples for a comprehensive analysis. Let the lab know it's urgent."
While preparations for further examinations were underway, the nurses and doctors tried to keep the unknown woman stable. An intravenous line was placed and fluids began flowing through her derm. The monitors continued to show jittery signals and the tension in the room increased.
"Call Dr. Shephard and Dr. Altmann. I want them here as quickly as possible!" He ordered as he continued to analyze the data on the screen. "And someone should inform the police. We have to find out who she is and what happened in order to prevent further damage."
The exam room was now in a coordinated state of emergency and in a room that was normally a place of rescue, the medical team battled uncertainty and a race against time to save a woman's life. He was abuzz as the neurosurgeon and cardiologist burst through the door almost simultaneously with quick steps. Their eyes were focused, the rubber of their Crocs squeaking in unison with the machines.
"Shephard, the patient is exhibiting unstable neurological signs. The CT scan and blood results are pending," she informed Hunt as he cleared the way for her to the bed.
Amelia nodded curtly and fully entered the room, closing the door behind her. A glance at the monitor and the papers on the tablet caused her eyes to flash briefly before she focused back on the patient. However, as she leaned over the lounger, she froze.
Her features slipped away, the slight smile on her lips fading as she realized who was in front of her. The woman on the lounger was none other than you. Hunt and Keppner stared at her as she noticed her reaction, not understanding why she didn't move forward with her work. "Amelia, we have a critical situation here. The patient's identity is unknown and her values are concerning. We urgently need your expertise!"
Amelia shook her head slightly, as if she could push reality away. Her heart raced as she double-checked that her eyes weren't playing tricks on her. "This is y/n. Y/n y/l/n. She's my girlfriend. Find her family, get them here!" A strangled sound escaped her throat and the world around her seemed to stand still for a moment as she processed the shock.
The emotional rollercoaster went through all the ups and downs, from worrying about you to the overwhelming need to stay in control. Her hands shook slightly as she reached for your lifeless and bloody hand.
"Y/n," Amelia whispered with a strangled sound in her voice and the two doctors and friends of the neurosurgeon were also dumbfounded, their breath catching in their throats. "What happened to you?"
Owen Hunt moved closer and tried to reassure her, while also conveying the urgency and explaining the neurological details. But Amelia only heard fragments. Her gaze was lost in your eyes, which were closed as if you were in a deep sleep.
"Amelia, I know it's hard. But we have to act immediately. The CT results are crucial and we have to find out what happened to her to prevent something worse. She could die!" April urged, concerned about her colleague's professionalism.
But Amelia couldn't let go. She ignored the two of them, her focus solely on you. The world outside the exam room seemed to fade as she held your hand tightly. "Y/n, you have to hold on. You can do this," she whispered in your ear, tears of despair welling up in her eyes. "You're strong, you know? We'll get through this together."
In her emotional despair, an internal struggle unfolded within Amelia. Her professional self fought against her personal connection to you. The shouts of other doctors and nurses became a muffled background noise as she refused to loosen her grip on your cold hand.
"Amelia," Owen Hunt spoke in a calm but firm voice. "We need you now. She needs you now. Let's find out what happened to her together.
A conflict between duty and personal pain raged within Amelia. Finally, she reluctantly gave in and removed her hand from yours. However, her gaze remained focused on you, and concern for you was reflected deep in her eyes. She struggled with fear for you as she prepared to resume her professional role as a neurosurgeon.
A deep breath flowed through her body and with a firm resolve she wiped the tears from her cheeks and turned her gaze to the surroundings. "Dr. Hunt, take her to the CT immediately. She's probably having a brain bleed." she spoke, her voice firm. The neurosurgical focus returned fully, analyzing the medical indicators.
The trauma surgeon nodded in agreement and began giving the necessary instructions, getting you up to the CT scanner. Amelia stayed at your side, letting go of your hand for a moment to oversee the diagnostic process.
The minutes that passed felt like hours. The results of the CT scan appeared on the screen, and Amelia scanned the images with a trained eye. She analyzed each region of the brain, looking for signs of bleeding, injury or other abnormalities. The intensity of her concentration was palpable, and the medical staff eagerly awaited her assessment.
"We have severe damage to the frontal lobe," Amelia explained, swallowing hard as she continued to study the images. "It looks like a severe traumatic brain injury. We need to operate immediately to relieve the pressure and prevent further damage."
The team immediately began preparing for the operation. The sterile atmosphere of the operating room seemed to embrace Amelia as her professional role took over. In her surgical uniform, surrounded by a team of experienced professionals, she struck her familiar Superman pose and focused on the procedure ahead.
During the operation, which lasted several hours, your girlfriend showed an impressive mix of calm and precision. Her hands worked in sync with the instruments as she gently treated the damaged tissue. Monitors in the operating room recorded progress, and the medical team closely followed their experienced leader's every move.
After what seemed like endless hours, but which passed like seconds, she finally closed the last stitches and the atmosphere relaxed slightly, but the uncertainty about the outcome of the operation weighed heavily on her.
Amelia let out a frustrated gasp before exiting the operating room, tearing off her gloves and hood. She immediately went to the waiting area to inform your siblings and parents. The tension in her chest eased as she saw the expectant looks of the people who were now her family and your sister immediately threw her arms around her.
"The operation is complete," Amelia began, trying to keep her voice steady as she also clung to your sister to keep her emotions at bay. "It was a complex brain injury for reasons still unknown, but I did everything I could. The next step now is to wait and hope she remains stable."
Your family breathed a sigh of relief as Amelia explained more details about the condition and cooperation with the police. Her words were reassuring to your sister, but she still felt the knot in her stomach. The outcome of the operation was uncertain, and there was no way of knowing whether you would ever wake up and be your old self again.
In the silence of the hospital hallway, as she left the waiting people behind, a moment of exhaustion overcame her. Her eyes wandered back to the exam room where she found you in. The image of you on the lounger didn't fade, but Amelia found comfort in the fact that she had saved you. Now things could only go uphill and she couldn't wait to look into your beautiful eyes again.
#amelia shephard#amelia shephard fanfiction#amelia shephard fanfic#amelia shephard imagine#amelia shephard imagines#amelia shephard x you#amelia shephard x reader#amelia shephard x female reader#amelia shephard oneshot#greys anatomy#greys anatomy fanfiction#greys anatomy fanfic#greys anatomy imagine#greys anatomy imagines#greys anatomy oneshot#greys anatomy x you#greys anatomy x reader#greys anatomy abc#fanfiction#fanfic#oneshot#imagines#imagine#writeblr#writers on tumblr#writing community#creative writing
119 notes
·
View notes
Text
Cardiophile Turn On/Off
I got this from @/heartbinary who got it from @/torture-steth-repeat
I wanted to do it myself to not only have some boundaries but also so people can get to know me a tad bit better
💚 = Turn on
💔 = Turn off
🤍 = Neutral/Like it in a non-sexual way
Section 1: Cardiophilia basics
1. My heart being listened to: 💚
2. Listening to others' hearts: 💚
3. Fast heartbeats: 💚
4. Slow heartbeats: 🤍
5. Naturally irregular heartbeats: 💚
6. Deliberately irregular heartbeats: 💚
7. Heart via stethoscope: 💚
8. Heart via EKG: 💚
9. Heart via Doppler: 🤍
10. Heart via ultrasound: 💚
11. Carotid (throat) pulse: 💚
12. Femoral (groin) pulse: 🤍
13. Radial (wrist) pulse: 🤍
14. Chest/belly pulse: 💚🤍
15. Ear stething: 💚
Section 2: Dark Cardiophilia
1. Shocking a healthy heart: 💚
2. Pressure/crushing a healthy heart: 💚
3. Drowning + heart monitoring: 💚
4. Suffocation + heart monitoring: 💚
5. Choking + heart monitoring: 💚
6. Drugs used to affect the heart: 💚
7. Knifeplay + heart monitoring: 💚
8. Needle or injection into the heart: 💚
9. Gunplay (shooting the heart): 💚
10. Being dominated (in a cardiophilia way): 💚
11. Dominating someone else (in a cardiophilia way): 💚
12. Consensual non-consent (CNC) play: 🤍
13. Heart rips: 💔
14. Fucked into cardiac arrest: 💚
15. Heart being fucked: 🤍
16. Heart being licked or bitten: 🤍
17. Heart being eaten: 🤍
18. Hands squeezing the heart directly: 💚
19. 'Unhappy endings' (RIP) for dark cardiophilia: 💔
Section 3: Medfet/Resus
1. Blood pressure readings: 💔
2. Medical equipment: 🤍
3. Medical exam roleplay: 🤍
4. Resuscitation via CPR: 🤍
5. Resuscitation via defibrillator: 🤍
6. Resuscitation via AED: 🤍
7. Cardiac arrest: 💚
8. Respiratory arrest: 🤍
9. Sex and resus combined: 💔
10. 'Unhappy endings' (RIP) for resus: 💔
11. Anesthesia: 💔
12. Breathing masks: 🤍
Section 4: Graphic
1. Open heart surgery footage: 💚
2. Real animal hearts: 💔
3. Real human hearts outside the body: 💚
4. Real human hearts in autopsies: 🤍
Section 5: Adjacent Kinks
1. Gyno medical exams: 💔
2. Pregnancy/breeding: 🤍
3. Belly sounds: 💔
4. Cardiophilia + furry: 💚
5. Vampires: 🤍
6. Necrophliia: 💔
Section 6: 😏
1. Reading someone's bio before engaging with them: 💚
2. Asking about boundaries: 💚
3. Respecting those boundaries: 💚
4. Good spelling: 🤍
#i hope i did this right lmao#cardiophilia#cardiophile#roxie speaks#heartbeat kink#heartbeat#dark cardiophilia
44 notes
·
View notes
Text





Sebastian is at the doctor's office for a sports checkup. The doctor performs the usual heart exam both at rest and after some exercises, along with other checkups on the exam table.
Despite some respiratory issues, no major problems are found, so the doctor gives him the certificate.
Watch the preview here: https://youtu.be/adKrxSoZi1o
Full version $14.90
29 notes
·
View notes