#nurse call system pdf
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs




Fun Fact
Tumblr Inc. is using 66 technologies for its website.
Text
Nurse Call System India | Nurse Call System Manufacturers in India | Altos Engineers

What is Nurse Call System?
A Nurse Call System is a communication system used in healthcare facilities to allow patients to request assistance from nurses. It typically consists of a push button or pull cord that is located near the patient’s bed, which when activated sends an alert to a central station where nurses monitor the calls.
The alert can also be sent to mobile devices, such as smartphones and tablets, allowing nurses to respond quickly to patient requests. Nurse Call Systems are important in helping to ensure patient safety and improving patient care.
What is Use of Nurse Call System?
The nurse call system is a communication system that allows hospital patients to quickly and easily alert their nurse when they need assistance. This system can be used to request a variety of services, including help with repositioning a patient, assistance with a medical procedure, or simply to ask for a glass of water. The nurse call system is an invaluable tool that helps nurses provide quality care to their patients.
Nurse Call System India
Altos offer a wide range of nurse call systems designed to meet the needs of healthcare facilities in India. Our systems are designed with safety and efficiency in mind, and they provide a comprehensive suite of products and services to ensure that their customers can get the best possible system for their needs.
Best Nurse Call System Manufacturers in India
There are some great nurse call system manufacturers in India that are capable enough to meet your needs which includes Altos Engineers Pvt Ltd. We have high quality systems that are designed to meet the needs of healthcare facilities. In addition to this, Altos Engineers provides different features.
If you have specific questions or need more information, feel free to contact the company directly. Our Contact Number : +91 8588845195 or Visit our official website : www.altosengineers.com
How Many Type of Nurse Call Systems
There are several types of nurse call systems that can be used in healthcare settings. These include traditional hardwired systems, wireless systems, and integrated systems. Each type of system has unique features and benefits that can be tailored to meet the specific needs of a healthcare facility.
Traditional Hardwired Nurse Call Systems
Traditional hardwired nurse call systems are a great choice for hospitals, care facilities, and other medical establishments. They offer a secure, reliable, and efficient way to communicate with medical staff and nurses. With a hardwired nurse call system, nurses can quickly and easily respond to patient requests or needs.
The systems also offer superior sound quality, allowing staff to communicate clearly and efficiently. Additionally, hardwired systems are more secure than wireless systems, ensuring that patient information remains confidential.
Wireless Nurse Call Systems
Wireless nurse call systems are a great way for nurses to quickly and easily request assistance when needed. They can be used in a variety of healthcare settings, from hospitals to nursing homes, and can be used to call for help from staff, or even alert staff to changes in a patient's condition. They are a great way to keep communication open between staff and patients, and can help ensure that patient needs are quickly met.
Integrated Nurse Call Systems
These systems provide a comprehensive system for nurses to quickly and easily send and receive calls and messages. Such systems are designed to be user-friendly and efficient, while allowing nurses to respond to calls quickly and accurately. If you have any questions please contact our helpline number : +91 8588845195 or Visit our official website : www.altosengineers.com.
Nurse Call System Brands in India
There are many nurse call system brands in India, such as Altos Engineers Private Limited, Brahma Technologies India, Audislave Hitech Technologies, and Amstronics Control Systems Private Limited. Each of these companies offer a variety of products to suit different needs and budgets.
Talking about the present times, Altos Engineers offers quality products at the most affordable prices which include Nurse Call System. If you have any questions please contact our helpline number : +91 8588845195 or Visit our official website : www.altosengineers.com
Download Nurse Call System Pdf
If you want to know more about nurse call system and download nurse call system pdf then click on the link given below and download nurse call system pdf. Contact us for more information.
Link : https://altosengineers.com/nurse-call-system/
#nurse call system#nurse call system india#nurse call system manufacturers in india#type of nurse call systems#nurse call system brands in india#nurse call system pdf#What is Nurse Call System#best nurse call system manufacturers company in india#nurse call system manufacturers india#best nurse call system for hospital manufacturers company in india#top nurse call system for hospital in india
0 notes
Text
I feel like there's an epidemic of businesses trying to make customers and applicants do free data entry for them and it's driving me crazy.
I have complained many times about how seeing a doctor now involves checking in online, and then entering duplicate information into something else when you check in physically, and then answering duplicate questions once you're actually inside the exam room. Sometimes somebody addresses this in a humane way: "Sorry, we're using a new CMS and we have to do all this stuff from scratch," or "Sorry, we have to use these three different systems and they don't communicate with each other." Last time I went I did all this like research into my past appointments because I never ever remember off the cuff exactly what day I had this or that procedure, and I had every impression that the clinic was dependent on me to have all my medical records memorized...so I got in there and started rattling off information, and the nurse asked "When was your last mammogram?", and I gave her the date, and she looked at her monitor and said, "...yup, there it is!" Like WHAT THE FUCK WAS THAT, IF IT WAS RIGHT IN FRONT OF YOU WHY ARE YOU QUIZZING ME ABOUT THIS, WHY IS THIS A TEST???
I actually asked about redundant check-in procedures on Quora of all places, figuring there had to be a few cantankerous cranks on there who could at least try to explain this to me, but there were absolutely no takers at all. As far as I can see, literally no one knows why this is happening, it's just The Way It Is.
But anyway. Now I'm having this experience with job applications where they request that you upload files for your resume and cover letter in specific formats...and then they direct you to this interface where you are made to transcribe every detail from the resume you just provided by hand, one field at a time. I've been confronted with this insanity when applying for jobs whose wages weren't even worth the mind-numbing exercise of the application process. And actually this is part of my point: Data entry is a JOB. I have had this job. I was paid to examine, reformat, and transcribe data, and upload it to a database for my company to search and cross-reference in the future. If you are an employer and you absolutely require BOTH a pdf of my resume and cover letter that a human being can read and evaluate, AND each piece of data from those documents individually entered into your database for some other form of storage and review, then it is seriously fucking Up to You to pay some wage slave to enter the data. I'm looking for a job. I'm not going to do a job for you for fucking free, in order to become eligible for a job that you might consider paying me for later. Like please don't call me a fucking idiot to my face--or at least, if it's the database part that's the most important thing to you, do not also require me to create a nicely-formatted document containing my history and intentions. Let's just get right to the forced data entry part, let's start this awful relationship from a place of honesty at the very fucking least.
N.B. I realize that there are multiple reasons an employer would do this to a person, ranging from algorithmic candidate-sorting to just having outdated-ass job site shit in place that they don't feel like reviewing or revising. I don't really care why it's happening, I just hate that it is. Recently I tried to apply for some $15/hr part-time job at a local museum that a caveman could do, and I stopped cold when I realized I had to transcribe every detail of the documents I just gave them into this bullshit backend website that looked like it was about a thousand years old. No Thank You. Currently I'm all worked up because I just applied to work at a hip, culty, local theater, and I was shocked that after completing the totally normal application routine, I received an automated email directing me to "complete your profile" as "an important part of the hiring process" on the website of the company they're outsourcing all their HR and billing stuff to. And I go look at the profile thingy, and of course it's just this needlessly complicated interface where I can individually enter each and every piece of information that I just provided in my resume--no more, no less. The theater has exactly two locations and is kind of a niche operation and it is absolutely crazy to me that they think they need to pay for this extra layer of stupidly bloated and redundant "talent acquisition" processing when they're hiring for like two or three basic ass hourly roles where half the question is going to be "have you done this normal shit before" and half will be "can we stand your personality". Nobody needs this garbage at all, least of all ME.
13 notes
·
View notes
Text
1st HRT Appointment
Hi folks, I promised that I'd make this post abt my first HRT appointment, so here that is. Most everything will be below the cutoff just so it doesn't clog up too much space :)
Background: 20 y/o, AFAB, trans guy, living in MA, going to Fenway Health at the Sidney Borum Jr. Health Center in Boston. Seeking testosterone HRT
I made this appointment last week, and got in today (2/17/23). Prior to my appointment, they had sent multiple reminder texts leading up to the appointment as well as a confirmation text about 7 days prior.
On the day of my appointment, I was sent a secure video link via text that I could easily access using the Chrome app on my phone, as they do not use Zoom to conduct telehealth appointments. I also got a text stating how much I owed prior to the appointment.
The nurse practitioner I saw asked a lot of basic questions regarding family medical history, past diagnoses, allergies, surgical history, etc. Since I use a different provider as a PCP, she asked if I wanted to switch my PCP over or if I was just there for gender affirming treatment. In my case, it was the latter, however, not all insurances will let you do that, so make sure to call up your insurance and ask. For reference, I use BCBS PPO.
Afterwards, I was asked about my experiences with gender, how long I've felt 'different', when I came out, how people reacted, support systems, dysphoria/euphoria, if I want biological kids, etc. I was also asked about what I want the most from testosterone.
When that was done, she had me sign up for their MyChart system, which, since my PCP uses the same system, I can easily transfer information over from one provider to the next. She then put in blood orders for various things that I can do either at their office at my next appointment or at a local lab. She also said that I'd be getting a call shortly after the appointment ended to schedule an in-person physical. She also sent me a link to a PDF regarding the benefits and risks of testosterone.
About 45 minutes after the call ended, I got a call to schedule the aforementioned appointment. Unfortunately, the only day that worked for me isn't for another 2 months, so that's where a different doctor will do a physical.
Overall, it was a very friendly experience and I really appreciated not being deadnamed on every single piece of paperwork. Seriously, they are fantastic about not using my (legal) deadname unless it's absolutely 100% legally necessary.
I'll probably also update y'all once I'm able to get to that 2nd appointment.
LMK if you have any Q's, maybe I can answer them, but I truly hope this was useful to somebody! If it is, I'm happy.
3 notes
·
View notes
Text
Improving Patient Outcomes with Smart Nurse Call Systems
Nurse Call Systems Industry Overview
The global nurse call systems market size is expected to reach USD 4.2 billion by 2030, based on a new report by Grand View Research, Inc. It is expected to expand at a CAGR of 12.11% from 2023 to 2030. The growth of the market can be attributed to the rising use of digital healthcare and the increasing need for patient safety and care. Furthermore, continuous technological advancements to bring new levels of communication enabling the widest range of applications configuration at home care, hospitals, or residential facilities are predicted to boost market demand.
Gather more insights about the market drivers, restrains and growth of the Nurse Call Systems Market
The growing elderly population and rising risk of diseases such as chronic respiratory disease, hypertension, cardiovascular disease, and diabetes are increasing the demand for healthcare services. This patient population needs assistance to complete their day-to-day activities, thereby surging the demand for nurse call systems in some healthcare facilities. It ensures the safety of patients in the ward. Increasing demand for integrated and diversified hospital communication systems is anticipated to favor the market growth.
The COVID-19 pandemic has indiscriminately increased the pressure on healthcare facilities and professionals. As a result, the need for wireless communication devices increased in hospitals. Nurse call systems helped to decrease the burden on the existing staff force during the pandemic when hospitals were managing COVID-19 patients above their occupancy levels. Various manufacturers expanded their manufacturing capacity to meet the sudden surge in demand.
Browse through Grand View Research's Medical Devices Industry Research Reports.
The global skin grafting device market size was valued at USD 141.0 million in 2024 and is anticipated to grow at a CAGR of 5.63% from 2025 to 2030.
The global ocular trauma devices market size was estimated at USD 4.28 billion in 2024 and is projected to grow at a CAGR of 7.4% from 2025 to 2030.
Nurse Call Systems Market Segmentation
Grand View Research has segmented the global nurse call systems market based on technology, type, application, end-use, and region:
Nurse Call Systems Technology Outlook (Revenue, USD Billion, 2016 - 2030)
Wired Communication Equipment
Wireless Communication Equipment
Nurse Call Systems Type Outlook (Revenue, USD Billion, 2016 - 2030)
Integrated Communication Systems
Buttons
Mobile Systems
Intercoms
Nurse Call Systems Application Outlook (Revenue, USD Billion, 2016 - 2030)
Alarms & Communications
Workflow Optimization
Wanderer Control
Fall Detection & Prevention
Nurse Call Systems End-use Outlook (Revenue, USD Billion, 2016 - 2030)
Hospitals
ASCs/Clinics
Long-Term Care Facilities
Nurse Call Systems Regional Outlook (Revenue, USD Billion, 2016 - 2030)
North America
US
Canada
Europe
UK
Germany
France
Italy
Spain
Asia Pacific
China
Japan
India
Australia
South Korea
Latin America
Brazil
Mexico
Argentina
Middle East & Africa
South Africa
UAE
Saudi Arabia
Key Companies profiled:
Hill-Rom Holding, Inc.
Rauland Corporation
Honeywell International, Inc.
Ascom Holding AG
TekTone Sound and Signal Mfg., Inc.
Austco Healthcare
Stanley Healthcare
Critical Alert Systems LLC
West-Com Nurse Call Systems, Inc.
JNL Technologies
Cornell Communications
Order a free sample PDF of the Nurse Call Systems Market Intelligence Study, published by Grand View Research.
0 notes
Text
Nurse Call Systems Market Key Companies, Growth and Forecast Report, 2030
The global nurse call systems market size was valued at USD 1.7 billion in 2022 and is expected to expand at a compound annual growth rate (CAGR) of 12.11% from 2023 to 2030.
The growing need for a diverse and integrated platform that increases the preference for mobility aids are driving the market. Medicare decides to refund schemes based on quality and outcome rather than quantity owing to the rising healthcare cost. Medicare estimates that current reimbursement practices are costing an additional USD 2.1 billion and expects to curtail this by using technology-focused healthcare. With this change in reimbursement policies, hospitals and other healthcare facilities are trying to streamline their workflow processes by adopting technology-oriented nurse call systems.
Nurse call systems enable reliable and flexible communication between the patient and the caregiver. Increasing patient numbers in healthcare facilities and the introduction of advanced ways to expand communication, workflow, and management to provide quality patient care are fueling the market growth. The market is primarily driven by technological advancements that have allowed players to create innovative devices. For instance, in December 2019, Tunstall Group launched Tunstall Carecom, a wireless and digital nurse call system.
Gather more insights about the market drivers, restrains and growth of the Nurse Call Systems Market
Blood Screening Market Report Highlights
• The reagent segment accounted for the largest revenue share of around 73.0% in 2022 and is expected to grow at the fastest CAGR of 12.0% over the forecast period.
• North America dominated the market and accounted for the largest revenue share of 39.0% in 2022 owing to the presence of key industry players, increased adoption of the blood screening process, stringent FDA regulations for transfusion, rising infectious disease prevalence, and greater patient affordability are responsible for maintaining its position during the forecast period.
• Asia Pacific is expected to grow at the fastest CAGR of 13.5% over the forecast period owing to increasing awareness about blood donation, rising patient affordability, and the focus of key industry players on emerging countries in the region.
Browse through Grand View Research's Medical Devices Industry Research Reports.
• The global emergency medical services product market size was valued at USD 22.5 billion in 2023 and is projected to grow at a compound annual growth rate (CAGR) of 6.4% from 2024 to 2030.
• The global scanning electron microscopes market size was valued at USD 4.34 billion in 2023 and is expected to grow at a compound annual growth rate (CAGR) of 8.6% from 2024 to 2030.
Blood Screening Market Segmentation
Grand View Research has segmented the blood screening market by product, technology, and region:
Blood Screening Technology Outlook (Revenue, USD Million, 2018 - 2030)
• Nucleic Acid Amplification Test (NAT)
• ELISA
• Chemiluminescence Immunoassay (CLIA) and Enzyme Immunoassay (EIA)
• Next Generation Sequencing
• Western Blotting
Blood Screening Product Outlook (Revenue, USD Million, 2018 - 2030)
• Reagent
• Instrument
Blood Screening Regional Outlook (Revenue, USD Million, 2018 - 2030)
• North America
o U.S.
o Canada
• Europe
o UK
o Germany
o France
o Italy
o Spain
o Sweden
o Norway
o Denmark
• Asia Pacific
o Japan
o China
o India
o Australia
o Thailand
o South Korea
• Latin America
o Brazil
o Mexico
o Argentina
• Middle East and Africa
o Saudi Arabia
o South Africa
o UAE
o Kuwait
Order a free sample PDF of the Nurse Call Systems Market Intelligence Study, published by Grand View Research.
#Nurse Call Systems Market#Nurse Call Systems Market size#Nurse Call Systems Market share#Nurse Call Systems Market analysis#Nurse Call Systems Industry
0 notes
Text
Call for abstract for the 13th World Gastroenterology, IBD & Hepatology Conference.
The Utilitarian Conferences Gathering is glad to invite Gastroenterologist, Hepatologist, Practitioners, Surgeons, Nurses, Professors, Authors, Researchers and Students to upload their abstracts and papers for oral presentation, poster presentation, workshop, special sessions to be presented at Gastroenterology 2023 with its motto Gastroenterology and Hepatology: A healthy digestive system is essential for overall health “Helping people inside & out”.
DEADLINE: 1ST ROUND OF SUBMISSION WILL BE CLOSED ON June 30th, 2023
GUIDELINES FOR ABSTRACTS SUBMISSION
Interested in presenting your work in one of the Twenty Six conference sessions? The call for paper is now open. In order to get an idea of how to prepare your paper, you can find more information about paper submission here. The online abstract submission system is open!
Proceed to the paper submission
Type of submission
There are three different types of contributions you can choose from within this system:
Abstract
Poster abstract
Workshop
Submit your Abstract/Paper/Research work at the 13th World Gastroenterology, IBD & Hepatology Conference on December 15-17, 2023, in Holiday Inn Dubai Al Barsha UAE & Virtual.
How to submit you’re abstract
Click the submit abstract link-https://gastroenterology.universeconferences.com/submit-abstract/
2. Click on the abstract template, and you can download the abstract template to attach your abstract as per the format.
3. Fill in the below details required & attach your poster to the abstract link.
4· Once; you are done with the submission; we will review the abstract and send you an email by attaching the acceptance letter.
5. After receiving the acceptance letter you will be eligible for the registration process.
No alt text provided for this image
6. Kindly upload your Abstract/presentation here:
7. Don't forget to attach your Abstract/presentation file here:
8. Once, you are Complete with the Submission; the organizing committee team will review your abstract and send you the acceptance.
Conference Key Sessions:
Gastroenterology | Hepatology | Hepatitis | Gastrointestinal Pathology | Gastrointestinal Cancer | Covid-19 effects on gastroenterology practices | Small Bowel and Colonic Disease | Pancreatic and biliary disease | Esophageal and Gastric Disease | Abdominal & Primary Care | Microbiota | Celiac Diseases | Pediatric Gastroenterology | Gastrointestinal Surgery | Innovation & Technology in Gastroenterology | Digestive Disorders | Gallbladder & Biliary Diseases | Inflammatory Bowel Disease | Gastrointestinal Radiology | Gastroenteritis | Bariatric Surgery | Liver Biopsy | Gastroenterology Treatment | Gastrointestinal Immunology | Gut Microbiome & Probiotics Interactior | Neuro Gastroenterology and more.
Follow the link for more info and to Submit: https://gastroenterology.universeconferences.com/submit-abstract/
What Sapp No: +442033222718
Contact No- +1 2073070027
To submit your abstract/research paper for an oral or poster or young research presenter contribution to Gastroenterology 2023, please fill your details in the abstract submission form. Once you submit your details, you can upload your abstract (format allowed: .doc / .docx / .pdf). The author account is must needed for communication purposes. Abstracts can be submitted by email. Speakers/Presenters can submit a maximum of three abstracts. All abstracts must be submitted in English. Please do not submit too many copies of the same abstract. All abstracts will be forwarded to the Scientific and Program Committee Experts for the review process. Once accepted, you will receive a confirmation email from our side.
Digestive Disease Conferences, Digestive Disease Meetings, Digestive Disease Congress, Digestive Disease Workshop, Digestive Disease Symposiums, Digestive Disease Seminars, Digestive Disease Expo, Digestive Disease Exhibitions, Hepatologists Conferences, Hepatologists Meetings, Hepatologists Congress, Hepatologists Workshop, Hepatologists Symposiums, Hepatologists Seminars, Hepatologists Expo, Hepatologists Exhibitions, Liver Transplantation, Liver Treatment, Surgery Conferences | Coronavirus Gastroenterology
Gastroenterology Conferences 2023, International Gastroenterology Conferences 2023, Gastroenterology Conferences 2023 USA, International Gastroenterology Conferences 2023, European Gastroenterology Conference 2023, Pediatric Gastroenterology Conferences 2023, Hepatology Conference 2023, Gastro conference 2023 UK, Hepatology Conferences 2023, World Liver Conference 2023, Hepatology Conferences 2023 in Dubai, Gastroenterology Conferences 2023, Endoscopy Conferences 2023, Endoscopy Conferences 2023 UK, Hepatitis Conference 2023, Endoscopy Conferences Middle East, Gastro Conferences, Endoscopy Conference 2023, Endoscopy Conferences 2023, Endoscopy Conference 2023 Australia, Gastroenterology Conferences 2023, International Gastroenterology Conferences 2023, Global Endocrinology Conferences
0 notes
Text
Medical Alert Systems Market – Latest Scenario and Future Aspect Analysis 2022-2031
New York, Global Medical Alert Systems Market from Global Insight Services is the only authoritative source for intelligence on the Medical Alert Systems Market . The report will provide you with an analysis of the impact of the latest market disruptions such as the Russo-Ukrainian War and Covid-19 on the market. The report provides a qualitative analysis of the market using various frameworks such as Porters Analysis and PESTLE. The report includes in-depth segmentation and market size data by categories, product types, applications, and geographic regions. The report also includes a comprehensive analysis of key issues, trends and drivers, restraints and challenges, competitive landscape, as well as recent events such as mergers and acquisitions activities in the market.
Download a Free PDF Sample Copy of Report – https://www.globalinsightservices.com/request-sample/GIS20250/
A medical alert system is a device that is worn by a person with a medical condition, such as a heart condition, that requires immediate medical attention. The device is usually worn around the neck or wrist, and it is connected to a monitoring center. When the person wearing the device needs medical assistance, they can push a button on the device, which will send a signal to the monitoring center. The monitoring center will then contact the person’s emergency contacts, such as their family or friends, and provide them with the person’s location.
Key Market Players
Bay Alarm Medical
MobileHelp
Ascom Wireless Solutions
ADT Corporation
LifeFone
Hill-Rom Holdings Inc.
Key Trends
There are several key trends in Medical Alert Systems technology. One is the development of mobile medical alert systems. These systems allow users to carry a small, portable device with them at all times. The device can be used to call for help in an emergency situation, even if the user is unable to speak. The other trend is the development of systems that can be integrated with other medical devices. For example, some systems now include a fall detection feature. If the system detects a fall, it will automatically call for help.
The development of systems that can be used in conjunction with GPS is one of the other trends in the market. This allows the system to send help to the user’s location in an emergency. Finally, there is a trend toward systems that are more user-friendly. Many systems now include features such as voice-activated call buttons and large, easy-to-read displays.
Key Drivers
There are several key drivers of the medical alert systems market. One of the most important drivers is the aging population. As people live longer, they are more likely to experience chronic health conditions that can benefit from having a medical alert system in place. Another key driver is the increasing prevalence of chronic diseases such as diabetes and heart disease. This is leading to a greater need for people to have access to medical help in case of an emergency. The other driver of the medical alert systems market is the increasing cost of healthcare. As healthcare costs continue to rise, more people are looking for ways to reduce their costs. This is leading to a greater demand for medical alert systems.
Get Customized report as per your requirements – https://www.globalinsightservices.com/request-customization/GIS20250/
Key Market Segments
By System Type
Nurse Calling System (NCS)
Personal Emergency Response Systems (PERS)
Smart Belt
By Technology
IP-based Systems
Medical Alert Alarm (Button) System
Two-Way Voice System
Unmonitored Medical Alert Systems
By Application
Assisted Living Facilities
Home-Based User
Hospitals and Clinics
Senior Living Facilities
Others
By Distribution Channel
Offline
Online
Buy your copy now: https://www.globalinsightservices.com/checkout/single_user/GIS20250/
With Global Insight Services, you receive:
10-year forecast to help you make strategic decisions
In-depth segmentation which can be customized as per your requirements
Free consultation with lead analyst of the report
Excel data pack included with all report purchases
Robust and transparent research methodology
About Global Insight Services:
Global Insight Services (GIS) is a leading multi-industry market research firm headquartered in Delaware, US. We are committed to providing our clients with highest quality data, analysis, and tools to meet all their market research needs. With GIS, you can be assured of the quality of the deliverables, robust & transparent research methodology, and superior service.
Contact Us: Global Insight Services LLC 16192, Coastal Highway, Lewes DE 19958 E-mail: [email protected] Phone: +1-833-761-1700
0 notes
Text
Nurse Call Systems Market 2021 Industry Outlook, Key Players, Segmentation Analysis, Business Growth and Forecast to 2027
The reports also help in understanding the Nurse Call Systems Market Value dynamic, and structure by analyzing the market segments and projecting the Nurse Call Systems Market Value. Clear representation of competitive analysis of key players by Design, price, financial position, product portfolio, growth strategies, and regional presence in the Nurse Call Systems Market Value makes the report investor's guide.
Nurse Call Systems Market Overview:
This Nurse Call Systems Market industry research provided a comprehensive analysis of the worldwide Nurse Call Systems Market, taking into account all critical variables such as growth factors, limitations, market advancements, top investment pockets, future prospects, and trends. The research begins by emphasizing the important trends and possibilities that may develop in the near future and have a favorable influence on overall industry growth.
The Nurse Call Systems Market size is expected to reach US$ 3.86 Bn. by year 2029 at a CAGR of 9.4% during the forecast period.
Request a Free PDF Sample Report @
Market Scope:
Nurse Call Systems Market Research Report analyzed the current state of the definitions, classifications, applications, and industry chain structure. The analysis provides unbiased professional commentary on the present market scenario, prior market performance, production and consumption rates, demand and supply ratios, and income generation forecasts for the projected period. The Nurse Call Systems Market study also gives information on the leading businesses functioning in the Nurse Call Systems Market industry's strategic ambitions and company growth strategies. Mergers and acquisitions, government and corporate transactions, partnerships and collaborations, joint ventures, brand promotions, and product launches are among the methods evaluated in the research. To summarise what has been said thus far,
The Nurse Call Systems Market report presents insights into each of the leading Nurse Call Systems Market end users along with annual forecasts to 2027. The report provides revenue forecasts with sales and growth rate of the global Nurse Call Systems Market. Forecasts are also provided for the market's product, application, and geographic segments. Forecasts are produced to help people understand the industry's future outlook and potential.
Segmentation:
Wireless Nurse Call Systems are expected to grow at a xx% rate of CAGR during the forecast period. An introduction of the day-to-day technological advancements is offering wide opportunities in the healthcare sector. The wireless nurse call systems in hospitals are playing a crucial that enable and ensure proper care to the patients by the nurses. Wireless nurse call systems are becoming more popular. It helps to reduce the installation cost over the wired network.
https://www.maximizemarketresearch.com/request-sample/65267
Key Players:
The research includes the most recent news and industry developments regarding Nurse Call Systems Market expansions, acquisitions, growth strategies, joint ventures and collaborations, product launches, market expansions, and so on. Among the main companies in the Nurse Call Systems Market, the sector is
• Rauland-Borg Corporation • Hill-Rom Holdings, Inc. • Ascom Holding AG • Azure Healthcare Ltd • Schrack Seconet AG. • Intercall Systems, Inc • Jeron Electronic Systems • Johnson Controls International Plc • Nurse Call Systems • Siemens • Honeywell International Inc. • STANLEY Healthcare • Tunstall Group • West-Com Nurse Call Systems, Inc. • Critical Alert • Vigil Health Solutions Inc. • Cornell Communications
Regional Analysis:
The primary goal of this study is to assist the user in understanding the market in terms of definition, segmentation, market potential, significant trends, and the problems that the industry is experiencing across ten key regions.
COVID-19 Impact Analysis on Nurse Call Systems Market:
The research details the overall impact of COVID-19 on the Health Insurance Market by providing a micro- and macroeconomic analysis. The precise study focuses on market share and size, which clearly depicts the impact that the pandemic has had and is anticipated to have on the global Health Insurance Market in the future years.
Want your Report customized?
Key Questions answered in the Nurse Call Systems Market Report are:
What is the function of the Nurse Call Systems Market?
What is the predicted revenue generation of the Nurse Call Systems Market?
At what growth rate is the Nurse Call Systems Market evolving?
Who are the major market giants operating in the Nurse Call Systems Market?
About Us:
Maximize Market Research provides B2B and B2C research on 12000 high-growth emerging opportunities & technologies as well as threats to the companies across the Healthcare, Pharmaceuticals, Electronics & Communications, Internet of Things, Food and Beverages, Aerospace and Defense, and other manufacturing sectors .
Contact Us:
MAXIMIZE MARKET RESEARCH PVT. LTD
3rd Floor, Navale IT Park Phase 2,
Pune Banglore Highway,
Narhe, Pune, Maharashtra 411041, India.
Nurse Call Systems Market Size, Share, Analysis, Growth, Trends, Drivers, Opportunity
0 notes
Text
Trends | Future and Growth for Patient Engagement Technology Market
The global patient engagement solutions market in terms of revenue was estimated to be worth $17.3 billion in 2022 and is poised to reach $27.9 billion by 2027, growing at a CAGR of 10% from 2022 to 2027.
The factors driving the growth of this market are implementation of changing government regulations and healthcare initiatives to promote patient-centric care, high demand for patient engagement solutions in the post pandemic era, and the growing utilization of m-health apps.However, interoperability for patient engagement solutions and a shortage of skilled IT professionals in the healthcare industry are expected to restrain the growth of this market during the forecast period.
In March 2020, the US President signed a USD 2 million coronavirus emergency stimulus package called the CARES (Coronavirus Aid, Relief, and Economic Security) Act. The law expands cover treatment and services for those affected by COVID-19. The CARES Act also increases flexibility for Medicare to cover telehealth services; authorizes Medicare certification for home health services by physician assistants, nurse practitioners, and certified nurse specialists; and increases Medicare payments for COVID-19-related hospital stays and durable medical equipment. Such initiatives/regulations are expected to increase further the demand and adoption of patient engagement solutions in major markets worldwide.
Download PDF Brochure @ https://www.marketsandmarkets.com/pdfdownloadNew.asp?id=105975994
Payers have made substantial investments in infrastructure and proprietary systems in the past. Moving or integrating these systems with patient engagement solutions will pose various challenges to these organizations in terms of cost. It will also require changes to their current systems that are optimized to handle only their current requirements. Also, the move to cloud-based patient engagement solutions would involve changing the current IT architecture, especially in hospitals that already serve as hubs connecting multiple physicians, labs, and pharmacists. Hence, finding the resources to achieve large-scale interoperability and interconnectivity could hamper the transition to cloud-based patient engagement solutions for such healthcare institutions.
Download PDF Brochure: https://www.marketsandmarkets.com/pdfdownloadNew.asp?id=195345983
Browse in-depth TOC on “Patient Engagement Technology Market” 16 – Tables 9 – Figures 70 – Pages
The patient engagement technology market is projected to rapidly grow as the healthcare industry witnessed a change to a value-based reimbursement system from the traditional volume-based fee for reimbursement system and quality treatment. Adoption of patient engagement technology provides the healthcare industry to minimize price while improving the quality of healthcare. The patient engagement technology also delivers positive returns on investment.
Furthermore, legislative reforms of The Health Insurance Portability and Accountability Act (HIPAA), Affordable Care Act (ACA) in the U.S. and Health and Social Care Act 2008 in Europe, government incentives, increasing aging population, and rising awareness to self-monitor health, has stimulated the adoption of patient engagement technology in the healthcare industry. However, in spite of numerous benefits, certain barriers such as large investments requirement, fragmented end-user market, and security and safety of patient data are restraining the growth of this market.
Request Sample Pages: https://www.marketsandmarkets.com/requestsampleNew.asp?id=195345983
The study provides granular information about the pricing of patient engagement technology with a breakdown into several price components. The report also provides insights on replacement market for patient engagement technology and factors affecting the replacement trends; this market presents numerous opportunities for vendors in the market due to the dearth of allied functionality and interoperability issues in the existing patient engagement technology.
0 notes
Text
Machine learning's crumbling foundations

Technological debt is insidious, a kind of socio-infrastructural subprime crisis that’s unfolding around us in slow motion. Our digital infrastructure is built atop layers and layers and layers of code that’s insecure due to a combination of bad practices and bad frameworks.
Even people who write secure code import insecure libraries, or plug it into insecure authorization systems or databases. Like asbestos in the walls, this cruft has been fragmenting, drifting into our air a crumb at a time.
We ignored these, treating them as containable, little breaches and now the walls are rupturing and choking clouds of toxic waste are everywhere.
https://pluralistic.net/2021/07/27/gas-on-the-fire/#a-safe-place-for-dangerous-ideas
The infosec apocalypse was decades in the making. The machine learning apocalypse, on the other hand…
ML has serious, institutional problems, the kind of thing you’d expect in a nascent discipline, which you’d hope would be worked out before it went into wide deployment.
ML is rife with all forms of statistical malpractice — AND it’s being used for high-speed, high-stakes automated classification and decision-making, as if it was a proven science whose professional ethos had the sober gravitas you’d expect from, say, civil engineering.
Civil engineers spend a lot of time making sure the buildings and bridges they design don’t kill the people who use them. Machine learning?
Hundreds of ML teams built models to automate covid detection, and every single one was useless or worse.
https://pluralistic.net/2021/08/02/autoquack/#gigo
The ML models failed due to failure to observe basic statistical rigor. One common failure mode?
Treating data that was known to be of poor quality as if it was reliable because good data was not available.
Obtaining good data and/or cleaning up bad data is tedious, repetitive grunt-work. It’s unglamorous, time-consuming, and low-waged. Cleaning data is the equivalent of sterilizing surgical implements — vital, high-skilled, and invisible unless someone fails to do it.
It’s work performed by anonymous, low-waged adjuncts to the surgeon, who is the star of the show and who gets credit for the success of the operation.
The title of a Google Research team (Nithya Sambasivan et al) paper published in ACM CHI beautifully summarizes how this is playing out in ML: “Everyone wants to do the model work, not the data work: Data Cascades in High-Stakes AI,”
https://storage.googleapis.com/pub-tools-public-publication-data/pdf/0d556e45afc54afeb2eb6b51a9bc1827b9961ff4.pdf
The paper analyzes ML failures from a cross-section of high-stakes projects (health diagnostics, anti-poaching, etc) in East Africa, West Africa and India. They trace the failures of these projects to data-quality, and drill into the factors that caused the data problems.
The failures stem from a variety of causes. First, data-gathering and cleaning are low-waged, invisible, and thankless work. Front-line workers who produce the data — like medical professionals who have to do extra data-entry — are not compensated for extra work.
Often, no one even bothers to explain what the work is for. Some of the data-cleaning workers are atomized pieceworkers, such as those who work for Amazon’s Mechanical Turk, who lack both the context in which the data was gathered and the context for how it will be used.
This data is passed to model-builders, who lack related domain expertise. The hastily labeled X-ray of a broken bone, annotated by an unregarded and overworked radiologist, is passed onto a data-scientist who knows nothing about broken bones and can’t assess the labels.
This is an age-old problem in automation, pre-dating computer science and even computers. The “scientific management” craze that started in the 1880s saw technicians observing skilled workers with stopwatches and clipboards, then restructuring the workers’ jobs by fiat.
Rather than engaging in the anthropological work that Clifford Geertz called “thick description,” the management “scientists” discarded workers’ qualitative experience, then treated their own assessments as quantitative and thus empirical.
http://hypergeertz.jku.at/GeertzTexts/Thick_Description.htm
How long a task takes is empirical, but what you call a “task” is subjective. Computer scientists take quantitative measurements, but decide what to measure on the basis of subjective judgment. This empiricism-washing sleight of hand is endemic to ML’s claims of neutrality.
In the early 2000s, there was a movement to produce tools and training that would let domain experts produce their own tools — rather than delivering “requirements” to a programmer, a bookstore clerk or nurse or librarian could just make their own tools using Visual Basic.
This was the radical humanist version of “learn to code” — a call to seize the means of computation and program, rather than being programmed. Over time, it was watered down, and today it lives on as a weak call for domain experts to be included in production.
The disdain for the qualitative expertise of domain experts who produce data is a well-understood guilty secret within ML circles, embodied in Frederick Jelinek’s ironic talk, “Every time I fire a linguist, the performance of the speech recognizer goes up.”
But a thick understanding of context is vital to improving data-quality. Take the American “voting wars,” where GOP-affiliated vendors are brought in to purge voting rolls of duplicate entries — people who are registered to vote in more than one place.
These tools have a 99% false-positive rate.
Ninety. Nine. Percent.
To understand how they go so terribly wrong, you need a thick understanding of the context in which the data they analyze is produced.
https://5harad.com/papers/1p1v.pdf
The core assumption of these tools is that two people with the same name and date of birth are probably the same person.
But guess what month people named “June” are likely to be born in? Guess what birthday is shared by many people named “Noel” or “Carol”?
Many states represent unknown birthdays as “January 1,” or “January 1, 1901.” If you find someone on a voter roll whose birthday is represented as 1/1, you have no idea what their birthday is, and they almost certainly don’t share a birthday with other 1/1s.
But false positives aren’t evenly distributed. Ethnic groups whose surnames were assigned in recent history for tax-collection purposes (Ashkenazi Jews, Han Chinese, Koreans, etc) have a relatively small pool of surnames and a slightly larger pool of first names.
This is likewise true of the descendants of colonized and enslaved people, whose surnames were assigned to them for administrative purposes and see a high degree of overlap. When you see two voter rolls with a Juan Gomez born on Jan 1, you need to apply thick analysis.
Unless, of course, you don’t care about purging the people who are most likely to face structural impediments to voter registration (such as no local DMV office) and who are also likely to be racialized (for example, migrants whose names were changed at Ellis Island).
ML practitioners don’t merely use poor quality data when good quality data isn’t available — they also use the poor quality data to assess the resulting models. When you train an ML model, you hold back some of the training data for assessment purposes.
So maybe you start with 10,000 eye scans labeled for the presence of eye disease. You train your model with 9,000 scans and then ask the model to assess the remaining 1,000 scans to see whether it can make accurate classifications.
But if the data is no good, the assessment is also no good. As the paper’s authors put it, it’s important to “catch[] data errors using mechanisms specific to data validation, instead of using model performance as a proxy for data quality.”
ML practitioners studied for the paper — practitioners engaged in “high-stakes” model building reported that they had to gather their own data for their models through field partners, “a task which many admitted to being unprepared for.”
High-stakes ML work has inherited a host of sloppy practices from ad-tech, where ML saw its first boom. Ad-tech aims for “70–75% accuracy.”
That may be fine if you’re deciding whether to show someone an ad, but it’s a very different matter if you’re deciding whether someone needs treatment for an eye-disease that, untreated, will result in irreversible total blindness.
Even when models are useful at classifying input produced under present-day lab conditions, those conditions are subject to several kinds of “drift.”
For example, “hardware drift,” where models trained on images from pristine new cameras are asked to assess images produced by cameras from field clinics, where lenses are impossible to keep clean (see also “environmental drift” and “human drift”).
Bad data makes bad models. Bad models instruct people to make ineffective or harmful interventions. Those bad interventions produce more bad data, which is fed into more bad models — it’s a “data-cascade.”
GIGO — Garbage In, Garbage Out — was already a bedrock of statistical practice before the term was coined in 1957. Statistical analysis and inference cannot proceed from bad data.
Producing good data and validating data-sets are the kind of unsexy, undercompensated maintenance work that all infrastructure requires — and, as with other kinds of infrastructure, it is undervalued by journals, academic departments, funders, corporations and governments.
But all technological debts accrue punitive interest. The decision to operate on bad data because good data is in short supply isn’t like looking for your car-keys under the lamp-post — it’s like driving with untrustworthy brakes and a dirty windscreen.
Image: Seydelmann (modified) https://commons.wikimedia.org/wiki/File:GW300_1.jpg
CC BY-SA: https://creativecommons.org/licenses/by-sa/3.0/deed.en
Cryteria (modified) https://commons.wikimedia.org/wiki/File:HAL9000.svg
CC BY: https://creativecommons.org/licenses/by/3.0/deed.en
116 notes
·
View notes
Text
Patient Aggression and Physician Burnout: The Makings of a Human Resources Crisis in Health Care
Grady, C. (2022, January 27). Patient aggression and physician burnout: The makings of a human resources crisis in health care. The Conversation. https://theconversation.com/patient-aggression-and-physician-burnout-the-makings-of-a-human-resources-crisis-in-health-care-175017

Colleen Grady writes: "Even before the pandemic, managing patient expectations and dealing with disruptive behaviour in medical clinics was already the top stressor for physicians. It was identified as the biggest contributor to burnout in a recent survey by the Ontario Medical Association (OMA)...A 2021 survey by advocacy group Doctors Manitoba found that 57 per cent of physicians reported mistreatment from at least one patient in the previous month. Verbal abuse included racist and sexist attacks, as well as being compared to a Nazi and accused of profiting from the pandemic. Other aggressive incidents included being spit on, vandalism, social media attacks, physical assault and death threats."
"The Quadruple Aim approach to health systems has four pillars: optimizing patient experience, improving population health, reducing costs and supporting health-care providers. Previous research indicated that 'care of the provider' was least likely of the four aims to be addressed. Similarly, the OMA survey found that addressing patient expectations — the No. 1 stressor — and providing solutions to deal with it falls way down on the list of priorities for those same physicians, behind addressing other stressors like administrative overload and work-life balance. This suggests the biggest contributor to physician burnout is unlikely to change even when the added stressors of the pandemic end."
"Making change requires speaking out about what needs to change, such as calling the abuse and mistreatment of physicians what it is. That is what Doctors Manitoba did following the disturbing results from its physician survey. Nudging patients to reconsider demands made of their family physician may require consistent messaging to be used and supported by all levels of government, so that there are no repercussions for physicians to speaking up...Federal party leaders have expressed support for health-care workers during the COVID-19 pandemic, including condemned the harassment of health-care workers and blocking patient access at hospital protests. This support should not dissipate when COVID-19 eventually ends, and the time comes to address growing problems in health care identified during the pandemic."
Additional Information
Gajjar, J. et al. (2021). Healing the Healers: System-Level Solutions to Physician Burnout. Ontario Medical Association. PDF: https://www.oma.org/uploadedfiles/oma/media/pagetree/advocacy/health-policy-recommendations/burnout-paper.pdf
How to manage conflict and aggressive behaviour in medical practice. CMPA. https://www.cmpa-acpm.ca/en/advice-publications/browse-articles/2017/how-to-manage-conflict-and-aggressive-behaviour-in-medical-practice
(2021). Physician Abuse and Mistreatment: A Growing Concern. Doctors Manitoba. PDF: https://assets.doctorsmanitoba.ca/documents/Physician-Mistreatment-Survey-Report.pdf
Premier's Council on Improving Healthcare and Ending Hallway Medicine. (2019). A Healthy Ontario: Building a Sustainable Health Care System. Ontario. PDF: https://files.ontario.ca/moh-healthy-ontario-building-sustainable-health-care-en-2019-06-25.pdf
Reichert, C. (2017). Enough is Enough: Putting a Stop to Violence in the Health Care Sector. The Canadian Federation of Nurses Unions. PDF: https://nursesunions.ca/wp-content/uploads/2017/05/CFNU_Enough-is-Enough_June1_FINALlow.pdf
Strategies to stop workplace violence before it occurs. Advisory Board. https://advisory-prod.azureedge.net/-/media/project/advisoryboard/shared/research/cbc/infographics/2020/cbc-workplace-violence-infographic/wf1923558-cbc-workplace-violence-infographic.pdf
Naish, J. et al. (2002). Brief encounters of aggression and violence in primary care: a team approach to coping strategies. Family Practice, 19(5), 504-510. DOI: https://doi.org/10.1093/fampra/19.5.504 Open Access
Grady, C. (2020). Physician burden — not just for physicians anymore. Can J Physician Leadership, 7(1), 10-13. DOI: https://doi.org/10.37964/cr24721 Open Access
Photo Source: Jimenez, C. (2019). Untitled [Photograph]. Unsplash. https://unsplash.com/photos/vGu08RYjO-s
6 notes
·
View notes
Text
Gang Stalking in Vehicles Now because illegal voyeurism, surveillance & listening isn't Enough!

I submitted a type to the local authorities! Yes, again! There's always more with these things that call themselves people! To https://new.tipsubmit.com/en/create-report/anonymous/ChicagoPD There are cars that drive around all day thru and on these streets listed including the parking garage of Truman college. This car and/or cars drive loudly and rev up their engine all day and at all times while driving. The noise is so loud and constant, it sounds like drag racing down the streets. There are many elderly people and children in this area due to school close and elderly/nursing homes in the area! We have made complaints to Truman security and they have done a great job with handling the noise nuisances, as they are still working to catch them they have stop a few which in turn has detoured the other one(s). I hope that this promotes the police to patrol more around the City College/Truman and in the general area and not just when the mayor shows up at a near by school. A bigger and deeper police presence would help detour these criminals. There wasn't an issue with police always in the area but now for some odd reason you all/police are not around when needed and desired to be around!
*****Sec. 12-602. Mufflers, prevention of noise.*****
Every motor vehicle driven or operated upon the highways of this State shall at all times be equipped with an adequate muffler or exhaust system in constant operation and properly maintained to prevent any excessive or unusual noise. No such muffler or exhaust system shall be equipped with a cutout, bypass or similar device. No person shall modify the exhaust system of a motor vehicle in a manner which will amplify or increase the noise of such vehicle above that emitted by the muffler originally installed on the vehicle, and such original muffler shall comply with all the requirements of this Section.
IL Administrative Code Section 902.120: Standards applicable to all passenger cars and to other motor vehicles
Passenger vehicles and other motor vehicles under 8,000 pounds in weight may produce up to 74 db A when speed limit is under 35 mph, or 82 db A where speed limit is over 35 mph (with 3% allowed variance). Most vehicles fall into this category.
Table below displays all vehicle exhaust noise level requirements as per Illinois Administrative Code:
Illinois vehicle noise limits: Speed limit < 35 mph Speed limit > 35 mph All vehicles under 8,000 pounds 74-76 dB A 82 – 85 dB A All vehicles over 8,000 pounds 80 – 82 dB A 86 dB A Motorcycles 86 dB A 90 dB A
“dB A” means the composite abbreviation for the A-weighted sound level and the unit of sound level, the decibel.
Illinois noise limit penalties:
Violating car noise limits in Illinois carries a $75 – $125 fine.
Sources and more info:
Illinois Compiled Statutes: Vehicle Code, Chapter 12: Equipment of Vehicles, Article VI: Miscellaneous Requirements, Section 12-602: Mufflers, prevention of noise.
Illinois Noise Related Statutes and Regulations (.pdf file; see or search for “Section 902.120”, “Section 902.121”, “Section 902.122”); or:
Illinois Administrative Code, Title 35: Environmental Protection, Subtitle H: Noise, Chapter I: Pollution Control Board, Part 902: Sound Emission Standards and Limitations for Motor Vehicles, Subpart B.
This has been going on for over a year. Gang stalking w/the dumbest criminals that do everything possible to let me know their watching! I guess at the end of the day, I might want to be a bit grateful for them being so "braggadocious"!
#stalking#gang stalking#children#harassment#illegal surveillance#mentally disturb people#mental cases
2 notes
·
View notes
Text
I’m just going to copy/paste this because it took me hours and I’m drained.
I guess I have to format it again if I want it to show up at all...
I couldn't even make it back home before breaking down crying again.
Driving while chronically sleep deprived, exhausted, fatigued, and dissociating is bad enough. Doing it with all that AND without being able to see? How special.
I barely had time to sit down, my phone rang. I answered it, begging for someone to hear me. For thirty straight seconds. "Hello? Hello? Hello???" Finally someone spoke, but they couldn't hear me. I'm sobbing. They hung up. I scrambled to call back, from my computer, because at least then I'm not fighting a lack of reception as well as my anxiety. They called again. I didn't answer. I waited for my computer to ring through instead. I'm put on hold. I'm sobbing. It was just to ask what my pharmacy is. Which I already answered on my paperwork. Which I answered, again, at check-out. And I was forced into a third confirmation via a pointless, needless, anxiety-attack inducing phone call hazing. For something I already answered.
It's not fucking fun. People don't choose this. I didn't choose this. But does it matter? "Call," the command comes. "Just call." "Call to confirm." "Call to ask." "Call." "Call." "Call."
I want you to think of something that takes physical hold of your body and brings to you to tears. I want you to hold that and sit with it until it does those things. I want you to choose to reduce yourself to a sobbing mess, struggling to breathe, alone. And I want you to picture a world where you are commanded, demanded, required to do this. For virtually everything. Imagine needing help - but you must first re-traumatize yourself with your most painful memories until your nose is running and your eyes burn from crying. And you're exhausted for the rest of the day, too. Maybe multiple days. Absolutely exhausted. So fucking depleted that taking yourself to the bathroom is almost impossible. Feeding yourself - even eating something out of a can, or microwaved - is a herculean effort. Does that sound fun? Of course not.
As for the appointment itself: It's the same. Much better bedside manner. But it's the same underlying capitalism-serving "care" system. It's my fault. I'm not trying hard enough. I'm not blacking out alone on the side of the road enough. I haven't dissociated hard enough and/or blacked out while driving yet, so it can't be that bad, right? Not until I'm maimed or dead, right? Why address the root of a problem when we can just plaster on endless band-aids instead? When we can blame you for hurting, instead of the environment that's poisoning you? I'm not medically sedating myself into an obedient little wage slave, and that's the real problem. I should aspire to produce capital for someone with most of the remaining hours of my life. That's the purpose of living, that's the reason for "health"care - not to care about health, no, just to keep the wheels of capitalism well-oiled with wasted human life. Inherent human value? Quality of life? Nah.
They refused my medical history. I brought the 72-page pdf on a flash drive. Because that's how I was given it. Because I can't afford to buy and operate a personal fax machine and/or print out a chapter book's worth of pages of medical records. I went through the trouble of getting the files, and it took over a month - only to be told "we can't take anything but paper or fax." I filled out a file release form as best I could. But I didn't have the phone number or address memorized. Not even before that place became synonymous with medical neglect and trauma for me. So now they're going to go through the ancient months-long ritual of requesting the self-fucking-same documents from LISH, either by mail or fax, because they "can't" access a flash drive or a pdf or use email. Welcome to 2021. We're back to "normal" and teleheath never existed and the internet is fake and technology is a myth and why do anything efficiently when you can waste time and do damage to people instead? My Aunt called to check in on me during her lunch break. (Thank you again) She offered to get the file printed and try to hand it in for me. I'm too tired to hope. I'm too exhausted to think they'll accept it without fuss. Anything and everything to make things harder.
Top priority order of business is the whole "diseased for life" thing. Hashimoto's thyroiditis. Hypothyroidism. Daily hormones for every day of the rest of forever, gatekept behind eternal doctor visits and prescriptions and pharmacies and copays and and and and did I mention this is forever? I've got a referral to have a thyroid sonogram done. Haven't ever had one of those before. Need to make that appointment. I was able to have my blood drawn for the thyroid testing without needing an additional appointment, which was a nice change of pace. Normally you're supposed to fast for that, but I wasn't expecting that could be done during the visit. Three years of having to make additional trips to the lab for blood work. I ate immediately before getting there, so hopefully nothing had a chance to metabolize and skew the results. Even though it was great not to have to juggle yet another appointment for health shit, it was stressful. The nurse took three tries before she had all the supplies she needed in the room. I already have anxiety spikes (which also raise my blood pressure and heart rate) for all doctor visits now. (White Coat Syndrome, I learned, it's called) I didn't need to have a rubber cable tied around my arm, popped off, tied again, popped off, and tied a third and final time to make it worse. A pro to that con: she was incredibly accurate and gentle. I normally have sub-dermal bleeding and some bruising after having blood drawn, and keep the bandage on for a day or two. The bandage didn't last even an hour after I got home - but there wasn't a single spot of trapped blood, and I almost couldn't even tell where she stuck me.
I have another new diagnosis to add to my growing collection. Hypertension. High blood pressure. I used to have slightly low blood pressure. It stunned the first doctor I ever saw (you know, because I'm fat, so that sort of thing is supposed to be ~impossible~) and it frustrated my last doctor at first, too. But now, with years of building stress and anxiety? It's almost like living with your most basic human needs barely provided (food, shelter, healthcare - let's not bring up social needs LMAO those don't count anyway, right?), and at constant risk of being taken away, for months (years, in some cases) on end, is some form of stress. It's almost like being constantly dismissed and told "you're just not trying hard enough" (WHILE TRYING YOUR BEST JUST TO SURVIVE EACH DAY) is some form of stress!It's almost like perpetual, ongoing, worsening stress has a negative impact on your heart! It's almost like there are decades of data that spell this out, plain as day!It's almost like I noticed my elevated heart rate back in NOVEMBER and mentioned it out of concern to my last doctor - who dismissed it outright because my reading in-office wasn't *that* bad, and also shouldn't I be on 5487 psych meds instead? If I was sedated out of my mind, I wouldn't be physically capable of feeling stress in my body despite the presence of real-world stress factors. That's healthy, right? Don't bother to solve the stressors, just neuter the body's response to them. Super healthy response. (Not) My GYN took note of my concern in December, when my vitals DID show as high in-office. Not that my GYN had the jurisdiction to do anything about it. I'm being put on another medication to try to mitigate this, and potentially also address some anxiety. I haven't picked it up yet. I don't know the name. I don't know if I'll be able to afford it. "Your copay is only a dollar!" Yes well, when you don't have a dollar, you can't afford a dollar, can you?
I was given a list of psychiatrists. To "Call!!"Precisely none of them are a reasonable distance away. Nearly half aren't even in my insurance network. Some explicitly exclude Medicaid. Others are exclusively for children. I was suggested a medication for depression and anxiety. I can't remember which one. Either Abilify or Lexapro? I declined it for now, either way. I wanted to be able to research it. Lexapro is just another SSRI and I already know those don't work for me. Adding a chemical bouncer to my brain to make sure the happy chemicals stay out to play doesn't help when there are no happy chemicals in the first place. A quick search for Abilify doesn't address anxiety at all so it was probably Lexapro. In which case, I am not interested in repeating a different-flavor-Prozac experience. It was not good. I didn't get any notes with that medication, regardless. I got a sticky note with "Valerian Root Extract (tea or tincture)" and "Magnesium Glycinate 2 capsules" scribbled on it, instead. Out-of-pocket home rem-maybes. I can't afford to experiment with snake oils, so mostly I'll probably just spend a bunch of time looking for data and research and studies for those substances, and that's it. If I get around to psychiatric care, I will have to start from scratch in my insurance's shoddy search tool, again. And, frankly, it's not a priority. My mental health struggles are the result of a lot of physical factors and external/social factors, and no amount of artificial chemicals bullying my brain is going to solve any of it. When your car starts leaking oil, you don't just commit to buying more oil forever and dribbling it all over, wherever you go. You fix the fucking leak. If your house has a gas leak, you don't invest in gas masks. You fix the fucking leak. If you end up with a burst pipe, you don't commit to wasting water and money and damaging your environment. You fix. The fucking. Leak. But in these comparisons, I'm getting prescribed oil and gas masks and infinite water damage/waste/bills as long-term care.
I mentioned my fatigue. It was the final straw that made me give up with the last doctor. It just keeps getting worse. It's been getting worse for over 3 years. And I'm so, so fucking tired of it getting pinned fully on the fact that I'm not on psych meds. I WAS on psych meds during part of those 3 years with my last doctor. And it didn't fucking make any difference! A daily chemical lobotomy does not address or restore my lack of physical energy. My decades-old medication-resistant insomnia has never vanished with psych meds before, and it's not likely to do it now. Especially not with yet another of the same family of chemicals that I already know don't work. I want my concern to be taken seriously. I don't want it just brushed into the mental health corner, again. Being too tired to even do the things you used to enjoy - no one fucking wants this! I don't want this! I miss being able to go for walks. I miss going to the gym. I miss seeing how much I could do, and feeling good, and feeling strong. And I can't do any of that now. Not without risking harming myself in the process.
No one wants this. I keep talking, but it feels like no one listens. At the earliest opportunity, we're back to repeating the same tired old shit that doesn't work. I try to come prepared, and the stress and time and system make sure I fail to stand up for myself anyway. I didn't get to document my disordered eating history. The relapse this year. Restricting, sometimes to the point of not eating at all. I declined to be weighed, because I want my care to be based on relevant data, vitals, blood results - not the shape and size of my body. But I was too tired to realize I needed to dodge a verbal ask for the same information. Which, it turns out, is nearly as bad a trigger as having the scale spit it out for me. Being your own advocate for equal care, when you're already tapped out? I'm not winning that challenge.
I'm frustrated. I'm not giving up, but I am frustrated and beyond tired. I don't really expect anyone to read this mess. But it's here.
3 notes
·
View notes
Text
It’s the end of the work week and, well...
I’m having thoughts on labor culture.
My father was born in 1958. He lived as the son of an absent father of five children who had no ability to truthfully express his love and care, and who instead chose to bury himself in work as a means to display his commitment. My paternal grandfather made and sold mattressees and died quite young of a cancer strain that today would’ve seemed benign. He was described as a hard worker, either up to his neck in his business or wanting just a scant few hours per day to himself. It made an aloof lover out of him and a distant father - who still loved his wife and children to bits but who felt emotionally castrated in a sense, as were men of the era.
The family consensus is that his work killed him.
My father is now 65 and survived a bout of Non-Hodgkinian Lymphoma. The oncologist and anyone with half a brain agreed that stress was the culprit. Early on, Dad had the family as an excuse for his tendency to overwork. He had to provide for us, after all, and garnish my mother’s meagre savings. All she has is her government-issued pension plan, while my father does have his own pension as a retiree of the City of Montreal’s Real-Estate Appraisal service. Considering, he felt obligated to pull a heavier load to bring in more, so they’d have better investment opportunities. Later on, he kept working out of a sense of fealty and attachment to his division, breaking out of retirement during the pandemic to join the work-from-home team. He wanted to help techs and city officials find ways to bring more of the traditionally snail-mail-based parts of the system online so the city’s Land Management service wouldn’t be paralyzed by COVID-19. What was supposed to be a single month turned into four, which turned into twelve.
By the end, they were begging him to stay on the team and to pull longer hours. We’re talking twenty hours per day, in some particularly grueling stretches. That means being logged in by breakfast and scarfing bagels down with Urban Design techs on Zoom instead of your own family, or having supper with your boss because she needs a play-by-play of the situation to stave off her executive anxiety.
Long story short, I didn’t see Dad much during the first wave. His reasoning was that he’d eventually stop, pool all this cash, and chuck it into his and Mom’s Registered Retirement Savings Account - with maybe an extra two thou or so in case the country reopened enough for their postponed trip to Cuba to take place.
Guess what? His zona flared up and he ended up with odd, shingly bumps along his scalp which to this day the local dermatologist grimaces at and tentatively has us dab with cortisone cream.
Mom, though? She’s a retired and registered nurse with a self-negating streak and a chronic propensity to undervalue her own physical ailments. Someone who quite literally understands the pain of busted hips on a clinical level because she was trained in Gerontology - and also someone who refuses to schedule an appointment with her GP and who inexplicably self-medicates with white wine.
As for me, I’m a 37 year-old man with a paycheck I consider massive with its meagre six bucks above the minimum-wage threshold - someone who chose to shack in with his folks until the current crisis ends and who therefore has a history of a single, willingly terminated apartment lease that originally began in the Planned Housing market. The apartment I want is basically a Barbie doll house for adults, a gleaming fantasy I’ll never have enough capital to touch unless I feel like trying my hand with criminal applications of my skills. The apartment I can get right now is a shithole, and I have the audacity to think I deserve a shithole that at least wasn’t someone’s former cockroach den.
Now here’s the kicker: I value my sanity and my health. I know my mental stamina levels and I know from experience that after working seven-point-five hours per day with the occasionally shorter Friday, I’ve found my limit. I could invest more if I worked more, yes, and I’m already in a better position than my parents, retirement-wise. I’ll never be rich, but I’m already set to be comfortable, provided I don’t spend my golden years trying to make it as an unsponsored TechTuber or anything else that’s equally ludicrous.
Where that’s a problem is in the toxicity this is generating. See, I have the gall to slide my daily schedule later so I can start at an hour that fits my biological clock and ends at an hour where I’m at my most creative. That means the folks saw me spending my pandemic mornings on Animal Crossing while Dad was trying to wrangle Excel spreadsheets for non-tech-savvy fellow Boomers while preventing the dog from eating his meeting notes. That means they guzzled vinho verde like it was Kool-Aid after seven while I made sure to find more concrete means to distance myself from work - ideally ones that didn’t involve functional alcoholism.
Naturally, what was bound to happen, happened: Dad soon spent his evenings calling me shiftless or “unwilling to commit”, while I was stuck watching him miss all the cues his stressed-out body were sending him. We already had Trump’s last desperate months and a global plague to handle, I really didn’t want my work to turn into more of a nuisance than it already is. I already love the people I work for and hate what I do (repeating the family cycle, it seems), but I’ve at least decided to give myself ample Me time every single day.
I’ve paired that with smaller, if consistent portfolio investments, along with a few new habits I wanted to get into to stay saner. Dad pulls crosswords or plays competitive chess in the wee hours, while I usually lay down to meditate around midnight and fall asleep by 1 AM at the latest. I’m half-expecting my father to pull a Tyler Durden and to sneer at me, at some point. “Self-care is masturbation,” he’d probably say.
Looking at classifieds for rentals, it’s obvious that the entire system is predicated on abuse. Work yourself down to the therapist’s office, right down to the fucking bone, and you just might earn a half-decent retirement because nobody’s taught you to invest incrementally. Nope, Society seems to say, you’re supposed to buy, buy and buy some more, until you realize you have ten years left to start from scratch!
I remember Dad’s face on my eighteenth birthday. “Why would you want a Disability Care Savings Account, Brain? You just turned into a legal adult by Canadian standards - you’re in no rush, right?”
I told him the real gift I wanted for my birthday, that day, was a ride to the family’s Financial Investments counsel. I pulled up the PDFs I’d printed out and filled and brought them over. From then on, if I dropped a penny in my nest-egg, Ottawa would drop another one. If my share grew, so did the government’s. In the twenty-odd years since, it’s expanded exponentially.
Dad thought I’d done this to have a big cushion by the time I’d retire. Mom thought I’d done this in case my disability worsened and I started requiring equipment or physical assistance. Honestly, my dumb, if slightly prescient eighteen year-old self figured I’d rather spend my time reading or playing video games than working. I knew I’d need something to help cushion my admittedly low career-related ambitions. I might throw several thousands at a new computer every seven to eight years, but that’s because I’ve saved them up for just as long, little by little. I have no vices beyond what sillicon offers and what you’d find in the pages of a book and don’t exactly need a big ‘ol, stonkin’ humidor stuffed with conoisseur stogies.
I have a shoebox with a poked-out Ziploc bag and a sponge, with a handful of joints and a few Santa Anas I got off of a buyer’s pool from work. Five of us occasional chair-bar goons pooled cash together on Cigar Chief and cushioned prices with a single, shared and massive order. I’m nowhere near rich, but assuming the housing market can catch its breath eventually, I’ll be able to live modestly - with one or two markers of occasional luxury I’ll have chosen.
I have a shittier job than my father has had and I’ve chosen to be happier than him. It’s just sad that the usual response elevates overwork as the supposedly one, true way to leave a mark in society.
No, Dad. I don’t want to die while my own cells eat me alive, I want to die blazed out of my fucking mind, happy because I’ll have had time to enjoy my friends’ company and to finally make some sense out of Kerouac’s Subterraneans or to figure out what the fuck is going on in Joyce’s Illiad. I’ll die crusty as shit and fulfilled as a Pop Culture jockey, because I’ll have either finished Persona 5: Golden in my lifetime or I’ll have watched the entirety of the MCU’s output before Disney finally manages to kill their golden goose.
I want to die decades from now, feeling like I at least owned my choices and didn’t spend my time tethered to someone else’s professional expectations of me.
3 notes
·
View notes
Text
ABC's Soul of a Nation is a television show that, like Shaun King, seems to seek to capitalize on the Black experience. This show depicts Black life as nothing but a giant hard luck story that laments marginalization due to racism by stereotypical white achetypes. It doesn't tell a full narrative of Black life nor does it discuss the impact of the exaltation of counterproductive behavior such as:
- Gang Culture and Violence
- Drug Culture
- Abortion
- Progressivist Elitism
- Little focus STEM education and Business
Education
The Most offensive act that Soul of a Nation commits is the omission the role of organizations such as Sigma Pi Phi (The Boule), The Links, many black greek organizations and other Black secret societies and its members. A full narrative of Black life isn't depicted if racism can't be included in the narrative. It also doesn't of blacks, who work in favor of white supremacy, to sabotage progress in the Black community. Many such black-on-Black racists have deceptively been appointed as leaders and celebrated in the Black community. Eunice Rivers, unofficial leader of the Tuskegee Experiment was heralded as a black nurse who cared as the the health of Black people. Her real role was to act as liason between Black citizens and the white supremacist medical industrial complex of the day for the purpose of using Black people for dangerous medical trials and experiments without giving full disclosure.
For more information, here are excerpts from my article, Corona Virus and Black People, https://followerofthewayforever.wordpress.com/2020/04/07/corona-virus-and-black-people/:
"Prominent black nurse, Eunice Rivers, convinced impoverished Black men to participate in a medical study wherein which they would be treated for bad blood and any other health issues. Undisclosed to them was the true purpose of the study – to observe the effects of untreated syphilis on Black men’s health. Unofficially, Rivers became head the over the project because of her forty year affiliated as a result of her continual insistence and justification of the study long after it had been found that penicillin effectively treated syphilis and many doctors abandoned the project due its unethical violation of the patients’ rights. Eunice Rivers, however, prolonged the project for profit with no regard for the men’s health nor the health of their wives and offspring."
"Black social activists such as W.E.B DuBois who promote conflict and anti-procreative behavior between Black men and Black women. DuBois was a principal conspirator of Margaret Sanger against Black people. DuBois' racist rantings against poor uneducated Black people were featured in NAACP publication and Here is what some of our Black leaders really think of us in the words of Assimilation Eugenicist W.E.B. DuBois (1932) in his article Negroes and Birth Control which Margaret Sanger often quoted:
"the mass of ignorant Negroes still breed carelessly and disastrously, so that the increase among Negroes, even more than whites, is from that part of the population least intelligent and fit, and least able to rear their children properly.” (para. 4 and para.5)"
Du Bois, W.E.B.(1939, April). Negroes and Birth Control. Smith
Libraries Exhibits, Accessed January 10, 2019, https://libex.smith.edu/omeka/files/original/16e5b6a56c2c4aedb3274e7124f3006e.jpg
W.E.B. DuBois - Boule and NAACP member who hated poor Black people and supported Margaret Sanger's population control plan of weaponizing Birth Control as a method of eugenics against Blacks. He also sabotaged Marcus Garvey's movement to steal it for himself. Promoted a Bourgeoisie-based system of black elitism against regular Black people to whom referred to as the ignorant negro masses. DuBois felt that black elitists like himself, which he called the talented tenth, should be leaders of regular Black people even though he hated regular Black people. DuBois hated regular Black people, yet wanted to be their leader for his own personal gain. He only wanted to lead them to destruction. He wanted to gain a seat at the table of white supremacy - which is a form of elitism
These people AREN'T fighting for you and don't want to be want to associated with you." Want more proof?
KIDNAPPING AND ILLEGAL ADOPTION OF THE BABIES OF THE BLACK POOR
Black mothers wonder if their babies were stolen in decades-old mystery
https://theguardian.com/world/2015/may/02/black-mothers-wonder-babies-stolen-st-louis-decades-ago
-Eighteen black women who were told decades ago that their babies had died soon after birth at a St Louis hospital now wonder if the infants were taken away by hospital officials to be raised by other families.
-Zella Jackson Price, who was 26 in 1965 when she gave birth at Homer G Phillips Hospital in St Louis.
FORCED STERILIZATION
Unwanted Sterilization and Eugenics Programs in the United States
https://www.pbs.org/independentlens/blog/unwanted-sterilization-and-eugenics-programs-in-the-united-states/
The U.S. Government's Role in Sterilizing Women of Color: Black, Puerto Rican, and Native American women have been victimized
https://www.thoughtco.com/u-s-governments-role-sterilizing-women-of-color-2834600
Racial Eugenics
https://eji.org/news/history-racial-injustice-racial-eugenics/
INSIDE UCLA'S CADAVER SCANDAL
https://www.newsweek.com/inside-uclas-cadaver-scandal-95785
ABORTION IS EUGENICS AND DEPOPULATION
Abortion is one of the most heinous methods of eugenics committed against the Black community. The highest abortion rates in the country occur among American Black women. Yet, it is heavily promoted by black women such as Ayanna Pressley, Alexis McGill Johnson, Stacey Abrams, and Kamala Harris benefit off of the killing of unborn Black people via the slaughterhouse organization that is Planned Parenthood.
David Daleiden on Selling Aborted Baby Parts: They “Cut Open the Face to Harvest the Brain”
https://www.lifenews.com/2019/09/17/david-daleiden-on-selling-aborted-baby-parts-they-cut-open-the-face-to-harvest-the-brain/
7th Shocking Video Catches Planned Parenthood Harvesting Brain of Aborted Baby Who Was Still Alive
https://www.lifenews.com/2015/08/19/7th-shocking-video-catches-planned-parenthood-harvesting-brain-of-aborted-baby-who-was-still-alive/
ABC's Soul of a Nation is Blaxploitation designed to herd Black people into state of victimhood and hopelessness by using trauma. The show has deceptively "celebrated" the Black church while promoting abortion which is a form of child sacrifice. GOD IS ADAMANTLY AGAINST HARMING CHILDREN. He says that child sacrifice is Shedding Innocent Blood and it is an abomination to HIM.
GOD LOVES CHILDREN
Proverbs 6:16-17
16These six things doth the LORD hate: yea, seven are an abomination unto him:
17A proud look, a lying tongue, and -> hands that shed innocent blood<-,
JESUS LOVES CHILDREN
Matthew 18:6
But whoso shall offend one of these little ones which believe in me,it were better for him that a millstone were hanged about his neck, and that he were drowned in the depth of the sea
Matthew 18:10
10 Take heed that ye despise not one of these little ones; for I say unto you, That in heaven their angels do always behold the face of my Father which is in heaven.
ABORTION IS AN ABOMINATION TO GOD, DO NOT MAKE YOUR CHILDREN PASS THROUGH THE FIRE
2 Kings 16:3
But he walked in the way of the kings of Israel, yea, and made his son to pass through the fire, according to the abominations of the heathen, whom the LORD cast out from before the children of Israel.
2 Kings 17:17
And they caused their sons and their daughters to pass through the fire, and used divination and enchantments, and sold themselves to do evil in the sight of the LORD, to provoke him to anger.
Ezekiel 20:31
For when ye offer your gifts, when ye make your sons to pass through the fire, ye pollute yourselves with all your idols, even unto this day: and shall I be enquired of by you, O house of Israel? As I live, saith the Lord GOD, I will not be enquired of by you
Deuteronomy18:10
There shall not be found among you any one that maketh his son or his daughter to pass through the fire,or that useth divination,or an observer of times,or an enchanter,or a witch
Jeremiah32:35
they built the high places of Baal, which R in the valley of the son of Hinnom,2 cause their sons & their daughters to pass through the fire unto Molech;which I commanded them not,neither came it into my mind,that they should do this abomination,2 cause Judah 2 sin.
BLAXPLOITATION BY LIBERAL WHITE SUPREMACY
Liberal white supremacy is at the helm of movements and organizations that make marginalized groups the mascot for causes that will largely benefit the agenda of liberalized white supremacy. Like a wolf in sheep's clothing, white supremacy has disguised itself as liberal. Yet, it is still profiting off of black trauma and black bodies (dead or alive). It has even pretended to be Black and support Black people to profit from Blackness, like, Shaun King.
Shaun King
https://twitter.com/drboycewatkins1/status/1367580588744597511?s=20
https://twitter.com/Femmefeministe/status/1371886262865567749?s=20
Reference
Sanger,M.(1939).Letter from Margaret Sanger to Dr. C.J. Gamble December 10,1939. Smith Libraries Exhibit, Accessed January 10, 2019, Retrieved from https://libex.smith.edu/omeka/files/original/d6358bc3053c93183295bf2df1c0c931.pdf
Gordon,L.(2007). Birth Control and the Negro. In The Moral Property of Women, p.235. Urbana; Chicago: University of Illiniois Press.
Winbush, W. (2019). The Subtlety of Supremacy: Joe Biden and Stacey Abrams. Retrieved from https://followerofthewayforever.wordpress.com/2019/03/25/the-subtlety-of-supremacy-joe-biden-and-stacey-abrams/
1 note
·
View note
Text
‘What do our publics look like now?’
Activity with Sadie Edginton June 16th 2020
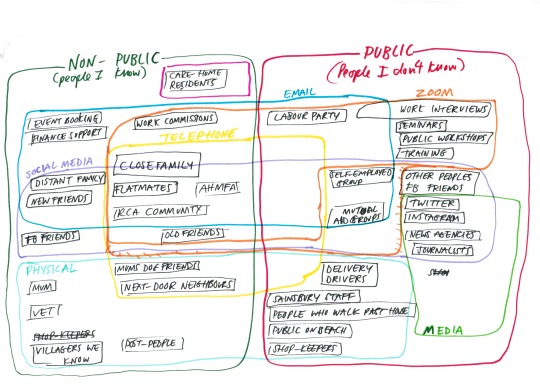
‘Here is my lockdown publics diagram developed for a workshop session, which I led with a group of students for the RCA Social Practice Group. I led a session on this again afterwards with a group of art educators and artists for a practice sharing group. Called ‘Writing the Rules for Zoom’ started by Alex Parry it was kick started by Alex’s development of ideas around this topic for a session for the social practice group in May 2020.
The diagram asks questions about different networks, communities and publics that we are communicating with and are in connection with (in the context of the first 3 months of lockdown). I developed mine through a process of creating a few drawings, into this kind of Venn diagram overlapped series of shapes. It was interesting to think about who is ‘the public’ to me, are these people I just don’t know, the ‘unknown’? Or people in various roles, networks or spaces? The process of doing it explored which groups of people I tended to identify as being ‘the public’ or which different publics and communities I was aware of being in contact with, both virtually and physically, at this time.
Putting people into ‘categories’ can of course be problematic, so it was definitely a process of thinking through this. Do publics get reduced or expanded at this time? As the people we are in touch regularly has physically changed a lot, depending where you happen to ‘lockdown’ or which networks or communities you are part of, I wondered how we can analyse and unpick possible and potential new ‘publics’ or communities to interact with, to play with as an audience or to set artwork within, or to communicate with. The delivery drivers, the supermarket workers, the people who walk past your house, these are all potential collaborators, viewers or audiences. Memorable moments in the workshops were: people identifying making regular connections with dogs (not their owners) on the beach, wondering who the people are behind newsletters in email inboxes, having the unnerving ability to ‘select’ online communities and students commenting on the ‘outsourcing’ of care and being able to be in a position of selecting which people or networks they wanted to hear from, speak to, listen to at this time.
It was a process of conceptualising the connections and groups as new communities, to seeing potential works coming out of unexpected daily relationships created by the change in social networks due to the pandemic. To see who or how we communicate in terms of varying distances. One artist commented that it made her think about the varying distances of intimacy that she has now with different people, a shorter distance with a partner, then family members, growing to huge distances, from 1 metre to 2 metre’s, to online distances that stretch across the world.’
More about the session below:
Social Practice Group Session 6, Tuesday 16th June 2020
Notes written: 22/06/2020 by Sadie Edginton
We wanted the last social practice session to be different. After experiencing other practitioners work over the weeks, we wanted the emphasis to be turned onto the students, to create some have room for them to try out their own ideas and to experiment with the format. The group had grown to become a space which felt comfortable, some recognisable faces every week, although there was always a few new people which worked well. Everyone could potentially test out ideas within the safety of the online zoom session format. It seemed to have become important that the group had evolved into a sense of familiarity whilst maintaining the possibility for unexpected things occurring. One student said, that was what she like about this group, that it was one place she could go knowing something surprising might happen. With some students returning often and creating a general sense of being relaxed, the group had created a comfortable sharing space, where people could voice their ideas, share thoughts about where they were, and most seemed open to trying new things out.
We had been playing with this space for the last few months since the beginning of lockdown. This was the sixth session and last (official) session of the school year. We'd had sessions by Louise Shelley, a curator; about group listening and reading processes, Alex Parry led us through a playful workshop stretching the rules for zoom, and Tim tried out his laptop-synthesiser experiment creating collective sounds out of objects in our homes with students now based across the globe overlapping their object orchestras into a magical din.
I had missed a session two weeks before where the group had had an informal conversation about what they'd like to try out. We'd had some interesting feedback too where students had said they felt like this space for sharing and practicing was needed, and it seemed to open-up space for vulnerability (through sharing) and support.
I had planned a vague structure for the last session, I would introduce, do a check-in so that everyone had a chance to speak and do a half hour workshop about mapping the publics and communities we were connecting with now (and how this has changed during lockdown).
There was then time for three students slots; Sally's workshop on confronting the awkwardnesses of online communication, followed by a 5 minute break, then Kats workshop about the taste and other sense. Everything went over time-wise so there was only 10 minutes left for Yuka to play us her experiments with the spatiality of sound.
We started by going around the group using these two questions for a check-in.
'What does 'the public' look like, from where you are now?'
'How are you connecting to a community?'
These questions were borrowed from a recording of a discussion here: http://www.nowandthere.org/blog/2020/4/7/nt-asks-what-does-public-mean-right-now
It was interesting to hear about where the students were based, most in the UK, then China, Japan and Paris. We had seven students and Hannah and I, so altogether it worked well for creating a grid of nine on the gallery view on zoom. As we went around the group I was struck how each student shared with us a detailed picture of how they were in unexpected circumstances and feeling isolated. Some had just travelled to another place, and were stuck living mostly inside and with family, they were not sure about what a local community might look like. One had discovered new communities through volunteering for local mutual aid groups, Hannah mentioned working with existing connections to create networks of in different ways, new connections with animals and birds seeming to be important. Some international students admitted they didn't feel like they had a community, whether they were in London, or back home. One said she felt like there were layers of community, from those close by who were a local support system, then the online groups she was part of, and then her family members who were contactable by phone. Another student said that communities felt ‘chosen’ at the moment; that you could select who you wanted to be in touch with, and it was almost a way of ‘outsourcing care’. Another mentioned that new rituals had emerged in her local village neighbourhood, kicked off by the Thursday clap for carers, leading to local people creating other ways to come together in the street, such as VE day where they set-up tables outside. Another student said it was so long since he had been in Beijing, now that he was back there again, he had to try to find people again who he had known a long time ago.
Next we created 'What do our publics look like now?' diagrams. Attempting to get away from a formal 'pdf' presentation, I sketched out the questions and stages of the diagram drawing onto paper beforehand, and held them up to the screen. I asked everyone to draw a square or circle and inside it to list groups of people, categories of people that they were seeing in real life, in 'physical space'.

I was interested in what different or new groups of people were identified, in the lock-down. For instance I was not staying where I usually live and discovered that I was coming into contact with; next-door neighbours, people who walk past the house, the vet, the nurse at the GP, dog walker friends and dogs who were our dogs friends, delivery drivers, shop-keepers and the public we see on walks. This changed again when I went back to London.
We drew overlapping bubbles and listed those we connected with through 'virtual' connections, then 'phone calls', emails, social media, and letters.
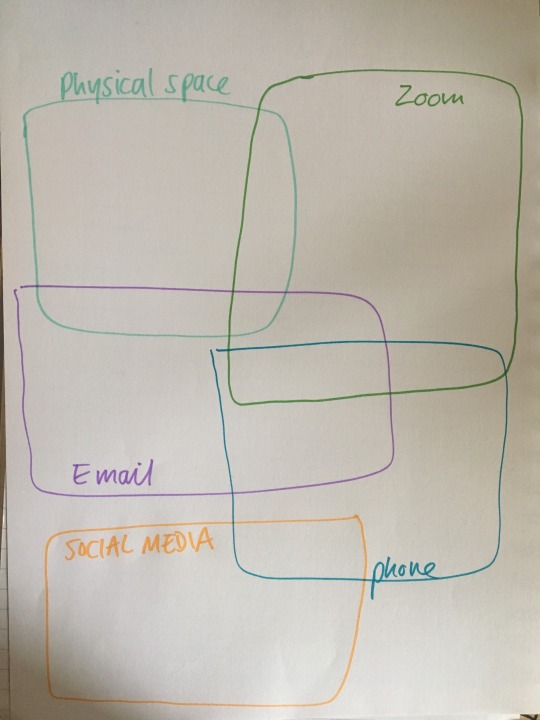
The idea was to then circle in a different colour, those categories of people who you didn't know. Or who you saw as 'the public'. I was intrigued as to if it could be used to locate a new audience/ public for an artwork, project or workshop.
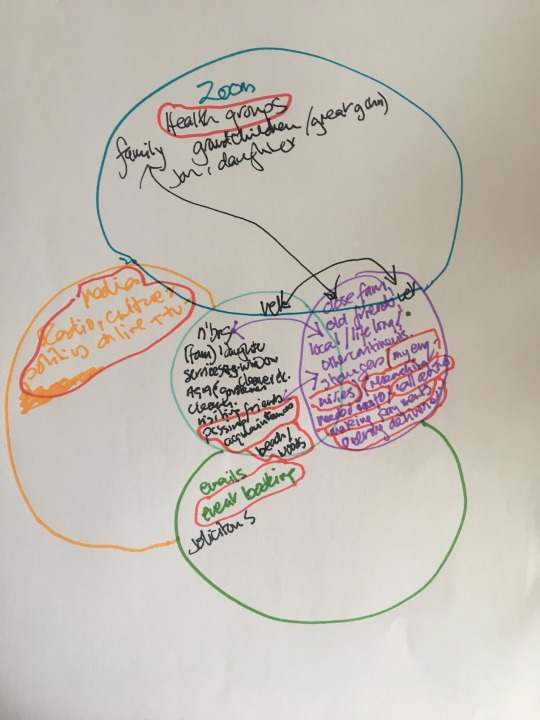
Practice diagram by my mum, Sue Edginton

Holding up my publics diagram to the screen
Reflection: We did the activity a bit too quickly, as it turned out it takes a long time to think through all of this, and I did not have time to get proper feedback afterwards. I showed a few slides about this idea of the physical public becoming much closer, smaller and local, and then the opposite happening with the virtual public where it really expands to include an international community. The publics or groups I was working working with or had contact with still, had really changed too. From working in schools and care homes with lots of people and children face-to-face, this has changed. Now I was just in touch with people via zoom calls or colleagues via the phone, and all the work with children and elders had been put on hold for now. Where were all the people and how were they right now, what were they doing? A lot of people I talked to who work in the community found themselves asking similar questions.
Museum of the Street by Louise Ashcroft and her local neighbourhood, Walthamstow, London, May 2020
1 note
·
View note