#medical diagnostic software
Text
Advancements in Diagnostic Software: A New Era for Healthcare
The advent of sophisticated diagnostic software is transforming the healthcare industry by enhancing the precision and efficiency of medical evaluations. Leveraging advanced technologies such as artificial intelligence and machine learning, these systems are capable of analyzing complex medical data with high accuracy. This technological leap reduces diagnostic errors and improves the reliability of medical assessments.
A notable feature of modern diagnosis software is its ability to integrate seamlessly with existing healthcare systems. This integration facilitates efficient data exchange and streamlines administrative processes, allowing healthcare professionals to focus more on patient care rather than on managing information.
Additionally, the software supports personalized medicine by processing vast amounts of patient data to create tailored treatment plans. This approach not only improves treatment outcomes but also optimizes resource utilization within healthcare facilities.
Despite its many benefits, the implementation of diagnostic software does come with challenges, such as ensuring compatibility with legacy systems and maintaining robust data security. However, ongoing advancements in technology continue to address these issues, enhancing both the functionality and safety of these systems.
In summary, modern medical diagnostics software is a critical advancement in healthcare, driving improvements in diagnostic accuracy, operational efficiency, and patient care.
#medical diagnosis software solutions#medical diagnostic software#medical diagnostic#diagnosis software#medical diagnostic apps#MEDICAL DIAGNOSTIC SOFTWARE DEVELOPMENT SERVICES#medical diagnostic solutions
0 notes
Text
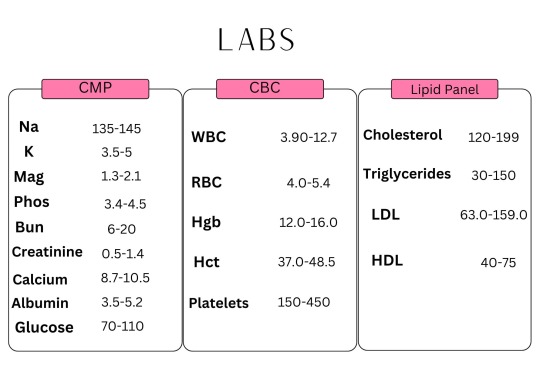
#icunurse#nursing school#nursing#etsy#icucare#hospital#icu#health and wellness#healthcare#diagnosis#diagnostic management software#medblr#patientcare#patientsafety#medical care#bloodwork#labs#note cards#reference#nursing studyblr#nursing student
5 notes
·
View notes
Text
QMS & Risk Management for IVD Manufacturers
IVD manufacturers must comply with strict regulations to ensure product safety and quality. A well-implemented Quality Management System (QMS) and risk management strategy help manufacturers meet regulatory standards, minimize risks, and improve overall product reliability. This content offers insights on regulatory frameworks like ISO 13485 and FDA 21 CFR Part 820, designed to support manufacturers in the medical diagnostics industry.
For more info: https://www.makrocare.com/blog/developing-and-maintaining-a-qms-for-ivds/
0 notes
Text

Surgical Innovation & Medical Device Diagnostic Applications
We’ve engaged in device firmware, EMR/EHR integration, digitized & automated operation room workflow, ensuring data security with HIPAA & FDA compliances.
More - https://dashtechinc.com/blog/transformative-technologies-advancing-patient-care-through-next-gen-embedded-medical-device-software-development/
#medical device software#“medical & healthcare”#“Surgical Innovation”#“ Medical Device Diagnostic Applications”
0 notes
Text
#Ayurveda diagnostic software#ayurveda EHR#Ayurveda management software#Ayurveda patient management software#Ayurvedic assessment form USA#Ayurvedic clinic software#Ayurvedic clinics India#Ayurvedic clinics UK#ayurvedic diagnostic software#Ayurvedic health assessment India#Ayurvedic health questionnaire United States#Ayurvedic medicine software#Ayurvedic pharmacy software#Ayurvedic practice management software#Ayurvedic practitioners USA#ayurvedic software#Ayurvedic therapies in Sri Lanka#Ayurvedic wellness centers Nepal#Ayurvedic wellness centers Sri Lanka#Ayurvedic wellness software#Electronic health records (EHR) for Ayurveda#Electronic Medical Records Software#emr software#Healthcare management system#Panchakarma treatment software#WhatsApp appointment booking system#WhatsApp online appointment booking
0 notes
Text
Embark on a Whimsical Word Adventure with EtherQuipsQuest – The Mad Libs Game That Turns Your Day into a Laugh Riot
Something Good Came Out Of COVID
I absolutely loved playing the game Mad Libs from the first time someone in my class a recess in the field played a game with me, I was hooked. It’s such a great icebreaker, and for an awkward kid who just moved to NorthEast from Houston, Texas there was nothing better that to share a carefree and hilarious moment with a game or two at recess.
I aimed to craft a…
View On WordPress
#Awkward Moments#Bus Wait#Casual Hangout#Childhood Memories#City College of San Francisco#Conversation Starter#COVID Lockdown#Diagnostic Medical Imaging Program#EtherQuipsQuest#Feature Enhancements#Free Game#Fun Moments#Game Development#Ice Breaker#Icebreaker#JotForm Software#Mad Libs#Moving#New Friends#Online Application#Party Game#Pocket-Sized Game#Prototype Stage#Pub Game#Recess#Work Break
0 notes
Text
Great Big Good Omens Graphic Novel Update
AKA A Visit From Bildad the Shuhite.
The past year or so has been one long visit from this guy, whereupon he smiteth my goats and burneth my crops, woe unto the woeful cartoonist.
Gaze upon the horror of Bildad the Shuhite.

You kind of have to be a Good Omens fan to get this joke, but trust me, it's hilarious.
Anyway, as a long time Good Omens novel fan, you may imagine how thrilled I was to get picked to adapt the graphic novel.
Go me!

This is quite a task, I have to say, especially since I was originally going to just draw (and color) it, but I ended up writing the adaptation as well. Tricky to fit a 400 page novel into a 160-ish page graphic novel, especially when so much of the humor is dependent on the language, and not necessarily on the visuals.
Not complainin', just sayin'.
Anyway, I started out the gate like a herd of turtles, because right away I got COVID which knocked me on my butt.
And COVID brain fog? That's a thing. I already struggle with brain fog due to autoimmune disease, and COVID made it worse.
Not complainin' just sayin'.
This set a few of the assignments on my plate back, which pushed starting Good Omens back.
But hey, big fat lead time! No worries!
Then my computer crawled toward the grave.
My trusty MAC Pro Tower was nearly 15 years old when its sturdy heart ground to a near-halt with daily crashes. I finally got around to doing some diagnostics; some of its little brain actions were at 5% functionality. I had no reliable backups.
There are so many issues with getting a new computer when you haven't had a new computer or peripherals in nearly fifteen years and all of your software, including your Photoshop program is fifteen years old.
At the time, I was still on rural internet...which means dial-up speed.

Whatever you have for internet in the city, roll that clock back to about 2001.
That's what I had. I not only had to replace almost all of my hardware but I had to load and update all programs at dial-up speed.
Welcome to my gigabyte hell.
The entire process of replacing the equipment and programs took weeks and then I had to relearn all the software.
All of this was super expensive in terms of money and time cost.
But I was not daunted! Nosirree!
I still had a huge lead time! I can do anything! I have an iron will!
And boy, howdy, I was going to need it.
At about the same time, a big fatcat quadrillionaire client who had hired me years ago to develop a big, major transmedia project for which I was paid almost entirely in stock, went bankrupt leaving everyone holding the bag, and taking a huge chunk of my future retirement fund with it.
I wrote a very snarky almost hilarious Patreon post about it, but am not entirely in a position to speak freely because I don't want to get sued. Even though I had to go to court over it, (and I had to do that over Zoom at dial-up speed,) I'm pretty sure I'll never get anything out of this drama, and neither will anyone else involved, except millionaire dude and his buddies who all walked away with huge multi-million dollar bonuses weeks before they declared bankruptcy, all the while claiming they would not declare bankruptcy.
Even the accountant got $250,000 a month to shut down the business, while creators got nothing.
That in itself was enough drama for the year, but we were only at February by that point, and with all those months left, 2023 had a lot more to throw at me.
Fresh from my return from my Society of Illustrators show, and a lovely time at MOCCA, it was time to face practical medical issues, health updates, screening, and the like. I did my adult duty and then went back to work hoping for no news, but still had a weird feeling there would be news.

I know everyone says that, but I mean it. I had a bad feeling.
Then there was news.
I was called back for tests and more tests. This took weeks. The ubiquitous biopsy looked, even to me staring at the screen in real time, like bad news.
It also hurt like a mofo after the anesthesia wore off. I wasn't expecting that.
Then I got the official bad news.
Cancer which runs in my family finally got me. Frankly, I was surprised I didn't get it sooner.
Stage 0, and treatment would likely be fast and complication-free. Face the peril, get it over with, and get back to work.
I requested surgery months in the future so I could finish Good Omens first, but my doc convinced me the risk of waiting was too great. Get it done now.
"You're really healthy," my doc said. Despite an auto-immune issue which plagues me, I am way healthier than the average schmoe of late middle age. She informed me I would not even need any chemo or radiation if I took care of this now.

So I canceled my appearance at San Diego Comic Con. I did not inform the Good Omens team of my issues right away, thinking this would not interfere with my work schedule, but I did contact my agent to inform her of the issue. I also contacted a lawyer to rewrite my will and make sure the team had access to my digital files in case there were complications.
Then I got back to work, and hoped for the best.
Eff this guy.
Before I could even plant my carcass on the surgery table, I got a massive case of ocular shingles.
I didn't even know there was such a thing.
There I was, minding my own business. I go to bed one night with a scratchy eye, and by 4 PM the next day, I was in the emergency room being told if I didn't get immediate specialist treatment, I was in big trouble.
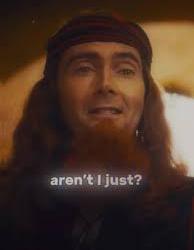
I got transferred to another hospital and got all the scary details, with the extra horrid news that I could not possibly have cancer surgery until I was free of shingles, and if I did not follow a rather brutal treatment procedure - which meant super-painful eye drops every half hour, twenty-four hours a day and daily hospital treatment - I could lose the eye entirely, or be blinded, or best case scenario, get permanent eye damage.
What was even funnier (yeah, hilarity) is the drops are so toxic if you don't use the medication just right, you can go blind anyway.
Hi Ho.
Ulcer is on the right. That big green blob.
I had just finished telling my cancer surgeon I did not even really care about getting cancer, was happy it was just stage zero, had no issues with scarring, wanted no reconstruction, all I cared about was my work.
Just cut it out and get me back to work.
And now I wondered if I was going to lose my ability to work anyway.
Shingles often accompanies cancer because of the stress on the immune system, and yeah, it's not pretty. This is me looking like all heck after I started to get better.

The first couple of weeks were pretty demoralizing as I expected a straight trajectory to wellness. But it was up and down all the way.
Some days I could not see out of either eye at all. The swelling was so bad that I had to reach around to my good eye to prop the lid open. Light sensitivity made seeing out of either eye almost impossible. Outdoors, even with sunglasses, I had to be led around by the hand.
I had an amazing doctor. I meticulously followed his instructions, and I think he was surprised I did. The treatment is really difficult, and if you don't do it just right no matter how painful it gets, you will be sorry.
To my amazement, after about a month, my doctor informed me I had no vision loss in the eye at all. "This never happens," he said.
I'd spent a couple of weeks there trying to learn to draw in the near-dark with one eye, and in the end, I got all my sight back.
I could no longer wear contact lenses (I don't really wear them anyway, unless I'm going to the movies,) would need hard core sun protection for awhile, and the neuralgia and sun sensitivity were likely to linger. But I could get back to work.
I have never been more grateful in my life.
Neuralgia sucks, by the way, I'm still dealing with it months later.
Anyway, I decided to finally go ahead and tell the Good Omens team what was going on, especially since this was all happening around the time the Kickstarter was gearing up.
Now that I was sure I'd passed the eye peril, and my surgery for Stage 0 was going to be no big deal, I figured all was a go. I was still pretty uncomfortable and weak, and my ideal deadline was blown, but with the book not coming out for more than a year, all would be OK. I quit a bunch of jobs I had lined up to start after Good Omens, since the project was going to run far longer than I'd planned.
Everybody on the team was super-nice, and I was pretty optimistic at this time. But work was going pretty slow during, as you may imagine.
But again...lots of lead time still left, go me.
Then I finally got my surgery.
Which was not as happy an experience as I had been hoping for.
My family said the doc came out of the operating room looking like she'd been pulled backwards through a pipe, She informed them the tumor which looked tiny on the scan was "...huge and her insides are a mess."
Which was super not fun news.
Eff this guy.

The tumor was hiding behind some dense tissue and cysts. After more tests, it was determined I'd need another surgery and was going to have to get further treatments after all.
The biopsy had been really painful, but the discomfort was gone after about a week, so no biggee. The second surgery was, weirdly, not as painful as the biopsy, but the fatigue was big time.
By then, the Good Omens Kickstarter had about run its course, and the record-breaker was both gratifying and a source of immense social pressure.
I'd already turned most of my social media over to an assistant, and I'm glad I did.
But the next surgery was what really kicked me on my keister.

All in all, they took out an area the size of a baseball. It was hard to move and wiped me out for weeks and weeks. I could not take care of myself. I'd begun losing hair by this time anyway, and finally just lopped it off since it was too heavy for me to care for myself. The cut hides the bald spots pretty well.
After about a month, I got the go-ahead to travel to my show at the San Diego Comic Con Museum (which is running until the first week of April, BTW). I was very happy I had enough energy to do it. But as soon as I got back, I had to return to treatment.
Since I live way out in the country, going into the city to various hospitals and pharmacies was a real challenge. I made more than 100 trips last year, and a drive to the compounding pharmacy which produced the specialist eye medicine I could not get anywhere else was six hours alone.
Naturally, I wasn't getting anything done during this time.
But at least my main hospital is super swank.


The oncology treatment went smoothly, until it didn't. The feels don't hit you until the end. By then I was flattened.
So flattened that I was too weak to control myself, fell over, and smashed my face into some equipment.

Nearly tore off my damn nostril.
Eff this guy.

Anyway, it was a bad year.
Here's what went right.
I have a good health insurance policy. The final tally on my health care costs ended up being about $150,000. I paid about 18% of that, including insurance. I had a high deductible and some experimental medicine insurance didn't cover. I had savings, enough to cover the months I wasn't working, and my Patreon is also very supportive. So you didn't see me running a Gofundme or anything.
Thanks to everyone who ever bought one of my books.
No, none of that money was Good Omens Kickstarter money. I won't get most of my pay on that for months, which is just as well because it kept my taxes lower last year when I needed a break.
So, yay.
My nose is nearly healed. I opted out of plastic surgery, and it just sealed up by itself. I'll never be ready for my closeup, but who the hell cares.
I got to ring the bell.

I had a very, VERY hard time getting back to work, especially with regard to focus and concentration. My work hours dropped by over 2/3. I was so fractured and weak, time kept slipping away while I sat in the studio like a zombie. Most of the last six months were a wash.
I assumed focus issues were due (in part) to stress, so sought counseling. This seemed like a good idea at first, but when the counselor asked me to detail my issues with anxiety, I spent two weeks doing just that and getting way more anxious, which was not helpful.
After that I went EFF THIS NOISE, I want practical tools, not touchy feelies (no judgment on people who need touchy-feelies, I need a pragmatic solution and I need it now,) so tried using the body doubling focus group technique for concentration and deep work.
Within two weeks, I returned to normal work hours.
I got rural broadband, jumping me from dial up speed to 1 GB per second.
It's a miracle.

Massive doses of Vitamin D3 and K2. Yay.
The new computer works great.
The Kickstarter did so well, we got to expand the graphic novel to 200 pages. Double yay.
I'm running late, but everyone on the Good Omens team is super supportive. I don't know if I am going to make the book late or not, but if I do, well, it surely wasn't on purpose, and it won't be super late anyway. I still have months of lead time left.
I used to be something of a social media addict, but now I hardly ever even look at it, haven't been directly on some sites in over a year, and no longer miss it. It used to seem important and now doesn't.
More time for real life.
While I think the last year aged me about twenty years, I actually like me better with short hair. I'm keeping it.

OK. Rough year.
Not complainin', just sayin'.
Back to work on The Book.
And only a day left to vote for Good Omens, Neil Gaiman, and Sandman in the Comicscene Awards. Thanks.
2K notes
·
View notes
Text
Maybe it isn't that I actually hate medical professionals? They just suck and are weird sometimes, and a lot of them shouldn't be practicing, but I don't hate them as a group, like, personally.
What I hate is their ability to make my life harder in ways that are often completely opaque to me, and a lot of the crap things they do are not really possible to challenge. And I hate the fact that holding them responsible fort dogshit behavior in any way that will actually benefit me is almost always impossible.
And I also hate the fact that they have to do stupid things sometimes because that's how the system is set up, and those things sometimes mean patients actually get harmed. They aren't fond of that part either! They don't want the system to be the way it is! But they don't have a choice, so sometimes people like me get forced by bureaucracy into doing things that are re-traumatizing. And I can't imagine that feels good for them at all, knowing that their patients are sometimes only "consenting" because that bureaucracy will not let them be helped in any other way. Which isn't consent at all. I imagine that must be pretty traumatizing for them, too, sometimes.
If it were easier to actually access medical care without tremendous delays in this country right now I would have much less trouble finding providers who are good at what they do and are not horrible people, and who have clinic staff who can do their fucking job.
Oh and I also don't appreciate how evasive and unwilling to commit they are out of fear of being held to an answer that turns out to be inaccurate, but I can't make an informed decision about my own care unless they give me at least some information about probabilities and trajectories and typicalities. Genuinely, how the fuck am I supposed to navigate that shit. I get that some patients are really fucking difficult, but I should be able to get a special stamp on my file or something that says I understand that sometimes medicine isn't an exact science and the best answers that my doctors can give may not always prove to be accurate in the long term. I know they don't like being in that situation either.
A lot of medical professionals are fucking assholes, and unfortunately the ones who are not are still hamstrung by a system set up to actively prevent people from getting care.
I miss my old doctor. He gave no shits about anything that wasn't the patient. He prescribed scheduled meds based on what the patient needed and not based on fear of consequences potentially being imposed on him by the punitive patient-hostile drugs-are-bad moral panic machine developed to force suffering people into buying more dangerous drugs off the street in order to prevent far fewer people from maybe getting high off of drugs that at least weren't laced with lethal substances. (The purpose of a system is what it does.) Did he get sanctioned and become locally unhireable? Unfortunately yes he did. Does he now provide concierge care to rich people? Yes he does. He found a way to make it work, God bless him.
Everything about the medical system in this country is fucked. Hospitals, doctors, nurses, pharmacies, pharmacists, pharmacy techs, phlebotomists, clinic administrative staff, insurance companies, medical schools and schooling, licensing boards, drug advertising to both providers and patients, pharmaceutical reps, researchers, research, publishing, medical trials, pharmaceutical companies, manufacturers and distributors, medical equipment, charting software, billing and billing codes, diagnostic criteria, charity and low income services, accessible transportation, home care, the lack of independent individual patient advocates, dietitians and nutritionists, access to physical and occupational therapy and physical and occupational therapists, the massive bigotry of every kind rampant in every corner of the medical field, social work, senior care and assisted living, deprioritization of informed consent and harm reduction, disability applications, inaccessibility of medical records, especially psychiatric notes which are specifically allowed to be withheld from patients, lack of continuity of care for disadvantaged people, care that is equitably accessible to disabled people, telemedicine, patient portals, phone systems, clinic hours, every single aspect of inpatient and outpatient psychiatry, facility security, all sorts of things going on with therapists who are nevertheless probably the least malicious group of people in this entire charade, aaaaaand patients themselves.
Also hospital toilets that are too tall and make it literally physically impossible for me to poop while I'm there waiting for somebody to come out of surgery. I just needed to take a crap, guys. You didn't need to make the toilets so tall that my feet didn't even touch the floor. It is very clean but there is no shitting for short people at St Francis.
348 notes
·
View notes
Text
50 ONE LEVEL CAREERS: Storytelling careers megapack by isy's the snake

Here is yet another career mod pack, but this one has no promotions, you just work and your job level stays at 1. As the title say this mod is best for story telling!
creator's notes-
This mod requires XML Injector by Scumbumbo. You can find it here.
Pay attention if you don't already have it for another mod! In that case, you do not need to re-install it. Be sure it is updated for the last patch.
XML Injector is a mod required for some mods to work. So, you install it as any other mod in your Mods folder, no more than one subfolder deep.
This mod has been updated for the version 1.99.305 of the game (second update after Horse Ranch).
It doesn't required any DLC to work. Base game compatible
I've adopted this mod from the amazing ItsKatato who, due to her hiring at EA, couldn't continue to mod. I have made some changes:
• I have changes all the pics of the careers — now they all show Sims (please check the credits paragraph at the end to see who was the amazing raccoon who helped me);
• I have updated the mod for the Horse Ranch patch;
• I have cleared ALL the tuning errors;
• Fixed the description of some careers who appeared to be missing.
Now, here we go with the explanation of the mod (originally written by ItsKatato, edited by me):
Katato said: "Have you ever had a story planned out for your sims but you can't find the perfect career for them? Most of the time when I find the career it ends up being a complicated career with a bunch of promotion tasks and extra stuff. Well, I've made a pack of a bunch of single-level careers. All your sim has to do is go to work, that's it. This is perfect for the non-important sims in your life, like the forgotten children of your legacy challenge."
In short: those are 50 careers you can use for NPCs Sims or random Sims you do not want to care about. As Amethyst said: "Go to work, make money, leave me alone". Your Sims won't need any task to perform to upgrade and get a promotion, as well as they do not really need an ideal mood to go to work since it won't change their performance. They just go and do their job.
And now the list of all careers:
1. Anesthetiologist
2. Cartographer
3. Chiropractor
4. Compliance Officer
5. Data Scientist
6. Dental Hygienist
7. Dentist
8. Diagnostic Medical Sonographer
9. Financial Advisor
10. Financial Manager
11. Genereal Surgeon
12. Genetic Counselor
13. Home Health Aide
14. Information Security Analyst
15. IT Manager
16. Interpreter And Translator
17. Lawyer
18. Marriage And Family Therapist
19. Massage Therapist
20. Mathematician
21. Mechanical Engineer
22. Medical And Health Services Manager
23. Nurse Anesthetist
24. Nurse Practitioner
25. Obstetrician And Gynecologist
26. Occupational Therapist
27. Operations Reasearch Analyst
28. Optometrist
29. Oral And Maxillofacial Surgeon
30. Orthodontist
31. Orthotist And Prosthetist
32. Paralegal
33. Pediatrician
34. Personal Care Aide
35. Phlebotomist
36. Physical Therapist
37. Physical Therapist Assistant
38. Physician
39. Physician Assistant
40. Pilot
41. Podiatrist
42. Prosthodontist
43. Psychiatrist
44. Registered Nurse
45. Respiratory Therapist
46. Software Developer
47. Speech-Language Pathologist
48. Statician
49. Substance Abuse And Behavioral Disorder Counselor
50. Veterinarian
51. Web Developer
52. Wind Turbine Technician
lets give some of our love and support to isy!
download
#sims 4 cc#sims 4 download#sims 4#sims 4 gameplay#the sims 4#sims 4 custom content#sims 4 mods#the sims 4 mods#the sims 4 custom content#ts4#sims 4 careers#sims 4 career#ts4 careers#ts4 career#s4 career#s4 cc#s4 download#s4cc#s4ccfinds#s4 custom content#sims 4 storytelling#sims 4 story#the sims 4 download#ts4 mods#the sims 4 cc#ts4 custom content#thesims4#sims4
236 notes
·
View notes
Text
Determined to use her skills to fight inequality, South African computer scientist Raesetje Sefala set to work to build algorithms flagging poverty hotspots - developing datasets she hopes will help target aid, new housing, or clinics.
From crop analysis to medical diagnostics, artificial intelligence (AI) is already used in essential tasks worldwide, but Sefala and a growing number of fellow African developers are pioneering it to tackle their continent's particular challenges.
Local knowledge is vital for designing AI-driven solutions that work, Sefala said.
"If you don't have people with diverse experiences doing the research, it's easy to interpret the data in ways that will marginalise others," the 26-year old said from her home in Johannesburg.
Africa is the world's youngest and fastest-growing continent, and tech experts say young, home-grown AI developers have a vital role to play in designing applications to address local problems.
"For Africa to get out of poverty, it will take innovation and this can be revolutionary, because it's Africans doing things for Africa on their own," said Cina Lawson, Togo's minister of digital economy and transformation.
"We need to use cutting-edge solutions to our problems, because you don't solve problems in 2022 using methods of 20 years ago," Lawson told the Thomson Reuters Foundation in a video interview from the West African country.
Digital rights groups warn about AI's use in surveillance and the risk of discrimination, but Sefala said it can also be used to "serve the people behind the data points". ...
'Delivering Health'
As COVID-19 spread around the world in early 2020, government officials in Togo realized urgent action was needed to support informal workers who account for about 80% of the country's workforce, Lawson said.
"If you decide that everybody stays home, it means that this particular person isn't going to eat that day, it's as simple as that," she said.
In 10 days, the government built a mobile payment platform - called Novissi - to distribute cash to the vulnerable.
The government paired up with Innovations for Poverty Action (IPA) think tank and the University of California, Berkeley, to build a poverty map of Togo using satellite imagery.
Using algorithms with the support of GiveDirectly, a nonprofit that uses AI to distribute cash transfers, the recipients earning less than $1.25 per day and living in the poorest districts were identified for a direct cash transfer.
"We texted them saying if you need financial help, please register," Lawson said, adding that beneficiaries' consent and data privacy had been prioritized.
The entire program reached 920,000 beneficiaries in need.
"Machine learning has the advantage of reaching so many people in a very short time and delivering help when people need it most," said Caroline Teti, a Kenya-based GiveDirectly director.
'Zero Representation'
Aiming to boost discussion about AI in Africa, computer scientists Benjamin Rosman and Ulrich Paquet co-founded the Deep Learning Indaba - a week-long gathering that started in South Africa - together with other colleagues in 2017.
"You used to get to the top AI conferences and there was zero representation from Africa, both in terms of papers and people, so we're all about finding cost effective ways to build a community," Paquet said in a video call.
In 2019, 27 smaller Indabas - called IndabaX - were rolled out across the continent, with some events hosting as many as 300 participants.
One of these offshoots was IndabaX Uganda, where founder Bruno Ssekiwere said participants shared information on using AI for social issues such as improving agriculture and treating malaria.
Another outcome from the South African Indaba was Masakhane - an organization that uses open-source, machine learning to translate African languages not typically found in online programs such as Google Translate.
On their site, the founders speak about the South African philosophy of "Ubuntu" - a term generally meaning "humanity" - as part of their organization's values.
"This philosophy calls for collaboration and participation and community," reads their site, a philosophy that Ssekiwere, Paquet, and Rosman said has now become the driving value for AI research in Africa.
Inclusion
Now that Sefala has built a dataset of South Africa's suburbs and townships, she plans to collaborate with domain experts and communities to refine it, deepen inequality research and improve the algorithms.
"Making datasets easily available opens the door for new mechanisms and techniques for policy-making around desegregation, housing, and access to economic opportunity," she said.
African AI leaders say building more complete datasets will also help tackle biases baked into algorithms.
"Imagine rolling out Novissi in Benin, Burkina Faso, Ghana, Ivory Coast ... then the algorithm will be trained with understanding poverty in West Africa," Lawson said.
"If there are ever ways to fight bias in tech, it's by increasing diverse datasets ... we need to contribute more," she said.
But contributing more will require increased funding for African projects and wider access to computer science education and technology in general, Sefala said.
Despite such obstacles, Lawson said "technology will be Africa's savior".
"Let's use what is cutting edge and apply it straight away or as a continent we will never get out of poverty," she said. "It's really as simple as that."
-via Good Good Good, February 16, 2022
#older news but still relevant and ongoing#africa#south africa#togo#uganda#covid#ai#artificial intelligence#pro ai#at least in some specific cases lol#the thing is that AI has TREMENDOUS potential to help humanity#particularly in medical tech and climate modeling#which is already starting to be realized#but companies keep pouring a ton of time and money into stealing from artists and shit instead#inequality#technology#good news#hope
202 notes
·
View notes
Text
PPTH Staff Directory
Administration
Hen Nenaginad, Dr. Cuddy’s personal assistant (@toplessoncology), ask blog @ppthparttimer
Cardiology
Sydney Forrest, Head of Cardiology (@wilsons-three-legged-siamese), ask blog @ask-head-of-cardio
Custodial
Bruce N. Valentine (@ghostboyhood), ask blog @the-cleaning-guy
Diagnostics
Haven Ross House (@birdyboyfly), ask blog @ultimate-diagnostician-haven
Teagan Sinclair, Gynecologist (@robbinggoodfellows), ask blog @ask-teagan-sinclair
Cosmo Anderson, House's personal assistant (@cupofmints), ask blog @underpaid-assistant
Emergency Medical Services
Dr. Kadee Montgomery, Head of Emergency Medical Services and Infectious Disease Specialist (@privatehousesanatomy), ask blog @kadeejeanmontgomery
Anji Foxx-Knight, Ambulance Operator and Automotive Technician (@rainismdata), ask blog @technician-para-driver
Fritz Litte, ER Doctor, ask blog @erdocfritz
Dr. Rylan Hopps, ER Physician (@dndadsbara), ask blog @nervous-physician
Endocrinology
Ev Price, Head of Endocrinology (@sillyhyperfixator), ask blog @ppth-endocrinology-head
Dr. Katherine “Kate” Rooke, Endocrinologist (@katttkhaos), ask blog @drkrooke
Epidemiology
Dr. Arwen Callejas, Head of Epidemiology (@addicbookedout)
Emilie Martin, Epidemiologist (@picking-dandelions-and-tunes)
Forensics
Stevie “Bird” Corcoran, Forensic Scientist and Teacher (@1mlostnow), ask blog @head-of-forensics
Melvin Rideau, Forensic Technician (@datas-boobs), ask blog @ppth-forensic-technician
Hematology
Ivan Andrews, Hematologist (@kleinekorpus)
IT
Andrew Hayes, Software Engineer (@tired-and-bored-nerd), ask blog @ask-ppths-it-guy
Lab
Anatol Dybowski, Head Lab Scientist (@tino-i-guess), ask blog @ppth-lab-head
Legal
Valerie Carr, Legal Consultant (@writing-and-sillies), ask blog @ask-ppth-legal
OB-GYN
Dr. Fluoxetine Pearl, Head of OB-GYN (@asclexe), ask blog @ppth-obgyn-dept-head-real
Dr. Katherine Rhodes, Head of NICU and ICU (@privatehousesanatomy), ask blog @katherineelainerhodes)
Danny Begay, Gynecologist (@hemlocksloadofbull), ask blog @ask-danny-in-gynecology
Oncology
Dr. Francesca Scott, Head of Oncology (@birdyboyfly), ask blog @ask-head-of-oncology
Leo Fitsher, Nurse (@asclexe)
Ophthalmology
Maddox “Maddie” N. Jagajiva, Ophthalmologist (@rainismdata), ask blog @dr-visionary-counselor
Pediatrics
Dr. Nanette “Ninny” Amesbury, Head of Pediatrics (@desire-mona)
Eddie Sting, Head of Pediatrics (@cherrishnoodles), ask blog @ask-head-of-pediatrics
Romeo "Vinny" Vincent, ENT nurse (@wilsons-three-legged-siamese), ask blog @earsandthroatnursey
Melanie Byrd, Pediatric Orthopedist (@tired-and-bored-nerd), ask blog @ppth-baby-bone-doc
Marie, Pediatrician (@marieinpediatrics-stuff)
Dr. Sophie Baker, Pediatric Neurosurgeon (@privatehousesanatomy), ask blog @sophieeloisebaker
Plastics
Gabriella “Gabi” Kramer, Plastic Surgeon (@1mlostnow), ask blog @plastic-surgeon-gabi
Psychiatry/Psychology
Lena Ehris, Head of Psychiatry (@jellifishiez), ask blog @head-of-psychiatry
Dr. Venus Watanabe, Head of Psychiatry (@chocovenuss)
Dr. Madlock, Head of Psychology (@sushivisa)
Domingo Estrada, Social Worker (@robertseanleonardthinker), ask blog @ppth-socialworker
Dr. Kieran F. Campbell, Psychiatrist and Geneticist (@kim-the-kryptid), ask blog @consult-the-geneticist
Pulmonology
Reina Linh Rivera, Head of Pulmonology (@prettypinkbubbless)
Dr. Milana Walker (@evilchildeyeeter), ask blog @dr-redbull-addict
Radiology
Dr. Eneko Ruiz-Arroyo, Head of Radiology (@katttkhaos), ask blog @headoradiology
Beth Klein, Radiology Tech (@emptylakes)
Steven Sandoval, Radiologist (@endofradio)
Patients
Ilja "Illusha" Vancura, Head Archivist at Rutgers Med (@scarriestmarlowe), blog @vancurarchivist
Francesco Cage, Best girldad patient (@dndadsbara), ask blog @francesco-cage
Joey Abrams, Forensics Student - kind of (@1mlostnow), ask blog @joey-is-fine
OOC: Hi, I'm Birdy, and I run this PPTH blog! I'm 19, agender, aroace, and use they/them pronouns.
If you have an OC or a post that you would like for me to add to the blog, please feel free to send me an ask/message! If I follow you back, it'll be at my main blog, @birdyboyfly.
56 notes
·
View notes
Text
Revolutionizing Healthcare: The Future of Medical Diagnostics Software
The landscape of healthcare is undergoing a profound transformation with the rise of advanced medical diagnostics software, which is setting new benchmarks for accuracy and efficiency in patient care. This state-of-the-art technology is redefining diagnostic processes, offering unprecedented precision and speed in identifying and managing medical conditions.
Modern diagnosis software harnesses the power of artificial intelligence (AI) and sophisticated algorithms to analyze extensive medical data. This includes integrating information from medical imaging, laboratory results, and electronic health records. By processing this data with remarkable speed, the software aids clinicians in making more accurate diagnoses. For example, AI algorithms can detect minute irregularities in imaging scans that might be missed by the human eye, leading to earlier and more reliable identification of diseases such as cancers and neurological disorders.
One of the key innovations in this field is the ability of diagnostics software to integrate data from various sources into a cohesive view of the patient’s health. This holistic approach ensures that all relevant information is considered, improving the accuracy of diagnoses and enabling tailored treatment plans that address individual patient needs.
Additionally, the real-time data analysis capabilities of these tools allow for continuous monitoring of patient health. This proactive approach helps in identifying potential issues before they develop into serious conditions, facilitating timely interventions and personalized care strategies.
In summary, advanced medical diagnostics software is revolutionizing patient care by providing a higher level of diagnostic accuracy and efficiency. Through the use of AI, comprehensive data integration, and real-time monitoring, these tools are empowering healthcare professionals to deliver more precise and individualized care, ultimately enhancing patient outcomes and overall healthcare quality.
#medical diagnosis software solutions#medical diagnostic software#medical diagnostic#diagnosis software#medical diagnostic apps#MEDICAL DIAGNOSTIC SOFTWARE DEVELOPMENT SERVICES#medical diagnostic solutions
0 notes
Text
Getting past ‘it’s IBS’ (Xi Chen, Aeon, June 04 2024)
"In the late 1980s, aged 12, Taryn was taken to her doctor’s office with cramping, bloating, and constipation after eating, and was told that she had ‘a nervous stomach’.
As a white girl growing up in New Jersey, she met a stereotype, and when initial bloodwork and imaging was negative for evidence of a ‘real’, or organic disease in her gut, one of Taryn’s doctors began writing in her charts that she had irritable bowel syndrome (IBS), a misdiagnosis that would follow Taryn for life.
At the time, IBS was considered by many to be a medically unexplained and therefore controversial illness, keeping company with conditions such as fibromyalgia and chronic fatigue syndrome.
As a result, it carried the stigma of being a psychosomatic illness, caused primarily by stress and anxiety, and Taryn was sent home with prescriptions for diet and exercise. (…)
Today, unlike in the 1990s, it is well established that conditions like IBS, collectively known as disorders of gut-brain interaction (DGBIs), are real diseases that disrupt the communication between the nervous system of the brain and spine, and the nervous system of the intestines.
First mentioned in the book The Irritable Gut (1979) by the gastroenterologist W Grant Thompson, the conditions were labelled ‘functional’ disorders – characterised not by structural damage to the hardware of the gut, but by a glitch in its ‘software’, in other words, its nervous system, charged with processing, receiving or relaying information coming in or going out.
Software is not as easily observed as hardware, however, and much of academic medicine views the mind and the body as two separate and distinct entities, a viewpoint called mind-body dualism.
Over time, and despite the more nuanced meaning intended by Thompson, the term ‘functional’ became associated exclusively with disorders of the mind.
This is part of the reason why there is still stigma against conditions like IBS, and why attempts to establish diagnostic criteria for IBS in particular suffered from vagueness. (…)
When academics read that IBS patients have higher rates of anxiety and depression, or that antidepressants are a treatment for IBS, many assume that this is because psychiatric symptoms cause symptoms of IBS without considering the inverse, that chronic undiagnosed abdominal pain predisposes patients to having mood disorders.
The real reason these drugs are effective, however, is that, in utero, the precursor cells for our gut and our brain actually share the same nervous system, and only later separate in embryonic development.
As a result, the two nervous systems utilise the same neurotransmitters, such as serotonin, to send messages between neurons.
This is why we sometimes feel butterflies in our stomach when we’re nervous, and why stress and anxiety often worsen symptoms of IBS, but do not necessarily cause it.
As Brown’s quote above implies, the stereotype of the anxious patient in pain applies not only to IBS but all patients who present to clinics with vague abdominal distress (including those with non-gastrointestinal conditions like endometriosis, who experience delayed diagnosis because providers take women’s pain less seriously than men’s).
A classic example is peptic ulcer disease, a cause of severe abdominal pain that for decades was denounced as a psychosomatic illness until Barry Marshall and Robin Warren discovered in 1983 that it was caused by a species of bacteria.
Before their findings, peptic ulcers were managed with diet and, frequently, surgery, when what patients needed were antibiotics. (…)
In my opinion, the root of the problem is medical education itself.
Unless a medical trainee becomes a gastroenterologist, it is unlikely that they will receive any specialised education in IBS, let alone the history of IBS research proving it to be an organic condition, despite 40 per cent of the general population having functional gastrointestinal disorders.
Partly, this is because a majority of medical education in countries including the US, the UK and Canada takes place in academic centres associated with hospitals, where medical students will probably never encounter a patient for whom their IBS symptoms are the primary reason for them appearing in the emergency room, and especially not for their admission to the hospital itself.
As a consequence, medical students also don’t get their knowledge of IBS tested by board examinations.
This speaks to the fact that, echoing Osler, IBS generally doesn’t kill patients, and our current healthcare system values measures of mortality and cure in response to acute complaints more than quality of life and the management of suffering from chronic issues such as IBS.
The same could be said about long COVID (which, to this day, is sometimes challenged as illegitimate) and chronic fatigue syndrome, where sufferers are often sent off to a psychiatrist for care.
The thinking is that these ongoing problems, where there is no mainstream route for testing and treatment, are not as important for medical students to know about compared with, say, a patient crashing after a cardiac arrest, even though most of the global disease burden across the developed and the developing world is caused by chronic, not acute, illness. (…)
These demographic patterns don’t explain who really has the disease – they just reveal medical and social bias and entrenched stereotypes: women are perceived as hysterical and diagnosis-seeking, while men are stoic and avoidant, for instance; or white women are thought to tolerate less pain than people of colour.
None of this, in reality, is true – but it is part of the reason why so many patients assume that what they suffer from won’t be justified by the presence of organic disease and therefore doesn’t warrant a doctor’s visit in the first place.
Such patients, treated so poorly within the medical mainstream, now have a community and identity of their own in the Wild West of alternative medicine that flourishes online.
Such groups, seeking to empower themselves and especially hoping to get well, today stand at loggerheads with the practices and physicians they have left behind.
Some accuse their former doctors of gaslighting them, and they deserve to be heard.
Much of what I have discussed regarding misdiagnoses of IBS assumes that healthcare providers, even when in error, always have good intentions and are sincere about using the diagnosis to clarify the patient’s medical case.
There were several elements of Taryn’s story, however, and in my own experiences of how DGBIs are taught in medical school, that make it difficult for me to believe that this assumption holds in most doctor visits.
Although one could argue that the blasé diagnoses of IBS and disordered eating for Taryn could be down to simple carelessness and negligence, honest errors, or someone being ‘just a bad doctor’, it’s obvious to me that a pattern was developing with Taryn’s interactions with different providers who weren’t taking her lived experience itself seriously, just as I had stopped taking my own experiences seriously.
What holds our stories together, I believe, is this phenomenon where both of our perceptions of our own ability to know what’s true or not were put into question."
11 notes
·
View notes
Text
The invention of the basic BCI was revolutionary, though it did not seem so at the time. Developing implantable electronics that could detect impulses from, and provide feedback to, the body's motor and sensory neurons was a natural outgrowth of assistive technologies in the 21st century. The Collapse slowed the development of this technology, but did not stall it completely; the first full BCI suite capable of routing around serious spinal cord damage, and even reducing the symptoms of some kinds of brain injury, was developed in the 2070s. By the middle of the 22nd century, this technology was widely available. By the end, it was commonplace.
But we must distinguish, as more careful technologists did even then, between simpler BCI--brain-computer interfaces--and the subtler MMI, the mind-machine interface. BCI technology, especially in the form of assistive devices, was a terrific accomplishment. But the human sensory and motor systems, at least as accessed by that technology, are comparatively straightforward. Despite the name, a 22nd century BCI barely intrudes into the brain at all, with most of its physical connections being in the spine or peripheral nervous system. It does communicate *with* the brain, and it does so much faster and more reliably than normal sensory input or neuronal output, but there nevertheless still existed in that period a kind of technological barrier between more central cognitive functions, like memory, language, and attention, and the peripheral functions that the BCI was capable of augmenting or replacing.
*That* breakthrough came in the first decades of the 23rd century, again primarily from the medical field: the subarachnoid lace or neural lace, which could be grown from a seed created from the patient's own stem cells, and which found its first use in helping stroke patients recover cognitive function and suppressing seizures. The lace is a delicate web of sensors and chemical-electrical signalling terminals that spreads out over, and carefully penetrats certain parts of the brain; in its modern form, its function and design can be altered even after it is implanted. Most humans raised in an area with access to modern medical facilities have at least a diagnostic lace in place; and, in most contexts, they are regarded as little more than a medical tool.
But of course some of the scientists who developed the lace were interested in pushing the applications of the device further, and in this, they were inspired by the long history of attempts to develop immersive virtual reality that had bedevilled futurists since the 20th century. Since we have had computers capable of manipuating symbolic metaphors for space, we have dreamed of creating a virtual space we can shape to our hearts' content: worlds to escape to, in which we are freed from the tyranny of physical limitations that we labor under in this one. The earliest fiction on this subject imagined a kind of alternate dimension, which we could forsake our mundane existence for entirely, but outside of large multiplayer games that acted rather like amusement parks, the 21st century could only offer a hollow ghost of the Web, bogged down by a cumbersome 3D metaphor users could only crudely manipulate.
The BCI did little to improve the latter--for better or worse, the public Web as we created it in the 20th century is in its essential format (if not its scale) the public Web we have today, a vast library of linked documents we traverse for the most part in two dimensions. It feeds into and draws from the larger Internet, including more specialized software and communications systems that span the whole Solar System (and which, at its margins, interfaces with the Internet of other stars via slow tightbeam and packet ships), but the metaphor of physical space was always going to be insufficient for so complex and sprawling a medium.
What BCI really revolutionized was the massively multiplayer online game. By overriding sensory input and capturing motor output before it can reach the limbs, a BCI allows a player to totally inhabit a virtual world, limited only by the fidelity of the experience the software can offer. Some setups nowadays even forgo overriding the motor output, having the player instead stand in a haptic feedback enclosure where their body can be scanned in real time, with only audio and visual information being channeled through the BCI--this is a popular way to combine physical exercise and entertainment, especially in environments like space stations without a great deal of extra space.
Ultra-immersive games led directly, I argue, to the rise of the Sodalities, which were, if you recall, originally MMO guilds with persistent legal identities. They also influenced the development of the Moon, not just by inspiring the Sodalities, but by providing a channel, through virtual worlds, for socialization and competition that kept the Moon's political fragmentation from devolving into relentless zero-sum competition or war. And for most people, even for the most ardent players of these games, the BCI of the late 22nd century was sufficient. There would always be improvements in sensory fidelity to be made, and new innovations in the games themselves eagerly anticipated every few years, but it seemed, even for those who spent virtually all their waking hours in these spaces, that there was little more that could be accomplished.
But some dreamers are never satisfied; and, occasionally, such dreamers carry us forward and show us new possibilities. The Mogadishu Group began experimenting with pushing the boundaries of MMI and the ways in which MMI could augment and alter virtual spaces in the 2370s. Mare Moscoviensis Industries (the name is not a coincidence) allied with them in the 2380s to release a new kind of VR interface that was meant to revolutionize science and industry by allowing for more intuitive traversal of higher-dimensional spaces, to overcome some of the limits of three-dimensional VR. Their device, the Manifold, was a commercial disaster, with users generally reporting horrible and heretofore unimagined kinds of motion-sickness. MMI went bankrupt in 2387, and was bought by a group of former Mogadishu developers, who added to their number a handful of neuroscientists and transhumanists. They relocated to Plato City, and languished in obscurity for about twenty years.
The next anybody ever heard of the Plato Group (as they were then called), they had bought an old interplanetary freighter and headed for the Outer Solar System. They converted their freighter into a cramped-but-servicable station around Jupiter, and despite occasionally submitting papers to various neuroscience journals and MMI working groups, little was heard from them. This prompted, in 2410, a reporter from the Lunar News Service to hire a private craft to visit the Jupiter outpost; she returned four years later to describe what she found, to general astonishment.
The Plato Group had taken their name more seriously, perhaps, than anyone expected: they had come to regard the mundane, real, three-dimensional world as a second-rate illusion, as shadows on cave walls. But rather than believing there already existed a true realm of forms which they might access by reason, they aspired to create one. MMI was to be the basis, allowing them to free themselves not only of the constraints of the real world (as generations of game-players had already done), but to free themselves of the constraints imposed on those worlds by the evolutionary legacy of the structures of their mind.
They decided early on, for instance, that the human visual cortex was of little use to them. It was constrained to apprehending three-dimensional space, and the reliance of the mind on sight as a primary sense made higher-dimensional spaces difficult or impossible to navigate. Thus, their interface used visual cues only for secondary information--as weak and nondirectional a sense as smell. They focused on using the neural lace to control the firing patterns of the parts of the brain concerned with spatial perception: the place cells, neurons which periodically fire to map spaces to fractal grides of familiar places, and the grid cells, which help construct a two-dimensional sense of location. Via external manipulation, they found they could quickly accommodate these systems to much more complex spaces--not just higher dimensions, but non-Euclidean geometries, and vast hierarchies of scale from the Planck length to many times the size of the observable universe.
The goal of the Plato Group was not simply to make a virtual space to inhabit, however transcendent; into that space they mapped as much information they could, from the Web, the publicly available internet, and any other database they could access, or library that would send them scans of its collection. They reveled in the possibilities of their invented environment, creating new kinds of incomprehensible spatial and sensory art. When asked what the purpose of all this was--were they evangelists for this new mode of being, were they a new kind of Sodality, were they secessionists protesting the limits of the rest of the Solar System's imagination?--they simply replied, "We are happy."
I do not think anyone, on the Moon or elsewhere, really knew what to make of that. Perhaps it is simply that the world they inhabit, however pleasant, is so incomprehensible to us that we cannot appreciate it. Perhaps we do not want to admit there are other modes of being as real and moving to those who inhabit them as our own. Perhaps we simply have a touch of chauvanism about the mundane. If you wish to try to understand yourself, you may--unlike many other utopian endeavors, the Plato Group is still there. Their station--sometimes called the Academy by outsiders, though they simply call it "home"--has expanded considerably over the years. It hangs in the flux tube between Jupiter and Io, drawing its power from Jupiter's magnetic field, and is, I am told, quite impressive if a bit cramped. You can glimpse a little of what they have built using an ordinary BCI-based VR interface; a little more if your neural lace is up to spec. But of course to really understand, to really see their world as they see it, you must be willing to move beyond those things, to forsake--if only temporarily--the world you have been bound to for your entire life, and the shape of the mind you have thus inherited. That is perhaps quite daunting to some. But if we desire to look upon new worlds, must we not always risk that we shall be transformed?
--Tjungdiawain’s Historical Reader, 3rd edition
81 notes
·
View notes
Text
17 // diagnostic (extra credit)

Welcome to SelfMed, your online personal medical evaluation assistant! If this is a medical emergency, please contact local authorities or Trauma Team for immediate help.
How can SelfMed assist you today?
>> diagnosis
Please list up to five major symptoms for a diagnosis using our QuickMatch™ technology.
[1] fever
[2] headache
[3] mania
[4] hallucinations
[5] not recognizing faces
———
QuickMatch™ Potential Diagnoses*
The symptoms listed are a complete or partial match to the diseases and disorders below:
Click for more information and recommended treatment options.
Schizophrenia [+]
Post-Traumatic Stress Disorder (PTSD) [+]
Cyberpsychosis [–]
Cyberpsychosis is a collective term for all psychotic and anxiety-related personality disorders caused by hardware implanted in the body and any and all behavioral mods, including software. Often this begins as changes to the personality, followed by increasingly erratic and even violent behavior. Some medications and substance abuse can worsen these behaviors.
Recommended treatment options:
- Therapy
- Implant deactivation and/or removal
- Bethaloperidol
While antipsychotics are widely used to slow the onset of cyberpsychosis, therapy has also proven effective for some patients after years of treatment. Those experiencing aggressive cyberpsychotic symptoms such as violent outbursts should be kept away from public spaces and denied access to weapons until they can be incapacitated, restrained, and removed for treatment.
If you or someone you know is experiencing symptoms of cyberpsychosis that result in erratic or violent behavior, remove yourself from any potentially dangerous situations and call MaxTac. Do NOT interrupt MaxTac officers during an ongoing violent situation. DO put as many walls between the situation and yourself as is possible to avoid stray projectiles and bodily harm.
*QuickMatch™ diagnoses are a quick-screening technology and should not be used to replace the services of a trained medical professional.
———
Your free trial SelfMed membership is valid for the next [7 DAYS].
By upgrading to a premium membership, you can access an additional seven diagnoses. Would you like to upgrade to a SelfMed premium membership today? (€$199 per mo.)
Enter promo code HEALTH10NOW for a limited time offer of 10% your first month of premium service!
———
Is there something else SelfMed can assist with?
>> nethaloperidol
We’re sorry, but we didn’t recognize that prompt.
Is there something else SelfMed can assist with?
>> bethaloperidol
Searching “bethaloperidol” yielded the following articles:
Bethaloperidol [–]
Bethaloperidol is an antipsychotic used to treat a broad range of disorders, ranging from Schizophrenia to hyperactivity. When prescribed by a doctor in combination with therapy, bethaloperidol has been proven effective in helping patients recover. Bethaloperidol can be taken in pill form or through injection. The most widely used brands are Bethal and Novadol.
Though black market bethaloperidol is frequently sold, it is not created in a lab environment where product quality is overseen, it is likely a cheaper alternative that will not address symptoms adequately, and/or it has been cut with other drugs that could be a potentially dangerous cocktail. Brand names are always recommended and more effective than their black market counterparts.
———
Searching for the nearest retailer that carries BETHALOPERIDOL? We’ve found 10 locations near you, less than 5 minutes away!
Upgrade to a premium membership to find trusted pharmaceutical outlets near you. (€$199 per mo.)
Enter promo code HEALTH10NOW for a limited time offer of 10% your first month of premium service!
———
Is there something else SelfMed can assist with?
>> ripperdoc
Searching “ripperdoc” yielded the following articles:
Ripperdocs: the new GP or back alley surgeon? [+]
Top 10 most horrifying ripperdoc patient stories [+]
Confessions of a street doctor: ripper reveals all [+]
Is there something else SelfMed can assist with?
>> nearest ripperdoc
We’re sorry, but we didn’t recognize that prompt.
Is there something else SelfMed can assist with?
>> fuck off
———
Thank you for using SelfMed!
Your feedback matters! Please rate your experience.
☆☆☆☆☆
#ffxivwrite2023#[ ffxivwrite2023 ]#[ cyberpunk ]#sunday is au day#sometimes writing cyberpunk means exercising the corporate copywriter in me for cynical purposes
15 notes
·
View notes
Text
Mass Effect Lore: Common technologies in the 2180's (Part 1: Omnitool)
This post is both a collection of canon technologies in the Mass Effect universe, and personal headcanon which may be borrowing common concepts from sci fi.
Part 1 will be dedicated to solely the omnitool, because omnitools provide the user with such a huge amount of features that they deserve their own post.
What is an omnitool?
The omnitool is a microchip implanted underneath the skin which upon activation, can project a holographic screen as well as a holographic keyboard to navigate said screen. However, omnitools can also be navigated via voice demands. Omnitools provide a variety of functions and can do pretty much anything that a computer, smart watch, phone, calculator or tablet could do.
Omnitool activation could be done vocally via a spoken password or in a tactile manner such as touching one‘s forearm in a certain rhythm and pattern.
Microfabricators can generate objects out of microplastic particles, but it isn‘t possible for an object to generate if the omnitool consists merely an implant under the skin. (I don‘t see how that‘s possible without space magic..)
Therefore an additional bracelet has to be worn, which contains the microparticles out of which an object can be forged.
The omnitool can be synced with the translator implant, updating the translator with new translation software.
What can the omnitool do?
Canon:
Allows communication via voice calls, video calls, voice messages and text messages
Provides intranet, internet and extranet access
Allows upload and download of data
Can be used for videography and photography
Can be used to play music
Can provide a flashlight
Provides a wide array of general programs, calendars, navigation programs and maps, note apps, alarms, games and more
Can be used for hacking, coding and decryption
Special programs can be used to utilize the microfabricator to form objects; if the bracelet is charged with certain particles it can also be used to fire particles which are commonly used for combat (incinerate or cryo blast function, for instance)
But that‘s the boring shit. That‘s what phones, tablets and computers can do nowadays, and the combat stuff is covered in the game.
Here‘s my headcanons added to it.
What special functions can an omnitool have?
It can fire fire extinguishing particles. (No pun intended) Meaning that little bracelet actually could serve as a fire extinguisher, using microparticles to extinguish fire.
The microfabricator should be able to forge any tool, such as a screwdiver out of microplastic. That explains why quarians seem to be able to fix things with just their omnitool. No need to take a toolbox with you when you‘ve got your omnitool.
Omnitools should be able to do anything that an advanced calculator can, meaning omnitool calculators provide more functions than a regular phone or tablet calculator. Basically that chip has a build in college level calculator.
Communication aid programs coupled with visors or smart lenses can scan and analyze the body language and facial expressions of conversation partners, listing likely interpretations for those who struggle to read other species.
More advanced omnitool models should be able to aid you with repairs, as well. Take a scan of a broken piece of tech and the omnitool might come up with a diagnostic of it and giving suggestions how to fix it. That would explain why everyone in ME seems so tech savvy - actually the omnitool just provides a ton of help.
Omnitools are capable of measuring pulse, heart rate, blood oxygen, blood sugar levels and blood pressure. They also can monitor sleep quality and duration. Steps taken during the day and stability of walking. Basically they have all the functions of a smart watch.
Just like you can fire a neural shock to disable someone, you can fire a targeted shock in form of a heart defibrillator to revive someone.
Other medical programs provide build in fever thermometer scanners.
Omnitool scans using medical scanners can also provide diagnostic aid, scanning for abnormalities and injuries. The most advanced models are capable of scanning broken bones, essentially having the function of x ray scans.
Certain programs give the user the ability to stimulate the vagus nerve to aid against stress or depression. If nerve stim programs for sexual stimulation are a thing, then this should be within the realms of possibility too. It is possible that this might require a piece of hardware to be synced to, however.
Omnitools also make great morning alarm clocks, being capable of emitting light that emulates a sunrise filling the entire room to wake up a person. The vital scanner takes note of your awakening, which causes the alarm to slowly stop, dimming the lightning and turning down the music volume (if you’ve set a music alarm) slowly.
Some people also like receiving comfortable vibrations through their body through their omnitool to wake up from their sleep.
Other handy stuff that you could fabricate using the microplastic fabricator (aside from blades and tools): cutlery, bowls and cups, razor blades, hair brushes and combs, scissors. Yeah, you‘re gonna have kids in class who forgot to bring their scissors and cut out stuff with omnitool fabricated scissors.
9 notes
·
View notes
Last Seen Blogs




