#malaria blood report
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
The total number of visits Tumblr.com received during January 2021 is 327 million.
Text
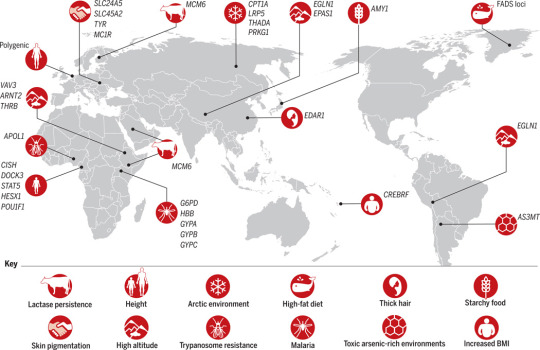
Recent evolutionary adaptations to the environment in human populations, from Going global by adapting local: A review of recent human adaptation (Fan et al., 2016). The icons show the type of adaptation recorded in various parts of the world, and the acronyms besides (e.g. EDAR1) are the names of the involved genes. Also see Genome-wide detection and characterization of positive selection in human populations (Sabeti et al., 2009), Population Genomics of Human Adaptation (Lachance & Tishkoff, 2013).
Some examples are:
Lactase persistence in Europe, Near East, and East Africa, allowing the digestion of milk in adult age (by default, the lactase required to digest milk sugar would only be produced by infants; this was just a matter of removing a timed switch).
Similarly, greater production of amylase, which breaks down starch, is reported in Europe and Japan (diet based on farmed grains) and among the Hadza of Tanzania (diet based on starchy tubers).
Improved conversion of saturated into unsaturated fatty acids in the Arctic Inuit peoples. This makes it easier to live on a diet of fish and marine mammals in an environment where plant food is scarce.
Smaller stature ("defined as an average height of <150 cm in adult males") in the "pygmy" peoples (Aka and Mbuti) of Central Africa, and other hunter-gatherer peoples in equatorial Asia and South America. This helps shed heat in a hot humid climate where sweat does not evaporate.
More efficient fat synthesis in the Samoa, helping with energy storage at the price of more risk of obesity or diabetes with a richer modern diet.
Improved resistence to malaria, sleeping sickness (trypanosome), and Lassa fever in Subsaharan Africa. Fighting off against parasites is especially difficult (since unlike the inorganic environment, parasites also evolve), so this resistence often comes at a cost, such as anhemia, but is still a great advantage on net. Some improved resistence to arsenic poisoning is noted in an Argentinian population.
Denser red blood cells on the Andean, Ethiopian, and Tibetan highlands, to carry more oxygen which is scarcer at high altitude. I recall from elsewhere that this might increase the risk of thrombosis or strokes due to obstructed blood vessels.
Less melanin (which blocks UV light) and therefore lighter skin color in Eurasia. Melanin shields skin cells from damage due to UV radiations, but some UV light is necessary for the synthesis of vitamin D.
A change in the gene EDAR1, resulting in denser head hair, slightly different tooth shape, and fewer sweat glands (all skin annexes), appears strongly selected for in East Asia, but as far as I can find the advantage of this mutation is still unknown.
From another article (Ilardo et al., 2018): the Sama Bajau people of Indonesia, who have a long tradition of free-diving in apnea, seem to have developed larger spleen to store more oxygenated blood during dives.
33 notes
·
View notes
Text
Debridement
By Michael S. Harper
Debridement
Black men are oaks cut down. Congressional Medal of Honor Society United States of America chartered by Congress, August 14, 1958; this certifies that STAC John Henry Louis is a member of this society. “Don’t ask me anything about the medal. I don’t even know how I won it.” Debridement: The cutting away of dead or contaminated tissue from a wound to prevent infection. America: love it or give it back.
Corktown
Groceries ring
in my intestines:
grits aint groceries
eggs aint poultry
Mona Lisa was a man:
waltzing in sawdust
I dream my cards
has five holes in it,
up to twenty holes;
five shots out of seven
beneath the counter;
surrounded by detectives
pale ribbons of valor
my necklace of bullets
powdering the operating table.
Five impaled men loop their ribbons
’round my neck
listening to whispers of valor:
“Honey, what you cryin’ ’bout?
You made it back.”
Caves
Four M-48 tank platoons ambushed
near Dak To, two destroyed:
the Ho Chi Minh Trail boils,
half my platoon rockets
into stars near Cambodia,
foot soldiers dance from highland woods
taxing our burning half:
there were no caves for them to hide.
We saw no action,
eleven months twenty-two days
in our old tank
burning sixty feet away:
I watch them burn inside out:
hoisting through heavy crossfire,
hoisting over turret hatches,
hoisting my last burning man
alive to the ground,
our tank artillery shells explode
killing all inside:
hoisting blown burned squad
in tank’s bladder,
plug leaks with cave blood:
there were no caves for them to hide—
In the Projects
Slung basketballs at Jeffries
House with some welfare kids
weaving in their figure eight hunger.
Mama asked if I was taking anything?
I rolled up my sleeves:
no tracks, mama:
“black-medal-man ain’t street-poisoned,”
militants called:
“he’s an electronic nigger!”
“Better keep electronic nigger 'way.”
Electronic Nigger?
Mama, unplug me, please.
A White Friend Flies In from the Coast
Burned—black by birth,
burned—armed with .45,
burned—submachine gun,
burned—STAC hunted VC,
burned—killing 5-20,
burned—nobody know for sure;
burned—out of ammo,
burned—killed one with gun-stock,
burned—VC AK-47 jammed,
burned—killed faceless VC,
burned—over and over,
burned—STAC subdued by three men,
burned—three shots: morphine,
burned—tried killing prisoners,
burned—taken to Pleiku,
burned—held down, straitjacket,
burned—whites owe him, hear?
burned—I owe him, here.
Mama’s Report
“Don’t fight, honey,
don’t let ’em catch you.”
Tour over, gear packed,
hospital over, no job.
“Aw man, nothin' happened,”
explorer, altar boy—
Maybe it’s ’cause they killed people
and don’t know why they did?
My boy had color slides of dead people,
stacks of dead Vietnamese.
MP’s asked if he’d been arrested
since discharge, what he’d been doin’:
“Lookin’ at slides,
looking’ at stacks of slides, mostly.”
Fifteen minutes later a colonel called
from the Defense Department, said he’d won the medal;
could he be in Washington with his family,
maybe he’d get a job now; he qualified.
The Democrats had lost, the president said;
there were signs of movement in Paris:
Fixing Certificates: Dog Tags: Letters Home
Our heliteam had mid-air blowout
dropping flares—5 burned alive.
The children carry hand
grenades to and from piss tubes.
Staring at tracer bullets
rice is the focal point of war.
On amphibious raid, our heliteam
found dead VC with maps of our compound.
On morning sick call you unzip;
before you piss you get a smear.
“VC reamed that mustang a new asshole”—
even at movies: “no round-eye pussy no more”—
Tympanic membrane damage: high gone—
20-40 db loss mid-frequencies.
Scrub-typhus, malaria, dengue fever, cholera;
rotting buffalo, maggoted dog, decapped children.
Bangkok: amber dust, watches, C-rations,
elephanthide billfolds, cameras, smack.
Sand&tinroof bunkers, 81/120 mm:
“Health record terminated this date by reason of death.”
Vaculoated amoeba, bacillary dysentery, hookworm;
thorazine, tetracycline, darvon for diarrhea.
'Conitus’: I wanna go home to mama;
Brown’s mixture, ETH with codeine, cortisone skin-creams.
Written on helipad fantail 600 bed Repose;
“no purple heart, hit by ’nother marine.”
“Vascular repair, dissection, debridement”:
sharp bone edges, mushy muscle, shrapnel: stainless bucket.
Bodies in polyethylene bag: transport:
'Tan San Nhat Mortuary’
Blood, endotracheal tube, prep
abdomen, mid-chest to scrotum—
“While you’re fixin' me doc,
can you fix them ingrown hairs on my face?”
“They didn’t get my balls, did they?”
50 mg thorazine—“Yes they did, marine!”
Street-Poisoned
Swans loom on the playground
swooning in the basket air,
the nod of their bills
in open flight, open formation.
Street-poisoned, a gray mallard
skims into our courtyard with a bag:
And he poisons them—
And he poisons them—
Electronic-nigger-recruiter,
my pass is a blade
near the sternum
cutting in:
you can make this a career.
Patches itch on my chest and shoulders—
I powder them with phisohex
solution from an aerosol can:
you can make this a career.
Pickets of insulin dab the cloudy
hallways in a spray.
Circuits of change
march to an honor guard—
I am prancing:
I am prancing:
you can make this a career.
Makin’ Jump Shots
He waltzes into the lane
’cross the free-throw line,
fakes a drive, pivots,
floats from the asphalt turf
in an arc of black light,
and sinks two into the chains.
One on one he fakes
down the main, passes
into the free lane
and hits the chains.
A sniff in the fallen air—
he stuffs it through the chains
riding high:
“traveling” someone calls—
and he laughs, stepping
to a silent beat, gliding
as he sinks two into the chains.
Debridement: Operation Harvest Moon: On Repose
The sestina traces a circle in language and body.
Stab incision below nipple,
left side; insert large chest tube;
sew to skin, right side;
catch blood from tube
in gallon drain bottle.
Wash abdomen with phisohex;
shave; spray brown iodine prep.
Stab incision below sternum
to symphis pubis
catch blood left side;
sever reddish brown spleen
cut in half; tie off blood supply;
check retroperitoneal,
kidney, renal artery bleeding.
Dissect lateral wall
abdominal cavity; locate kidney;
pack colon, small intestine;
cut kidney; suture closely;
inch by inch check bladder,
liver, abdominal wall, stomach:
25 units blood, pressure down.
Venous pressure: 8; lumbar
musculature, lower spinal column
pulverized; ligate blood vessels,
right forearm; trim meat, bone ends;
tourniquet above fracture, left arm;
urine, negative: 4 hours; pressure
unstable; remove shrapnel flecks.
Roll on stomach; 35 units blood;
pressure zero; insert plastic blood
containers, pressure cuffs; pump chest
drainage tube; wash wounds sterile
saline; dress six-inch ace wraps;
wrap both legs, toe to groin; left arm
plaster, finger to shoulder: 40 units blood.
Pressure, pulse, respiration up;
remove bloody gowns; scrub; redrape;
5 cc vitamin K; thorazine: sixth
laparotomy; check hyperventilation;
stab right side incision below nipple;
insert large chest tube; catch blood drain bottle ...
The Family of Debridement
Theory: Inconvenienced subject will return to hospital
if loaned Thunderbird
Withdrawn. Hope: Subject returns,
Treatment:
Foreclosure for nine months unpaid mortgage;
wife tells subject hospital wants deposit,
Diseased cyst removal:
'Ain’t you gonna give me a little kiss good-bye’
Subject-wife: To return with robe and curlers—
Subject tells friend he’ll pay $15 to F’s stepfather
if he’ll drive him to pick up money owed him.
“This guy lives down the street,
I don’t want him to see me coming.”
“It looked odd for a car filled with blacks
to be parked in the dark in a white neighborhood,
so we pulled the car out under a streetlight
so everybody could see us.”
Store manager: “I first hit him with two bullets
so I pulled the trigger until my gun was empty.”
“I’m going to kill you, you white MF,” store manager
told police. Police took cardload, F and F’s parents for
further questioning. Subject died on operating table: 5 hrs:
Subject buried on grass slope, 200 yards
east of Kennedy Memorial,
overlooking Potomac and Pentagon,
to the south,
Arlington National Cemetery.
Army honor guard
in dress blues,
carried out assignment
with precision:
2 notes
·
View notes
Text
Leishmaniasis
Case Reports, like we're on a episode of house
23M in Kenya, presenting with months of LOW, persistent fevers, and abdo fullness, found to have massive splenomegaly.
examination: massive splenomegaly (10 cm below costophrenic margin, and will definitely cross midline) and hepatomegaly
pancytopaenic on bloods, plt's down to 40s
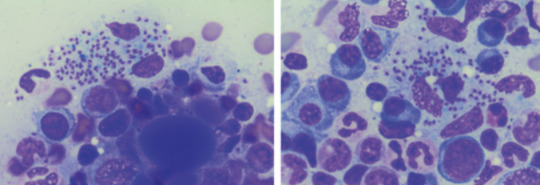
diagnosis confirmed on BMAT (parasite seen)
normal HIV, liver and kidney function
Bodies seen on the BMAT below are part of the lifecycle of the parasite that is intracellular, hence you can see the macrophages/neutrophils loaded with them, even bursting
What is it:
think of it when you get a patient with pancytopaenia and hepatosplenomegaly, who either traveled to or is in/from a tropical/subtropic region (where sand flies are)
cause - protozoa parasite Leishmania, transmitted by infected sandflies
Epidemio (when to consider it)
tropics, subtropics (South America, Asia, AFrica), Southern Europe
Microbiology/Transmission
parasite, replicates intracellularly (Leishmania donovani)
transmitted in sand flies (can be unnoticeable and usually bite in dawn or dusk - evenings or night), can also be transmitted via needles/blood
more common in rural areas
I've simplified this, but is more extensively covered in StatPearls and Wiki (there's different species of Leish and sandflies that transmit it)
once bitten, the protozoa are phagocystosed by skin macrophages, which then becomes full of the "bodies" (part of the lifecycle). Eventually these burst to release more of the bodies that infect more macrophages
they eventually are spread via blood to liver/spleen/BM and LNs
Random history:
ancient, records of disease date back to Egyptian mummies from 3000 BC --> positive DNA amplication for Leishmania and on papyrus from 1500 BC
multiple physicians from different times have described the disease, but it's named for 2 who described the parasite's intracellular ovoid body stage in smears from infected patients in India: Lt General William Boog Leishman and Captain Charles Donovan (Ronald Ross named the bodies after the 2 --> "Leishman Donovan bodies"
significant disease in Allied troops in Sicily in WWII, called "jericho buttons" (image on wiki from a WWI trooper serving in the middle east)

Leishman: Scottish pathologist and British Army medical officer, later it's director general in the 20s, did extensive research into the parasite named for him by Sir Ronald Ross. He mistook the parasite he observed for trypanosomes (cause of Chagas in South America and African sleeping sickness in Africa)
Donovan: Irish parasitologist, medical officer in India, observed an epidemic across India just after the rebellion of 1857, discovered the "bodies" in spleen tissue as the causative agent for what the locals called "kala azar" (severe visceral leishmaniasis - see below)
Donovan also discovered the "bodies" of Klebsiella granulomatis, hence these too are named after him (cause of ulcerative granulomas)
It became scandalous as both wanted credit for the "discovery" of this newly identified organism. So Sir Ronald Ross named it for both of them.
Sir Ron, by the way, won a Nobel in Medicine for discovering that malaria is transmitted via mossies (this was also a source of scandal, he was meant to share it with another physician who he accused of fraud - and they never received the award)
finally, it was actually a Russian physician who identified it first, but well, he published in a little known Russian journal which was promptly forgotten.
Clinical features
cutaneous type vs visceral organ type (spleen, liver, bones)
From wiki

can be asymptomatic
cutnaeous: can be there for years and resemble leprosy, causes an open chronic wound (most common), incubation 2-4 weeks on average (nodules at site of inoculation that eventually form ulcers), can heal spontaneously in 2-5 yrs
in diffuse cutaneous cases, can affect face, ears, extensor surfaces
can be muscosal = eg nasal symptoms/epistaxis, severe: perforated septum, this occurs in 1/3 after resolution of cutaenous symptoms (can be severe/lifte threatning, as it can affect vocal cords and cartilage, but oddly not bone)
visceral (incubation periods of up to years until immuncompromise): fever, weight loss, hepatosplenomegaly (spleen more than liver), pancytoaepnia, high total protein and low albumin with hypergammaglobulinaemia
this has seasonal peaks related to sandfly habits and humidity
interestingly it is an infective cause of massive splenomegaly, such that it crosses the midline
Extreme - but noticeable hepatosplenomgealy/abdo fullness, from medscape

can be atypical in HIV co infected patients, LAD in seom regions like Africa
Kala azar = black fever in some severe cases (fatal due to secondary mycobacterial infection or bleeding), refers to damage fto spleen, liver and anaemia
invstigations:
serology not great (minimal humoral response to the parasite), so often requires histopath (tissue sample) for which BMAT is safest in visceral organ involvement
visualisation of amastigotes (or Leishman-Donovan bodies), as intracellular --> can be seen in macrophages (small round bodies) post Giemsa staining
PCR of DNA also possible (as done in the Egyptian mummies)
Image source:

Treatment
liposomal amphotericin B (holy shit strong stuff) in visceral, PO: miltefosine (caution in pregnancy), all have significant ADRs, or paromycin. however, mortality of 10% if visceral left untreated
mixed results with azoles
in HIV co infection - start the HAARTs! can improve survival, mortality is 30% in HIV patients
cutaneous: stibolgluconate (have never heard of these drugs) and megluaine antimoniate, but limited disease often spotnaeously gets cleared by the innate system
prevention:
use DEET insect repellant at dawn and dusk
loose fitting clothing that covers all skin
no vaccine (were attempts at vaccinating dogs, which decreased rates)
sandflies are smaller than mossies, so requires small netting

Differentials for hepatosplenomegaly

Sources:
WHO guidelines
CDC guidlelines
Wiki - Haven't covered pathophysio, but wiki does extensively
StatPearls
DermNet - great resource for all things derm, that my derm colleagues pointed out to me
10 notes
·
View notes
Text
Re-emergence of Oropouche virus between 2023 and 2024 in Brazil: an observational epidemiological study

Background
Oropouche virus is an arthropod-borne virus that has caused outbreaks of Oropouche fever in central and South America since the 1950s. This study investigates virological factors contributing to the re-emergence of Oropouche fever in Brazil between 2023 and 2024.
Methods
In this observational epidemiological study, we combined multiple data sources for Oropouche virus infections in Brazil and conducted in-vitro and in-vivo characterisation. We collected serum samples obtained in Manaus City, Amazonas state, Brazil, from patients with acute febrile illnesses aged 18 years or older who tested negative for malaria and samples from people with previous Oropouche virus infection from Coari municipality, Amazonas state, Brazil. Basic clinical and demographic data were collected from the Brazilian Laboratory Environment Management System. We calculated the incidence of Oropouche fever cases with data from the Brazilian Ministry of Health and the 2022 Brazilian population census and conducted age–sex analyses. We used reverse transcription quantitative PCR to test for Oropouche virus RNA in samples and subsequently performed sequencing and phylogenetic analysis of viral isolates. We compared the phenotype of the 2023–24 epidemic isolate (AM0088) with the historical prototype strain BeAn19991 through assessment of titre, plaque number, and plaque size. We used a plaque reduction neutralisation test (PRNT50) to assess the susceptibility of the novel isolate and BeAn19991 isolate to antibody neutralisation, both in serum samples from people previously infected with Oropouche virus and in blood collected from mice that were inoculated with either of the strains.
Findings
8639 (81·8%) of 10 557 laboratory-confirmed Oropouche fever cases from Jan 4, 2015, to Aug 10, 2024, occurred in 2024, which is 58·8 times the annual median of 147 cases (IQR 73–325). Oropouche virus infections were reported in all 27 federal units, with 8182 (77·5%) of 10 557 infections occurring in North Brazil. We detected Oropouche virus RNA in ten (11%) of 93 patients with acute febrile illness between Jan 1 and Feb 4, 2024, in Amazonas state. AM0088 had a significantly higher replication at 12 h and 24 h after infection in mammalian cells than the prototype strain. AM0088 had a more virulent phenotype than the prototype in mammalian cells, characterised by earlier plaque formation, between 27% and 65% increase in plaque number, and plaques between 2·4-times and 2·6-times larger. Furthermore, serum collected on May 2 and May 20, 2016, from individuals previously infected with Oropouche virus showed at least a 32-fold reduction in neutralising capacity (ie, median PRNT50 titre of 640 [IQR 320–640] for BeAn19991 vs <20 [ie, below the limit of detection] for AM0088) against the reassortant strain compared with the prototype.
Interpretation
These findings provide a comprehensive assessment of Oropouche fever in Brazil and contribute to an improved understanding of the 2023–24 Oropouche virus re-emergence. Our exploratory in-vitro data suggest that the increased incidence might be related to a higher replication efficiency of a new Oropouche virus reassortant for which previous immunity shows lower neutralising capacity.
Read the paper.
#brazil#politics#science#healthcare#epidemiology#oropouche#brazilian politics#image description in alt#mod nise da silveira
2 notes
·
View notes
Text














World Heart Day
Heart Day is part of an international campaign to spread awareness about heart disease and stroke prevention. This is the perfect day to quit smoking, get exercising and start eating healthy – all in the name of keeping your ticker in good working order, and improving the health and well being of people the world over.
Learn about World Heart Day
The World Heart Federation have found that heart disease and strokes are the world’s leading cause of death, killing 17.1 million people every year – that’s more than victims of cancer, HIV and AIDS and malaria.
Overeating, lack of exercise, unhealthy diets and high blood pressure, cholesterol and glucose levels are all factors which can trigger heart disease and threaten our own lives, and those of loved ones. Heart Day was set up to drive home the message that heart problems can be prevented.
History of World Heart Day
The aim is to improve health globally by encouraging people to make lifestyle changes and promoting education internationally about ways to be good to your heart. This lesson is becoming increasingly relevant as reports of obesity, poor diet and physical inactivity in children and young people become more and more common.
Events take place to promote healthy hearts. Charities and other organisations coordinate walks and runs, health checks, public talks, shows and exhibitions to name a few of the interesting and informative events which mark the day. So on Heart Day, get involved, eat your fruit and veg and get outside; both you and your heart will feel the benefits.
World Heart Day is celebrated every year. It was created by the World Heart Federation. The first World Heart Day took place back in 2000. Since then, in 2012, leaders from around the globe committed to the reduction of worldwide mortality from non-communicable diseases by 25 percent by 2025.
Did you know that almost half of the NCD deaths happen because of cardiovascular disease? This makes it the biggest killer across the world. Therefore, World Heart Day is the perfect platform for the community to come together in the battle against cardiovascular disease and lower the worldwide disease burden.
How to observe World Heart Day
As World Heart Day is all about drawing people’s attention to heart diseases and illnesses, as well as the range of health issues that are associated with this, it makes sense to raise awareness and also improve your own understanding. We would recommend taking some time to do a bit of research about heart conditions and risk factors. You can then use your online platforms and your social groups in order to raise awareness.
There are both non-governmental and governmental organizations that take part in this date around the world. They do this through the organization of science fairs, exhibitions, fitness sessions, public talks, walks, and marathons. Some famous buildings, monuments, and landmarks opt to go red on this date so that they can show their support for cardiovascular disease awareness.
If you are opting to celebrate this day, it is important to try and be more attentive to your own heart health. There are a number of different ways that you can do this. This includes following a healthy diet, quitting alcohol, stopping smoking, and getting involved in physical exercises. It is also important to have your cholesterol, blood pressure, and heart checked on a regular basis.
It is a good idea to take a look online to see if there are any events that are going on in your local area. If there are not, how about organizing an event yourself? All you need is an idea that is going to get the community involved and raise awareness for heart disease. This could be anything from a fun run to a community fair. It is up to you.
You don’t need to do an event on such a big scale either. You could gather your friends and family members and host a fun event, educating them on the issues and asking them to make a donation. Other ways to fundraise include making crafts and then donating the proceeds to a heart foundation or charity.
There are a lot of different charities and organizations that are doing great work when it comes to raising awareness and finding cures for different heart problems. We are sure that they would appreciate a donation, whether this is a donation of your time, money, or both! After all, anything that you can do can make a difference to someone’s life, so do not underestimate the role that you can play.
Source
#Davie Village#Vancouver#Forever in my Heart by James Cable#Alamosa#Napa#Paradise#Heartfullness Vegas by Katy Boynton#Take Heart by Patricia Vader#World Heart Day#WorldHeartDay#29 September#public art#sculpture#USA#Canada#travel#original photography#Distillery Historic District#Toronto#summer 2015#2019#vacation#cityscape#architecture#Glenn Gould Gathering by Ruth Abernethy#Sacred Heart of Jesus#Trois-Rivières#Hotel Château Gütsch#Luzern#Lucerne
2 notes
·
View notes
Text
In Jalan Raya Pos, Jalan Daendels, Pramoedya reveals the murkiest side of mass killing in the building of this highway, which was laid down with the blood and tears of thousands of locals whose corpses littered the road. Jl. Raya Pos was built and widened under the direction of Dutch East Indies Governor Herman Willem Daendels (1762-1818) and spanned the cities of Anyer, Cilegon, Serang, Tangerang, Batavia, Depok, Bogor, Cianjur, Cimahi, Bandung, Sumedang, Cirebon, Brebes, Tegal, Pekalongan, Semarang, Demak, Kudus, Rembang, Tuban, Gresik, Surabaya, Sidoarjo, Pasuruan and Probolinggo, ending in Panarukan. The idea of building Jl. Raya Pos struck Daendels on April 29, 1808, while on a tour from Buetenzorg, or Bogor, to Semarang and to Oosthoek, or East Java. On May 5 that year, he decided to construct en route a 250-kilometer road from Bogor to Karangsembung in Cirebon. The road was designed to reach a width of 7.5 meters where possible. In building the road along the Java Sea coastline, forced laborers were not only worn out but also suffered from malaria. Most workers perished from exhaustion, harsh treatment and malaria as they were draining marshland. The same was true in areas where the road had to penetrate difficult terrain like in Ciherang Sumedang, now known as Cadas Pangeran, where they were forced to build through hilly zones with only simple tools. Under such tough conditions, the first reported death toll reached 5,000; but a report from British sources put the number of people who died in the construction of Jl. Raya Pos at 12,000. This, however, was only the recorded toll, and the actual number is believed to have been greater. No official commissions have ever investigated the case.
Jalan Raya Pos, Jalan Daendels
#indonesia#never forget#You can't convince yesterday's colonizer that today's colonizer is wrong.#netherlands
4 notes
·
View notes
Text
Convenient Blood Test at Home: A Hassle-Free Solution
With busy schedules and health concerns on the rise, getting a blood test at home in Ahmedabad, Surat, Vadodara, and Delhi NCR is now easier than ever. Home-based diagnostic services offer a seamless and stress-free way to monitor your health without the need to visit a lab. In this blog, we explore the benefits, process, and availability of blood test services at home in Ahmedabad and other major cities.

Why Choose a Blood Test at Home?
Opting for a blood test at home in Surat, Vadodara, or Delhi NCR has multiple advantages:
Time-Saving: No need to wait in long queues at diagnostic centers.
Comfort and Convenience: Get tested from the comfort of your home.
Safe and Hygienic: Reduces exposure to infections in crowded places.
Accurate and Quick Reports: Receive timely results for better health management.
Personalized Services: Professional lab technicians ensure precise sample collection.
Blood Test at Home in Ahmedabad: Reliable & Fast
If you're looking for a blood test in Ahmedabad, home collection services provide a quick and efficient way to get tested. From routine checkups to specialized diagnostics, you can book tests like:
Complete Blood Count (CBC)
Thyroid Function Tests (T3, T4, TSH)
Diabetes Profile (HbA1c, Fasting Blood Sugar)
Liver and Kidney Function Tests
Vitamin Deficiency Tests
These services ensure that you can monitor your health with ease and accuracy.
Blood Test at Home in Surat: Quality Diagnostic Services
Residents of Surat can now benefit from home blood test services that prioritize accuracy and hygiene. The entire process is simple:
Online Booking: Select your required test and book an appointment.
Sample Collection: A certified technician arrives at your home.
Lab Testing: The sample is analyzed at a NABL-certified lab.
Report Delivery: Digital reports are shared within 24-48 hours.
With trained professionals handling sample collection, you can be assured of precise and reliable results.
Blood Test at Home in Vadodara: Hassle-Free Health Monitoring
For individuals in Vadodara, getting a blood test at home is now convenient and affordable. Whether it’s a full body health checkup or specific diagnostic tests, professionals ensure that the process is seamless and stress-free. Also visit Blood test at home Vadodara.
Popular Tests Available in Vadodara:
Lipid Profile (Cholesterol, Triglycerides, HDL, LDL)
Hormone Tests (Testosterone, Estrogen, Cortisol)
Allergy Tests
COVID-19 RTPCR and Antibody Tests
Dengue, Malaria, and Typhoid Tests
Blood Test at Home in Delhi NCR: Advanced Healthcare at Your Doorstep
With Delhi NCR’s fast-paced life, getting a blood test at home saves both time and effort. Certified pathology labs now offer doorstep sample collection, ensuring convenience and safety.
Advantages of Home Blood Testing in Delhi NCR:
NABL and ISO-certified laboratories ensure accuracy.
Highly trained phlebotomists maintain hygiene standards.
Digital reports make it easy to share with doctors.
Affordable pricing with insurance-covered tests.
How to Book a Blood Test at Home?
Booking a blood test in Ahmedabad, Surat, Vadodara, or Delhi NCR is quick and easy:
Choose a Trusted Diagnostic Service: Research and select a reputed provider.
Select Your Test: Pick from a list of available tests.
Schedule an Appointment: Choose a convenient date and time.
Get the Test Done: A trained professional collects your sample.
Receive Your Reports: Get digital reports for easy reference.
Prioritize Your Health with At-Home Blood Testing
Getting a blood test at home in Delhi NCR, Ahmedabad, Vadodara, and Surat is a step towards hassle-free healthcare. It saves time, ensures safety, and provides accurate results without any inconvenience. Book your test today and stay ahead in your health journey!
#bloodtestathomeahmedabad#bloodtestathomesurat#bloodtestathomevadodara#bloodtestathomedelhincr#bloodtestahmedabad
0 notes
Text
How to Choose the Best Pathology Lab in Ghatkopar, Mumbai?

Finding a reliable Pathology Lab in Ghatkopar, Mumbai is crucial for accurate medical testing and timely diagnosis. Whether you need a routine blood test or advanced diagnostics, selecting a trustworthy lab ensures quality healthcare. At Aspira Diagnostics, we provide precise reports, cutting-edge technology, and expert consultation to help you stay on top of your health.
What Are the Key Factors in Choosing a Pathology Lab in Ghatkopar, Mumbai?
Accreditation and certifications (NABL-approved labs).
Use of advanced diagnostic equipment.
Qualified and experienced pathologists.
Fast and reliable report delivery.
Online test booking convenience.
What Tests Are Available at a Pathology Lab in Ghatkopar, Mumbai?
A trusted Pathology Lab in Ghatkopar, Mumbai offers:
Routine blood and urine tests.
Diabetes, cholesterol, and thyroid screenings.
Cancer markers and biopsy tests.
Infectious disease tests like dengue, malaria, and COVID-19.
Vitamin and hormone profile tests.
How Can You Book an Appointment at a Pathology Lab in Ghatkopar, Mumbai?
Visit Aspira Diagnostics for online test booking.
Call our helpline for assistance.
Walk in for instant sample collection.
Schedule a home sample collection for convenience.
Why Is Aspira Diagnostics the Best Pathology Lab in Ghatkopar, Mumbai?
NABL-certified for high-quality testing.
Latest diagnostic tools for precise results.
Affordable pricing with no hidden charges.
Quick turnaround time for test reports.
Free doctor consultation with select tests.
How to Locate a Reliable Pathology Lab in Ghatkopar, Mumbai?
Finding a Pathology Lab in Ghatkopar, Mumbai is easy with Google Maps. Aspira Diagnostics is conveniently located for easy access.
For trustworthy medical testing, choose Aspira Diagnostics today!
0 notes
Text
Right, I elected to rewrite the lord for the Free People’s Militia, so I hope you enjoy
The Free People’s Milita
The founding of the Free People’s Militia is not exactly something that can be pinned down, as it is fundamentally an unorganized group and not all of them operate under the same name. However, the general agreed upon origin is within the winter of January 17th, 2268.
After the Bombardment of 2267 left Poland’s, and much of the world’s, ability to make war all but destroyed, so the initial invasion of the Gan’Tel Cohiliton went unopposed. Officially, they annexed the entire planet, their superior technology and numbers overwhelming the human forces in a month. But, though they controlled the planet, history has shown us that no conquered group goes down without a fight. It only took a week for whispers of rebellion to begin to form. The rural areas of Poland were left rarely policed, as they focused on the densely populated cities. These whispers grew louder, weapons were stockpiled, plans were laid, and war was planned. Such planning took place all over Poland, and all over the planet as well. The only question that stood was who would start first.
That answer came during a nasty blizzard in January, where a group known as the Wolni Ludzie began the campaign to take back Łódź. Reports state that at 0300, during the peak of the storm, an IED went off around the Coalition's barracks in the center of the city, prompting the established sleeper cell to burst to life. The Coalition was the one who was blindsighted now, unprepared for the attack and ill prepared for the raging storm, they were fighting on the backfoot, fighting ghosts in the snow. This rebellion would have been easy to crush, however, in a coordinated move, the Vieille Garde began their moves to take back Parris in France, and Taskforce Iron exploded in action across the Rhineland, not helping matters was that many groups of rebellion in Poland began to unite under the banner of the Wolni Ludzie, the small militia growing into a formidable army. The Invaders were stretched thin, and it wasn’t long till they had to concede Łódź in order to save more important sights.
It was a small victory, barely an inconvenience on the grand scale, but it made a point. Humanity would not go quietly into that cold night. And as word spread, more and more uprising began. Some ill fated, some short lived, but others were successful, raising hell and gaining territory as more formal armies began to mobilize, the engines of war greased by blood. Of course, the Wolni Ludzie were not the only ones fighting the good fight.
In Brazil, a group known as the Novo Cangaço formed nearly immediately after the invasion. Operating out of the deserts, they practiced social banditry, like their predecessors. Harassing supply lines and stealing to make a buck, giving it back to the people. They were well liked, but few were willing to revolt against such an indestructible foe, at least, until Łódź showed them a crack in the armor. Suddenly, the Coalition became bogged down in the cities, as groups of rebels and bandits, trained by the former military police and criminals, began to engage them in bloody skirmishes within the streets. The jungles were worse, after all, the adage of “Eles queriam lutar contra os soldados, mas o que encontraram foram animais” was coined by them. The invaders died to poisoned darts and starving beasts, dropped from malaria and shot by nightmares hiding in the trees.
While in the USA, a place nearly flattened by the Invader’s bombardment, the Smoky Mountain Force survived. They appeared soon after the Wolni Ludzie, within invaders who needed to traverse the mountains creating the phrase “Those mountains eat you”. They died, killed by traps and gunned down by unseen foes. Many invaders were found rotting at the bottom of cliffs or laying half composted by the soil. Those who entered the forests of the Appalachans would be lost in a maze of woodlands and hunted by both man and beast. The Smoky Mountain Force operated as independent cells, hunters who control certain parts of the mountains, who are tasked with partoling it and rigging up traps. Armed with superior firepower than most militias, as due to America’s lackluster gun laws, it wasn’t hard to find a lot of leftover weapons not among the military during the bombardment. Along with this, paranoia was slowly spread by the Mountain Force, utilizing the pre-existing identity of supernatural phenomena among the hills and woods, some cells go as far as to operate mainly at night, lighting fires and stalking those in the woods, slowly but surely driving fear into them. Many Coalition soldiers came to believe the ridge was haunted, aproled by the damned, that monsters prowled the ridges and peeked out from the treeline. Even if the higher ups didn’t believe this for a second, just being in the woods is enough to lower the morale of any soldier there before he bodies even start dropping. Hell is real for the Coalition, and it is called the Appalachia.
United Front Masterpost
#united front#poland#brazil#appalachia#indie game#indie wargame#wargame#wargaming#creative writing#writing#my writing#please reblog#I pray to god I didn’t accidentally play into any stereotypes in this small dump#if I did please tell me so I can rectify it#world building
1 note
·
View note
Text
Planning an Overseas Trip? Visit Travel Medicine Clinic in Melbourne Before Journey
For those who intend to travel to foreign countries, the travel medicine clinic in Melbourne provides necessary vaccinations, health advice, and preventive care. Health risks vary by region and include infectious diseases such as typhoid, hepatitis, and malaria. Medical travel doctors assess the patient's past health recommend the necessary vaccinations and advise on how to stay healthy while travelling overseas, among other things.

When oral supplements are ineffective for treating anaemia or iron deficiency, intravenous iron infusion at a leading iron infusion GP clinic is a very good alternative. Because iron infusion is given by intravenous drip, it enters the bloodstream immediately, has a faster rate of absorption, and rapidly replenishes energy. Some of these symptoms, such as weakness, dizziness, and exhaustion, may significantly improve after therapy. A medical expert continuously monitors the operation to guarantee its efficacy and safety. Those with chronic illnesses who require rapid iron replacement or those with malabsorption issues will find this strategy particularly helpful.
A Variety of General Health Services Provided by Top Health Clinics
As knowledge grows, people's concerns about their skin are growing, and they wish to get rid of the problems. A skin clinic can provide the appropriate medical care to identify skin problems and provide a remedy that doesn't have serious side effects. In order to avoid further health issues, skin lesions must be removed by medical professionals with the necessary training and experience. Melanoma and non-melanoma are the two forms of skin cancer that may be identified and treated at the earliest stage by trained medical professionals.
Pathology services are necessary to analyse blood, urine, and tissue samples in order to diagnose and treat a variety of medical problems. These tests are used to assess general health, track chronic illnesses, and find infections. Physicians may recommend the best course of therapy for their patients when pathology reports are timely and reliable. Modern pathology labs use state-of-the-art equipment to provide accurate and trustworthy diagnosis services. Regular pathology testing is part of preventive healthcare, which aids in both the individual's overall health and the early diagnosis of disease.
For any general health concerns, get in touch with the top clinics, make an appointment right now, and lead a healthy life.
Source
0 notes
Text
¶ … Care of Cancer Cancer has overtaken HIV / AIDS and malaria to top the list of headaches for medical departments and policy makers alike. In 2012, cancer claimed a massive 8.2 million lives, with breast, colorectal, stomach, lung, and liver cancers accounting for more than three-quarters of these. Alcohol and tobacco use, lack of physical activity, low vegetable and fruit intake, and high body mass index have been found to be responsible for a significant 30% of cancer deaths, with tobacco use causing 70% of the 1.59 million global lung cancer deaths reported in 2012. Metastasis, the process occasioned or characterized by unusual growth of abnormal cells, which end up invading adjacent parts, eventually extending to neighboring organs, is the mainspring of death from cancer. The World Health Organization projects that annual cancer cases will hit 22 million by the year 2020, but maintains that mortality can be reduced if cases are diagnosed, and treated early. However, the high levels of ignorance among the public, and the fact that most people consider 'cancer' a taboo subject present significant obstacles to the fight against cancer. It is time we took initiative and fed the public with the right information regarding the causes, development, and complications of cancer, as well as the available treatments, and the undesirable effects of such treatments. Diagnosis and Staging of Cancer Cancer diagnosis begins with a physical examination and a review of the medical history of the individual, especially the history of symptoms. Caregivers will often order an electrolyte- level or a complete blood count, and in some cases, a blood study such as the prostate specific antigen test (NCI, n.d.). Such imaging studies as ultrasounds, MRI scans, CT, and X-rays are key tools used by physicians to detect abnormalities, including cancer, in the body (NCI, n.d.). Alternatively, physicians can use endoscopy tests to visualize cancerous tissues in the bronchi, throat, and intestinal tract (Schrevens et al., 2004). However, for lymph nodes, as well as the inside of bones, whereby proper visualization could be problematic; radionuclide scanning, a test that involves injecting a weak radioactive substance, whose concentration increases when in contact with abnormal tissue could be used (Schrevens et al., 2004). Once abnormalities have been located, the physician extracts and examines the tissue sample obtained from the localized area, in a procedure referred to as a biopsy (Schrevens et al., 2004). If the examined tissues are found to be cancerous, the physician embarks on the staging process to determine the amount of cancer there is in the body, and its exact location (NCI, n.d.). Staging enables a physician to choose the best possible treatment and predict the course that the cancer is likely to take; for instance, breast cancer in the early stages can be treated through radiation and surgery; whereas chemotherapy would be effective for an advanced stage of the same (Schrevens et al., 2004). The TNM system is the most widely-used staging system around the world. In this system, every cancer is allocated a value, which could either be a number or letter describing the metastases, node; where T. stands for tumor, and assesses its extent; N. stands for nodes, and helps in the assessment of cancer's spread to lymph nodes closer by; and M. denotes metastasis, and aids in assessing whether the disease has reached other parts and organs. The T, N, and M. figures range from 1 to 4, with larger numbers indicating a larger, more extensive tumor (NCI, n.d.). T0, N0, and M0 indicate that the cancer has not spread to neighboring lymph nodes, or to other parts of the body (NCI, n.d.). However, not all cancers are staged using the TNM system; spinal cord and brain cancers are staged using their grades and cell types; lymphomas are staged using the Ann Arbor classification; and cervical, uterine, ovarian, and vaginal cancers are staged using FIGO (NCI, n.d.). Complications of Cancer Chemical Changes in the Body: cancer interferes with the normal chemical balance in the body, increasing the risk of serious complications. Confusion, constipation, frequent urination, and excessive thirst are some of the symptoms of chemical imbalances common to cancer patients (Epstein et al., 2012). Problems of the Brain and the Nervous System: cancer exerts undue pressure on the nearby nerves, causing loss of function and visceral, somatic, or neuropathic pain on one side of the body (Epstein et al., 2012). Cancers touching on the brain often cause stroke-like symptoms and headaches ranging from mild to severe (Epstein et al., 2012). Seizures and Difficulty Walking: the body would often react to cancer, like it would in the case of any other disease; however, cancer patients sometimes have unusual immune system reactions referred to as paraneoplastic syndromes, where the body reacts by attacking healthy cells, leading to such symptoms as seizures (Epstein et al., 2012). Metastasis: this refers to the spread of cancerous cells through the lymphatic system, to other organs of the body (NCI, n.d.). This is a dangerous complication, responsible for most of the cancer deaths, because it makes treatment difficult, and reduces an individual's chances of recovering fully (NCI, n.d.). Available Cancer Treatments There are various methods of treating cancer; the method chosen depends on the type of cancer, as well as on the stage of the cancer. Surgery: a procedure of surgery is conducted to isolate, and remove the cancer, especially if it has not spread to other body parts and organs (Kelvin & Tyson, 2010). Surgery offers the greatest chance of cure, because it is only used if the cancer has not spread. Chemotherapy: this is where drugs or medicine are used to treat cancer (Kelvin & Tyson, 2010). Chemotherapy could be administered orally (as a tablet), or through intravenous injections lasting anywhere between several hours, and several days (Kelvin & Tyson, 2010). Radiation Therapy: this is the use of high-energy waves or particles to damage or destroy cancer cells (Kelvin & Tyson, 2010). Targeted Therapy: this is a newer type of cancer treatment regimen that uses drug substances to precisely identify cancer cells, and attack only these, while doing very minimal damage to unaffected cells (Kelvin & Tyson, 2010). Immunotherapy: this kind of treatment makes use of an individual's immune system by either training it to attack cancer cells specifically, or boosting it in a general way (Kelvin & Tyson, 2010). However, this treatment method has been overshadowed by chemotherapy and radiation therapy. Hyperthermia: this method uses heat to attack, and disintegrate cancer cells. Although the idea of making use of heat in cancer treatment is not entirely new, early hyperthermia attempts yielded mixed results. However, more efficient tools have been developed, and hyperthermia is under scrutiny for utilization against various cancer types (Kelvin & Tyson, 2010). Stem Cell Transplants: in this case, bone marrow and peripheral blood transplants are used to clear cancer cells, and replace them with non-cancerous tissues (Kelvin & Tyson, 2010). Side Effects of Cancer Treatment Although they may totally rid a patient off cancer, cancer treatment solutions produce serious side effects, which can have a considerable impact on an individual's quality of life. Radiation therapy, for instance, causes a number of short-time side effects, including skin irritation, throat pain, and hoarseness (Epstein et al., 2012). The long-term effects of the same are even more serious; for instance, radiation could occasion oral cavity damage to the jawbone and the salivary glands, leaving patients with permanent jaw pains and cavities, and "a chronically dry mouth" (Epstein et al., 2012). Chemotherapy too leaves in its wake several undesirable side effects, the most common of which are a weak immune system, nausea, and hair loss (Epstein et al., 2012). Cancer patients naturally experience psychological issues, sadness, and anxiety in response to diagnosis and treatment; and may, in that regard, be at an increased risk of suicide (Epstein et al., 2012). The National Cancer Institute (NCI) reports that cancer patients are 2-10 times more likely to commit suicide than the rest of the population. Methods of Lessening the Side Effects of Cancer Treatment Methods of lessening the undesirable effects of cancer treatment could be behavioral or even clinical. Some of the behavioral elements that a patient can embrace to protect their heath during cancer treatment include eating a healthy, balanced diet; allowing themselves adequate time to rest; and seeking expert advice before using any chemicals, soaps, or lotions on the skin in the treatment area (Redd, Montgomery & DuHamel, 2001). Radio-protective drugs are a clinical method of lessening the side effects of cancer care (Redd, Montgomery & DuHamel, 2001). These drugs are advanced before radiation therapy to protect the normal tissues around the treatment area. Amifostine is the most commonly-used radioactive drug used to protect head and neck cancer patients from the mouth problems caused by radiation treatment (Redd, Montgomery & DuHamel, 2001). Other behavioral techniques that doctors use to lessen the undesirable effects (particularly those that happen to be aversive) of cancer treatment include; i) contingency management -- advancing "rewards to increase the patient's adherence to the treatment regimen" (Redd, Montgomery & DuHamel, 2001, p. 811); ii) cognitive destruction -- blocking the patient's aversive stimuli by engaging them in absorbing and more interesting activities during the treatment procedure; iii) relaxation training - teaching the patient to identify a relaxation state which is scientifically thought to lessen pain during the treatment procedure; and iv) systematic desensitization -- altering a patient's aversive stimuli by "gradually introducing feared stimuli/events in a hierarchical manner, beginning with the least feared stimuli" (Redd, Montgomery & DuHamel, 2001, p. 812). Conclusion Cancer has become not only a serious health concern, but also a leading cause of death across the world. For instance, it is important to note that in 2012, cancer claimed 8.2 million lives. WHO projects that the rising trend will continue over the next decade. There is a lot of misinformation, particularly on the causes and treatment of cancer. This misinformation has been responsible for most deaths as it makes people shy away from early diagnosis, only seeking treatment when cancer has reached advanced levels. Cancer patients face many psychological and physical side effects of care, but there are methods of reducing the extent of the same. Of even more significance is that cancer can be totally cured if it is diagnosed and treated early. References Epstein, J.B., Thariat, J., Bensadoun, R.J., Barasch, A., Murphy, B.A., Kolnick, L., Popplewell, L. & Maghami, E. (2012). Oral Complications of Cancer and Cancer Therapy: from Cancer Treatment to Survivorship. CA Cancer J. Clin, 62(6), 400-422. Kelvin, J.F. & Tyson, L. (2010). 100 Questions and Answers about Cancer Symptoms and Cancer Treatment Side Effects (2nd ed.). Sudbury, MA: Jones and Bartlett Publishers. NCI. (n.d.). Cancer Staging. National Cancer Institute. Retrieved 8 July 2014 from http://www.cancer.gov/cancertopics/factsheet/detection/staging Redd, W.H., Montgomery, G.H. & DuHamel, K.N. (2001). Behavioral Interventions for Cancer Treatment Side Effects. Journal of the National Cancer Institute, 93(11), 810-823. Schrevens, L., Lorent, N., Dooms, C. & Vansteenkiste, J. (2004). The Role of PET Scan in Diagnosis, Staging, and Management of Non-Small Cell Lung Cancer. The Oncologist, 9(6), 633-643. Read the full article
0 notes
Text
Fever Screening Panel Test: A Key Diagnostic Tool for Accurate Results
Fever is one of the most common symptoms associated with infections and various medical conditions. While fever itself is not a disease, it serves as a warning sign indicating an underlying health issue. Identifying the root cause of fever is crucial for effective treatment, and this is where the Fever Screening Panel Test plays a pivotal role. This diagnostic tool helps healthcare professionals pinpoint the exact cause of fever, allowing for timely and accurate medical intervention.
Understanding the Fever Screening Panel Test
A Fever Screening Panel test is a comprehensive diagnostic approach that examines multiple factors contributing to fever. It includes a series of blood and urine tests designed to detect bacterial, viral, parasitic, or fungal infections. The test provides valuable insights into the patient's immune response, organ function, and presence of any inflammatory markers.
Components of a Fever Screening Panel Test
The fever screening panel consists of several essential tests, each targeting specific infections and conditions. These include:
Complete Blood Count (CBC) – Evaluates white blood cell levels, hemoglobin, and platelet count to detect infections and anemia.
Erythrocyte Sedimentation Rate (ESR) – Measures inflammation in the body, indicating bacterial or autoimmune conditions.
C-Reactive Protein (CRP) Test – Identifies inflammation and potential bacterial infections.
Blood Culture – Detects bacterial or fungal infections in the bloodstream.
Malaria Test – Confirms the presence of malarial parasites.
Dengue NS1 Antigen and IgM/IgG Antibodies Test – Diagnoses dengue fever.
Typhoid Test (Widal or Typhidot) – Determines typhoid fever caused by Salmonella bacteria.
Liver and Kidney Function Tests – Assesses organ health affected by infections.
Urine Routine and Culture Test – Identifies urinary tract infections (UTIs).
COVID-19 RT-PCR or Antigen Test – Detects SARS-CoV-2 virus, especially in cases with flu-like symptoms.
Importance of the Fever Screening Panel Test
Accurate Diagnosis – This test eliminates the guesswork in fever diagnosis by identifying the exact cause.
Timely Treatment – Early detection enables prompt medical intervention, reducing complications.
Differentiating Between Infections – Helps distinguish between bacterial, viral, or parasitic infections, ensuring appropriate treatment.
Preventing Unnecessary Medication – Avoids the misuse of antibiotics when the fever is caused by a viral infection.
Monitoring Disease Progression – Physicians can track recovery and make necessary adjustments to treatment plans.
Who Should Take the Fever Screening Panel Test?
This test is highly recommended for individuals who experience:
Persistent fever lasting more than three days.
High fever accompanied by chills, body aches, or fatigue.
Fever with symptoms like rash, nausea, vomiting, or breathing difficulties.
Travel history to regions prone to vector-borne diseases like malaria or dengue.
Weak immune systems or underlying chronic illnesses such as diabetes or hypertension.
How is the Test Conducted?
The fever screening test requires a simple blood and urine sample. The process includes:
Sample Collection – A trained technician collects blood and urine samples in a sterile environment.
Laboratory Analysis – The samples undergo detailed analysis using advanced diagnostic equipment.
Report Generation – The test results are compiled, highlighting the detected infections and abnormalities.
Doctor Consultation – A healthcare professional reviews the results and recommends suitable treatment.
Conclusion
The Fever Screening Panel Test is a crucial diagnostic tool that ensures accurate and timely detection of fever-related illnesses. By identifying the root cause of fever, it aids in effective treatment, prevents complications, and improves patient recovery. If you or a loved one experiences unexplained fever, consulting a healthcare provider for a fever screening panel test can be a life-saving decision. Prioritizing early diagnosis is key to managing infections efficiently and safeguarding overall health.
0 notes
Text
Brucellosis
Case Report
a 45M goat herder in Malaysia develops 3 weeks of fevers, lethargy, night sweats and headache
history revealed he drank unpasteurised milk from said goats, which he also sold to consumers
blood cultures were negative and he tested negative for more common tropical diseases such as malaria, dengue, typhus and lepto
eventually he tested positive for brucella serology, unfortunately about 80 people also developed brucellosis from drinking milk from his farm, and a few lab staff also picked it up from handling their blood samples
consider this differential in PUO

Microbiology
causative organism: Brucella melitensis
gram negative coccobacillus, facultative intracellular
hardy bacteria that can survive prolonged periods in meat/dairy products unless pasteurised/cooked as well as dust & surfaces
picked up in the intestinal submucosa on ingestion and transported by macropahges to lymphoid tissue
it then has the possibility of spreading haematogenously in the liver, spleen, joints etc. causing systemic or localized infection
Transmission
zoonoses (animal associated)
in particular: feral pigs, so hunters are often at increased risk (due to handling the carcasses), but also cattle, sheep, goat and dogs
outbreaks often associated with consumption of unpasteurized milk from infected animals

Epidemiology
global and notifiable disease in most countries
endemic to Mediterraena, South America and the indian subcontinent
in Australia - largely QLD and NT, but now NSW
Increased risk groups (i.e. what to ask on history and what clues on history to consider for brucellosis)
regular contact with animals (herders, abbatoir workers, vets - there are case reports of lab workers who pick up brucellosis etc)
people who ingest unpasteurized dairy/milk, or the undercooked meat of infected animals
History
first described by another European white man, Dr. George Cleghorn, British Army Surgeon in minorca in 1751 on the island of Malta following the Crimean war

it was named for another British white man, Sir David Bruce who led a commission into a fever outbreak among the army in Malta before they found the organism causing the disease (Sir Themistocles Zammit identified that goats transmit it in milk)
Sir bruce also discovered that trypanosoma brucei (also named for him) was the microbe responsible for animal trypanosomiasis/sleeping sickness. incidentally, he was born in Melbourne Australia
trivia with the Crimean war - was ironically a war fought between Russia and the UK + it's Western Allies and the empire that preceded Turkey (Ottoman)
Today the Crimean war is more well known for producing Florence Nightingale, founder of modern nursing and yay, finally a woman in random medical history that hardly is related to brucellosis.
Clinical features
PUO - cyclical fevers, fatigue, headache, insomnia, myalgias/arthralgias, weight loss, anorexia (fairly non specific, but also systemic)
incubation times can be long, which can be deceptive, reportedly up to 50 yrs from first exposure
otherwise, most cases it ranges from 3 days to several week, on average, expect 2-4
sometimes: hepatosplenomegaly
critical on history to clarify travel/living situation or contacts and consumption of unpasteurised dairy or undercooked meat
localized disease also possible, depending on organs involved
up to 40% will report peripheral arthritis, sacroillitis and spondylititis (kinda sounds like ank spa), at worst can cause osteomyelitis and septic arthritis
endocraditis is a rare but serious complication, with a 5% mortality rate, outside of this it's rarely fatal
if the lungs are affected, cough and SOB can occur but hte CXR will be lcear
GBS has been reported to occur following infection
hepatic abscess and granulmoa in a few
also possible: epididymoorchitis and skin manifestations like erythema nodosum
ocular changes like uveitis, cataracts etc.
it really feels rheum flavoured.
Investigations
hints on basic bloods - neutropaenia and anaemia, thromobcytopaenia in the case of hepatosplenomegaly or ITP
raised ESR and CRP, ALP and LDH
elevated LFTs in hepatomegaly
but diagnosis: blood cultures --> can take weeks as slow growing (due to aerosol transmission, must be handled in a biohazard hood as with the case report)
key really: serology is the most commonly used tool
PCR can also be used, including 16S
tissue also an option depending on organ affected
Management:
atypical cover: azith and doxy
several weeks of treatment usually - i.e. if uncomplicated, doxy for 6 weeks (however relapses are common on monotherapy, up to 40%), often rifampicin 600 mg daily for 6/52 is also added or gentamicin
where doxy can't be used, bactrim is the alternative

Sources
CDC guideilnes
WHO guidelines
ETG - behind a paywall, if your institution covers it, uptodate is gold standard, that said, plenty of free resources that provide a great start
Wikipaedia
Statpearls
Case report (There's actually a lot of background pathophysio, investigations and treatment listed in case reports and many are free)
#brucella#brucellosis#crimean war#medblr#infectious diseases#infectious disease#bacteriology#microbiology
8 notes
·
View notes
Text


Are Birds Still Experiencing the Doppler Effect?
The Doppler effect is a change in the frequency of light or sound due to the source of the observer moving. When the observer is moving closer to the origin, the frequency increases symbolized usually as a ripple effect. A ripple effect can be projected as a pattern within water that has increased ramifications beyond the original catalyst of elements. Human interaction introducing an increased amount of pesticides to the United States has caused a frequency disturbance to some colonies of birds beyond the original composition of elements. The pesticide DDT, Dichlorodiphenyltrichloroethane, was invented to kill insects such as mosquitoes, however, DDT was dramatically killing bird populations. Stagnant water is a breeding ground for mosquitoes spawning a parasitic disease fought using DDT. This disease is called malaria.
Malaria, a vector-borne disease, is also described as a protozoan disease that is eukaryotic, a multicellular organism known as parasite plasmodium. The plasmodium parasites infect the human through penetrating the skin from a mosquito proboscis multiplying plasmodium inside each red blood cell. An outpouring effect is caused by the multiplying parasites inside the human body. Malaria. (2024). IntechOpen described symptoms of the disease may include fever, sweating, and chills” that appear 10–15 days after the mosquito bite; in addition, headache and vomiting, among others,” In other words, it is an executing disease leading to death if not treated. Unlike anaphylaxis, the CDC reported that malaria in 2022 hit globally, an estimated 249 million cases, leading to 608,000 malaria deaths that year.
.
Scientists have engineered mosquitoes so that their genes attack the parasite within the mosquito as it grows into an adult. This minimizes the substance of the parasites while keeping fertility persistent for the mosquito. This recent engineering is the best yet seeing how mosquitoes are major pollinators. The most recent malaria vaccine today reported by the (2021) WHO, World Health Organization, is in its second phase trial called the R21. Researchers also published in 2021 that children aged 5-17 months received three shots in eight weeks and a booster 12 months later, the R21 vaccine was 77 percent effective at stopping malaria. This method of controlling malaria is introverted, however, let's look at the extroverted methods of controlling the disease. Such as the spraying of the chemical DDT on residential homes. This pesticide, DDT, is odorless, tasteless, and colorless, maintaining characteristics of a ghost.
America used DDT to control the spread of Malaria abroad during World War II. Evidence from EPA states that in 1970-72, DDT usage in the U.S. over 80 percent was applied to cotton crops, with the other 20 percent being used mainly on peanut and soybean crops. In the midst of mitigating malaria birds were affected in the crossfire. Known to the world in 1940 as the insecticide to combat malaria. Furthermore, the U.S. Fish and Wildlife Service researchers proved that DDT was a reason for the birds thinning eggshells negatively affecting population size in most bird species. The U.S. Fish and Wildlife National refuges states that in 2025 populations of bald eagles are now increasing. Bald Eagles' claim to exist in this modern era is based on the banned pesticide in the U.S. An obliteration of the pesticide took place in 1972 by William D. Ruckelshaus to help the ecological future.
According to the EPA, the Environmental Protection Agency, 1970, began regulatory actions to prohibit DDT's use because of mounting evidence that the pesticide has negative effects on humans. Today, in the year 2025, the insecticide is known by U.S. and international authorities as a probable human carcinogen causing cancer. Puddles of motionless water scattered across the continent while efforts of spraying using DDT still take place in Sub-Saharan Africa.
0 notes
Text














World Heart Day
Heart Day is part of an international campaign to spread awareness about heart disease and stroke prevention. This is the perfect day to quit smoking, get exercising and start eating healthy – all in the name of keeping your ticker in good working order, and improving the health and well being of people the world over.
Learn about World Heart Day
The World Heart Federation have found that heart disease and strokes are the world’s leading cause of death, killing 17.1 million people every year – that’s more than victims of cancer, HIV and AIDS and malaria.
Overeating, lack of exercise, unhealthy diets and high blood pressure, cholesterol and glucose levels are all factors which can trigger heart disease and threaten our own lives, and those of loved ones. Heart Day was set up to drive home the message that heart problems can be prevented.
History of World Heart Day
The aim is to improve health globally by encouraging people to make lifestyle changes and promoting education internationally about ways to be good to your heart. This lesson is becoming increasingly relevant as reports of obesity, poor diet and physical inactivity in children and young people become more and more common.
Events take place to promote healthy hearts. Charities and other organisations coordinate walks and runs, health checks, public talks, shows and exhibitions to name a few of the interesting and informative events which mark the day. So on Heart Day, get involved, eat your fruit and veg and get outside; both you and your heart will feel the benefits.
World Heart Day is celebrated every year. It was created by the World Heart Federation. The first World Heart Day took place back in 2000. Since then, in 2012, leaders from around the globe committed to the reduction of worldwide mortality from non-communicable diseases by 25 percent by 2025.
Did you know that almost half of the NCD deaths happen because of cardiovascular disease? This makes it the biggest killer across the world. Therefore, World Heart Day is the perfect platform for the community to come together in the battle against cardiovascular disease and lower the worldwide disease burden.
How to observe World Heart Day
As World Heart Day is all about drawing people’s attention to heart diseases and illnesses, as well as the range of health issues that are associated with this, it makes sense to raise awareness and also improve your own understanding. We would recommend taking some time to do a bit of research about heart conditions and risk factors. You can then use your online platforms and your social groups in order to raise awareness.
There are both non-governmental and governmental organizations that take part in this date around the world. They do this through the organization of science fairs, exhibitions, fitness sessions, public talks, walks, and marathons. Some famous buildings, monuments, and landmarks opt to go red on this date so that they can show their support for cardiovascular disease awareness.
If you are opting to celebrate this day, it is important to try and be more attentive to your own heart health. There are a number of different ways that you can do this. This includes following a healthy diet, quitting alcohol, stopping smoking, and getting involved in physical exercises. It is also important to have your cholesterol, blood pressure, and heart checked on a regular basis.
It is a good idea to take a look online to see if there are any events that are going on in your local area. If there are not, how about organizing an event yourself? All you need is an idea that is going to get the community involved and raise awareness for heart disease. This could be anything from a fun run to a community fair. It is up to you.
You don’t need to do an event on such a big scale either. You could gather your friends and family members and host a fun event, educating them on the issues and asking them to make a donation. Other ways to fundraise include making crafts and then donating the proceeds to a heart foundation or charity.
There are a lot of different charities and organizations that are doing great work when it comes to raising awareness and finding cures for different heart problems. We are sure that they would appreciate a donation, whether this is a donation of your time, money, or both! After all, anything that you can do can make a difference to someone’s life, so do not underestimate the role that you can play.
Source
#Davie Village#Vancouver#Forever in my Heart by James Cable#Alamosa#Napa#Paradise#Heartfullness Vegas by Katy Boynton#Take Heart by Patricia Vader#World Heart Day#WorldHeartDay#29 September#public art#sculpture#USA#Canada#travel#original photography#Distillery Historic District#Toronto#summer 2015#2019#vacation#cityscape#architecture#Glenn Gould Gathering by Ruth Abernethy#Sacred Heart of Jesus#Trois-Rivières#Hotel Château Gütsch#Luzern#Lucerne
2 notes
·
View notes