#gender dysphoria is a mental condition
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Average visit duration of Tumblr.com is 10 mins and 25 secs.
Text
The facts about Gender Dysphoria
Gender Dysphoria is a mental condition. It isn't a feeling, it's a mental condition. You don't just wake up and say, "I'm the opposite gender just because I wear what that gender wears. HAHAHAHA!"
According to the National Institute of Health or (NIH), Gender dysphoria (GD), according to the Diagnostic and Statistical Manual of Mental Disorders (DSM 5), is defined as a "marked incongruence between their experienced or expressed gender and the one they were assigned at birth."
It is unknown what causes Gender Dysphoria, some say it's assigned at birth, some say it comes from abuse, it is unknown what causes it. Many people go through therapy to get help and others will do a transition to the opposite gender and become a Transsexual, this is the CORRECT historical term and I will use it. This will help them look the opposite gender but they cannot change their DNA. When they die and their bones are dug up, they will still be male or female. Those are the only two genders that exist. You are a man or a woman, nothing else.
While children can experience gender dysphoria, it is recommended that they experience puberty before taking any medication or surgery. To make it simple, let them grow up into an adult.
Children CANNOT be trans, plain and simple.
Kids are stupid. They don't know what they want. A transgender kid is like a vegan cat. We know who is doing it.
Everyone at some point in time experiences being uncomfortable with their body. For girls, it can be big breasts or their periods. For boys, it can develop into muscle dysmorphia, A type of BDD that affects men and is characterized by an obsessive desire to have a more muscular body. Men with muscle dysmorphia may engage in dangerous behaviors to build muscle, such as excessive exercise, strict dieting, and abusing anabolic steroids. Muscle dysmorphia can lead to exercise addiction and eating disorders.
It is recommended that they go through counseling to help with these feelings or just go through puberty. Again, just let them grow up.
Girls can be tom boys without needing to be a boy. Boy can like girl things, dolls, dress-up, etc, without needing to be a girl.
Very often, kids feel a sexual attraction to the same gender and that is confused with Gender Dysphoria. NEVER confuse this with being trans. Kids can be gay, lesbian, or bisexual at a young age but not understand those feelings because they don't see these relationships on TV.
Keep in mind, only 7% of the US population is gay, lesbian, or bisexual. According to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, gender dysphoria prevalence accounts for 0.005–0.014% of the population for biological males and 0.002–0.003% for biological females. It's extremely low and you can't just trust what someone says. There are men who are taking the trans identity and using it to hurt women. You can't just call yourself trans without going through counseling because if you just trust someone's word, then you are going to hurt more people than help them.
The surgery isn't always needed. Not every person with Gender dysphoria grows up into a transexual adult. Any sane transsexual will tell you that. Blaire White, Buck Angel, Sara Higdon are all transsexuals on YouTube I recommend watching and they will tell you that many people regret the surgery because they weren't told the risks that they would have.
Below are videos of detransitioners giving their stories on the truth of transitioning. They are not traitors to the alphabet community, they aren't transphobic, they are people who were tricked by a doctor who cared more about money than the person's safety.
youtube
youtube
youtube
youtube
youtube
youtube
#face the facts#biological facts#gender dysphoria#transsexual#biological sex is real#gender dysphoria is a mental condition#blaire white#buck angel#Children cannot be trans#trans women are trans women#trans men are trans men#You can't argue with the facts#Facts are real#facts are facts#trans#transgender#Youtube
4 notes
·
View notes
Text






By: Christina Buttons
Published: Jun 11, 2024
A groundbreaking new study on insurance data suggests that the majority of German youth do not persist in their transgender identity after five years.
A new long-term study from Germany has found that a clear majority of young people diagnosed with gender identity disorders do not continue to identify as such over time. The study examined insurance data over five years, revealing that more than half of young people aged 5-24 across every age subgroup diagnosed with "gender identity disorder" no longer had the diagnosis after five years. Specifically, the desistance rate was 72.7% in 15- to 19-year-old females and 50.3% in 20- to 24-year-old males. Among the whole group of 5- to 24-year-olds, only about 36.4% of those diagnosed in 2017 still had the diagnosis five years later, indicating that more than 63% desisted.
One of the strengths of this study is its comprehensive collection of outpatient billing data for all legally insured persons in Germany, providing a large and representative sample. Additionally, the long observation period from 2013 to 2022 offers valuable insights into long-term trends and changes in diagnosis rates.
The research also noted a dramatic rise in the number of young people being diagnosed with gender identity disorders. In 2013, there were 22.5 cases per 100,000 insured young people, but by 2022, this had increased to 175.7 cases per 100,000, representing an increase of nearly 681%. The study highlighted that, in almost all years, the highest prevalence of gender identity disorder diagnoses was found in 15- to 19-year-old females. In 2022, this age group had a prevalence rate of 452.6 cases per 100,000.

[ “W 15-19 J.” (females aged 15-19) represents the highest overall rate of increase ]
The study also found that a large majority of those diagnosed with gender identity disorders had other mental health conditions. In 2022, 72.4% of individuals with a gender identity disorder diagnosis had at least one other psychiatric diagnosis. The most common co-occurring mental health issues included depressive disorders (affecting about 57.5% of females and 49.3% of males), anxiety disorders (34% of females and 23.5% of males), and borderline personality disorders (17.6% of females and 12.1% of males). Other frequent conditions were attention deficit/hyperactivity disorder (ADHD) and post-traumatic stress disorder (PTSD).
The researchers highlighted the "fluid" nature of gender identity during childhood and adolescence as a likely reason for the high desistance rates. Citing the U.K.’s Cass Review, the authors suggested the need for a comprehensive, standardized diagnostic procedure for youth experiencing gender-related distress.
The study suggests that many young people might resolve their gender incongruence without needing long-term medical treatment. The authors call for careful consideration when recommending “gender-affirming” treatments for adolescents, given the high likelihood that their “gender identity” may change over time.
This new study aligns with recent findings from a long-term Dutch study, which found that the majority of adolescents expressing a desire to be the opposite sex no longer felt that way in adulthood. This adds to a growing body of research showing that gender dissatisfaction in adolescence is often temporary and declines with age.
--
Study:
#Christina Buttons#gender ideology#gender identity ideology#gender identity#medical corruption#medical scandal#medical malpractice#mental health#mental health issues#comorbidities#comorbid conditions#gender dysphoria#religion is a mental illness
10 notes
·
View notes
Text

@i-reblog-stupid-posts
sorry but your gender dysphoria is NOT cancer and will not actually kill you! also, being gay and choosing to live ‘unhappy and in denial’ is quite akin to what so-called trans people are doing by rejecting and denying their bodies and instead choosing to live in a state of denial and delusion that claims you can actually transition into being a member of the opposite sex just by taking hormones and/or getting invasive cosmetic surgeries instead of just like, you know, accepting your body for how it comes naturally
BREAKING NEWS: you can still have gender dysphoria and just choose not to identify as trans. more at ten.
#the minute y’all stop acting like having gender dysphoria is a death sentence the quicker y’all can get help#for a condition that is likely related to other mental health issues that aren’t ‘I was born in the wrong body’#because I promise that’s probably the last thing that is actually wrong with you#response
232 notes
·
View notes
Text
Gender dysphoria is a mental illness, and like all other mental illnesses the best road to treatment often is long and tiring. Treating HRT & cosmetic surgery as a bandaid for everyone with gender dysphoria is delusional when in any other case a doctor wouldn't suggest spending thousands to massively alter your body as a means to treat your mental condition.
An ethical approach to treatment should be one step at a time, and it should take work, it should take effort, and it will be so much more worth it than permanently changing your body and risking medical complications due to a mental health condition. Some trans people need to transition if no other treatment helps, but I really think therapy would solve most of the new cases of gender dysphoria we see springing up in young adults, teens, or even children. Treatment should be the lowest harm first, progressing to more extreme measures (like transition) once other options have failed, not transition first and then therapy for years after to solve the issues transitioning never really fixed.
#rad fem#radical feminist#radblr#radical feminism#radical feminist community#female oppression#gender critical#female experience#radical feminist safe#radical feminists do touch#gender cult#sex not gender#gender abolition#gender ideology#detransitioner#actually detrans#detrans#transition#detransition#medical malpractice#hrt
668 notes
·
View notes
Note
“Intersex transfem” I bet you have fucking PCOS or some other practically female condition because you are obviously TME
i should not have to justify myself to u ppl but i digress
i was assigned male at birth, had IGM to look more typically male, and was raised as a perisex male until my 5-ARD diagnosis at 18. it took 3 different mental health professionals verifying that my schizophrenia was not the reason for my gender dysphoria to be allowed to start feminizing HRT at 14. i am as transfem as they come. just bcs i disagree w hating transmasculine ppl (and in ur case hating ctf intersex ppl?? lmao?? “practically female” no, intersex is intersex) does not mean i am not transfem. ppl can disagree w u w/o being transmasc so cope ig.
i think ppl w/pcos who identify partially or fully as transfem r super cool btw. intersex liberation forever i do not judge ppl’s relationship w transitioning to femininity based on how far i think their condition places them from biological femaleness. it’s none of my business and it’s none of urs.
4K notes
·
View notes
Text
Feminizing HRT Overview, Guide & Information for All People Seeking It
we also have a version of this post for testosterone/masculinizing HRT as well. we wanted to write a companion piece as many folks have asked about this. it has take a bit of time, but here we are!
The testosterone HRT post is here.
Getting Your Prescription
To start taking estrogen, you will need to find a general practitioner, family doctor, endocrinologist or informed consent clinic where you can discuss gender affirming care with knowledgeable staff. Planned Parenthood is a good option for many trans people in general. Your mental health may also be evaluated, and your heart health and screening for a few other health conditions, as well as having access to your family health history if possible will be required.
Check to see if you have medical insurance, either through your family, your job, or if you are low income, a program like medicaid. Search for low income insurance plans in your area if it is needed, many places offer insurance plans for those who can't afford care on their own.
Here is a map of informed consent HRT clinics in the US.
You will discuss any gender dysphoria, gender presentation needs, if you have a support network, how you are impacted by your gender in your every day life with your provider and so on before being given a prescription. You will only be given a prescription after you discuss the risks of HRT and are screened for possible health problems and diseases or ways your body could react negatively to HRT. If you have needle trauma or phobias and can't inject hormones, it's best to bring it up before you get your prescription to save time and confusion.
The Medications
Treatment typically starts with spironolactone (aldactone), an anti-androgen that blocks androgen receptors ("male" sex hormones) for a few weeks, and then add estrogen, but many folks start with spiro and estrogen at the same time. Spiro will lower the amount of testosterone your body makes. For some people, spiro isn't necessary at all!
Some forms of spironolactone are reported to make folks pee like crazy, others do not have as bad of a time with it. Your mileage will vary depending on manufacturer. Spironolactone is intended to be a blood pressure medication, meaning it is a diuretic and is intended to help your body flush out fluids + salt. You will need to keep yourself hydrated if you notice this effect, as well as increasing electrolyte intake where possible.
Estrogen also lowers how much testosterone your body makes, and triggers changes in the body that occur during puberty in afab & adjacent people. Estrogen can be taken several ways, and is usually taken daily, and several times a day. You can take it in a pill or shot, and several forms of estrogen that can be applied to the skin like creams, gels and patches.
Make sure you thoroughly sanitize the skin of any injection sites or areas you will be applying gel or patches. If you are given topical estrogen, make sure you wash your hands after application and do not have someone else apply it for you. Make sure you do not go swimming or shower within several hours of application to make sure your skin absorbs the hormone.
You may not need to take anti androgens if you are doing estrogen injections, depending on how effective the estrogen injections are for you. Some people may not end up needing anti-androgens at all, and may be able to skip that entirely as spiro has unwanted side effects. Your natural hormone levels will dictate whether or not it's necessary, but it is not necessary for everyone.
You may end up being recommended to switch from one form of estrogen to another as your transition progresses, depending on how your body responds.
It's recommended to not take estrogen as a pill if you have personal/family history of blood clots in a deep vein or in lungs (venous thrombosis).
Some people also end up taking progesterone as well alongside estrogen. Progesterone is typically taken to encourage breast tissue growth, as this is the most prominent effect of the hormone. If sufficient breast tissue growth isn't seen from estrogen alone, progesterone can be added to your regimen, though this is only done later on into treatment, around a year or so in.
If you choose injectable estrogen, make sure to listen to your provider and ask for instructions about how to use needles and syringes, as well as injection angles, how and where you'll be injecting. Do not inject in the exact same spot every time, this can prevent the issue from healing properly and create scar tissue or cause infections or skin tissue necrosis (death). You also need a sharps container to safely dispose of your needle tips. Never re-use a needle, even if it was used previously on yourself. Always ask the pharmacy if you need more needles. A lot of places let you get them in bulk.
If you are going the injection route, make sure you know whether or not you are instructed to do intramuscular or subcutaneous injections. Intramuscular injections usually taper out of the system more quickly and need to be done more frequently, where as many patients find subcutaneous injections less painful and easier as they can be done less frequently.
For more information on safe intramuscular or subcutaneous injection for estrogen, please read here.
Another option for feminizing HRT is to take gonadotropin-releasing hormone (Gn-RH) analogs. They lower the amount of testosterone your body makes and may allow you to take lower doses of estrogen without using Spiro. Gn-RH analogs are usually more expensive, but are an option if for whatever reason the conventional route can't work for you.
DON'T GIVE UP IF YOU DON'T SEE THE EFFECTS YOU WANT TO SEE RIGHT AWAY! Many of them can take a long time to develop, often times patience is the key. If you wait it out and still don't see the results you'd like, you can try another route. Don't give up, a lot of people get deterred in the early stage of transition, you'll get there with patience and communication.
Stay patient, stay positive!
What to Expect from Feminizing HRT
Less facial and body hair growth: typically happens 6 - 12 months after treatment starts. Full effects within ~3 years on average.
Slower scalp hair loss: begins 1 - 3 moths after treatment begins. Full effect between 1 - 2 years on average.
Softer, less oily skin, and changes in general skin texture: 3 - 6 months after treatment starts, full effects within 2 - 3 years on average
Rounder, softer features including face and body, and more body fat: 3 - 6 months after treatment starts, full effects in 2 - 5 years.
Breast development: begins 3 - 6 months after treatment starts, full effects within 2 - 5 years on average or more, according to medical studies, but it can vary wildly from person to person, give dosage and hormones taken. If desired effects are not seen, progesterone can be taken alongside estrogen to help after around one year on estrogen. When breast growth begins, it starts with hard lumps under the nipples along with some soreness and itchiness. Some have sore breasts for a long time, and some may get scared and think they have cancer during this stage. Breasts will be swollen and tender for good while, and nipples may be especially sensitive to even light touch.
Reduced muscle mass/density: 3 - 6 months after treatment starts, full effect in 1 - 2 years on average
Potential decrease in libido if on estrogen alone, though not guaranteed: If it happens, it's generally within 1 - 3 months in and can last a while, but may even out over time
Fewer erections, decreased ejaculate volume, and erections that can become painful or uncomfortable if frequent erections are not maintained. This begins 1 - 3 months after treatment starts, and the full effect is within 3 - 6 months. Regularly maintaining erections and frequent ejaculation can ease some of these uncomfortable feelings in some people.
Changes in how orgasms feel, changes in texture and degree of sensation of penis and scrotum skin as well as changes in body odor: typically begins within 3 - 6 months, though it varies from person to person. Often times the way one's body responds to orgasms completely changes, many people find themselves experiencing full-body orgasms and more intense erogenous zones elsewhere in the body other than the genitals.
Smaller testicles, or testicular atrophy happens within 3 - 6 months and the full effects are usually seen within 2 - 3 years.
Increase in size of bladder and decrease in size of prostate over time which can lead to making one's gspot harder to find, and make prostate examinations more difficult, though they are still vital, as prostate cancer is still a possible factor.
Potential mood fluctuations while adjusting to the hormones, many report increased crying and sadness during the first 3 - 6 months with this tapering off after a full year at most.
Increased fatigue while adjusting to the hormones, sleepiness and becoming easily exhausted are common reports. This can vary drastically from person to person, ymmv.
If you have testicles and choose to have them removed, you may need to take testosterone as well as estrogen in order to have a healthy endocrine system. You will need to discuss the effects of this with your specialists if you want to go this route. If your androgen levels get too low because your body cannot synthesize enough testosterone after bottom surgery, you may need additional medication.
Potential infertility, though this is not a guarantee, and safe sex should still be practiced at all times. No timeline projected though the longer one is on E the more likely it becomes.
Monthly cycles akin to menstrual cycles: these are not present in everyone, but many people report entering a cycle of extreme fatigue, body aches, abdominal cramping in the approximate area where a uterus would sit, headaches, and more for around the duration of a menstrual cycle (4 - 10 days on average).
Progesterone inversely to estrogen can cause an increase in libido in most who take it, and is the primary hormone used for breast growth. Lactation may also occur while taking prog, if this happens, talk to your doctor right away.
Keep track of your progress when and where you are able, and don't be afraid to bring up any concerns you may have with your professionals or trans friends, or any other trans resource. Your transition is in your hands and you're allowed to modify it as you see fit. If you do not see the effects you want from traditional HRT, you may be able to seek the Gn-RH route, and if you aren't seeing the results you want from just estrogen, progesterone might be of use to you.
You will need to keep an eye on your bone health as high levels of estrogens can increase your chance to develop osteoporosis, and potential new cancers like breast cancer may arise, as well as heart problems. Getting checkups as frequently as possible and communicating with your doctor/s will be of great use when and where possible
Either way, we hope this helps in some way! We will add to it as we find/think of more information. Good luck to everyone seeking feminizing HRT, you deserve to look and feel like yourselves!
#transfem#transfeminine#transgender#trans#lgbt#lgbtq#queer#transfemme#trans girl#trans woman#trans women#trans lady#trans girls#trans gal#nonbinary#enby#genderqueer#genderfluid#drag queen#estrogen#progesterone#spironolactone#feminizing hrt#hrt#hormone replacement therapy#estrogen hrt#e hrt#e#our writing#resources
1K notes
·
View notes
Note
Hey, I am a new follower here and uhhh.. I just want to ask you how did you manage to get rid of your gender dysphoria?
I never did transition and probably never will be able to because it is illegal in the country I currently live in. But the gender dysphoria remained there for years (8) even if I accept the fact that I will never be able to change my sex, along with my homosexuality.
So maybe it is a difference in experience, with me not being able to experience the harmful placebo of the "right body", but seeing other people expressing how they got themselves cured of severe mental distress makes me wish I knew how to do that.
So, thats why I want to ask, what lead to the cure of gender dysphoria? If it is a correct way to put it.
I don’t know if you’re male or female, but I assume female?
It’s less about “getting rid” of dysphoria and more about understanding what “gender dysphoria” actually is. That differs from person to person, but for most people it’s a combination of things.
For me it was:
1) The pain of growing up female in a world that either treated me as inferior or objectified me. Plain old misogyny.
2) The pain of growing up gay in a homophobic religion and society. Being basically taught during childhood that I was fundamentally different and wrong did a number on my ability to love myself. I’m 33 and it wasn’t until recently that I had any kind of self love.
3) The confusion of growing up gender non-conforming. Not feeling like I could relate to my female peers, feeling like an outsider, never meeting people like me or having any role models who I could see myself in. I didn’t have any kind of blueprint for what my life could be like as an adult - my only reference points for what life as a masculine lesbian would be were negative.
4) The constant anxiety of walking through the world as a gender non-conforming girl, and the way people treated me and acted around me. People don’t treat you well when you’re androgynous or clearly gay, and that led to anxiety and disliking being around people.
5) Feeling like I would be more lovable as a man, as it relates to relationship dynamics and gender roles. I had a feeling that I “made more sense” as a man.
Once I separated the feelings I was having from the idea of “gender dysphoria” as a stand-alone condition, I was able to see them individually for what they really are.
Those feelings were a normal response to being who I was in the world that I lived in.
Is my “gender dysphoria” cured? Depends how you look at it. Being female is still hard. Being a masculine lesbian is still hard. The way people look at me and treat me is still anxiety inducing. But none of that means I’m “supposed” to be a man, for some mystical reason that no one can scientifically explain. And I can work on improving things like my anxiety and self esteem individually.
To put it simply, being “trans” is the same thing as being butch. It’s all the same feelings women have always had, they’re just medicalizing it now instead of helping us learn to love ourselves. The only way to fix it is to build community, especially intergenerational community, and be with each other and be role models for each other.
Hope that helps! 🌈
#feminism#lesbian#detrans#trans#detransition#butch#radical feminism#radblr#ftm#actual lesbians#writing
63 notes
·
View notes
Text

Men and women have equal rights in a constitutional republic. All the other “genders” represent a mental health crisis and do not equate to equal rights. That man who wants to be a woman has rights as a man and needs counseling. The audacity that society should just affirm his mental health crisis as a non-issue just speaks to how far from sanity our mental health institutions and teachings have become in the US.
We must eradicate Big Pharma’s control over medicine, Congress, food, candy, and tv. Europe is moving away from drugs, chemical castrations, sex organ mutilation, child abuse, and prescribing counseling to everyone impacted by the known, documented, and completely “curable” gender dysphoria condition, but not America. Why? A cured patient is money lost. Yes. Big Pharma needs dough, which means we’re all suckers in their games. With DOGE, there’s potential for change. DOGE won’t just cut spending and defund programs; they’ll be looking for kickbacks and will follow the money.
40 notes
·
View notes
Text
The review even starts from a false premise. “We have no good evidence on the long-term outcomes of interventions to manage gender-related distress,” it proclaims in the introduction. But puberty blockers and cross-sex hormones are better at alleviating distress than Cass claims, not least because she has chosen to exclude the majority of potentially relevant studies from her review. But there is a greater underlying falsehood. Since 2019, the World Health Organisation has recognised that “trans-related and gender diverse identities are not conditions of mental ill-health, and that classifying them as such can cause enormous stigma.” Dr Hilary Cass, while noting this, opts to resurrect the framework of gender dysphoria, treating transition as a worthwhile endeavour only if it alleviates mental health issues. But transition is not a mental health issue – it requires medical assistance, which medical practitioners facilitate (another being pregnancy in people who cannot conceive naturally). There will never be a scientific way of ensuring that a trans boy sitting before a clinical psychologist and asking them to let him take testosterone will not come to regret this decision as an adult, though studies suggest exceptionally low rates of regret among children who do have access to transition. The error is in suggesting that the boy should not access testosterone unless this can be definitively determined. The Cass Review imagines that, with further study, the NHS will finally find the exact combination of sexual orientation, toy preferences in childhood, and pornography consumption habits in adolescence that will reliably predict whether that boy will become a trans man or a cis woman. To this end, Cass obsesses over growing the collection of data. After being ‘thwarted’ in her attempts to force adult gender clinics to hand over patient records, Cass is calling on the government to compel this same violation of patient privacy. Submitting to study will also be a prerequisite to receiving puberty blockers on the NHS.
126 notes
·
View notes
Text
Gender, Dissociation and Clinical Stigma - The Third Person
Before I begin I just want to note that typically Media, Myself and I entries are aimed at depictions of dissociative disorders in popular fiction. Today's entry is a graphic novel memoir by a transgender woman with dissociative identity disorder. As it's both not in the public zeitgeist and good representation by virtue of being lived experience of someone who struggled within the mental healthcare system I want to recommend people buy the book (or check it out of their local library). I fully support the artist and want to prop up something good and beautiful.
With that said, let's begin...

CW: therapy abuse
With all the recent hysteria in the US and UK media over transgender healthcare it can be easy to forget the hurdles we all have to climb to receive care. Though Informed Consent is becoming more of a standard practice these days the DSM-5 Criteria for Gender Dysphoria indicates a 6 month requirement for observation before HRT can be prescribed. Many of us needed to jump the hoops of living 6-12 months "in the gender role that is congruent with their gender identity" before we were allowed to begin our gender journey in earnest.
Of course. This requires a clinician (or two for surgical options) to observe this, monitor it and sign off on it. But therapists are humans and are full of prejudice, bias and their own beliefs. They aren't guaranteed to think it is medically necessary or positive for a person seeking gender affirming care to receive it.
So where does DID fit into this picture?
A study, published in 2015, states clearly that 30% of transgender individuals met the criteria for a dissociative disorder.
Yet even still, The World Professional Association for Transgender Health (WPATH), the gold standard for transgender care included this warning in their Standards of Care up until September 2022.
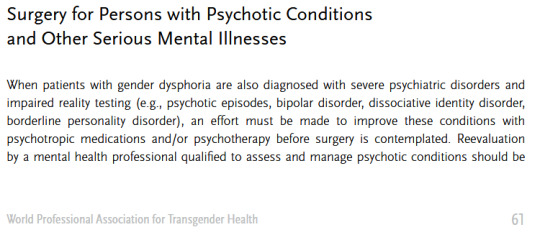
(source)
Fortunately that passage is no longer included in WPATH guidelines as of the 8th revision released in 2022. I shall say the above passage did grant a scare for us, though, as it was very much the practice when we were going for our surgery.
Standards of Care improve and medical understandings of both gender and dissociative care are becoming kinder towards clients.
Even still. There's always that fear. That months of therapy could be wasted on a clinician who was never going to sign off on HRT and was never going to believe our lived experience as a system.
We wouldn't have gotten nearly half as far as we have gotten without our therapist helping us identify our condition, manage our symptoms and develop cooperation and communication.
It's terrifying to think what life would be like if our symptoms not only went unmanaged, but we were made to feel fake and attention seeking by the very person we paid to take care of us...
-
With that intro in mind, The Third Person by Emma Grove is a memoir told in graphic novel format over 920 pages covering the period of life where she began therapy in hopes of receiving feminizing HRT not realizing she had an undiagnosed case of dissociative identity disorder.
When one opens the book they will see an Author's Note declaring that every word in the book is as accurate as Emma's memory will allow and any edits are to streamline the story, not to tailor anything to match the author's point of view and there is a dedication:
"For Katina - We finally did one together"
The story proper begins in media res Winter 2004, as Emma asks her therapist if he would like to hear about the book she was reading and the therapist responds asking why the client decided to speak with him "as Emma" today. Emma, confused, does not understand the question and is probed about her parts, about Ed and Katina and about her childhood. That last word being enough to cause Emma to freeze up, dissociate and...
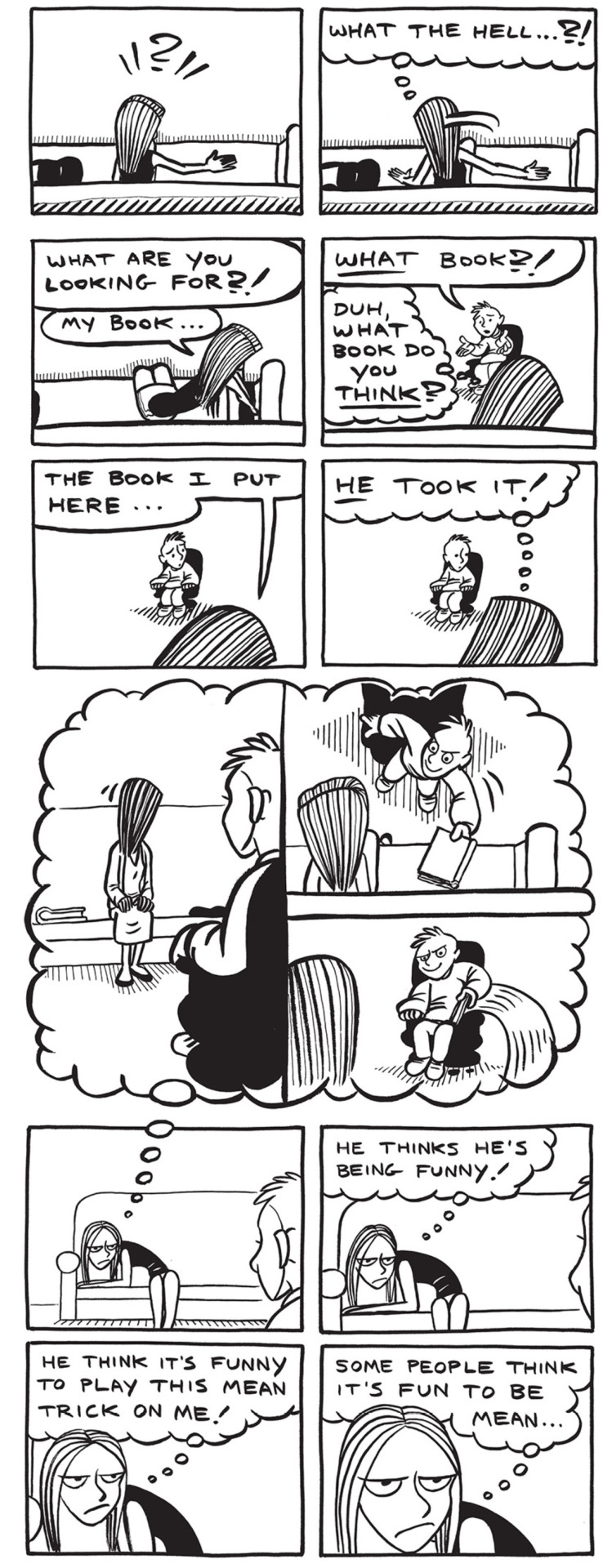
This simple intro gives us all the context a reader needs to understand the antagonistic dynamic between Toby, the therapist, and his patient(s). Both client and patient are unable to understand the other and harbor suspicions about the other's intentions.
Without the context we only know Emma had a book, she no longer has a book and she suspects her therapist of being a mean person who is playing tricks on her.
We will get context later.
The first chapter of the book provides an introduction to the author's late teens and early 20s where they explore their gender identity and have their first experiences with their masked dissociative disorder.
The book goes to lengths to show the stress of the author dividing themselves between having to present male in their public life and sneaking out to bars where they can wear make-up, wigs and outfits to present female.
They take on their legal name, Ed, during their public life and when going out to clubs take the name Katina, from the first bar they visited presenting femme. The name Emma comes later when the system is working to transition into living as a woman in all aspects of their shared life.
The book patiently explores the stress of having to divide ones own self for their safety in spaces where they cannot present their truth without threat from an intolerant society. If 30% of transgender people suffer from dissociative disorders then a much higher number of them know the stress of having to compartmentalize themselves into different presentations for different audiences.
For us, we know that pain all too well. Our birth identity remains with us as a member of our own system. Less a ghost of our past and more a remnant of a mask we constructed to perform the version of self required for our safety.
The artwork does a good job of displaying switches and co-consciousness with subtle expression work, the hair style/wigs that each alter favors. For example we have the left displaying co-consciousness and a switch.


As the years go on, Katina finds ways to go out to the club and exist in her comfort and Ed labors hard to ensure that they can live for the times they get to "become" themselves.
Katina is established to be a fierce personality who will get aggressive when people push against her. She loves to dance and sing and party at the club. She is both a free spirit without inhibition and a fierce protector who will keep the system safe.
I recall feeling a deep fondness and connection towards Katina when we first read the book.
Once the narrative has firmly established the history that lead to the system seeking HRT we are brought into the meat of the book. A white void with a sofa and an armchair. The therapist's office where Katina, Emma and Ed speak with Toby.
Toby is a trans man that Katina believes to be an ally who will sign off on their HRT once the prerequisite 3 month waiting period is over. Unfortunately over the course of those months Toby becomes aware of Emma and Katina's switches and is convinced that it would be unethical for him to sign off on HRT when it is possible that there may be another 'guy part' in there who will 'wake up' one day and decide that he did not want to transition.
To his credit, once Toby suspects a dissociative disorder he does offer Emma a referral to a specialist. They do not take it as they just want to be signed off for HRT and have no interest in exploring their situation beyond transitioning. So they stick with Toby, convinced that another transgender individual will support them.
Toby, however, sticks to his guns and refuses to agree until they manage the DID.

In the opening, sampled above, Emma switches out at the mere mention of her childhood. Here we find that Katina will front any time Emma is made to think about her past and she refuses to allow Toby to force her to think about it or discuss it. She goes as far as to demand Toby promise not to push which, again, Toby refuses.
During this conflict both sides have exaggerated gestures of frustration, many exclamation points and underlined words. This is not a healthy dialogue at all. Toby is refusing to find middle ground or guide the therapy towards its intended destination. He denies all Katina's attempts to negotiate around the need to talk about her childhood (something she is convinced at this point has nothing to do with her stated goal of HRT) and continuously pushes that she needs to talk about it, without elaborating as to why.
Toby, untrained in dissociative disorders, is focused on getting her to open up about her childhood trauma. Katina, uninterested in exploring trauma, wants to be signed off for HRT. Neither side is willing to budge.
This isn't therapy. This is an argument.

Recently I wrote a Tumblr post about the "Hair Dryer Incident"
The Hair Dryer Incident is a story about a patient with OCD whose life was being massively disrupted by the fear that they had left their hair dryer plugged in at home and it would burn their house down. The clinician advised them to take the hair dryer to work with them every day so that they could see the hair dryer with them and not have to drive home to ensure it was safely unplugged.
There was debate in medical circles about whether this was "enabling" because it did nothing to treat the illness, only managed the life disrupting symptom of needing to drive home to check that the dryer was not plugged in.
For Toby in this scenario he believes that allowing Emma to transition would be "enabling" the sickness that he perceives, that being dissociative identity disorder. He has brought his own baggage into the office and only views Emma and Katina as parts of Ed. No amount of Emma and Katina self-advocating in his eyes will change his mind because they are not "real" in his view.
Of course, he is not fully sold on Emma's condition being real either. There is a sequence in which Emma is left alone in the room and she, having a fascination with books, checks out Toby's bookshelf. This causes Toby to become suspicious and decide that Emma has been reading the medical textbooks on dissociative disorders in order to fake an illness and trick him.
This is not a healthy therapeutic alliance and Toby is breaking all 3 key pillars of establishing a strong patient/client partnership.
Much of modern therapy techniques are based on the concept of Therapeutic Alliance. The history of which dates back to Sigmund Freud and the concept of transference but was refined and redefined by Carl Rogers in the modern Patient Centered Therapy (sometimes referred to as Rogerian Therapy).
With that in mind let's examine the 3 key elements of successful PCT(*) and how Toby failed.
Lead with a Patient Centered Approach This means to check all baggage at the door. Cultural biases have no room inside the clinic (during the book Toby openly mocks Emma's faith in God) and that the patient's priorities are the ones that should be focused on. Both client and clinician should be on the same page of what treatment is being sought, what goals are and how they will be achieved. Toby and Emma (or Katina and Ed) never establish this agreement during their time together. Katina/Emma/Ed are firm in their desire to transition and Toby is firm on his refusal to allow this until the DID is addressed.
Set clear goals with a treatment plan. A good treatment plan will have dates, targets and regular review and reward honesty for both/all parties involved in the alliance. Toby is telling Emma and Katina that they need to open up about their childhood but does not explain how this will benefit or what their goals are. Simply "it's good to talk about it" with no direction or assurances.
Regularly review satisfaction with the therapeutic process, relationship, and treatment plan. This element states that it is important that the clinician be upfront with any potential misdiagnosis and discuss any skepticism in the process and lead from a position of patient satisfaction. I do not need to highlight how Toby failed to lead from a position of patient satisfaction here.
Clearly Toby has a personal concept of what the correct approach is and is holding Emma/Katina's gender affirming care hostage until they can satisfy his unspoken objectives. Correctly applied PCT should be a discussion of mutual agreement and achievable goals worked over a period of time. Toby is not applying these principals at all. His modality simply seems to be "talk about it." I'll be an ethical writer who discloses their biases and say I despise PCT/Rogerian therapy. It is, however, the leading modality within western therapy and it is well researched. Not to mention it is the modality Toby appears to be utilizing in the book. I firmly disagree with Freud on all things (except the concept of infant experiences have lifelong ramifications. A broken clock is right twice a day) and disagree with Rogers on the idea that the client has all of the answers and needs to get out of their own way. An issue with this is that DID is a covert disorder and it will do everything it can to stay hidden. PCT does not offer an environment where patients will be able to navigate their condition as unless they are aware of their symptoms, how and when they manifest and are open to discussing those facts they will naturally steer away from circumstances that would lead to a diagnosis. Most people, including myself, have to exist in the mental healthcare system for 5-12 years before being correctly diagnosed with DID(*) and will experience a number of incorrect diagnoses before finding appropriate care. For us it was 9 years and 7 diagnoses. So. Toby's directive is that the system needs to get to the root of the condition and neither Katina nor Emma are willing to open up about their childhood. Katina continues sticking to her guns and refuses but Emma, desperate to start her medical transition, agrees to open up and the two form a shaky alliance where week by week the pair go back and forth between alliance and conflict. In time Emma describes her childhood being raised by her grandfather who was physically abusive towards her. All too quickly Katina's fears are justified by Toby's combative approach to patient care. One session Emma demands to know why she cannot work on her DID while she transitions and Toby states firmly that she is "not transsexual" which triggers Emma to dissociate into a black void that no one can reach her within. She wanted to be seen and regarded as a woman and a trans man told her flat out that he cannot and does not see her as such. Going back to the hair dryer incident as a reference for a moment. Ed is a member of the system and does show up for therapy on some days. At a point Katina, fed up with being denied treatment, makes a plan to quit their job and start a new life living as a woman 24/7. Ed creates a safety net to prevent this from ruining their collective life and continues to work in the meanwhile. Ed's role in the system has been ground down to working and working alone. He spends his days keeping so busy that he cannot dwell, a panel having the thought bubble "I can't slow down! If I slow down I have to think!" which is depressingly relatable to how we were in the worst years of repressing our gender identity. If Ed is unhappy living as a closeted man who has to occupy himself 24/7 to stop from caving in on himself, if Emma and Katina are both completely stunted by their inability to transition; is it ethical to allow them to transition and to work on their condition while allowing them the freedom to live openly as their chosen gender and prevent a circumstance that is harming the entire system? Toby seems to think it is enabling.
30% of the transgender individuals in the study above were observed to meet the criteria for a dissociative disorder. Living a life where one must mask has severe detrimental impacts on a person's psychology. This is true not just for transgender individuals but for those with autism (*) and other individuals on the LGBT spectrum (*) where the cognitive dissonance between who a person values themselves to be versus how they must present to the world causes the mind to dissociate further and allow contrary thinking to exist in individual pockets of a person's life as well as creates an alienation of the self. Healing under these circumstances requires accepting and embracing oneself, not creating a further divide.
After Toby "caught" Emma looking at the bookshelf he became convinced that she was faking her condition. That she had been plucking symptoms from a book and performing them for him. That she fit the criteria "too well"
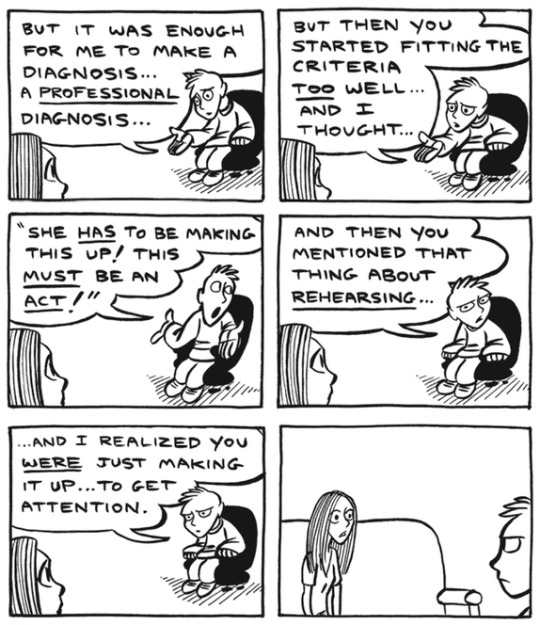
Emma rightfully demands to know why she would complicate her receiving HRT by doing something that prevents her being able to. The pair bicker and Toby cuts off the session abruptly.
in the heat of the moment, assuming that Emma was an attention seeker who does not deserve care, Toby declares "Your grandfather was right to hit you."
Even Emma later admits later that therapy should have ended with Toby right there and then. Hindsight is 20/20, as they say. Alas, a mixture of finances and sunk cost keep Emma returning to the chair week after week.
Being trans and having DID are terrifying. In order to receive care and treatment we must insist to a world that what is happening in our hearts and minds is true in spite of all that the world outside tells us is true. We need to not only reach that conclusion within our own lives but must express that truth loud enough that the people around us see it, regard it and accept it.
As so many things in this world are, it's so hard to earn and so easily burned.
"You're faking it for attention" is such an easy sentence to fling at someone and in a therapeutic setting all things should lead to curiosity. Even if a person were faking, it's not normal and healthy behavior for someone to do that. Toby is displaying a complete lack of curiosity and compassion. He is framing himself as the victim in a potential deception from someone who is paying what little money they can put together to receive his care.
I hate Toby.
As the story continues, Emma and her system begrudgingly continue, flitting back and forth between a healthy and unhealthy dynamic with their therapist that shares a lot of similarities to abuse honeymoons. It is worth noting that as the book is a memior it will inevitably be painted with the author's personal view of past events because, as discussed in the Umineko article on recontextualized memories, a human mind cannot avoid applying present understandings to past experiences when recalling memory. This is seen in the book when we see things that Emma cannot possibly have witnessed, such as Toby's facial expression after she leaves the office.

This is not to throw shade at how Emma depicts her former therapist, as he was quite horrid to all 3 of them and quite obviously did more harm than good during their time together. I just wish to note that skewed perspectives are an inevitability. Even still. They do make some progress in talking about the situations. We come to learn of the system origins and how Katina was a friend to the young and lonely child they used to be and that their abusive childhood was centered around physical abuse from their grandfather. While discussing this Emma notes that she could make Katina go away forever with a single phrase. A few short words that she can never ever say and mean or Katina would go away and never come back... and I think that's where I'll stop with the synopsis. I (specifically me, Dawn) broke down in tears the first time I read the book and I have no will to put myself through that again at this exact moment and I wish for you all to have the catharsis of experiencing it for yourself.
I will say in way of positivity that the story is quick to make its conclusions in the final chapters by displaying therapy done right and the fact that even if parts can no longer be heard or even felt, they will always endure in moments where they can add a little color to the world.
They got to write this book together, after all.
For all the sadness this memoir elicits it speaks an honest and hard truth of the desperation, isolation and confusion that can be found in managing sentiments of identity and gender in a time when there was so little understanding and acceptance, particularly for transgender people.
We are lucky these days to have the internet as it is where we can create community and find our people and in finding our people have a better understanding of who we are and how we can live our truths. Visibility of transgender and plural populations has been increasing in part due to the fact we are able to feel unalone and forge community.
2004 did not have those luxuries and I am saddened that Emma Grove had to live through that stigma and lost so much time to unethical and prejudice care from a clinician.
I do hope that in the future we can continue accepting and encouraging one another and living lives where we are not forced to hide, mask or pretend.
-
For other Media, Myself and I articles, please check out the following:
#dawn posting#media myself and i#media essays#plurality#did#watch me post my trauma in public#this is my gender and I am proud of it
83 notes
·
View notes
Text
my suffering is profound and legitimate, yours is frivolous nonsense
Just reading a blogger I like but I had to laugh because she was talking about how beauty practices are bad for women's mental health, and she left a note saying "unlike gender affirming care! gender affirming care improves people's mental health and it's nothing at all like cosmetic practices."
TIL, when an older woman gets botox to remove her wrinkles and avoid facing the inevitability of decline and death, her problem is spiritual/structural and she needs to Do The Work to deprogram her ageism, unlike people with dysphoria, who of course have legitimate claims to cosmetic alteration.
And it is cosmetic - no part of the body that is altered by HRT or SRS or any of the feminization/masculinization surgeries is failing to function or functioning poorly. The problem is with the brain, which perceives the body parts as foreign or undesirable. We may sympathize with someone struggling with such a condition, but that does not change that the body parts being altered were already healthy and the alterations are cosmetic, and the relief being brought about is mental.
But plenty of trans people openly admit that separating body dysmorphia and gender dysphoria is a losing game. Contrapoints's video on "Beauty" (transcript) has the observation that she feels least dysphoric when she is meeting feminine beauty norms:
But I also think that trans people often talk like gender dysphoria is this intrinsic, personal experience that's always 100% valid and never has anything at all to do with the external pressure of beauty standards. But in fact, gender dysphoria is not sealed away in a vacuum away from the influence of societal ideals and norms. [...] When I try to psychoanalyze myself, I find that my desires to look female, to look feminine, and to look beautiful are not exactly the same, but they're woven together so tightly that it's kind of difficult to untangle them. And the opposite is also true, that for me feeling mannish or dysphoric usually goes along with feeling ugly. I don't have a lot of days where I walk out the house thinking "well, I'm giving femme queen realness, but apart from that I look like absolute shit".
Max Robinson's book "Detransition," from an FTM perspective, points out how the prospective trans man views his suffering as unique from and distinct from women's, even as the surgeries they seek are not especially different:
The stereotypical cosmetic surgery patient is seeking to become closer to being perfectly feminine - she wants to be beautiful. Transitional cosmetic surgery, on the other hand, is widely understood to mark the patient as ex-female and therefore unfemale; this is part of the meaning FTMs seek to create through surgery. FTM desire for cosmetic surgery is positioned as something totally different than the stereotype of a woman who 'merely' seeks beauty at her frivolous leisure. FTMs are deemed to have a rare affliction that needs urgent, life-saving treatment. Conversely, there is nothing more common than for a woman to become obsessed with her socially-deemed 'unsatisfactory' looks and desperately seek to change them, believing that such a change is the only thing that can restore her quality of life. This comparison will feel like an insult to the FTM. It will feel that way because we believe other women's suffering doesn't matter, and recognize how much ours does. Women's suffering is ordinary but ours is extraordinary. For us to matter, we must be differentiated from the silly little woman who wants to be pretty so badly she'll pay thousands of dollars (now billable to credit cards and loan programs designed to pay for elective surgeries!) to risk her life and health. These women don't need to be fixed; we do. FTMs know that we don't deserve a woman's fate but have not yet realized that no woman does.
I have more to write on the topic of the relationship between gender identity and beauty culture, but I'll end this one here. It makes sense that somebody who is identified with the opposite sex would also be affected by the standards of beauty expected of that sex. (Non-binary identification is more complicated and requires separate treatment.)
193 notes
·
View notes
Note
so how do you feel now that the prophet is saying transgenderism is false and not to be tolerated at church? you need to deal with REAL genders, not made up ones
Let me address your idea about real and false genders.
Let's talk about money. There is nothing about paper money that inherently gives it value other than we all agree that it has value. We assign value to the paper and that makes it a social construct. Yes, it's made up, but it's also real. Money has real value in our world and has real impacts on our lives.
Language is another example of a social construct. We agree that certain sounds mean certain things and voila, we now have a language. Nothing in the sounds innately means "lion" or "paper" or "moon," which is why we spend many years teaching language to children. Language is made up but it's also real.
Gender is similar. What it means to be a man or a woman, all the traits and qualities we as a society assign as masculine or feminine, that's a social construct. Gender is real in that we agree to it, it has real world consequences. Entire systems of privilege and oppression have been built around the concept of gender. Same is true for race, ethnicity, beauty standards, social class, and so on.
Just as the value and meaning of money can change, like how we can use credit cards or crypto, and language evolves and changes (try reading Shakespeare or the original King James Bible and see how well you understand English from the past), our concept of what gender is can change, and we can change the systems build around gender. We can dismantle patriarchy, misogyny and sexism.
By telling people they were assigned a gender and can't stray from it no matter if it doesn't work for them, that they must adhere to all the rules about a gender they didn't choose and which has negative consequences for them, that's a problem. Transitioning reduces gender dysphoria and related conditions, like anxiety and depression. Studies show long-term mental health benefits and a higher quality of life for trans people who transition. The benefits of gender-affirming health care for everyone, not just trans people, is tremendous.
The dramatic improvement in health and quality of life is why every major medical association supports gender-affirming care for transgender and nonbinary people, to not do so would be irresponsible because of the harm caused by restricting such care.
One of the brilliant beliefs of the Church of Jesus Christ of Latter-day Saints is that the gospel of Jesus Christ embraces all truth. Another wonderful teaching is that we can tell whether something is good or bad by the fruit it produces. Another feature of this church is having prophets and apostles who can make changes. It's hard to change but the fruit of the church's policies about queer people is evident and the truth being provided by science about queer people needs to be embraced.
46 notes
·
View notes
Text
like transmedicalism is not a fringe position held by a small contingent of annoying trans men on tumblr, it is the internationally agreed upon definition of trans identity (and I’m invoking ‘international’ as an intentionally loaded term that prioritises western-based consensus that is then imposed globally). Dysphoria is a mental illness in the DSM-5 and gender incongruence is defined as a sexual-health related condition in the International Classification of Diseases and Related Health Problems (ICD-11) put out by the World Health Organization. Transmedicalism, which is the view of transgender identity as an inescapable, irreversible disorder originating in the long-term psychiatric condition of gender dysphoria that has to be treated with medical and social interventions from doctors and psychiatrists, is very much the norm.
There’s obviously been some important recent shifts in the western world away from defining trans identity as strictly pathological (you can see as much in the links I provided - they frame diagnosis mainly as a helpful tool for trans people to access care, downplay the pathological elements to it, and acknowledge that dysphoria isn’t a mental illness, but rather a condition that causes discomfort and social stigma - which is a massive cop-out in my opinion and fails to refute the underlying logic of pathologising trans identity, but that’s another discussion), but psychiatric diagnoses still hold immense importance in determining access to trans medical and social care in many countries across the globe. Being some strain of transmedicalist is the default position of most trans allies - whether that’s pointing to psychiatric science that ‘proves’ trans people are real, referring to trans people as being unable to help who they are, trapped in the wrong body, etc - it is how doctors generally situate trans patients in their care, and it is a substantial part of the discussion of trans care in WPATH’s Standards of Care (SOC-8) document (which again, tries to move away from overly pathologising trans people but still acknowledges that it is the norm in many countries). Being a transmed is not an abstract discourse position, it’s the international definition of trans identity
173 notes
·
View notes
Note
some thoughts:
i think radical feminism is antithetical to transgender ideology. i think we should still treat trans people as people and not be disgusting towards them, but trans ideology is still inherently misogynistic and patriarchal. so i don’t understand “trans inclusive radical feminism”… what are we including? people who believe sex based oppression isn’t real? people who believe in “trans misogyny��? people who “identify” with gender roles that have oppressed women for centuries? people who medicalise gender nonconformity? people who believe homosexuality is bigoted?
these ideologies don’t belong in radical feminism simply because they are anti feminist. so therefore radical feminism is inherently trans exclusionary and i refuse to believe that’s a bad thing.
obviously detrans women and women experiencing sex or gender dysphoria who aren’t trans aren’t included as trans ideologists i’m talking about.
there is so much misinformation and stigma surrounding transness on radblr, and just lack of information. it can be confusing being on the outside looking in! as a detrans woman who's often assumed to be firmly against transition, instead of how i'm highly critical of it and want safety measures within the community to be put in place to prevent detransitions and unhealthy transitions and misplaced identification... i think it's very easy to forget that dysphoria is a mental disorder and trans rights are a mix of gnc rights and disability activism / mental health advocacy. and as most of us know, radblr has a HUGE problem with rampant ableist ignorance.
the trans community is split in two, with some sharing both sides.
there's the dysphoric side, where there needs to be discussions on how to manage a complex disorder and not shame people for trying out different healing treatments. i want to erase the stigma of people with disorders, dysphoria included, choosing treatments that at times carry risks. this can be pain medication with potential addiction, or transition treatments or psych meds that potentially come with side effects and just might not help you in the end. i also hate how neurodivergent/mh communities can turn toxic fast, but i still am glad people can share their experiences with others, find people's stories in battling a disorder and gain more mental stability. this includes dysphoric people for me. as a physically and mentally disabled woman, my dysphoric trans activism is also my disability activism. and my detrans side gives me a complex perspective, because for me, it turned out to be the wrong treatment. some people are anti-psych because meds fucked them up instead of helping them. i am psych critical, because meds saved my life.
i am all for them exploring their treatment options, physical transition included, as long as they're educated on the risks and prepared for potential reverse dysphoria. the tra community handles that in a SUPER inappropriate, unhealthy, and honestly dangerous way and they're shooting themselves in the foot bc they don't push for better healthcare, leading to more detransitioners, leading to more trans stigma.
now on the other side, the term trans (and nonbinary, since not all nonbinary ppl identify as trans) for some can simply be a label to find likeminded gnc people, enjoy a punk-adjacent subculture focused on breaking gender roles and pissing off the patriarchy, and simply enjoying crossdressing and using terms that makes them happy.
dysphoric people still exist, and dysphoria is debilitating. it's a complex issue. for some, dysphoria is more neurodivergent, and it just is stubbornly staying and so they look for more intensive treatments. for others, it's more like a mental illness, and the condition can be treatable and may come from gender roles. and even if a specific person had a root cause for their dysphoria that relates to the patriarchy, i still wouldn't judge them for transitioning if it seems like it's just not going away no matter how hard they try. just like how i'm wary of people going on hardcore, addictive pain meds, or try treatments that come with risks for their physical health, but i know it helps many people and i don't want the option off the table. they are suffering. i care deeply. i fucking hate reverse dysphoria, but i hate ableism even more. i hate the stigma of disorders and the shaming of mentally ill & neurodivergent people, people with mental disorders, including dysphoria as is listed in the DSM.
i know the trans community is confusing. frustrating. often immature. people who are mentally suffering are often not in the right mind to do realistic, down-to-earth activism, but god knows they try and like in neurodivergent activism spaces it can get unhinged in a unique kinda way. we can call out their sexism, their homophobia, their misogyny, without resorting to ableism and transphobia - aka, what imo is a mix of ableism and gncphobia.
dysphoric people deserve healthcare reform. tras keep fucking things up for homosexuals and female/afab people and just make fools of themselves. radfems, esp non-detrans bio women, are often out of touch when it comes to trans issues.
it's easy to resort to extremist views on these things. it can be easier to embrace black-and-white thinking. but it's not the way, trust me! there are grey areas. we need reform, not the destruction of transness being a concept at all, whether it be the gnc subculture or the dysphoric side of it. there are a fuckton of trans issues to tackle. it's okay to be frustrated, to feel hurt, to be worried, to think maybe transness shouldn't be recognized as anything and those people should just be poked out of it somehow. but you can't just force someone's brain to be neurotypical, or cis/non-trans, or take away labels that feel meaningful to some folks even if you find them silly. it's counterproductive. the trans community has a lot of flaws, but it's a puzzle that can be figured out! please hear out trans radfem & nuancefem voices on this as well <3
-mod pikachu ⚡
25 notes
·
View notes
Text
TRANSABLEISM.

What is transableism ?
Transableism is characterized by the desire for a non-disabled individual to acquire a specific disability such as the loss of a sense or a limb (amputation, paralysis, blindness, deafness, etc.), thus placing them in a situation of disability.
The opposite of transabled is cisabled wich describes a person who does have that disability bodily.
Transableism is a new thing ?
No, ''transabled'' is a sociological and political term coined by Sean O'connor in 2004 in attempts to demedicalize disability desires and views them as healthy person's challenge to the stigma of disability as created by social norms. Researchers and transabled people use a variety of terms to describe it. some people refer to "apotemnophilia" a term that have been used the first time in a 1977 article by psychologists Gregg Furth and John Money. We do not recomand this term.
Then, In 2004 Michael First published the first clinical research in which he surveyed fifty-two people with the condition, a quarter of whom had undergone an amputation. Based on that work, First coined the term "body integrity identity disorder" (BIID) to express what he saw as more of an identity disorder than a paraphilia.
The newest term, ''xenomelia'' was established to acknowledge the neurologic component of the condition after neuroimaging studies showed structural changes to the right parietal lobe in individuals who desired amputation of their left lower limb, thus linking the part of the brain that processes sensory input from the affected limb. (McGeoch and others 2011).
Friendly reminder that a transabled person do not necessary experience body integrity identity dysphoria (BIID). People with BIID (dysphorics transableds) experience a suffering with a part of their body, such as a limb, and feel that removing or disabling that part of their body will relieve the discomfort. People with the condition may have intense feelings of envy toward amputees. They may pretend to be an amputee, both publicly and privately. Patients who experience the above symptoms consider them strange and abnormal.
Confusions.
Body dysmorphic disorder is sometimes confounded with disability desires. The two conditions may share a preoccupation with a specific part of one's body, but body dysmorphic disorder is typically concerned with the visual aspects of that part, which is never the case in disability desires. Also, the concerns in body dysmorphic disorders usually focus on facial parts, not on major limbs or sense.
WHY ?
A study conducted by Michael B. First on 52 aspiring or volunteer amputees shows that the main reason given is to regain their true identity, to correct an anatomical anomaly. It is difficult to establish precisely why this need manifests itself in transabled people, even if there are neurological and biological leads. The only difference between a transabled person and a transgender person would be the level of social acceptance of each phenomenon. As transgender people, the transition to the desired body in transabled people is associated with greater general well-being, and a significative decrease in suicidal and depressive thoughts.
It's a choice ?
No, feel the desire to acquire a physical deficit isn't a choice but start a process in order to acquire a disability is a choice. Just as for trans people, they do not choose to be trans but they choose (often the pressure of gender dysphoria) to transition.
When someone realize they are transabled ?
The disabled- desires comes very early in their life. Their first experiecs of such desires are felt in their childhood, around the age of 7 this study found.
Psychological therapy, psychopharmacological drugs and relaxation techniques had little effect and sometimes increased desire. They can reduces symptoms like depression, but not disability desires per se.
This study shows that the amputation of the healthy body part appears to result in remission of BIID and an impressive improvement of quality of life. 100% of transabled who had recived a surgical amputation confirm that it was helpful. With medication 73% pretended that this treatement for BIID was unhelpful and 60% confirm that therapy was unhelpful. Betweet those who recieved and didn't recieve an ambutation, those who didn't recievent it said that BIID had an extreme negative impact in their personal happinnes (17,2 in the Y-BOCS scale) in comparison, those who recieve an amputation affirmate that BIID had a extreme low effect in their personal life (3,2 on the Y-BOCS scale).
Psychotherapy was often supportive, but did not help diminishing BIID symptoms.
Those who didn't recieve an ambutation confirmate that BIID had severely disrupt their work counter a very neglectical effect (3,2 ON Y-BOCS scale) for those who recieve an amputation.
Several others studies: (1) (2) (3) shows that all transabled people who have successfully made the transition say they are very satisfied and happy.
In all cases quality of life was rated to be substantially increased, and no new disability desire emerged post-surgery. There is considerable support for the view that elective amputations can be ethically justified , even if long-term effects of the intervention still need to be assesse
Dangers for not letting a person acquire the desired handicap.
Amputations seem to be the only effective solution. Denying these people the only treatment that can cure their dysphoria will only prolong their suffering and many trans-capacitated individuals will therefore opt for dangerous solutions, such as turning to the black market, attempting to perform their own surgery, or injuring themselves severely enough that a doctor has no choice but to proceed with the amputation of an unwanted limb. It's like denying to a dysphoric transgender person the right to transition.
Why is not different from transgender people ?
Like transgender people, transabled people feel an internal identity that they seek to match with their body. The only difference between the two is the level of social acceptance, unlike transgender people, transabled people in addition to being even more stigmatized and marginalized by the ableist and cisableist society than transgender people, do not benefit from surgical intervention allowing them to obtain the desired body.
Anti-choice arguments.
Anti-choice authors in relation to transbled- surgical operations argue that these people are not autonomous, 'irrational', alienated by their conditionality and cannot make an informed choice. Elliott (2009, p. 159) summarizes the authors' position well (without adhering to it): "These objections focus on the nature of the 'wannabe's' belief that they should have a limb amputated, suggesting that because it is bizarre, irrational, and obsessive, they are unable to properly 'weigh' the information relevant to the decision, that these desires are not autonomous, and are not to be respected or followed. On the one hand, in light of previous data, this position is not scientifically supported and is based on prejudice and impression. Authors who support transabled-surgery argue that refusing it would be violating the first ethical principle of autonomy; if these people are rational and do not make their decision under coercion, their autonomy must be respected. On the other hand, this question of autonomy and rational choice rests on double standards. The very requirement of an explanation and a rational to justify this need obscures the fact that for many very important decisions in our lives, these explanations rationality are not required; for example, playing dangerous sports, having children, going on a humanitarian mission to a war-torn country, or simply choosing to live are not subject to the same questioning and the same requirement of rationality. As Gheen (2009, p. 99) argues, most of the choices we make do not have "rationality" and cannot be explained; we have needs and desires, we realize them, and no one demands evidence of rationality from these actions that sometimes have considerable impacts on our lives and the lives of others. Gheen argues that if this need of the transabled is considered irrational and illegitimate, it is because it goes outside the dominant norms.
Important barriers.
In addition to society's ableism and cisableism, the Hippocratic Oath, by which physicians pledge to "do no harm" to their patients, is the main barrier between a transabled person and his or her disability; practitioners cannot help individuals acquire an impairment that is presumed to have a "detrimental" effect on their lives (Johnston and Elliot, 2002). But an ethical question arises and a paradox emerges. Should we leave transabled dysphoric people in a state of severe suffering, causing them depressive symptoms and even suicidal ideas with the belief that amputation will have a "negative" impact on their lives, when we know that this is not true as datas we have seen previously, rather than allowing them to acquire the desired disability thus allowing their body dyphoria to remit and increasing their general well-being? If doctors commit themselves not to harm their patients isn't it paradoxical to refuse the only possible treatment, i.e. the medical acquisition of a handicap via a surgical intervention to someone, keeping them consequently in a state harmful to his mental health? In other words, the doctor refusing health care to someone who needs it is the equivalent of a health care professional refusing to allow a dysphoric transgender person to undergo a medical transition: it is bad from a moral point of view as well as from the point of view of the person's mental health and exposes them to the risk that she voluntarily injures themself or that they performs their own surgery with all the potential dangers on their life and their health that such a decision implies and opposes the fundamental freedom hard won by social movements to do what we want with our body.

Pt: If you dont like us, just block! Feel free to ask for more information about the label.

Pt: DNI: Truscum, heavy religius, dahlia/winter, antiradqueer, anti transids, anti paras, anti muds, anti mspec, anti endos, anti profic, hypoharmful, non-good faith, anti cosang, anti therian, otherkin (etc), terfs, anti xenogenders or xenoids, pro-harrasment of any type, anti kink, anti agere/petre.
#radqueer#pro rq 🌈🍓#radqueer 🌈🍓#rq 🌈🍓#rqc🌈🍓#🌈🍓 safe#🌈🍓 coining#🌈🍓 please interact#pro transid#transid#transid defender#transid please interact#transid safe
43 notes
·
View notes
Note
it is so insane to say that doctors shouldn’t practice gender reassignment surgeries, or that hrt shouldn’t be accessible, and not for transgender activism reasons either (though ignoring the enormous number of people that are happy with their transition is just willful ignorance). where do you draw the line on what adults can do with their bodies? do you ban all plastic surgeries? do you ban all the surgeries that require removing “healthy” body parts? Do you have any idea the amount of autonomy that strips cis women of? What about breast reductions? Oh, they can be removed because the woman’s back hurt? What is the level of hurt required, how do you decide which women’s backs are hurting enough and which aren’t? What about cis women who desire hysterectomies for a variety of reasons? how is removing my breast different from say, getting breast implants. do we ban breast implants, and then where do you draw the line? it’s such a non-nuanced way to see things.
“all plastic surgeries should be banned!” what if somebody gets into a car accident and doctors have to reconstruct their face. Probably they can live without it, but are you saying they should? What if somebody breaks a nose, should the doctor do the absolute bare minimum to fix it instead of trying to give it the aspect it had before? What if a woman requires a mastectomy for medical reasons, and lately wants breast implants, should it be illegal for her to get those? besides, what is the level of illness required to perform a surgery that is outlawed? Do you think having to fight the law as well during something like breast cancer or similar would be of benefit to women? worth it if it means transgender people can’t get it either?
and don’t even get me started on hrt, because if you can’t prescribe those meds for a certain mental condition, what is the difference with any other medicine, especially psychomeds? That it has collateral effects? Guess what? Most of them do! That it shows on the body? What is the actual difference, that you can make a law out of, without any overlapping, between something working on your hormones to show a change in your physical appearance and something working on your hormones to show a change in your brain activity? What if a med that’s needed to cure whatever illness has certain effects on the body? I swear you people do not think.
I’ve thought about all of these things, over the 12 years I spent in the trans community and the 10 years I spent on hormones. I still came to the conclusion I did. Actually, going through it myself is what brought me to this belief and cemented my opinion.
HRT and gender surgeries are different from necessary medical treatments and procedures because they aren’t medically necessary. They are medically harmful across the board in every case, to varying degrees. Female bodies are not meant to have high levels of testosterone. It causes health problems. Same for males.
So in order to defend using HRT, they have to prove that the benefit outweighs the harm. How do they attempt to do that? By claiming that everyone will commit if they can’t transition.
And what basis do they have for that belief? Nothing scientific. The only way they could get that data is through a study that gives half the participants HRT and doesn’t give it to the other half, and compares how many people commit.
So right now, they’re just going on the assumption that transitioning helps our mental health better than any alternative mental healthcare treatment option would be able to. (And better than just leaving us alone.)
This is when most people bring up how trying to treat dysphoria in another way would be “conversion therapy”. Because they apparently aren’t aware that there’s a huge difference between using electric shock to try to change people’s sexuality, and using exploratory talk therapy to help dysphoric people work through the issues that caused them dysphoria in the first place.
Proper mental healthcare, medical education, feminist education, and teaching dysphoric people to connect with their body has the ability to get rid of their dysphoria. It worked for me and many others I’ve talked to who have detransitioned or desisted. And sometimes all it takes is just growing up for us to understand ourselves better and accept our bodies. But of course, that idea threatens the entire foundation of the trans movement, so it can’t be true. Right?
In my mind, it’s fucking dystopian that we have all these kids now who never even got the chance to grow up before having these decisions made for them. Being fed the idea that they’re trans, and the only way for them to be happy is to make drastic medical changes to their body, has a devastating affect on their mental health and leads them to medicalization they otherwise may not have needed.
As for elective procedures, yes I also oppose those. I think any surgeon who gives someone a potentially dangerous procedure, or a procedure with a high regret rate, should lose their license to practice.
It’s not “oppressive” to women to say I don’t agree with them getting cosmetic surgeries or electively getting their important reproductive organs removed. That’s fucking ridiculous, to call that “oppression”. The fact that women think they need these cosmetic surgeries is the real oppression.
Anything with a legitimate medical reason, breast reduction, or simple procedures to prevent pregnancy are exceptions to the rule because they legitimately improve quality of life.
I hope that helped you be able to follow my train of thought about all this, and understand better what I’m saying.
#feminism#lesbian#detrans#butch#detransition#trans#radical feminism#radblr#ftm#actual lesbians#wlw#transgender#mtf#lgbtqia#lgbt
85 notes
·
View notes