#exogenous testosterone
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Forty percent of Tumblr users are between the ages of 18 to 25.
Text
By: Michael Searles
Published: May 26, 2024
Transgender men are suffering from “postmenopausal” problems like incontinence in their 20s because of taking testosterone, a study has revealed.
Experts analysed 68 transgender men who were taking the cross-sex hormone to change their identity from female to male and found that 95 per cent had developed pelvic floor dysfunction.
The participants, who were as young as 18 and had an average age of 28, had bladder and bowel symptoms that medics would expect to see in a woman after the menopause.
Experts said the impact of the sex-changing drugs on bodily functions are under-researched and under-reported, with people “not being informed of the risks at gender clinics”.
Around 87 per cent of the participants had urinary symptoms such as incontinence, frequent toilet visits and bed-wetting, while 74 per cent had bowel issues including constipation or being unable to hold stools or wind in. Some 53 per cent suffered from sexual dysfunction.
The researchers said the rate of urinary incontinence, where urine unintentionally leaks, was around three times higher in transgender men than women, affecting around one in four compared to eight per cent of the general female population.
Other trans men suffered from frequent urinating including during the night, burning sensations, hesitancy, urgency and difficulty in going, while others had issues defecating.
Almost half had an “orgasm disorder”, while a quarter suffered from pain during sexual intercourse.
Experts warned that the drugs were putting young people on “exactly the same trajectory” as those going through the menopause. A third of the participants in the study were students.
Elaine Miller, a pelvic health physiotherapist and member of the Chartered Society of Physiotherapy, said: “A lot of women are absolutely fine until the menopause and then they start to get leaky. That appears to be exactly the same trajectory for female people who take cross-sex hormones, but there hasn’t been much in the way of research.”
She said she had worked with around 20 detransitioners who sought help for pelvic floor issues - and many more from around the world had been in touch - but that there was a “stigma” around incontinence and that people were “embarrassed” and minimised the issue.
“Wetting yourself is something that just is not socially acceptable, and it stops people from exercising, it stops them from having intimate relationships, it stops them from travelling, it has work impacts,” she said.
“The impact a bit of leaking has on these young people’s lives is huge. It really needs to be properly discussed within gender clinics because I would expect that almost 100 per cent of female people that take cross-sex hormones will end up with these problems,” she added, noting that the study was “robust” and probably underplayed the issue.
“It’s really sad when we hear people say, ‘nobody ever told me this’, and they should have been informed of the risks in gender clinics.”
The menopause causes a loss of muscle mass and body strength, which affects the pelvic floor and can cause incontinence.
Women who start the menopause early or prematurely, under the age of 45, should be offered Hormone Replacement Therapy (HRT) on the NHS because the oestrogen can help prevent the onset of conditions such as coronary heart disease, osteoporosis and dementia.
Taking testosterone may accelerate the menopausal process because it stops the ovaries from functioning and reduces the amount of oestrogen the body produces.
Testosterone is also known to affect muscle mass and hair loss, and has been linked to blood clots and gallstones, but there has been little research into pelvic floor issues and incontinence.
Ms Miller said the treatment for trans men was “the same as with any other postmenopausal female, which seems kind of ludicrous when you’re talking about people that are in their early 20s”.
“It’s making sure they are not constipated, getting them into a routine where they are not dehydrating themselves because they’re worried about having an accident. A lot of it is about bladder and bowel education about what is normal, and doing pelvic floor exercises, which can make a big difference,” she added.
Kate Barker, chief executive at the LGB Alliance, said the group had “consistently spoken out about the damage done by these experimental surgeries, the overwhelming majority of which are carried out on LGB [lesbian, gay and bisexual] people”.
“Our annual conference has heard testimony from detransitioners who live every day with the consequences of actions they took when they were very young - sometimes in their teens - including permanent sterilisation and loss of sexual function,” she said. “This has finally been officially confirmed by the Cass Review.”
The Cass Review saw the NHS stop prescribing puberty blockers outside of clinical trials and a pause to cross-sex hormones being given to under 18s. It called for more care to be given in the treatment of under 25s and the health service is reviewing adult clinics as a result.
The authors of the study, led by Lyvia Maria Bezerra da Silva at the Federal University of Pernambuco, Brazil, said the findings “showed a high frequency of at least one of the pelvic floor dysfunction symptoms” and that more research into the impact of testosterone was needed because the “long-term effects are still unknown”.
The research was published in the International Urogynecology Journal.
[ Via: https://archive.today/wNl3q ]

--
Abstract
Introduction and Hypothesis
The objective of this research is to explore the effects of hormone therapy using testosterone on pelvic floor dysfunction (PFD) in transgender men. We hypothesize that PFD might be prevalent among transgender men undergoing hormone therapy. Therefore, this study was aimed at verifying the frequency of these dysfunctions.
Methods
A cross-sectional study was conducted between September 2022 and March 2023 using an online questionnaire, which included transgender men over 18 years old who underwent gender-affirming hormone therapy. Volunteers with neurological disease, previous urogynecology surgery, active urinary tract infection, and individuals without access to the internet were excluded. The questionnaire employed validated tools to assess urinary symptoms, such as urinary incontinence (UI), as well as sexual dysfunction, anorectal symptoms, and constipation. The data were analyzed descriptively and presented as frequencies and prevalence ratios with their respective confidence intervals (95% CI), mean, and standard deviation.
Results
A total of 68 transgender men were included. Most participants had storage symptoms (69.1%), sexual dysfunction (52.9%), anorectal symptoms (45.6%), and flatal incontinence (39.7%). Participants with UI symptoms reported moderate severity of the condition.
Conclusions
Transgender men on hormone therapy have a high incidence of PFD (94.1%) and experience a greater occurrence of urinary symptoms (86.7%).
#Colin Wright#Transgender Trend#medical scandal#medical mutilation#medical malpractice#testosterone#exogenous testosterone#female biology#pelvic floor dysfunction#menopause#hormones#sex hormones#wrong sex hormones#cross sex hormones#urinary incontinence#incontinence#religion is a mental illness
6 notes
·
View notes
Text
Sorry I am still thinking about theater and movement, as always after physical therapy.
In Polish when someone plays a role on stage or screen, the common verb is "wcielać/wcielić się" (w rolę, w postać), enter into the character's body, but it's reflexive, you enter into that body and assume its form as your own. And that comes down to movement, to "animation," which can be studied, whether in physical therapy or theater school. You can learn to play a different character once you figure out how the body works, how it moves. I think really actually Discovering this and paying attention to it in the world around me made me start noticing sex, as like, a latent potential in the body. I am being so serious by the way
#Everything with me starts with abstraction before it gets concrete#And I think I reasoned my way to the existence of human sexuality via physical therapy and. Theater#Thanks indirectly Vampire Show#And weed and exogenous testosterone obviously
18 notes
·
View notes
Text
finally have an actual job so maybe I can stop being a hermit and get officially divorced and feel sort of financially stable and possibly try dating again and get a cat ??? is that allowed? no I probably shouldn't unless I get a bigger place and can have two cats to be friends
downside is when the fuck am I supposed to draw dumb comics if I'm working for hours and hours a day? Hell and suffering on earth. maybe i should get an iPad or a whatthefuck ever and draw on the commute so I don't lose even more of my meager art skills
#personal bullshit#i have never had what is traditionally considered a Real Job#this is my first 8 to 4 type job#tbqh if i could have just done teaching assistant work without the whole grad student shit that would have been cool#but i just couldn't anymore#no one there helped me when i needed it#a super huge fuck you to all of the mandatory training i had to do re: intimate partner violence and abuse#well anyway it's fucking done and who cares if i wasted 8ish years of my only life (:#now i get to help people make babies#which is not at all what i thought i would do#but hey at least it feels meaningful#and i get to wear scrubs all the time which is nice because they're kind of shapeless and make me look slightly more masc esp with binding#wonder if i could donate oocytes#im sure as fuck not gonna use them#might be too old tho#give bad eggs#also might have too much testosterone in my system now#0 idea how that works except at some point they expect me to stop menstruating#but my dumb reproductive parts are too strong too powerful will not be stopped by some pitiful exogenous T#anyway i really need to try to sleep#and stfu#but yeah maybe i can think about moving and getting 2 cats
17 notes
·
View notes
Text
!! Didn't post because I Forgor, but I passed my 1 year anniversary of being on testosterone a few weeks ago!
#low dose testosterone is GREAT this post is low dose T propaganda#if ever you have felt the desire to experiment with exogenous sex hormones. this is a sign to do it.#mela speaks
4 notes
·
View notes
Text
i love dudes so much........ they're so hot. man
1 note
·
View note
Text
Managed to jack off in the shower like a cis guy using my dick growth
0 notes
Text
i really like physical 100 but the winner will always be a 6’ crossfitter if all of the challenges are high volume high intensity nightmares. idk like could we perhaps get an obstacle course in here or perhaps some calisthenics. give other people a chance to shine
#like i guess that’s the peak of physical fitness. it’s bad for you though#also people are mad about steroid users. let them live everyone does it. let’s all inject exogenous testosterone together#like my thing is. who cares. it’s not an indicator of performance. high volume high intensity training is. also being 6’ 185lbs#.txt
0 notes
Text
OH RIGHT IM LATE ON MY SHOT
ew I just got a kind of dysphoric feeling I havent had since I was like 15. what the fuck.
#I got this crippling feeling my testes are slowly poisoning me but they are safely deactivated.#also like. I take exogenous testosterone. I want that shit in my body.
6 notes
·
View notes
Text

Thank you exogenous testosterone for the preponderance of 18 year olds in the gym who look 40, covered fully in body hair and thick mature muscle hanging off every inch, complete with deep baritone voices, the cocky swagger of full grown alpha males and considerably aged facial features. Contrary to what you might read in the press, we are living in an age that rightly exalts masculinity and encourages it in young males.
90 notes
·
View notes
Note
hi! i was wondering your opinions on how hrt affects the body? i hold a lot of radfem beliefs but i am trans (taking testosterone). would being a woman to you have to be completely about chromosomes? for example, trans men years on T do not have the same genetic makeup as cis women. same with trans women on E, their genetic makeup would be very different to cis men, and would more correlate to cis women. does this factor in who you consider female/male or having experience as women?
Hi there, thanks for reaching out.
Firstly, I think you may be a bit confused. Taking exogenous hormones does not affect your genetic makeup. Your dna will stay the same unless you're exposed to something extreme like radiation - this is a good thing because dna mutation is bad for you and causes cancer! Your genetic sex is immutable, a person with XY chromosomes cannot have their dna altered to have XX chromosomes instead.
Hormones will affect the expression of your genes, for example turning on facial hair production in women who are taking testosterone. This is why those patterns of facial hair, even in women, differ from person to person. The genes for it were already there, but hormone replacement therapy uses the endocrine system to change what signals get sent to your genes to tell them what features to express.
Beyond chemically induced genetic expression, there are particular physical features in males that do not occur in males, and vice versa. This is a feature of the /ancient/ evolution of sexual reproduction. Despite the variety of metaphysical beliefs about identity and personhood, the truth is that humans evolved to reproduce between two sexes, and human beings cannot change sex. Every cell of your body has your sex encoded within it. This affects us physically in many ways. I and most feminists believe that this fact should be irrelevant to any person's ability to pursue their passion, be themselves, and love who they love. Even so, recognition of biological sex is something important. This is really critical in a medical context. For example: men who receive a blood transfusion from a pregnant or recently pregnant woman have an increased risk of death by transfusion-related lung injury. Another example: tracheostomy tubes differ in size depending on sex due to dimorphism in average tracheal diameter. A women who is reported as a male risks considerable injury by having a male sized tracheostomy tube forced into her windpipe. A considerable amount of medications differ in dose effectiveness and side effects based on biological sex. Something as straightforward as a heart attack has different symptoms depending on if the patient is female or male. Denial of biological sex is dangerous, and as it stands, medical science has not advanced enough to change the biological sex of an individual. If you are born male, you will stay male for your entire life. You say that a transwoman who has taken estrogen is more genetically similar to a woman, I'm sorry but that simply isn't true. A male person will always be more genetically similar to other males than to a female person.
Determination of sex is very simple, it's about the easiest genetic test to do. They have kits for high school classrooms to try out ffs. We need to leave the "meaningful sex change is possible through medical intervention" thing in the past, all we accomplish with that is giving people false hope and an unattainable goal to fixate on. Sex is real and immutable, I wish it didn't matter, but it does.
And why it matters is, maleness and femaleness have become inseparable from certain stereotypes and assigned qualities by societies in human history. Overwhelmingly, the male people subjugate the female people. Since men, male humans, discovered womens' ability to give birth could be taken advantage of, it was capitalized upon. And this is the foundation of patriarchal society. Religions were founded to justify this as the will of god. To deny that women have historically been persecuted due to their sex is, well, misogynistic. There is no "woman feeling" that makes us targets for child marriages, FGM, trafficking/prostitution, and other horrors from the minute we're born and even before. No, it's the sex we were born with that makes the world think it can decide our fate. In fact, the way that people treat male children differently from female children is so different so early, that we are genuinely unable to study human behaviour unaffected by gendered expectations. This is what feminists are talking about when they discuss "socialization". There is not a single man on the planet who knows exactly what it's like to see the world from a woman's eyes, no matter how feminine that man is. Womanhood isn't something you can achieve or acquire through effort: you were either born a woman or you weren't, just like you were either born with detached earlobes or not. It's so simple.
All that to get to my final point: Yes, I believe the definition of womanhood comes down to biology, because anything beyond that is a meaningless stereotype. Women can do anything, be anyone, look any way they want, go through any experience they do. The one thing they have in common is that they are female adult human beings. There is not way to fail at being a woman or do it wrong, you just are. Womanhood is the experience of having been a female person in this world, and nothing else. There are certain things only female human beings need, like abortion and female contraceptive rights, access to spaces where we can be safe from our subjugators (male human beings), and the ability to define ourselves and fight for our collective rights.
(At this point you may object and point out that male people who identify as trans women are also subject to violence and scorn from men: unfortunately that is often the case, but this does not make male people who identify as women, well, female. We need solutions for them that do not involve requiring women to sacrifice our comfort and safety for the sake of a particular subset of men, because of the inherent risks involved and the fact that women do not owe men anything even when those men have it bad.)
One last thing: my opinion is that prescribing exogenous cross-sex hormones is unethical (so are all elective cosmetic medical procedures but that's a post for a different day). I understand the distress that gender dysphoria inflicts on people, however the ill effects of hrt are too numerous to condone. The huge increase in risk of stroke with estrogen, heart disease and uterine atrophy with testosterone, and the way that trans medicine studies are notorious for losing followup with patients after a year or less... it's short sighted and frankly, financially motivated. The amount of trans patients who are prescribed hormones without access to an endocrinologist, it's honestly infuriating. People deserve the best care possible, not lab rat bullshit where they cut you loose when it's not working out. I won't judge anyone for what they do to themselves to cope with distress, but I want everyone, especially girls, to be aware of the lifetime effects medical decisions may have, and that you also can find happiness within yourself without hurting your body.
Thanks again for your question, be well ✌️
212 notes
·
View notes
Note
More questions on the topic of Trans Vox (hopefully ur not sick of them by now lol :p)
Does he take testosterone in your 666 series?? If he did, would he have to figure out a way to make it himself or do you think there’s another reliable way to access that kind of thing in hell? How would taking T interact with his half human/ half machine body?? Did he just figure out how to lower his voice, get a dick, and call it a day w/out having to even think of any of this? I guess he probably wouldn’t have thought of this originally considering his time period haha.
Sorry if this is overwhelming. Feel free to ignore me, I’m just intensely excited about your series and wanna absorb as much knowledge as I can about the characters.
Personally, I'm fucking in love with biomechanical character concepts, so I'm fully and utterly on team "Vox's biology is extremely customizable and he went hog wild with it." I am SO glad you asked because this is a very fun subject to me! <3
In the headcanon of 666, he's a really uncanny amalgamation of man and machine. There are obviously limits to what can be done or what kind of invasiveness is required to do certain things, but they're less inherent to the human condition and more, just... kind of random! Thanks, hell!
He has lungs! They help him breathe and are also part of his ventilation system and vent partly out from his sides. His voice is a speaker that doesn't depend on his ability to breathe. Despite these things, both his breathing and his speaking are affected by his feelings and each other because his psychosomatics are coded into his hardware.
So when it comes to Vox being trans in 666 and whether he's on T: That depends on what you count as "taking" hormones! He does not give himself a weekly shot of exogenous hormones. He does, however, have parts of his endocrine and autonomic nervous systems accessible as literal code, which has long been modified to behave appropriately to his preferences as far as hormonal regulation is concerned, kind of like changing your own DNA! This isn't something he can just adjust on the fly, and even adjusting it at all is like fucking with a computer's base code. He might end up with hyperthyroid disregulation or just plain brick himself if he fucks up. I also imagine that doing something like that also didn't occur to him for quite a while, long after he'd modified the more accessible physical stuff.
Ironically, what would be surgical in real life is easier for Vox in comparison. He's had to swap out his entire head at least once in the past to upgrade: replacing his vocal speaker and swapping his primary sexual characteristics is easier than what amounts to brain surgery.
#ask#personal#Anonymous#666 live on air#vox#trans vox#hazbin hotel#my writing#NEVER SICK OF THESE THANK YOU V V MUCH
107 notes
·
View notes
Text
Also I finally restarted T last night after 6+ months off due to losing insurance then complications with insurance once it was reinstated. Anyway I need to embroider a sampler in bright red Gothic boldplate text and hang it above my bed. And the sampler will say WHEN YOU ARE DISSOCIATING SO BADLY IT FEELS LIKE YOUR VERY CONSCIOUSNESS IS FLICKERING IN AND OUT OF THE PRESENT TENSE LIKE A PATCHY RADIO SIGNAL. AND YOU THINK "HEY THIS IS HOW IT FELT WHENEVER I GOT MY PERIOD, WEIRD." AND IT GOES AWAY WITH THE APPLICATION OF EXOGENOUS TESTOSTERONE. THAT IS VERY SIMPLE STRAIGHTFORWARD HORMONAL GENDER DYSPHORIA. AND YOU CAN ALLEVIATE IT WITH HORMONE REPLACEMENT THERAPY. YOU ARE TRANSGENDER. DUMBASS
38 notes
·
View notes
Text
since making the kristen stewart "who wants to tell her" post that led to nuclear infighting in its notes, i have gotten several asks about if i think the mere possibility of someone going on testosterone is a good thing or a bad thing, and it's like. look buddy. i'm a fallout new vegas blog. what do you THINK my opinions on exogenous hormones are
58 notes
·
View notes
Text
something I think stone butch disco made a great point of is that female masculinity is not on a continuum with male masculinity. if it was, that posits maleness and the possession of male secondary sex characteristics (or male-like) as being at the top of the scale, the most masculine. this only reifies the idea that sex characteristics are inherently masculine or feminine, aka gender essentialism, despite many TRAs claims to the contrary. it is ironically very binary thinking. those pursuing transition through the form of cosmetic surgeries and exogenous testosterone are pursuing maleness, not masculinity.
it’s important to remember and reaffirm again and again that sex characteristics are neutral, not inherently masculine and feminine (and ultimately, nothing is; masculinity and femininity are arbitrary labels assigned socially in order to maintain sex roles)
11 notes
·
View notes
Note
can u elaborate on irregular hrt and osteoporosis… #irregularhrtgang
having low levels of both estrogen and testosterone at the same time is a major risk factor for a number of issues, osteoporosis/osteopenia among them. when you take exogenous hormones (HRT), your endogenous hormone production generally decreases to compensate: you only need so much sex hormone, so for example if you're taking T you'll generally produce much less E. stop or reduce your T doseage, and generally your E levels will rise again, keeping your overall endocrinological function going. however, that doesn't happen overnight; the same way that when you start HRT it takes a few weeks or months for your hormone levels to stabilise, if you are irregular with your doses then your endocrine system can end up in a kind of game of 'catch-up', where it's often not fully compensating for the lower levels of exogenous T because you're sporadically chucking a full or higher doseage in. missing a dose once in a while or being a few days late is generally not a big deal, but if you're spending years on end with significant irregularity in your hormone regimen, it definitely can become a problem. as far as avoiding osteoporosis goes, you're fine if you're either E-dominant or T-dominant---but you do want to have in-range values of one. perpetually or frequently low levels of both are where you'll run into issues.
this is obviously a bit more complicated for people whose HRT involves a blocker for their endogenous hormones (more common with feminising HRT but sometimes also a part of masculinising HRT) because in that case the endocrine system's ability to compensate for lower or stopped exogenous hormones will also depend on whether you're still taking the blocker, how long it works for, &c. however the general point still stands: you want to make sure that you have sufficient levels of T or E (you can look up the general medical targets; the numbers vary somewhat by age). an adjustment period as you switch dominant hormones or change your dose once in a while is not a big deal; chronic irregularity can be, especially if you are young because a great deal of bone accretion normally occurs in your teens and 20s, and loss of bone mineral density is generally not fully reversible.
46 notes
·
View notes
Text
What does it mean that Homelander is the only supe that has Compound V incorporated into his DNA? And that he can pass it down to progeny?
A short essay no one asked for (but inspired by @saintmathieublanc ‘s poll about whether HL and Ryan can be depowered)
Reading 1: literal
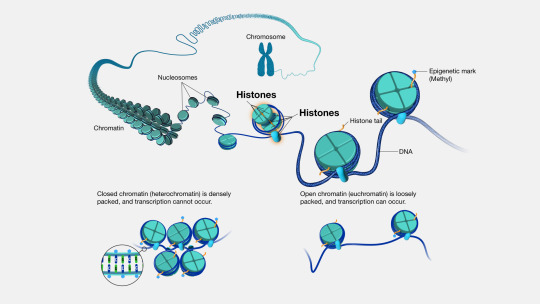
His DNA consists of Compound V. Which means that Compound V is a nucleotide analogue, a proteinaceous component of histones around which DNA wraps and gets packed into a chromosome, or some kind of non-organic chemical that binds to DNA (DNA intercalators). I actually kind of like the idea that Compound V is a part of histones, because you could handwavely imagine it gets incorporated haphazardly and affects the expression of random genes, turning them on or off, hence its varied effects.
Reason 1 none of these seem likely: DNA replicates constantly, not only during embryonic development but throughout your life. Having DNA be modified but not requiring a constant influx of new Compound V means that the DNA would eventually dilute out to become normal.
Reason 2 these aren’t likely: a proteinaceous histone component injected into infants wouldn’t really exert any effects. Wouldn’t even go into cells. A nucleotide analog or a DNA intercalator chemical could go into cells and effectively act as a DNA damaging agent (this is how some chemo works, in fact). Hard to imagine how randomly damaging DNA would result in gaining of abilities, but I guess formally possible if the damage is somehow directed. The randomness of powers gained could potentially be compatible with “random damage”. But what would then be the difference between Homelander and other supes? The Compound V would then be “part of the DNA” in both cases
Reading 2: which I favor
Compound V is a hormone. Hormones are something one could inject into a baby to exert profound effects, even if only done once. What’s not clear of course is why the hormone exerts such different effects in different babies. One handwavy model is that, unlike testosterone or estrogen or melatonin or adrenaline, with defined programs being triggered, Compound V is a hormone that creates artificial stresses in the body that tissue will respond to adaptively, and that this process is stochastic/random. This would be consistent with Compound V being better as something taken as a child- more tissue plasticity.
What does it mean that Homelander’s DNA “contains Compound V” in this schema? Hormones aren’t part of DNA. But they could have engineered a gene that encodes an enzyme (or a set of genes encoding a set of enzymes) that generate Compound V out of a common steroid precursor like cholesterol. They may also have encoded whatever receptor in the human body binds Compound V to be expressed more highly or in specific tissue in the body, but this is less crucial. This would even be somewhat realistic for 1981 era biotech. In this scenario, Homelander has been exposed to Compound V throughout embryonic development (earlier than everyone else), and has the ability to make more all the time. This would be consistent with it being heritable: Ryan didn’t need any exogenous Compound V, he had the genes to generate it himself.
If Soldier Boy’s radiation undoes the effects of Compound V out of people who have had one exposure, this would mean his radiation would be less effective on Homelander and Ryan: they would eventually generate more Compound V and with time presumably regain their powers. And that’s my final answer to @saintmathieublanc ‘s poll 🧐
#compound V logistics#no one:#literally no one:#me: writes essay about stuff neither the Boys writers nor Garth Ennis devoted any thought to#homelander#homelander meta#biology#the boys#the boys tv#mystuff
128 notes
·
View notes