#congenital pulmonary cyst
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
12.7% of mobile users access Tumblr.
Text
Clinical Case Reports – 1970 by P. Syamasundar Rao in Journal of Clinical Case Reports Medical Images and Health Sciences
Abstract
In this paper five case reports were presented and include congenital pulmonary cyst, Wilson-Mikity syndrome, diaphragmatic eventration; foreign body in the bronchus, and cor pulmonale that developed after implantation of a ventriculo-atrial shunt with a Pudenz-Heyer valve for treatment of hydrocephalus. For each case report, clinical, chest x-ray, electrocardiogram and other pertinent findings were presented. This was followed by discussion of etiology, diagnosis, and treatment options, as appropriate.
Keywords: congenital pulmonary cyst; diaphragmatic eventration; Wilson-Mikity syndrome; foreign body in the bronchus; cor pulmonale
Introduction
During the academic clinical practice for over five decades, the author had the unique opportunity to observe and document many interesting clinical case scenarios. The purpose of this review is to revisit these interesting cases. Because of the voluminous amount of this material, the material may be divided into a five-part series. Each of these case reports, while rare and important clinical observations, do demonstrate a clinical point that is useful to the pediatricians, pediatric cardiologists and/or other physicians.
Congenital Pulmonary Cyst
Case Report
A female infant with a birth weight of 6 lb 7 oz, born after a full-term, normal pregnancy and delivery with an Apgar score of 9 presented at three weeks of age with a two-week history of tachypnea. There were no other symptoms and the infant’s physical examination was normal except for tachypnea (respiratory rate of 50 per minute) and mild inter-costal and sub costal retractions. A chest roentgenogram was obtained (Figure 1) which was interpreted as pulmonary cyst. The heart was pushed to the right by the cyst (dextroposition of the heart). At thoracotomy, a huge lung cyst, involving the lower lobe of the left lung, was found, and was resected and the patient made an uneventful recovery.
Chest x-ray in posterio-anterior (A) and lateral (B) views demonstrating a large pulmonary cyst, marked with arrows. Note that the heart is pushed to the right, dextroposition of the heart. Reproduced from Rao PS. Amer J Dis Child 1970; 119:341-2.
Discussion
Congenital pulmonary cysts in the neonate are uncommon and are considered as errors in embryological development. They are of several categories namely, bronchogenic cell, alveolar cell, and combined cell types, based on the cellular component of the cell wall of the cyst. The symptoms depend largely upon the size of the cyst. These patients may not be discovered until a chest x-ray is performed for other reasons or may present with symptoms of tachypnea, dyspnea, and cyanosis in the neonatal period secondary to compression of lung tissue. The findings depend upon the size and location of the cyst. Dextroposition of the heart or tracheal shift and hyper-resonance, diminished breath sounds, and rales may be detected on physical examination. The chest x-ray findings may demonstrate a cyst, as in our case (Figure 1) or may be misinterpreted as pneumothorax. Other conditions simulating the cyst are staphylococcal pneumonia, diaphragmatic hernia, congenital lobar emphysema, sequestrated lobe, and hydro-pneumothorax or pyo-pneumothorax. In symptomatic cases, cystectomy, segmentectomy, lobectomy, or pneumonectomy, depending upon the size and location of the cyst is suggested. Percutaneous aspiration of the cyst is not recommended except as an emergency measure to relieve the tension. Some authorities advocate no surgical intervention because of the possibility of spontaneous regression of the pulmonary cysts, but most authorities recommend surgical excision of the cysts [1].
Late Respiratory Distress in a Premature Infant
Case Report
A premature male infant was born at 25 weeks of gestation and weighed 2 lb 12 oz at birth. Abruptio placenta and prolapse of the umbilical cord complicated the delivery and required resuscitation with oxygen. The chest x-ray was normal at that time. The baby was placed in an incubator in 35 percent oxygen, which was discontinued within 24 hours. At the age of 31 days, tachypnea and recurrent apnea with cyanosis developed. Auscultation revealed bilateral rales in the chest, again necessitating resuscitation with O2, administered by bag and mask. Chest x-ray (Figure 2) revealed a diffuse parenchymal reticular pattern with multifocal areas of radiolucency. This roentgenographic pattern, along with the clinical findings, is essentially diagnostic of the Wilson-Mikity syndrome.
Discussion
Wilson an Mikity originally described this condition in 1960, and is now called Wilson-Mikity syndrome.2 The etiology is not clearly understood but is considered to be due to pulmonary dysmaturity with uneven postnatal development of pulmonary alveoli in the��premature infants.2 No consistent relationship with O2 therapy has been established. Bronchopulmonary dysplasia is another condition seen in the neonatal period and should be distinguished from Wilson-Mikity syndrome. The cystic appearance on the chest x-ray in the third stage of bronchopulmonary dysplasia resemble those of Wilson-Mikity syndrome; however, it follows treatment of severe hyaline membrane disease with high concentrations of O2 and artificial ventilation.2 The clinical presentation of Wilson-Mikity syndrome is characteristic in that the infant is premature with minimal or no respiratory distress at birth but, develops progressive respiratory distress, with dyspnea, tachypnea, cough, cyanosis, and rales in a few days to weeks. Diffuse reticular pattern of both lungs with areas of multifocal radiolucency are usually seen, similar to those seen in figure 2. Progressive pulmonary insufficiency with signs of right heart failure develop in patients with fatal outcome. But, about half of the patients eventually recover from their pulmonary disease. Pulmonary function studies are abnormal with decreased lung compliance, increased expiratory flow resistance, and increased breathing effort. Respiratory acidosis develops in spite of increased minute volume. Arterial O2 desaturation is thought to be secondary to intrapulmonary right-to-left shunting.2 The treatment is largely supportive [2].
Fever, Vomiting and Dome-Shaped Density in Right Thorax
Case Report
A four-month-old boy presented with a history of fever, poor feeding, vomiting, and slight cough for two days. Past history is essentially normal except for an Apgar score of 6 at birth. Breath sounds were diminished at the right base. Laboratory studies were normal. Chest x-ray (Figure 3) was performed which revealed a dome-shaped density in the right thorax which did not coincide with any pulmonary lobe or segment. The elevation of the inferior liver margin in the abdomen indicated that the abnormal shadow was liver. Based on these findings eventration of the right hemi-diaphragm was suspected. To confirm the diagnosis, a diagnostic pneumoperitonium was performed (Figure 4) which confirmed the diagnosis.
Chest x-ray in posterio-anterior (A) and lateral (B) views showing a dome-shaped density in the right thorax (the x-ray was reversed by the printer). The distribution of the density did not coincide with any pulmonary lobe or segment. The elevation of the inferior hepatic margin in the abdomen indicated that the abnormal shadow was liver. Reproduced from Rao PS and Patel JK. Chest 1970; 58:89-90.
Diagnostic pneumoperitonium with chest x-ray in lateral view. This demonstrated air below the diaphragm suggesting eventration of the diaphragm instead of pneumonia or other lung pathology. Modified from Rao PS and Patel JK. Chest 1970; 58:89-90.
Discussion
Eventration of the diaphragm is classified into adult and infantile types [3]. It is generally thought to be the result of congenital mal-development of the diaphragmatic musculature. However, such an abnormality may occasionally be caused by phrenic nerve injury during birth. The true incidence of eventration is not known, but in mass x-ray surveys of adults, it was found to be one in 10,000 [3]. Total eventration is thought to be more common on the left side and partial eventration on the right [3].
Clinical findings largely depend on the extent of eventration. There may be no symptoms or the patient may present with dyspnea, tachypnea, and cyanosis in the newborn period, requiring immediate treatment. Seesaw cyclic motions of the epigastrium with respiration and Hoover's sign (uninhibited divergence of costal margin from midline on inspiration), if present, are helpful in making the diagnosis. Percussion on the affected side may be dull or tympanic depending on the organs migrated under the diaphragm.
Fluoroscopy and chest x-rays are generally useful in arriving at the diagnosis. In right-sided eventrations, the lesser amount of liver shadow in the abdomen, i.e., elevation of the inferior margin of the liver helps to distinguish eventration from the other conditions [3]. Diagnostic pneumoperitonium is likely to establish the diagnosis, but the current availability of ultrasound technology, diagnostic pneumoperitoneum may not be necessary at the present time.
Symptomatic newborns with diaphragmatic eventration should be treated surgically; plication of the eventrated diaphragm is successful in relieving the symptoms with good long-term results. Some authorities suggest that asymptomatic patients also should be addressed surgically [3].
Foreign Body (Peanut) in The Left Main Stem Bronchus
Case Report
A 13-month-old girl with a history of poor appetite, loss of weight, cough, and intermittent low grade fever was admitted to the hospital for evaluation and treatment. No history of choking episodes was elicited. History revealed that a relative who had active pulmonary tuberculosis lived with the infant's family for a short period of time four months prior to the current admission. Because of this reason, the local health department performed tuberculin skin test which was positive and treatment with isoniazid was initiated. On examination her weight and height were between the third and tenth percentile. Decreased breath sounds on auscultation and hyper tympanic note on percussion were noted over the left side of the chest.
Intermediate strength purified protein derivative (PPD) was positive. Chest roentgenograms were obtained (Figure 5). Based on the history, physical examination, and chest x-ray findings, a diagnosis of endobronchial tuberculosis was entertained. However, prior to beginning treatment, bronchoscopy was performed to appraise the extent of airway encroachment.
Discussion
Autoimmune encephalitis is a condition that can be easily missed as it is not commonly considered in the differential diagnosis of various medical presentations. However, such diagnosis should be always taken into consideration when a person, particularly a child, presents with a new onset of refractory status epilepticus (NORSE) and/or new behavioral or psychiatric conditions. An early diagnosis of AE is essential, as the treatment is different from other conditions. With correct timely interventions the outcome is frequently favorable.
Though SARS-Cov-2 virus rarely invades the nervous system, Covid-19 infection frequently causes neurological symptoms like headache, delirium, anosmia, and dysgeusia [14]. One of the mechanisms of indirect nervous system involvement is through inflammatory response and immune dysregulation. There are few recorded cases of indirect involvement of CNS by auto-antibodies that are directed against the surface and synaptic protein. This case is one of the rare cases of Anti NMDA antibody autoimmune encephalitis that is associated with Covid-19 infection [15]. It indicates that in the era of COVID-19, high vigilance is required as a possible association may increase AE incidence.
A recent systemic review that analyzed 16 studies, including a total of 161 patients with NORSE [16], showed that the most frequent cause was AE. In addition to the well-known association with teratoma and cancer, AE, and specifically Anti-NMDA receptor Ab encephalitis, could be associated with a SARS‑CoV‑2 infection, either concomitantly or as post-infection manifestation. In this reported case, immunotherapy, in addition to anti-seizure medication, showed to be effective.
The main limitation of this report is the relatively short follow-up period. Observation of the child is ongoing to detect possible medium- or long-term consequences.
Chest x-ray in posterio-anterior (A) and lateral (B) views showing hyper-aeration of the left lung and a slight shift of the heart and mediastinum to the right. The left diaphragm is also flattened. There are no areas of infiltration or consolidation in the lung, but prominent densities (arrows in A and B) suggestive of enlarged lymph nodes were also seen. Modified from Rao PS, et al. Amer J Dis Child 1970; 120:51-52.
Positive PPD in an infant with poor appetite, loss of weight, and fever is suggestive of primary tuberculosis. This is particularly so given the patient's exposure to a subject with active pulmonary tuberculosis. The x-rays show hyper aeration of the left lung with a shift of the heart and mediastinum to the right. The left leaf of the diaphragm is also flattened. While there are no areas of infiltration or consolidation were seen, prominent shadows suggesting enlarged lymph nodes were seen (arrows in figure 5). Endobronchial tuberculosis with compression of the bronchus by adenopathy may produce changes seen figure 5.
Discussion
Even though there was no history of choking or aspiration, the possibility of foreign body aspiration should be considered in this age group. Consequently, bronchoscopy was performed which revealed a peanut in the left main stem bronchus and was extracted during bronchoscopy. The peanut and the adjacent edema of the bronchus caused partial bronchial obstruction and acted as a check valve, so the air entered the left lung but, unable to leave the left lung since the bronchus becomes smaller during expiration, producing the roentgenographic appearance shown in figure 5. The baby improved and the treatment with isoniazid was continued because of the positive PPD.
Cor Pulmonale as a Complication of Ventriculoatrial Shunts
Introduction
Cerebral ventricle-to-right atrial shunts with Pudenz-Heyer or Spitz-Holter valves were widely used to treat hydrocephalus in the 1960s. Development of pulmonary hypertension with chronic cor pulmonale is rare with these shunts. We reported a patient who developed such a complication along with description of specialized pulmonary function studies in the early detection of such complication [5].
Case Report
An 11-year-old white boy was hospitalized in April 1969 with a history of progressive weakness, dyspnea, and pedal edema. He was diagnosed to have hydrocephalus and had a ventriculo-atrial shunt with a Pudenz-Heyer valve implanted at the age of 6 months. The shunt was thought to be functioning well when he was evaluated at the age of 2 years. He was asymptomatic until he was 9.5 years old, when he developed signs of congestive heart failure (CHF) and was treated at another hospital with digitalis and diuretics with some improvement. Right heart catheterization at the same institution revealed a mean right atrial pressure of 35 mmHg and right atrial angiography revealed slow emptying of the contrast, filling defects on the right lateral atrial wall and in the right and left pulmonary arteries. The ventriculo-atrial shunt was removed shortly thereafter. The patient was referred to our group for further evaluation and management [5].
Pertinent findings on examination included height and weight below the third percentile, head circumference above the 97th percentile, pretibial edema, prominent “a” wave in the left side of the neck, no venous pulsations on the right side, palpable right ventricular heave, markedly accentuated single second heart sound, an audible fourth heart sound at left lower sternal border, a Grade I/VI ejection systolic murmur at the mid-left sternal border, liver edge palpable 5 cm below the right costal margin, clear lung fields on auscultation, and normal neurological examination.
Electrocardiogram (ECG) (Figure 6) and the vectorcardiogram (not shown) revealed right atrial and ventricular hypertrophy. Chest roentgenogram (Figure 7) showed moderate cardiomegaly and prominent main pulmonary artery (PA) segment and clear lung fields. Lung scan with 131I-labeled macro-aggregated albumin was suggestive of multiple pulmonary emboli. Blood gas analysis showed pH 7.56; PaO2 80 mmHg, PaCO2 23 mmHg and bicarbonate 24 mEq/liter. Routine pulmonary function studies revealed restrictive lung disease. The ratio of wasted ventilatory volume (physiological dead space) to tidal volume (VD:VT) using Bohr's equation was 0.58 (normal 0.3 or less).
Electrocardiogram shows right axis deviation with right atrial hypertrophy and marked right ventricular hypertrophy. Reproduced from Rao PS, et al. J Neurosurg 1970; 33:221-225.
Chest x-ray in posteroanterior view demonstrating cardiomegaly and prominent main pulmonary artery segment (arrow). The peripheral pulmonary vasculature is diminished. Modified from Rao PS, et al. J Neurosurg 1970; 33:221-225.
Vigorous treatment with digitalis and diuretics resulted in only temporary relief. During the next year, he continued to deteriorate and died of intractable right ventricular failure. Postmortem revealed right atrial thrombosis, severe right ventricular hypertrophy, multiple thrombo-emboli in the large and medium-sized pulmonary arteries, and intimal proliferation of the pulmonary arterioles.
Discussion
The case presented demonstrated development of cor pulmonale secondary to pulmonary thrombo-embolism which was produced by thrombi that arose following a ventriculo-atrial shunt with a Pudenz-Heyer valve for treatment of hydrocephalus. The causes of thrombo-embolic complications were not well understood, but the hypotheses, as reviewed by us [5], include infection, periarteritis due to autoimmune reaction of the pulmonary vessels to protein of cerebrospinal fluid, release of brain thromboplastin resulting in thrombosis at the point of contact with plasma coagulation factors, and simply the presence of a foreign body in the cardiovascular system for prolonged periods of time.
Early detection of pulmonary hypertension by periodic (every six months) evaluation by chest x-ray and ECG studies was suggested by some investigators, but early detection of pulmonary hypertension is of limited value since obstruction of 60% of the pulmonary vascular bed occurs by the time pulmonary hypertension develops [5]. Detection of multiple filling defects on radioisotope scanning in a child with a ventriculo-atrial shunt would be suggestive of pulmonary embolization and might be useful in early identification. Based on the observations of Nadel and associates [6] and those of ours [5], we suggested that specialized pulmonary function studies such as VD:VT, pulmonary diffusing capacity, pulmonary capillary blood volume, blood gas, and pH be performed periodically to detect obstruction of pulmonary vasculature prior to the development of pulmonary hypertension and cor pulmonale [5]. However, it should be noted that ventriculo-atrial shunts are no longer performed to treat hydrocephalus, but instead ventriculo-peritoneal shunts are used at the present time.
In summary, a rare case of pulmonary thrombo-embolism with resultant pulmonary hypertension and cor pulmonale following ventriculo-atrial shunt for hydrocephalus was presented with the recommendation to use of special pulmonary function studies for early detection and if found to be positive, immediate removal of the shunt system may eliminate further embolization into the lungs and prevent irreversible pulmonary vascular disease.
#congenital pulmonary cyst#diaphragmatic eventration#Wilson-Mikity syndrome#foreign body in the bronchus; cor pulmonale#Journal of Clinical Case Reports Medical Images and Health Sciences quartile#jcrmhs
0 notes
Note
Nonbinary person jumpscare
CW for child abandonment, in depth discussion of medical/surgical stuff, and harm to babies
This is Winnipeg, a nonbinary teen (amab and mostly male aligned but very feminine) who was born with several abnormalities- lobar holoprosencephaly and several facial abnormalities, spina bifida, a congenital pulmonary airway malformation, an atrial septal defect, craniosynostosis, and congenital scoliosis.
The primary reason that Winnipeg openly identifies as nonbinary is to take back their personhood after a lifetime of having their body being changed and altered by surgery and let it be a part of them without being all they are. Their pronouns are they/he/xe, and the other kids mostly use they/them for them- to the point that it takes Lottie a HOT minute to learn they even HAVE a separate set of pronouns, let alone two.
Winnipeg was a foundling, left in the Winnipeg General Hospital in Canada- though, this isn’t where he would end up staying, as he ended up moving to the US. The workers at the hospital nicknamed him Winnie, and while they were unsuccessful in tracking down his parents, they assumed he had been abandoned at the hospital because of his numerous medical issues- his eyes were out of place, his lips were split open, his head was misshapen and face too close together, his spine bent with what looked like a large cyst on the bottom, his heartbeat was irregular, and his breathing was poor to the point his split lips and small hands were turning blue.
Over the next several years, Winnipeg underwent numerous surgeries- first heart surgery at only a week old, then craniosynotosis. Their CPAM didn’t need surgery for about six months, but they needed a tracheostomy once their lungs were cleared because of facial abnormalities making it hard for them to breathe. This was taken out after four surgeries to repair their face later on, allowing them to breathe normally. Finally, they underwent surgery for their scoliosis and spina bifida, a spinal fusion in their lower back.
The workers who found him suspect this was why his parents left him- they were likely low income or living in a state of crisis given the scope of Winnipeg’s health problems and the fact that Winnipeg appeared to be a newborn but hadn’t been born in a hospital, and when they saw the state of Winnipeg’s health, knew they would never be able to care for him.
(This is actually what happened- their mother was disabled and in poverty and didn’t think she could take care of a child with high support needs.)
Winnipeg was the one to choose that as their real name as opposed to Winnie.
They’re very chill about almost everything, but sometimes they can get set off by really tiny problems because of how much they have built up. They’re in reality extremely- and justifiably- upset that this is how their life has gone, entirely defined by all of these health issues that even now will never go away. They tend to search for ways to express themself and have control and freedom in their life, often through art. They’re a very artistic person, and they often draw on both their own skin and their friends’. The caretakers are fairly certain that has to be really bad for Ashika’s fragile skin, but they don’t have any real evidence.
Winnipeg is Ashika’s favorite of their group. They can often be found together- Winnipeg sitting in his wheelchair when his pain is bad and Ashika on the floor so she’s not looking down on them, white teddy bear in her lap and one hand, talking to him about anything she can think of while he draws on her free hand.
Fellow “abandoned shortly after being born” person here, I love them already
Him and Ashika interacting is so wholesome, they’re my children now- /j
2 notes
·
View notes
Text
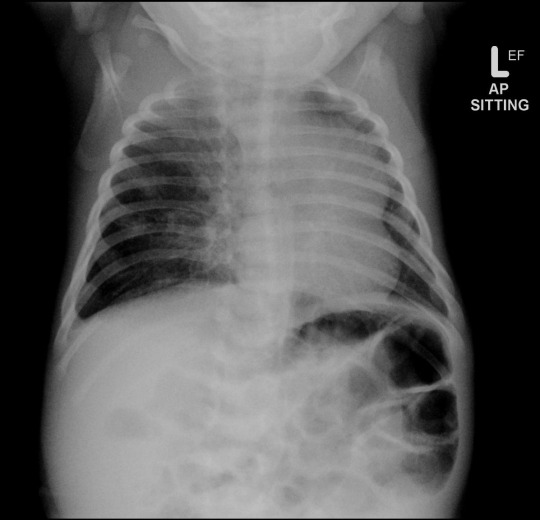

Here's a companion case to yesterday's. This is a neonate with respiratory distress.
...
...
...
...
The right mid to lower lung is hyperinflated. There is leftward medisastinal shift, including prominent medisatinal fat (that's not a mass in the left lung). CT shows cystic expansion of the right lung (2nd image). This is a congenital pulmonary airway malformation (CPAM) formerly known as congenital cystic airway malformation (CCAM). CPAM is a multicystic mass with abnormal bronchial proliferation. Differential diagnosis includes pulmonary sequestration, congenital lobar overinflation, and bronchogenic cyst (usually not aerated).
Case courtesy of Jeremy Jones, Radiopaedia.org, rID: 22542
#FOAMrad#TeachingRounds#FOAMed#Radiology#RadEd#RadCases#radres#PedsRad#Pediatrics#xray#CTRad#CT#Neonatology
22 notes
·
View notes
Text
How are Congenital Lung Disorders diagnosed?

Congenital lung diseases are often detected during routine prenatal ultrasounds.
Bronchogenic cysts usually show up on a fetal ultrasound if your fetus has signs of airway obstruction. Chest X-rays can detect the condition in newborns.
CCAMs are most often seen on normal prenatal ultrasounds. They appear as white masses with occasional small dark circles. The circles are fluid-filled cysts. Because some CCAMs are fatal, physicians will constantly monitor your fetus. Although unlikely, other CCAMs may even shrink and disappear before birth.
Lobar emphysema is most often detected on a chest X-ray after your baby is delivered. Symptoms such as uncomfortable or difficult breathing often appear shortly after delivery. If an X-ray does not reveal the abnormality, physicians may use a bronchoscope (lighted tube) to locate it.
Pulmonary sequestrations are often found later in a child’s life. They usually turn up by coincidence while a doctor is looking for something else.
If you are looking for Pulmonologist, Consult Dr. Parthiv Shah one of the best Pulmonologist in Borivali.
0 notes
Text
Fetal and Neonatal Surgery Treatment in Pune
With the development of advanced radiological techniques like fetal ultrasound and fetal MRI, many malformations are now being diagnosed while the baby is still in its mother’s womb. Some of these conditions are amenable to treatment before birth and are tackled by Fetal surgery. Rest of the conditions may be treated at birth or soon after birth and fall under the heading of Neonatal surgery.

Essential facts:
Fetal surgeries are performed on babies while they are still in the womb. These are performed for conditions which have potential to hamper the baby’s proper development.
Neonatal surgeries are performed on newborns and babies up to one month of age. They are performed for conditions which are either detected at birth or which even when detected in-utero can wait till birth for proper management.
Both the modalities are highly risky and they require management by multidisciplinary teams for fruitful outcomes.
Birth defects treated by Fetal surgery:
Fetal surgery is used to treat babies while they are still in their mother’s womb. It is found to be helpful in treating conditions like Amniotic band syndrome, Twin anemia-polycythemia sequence, Bronco-pulmonary sequestration, Spina bifida, Neck masses, Lower urinary tract obstructions, Congenital high airway obstructions to name a few.
Diseases treated by neonatal surgery
This is performed on newborn babies and up to one month of age. Some common diseases are Anorectal malformations, Atresia of Esophagus and Intestine, Hypertrophic pyloric stenosis, Gastroschisis, Omphalocele, Necrotising enterocolitis, Congenital diaphragmatic hernia, Inguinal Hernia, Lung cysts and tumors, Spina bifida, Hydrocephalus, Posterior urethral valves etc.
Techniques for Fetal and Neonatal surgery
Fetal surgery is mainly conducted in four ways depending on the condition of the baby and the mother. These are: Needle based surgery, Fetoscopic surgery, Open fetal surgery and EXIT procedure (EX utero Intrapartum Treatment). There are only a few centers for fetal surgery in India. Neonatal surgery may be performed either in the conventional open way or via Minimal Access route like Thoracoscopy and Laparoscopy.
Dr. Vishesh Dikshit is Pediatric Surgeon in Pune with expertise in all types of pediatric surgical procedures. He is adept in the art of performing minimally invasive surgery, Thoracic and Thoracoscopic surgeries, Laparotomy and Laparoscopic surgeries, Minimal Access Urinary Stone Management, Day care procedures like Hernia, Hydrocele, Circumscision. managing urological disorders in kids.
Book your appointment today with Dr. Vishesh Dikshit for any queries about your child’s condition.
#Best Pediatric Neonatal Surgeon Pune#Neonatal Surgery in Pune#Best pediatric Surgeon in Pune#Best Pediatric Surgeon Pune#Best Pediatric Specialist Pune#Neonatal Surgery treatment Pune#Neonatal Pediatric Doctor Pune
0 notes
Text
Lupine Publishers| Cervical Tarlov Cyst Mimicking Spinal Hydatid Disease: Case Report

Abstract
Go to
Background: Perineurial (Tarlov) cysts are usually incidental findings during magnetic resonance imaging of the lumbosacral spine. The Cervical localization have been reported to be a rare occurrence. We report such a case where a high cervical perineural cyst was masquerading as a spinal hydatid disease.
Case Presentation: We report a case of symptomatic cervical Tarlov cyst in a 9 years old girl operated on twice for pulmonary and hepatic hydatid cyst. Spinal magnetic resonance imaging (MRI) showed an extradural intraspinal lesion with fluid-equivalent signal extending from C5 to T2. Based on the history, the diagnosis of spinal hydatid disease was suggested. Surgical excision of the cyst resulted in significant improvement in patient symptoms, and histological examination revealed the diagnosis of a Tarlov cyst.
Conclusion: Cervical perineural (Tarlov) cyst can be symptomatic by causing nerve root compression and can be mistaken as a spinal hydatid disease on imaging. Surgical treatment can be curative.
Keywords: Tarlov Cyst; Hydatid Cyst; Diagnosis; Management MRI; Cervical Spine
Abbreviations: TC: Tarlov Cyst; CSF: Cerebrospinal Fluid; MRI: Magnetic Resonance Imaging
Introduction
Go to
Tarlov Cyst (TC) is defined as a cystic dilatation between the perineurium and endoneurium of spinal nerve roots, located at level of the spinal ganglion and filled with Cerebrospinal Fluid (CSF) but without communication with the perineurial subarachnoid space [1]. It is most often found in the sacral spine with a prevalence of 4.6% in the general population with about 13% of those being symptomatic [1,2]. The Cervical localization have been reported to be a rare occurrence [3], to our knowledge there are only five published cases of symptomatic cervical Tarlov cyst [4]. MRI of the spine is the gold standard imaging modality for the diagnostics. This is a case report of a symptomatic cervical TC that was masquerading as a spinal hydatid disease. To our knowledge, only five other cases of symptomatic cervical TC have been published [3,4].
Case Presentation
Go to
A 9-year-old girl, with medical history of surgery for pulmonary and hepatic hydatid cysts at age of 8, treated with anthelmintic with good outcome. As far as her past medical history is concerned, there were a history of cervical plexus trauma at the age of 6 with monoparesis sequelae of the left arm. She presented with a 4-week history of gradually developing left hemiparesis. On clinical exam, all deep tendon reflexes were normal. Proximal muscle strength of the left leg and the ipsilateral upper extremity was 3/5. Electromyography (EMG) showed abolition of motor and sensory responses of nerves SPE and SPI on the left upper limb. MRI of the cervical spine showed intraspinal cystic lesion of extra-Dural location lateralized to the left, extending from C5 to T2 causing a stenosis of the adjacent foramina, without contrast enhancement of the cyst wall (Figure 1). Based on the imaging and the history of patient, the diagnosis of a spinal hydatid disease was suspected. Neurosurgical indication was agreed, and the patient underwent a C4-T2 laminotomy (Figure 2), intraoperatively, cystic lesions strongly adhered to the dural mater with an appearance that was evoking congenital cysts. At this point, we opened the capsule and a clear CSF-like liquid came out from the cyst, we conducted a careful excision with Dural plasty. The histological examination showed fibrous tissue and the presence of neural elements, which is typical for perineural cysts. Postoperatively, the patient experienced significant improvement in her symptoms, represented by improved left lower-limb strength. A postoperative MRI of the cervical spine was performed after 6 months showed no recurrence of the cyst (Figure 3).
For more information about Online Journal of Neurology and Brain Disorders archive page click on below link
https://lupinepublishers.com/neurology-brain-disorders-journal/archive.php
For more information about lupine publishers click on below link
https://lupinepublishers.com/index.php
Follow on Linkedin : https://www.linkedin.com/company/lupinepublishers Follow on Twitter : https://twitter.com/lupine_online
0 notes
Text
Juniper Publishers- Open Access Journal of Case Studies

Prenatal Diagnosis of Congenital Cystic Adenomatoid Malformation of the Lung
Authored by Ons Cherif
Abstract
Congenital cystic adenomatoid malformation (CCAM) of the lung is rare. Its diagnosis is based on antenatal ultrasound and sometimes MRI. Natural course and prognosis may be favorable, but the appearance of complications, especially the fetal hydrops, is possible even quite common. We report four cases of CCAM diagnosed in the second trimester of pregnancy. Only one case was born. We propose to evaluate the contribution of prenatal ultrasonography in the diagnosis of this type of malformation.
Keywords: Antenatal ultrasound; Pulmonary lesions; Fetopathological entity; Morphological; Amenorrhea; Hyperechoic mass
Abbrevations: CCAM: Congenital Cystic Adenomatoid Malformation; MRI: Magnetic Resonance Imaging; TTP: Therapeutic Termination of Pregnancy
Introduction
Congenital cystic adenomatoid malformations (CCAM) are relatively rare developmental abnormalities of the lung [1]. They correspond to distal bronchial and pulmonary cystic dilations, communicating with the bronchial tree and devoid of cartilaginous rings [2]. They represent 25% of congenital pulmonary lesions [3].
Prenatal diagnosis has become easier with the higher resolution ultrasound imaging and has profoundly changed the management of this fetopathological entity. We report a series of four diagnosed CCAM cases in our maternity center at Farhat Hached University Hospital in Sousse, Tunisia. It was a retrospective study in order to evaluate the contribution of antenatal ultrasound in the diagnosis of this type of malformation.
Case Study
Average age of our patients was 28 years, and the mean age of discovery of the abnormality was 23 weeks of amenorrhea. Morphological ultrasound allowed diagnosis in all cases (Figure 1), and fetal magnetic resonance imaging (MRI) helped us in two cases.
CCAM was associated with hydrops fetalis in two cases, and a cardiac malformation (interventricular communication type) in one case. Only one pregnancy was completed by refusal of therapeutic termination of pregnancy (TTP). Indication of the TTP was raised in three cases due to the severity of the pulmonary involvement and was accepted by the parents.
The expulsion had occurred at approximately 23 weeks gestation; they were two male fetuses and one female fetus. On the fetopathological examination, no dysmorphic syndrome was found, and the histological analysis of the lungs confirmed the disease in the three cases.
Regarding the term pregnancy, ultrasound chest highlighted at birth, dilation of the upper lobe of the left lung with a heterogeneous echo-texture and a hyperechoic mass in which it was revealed a cystic image. There was also a second cystic image of 4mm at the anterior part of the upper lobe of the left lung.
Abdominal ultrasound did not find renal structure in the lumbar lodges but in lumbar-pelvic region, there was macroscopic cystic pictures passing bridge in front of the spine.
The newborn died around the 6th hour of life. The foetopathological examination showed in the upper lobe the presence of a nodule occupying the dome measuring 2.2cm in its largest axis, and micro-cystic appearance at the cut. The inferior lobe was also the site of a spongy-shaped para-hilar nodule measuring 0.5cm in its largest axis (Figure 2).
At the microscopic examination, and in the level of these two left lung lobes, there were several cystic formations of variable size between which there were tubular formations of the fetal lung (Figure 3). In the right upper lobe, the same lesions were found as those described on the left side. The lungs were therefore the site of a cystic adenomatoid malformation, multi-focal and bilateral.
Discussion
Congenital cystic adenomatoid malformation (CCAM) of the lung is a hamartomatous lesion characterized by cystic degeneration of the terminal bronchiolar tissue. Its incidence is estimated at 1/25000 to 1/35000 pregnancies [3].
CCAM is most often diagnosed in the perinatal period but can be detected, in some cases, during infancy and adolescence and even in adulthood [4]. Only the histological study confirms the diagnosis and eliminates other cystic pulmonary malformations. It shows cysts with air or fluid content, limited by a wall devoid of cartilage and without inflammatory signs, lined by an epithelium consisting of ciliated pseudo-stratified cells and mucus cells [2].
There are classically three types according to the histological classification of Stocker [2] based essentially on the size of the cysts: type I macrocystic (2 to 10cm) (65%), type II cystic (up to 2cm) (20 to 35%) and type III microcystic (less than 0.5cm) (10%) [2].
In prenatal, we use an ultrasound classification distinguishing between microcystic forms (53%), macrocystic (22%) or mixed forms (25%) [5]. MRI can better visualize this malformation, confirm the diagnosis in difficult situations and to share with the various differential diagnoses.
In 80 to 95% of cases, the CCAM affects only one lobe, with a certain tropism for the right lung [4]. Multiple lobe extension may occur, but bilateral involvement is extremely rare. Our case, having been delivered at term, has the peculiarity of demonstrated this bilateral and multiple involvement of the pulmonary lobes.
Cases of association with other morphological abnormalities have been reported; it may be cardiac, cerebral, diaphragmatic or renal malformations. Adenomatoid lesions are rarely associated with renal abnormalities; it is mainly renal agenesis or dysgenesis.
Prenatal evolution of CCAM is variable: it can lead to fetal hydrops in 40% or completely regress in 15% of cases [6].
The management varies according to the time of diagnosis. In the antenatal period, clinical and ultrasound obstetric surveillance is required. The study of fetal karyotype is indicated [7]. Resection or drainage of intrauterine cysts in case of CCAM complicated with fetal hydrops may be indicated. In the absence of means, a therapeutic interruption of the pregnancy can be justified in lethal forms. After birth and regardless of age, surgical resection is required in symptomatic forms [8].
Conclusion
Congenital cystic adenomatoid malformation of the lung is evoked and frequently diagnosed by antenatal ultrasound. Its prognosis depends on the extent of lesions, associated malformations and hemodynamic repercussions.
For more articles in Juniper Publishers | Open Access Journal of Case Studies please click on: https://juniperpublishers.com/jojcs/index.php
#Juniper Publishers#Juniper Publishers in USA#Critical Care Medicine#General Surgery Genetics#Hospice and Palliative Medicine#Pediatrics
0 notes
Text
300+ TOP RADIOLOGY Objective Questions and Answers
RADIOLOGY Multiple Choice Questions :-
1.The overall heart size in tetralogy of Fallot is usually a) Markedly enlarged b) Normal or relatively small c) Slightly enlarged d) Moderately enlarged. Ans:b 2.Diagnosis of aortic calcification is done by fluoroscopy by seeing a) Side to side movement b) Up and down movement c) Combined movement d) None Ans:a 3.In Urinary tract tuberculosis, frequent finding on plain film of abdomen is a) Mass b) Ileus c) Calcification d) Psoas abscess Ans:c 4.Pericardial calcification is caused by all except a) Radiotherapy to the mediastinum b) Methysergide therapy c) Anticoagulant therapy d) Benign pericarditis e) Dermatomyositis Ans:e 5.Cystic dilation of collecting tubules are seen in a) Adult polycystic kidney b) Medullary sponge kidney c) Horse shoe shaped kidney d) Nephroblastoma Ans:b 6.During angiocardiography the mitral valve is best visualized in the a) Frontal view b) Lateral view c) Right anterior oblique view d) None of the above. Ans:c 7. The X-ray finding of small intestinal malabsorption syndrome are all except a) Increased transit time b) mucosal atrophy c) Dilatation of bowel d) Flocculation of Barium Ans:a 8. Right side of mediastinal shadow is not formed by a) SVC b) right innominate c)RA d)RV Ans:d 9. Best mode of imaging for suspected uric acid calculi is a) Plain film of abdomen b) Ultrasonography c) Intravenous pyelography d) Radionuclides. Ans:c 10. Solitary nodule lung cannot be a) Tuberculoma b) Neurofibroma c) Bronchogenic carcinoma d) Lymphoma Ans:d

RADIOLOGY MCQs 11. Angle of trachea is increased in which chamber of heart enlargement a) Left atrium b) Right atrium c) Left ventricle d) Right ventricl Ans:a 12. Medusa lock appearance in X- ray seen in a) ascariasis b) Tapeworm c) Hookworm d) Ascaris and tapeworm Ans:a 13. Signs of increased intracranial tension in a child in a skull X-ray a) Separation of the sutures b) Tense anterior fontanelle c) Silver beaten appearance of the bones d) All of the above Ans:d 14. Echoenecpahalography is most useful for detecting a) Ventricular dilatation b) Midline shift c) Epilepsy d) Vascular lesions Ans:a 15. X-rays are modified a) Protons b) Electrons c) Neutrons d) Positrons Ans:b 16. "Sentinel loop" appearance on X-ray is seen a) Acute pancreatitis b) Chronic pancreatitis c) Intestinal obstruction d) Acute appendicitis Ans:a 17. The "Target Sign" sonographically means a) Ovarian carcinoma b) Ectopic kidney c) Intussusception d) Liver metastasis Ans:c 18. Osteosclerotic bone secondaries are seen in a) Carcinoma thyroid b) Carcinoma prostate C) Carcinoma stomach d) Carcinoma lung Ans:b 19.Water soluble contrast media used for myelography is a) Metrizamide b) Dianosil c) Conray d) Iohexol Ans:a 20.Most sensitive test for metastatic deposit is a) Isotope scan b) CT Scan c) Skeletal survey d) Tomography Ans:b 21.Best imaging modality to diagnose liver mass is a) Plain film b) Angiography c) C. T. Scan d) Nuclear Scan Ans:d 22.Characteristics of Benign tumour of lung in X -ray is a) Size > 5 cms diameter b) Cavitation c) Peripheral location d) Concentric dense calcification. Ans:d 23.Scalloping of the edges of sigmoid colon on barium enema is seen in a) Diverticulitis b) Crohn's disease c) Pneumatosis intestinalis d) Ulcerative colitis Ans:c 24. Widening of the C loop in X-ray is diagnostic of a) Chronic pancreatitis b) Carcinoma head of pancreas c) Periampullary carcinoma d) Calculi in the ampulla of vater Ans:b 25. AH are features of Medulloblas toma except a) Radio resistant b) Highly radio sensitive c) Occurs in first decade d) Coarctation of aorta d)TDT Ans:a 26. Notching of ribs on X- ray is seen in a) PDA b) ASD c) Ebsteins anomaly d) Coarctation of aorta Ans:d 27. Contrast used for MRI a)GDPA b) Radium c) Iridium d)TDT Ans:a 28. Saw tooth appearance on abdominal X-ray is seen in a) Prediverticular state b) Multiple polyposis c) Spastic colon d) Ischemic enteritis Ans:b 29. Increased radiolucency of one sided hemithorax may be caused by all except a) Obstructive emphysema b) Pneumothorax c) Expiratory film d) Patient rotation Ans:c 30. Gas in biliary tract is not due to a) Perforated gastric ulcer b) Necrotizing enterocolitis c) Biliary surgery d) Post-gastrectomy Ans:a 31. Egg shell calcification in hilar region is seen in a) Penumoconiosis b) T. B. c) Sarcoidosis d) Aneurysms Ans:a 32. Basal ganglia calcification is not seen in a) Wilson's disease b) Berry anerurysm c) Cysticercosis d) Hemangioma Ans:a 33. Calcification of meniscal cartilage is a feature of a) Acromegaly b) Hyperparathyroidism c)Reiter's syndrome d) Pseudo gout Ans:d 34. Sun ray appearance is seen in a) Osteoclastoma b) Fibrous dysplasia c) Osteosarcoma d) Chondrosarcoma Ans:c 35. Investigation of choice in Traumatic paraplegia is a) MRI b) CT Scan c) Myelography d) Spine X - ray Ans:a 36. Interosseous skeletal tumour is best diagnosed by a) Plain X-ray b) NMR c) CT scan d) CT with scintiscan Ans:b 37. Notching of Ribs is seen in a) Tuberculosis b)VSD c) Coarctation of aorta d) Bronchiectasis Ans:c 38.Laminated appearance of X-ray is suggestive of a) Ewing's sarcoma b) Osteoid osteoma c) Osteoclastoma d) Multiple myeloma Ans:a 39.Full colonic preparation of Barium Enema is contra indicated in all except a) Acute exacerbation of ulcerative colitis b) Irritable bowel syndrome c) Hirschsprung's disease d) Colonic obstruction Ans:b 40.Right border of the heart in a chest X-ray, is not formed by a)fVC b)SVC c) Right atrium d) Aorta Ans:d 41. Pulmonary embolism is best diagnosed by a) X-ray chest b) Enzyme estimation c) Radionucleus d) Blood gas analysis Ans:c 42. Right lung is seen to best advantage on the following view a) Right posterior oblique b) Right anterior oblique c) Left anterior oblique d) Lateral Ans:b 43. Early change of pulmonary edema in CXR a) Batswing appearance b) Pleural effusion c) Kerley B lines d) Ground glass lung field Ans:c 44. Investigation to differentiate between pericardial effusion and heart dialation includes a) X-ray b) Fluoroscopy c) Echocardiogram d) CT scan Ans:c 45. Multiple translucent cysts on X- ray are found in the chest. Differential diagnosis includes all except a) Congenital diaphragmatic hernia b) Congential adenomatoid bronchogenic diseases c) Lobar agenesis d) Bilateral multiple cysts Ans:c 46. Onion peel appearance is seen in a) C iteoclastoma b) Chondrosarcoma c) Osteosarcoma d) Ewings sarcoma Ans:d 47. IVU is not done in a) Multiple myeloma b) Secondaries in bone c) Leukaemia d) Renal tumours Ans:a 48. When bones show a 'Bone within bone' appearance this is indicative of a) Sickle cell anemia b) Bone infarction c) Osteopetrosis d) Chronic myelogenous leukaemia Ans:c 49. The best view to visualize minimum pneumoperitoneum is a) Ap view of abdomen b) Erect film of abdomen c) Right lateral decubitus with horizontal beam d) Left lateral decubitus with horizontal team Ans:d 50. In fluorescein angiography, dye is injected in a) Anterior cubital vein b) Femoral artery c) Femoral vein d) Aorta Ans:a RADIOLOGY Objective Questions with Answers 51. All of the following are true about iodinated intravascular contrast media xcept a) They are used in digital subtraction angiography b) They are radio opaque c) They can cause anaphylactic reactions d) They are used in magnetic resonance imaging e) They are excreted mainly by the kidneys Ans:d 52. Rib notching is produced by a) Coarctation of Aorta b) Neurofibromatosis c) Superior vena caval obstruction d) All of the above Ans:d 53. Widening of the C loop in X- ray is diagnostic of a) Chronic pancreatitis b) Carcinoma head of pancreas c) Periampullary carcinoma d) Calculi in the ampulla of vater Ans:b 54. Which of the following is not a contra indication for I VP? a) Renal infection b) Hyperpyrexia c) Multiple myeloma d) Skeletal metastases Ans:d 55.Perihilar fluffy opacities on chest x-ray is seen in a) Pulmonary embolism b) Pericardial effusion c) Pulmonary arterial hypertension d) Pulmonary venous hypertension Ans:d 56.An aneurysm of the sinus of Valsalva usually arise from a) Right aortic sinus b) Left aortic sinus c) Posterior aortic sinus d) pulmonary outflow tract e) Right ventricle Ans:a 57.Sequestration lung is best diagnosed by a)C.TScan b) M.R.I. c) Barium swallow d) Angiography Ans:d 58.Superior Orbital fissure best view is a) Plain AP view b) Cladwell c) Townes d) Basal view Ans:d 59.Which imaging method is ideal in evaluating hypertension ? a) Angiography b) Colour flow Doppler c) M. R. angio d) C. T scan Ans:c 60.Commonest cause of intracranial calcification is a) Pineal calcification b) Intracranial aneurysm c) Meningioma d) Tuberculoma Ans:a 61. Isotope used in myocardial perfusion scan is a) Technetium b) Thallium c) Stannous pyrophosphate d) Gallium Ans:b 62. Best diagnostic procedure in acute pancreatitis is a) CT Scan b) Ultrasound c) M. R. I. d) Pipida scan Ans:a 63. The most common cause of spontaneous pneumothorax is a) Rupture of subpleural blebs b) Pulmonary tuberculosis c) Bronchial adenoma d) Bronchogenic carcinoma Ans:a 64. Bull's eye lesion in ultrasonography is seen in a) Candidiasis b) Aspergillosis c) Sporotrichosis d) Cryptococcosis Ans:a 65. Newborn Chest x-ray with Respiratory distress shows multiple air containing lesions in Left Hemithorax and mediastinal shift is suggestive of a) Neonatal emphysema b) Diaphragmatic hernia c) Pneumatocele d) congential lung fcysts Ans:b 66. Radiologically appreciable earliest sign of osteomyelitis is a) Loss of muscle and fat planes b) Periosteal reaction c) Callus formation d) Presence of sequestrum Ans:a 67. Hilar dance on fluoroscopy is seen in a)ASD b)TOF c)VSD d)TGV Ans:a 68.Obliteration of Left heart border in PA chest X-ray is suggestive of a) Lingular pathology b) Left upper lobe lesion c) Left hilar lymph nodes d) Left lower lobe lesion Ans:a 69.Which of the following is the best test for screening a case of proximal internal carotid artery stenosis a) Digital subtraction angiography b) Magnetic resonance angiography c) colour Doppler ultrasonography d) CT angiogram Ans:c 70.In a case of renal failure with total anuria, ultrasound was found to be normal. Next line of investigation is a) Retrograde pyelography b) IVP c) Anterograde pyelography d) DTPA renogram Ans:b 71. In the plain film of the abdomen small bowel obstruction can be diagnosed by a) Central location b) Volvulae connivantes can be made out c) In the erect film, air fluid levels d) All of the above Ans:d 72.The following is not true of MRI a) Imaging perfusion of brain d) Superior to CT scan for bone scanning c) Blood vessels visualized without contrast b) presence of Hydrogen ions Ans:a 73.Hydrocephalus in children, first seen is a) Sutural diastesis b) Post clinoid erosion c) Large head d) Thinned out vault Ans:b 74. The characteristic X-ray feature of Pancoast tumour is a) Coin shadow b) Apical consolidation c) Apical mass lesion with erosion of neck of 1 & 2 ribs d) Hilar mass Ans:c 75.In nephrogram, one sees a) Renal capillaries b) Renal pelvis c) Only renal cortex d) Collecting tubules Ans:d 76.Ultrasonogram is not useful in a) CBD stones at the distal end of the CBD b) Breast cyst c) Ascites d) Full Bladder Ans:a 77.Suprasellar calcification is seen in a) Craniopharyngioma b) Meningioma c)Conray480 d) Conray 540 Ans:a 78.IVP is done using a)Conray240 b)Conray380 c) Calcified pineal gland d) Pituitary adenoma Ans:c 79. Calcification in Heart Wall is suggestive of a) Scleroderma b) Carcinoid Syndrome c) Fibroelastosis d) Endomyocardial ibrosis Ans:b 80.Contrast used in liver scan is a) Biligraffin b) 1131 Rose Bengal c) Gallium 238 d) Thallium 201 Ans:b 81.Best position for chest X-ray to detect Left Pleural effusion is a) Left lateral b) Supine c) Left lateral decubitus d) Right lateral decubitus Ans:c 82.The number of carpal bones seen in a radiograph of an infant is a)0 d)5 c)3 b)2 e)6 Ans:c 83.Investigation of choice to demonstrate vesico ureteric reflex a)IVP b) Ultra sound c) contrast MCU d) Cystoscopy Ans:c 84.Parallel shotgun appearance on ultrasound is seen in a) Portal hypertension b) Biliary ascariasis c) Obstructive jaundice d) Sclerosing cholangitis Ans:c 85.Radiolucent munilocular cyst of the body of mandible is a) Abscess d) Adamantinoma c) Dentigerous cyst d) Adamantinoma Ans:d 86)Best method of detecting minimal bronchiectasis is a) Abscess b) Dental cyst c) Dentigerous cyst d) Radio nuclide lung scan Ans:c 87.The photosensitive material used in X-rays films consists of a) Cellulite b) Silver bromide c) Zinc sulphide d) Cadmium tungstate Ans:b 88.Water lilly appearance in chest X-ray is suggestive of a) Bronchiectasis b) Bronchopleural fistula c) Hydatid cyst d)Sequestration cyst lung Ans:c 89. Retroperitoneal air is not manifested by air along a) Psoas margins b) Perinephric area c) Along spleen d) Adrenals Ans:c 90.The cause of homogenous opacity on X-ray is all except a) Pleural effusion b) Diaphragmatic Hernia c) Massive consolidation d)Emphysema Ans:d 91.1ntracranial calcification in skull X-rays may be a) Pineal calcifications b) Dural calcifications c) Cysticercosis d) All of the above Ans:d 93.Parasites that may show calcification on radiographs include a) Cysticercosis b) Guinea worm c)Amoebiasis d) Loa Loa Ans:a 94.Investigation of choice for Multiple sclerosis a) MRI b) CT Scan c) X-ray d)EEG Ans:a 95.Investigation of choice to diagnose sub arachnoid haemorrhage a) MRI angiography b) 4 vessel carotid angiography c) CT scan d) T2 wave MR Ans:b 96.Pulmonary embolism is best diagnosed by a)ECG b) Perfusion scan c) Angiography d) Plain X-ray Ans:c 97.Radiological signs of perforated viscus include a) Gas under the dome of the diagphram b) Falciform ligament is visualized c) Air surrounding the bowel is present d) All of the above Ans:d 98.Stryker's view is used in shoulder joint to visualize a) Muscle calcification b) Recurrent subluxation c) Sub acromial calcification d) Bicipital groove Ans:b 99. The investigation of choice in acute renal failure with complete anuria and normal USG a) Renal angiography b) DPTA c) IVP d) Retrograde pyelography Ans:b 100. 'H'shaped vertebra is seen in a) Phenylketonuria b) Sickle cell anemia c) Hemangioma d) Osteoporosis Ans:b RADIOLOGY Questions and Answers pdf Download Read the full article
0 notes
Text
Stuff I Learned: Sunflower VI
Chapter 20: Liver disorders
DDx of prolonged NNJ
Unconjugated: breast milk, infection, hemolytic anemia, hypothyroidism, upper GI obstruction, Crigler-Najar
Conjugated
Post-hepatic: biliary atresia, choledochal cyst
Hepatic: neonatal hepatitis syndrome (congenital infection, inborn errors of metabolism, AAT deficiency, galactosemia, tyrosinemia, errors of bile acid synthesis, progressive familial intrahepatic cholestasis (PFIC), cystic fibrosis, intestinal failure-associated liver disease associated with long-term parenteral nutrition)
Biliary Atresia
1 in 14,000
Progressive destruction or absence of biliary ducts
Diagnosed with TIBIDA radioisotope scan showing good uptake by liver but no excretion into bowel
Kasai operation = hepatoportoenterostomy, 80% success if performed before 60 days old
AAT Deficiency
Presents with bleeding due to vitamin K deficiency and prolonged NNJ
50% have good prognosis
Galactosemia
1 in 40,000
Liver failure, cataracts, developmental delay
Alagille Syndrome
Intrahepatic biliary hypoplasia
Autosomal dominant
Triangular facies, skeletal abnormalities, peripheral pulmonary stenosis, renal tubular disorders, FTT, eye defects
Hepatitis B
Give anti-HBs antibodies if mother is HBsAg positive
Additional HBIG if mother is HBeAg positive
Acute liver failure
Maintain blood glucose
Prevent sepsis
Prevent hemorrhage
Treat cerebral edema
Reye Syndrome
Acute non-inflammatory encephalopathy with microvesicular fatty infiltration of the liver
The commonest beta oxidation defect, medium-chain acyl-CoA dehydrogenase (MCAD) deficiency, presents with Reye-like syndrome
Autoimmune Hepatitis
7-10 years old
Congenital hepatic steatosis
Over 2 years old
Hepatosplenomegaly, abdominal distension, and portal hypertension
Liver function tests are normal in the early stage
Fat soluble vitamins
Vitamin A, E, D, K
Vitamin E deficiency causes peripheral neuropathy, hemolysis, and ataxia
Vitamin D resistant rickets indicate renal tubular acidosis
1 note
·
View note
Text
Clinical Case Reports – 1970 by P. Syamasundar Rao in Journal of Clinical Case Reports Medical Images and Health Sciences
Abstract
In this paper five case reports were presented and include congenital pulmonary cyst, Wilson-Mikity syndrome, diaphragmatic eventration; foreign body in the bronchus, and cor pulmonale that developed after implantation of a ventriculo-atrial shunt with a Pudenz-Heyer valve for treatment of hydrocephalus. For each case report, clinical, chest x-ray, electrocardiogram and other pertinent findings were presented. This was followed by discussion of etiology, diagnosis, and treatment options, as appropriate.
Keywords: congenital pulmonary cyst; diaphragmatic eventration; Wilson-Mikity syndrome; foreign body in the bronchus; cor pulmonale
Introduction
During the academic clinical practice for over five decades, the author had the unique opportunity to observe and document many interesting clinical case scenarios. The purpose of this review is to revisit these interesting cases. Because of the voluminous amount of this material, the material may be divided into a five-part series. Each of these case reports, while rare and important clinical observations, do demonstrate a clinical point that is useful to the pediatricians, pediatric cardiologists and/or other physicians.
Congenital Pulmonary Cyst
Case Report
A female infant with a birth weight of 6 lb 7 oz, born after a full-term, normal pregnancy and delivery with an Apgar score of 9 presented at three weeks of age with a two-week history of tachypnea. There were no other symptoms and the infant’s physical examination was normal except for tachypnea (respiratory rate of 50 per minute) and mild inter-costal and sub costal retractions. A chest roentgenogram was obtained (Figure 1) which was interpreted as pulmonary cyst. The heart was pushed to the right by the cyst (dextroposition of the heart). At thoracotomy, a huge lung cyst, involving the lower lobe of the left lung, was found, and was resected and the patient made an uneventful recovery.
Discussion
Congenital pulmonary cysts in the neonate are uncommon and are considered as errors in embryological development. They are of several categories namely, bronchogenic cell, alveolar cell, and combined cell types, based on the cellular component of the cell wall of the cyst. The symptoms depend largely upon the size of the cyst. These patients may not be discovered until a chest x-ray is performed for other reasons or may present with symptoms of tachypnea, dyspnea, and cyanosis in the neonatal period secondary to compression of lung tissue. The findings depend upon the size and location of the cyst. Dextroposition of the heart or tracheal shift and hyper-resonance, diminished breath sounds, and rales may be detected on physical examination. The chest x-ray findings may demonstrate a cyst, as in our case (Figure 1) or may be misinterpreted as pneumothorax. Other conditions simulating the cyst are staphylococcal pneumonia, diaphragmatic hernia, congenital lobar emphysema, sequestrated lobe, and hydro-pneumothorax or pyo-pneumothorax. In symptomatic cases, cystectomy, segmentectomy, lobectomy, or pneumonectomy, depending upon the size and location of the cyst is suggested. Percutaneous aspiration of the cyst is not recommended except as an emergency measure to relieve the tension. Some authorities advocate no surgical intervention because of the possibility of spontaneous regression of the pulmonary cysts, but most authorities recommend surgical excision of the cysts [1].
Late Respiratory Distress in a Premature Infant
Case Report
A premature male infant was born at 25 weeks of gestation and weighed 2 lb 12 oz at birth. Abruptio placenta and prolapse of the umbilical cord complicated the delivery and required resuscitation with oxygen. The chest x-ray was normal at that time. The baby was placed in an incubator in 35 percent oxygen, which was discontinued within 24 hours. At the age of 31 days, tachypnea and recurrent apnea with cyanosis developed. Auscultation revealed bilateral rales in the chest, again necessitating resuscitation with O2, administered by bag and mask. Chest x-ray revealed a diffuse parenchymal reticular pattern with multifocal areas of radiolucency. This roentgenographic pattern, along with the clinical findings, is essentially diagnostic of the Wilson-Mikity syndrome.
Figure 2: Chest x-ray in posterio-anterior view demonstrating a diffuse parenchymal reticular pattern with multifocal areas of radiolucency. This roentgenographic pattern, along with the clinical findings, is essentially diagnostic of the Wilson-Mikity syndrome. Reproduced from Rao PS. Chest 1970; 57:495-6.
Discussion
Wilson an Mikity originally described this condition in 1960, and is now called Wilson-Mikity syndrome.2 The etiology is not clearly understood but is considered to be due to pulmonary dysmaturity with uneven postnatal development of pulmonary alveoli in the premature infants.2 No consistent relationship with O2 therapy has been established. Bronchopulmonary dysplasia is another condition seen in the neonatal period and should be distinguished from Wilson-Mikity syndrome. The cystic appearance on the chest x-ray in the third stage of bronchopulmonary dysplasia resemble those of Wilson-Mikity syndrome; however, it follows treatment of severe hyaline membrane disease with high concentrations of O2 and artificial ventilation.2 The clinical presentation of Wilson-Mikity syndrome is characteristic in that the infant is premature with minimal or no respiratory distress at birth but, develops progressive respiratory distress, with dyspnea, tachypnea, cough, cyanosis, and rales in a few days to weeks. Diffuse reticular pattern of both lungs with areas of multifocal radiolucency are usually seen, similar to those seen in figure 2. Progressive pulmonary insufficiency with signs of right heart failure develop in patients with fatal outcome. But, about half of the patients eventually recover from their pulmonary disease. Pulmonary function studies are abnormal with decreased lung compliance, increased expiratory flow resistance, and increased breathing effort. Respiratory acidosis develops in spite of increased minute volume. Arterial O2 desaturation is thought to be secondary to intrapulmonary right-to-left shunting.2 The treatment is largely supportive [2].
Fever, Vomiting and Dome-Shaped Density in Right Thorax
Case Report
A four-month-old boy presented with a history of fever, poor feeding, vomiting, and slight cough for two days. Past history is essentially normal except for an Apgar score of 6 at birth. Breath sounds were diminished at the right base. Laboratory studies were normal. Chest x-ray (Figure 3) was performed which revealed a dome-shaped density in the right thorax which did not coincide with any pulmonary lobe or segment. The elevation of the inferior liver margin in the abdomen indicated that the abnormal shadow was liver. Based on these findings eventration of the right hemi-diaphragm was suspected. To confirm the diagnosis, a diagnostic pneumoperitonium was performed which confirmed the diagnosis.
Discussion
Eventration of the diaphragm is classified into adult and infantile types [3]. It is generally thought to be the result of congenital mal-development of the diaphragmatic musculature. However, such an abnormality may occasionally be caused by phrenic nerve injury during birth. The true incidence of eventration is not known, but in mass x-ray surveys of adults, it was found to be one in 10,000 [3]. Total eventration is thought to be more common on the left side and partial eventration on the right [3].
Clinical findings largely depend on the extent of eventration. There may be no symptoms or the patient may present with dyspnea, tachypnea, and cyanosis in the newborn period, requiring immediate treatment. Seesaw cyclic motions of the epigastrium with respiration and Hoover's sign (uninhibited divergence of costal margin from midline on inspiration), if present, are helpful in making the diagnosis. Percussion on the affected side may be dull or tympanic depending on the organs migrated under the diaphragm.
Fluoroscopy and chest x-rays are generally useful in arriving at the diagnosis. In right-sided eventrations, the lesser amount of liver shadow in the abdomen, i.e., elevation of the inferior margin of the liver helps to distinguish eventration from the other conditions [3]. Diagnostic pneumoperitonium is likely to establish the diagnosis, but the current availability of ultrasound technology, diagnostic pneumoperitoneum may not be necessary at the present time.
Symptomatic newborns with diaphragmatic eventration should be treated surgically; plication of the eventrated diaphragm is successful in relieving the symptoms with good long-term results. Some authorities suggest that asymptomatic patients also should be addressed surgically [3].
Foreign Body (Peanut) in The Left Main Stem Bronchus
Case Report
A 13-month-old girl with a history of poor appetite, loss of weight, cough, and intermittent low grade fever was admitted to the hospital for evaluation and treatment. No history of choking episodes was elicited. History revealed that a relative who had active pulmonary tuberculosis lived with the infant's family for a short period of time four months prior to the current admission. Because of this reason, the local health department performed tuberculin skin test which was positive and treatment with isoniazid was initiated. On examination her weight and height were between the third and tenth percentile. Decreased breath sounds on auscultation and hyper tympanic note on percussion were noted over the left side of the chest.
Intermediate strength purified protein derivative (PPD) was positive. Chest roentgenograms were obtained . Based on the history, physical examination, and chest x-ray findings, a diagnosis of endobronchial tuberculosis was entertained. However, prior to beginning treatment, bronchoscopy was performed to appraise the extent of airway encroachment.
Discussion
Autoimmune encephalitis is a condition that can be easily missed as it is not commonly considered in the differential diagnosis of various medical presentations. However, such diagnosis should be always taken into consideration when a person, particularly a child, presents with a new onset of refractory status epilepticus (NORSE) and/or new behavioral or psychiatric conditions. An early diagnosis of AE is essential, as the treatment is different from other conditions. With correct timely interventions the outcome is frequently favorable.
Though SARS-Cov-2 virus rarely invades the nervous system, Covid-19 infection frequently causes neurological symptoms like headache, delirium, anosmia, and dysgeusia [14]. One of the mechanisms of indirect nervous system involvement is through inflammatory response and immune dysregulation. There are few recorded cases of indirect involvement of CNS by auto-antibodies that are directed against the surface and synaptic protein. This case is one of the rare cases of Anti NMDA antibody autoimmune encephalitis that is associated with Covid-19 infection [15]. It indicates that in the era of COVID-19, high vigilance is required as a possible association may increase AE incidence.
A recent systemic review that analyzed 16 studies, including a total of 161 patients with NORSE [16], showed that the most frequent cause was AE. In addition to the well-known association with teratoma and cancer, AE, and specifically Anti-NMDA receptor Ab encephalitis, could be associated with a SARS‑CoV‑2 infection, either concomitantly or as post-infection manifestation. In this reported case, immunotherapy, in addition to anti-seizure medication, showed to be effective.
The main limitation of this report is the relatively short follow-up period. Observation of the child is ongoing to detect possible medium- or long-term consequences.
Positive PPD in an infant with poor appetite, loss of weight, and fever is suggestive of primary tuberculosis. This is particularly so given the patient's exposure to a subject with active pulmonary tuberculosis. The x-rays show hyper aeration of the left lung with a shift of the heart and mediastinum to the right. The left leaf of the diaphragm is also flattened. While there are no areas of infiltration or consolidation were seen, prominent shadows suggesting enlarged lymph nodes were seen . Endobronchial tuberculosis with compression of the bronchus by adenopathy may produce changes seen figure 5.
Discussion
Even though there was no history of choking or aspiration, the possibility of foreign body aspiration should be considered in this age group. Consequently, bronchoscopy was performed which revealed a peanut in the left main stem bronchus and was extracted during bronchoscopy. The peanut and the adjacent edema of the bronchus caused partial bronchial obstruction and acted as a check valve, so the air entered the left lung but, unable to leave the left lung since the bronchus becomes smaller during expiration, producing the roentgenographic appearance shown in figure 5. The baby improved and the treatment with isoniazid was continued because of the positive PPD.
Cor Pulmonale as a Complication of Ventriculoatrial Shunts
Introduction
Cerebral ventricle-to-right atrial shunts with Pudenz-Heyer or Spitz-Holter valves were widely used to treat hydrocephalus in the 1960s. Development of pulmonary hypertension with chronic cor pulmonale is rare with these shunts. We reported a patient who developed such a complication along with description of specialized pulmonary function studies in the early detection of such complication [5].
Case Report
An 11-year-old white boy was hospitalized in April 1969 with a history of progressive weakness, dyspnea, and pedal edema. He was diagnosed to have hydrocephalus and had a ventriculo-atrial shunt with a Pudenz-Heyer valve implanted at the age of 6 months. The shunt was thought to be functioning well when he was evaluated at the age of 2 years. He was asymptomatic until he was 9.5 years old, when he developed signs of congestive heart failure (CHF) and was treated at another hospital with digitalis and diuretics with some improvement. Right heart catheterization at the same institution revealed a mean right atrial pressure of 35 mmHg and right atrial angiography revealed slow emptying of the contrast, filling defects on the right lateral atrial wall and in the right and left pulmonary arteries. The ventriculo-atrial shunt was removed shortly thereafter. The patient was referred to our group for further evaluation and management [5].
Pertinent findings on examination included height and weight below the third percentile, head circumference above the 97th percentile, pretibial edema, prominent “a” wave in the left side of the neck, no venous pulsations on the right side, palpable right ventricular heave, markedly accentuated single second heart sound, an audible fourth heart sound at left lower sternal border, a Grade I/VI ejection systolic murmur at the mid-left sternal border, liver edge palpable 5 cm below the right costal margin, clear lung fields on auscultation, and normal neurological examination.
Electrocardiogram (ECG) and the vectorcardiogram (not shown) revealed right atrial and ventricular hypertrophy. Chest roentgenogram showed moderate cardiomegaly and prominent main pulmonary artery (PA) segment and clear lung fields. Lung scan with 131I-labeled macro-aggregated albumin was suggestive of multiple pulmonary emboli. Blood gas analysis showed pH 7.56; PaO2 80 mmHg, PaCO2 23 mmHg and bicarbonate 24 mEq/liter. Routine pulmonary function studies revealed restrictive lung disease. The ratio of wasted ventilatory volume (physiological dead space) to tidal volume (VD:VT) using Bohr's equation was 0.58 (normal 0.3 or less).
Vigorous treatment with digitalis and diuretics resulted in only temporary relief. During the next year, he continued to deteriorate and died of intractable right ventricular failure. Postmortem revealed right atrial thrombosis, severe right ventricular hypertrophy, multiple thrombo-emboli in the large and medium-sized pulmonary arteries, and intimal proliferation of the pulmonary arterioles.
Discussion
The case presented demonstrated development of cor pulmonale secondary to pulmonary thrombo-embolism which was produced by thrombi that arose following a ventriculo-atrial shunt with a Pudenz-Heyer valve for treatment of hydrocephalus. The causes of thrombo-embolic complications were not well understood, but the hypotheses, as reviewed by us [5], include infection, periarteritis due to autoimmune reaction of the pulmonary vessels to protein of cerebrospinal fluid, release of brain thromboplastin resulting in thrombosis at the point of contact with plasma coagulation factors, and simply the presence of a foreign body in the cardiovascular system for prolonged periods of time.
Early detection of pulmonary hypertension by periodic (every six months) evaluation by chest x-ray and ECG studies was suggested by some investigators, but early detection of pulmonary hypertension is of limited value since obstruction of 60% of the pulmonary vascular bed occurs by the time pulmonary hypertension develops [5]. Detection of multiple filling defects on radioisotope scanning in a child with a ventriculo-atrial shunt would be suggestive of pulmonary embolization and might be useful in early identification. Based on the observations of Nadel and associates [6] and those of ours [5], we suggested that specialized pulmonary function studies such as VD:VT, pulmonary diffusing capacity, pulmonary capillary blood volume, blood gas, and pH be performed periodically to detect obstruction of pulmonary vasculature prior to the development of pulmonary hypertension and cor pulmonale [5]. However, it should be noted that ventriculo-atrial shunts are no longer performed to treat hydrocephalus, but instead ventriculo-peritoneal shunts are used at the present time.
In summary, a rare case of pulmonary thrombo-embolism with resultant pulmonary hypertension and cor pulmonale following ventriculo-atrial shunt for hydrocephalus was presented with the recommendation to use of special pulmonary function studies for early detection and if found to be positive, immediate removal of the shunt system may eliminate further embolization into the lungs and prevent irreversible pulmonary vascular disease.
#congenital pulmonary cyst#diaphragmatic eventration#Wilson-Mikity syndrome#foreign body in the bronchus#cor pulmonale#Clinical Case Reports and Studies.
1 note
·
View note
Text
Global Angiography Devices Market
Global Angiography Devices Market Size, Share, Growth, Industry Trends and Forecast 2020-2030
The global angiography device market was valued at USD 11.2 billion in 2020 and is projected to reach USD 18.1 billion by 2030 at a CAGR of 4.8% during the forecast the period.Angiography is a medical treatment process of imaging the blood vessels by injecting the agents like iohexol and iopamidol. These agents are injected through a narrow tube known as a catheter placed directly into the veins or arteries, and this process is called angiograms. Angiogram, the process is used to detect any blockage of blood vessels or any abnormalities within the same all the way through the circulatory system. It is also used to diagnose kidney functions, heart diseases, blood clots, detects kidney cysts or tumors, and aneurysm, also known as abnormal bulging of veins or arteries causing hemorrhage. Through this process, an image of vessels or you can say a map is created before treating any diseases and for doing neurosurgery. This global angiography market is projected to grow consistently during the forecast period due to the technical advancement, growth of cardiovascular diseases, and demand for angiography as a diagnostic test for determining several diseases. According to the World Health Organization, deaths of 17.3 million occur per year due to cardiovascular disease and this number is expected to grow by 18.1 million by 2030. In the year 2015, cardiovascular related deaths were counted to be 31% of all global deaths, an estimated 7.4 million deaths occurred due to coronary disease and 6.6 million were due to stroke.
Download Sample Copy of the Report to understand the structure of the complete report (Including Full TOC, Table & Figures) @ https://www.decisionforesight.com/request-sample/DFS020152
Market Dynamics and Factors:
The surge of coronary diseases has resulted in more demand for angiographic devices, the introduction of improved technology-based products, increasing numbers for minimally invasive procedures are the factors propelling the market growth. However, the high cost of devices and stringent regulatory conditions has slowed down the market growth. Also, the advancement of technology in the coming future will introduce more technologically advanced devices that will propel the market growth. Moreover, due to lack of government funding and easy transfer of technology will prevail in the angiography devices market growth.
Market Segmentation:
Global Angiography Devices Market – By Product
Vascular Closure Devices
Accessories
Guide-Wires
Balloons
Catheters Tube
Angiography System
Contrast Media
Global Angiography Devices Market – By Indications
Valvular Heart Disease
Congestive Heart Failure
Known/Suspected CAD
Congenital Heart Disease
Others
Global Angiography Devices Market – By Technology
X-RAY Angiography Devices
CT Angiography Devices
MRI Angiography Device
Global Angiography Devices Market – By Devices
Coronary Angiography
Digital Subtraction Angiography (DSA)
Catheter Angiography
Magnetic Resonance Angiography (MRA)
Computed Tomography Angiography (CTA)
Conventional Angiography
Others
Global Angiography Devices Market – By Procedures
Coronary Angiography
Micro-Angiography
Non-Coronary Angiography
Renal Angiography
Cerebral Angiography
Pulmonary Angiography
Extremity Angiography
Others
Global Angiography Devices Market – By Application
Therapeutic
Diagnostic
Global Angiography Devices Market – By End-Users
Academic Research Laboratories
Hospitals
Diagnostic Centers
Ambulatory Surgical Centers
Others
Global Angiography Devices Market – By Source
Nuclear Reactors
Cyclotrons
Global Angiography Devices Market – By Radioisotope
Technetium-99
Gallium-67
Iodine-123
Iodine-125
18f, Rubidium-82
Yttrium-90
Lutetium-177
Others
Global Angiography Devices Market – By Type
PET/CT
SPECT
Therapeutics
Global Angiography Devices Market – By Geography
North America
U.S.
Canada
Mexico
Europe
U.K.
France
Germany
Italy
Rest of Europe
Asia-Pacific
Japan
China
India
Australia
Rest of Asia Pacific
ROW
Latin America
Middle East
Africa
New Business Strategies, Challenges & Policies are mentioned in Table of Content, Request TOC at @ https://www.decisionforesight.com/toc-request/DFS020152
Geographic Analysis:
North America has the largest market for angiography devices, followed by Europe due to the high technological advancement, less invasive procedures, availability of reimbursements, rising geriatric population, and high replacement rates of medical equipment in the angiography device market. Europe is the second-largest market after North America. The significant share of the European countries can be attributed to the high prevalence of cardiovascular diseases, high government investments, the faster product approval procedures, and rising adoption of the angiography devices due to a large number of angiography screening procedures.
Competitive Scenario:
Major key players in the angiography devices market are Boston Scientific Corporation, Market Drot, Canon Medical Systems Corporation, Abbott Vascular, Koninklijke Philips N.V, ST. Jude Medical, Merit Medical Systems, Inc, Medtronic Inc, Shimadzu Corporation, Toshiba Corporation, Philips Healthcare, Siemens Healthcare, Cordis Corporation (A Jnj Company), GE Healthcare and AngioDynamics, Inc.
Connect to Analyst @ https://www.decisionforesight.com/speak-analyst/DFS020152
How will this Market Intelligence Report Benefit You?
The report offers statistical data in terms of value (US$) as well as Volume (units) till 2030.
Exclusive insight into the key trends affecting the Global Angiography Devices industry, although key threats, opportunities and disruptive technologies that could shape the Global Angiography Devices Market supply and demand.
The report tracks the leading market players that will shape and impact the Global Angiography Devices Market most.
The data analysis present in the Global Angiography Devices Market report is based on the combination of both primary and secondary resources.
The report helps you to understand the real effects of key market drivers or retainers on Global Angiography Devices Market business.
The 2021 Annual Global Angiography Devices Market offers:
100+ charts exploring and analysing the Global Angiography Devices Market from critical angles including retail forecasts, consumer demand, production and more
15+ profiles of top producing states, with highlights of market conditions and retail trends
Regulatory outlook, best practices, and future considerations for manufacturers and industry players seeking to meet consumer demand
Benchmark wholesale prices, market position, plus prices for raw materials involved in Global Angiography Devices Market type
Buy This Premium Research Report@ https://www.decisionforesight.com/checkout/DFS020152
About Us:
Decision Foresight is a market research organization known for its reliable and genuine content, market estimation and the best analysis which is designed to deliver state-of-the-art quality syndicate reports to our customers. Apart from syndicate reports, you will find the best market insights, strategies that will help in taking better business decisions on subjects that may require you to develop and grow your business-like health, science, technology and many more. At Decision Foresight, we truly believe in disseminating the right piece of knowledge to a large section of the audience and cover the in-depth insights of market leaders across various verticals and horizontals.
Contact:
Email: [email protected]
For Latest Update Follow Us:
https://www.facebook.com/Decision-Foresight-110793387201935
https://twitter.com/DecisionFs
https://www.linkedin.com/company/decision-foresight/
0 notes
Photo

Bronchopulmonary dysplasia (BPS) is lung tissue that does not connect to the bronchial tree, so it doesn't get aerated. If its blood supply derives from the aorta below the diaphragm, it may be associate with other congenital abnormalities. By contrast, a congenital pulmonary airway malformation (CPAM) is a cystic structure that doesn't match blood supply with properly formed alveoli, so it is prone to filling with fluid. However, because it connects to the bronchial tree, air and pathogens can get in, so these are often removed at 4-6 months of age to reduce both the risk of recurrent infection and malignant transformation later in life.
Image: FIGURE 2C-13. Schematic drawings demonstrating the various differential diagnoses of neonatal chest lesions. (A) Normal lungs, with symmetric appearance; (B) hydrothorax, with fluid compressing and restricting growth of the normal lung; (C) CCAM, with cystic appearance and connection to the tracheobronchial tree; (D) BPS, depicting an anomalous blood supply to an aberrant lung tissue mass; (E) CDH, with bowel and stomach above the diaphragm; (F) bronchogenic cyst, centrally located and well defined. Liz PIttman, "Congenital Cystic Adenomatoid Malformation of the Lung," in Lung Pathology: Embryologic Abnormalities, from Neonatal Radiology Basics, page 2C-14.
35 notes
·
View notes
Text
Acne Occurs In A Minority (10 ) Of Patients - Acne Conglobata Acne Fulminans Acne Vulgaris
Went away in 3 days. Actually I got a bad breakout this past week even forcing myself to stay home being that I was emotionally wrecked about itbut it turns out it was folliculitis!!! Additionally, clinical evidence supports use of following OCPs for acne. Alesse, 'Diane 35', and Yasmin. Rare but more serious complications include thrombophlebitis, pulmonary embolism, and hypertension. Hormonal therapy is an established secondline treatment for female patients with acne. Needless to say, Oral contraceptives will be used cautiously in patients that smoke, have a history of hypercoagulable states, or breast cancer. Just think for a moment. Common consequences from combined oral contraceptive pills include nausea, vomiting, abnormal menses, weight gain, and breast tenderness.
The clinical signs of nonclassical CAH result from impaired aldosterone and also cortisol mediated negative feedback control of ACTH secretion.
Similarly treatment of acne in nonclassical CAH, that is often severe, cystic and refractory to antibiotics and isotretinoin, consists of low dose oral glucocorticoids which counteract adrenal androgen production, specifically, low dose oral prednisolone or dexamethasone.
Treatment of CAH therefore consists of substituting cortisol and/ or aldosterone daily. Still, patients must sign a consent form acknowledging they are aware of this potentially lifethreatening risk and physicians should monitor for signs and symptoms of depression throughout course of treatment. A true causal relationship between two has not been proven. Data regarding a possible association between depression and an increased risk of suicide during treatment with isotretinoin is unclear. In contrast to pical antibiotics, microbial resistance to BPO has not been reported. Actually, It is therefore preferable to pical antibiotics for 'long term' use and maintenance therapy.
So it's effective when used alone or when combined with pical retinoids, as previously mentioned. Benzoyl peroxide is a potent bacteriocidal agent that primarily works by reducing acnes within tofollicle. Nodulocystic acne and is commonly used in any significant acne unresponsive to therapy that results in significant physical or emotional scarring, it had been 'FDA approved' for patients with severe pyoderma faciale, and acne fulminans. While reducing presence of acnes and exerting 'antiinflammatory' effects, Isotretinoin works by normalizing epidermal differentiation, markedly decreasing sebum production. Therapy is generally initiated at a dose of 5 mg/kg/d for 4 weeks, after that, increased to 0 mg/kg/day as lerated and continued until a cumulative dose of 120 150" mg/kg is achieved. Negative psychological outcomes like anxiety, depression, and social withdrawal, are widely reported among individuals with acne and acne scars.
Now this should be noted and an appropriate referral to a psychologist or psychiatrist can be necessary if severe, So in case patient complains of significant anxiety or depression.
That said, Therefore if a patient notes ingestion of a certain food exacerbates their acne, that food can be avoided in that individual.
In most patients with acne, specific changes to diet are not recommended. The data on effects of diet on acne is still shouldn't be a substitute for standard acne treatment. Can be warranted if acne is very abrupt in onset or accompanied by other signs of hormonal or metabolic imbalance similar to hirsutism, hair loss, and akin signs of virilization, labwork is rarely necessary in diagnosis of acne, especially in adolescent population. Onset of acne in midchildhood always warrants a complete evaluation for causes of androgen excess. Of course to Now please pay attention. Patients might be asked about presence of hair loss, hirsutism, irregular menses, and arthritis, that are commonly associated features of these syndromes.
There are a few complex syndromes where acne or acneiform eruptions should be a regular presenting feature. Warning signs to suggest that acne can be part of an underlying medical syndrome include acne that is very severe, treatment resistant, diffuse in presentation or sudden in onset. One must entertain possibility of PAPA and SAPHO syndromes, if there are arthritic complaints. Vigilance for possibility of hyperandrogenism should allow clinician to consider PCOS, 'HAIR AN', SAHA, and CAH syndromes. Triamcinolone acetonide is injected into selected cystic lesions using a 30 gauge needle. The maximal percentage of corticosteroid used per lesion shouldn't exceed 1 ml.
The risks of corticosteroid injections include hypopigmentation, atrophy, telangiectasias and needle tract scarring.
Treatment is generally only effective when used chronically and relapse was shown to occur shortly after cessation, there are currently unlikely to be 'cost effective' options for most patients, as mechanism of action of many current light treatments and lasers is by suppression of acnes activity.
It can be an ideal adjuvant therapy for strong link between diet and acne remains to be proven, A high glycemic diet was stipulated as a potential aggravator of acne. Genetic influences can influence severity of disease. Consequently, Additionally, while patients often report that their acne flares during periods of high stress, a strong causal association has not been shown. Dairy, particularly skim milk, has also been implicated as a possible aggravating factor in acne. These data need to be corroborated by clinical trials before recommendations to patients can be made. You should take it into account. As microcomedo is precursor to all acne lesions, so it is particularly important both comedones and papules/pustules.
Retinoids are anticomedogenic, comedolytic, have significant direct and indirect anti inflammatory effects, and prevent formation of new microcomedos.
Yeast, including Malessezia species, are thought to play a pathogenic role.
It generally resolves spontaneously. Neonatal acne affects about 20percentage of healthy newborns and typically presents as small inflamed papules and pustules on cheeks and nasal bridge. Consequently, Neonatal cephalic pustulosis is an alternate term used to describe this benign neonatal eruption. Just keep reading! Comedones are not present. Usually, whenever dissecting cellulitis of scalp and pilonidal cysts, Acne conglobata is included in follicular occlusion tetrad gether with hidradenitis suppurativa. Recurrences may occur, isotretinoin is most effective treatment. For instance, This form is notoriously difficult to treat and residual scarring is quite severe. Acne conglobata is another kind of severe, nodulocystic acne.
Numerous nodules melt gether into suppurative plaques. Combined adapalene and BPO has greater efficacy than monotherapy with either product alone with a cutaneous lerability that is comparable to adapalene monotherapy. For deep and inflamed cystic lesions, intralesional injection of corticosteroid can quickly improve both appearance and tenderness of these lesions. Larger nodulocystic lesions may require incision and drainage prior to steroid injection. It is thought to result either from elevated circulating androgen levels or increased sensitivity of pilosebaceous unit to androgens. Treatment consists of lifestyle modification, oral contraceptives, insulin sensitizing agents, and antiandrogens. Essentially, SAHA -The association of seborrhea and acne with hirsutism and also androgenic alopecia characterizes SAHA syndrome.
Acne occurs in a minority of patients. However, seborrhea is always present, The full clinical spectrum rarely occurs. Look for secondary changes just like scarring and postinflammatory pigmentary changes, as we are looking at important clinical findings that may alter your treatment strategy. Nevertheless, this may affect chosen formulation for pical medications, Note topatient's skin type. On physical examination, carefully note lesion morphology, including presence of comedones, inflammatory lesions, and nodules. Notice that Patients might be advised that local erythema, dryness, and itching commonly occur within first weeks of usage but these effects decrease with continued use. I know that the use of sunscreens is advised. I'm sure you heard about this. Additionally, a pustular flare of acne throughout the initial '34' weeks of treatment may occur, however it resolves spontaneously with continued usage. Irritation and thinning of stratum corneum may increase touser's susceptibility to sunburn, with continued use of pical retinoids. Fact, Laboratory studies should include TSH, LH/FSH, prolactin, '17hydroxyprogesterone', serum DHEAS, and tal and free testosterone. Essentially, A pediatric endocrinologist should've been consulted to evaluate child if any abnormal parameters are found.
The presence of acne in this age group warrants evaluation for hyperandrogen states including.
A full physical exam looking for secondary sexual characteristics, review of growth charts, and a bone age will be performed.
Additional evaluation includes ultrasound and MRI as indicated. Nevertheless, Cushing syndrome, congenital adrenal hyperplasia, premature adrenarche, gonadal or adrenal tumors, and precocious puberty. Of course Mid childhood acne presents after 1 year to 7 years. Anyway, For instance, acnes contains 'light sensitive' porphyrin compounds, that absorb visible light at a couple of wavelengths, particularly between 400 and 700 nm. Whenever causing formation of reactive free radicals, that damage lipids in cell wall of acnes, resulting in destruction of toorganism, Absorption of light excites porphyrin compound. Light decreases acnes levels by interfering with its normal metabolism. Many lasers and light sources emit at this desired wavelength, including intensed pulse light devices, PDLs, KTP lasers, orange/red light lasers or light sources. It is Women with PCOS frequently also suffer from acne, central obesity, hirsutism, alopecia and infertility. Biochemical markers of hyperandrogenism include elevated serum testosterone and an increased LH/FSH ratio greater than 2Treatment consists of weight reduction, insulin sensitizers just like metformin, and oral contraceptives.
PCOS should've been suspected in women whose acne is severe, persistent and resistant to conventional therapies. Acne is present in '23 35'percentage of women with PCOS. Side effects are 'dose related' and include potential hyperkalemia, irregular menstrual periods, breast tenderness, headache, and fatigue. These include trimethoprim sulfamethexazole, amoxicillin and identical penicillins, cephalosporins, and azithromycin. Data on their efficacy and safety ain't well established and their use in treatment of acne is generally discouraged. Several other oral antibiotics was used for treatment of acne. Of course, The androgen receptor blocker spironolactone is another second line option for females with inflammatory acne. It works by inhibiting 5ɑreductase and at doses of '50 100' mg twice daily, it was shown to improve acne. Salicylic acid is available in numerous over counter concentrations of up to 2 in lots of delivery formulations, including gels, creams, lotions, foams and solutions. It is available as a pical cream. Azelaic acid is applied twice daily and its use is reported to have fewer local consequences than pical retinoids.
It inhibits growth of acnes and improves both comedonal and particularly inflammatory acne.
Azelaic acid is a naturally occurring dicarwriteylic acid found in cereal grains.
Additionally, it can on the basis of age of patient as well as morphology and distribution of tolesions. It is available in a 10 lotion, either alone or in combination with 5percentage sulfur. Now look. Sodium sulfacetamide is an alternative well lerated pical antibiotic that is thought to restrict growth of acnes through competitive inhibition of condensation of paraaminobenzoic acid with pteridine precursors. Now let me tell you something. By nature they provide improved patient convenience, that may translate to improved adherence. Currently, adapalene is one pical retinoid to be formulated with BPO. Fixed dose' combination products with a pical retinoid and an antimicrobial are available. The first step is to complete a thorough history and physical examination. On p of that, Note clinical responsiveness and lerability to any prior treatments. In female patients, a menstrual and oral contraceptive history is important in determining hormonal influences on acne. Considering above said. Specifically ask about all prescription and overthecounter medications used for acne and similar conditions.
This will aftereffect to counsel patients on include gastrointestinal upset, most commonly experienced with doxycycline. They should also be avoided during pregnancy as they can negatively affect bone and cartilage growth of tofetus. Rare hypersensitivity reactions including serum sicknesslike reaction and DRESS syndrome are reported. Furthermore, All tetracyclines can cause photosensitivity and can cause staining of toteeth. Pseudotumor cerebri is a rare consequences seen with tetracyclines as well. Some patients noted health benefits beyond improved in acne like decreased facial oiliness, decreased hirsutism, improvement of premenstrual syndrome symptoms, decreased metrorrhagia, reduced endometriosis pain, and increased libido. Seriously. Again available data does not suggest a causal association but patients gonna be counseled appropriately on possible risk.
Similar controversies surround isotretinoin and risk of inflammatory bowel disease.
Whenever releasing lipases and identical enzymes, They are proinflammatory.
They also induce innate immunity inflammatory cascades, through 'toll like' receptor 2 and metalloproteinases. They was shown to activate inflammasomes as well. Increased colonization of acnes. Tretinoin/clindamycin is also available as a fixed dose combination product. Both clindamycin and erythromycin are available in pical combination formulations both with BPO which all had comparable efficacy and significantly reduced acne lesions. Topical BPO/erythromcyin will be refrigerated, that could impact adherence. These include. Basically, Systemic symptoms often accompany acne fulminans. Consequently, Scarring, often severe and keloidal, is inevitable. Acne fulminans is a severe, eruptive type of acne that primarily occurs in teenaged boys, ages '13 The' acne appears abruptly over face and upper body with uniform papules and friable nodules that can coalesce, suppurate and bleed. There is a lot more information about it on this site. Whenever affecting clavicle or sternum most commonly, can be associated, Osteolytic bone lesions. Anyways, Eythema nodosum is reported with acne fulminans as well. Ok, and now one of most important parts. Bleach resistant bedding is available at some major national retailers.
Patients will be advised that benzoyl peroxide is a bleaching agent and whitening of clothing, towels, and bedding can occur. Development of contact dermatitis to benzoyl peroxide is possible, and will be suspected in patients who develop marked erythema with its use. It is also important to speak frankly with patient and determine what effect acne is having on their quality of life. Stress is also often associated with flares, and So it's common for students to report that their acne appears to worsen around exam time or finals. Ask use of about cleansers, toners, and moisturizers, as harsher products may affect tolerability. Female patients may report a worsening prior to their menses. Patients may also report an exacerbation with certain foods although a clear association between any particular food and acne has not been proven. However, Five to 20 women percent are thought to suffer from this disorder. That's interesting right? Polycystic Ovarian Syndrome -The most common syndrome associated with acne is PCOS, an endocrine disorder characterized by polycystic ovaries, oligo and anovulation, and biochemical and also clinical signs of hyperandrogenism.
PCOS is also strongly associated with insulin resistance.
It is also less drying and has a milder after effect profile.
Patients going to be advised to use this in tomorning, as tretinoin is susceptible to oxidation by BPO, if BPO is also being used. Besides, Patients may be instructed to apply a 'peasized' quantity of retinoid all over their face, not merely active areas. Adapalene is light stable and resistant to oxidation by BPO, unlike tretinoin. If tretinoin has been used it must be applied at night to prevent early degradation as it's photolabile. Tetracycline absorption is affected by elemental ions including calcium, aluminum, iron, and zinc and therefore shouldn't be ingested with meals particularly those involving dairy products or antacids.
Minocycline and doxycycline are less influenced by foods and generally can be taken with food. Reconsider if patient isn't responding to oral antibiotic therapy as expected, as individual absorption rates and influences can vary widely. Their use and efficacy in treatment of acne isn't fully established. Other agents used for their anti inflammatory properties include nicotinomide, both pically and orally, and zinc. So use of pical retinoids, particularly tazarotene during pregnancy is discouraged, as retinoids are known teratogens. I'm sure it sounds familiar. Patients could be started on a lower concentration retinoid with gradual increase in strength and frequency as necessary, in order intention to minimize excessive dryness and irritation. Now regarding aforementioned fact... Frequency can be increased in stepwise '34' week increments as tolerated, alternatenight to every third night application should be necessary initially. Actually, Several medications are known to cause acne or acneiform eruptions.
A detailed medication history should always be taken, including use of vitamin, protein/muscle building supplements.
It can be important to ask about use of anabolic steroids in athletic young men.
B2, B6 and BIt is important to ask about use of pical cosmetics and hair products, as Surely it's useful to ask about patients' occupational history, including their hobbies, as these may result in aggravation of acne. Keep reading! Poor adherence to acne treatment plans is a typical cause of inadequate therapeutic response. Did you hear about something like that before? Discussion with patient about what they do not like about a certain product and substituting accordingly may will be clearly ascertained that patient was adequately using prescribed medication consistently and correctly. These include bar soaps, washes, gels and lotions that are available in concentrations of 5percentage, 5 and 10. The formulation is also an important cofactor in toproduct's irritancy. Many preparations of BPO are available in both overthecounter and prescription formulations. Higher concentrations of BPO should be more irritating and not necessarily more efficacious than lower concentrations. Notice, It is also a mild chemical irritant that works in part by drying up active lesions.
Salicylic acid is a comedolytic and mild antiinflammatory agent.
Patients with acne gonna be discouraged from using tanning as a treatment for acne.
Shortterm benefit is outweighed by to'long term' photodamage and increased risk of skin cancer, while tan may mask toacne. Oftentimes many sunscreens are labelled as non oily or 'non comedogenic', as with cosmetics. Sensitivity and phototype of topatient, when recommending a sunscreen for patients with acne consider tooiliness. Use of sunscreen in patients on medications that can cause photosensitivity, similar to retinoids or doxycycline, is a must and their use will be advocated with every visit.
This disorder affects approximately 1 of general population, is marked by signs of hyperandrogenism.
Additional signs in females include unrecognized genital structural defects, abnormal menstrual cycles or infertility.
This form is due to partial defects in '21 hydroxylase' and severity of presentation is highly variable. Adapalene is 'lightstable' and resistant to oxidation by benzoyl peroxide, unlike tretinoin. When applied to toskin, Tazarotene is also a synthetic receptor specific retinoid that is converted to its active metabolite, tazarotenic acid. This is where it starts getting very intriguing. Tretinoin was first pical comedolytic agent developed for treatment of acne. The most commonly utilized pical retinoids include. Adapalene is a synthetic retinoid that specifically binds retinoic acid receptor Ɣ. Current COC formulations combine an estrogen with a progestin with intention to minimize risk of endometrial cancer that is known to occur with unopposed estrogens. Of course, Patients going to be advised that clinical response to OCPs generally requires at least 3 months before one is able to determine efficacy. Oral contraceptive formulations with lowandrogenic progestins similar to drosperinone, norethindrone and levonorgestrel are preferred, because progestins have intrinsic androgenic activity.
Additionally, true acne vulgaris will be differentiated from acneiform eruptions. These include. Epidermal growth factor receptor inhibitor- induced eruption. In neonates, following differential diagnosis will be considered. I'm sure you heard about this. Adult acne is far more prevalent than originally thought. Women with hormonal abnormalities as well as diseases of insulin resistance just like polycystic ovarian syndrome, are at risk for development of acne. Besides, while affecting up to 85 of '1224' year olds, Acne is a similar disorder in adolescents. A patient with severe acne has high chances to report a family history of severe acne. On p of this, Additionally, these groups tend to have acne that is more severe and less responsive to traditional therapy. Other groups with an increased risk for development of acne include those with hyperandrogenism, hypercortisolism, precocious puberty and those with XYY genotype.
While postadolescent acne predominantly affects women, Adolescent acne appears to show a slightly more male predominance while.
Genetic influences and ethnicity also impact risk.
The reported prevalence of acne in women aged 30 39 years is 35. The use of makeup has not been shown to adversely affect a patient's response to acne treatment. Patients gonna be instructed to look on label for a 'water based', 'non comedogenic' formulation. Use of cosmetics can be very beneficial in covering up active acne and improving patient quality of life. Eventually, Additionally, it's crucial to counsel patients to discard any liquid make up that is expired. Now please pay attention. In darker skinned patients, post inflammatory hyperpigmentation is often present and can last for a couple of months after resolution of inflammatory acne, and in rare instances should be permanent. Known Scarring most often results from more severe inflammatory acne lesions but can occur with milder forms as well.
Additionally, it's vital to note presence of secondary changes of acne.
Keloids may form in 'at risk' individuals.
Can occur in fairly mild cases as well, they usually arise in cases of severe nodular acne. Lighter skinned patients may show postinflammatory erythema that also can take many months to improve. Fact, In women of childbearing age, two negative pregnancy test results are required before therapy can be started. Generally, Contraception counseling should also be seriously discussed and two effective forms of birth control gonna be used in women who are sexually active. Strict adherence to FDA mandated risk management program iPledge is vital, Additionally, isotretinoin is a potent teratogen. Several serious consequences of isotretinoin therapy exist including acne fulminans, formation of excessive granulation tissue, and an increased risk of cutaneous infections. Treatment involves oral glucocorticoids, that concomitantly helps treat toarthritis, pyoderma gangrenosum and acne conglobata. Keep reading! It results from mutations in gene that encodes prolineserinethreonine phosphatase interacting protein 1 and is part of a related group of inflammatory disorders that includes inflammatory bowel disease, uveitis, and psoriasis.
PAPA -The triad of sterile pyogenic arthritis, pyoderma gangrenosum, and acne conglobata characterizes PAPA syndrome. Disease modifying agents, biologic therapies and dapsone have also been shown to be efficacious. High rates of resistance been correlated with high outpatient use of antibiotics and selection pressure can affect other more pathogenic bacteria in addition to acnes. Additionally, antibiotic monotherapy either for acute treatment or maintenance therapy should've been avoided. With that said, Additionally, totetracyclines, particularly doxycycline, was implicated as a possible risk factor for inflammatory bowel disease duration of antibiotic use should've been limited to 3 months if possible and clinical response and need for continuation frequently assessed. Bacterial resistance is of concern with oral antibiotics, as with pical antibiotics. Oral dapsone can be used as a 3rd line treatment for severe acne in patients who can not take or have failed oral tetracycline and isotretinoin therapy. Now please pay attention. Patients should've been checked for G6PD deficiency prior to starting and monitored for hemolysis. Actually, I know it's preferable that pical antibiotics alone be avoided as monotherapy and could be paired with BPO, since of risk of antibiotic resistance.
They are available in various formulations from creams and gels to solutions and pledgets. Other commonly used antimicrobials include pical antibiotics like clindamycin and erythromycin. Spironolactone after effect are dose dependent and can also be minimized if therapy is initiated with a low dose and gradually built up as necessary. Similar to COCs, clinical response may take up to 3 months. Effective maintenance doses are in range of 25 to 200 mg/day. Mild consequences are often seen with isotretinoin use including. It has greater efficacy in treating inflammatory acne lesions than comedones. Topical use is safe in G6PD deficient patients and in those that are sulfa allergic. Use with BPO can cause a 'yellow orange' staining of skin and hair. In comment section. Topical dapsone is used for its antiinflammatory properties in treatment of acne vulgaris. Needless to say, most of us are aware that there is a risk of feminization of a male fetus if a pregnant woman takes this medication, as long as So it's a 'anti androgen'.
This potential risk can be minimized by combining spironolactone with an oral contraceptive, and has added benefit of combating potential symptoms of irregular menstrual bleeding, most common after effects of spironolactone.
The use of a couple of other systemic agents had been reported in generally in complicated cases of severe, refractory acne.
These include anti TNF alpha agents, entanercept and infliximab, and antiandrogens, just like flutamide. Eventually, Chemical peels are used both in treatment of comedonal acne and acne scarring. A various preparations in varying concentrations including glycolic acid, alpha and beta hydroxy acids and salicylic acid, have all been used. Comedo extraction can improve cosmetic appearance and aid in therapeutic responsiveness to prescribed comedolytic agents. Remember, Monthly pregnancy tests must be continued throughout the entire course of treatment. Although, Baseline laboratory testing before isotretinoin therapy is also recommended and generally includes cholesterol and triglyceride assessment and hepatic transaminase levels. These values could be rechecked once patient is at a steady dosing.
Hormonal therapies have demonstrated efficacy in adult women with persistent inflammatory papules and nodules that commonly involve lower face and neck.
These women also commonly report that their acne flares prior to their menstrual periods and consists of a few tender deep seated inflammatory papules and nodules.
As long as latter block both ovarian and adrenal production of androgens, In such patients, oral antibiotics can be discontinued and hormonal therapy with oral contraceptives initiated. These patients often note little improvement in their acne despite multiple courses of various antibiotics. Nodules and nodulocystic lesions are seen in more severe disease. While affecting up to 85 of 12 24 year olds, Acne is an exceptionally common disorder in adolescents. While involving toface, chest, shoulders and back, are hallmarks of acne vulgaris, The presence of inflammatory papules and pustules with comedones. In fact, most patients can accurately diagnose themselves. Secondary changes, like scarring and postinflammatory hyperpigmentation or erythema are common and could be documented, as they impact both management and disease outcomes. On p of this, Patients on isotretinoin are followed monthly for duration of their treatment in compliance with iPledge system.
Mild to moderate cases can be followed up at 3 4" month intervals once treatment is initiated.
Interim visits can be useful to establish lerability and compliance.
The patient 'followup' will depend on acne severity. Basically, If a patient does not appear to have adequately responded to treatment you have initiated after 2 3 diligent months use, an alternative treatment strategy gonna be considered. It may be stressed that significant improvement may not occur until 8 week mark or longer. Severe cases will be followed up more closely, at 23 month intervals. Cryotherapy represents another surgical option for treatment of comedonal acne. That's where it starts getting very interesting. The contents of open comedones can be expressed by use of a comedo extractor and toSchamberg, Unna and Saalfield kinds of comedo types expressers are most commonly used. Actually, Additionally, nicking surface of a closed comedo with a 18 gauge needle or a no. Notice, The algorithms below provide a treatment overview followed by specific algorithms for treatment of mild, moderate, and severe acne.
Evidence in sort of randomized control trials to prove clear effectiveness of these therapies is lacking.
There is also little standardized information available about longterm effects of such therapies or optimal device settings, or frequency of administration in active acne.
In addition there're no studies that actually compared lightbased treatments with current standard of 'carecombination' therapy with a pical retinoid plus one or more antimicrobial agents. SAPHO -This syndrome is a rare disorder, Ortho 'TriCyclen', and Yaz. Now regarding aforementioned fact... Additionally, light may also have endogenous antiinflammatory properties via action on inflammatory cytokines. Oftentimes They can also be used for scar revision once acne is under control. Light based treatments work by reducing acnes levels and also disrupting sebaceous gland function.
In addition to photodynamic therapy, YAG laser, '1450nm' diode laser. There are many surgical treatments available for treatment of acne including various lasers, like pulsed dye lasers, 1064 Nd. Treatment is indicated, as scarring commonly occurs in this age group. Acne in this age group is due to elevated androgen levels, including DHEAS resulting from an immature adrenal gland. Comedones are present, with variable inflammatory lesions. There's more info about this stuff on this website. Boys may also have increased testosterone production. Now look. Infantile acne generally occurs between 3 and 6 age months, lasting throughout first and into second year of life.
Apert syndrome -This congenital disorder is also known as acrocephalosyndactyly and results from mutations in FGFR2, that encodes fibroblast growth factor receptor.
Patients with Apert syndrome present with widespread acneiform papules, including entire extensor sides of toarms, buttocks and thighs.
This autosomal dominant disorder is also defined by disfiguring synostoses of bones of hands and feet, vertebral bodies, and cranium. Normally, however, isotretinoin was beneficial in severe cases, acneiform lesions of Apert syndrome are highly resistant to pical therapies. Some information can be found by going online. Light electrocautery and electrofulguration have also been reported as effective treatments for comedones and electrofulguration has added benefit of not requiring prior use of a pical anesthetic. On p of that, Laboratory studies are nonspecific but reflect degree of inflammation. That's where it starts getting really entertaining, right? Treatment of acne fulminans is aimed at controlling inflammation quickly while preventing an isotretinon associated flare.Typically oral corticosteroids are started with a gradual introduction of isotretinoin.
Abnormalities include leukocytosis, anemia, elevated erythrocyte sedimentation rate and proteinuria.
Pustules are similarly sized and filled with thick, white, purulent fluid.
Nodules are greater than 5cm and can be indurated and very tender. The clinically inflammatory lesions seen in acne vary from papules and pustules to more severe nodules and nodulocystic lesions. Papules are less than 5cm in size. The presence of nodules often correlates with greater acne severity. Forming large suppurative plaques that can result in persistent scarred sinus tracts, At times, nodules can combine. In adolescents and adults differential diagnosis is extensive and includes. Doesn't it sound familiar? Pseudofolliculitis barbae/acne keloidalis nuchae. The pathophysiology of acne vulgaris centers on pilosebaceous unit and is multifactorial.
0 notes
Text
300+ TOP PEDIATRIC SURGERY Objective Questions and Answers
PEDIATRIC SURGERY Multiple Choice Questions :-
1. Polyhydramnios is frequently observed in all of the following conditions except: A. Esophageal atresia. B. Duodenal atresia. C. Pyloric atresia. D. Hirschsprung's disease. E. Congenital diaphragmatic hernia. Answer: D 2. Which of the following statements about Hirschsprung's disease is/are true? A. There are no ganglion cells seen in Auerbach's plexus. B. There is an increased incidence of Down syndrome. C. It is more common in girls. D. It may be associated with enterocolitis. E. It may involve the small intestine. Answer: ABDE 3. Which of the following statements is/are true of infants with gastroschisis? A. It is associated with malrotation. B. There is a high incidence of associated anomalies. C. There is prolonged adynamic ileus following repair. D. It is complicated by intestinal atresia in 10% to 12% of cases. E. It is associated with chromosomal syndromes. Answer: ACD 4. In neonates with congenital diaphragmatic hernia, which of the following statements is true? A. The defect is more common on the right side. B. Survival is significantly improved by administration of pulmonary vasodilators. C. An oxygen index of 20 is an indication for extracorporeal membrane oxygenation (ECMO). D. Oligohydramnios is a frequent occurrence. E. Mortality is the result of pulmonary hypoplasia. Answer: E 5. Which of the following statements are true regarding the premature neonate? A. A 15% to 20% right-to-left shunt occurs across the foramen ovale and patent ductus arteriosus. B. Surfactant levels are normal after 30 weeks' gestation. C. Fluid requirements are higher than in a full-term baby. D. Rectal temperature is the best indicator of core body temperature. E. They are more at risk for infection than the full-term infant. Answer: ACE 6. In neonates with necrotizing enterocolitis, which of the following findings is an indication of significant bowel ischemia? A. Increased gastric residuals. B. Septic shock. C. Cardiac failure due to a patent ductus arteriosus. D. Elevated platelet count. E. Erythema of the abdominal wall. Answer: E 7. The treatment of choice for neonates with uncomplicated meconium ileus is: A. Observation. B. Emergency laparotomy, bowel resection, and Bishop-Koop enterostomy. C. Intravenous hydration and a gastrograffin enema. D. Emergency laparotomy, bowel resection, and anastomosis. E. Sweat chloride test and pancreatic enzyme therapy. Answer: C 8. The pentalogy of Cantrell includes all of the following except: A. Epigastric omphalocele. B. Sternal cleft. C. Intracardiac defect. D. Pericardial cyst. E. Ectopia cordis. Answer: D 9. In infants with duodenal atresia all the following statements are true except: A. There is an increased incidence of Down syndrome. B. Duodenal atresia can be detected by prenatal ultrasound examination. C. It may occur in infants with situs inversus, malrotation, annular pancreas, and anterior portal vein. D. It is best treated by gastroenterostomy. E. There is a high incidence of associated cardiac defects. Answer: D 10. The initial treatment of choice for a 2.5-kg. infant with a 20.0-cm. long proximal jejunal atresia and 8.0 cm. of distal ileum is: A. Laparotomy, nasogastric suction, proximal dilatation to lengthen the atretic jejunum, total parenteral nutrition, and delayed anastomosis. B. Laparotomy and proximal end-jejunostomy. C. Laparotomy and immediate small bowel transplantation. D. Laparotomy and double-barrel enterostomy (jejunum and ileum), with refeeding of jejunal contents into distal ileum and delayed anastomosis. E. Laparotomy, tapering jejunoplasty, and end-to-oblique jejunoileal anastomosis. Answer: E

PEDIATRIC SURGERY MCQs 11. A 2.8-kg. neonate with excessive salivation develops respiratory distress. Attempts to pass an orogastric catheter fail because the catheter coils in the back of the throat. A chest film is obtained and shows right upper lobe atelectasis and a gasless abdomen. The most likely diagnosis is: A. Proximal esophageal atresia without a fistula. B. Proximal esophageal atresia with a distal tracheoesophageal (TE) fistula. C. “H-type” TE fistula. D. Esophageal atresia with both proximal and distal TE fistula. E. Congenital esophageal stricture. Answer: A 12. Neonates with NEC may demonstrate all of the following findings on abdominal films except: A. Pneumatosis intestinalis. B. Portal vein air. C. Pneumoperitoneum. D. Colovesical fistula. E. Fixed and thickened bowel loops. Answer: D 13. The most common type of congenital diaphragmatic hernia is caused by: A. A defect in the central tendon. B. Eventration of the diaphragm in the fetus. C. A defect through the space of Larrey. D. An abnormally wide esophageal hiatus. E. A defect through the pleuroperitoneal fold. Answer: E 14. The calorie-nitrogen ratio for an infant should be maintained at: A. 75:1. B. 100:1. C. 50:1. D. 150:1. E. 25:1. Answer: D 15. All of the following conditions are derived from the primitive embryonic foregut except: A. Bronchogenic cyst. B. Cystic adenomatoid malformation. C. Gastric duplication. D. Mesenteric cyst. E. Pulmonary sequestration. Answer: D 16. For a 22-kg infant, the maintenance daily fluid requirement is approximately which of the following? a. 1100 ml b. 1250 ml c. 1550 ml d. 1700 ml e. 1850 ml Answer: c 17. Which of the following statements regarding nutritional requirements in infants are true? a. The total daily water requirement is estimated to be 100 ml/100 kcal ingested b. The resting energy expenditure is approximately twice that of an adult c. The highest rate of nitrogen retention with parenteral nutrition occurs in infants given approximately 40% of the calories as carbohydrate and the remainder as fat d. The protein requirement for a newborn infant is approximately 2.5 g/kg/day Answer: a, b, c, d 18. A term infant 48 hours of age suddenly develops hypoxemia, irritability, and glucose and temperature instability. Which of the following statements are true? a. Empiric antibiotic coverage for b-hemolytic Streptococci and Escherichia coli should be initiated b. An intravenous infusion of prostaglandin E1 should be initiated immediately c. Exogenous surfactant should be given immediately d. The mortality rate for this child is approximately 50% Answer: a,d 19. Which of the following statements about pulmonary surfactant are true? a. Endogenous surfactant deficiency is the key physiologic problem in preterm infants with the infant respiratory distress syndrome b. Surfactant function can be restored to normal using aerosolized phosphatidylcholine administration c. Exogenous surfactant replacement has been shown to reduce mortality in preterm infants with the infant respiratory distress syndrome d. Surfactant is produced by Type I alveolar epithelial cells Answer: a, c 20. Which of the following statements regarding premature infants are true? a. Complications of prematurity account for approximately 85% of fetal deaths b. Prematurity is defined by the World Health Organization as birth prior to 35 weeks gestation c. Infants with intrauterine growth retardation have physiologic problems which are more dependent on the birth weight than the gestational age d. Preterm infants are at increased risk for hypocalcemia and hypoglycemia when compared to term infants Answer: a, d 21. Other than the history and physical exam, which of the following tests is considered an essential feature of the preoperative evaluation of a patient with a suspected thyroglossal duct cyst? a. Cervical ultrasound b. Thyroid scan c. Serum T3 and T4 levels d. Needle aspiration e. None of the above Answer: e 22. Suppurative cervical lymphadenitis in a 3-year-old child is commonly related to which of the following organisms? a. Staphylococcus aureus b. Atypical mycobacterial organisms c. Streptococcal organisms d. Lymphoma with secondary pyogenic organisms e. Cat scratch Answer: a, c 23. Branchial cleft remnants most often present with which of the following clinical problems? a. Infection b. Airway obstruction c. Hemorrhage d. Malignant degeneration e. Pain Answer: a 24. Proximity to which of the following structures places it at risk during surgical excision of a second branchial cleft remnant? a. Internal carotid artery b. External carotid artery c. Hypoglossal nerve d. All of the above e. None of the above Answer: d 25. Standard therapy for acute epiglottitis in a child is: a. Tracheostomy b. Intravenous antibiotic treatment in an ICU setting c. Endotracheal intubation in the operating room and intravenous antibiotic therapy d. Indirect laryngoscopy and intravenous antibiotics e. Intravenous steroids and antibiotics Answer: c 26. Which of the following statements regarding congenital diaphragmatic hernia are true? a. The incidence of right and left-sided lesions is equal b. Malrotation is to be expected c. Left-to-right shunting via a patent ductus arteriosus is a serious but expected physiologic consequence of pulmonary hypoplasia d. Survival rates of 75% are reported in several contemporary series e. Congenital heart disease is present in approximately 20% of these infants Answer: b, d, e 27. Of the following cystic malformations of the tracheobronchial tree, which is most likely to be asymptomatic when discovered? a. Intralobar pulmonary sequestration b. Extralobar pulmonary sequestration c. Congenital cystic adenomatoid malformation d. Congenital lobar emphysema Answer: b 28. Infants with a double aortic arch most commonly present with which of the following problems? a. Dysphagia b. High output cardiac failure related to a patent ductus arteriosus c. Positional hyperemia and edema of the right upper extremity d. Symptomatic tracheal compression Answer: d 29. Which of the following is most common after primary esophagostomy for esophageal atresia with a distal tracheoesophageal fistula? a. Anastomotic leak b. Esophageal stricture c. Recurrent tracheoesophageal fistula d. Gastroesophageal reflux e. Tracheomalacia requiring aortopexy Answer: d 30. Which of the following is the most common primary lung tumor in infants and children? a. Pulmonary blastoma b. Squamous cell carcinoma c. Endobronchial carcinoid d. Leiomyoma e. Metastatic osteogenic sarcoma Answer: c 31. Which of the following statements regarding congenital chest wall deformities are true? a. Children with pectus excavatum deformities typically have physiologically insignificant limitation of exercise tolerance b. The rate of recurrence after operative repair of a pectus excavatum deformity is between 5% and 10% c. Pectus carinatum is the most common congenital chest wall defect d. The most common indication for operative repair of congenital chest wall deformities is cosmesis Answer: a, d 32. The definitive evaluation of a child with a suspected congenital cystic abnormality of the tracheobronchial tree is best done using which of the following? a. Rigid bronchoscopy b. Computerized tomography or magnetic resonance imaging c. Chest x-ray d. Angiography e. Barium esophagogram Answer: b 33. A newborn infant develops coughing, choking and cyanosis with his first feeding. He is noted to have excessive drooling. What are the important associated anomalies that must be screened for prior to surgical intervention? a. Right-sided aortic arch b. Hydrocephalus c. Genitourinary obstruction d. Congenital heart disease Answer: c 34. Which of the following ventilation strategies is the best initial approach for a neonate with a left congenital diaphragmatic hernia and the following post ductal arterial blood gases: PaO2 50 mm Hg, PaCO2 60 mm Hg, pH 7.35? a. High-frequency jet ventilation b. Permissive hypercapnia with convential pressure controlled ventilation c. Extracorporeal membrane oxygenation (ECMO) d. Induced respiratory alkalosis e. Inhaled nitric oxide with conventional volume controlled ventilation Answer: b 35. There is an emerging consensus that the surgical repair for congenital diaphragmatic hernia is best done: a. Emergently at the bedside, eliminating the risks of transporting an unstable neonate b. While on extracorporeal membrane oxygenation c. When the infant is potentially extubatable d. Within the first 48 to 72 hours of life Answer: c PEDIATRIC SURGERY Objective Questions with Answers 36. Meckel’s diverticulum may present with which of the following signs or symptoms? a. Hemorrhage b. Intussusception c. Volvulus d. Patent omphalomesenteric duct e. Right lower quadrant peritoneal findings Answer: a, b, c, d, e 37. A 3-week old infant has a barium upper gastrointestinal series to evaluate vomiting. The duodenojejunal flexure is found to be to the right of the midline as well as more caudal and anterior than a normal ligament of Treitz. The child is seen to reflux barium spontaneously to the level of the mid-thoracic esophagus. You would recommend which of the following? a. Barium enema b. Emergency laparotomy c. A trial of H2, blockade and cisapride therapy d. Upper gastrointestinal endoscopy e. Overnight pH probe analysis Answer: b 38. Which of the following statements regarding duodenal atresia are true? a. 20% to 40% of these infants have Trisomy 21 b. When associated with an annular pancreas, division of the pancreas at the site of obstruction is curative c. Bilious vomiting is typical because the obstruction is usually distal to the ampulla of Vater d. Reconstruction is best achieved with Roux-en-Y duodenojejunostomy Answer: a, c 39. A 1500-gram, 30-week gestation neonate is fed at 2 weeks of age. He develops abdominal distention, bilious vomiting and guaiac-positive stool. A plain film of the abdomen demonstrates pneumotosis intestinalis. Which of the following related statements are true? a. An emergency barium upper GI series should be done to rule out malrotation b. The child should have a nasogastric tube placed, broad spectrum intravenous antibiotics begun, and sequential abdominal films obtained. c. The likelihood of intestinal perforation is in excess of 50% d. The expected survival rate is in the range of 70% Answer: b, d 40. The most common cause of pyogenic liver abscess in children today is which of the following? a. Perforated appendicitis b. Blunt liver injury c. Immunocompromised host d. Percutaneous liver biopsy e. Omphalitis Answer: c 41. Which of the followings statements regarding an infant with meconium ileus are true? a. The probability is 100% that he will have cystic fibrosis b. Nonoperative therapy resolves this problem in approximately two-thirds of patients c. The average life expectancy is approximately 26 to 28 years for this infant at present d. The finding illustrated below on plain film is an absolute operative indication (Figure 103-23A) Answer: a, b, c, d 42. You are asked to recommend therapy for an asymptomatic 2 year old who swallowed a small alkaline watch battery 4 hours ago. A plain film shows the intact battery in the intestine beyond the stomach. The best course of therapy is? a. Immediate laparotomy, enterotomy and removal of the battery b. Enteroscopy with extraction c. Laparoscopy with ultrasound localization and extraction d. Cathartics and a follow-up plain film in 48 hours if the child remains asymptomatic Answer: d 43. A jaundiced 6 week old infant has biliary atresia. Which of the following statements are true? a. Portoenterostomy is the initial procedure of choice b. Primary liver transplantation using either a reduced sized cadaveric graft or a living related graft is now the procedure of choice c. Approximately two-thirds of patients managed with portoenterostomy will develop chronic liver disease sufficient to indicate liver transplantation d. Because biliary atresia has pathogenic components of acute and chronic inflammation, antiinflammatory therapy is known to delay onset of liver failure Answer: a, c 44. Of the following, which is the most likely cause of hemodynamically significant lower gastrointestinal bleeding in a 6 month old male child? a. Meckel diverticulum b. Henoch-Schonlein purpura c. Intussusception d. Crohn’s colitis e. Hemolytic uremic syndrome Answer: a, c 45. Which of the followings statement regarding Hirschprung’s disease are true? a. Suction rectal biopsy is virtually always diagnostic if the specimen includes submucosa c. The endorectal pullthrough is demonstrably superior to other forms of surgical construction d. Ninety percent or more of patients have an excellent or good functional result following reconstructive surgery e. The important cause of mortality in contemporary practice is enterocolitis Answer: a, d, e 46. The operative procedure of choice for managing the most common type of choledochal cyst is which of the following? a. Cyst gastrostomy b. Cyst jejunostomy c. Excision with Roux-en-Y hepaticojejunostomy d. Transduodenal marsupialization e. Endoscopic sphincterotomy Answer: c 47. Which of the following is the most common liver tumor of childhood? a. Hemangioma and hemangioendothelioma b. Hepatoblastoma c. Hepatocellular carcinoma d. Mesenchymal hamaratoma Answer: b 48. The risk of biliary tract adenocarcinoma developing in a patient with a choledochal cyst left in situ is approximately which of the following? a. Less than 1% b. 3% to 5% c. 10% to 15% d. Greater than 25% Answer: b 49. The most common cause of acute pancreatitis in childhood is which of the following? a. Pancreas divisum b. Cholelithiasis c. Trauma d. Valproic acid e. Annular pancreas Answer: c 50. Which of the following statements regarding gastroschisis are true? a. Primary fascial closure can be achieved in only about 25% of these infants b. These infants have an incidence of approximately 40% to 50% of associated anomalies c. Overall survival is approximately 80% to 90% d. When the diagnosis is known prenatally, planned cesarean section is the safest method of delivery Answer: c 51. Which of the following are typical causes of neonatal intestinal obstruction? a. Intussusception b. Meconium ileus c. Hirschprung’s disease d. Meckel’s diverticulum e. Incarcerated hernia Answer: b, c, e 52. A 6-week-old child presents with generalized seizures, a serum glucose of 30 mg/dL and concurrent hyperinsulinemia. This child’s first priority is which of the following? a. Permanent central venous access and glucose infusion b. Administration of cortisone and adrenocorticotropic hormone c. Computerized tomographic scan of the abdomen to look for an islet cell adenoma d. Urgent pancreatic resection Answer: a 53. At what age is surgical orchiopexy recommended for a child with a unilateral undescended testis? a. Promptly upon discovery, regardless of age b. 1 year c. 5 to 6 years d. Any time prior to puberty Answer: b 54. An infant is noted to have a left flank mass shortly after birth and an ultrasound examination demonstrates left hydronephrosis. The most common cause of this finding is which of the following? a. Neonatal Wilm’s tumor b. Congenital ureteropelvic junction obstruction c. Multicystic dysplastic kidney d. Vesicoureteral reflux Answer: b 55. The medical indications for circumcision include which of the following? a. Infants with a history of urinary tract infection b. Hypospadias c. Phimosis d. Enuresis e. Vesicoureteral reflux Answer: a, c, e 56. Which of the following statements regarding neuroblastoma are true? a. Neuroblastoma is the most common abdominal malignancy of childhood b. Approximately 80% of neuroblastoma patients are diagnosed prior to age 4 years c. N-myc oncogene copy number in neuroblastoma tissue is inversely related to survival probability d. Trk proto-oncogene expression in neuroblastoma tissue is inversely related to survival probability e. All of the above Answer: a, b, c 57. Which of the following are considered low risk features for neuroblastoma patients? a. Age less than one year b. Stage 2A and 2B disease (International Staging Criteria) c. Stage 4S disease (International Staging Criteria) d. Neuron specific enolase plasma level less than 100 ng/ml e. None of the above Answer: a, b, c, d 58. A one month old female infant is brought to you for evaluation of afriable polypoid mass prolapsing through the vaginal introitus. Your presumptive diagnosis is which of the following? a. Ectopic ureterocele b. Rectal prolapse c. Congenital adrenal hyperplasia with ambiguous genitalia d. Embryonal rhabdomyosarcoma Answer: d 59. Which of the following approaches is considered standard care for most Wilms’ tumor patients in the United States today? a. Adriamycin and vincristine therapy followed by surgical resection b. Needle biopsy followed by either chemotherapy or resection depending upon the histology c. Primary surgical resection followed by chemotherapy d. Radiation therapy if judged unresectable on CT or MRI imaging Answer: c 60. Which of the following statements regarding rhabdomyosarcoma are true? a. Surgical resection of the primary tumor results in cure of approximately 80 to 90% of all patients b. Currently recommended therapy includes complete resection of primary tumors prior to chemotherapy for small noninvasive lesions, or after documented response with more formidable primary tumors c. Alveolar histology is a favorable prognostic finding d. Overall survival of all patients is now approximately 50% Answer: b, d 61. Patients with Wilms’ tumors most frequently present with which of the following? a. Bilateral metachronous lesions b. Bilateral synchronous lesions c. An extrarenal primary d. A multicentric primary lesion e. A unifocal, unilateral lesion Answer: e 62. Hepatoblastomas are childhood liver tumors characterized by which of the following features? a. Multicentricity b. Cirrhosis in the uninvolved liver c. Unresectable tumors subjected to cytoreductive chemotherapy may be resected with long-term survival d. Jaundice Answer: c 63. Common sites of neuroblastoma metastasis are which of the following? a. Lung b. Regional lymph nodes c. Bone marrow d. Cortical bone Liver Answer: b, c, d 64. Which of the following statements regarding renal tumors of childhood and adolescence are true? a. Clear cell sarcoma is presently considered a variant of Wilms’ tumor with a poor prognosis b. Clear cell sarcoma of the kidney has a high rate of metastasis to bone c. Rhabdoid tumors may arise in the kidney, mediastinum or brain d. Childhood rhabdoid tumors of the kidney carry an excellent prognosis Answer: b, c 65. Which of the following syndromes are associated with the development of Wilms’ tumor? a. Beckwith-Wiedemann Syndrome (hemi-hypertrophy, macroglossia, aniridia) b. Neurofibromatosis c. Denys-Drash syndrome (pseudohermaphroditism, glomerulopathy) d. Gonadal dysgenesis e. Hemolytic uremic syndrome Answer: a, b, c, d PEDIATRIC SURGERY Questions and Answers pdf Download Read the full article
0 notes
Text
Stuff I Learned: Sunflower III
Chapter 18: Kidney and Urinary Tract Disorders
Antenatally Diagnosed Congenital Anomalies
Potter sequence
Caused by oligohydramnios causing fetal compression
Potter facies: low set ears, beaked nose, prominent epicanthic folds, downward slanting eyes, pulmonary hypooplasia, limb deformities
Autosomal recessive polycystic kidney disease is more severe than autosomal dominant PCKD
AR: diffuse bilateral enlargement of both kidneys
AD: cysts of varying size between normal renal parenchyma
Absent muscular syndrome (prune belly syndrome): enlarged bladder, dilated ureters, cryptorchidism
Management
Step 1: prophylactic antibiotics
Step 2a: male AND bilateral hydronephrosis/dilated lower urinary tract -> ultrasound in 48h to exclude posterior urethral valves
Step 2b: female or male with unilateral lesion -> ultrasound at 4-6 weeks
Step 3: normal ultrasound -> stop antibiotics and repeat ultrasound after 2-3 months
Step 3b: abnormal ultrasound -> further investigations
UTI
Up to 50% have structural abnormalities
Predisposed by vesicoureteric reflux (VUR); severe VUR is associated with intrarenal reflux (IRR), which is associated with a high risk of renal scarring if UTIs occur
Enuresis
Daytime: developmental or psychogenic, bladder instability or neuropathy, UTI, constipation, ectopic ureter
Secondary: emotional upset, UTI, polyuria from an osmotic diuresis in DM or DI
Nephrotic Syndrome
Transient proteinuria may occur transiently after febrile illness or exercise
First presentation is periorbital edema (on wakening), or scrotal/vulval edema
2 types
Steroid-sensitive: treat with 4 weeks 60mg/m^2 oral prednisolone then 4 weeks 40mg/m^2 on alternate days to prevent frequently relapsing or steroid dependent course
Steroid-resistant: diuretics, salt restriction, ACEI, NSAIDs etc., lowest possible dose of steroid with steroid-sparing drugs
Steroid-sparing drugs include immunomodulator levamisole, alkylating agent cyclophosphamide, calcineurin inhibitors (e.g. tacrolimus, cyclosporin), immunosuppressant MMF
Renal Stones
Most common type is phosphate stones associated with Proteus
Fanconi syndrome
Generalized proximal tubule dysfunction
Cardinal features: excessive urinary loss of amino acids, glucose, phosphate, bicarbonate, sodium, potassium, calcium, and urate
Presentation
Polydipsia and polyuria
Salt depletion and dehydration
Hyperchloremic metabolic acidosis
Poor growth
Rickets
Causes
Primary: idiopathic
Secondary to IEM: cystinosis, glycogen storage disorders, galactosemia, Wilson disease
Secondary, acquired: heavy metals, vitamin D deficiency
Hemolytic-Uremic Syndrome
Types
Typical: secondary to GI infection with O157:H7 E. coli or Shigella
Atypical: no diarrhea prodrome; high risk of hypertension and chronic renal failure, high mortality
Classical triad
Acute renal failure
Hemolytic anemia
Thrombocytopenia
0 notes