#causes of urinary incontinence
Text
urinary incontinence causes symptoms and treatment
Urinary incontinence (UI) is a common condition that affects millions of people worldwide, particularly women and the elderly. It is characterized by the involuntary loss of urine, leading to social embarrassment and a decreased quality of life. Understanding the causes, symptoms, and treatment options for urinary incontinence is crucial for managing this condition effectively.
Causes of Urinary Incontinence:
Several factors can contribute to urinary incontinence, including weakened pelvic floor muscles, nerve damage, urinary tract infections (UTIs), and hormonal changes. Other causes may include obesity, pregnancy and childbirth, prostate issues in men, and certain medications that affect bladder function. Additionally, neurological disorders such as multiple sclerosis (MS) and Parkinson's disease can also lead to urinary incontinence.
Symptoms of Urinary Incontinence:
The symptoms of urinary incontinence can vary depending on the type of incontinence. Stress incontinence, which is caused by physical activities that put pressure on the bladder, can result in urine leakage during coughing, sneezing, or exercising. Urge incontinence, on the other hand, is characterized by a sudden and intense urge to urinate, followed by an involuntary loss of urine. Mixed incontinence involves a combination of stress and urge incontinence symptoms.
Treatment of Urinary Incontinence:
Treatment options for urinary incontinence depend on the underlying cause and the severity of the condition. For mild cases, lifestyle changes such as bladder training, pelvic floor exercises (Kegels), and dietary modifications can be effective. In more severe cases, medication may be prescribed to relax the bladder muscles or reduce urinary urgency. In some cases, surgery may be recommended to repair or support the structures that control bladder function.
It's important to consult with a healthcare provider for an accurate diagnosis and personalized treatment plan. With the right approach, urinary incontinence can be effectively managed, allowing individuals to regain control over their bladder and improve their quality of life.
#urinary incontinence treatment#urinary incontinence#causes of urinary incontinence#symptoms of urinary incontinence#treatment of urinary incontinence#best treatment for urinary incontinence
1 note
·
View note
Text
I fucking slept most of the day. Because I’m in a situation that is highly draining to me. Because I’m disabled and in pain.
I’m so sorry that the most I can do for my community is stand up for terminology which then allows them to speak more easily about that transandrophobia they have faced. That all I can do is help people to have words to put to their experiences, which is certainly not useful and is just pissing and whining. /s
#about me#by the way urinary incontinence is part of what my disabilities cause issues with#I’ve always despised the whole ‘pissing’ thing#like…yes I am spending a lot of time pissing?#do you have a problem with that?#like actually?#or do you just want to sound cool by using one of the ‘in’ insults?
8 notes
·
View notes
Text
#urinary incontinence#urinaryhealth#urinary incontinence treatment#urinary incontinence causes#urinary incontinence symptoms#urinary tract infection#urinary tract health#urinary system#treatment of urinary incontinence
0 notes
Text
Explore the nuances of urinary incontinence in women, delving into its types and causes. This insightful guide sheds light on the various factors contributing to this condition, empowering women with knowledge to seek informed medical advice for effective management and improved quality of life.
#urinary incontinence in women#urine leakage in women#urinary incontinence treatment#urinary incontinence cause#types urinary incontinence
0 notes
Text
your uterus is not an optional organ. i repeat: your uterus is NOT AN OPTIONAL ORGAN. every so often i see people (mostly tras) talking about how it's actually so cool and fun to modify your body and how you don't really need an uterus if you don't want to have children. this is blatant and dangerous misinformation.
hysterectomy should be considered ONLY if a woman has serious health conditions (multiple/huge leyomiomas or fibromyomas, severe endometriosis, cancer etc.). the amount of information related to adverse effects of hysterectomy is catastrophically small, however the complications can be severe, including but not limited to vaginal prolapse, urinary incontinence, adhesions and fistulae formation. notice that all of the above is related to removal of the uterus itself without the surrounding organs (eg ovaries) and i can't even begin to describe the amount of stress your body goes under after removal of these as well. i'm not even talking about the non-specific complications (peritonitis, various wound infections, possible anaphylaxia caused by anesthesia etc.).
there are no optional or unnecessary organs in your body, each of them occupies its own place and the removal of said organ can lead to the displacement and dysfunction of others. you're putting yourself on a goddamn surgical table. this is not a "fun and easy way to get rid of your periods", this is a removal of a body part.
i work in an operating room. i've seen enough hysterectomies. there is no sane reason to do this to yourself without having indications for this surgery.
2K notes
·
View notes
Photo

At Women’s Health Care Specialists in Greenbelt, Maryland board-certified Navita Modi, MD, FACOG, and urinary disease treatment greenbelt md her obstetrics and gynecology team provide exceptional, personalized health care using a holistic approach for women of all ages. The practice specializes in preventing OB/GYN illnesses though wellness care and treating chronic disorders if they arise.
Book Your Appointment call us: Phone: 301-812-3400 7525 Greenway Center Dr, Suite 202, Greenbelt, MD 20770
#Obstetrics and Gynecology in Greenbelt MD#urge incontinence causes treatment in greenbelt#womens primary care greenbelt md#osteoarthritis treatment greenbelt#osteoporosis treatment greenbelt#fnp greenbelt#fnp greenbelt md#doctor of nurse practice greenbelt#urinary Incontinence treatment near me greenbelt
0 notes
Text
╰┈➤ ꒰🍓💌🥛 ┊boba time ┊ Hana ; #02 ꒱
『♡』 Post-Partum urinary incontinence is the bane of your existence, ruining everything, but Katsuki kisses you like it doesn’t matter.
『♡』 having a baby and all that comes with it, post partum anxiety, urinary incontinence, comfort, suggestive scene, insecurity, healthy relationship, pet names : bunny, angel, baby, f!reader
You keep peeing on yourself and it’s fucking infuriating. The stitches have healed and you’re coming along nicely but you just keep peeing on yourself.
You love Hana, her pretty little blonde curls and red eyes. You love her giggles and her cries, even when she makes you cry. But you keep peeing on yourself and it’s the most embarrassing part of having a baby thus far.
Katsuki doesn’t mind, he laughs a little with the baby in his arms when you shove her to him. He watches you waddle to the bathroom grumbling and muttering curses.
It really doesn’t bother him, but it bothers you.
Hana stretched your pelvic floor to hell and back and now, as the doctor said it, you have urinate incontinence.
You change your pad in a haste, wiping gently with a baby wipe and look in the mirror. A cry comes from the other room and you shoot out, darting toward your husband.
“What happened?!” You bite, rushing over to the pair.
Nothing. Nothing happened. Hana is happily sucking down a bottle of breast milk in her fathers arms. She’s getting milk drunk, happy as can be, and he’s bouncing her and humming.
“What’re you talkin’ about baby?” Katsuki mumbles, head tilted to look at your eyes.
“I-I thought I heard her crying..” You mumble and he gives you a pitiful look.
Katsuki moves to sit on the couch, flicking on some random shoujo anime he swears he doesn’t watch. And you follow suit, sitting next to him on the black leather.
His spare arm wraps around you, pulling you closer to his body. His other thick, muscular arm holds Hana and the bottle. He’s gotten amazing at that, multitasking.
Plush lips come down to the top of your head and he murmurs reassurance. You turn and curl into him, breathing in the familiar scent of him.
It’s interesting, smelling the mix of caramel and baby powder all at once. It isn’t something you though you’d find comfort in until now. You feel with your arm for the throw blanket and drape it over the two of you.
“What’s wrong angel?” He ponders, watching the way you close your eyes slowly and sigh in response.
The anime girls on the show are confessing their undying love with roses and bento boxes. It’s kind of cute.
Hana let’s out a satisfied noise and he pulls the bottle from her mouth with a pop, setting it to the side. You lick your thumb and wipe the excess milk from her face and giggle at her features scrunching up in disagreement.
“Just.. worried? What if something happens, you know? And and i- I can’t stop freaking peeing on myself. Even if it’s just a little. I don’t see why you’d be interested in me when I’m constantly- just- yeah.” You let out, breathless and frustrated.
Katsuki hums, leaning down to kiss your forehead. He unwraps his heavy arm from around your middle and turns, lifting your face using his thumb and hand. And he kisses you.
He kisses you deep and slow, sighing into it. And he breaks away when Hana makes a noise, bouncing her momentarily before going back in.
His lips are so soft and remind you of the first time you ever kissed. It reminds you of the day he asked you to marry you. The day he found out you were pregnant.
And his tongue is hot and heavy in your mouth. Patiently exploring and soothing the deep need in your bones to feel wanted.
“I don’t care that you’re peeing on yourself. I don’t care that you need to wear pads cause of it n’ I damn sure haven’t lost interest.” He breaks the kiss, forehead pressing to yours.
You open your mouth, then close it again, then speak.
“But you haven’t touched me..” You whisper, tears pricking your eyes.
“Oh bunny, is that what this is about?” He rasps, worried and kissing over your cheeks where tears begin to spill.
You nod and tremble in his grip.
“The only reason I haven’t fucked you on every surface in our house, haven’t licked every inch of your body, is because you’ve been tired, baby.” His thumb brushes over your lip and he kisses you again, softly.
“I’ve seen how much work you’ve been doing with Hana n’ all. And you’ve been so upset with yourself cause of the peeing situation I thought’cha weren’t ready, angel.” He explains.
Relief washes over your features and you sigh, weight lifted from your chest. You grab him by the jaw and kiss him as hard as you can. He deepens it, and only breaks when Hana begins to make noise.
“Is that- is that really why ?” You murmur, eyes wide and full of hope.
Katsuki nods, crimson eyes boring into your own. His arm bounces your daughter over and over, keeping her snoozing against the fat near his pec.
You spend some time watching the anime, drinking water and lightly snacking. Mundane things, domestic things. Everything that makes life worth it.
He gets up, walking through the house and into the nursery and places her in the crib for her nap time. When he gets back, Katsuki all but slings you into his lap.
You don’t have sex, but the shoujo anime is drowned out in the back regardless. He takes his time with you, exploring new ridges and curves of your body.
Momentarily, you worry about the pad pressing against him. Just how embarrassing it is, at least to you. But that goes away when he kisses up your throat and groans out a praise.
“You’re the sexiest thing on this planet.” He declares, nipping at your jaw, fingers digging into the plush of fat above your hip.
“So glad I made you a momma..” He murmurs, kissing your mouth. And you look to find him staring at you with love struck eyes, looking over your entire body.
He looks between you and let’s put a breathy sigh watching your hips rock into his. Satisfied, he tries to take it a little bit further.
And you forgot about all the water you had. You forgot about the fact that you’ll pee on yourself a little too easily.
So he jostles you, pulling you down so he can get a little more friction. And when he tries to adjust himself by scooching up more, your thin pad gets soaked through.
You screech, embarrassed that you just wet yourself while making out with your husband. It reminds you all too well of every little awkward thing you’ve ever done.
And he doesn’t care, he just ignores it, for a moment. Grabs you by the back of the head and kisses you nice and deep, squeezing your ass. He pats then, telling you to go ahead and change.
When you come back, you don’t notice that he’s changed his sweats to the most similar he could find. You don’t need to know that it got on his pants.
#yes there’s gonna be a whole series about life with a baby#no you can’t stop me#i love accurate post partum and pregnancy#mwa#katsukiizmoon#bakugou x reader#bakugou x you#bakugou fluff#bakugo x reader#tw: ppa#bakugou fanfiction#bakugou katsuki#bakugou x y/n#katsuki bakugo x reader#katsuki x y/n#bakugou katsuki x reader#bakugo x self insert#bakugo x you#bakugo x yn#yn x bakugou#katsuki bakugo fluff#katsuki bakugo fanfiction#bakugo katsuki x reader#katsuki x you#masterlist#peaches writes#strawberry cake#boba time#Hana Series
1K notes
·
View notes
Text
Waking Up Unconscious Characters
on the topic of whump!
if you want somebody to attempt to wake an unconscious character, here's how we do it when waking you from anaesthesia:
always speak in a loud and clear voice. we need to make sure they can hear us.
identify ourselves. this includes what our role is so, "this is (my name), i'm your anaesthetist/doctor." sometimes i will also say, "we met before," just to try jog their memory a little bit.
use the patient's name.
comfort and reassure. we avoid saying, "everything's okay," or similar but we will say, "this is normal," "we're looking after you," "the procedure went well," etc.
"(name), open your eyes for me. i need you to open your eyes now." notice it's a command, not "can you open your eyes for me?" when patients are confused, we sometimes see a sort of "i can but i won't" response. can't leave room for confusion, we need to be direct.
tap their shoulder firmly, if possible. obviously, if they've just had surgery on their shoulder or have a shoulder injury we might tap a leg or their chest instead. we will also loudly and clearly speak to them while doing this.
apply painful stimuli. this doesn't mean we're hitting them. we're stimulating a patient to get a response to assess LOC. mandibular pressure is the common one in anaesthesia, if it was the surgical site or if there is an injury there we won't do it, we might do the trapezius squeeze instead.
"hey, (name), this is (my name), your anaesthetist. you're just waking up from surgery, alright?" let them know what's going on, identify yourself again. keep using their name.
once they open their eyes, acknowledge it. i say, "there we go, hello again, (name)," and then reiterate the above.
tell them to stay still, talk them through what we're doing. "stay still for a second, we're taking the tube out, okay?" if a character is going to be moving or touching the injured character, even if they are still unresponsive, they should explain what they're doing. "i'm putting you on your side," "i'm just checking you for injuries," "it looks like you've hurt your arm, i'm going to take a look."
here's some responses people have when waking up from anaesthesia (often they do not remember this):
crying a lot. this is very common and usually if we ask why they're crying, they say they don't know so we tend to just assure them that this is normal and it will pass. we also often see this if a procedure went for longer than anticipated and the bladder is distended.
combative responses. some patients wake up swinging because they're confused, in pain, etc. some wake up combative because the procedure went for longer than anticipated and their bladder is distended too, that's a common cause of aggression on emergence.
urinary incontinence. it happens, we assure them that it's normal and not to be embarrassed, clean them up and cover them. sometimes it happens before they're 'awake'.
flirting or declarations of love. it sounds weird but it happens. it also happens when we're putting them under too. i had a patient tell me that i have beautiful eyes and make kissy faces at me once.
some people get erections. it's sometimes seen in response to certain anaesthetic agents. maybe not whump material but it's interesting so there you go.
immediately trying to move, pull monitors off or IVs out, etc.
singing. now, i haven't seen this super often and it's not full singing but they try their best. i had a patient mumble-singing the lyrics to funky cold medina once (instrumental included), he had no recollection of it later.
non-purposeful movement. thrashing, writhing, turning, etc with no intention.
crying, combative responses, non-purposeful movement, etc are known as 'emergence agitation' (EA).
i hope that helps a bit and gives some ideas!
#whump#whump prompt#anaesthetist#anaesthesia#healthcare#medical#medicine#whump writing#writing tips#writing help#writing advice#fanfic help#ao3 fanfic#fanfic
73 notes
·
View notes
Note
hi, unless i’m imaging things i think you’ve mentioned having written an article about different treatments for vaginal atrophy. do you have a link?
Hey there, Anon!
I have a big, exhaustive guide to vaginal and vulvar stimulation, and I do discuss the impact of vaginal atrophy and a few options toward treating it, but it doesn't go into specific detail.
Vaginal atrophy is caused by decreased estrogen production, and effectively what happens is that the soft, wet tissue on the inside of your vagina - the parts that are formed of mucous membranes - become thinner and dryer. This can lead to pain during sex, difficulty getting sufficiently loose or lubricated for penetration, and it can make the skin there tear a lot more easily, because when it's thinner it's less flexible and has less support from the surrounding tissues, not to mention the increased friction from lack of lubrication.
It's important to remember that while we're at our wettest during sexual arousal, the inside of the vagina - much like the head of the penis inside the foreskin - should always be a little bit wet. That wetness is really important to the vagina performing its regular activities, keeping itself clean and healthy, and not receiving too much friction just from things like walking around.
Even your rectum has important mucous inside it to keep things running a bit more smoothly and to ensure it's never too dry, and this is why too many enemas in a short period can be bad for your anal and rectal health, and your anus is a lot more closed naturally than your vagina, you know?
While more lube during sex is often the first thing people bring up in response to vaginal dryness, that's actually only one facet of potential issues - for people who are on T, for people going through menopause, for people who for whatever reason have an E deficiency or insufficient E in this area, it can cause other problems too - your vaginal canal might get a bit shorter, muscle weakness in the area (especially of the pelvic floor) can make you need to pee more often and more urgently, you might have some spotting, abdominal pain, uncomfortable or burning sensations when urinating.
In combination with the fact that vaginal atrophy can make you more prone to injury, your bacterial flora can be thrown out of whack by this process too, and these are really really important to maintaining a healthy vagina, producing appropriate amounts of discharge, but also to fighting off infection - vaginal atrophy is also associated with recurrent UTIs and other infections.
So, what can we do?
Firstly, pelvic floor exercises are unbelievably helpful, and everyone should be doing them regularly, regardless of gender or genital make-up.
Here's an NHS guide """for women""" but it mostly doesn't use any gendered language for your actual body parts:
These exercises will help strengthen your pelvic floor, and strengthening these muscles will not only help with stuff like potential urinary incontinence or give you a tighter grip that you can better control during penetration (more control in this area can also help you if you're prone to reflexive tightness under stress, e.g. with vaginismus), but when those muscles are stronger and have more density to them, they provide more support to the surrounding area, which can help blood flow and give more structure to the tissues we're trying to support.
Secondly, as well as good lubricants, there also exist vaginal moisturizers - depending on the extent of your atrophy and how much it's a problem (it might be worse, for example, at some points of the month than others), these might help - you apply them every few days and they help your vagina maintain its lubrication.
If pelvic floor exercises and lube and moisturizer isn't helping, your next step is different forms of estrogen - your medical provider will need to tell you what's available in your area and to you particularly, but there's honestly all sorts.
You can get topical estrogen gels and creams that you smear inside the vagina, you can get suppositories that you insert and are then absorbed, you can get rings that you insert and then stay in place for a few months, slowly releasing E over time.
If you're using testosterone, it's more likely that your medical provider would suggest these latter than taking E orally - the great thing about these topical applications is that the E stays very localised to your pelvic region where you need it, much like when you get an IUS and the progesterone stays relatively localised. Taking E orally, you're introducing estrogen to your whole system, and depending on your current hormone cocktail, it might be harder to figure out dosage and effect, especially over time.
If your medical provider hears you're experiencing vaginal atrophy and, if you say that lube and moisturizer aren't sufficient, they immediately suggest moving to vaginal dilators or pain killers, or if they talk about easing your "discomfort" during sex (especially with a presumed male partner) without talking about pleasure or satisfaction, or especially if you've brought up vaginal atrophy for reasons other than sex and their priority immediately jumps to the imaginary partner they want you to be satisfying, I would recommend getting a new medical provider as soon as possible, and probably telling that one to shut the fuck up.
Many doctors, as we know, are scumbags, but some particularly cunty ones' automatic focus for someone with a vagina is that you're providing sex to your (cishet male) partner - they automatically focus less on your pleasure or satisfaction, let alone your health, and more on the idea of reducing pain you're experiencing enough that you'll let that partner fuck you as much as they desire to.
This is not a medical provider that has your best interests at heart, and if they don't afford you humanity in this area, I would have doubts as to others.
If you're having difficulty with a medical provider, I would always, always advise:
Bringing a chaperone with you. You're entitled to a chaperone, you can always bring one, a lot of the time they'll want to say a chaperone can stay out of the room "for your comfort/privacy" but for your comfort and safety, you can also bring them in with you.
A chaperone might be a friend or family member or partner, and they don't even need to say anything a lot of the time - just having a witness there can make a medical provider think twice about bullying a patient. I've served as a medical chaperone for quite a few friends, especially because I'm a thin white man, and even as a faggot, doctors humanise me slightly more than they do friends of mine who are perceived as women, who are POC, who are fat, etc.
Ask your doctor the reasoning behind denying a course of treatment, and ask them to document that they are refusing treatment at this time. Once they write it down, it becomes something that's documented and that they can't deny in court, which tends to make them a bit more flexible.
Don't be afraid to go into the doctor having done a bit of your own research. Doctors will tell you not to google things as many doctors have fragile egos and become nervous at empowered patients - with particularly egotistic doctors, you can always phrase your research in the form of questions to make them feel like you're appropriately aggrandising them. "Are there suppositories for this, or creams? Could my UTIs be related to my vaginal dryness? My mother mentioned vaginal atrophy during her menopause, but I didn't really understand what it was. Could you explain? Could that be me?"
Cisgender women are generally better doctors than cisgender men (statistically, despite being underpaid and underrepresented), but obviously cisgender people are often... very cisgender, and cisgender women can be even more painfully cisgender than cisgender men. Most providers won't bat an eyelid at you requesting a female doctor over a male one for a gynecological concern, but you can't go around asking for the most clocky doctor they've got in the back.
What you can do if you're having trouble at your GP is look for your local GUM (Genito-Urinary Medicine) clinic, and see if they'd see you and talk to you about vaginal atrophy - I know several trans people who work as nurses and practitioners in the GUM field, and in general, GUM practitioners will be way more chill about this field.
Unlike your GP, there's no chance of them getting flustered, nervous, or religiously conservative about sex or genitalia, and GUM practitioners are often more chill about queer, trans, and intersex patients because they already see us a lot more, whether because queer people are more on-the-ball about STI testing, or just because many of us enter sex work, and they're more likely to see sex workers. The benefit of this, though, is that you're almost certainly not going to be their first or only patient with x or y element of your body or identity, which can mean they humanise you a bit better and are generally less shit.
I hope that helps, Anon!
261 notes
·
View notes
Text
Female reproductive health terms you should know!
(terfs not welcome)
Dysmenorrhea: Period pain that isn't normal, i.e. any pain more than Mild cramping.
Dyspareunia: painful intercourse
Oligomenorrhea: lighter, shorter menstrual flow.
Menorrhagia: heavier, longer menstrual flow.
Ovarian cysts: a mass on or in one's ovary, can be resolved on its own, or can remain and cause complications such as a rupture.
Polycystic ovary syndrome: a chronic condition causing cysts to reoccur on the ovaries and enlarging them. Symptoms include:
Irregular periods
hormonal imbalance
facial hair
weight gain
painful periods/ ovulation
infertility
People with PCOS are at higher risk for endometrial cancer, type II diabetes heart problems and high blood pressure.
Endometriosis: A chronic condition in which a tissue similar to, but different than, the endometrial lining grows outside of the uterus instead of inside. During menstruation this tissue sheds and has nowhere to go, thus irritating surrounding organs.
Symptoms include:
Irregular periods
Dysmenorrhea
Widespread pain
Painful ovulation
Vomiting, fainting, chills, sweating, fever and brain fog during menstruation
Infertility
Severe bloating
This also puts people at a higher risk for endometrial and ovarian cancer. There are four stages to Endo as it is a progressive disease, with 3/4 being more severe. The average time it takes to be diagnosed is 7 years.
Adenomyosis: A chronic disease similar and comorbid to endometriosis in which a tissue similar to the endometrial lining grows inside of the uterine wall. Symptoms are nearly identical to endometriosis but more difficult to detect.
Many people are diagnosed post menopause, by fault of the medical system, but it can and does develop much before then.
Ovarian cancer: cancer of the ovary(ies).
Endometrial cancer: cancer of the endometrium, the inner lining of the uterus.
Endometrial cyst, or chocolate cyst: cystic lesions from endometriosis.
Tilted uterus: the uterus is positioned pointing towards the back or severely to the front of the pelvis instead of a slight tilt towards at the cervix. Can cause painful sex and periods.
Pelvic floor dysfunction: inability to control your pelvic muscles. Comorbid with many things and is highly comorbid with endometriosis. Can cause pain and incontinence.
Vulvodynia: chronic and unexplained pain at the opening of the vagina.
Interstitial cystitis: a chronic condition where cysts form on the inside of the bladder and urinary tract and cause symptoms similar to that of a UTI.
Pre-eclampsia: a condition occurring in pregnancy where the blood supply between the fetus and the pregnant person is affected and can cause irregular blood pressure, swelling, and in more severe cases headache, nausea and vomiting, a burning sensation behind the sternum, shortness of breath and potentially death if untreated.
Endometritis: an infection or irritation of the uterine lining. Is not the same as endometriosis and is treatable but can cause pain, bleeding, swelling, general discomfort and fever, and more.
Pelvic inflammatory disease: an infection of the reproductive organs
Ectopic pregnancy: a pregnancy that is attached to the outside of the uterus. Can be fatal if left untreated.
There are many more I could probably add but if you see something missing, please add it!
#reproductive health#endometriosis#adenomyosis#pcos awareness#reproductive health awareness#chronic illness#polycystic ovarian syndrome#ovarian cancer#reproductive rights
218 notes
·
View notes
Note
Begging you to stop assuming that trans people are just gay people who can't admit to being gay. I'm bi regardless of whether I'm the woman the body I was born into is supposed to make me or the man that I feel like I was supposed to be. I won't say that no one has ever transitioned to avoid homophobia, but there are better ways to address that than to stop genuinely transsexual people from transitioning.
I've been in therapy for 27 years. Since puberty sunk its teeth in me. NOTHING is going to make me feel like being a woman is the right fit for me and trying to force myself to fit into that box has made me suicidal for decades. Convincing myself I could just be a masculine woman barely soothed any of that. I'm sorry that transition wasn't the right fit for you, and you deserve all of the support you need for that, but it's no more fair to force me to be a woman just because of the body that I was born into than it would be to force you to keep identifying as a man and taking hormones.
I don’t know you and it’s none of my business how you live your life.
My opposition to transition is primarily due to the medical risks of testosterone therapy on women.
Testosterone causes our reproductive organs to atrophy, potentially irreversibly. I’ve heard stories of people who develop chronic pain, persisting even after stopping T. People whose ovaries no longer work correctly after only a few years on T, causing various problems from low hormone production. People with urinary incontinence and pelvic floor issues caused by T essentially putting them into early menopause. PCOS worsening. Ovaries twisting. People who have had unnecessary gynecological surgeries due to the effects of T. People with chronic chest pain after top surgery. People who developed arthritis in their joints, or autoimmune conditions while on T. People who had mental health crises triggered by being on testosterone. People with chronic debilitating vocal pain or clitoral pain due to the effect on those areas. People who developed cholesterol or blood pressure problems only after being on T, causing them to be at higher risk for heart health issues.
That’s just off the top of my head, and that’s just things I’ve personally witnessed in myself and friends, both trans and detrans.
Live your life, do what makes you happy. I’m not going to stop talking about this health crisis that’s currently affecting young women, many of whom are just gay or tomboys, and would eventually become fine with themselves if they were able to grow up with masculine female role models and actual feminist education.
Even if there was a small minority of “true transsexuals”, even if you are one of them, that doesn’t make what I’m saying wrong or unimportant. You can’t deny that women are getting harmed by transition.
34 notes
·
View notes
Note
do you know if theres any harmless tailless genes that can be present in american feral cat colonies? theres a big problem with feral cats where i live and recently a kitten (maybe 6-8 months) has appeared near my property but she has no tail at all, not even a little bob. im extremely worried that the manx gene might be present in the feral colony, even though she's the only one ive seen with no tail. she's too young for it to have been an accident or an amputation, i think, and it looks completely natural. she's super skittish so unfortunately i dont have any pictures
To the best of my knowledge there are 2 types of bobtail genes that have been documented.
The “asian bobtail” is caused by a HES7 mutation. This results in a short, kinked but not absent tail and isn’t associated with any health issues. This gene is responsible for Japanese Bobtails and likely the cause for other Eastern bobtail breeds such as the Kurilian and Mekong.
The “natural bobtail” is caused by a T-Box mutation. The expression of this gene is highly variable and not predictable, ranging from a decreased tail length to an entirely absent tail. This gene is responsible for the Manx and has also been documented in other Western bobtail breed such as the American Bobtail and Pixiebob.
The “manx gene” appears to be somewhat present in American feral populations, as evidenced by the presence of “manx syndrome” in affected moggies.
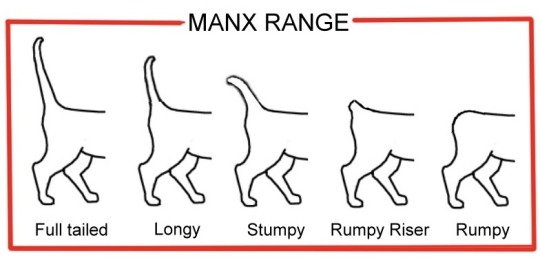
Bunni has a “stumpy” tail and is afflicted with manx syndrome effecting her gait and resulting in urinary incontinence, needing her bladder expressed manually throughout the day.
Cora has a “stumpy” tail and is effected by manx syndrome resulting in a degree of fecal incontinence which is managed reasonably well on a prescription diet.
Will doesn’t have a listed tail-length but is somewhere on the manx spectrum and has both urine and fecal incontinence due to manx syndrome.
Linguine has a “stumpy” or “longy” tail, based on the one image where it’s visible, and due to manx syndrome experiences urinary incontinence when she’s asleep.
Bob had a “rumpy riser” tail and is fully incontinent due to manx syndrome but wears a diaper without a problem.
Rumpie is a “rumpy” with no tail who has a gait effected by manx syndrome and a degree of incontinence.
Cece is a “rumpy” with no tail and has issues with constipation and doesn’t always make it to the litterbox as a result of manx syndrome.
Bunny, Monkey, Billy Cat and Olaf are all tailless “rumpy” cats with degree of incontinence. Bunny is also lame in a hind leg.
Research has indicated that tailless cats experience a significantly increased rate of manx syndrome - although it can effect any tail length where the gene is present, as seen by some of these adoptable cats.
So that does put your feral at a statistical disadvantage but it isn’t a guarantee she’ll have any clinical symptoms of manx syndrome. That’s part of what makes this gene so insidious, we know rumpy cats are most likely to be impacted but beyond that it’s anyones guess which cats will display symptoms and how severe.
I think these random-bred moggies being mislabeled as manx or manx mixes is the one time I’m not bothered by breed misrepresentation, as the issues the experience are the same as the real deal and it raises awareness of manx syndrome.
More information on manx syndrome for those interested:
Genetic Welfare Problems of Companion Animals: Manx Syndrome
Manx Syndrome in Cats
Manx Syndrome and Spinal Bifida
63 notes
·
View notes
Link
Urinary incontinence is the involuntary leakage of urine. Symptoms include frequent urination, urgency, and urine leakage during activity or at rest. Causes can include weakened pelvic muscles, nerve damage, and certain medications. Diagnosis involves a medical history, physical exam, and possibly testing. Treatment may include exercises, medications, or surgery. Prevention measures include maintaining a healthy weight and avoiding bladder irritants.
#urinary incontinence#incontinence#urinary incontinence treatment#Symptoms urinary incontinence#Causes urinary incontinence
0 notes
Text
Blake: Not jerking off is cringe. And you know what else is cringe? Urinary incontinence. Did you know one of the most common causes of kidney stones is holding in your piss?
Blake: Do you want that? Do you WANT kidney stones? Your body is a machine that turns food into cum and diet soda into piss.
Blake: Go piss right now! I'll watch. To make sure you piss.
21 notes
·
View notes
Note
I've heard that chihuahuas are hard to potty train, did you find this to be the case with your girls?
Hmm. Both yes and no.
To start off I will say a significant amount of the problems I have had are because I refuse to do the potty pad thing. Poop goes outside and that is non-negotiable. I'm not teaching my dogs that it's acceptable to go in the house. The rest are because Tater is somewhat incontinent due to her CM/SM.
Fae is perfectly capable of being potty trained. This comes with somewhat of an asterisk because if it is cold, raining, or snowing, she will do her absolute damnedest to not go outside and will do it in the house. Usually under my bed, which caused her to be evicted from my room during the winter months. She also can't hold it if she is out of her crate for longer than about 6 hours, but can hold it if she's in her crate through my work day or overnight. She also can hold it if she's sleeping in bed with me but not if she's been left on the floor overnight. She's weird.
That being said, during the period that I had a pad out for Tater when she was first diagnosed, Fae would make sure to go on the pad, so this problem would literally resolve overnight if I just provided a pad for them to use if they needed one. The chihuahuas are both poop eaters and also Fae will shred a pad she can access so not only do I not want to teach them that it's okay to potty in the house but it also creates new problems I don't want to deal with.
Tater was very similar to Fae before her CM caused a bunch of neurological issues including both fecal and urinary incontinence. With medication, that for the most part has stopped, though she does still occasionally leak in her sleep as I will start to smell urine on the blankets in their crate if I don't wash them regularly. Again she doesn't seem to do it if she's sleeping in bed with me, so I don't know if it's a comfort thing or what. While she was incontinent she would try her best to hit the pad - I'd usually find a trail leading from her bed to the pad and back. So she did want to go on the pad, she just had some mechanical malfunctions.
Keeping all this in mind, I also want to say that the most annoying to potty train dog in my house would be Sushi. If GSMD have one serious fault as a breed it is that they are notoriously difficult to housebreak. I had at least weekly full bladder releases in the house from Sushi until she was over a year old. She would pee while just walking around in my house, not even stopping to squat, so there would be a piss river all over my floor. I probably bought half the company's stock of nature's miracle during this time. Swissies are known for being incredibly incredibly dirty in this aspect and unfortunately Sushi was no exception. It's something that makes me a little reluctant to get another, if only because I got really tired of urine everywhere really, really fast. I could get another chihuahua just as annoying about going outside as my two, and I'd rather that over dealing with 100lb dog piss rivers again.
18 notes
·
View notes
Text
Divided Anatomy Syndrome (DvAS)


A MUD that affects systems [cis or trans], where the body's anatomy is divided among alters. One may be more connected to a specific body part than the others are.
Body parts don't only have to be external (such as limbs), but could also be internal- for example, one alter may be more bodily connected to the lungs, and when they aren't fronting, it may take more effort to breathe; or, one alter may be more bodily connected to the bladder, and when they aren't fronting, others may experience incontinence, bedwetting, or leaks, not be able to feel when the bladder is full, and even be unable to tell when the body has a UTI or other bladder/urinary symptoms.

Symptoms:
Some body parts may belong to one alter, who has better control over those body parts even when not fully fronting/conscious
Some body parts may feel numb or dull when the alter they belong to isn't in front
Some body parts may be harder or impossible to control without help from the alter it belongs to
An alter may be able to control their body part(s) even when not fronting/conscious or while in innerworld, while being forced out of front, while others are trying to hold them back [in sys], etc.
Other alters may be able to control another's body parts better if they have a strong connection to them
The feeling of numbess and the inability to control a body part that belongs to someone who isn't fronting may cause further dissociation and distress to other alters in the system


17 notes
·
View notes
Last Seen Blogs

malyutka13
Flanker

coolfayebunny
“We Are One Species, We Are Star Stuff”
Carl Sagan

gandalf-the-fool
The Undying Lands
annexr
AnnexR
