#Cytokine Storms
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
BuzzFeed published a report claiming that Tumblr was utilized as a distribution channel for Russian agents to influence American voting habits during the 2016 presidential election in Feb 2018.
Note
As someone who once did a little amateur research about the 1812 flu in particular (needed the info for a story I was writing at the time), one of the ways in which that flu was particularly deadly was that it didn't just take out people who were weakened by their youth/age or a secondary illness that was already compromising their immune system (which most flus can do). It took down otherwise healthy people like a scythe going through wheat, because it caused an effect known as a 'cytokine storm', which for simplicities sake I generally liken to your immune system having an allergic reaction to the virus. It triggers your system into responding so hard to it (releasing way too many cytokines, a natural inflammatory signalling molecule) that your own immune system causes organ failure and death. IIRC they figured this out from sequencing samples of the virus retrieved from corpses that had been interred in permafrost (it's been over a decade, forgive me if I'm misremembering).
One of the reasons COVID is so deadly is it also causes cytokine storms in otherwise healthy people (among other effects). The 2003 SARS epidemic is also believed to have had them as a contributing factor in its lethality. And this is just one of the many ways in which particular strains of flu viruses can be more deadly than others.
Given the high mutability of the flu virus, it's basically a dice-roll as to what effects a particular strain of the virus will have. Get the wrong collection of them (easily transmitted and lurks for a while before symptoms begin emerging and triggers cytokine storms, for instance) and you get something that can spread far and fast, and can kill even the healthiest person within a day or two of the infection actually becoming detectable outside of specialized tests.
Moral of this story: Get your flu shots every year unless you are medically unable to have them. Better to have had it and not need it than the reverse.
Hi! This is kind of a weird question but how/why was influenza (and other diseases that we have vaccines for now) so deadly 100-200 years ago? Obviously vaccines help tremendously, and probably immunity over time, but are there other reasons that the flu was a much bigger deal a century ago? Sorry if this is oddly specific, but my current project is historical. Thank you!
This is a very interesting question and there are a couple of different ways of looking at it.
Let's start with influenza:
[Note: it's surprisingly difficult to get good worldwide flu data, so I'm going to use US numbers for the purposes of this post.]
I think the first thing to understand is that unlike many other infectious diseases, influenza is substantially different every year. That means that the immunity that you build in 2017 from either the flu or the flu shot won't necessarily help prevent you from getting the flu in 2023. By then it will be a different enough virus that your previous immunity won't be as helpful. Though it might make it a little milder. But keep reading, I'll give you some fun facts to share at parties:
We name flu (A) viruses based on two different proteins on the surface of the virus. The proteins are "H" and "N". There are 16 different "H" proteins, and 9 different "N" proteins that we currently know of. The combination of the two forms the "name" of a particular flu virus. Think H1N1, or H5N6, or any other combination. Each combination has their own attributes, which contributes to how infectious or deadly they are in any given year. And which ones circulate are different every year.
Just mathematically, that's a lot of substantially different flu viruses. Hundreds of them, in fact. And you have to build immunity to each one individually. You could, say, build immunity to H2N5, but that would do little to save you from next year's H4N3. And not only that, but within a single type there are many smaller variations. For example, say you got H5N3, but then it went and mutated. If you then got exposed again, you might have some immunity to new!H5N3, but it could also be just different enough that you still get sick.
Like I said above, different types of flu virus are deadlier or spread faster than others. H5N1 (a type of avian flu with a human mortality rate of 52%) is terrifyingly deadly but fortunately doesn't spread particularly well, while H1N1 (the star of both the 1918 and 2009 flu seasons) spreads rapidly and kills primarily young adults (weird, since flu usually kills babies and old people).
This is why in 2009 we did the whole "close the schools vaccinate the teens hide the president" routine. Because if it was *that* H1N1 we were all about to be screwed in ways we had never experienced before. Fortunately it wasn't, but thank goodness we did it. Also if you got vaccine #2 in 2009, you are also protected against the 1918 strain of H1N1. You're gonna be a hit at parties with that one.
Now, if you look at only deaths (not the best measure, but one with some emotional punch), within the last decade alone we have years where 12,000 people died of flu in the US (2011-2012) and years where that number is as high as 61,000 (2017-2018). These numbers are similar throughout recent history (relative to population), but then you get years like 1968 (where 100,000 people died in the US) and 1957 (where 116,000 died), and then sometimes you get these wild whopping years like 1918 where 675,000 died (equivalent to 1,750,000 people dying in today's US population). These fluctuations have happened since Hippocrates was around, and probably long before that, and there's really nothing to suggest it's getting any milder in any statistically significant way.
Now, outside of these natural fluctuations, we do have some ways of driving down these numbers. We do have a vaccine. It is different every year, based on our prediction of what the most likely or dangerous types of flus will be this year. Fortunately, you do get to keep this immunity for some time, so you can look at the flu vaccine as a personal collection of different flu viruses you have immunity to- you can collect 2-3 different ones every year in one shot and you didn't even have to catch them!! Yay! Unfortunately, since we never reach herd immunity with the flu vaccine, and we can't perfectly predict and incorporate all the strains that will circulate in a given year, while you do get some protection, it's not ever perfect. But it *is* still worth it.
We also have other feats of modern medicine as backup to the flu vaccine. We have oxygen, antiviral drugs like tamiflu, immune modulating drugs, and technology like ventilators to help keep people alive in ways we would not be able to in previous generations. So that's also an advantage. Unfortunately, these don't always work either, and we are still at the whim of those yearly fluctuations in influenza virus deaths.
And really, if you ask any epidemiologist, covid is just a little trial run for the next Big One. Which is both extremely likely to be a flu virus and which we're statistically overdue for.
TL;DR: The flu isn't getting milder so much as it varies wildly in severity every year. The next major flu pandemic is probably going to be in our lifetimes, so start collecting your flu immunity now if you haven't yet. New collections drop every August and are available until April. Get em' while they're hot. This year's included a 2009-like strain of H1N1 and a delightful H3N2 number from Hong Kong.
As for All the Other Vaccine Preventable Illnesses:
*ahem*
Yes, it's vaccines. It's obviously vaccines. Its basically only vaccines. Anyone who has ever told you it's not vaccines is lying. No other major discovery of modern medicine has ever saved as many lives, prevented as many disabilities, and created as many opportunities for a life well lived as vaccines have. No antiviral drug, no antibiotic, no ventilator can even hold a candle to vaccines. The answer is f*cking vaccines*.
I hope I have made myself clear.
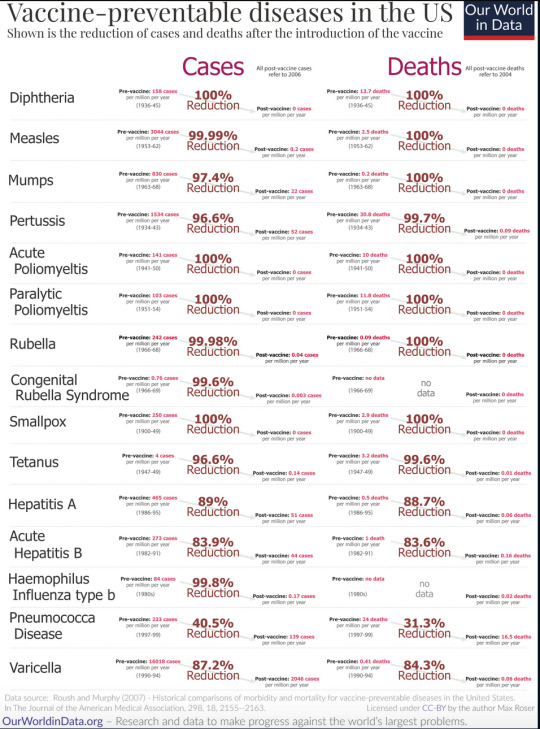
Enjoy this table:
*Yes I do have a masters degree in public health and am a registered nurse that interacts with the public regularly, how did you know?
-Ross @macgyvermedical
4K notes
·
View notes
Text

Some of the most serious #COVID19 outcomes can result from certain viral protein fragments produced by #SARSCoV2 resembling zombie complex overstimulating the immune system, thereby causing rampant inflammation in widely different contexts such as #cytokinestorms and lethal #bloodcoagulation: UCLA study
https://newsroom.ucla.edu/releases/viral-protein-fragments-behind-serious-covid-19-outcomes
0 notes
Text

A recent study in Nature Communications suggests that by 24 months, signs of heightened immune activity in most long-COVID patients will have returned to normal levels. Pictured above is a composite colored scanning electron micrograph of immune cells—including a single macrophage, two dendritic cells, and numerous white blood cells—involved in a cytokine storm, a life-threatening immune disorder. Cytokines are important for normal immune response, but when too many are released simultaneously it can be harmful.
COMPOSITE MICROGRAPH BY STEVE GSCHMEISSNER, SCIENCE PHOTO LIBRARY
#steve gschmeissner#photographer#national geographic#composite micrograph#science photo library#nature communications#long-covi#immune cells#cytokine storm#immune disorder#health#nature
13 notes
·
View notes
Text
I love that regulatory T cell is a spectrum of “If you even lay a finger on this cell, I will beat your ass so hard they can’t find the pieces to take you to the spleen” to “This sign says that’s a no no”
#cells at work#hataraku saibou#Lactobacillus posts#on an unrelated note#Do you think she has a button that says ‘ignore helper T cells orders’#for whenever he goes cytokine storm mode
5 notes
·
View notes
Text
Follow an account that posts vintage eBay jackets and hats and I have never needed an accessory more than this snapback in my whole entire life
#ALLERGY 2000#Y2K: MAST CELL MAYHEM#MILLENNIUM: CYTOKINE STORM#IgE-MAIL: Y2K AND THE CYBER ALLERGY CRISIS
10 notes
·
View notes
Text
There is something so deeply intriguing to me about the possibility of your impact on society being that of therapist's notes, medical observations, lab records, or possibly even a coroner's examination. Yet you, the patient, will never know exactly what these secret tomes of knowledge hold. You cannot ask for them. You cannot search your name in them. You cannot read them unobjectively. You just have to trust that even long after you've seen said practitioner, that the observations made about you will paint an accurate picture of the person they had to help in a medical setting. No matter how disturbing the tale may unfold.
⬖.Exe
#exe talkz#medical horror#sciencecore#lab records#mad science#mad scientist#lab report#i'm thinking about the TGN1412 cytokine storm incident once again
2 notes
·
View notes
Text
the most annoying thing in the world is Googling an immunology term and only getting 50,000 COVID articles written by non-scientists who don’t have any idea what they’re talking about in order to “educate” a population that’s relying on the news for important information about their health. The amount of misinformation is ASTOUNDING. And I don’t even mean “regular” COVID misinformation about things like Bill Gates and ivermectin, I mean misinformation generated by people who seem like they’re earnestly trying to help but who do not have ANY qualifications to be acting like an authority about virology
#trying to find ANY decent article on how hypercytokinemia leads to ARDS#I definitely spelled that wrong but. you know what I mean.#and half of the results are just people saying insane shit about cytokine storms#like man shut UP
2 notes
·
View notes
Text
bitcoin
I am now a bajillionare
i just found out merriam webster has a time traveler feature that tells you some of the words that were “born” the same year as you. it’s pretty neat yall should do this
280K notes
·
View notes
Text
Case of Necrotizing Pancreatitis following COVID-19 Infection by Faezeh Sehatpour in Journal of Clinical Case Reports Medical Images and Health Sciences

ABSTRACT
New aspects of COVID-19 are increasingly being recognized. Although the virus is mainly known to affect the lungs, involvement of other organs including the heart, liver, gastrointestinal, renal and pancreas is also detected. Acute pancreatitis is detected as one of both the early and late presentations of COVID -19. Cytokine storm or the presence of angiotensin-converting enzyme 2 (ACE2) receptor in pancreatic cells, are both two causes of pancreatic injury in COVID-19 infection. In this study, we reported a 25-year-old man admitted to our department with the impression of necrotizing pancreatitis concomitant with COVID-19 infection. Patient's lab data, imaging and outcomes were documented in full detail.
Abbreviations:
WBC, white blood cell;HB, hemoglobin; MCV, mean corpuscular volume; PLT, platelet; BUN, blood urea nitrogen; Na, sodium; K, potassium; ; AST, aspartate aminotransferase; ALT, alanine aminotransferase; ALK.P, alkaline phosphatase; ALB, albumin; LDH, Lactate dehydrogenase ; CPK, creatine phosphokinase; CRP,c-reactive protein; AFP,alpha-fetoprotein; CEA,carcinoembryonic antigen; CA19-9,cancer antigen 19-9; Immunoglobulin G4.
INTRODUCTION
The Covid-19 pandemic is an ongoing pandemic that started in December 2019 and spread rapidly around the word. COVID-19 was caused by severe acute respiratory syndrome corona virus 2 (SARS-CoV-2), first identified in Wuhan, China. So far, more than 200 countries have been affected by the pandemic. (1)
New aspects of COVID-19 are increasingly being recognized. Although the virus is mainly known to affect the lungs, involvement of other organs including the heart, liver, gastrointestinal, renal and pancreas is increasingly being reported. (2)
The involvement of the gastrointestinal system is maybe due to the expression of the angiotensin-converting enzyme2 (ACE2) on the hepatocyte, cholangiocyte and other parts of the GI tract. (3) In a recent survey, acute pancreatitis was detected as one of both early and late presentations of COVID -19. (4-6) However, it is still unclear whether SARS-COV-2 directly affects pancreatic cells because of ACE2, if it is a cytokine storm which causes pancreatic injury. (7)
We reported a case of COVID-19 with subsequent acute necrotizing pancreatitis.
CASE REPORT
A 25-year-old man without any known medical disease presented to our emergency department with progressive epigastric pain, nausea and vomiting and anorexia one week prior to admission. He has no history of alcohol consumption. He also had a history of admission to another hospital about two weeks ago with a diagnosis of COVID-19 pneumonia. On admission, he has a blood pressure of 115/75 mm HG, a heart rate of 100 beats per minute, a temperature of 37.1 ⁰C and oxygen saturation of 95% while the patient is breathing in the room air. Primary investigations summarized in Table-1. Amylase and lipase were 146 IU/L and 82 IU/L respectively. Nasal swab test for COVID-19 (RT-PCR for SARS-CoV-2) was positive. Abdominal sonography showed markedly prominent pancreas with in homogeneous parenchymal echogenicity and large cystic lesion arising from the pancreas, in favor of acute complicated pancreatitis with pseudo cyst. The gall bladder has a normal size and wall thickness without any gall stones. The pancreatic duct was not dilated. Due to the finding of abdominal ultra sound, CT scan of abdomen was done on him which revealed an enlarged pancreas with necrosis of the main portion of pancreatic parenchyma. Large cystic lesion measuring 15×7×11 cm in size arising from the pancreatic neck with extension to the right and left side of the abdomen suggestive of large pancreatic pseudo cyst (figure1). Lung HRCT (low dose) also showed bilateral peripheral ground glass opacities in favor of COVID-19 pneumonia (figure2). According to the findings of a physical exam, laboratory data and clues in imaging immediate management of acute necrotizing pancreatitis (invasive intravenous hydration and pain control) was started for him. He was finally discharged from the hospital with a full recovery.
Table 1: laboratory data
Figure 1: Abdominal CT scan: large loculated pseudo cystic structure measuring about 158mm*100mm in lesser sac due to post pancreatitis pseudo cyst formation.
Figure 2: lung HRCT: multiple ground glass and bilateral pleural effusion
DISCUSSION
Acute pancreatitis is an acute inflammation of the pancreas characterized by abdominal pain, nausea, vomiting and elevated exocrine pancreatic enzymes; amylase and lipase. Gallstones and chronic alcohol abuse are the most common causes of acute pancreatitis. Viruses are uncommon causes of acute pancreatitis. Pancreatitis has been reported with several viruses, including mumps, coxsackievirus, hepatitis A and B virus, cytomegalovirus, varicella-zoster, herpes simplex and human immunodeficiency virus. (8)
Although we have not conclusively proven the presence of the virus in the pancreas, the causes of COVID-19 and acute pancreatitis and the lack of other clear causes for pancreatitis strengthen the relationship between the two diseases. In this study, the patient presented with necrotizing COVID-19in 19 in the early post period of COVID-19 infection.
In Fan Wang and colleagues' survey, 52 COVID-19 cases followed and showed that 17% of COVID-19 patients developed pancreatic injury and presented with mild elevated pancreatic enzymes; serum amylase and lipase without clinically severe pancreatitis. The possibility of drug induced acute pancreatitis in patients who have received medication due to COVID-19 is also expressed as one of the reasons for acute pancreatitis in COVID-for19 infection. (9) Saffa Saeed Al Mazrouei and his teammates reported a 24-year-old patient with acute non-necrotizing pancreatitis with concurrent COVID-19. No evidence of pseudo cyst or abscess was detected in his imaging. (10)
Pancreatic damage can be due to the direct effect of the virus on pancreatic cells or indirectly secondary to the immune system. In another study in Wuhan, it showed that ACE2 was expressed in the pancreas higher than the lung in the normal population, indicating that SARS-CoV-2 can bind to ACE2 in the pancreas and cause pancreatic cell damage. (7, 11)
Acute pancreatitis is one of the presentations or complications of COVID-19 infection. Further investigation with samples is needed to reveal the pathophysiology, presentation, treatment and prognosis of acute pancreatitis in COVID-19 infection.
For more information: https://jmedcasereportsimages.org/about-us/
For more submission : https://jmedcasereportsimages.org/
#COVID-19#Cytokine storm#blood cell;HB#aminotransferase#CRP#c-reactive protein#carcinoembryonic antigen#alpha-fetoprotein#anorexia#RT-PCR for SARS-CoV-2#HRCT#Faezeh Sehatpour#jcrmhs
0 notes
Text
normal about medicine im soooo normal about how the human body works
#chewing through metal#on one hand im so tired of fish experiments on the other hand. antibiotics#im normal im fine just don’t bring up spanish flu or tuberculosis or polio or cytokine storms or#‘j don’t u have massive trauma around disease and panic at the sound of coughing’ SHUT UP im multifasceted
0 notes
Text
also preserved on our archive
By Erica Sloan
These days, it’s tempting to compare COVID-19 with the common cold or flu. It can similarly leave you with a nasty cough, fever, sore throat—the full works of respiratory symptoms. And it’s also become a part of the societal fabric, perhaps something you’ve resigned yourself to catching at least a few times in your life (even if you haven’t already). But let’s not forget: SARS-CoV-2 (the virus responsible for COVID) is still relatively new, and researchers are actively investigating the toll of reinfection on the body. While there are still a lot of unknowns, one thing seems to be increasingly true: Getting COVID again and again is a good deal riskier than repeat hits of its seasonal counterparts.
It turns out, SARS-CoV-2 is more nefarious than these other contagious bugs, and our immune response to it, often larger and longer-lasting. COVID has a better ability to camouflage itself in the body, “and it has the keys to the kingdom in the sense that it can unlock any cell and get in,” says Esther Melamed, PhD, an assistant professor in the department of neurology at Dell Medical School, University of Texas Austin, and the research director of the Post-COVID-19 program at UT Health Austin. That’s because SARS-CoV-2 binds to ACE2 receptors, which exist in cells all over your body, from your heart to your gut to your brain. (By contrast, cold and flu viruses replicate mostly in your respiratory tract.)
It only follows that a bigger threat can trigger an outsize immune response. In some people, the body’s reaction to COVID can turn into a “cytokine storm,” Dr. Melamed tells SELF, which is characterized by an excessive release of inflammatory proteins that can wreak havoc on multiple organ systems—not a common scenario for your garden-variety cold or flu. But even a “mild” case of COVID can throw your immune system into a tizzy as it works to quickly shore up your defenses. And each reinfection is a fresh opportunity for the virus to win the battle.
While you develop some immunity after a COVID infection, it doesn’t just grow with each additional hit. You might be thinking, “Aren’t I more protected against COVID and less likely to have a serious case after having been infected?” Part of that is true, to an extent. In the first couple years after COVID burst onto the scene, reinfections were generally (though not always) milder than a person’s initial bout of the virus. “The way we understand classic immunology is that your body will say to a virus [it’s seen before], ‘Oh, I know how to deal with you, and I’m now going to deal with you in a better way the second time around,’” says Ziyad Al-Aly, PhD, a clinical epidemiologist at Washington University in St. Louis School of Medicine and the chief of research and development at the Veterans Affairs St. Louis Health Care System.
But any encounter with COVID can also cause your immune system to “go awry or develop some form of dysfunction,” Dr. Al-Aly tells SELF. Specifically, “immune imprinting” can happen, where, upon a second (or third or fourth) exposure to the virus, your immune cells launch the same response as they did for the initial infection, in turn blocking or limiting the development of new antibodies necessary to fight off the current variant that’s stirring up trouble. So, “when you get hit an [additional] time, your immune system may not behave classically,” Dr. Al-Aly says, and could struggle with mounting a good defense.
Pair that dip in immune efficiency with the fact that your antibody levels also wane with time post-infection, and it’s easy to see how another hit can rock your body in a new way. Indeed, the more time that passes after any given COVID infection, the less of a “competitive advantage” you’ll have against any future one, Richard Moffitt, PhD, an associate professor at Emory University, in Atlanta, tells SELF. His research found that, while people who got sick initially during the delta phase were less likely to get reinfected during the first omicron wave (as compared to folks who were infected in a prior period), that benefit leveled off with following omicron variants.
There’s also the fact that no matter how your immune system has responded to a prior strain (or strains!) of the virus, it could react differently to a new mutation. “We tend to think of COVID as one homogeneous thing, but it’s really not,” Dr. Al-Aly says. So even if your body successfully thwarted one of these intruders in the past, there’s no guarantee it’ll do the same for another, now or in the future, he says.
Getting COVID again and again is especially risky if it previously made you very ill. Dr. Moffitt’s study above also found that the “severity of your first infection is very predictive of the severity of a reinfection,” he says. Meaning, you’re more likely to have a severe case of COVID—for instance, requiring hospitalization or intensive care, such as ventilation—when reinfected if you had a rough go of it the first time around.
It’s possible that some folks are more prone to an off-kilter immune response to the virus, which could then happen consistently with reinfections. The antibodies created in people who’ve had severe cases “may not function as well as those in folks who’ve had mild infections or were able to fight the virus off,” Dr. Melamed says. Though researchers don’t fully understand why, some people’s immune systems are also more likely to overreact to COVID (remember the cytokine storm?), which can cause serious symptoms—like fluid in the lungs and shortness of breath—whenever they’re infected.
Being over the age of 65, having a chronic illness or other medical condition, and lacking access to health care have all been shown to spike your risk of serious outcomes with a COVID infection, whether it’s your first or fifth fight with the virus.
But you’re not home free if you’ve only had, say, a brief fever or cough with COVID in the past; Dr. Moffitt points out that a small subset of people in his research who had minor reactions with their initial infection went on to be hospitalized with a repeat hit. The probability of that might be lower, but it’s still a possibility, he says.
Even if you’ve only had “mild” cases, each reinfection strains your body, upping your chances of developing long COVID. A 2022 study led by Dr. Al-Aly found that COVID reinfections also increase your risk of complications across the board, regardless of whether you recovered just fine in the past or got vaccinated. In particular, it showed that reinfection raises the likelihood that you’ll need hospitalization; have heart or lung problems; or experience, among other possible issues, GI, neurological, mental health, or musculoskeletal symptoms. “We use the term ‘cumulative effects,’” Dr. Al-Aly says, “so, multiple hits accrue and then leave the body more vulnerable to all the potential long-term health effects of COVID.”
That doesn’t mean your experience of a second (or third or fourth) infection will necessarily be worse, in and of itself, than what you felt during a prior case. But with each new hit, a fresh batch of the virus seeps into your system, where, even if you have a mild case, it has another chance to trigger any of the longer-term complications above. While the likelihood of getting long COVID (a constellation of symptoms lingering for three months or longer post-infection) is likely greatest after initial infection, “The bottom line is, people are still getting diagnosed with long COVID after reinfection,” Dr. Moffitt says.
Researchers don’t totally know why one person might deal with lasting health effects over another, but it seems that, in some folks, the immune system misfires, generating not only antibodies to attack the virus but also autoantibodies that go after the body’s own healthy cells, Dr. Al-Aly says. This may be one reason why COVID has been linked to the onset of autoimmune conditions like psoriasis and rheumatoid arthritis.
A different hypothesis suggests that pieces of the virus could linger in the body, even after a person has seemingly “recovered” (reminder that SARS-CoV-2 is scarily good at weaseling its way into all sorts of cells). “Maybe the first time, your immune system was able to fully clear it, but the second time, it found a way to hang around,” Dr. Al-Aly posits. And a third theory involves your gut microbiome, the community of microbes in your GI tract, including beneficial bacteria. It’s conceivable that “when we get sick with COVID, these bacteria do, too, and perhaps they recover [on initial infection], but not on the second or third hit,” he says, throwing off your balance of good-to-bad gut bugs (which can impact your health in all sorts of ways).
Another unnerving possibility: The shock to your system triggered by COVID may “wake up” a latent (a.k.a. dormant) virus or two lurking in your body, Dr. Melamed says. We all carry anywhere from eight to 12 of these undetected bugs at a time—things like Epstein-Barr, varicella-zoster (which causes chickenpox and shingles), and herpes simplex. And research suggests their reactivation could be a contributing factor in long COVID. Separately, the systemic inflammation often created by COVID may spark the onset of high blood pressure and increased clotting (which can up your risk of stroke and pulmonary embolism), as well as type 2 diabetes, Dr. Melamed says.
There’s no guarantee that any given COVID infection snowballs into something debilitating, but each hit is like another round of Russian roulette, Dr. Al-Aly says. From a sheer numbers standpoint, the more times you play a game with the possibility of a negative outcome, the greater your chances are of that bad result occurring. And because every COVID case has at least some potential to leave you very ill or dealing with a host of persistent symptoms, why take the risk any more times than you need to?
Bottom line: You should do your best to avoid COVID reinfection and bolster your defenses against the virus. At this stage of the pandemic’s progression, it’s not realistic to suggest you can avoid any exposure to the virus, given that societal protections against its spread have been rolled back. But what you should do is take some common-sense precautions, which can help you avoid any contagious respiratory virus. (A cold or the flu may not pose as many potential health risks as COVID, but being sick is still not fun!)
It’s a good idea to wear a mask when you’re in a crowded environment (especially indoors), choose well-ventilated or outdoor spaces for group hangouts, and test for COVID if you have cold or flu-like symptoms, Dr. Al-Aly says. If you do get infected, talk to your doctor about whether your personal risk of a severe case is enough to qualify for a Paxlovid prescription (which you need to take within the first five days of symptoms for it to be effective).
The other important thing you should do is get the updated COVID vaccine (the 2024-2025 formula was recently approved and released). Unlike getting reinfected, the vaccine triggers “a very targeted immune response…because it’s [made with] a specific tiny part of the virus,” Dr. Melamed says. Meaning, you get the immune benefit of a little exposure without the potential of your whole system going haywire. Getting the current shot also ensures you restore any protection that has waned since you received a prior jab and that you have an effective shield against the dominant circulating strains. Plus, research shows that being vaccinated doesn’t just lower your chances of catching the virus; it also reduces your risk of having a severe case or winding up with long COVID if you do get it.
So, too, can the deceivingly simple act of keeping up with healthy habits—like exercising regularly, eating nutritious foods, and clocking quality sleep. Maintaining this kind of lifestyle can help you stave off other health issues that could increase your risk of harm from COVID, Harlan Krumholz, PhD, a cardiologist at Yale University and founder of the Yale Center for Outcomes Research and Evaluation (CORE), tells SELF. “Given that we will be repetitively exposed to the virus, the best investments we can make are in our baseline health,” he says.
Doing any (or all!) of the above is a big act of compassion for yourself, the people you love, and your greater community. “For the average person, it’s like, ‘Oh, COVID is gone,’ but they’re just not seeing the impact,” Dr. Al-Aly says, noting the invisibility of long COVID symptoms like disorienting brain fog and crushing fatigue. The truth is, in plenty of people, just one more infection could be the difference between living their best life and facing a devastating chronic condition.
#mask up#covid#pandemic#covid 19#wear a mask#public health#coronavirus#sars cov 2#still coviding#wear a respirator#lokng covid
137 notes
·
View notes
Text
stick and poke ghost pepper photobomb
I'm stealing this from Twitter

Here's the link
I am a high-definition gateway drug body double!
30K notes
·
View notes
Note
so I’ve always had dermatographia, but since getting Covid for the 4th time this fall, I also am spontaneously breaking out on hives on my back a couple times per week. It doesn’t seem to do much, just kind of itches and then goes away after a half hour. I have no known allergies. Do you think this is indicative of some kind of mast cell issue? I can’t tell if this is an episode of weird body, meh, or a red flag of a huge impending problem.
There was a study released this year about long-covid and how it can result in symptoms similar to MCAS.
Let's see if I can find it... Ah. Here.
So, obviously, we won't know the full ramifications of covid for probably decades, but in the meantime, there is some evidence to suggest that long-covid patients show abnormal mast cell release of excessive cytokine (among other things), which is, well, when it fucks up, it fucks up.
That's what made the cytokine storms patients were experiencing in the early days of covid so dangerous. It's like the immune system equivalent of throwing napalm onto a housefire.
(I also suspect that's why so many front-line doctors now believe in the severity of MCAS. They were watching this shit happen in real-time.)
So, is it possible your recurrent covid infections have led to a bit of mast cell instability and causing spontaneous hives? Speaking anecdotally from the sheer volume of emails people have sent me and the MCAS forums now flooded with people who got covid and can't stop itching, yeah, it's possible.
But it's also possible it won't progress beyond that point.
I'd advise keeping an eye on it and talking to your doctor if you have concerns.
Also, maybe look into getting re-tested for allergies. Allergies can develop at any time in your life, and there could be another explanation for the hives.
Basically, don't panic, but do take care of yourself and watch for any other symptoms. Don't ignore any sudden new food allergies or gastro or cardio symptoms. The sooner MCAS is treated, the easier it is to manage. Mine had decades to run rampant on my body to get to the stage it was at. It doesn't have to be that way for everyone.
Take care, and I hope the hives stop!
201 notes
·
View notes
Text
hi, I am ok rn 👍🏻 sorry for anyone I worried, I had a really bad panic attack because I wasn't sure what was going on with my body and I web'md. I was really overworked and it spiked my heart rate
In still a lot of pain and nausea, but I will head to the hospital if I don't feel better in a day or two. I talked to my nurse family member and my dad spoke to the Dr to see if this was a cytokine storm or my pcos or the possible pots. thank you to everyone who offered prayers and kind words, I feel embarrassed posting so many things but also really appreciate everyone's kindness and prayers. Thank you guys!!!!!

my cat, Faramir
295 notes
·
View notes
Text
lycanum heisenberg hcs / info
Omega-lycans are Cadou-infected potential lycans who do not survive to become a full lycan, or have general failure to thrive as a lycan. Most of them are allergic to their own MAOA and OXTR receptors and die from multiple acute neurotransmitter deficiencies, as well as cytokine storms/septic shock and brain damage.
Beta-lycans are Cadou-infected lycans who have near-total death of the cells that produce Monoamine Oxidase A, polymorphisms mainly consisting of L/L along SLC6A4, HTR2A and HTR2B, very low 5-Hydroxyindoleacetic Acid (to the point of, at times, coma/stupor), disturbance of DRD4, and significant prefrontal cortex damage.
Alpha-lycans are Cadou-infected lycans who retain some MAOA receptor regulation, whose polymorphisms of SERT do not test out to low 5-Hydroxyindoleacetic Acid (or do so only in prolongued sun and heat), have a disturbance of DRD4, and do not have significant prefrontal cortex damage. They are almost always severely brainwashed and, like Type-II Plagas, rarely, if ever, live in reality, often experiencing intense delusions as a result of hallucinations 'set' by a Mother Lycan. Their brains on MRIs are riddled with lesions associated with the death of dopamine receptors, which is thought to explain much of the hallucinatory effect.
Mother Lycans are Cadou-infected lycans who retain MAOA receptor regulation, test out for low 5-Hydroxyindoleactic Acid, have a disturbance of DRD4, but have little to no prefrontal cortex damage. Their brains are largely intact, leading to little to no loss of intellect. They have very little light tolerance and typically suffer from severe bodily hirsutism after the onset of mycosis in an attempt of the molds' self-defense. A Mother Lycan can avoid hair and skin mutation by remaining in the dark. Mother Lycans are not necessarily genderlocked, but are named after Mother Miranda. Eveline is also, technically, a Mother Lycan, though a far more stable one.
Cadou are a mix of a fungal root sample in nematodes infected with a T-virus strain that causes mutation under extreme heat stress, which can cause uncontrollable heat itself and calcify its' host if stress and heat exposure are maintained. It is functionably similar to Uroboros and C. Almost every megamycete is contaminated by some degree of T-virus, but only Cadou manufactured by Mother Miranda have various T-virus strains within them, most of which are what she had on hand, Uroboros.
Eveline's mold has t-Phobos properties, leading to her similarities shared with Natalia Korda, up to and including norepinephrine causing mutations.
Karl Heisenberg:
Health
He was able to adapt better to Cadou implantation because he had a mutated immune system with less astrocyte activity and would have likely suffered from dementia in his early fourties if he wasn't turned.
He's a Mother Lycan who retained MAOA receptor regulation.
He is one of the only lycans to preserve his serotonin - his SERT tests out normally in light. He has no disturbance of DRD4 and no MRI dopamine deficiency lesions, but still has localized areas of ischemia where the Cadou nematodes caused bleeding.
His factory megamycete is only visible to the non-infected. The infected perceive it as pulsating wooden cogs and levers with leaves and vines unless they are primed before arriving.
The megamycete is mostly morally neutral, having no consciousness of its' own and instead being unconsciously operated by Karl. His "wolfpack" looks normal to infected when in the factory, but they fade to their true appearance when they leave, leading them to spend most of their time in it.
A close proximity to the megamycete is rejuvenating and extends the lifespan and intellect of beta-lycans, as well as slowly repairing their wounds at the cost of further appearance mutations. Its' presence can keep an omega-lycan from perishing for a month or two.
Dead beta-lycans Karl is close to are typically ceremonially buried in the megamycete, where their memories and consciousness can blend and "live on". Particularly intelligent beta-lycans have a bigger sense of self and blend less, causing influential beta-lycans to project as wolfy ghost-like guides to the infected, though they look terrifying, are often incomplete, and have trouble communicating with non-Cadou infected, causing misunderstandings about their nature among locals that break into the factory.
Lycanum-strain Cadou mycosis is a self-perpetuating spiral due to its' association with wolves feeding into its' ouroboros, causing residents of the factory to act particularly wolfish. Often, long-term infection mutates the feet into becoming ditigrade and the tailbone grows outward. The afflicted's canines (of which almost all teeth eventually fall out to be replaced by canines) grow outward. Ghrelin and motilin production dramatically increase, causing perpetual hunger. The Cadou causes a need for high protein intake.
Mental
Mother Miranda tried to brainwash him with a combination of corporal punishment and eugenics teachings to soften him with the suggestibility of mycosis and Cadou infection (when in contact with an Alpha or Mother Cadou strain), the aggression and anger of the mycosis infection's effect on the brain, and to strengthen the ideal of eugenics for the purpose of using him to create lycans until she could find a suitable host for her daughter.
He developed a homicidal desire to murder her and pretended to accept her world view as a way of avoiding death, his desire causing her own aggression to slowly spiral out of control until she began to notice mutations on her skin. She fled the factory to preserve her body's integrity, leaving Karl with a tribe of feral Omega-lycans, Beta-lycans, and a tiny megamycete.
Miranda, in her mounting stupor and fear, used stolen anti-parasitics to seal off the factory. Infected who enter erroneously tie their death rate to the factory itself instead of the potent anti-parasitics, giving it an awful reputation.
Karl and the wolfpack are often forced to rely on cannibalism to survive, as Karl is one of the only people capable of exiting the factory safely. This degrades their psyches considerably, bolstered by constant hallucinations and shaky sanity from most residents of the factory having been tortured by Miranda.
Miranda still arranges meetings, but Karl is not present. Due to Karl's effect on Miranda and Dimitrescu as the dominant consciousness of the factory megamycete, Dimitrescu (very shakily) tolerates him and views him like a human pet, but Miranda avoids him.
Misc
Karl does his best to provide for the residents by providing them with snack cakes and foods he buys from the Merchant. He provides the Merchant a combination of crafted weapons, pottery and art by residents, and completes errands.
He is mostly tech-illiterate but can fix pneumatic systems, operate DOS and Amiga, and to a small degree zOS and Solaris. He can read engineering schematics for electronic engineering but can't build complex electronics due to lack of modern, trustworthy cap/resistor/etc production. He is a genius at analog machinery and clockwork and can craft homemade music boxes and watches easily.
Ethan Winters, Mia, Jill, Notes
Ethan Winters is considered a Full Mycote. He is abnormally stable, presenting with no outward mutations because he, too, lacks DRD4 issues and dopamine deficiency lesions. This is because he erroneously carries the marker of a mold cluster supermycete, meaning he hosts his own consciousness within himself and can propel it, like his daughter, through other clusters. His brain is the location of the supermycete. One side effect of this is that he needs constant haircuts and has to shave a near-full neckbeard every single morning, a result of the mold attempting to grow out.
Rosemary Winters is a Full Mycote with a supermycete where much of her intestines and uterus would be. She has no bladder, no large intestine, no uterus, no ovaries, no pancreas, and no spleen. Her consciousness is within herself, and she unintentionally, unconsciously picks up bits of the consciousnesses of other mycotes. She has a large amount of her father's consciousness copied within her supermycete unintentionally.
Jill Valentine's T-Virus infection causes her to become infected with a strain of the Progenitor virus that technically meets Wesker's satisfactory desire of a virus free of negative effects, unbeknownst to him. After the Alcatraz incident, in 2021, she ends up in Romania on a hunt from the BSAA to find Rosemary and Ethan Winters, who she sympathizes deeply with. Attempting to enter Castle Dimitrescu infects her with the mold, but because Karl had been acting as a housekeeper recently, she is infected with Karl's strain. Because of this and her existing infection, she retains physical normalcy, though she is still subject to hallucinations that are memories of Miranda's torture. Realizing this, her hatred and paranoia for Miranda increases. It also provides her with information about Miranda she otherwise would never have as she is forced to experience visual and auditory hallucinations that increase relative to her proximity to Karl or his "wolfpack".
Jill's understanding of the situation and natural proclivity primes her to tolerate the mold in a way similar to Ethan Winters, allowing her to tell when something is or is not real. Hallucinations and psychological effects, such as the urge to remain in the factory for safety, or the hallucination of the "wolfpack" bearing S.T.A.R.S emblems occur more often in the factory due to the presence of the Karl-dominant megamycete.
Dimitrescu views Karl in a flux state of disgust and pity depending on her proximity to the megamycete and how much of Karl's strain is growing around her castle. The level of delusion she lives in reacts oddly with Karl's inadvertent delusion, which means she might treat him like a literal pet dog if she's particularly afflicted. She feels a degree of "wrongness" when she becomes this afflicted as a result of Miranda's priming, so it's rare for it to last long.
Dimitrescu's daughters live in their delusion constantly, so they treat Karl like an actual dog, which abates much of Dimitrescu's aggression towards him. He absolutely hated it in the beginning, but now he just... leans into it to avoid going insane. Sometimes he gets kicked out for trying to save victims, but the degredation of his morals surrounding torture and cannibalism over years of exposure and trauma make him avoid it and curry their favor more often. Besides, they occasionally provide his wolfpack with a source of food, a rarity he cannot deny.
His factory is quasi-functional. Lycans are often too sick to work, but those that retain enough intellect can feel the urge to do what Karl desires, and as he desires a working factory, it stays in strangely good condition and sometimes produces items. It is a shifting terrain because of retrofitting for personal projects. Despite being maintained, it is horrifyingly filthy.
#resident evil#resident evil 8#resident evil village#karl heisenberg#re village#lady dimitrescu#lycanum karl#/dev/writing/#tw medical#tw blood#tw emetophobia#tw drugs#tw unreality
12 notes
·
View notes


