#Carcinoma
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr has 16.74 million mobile monthly users in the US.
Text
The world awaits more news about the King's health and wellbeing.

King Charles III has a form of cancer. The prayers & good wishes of the British Commonwealth will follow him throughout his new journey.
#His Majesty King Charles III#Buckingham Palace#carcinoma#BPH#Commonwealth#Head of State#wellness journey#UK
44 notes
·
View notes
Text










#olympic orchids#night flyer#zoologist perfume#zoologist#bat#ellen covey#cannibal holocaust#ruggero deodato#carcinoma#marian dora
8 notes
·
View notes
Text

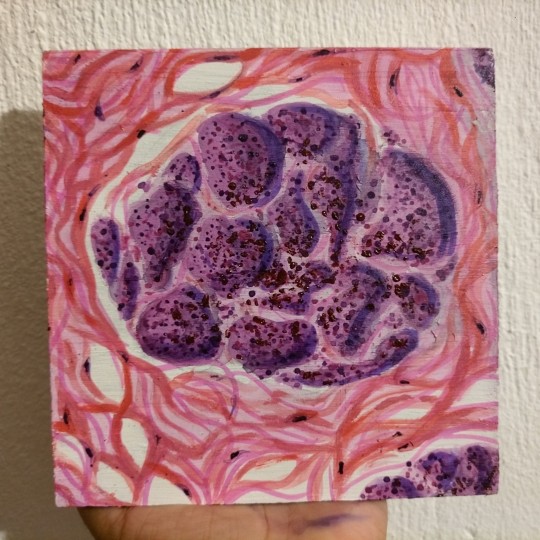

Lobular carcinoma of the breast 🧫💓
Ah yes, una pintura de una imagen histologica ajsjjs. Desde que empecé el semestre y vi por primera vez una laminilla quise pintar algo de ello y pues aproveché el carcinoma de mama (qué era la imagen histologica favorita de mi maestro favorito) para pintarsela de regalo por el fin del semestre sjsjsjs. Le gustó aunque al principio pensó que era un glomérulo, ya después dijo que sí parecía glándula jaksjaja

Él es mi tío aunque no lo sepa jajaja
4 notes
·
View notes
Text

Passei uns minutos pensando em como iniciar esta postagem. Na verdade eu ainda nem sei a melhor forma, mas vamos lá.
Tempos atrás eu postei aqui no #Tblr um exame que fiz #PAAF (punção aspirariva por agulha fina) e, contei como é chatinho e dolorido.
Ontem 23/02/2024 recebi o diagnóstico deste exame. Veio em palavras assustadoras: tumor, câncer e depois disso meu cérebro ficou tentando processar exatamente o que eu tinha ouvido. Mas deixa eu dar um nome mais pomposo: carcinoma papilifero é o nome do meu câncer de tireoide. O nome pomposo não me faz sentir melhor, o tratamento é cirurgico, então, bem... não dá para ficar feliz com nada disso.
Depois da consulta com o endócrinologista, fui fazer uns exames. A real é que minha fica ainda não havia caído, eu estava tranquila, contei para meu namorado, depois pra minha mãe porque ia precisar de algumas ajudas para correr atrás de uns médicos e coisa é tal. Trabalhei nesse dia, vida normal. Eu acho que realmente não havia processado direito o impacto da notícia.
O problema mesmo veio hoje cedo, eu tive um sono meio conturbado, mas assim que acordei a ficha caiu. Eu tenho um câncer!
A angustia bateu, e só então veio o pensamento: "Vou ter que retirar minha tireoide inteira e por onde mais seria feita essa ciruriga? pelo pescoço, é claro!" Peguei o celular e pesquisei sobre a cirurgia, a primeira coisa que vi foram as cicatrizes dessa cirurgia. A minha pressão caiu na hora, me veio um mal estar, uma bagunça na cabeça, os pensamentos enlouqueceram, um aperto no peito que parou na garganta, foi um mix de emoções que eu nunca havia experimentado. Voltei para a cama meio tonta e só então, eu chorei.
Mas eu precisava ir para o trabalho ainda, quando emenizou todas as sensações, eu fui, dirigi meio inerte até a empresa. Quando cheguei compartilhei o assunto com uma colega de trabalho porque, claramente, vu começar a precisar de apoio nas atividades, quando eu tiver que sair para consultas, exames e a própria cirurgia. Caí no choro!
A verdade é que conforme as horas passam, eu fico mais confusa, mais tensa, triste, mas principalmente com bastante medo.
Agora é 1h da manhã e eu não consigo dormir, fui deitar muito cedo umas 21h levantei mais ou menos 23h pelo medo. A cabeça está uma bagunça, chorei, andei pela casa e comecei então a buscar pessoas que já tenham passado por isso, ora vejo um relato ruim, ora um menos ruim. Não sei bem o que pensar ainda e, eu acho que é bem normal todo esse mix de sensações. E é bem desesperador. Entre pensamentos e choro, eu estou tentando ficar bem (pelo menos para conseguir dormir).

Acabei de ver um depoimento de uma moça em outra rede, que passou pela mesma coisa e de alguma forma me trouxe um pouco de calma, eu não sei até quando, mas por enquanto consegui arrumar uma energia e escrever esse post.
Eu não sei o que vai acontecer, eu estou um pouco desesperada e ansiosa para resolver o problema. Mas é final de semana agora é não tenho muito o que fazer. A cabeça está a mil e acho que nunca usei um emoji que coubesse tanto 🤯.
Preciso respirar, trabalhar a aceitação e confiar que vai dar tudo muito certo. Estou com muito medo de tudo isso, mas vou com medo mesmo.
Não vou poupar as fotos dos meus últimos momentos com meu pescoço sem uma cicatriz.
Mesmo que sejam fotos em que tenha acabado de chorar 🤷🏻♀️
Agora meu próximo passo é tentar ficar calma e construir a minha rede de apoio, amanhã é o dia que começo a falar com a minha família, que vai ser fundamental em minha nova jornada. E contar com pessoas disponíveis para mim vai ser de muito conforto!
Alguns amigos (mas pouquíssimos) também vou falar sobre, isso porque vou precisar me ausentar de eventos, encontros e vários momentos importantes com eles. E como tenho pessoas que são importantes para mim, vou compartilhar de forma leve. Apenas para que entendam a minha distância, pelo menos por um tempo!
A gente nunca acha que vai acontecer com a gente, né?
Mas a gente não tem controle de nada =(
E as coisas só acontece.
Agora é o meu momento de resiliência!
#joy#delajoy#brazil#câncer de tireoide#carcinoma#papilifero#pescoço#desfios#relatos#my diary#tumblertime#mental health#depressão#myself#desabafo#tiroides#salud mental#soledad#empatia#resilience#resiliência#empathy#me#health#thyroid cancer#thyroid#tireoidectomia
2 notes
·
View notes
Text
#NowPlaying: "YJBM Science News Podcast: Episode 8" by YaleUniversity
#Nowplaying#Newmusic#SoundCloud#science#news#Yale#healthcare#PFAS#forever#chemicals#colorectal#carcinoma#problematic#alcohol#use#genetics#hip hop#rnb#electronic#jazz#lofi
2 notes
·
View notes
Text
CReI. Roma: WORLD CANCER DAY '25 IL MESSAGGIO CREI: L'UNITA' DEGLI SPECIALISTI PER ASSICURARE PREVENZIONE, DIAGNOSI E CURA
COLLEGIO REUMATOLOGI ITALIANI: WORLD CANCER DAY '25 IL MESSAGGIO CREI: L'UNITA' DEGLI SPECIALISTI PER ASSICURARE PREVENZIONE, DIAGNOSI E CURA
COLLEGIO REUMATOLOGI ITALIANI: WORLD CANCER DAY ’25 IL MESSAGGIO CREI: L’UNITA’ DEGLI SPECIALISTI PER ASSICURARE PREVENZIONE, DIAGNOSI E CURA ROMA, 4 FEBBRAIO 2025 – “Uniti dall’unicità”: questo il tema del World Cancer Day 2025, giornata in cui tutti i sistemi sanitari, i cittadini, i pazienti e le società sono chiamati a riflettere sugli obiettivi da raggiungere per vincere la sfida complessa…
#Alessandria today#Antonio Giordano#Approccio Olistico#benessere del paziente#carcinoma#collaborazione specialistica#COLLEGIO REUMATOLOGI ITALIANI#CReI#cura dei tumori#Daniela Marotto#diagnosi precoce#etica medica#Giornata mondiale contro il cancro#Google News#immunologia#infiammazione e tumori#Innovazione medica#italianewsmedia.com#linfoma#malattie autoimmuni#malattie reumatiche#medicina integrata#medicina moderna#medicina personalizzata#onco-reumatologia#oncologi#Oncologia#pazienti oncologici#Pier Carlo Lava#Prevenzione oncologica
0 notes
Text
Transitional cell carcinoma
DOI:10.5281/zenodo.14600717 Transitional cell carcinoma (TCC), or urothelial carcinoma, is the predominant form of bladder cancer, accounting for 90-95% of global cases. It ranks as the fourth most common cancer in men and the tenth in women in the United States, with higher incidences in developed regions. TCC predominantly affects older adults, particularly males over 50, representing a…
#Carcinoma#Cystoscopy#Dysuria#Hematuria#Obturator Nerve#Obturator Neuropathy#Transitional cell carcinoma#Urothelial Carcinoma
0 notes
Text
Basal cell carcinoma resection in an Ecuadorian patient with Gorlin-Goltz syndrome by Andrea Villarreal-Juris in Journal of Clinical Case Reports Medical Images and Health Sciences
Abstract
Gorlin-Goltz syndrome is an inherited dominant autosomal disorder characterized by a predisposition to numerous cancers. The clinical-pathological findings of this syndrome are very diverse. The objective of this report is to present an Ecuadorian patient with Gorlin-Goltz syndrome who underwent surgical resection of basal cell carcinoma compatible lesions.
Conclusion: Gorlin-Goltz syndrome encompasses a variety of clinical signs and symptoms, including important oral manifestations and skin lesions that must be recognized to achieve an early specialty referral, thus reducing the risk of malignancy through a multidisciplinary treatment.
Keywords: Basal Cell Nevus Syndrome, Gorlin-Goltz syndrome, Carcinoma, Basal Cell
Introduction
Gorlin-Goltz (G-G) syndrome or nevoid basal cell carcinoma syndrome (NBCCS) is a dominant autosomal genetic disorder with high penetrance. Fifty percent of patients who suffer from it have a mutation in the long arm of chromosome 9q22.3 in the area of the PTCH gene (protein patched homolog) (1–3), a homologue of the Drosophila patched gene (PTC), which encodes a transmembrane receptor protein (4). This protein binds to a soluble factor of the hedgehog family (Hh), thus activating the Smo (smoothened) receptor, which unblocks the transcription of several growth factors. Therefore, the PTCH gene is an oncosuppressor that is part of the Sonic Hedgehog Homolog (Shh) signaling pathway and is crucial in embryonic development, cell division control, and tumor growth (5).
Its approximate prevalence is 1 in 57000 to 1 in 256000 and the ratio of males to females is 1:1 (6). Binkley and Johnson reported this syndrome for the first time in 1951 (7), then, in 1960, Gorlin and Goltz described the association between multiple basal cell carcinoma, odontogenic keratocysts (OKC) and bifid ribs, which account for the characteristic triad (8). In 1977, Rayner et al. added additional features, including calcification of the falx cerebri and palmar/plantar fossae (9).
According to the criteria of Kimonis et al., the diagnosis of G-G syndrome requires the coexistence of at least two major criteria or one major and two minor (10).
The characteristic that is usually diagnosed first is OKC, because it can be detected during the first decade of life and appears in almost 80% of G-G syndromes.
Other manifestations include palmar and plantar ulcers that appear as shallow pits, caused by partial or complete absence of the corneal layer, which can also appear along the sides of the hands and fingers and even on the tongue; spina bifida (10,11); medulloblastoma (can be an epiphenomenon of G-G, especially in children who are ≤5years-old) (12); cardiac tumors, including fibromas and ventricular histiocytomas, usually congenital (13); hypertelorism, congenital cataract, nystagmus, coloboma and strabismus (14); and ameloblastoma (extremely rare) (15,16).
Early diagnosis of G-G syndrome and its subsequent treatment are very important due to neoplasm susceptibility (2).
The case of a patient with a previous diagnosis of Gorlin-Goltz syndrome who presented multiple lesions compatible with basal cell carcinoma is presented below.
Case Report
A 35-year-old male, living in Quito, Ecuador, without allergies; no history of tobacco or alcohol intake. His mother and his brother presented Gorlin-Goltz syndrome (G-G).
The patient presents hereditary and congenital G-G syndrome (multifocal basal cell carcinoma and maxillary keratocysts), whose manifestations began at the age of 22. He underwent surgery for bilateral keratocysts at the age of 25, and multiple biopsies of the upper left eyelid were taken since 2012. In August 2015, with a positive tumoral activity biopsy report, a wide resection involving 60% of the left upper eyelid plus flap reconstruction was performed.
Physical examination revealed multiple surgical scars on the left upper eyelid with tumoral activity on the eyelid margin, as well as on the outer third of the ipsilateral lower eyelid and on the right side.
In October, a wide resection of the left upper and lower eyelid was planned, plus reconstruction and transoperative study, which are performed without complications.
Subsequently, the patient attended scheduled control, reporting the presence of a left superciliary nodular lesion. Physical examination revealed multiple lesions located in the left superciliary region, left helix, concha, and antihelix, in the inner corner of the left lower eyelid, in the left parieto-temporal and occipito-temporal regions, and other small bilateral genian lesions. There were no alterations in the flap. Left external campimetry was limited. It was decided to perform a facial bone and skull simple and contrasted tomography (CT) and laboratory tests.
Then, resection of the previously mentioned lesions and resection of the lower eyelid with transoperative study, shield-type incision and external canthoplasty of the lower left eyelid was planned. A plastic surgeon was included in the surgical team.
Altogether, 9 skin lesions located in the left superciliary, left frontal, interparietooccipital, posterior occipital, auricular, and left retroauricular regions were resected, which were positive for basal cell carcinoma.
In the subsequent control, the patient's campimetry showed improvement.
DISCUSSION
Reports about Gorlin-Goltz syndrome are scarce in the literature (17). The rarity and phenotypic variability of this syndrome causes a delay in its diagnosis. Syndromicassociated keratocystic odontogenic tumors are often treated in the same way as nonsyndromic cases (18) and associated systemic signs can easily be missed due to lack of understanding of the syndrome. In addition, their characteristics vary globally, so doctors and even dentists must identify them in a timely manner, considering those that are more prevalent in their population or similar populations (19,20).
The pathogenesis of basal cell carcinoma (BCC) is thought to involve increased sensitivity to ultraviolet light and to involve ineffective mechanisms that repair UVinduced DNA damage. In any case, this theory is not accepted by all authors since these lesions can also appear in areas that have not been exposed to sunlight. Especially in children, patients with G-G syndrome who undergo radiotherapy for other cancers have shown to be at increased risk of radiation-induced BCC (21).
In 50% of patients with G-G syndrome, jaw keratocysts appear, characterized by a thin surrounding layer of epithelial cells, which tend to reappear locally after excision in 6 to 60% of cases, therefore, the indication for surgery should be carefully considered, also due to the possibility of intensive clinical and instrumental monitoring (22).
In recent years, new drugs have been developed to inhibit certain components of the sonic hedgehog signaling pathway. In 2013, the FDA approved vismodegib, the first small molecule to target this pathway (11). Although these agents seem promising options for patients with G-G syndrome, their efficacy is limited by adverse effects and the development of resistance (23). Logically, a more aggressive approach is necessary if basal cell carcinoma is suspected; subsequently, depending on the lesion site and the surgery type, a reconstruction can be performed, as in the case presented in this article (24,25).
CONCLUSION
Gorlin-Goltz syndrome encompasses a variety of clinical signs and symptoms, including important oral manifestations and skin lesions that must be recognized to achieve early referral to a specialty, thus reducing the risk of malignancy through multidisciplinary treatment.
Ethical responsibilities
In this case report, the informed consent of the patient was obtained. Its elaboration and all the inherent details were based on the Declaration of Helsinki.
#Basal Cell Nevus Syndrome#Gorlin-Goltz syndrome#Carcinoma#Basal Cell#JCRMHS#Clinical decision making#Clinical Images journal
1 note
·
View note
Text
Is Mesothelioma a Carcinoma?
Introduction Mesothelioma is a rare but aggressive form of cancer that develops in the lining of the lungs, abdomen, or heart. Given its unique characteristics and its link to asbestos exposure, many people wonder if mesothelioma falls under the category of carcinoma. This article explores whether mesothelioma is classified as a carcinoma and provides insights into its nature and causes.
Contact Us Now For a Free Consultation
1. What Is a Carcinoma? Carcinomas are cancers that originate in the epithelial cells, which form the lining of organs and tissues throughout the body. They are among the most common types of cancers.
Typically found in organs like the lungs, breasts, prostate, and colon.
Arise from cells that cover internal or external body surfaces.
2. Is Mesothelioma Considered a Carcinoma? While mesothelioma and carcinoma share similarities, they are not the same. Mesothelioma develops in the mesothelium, a protective layer covering internal organs, whereas carcinomas begin in epithelial cells.
Mesothelioma origin: Mesothelium (lining of lungs, abdomen, heart).
Carcinoma origin: Epithelial cells (lining tissues and organs).
3. Differences Between Mesothelioma and Carcinoma Understanding the distinction between these two cancer types helps in diagnosing and treating them correctly.
Mesothelioma: Rare, linked directly to asbestos exposure, difficult to diagnose.
Carcinoma: More common, can develop from a variety of causes, generally easier to identify early.
4. How Does Asbestos Exposure Relate to Mesothelioma? Exposure to asbestos fibers is the primary cause of mesothelioma. When inhaled, these fibers become lodged in the lining of the lungs or abdomen, leading to inflammation and scarring that can trigger tumor growth.
High-risk occupations: Construction workers, shipbuilders, and factory workers.
Latency period: Symptoms may take 20-50 years to appear after exposure.
5. Is Mesothelioma Treatable? While there is no cure for mesothelioma, treatment options aim to control the disease, alleviate symptoms, and improve quality of life.
Treatment options include:
Surgery (to remove tumors)
Chemotherapy (to shrink tumors)
Radiation therapy (to target specific areas)
6. Why Is It Important to Understand the Difference Between Carcinoma and Mesothelioma? Differentiating between carcinoma and mesothelioma is crucial for determining the most effective treatment plan. Misdiagnosis can lead to inappropriate therapies, potentially reducing a patient’s quality of life.
Accurate diagnosis: Essential for optimal treatment.
Specialist consultation: Recommended for tailored care.
Conclusion Mesothelioma is not classified as a carcinoma but rather as a type of cancer that affects the mesothelium. Understanding its unique nature, causes, and available treatments can help those diagnosed navigate their options more effectively. If you or a loved one has been exposed to asbestos, seeking medical advice early is key to managing risks.
FAQs
Is mesothelioma always caused by asbestos exposure? Yes, the majority of mesothelioma cases are linked to prolonged asbestos exposure, although rare cases without such exposure exist.
Can mesothelioma be misdiagnosed as carcinoma? Yes, due to overlapping symptoms and imaging results, mesothelioma can sometimes be misdiagnosed as carcinoma. A biopsy is often required for accurate diagnosis.
What are the early symptoms of mesothelioma? Symptoms include shortness of breath, chest pain, persistent cough, and unexplained weight loss.
Is mesothelioma hereditary? Mesothelioma is not typically inherited, but some genetic factors can increase vulnerability to asbestos-related conditions.
What is the prognosis for mesothelioma? Prognosis depends on factors like stage of the cancer, patient age, and overall health, but the disease is generally aggressive with a lower survival rate.
Why is early detection of mesothelioma difficult? Due to its long latency period and symptoms that mimic other conditions, mesothelioma is often diagnosed at an advanced stage.
0 notes
Text
🔴🟡🟢 ABCDE DEL MELANOMA

1 note
·
View note
Video
youtube
ULJE CRNOG KIMA – DJELOVANJE KAO LIJEK ZA SVE BOLESTI! (Kako i koliko ga...
#youtube#black cumin#black cumin oil#black cumin seed oil#ulje crnog kima#astma#bronhitis#psoriasis#psorijaza#multiple sclerosis#multiple sclerosis warriors#cancer#cancer warriors#chemotherapy#carcinoma#tumor#neurodermatitis#ekcemi#edemi#seborrheic dermatitis#insomnia#menstrual health
0 notes
Text










#olympic orchids#night flyer#zoologist perfume#zoologist#bat#ellen covey#cannibal holocaust#ruggero deodato#carcinoma#marian dora
6 notes
·
View notes
Text
#federicodeho#gabrieleantonini#prostheticsurgery#robotdavinci#varese#ralp#prostatectomy#infrapubic#penissurgery#deficitectomy#carcinoma
0 notes
Text
Câncer no fígado: 5 sintomas que podem ser confundidos com indigestão
Os sinais de câncer de fígado podem ser facilmente confundidos com sintomas de indigestão devido à sua natureza inicialmente não específica. Embora muitas vezes ignorados ou atribuídos a problemas digestivos comuns, é importante estar atento a esses sinais, pois podem indicar um problema mais sério. Tipos de câncer de fígado O câncer de fígado pode ser de dois tipos: primário (que começa no…

View On WordPress
#angiossarcoma#carcinoma#câncer#Câncer no fígado#colangiocarcinoma#desconforto abdominal#dor abdominal#hepatocarcinoma#indigestão#intestino grosso#problemas digestivos#saúde#tumor maligno
1 note
·
View note
Text

Se rappeler de la structure tubulaire et papillaire de façon rudimentaire
0 notes
Text

Call for Abstract: Track 2 : Hepatology We are happy to announce the call for abstracts for the 14th World Gastroenterology, IBD & Hepatology Conference from December 17-19, 2024, in Holiday Inn Dubai, UAE & Virtual. Submit your abstract/papers here: https://gastroenterology.universeconferences.com/hepatology/ WhatsApp us: https://wa.me/442033222718?text=
#Hepatology#LiverHealth#LiverDisease#Hepatitis#Cirrhosis#FattyLiver#LiverTransplant#LiverCancer#HepB#HepC#LiverPathology#LiverCare#HepatologyConference#LiverImaging#Hepatocellular#Carcinoma
0 notes