#Additional director medical and health
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
In 2020, Tumblr had 29.4 million users in the US.
Text
RTI Appeal Insights: DG Karmik's Role
Welcome UPICR20240000149 UTTAR PRADESH INFORMATION COMMISSIONSecond Appeal under section 19(3) of the Right to Information Act, 2005Appeal Registration Number – A-20250101421Appeallent’s ParticularsApplied Date : 17/01/2025 10:37:04 AM Name Yogi M P SinghGender MaleState UTTAR PRADESHDistrict MIRZAPURTown/Village मिर्जापुरPincode 231001Mobile Number 7379105911Email [email protected]…
#Additional director medical and health#Directorate medical and health#JD DG Karmik#Medical and health
2 notes
·
View notes
Text
RNN:
The resistance forces activated sirens in Jenin after discovering a zionist army special forces unit, prompting their vehicles to withdraw from the "Dotan" checkpoint.
A wide-scale invasion by the occupation army has been launched into Jenin following the announcement of an enemy military operation targeting the city and its refugee camp.
The IOF launched an airstrike on a vehicle and at least one martyr has arrived at Jenin Governmental Hospital.
Several injuries by IOF bullets are reported.
Fierce armed clashes erupted as resistance groups confront the invasion.
An IOF helicopter is opening fire with machine guns in the vicinity of the Jenin refugee camp.
Local sources report that Palestinian Authority Security Forces' vehicles have withdrawn from the vicinity of the Jenin refugee camp following the wide-scale invasion by the occupation army.
[…]
The occupation is preventing medical teams from reaching martyrs and injuries.
The IOF is directly opening fire on civilians, including a family in a car.
[…]
An israeli sniper opens fire on an elderly Palestinian in the streets of Jenin.
[…]
Palestinian Minsitry of Health (Update 4:00 PM):
8 martyrs have ascended and more than 35 are injured as a result of the occupation's aggression on Jenin.
[…]
Occupation forces bombed the neighborhood of Joura Al-Dahab in Jenin camp with local reports indicating the IOF had targeted a group of paramedics.

A child was injured by shrapnel from the occupations bullets in Jenin camp.
[…]
For the third time today, the zionist army has carried out another bombing in Jenin camp in the Al-Damej neighborhood.
A martyr has ascended and one person is wounded as a result, raising the total number of martyrs in Jenin today to 9.
[…]
Updates from Jenin:
The IOF continues its treacherous aggression against Jenin and its camp.
Violent clashes were between the resistance and the occupation forces in the "Talaat al-Ghabz" area surrounding Jenin camp, during which a heavy explosive device was detonated, according to Quds News Network. In addition, the resistance targeted the occupation forces with an explosive device near the entrance to the town of Yamoun, west of Jenin.
The Ministry of Health reports 9 martyrs and about 40 wounded as a result of the ongoing aggression.
Over five airstrikes have been carried out by the occupation on Jenin Camp and its surroundings since the incursion began this morning.
Dr. Nader Ershid, Dr. Khaled Zakarneh, Dr. Abdullah Al-Zahir, nurse Mohammed Amarna, and nurse Ashraf Alawneh were injured by IOF gunfire in various locations near Jenin Governmental Hospital, Al-Amal Hospital, and Al-Razi Hospital, according to Director of Jenin Governmental Hospital, Wisam Bakr.
In addition, the IOF hindered the work of medical teams and prevented them from reaching casualties. Meanwhile, the treacherous PA Security Forces who withdrew minutes before the incursion stormed Jenin Governmental Hospital and raided the room of the martyr Khalil Al-Saidi, searching for those wounded by the occupation's bullets, and assaulted the mothers of the martyrs, according to local sources.
The IOF arrested a young man after injuring him and besieging a house in the town of Ti'nik, northwest of Jenin.
The forces fired shoulder-launched rockets on several instances. Several injuries by IOF bullets were reported including the mother of martyr Karim Abu Subaih who was shot in the leg.
Bulldozers continue to destroy the infrastructure in various areas.
182 notes
·
View notes
Text
also preserved on our archive
By Erica Sloan
These days, it’s tempting to compare COVID-19 with the common cold or flu. It can similarly leave you with a nasty cough, fever, sore throat—the full works of respiratory symptoms. And it’s also become a part of the societal fabric, perhaps something you’ve resigned yourself to catching at least a few times in your life (even if you haven’t already). But let’s not forget: SARS-CoV-2 (the virus responsible for COVID) is still relatively new, and researchers are actively investigating the toll of reinfection on the body. While there are still a lot of unknowns, one thing seems to be increasingly true: Getting COVID again and again is a good deal riskier than repeat hits of its seasonal counterparts.
It turns out, SARS-CoV-2 is more nefarious than these other contagious bugs, and our immune response to it, often larger and longer-lasting. COVID has a better ability to camouflage itself in the body, “and it has the keys to the kingdom in the sense that it can unlock any cell and get in,” says Esther Melamed, PhD, an assistant professor in the department of neurology at Dell Medical School, University of Texas Austin, and the research director of the Post-COVID-19 program at UT Health Austin. That’s because SARS-CoV-2 binds to ACE2 receptors, which exist in cells all over your body, from your heart to your gut to your brain. (By contrast, cold and flu viruses replicate mostly in your respiratory tract.)
It only follows that a bigger threat can trigger an outsize immune response. In some people, the body’s reaction to COVID can turn into a “cytokine storm,” Dr. Melamed tells SELF, which is characterized by an excessive release of inflammatory proteins that can wreak havoc on multiple organ systems—not a common scenario for your garden-variety cold or flu. But even a “mild” case of COVID can throw your immune system into a tizzy as it works to quickly shore up your defenses. And each reinfection is a fresh opportunity for the virus to win the battle.
While you develop some immunity after a COVID infection, it doesn’t just grow with each additional hit. You might be thinking, “Aren’t I more protected against COVID and less likely to have a serious case after having been infected?” Part of that is true, to an extent. In the first couple years after COVID burst onto the scene, reinfections were generally (though not always) milder than a person’s initial bout of the virus. “The way we understand classic immunology is that your body will say to a virus [it’s seen before], ‘Oh, I know how to deal with you, and I’m now going to deal with you in a better way the second time around,’” says Ziyad Al-Aly, PhD, a clinical epidemiologist at Washington University in St. Louis School of Medicine and the chief of research and development at the Veterans Affairs St. Louis Health Care System.
But any encounter with COVID can also cause your immune system to “go awry or develop some form of dysfunction,” Dr. Al-Aly tells SELF. Specifically, “immune imprinting” can happen, where, upon a second (or third or fourth) exposure to the virus, your immune cells launch the same response as they did for the initial infection, in turn blocking or limiting the development of new antibodies necessary to fight off the current variant that’s stirring up trouble. So, “when you get hit an [additional] time, your immune system may not behave classically,” Dr. Al-Aly says, and could struggle with mounting a good defense.
Pair that dip in immune efficiency with the fact that your antibody levels also wane with time post-infection, and it’s easy to see how another hit can rock your body in a new way. Indeed, the more time that passes after any given COVID infection, the less of a “competitive advantage” you’ll have against any future one, Richard Moffitt, PhD, an associate professor at Emory University, in Atlanta, tells SELF. His research found that, while people who got sick initially during the delta phase were less likely to get reinfected during the first omicron wave (as compared to folks who were infected in a prior period), that benefit leveled off with following omicron variants.
There’s also the fact that no matter how your immune system has responded to a prior strain (or strains!) of the virus, it could react differently to a new mutation. “We tend to think of COVID as one homogeneous thing, but it’s really not,” Dr. Al-Aly says. So even if your body successfully thwarted one of these intruders in the past, there’s no guarantee it’ll do the same for another, now or in the future, he says.
Getting COVID again and again is especially risky if it previously made you very ill. Dr. Moffitt’s study above also found that the “severity of your first infection is very predictive of the severity of a reinfection,” he says. Meaning, you’re more likely to have a severe case of COVID—for instance, requiring hospitalization or intensive care, such as ventilation—when reinfected if you had a rough go of it the first time around.
It’s possible that some folks are more prone to an off-kilter immune response to the virus, which could then happen consistently with reinfections. The antibodies created in people who’ve had severe cases “may not function as well as those in folks who’ve had mild infections or were able to fight the virus off,” Dr. Melamed says. Though researchers don’t fully understand why, some people’s immune systems are also more likely to overreact to COVID (remember the cytokine storm?), which can cause serious symptoms—like fluid in the lungs and shortness of breath—whenever they’re infected.
Being over the age of 65, having a chronic illness or other medical condition, and lacking access to health care have all been shown to spike your risk of serious outcomes with a COVID infection, whether it’s your first or fifth fight with the virus.
But you’re not home free if you’ve only had, say, a brief fever or cough with COVID in the past; Dr. Moffitt points out that a small subset of people in his research who had minor reactions with their initial infection went on to be hospitalized with a repeat hit. The probability of that might be lower, but it’s still a possibility, he says.
Even if you’ve only had “mild” cases, each reinfection strains your body, upping your chances of developing long COVID. A 2022 study led by Dr. Al-Aly found that COVID reinfections also increase your risk of complications across the board, regardless of whether you recovered just fine in the past or got vaccinated. In particular, it showed that reinfection raises the likelihood that you’ll need hospitalization; have heart or lung problems; or experience, among other possible issues, GI, neurological, mental health, or musculoskeletal symptoms. “We use the term ‘cumulative effects,’” Dr. Al-Aly says, “so, multiple hits accrue and then leave the body more vulnerable to all the potential long-term health effects of COVID.”
That doesn’t mean your experience of a second (or third or fourth) infection will necessarily be worse, in and of itself, than what you felt during a prior case. But with each new hit, a fresh batch of the virus seeps into your system, where, even if you have a mild case, it has another chance to trigger any of the longer-term complications above. While the likelihood of getting long COVID (a constellation of symptoms lingering for three months or longer post-infection) is likely greatest after initial infection, “The bottom line is, people are still getting diagnosed with long COVID after reinfection,” Dr. Moffitt says.
Researchers don’t totally know why one person might deal with lasting health effects over another, but it seems that, in some folks, the immune system misfires, generating not only antibodies to attack the virus but also autoantibodies that go after the body’s own healthy cells, Dr. Al-Aly says. This may be one reason why COVID has been linked to the onset of autoimmune conditions like psoriasis and rheumatoid arthritis.
A different hypothesis suggests that pieces of the virus could linger in the body, even after a person has seemingly “recovered” (reminder that SARS-CoV-2 is scarily good at weaseling its way into all sorts of cells). “Maybe the first time, your immune system was able to fully clear it, but the second time, it found a way to hang around,” Dr. Al-Aly posits. And a third theory involves your gut microbiome, the community of microbes in your GI tract, including beneficial bacteria. It’s conceivable that “when we get sick with COVID, these bacteria do, too, and perhaps they recover [on initial infection], but not on the second or third hit,” he says, throwing off your balance of good-to-bad gut bugs (which can impact your health in all sorts of ways).
Another unnerving possibility: The shock to your system triggered by COVID may “wake up” a latent (a.k.a. dormant) virus or two lurking in your body, Dr. Melamed says. We all carry anywhere from eight to 12 of these undetected bugs at a time—things like Epstein-Barr, varicella-zoster (which causes chickenpox and shingles), and herpes simplex. And research suggests their reactivation could be a contributing factor in long COVID. Separately, the systemic inflammation often created by COVID may spark the onset of high blood pressure and increased clotting (which can up your risk of stroke and pulmonary embolism), as well as type 2 diabetes, Dr. Melamed says.
There’s no guarantee that any given COVID infection snowballs into something debilitating, but each hit is like another round of Russian roulette, Dr. Al-Aly says. From a sheer numbers standpoint, the more times you play a game with the possibility of a negative outcome, the greater your chances are of that bad result occurring. And because every COVID case has at least some potential to leave you very ill or dealing with a host of persistent symptoms, why take the risk any more times than you need to?
Bottom line: You should do your best to avoid COVID reinfection and bolster your defenses against the virus. At this stage of the pandemic’s progression, it’s not realistic to suggest you can avoid any exposure to the virus, given that societal protections against its spread have been rolled back. But what you should do is take some common-sense precautions, which can help you avoid any contagious respiratory virus. (A cold or the flu may not pose as many potential health risks as COVID, but being sick is still not fun!)
It’s a good idea to wear a mask when you’re in a crowded environment (especially indoors), choose well-ventilated or outdoor spaces for group hangouts, and test for COVID if you have cold or flu-like symptoms, Dr. Al-Aly says. If you do get infected, talk to your doctor about whether your personal risk of a severe case is enough to qualify for a Paxlovid prescription (which you need to take within the first five days of symptoms for it to be effective).
The other important thing you should do is get the updated COVID vaccine (the 2024-2025 formula was recently approved and released). Unlike getting reinfected, the vaccine triggers “a very targeted immune response…because it’s [made with] a specific tiny part of the virus,” Dr. Melamed says. Meaning, you get the immune benefit of a little exposure without the potential of your whole system going haywire. Getting the current shot also ensures you restore any protection that has waned since you received a prior jab and that you have an effective shield against the dominant circulating strains. Plus, research shows that being vaccinated doesn’t just lower your chances of catching the virus; it also reduces your risk of having a severe case or winding up with long COVID if you do get it.
So, too, can the deceivingly simple act of keeping up with healthy habits—like exercising regularly, eating nutritious foods, and clocking quality sleep. Maintaining this kind of lifestyle can help you stave off other health issues that could increase your risk of harm from COVID, Harlan Krumholz, PhD, a cardiologist at Yale University and founder of the Yale Center for Outcomes Research and Evaluation (CORE), tells SELF. “Given that we will be repetitively exposed to the virus, the best investments we can make are in our baseline health,” he says.
Doing any (or all!) of the above is a big act of compassion for yourself, the people you love, and your greater community. “For the average person, it’s like, ‘Oh, COVID is gone,’ but they’re just not seeing the impact,” Dr. Al-Aly says, noting the invisibility of long COVID symptoms like disorienting brain fog and crushing fatigue. The truth is, in plenty of people, just one more infection could be the difference between living their best life and facing a devastating chronic condition.
#mask up#covid#pandemic#covid 19#wear a mask#public health#coronavirus#sars cov 2#still coviding#wear a respirator#lokng covid
245 notes
·
View notes
Text
For much of living memory, the United States has been a global leader of scientific research and innovation. From the polio vaccine, to decoding the first human chromosome, to the first heart bypass surgery, American research has originated a seemingly endless list of health care advances that are taken for granted.
But when the Trump administration issued a memorandum Monday that paused all federal grants and loans—with the aim of ensuring that funding recipients are complying with the president’s raft of recent executive orders—US academia ground to a halt. Since then, the freeze has been partially rescinded for some sectors, but it largely remains in place for universities and research institutions across the country, with no certainty of what comes next.
“This has immediate impact on people’s lives,” says J9 Austin, professor of psychiatry and medical genetics at the University of British Columbia. “And it’s terrifying.”
The funding freeze requires agencies to submit reviews of their funded programs to the Office of Management and Budget by February 10. The freeze follows separate orders issued last week to US health agencies—including to the National Institutes of Health, which leads the country’s medical research—to pause all communications until February 1 and stop almost all travel indefinitely.
The confusion is consummate. If the funding freeze continues through February, and even beyond, how will graduate students be paid? Should grant applications—years long in the writing—still be submitted by the triannual grant submission deadline on February 5? What does this mean for clinical trials if participants and lab techs can’t be paid? Will all that research have to be scrapped thanks to incomplete data?
Even if Trump fully reverses the freeze on research funding, the damage, multiple sources say, has been done. Although for now the funding freeze is temporary, the administration has shown how it might wield the levers of government. The implication is that withdrawing funding could be done more permanently, and could be done to individual institutions, individual organizations, both private and public. This won’t just set a precedent for the large East Coast or West Coast universities, but those located in both red and blue states alike.
While always an imperfect arrangement, science in the US is largely funded by a complex system of grant applications, reviews by peers in the field (both of which have had to be halted as part of the communications pause), and the competitive distribution of NIH funds, says Gerald Keusch, emeritus professor of medicine at Boston University and former associate director of international research for the NIH. According to its website, the NIH disburses nearly $48 billion in grants per year.
When it comes to medical research, America truly is first, and if it abdicates that position, the void left behind has global ramifications. “In Canada, we have always looked to NIH as an exemplar of what we should be trying to do,” says Austin, speaking to me independently of any roles and affiliations. “Now, that’s collapsed.”
Science is, in its very nature, collaborative. Many consortiums and alliances within scientific fields cross borders and language barriers. Some labs may be able to find additional funding from alternative sources such as the European Union. But it is unlikely that a continued withdrawal of NIH funding could be plugged by overseas support. And Big Pharma, with its seemingly endless funds, is unlikely to step up either, according to sources WIRED spoke with.
“This can’t be handed off to drug companies or biotech, because they’re not interested in things that are as preclinical as a lot of the work we’re discussing here,” says a professor of genetics who agreed to speak anonymously out of fear of retribution. “Essentially, there’s a whole legion of university-based scientists who work super damn hard to try to figure out some basic stuff that eventually becomes something that a drug company can drop $100 million on.”
The millions of dollars awarded to high-achieving labs is used to fund graduate students, lab techs, and analysts. If the principal investigator on a research team is unsuccessful in obtaining a grant through the process Keusch describes, often that lab is closed, and those ancillary team members lose their jobs.
One of the potential downstream effects of an NIH funding loss, even if only temporary, is a mass domestic brain drain. “Many of those people are going to go out to find something else to do,” the professor of genetics says. “These are just like jobs for anything else—we can’t not pay people for a month. What would the food service industry be like, for example, or grocery stores, if they don’t pay somebody for a month? Their workers will leave, and pharma can only hire so many people.”
WIRED heard over and over, from scientists too fearful for their teams and their jobs to speak on the record, that it won’t take long for the impact to reach the general population. With a loss of research funding comes the closure of hospitals and universities. And gains in medical advancement will likely falter too.
Conditions being studied with NIH funding are not only rare diseases affecting 1 or 2 percent of the population. They’re problems such as cancer, diabetes, Alzheimer’s—issues that affect your grandmother, your friends, and so many people who will one day fall out of perfect health. It’s thanks to this research system, and the scientists working within it, that doctors know how to save someone from a heart attack, regulate diabetes, lower cholesterol, and reduce the risk of stroke. It’s how the world knows that smoking isn’t a good idea. “All of that is knowledge that scientists funded by the NIH have generated, and if you throw this big of a wrench in it, it’s going to disrupt absolutely everything,” says the genetics professor.
While some are hopeful that the funding freeze for academia could end on February 1, when the pause on communications and therefore grant reviews is slated to lift, the individuals WIRED spoke with are largely skeptical that work will simply resume as before.
“When the wheels of government stop, it’s not like they turn on a dime and they just start up again,” says Julie Scofield, a former executive director of NASTAD, a US-based health nonprofit. She adds that she has colleagues in Washington, DC, who have had funding returned to their fields, and yet remain unable to access payment through the management system.
Austin says that already the international scientific community is holding hastily arranged online support groups. Topics covered range from the banal—what the most recent communication from the White House implies—to how best to protect trainees and the many students on international visas. But mostly they’re there to provide support.
“I’ve had a lot of messages from people just expressing gratitude that we could actually get together,” Austin says. “There’s just so much unaddressable need. None of us has the answers.”
Scientists, perhaps more than any other profession, are trained to “learn and validate conclusions drawn from observation and experimentation,” says Keutsch. That applies to the current situation. And what they observe during this pause of chaos does not portend well for the future of the United States as a pinnacle of scientific excellence.
“If people want the United States to head toward being a second-class nation, this is exactly what to do. If the goal is, in fact, to make America great, this is not a way to do it,” says the genetics professor. “This is not a rational, thoughtful, effective thing to do. It will merely destroy.”
This story has been written under a pseudonym, as the reporter has specific and credible concerns about potential retaliation.
139 notes
·
View notes
Text
Wind-blown avian feces may be route of transmission for bird flu, Minnesota's infectious disease expert warns
Dr. Michael Osterholm is a medical detective and Director of the Center for Infectious Disease Research and Policy, or CIDRAP, at the University of Minnesota. Osterholm has nearly 50 years of investigating infectious disease outbreaks and public health threats. Osterholm hosts a podcast at the University of Minnesota called "Osterholm Update," where he discusses latest disease and outbreak news headlines. On episode 175 titled, "Drinking From a Fire Hose: Are We Drowning?," Osterholm and his co-host, Chris Dall, discuss growing concerns regarding bird flu — or H5N1 — making the jump from animals to humans. According to Osterholm, there has been an additional 89 confirmed flocks with high path avian influenza within the last 30 days alone. Areas affected include Georgia, Indiana, Ohio, California, New York, Minnesota and Maryland. Osterholm says that the primary kind of birds impacted by the flu is migratory waterfowl, like geese and ducks, and these birds often hang out in farm fields where they defecate. Then, the wind picks up particles of the infected feces, spreading the virus far and wide.
[...]
"Today, I am certain that we are seeing clouds of dust with bird feces in that, and we are beginning to see what I would consider to be almost an environmental type disease, similar to the transmission that we see with Coccidioidomycosis, what we call Valley fever, where in fact that's a fungus that grows in the environment. And then on windy days it blows with the dust and you inhale it. I think we're going to see the same thing with H5N1. That's why so many of these barns are now positive," said Osterholm on his podcast. Now that the virus has gone airborne, Osterholm believes we're going to start seeing more and more cases in humans with no explanation for why they occurred. Meaning, people are going to get sick without even coming in contact with the infected animal.
#if you haven't been masking PLEASE start masking again#shit never got better and it's about to get way worse#news#bird flu#usa
50 notes
·
View notes
Text
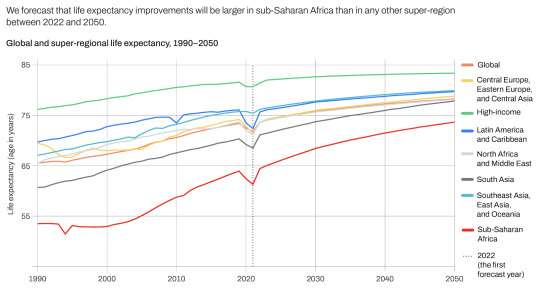
"Global life expectancy is forecasted to increase from 73.6 years of age in 2022 to 78.1 years of age in 2050 (a 4.5-year increase).
Life expectancy increases are projected to be greater in countries with lower life expectancies, reducing global disparities.
There will be a continued shift in disease burden from communicable, maternal, neonatal, and nutritional diseases to non-communicable diseases (NCDs).
The latest findings from the Global Burden of Disease Study (GBD) 2021, published today in The Lancet [May 17, 2024], forecast that global life expectancy will increase by 4.9 years in males and 4.2 years in females between 2022 and 2050.
Increases are expected to be largest in countries where life expectancy is lower, contributing to a convergence of increased life expectancy across geographies. The trend is largely driven by public health measures that have prevented and improved survival rates from cardiovascular diseases, COVID-19, and a range of communicable, maternal, neonatal, and nutritional diseases (CMNNs)...
Global life expectancy is forecasted to increase from 73.6 years of age in 2022 to 78.1 years of age in 2050 (a 4.5-year increase). Global healthy life expectancy (HALE) – the average number of years a person can expect to live in good health – will increase from 64.8 years in 2022 to 67.4 years in 2050 (a 2.6-year increase).
[Note: I cut out significant chunks of this article because they're being really shitty about "disability-adjusted life years," where they explicitly say that years lived as a disabled person don't count/don't count as much. Fuck that! Our lives are worth living!!!! Sincerely, your local disabled blogger.]
“In addition to an increase in life expectancy overall, we have found that the disparity in life expectancy across geographies will lessen,” said Dr. Chris Murray, Chair of Health Metrics Sciences at the University of Washington and Director of the Institute for Health Metrics and Evaluation (IHME). “This is an indicator that while health inequalities between the highest- and lowest-income regions will remain, the gaps are shrinking, with the biggest increases anticipated in sub-Saharan Africa.” ...
The Global Burden of Disease Study (GBD) is the largest and most comprehensive effort to quantify health loss across places and over time. It draws on the work of nearly 12,000 collaborators across more than 160 countries and territories. GBD 2021 – the newly published most recent round of GBD results – includes more than 607 billion estimates of 371 diseases and injuries and 88 risk factors in 204 countries and territories. The Institute for Health Metrics and Evaluation coordinates the study."
-via Institute for Health Metrics and Evaluation, May 17, 2024
--
Note: Obviously we need to make these gaps/disparities close completely!!! And it's also really good to see that we're on the right track.
I genuinely believe that the medical revolution that has just started this decade, along with the huge increase and revolution in communication technology, will make improvements in health and life expectancy come even faster than forecasted. Especially in low-income and low-life-expectancy countries
135 notes
·
View notes
Text

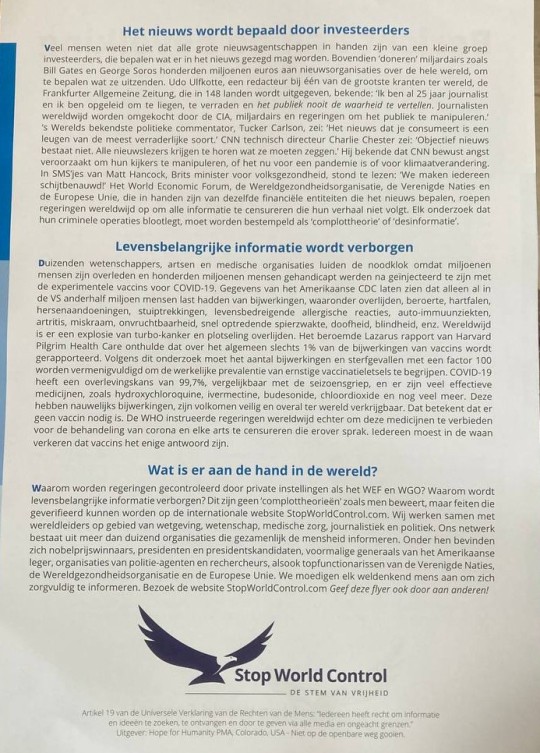
Patriots in the Netherlands are walking the streets dropping flyers at the homes of citizens in hopes of awakening the people. According to Rem64 it is having great success. He sent me the flyer and I translated it to English so everyone can read it. 👇
Message to the population The information below is distributed worldwide by hundreds of scientific, legal and political organizations to inform humanity. Evidence for the stated facts can be found in the detailed evidence reports on StopWorldControl.com
The World Economic Forum wants to shape your life The world's richest come together at the World Economic Forum in Davos, Switzerland. The founder of the WEF, Klaus Schwab, is known for statements such as: We determine the future and We infiltrate governments. The WEF trains Young Global Leaders who are positioned in governments around the world. French President Macron, Canadian Prime Minister Trudeau and German Chancellor Merkel are Young Global Leaders of the WEF. The Netherlands and Belgium also work closely with the WEF and serve their agenda. Part of this agenda is to replace privacy with transparency. They want every detail of your life to be known soon: what you do, who you meet with, what you eat, what you buy... The WEF announces that new technologies will record everyone's thoughts, feelings and dreams in the cloud , where governments have access to this intimate data. To combat climate change, the WEF wants to abolish all private property. You will have to rent everything: houses, cars, work tools, etc. The WEF calls for blocking sunlight by massively releasing chemicals into the air. The WEF encourages the normalization of pedophilia, while the UN and WHO instruct all schools to teach sexual techniques to small children in kindergarten, so that they start having sex as young as possible, with people of any age or gender. As absurd as these plans sound, they are promoted by the WEF, the UN, the EU, the WHO and companies such as. Google and Facebook. They are part of the sustainability goals of Agenda 2030, which are supported by governments worldwide. All evidence of this can be found on StopWorldControl.com
The World Health Organization wants to rule the world The World Health Organization is being legally restructured as an effective global dictatorship, able to impose binding mandates on all countries whenever they declare a pandemic. However, the WHO is a private organization that operates outside any democratic process. One of the WHO's main backers is Bill Gates, who has no medical training whatsoever, yet is promoted as the medical authority around the world. As the world's largest vaccine dealer, his health advice is to inject everyone all the time, making him billions of dollars. WHO Director-General Tedros Ghebreyesus also has no medical training. Yet Gates and Tedros dictate to all the millions of medical experts worldwide what they can and cannot do. Article 18 of the proposed Pandemic Treaty allows the WHO to shut down any source of information that does not align with what they want all of humanity to believe. This means censoring millions of experts in every field. Only what the WHO and Bill Gates say should be heard. Do you want undemocratic organizations to become dictators over your life and over all humanity? Do you want all objective scientific and medical information to be hidden so that you only hear what a single private institution wants you to believe? Do you want to be forced to receive dangerous injections for the rest of your life, without being informed about the risks? If you do not agree with this course of action, we invite you to inform yourself carefully at StopWorldControl.com
The news is determined by investors Many people do not know that all major news agencies are owned by a small group of investors, who determine what can be said in the news. In addition, billionaires such as Bill Gates and George Soros donate hundreds of millions of euros to news organizations around the world, to determine what they broadcast Udo Ulfkotte, an editor at one of the largest newspapers in the world, the Frankfurter Allgemeine Zeitung which is published in 148 countries well-known I have been a journalist for 25 years and I have been trained to lie, betray and never tell the public the truth, journalists) are being bribed worldwide by the CIA, billionaires and governments to manipulate the public The world's best-known political commentator, Tucker Carlson, she The news you consume is a lie of the most insidious kind CNN technical director Charlie Chester said: There is no such thing as objective news. All newsreaders are told what to say. He admitted that CNN deliberately creates fear to manipulate their viewers, whether it is about a pandemic or climate change. Texts from Matt Hancock, British Health Secretary, read: We are making everyone scared? The World Economic Forum, the World Health Organization, the United Nations and the European Union, which are owned by the same financial entities that control the news, are calling on governments worldwide to censor any information that does not follow their narrative. Any investigation that exposes their criminal operations should be labeled conspiracy theory or disinformation.
Vital information is hidden Thousands of scientists, doctors and medical organizations are sounding the alarm as millions of people have died and hundreds of millions of people have been disabled after being injected with the experimental vaccines for COVID-19. Data from the US CDC shows that in the US alone, one and a half million people suffered from side effects including death, stroke, heart failure, brain disorders, convulsions, life-threatening allergic reactions, autoimmune diseases, arthritis, miscarriage, infertility, rapid onset muscle weakness, deafness, blindness, etc. Worldwide there is an explosion of turbo cancer and sudden death. Harvard Pilgrim Health Care's famous Lazarus report revealed that overall, only 19% of vaccine side effects are reported. According to this study, the number of adverse events and deaths must be multiplied by a factor of 100 to understand the true prevalence of serious vaccine injuries. COVID-19 has a 99.7% survival rate, comparable to the seasonal flu, and there are many effective medications, such as hydroxychloroquine, ivermectin, budesonide, chlorine dioxide and many more. These have hardly any side effects, are completely safe and available everywhere in the world. This means that no vaccine is needed. However, the WHO instructed governments worldwide to ban these drugs for the treatment of corona and to censor any doctor who spoke about it, that vaccines are the only answer.
What's going on in the world? Why are governments controlled by private institutions like the WEF and WHO? Why is vital information hidden? These are not conspiracy theories as claimed, but facts that can be verified on the international website StopWorldControl.com. We work with world leaders in the fields of law, science, medical care, journalism and politics. Our network consists of more than 100 organizations that jointly inform humanity. They include Nobel laureates, presidents and presidential candidates, former generals of the US army, organizations of police officers and investigators, as well as top officials of the United Nations, the World Health Organization and the European Union. We encourage every right-thinking person to inform themselves carefully Visit the website StopWorldControl.com Pass this flyer on to others.
Stand Strong! Stand United! Be Prepared!
✨ 🛡️ 🇳🇱 WWG1WGA 🇺🇸 ⚔️ ✨
#pay attention#educate yourselves#educate yourself#knowledge is power#reeducate yourself#reeducate yourselves#think for yourselves#think about it#think for yourself#do your homework#do your own research#do some research#ask yourself questions#question everything#netherlands
252 notes
·
View notes
Text
Gaza’s Turkish-Palestinian Friendship Hospital ‘severely damaged’ in Israeli strike
Oct 30th, 17:05 GMT
The Ministry of Health in Gaza has said that the Turkish-Palestinian Friendship Hospital has suffered severe damage in a fresh Israeli air attack.
The bombing hit the third floor of the hospital, with photos showing the impact of the strike.
(Link to tweet showing photos)
Israeli attack on cancer hospital is ‘first direct hit on medical facility’: Director
Oct 30th, 18:21 GMT
Ayman Nobani, reporting from Nablus, Occupied West Bank
The attack on a Turkish-funded cancer treatment hospital in Tal al-Hawwa, a district in Gaza City’s southwest, is the “first direct hit on a medical facility,” its director has said.
“The third floor, which is for administering anesthesia, was directly hit by Israeli shelling, which destroyed walls, windows, oxygen tank lines, water pipes and electricity lines, said Sobhi Skeik, director of the Turkish-Palestinian Friendship Hospital.
There were no patients or medical team on that floor during that time.
“The hit took place at 5:30pm local time but since yesterday, the environs of the hospital have been getting repeatedly struck by Israeli shelling,” he said.
In Gaza, there are 10,000 cancer patients. The hospital only has 156 beds, in addition to 100 beds for daily use, Skeik explained.
“We are worried that the hospital will be struck again and that our patients will get killed in their beds, and we are worried about the well-being of our staff, but we will continue to do our work. This is our duty.”
WHO unable to resupply Shifa and al-Quds hospitals, says official
Oct 30th, 19:25 GMT
The World Health Organization (WHO) says it has not been able to resupply two hospitals in northern Gaza, Shifa and al-Quds, because the UN deemed the level of risk unacceptable.
“It’s a disaster on top of a disaster. Health needs are soaring and our ability to meet those needs is rapidly declining,” said Rick Brennan, WHO’s regional emergencies director, adding a ceasefire was needed to enable a larger humanitarian operation.
A third of Gaza’s hospitals and 71 percent of clinics are nonfunctioning, he said.
WHO is continuing to resupply hospitals and clinics in southern Gaza, but relief delivered so far overall in the Strip is a “drop in the ocean”, Brennan added.
‘Nowhere safe’ for Palestinian patients to go amid Israel’s hospital evacuation push: UN official
Oct 30th, 20:10 GMT
Lisa Doughten of the Office for the UN Coordination of Humanitarian Affairs (OCHA) says “life hangs by a thread” for premature Palestinian newborns and patients relying on dialysis in hospitals in the Gaza Strip that are facing a lack of fuel.
“Some 9,000 cancer patients are not receiving adequate care,” she told the UN Security Council, expressing concern over the Israeli military’s warnings to evacuate healthcare facilities in the besieged enclave.
“There is nowhere safe for these patients to go, and for those on life support and babies on incubators, moving will certainly be a death sentence.”
#palestine#free palestine#al jazeera#i don’t know how i still have it in me to be shocked anymore#but im just stunned#nobody is doing fucking ANYTHING
268 notes
·
View notes
Text
Nadra Nittle and Shefali Luthra at The 19th:
President Joe Biden’s administration on Monday announced a plan that would eliminate out-of-pocket expenses for most birth control for a majority of Americans. Officials called the proposed rule, which affects people with private health insurance, the most significant expansion of contraception coverage under the Affordable Care Act (ACA) in over a decade. They estimate it could benefit 52 million women of reproductive age. “For the first time ever, women would be able to obtain over-the-counter contraception without a prescription at no additional cost, and health plans would have to cover even more prescribed contraceptives without cost sharing,” said Jennifer Klein, assistant to the president and director of the White House Gender Policy Council, in a call with reporters. The proposed rule would alleviate a significant financial burden for millions of Americans. The 2010 health law already required private health plans to cover at least one form of birth control for beneficiaries without any out-of-pocket costs. Research shows that the benefit has contributed to higher use of contraception, lower health care expenditures by women, and may have helped lower rates of unintended pregnancy.
But applying the contraception mandate to over-the-counter methods has been difficult. If enacted, the proposed rule would require health plans cover forms of birth control such as condoms and emergency contraception – both typically bought without a prescription – as well as a new over-the-counter hormonal birth control pill. That pill, known as Opill, hit retail shelves earlier this year, and a six-month supply costs about $90. Democrats have pushed for years to strengthen enforcement of the ACA’s existing birth control mandate, citing reports of poor enforcement and of women receiving surprise bills for contraceptives that should have been covered. A 2021 survey by KFF, a nonpartisan health policy research, polling and journalism organization, found that 1 in 5 women with private insurance said they had paid something out of pocket for birth control. Biden administration officials reiterated those concerns.
[...] Some Republican state lawmakers have been clear about their intentions to restrict birth control as well as abortion. Conservatives in Congress have called for the defunding of Title X, a federal program offering family planning and related health care services. They have also blocked federal legislation to protect contraception access. Harris, in contrast, has maintained that “contraception is health care.” Since Roe was overturned in June 2022, Harris has discussed the repercussions of limiting women’s health care during more than 100 events, according to Kristine Lucius, deputy assistant to the president and domestic policy adviser to the vice president.
Harris has also criticized Republican efforts to repeal the ACA, which covers nearly 50 million Americans. Among those protected by the law are more than 100 million people with preexisting medical conditions. The law has already allowed millions of women to save on contraception costs. The proposed rule will likely have a 60-day comment period, meaning that it will be finalized in 2025, officials said during the call, making it uncertain if it would still take effect if former President Donald Trump is elected. Trump’s position on contraception hasn’t been clear. In May, he gave an interview in which he suggested he would consider certain restrictions, but he later said he would not impose any. Project 2025, which Trump has distanced himself from — even though its writers have ties to both him and his running mate, Sen. JD Vance — does support restricting some forms of contraception.
The Biden Administration announced on Monday a plan that would eliminate out-of-pocket spending for most birth control items by not requiring a prescription for birth control. This would be a significant expansion of contraception coverage under the Patient Protection and Affordable Care Act (PPACA).
See Also:
AP, via HuffPost: White House Proposes That Health Insurance Fully Cover Over-The-Counter Birth Control
#Contraception#Biden Administration#Birth Control#Health Care#Obamacare#Patient Protection and Affordable Care Act#PPACA#Morning After Pill#Health Insurance#Reproductive Health
30 notes
·
View notes
Text
by Rachel O'Donoghue
Allegations of a cruel massacre and graphic accounts of the reportedly bloody aftermath were published online by global media within hours of what Israel later confirmed to be a precision strike on a Hamas command center situated within a school complex in Gaza on August 10.
The Associated Press led the charge, publishing its first story just over an hour later that morning, describing the strike as “one of the deadliest attacks of the 10-month Israel-Hamas war.” Relying on figures from the Hamas-run Palestinian health authorities, AP claimed that at least 80 people had been killed, with nearly 50 others wounded.
In a subtle bit of editorializing, AP suggested that innocent women and children were likely among the casualties, while also highlighting that this was the “latest of what the U.N. human rights office called ‘systematic attacks on schools’ by Israel,” reportedly leaving hundreds dead, including women and children.
Soon after, a more extensive AP story was prepared for syndication and subsequently repackaged and republished by the news service’s prominent media clients, including The Washington Post, NPR, and POLITICO.
Among those quoted in AP’s more detailed report is Dr. Fadel Naim, described as the director of Al-Ahli Hospital in Gaza, where many of the reported casualties were taken. Naim is quoted as saying his hospital received 70 bodies with what he described as the most severe injuries he had seen since the war began.
Naim’s comments are followed by testimony from “witness Abu Anas,” whom AP mentions was clutching prayer beads as he recounted how multiple strikes hit people who were praying, washing, and sleeping upstairs, including children, women, and the elderly.
A quick look into the online presence of Dr. Fadel Naim, the man AP relied on for their Gaza death toll, reveals that in addition to being a medical professional, he is closely aligned with Hamas—so much so that the recently-eliminated Hamas leader, Ismail Haniyeh, was a guest at his daughter’s wedding.

On October 7, 2023, Dr. Naim celebrated the Hamas massacre that initiated the conflict by posting an image of paragliders over a map of Israel, accompanied by a religious call to arms. The following day, he escalated his rhetoric, urging Gazan civilians to ignore Israeli evacuation warnings for areas targeted by airstrikes—essentially encouraging higher civilian casualties to serve propaganda efforts.
31 notes
·
View notes
Note
For the prompts, H3?
Fanfic Menu Challenge
"By all accounts, Miss Madison, you're in perfect health."
Margo was an engineer, not a doctor. Looking at the x-rays and blood test results, it did appear as if she was fine. But Margo knew her body. She knew when something was wrong. In the small doctor's office of the flight surgeon, she crossed her arms and stared him down. "Check again."
It had started exactly three months ago. At the time, Margo thought it had been stress: Lenara Catiche had been announced as the new director of Roscosmos, with her predecessor, Sergei Nikulov, nowhere in sight. Polite enquiries to Star City had remained unanswered. The concern over Sergei had led to many sleepless nights, many uneaten dinners. But Margo had put her concern to one side: she'd see him at the next IAC conference, no doubt; he was probably working on something top-secret, like the Mars mission or a probe to Ganymede. Nothing to worry about.
But then she'd developed a cough. Pain in her chest. Pain in the small of her back. The second she'd coughed up blood in front of Emma, Margo had been booked in for a litany of medical tests.
The flight surgeon sighed. "Miss Madison, I'm sorry but according to every test we have, there is nothing wrong with you. You're in perfect health. Blood pressure is a little high, but—"
"—so what causes the pain? The coughing up blood?"
He shook his head. "I'm sorry, Miss Madison. We can run some more tests but they'll come back exactly the same."
Margo was used to getting answers. Used to working the problem and finding a solution. She left the flight surgeon's office unsettled, uncertain as to what was happening in her own body. Margo had made it off the elevator and three other paces before she was hit with another wave of pain, as if she was being kicked in the side. Brutal blows rained down upon her body and she clutched the wall for purchase. An arm suddenly held her, anchored her. It was only when Margo had been ushered to her office did she realise it was Aleida.
She knelt in front of Margo. Her mouth fumbled for words. "Are you–are you okay?"
Margo nodded, once. "According to the flight surgeon, I'm fine."
"You've been coughing up blood." Margo's gaze snapped to Aleida's. She shook her head. "I saw you, once, in here. It's only me and Emma that know. Are you sure you're okay?"
"I honestly don't know." Margo leant back against one of the chairs in her office. "I could do with a drink. Brandy?"
"Sure."
It had been a while since she and Aleida had just sat and talked. Aleida had been so occupied with the Mars mission; Margo had been overwhelmed by what had happened in London, the engine designs, now all this. It was good to talk: to hear bout Javi and Victor and Octavio. Margo filled in a few gaps that Emma hadn't divulged, with the latest addition of the flight surgeon's findings. According to him, there was nothing wrong with Margo Madison. Margo thoroughly disagreed.
Aleida rolled the glass between her palms. "Can you go see a specialist?"
"I can find someone but if the press got hold of it? Undermining my own flight surgeon?" Margo sighed. "But I looked at the scans, Aleida. The blood tests. The ultrasound. There's nothing there."
Aleida paused, thought, then laughed to herself. Margo stared at her, wondering what about her condition was so amusing. She eventually divulged what she found so funny. "No, no, it's not funny. Not at all. I was just thinking of this friend from high school, Lara; I crashed on her couch for a while. She was obsessed with fables and fairy tales – the really old ones where people were turned into sea foam and wore iron shoes. She told me all about this story where these two people were meant to be together and they were torn apart and the only way they knew the other was still alive was because they could feel the other person's pain." Aleida took a mouthful of her drink. "It's ridiculous, I know. Just trying to work the problem and my brain went there."
Margo stared at the bottom of her brandy glass. Fairy tales and fables. Ridiculous. But she thought about Sergei's disappearance from Roscosmos. She thought about the noose around his neck in London and how, in that moment that had felt like an hour, she had struggled to breathe. It was insane. She wasn't a fairy princess who needed a kiss from her true love and Sergei wasn't going to climb a castle wall or fight a dragon or wake her up from a glass coffin. Margo had rarely indulged in the idea of romantic love, let alone the concept of soulmates. But—
"What if it was true?" Aleida laughed again until she saw the sombre expression on Margo's face. "What if the person I love is being tortured on a daily basis by the KGB and I can feel every single time they hurt him? What do I do with that?"
Oh God, Sergei. What are they doing to you? To us?
28 notes
·
View notes
Text
RTI Second Appeal by Yogi M P Singh in Mirzapur
Welcome UPICR20240000149 UTTAR PRADESH INFORMATION COMMISSIONSecond Appeal under section 19(3) of the Right to Information Act, 2005Appeal Registration Number – A-20241200463Appeallent’s ParticularsApplied Date : 07/12/2024 03:36:28 AM Name Yogi M P SinghGender MaleState UTTAR PRADESHDistrict MIRZAPURTown/Village मिर्जापुरPincode 231001Mobile Number 7379105911Email [email protected]…
#Additional director medical and health#foi#india#Joint Director Medical and health#law#news#politics#Private practise of government doctors
6 notes
·
View notes
Text
RNN
(3 updates combined)
IOF drones are shooting and dropping bombs on Kamal Adwan Hospital, targeting medical staff and the only electricity generator in the hospital.

The IOF directly targeted Kamal Adwan Hospitals resulting in injuries among doctors, nurses, medical staff and threatening the life of patients.
At least six medical staff are wounded, some of them seriously, and the oxygen station has been disrupted, threatening the lives of the wounded in intensive care.

Journalist Anas Al-Sharif: “Dr. Shurooq Al-Rantisi, did not stop performing her duty for a single moment, despite the siege, arrest, hunger and thirst. In the first picture, she was performing her humanitarian duty in rescuing the wounded, and in the second picture she appears injured after the medical personnel were targeted by the ‘israeli’ occupation forces a short while ago.”
In addition, the nurse Abdul Moneim Al-Sharafi was directly targeted inside the yard of Kamal Adwan Hospital, which resulted in his serious injury in the northern Gaza Strip.
The occupation's drones targeted the medical staff again while they were trying to retrieve the wounded from the first attack inside the hospital.


The health condition of a premature baby the Hospital has deteriorated due to the lack of oxygen after the bombing of the only generator in the hospital, with no means to repair it.
Kamal Adwan Hospital Director and medical staff have refused to implement the occupation's decision to evacuate the hospital.
The Director of Kamal Adwan, Dr. Hossam Abu Safiya stated:
“Our humanitarian duty requires us to remain in northern Gaza as long as there are patients and wounded.”
[New Update] Occupation forces continue their attack on Kamal Adwan Hospital:
Drones have targeted the hospital’s water supply infrastructure, following the earlier bombing of its sole power generator and oxygen station.
IOF drones are besieging the medical staff inside the hospital, and none of them can leave or explore what is happening around the hospital.

[New Update] BREAKING: IOF quadcopter drones are now bombing Al-Awda Hospital, shortly after bombing Kamal Adwan Hospital in the northern Gaza Strip.
53 notes
·
View notes
Text
Also preserved in our archive
Published March 2023. Still relevant.
What The magnitude and quality of a key immune cell’s response to vaccination with two doses of the Pfizer-BioNTech COVID-19 vaccine were considerably lower in people with prior SARS-CoV-2 infection compared to people without prior infection, a study has found. In addition, the level of this key immune cell that targets the SARS-CoV-2 spike protein was substantially lower in unvaccinated people with COVID-19 than in vaccinated people who had never been infected. Importantly, people who recover from SARS-CoV-2 infection and then get vaccinated are more protected than people who are unvaccinated. These findings, which suggest that the virus damages an important immune-cell response, were published today in the journal Immunity.
The study was co-funded by the National Institute of Allergy and Infectious Diseases (NIAID), part of the National Institutes of Health, and led by Mark M. Davis, Ph.D. Dr. Davis is the director of the Stanford Institute for Immunity, Transplantation and Infection and a professor of microbiology and immunology at Stanford University School of Medicine in Palo Alto, California. He is also a Howard Hughes Medical Institute Investigator.
Dr. Davis and colleagues designed a very sensitive tool to analyze how immune cells called CD4+ T cells and CD8+ T cells respond to SARS-CoV-2 infection and vaccination. These cells coordinate the immune system’s response to the virus and kill other cells that have been infected, helping prevent COVID-19. The tool was designed to identify T cells that target any of dozens of specific regions on the virus’s spike protein as well as some other viral regions. The Pfizer-BioNTech vaccine uses parts of the SARS-CoV-2 spike protein to elicit an immune response without causing infection.
The investigators studied CD4+ and CD8+ T-cell responses in blood samples from three groups of volunteers. One group had never been infected with SARS-CoV-2 and received two doses of the Pfizer-BioNTech COVID-19 vaccine. The second group had previously been infected with SARS-CoV-2 and received two doses of the vaccine. The third group had COVID-19 and was unvaccinated.
The researchers found that vaccination of people who had never been infected with SARS-CoV-2 induced robust CD4+ and CD8+ T-cell responses to the virus’ spike protein. In addition, these T cells produced multiple types of cell-signaling molecules called cytokines, which recruit other immune cells—including antibody-producing B cells—to fight pathogens. However, people who had been infected with SARS-CoV-2 prior to vaccination produced spike-specific CD8+ T cells at considerably lower levels—and with less functionality—than vaccinated people who had never been infected. Moreover, the researchers observed substantially lower levels of spike-specific CD8+ T cells in unvaccinated people with COVID-19 than in vaccinated people who had never been infected.
Taken together, the investigators write, these findings suggest that SARS-CoV-2 infection damages the CD8+ T cell response, an effect akin to that observed in earlier studies showing long-term damage to the immune system after infection with viruses such as hepatitis C or HIV. The new findings highlight the need to develop vaccination strategies to specifically boost antiviral CD8+ T cell responses in people previously infected with SARS-CoV-2, the researchers conclude.
Article F Gao, et al. Robust T cell responses to the Pfizer/BioNTech vaccine compared to infection and evidence of attenuated CD8+ T cell responses due to COVID-19. Immunity DOI: 10.1016/j.immuni.2023.03.005(link is external). (2023). www.cell.com/immunity/fulltext/S1074-7613(23)00125-5
#mask up#public health#wear a mask#pandemic#covid#wear a respirator#covid 19#still coviding#coronavirus#sars cov 2#long covid#covid is airborne#covid is not over#covid conscious
35 notes
·
View notes
Text
Protecting Children from Chemical and Surgical Mutilation
Issued January 28, 2025.
By the authority vested in me as President by the Constitution and the laws of the United States of America, it is hereby ordered:
Section 1. Policy and Purpose. Across the country today, medical professionals are maiming and sterilizing a growing number of impressionable children under the radical and false claim that adults can change a child's sex through a series of irreversible medical interventions. This dangerous trend will be a stain on our Nation's history, and it must end.
Countless children soon regret that they have been mutilated and begin to grasp the horrifying tragedy that they will never be able to conceive children of their own or nurture their children through breastfeeding. Moreover, these vulnerable youths' medical bills may rise throughout their lifetimes, as they are often trapped with lifelong medical complications, a losing war with their own bodies, and, tragically, sterilization.
Accordingly, it is the policy of the United States that it will not fund, sponsor, promote, assist, or support the so-called "transition" of a child from one sex to another, and it will rigorously enforce all laws that prohibit or limit these destructive and life-altering procedures.
Sec. 2. Definitions. For the purposes of this order:
(a) The term "child" or "children" means an individual or individuals under 19 years of age.
(b) The term "pediatric" means relating to the medical care of a child.
(c) The phrase "chemical and surgical mutilation" means the use of puberty blockers, including GnRH agonists and other interventions, to delay the onset or progression of normally timed puberty in an individual who does not identify as his or her sex; the use of sex hormones, such as androgen blockers, estrogen, progesterone, or testosterone, to align an individual's physical appearance with an identity that differs from his or her sex; and surgical procedures that attempt to transform an individual's physical appearance to align with an identity that differs from his or her sex or that attempt to alter or remove an individual's sexual organs to minimize or destroy their natural biological functions. This phrase sometimes is referred to as "gender affirming care."
Sec. 3. Ending Reliance on Junk Science. (a) The blatant harm done to children by chemical and surgical mutilation cloaks itself in medical necessity, spurred by guidance from the World Professional Association for Transgender Health (WPATH), which lacks scientific integrity, in light of the scientific concerns with the WPATH guidance:
(i) agencies shall rescind or amend all policies that rely on WPATH guidance, including WPATH's "Standards of Care Version 8"; and
(ii) within 90 days of the date of this order, the Secretary of Health and Human Services (HHS) shall publish a review of the existing literature on best practices for promoting the health of children who assert gender dysphoria, rapid-onset gender dysphoria, or other identity-based confusion.
(b) The Secretary of HHS, as appropriate and consistent with applicable law, shall use all available methods to increase the quality of data to guide practices for improving the health of minors with gender dysphoria, rapid-onset gender dysphoria, or other identity-based confusion, or who otherwise seek chemical or surgical mutilation.
Sec. 4. Defunding Chemical and Surgical Mutilation. The head of each executive department or agency (agency) that provides research or education grants to medical institutions, including medical schools and hospitals, shall, consistent with applicable law and in coordination with the Director of the Office of Management and Budget, immediately take appropriate steps to ensure that institutions receiving Federal research or education grants end the chemical and surgical mutilation of children.
Sec. 5. Additional Directives to the Secretary of HHS. (a) The Secretary of HHS shall, consistent with applicable law, take all appropriate actions to end the chemical and surgical mutilation of children, including regulatory and sub-regulatory actions, which may involve the following laws, programs, issues, or documents:
(i) Medicare or Medicaid conditions of participation or conditions for coverage;
(ii) clinical-abuse or inappropriate-use assessments relevant to State Medicaid programs;
(iii) mandatory drug use reviews;
(iv) section 1557 of the Patient Protection and Affordable Care Act;
(v) quality, safety, and oversight memoranda;
(vi) essential health benefits requirements; and
(vii) the Eleventh Revision of the International Classification of Diseases and other federally funded manuals, including the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition.
(b) The Secretary of HHS shall promptly withdraw HHS's March 2, 2022, guidance document titled "HHS Notice and Guidance on Gender Affirming Care, Civil Rights and Patient Privacy" and, in consultation with the Attorney General, issue new guidance protecting whistleblowers who take action related to ensuring compliance with this order.
Sec. 6. TRICARE. The Department of Defense provides health insurance, through TRICARE, to nearly 2 million individuals under the age of 18. As appropriate and consistent with applicable law, the Secretary of Defense shall commence a rulemaking or sub-regulatory action to exclude chemical and surgical mutilation of children from TRICARE coverage and amend the TRICARE provider handbook to exclude chemical and surgical mutilation of children.
Sec. 7. Requirements for Insurance Carriers. The Director of the Office of Personnel Management, as appropriate and consistent with applicable law, shall:
(a) include provisions in the Federal Employee Health Benefits (FEHB) and Postal Service Health Benefits (PSHB) programs call letter for the 2026 Plan Year specifying that eligible carriers, including the Foreign Service Benefit Plan, will exclude coverage for pediatric transgender surgeries or hormone treatments; and
(b) negotiate to obtain appropriate corresponding reductions in FEHB and PSHB premiums.
Sec. 8. Directives to the Department of Justice. The Attorney General shall:
(a) review Department of Justice enforcement of section 116 of title 18, United States Code, and prioritize enforcement of protections against female genital mutilation;
(b) convene States' Attorneys General and other law enforcement officers to coordinate the enforcement of laws against female genital mutilation across all American States and Territories;
(c) prioritize investigations and take appropriate action to end deception of consumers, fraud, and violations of the Food, Drug, and Cosmetic Act by any entity that may be misleading the public about long-term side effects of chemical and surgical mutilation;
(d) in consultation with the Congress, work to draft, propose, and promote legislation to enact a private right of action for children and the parents of children whose healthy body parts have been damaged by medical professionals practicing chemical and surgical mutilation, which should include a lengthy statute of limitations; and
(e) prioritize investigations and take appropriate action to end child-abusive practices by so-called sanctuary States that facilitate stripping custody from parents who support the healthy development of their own children, including by considering the application of the Parental Kidnapping Prevention Act and recognized constitutional rights.
Sec. 9. Enforcing Adequate Progress. Within 60 days of the date of this order, the heads of agencies with responsibilities under this order shall submit a single, combined report to the Assistant to the President for Domestic Policy, detailing progress in implementing this order and a timeline for future action. The Assistant to the President for Domestic Policy shall regularly convene the heads of agencies with responsibilities under this order (or their designees) to coordinate and prepare for this submission.
Sec. 10. Severability. If any provision of this order, or the application of any provision to any person or circumstances, is held to be invalid, the remainder of this order and the application of any of its other provisions to any other persons or circumstances shall not be affected thereby.
Sec. 11. General Provisions. (a) Nothing in this order shall be construed to impair or otherwise affect:
(i) the authority granted by law to an executive department or agency, or the head thereof; or
(ii) the functions of the Director of the Office of Management and Budget relating to budgetary, administrative, or legislative proposals.
(b) This order shall be implemented consistent with applicable law and subject to the availability of appropriations.
(c) This order is not intended to, and does not, create any right or benefit, substantive or procedural, enforceable at law or in equity by any party against the United States, its departments, agencies, or entities, its officers, employees, or agents, or any other person.
9 notes
·
View notes
Text
Let's call it what it is--human sacrifice. When study after study, AND real world examples show that universal health care saves lives AND money, we need to just admit that the US intentionality sacrifices over 40,000 people a year in the name of enriching insurance company executives. It's no different than strapping over 40,000 people a year to an altar, and having a priest ritually cut out their hearts to give Joe CEO his seventh yacht.
"Oh, but there aren't enough doctors!" Countries with universal health care don't have that problem because they don't have the AMA lobbying to make sure doctors are in short supply, and they also don't have exorbitant higher education tuition to restrict the profession to the wealthy, and those willing to take a risk and go into crushing debt.
"But I don't want the gummint in charge of my health care!" You don't want a board of medical professionals appointed by elected officials in charge of your health care?
Right now your health care is decided by a computer, and by a kid with no medical training reading a script off of a computer screen, and by a board of directors (most of whom also have no medical training), all of which deny as many claims as they can possibly get away with, in order to enrich shareholders.
Capitalism is a religion that worships profit, and engages in human sacrifice to ensure as much additional profit for billionaires as possible.
86 notes
·
View notes