Statistics
We looked inside some of the posts by pathparazzi and here's what we found interesting.
Average Info
Notes Per Post
19
Likes Per Post
13
Reblog Per Post
6
Reply Per Post
0
Time Between Posts
1 month
Number of Posts By Type
Text
9
Photo
8
Last Seen Tumblr Blogs





Fun Fact
When “GIF” was named word of the year in 2012, Oxford Dictionaries U.S.A. credited Tumblr for pushing the word.
Text
Thoughts re: Catching Mistakes
It is now November, and still I have not received an acknowledgement for helping a colleague avoid a disastrous outcome due to a severe misdiagnosis. Here's an abridged telling:
Older patient with a longstanding, stable renal mass now has a brain mass. Brain mass was sampled, read as metastatic RCC. No GU-trained person laid eyes on it. I got the case for tumor board and it's very clearly not an RCC of any sort. I stain it up and show it around and everyone agrees - primary CNS neoplasm. Renal mass is biopsied and morphologies are not the same. The neuropath team ends up getting the case back and they struggle with it for a bit before sending it off for molecular testing. Lo and behold, it's a primary CNS neoplasm. They then act like they knew all along that it wasn't a GU primary.
I don't want to come off as petty or arrogant or holier than thou - I've certainly made my share of diagnostic errors -, but I think that in a professional setting where collegiality is consistently encouraged and also touted as a huge element in the promotion/tenure process, then this lack of acknowledgement feels somewhat insulting, especially when I've helped a patient avoid unnecessary surgery and therapy. I'd like to think that maybe I've also staved off a lawsuit as well.
I understand that catching mistakes is inherent to the checks and balances that exist in academia. I am doing my job and while that alone doesn't merit any special praise, I feel that helping colleagues out of a tricky spot should at least merit a 'thank you'. Whenever I make a mistake, I pray that the patient hasn't been affected, and I thank my colleagues for having my back. They know I have theirs and vice versa.
Instead, I was met with a doubling down on an incorrect diagnosis. Molecular testing was sent out under the guise of "rule out metastatic RCC" and again, no one on neuropath ran their thoughts by a GU-trained pathologist, just like they didn't when the initial report was signed out. In the end, the molecular data pointed to a primary CNS neoplasm.
There are elements of irresponsibility here, and the damage has been done. The medical record still mostly shows that this patient has metastatic RCC when they do not, and I wonder if they would have received better or more targeted therapy had they been properly diagnosed earlier in the year.
But I shouldn't be surprised by any of this. If this past year and a half has taught me anything, academicians (and institutions) have egos, and they do not take kindly to being wrong, even if they say they can take it.
0 notes
Text
Thoughts re: Academia
I haven't been on this blog at all and there's really not much I can say other than I haven't had the time or energy. Being a functioning adult is brutal at times, and in academic medicine, I felt robbed of myself. Even when I am not on service, I feel loath to do anything productive. My apartment remains in a state of partial disarray at any given time. I see chores that take no time pile up in front of me. I should clean that spill on the floor or put those towels away, yet I don’t. I don’t remember being like this even when I was burned out in training or during the early pandemic.
I have been working at a mid-tier academic center for the past year now, and so much has happened since I first started posting on this Tumblr. During the end of my fellowship, my fellowship director was removed from the premises for an investigation that resulted in no wrongdoing. After almost forty years of service to his institution, which refused to defend him, he resigned. A devastating loss for that department. Why stay at a place where the people you trained turn on you and the institution you helped to bring to prominence abandon you?
I nearly didn’t get a job because of how badly my current institution’s HR system was so utterly understaffed that I had to onboard myself, only for them to cancel the contract on the day before I started. And then they nearly forgot to send the amended contract to me and they sent it to the wrong email. One of my colleagues’ loved ones was murdered by their progeny. One of the residents had a life-threatening stroke. One assistant’s house burned down and lost everything including her beloved pet. One of the senior trainees was such a shitshow and they quit in the middle of their training in bad standing after terrorizing us and the clinical services for the better part of their time here.
It has been an absolutely dramatic year, and I have experienced enough racism and several professional slights against me that I’m simply over it. As lovely and wonderful as my director is as a person, this does not translate to good leadership. I am angry at them because they lied to me about what this job entailed and what I could get out of it, that I would have a proper mentor instead of someone long in the twilight of their career, who hasn’t even seen what I have in our respective subspecialties. I feel that this place has robbed me of a year of my life, and I have nothing to show for it except work experience. Maybe I’m being too critical.
I have no friends in the area except two people who are so hard to hang out with. They’re incredibly bright and well-educated, but they are also incredibly boring. I rarely use that term on people, but they are socially inept at worst and heavily disconnected from pop culture and current events at best. The friends I had have moved away or are in the process of moving out. When I leave, it’ll be a clean exit. I will owe them nothing.
The academic pathology scene is nothing short of chaotic presently. Hopkins is bleeding people. BIDMC is shoring up in the wake of the Dana Farber merger, but knowing how administratively incompetent that hospital is at the higher levels, it’s nowhere near ready to absorb an expected 40-50% increase in specimen volume. Hiring is slow and unhurried when the process should be expedited and prioritized.
Brigham and Mass General aren’t exactly doing well for themselves, given that so many of their staff are leaving after long careers there. Oregon Health and Sciences is experiencing some sort of staffing malfunction because the person who helped to recruit me left for private practice and they haven’t been able to hire anyone senior.
That said, I am going into private practice. I was afraid to do so earlier, but I think it is ultimately the way to go. I sent in my CV one day and immediately received a phone call the next. Things have moved along fast and efficiently with also a bit of breathing room built in. There’s less bullshit, and people are happier overall.
I am also coming to terms with the fact that I need a work-life balance. People say that academia has work-life balance, but those people are lying. I used to see so many people come in on the weekends or stay late to write papers and do ancillary work. It’s only now post-pandemic that people are realizing that they’re wasting their lives constantly writing and for what? To get a pat on the back? To get a little line on their CV so years down the road they can be called full professor? I think people are learning to choose themselves and I applaud that. Academia has been a shitshow and it needs to reform and pay these brilliant, hardworking, self-sacrificing people what they are worth if it is to go on in a meaningful way.
Moving forward, I’m hoping to revive this corner of my life by posting pictures of pathology every so often. Knowledge is meant to be shared, and I’ve always wanted to make a slide repository/image archive for those who are looking. It'll hopefully be my little hobby that keeps me somewhat sane.
0 notes
Text
Thoughts re: Job Hunting
Today, I received a rejection email from a prospective employer. What surprised me was that neither the chairman, whom I'd met several times, nor the AP director (APD) who would have been my immediate boss had reached out for follow-up before this email made its way to my inbox. All I got was a formulaic letter from HR telling me that they were considering other candidates.
I am at the end of my job hunt so I feel more at liberty to discuss my thoughts on this particular interview, several aspects of which have been anonymized. And before I go on, I'm going to go back in time to the beginning to give some context.
When I applied, I had not expected an interview from this institution for a couple of reasons:
First, they wanted someone with job experience. As I've seen on several academic job postings, they read something like "entry-level position, 5-10 years experience required", and this posting was essentially no different. Also, we are in a critical pathology shortage that will likely last for years to come and the application pool is largely fresh grads so...
Second, I learned not to expect anything from online job applications because in spite of the "booming job market" for pathologists and the wide net I'd cast, I barely heard back from anyone.
For instance, I applied for a job near the place I trained for residency, as they were in a hiring frenzy and I wanted to be close to the city. I submitted my application online and emailed their chair directly to express my interest in the position. Months passed, I heard nothing, and then the job postings vanished. A separate job posting close to family and friends took three months for a response, and this was after several attempts on my part, as well as my colleagues, to reach out. It has not been an easy journey by any means, so I'm grateful to be near the end of it all.
So, back to this job listing. I was pleasantly surprised to learn my director (whom I semi-jokingly call God) had spoken to the APD there who was a former colleague of his. God had given me a glowing recommendation, as had my previous director, so this APD opted to interview me to gauge compatibility and interest.
We met later over Zoom. The conversation was somewhat stilted - he was interviewing me while covering service - and our conversation ended after he got called away during a natural lull. While I had some reservations, I suppressed them mainly because he was just one person in what could potentially be a whole chain of people I could call my colleagues.
Next up was the chairman. He was loquacious and boastful of his department, the hospital system, and the city as well. One thing he liked to harp on was that they were flush with money and that they would not leave me wanting for anything. He talked up the specialties I'd be interested in and the fact that this city was great for single people (something he technically shouldn't have inquired about but I have no issue answering). I figured that this would be quite an opportunity and a whole new world if this all worked out.
Over the next few weeks, multiple emails were exchanged. They booked me a flight and a stay at a hotel. I won't go into the details of everything that transpired in between, so I'll skip ahead to the interview.
I was very impressed by how meticulously all of these logistics had been planned. There was a driver awaiting me at the airport, and the driving service had my number on hand. I was picked up, offered water, and driven to the hotel, which was much nicer than I anticipated. Because my flight arrived relatively late into the night, I quickly unpacked and went to bed.
The itinerary was spread out over 2 days and it was set up in such a way that I would meet with the chairman 3 separate times but nowhere was it on the schedule that I would meet with the APD at any point. (I would later find out he was out of town on scholarly business.) It only included attendings from one of the specialties I would be signing out.
Day one. I was picked up and driven to the hospital. I did not realize how big and sprawling this campus was until I arrived. Several hospitals existed under one academic umbrella over several city blocks and throughout my interview, I would be transported to several different locations as well as entirely different hospitals.
I had a very long first meeting with the chairman. Again, he was a talker, and I was mildly wishing that I could just move on to the other interviews.
The interviewers/my potential colleagues at this first hospital were...alright. I couldn't help but notice that something seemed off during our interactions, and I got the sense that I wouldn't particularly get along with them past a professional standpoint. They seemed somewhat overworked and rigid. There seemed to be no space for chit-chat, only shop talk. And I did not notice any camaraderie.
For the service I would be covering, I learned that they had 3 pathologists for what seemed to be an obstructively busy workload, and no one seemed happy with this arrangement. They all told me that it was "busy but doable" more or less and that I would have support.
Midday, I gave my job talk which I thought went rather well. Of course, the chairman seemed very excited at the topic and even decided to invite someone who specialized in that field to attend.
I had more interviews later on, some of which felt particularly irrelevant to my field, and then I was dropped off at the hotel to rest and await dinner with the chairman.
He picked me up in his car and he took me out to a somewhat upscale restaurant that he frequented, to the point that the waitstaff recognized him. Two others joined us, one of whom would be a potential colleague as well, and the four of us had a good time for the most part.
However great dinner was, I felt uncomfortable with the chairman bringing up politics and my home country, and then passing summary judgment on it as if he knew best. If you couldn't already tell, he's an older white man, and he felt that he knew my home country better than I did. I tried to explain the reality of it, but he did not seem to care. It lent a brief awkwardness to the conversation, and then I changed the topic as smoothly as I could.
Afterwards, I was dropped off at the hotel and then I went to bed.
Day two. I gave a slide session with the residents. Only 3 out of 29 showed up with a bunch joining virtually (and silently). I was not particularly impressed with them except for one who nailed these differentials better than the senior who was present.
The rest of the day, I interviewed the other half of the colleagues in my specialty, and they practiced at a separate hospital. The moment I arrived, I could tell that they were happier, and that they liked each other. Their doors were open, and two of them were just casually chatting away until I walked in.
I had a blast with these people, whom I sadly wouldn't even get to work with if I got the job, and what I found interesting was that they all preferred to be at this hospital, not the main academic building where I'd interviewed yesterday. Their workflow seemed flexible and there was backup, unlike the other hospital.
After lunch, I ended up meeting with the special guest the chairman had invited to my job talk. We met in his office, and I didn't expect for him to insult me or the group I'd worked with. I didn't quite know what to say and he didn't seem to want to hear it either, just that he had better stuff than we did and that it was more expensive. It’s like the rich kid shaming the poor kid for wearing Gap clothes while he’s wearing Armani. Cool story, brah, you missed the entire point of the talk.
My last meeting of the day was with the chairman and my goodness, the guy could talk. He left the ball in my court, telling me that if I wanted to continue pursuing this job, then he would generate an offer letter and the like, so on and so forth. I let him know that I still had interviews and that I would reach out after everything was done so as to not waste his time. He seemed vaguely disappointed with that answer and wanted me to give him an answer sooner rather than later.
Before long, I was whisked away to the airport and I didn't even get a chance to change out of my suit.
// The "Postmortem" //
So, I was a little surprised to find such an impersonal rejection letter. I expected someone to reach out in the time that followed to gauge interest, and there was nothing. I didn't hear from the chair or the APD in the weeks that followed. Granted, I also could have reached out but I was interviewing elsewhere and busy being on service and he knew that.
I really don't know what their team's impression of me was, but I thought it was generally positive. My impression, however, was littered with red flags and these are the ones I can think of off the top of my head. :
One of the wonderfully competent admin I was with told me that only a few people had applied for this position and no one seemed to want it
The chairman. He himself was a giant red flag...
I learned that he didn't actually know what my job workflow would be like
The politics issue at dinner and the fact he'd asked if I were single or married more than once
He also insulted my talk somewhat
The constant mention of having money...but the hospital not seeming to know how to use it well
Boasting so much to the point he actually lied to me about certain facts
The lack of awareness that pathology as a whole is facing such a terrible predicament
The only people I didn't really vibe with were the people I would be working constantly with, and they seemed overworked and unhappy
The lack of contact and follow-up with the APD
It seemed that several attendings I talked to had to give something up in order to advance in their careers
The complete and utter lack of masking inside the hospital seemed alarming
Being insulted by a guy who didn't understand what my talk was about
As for the rejection, a friend suggested that perhaps they got their top pick (which seems unlikely given how few people applied), or that someone else answered sooner. Either way, I hope whoever they hired will be happy there.
0 notes
Photo
Find the mast cell!
1 note
·
View note
Photo
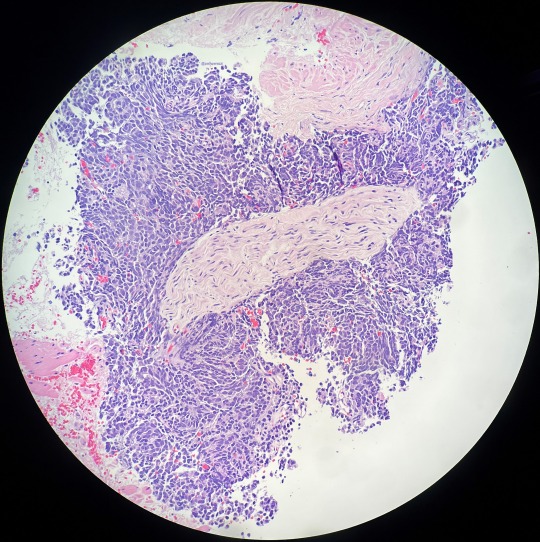
Perineural invasion by a small cell carcinoma. I usually don’t see this big of a nerve being invaded.
0 notes
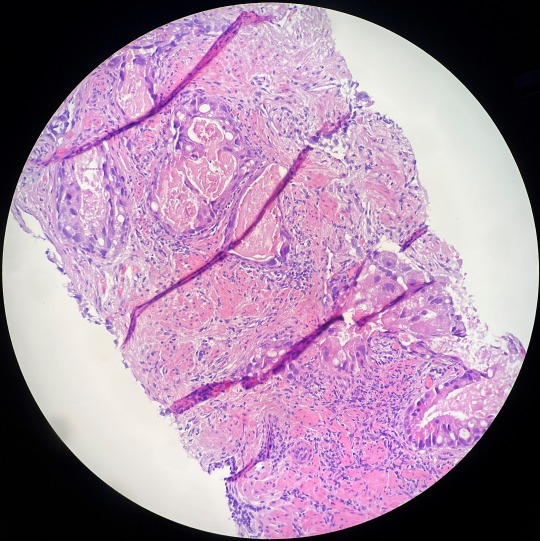
Photo
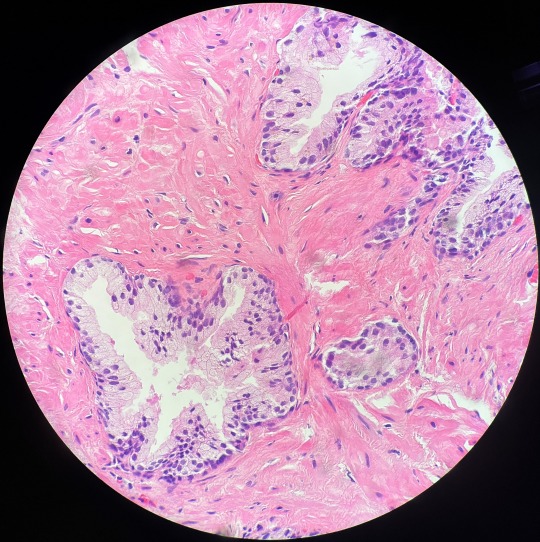
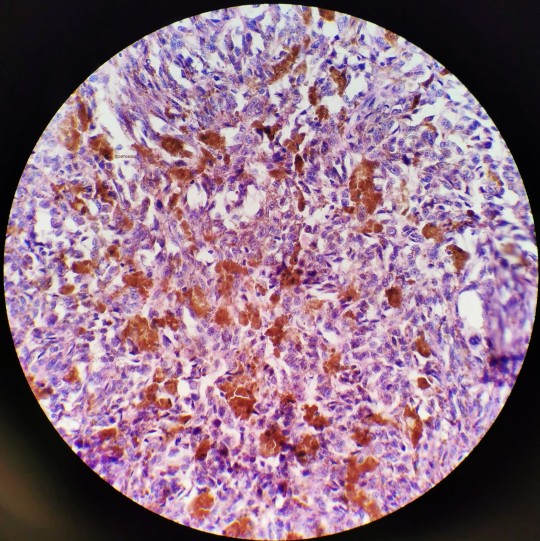
Most of this nephrectomy showed a clear cut, slam dunk case of a renal oncocytoma. Then you had a couple of areas where this second population of cells showed up. They didn’t stain like an onco (CK7 positive) and later found to have GPNMB staining as well. It’s a curious clone and we don’t know the significance of it. I wonder if I’ll ever see a second case.
1 note
·
View note
Text
Rewatching Grey’s Anatomy and debating whether or not I should do a critique as someone who originally enjoyed the series before being a doctor but is now in the fold (just the first two seasons because anything after that is not as enjoyable).
0 notes
Photo
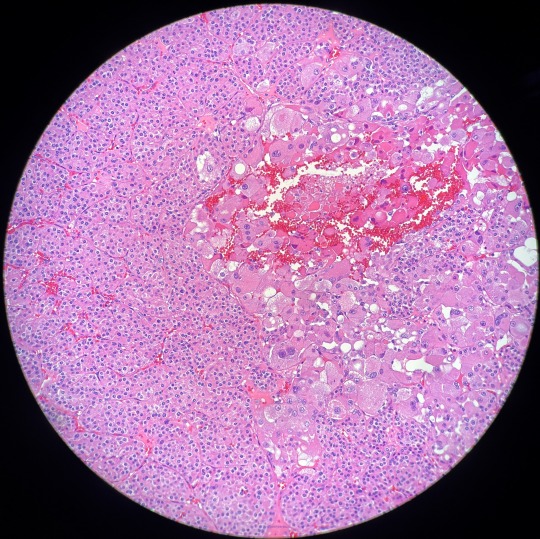
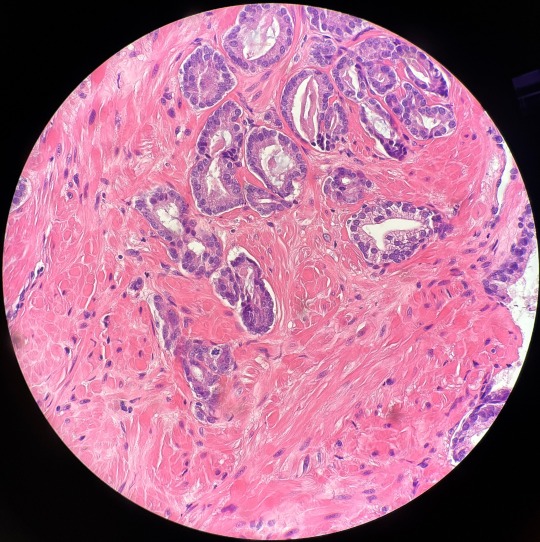
This one’s pretty wild - pleomorphic intraductal carcinoma of the prostate. Intraductal carcinoma is already bad news bears, but it rarely looks this ugly. Generally speaking, prostatic adenocarcinoma morphology tends to be on the blander side. This was rare enough to earn a “cool” from my attending.
0 notes
Photo
Prostatic adenocarcinoma, 336/GG1. My only reason for posting this is because it’s rare to see mites in prostate cancer, and yet here we are! Sometimes you’ll even find apoptotic bodies, but by and large, those things mean nothing in the broader context of the diagnosis so we don’t mention them.
0 notes
Photo
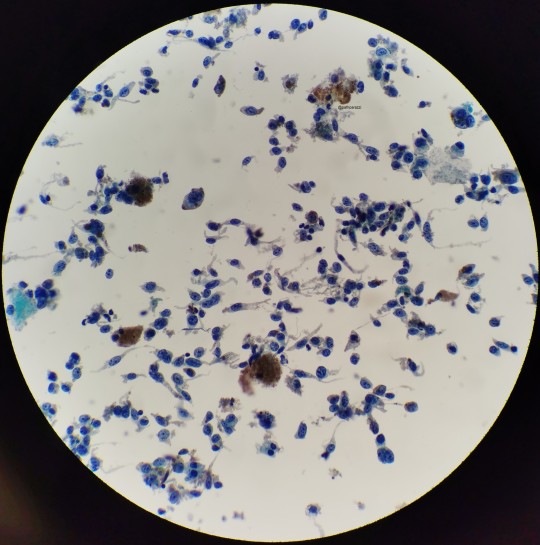
I believe all three of these images belong to the same case I had as a cyto fellow.
This is a pretty slam dunk case of melanoma that had metastasized to the hilar lymph nodes. I remember my attending asking for the history before he saw the slide, to which I told him to just look. Naturally, you’d want to make sure that it isn’t just hemosiderin but given the history of melanoma in the patient’s chart, no stains were needed. Sad case though.
0 notes
Photo
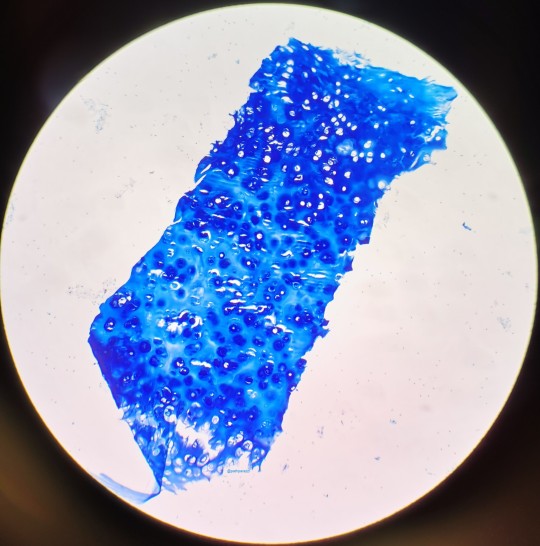
Something mundane - a fragment of cartilage from an EBUS procedure seen on a cell block stained with AFB if memory serves.
0 notes
Photo
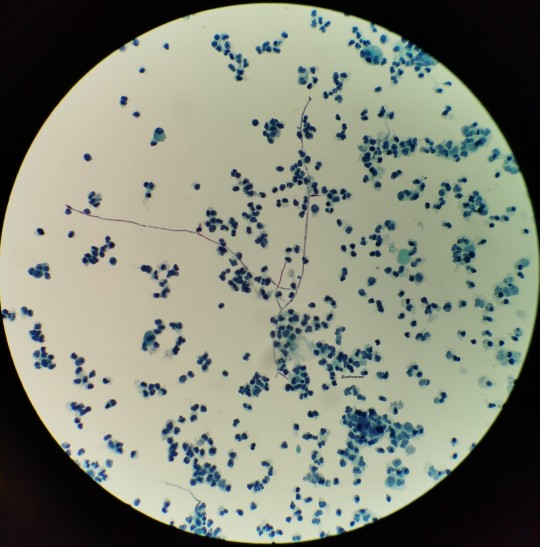
The top photo is Candida in a urine from a case I had (if memory serves), the bottom from my friend who was cyto fellow then. Needless to say, hers was much more impressive. That’s a lotta pseudohyphae!
2 notes
·
View notes
Text
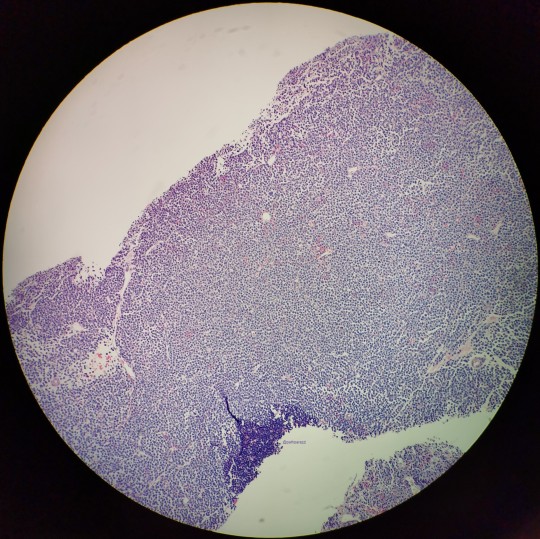
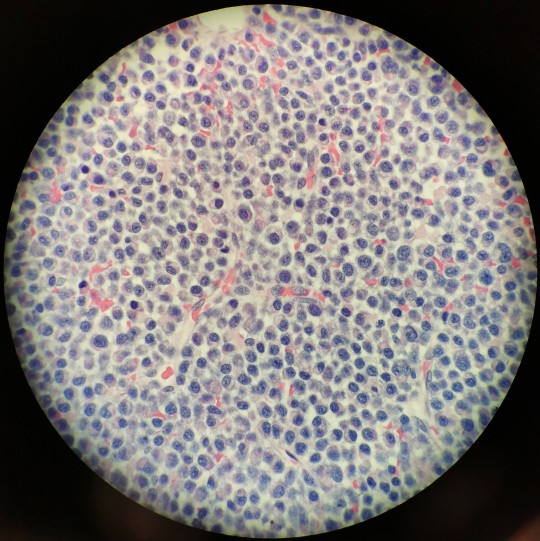
This was a biopsy of a thigh mass in a man. Initially, my untrained eyes thought this was a rhabdomyosarcoma, probably because I really wanted to diagnose a zebra. Showed it to my attending who immediately identified it as a plasmacytoma, and after he said it, it became so obvious.
0 notes
Text
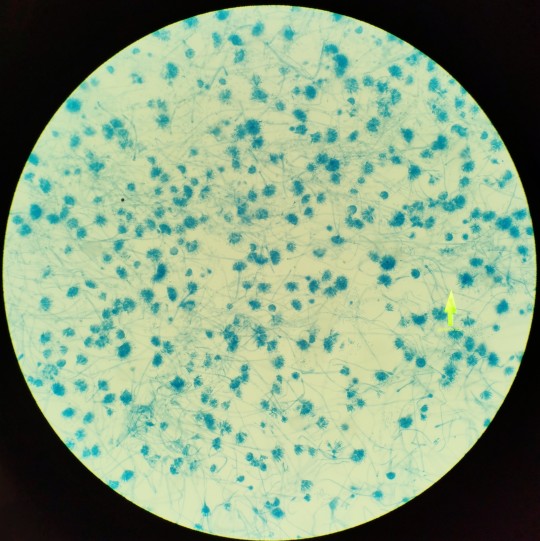
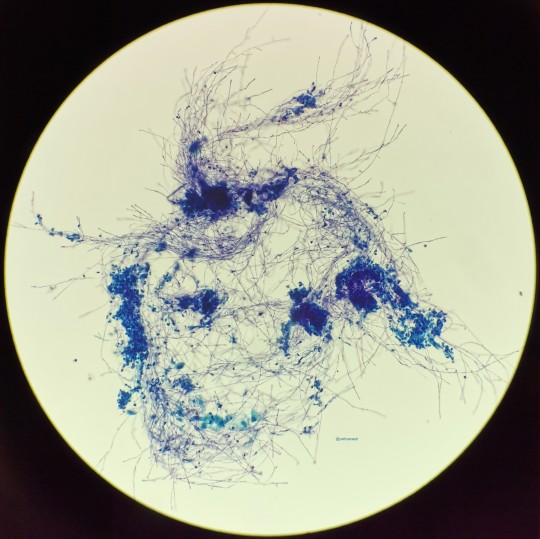
Lactophenol cotton blue - Aspergillus versicolor. Don't ask me how I know this, this was speciated well after I took the picture. It is recognizably, however, Aspergillus.
10 notes
·
View notes
Text
An Ode to Admins
My encounters with medical admin (from medical school to residency to the state bureaucracy itself) can be boiled down to the tried and true dichotomy - useful ones and useless ones.
Useful admin vary in age, exist in the minority, and they know exactly what they're doing. They know how to help and they are self-aware enough to know their worth to the place. These people are the links in the chain holding the place together, the proverbial duct tape binding and holding the universe together. Treasure them. Cherish them. Give them incentives to stay. Because when they leave, their replacement will likely suck.
Useless admin, to put it nicely, are the equivalent of nipples in men - vestigial and unnecessary. They are the human equivalent of the Dunning-Kruger effect, hailing from the "peak of Mount Stupid". Their sense of worth (and also salary) is deeply overinflated, and no one, not even them, knows exactly what their role at the institution is.
Chances are if you've encountered them, you've regretted it. You may have been sent to a different place that sent you straight back to that same admin who'll then pass you along to another hopeless, hapless schmuck. You may have received an urgent email at 4:58 PM on a Friday and by the time you call back to address it, they'll have left for the weekend. You may have received an email with five different fonts in different colors with different italics that would blind most mammals and the contents are 90% useless.
Sometimes, I wonder if it's the nature of the beast that attracts the useless people to admin jobs. Did these people peak in high school? Did these people even get to graduate? I'm honestly curious because my colleagues and I have all spent way too much time doing their work at our expense, and before I die, I want to make it known that med admin in general do nothing other than use precious oxygen that could have been someone else's. They are superfluous and add absolutely nothing of value to any organization they belong to. I do not care if they are three years away from retirement and have been here for three decades. In my opinion, they have been there three decades too long and that's three decades worth of paychecks wasted.
Perhaps I'm overly harsh because I'm in a terribly bitter state of mind presently, but given my collective experience over the past 10 years in different states and hospitals, my statement stands true across the board.
Maybe I've just played the game wrong all this time. Maybe I should have had no ambition to be good at anything in life and instead pursued an administrative career. Clearly, those who are incompetent are not fired for their lack of skills, but instead are rewarded for it. Maybe in the next life, I'll be a slug because that's about the same thing, right?
0 notes
Text
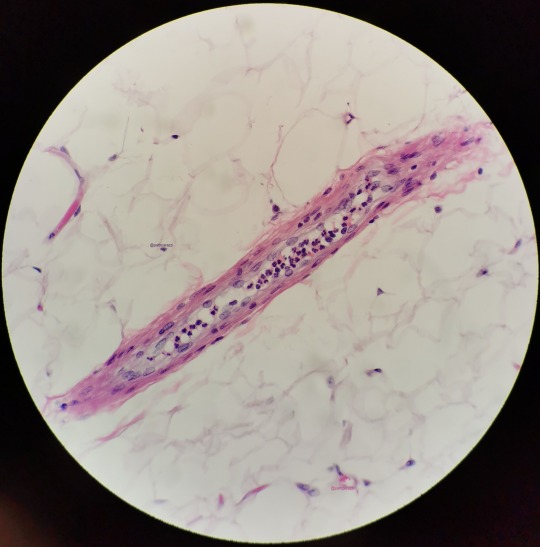
This one's pretty mundane - cross section of a blood vessel in the middle of mature adipose tissue. All the little neuts going along for the ride.
1 note
·
View note
Text
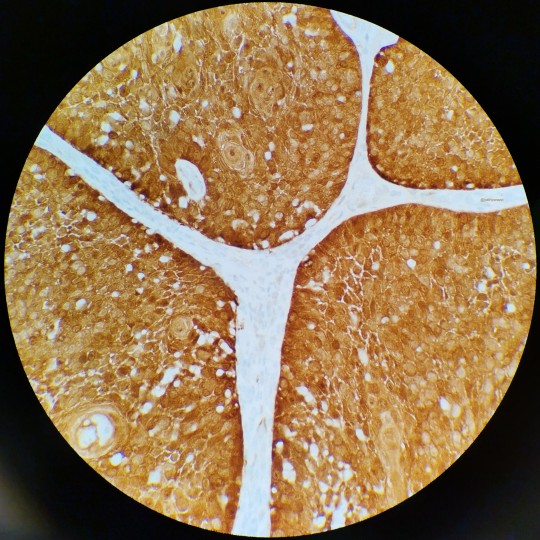
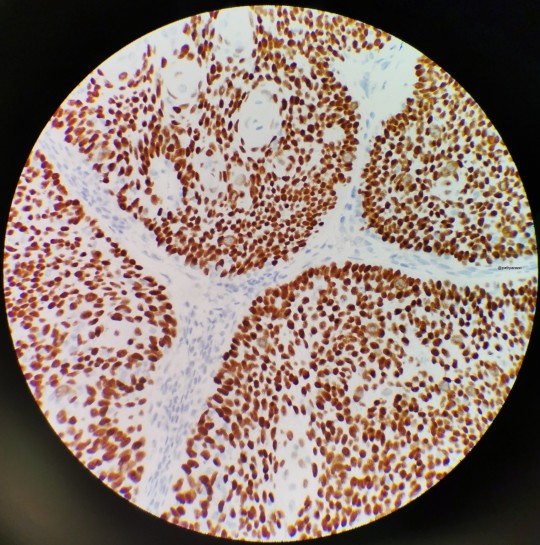
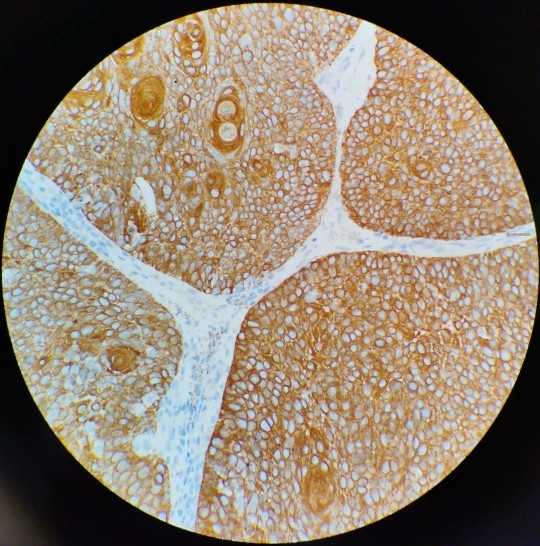
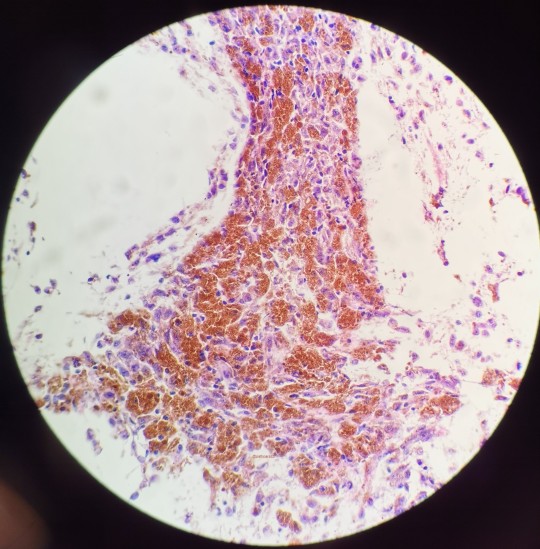
This was a consult case from an affiliate hospital. If memory serves, this was a squamous cell carcinoma of the tonsil, which means by default it's got access to the lymphatics and is poised to spread. The outside pathologist ordered p16 (left), p40 (center), and a cytokeratin AE1/AE3. Only the p16 was necessary, as HPV-association helps determine treatment and prognosis.
That said, this is a really nice example of different patterns of staining. You've got diffuse, block-like staining of p16, crisp nuclear p40, and sharp cytoplasmic outline of AE1/AE3. I don't know why I didn't take a photo of the H&E but alas.
4 notes
·
View notes