#streptomycin
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Average visit duration of Tumblr.com is 10 mins and 25 secs.
Text

The Science Research Diaries of S. Sunkavally, p 604.
#halogenation#corticosteroids#inflammation#blood glucose levels#rheumatoid arthritis#streptomycin#adrenal cortex#penicillamine#chlorpromazine#imidazole-N-methyl transferase#histamine#ascorbi acid#cortisol#Rubner's law#satyendra sunkavally#manuscript#cursive handwriting
0 notes
Text
Writing Notes: Plague

Plague - a serious, potentially life-threatening infectious disease that is usually transmitted to humans by the bites of rodent fleas. It was one of the scourges of early human history.
Endemic—A disease that occurs naturally in a geographic area/population group.
Epidemic—A disease that occurs throughout part of the population of a country.
Pandemic—A disease that occurs throughout a regional group, the population of a country, or the world.
There are 3 major forms of the disease: bubonic, septicemic, and pneumonic.
Bubonic Plague
Two to five days after infection, patients experience:
A sudden fever
Chills
Seizures
Severe headaches
Followed by the appearance of swellings or "buboes" in armpits, groin, and neck
The most commonly affected sites are the lymph glands near the site of the first infection.
As the bacteria multiply in the glands, the lymph node becomes swollen.
As the nodes collect fluid, they become extremely tender.
Occasionally, the bacteria will cause an ulcer at the point of the first infection.
Buboes—Smooth, oval, reddened, and very painful swellings in the armpits, groin, or neck that occur as a result of infection with the plague.
Septicemic Plague
Bacteria that invade the bloodstream directly (without involving the lymph nodes) cause septicemic plague. (Bubonic plague also can progress to septicemic plague if not treated appropriately.)
Does not involve the lymph glands is particularly dangerous because it can be hard to diagnose the disease.
The bacteria usually spread to other sites, including the liver, kidneys, spleen, lungs, and sometimes the eyes, or the lining of the brain.
Symptoms include:
Fever
Chills
Prostration
Abdominal pain
Shock
Bleeding into the skin and organs
Septicemia—The medical term for blood poisoning, in which bacteria have invaded the bloodstream and circulates throughout the body.
Pneumonic Plague
May occur as a direct infection (primary) or as a result of untreated bubonic or septicemic plague (secondary).
Primary pneumonic plague is caused by inhaling infective drops from another person or animal with pneumonic plague.
Symptoms, which appear within 1-3 days after infection, include:
A severe, overwhelming pneumonia
Shortness of breath
High fever
Blood in the phlegm
If untreated, half the patients will die.
If blood poisoning occurs as an early complication, patients may die even before the buboes appear.
Life-threatening Complications of Plague include:
Shock
High fever
Problems with blood clotting
Convulsions
Bioterrorism—Use of disease agents to terrorize/intimidate a civilian population.
Treatment
As soon as plague is suspected, the patient should be isolated, and local and state departments notified.
Drug treatment reduces the risk of death to less than 5%.
The preferred treatment is streptomycin administered as soon as possible.
Alternatives include gentamicin, chloramphenicol, tetracycline, or trimethoprim/sulfamethoxazole.
Prevention
Anyone who has come in contact with a plague pneumonia victim should be given antibiotics, since untreated pneumonic plague patients can pass on their illness to close contacts throughout the course of the illness.
All plague patients should be isolated for 48 hours after antibiotic treatment begins. Pneumonic plague patients should be completely isolated until sputum cultures show no sign of infection.
Residents of areas where plague is found should keep rodents out of their homes.
Anyone working in a rodent-infested area should wear insect repellent on skin and clothing.
Pets can be treated with insecticidal dust and kept indoors.
Handling sick or dead animals (especially rodents and cats) should be avoided.
Vaccines
Plague vaccines have been used with varying effectiveness since the late 19th century.
Experts believe that vaccination lowers the chance of infection and the severity of the disease. However, the effectiveness of the vaccine against pneumonic plague is not clearly known.
Vaccinations against plague are not required to enter any country.
Because immunization requires multiple doses over a 6–10 month period, plague vaccine is not recommended for quick protection during outbreaks.
Moreover, its unpleasant side effects make it a poor choice unless there is a substantial long-term risk of infection.
The safety of the vaccine for those under age 18 has not been established.
Pregnant women should not be vaccinated unless the need for protection is greater than the risk to the unborn child.
Even those who receive the vaccine may not be completely protected.
The inadequacy of the vaccines available as of 2014 explains why it is important to protect against rodents, fleas, and people with plague.
A team of researchers in the UK reported in the summer of 2004 that an injected subunit vaccine is likely to offer the best protection against both bubonic and pneumonic forms of plague.
Source ⚜ More: Writing Notes & References ⚜ Virus & Vaccine
#writing notes#plague#writeblr#dark academia#spilled ink#literature#writers on tumblr#writing reference#poets on tumblr#medicine#writing prompt#poetry#creative writing#writing inspiration#writing ideas#light academia#horace vernet#writing resources
65 notes
·
View notes
Text











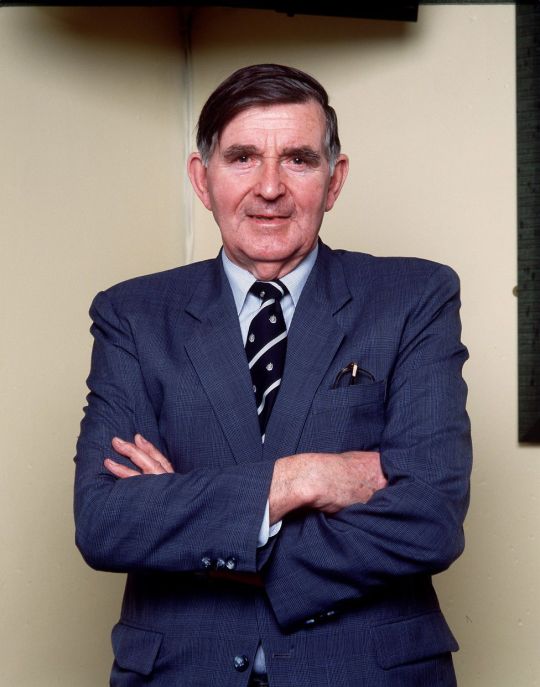
On January 19th 2010 Bill McLaren the voice of rugby died.
The BBC commentator known fondly as the voice of rugby, McLaren was the best rugby commentator of all time and by many has been described as one of the best men the world has ever seen.
He was unbiased, clear, knowledgeable, and his voice is part of the fabric of rugby in its greatest era. Scotland is proud that a Scotsman was the best rugby commentator, but he was more than that, he fought at Monte Cassino, one of the Second World War's bloodiest battles, and at one stage found himself in a ditch when he heard German voices just feet away. He was 20-years old.
I think most of us know that he should have been capped at the game he loved but tuberculosis robbed him of the chance. McLaren was born in that Borders and grew up to be a talented flanker.
Having made the Hawick first XV before the war, he played in a Scotland trial in 1947 and was on the verge of a full international cap when he contracted the tuberculosis which nearly killed him.
He was desperately ill and fading fast when the specialist asked him to be a guinea pig for a new drug called Streptomycin along with four others, three of them died but McLaren made what amounted to a miracle recovery. His first commentary was made while convalescing from TB, describing table tennis matches for the hospital radio.
McLaren studied Physical Education in Aberdeen, and went on to teach PE right through to 1987, coaching several players who went on to play for Scotland - Jim Renwick, Colin Deans and Tony Stanger.
It was through his junior reporting with the Hawick Express that he launched himself into a career of commentary, making his national debut for BBC radio in 1953, when Scotland were beaten 12-0 by Wales. The switch to television came six years later.
Scotland and Hawick sorely miss McLaren who died aged 86, he described his home town regularly by saying that a day out of Hawick "is a day wasted".
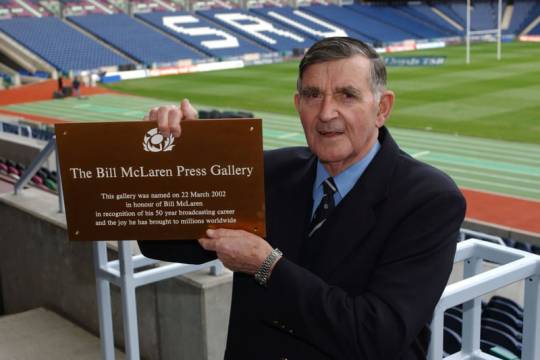
A proud moment in Bill's life would have no doubt been in 2002, when the press gallery at Murrayfield was named the Bill McLaren Press Gallery.
22 notes
·
View notes
Video
The Sea View Tuberculosis Hospital by Jonathan Haeber
The Sea View turberculosis complex was planned and built between 1905 and 1938. This is on the second floor of the women's ward of Sea View Hospital. Raymond F. Almirall designed the patterns that adorn the parapet of these buildings. Sea View was the largest and most costly municipal facility for the treatment of tuberculosis of its date in the United States. By 1961 Sea View's patients no longer needed residency, as "miraculous" new drugs, notably the antibiotic Streptomycin, allowed for a swift and inexpensive cure.
99 notes
·
View notes
Text
In the first 6 years of life your child receives the following through vaccines:
•17,500 mcg 2-phenoxyethanol (antifreeze)
•5,700 mcg aluminum (neurotoxin)
•Unknown amounts of fetal bovine serum(aborted cow blood)
•801.6 mcg formaldehyde (carcinogen, embalming agent)
•23,250 mcg gelatin (ground up animal carcass)
•500 mcg human albumin (human blood)
•760 mcg of monosodium L-glutamate (causes obesity & diabetes)
•Unknown amounts of MRC-5 cells (aborted human babies)
•Over 10 mcg neomycin (antibiotic)
•Over 0.075 mcg polymyxin B (antibiotic)
•Over 560 mcg polysorbate 80 (carcinogen)
•116 mcg potassium chloride (used in a lethal injection)
•188 mcg potassium phosphate (liquid fertilizer agent)
•260 mcg sodium bicarbonate (baking soda)
•70 mcg sodium borate (Borax, used for cockroach control)
•54,100 mcg of sodium chloride (table salt)
•Unknown amounts of sodium citrate (food additive)
•Unknown amounts of sodium hydroxide (Danger! Corrosive)
•2,800 mcg sodium phosphate (toxic to any organism)
•Unknown amounts of sodium phosphate monobasic monohydrate (toxic to any organism)
•32,000 mcg sorbitol (Not to be injected)
•0.6 mcg streptomycin (antibiotic)
•Over 40,000 mcg sucrose (cane sugar)
•35,000 mcg yeast protein (fungus)
•5,000 mcg urea (metabolic waste from human urine)
•Other chemical residuals
(From the book, "What The Pharmaceutical Companies Don't Want You To Know About Vaccines" - By Dr.Todd M. Elsner)
Let this sink in. 🤔
#pay attention#educate yourselves#educate yourself#knowledge is power#reeducate yourself#reeducate yourselves#think for yourselves#think about it#think for yourself#do your homework#do some research#do your own research#ask yourself questions#question everything#medical malpractice#medical corruption#crimes against humanity
121 notes
·
View notes
Text
okay so i was reading about the crazy rat parabiosis experiments (they gave a rat a brain lesion to make it obese and then hooked its blood up to another rat. and the other rat didnt eat at all and starved. science) and i noticed this crazy diagram
so i checked the paper it's from, and...
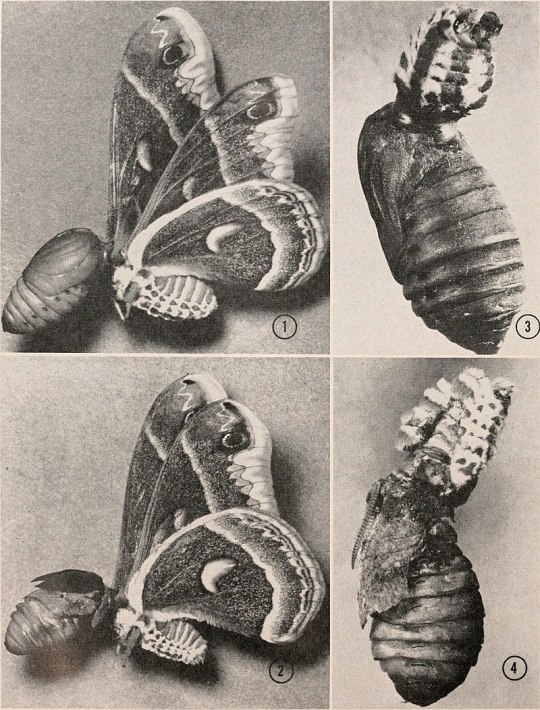
The moth was deeply anesthetized with carbon dioxide. The antennae and the fore and midlegs were excised and melted wax was applied with a drawing-pen to cover the entire head and prothorax. Then, with a single transverse cut, the head was removed to leave a collar of wax at the anterior open end of the prothorax. Crystals of an equal-part mixture of phenylthiourea and streptomycin sulfate wer placed in the wound along with enough Ringer's solution to fill the cavity
The pupal partner was deeply anesthetized with carbon dioxide and a disc of integument, about 4 mm. in diameter, was cut from the mesothoracic tergum. Th underlying epidermis was trimmed away with microscissors, care being taken t avoid any damage to the aorta which extends beneath the midline at this point. Melted wax was applied to the integument around the margin of the wound Crystals of phenylthiourea and streptomycin were placed in the wound and the cavity was filled with a few drops of Ringer's solution
The two animals were oriented in a cradle of plasticene and the wax-coated openings were brought into juxtaposition. The pupal abdomen was compressed until the pupal blood filled the narrow opening between the animals, all air being thereby displaced. The junction was then sealed with melted wax to yield a parabiotic preparation such as shown in Figure 1
The preparation was then removed from the anesthesia funn 25? C. Under this condition, the moth commonly initiated ener its wings. In order to prohibit this activity, the wings were pl jaws of a spring-loaded clothes-pin.
okay. so they stuck some moths and pupas together. insane, but like. whatever. i guess. EXCEPT heres what happened
Forty preparations were assembled, of which ten soon died and Table II summarizes the several types of experiments that were p each of the 30 viable preparations the pupal partner initiated adu within ten days at 25? C. Attention is directed to the effects of on the course of this developmen
When the headless partner was a male or female Polyphemus underwent normal adult development. The same was true in 7 of 8 preparations in which the headless partner was a female Cecropia moth. But in all ten prepations in which the headless partner was a male Cecropia moth, the pupa metamorphosed, not into a normal moth, but into a creature which retained lar of pupal cuticle (Fig. 2). It seems necessary to conclude that a male C moth, though headless and without any corpora allata, can somehow favor release of juvenile hormone within the parabiotic preparation
In the analysis of these experiments we have centered attention on the effe the parabiosis on the pupal partner. But, what about the developmental of the other half of the combination-the headless moth? For present purposes suffice it to say that in about a third of the preparations the developmental re of the pupa spread to the adult partner and caused the latter to molt. Th extended over both the thorax and abdomen, but never included the win old adult cuticle was detached from the underlying epidermis and replace smooth new cuticle which was of adult type, except for the generalized of scales or hairs.
this is fucked up huh. the pupa and the moth fucked each other up. neither of them metamorphosed right. also apparently the moths lived longer. moths...
48 notes
·
View notes
Text
Because streptomycin was isolated from a microbe discovered on New Jersey soil, and because of its activity against tuberculosis and Gram negative organisms, and in recognition of both the microbe and the antibiotic in the history of New Jersey, S. griseus was nominated as the Official New Jersey state microbe. The draft legislation was submitted by Senator Sam Thompson (R-12) in May 2017 as bill S3190 and Assemblywoman Annette Quijano (D-20) in June 2017 as bill A31900. The bill was passed on 2018-01-08 The bill designates Streptomyces griseus as New Jersey State Microbe (New Jersey Senate Bill 3190 (2017). Governor Phil Murphy signed the bill making it official in 2019.[39]
Brilliant
14 notes
·
View notes
Text
It always feels so bizarrely anachronistic when professors talk about the bubonic plague in class. What do you MEAN use streptomycin for The Black Plague. What’s next???? You gonna tell me how to do faerie abduction prophylaxis???? To send witches and heretics to a psych evaluation???? SHOULD I RUN MY TREATMENT PLAN BY THE POPE?????
#my post#how do I even tag this#medblr#I guess#absolutely insane we still have the black plague#why did we keep this one but not the dancing plague#that was much cooler#also sort of related but they found a dead rat at my teaching hospital today LMAO
13 notes
·
View notes
Text
Creativity, therefore, it is important for a Jesuit. Pope Francis, during a visit with the Jesuit priests and other staff members of La Civiltà Cattolica, had articulated a triad of important characteristics relevant to the cultural initiatives of the Jesuits. I turn my thoughts to that day, June 14, 2013. I recall that back then, in a conversation just before the meeting with the entire group, the pope had already informed me about this triad: dialogue, discernment, frontier. And he insisted particularly on the last point, quoting Pope Paul VI. In a well-known speech, Paul VI had spoken directly about the Jesuits: “Wherever in the church—even in the most difficult and extreme fields, in the crossroads of ideologies, in the social trenches—there has been and is now conversation between the deepest desires of human beings and the perennial message of the Gospel, Jesuits have been and are there.” I ask Pope Francis for a further explanation: “You asked us to be careful not to fall into ‘the temptation to tame the frontiers’: one must go out to the frontiers, not bring the frontiers home in order to paint them a bit artificially and tame them.” What were you referring to? What exactly did you wish to tell us? This interview, as you know, was organized by a group of magazines directed by the Society of Jesus: what invitation do you wish to extend to them? What should their priorities be? “The three key words that I commended to La Civiltà Cattolica can be extended to all the journals of the Society, perhaps with different emphases according to their natures and their objectives. When I insist on the frontier, I am referring in a particular way to the need for those who work in the world of culture to be inserted into the context in which they operate and on which they reflect. There is always the lurking danger of living in a laboratory. Ours is not a ‘lab faith,’ but a ‘journey faith,’ a historical faith. God has revealed himself as history, not as a compendium of abstract truths. I am afraid of laboratories because in the laboratory you take the problems and then you bring them home to tame them, to paint them artificially, out of their context. You cannot bring home the frontier, but you have to live on the border and be audacious.” I ask for examples from his personal experience. “When it comes to social issues, it is one thing to have a meeting to study the problem of drugs in a slum neighborhood and quite another thing to go there, live there and understand the problem from the inside and study it. There is a brilliant letter by Father Arrupe to the Centers for Social Research and Action on poverty, in which he says clearly that one cannot speak of poverty if one does not experience poverty, with a direct connection to the places in which there is poverty. The word insertion is dangerous because some religious have taken it as a fad, and disasters have occurred because of a lack of discernment. But it is truly important.” “The frontiers are many. Let us think of the religious sisters living in hospitals. They live on the frontier. I am alive because of one of them. When I went through my lung disease at the hospital, the doctor gave me penicillin and streptomycin in certain doses. The sister who was on duty tripled my doses because she was daringly astute; she knew what to do because she was with ill people all day. The doctor, who really was a good one, lived in his laboratory; the sister lived on the frontier and was in dialogue with it every day. Domesticating the frontier means just talking from a remote location, locking yourself up in a laboratory. Laboratories are useful, but reflection for us must always start from experience.”
-INTERVIEW WITH POPE FRANCIS by Fr Antonio Spadaro, August 19, 2013
2 notes
·
View notes
Text
Prevalence Of Staphylococcus Aureus In Nasal And Skin Of Apparently Healthy Food Handlers And Attendants In Restau by Iyevhobu Kenneth Oshiokhayamhe in Journal of Clinical Case Reports Medical Images and Health Sciences
Abstract
Food handlers play a major role in the transmission of food borne diseases which represents a global health burden. Carriage of Staphylococcus aureus, in general, and enterotoxigenic strains, in particular, is an important risk factor for the contamination of food. This study was undertaken to determine the prevalence and risk factors associated with nasal and skin carriage of Staphylococcus aureus among 150 food handlers working in different restaurant in Ekpoma. Thirty (10%) persons were found to be significant (P< 0.05) carriers of Staphylococcus aureus of which highest occurrence of 24 (16%) from anterior nasal nares and 6 (7.5%) from skin of food handlers and restaurant workers. Prevalence and distribution of Staphylococcus aureus in relation to gender among food handlers and restaurant workers, showed high occurrence in females of 17 (56.6%) than males 13 (43.3%) with no significant difference in comparison of variability (P>0.05). Susceptibility pattern of Staphylococcus aureus isolated from this study had high sensitivity pattern of 93% to Zennacef, 80% to Rocephin, 93% to Ciprofloxacin, 70% to Gentamycin, intermediate sensitivity to Septrin 53%, Streptomycin 50%, and resistant to Erythromycin 40%, Amoxacilin 36% and Ampiclox 17%. From this study, Staphylococcus aureus is the most prevalent among them isolates that colonizes the skin and mucosal surfaces of healthy food handlers and restaurant workers. These findings resurges the imperative need for protective measures including increased public awareness programs, regular monitoring of food handlers for food borne pathogens and intensive training on primary health care and hygiene and future research addressing effective methods for sustained eradication of Staphylococcal skin and nasal carriage are clearly warranted to reduce the high risk of subsequent infection. It is our opinion that concerted efforts need to be made to educate food handlers and restaurant workers on the importance of personal hygiene and the use of protective gadgets like nose masks while handling food products; since they serve as potential sources of staphylococcal food poisoning.
Keywords
Food, Handler, Staphylococcus, Restaurant, Nasal, Skin
INTRODUCTION
Staphylococcus aureus avoidable medical and economic burden, the true incidence and prevalence of pathogenic strain of foodborne diseases is difficult to quantify. Risk factors implicated in foodborne diseases as identified by Centers for Disease Control and Prevention included unsafe sources, inadequate cooking, improper holding, contaminated equipment and poor personal hygiene implicating that the food handler dimension is crucially important (FDA, 2009). Food handlers have been implicated in a plethora of foodborne diseases. It has been reported that one of the important pathogens often transmitted via food contaminated by infected food handlers is Staphylococcus aureus (Verkaik et al., 2011). Bacteria of the genus Staphylococcus are Gram-positive cocci that are microscopically observed as individual organisms (Francois and Schrenzelg, 2008). Staphylococcus aureus is pathogenic ubiquitous species and may be a part of human flora found in the axillae, the inguinal and perineal areas, and the anterior nares (Bayer et al., 1998). Von Eiff et al., (2001) described 3 patterns of carriage: those who always carry a strain, those who carry the organism intermittently with changing strains, and a minority of people who never carry Staphylococcus aureus (Bayer et al., 1998). Persistent carriage is more common in children than in adults (Iwase et al., 2010). Nasal carriers may be divided into persistent carriers with high risk of infection and intermittent or non-carriers with low risk of infection (Blot et al., 2002). Direct invasion through breaks in the skin or mucus membrane leads into the production of superficial local infections such as folliculitis, furuncles and abscesses (Wertheim et al., 2005). This versatile pathogen is very well adapted to colonize the human skin and the human body provides some major ecological niches for this species. The anterior nares is the most frequent carriage site for Staphylococcus aureus, nonetheless extranasal sites typically harbor the organism including the skin, perineum and pharynx (Wertheim et al., 2005; Verkaik et al., 2011).
Until recently, reports on food contamination by Staphylococcus aureus, were mainly limited to occasional detections in the environment, the source of food and food itself. However, it is reported that human carriers are the most important source for transmission and the association between food handlers and the transmission of food borne disease frequently presents an investigative challenge (Jordá et al., 2012). Consideration into risk factors, transmission routes and many aspects of prevalence of carriage of foodborne pathogens among food handlers to eliminate carriage is necessary. Bodies concerned with food safety are left to consider whether interventions such as decolonization, continued monitoring or restrictions in the occupational activities are required (National Disease Surveillance Centre, 2004). Although skin carriage of Staphylococcus aureus, is less reported than nasal carriage, little is known about the prevalence and risk of skin carriage of enterotoxigenic strains of Staphylococcus aureus, among food handlers. Accordingly, the current study investigated the prevalence and risk factors associated with anterior nasal nares and skin carriage of Staphylococcus aureus, amongst food handlers working in different restaurant in Ekpoma Edo State.
Healthy carriers are potential source of Staphylococcus aureus infection and spread to other body sites as well as to other individuals. Staphylococcus aureus have been found frequently as aetiological of a variety of human infections. Centre for disease control (CDC) reported Staphylococcus aureus as primary source of infections, which could be transferred from individual to another, The organism also elaborates toxins that can cause specific diseases or syndromes and likely participate in the pathogenesis of staphylococcal infection. Enterotoxin-producing strains of S aureus cause one of the most common food-borne illnesses (food poisoning). The most common presentation is acute onset of vomiting and watery diarrhea 2-6 hours after ingestion. The symptoms are usually self-limited. The cause is the proliferation of toxin-producing organisms in uncooked or partially cooked food that an individual carrying the staphylococci has contaminated (Matthews et al., 1997). This study is set determines the prevalence of Staphylococcus aureus from skin and nasal nares of apparently healthy food handlers in restaurant which could be the source of Staphylococcus aureus food contamination resulting to food born infection in Ekpoma.
MATERIALS AND METHODS
This project work from its inception, sample collection, sample analysis and compilation was carried out within a period of four months with a total of hundred Fifty Skin and nasal swab samples from different restaurant workers and food handlers in Ekpoma. A total of one hundred fifty (150) nasal and skin swab were randomly collected from male and female food handlers and restaurant workers grant consent.
Informed consent was requested and granted by the food handlers and restaurant workers under investigation. The concept of the study was explained to them and having understood its dimensions, granted their informed consent.
Sample Collection: One hundred and fifty specimen were collected randomly from males and females food handlers and restaurant workers within Ekpoma metropolis. The samples (150 nasal swabs and 150 skin swab). Nasal swab were collected in good light vision from subjects by bending their heads backward to collect the specimens deep down the anterior passages using a sterile swab stick. Both right and left nostrils were swabbed bearing labels as nasal swabs, sex, code number and date of collection. The swabs sticks were carefully returned to their sterile containers, sealed with adhesive tape and labelled accordingly. Skin swab was collected by swabbing their skin (especially their fore arm) with a swab moist with physiological saline aseptically and the swabs sticks were carefully returned to their sterile containers. Collected specimen was taken to the laboratory where bacteriological analysis was carried out immediately.
Procedure for Culture: The swab stick were used to make a primary inoculum on each agar surface (blood agar and chocolates agar plate). Spreading was done by streaking from the primary inoculum using a sterile inoculating wire loop to obtain discrete bacterial colonies. The plates were then incubated at 370C for 24 hours. Growth was observed after incubation, and the colonial morphology was studied carefully, noting the size, shape, edge, colour, consistency, haemolysis, elevation and opacity of the colonies. This was followed by Gram staining (Ochei and Kolhatkar, 2000).
Method for Detection of Staphylococcus aureus: The colonies that were yellow pigmented or cream white (Cheesbrough, 2000) were sub-cultured onto mannitol salt agar and selected for catalase (using H2O2) and coagulase tests (using plasma). Mannitol fermenting and slide coagulase positive isolates were identified as Staphylocuccus aureus.
Antibiotic Sensitivity Test: Antibiotic disc such as Erythromycin, Gentamycin, Streptomycin, Ciprofloxacin, Ampicillin, Septrine, Zinnacef, Amoxicilin and Rocephin (manufactured by Abtek Biologicals Ltd) were used to test the susceptibility of Staphylococci aureus isolates obtained. The test isolates were inoculated into sterile peptone water broth. The antibiotic discs were placed aseptically on the seeded plate. They were incubated at 370C for 24hours and examined for zones of inhibition. The zones of inhibition were measured in millimetres and recorded. Antibiotic zones less than 10mm in diameter were recorded as been resistant (R) by the organism while those with diameters of 10mm and above were recorded as sensitive (S)
Statistical Analysis: The collected data was expressed as Frequency and percentage. Comparison of qualitative variables was made using chi-square test. In all cases studied, the difference having p<0.05 were considered statistically significant using interactive calculation Chi square tool software (version 18).
RESULTS
Based on standard bacteriological analytical methods, from investigation of 300 samples of [nasal swab (150), skin swab (150)] from food handlers and restaurant workers in Ekpoma, revealed 30(10%) distribution of Staphylococcus aureus prevalence with the highest occurrence of 24 (16%) from nasal swab and 6 (7.5%) from skin swab. Other growths of non-Staphylococcus aureus were excluded from this study. The significant difference of Staphylococcus aureus isolates distribution among samples in this study was statistically significant (P< 0.05) with X2cal=26.057 p-value 0.000.
X2cal=26.057, Degree of freedom=2, p-value=0.0000 Key: N - Number , S. aureus: Staphylococcus aureus
X2cal=18.04, Degree of freedom=2, p-value=0.000, Key: N - Number
X2 cal=1.663, Degree of freedom=1, p-value=0.435, (p>0.05).
KEY:CN-Gentamycin, Z-Zennacef, R-Rocephin, CPX- Ciprofloxacin, SXT-Septrin, S-Streptomycin, E-Erythromycin AM- Amoxacilin , APXAmpiclox
DISCUSSION
Staphylococcus species are regional flora of the skin and mucus membrane of the body, certain species have been found frequently as aetiological agent of a variety of human and animal infections. The most common among these infections are the superficial supportive infection caused by Staphylococcus aureus. Infection can result to life threatening conditions disease spectrum which includes abscesses, septicemia, osteomyelitis, endocarditis and cellulitis, pneumonia, in addition to various toxin mediated diseases as toxic shock syndrome and staphylococcal food poisoning. The variety of such spectrum of clinical manifestations is mostly dependent on the numerous virulence factors produced by each strain (Vasconcelos and da Cunha, 2010). The ingestion of the preformed toxins produced by Staphylococcus aureus (enterotoxigenic strains) in food often results to the development of food poisoning. Findings from this investigation indicate a significant (P< 0.05) distribution of Staphylococcus aureus of 30(10%) prevalence with the highest occurrence of 24 (16%) from anterior nasal nares of food handlers and restaurant workers, 6 (7.5%) from skin swab which is in agreement with investigation reported by Mous-tafa et al., (2013) of 10.5% Nasal Carriage of Staphylococcus aureus and Risk Factors among Food Handlers-in Egypt. The findings from this studied in relation to area of study, was not in agreement with findings report by Eke et al., (2015), with a wide variation of 60% prevalence from 100 nasal swab analysis of food handlers and restaurant workers in Ekpoma. The reduced significant prevalence from this study is proportionately an improve hygiene of food handlers and workers in restaurant. This study variables revealed that gender, age, marital status nor level of education had no significant effect with respect to the nasal and skin carriage of Staphylococcus aureus. This study findings also reveal anterior nasal nares of food handlers and restaurant workers to harbour pathogenic Staphylococci species [Staphylococcus aureus 24(16%) to that of their skin 6(7.5%) with significant increase difference of (P>0.05) P- value 0.000].
Prevalence and distribution of Staphylococcus aureus in relation to gender among food handlers and restaurant workers, showed high occurrence in females food handlers and workers of 17 (56.6%) than males 13 (43.3%) with no significant difference in comparison of variability (P>0.05) and not in agreements with the findings by Eke et al., (2015), which report males food handlers to have high prevalence than the females in Ekpoma. The disparity of this report may be due to the subject who consent to participate as at time of study in regards to gender present in restaurant.
The sensitivity pattern of Staphyloccus aureus isolated from this study had high susceptibility to Gentamycin, Zennacef, Rocephin, Ciprofloxacin intermediate to Septrin, Streptomycin, and resistant to Amoxicillin, Erythromycin and Ampiclox which in agreement with the study reported by Eke et al., (2015). From this research it can be suggested that skin and nasal nares harbours Staphylococcus aureus which can be source of enterotoxigenic stains causing food born infection observed in our restaurant this days.
From all the organisms known to cause food born infection, Staphylococcus aureus is the most prevalent among them that is easily isolated and it colonizes the skin and mucosal surfaces of healthy individuals. The isolation of this organism learned to us that, as a microflora, it has a high percentage of causing infectious disease related to illness. Evidence from the result obtained has show that the skin and nasal nares has carrying capacity of Staphylococcus aureus. In contrast, healthy individuals as worker and food handlers in restaurant are risk factor of food born infection (food poisoning).
In conclusion, a relatively high prevalence rate of Staphylococcus aureus in nasal nares and skin carriage was recorded among the investigated food handlers. Moreover, 10% of the investigated carriers harboured Staphylococcus aureus in their anterior nares increasing the likelihood of transmission of the pathogen to the handled food. These findings resurges the imperative need for protective measures including increased public awareness programs, regular monitoring of food handlers for food borne pathogens and intensive training on primary health care and hygiene. Finally, the current findings clearly highlight the significance of implementation of efficient quality control systems in areas of direct contact with food product as good manufacturing practices and standard operational procedures and future research addressing effective methods for sustained eradication of Staphylococcal skin and nasal carriage are clearly warranted to reduce the high risk of subsequent infection.
CONFLICT OF INTEREST
The authors declare no conflicts of interest. The authors alone are responsible for the content and the writing of the paper.
FUNDING
This research did not receive any grant from funding agencies in the public, commercial, or not-for-profit sectors.
AUTHORS’ CONTRIBUTIONS
Iyevhobu, K.O. and Obodo, B.N., conceptualized the laboratory work and provided scientific guidance, Momoh A.R.M., Airefetalor, A.I. and Okobi, T.J. designed and wrote the manuscript while Etafo, J. and Osagiede, E.K. conducted experiments.
ACKNOWLEDGEMENTS
The authors would like to thank all the Laboratory and technical staffs of the department of Medical Laboratory Science, Ambrose Alli University Ekpoma, Edo State for their excellent assistance and St Kenny Research Consult, Ekpoma, Edo State for providing medical writing support/editorial support in accordance with Good Publication Practice (GPP3) guidelines.
#Restaurant#JCRMHS#Nasal#staphylococcal food#Research Article in Journal of Clinical Case Reports Medical Images and Health Sciences#Susceptibility pattern#Handler#Skin#Staphylococcus#Food
3 notes
·
View notes
Text
Actinomycetota
Group: Terrabacteria
Gram-stain: Positive
Etymology: For Actinomyces bovis. From the Greek "aktis", meaning "ray", and "myketes", meaning "fungus". Some bacteria in this phylum form fungus-like branched colonies, hence the name: "ray fungus". Note the similarity to mycelium networks.
About: Actinomycetota contains tuberculosis (Mycobacterium tuberculosis), the leading cause of death by bacterial infection. It is also the second leading cause of death by any infectious disease, only surpassed by COVID-19. Many other members of the genus Mycobacterium are also pathogenic, such as Mycobacterium leprae, which is responsible for Hansen's disease (better known as leprosy).
But Actinomycetota is far from all bad. In fact, it is possibly the most studied and used bacterial phylum in terms of medical, agricultural, environmental, and biotechnological applications. Actinomycetota play a huge role in nutrient cycling in soil ecosystems, making them crucial for maintaining the health of soil. They are therefore a pillar of modern agriculture. Some Actinomycetota are nitrogen-fixing, and can be symbiotic with trees. The phylum is also a source of antibiotics, especially with the genus Streptomyces: these bacteria naturally produce several antimicrobials (including streptomycin), and thus have use both in medicine and as a natural pesticide against other microorganisms in the soil.
Actinomycetota colonies have long been noted to resemble those of fungi, and early researchers originally believed that this phylum was a fungi. Indeed, Actinomycetota and fungi share similar roles, being largely decomposers. However, the much smaller Actinomycetota fill their own ecological niche.
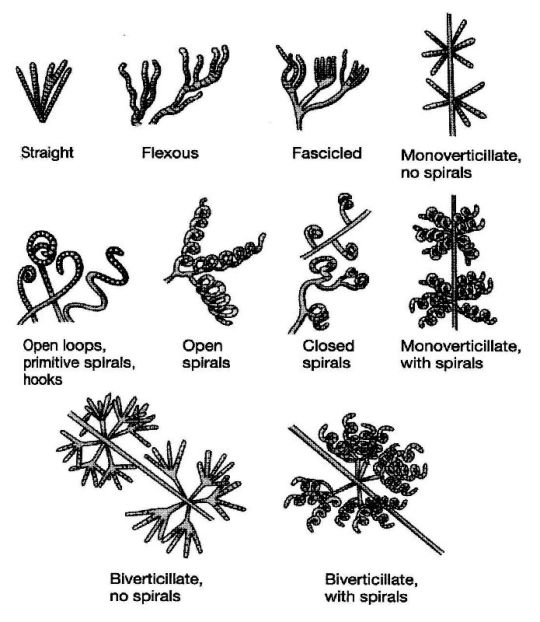
In terms of reproduction, Actinomycetota and fungi are especially similar. Actinomycetota produce spores, but not just endospores: they also form spores using external structures called "hyphae". Hyphae are branched, filamentous structures that make up what is called a "mycelium", and can have a variety of shapes. Many hyphae, including those in Actinomycetota, are reproductive structures that subdivide to create spores. This is a process ubiquitous among fungi but limited to pretty much only the Actinomycetota phylum of bacteria. The below image depicts some possible hyphae structures in Streptomyces bacteria:
In addition to all this, Actinomycetota may contain the oldest living organisms on earth, which could have been frozen in Siberian or Antarctic ice for thousands (or millions) of years. While Actinomycetota do produce durable endospores, it is also theorized that they may also be able to survive in a frozen but non-dormant state: not reproducing, but still metabolizing, and thus being able to repair their DNA.
While the theory is speculative, evidence of metabolic activity has been detected from soil samples after more than 600,000 years of permafrost, studied under ambient conditions (i.e. not thawed to trigger endospore germination). We have actually cultivated Actinomycetota from other ancient permafrost samples, such as 28,000 year old mammoth poop.

6 notes
·
View notes
Text
Is it safe to closely interact with marmots?

Marmots, or groundhogs, are cute but risky.
They host bubonic plague, a zoonotic disease caused by Yersinia pestis, spread by fleas. Many think plague is extinct, but it persists naturally. Infected rodents like marmots can transmit it to humans. Untreated, plague can be fatal, especially pneumonic plague, spreading through droplets with over 90% mortality. Streptomycin is the preferred antibiotic, significantly reducing mortality if administered early.

2 notes
·
View notes
Text


On January 19th 2010 Bill McLaren the voice of rugby died.
The BBC commentator known fondly as the voice of rugby, McLaren was the best rugby commentator of all time and by many has been described as one of the best men the world has ever seen.
He was unbiased, clear, knowledgeable, and his voice is part of the fabric of rugby in its greatest era. Scotland is proud that a Scotsman was the best rugby commentator, but he was more than that, he fought at Monte Cassino, one of the Second World War's bloodiest battles, and at one stage found himself in a ditch when he heard German voices just feet away. He was 20-years old.
I think most of us know that he should have been capped at the game he loved but tuberculosis robbed him of the chance. McLaren was born in that Borders and grew up to be a talented flanker.
Having made the Hawick first XV before the war, he played in a Scotland trial in 1947 and was on the verge of a full international cap when he contracted the tuberculosis which nearly killed him.
He was desperately ill and fading fast when the specialist asked him to be a guinea pig for a new drug called Streptomycin along with four others, three of them died but McLaren made what amounted to a miracle recovery. His first commentary was made while convalescing from TB, describing table tennis matches for the hospital radio.
McLaren studied Physical Education in Aberdeen, and went on to teach PE right through to 1987, coaching several players who went on to play for Scotland - Jim Renwick, Colin Deans and Tony Stanger.
It was through his junior reporting with the Hawick Express that he launched himself into a career of commentary, making his national debut for BBC radio in 1953, when Scotland were beaten 12-0 by Wales. The switch to television came six years later.
Scotland and Hawick sorely miss McLaren who died aged 86, he described his home town regularly by saying that a day out of Hawick "is a day wasted".
A proud moment in Bill's life would have no doubt been in 2002, when the press gallery at Murrayfield was named the Bill McLaren Press Gallery.
A proud moment in Bill's life would have no doubt been in 2002, when the press gallery at Murrayfield was named the Bill McLaren Press Gallery.
7 notes
·
View notes
Text
These were also in Colorado Springs, Colorado Springs was full of them and they are still occasionally found in people’s yards today. I visited one in the Pioneer museum in Colorado Springs.
The problem is TB patients had a very chance of suffering from pneumonia once TB went into remission. It’s happened in tons of my case studies. If Arthur could have survived both TB AND pneumonia, then he would have been considered “Ok”. Not good, but “Ok”. However, I can’t predict how long he would have lived afterwards. Some TB patients had tuberculosis come in a second wave. This is, unfortunately, very common. Some people lived a few months, a few years and some lived decades after surviving the second wave.
Fortunately, survival after two waves include people who lived hard, like Arthur. Trudeau lived till 68, and that is after 2 bouts of TB and pneumonia, with the third wave of TB being his cause of death.This is very likely a reason why Arthur would have been in New Austin if they had kept him in the epilogue and continued the TB storyline. I personally do NOT think John was ever going to kill him.
MISC NOTES:Related to RDR: Important side note: Sex workers were especially blamed for spreading TB which makes sense because of the contact with multiple people, but it’s not that different than someone who works at a factory every day, runs a shop or works at the docks, or in similar situations. Anyone could spread it. This is why it is actually technically very offensive to ask someone like Abigail if she had TB because it would be a way to imply she is unclean as a person. (Which people in the game already believe with some of the fandom similarly treating her poorly.) The history of sex work is my other specialty, so I am very familiar with their history. I will say, from what I gathered, sex workers did NOT seem to be that much more affected than others, but at the same time, we don’t have a lot of records of people who weren’t white upper-class Christian men. So we have these records if these people were arrested, but remember that all of the examples of people I mentioned were viewed as second-class citizens. Therefore, we have hardly any records of sex workers as actual people and historians have to be creative to find other ways to research them properly. Modern day: TB is also becoming antibiotic-resistant at a frightening pace. This will become a massive problem. Treatment requires at least two antibiotics - streptomycin being the main choice for the primary antibiotic. This treatment lasts months, and these antibiotics are insanely strong. They can really mess with the body’s system. I’ve seen it. My father was one of the lucky ones only having to take the pills for 8 months. Many others take it from a year to even 18 months. Other people take the pills and undergo radiation therapy to treat TB.
Modern science can’t produce enough new antibiotics to outpace it, but alternative treatments do appear to be promising. If you want me to write more about TB or for any other history questions, feel free to send me an anon/message.
Tuberculosis and the Wild West
Spoilers for RDR2 , but it’s been since 2018, y’all. Trigger warnings for serious talk of severe terminal illness and severe stigma. As of 12/20 or 20/12, I have fixed some of the wording and added a few new things so please seriously head the warnings. Ok, first, some background: I’ve been studying TB since 2018; my father had a form of TB twice. I’m a historian, and one of my specialties is the history of medicine. Of course, you don’t need to be a historian to write something like this. Also, please “like” and reblog, this sort of content takes time. Tons of pics of buildings, and info below of the “lore” and IRL people.
Background info about TB that y’all need to know: TB is still horrifically deadly and still a leading cause of death. To give you all an idea about how recent genuine scientifically proven treatments were- antibiotics targeting TB were not discovered until the late 40s. However, sanatoriums (TB hospitals) and similar TB-related places didn’t all close until 1970. My sister was born in 1977. To give you all an idea of how treeified people were of this disease, think of the stigma with the AIDS/HIV crisis in the 1980s or the early fears surrounding Covid.
TB is one of the three oldest diseases dating back to Ancient Egypt with early evidence appearing through ancient mummies. Starting around the 18th century, western people believed TB was a disease of the elite granting someone ethereal beauty, writing prowess, and artistic talents. It was known as a “romantic disease” and a “beautiful death” - both of which we know aren’t true. Some western beauty standards are influenced by TB including rouged lips, blush, pale skin and a thin figure accentuated with corsets. However, the appearance was due to the patient wasting away. Patients actually had bloodied lips, feverish cheeks, a pale complexion from the illness and losing a large amount of body weight. That’s why TB was initially called consumption.(There have been many other names for TB including the White Plague and Captain of All These Men of Death and phthisis which is Greek in origin.) However, people eventually woke up and realized, “Oh wait, this isn’t so sexy” The disease spread like wildfire, especially in the cities affecting whole families as was seen with Doc Holliday. Soon, society blamed anyone who wasn’t a white upperclass person AND those who were "immoral . They believed it was someone’s own fault if they had the disease. People held a very e*gen*c view of the disease believing their activities or who their families were caused this. Immoral in this instance includes thieves, sex workers, bar workers, drunkards, violent people, women who had children out of wedlock, said child born out of wedlock, and homeless people. Obviously, this isn’t true. It was overcrowded spaces, poor hygienic practices, but also animals, especially cows and deer. Ironically, the deer/stag plays a huge role in RDR 2. A few aspects from RDR 2 were inspired by Doc Holiday, one of the greatest gunslingers and outlaws in American history. His talents with the gun were considered by some as otherworldly. He and Wyatt Earp are most famous for the shoot-out at the OK Corral. Doc was dying of TB and headed west in order to potentially receive some medical attention, but found out that being an outlaw was great fun. Watch Tombstone for a fictionalized version of him. He had a very colorful life, but died of TB in Glenwood Springs, Colorado, at the age of 36. The same age as you know who.

This leads us to RDR 2 itself. The short answer about survival is potentially yes, but with some major stipulations. I have traveled across the country studying TB and visiting TB sites and have seen these locations firsthand. Read further to read how survival was possible and for pictures of key locations.
Weiterlesen
824 notes
·
View notes
Text
In the 1940s, as new antibiotics had begun to appear on the horizon, physicians had encountered an important quandary: how might one objectively test the efficacy of any novel drug? At the Medical Research Council in Britain, the question had taken on a particularly urgent and rancorous note. [...] The drug [Streptomycin] was in critically short supply, with doctors parrying to use even a few milligrams of it to treat a variety of other infections. To ration streptomycin, an objective experiment to determine its efficacy in human tuberculosis was needed. But what sort of experiment? An English statistician named Bradford Hill (a former victim of TB himself) proposed an extraordinary solution. Hill began by recognizing that doctors, of all people, could not be entrusted to perform such an experiment without inherent biases. Every biological experiment requires a “control” arm—untreated subjects against whom the efficacy of a treatment can be judged. But left to their own devices, doctors were inevitably likely (even if unconsciously so) to select certain types of patients upfront, then judge the effects of a drug on this highly skewed population using subjective criteria, piling bias on top of bias. Hill’s319 proposed solution was to remove such biases by randomly assigning patients to treatment with streptomycin versus a placebo. By “randomizing” patients to each arm, any doctors’ biases in patient assignment would be dispelled. Neutrality would be enforced—and thus a hypothesis could be strictly tested. Hill’s randomized trial was a success. The streptomycin arm of the trial clearly showed an improved response over the placebo arm, enshrining the antibiotic as a new anti-TB drug. But perhaps more important, it was Hill’s methodological invention that was permanently enshrined. For medical scientists, the randomized trial became the most stringent means to evaluate the efficacy of any intervention in the most unbiased manner.
Siddhartha Mukherjee, The Emperor of All Maladies
10 notes
·
View notes
Text
Sensory Loss in the Aged Psychology Take Home Exam Hearing loss that interferes with the ability to understand spoken language is a disability that creates difficulty in a variety of circumstances. A hearing deficit is especially serious for children as it may interfere with their ability to learn necessary life skills. For the adult hearing loss may interfere with their social life or with their ability to work and remain a contributing member of society. The extent of the hearing loss and the degree to which it interferes with a person's ability to work determine which measures may be appropriate and in which circumstances. The ultimate goal of hearing loss treatment is to improve the person's ability to function in life. The improvement in their quality of life must justify the cost. The following will explore the different treatment options available and when their use may justify the cost. The following will examine several cases of hearing loss and discuss appropriate interventions in each case. Hearing Loss as a Result of Ageing There are many causes of hearing loss as we grow older. Some of these factors include exposure to noise. A loud sudden noise can cause hearing loss, as can long-term exposure to slightly elevated levels of noise. Damage to the tiny hair cells in the cochlea is known as sensorineural hearing loss (RNID, 2003). This type of damage can be caused by certain diseases such as mumps, measles, rubella, Multiple sclerosis and Meniere's disease (RNID, 2003). Exposure to certain drugs can also damage these structures including aspirin, quinine, streptomycin and gentamicin (RNID, 2003). Damage of this type can be sudden or gradual. Some types of gradual hearing loss are genetic. Regardless of the cause, the treatment of this type of hearing loss is highly dependent upon the amount of loss of quality of life that it causes. Obviously, it the hearing loss affects job or career then this would be considered more important than for someone that is only affected in social situations that occur a few times a year. Hearing aids are often the first treatment option, particularly in cases of mild to moderate hearing loss. In some cases, such as where the loss is significant and causes a considerable impairment in the person's life cochlear implants may be a permanent answer. In hearing loss where the cochlea has been damaged to the point where they no longer transmit sound, a prosthetic implant may be the answer. This device bypasses the cochlea and directly stimulates the auditory nerve via a series of tiny electrodes. This surgery should only be considered for those that have a severe or total hearing loss because the procedure destroys any remaining hair cells, which causes any useful hearing that the person had before the surgery to be lost (V.M. Bloedel Hearing Research Center Website). A hearing aid is the best alternative for those that do not have a complete or near complete loss. Those who became deaf after they learned to speak and those that receive a cochlear implant soon after becoming deaf receive the greatest benefits from surgery (V.M. Bloedel Hearing Research Center Website). In a study regarding quality-of-life regarding Cochlear implants vs. hearing aids, it was found that Cochlear implant users demonstrated twice the quality of life improvement as hearing-aid users. Users were found to benefit the physical, psychological and social realms for those that had received cochlear implants (Cohen & Haynes, 2004). However, the patient must be aware that they may not be able to participate in certain activities such as swimming or taking a sauna as this may damage the device (Arabi, 2004). Question of Cost As with all types of medical decisions the benefit to the patient is the ultimate concern. However, this must also be weighed with the financial impact. The benefits of the procedure may not always outweigh the costs in some cases. According to the Hearing Aid Price Guide (2006) there are over 8 different manufacturers of different devices. Prices range from around $1,500 to $2,500 dollars, depending on the manufacturer and type. A hearing aid need replaced every 5-7 years, depending on care (Earinfo, 2006). This means that the earlier a person gets a hearing aid, the more it will costs over their lifetime. For a twenty-year-old, it may be cheaper over the person's lifetime to opt for a cochlear implant. A cochlear implant has an average cost of $19, 745. Medicaid typically only pays $14,000, sometimes as low as $3,000 (Cochlear.org, 2006a). Costs can soar upwards of $60,000 depending on circumstances (Cochlear.org, 2006b).Various signal processors in the devices are responsible for different outcomes for patients (Spahr and Dorman, 2004). Summerfield and associates (2002) found that quality of life measured in unit costs was greater in unilateral, rather than bilateral cochlear implants. The question of whether insurance should pay for hearing aids is a topic of considerable debate. The current standpoint on funding for hearing loss appear to be the same whether one requests funding for a hearing aid or a cochlear implant. There is little difference in the outcome between Medicare, Medicaid, or private insurance (Listen-up-org). The reasoning for this is that hearing loss is an inconvenience, but it not considered to pose any real threat to the person. It can be argued that the societal costs for either a hearing aid or a cochlear implant are offset by the productivity of the person in the workforce. Insurance should pay for either device as is determined to be appropriate by the physician. Hair Regeneration new technique for restoring hearing has recently begun to be explored. Hair cell regeneration is the latest technique to be explored for a possible solution in cochlear hair loss. At the current time the technique has only been tried on mice (Bauman, 2004). Human cochlear hair regeneration is not as easy as it would at first seem. Researchers face many challenges in this process. The first is that the cochlea contains two types of cells, hair cells and supporting cells. When a hair cell dies the surviving support cell must receive the correct signals to be turned on (Bauman, 2004). Cell differentiation poses the greatest difficulty in the ability to regenerate human cochlear hairs. It is likely that at some time in the future researchers will unlock the mystery to how to regenerate highly specialized cells such as these. However, at the current time, they are not even close to being able to devise something that is even close to workable in a human being. There are many challenges including the problem that sometimes the new cells fail to work in guinea pigs (Pobojewsky, 2003). This research is not likely to be abandoned, but it will be many years into the future before if provides a viable alternative for humans suffering hearing loss. QUESTION 2. The sense of smell is often placed low on the list of importance when it comes to sensory loss. The senses of hearing and sight are often much higher in importance with a loss of sense of smell hardly gaining any attention. Loss of a sense of smell and its accompanying loss of a sense of taste are a common complaint among the elderly. However, this typically receives little attention from the medical community. A loss of the sense of smell can have an important impact on the lives of the elderly. The first effect that must be considered is the effect on the sense of taste. A majority of our sense of taste relies on the olfactory sense. When the sense of smell is reduced or gone, the person may report that food tastes bland. This may effect their appetite and be a culprit in unwanted weight loss (Mathey et al., 2001). Another problem associated with a loss of sense of smell is that the person may not be able to detect odors that indicate danger, such as the smell of natural gas (Cain and Stephens, 1986). A loss of smell was found to be problematic in a large portion of elderly people taking part in the recent study (Murphy et al., 2002). Reiter and Constanzo (2003) found that a loss of smell significantly decreases a person's quality of life. They pointed out several professions that depend on a sense of smell, such as a chef. Loss of a sense of smell could have as much of an impact on the ability of the person to function in daily life and to hold a career as the loss of any other sense, yet many do not see it that way. It is generally agreed among scholars and the medical profession that some loss of smell occurs as a natural part of the aging process (NIDCO, 2006). Exposure to chemicals can cause a loss of a sense of smell (NIDCO, 2006). Currently, there is no treatment for a loss of sense of smell. However, there are assistive devices available for those that may not smell natural gas (NIDCO). Vitamin deficiencies, malnutrition and diabetes are linked to a loss of smell (NIDCO). If an underlying condition is the cause of the loss, then the logical procedure would be to treat the underlying cause. In some cases the sense of smell may return and for others the loss will be permanent. Research supports the existence of changes in smell due to age. The causes of this loss are varied. There has not been considerable research into searching for a treatment as with other sensory declines. Loss of out sense of smell is not considered to be of greater consequence in our society. With the rare exception of those whose careers depend on it, there is little societal impact caused by a loss of sense of smell. For the person, they may not enjoy all of the things that they used to, but it does not carry any significant impairment with it. There has been no formal effort dedicated towards research to restore the sense of smell, exclusive of any underlying conditions. The loss of a sense of smell is considered to go along with certain diseases or physical abilities. The underlying condition for the loss is treated and the sense of smell may come back. However, a loss of sense of smell is not treated as a condition in itself, but is treated alongside another condition. A loss of sense of smell may mean placing the person in danger and may place them at greater risks for certain hazards, but in general, this is not considered to be something that cannot be overcome with assistive devices. Works Cited Arabi, A. (2004) Cochlear Implants: My Perspective. Term Paper. NBB421 - Effects of Aging on Sensory and Perceptual Systems. Professor Halpern. Friday, December 3, 2004. Cornell University, Ithaca, NY. Bauman, N. (2004) Hair Cell Regeneration -- Overcoming the Challenges. Center For Hearing Loss Help. November 2004. http://www.hearinglosshelp.com/articles/haircellchallenge.htm. Accessed December 15, 2006. Cain, W., Stevens, J. (1989) Uniformity of olfactory loss in aging. Ann. N.Y. Acad. Sci. 561, 29-38. Cochlear Implants. The Virginia Merrill Bloedel Hearing Research Center at the Cochlear.org (2006a) Total Costs for the Procedure. http://www.cochlear.org/sys-tmpl/cochlearimplantcosts/. Accessed December 15, 2006. Cochlear.org (2006b) Cost Effectiveness. http://www.cochlear.org/sys-tmpl/costeffectiveness/. Accessed December 15, 2006. Cohen, S.M., Haynes, D.S. (2004). Quality of life in hearing-impaired adults: The role of cochlear implants and hearing aids. Otolaryngology - Head and Neck Surgery. 131 (4): 413-422. Earinfo.com (2006). Will My Hearing Aids Eventually Need to be Replaced? http://www.earinfo.com/hearing-aids-replace.html. Accessed December 15, 2006. Hearing Planet (2006). Siemens. http://www.hearingplanet.com/Library/siemens-hearing-aids.html. Accessed December 15, 2006. Listen-Up.prg (2006). Sources of Hearing Aid and Cochlear Implant Funding. http://www.listen-up.org/haidfund.htm#ins. Accessed December 15, 2006. Mathey, M., Siebelink, E., de Graaf, C., van Staveren, W. (2001) Flavor enhancement of food improves dietary intake and nutritional status of elderly nursing home residents. J. Gerontol. A Biol. Sci. Med. Sci. 56, M200-M205 Murphy, C., Schubert, C., Cruickshanks, K., Klein, B., Klein, and Nondahl, D. (2002). Prevalence of olfactory impairment in older adults. JAMA 288, 2307-2312. National Institute on Deafness and Other Communication Disorders. (NIDCO) (2006). http://www.nidcd.nih.gov/health/smelltaste/smell.asp. Accessed December 15, 2006. Pobojewski, S. 2003. Gene Therapy Grows New Auditory Hair Cells in Mammals. Phoenix Rising. http://www.phoenixrising.ca/detail.asp?ArtID=79.p. 1. Rawson, N. (2006). Olfactory Loss in Aging. Sci. Aging Knowl. Environ., February 2006. 2006 (5); 6, 8 Reiter, E. And Constanzo, R. (2003).The Overlooked Impact of Olfactory Loss: Safety, Quality of Life and Disability Issues. December 2003. 6 (1): 1-7. RNID. (2003). Hearing Loss. http://hcd2.bupa.co.uk/fact_sheets/Mosby_factsheets/Hearing_Loss.html. Accessed December 15, 2006. Spahr, A., and Dorman, M. (2004) Performance of Subjects Fit With the Advanced Bionics CII and Nucleus 3G Cochlear Implant Devices. Arch Otolaryngol Head Neck Surg. 2004;130:624-628. Summerfield, A., Marshall, D., Barton, G., and Bloor, K. (2002). A Cost-Utility Scenario Analysis of Bilateral Cochlear Implantation Arch Otolaryngol Head Neck Surg, Nov 2002; 128: 1255-1262. http://depts.washington.edu/hearing/CochlearImplant.html. Accessed December 15, 2006. Read the full article
0 notes