#pyelolithotomy
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs




Fun Fact
If you dial 1-866-584-6757, you can leave an audio post for your followers.
Text
Right laparoscopic pyeloplasty with pyelolithotomy
Source
1 note
·
View note
Text
Revisions for Reporting Nephrolithotomy & Pyelolithotomy (CPT code 50080, 50081)
Some important changes were made to two existing urinary system procedural codes (CPT code 50080, 50081) for the CPT 2023 code set. The changes involved updating many terms commonly used in the past for urinary procedures that no longer reflect current clinical practice and resulted in new introductory guidelines, code descriptor revisions, and new parenthetical … Read more Revisions for…
View On WordPress
0 notes
Text
Laparoscopic Kidney Stone Removal Surgery By Dr. Mayur Dalvi
Kidney stones are a common urological problem affecting millions of people worldwide. While small stones can pass through the urinary tract without any intervention, larger stones may require surgical removal. One of the most effective and least invasive procedures for removing kidney stones is laparoscopic kidney stone removal surgery. In this Blog, we will discuss everything you need to know about laparoscopic kidney stone removal surgery with inputs from Dr. Mayur Dalvi, a leading urologist with extensive experience in this field.
What is Laparoscopic Kidney Stone Removal Surgery ?
The procedure of laparoscopic pyelolithotomy, also known as laparoscopic kidney stone removal surgery, is used to remove kidney stones that are too large to pass through the urinary tract. This procedure involves making small incisions in the abdomen and using a laparoscope to view and remove the stones from the kidney.
When is Laparoscopic Kidney Stone Removal Surgery Recommended ?
Laparoscopic kidney stone removal surgery is recommended for patients with larger kidney stones (more than 2 cm) that cannot be removed through non-surgical means, such as shock wave lithotripsy or ureteroscopy. This procedure is also recommended for patients with anatomical abnormalities or other conditions that make other surgical options risky.
How is Laparoscopic Kidney Stone Removal Surgery Performed ?
Laparoscopic kidney stone removal surgery is performed under general anesthesia. The procedure involves the following steps:
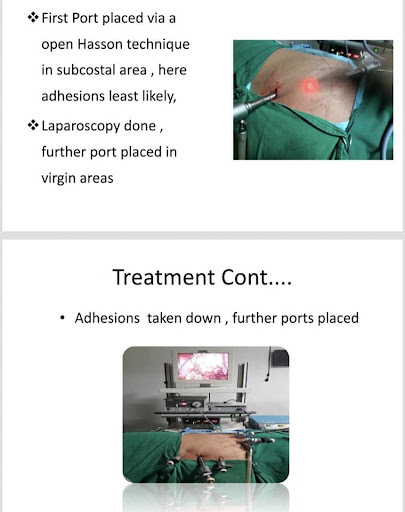
Making small incisions: The surgeon makes several small incisions (usually 3-4) in the abdomen, each measuring less than 1 cm.
Inserting the laparoscope: A laparoscope, a thin, flexible tube with a camera, is inserted through one of the incisions. The camera transmits images to a monitor, allowing the surgeon to view the kidney.
Removing the stone: The surgeon uses specialized instruments, such as graspers and scissors, to locate and remove the stone from the kidney remove larger stones, the surgeon may need to make an additional incision in some cases. Closing the incisions: Once the stone is removed, the surgeon closes the incisions with sutures or surgical glue.
What are the Advantages of Laparoscopic Kidney Stone Removal Surgery ?
Laparoscopic kidney stone removal surgery has several advantages over traditional open surgery, including:
Minimally invasive: This procedure involves making small incisions, which results in less pain, scarring, and a shorter recovery time.
Shorter hospital stays: Most patients are able to leave the hospital within 1-2 days after the procedure.
Reduced risk of complications: The risk of complications, such as bleeding, infection, and injury to surrounding organs, is lower with laparoscopic surgery compared to open surgery.
Higher success rates: Laparoscopic kidney stone removal surgery has a higher success rate than non-surgical treatments for larger kidney stones.
What is the Recovery Process Like After Laparoscopic Kidney Stone Removal Surgery?
The recovery process after laparoscopic kidney stone removal surgery varies depending on the patient's overall health and the size of the kidney stone removed. Most patients can expect to resume normal activities within 2-3 weeks after the procedure. However, strenuous activities and heavy lifting should be avoided for at least 2-3 weeks to allow the incisions to heal properly. Your surgeon may also prescribe pain medication and antibiotics to manage pain and prevent infection.
Summary
For patients with larger kidney stones that cannot be removed non-surgically, laparoscopic kidney stone removal surgery is a safe and effective option. Dr. Mayur Dalvi, a renowned urologist with extensive experience in laparoscopic kidney stone removal surgery, is a recommended doctor for patients seeking this operation
#laparoscopic kidney stone removal surgery#kidney stones#urology#minimally invasive surgery#surgical procedure#laparoscopy#pyelolithotomy#non-surgical treatment#open surgery#recovery process#Dr. Mayur Dalvi
0 notes
Text
Kidney Stone Specialist
A kidney stone specialist is involved in the diagnosis and treatment of kidney stones. Depending on the case, the kidney stone specialist may recommend selecting one of four different surgeries. A non-invasive extracorporeal shock wave lithotripsy (ESWL) involves using sound waves to break up the kidney stones into smaller pieces so that they can pass through the bladder. Percutaneous nephrolithotomy (PCNL) is a process of inserting a tube into the patient’s back to remove or break up large kidney stones.

A kidney stone specialist may also recommend a ureteroscopy (URS), a procedure that involves passing a fiber optic camera into the ureter and kidney to remove or break up the stones. The final procedure to treat kidney stones is a pyelolithotomy, which involves removing a stone from within the renal pelvis or from the ureter.
2 notes
·
View notes
Text
Kidney Stone Center
A kidney stone center provides treatment and care to individuals suffering from kidney stones, a common disorder of the urinary tract. A few treatment options typically performed by health practitioners at a kidney stone center include a non-invasive extracorporeal shock wave lithotripsy (ESWL), percutaneous nephrolithotomy (PCNL), ureteroscopy (URS) and pyelolithotomy.
Each of these procedures takes a different approach to breaking up and or removing the kidney stone. Patients with kidney stones may also be prescribed alpha-blockers, a type of medication that works to relax the muscles in the ureter and help pass the kidney stones. Visit a kidney the stone center today for specialized treatment.
1 note
·
View note
Photo

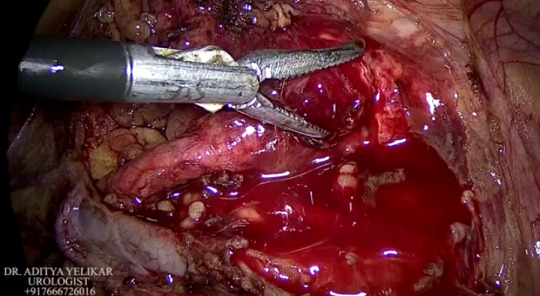
Long standing neglected stones can make your kidneys non functional. Presenting one such case which we managed laparoscopically. He had a past history of pyelolithotomy on the same side. Dr.Soumyan Dey is the best doctor for Laparoscopic nephrectomy surgery. He performs the surgery successfully.
0 notes
Text
Lupine Publishers | Lasertripsy For the Controlled Coarse Fragmentation of Urinary Tract Stones
Lupine Publishers | JOURNAL OF UROLOGY & NEPHROLOGY STUDIES
Abstract
Development of novel methods for controlled coarse fragmentation of urinary tract stones may help to minimise the risk of urinary tract infection and prevent the small stone fragments, responsible for residual stone formation, from entering into the calyxcalcification system of a kidney. The experimental results demonstrated that the following parameters of a pulsed laser operating at the 2097 nm (or the 1967 nm) wavelength were optimal for a controlled fractioning of the stones in air: the pulse duration of 20-30 ns, the repetition rate of 200-1000 Hz (or more), and pulse energy of 45-55 mJ. The relatively small pulse energy coupled with the high repetition rate enabled the destruction of concrements into fragments small enough to be removed with the amplatz.
Keywords:Lithotripsy, Urolithiasis, Lasers
Introduction
Decades of endoscopic surgery of urolithiasis using fine fragmentation of stones have revealed its deficiencies, one of which is the complication of contact laser lithotripsy - the development of an infectious inflammatory process in kidneys due to bacterial dissemination of flora from stone biofilms [1]. Importantly, even in the case of sterile urine, some microorganisms were found in the urinary tract stones in 25% to 41% of all cases according to published reports [2,3]. The problem of the development of complications in the endoscopic treatment of urolithiasis, coupled with increased antibiotic resistance, is becoming more urgent. The search for new methods for controlled coarse fragmentation of stones will minimize the risk of possible infection and help to prevent the loss of small fragments of stones in the calyxcalcification system of a kidney, which were found to be responsible for residual stone formation.
Purpose
Search for the regime of laser lithotripsy that will ensure effective fragmentation of the urinary calculi and at the same time avoid their uncontrolled finely fragmented fracture.
Materials and Methods
The effect of a laser crushing of 25 urinary tract stones ex vivo was studied. The used stones are crushed after nephrolitho extraction and pyelolithotomy, nephrectomy. In the experiment, only undistracted (entirely extracted) stones were examined, which were placed in physiological saline until the moment of the laser action. A Ho3+:YAG laser pumped by a Tm3+ fiber laser was used in the first experiments. The Ho3+:YAG laser operated in a pulsed regime at the 2097 nm wavelength and the 20-40 ns pulse duration. The Ho3+:YAG pulse repetition rate was varied from 0.2 to 40 kHz, while the pulse energy changed within 0.5-55 mJ at the average output power of up to 35 W. In the second experiments, another pump laser based on Tm3+-doped Lu2O3 ceramic at 1967 nm wavelength was in turn pumped by a Raman-shifted Er3+ fiber laser at the 1670 nm wavelength. The pulsed Tm3+:Lu2O3 laser had a pulse duration of 30-40 ns and the pulse frequency of 14-25 kHz. It operated with the average output power from 100 mW to 10 W. Both Ho3+:YAG and Tm3+:Lu2O3 lasers were manufactured at the IAPRAS (Nizhny Novgorod) [4,5]. The efficiency of the laser stone interaction was estimated by measuring the time required for stone perforation. The created stone channel was inspected visually and by using transmitted light microscopy (Figure 1).
Figure 1: Results of Ho3+:YAG laser irradiation of the urinary tract stones; A - stone fracturing along the fault line (indicated by an arrow); B - fragments of a stone; C – examination of the perforated stones using transmitted light microscopy (10× lens, 10× eyepiece).
Technique of the Experiment
The stones were removed from the normal saline (0.9% NaCl) and placed on an optical table. The Ho3+:YAG laser beam (or the Tm3+:Lu2O3 laser beam) was focused into the stone using lenses with the effective focal length from 21 mm to 200 mm (the estimated laser beam diameter on a stone changed from 0.1 to 1 mm, measured at the e-2 intensity level). The time required for complete stone perforation or stone fracturing along the fault line was measured. The inspection of the received stone channel was performed visually and by using transmitted light microscopy (Leica DMLS microscope, 10× lens, 10× eyepiece).
Results
The diameter of the stones used in experiments was 8 to 20 mm. Their microstructural density of the stones was from 161 to 1933 HU. The perforation time was measured from 2 to 300 seconds depending on the stone density, spatial dimensions, and chemical composition. The success rate of stone fracturing using the Ho3+:YAG laser at 2097 nm with the 10 kHz and 30 kHz pulse repetition rate and 0.17-2.3 mJ pulse energy was 89% (8 out of 9 attempts were successful). The microstructural density of these stones was from 161 HU up to 1566 HU.
The success rate of stone fracturing using the Tm3+:Lu2O3 laser at 1967 nm with the 15 kHz frequency and 0.4-0.6 mJ pulse energy was 43% (3 out of 7 attempts were successful). The microstructural density of the stones in this set of experiments was from 401 HU up to 1933 HU. A series of experiments revealed that the optimal operation mode of the 2097 nm Ho3+:YAG laser for controlled fracturing of urinary tract stones (in air) was a pulsed regime with the repetition rate of 200 to 1000 Hz (or more), pulse duration of 20-30 ns, and pulse energy of 45-55 mJ. In other words, the laser regime with a relatively small pulse energy (a few tens of mJ), but a high repetition rate (hundreds of hertz - kilohertz), enabled coarse fragmentation of concrements into fragments small enough to be removed with the amplatz
Conclusion
Prevention of kidney infections after the nephrolithotrypsy procedure can be ensured by a controlled, laser-enabled coarse fragmentation of urinary tract stones. This method allows to avoid scattering of the contents of the stones in a renal cavity system by selecting the laser regime optimal for contact lithotripsy. In the case of a pulsed Ho3+:YAG laser operated at the 2097 nm wavelength with the pulse energy of 2-55 mJ, pulse duration of 20-40 ns, and pulse repetition rate of 0.2-1 kHz (or more), the urinary tract stones were efficiently fragmented into pieces small enough to be removed from the kidney by percutaneous puncture nephrolithoextraction which, in turn, allowed to prevent infectious and inflammatory processes in kidneys due to minimal microbial dissemination of tissues.
Acknowledgments
This work was supported in part by the Russian Foundation for Basic Research (grant №16-07-00655)
Follow on Linkedin : https://www.linkedin.com/company/lupinepublishers Follow on Twitter : https://twitter.com/lupine_online
0 notes
Text
Juniper Publishers- International Journal of Nephrology: Endourological Management of Forgotten Double J Ureteral Stents: A Single Centre Study
Background: Double J (DJ) ureteral stent is being used in various urological and non-urological procedures. Indications for double J ureteric stents includes; to negotiate the obstruction and maintain adequate drainage from kidneys, help in localization and prevention of ureteral injuries during various gynecological and general surgical procedures and as an adjunctive procedure to extra corporeal shock wave lithotripsy (ESWL). A forgotten DJ stent is not uncommon in developing countries and is particularly seen in patients with poor socioeconomic status. These patients present with flank pain, hematuria, irritative voiding lower urinary tract symptoms (LUTS) and even lend up with features of renal failure. Management of forgotten DJ ureteral stents is not only important for patient's perspective but also for the surgeon's prospect due to its medico-legal implications.
Methods: Retrospective data search from 2008-2015 revealed 47 patients admitted with forgotten ureteral stent includes (broken and encrusted) were managed endoscopically. Patients were evaluated with X-ray, ultrasonography of Kidney ureter and bladder region (KUB), intravenous urography (IVU) and non-contrast computed tomography, renal function test (where indicated). Endourological procedure for DJ stent removal was decided according to the location of stents.
Results: A total of 47 patients (males: 34, females: 13) were included in the study. The mean age of patients was 23.53 years (range 4-65 years), mean duration of stent insertion was 39 months (4-68 months). Fifteen patients (31.9%) had stent insertion following percutaneous nephrolithotomy, 8 (16.96%) following ureteroscopic lithotripsy (URSL), 3 (6.3%) following pyeloplasty, 10 (21.2%) following ureterolithotomy, 6 (12.72%) following pyelolithotomy and 3 (6.3%) following ureteric re-implantation. Two patients (4.2%) had DJ insertion for bilateral upper ureteric calculus with deranged renal function.
Conclusion: Forgotten double J ureteral stent still a common and preventable complication in developing nations, patients may lend up in renal failure. Its removal is a challenging task.
0 notes