#ovum 10
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Mobile Tumblr US users spend an average of 4.04 minutes per session on the app.
Text
The Frog and the Infant/Just a Side
Author’s Notes: Angst! No idea if there’ll be comfort later! (But this is Epic & SaSi, so you knew that lol)
Warnings: Unreality/internal inconsistency/other shenanigans?
ping list: @randomnerd737
“Alright, my brothers, listen closely: Tonight we find a way to stay. 10 years of war killing us slowly, but now we’ll all be on our way!
Janus burst into the darkly-lit room, a shaft of moonlight illuminating the half-blackened tree growing in its center. He stumbled to a halt, blinking and slightly lowing his sword, unsure how he was supposed to fight a tree plume of smoke. Or what it was doing in this walled garden child's room.
Janus put down his sword staff and stepped closer to the smoke infant.
Creativity looked up to him and smiled.
“What sort of imminent threat does he pose, That I cannot avoid?” “He’s the ovum of none other than, Your very own Prince and Duke, Know that he will grow from a boy to a ruler, One fueled by rage, as he grows up in age, If you don’t split him now, you’ll have no-one left to save!”
Janus hated dreams. Specifically, he hated dreams that felt real, but that he knew weren’t.
He’s the best liar in the Thomasphere, thank you very much - But sometimes, especially when Thomas was sick, Janus swore the Subconscious liked to challenge him on that.
And when Thomas was dreaming, while sick? Forget about it.
He’d speculated about it with Remus, who’d rattled off something about lucid dreams, self-awareness, self-care, and paracausality, before veering off to tell Janus a “fun fact” about sea monsters on old maps.
Remus… The “other” Creativity.
Named, by his own brother, one of the “Dark Sides.”
The Others.
“I could raise him as my own!” “You know they will not condone,” “I’ll send him far away from home!” “He’ll find you wherever you go,” “Make sure that he’s never alone!” “The world will make him known,”
Janus picked Creativity off the tree out of the cradle, and held him close.
He knew - Oh, he knew - that not splitting Creativity would be their downfall. They couldn’t survive if he hadn’t didn’t. Had he?
He had to do it. For Thomas, he would do it.
“Your bridges will burn, that’s something you won’t lose. All you can choose is whose.”
But… he hadn’t, had he?
No, no… That’s not right - No! No! No!
This damned place!
He hated songs dreams. They sucked you in, had you believing the most emotional nonsensical things.
He’d rather hold the strings, thank you.
He wouldn’t let him the Subconscious do this.
“You’re as old as he was, When I had to start…”
They’d been so young, when…
Janus looked down, as Creativity grabbed onto his shirt with a small hand, and his heart…
Oh, his heart.
He couldn’t do this! He knew this would haunt had haunted him. Would had this been worth the pain?
But he would pay the price… and Thomas would could never know.
Janus took a bit of ribbon from his helmet, and tied it over the Infant’s eyes.
He pressed a kiss to Creativity’s forehead, and set him down on the floor.
He grabbed his sword, held it up with both hands…
And planted his staff next to Creativity, stuck firmly in the damp garden earth.
Janus turned away - He didn’t want this.
Janus leaned his staff up against the tree.
He didn’t want this.
Janus turned away from the tree cradle, and picked up the Infant.
He didn’t want this.
Janus wrapped him in a blanket.
He didn’t want this.
Janus carried the Infant out towards the garden wall balcony.
He didn’t want this.
Janus held the package out over the wall.
He had to keep Thomas safe.
Janus didn’t want this.
“…Forgive me.”
#sanders sides#janus sanders#epic the musical#(sort of) crossover#unreality#<- tagging just in case#neon’s writing#the frog and the infant
11 notes
·
View notes
Text

The legal and health effects of Dobbs
Two years ago, the reactionary majority on the Supreme Court did something that no other cohort of justices had done in the history of our nation: It extinguished an existing constitutional right. In a single decision, it denied women equal protection under the Constitution and demoted them to a subservient status with fewer rights than a fertilized ovum.
It is difficult to measure health effects for large populations in a short period of time. Still, the emerging evidence is that Dobbs is increasing the number of risky and dangerous pregnancies, resulting in increased infant and maternal mortality. Predictably, the most extreme effects are felt by women of color and women who live near or below the poverty line.
A study published in Journal of the American Medical Association (JAMA) examined the health effects of Texas’ 2021 ban on abortion. See JAMA Pediatrics, Infant Deaths After Texas’ 2021 Ban on Abortion in Early Pregnancy.
The finding of the JAMA investigation was that “recorded infant deaths in Texas and 28 comparison states found that the Texas abortion ban was associated with unexpected increases in infant and neonatal mortality in 2022.” Moreover, the results show that Texas experienced a “12.9% increase [in infant mortality], whereas the rest of the US experienced a comparatively lower 1.8% increase.”
The state abortion bans post-Dobbs are also affecting maternal health. Again, the relatively short time since Dobbs makes it difficult to conduct studies, but statistical modeling predicts a significant increase in maternal mortality—with women of color and women living near or below the poverty line showing the greatest risk. See Nicole Narea’s excellent analysis in Vox, What two years without Roe looks like, in 8 charts.
I recommend Narea’s entire article to your attention. The article covers the legal and medical changes in abortion healthcare since Dobbs. The article also discusses efforts to create statistical models predicting maternal mortality in the absence of access to abortions:
So for now, the best information is based on statistical modeling. Researchers at the University of Colorado Boulder projected based on 2020 data on maternal outcomes that, if no abortions were performed nationally, there would be an overall 24 percent increase in maternal deaths after a year. Black mothers would see the biggest increase in mortality.
Finally, OBGYNs have said that their ability to provide reproductive care that meets the medical standard of care has been impacted:
In states where abortion is banned or restricted, for example, six in 10 OBGYNs say their decision-making autonomy has become worse since the Dobbs ruling.
The article also discusses the political dimensions of the post-Dobbs landscape. It repeats a common talking point promoted by (mostly) male political consultants who claim that abortion will not be a decisive factor in 2024. They are wrong—largely because they ignore actual results in 2022 and special elections post-Dobbs and instead rely on flawed polling.
For example, as reported in the Vox article, the survey question that prompts the dismissive attitude toward abortion is this: “What is the most important issue facing the country?” The answers are (in order of frequency of response), “Government,” Immigration,” Inflation,” and “Abortion.”
With all due respect (which is almost none), the question is so poorly phrased as to be meaningless—at least to the extent that it supposedly tests attitudes toward the importance of abortion. It asks about the most important issue “facing the country.” A sensible and reasonable answer to our national crisis is “government”—which encompasses the rule of law, democracy, the Supreme Court, voter suppression, and individual liberty, including reproductive rights. Saying that “government” is the most important issue facing the country does nothing to diminish the importance of reproductive liberty to the women and men affected by Dobbs.
Moreover, “Immigration” is a code word for “I am a MAGA voter.” If the designers of the survey couldn’t figure that out, they should find a new line of work.
And, of course, everyone is concerned about inflation—which is a surrogate for “I am not one of the top 2% that lives on investment returns.” In other words, it is everyone who works for a living saying that their daily economic struggle is the top issue facing America—which says nothing about the passion and anger that surrounds restrictions on reproductive liberty.
I am not a pollster, but I have met people, including women. And anyone who believes that abortion will not be a decisive factor in the 2024 election needs to look up from the spreadsheets and social media to engage with the tens of millions of women and men who are of childbearing age. They care deeply about reproductive liberty and are going to vote on that issue up and down the ballot. Don’t let any political consultant tell you otherwise!
Supreme Court grants review of state bans on gender affirming care
The Supreme Court granted review of Tennessee’s ban on gender affirming care. The grant of review is an ominous sign, as explained by Erin Reed in their Substack, Erin in the Morning, Supreme Court Takes Up Trans Care Ban In Tennessee, With Potentially Huge Impacts.
(Erin In The Morning is the leading source on Substack for news regarding legal developments regarding transgender rights. If you or someone you know is interested in or affected by such developments, I highly recommend the newsletter.)
Per Erin Reed,
On Monday morning, the Supreme Court announced it would take up whether gender-affirming care bans for transgender youth violate equal protection rights under the U.S. Constitution. The case under consideration involves the gender-affirming care ban in Tennessee, where the 6th Circuit Court of Appeals allowed the ban to take effect. The court ruled that transgender people do not have equal protection rights under the Constitution, citing the Dobbs decision overturning abortion and Geduldig v. Aiello, a ruling on pregnancy discrimination that has gained new traction in conservative courts targeting transgender individuals.
It cannot be said often enough: Transgender people are people. Period. They are entitled to the full protection of the Constitution and the laws of the US. But it appears that the Supreme Court is intent on repeating their travesty in Dobbs—creating a second-class citizenship status based on gender identification.
First Roe v. Wade, next transgender rights, then LGBTQ+ rights (including same-sex marriage), and then contraception. The reactionary majority is coming for it all. They are telling us as loudly and clearly as they can.
The Supreme Court is on the ballot in 2024—we must win both chambers of Congress and the presidency so we can expand the Court and release the death grip of the reactionary majority on the Constitution!
[Robert B. Hubbell Newsletter]
#women's rights#human rights#abortion ban#SCOTUS#Robert B. Hubbell#Robert B. Hubbell Newsletter#election 2024#reproductive rights#Roe v. Wade#Dobbs#legal and health effects of Dobbs
5 notes
·
View notes
Text
12 Days of Smuff: Day 10
Day 10: Bed sharing + accidental stimulation.
Robert Fischer (Inception) x Eva Smith
Cw: dry humping, mentions of a blighted ovum/miscarriage, angst, some smut


It had been a bad idea.
In a moment of vulnerability, Eva had asked him to stay with her and he had.
Robert had offered to stay in the guest room or sleep on the floor, but Eva had shaken her head and asked him to sleep with her.
There was too much history between them for this to work. He couldn’t forget her no matter how much he tried and she couldn’t move on because their last night together resulted in the worst case scenario.
Had anyone told him he’d be here holding her because they’d have to see a doctor for an embryo that didn’t form, Robert would’ve siced security on them.
But here he was holding his ex girlfriend who used him to keep her company above the water because tomorrow they’ll pretend nothing ever happened and go their separate ways.
“I was wondering where my pajamas went.” The Fischer Morrow heir comments as tried his best to remember they were over and the sex they had last week was merely a fluke.
“I had intended to give them back, but then I remembered you still have some of my panties and I thought they were worth about the same, in sentimental value at least.” The dark haired woman moved slightly as she got comfortable and he pretends he’s fine when her ass brushed against his dick.
“Sorry.” She said before moving away to prevent it from happening again, but it would once Eva fell asleep.
“Don’t apologize, remember when I was high on painkillers after my surgery?” Rob would be lying if he didn’t miss all those times they’d cuddle and end up fucking because the accidental stimulation was enough to drive him fucking insane.
So many times where she’d rub against him ---on purpose as well as in her sleep--- and he’d be waking up rock hard and wanting nothing more than to fuck her good morning.
But they can’t do that, because after tomorrow it is over for good.
Or so they’ve been telling themselves this past week.
“Oh, how could I? You were like a very horny puppy most of the week.” She answered bemused. She’d been on edge all evening, terrified about tomorrow even if the procedure was rather simple and the doctor the best in California.
It was good for her to regain her usual good humor. Even it drudge up memories that had the both of them wanting to regain what they lost.
He wanted to, but he had agreed to her terms because he didn’t want to push. She’d used him and she didn’t feel worthy of him, and Robert has disappointed his father enough to know he’s a fucking dumbass when comes to love.
“Six weeks without sex was a nightmare for you too, Evie.” Robert pointed out and fought the urge to thrust his hips seeking out her ass to rut against it like a horny teenager.
“I missed you.” Evie admits and does something worse than grinding against him, she seeks out his hand and holds it like she used to do when she was troubled.
“I missed you too.” Robert admits as he interlaced his fingers with hers and held her tightly.
“I know I said I didn’t want us to give us another try ,but ---” she stops herself fighting with the proud part of her that thinks she knows what’s best for the both of them.
“A do over would be nice. Once you’re recovered, if you need time to come around to it.” He doesn’t let her change her mind and once again considered not going to Sydney this week.
He didn’t need to think about it, he’s had plenty of time this week. Robert had wanted his pound of flesh that day at her office, but then he ended up looking forward to seeing her each evening. Even as ‘friends’ he couldn’t imagine a better person to share his life with.
“No dream sharing this time.” Eva sets a new boundary, one he doesn’t pretend to agree with…for now.
“Agreed.”
This time he is the one rubbing his growing erection against her ass and this time they don’t stop doing it. Between her presence and knowing there’s still hope for them, Robert can’t seem to get himself under control.
Never been good at self-control, anyways.
“Doctor didn’t say anything about not having sex before the procedure, you know.” She supplies as a sigh escapes her lips.
“We don’t have to do it, Evie.” He protests half embarrassed at their predicament. The other half of him is letting his ex girlfriend ---or just girlfriend since its inevitable that they’ll be getting back together by morning--- take his hand under her shirt and very obediently playing with her tits.
That time last week in the dining room had been a frantic fuck, of thinking that just one last time would be enough. Right now it was knowing that desire won’t go away and why the should they deny themselves something they desperately needed.
“What I wanted you to fuck me, Robert?” such a crude question she said as he slid his free hand past the waistband of her sleeping shorts. “What if I told you the mere knowledge of feeling you like this has me thinking about all those times we fucked until I couldn’t remember my own name?"
And she wasn’t lying, her pussy was wet and hot as his fingers toyed with it.
“Then I’d say your wish is my command.” His father was right in being disappointed with him, Robert could never live without Eva and this week had only proven it.
Robert’s hand leaves her chest and with ease he freed his aching cock from its confines as he entered her from behind with a groan.
No woman had been able to satisfy him like she did, and now he knows no one ever will.
He rocks against her, takes his time seeking ti make the night last as long as possible. Knowing Eva she may change her mind by the time the sun rose.
But for tonight, he is hers, she is his and nothing exists beyond the moment.
“Did you try to forget me like I did?” he asks thinking how she’d pretended not to care that his latest conquest had kept calling last week.
“No, didn’t want to.” She shook her head as he reminded her no other person could ever make feel like this.
They were made for each other, if such a thing existed. As if they had always been lifetimes ago.
He didn’t believe in soulmates, but she did.
“Then why fight it, why push me away, Evie?” he asks and clenched beautifully around his cock and Robert thanked his lucky stars there was no need for caution tonight.
“I don’t want to hurt you again.” The brunette answered as she lost herself to the pleasure.
As much as he wanted to make it last, it isn’t long before he takes her over the edge with him.
He doesn’t let go of her, not yet. “You won’t hurt me, I’m not as fragile as you think, sweetheart.”
3 notes
·
View notes
Text

I don’t know how I feeeeeeeeel I’m just jittery and unable to settleeeeeeeeeeee 26 hours of waiting to go bleh. liz & alex are househunting all morning and early afternoon. I need a project to distract myself but also I just kind of want to mindlessly scroll and let myself float in this weird bleh state of limbo. but let’s see how about this:
9-10:30 mindlessly scroll or maybe read fic
10:30-11:30 maybe walk the dogs and listen to a hockey podcast or idk maybe not or go for a short run or something idk
11:30-1 hang out with liz/alex on their break
1-2 shower/get ready
2-6ish hang out… maybe go to the lake… idk
6:30 dinner with everyone + my sister
watch the bear
blah blah that should kill the day and then tomorrow I’ll just have to kill time from like 6am to 10:30am 🫠🫠🫠
gonna talk out some stuff behind the cut
here are the possible outcomes tomorrow:
everything looks fine and my doctor confirms the pregnancy is still viable
doctor determines the pregnancy is ectopic and counsels taking meds to end things
doctor determines the pregnancy is located in the uterus but isn’t developing normally (blighted ovum or missed miscarriage or something else) and counsels a D&C or waiting to miscarry or further testing
doctor can’t make a determination and schedules me for further bloodwork and/or ultrasounds once I’m further along
I decided I wanted to go on my own because I don’t want to feel responsible for managing or responding to someone else’s reaction on top of my own… if it’s bad news I want time to process it by myself before I have to talk to anybody. I am going to walk to the appt tomorrow morning and if it’s bad news I’ll probably want to go on a long walk around the neighborhood to be by myself with my feelings for a while. liz and alex have a couple other viewings scheduled shortly after so I can just wander around till they leave and then go back to the house to be alone for an hour or two. there was a period of time earlier in the week where I thought I wouldn’t get too upset again because I did so much pre-grieving last week when I got the first results back and I felt kinda hollowed out by that, but unfortunately five days of renewed hope and hopeful planning has kinda erased all that pre-grieving and now I think I’ll just be really, really sad again. like I’m already crying about it now and we’re still 26 hours out from any new information. I just want this baby to make it! I just want this to be it! but I know there’s a decent chance things won’t work out. I’m seven weeks tomorrow and still so very firmly in “it’s way too early // the risk of things not working out is still way too high” territory. I just wish I could fast forward to tomorrow morning. it feels like the first IUI cycle where I hadn’t yet accustomed myself to waiting or learned how to stop calendar watching and so every single second just seemed to drag by impossibly slowly. aghhhhhh okay. I just feel like I would feel more if I was really pregnant instead of just intermittently queasy and irritable. but I felt exactly like this last weekend when I was convinced my symptoms were gone and it turned out my HCG levels were busy tripling in that time. so idk idk. just want this day to PASS
7 notes
·
View notes
Text
Rimilda, Bastard Daughter of all Great Ones: [ageless]
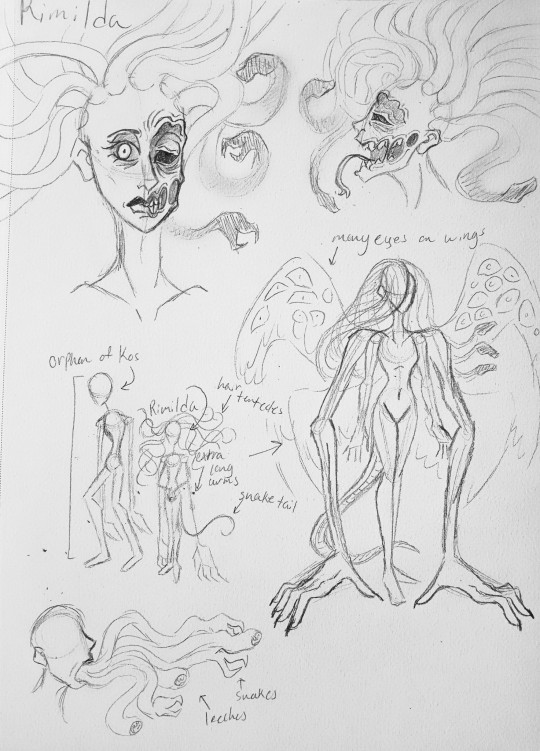
"All sounds range in tone, yet silence rings the loudest... Child of many, yet child of none... Bastardized child of a wedlock marriage, born into the world by empty womb... Birth by the blood of the limitless mother of all and her harem of souls... Parasite of the eggs of a whore, a holy nun, and an undead queen who lost her young to creatures untold... Fed by the blood of all cursed creatures of the night... Bonded to the blood of all Great Ones... Wrapped in the silver silk of arachnids... Fall, fall, fall into the arms of your mother, young Guardian of Yharham... Bare the face only They could love, with three pairs of wings to soar and quadruple the arms to wield your blades... And forever protect your name, O' Great One Rimilda."
Dissonantia— disguised as a hunter with a sickle + chain whip as her merge weapon, wearing a victorian era metal alicorn mask (like how Elise the Crow wears a bird mask) that has a curved horn, empty eye sockets and nostrils, and it's mouth is agape so Dissonantia can breathe out fire— created an "embryo" made out of her blood and the DNA of all of her spouses, the ovums of a whore (Adriana), a nun (Adelle), and a queen (Yharham), the blood of the drunken (almost every "normal" enemy in the game), a drop of blood from every Great One, and protected by the spiders' silk to form an artificial womb.
Rimilda was born similar to a butterfly, crawling up the side of the cocoon and slowly stretching and spreading out her feathered wings after ripping out of the spider webbing at the bottom, the fluids from her artificial womb pouring out.
Her face similar to Twisted Alice Angel from BATIM and BATDR, with the deformed side of her face covered with eyes and blemishes. Her right eye is a pale blue with a visible pupil, while her left eye is slightly swollen and completely black.
She has a forked tongue that acts similar to reptilian tongues.
Her body shape is slim and petite, half as tall as the Orphan of Kos. She has the same skin tone as him.
She thinks of him as an older brother figure.
She is mute most of the time, only talking to those who are worth her time.
She has six wings similar to Mergo's Wet Nurse, but with many shiny black eyes on them.
She has four arms, with the upper ones stretched out adorned with larger hands.
She has a serpent tail similar to the Godskins from Elden Ring.
Slimy purple snakes and black leech-like tendrils can come out of her mouth during a five-second grapple attack, biting the player and taking their health by 10 points.
She can be heard humming the Winter Lanterns' song from time to time.
She can form a blood whip by using her old umbilical cord that's attached to a bloody spiked morningstar. (Link)
She was given an unbreakable lanternflail. (Link)
She is constantly hungry, and often snacks on dead corpses to avoid eating the living if there isn't actual food nearby.
Her hair is made out of Kos's hair tentacles that slowly turn into black snakes at the tips. (Link)
She can become a giant hydra dragon (search up "false hydra") when "defeated" for the first round of a battle. (Link)
#oc#original character#cyan#open to rp#tw gore#bloodborne#blood bending#blood bending dnd#orphan of kos#great ones#eldritch gods#eldritch horror#eldritch#tw snakes#tw eyes#Bloodborne oc
4 notes
·
View notes
Text
《Mighty Shine》入荷情報。10/24
おはようございます。
Mighty Shine(2024秋冬)より、新作のワッチロールが入荷です。
トレンドな、ショートタイプのロールワッチです。
《Mighty Shine》ROLL WATCH 2
ブラック・ブラウン・ネイビー・グレー色/5,280円(税込)





商品詳細は、店頭・オンラインストアでご確認ください。
Mighty Shine(商品一覧)
取扱店舗:OVUM
0 notes
Text
(June 2023) Δ O-01 Shellbreaker and Δ E-10 Rooster





Note that the above images aren't in their original order, so things might seem a bit off in the post bodies under the cut. (Also I think I didn't upload that first one originally?)
Warning, very long:
Still a bit of a work in progress, but since I didn't have the wherewithal to draw any people tonight (but still had the urge to draw), I figured I'd take a shot at refining the design for Dr. Jos's mech. I was going for something a bit egg-y in shape, but the end result wound up a bit... Devil robot-y? I dunno, maybe I'll call it the Deviled Egg or something. (I am mostly joking)
Transcript:
Jos's mech
something "egg" themed?
looks kinda like a Devil robot...
[small drawing of the Yellow Devil] bumo bumo~
skates like Volnutt or L-Gaim (or Bowser...) (next to the mech sliding forward on hover-skate feet)
(rough scale) (by a small, crude drawing of Jos next to the mech)
three-digit claw (or not? maybe proper hand?)
rocket for jumps (pointing to a large booster on its back)
coolant? fuel? (pointing to the lower half of its gun arm)
jets for skating? (pointing to a row of small jets on its ankles)
Fun fact, this mech is based on an old Lego mech I made back in 2010 or so, in middle school (which was contemporary with sorXa's previous iteration):

The pilot wasn't really anyone in particular, just some generic mech pilot I cobbled together to match the vibe of the mech itself.
---
Finally named Jos's mech, and hashed out a mech for sorXa as well (which I don't think she'd use much, but she did have one in her previous iteration)!
For the Shellbreaker, I think I'm sticking with the talons - there's something about the look of them I really like, even if they're not 100% practical for everything it might need them for (like manipulating objects). I'm also not sure how I feel about it having a sword - I like the idea of it being a sort of "shock troop" mech, in which case being more heavily equipped would make sense, but on the other hand I view energy blades as more sorXa's thing than Jos's. Its previous iteration did have a chainsaw, but that doesn't really suit my tastes at the moment. The "Δ" is going to be associated with the name of the organization they belong to, I think, and the O is for "Ovum-class" (not officially classed for the same reasons that Jos isn't an officially licensed pilot or legally a doctor - bit hard to get official certifications if you're an outlaw).
The Rooster is actually based on sorXa's old Lego mech, which I still have a version of (see below), and uses its old alphanumeric designation (Δ E-10). It was originally a fair bit larger than it is now, but I shrank it down since using a mech isn't sorXa's primary thing, so I figure it'd be better for her to have a mass-produced lightweight mech commandeered from the enemy instead of something bespoke and heavy-duty like Jos. The "E" is for "Egret-class", a type of mech widely used for its good mobility in urban environments. Its long legs make it adept at wading through streets, and its light weight and thrusters help it leap over or onto short buildings, overpasses, and other otherwise difficult-to-navigate vertical obstacles. Its Gatling cannon only has three barrels, in line with its overall lower offensive capabilities compared to other classes. (Post-hoc note: I don't know what I was on about, I'm pretty sure that's not how Gatling cannons work)
Transcripts below:
Jos's mech concepts Δ O-1 "Shellbreaker" (note: I forgot a 0 here when writing it originally, though arguably it's unnecessary for a unique mech that will never have 10 or more units produced)
wheel shape (sic) cockpit (next to diagrams of how the cockpit fits into the mech; imagine one of those mouse wheels that has horizontal scrolling, kinda)
Δ E-10 "Rooster"
light frame, high mobility (esp. vertical) ~11'8" / ~3.5m (height of mech) 6'3" / 190 cm (height of sorXa) (approx. scale)
see Shellbreaker for sword details (next to the Rooster holding an inactive beam sword)
comes out of wrist? (like L-Gaim) (next to a very rough diagram of how said beam sword would be stored in its forearm, and then guided out into its hand, with a cable running back into its wrist for power)
Here're some images of what the Rooster used to look like, ca. 2010 and... I dunno, 2015 or so maybe? (so late middle school and mid-to-late high school), respectively:


Post-hoc addendum: You can also see what sorXa's previous iteration looked like here :^)
#mech#mecha#mech design#mecha design#concept art#Δ O-01 Shellbreaker#Dr. Jos Bonheur#Δ E-10 Rooster#sorXa#Machine at Arms#Aqueous OC#Aqueous sketch#Clara's Cohost backlog#Queuetaro Kujo
1 note
·
View note
Text











The following selection of 10 'Lode Coen Renaissance' artworks will be published in the Gangemi Contemporary Arts CAPSULE Catalogue October 24 - November 8 in ROME.
Titles top to bottom: Waves, The Devil & the Maiden, Venus Mermaid, The Emperor Gold Tarot, Origin Ovum Venus, Lord & Lady Dracula, It's a Beautiful Day, Hopper Train, Chinese Princess with a Young Snow Leopard, Adam & Eve, a Different Garden of Eden.
3 of those: Adam & Eve, Chinese Princess and Origin Ovum Venus will be exhibited as physical original artworks 50x70cm Chromaluxe. Curated by Monica Ferrarini. More info on https://lodecoen-renaissance.tumblr.com
0 notes
Text










The following selection of 10 'Lode Coen Renaissance' artworks will be published in the Gangemi Contemporary Arts CAPSULE Catalogue October 24 - November 8 in ROME.
Titles top to bottom: 1. Waves, 2. The Devil & the Maiden, 3. Venus Mermaid, 4. The Emperor Gold Tarot, 5. Origin Ovum Venus, 6. Lord & Lady Dracula, 7. It's a Beautiful Day, 8. Hopper Train, 9. Chinese Princess with a Young Snow Leopard, 10. Adam & Eve, a Different Garden of Eden.
3 of those: Adam & Eve, Chinese Princess and Origin Ovum Venus will be exhibited as physical original artworks 50x70cm Chromaluxe. Curated by Monica Ferrarini. More info on https://lodecoen-showcase.tumblr.com
0 notes
Text
PCOS AND AYURVEDA : A Holistic Approach to Managing Polycystic Ovary Syndrome

PCOS or Poly Cystic Ovarian Syndrome is a group of disorders affecting women of reproductive age and one among the common reasons found today for irregular menstrual cycle. Say it because of sedentary lifestyle or food habits, it sure is a menace for womanhood.
According to WHO, PCOS affects 116 million worldwide, PCOS affect approx. 10 percentage women in the reproductive age.
What is PCOS?
It is a disorder where the ovaries produce higher than normal level of male hormones (androgen) causing an imbalance in the system leading to trouble in normal ovulation and release of eggs (Ovum). Some of the ovum develops into fluid filled sacks called cyst which may even grow bigger in size.
WHAT CAUSES PCOS?
It is an endocrine disorder directly connected to the level of hormones in the body.
1. Increased level of male hormones (Androgen) — A smaller level of male hormones presents in every woman. Whereas its increase leads to imbalance triggering male traits such as extra hair growth, male pattern baldness and acne.
2. Increased level of Insulin — Insulin is a hormone regulating blood glucose level in the body. It helps in conversion of the food we eat into energy. Those with unhealthy eating habits, little to no-exercise, overweight or obese have higher chances of increase in blood glucose level and insulin resistance, which means their cells can’t take up insulin properly. When cells can’t use insulin properly, the demand in body rises thus triggering pancreatic cells to produce more insulin for supply. This extra insulin circulates in the body which in turn triggers ovaries producing male androgen.
3. Inflammation — Studies have linked excess inflammation to higher androgen levels. Inflammatory condition might be a contribution of overweight too.
HOW YOU KNOW YOU HAVE PCOS?
Some woman gets early symptoms whereas some go unnoticed until they find difficulty getting pregnant. You should notice it when there is,
· Irregular periods · Heavy menstruation · Excessive hair growth · Thinning of hair · Weight gain · Acne · Darkening of the skin in body creases like on neck, groin and under the breasts. · Headache
WHY PCOS A CONCERN?
Infertility: Fertilization happens only if there is a release of ovum. Woman who don’t ovulate thus find it difficult to conceive and is a major cause of infertility in woman. Metabolic diseases: Obesity and PCOS go hand in hand, slowing the metabolism. Hence woman with slow metabolic rate have higher chances of high blood sugar, LDL cholesterol, high blood pressure.
CAN ONE CONCEIVE WITH PCOS?
Woman with PCOS have trouble getting pregnant, if conceived they have higher chances of premature child birth, miscarriage, high blood pressure and gestational diabetes. However, woman with PCOS can get pregnant with infertility treatments.
ROLE OF AYURVEDA IN MANAGING PCOS
Efficiency of Ayurveda treatments and regimen are found in studies regarding management of PCOS.
Ayurveda focuses on balancing the metabolism and maintaining equilibrium of bio-energies. The metabolism which is lowered ion PCOS will be boosted with Ayurveda treatments and increases chances of conception. Ayurveda uses herbal formulations to correct the hormonal imbalance and regulates the normal rhythm of body. It also requires you to go through various types of therapies and maintain a balanced diet. All these play a vital role in overcoming PCOS - related problems.
The holistic approach includes a combination of dietary changes, lifestyle modifications, herbal remedies, and therapies aimed at restoring balance to the doshas and promoting overall health.
Read more....
0 notes
Text
AZEEZ ISMAIL:
360 NURSING BULLETS: Maternity and Newborn Nursing Reviewer
1.BASIC MATERNITY CONCEPTS
The male sperm contributes an X or a Y chromosome; the female ovum contributes an X chromosome.
Fertilization produces a total of 46 chromosomes, including an XY combination (male) or an XX combination (female).
Organogenesis occurs during the first trimester of pregnancy, specifically, days 14 to 56 of gestation.
Implantation in the uterus occurs 6 to 10 days after ovum fertilization.
The chorion is the outermost extraembryonic membrane that gives rise to the placenta.
The corpus luteum secretes large quantities of progesterone.
From the 8th week of gestation through delivery, the developing cells are known as a fetus.
The union of a male and a female gamete produces a zygote, which divides into the fertilized ovum.
Spermatozoa (or their fragments) remain in the vagina for 72 hours after sexual intercourse.
If the ovum is fertilized by a spermatozoon carrying a Y chromosome, a male zygote is formed.
Implantation occurs when the cellular walls of the blastocyte implants itself in the endometrium, usually 7 to 9 days after fertilization.
Implantation occurs when the cellular walls of the blastocyte implants itself in the endometrium, usually 7 to 9 days after fertilization.
Heart development in the embryo begins at 2 to 4 weeks and is complete by the end of the embryonic stage.
2.MENSTRUATION
If a patient misses a menstrual period while taking an oral contraceptive exactly as prescribed, she should continue taking the contraceptive.
The first menstrual flow is called menarche and may be anovulatory (infertile).
3.BREASTFEEDING
When both breasts are used for breastfeeding, the infant usually doesn’t empty the second breast. Therefore, the second breast should be used first at the next feeding.
Stress, dehydration, and fatigue may reduce a breastfeeding mother’s milk supply.
To help a mother break the suction of her breastfeeding infant, the nurse should teach her to insert a finger at the corner of the infant’s mouth.
Cow’s milk shouldn’t be given to infants younger than age one (1) because it has a low linoleic acid content and its protein is difficult for infants to digest.
A woman who is breastfeeding should rub a mild emollient cream or a few drops of breast milk (or colostrum) on the nipples after each feeding. She should let the breasts air-dry to prevent them from cracking.
Breastfeeding mothers should increase their fluid intake to 2½ to 3 qt (2,500 to 3,000 ml) daily.
After feeding an infant with a cleft lip or palate, the nurse should rinse the infant’s mouth with sterile water.
Human immunodeficiency virus (HIV) has been cultured in breast milk and can be transmitted by an HIV-positive mother who breast-feeds her infant.
Colostrum, the precursor of milk, is the first secretion from the breasts after delivery
A mother should allow her infant to breastfeed until the infant is satisfied. The time may vary from 5 to 20 minutes.
Most drugs that a breastfeeding mother takes appear in breast milk.
Prolactin stimulates and sustains milk production.
Breastfeeding of a premature neonate born at 32 weeks gestation can be accomplished if the mother expresses milk and feeds the neonate by gavage.
A mother who has a positive human immunodeficiency virus test result shouldn’t breastfeed her infant.
Hot compresses can help to relieve breast tenderness after breastfeeding.
Unlike formula, breast milk offers the benefit of maternal antibodies.
4.NEONATAL CARE
The initial weight loss for a healthy neonate is 5% to 10% of birth weight.
The normal hemoglobin value in neonates is 17 to 20 g/dl.
The circumference of a neonate’s head is normally 2 to 3 cm greater than the circumference of the chest.
After delivery, the first nursing action is to establish the neonate’s airway.
The specific gravity of a neonate’s urine is 1.003 to 1.030. A lower specific gravity suggests overhydration; a higher one suggests dehydration.
During the first hour after birth (the period of reactivity), the neonate is alert and awake.
The neonatal period extends from birth to day 28. It’s also called the first four (4) weeks or first month of life.
A low-birth-weight neonate weighs 2,500 g (5 lb 8 oz) or less at birth.
A very-low-birth-weight neonate weighs 1,500 g (3 lb 5 oz) or less at birth.
Administering high levels of oxygen to a premature neonate can cause blindness as a result of retrolental fibroplasia.
An Apgar score of 7 to 10 indicates no immediate distress, 4 to 6 indicates moderate distress, and 0 to 3 indicates severe distress.
To elicit Moro’s reflex, the nurse holds the neonate in both hands and suddenly, but gently, drops the neonate’s head backward. Normally, the neonate abducts and extends all extremities bilaterally and symmetrically, forms a C shape with the thumb and forefinger, and first adducts and then flexes the extremities.
An Apgar score of 7 to 10 indicates no immediate distress, 4 to 6 indicates moderate distress, and 0 to 3 indicates severe distress.
If jaundice is suspected in a neonate, the nurse should examine the infant under natural window light. If natural light is unavailable, the nurse should examine the infant under a white light.
Vitamin K is administered to neonates to prevent hemorrhagic disorders because a neonate’s intestine can’t synthesize vitamin K.
Variability is any change in the fetal heart rate (FHR) from its normal rate of 120 to 160 beats/minute. Acceleration is increased FHR; deceleration is decreased FHR.
Fetal alcohol syndrome presents in the first 24 hours after birth and produces lethargy, seizures, poor sucking reflex, abdominal distention, and respiratory difficulty.
In a neonate, the symptoms of heroin withdrawal may begin several hours to 4 days after birth.
In a neonate, the symptoms of methadone withdrawal may begin 7 days to several weeks after birth.
In a neonate, the cardinal signs of narcotic withdrawal include coarse, flapping tremors; sleepiness; restlessness; prolonged, persistent, high-pitched cry; and irritability.
The nurse should count a neonate’s respirations for one (1) full minute.
Chlorpromazine (Thorazine) is used to treat neonates who are addicted to narcotics.
The nurse should provide a dark, quiet environment for a neonate who is experiencing narcotic withdrawal.
Drugs used to treat withdrawal symptoms in neonates include phenobarbital (Luminal), camphorated opium tincture (paregoric), and diazepam (Valium).
In a premature neonate, signs of respiratory distress include nostril flaring, substernal retractions, and inspiratory grunting.
Respiratory distress syndrome (hyaline membrane disease) develops in premature infants because their pulmonary alveoli lack surfactant.
Whenever an infant is being put down to sleep, the parent or caregiver should position the infant on the back. Remember the mnemonic “back to sleep.”
The percentage of water in a neonate’s body is about 78% to 80%.
To perform nasotracheal suctioning in an infant, the nurse positions the infant with his neck slightly hyperextended in a “sniffing” position, with his chin up and his head tilted back slightly.
After birth, the neonate’s umbilical cord is tied 1″ (2.5 cm) from the abdominal wall with a cotton cord, plastic clamp, or rubber band.
When teaching parents to provide umbilical cord care, the nurse should teach them to clean the umbilical area with a cotton ball saturated with alcohol after every diaper change to prevent infection and promote drying.
Ortolani’s sign (an audible click or palpable jerk that occurs with thigh abduction) confirms congenital hip dislocation in a neonate.
Cutis marmorata is mottling or purple discoloration of the skin. It’s a transient vasomotor response that occurs primarily in the arms and legs of infants who are exposed to cold.
The first immunization for a neonate is the hepatitis B vaccine, which is administered in the nursery shortly after birth.
Infants with Down syndrome typically have marked hypotonia, floppiness, slanted eyes, excess skin on the back of the neck, flattened bridge of the nose, flat facial features, spade-like hands, short and broad feet, small male genitalia, absence of Moro’s reflex, and a simian crease on the hands.
The nurse instills erythromycin in a neonate’s eyes primarily to prevent blindness caused by gonorrhea or chlamydia.
A fever in the first 24 hours postpartum is most likely caused by dehydration rather than infection.
Preterm neonates or neonates who can’t maintain a skin temperature of at least 97.6° F (36.4° C) should receive care in an incubator (Isolette) or a radiant warmer. In a radiant warmer, a heat-sensitive probe taped to the neonate’s skin activates the heater unit automatically to maintain the desired temperature.
Neonates who are delivered by cesarean birth have a higher incidence of respiratory distress syndrome.
When providing phototherapy to a neonate, the nurse should cover the neonate’s eyes and genital area.
The narcotic antagonist naloxone (Narcan) may be given to a neonate to correct respiratory depression caused by narcotic administration to the mother during labor.
In a neonate, symptoms of respiratory distress syndrome include expiratory grunting or whining, sandpaper breath sounds, and seesaw retractions.
Cerebral palsy presents as asymmetrical movement, irritability, and excessive, feeble crying in a long, thin infant.
The nurse should assess a breech-birth neonate for hydrocephalus, hematomas, fractures, and other anomalies caused by birth trauma.
In a neonate, long, brittle fingernails are a sign of postmaturity.
Desquamation (skin peeling) is common in postmature neonates.
The average birth weight of neonates born to mothers who smoke is 6 oz (170 g) less than that of neonates born to nonsmoking mothers.
Neonatal jaundice in the first 24 hours after birth is known as pathological jaundice and is a sign of erythroblastosis fetalis.
Lanugo covers the fetus’s body until about 20 weeks gestation. Then it begins to disappear from the face, trunk, arms, and legs, in that order.
In a neonate, hypoglycemia causes temperature instability, hypotonia, jitteriness, and seizures.
Premature, postmature, small-for-gestational-age, and large-for-gestational-age neonates are susceptible to this disorder.
Neonates typically need to consume 50 to 55 cal per pound of body weight daily.
During fetal heart rate monitoring, variable decelerations indicate compression or prolapse of the umbilical cord.
A neonate whose mother has diabetes should be assessed for hyperinsulinism.
The best technique for assessing jaundice in a neonate is to blanch the tip of the nose or the area just above the umbilicus.
Milia may occur as pinpoint spots over a neonate’s nose.
Strabismus is a normal finding in a neonate.
Respiratory distress syndrome develops in premature neonates because their alveoli lack surfactant.
Rubella infection in a pregnant patient, especially during the first trimester, can lead to spontaneous abortion or stillbirth as well as fetal cardiac and other birth defects.
The Apgar score is used to assess the neonate’s vital functions. It’s obtained at 1 minute and 5 minutes after delivery. The score is based on respiratory effort, heart rate, muscle tone, reflex irritability, and color.
Erythromycin is given at birth to prevent ophthalmia neonatorum.
In the neonate, the normal blood glucose level is 45 to 90 mg/dl.
Hepatitis B vaccine is usually given within 48 hours of birth.
Hepatitis B immune globulin is usually given within 12 hours of birth.
Boys who are born with hypospadias shouldn’t be circumcised at birth because the foreskin may be needed for constructive surgery.
In neonates, cold stress affects the circulatory, regulatory, and respiratory systems.
Fetal embodiment is a maternal developmental task that occurs in the second trimester. During this stage, the mother may complain that she never gets to sleep because the fetus always gives her a thump when she tries.
Mongolian spots can range from brown to blue. Their color depends on how close melanocytes are to the surface of the skin. They most commonly appear as patches across the sacrum, buttocks, and legs.
Mongolian spots are common in non-white infants and usually disappear by age 2 to 3 years.
Vernix caseosa is a cheeselike substance that covers and protects the fetus’s skin in utero. It may be rubbed into the neonate’s skin or washed away in one or two baths.
Caput succedaneum is edema that develops in and under the fetal scalp during labor and delivery. It resolves spontaneously and presents no danger to the neonate. The edema doesn’t cross the suture line.
Nevus flammeus, or port-wine stain, is a diffuse pink to dark bluish red lesion on a neonate’s face or neck.
The Guthrie test (a screening test for phenylketonuria) is most reliable if it’s done between the second and sixth days after birth and is performed after the neonate has ingested protein.
To assess coordination of sucking and swallowing, the nurse should observe the neonate’s first breastfeeding or sterile water bottle-feeding.
To establish a milk supply pattern, the mother should breast-feed her infant at least every 4 hours. During the first month, she should breast-feed 8 to 12 times daily (demand feeding).
To avoid contact with blood and other body fluids, the nurse should wear gloves when handling the neonate until after the first bath is given.
If a breast-fed infant is content, has good skin turgor, an adequate number of wet diapers, and normal weight gain, the mother’s milk supply is assumed to be adequate.
In the supine position, a pregnant patient’s enlarged uterus impairs venous return from the lower half of the body to the heart, resulting in supine hypotensive syndrome, or inferior vena cava syndrome.
Tocolytic agents used to treat preterm labor include terbutaline (Brethine), ritodrine (Yutopar), and magnesium sulfate.
A pregnant woman who has hyperemesis gravidarum may require hospitalization to treat dehydration and starvation.
Diaphragmatic hernia is one of the most urgent neonatal surgical emergencies. By compressing and displacing the lungs and heart, this disorder can cause respiratory distress shortly after birth.
Common complications of early pregnancy (up to 20 weeks gestation) include fetal loss and serious threats to maternal health.
If the neonate is stable, the mother should be allowed to breast-feed within the neonate’s first hour of life.
The nurse should check the neonate’s temperature every 1 to 2 hours until it’s maintained within normal limits.
At birth, a neonate normally weighs 5 to 9 lb (2 to 4 kg), measures 18″ to 22″ (45.5 to 56 cm) in length, has a head circumference of 13½” to 14″ (34 to 35.5 cm), and has a chest circumference that’s 1″ (2.5 cm) less than the head circumference.
In the neonate, temperature normally ranges from 98° to 99° F (36.7° to 37.2° C), apical pulse rate averages 120 to 160 beats/minute, and respirations are 40 to 60 breaths/minute.
The diamond-shaped anterior fontanel usually closes between ages 12 and 18 months. The triangular posterior fontanel usually closes by age 2 months.
In the neonate, a straight spine is normal. A tuft of hair over the spine is an abnormal finding.
Prostaglandin gel may be applied to the vagina or cervix to ripen an unfavorable cervix before labor induction with oxytocin (Pitocin).
Supernumerary nipples are occasionally seen on neonates. They usually appear along a line that runs from each axilla, through the normal nipple area, and to the groin.
Meconium is a material that collects in the fetus’s intestines and forms the neonate’s first feces, which are black and tarry.
The presence of meconium in the amniotic fluid during labor indicates possible fetal distress and the need to evaluate the neonate for meconium aspiration.
To assess a neonate’s rooting reflex, the nurse touches a finger to the cheek or the corner of the mouth. Normally, the neonate turns his head toward the stimulus, opens his mouth, and searches for the stimulus.
Harlequin sign is present when a neonate who is lying on his side appears red on the dependent side and pale on the upper side.
Because of the anti-insulin effects of placental hormones, insulin requirements increase during the third trimester.
Gestational age can be estimated by ultrasound measurement of maternal abdominal circumference, fetal femur length, and fetal head size. These measurements are most accurate between 12 and 18 weeks gestation.
Skeletal system abnormalities and ventricular septal defects are the most common disorders of infants who are born to diabetic women. The incidence of congenital malformation is three times higher in these infants than in those born to nondiabetic women.
Skeletal system abnormalities and ventricular septal defects are the most common disorders of infants who are born to diabetic women. The incidence of congenital malformation is three times higher in these infants than in those born to nondiabetic women.
The patient with preeclampsia usually has puffiness around the eyes or edema in the hands (for example, “I can’t put my wedding ring on.”).
Kegel exercises require contraction and relaxation of the perineal muscles. These exercises help strengthen pelvic muscles and improve urine control in postpartum patients.
Symptoms of postpartum depression range from mild postpartum blues to intense, suicidal, depressive psychosis.
The preterm neonate may require gavage feedings because of a weak sucking reflex, uncoordinated sucking, or respiratory distress.
Acrocyanosis (blueness and coolness of the arms and legs) is normal in neonates because of their immature peripheral circulatory system.
To prevent ophthalmia neonatorum (a severe eye infection caused by maternal gonorrhea), the nurse may administer one of three drugs, as prescribed, in the neonate’s eyes: tetracycline, silver nitrate, or erythromycin.
Neonatal testing for phenylketonuria is mandatory in most states.
The nurse should place the neonate in a 30-degree Trendelenburg position to facilitate mucus drainage.
The nurse may suction the neonate’s nose and mouth as needed with a bulb syringe or suction trap.
To prevent heat loss, the nurse should place the neonate under a radiant warmer during suctioning and initial delivery-room care, and then wrap the neonate in a warmed blanket for transport to the nursery.
The umbilical cord normally has two arteries and one vein.
When providing care, the nurse should expose only one part of an infant’s body at a time.
Lightening is settling of the fetal head into the brim of the pelvis.
5.PRENATAL CARE
In a full-term neonate, skin creases appear over two-thirds of the neonate’s feet. Preterm neonates have heel creases that cover less than two-thirds of the feet.
At 20 weeks gestation, the fundus is at the level of the umbilicus.
At 36 weeks gestation, the fundus is at the lower border of the rib cage.
A premature neonate is one born before the end of the 37th week of gestation.
Gravida is the number of pregnancies a woman has had, regardless of outcome.
Para is the number of pregnancies that reached viability, regardless of whether the fetus was delivered alive or stillborn. A fetus is considered viable at 20 weeks gestation.
A multipara is a woman who has had two or more pregnancies that progressed to viability, regardless of whether the offspring were alive at birth.
Positive signs of pregnancy include ultrasound evidence, fetal heart tones, and fetal movement felt by the examiner (not usually present until 4 months gestation
Quickening, a presumptive sign of pregnancy, occurs between 16 and 19 weeks gestation.
Goodell’s sign is softening of the cervix.
Quickening, a presumptive sign of pregnancy, occurs between 16 and 19 weeks gestation.
Ovulation ceases during pregnancy.
Immunity to rubella can be measured by a hemagglutination inhibition test (rubella titer).
This test identifies exposure to rubella infection and determines susceptibility in pregnant women. In a woman, a titer greater than 1:8 indicates immunity.
To estimate the date of delivery using Naegele’s rule, the nurse counts backward three (3) months from the first day of the last menstrual period and then adds seven (7) days to this date.
During pregnancy, weight gain averages 25 to 30 lb (11 to 13.5 kg).
Rubella has a teratogenic effect on the fetus during the first trimester. It produces abnormalities in up to 40% of cases without interrupting the pregnancy.
At 12 weeks gestation, the fundus should be at the top of the symphysis pubis.
Chloasma, the mask of pregnancy, is pigmentation of a circumscribed area of skin (usually over the bridge of the nose and cheeks) that occurs in some pregnant women.
The gynecoid pelvis is most ideal for delivery. Other types include platypelloid (flat), anthropoid (ape-like), and android (malelike).
Pregnant women should be advised that there is no safe level of alcohol intake.
Linea nigra, a dark line that extends from the umbilicus to the mons pubis, commonly appears during pregnancy and disappears after pregnancy.
Culdoscopy is visualization of the pelvic organs through the posterior vaginal fornix.
The nurse should teach a pregnant vegetarian to obtain protein from alternative sources, such as nuts, soybeans, and legumes.
The nurse should instruct a pregnant patient to take only prescribed prenatal vitamins because over-the-counter high-potency vitamins may harm the fetus.
High-sodium foods can cause fluid retention, especially in pregnant patients.
A pregnant patient can avoid constipation and hemorrhoids by adding fiber to her diet.
A pregnant woman should drink at least eight 8-oz glasses (about 2,000 ml) of water daily.
Cytomegalovirus is the leading cause of congenital viral infection.
Tocolytic therapy is indicated in premature labor, but contraindicated in fetal death, fetal distress, or severe hemorrhage.
Through ultrasonography, the biophysical profile assesses fetal well-being by measuring fetal breathing movements, gross body movements, fetal tone, reactive fetal heart rate (nonstress test), and qualitative amniotic fluid volume.
Pica is a craving to eat nonfood items, such as dirt, crayons, chalk, glue, starch, or hair. It may occur during pregnancy and can endanger the fetus.
A pregnant patient should take folic acid because this nutrient is required for rapid cell division.
A woman who is taking clomiphene (Clomid) to induce ovulation should be informed of the possibility of multiple births with this drug.
During the first trimester, a pregnant woman should avoid all drugs unless doing so would adversely affect her health.
The Food and Drug Administration has established the following five categories of drugs based on their potential for causing birth defects: A, no evidence of risk; B, no risk found in animals, but no studies have been done in women; C, animal studies have shown an adverse effect, but the drug may be beneficial to women despite the potential risk; D, evidence of risk, but its benefits may outweigh its risks; and X, fetal anomalies noted, and the risks clearly outweigh the potential benefits.
Para is the number of pregnancies that reached viability, regardless of whether the fetus was delivered alive or stillborn. A fetus is considered viable at 20 weeks gestation.
A multipara is a woman who has had two or more pregnancies that progressed to viability, regardless of whether the offspring were alive at birth.
Positive signs of pregnancy include ultrasound evidence, fetal heart tones, and fetal movement felt by the examiner (not usually present until 4 months gestation.
Quickening, a presumptive sign of pregnancy, occurs between 16 and 19 weeks gestation.
Goodell’s sign is softening the cervix.
Quickening, a presumptive sign of pregnancy, occurs between 16 and 19 weeks gestation.
Ovulation ceases during pregnancy.
Immunity to rubella can be measured by a hemagglutination inhibition test (rubella titer).
This test identifies exposure to rubella infection and determines susceptibility in pregnant women. In a woman, a titer greater than 1:8 indicates immunity.
To estimate the date of delivery using Naegele’s rule, the nurse counts backward three (3) months from the first day of the last menstrual period and then adds seven (7) days to this date.
During pregnancy, weight gain averages 25 to 30 lb (11 to 13.5 kg).
Rubella has a teratogenic effect on the fetus during the first trimester. It produces abnormalities in up to 40% of cases without interrupting the pregnancy.
At 12 weeks gestation, the fundus should be at the top of the symphysis pubis.
Chloasma, the mask of pregnancy, is pigmentation of a circumscribed area of skin (usually over the bridge of the nose and cheeks) that occurs in some pregnant women.
The gynecoid pelvis is most ideal for delivery. Other types include platypelloid (flat), anthropoid (ape-like), and android (malelike).
Pregnant women should be advised that there is no safe level of alcohol intake.
Linea nigra, a dark line that extends from the umbilicus to the mons pubis, commonly appears during pregnancy and disappears after pregnancy.
Culdoscopy is a visualization of the pelvic organs through the posterior vaginal fornix.
The nurse should teach a pregnant vegetarian to obtain protein from alternative sources, such as nuts, soybeans, and legumes.
The nurse should instruct a pregnant patient to take only prescribed prenatal vitamins because over-the-counter high-potency vitamins may harm the fetus.
High-sodium foods can cause fluid retention, especially in pregnant patients.
A pregnant patient can avoid constipation and hemorrhoids by adding fiber to her diet.
A pregnant woman should drink at least eight 8-oz glasses (about 2,000 ml) of water daily.
Cytomegalovirus is the leading cause of congenital viral infection.
Tocolytic therapy is indicated in premature labor, but contraindicated in fetal death, fetal distress, or severe hemorrhage.
Through ultrasonography, the biophysical profile assesses fetal well-being by measuring fetal breathing movements, gross body movements, fetal tone, reactive fetal heart rate (nonstress test), and qualitative amniotic fluid volume.
Pica is a craving to eat nonfood items, such as dirt, crayons, chalk, glue, starch, or hair. It may occur during pregnancy and can endanger the fetus.
A pregnant patient should take folic acid because this nutrient is required for rapid cell division.
A woman who is taking clomiphene (Clomid) to induce ovulation should be informed of the possibility of multiple births with this drug.
During the first trimester, a pregnant woman should avoid all drugs unless doing so would adversely affect her health.
The Food and Drug Administration has established the following five categories of drugs based on their potential for causing birth defects: A, no evidence of risk; B, no risk found in animals, but no studies have been done in women; C, animal studies have shown an adverse effect, but the drug may be beneficial to women despite the potential risk; D, evidence of risk, but its benefits may outweigh its risks; and X, fetal anomalies noted, and the risks clearly outweigh the potential benefits.
A probable sign of pregnancy, McDonald’s sign is characterized by an ease in flexing the body of the uterus against the cervix.
Amenorrhea is a probable sign of pregnancy.
A pregnant woman’s partner should avoid introducing air into the vagina during oral sex because of the possibility of air embolism.
The presence of human chorionic gonadotropin in the blood or urine is a probable sign of pregnancy.
Radiography isn’t usually used in a pregnant woman because it may harm the developing fetus. If radiography is essential, it should be performed only after 36 weeks of gestation.
A pregnant patient who has had rupture of the membranes or who is experiencing vaginal bleeding shouldn’t engage in sexual intercourse.
A pregnant staff member should not be assigned to work with a patient who has cytomegalovirus infection because the virus can be transmitted to the fetus.
A pregnant patient should take an iron supplement to help prevent anemia.
Nausea and vomiting during the first trimester of pregnancy are caused by rising levels of the hormone human chorionic gonadotropin.
The duration of pregnancy averages 280 days, 40 weeks, 9 calendar months, or 10 lunar months.
Before performing a Leopold maneuver, the nurse should ask the patient to empty her bladder.
Pelvic-tilt exercises can help to prevent or relieve backache during pregnancy.
The nurse must place identification bands on both the mother and the neonate before they leave the delivery room.
Dinoprostone (Cervidil) is used to ripen the cervix.
Because women with diabetes have a higher incidence of birth anomalies than women without diabetes, an alpha-fetoprotein level may be ordered at 15 to 17 weeks gestation.
Painless vaginal bleeding during the last trimester of pregnancy may indicate placenta previa.
The hormone human chorionic gonadotropin is a marker for pregnancy.
With advanced maternal age, a common genetic problem is Down syndrome.
Methergine stimulates uterine contractions.
The administration of folic acid during the early stages of gestation may prevent neural tube defects.
A clinical manifestation of a prolapsed umbilical cord is variable decelerations.
The nurse should keep the sac of meningomyelocele moist with normal saline solution.
If fundal height is at least 2 cm less than expected, the cause may be growth retardation, missed abortion, transverse lie, or false pregnancy.
Fundal height that exceeds expectations by more than 2 cm may be caused by multiple gestation, polyhydramnios, uterine myomata, or a large baby.
A major developmental task for a woman during the first trimester of pregnancy is accepting the pregnancy.
A pregnant patient with vaginal bleeding shouldn’t have a pelvic examination.
In the early stages of pregnancy, the finding of glucose in the urine may be related to the increased shunting of glucose to the developing placenta, without a corresponding increase in the reabsorption capability of the kidneys.
A patient who has premature rupture of the membranes is at significant risk for infection if labor doesn’t begin within 24 hours.
Infants of diabetic mothers are susceptible to macrosomia as a result of increased insulin production in the fetus.
To prevent heat loss in the neonate, the nurse should bathe one part of his body at a time and keep the rest of the body covered.
A patient who has a cesarean delivery is at greater risk for infection than the patient who gives birth vaginally.
The occurrence of thrush in the neonate is probably caused by contact with the organism during delivery through the birth canal.
Maternal serum alpha-fetoprotein is detectable at 7 weeks of gestation and peaks in the third trimester. High levels detected between the 16th and 18th weeks are associated with neural tube defects. Low levels are associated with Down syndrome.
An arrest of descent occurs when the fetus doesn’t descend through the pelvic cavity during labor. It’s commonly associated with cephalopelvic disproportion, and cesarean delivery may be required.
A late sign of preeclampsia is epigastric pain as a result of severe liver edema.
In the patient with preeclampsia, blood pressure returns to normal during the puerperal period.
To obtain an estriol level, urine is collected for 24 hours.
An estriol level is used to assess fetal well-being and maternal renal functioning as well as to monitor a pregnancy that’s complicated by diabetes.
The period between contractions is referred to as the interval, or resting phase. During this phase, the uterus and placenta fill with blood and allow for the exchange of oxygen, carbon dioxide, and nutrients.
In a patient who has hypertonic contractions, the uterus doesn’t have an opportunity to relax and there is no interval between contractions.
As a result, the fetus may experience hypoxia or rapid delivery may occur.
Two qualities of the myometrium are elasticity, which allows it to stretch yet maintain its tone, and contractility, which allows it to shorten and lengthen in a synchronized pattern.
During crowning, the presenting part of the fetus remains visible during the interval between contractions.
Uterine atony is failure of the uterus to remain firmly contracted.
The major cause of uterine atony is a full bladder.
If the mother wishes to breastfeed, the neonate should be nursed as soon as possible after delivery.
A smacking sound, milk dripping from the side of the mouth, and sucking noises all indicate improper placement of the infant’s mouth over the nipple.
Before feeding is initiated, an infant should be burped to expel air from the stomach.
Most authorities strongly encourage the continuation of breastfeeding on both the affected and the unaffected breast of patients with mastitis.
Neonates are nearsighted and focus on items that are held 10″ to 12″ (25 to 30.5 cm) away.
In a neonate, low-set ears are associated with chromosomal abnormalities such as Down syndrome.
Meconium is usually passed in the first 24 hours; however, passage may take up to 72 hours.
Obstetric data can be described by using the F/TPAL system:
F/T: Full-term delivery at 38 weeks or longer
P: Preterm delivery between 20 and 37 weeks
A: Abortion or loss of fetus before 20 weeks
L: Number of children living (if a child has died, further explanation is needed to clarify the discrepancy in numbers).
Parity doesn’t refer to the number of infants delivered, only the number of deliveries.
Women who are carrying more than one fetus should be encouraged to gain 35 to 45 lb (15.5 to 20.5 kg) during pregnancy.
The recommended amount of iron supplement for the pregnant patient is 30 to 60 mg daily.
Drinking six alcoholic beverages a day or a single episode of binge drinking in the first trimester can cause fetal alcohol syndrome.
Chorionic villus sampling is performed at 8 to 12 weeks of pregnancy for early identification of genetic defects.
In percutaneous umbilical blood sampling, a blood sample is obtained from the umbilical cord to detect anemia, genetic defects, and blood incompatibility as well as to assess the need for blood transfusions.
Hemodilution of pregnancy is the increase in blood volume that occurs during pregnancy.
The increased volume consists of plasma and causes an imbalance between the ratio of red blood cells to plasma and a resultant decrease in hematocrit.
Visualization in pregnancy is a process in which the mother imagines what the child she’s carrying is like and becomes acquainted with it.
Mean arterial pressure of greater than 100 mm Hg after 20 weeks of pregnancy is considered hypertension.
Laden’s sign, an early indication of pregnancy, causes softening of a spot on the anterior portion of the uterus, just above the uterocervical juncture.
During pregnancy, the abdominal line from the symphysis pubis to the umbilicus changes from linea alba to linea nigra.
The treatment for supine hypotension syndrome (a condition that sometimes occurs in pregnancy) is to have the patient lie on her left side.
A contributing factor in dependent edema in the pregnant patient is the increase of femoral venous pressure from 10 mm Hg (normal) to 18 mm Hg (high).
Hyperpigmentation of the pregnant patient’s face, formerly called chloasma and now referred to as melasma, fades after delivery.
The hormone relaxin, which is secreted first by the corpus luteum and later by the placenta, relaxes the connective tissue and cartilage of the symphysis pubis and the sacroiliac joint to facilitate passage of the fetus during delivery.
Progesterone maintains the integrity of the pregnancy by inhibiting uterine motility.
LABOR AND DELIVERY
During labor, to relieve supine hypotension manifested by nausea and vomiting and paleness, turn the patient on her left side.
During the transition phase of the first stage of labor, the cervix is dilated 8 to 10 cm and contractions usually occur 2 to 3 minutes apart and last for 60 seconds.
The first stage of labor begins with the onset of labor and ends with full cervical dilation at 10 cm.
The second stage of labor begins with full cervical dilation and ends with the neonate’s birth.
The third stage of labor begins after the neonate’s birth and ends with expulsion of the placenta.
The fourth stage of labor (postpartum stabilization) lasts up to 4 hours after the placenta is delivered. This time is needed to stabilize the mother’s physical and emotional state after the stress of childbirth.
Unlike false labor, true labor produces regular rhythmic contractions, abdominal discomfort, progressive descent of the fetus, bloody show, and progressive effacement and dilation of the cervix.
When used to describe the degree of fetal descent during labor, floating means the presenting part is not engaged in the pelvic inlet, but is freely movable (ballotable) above the pelvic inlet.
When used to describe the degree of fetal descent, engagement means when the largest diameter of the presenting part has passed through the pelvic inlet.
Fetal stations indicate the location of the presenting part in relation to the ischial spine. It’s described as –1, –2, –3, –4, or –5 to indicate the number of centimeters above the level of the ischial spine; station –5 is at the pelvic inlet.
Fetal stations are also described as +1, +2, +3, +4, or +5 to indicate the number of centimeters it is below the level of the ischial spine; station 0 is at the level of the ischial spine.
Any vaginal bleeding during pregnancy should be considered a complication until proven otherwise.
During delivery, if the umbilical cord can’t be loosened and slipped from around the neonate’s neck, it should be clamped with two clamps and cut between the clamps.
During the first stage of labor, the side-lying position usually provides the greatest degree of comfort, although the patient may assume any comfortable position.
Fetal stations are also described as +1, +2, +3, +4, or +5 to indicate the number of centimeters it is below the level of the ischial spine; station 0 is at the level of the ischial spine.
Fetal stations indicate the location of the presenting part in relation to the ischial spine. It’s described as –1, –2, –3, –4, or –5 to indicate the number of centimeters above the level of the ischial spine; station –5 is at the pelvic inlet.
When used to describe the degree of fetal descent, engagement means when the largest diameter of the presenting part has passed through the pelvic inlet.
Amniotomy is artificial rupture of the amniotic membranes.
The three phases of a uterine contraction are increment, acme, and decrement.
The intensity of a labor contraction can be assessed by the indentability of the uterine wall at the contraction’s peak. Intensity is graded as mild (uterine muscle is somewhat tense), moderate (uterine muscle is moderately tense), or strong (uterine muscle is boardlike).
The frequency of uterine contractions, which is measured in minutes, is the time from the beginning of one contraction to the beginning of the next.
Before internal fetal monitoring can be performed, a pregnant patient’s cervix must be dilated at least 2 cm, the amniotic membranes must be ruptured, and the presenting part of the fetus (scalp or buttocks) must be at station –1 or lower, so that a small electrode can be attached.
Teenage mothers are more likely to have low-birth-weight neonates because they seek prenatal care late in pregnancy (as a result of denial) and are more likely than older mothers to have nutritional deficiencies.
The narrowest diameter of the pelvic inlet is the anteroposterior (diagonal conjugate).
During labor, the resting phase between contractions is at least 30 seconds.
The length of the uterus increases from 2½” (6.3 cm) before pregnancy to 12½” (32 cm) at term.
To estimate the true conjugate (the smallest inlet measurement of the pelvis), deduct 1.5 cm from the diagonal conjugate (usually 12 cm). A true conjugate of 10.5 cm enables the fetal head (usually 10 cm) to pass.
The smallest outlet measurement of the pelvis is the intertuberous diameter, which is the transverse diameter between the ischial tuberosities.
Electronic fetal monitoring is used to assess fetal well-being during labor. If compromised fetal status is suspected, fetal blood pH may be evaluated by obtaining a scalp sample.
In an emergency delivery, enough pressure should be applied to the emerging fetus’s head to guide the descent and prevent a rapid change in pressure within the molded fetal skull.
Massaging the uterus helps to stimulate contractions after the placenta is delivered.
When a patient is admitted to the unit in active labor, the nurse’s first action is to listen for fetal heart tones.
Nitrazine paper is used to test the pH of vaginal discharge to determine the presence of amniotic fluid.
A pregnant patient normally gains 2 to 5 lb (1 to 2.5 kg) during the first trimester and slightly less than 1 lb (0.5 kg) per week during the last two trimesters.
Precipitate labor lasts for approximately 3 hours and ends with delivery of the neonate.
As emergency treatment for excessive uterine bleeding, 0.2 mg of methylergonovine (Methergine) is injected I.V. over 1 minute while the patient’s blood pressure and uterine contractions are monitored.
Braxton Hicks contractions are usually felt in the abdomen and don’t cause cervical change. True labor contractions are felt in the front of the abdomen and back and lead to progressive cervical dilation and effacement.
If a fetus has late decelerations (a sign of fetal hypoxia), the nurse should instruct the mother to lie on her left side and then administer 8 to 10 L of oxygen per minute by mask or cannula.
The nurse should notify the physician. The side-lying position removes pressure on the inferior vena cava.
Oxytocin (Pitocin) promotes lactation and uterine contractions.
Because oxytocin (Pitocin) stimulates powerful uterine contractions during labor, it must be administered under close observation to help prevent maternal and fetal distress.
Molding is the process by which the fetal head changes shape to facilitate movement through the birth canal.
If a woman suddenly becomes hypotensive during labor, the nurse should increase the infusion rate of I.V. fluids as prescribed.
During fetal heart monitoring, early deceleration is caused by compression of the head during labor.
After the placenta is delivered, the nurse may add oxytocin (Pitocin) to the patient’s I.V. solution, as prescribed, to promote postpartum involution of the uterus and stimulate lactation.
If needed, cervical suturing is usually done between 14 and 18 weeks gestation to reinforce an incompetent cervix and maintain pregnancy. The suturing is typically removed by 35 weeks gestation.
The Food and Drug Administration has established the following five categories of drugs based on their potential for causing birth defects: A, no evidence of risk; B, no risk found in animals, but no studies have been done in women; C, animal studies have shown an adverse effect, but the drug may be beneficial to women despite the potential risk; D, evidence of risk, but its benefits may outweigh its risks; and X, fetal anomalies noted, and the risks clearly outweigh the potential benefits.
The mechanics of delivery are engagement, descent and flexion, internal rotation, extension, external rotation, restitution, and expulsion.
The duration of a contraction is timed from the moment that the uterine muscle begins to tense to the moment that it reaches full relaxation. It’s measured in seconds.
Fetal demise is death of the fetus after viability.
The most common method of inducing labor after artificial rupture of the membranes is oxytocin (Pitocin) infusion.
After the amniotic membranes rupture, the initial nursing action is to assess the fetal heart rate.
The most common reasons for cesarean birth are malpresentation, fetal distress, cephalopelvic disproportion, pregnancy-induced hypertension, previous cesarean birth, and inadequate progress in labor.
Amniocentesis increases the risk of spontaneous abortion, trauma to the fetus or placenta, premature labor, infection, and Rh sensitization of the fetus.
After amniocentesis, abdominal cramping or spontaneous vaginal bleeding may indicate complications.
To prevent her from developing Rh antibodies, an Rh-negative primigravida should receive Rho(D) immune globulin (RhoGAM) after delivering an Rh-positive neonate.
When informed that a patient’s amniotic membrane has broken, the nurse should check fetal heart tones and then maternal vital signs.
Crowning is the appearance of the fetus’s head when its largest diameter is encircled by the vulvovaginal ring.
Subinvolution may occur if the bladder is distended after delivery.
For an extramural delivery (one that takes place outside of a normal delivery center), the priorities for care of the neonate include maintaining a patent airway, supporting efforts to breathe, monitoring vital signs, and maintaining adequate body temperature.
The administration of oxytocin (Pitocin) is stopped if the contractions are 90 seconds or longer.
If a pregnant patient’s rubella titer is less than 1:8, she should be immunized after delivery.
During the transition phase of labor, the woman usually is irritable and restless.
Maternal hypotension is a complication of spinal block.
The mother’s Rh factor should be determined before an amniocentesis is performed.
With early maternal age, cephalopelvic disproportion commonly occurs.
Spontaneous rupture of the membranes increases the risk of a prolapsed umbilical cord.
Postpartum Care
Lochia rubra is the vaginal discharge of almost pure blood that occurs during the first few days after childbirth.
Lochia serosa is the serous vaginal discharge that occurs 4 to 7 days after childbirth.
Lochia alba is the vaginal discharge of decreased blood and increased leukocytes that’s the final stage of lochia. It occurs 7 to 10 days after childbirth.
After delivery, a multiparous woman is more susceptible to bleeding than a primiparous woman because her uterine muscles may be overstretched and may not contract efficiently.
The nurse should suggest ambulation to a postpartum patient who has gas pain and flatulence.
Methylergonovine (Methergine) is an oxytocic agent used to prevent and treat postpartum hemorrhage caused by uterine atony or subinvolution.
After a stillbirth, the mother should be allowed to hold the neonate to help her come to terms with the death.
If a woman receives a spinal block before delivery, the nurse should monitor the patient’s blood pressure closely.
A postpartum patient may resume sexual intercourse after the perineal or uterine wounds heal (usually within 4 weeks after delivery).
If a pregnant patient’s test results are negative for glucose but positive for acetone, the nurse should assess the patient’s diet for inadequate caloric intake.
Direct antiglobulin (direct Coombs’) test is used to detect maternal antibodies attached to red blood cells in the neonate.
Before discharging a patient who has had an abortion, the nurse should instruct her to report bright red clots, bleeding that lasts longer than 7 days, or signs of infection, such as a temperature of greater than 100° F (37.8° C), foul-smelling vaginal discharge, severe uterine cramping, nausea, or vomiting.
The fundus of a postpartum patient is massaged to stimulate contraction of the uterus and prevent hemorrhage.
Laceration of the vagina, cervix, or perineum produces bright red bleeding that often comes in spurts. The bleeding is continuous, even when the fundus is firm.
To avoid puncturing the placenta, a vaginal examination should not be performed on a pregnant patient who is bleeding.
A patient who has postpartum hemorrhage caused by uterine atony should be given oxytocin as prescribed.
After delivery, if the fundus is boggy and deviated to the right side, the patient should empty her bladder.
In the early postpartum period, the fundus should be midline at the umbilicus.
Pregnancy Complications
An ectopic pregnancy is one that implants abnormally, outside the uterus.
A habitual aborter is a woman who has had three or more consecutive spontaneous abortions.
Threatened abortion occurs when bleeding is present without cervical dilation.
A complete abortion occurs when all products of conception are expelled.
Hydramnios (polyhydramnios) is excessive amniotic fluid of more than 2,000 ml in the third trimester.
In an incomplete abortion, the fetus is expelled, but parts of the placenta and membrane remain in the uterus.
When a pregnant patient has undiagnosed vaginal bleeding, vaginal examination should be avoided until ultrasonography rules out placenta previa.
A patient with a ruptured ectopic pregnancy commonly has sharp pain in the lower abdomen, with spotting and cramping. She may have abdominal rigidity; rapid, shallow respirations; tachycardia; and shock.
A 16-year-old girl who is pregnant is at risk for having a low-birth-weight neonate.
A rubella vaccine shouldn’t be given to a pregnant woman. The vaccine can be administered after delivery, but the patient should be instructed to avoid becoming pregnant for 3 months.
Nonstress Test
A nonstress test is considered nonreactive (positive) if fewer than two fetal heart rate accelerations of at least 15 beats/minute occur in 20 minutes.
A nonstress test is considered reactive (negative) if two or more fetal heart rate accelerations of 15 beats/minute above baseline occur in 20 minutes.
A nonstress test is usually performed to assess fetal well-being in a pregnant patient with a prolonged pregnancy (42 weeks or more), diabetes, a history of poor pregnancy outcomes, or pregnancy-induced hypertension.
Placental Abnormalities
Placenta previa is abnormally low implantation of the placenta so that it encroaches on or covers the cervical os.
In complete (total) placenta previa, the placenta completely covers the cervical os.
In partial (incomplete or marginal) placenta previa, the placenta covers only a portion of the cervical os.
Abruptio placentae is premature separation of a normally implanted placenta. It may be partial or complete, and usually causes abdominal pain, vaginal bleeding, and a boardlike abdomen.
In placenta previa, bleeding is painless and seldom fatal on the first occasion, but it becomes heavier with each subsequent episode.
Nursing interventions for a patient with placenta previa include positioning the patient on her left side for maximum fetal perfusion, monitoring fetal heart tones, and administering I.V. fluids and oxygen, as ordered.
Treatment for abruptio placentae is usually immediate cesarean delivery.
A classic difference between abruptio placentae and placenta previa is the degree of pain. Abruptio placentae causes pain, whereas placenta previa causes painless bleeding.
Because a major role of the placenta is to function as a fetal lung, any condition that interrupts normal blood flow to or from the placenta increases fetal partial pressure of arterial carbon dioxide and decreases fetal pH.
Preeclampsia
Pregnancy-induced hypertension is a leading cause of maternal death in the United States.
Pregnancy-induced hypertension (preeclampsia) is an increase in blood pressure of 30/15 mm Hg over baseline or blood pressure of 140/95 mmHg on two occasions at least 6 hours apart accompanied by edema and albuminuria after 20 weeks gestation.
The classic triad of symptoms of preeclampsia are hypertension, edema, and proteinuria.
Additional symptoms of severe preeclampsia include hyperreflexia, cerebral and vision disturbances, and epigastric pain.
After administering magnesium sulfate to a pregnant patient for hypertension or preterm labor, the nurse should monitor the respiratory rate and deep tendon reflexes.
Eclampsia is the occurrence of seizures that aren’t caused by a cerebral disorder in a patient who has pregnancy-induced hypertension.
In a patient with preeclampsia, epigastric pain is a late symptom and requires immediate medical intervention.
In a pregnant patient, preeclampsia may progress to eclampsia, which is characterized by seizures and may lead to coma.
HELLP (hemolysis, elevated liver enzymes, and low platelets) syndrome is an unusual variation of pregnancy-induced hypertension.
Contraceptives
The failure rate of a contraceptive is determined by the experience of 100 women for 1 year. It’s expressed as pregnancies per 100 woman-years.
Before providing a specimen for a sperm count, the patient should avoid ejaculation for 48 to 72 hours.
If a patient misses two consecutive menstrual periods while taking an oral contraceptive, she should discontinue the contraceptive and take a pregnancy test.
If a patient who is taking an oral contraceptive misses a dose, she should take the pill as soon as she remembers or take two at the next scheduled interval and continue with the normal schedule.
If a patient who is taking an oral contraceptive misses two consecutive doses, she should double the dose for 2 days and then resume her normal schedule. She also should use an additional birth control method for 1 week.

0 notes
Note
09/27/2020 "WEIRD" AL'S SILENCE ON ALL SOCIAL MEDIAS, POSSIBLY BECAUSE OF HIS STATE, MAKES IT DIFFICULT TO KEEP CONSTANT REPORTS ON HIS LEVEL OF PREGNANCY. I BELIEVE AROUND NOW HIS BUMP WOULD BE VERY DIFFICULT TO HIDE FROM MOST PEOPLE, PERFECTLY ALIGNED WITH THE RAPID SPREADING OF "COVID-19" IN AMERICA. I BELIEVE FULLY IT IS A COINCIDENCE, AS BLAMING A WORLDWIDE PANDEMIC ON ONE MAN'S PREGNANCY IS FAR TOO CRAZY OF A THEORY WITH NO BACKING. ALTHOUGH I HAVE MY THOUGHTS ON THE SPREAD OF THIS VIRUS, I WILL KEEP THIS WEBSITE FOCUSED ON ONE TOPIC AND ONE TOPIC ONLY (AL'S PREGNANCY/THE EVENTUAL BIRTH OF HIS CHILD). HAVE YOU EVER FOUND IT SUSPICIOUS THAT THERE IS ABSOLUTELY NO CONCRETE EVIDENCE THAT "WEIRD AL" YANKOVIC'S WIFE WAS EVER PREGNANT, AND YET THEY HAVE A DAUGHTER? I BELIEVE THAT, ALTHOUGH HE'S BEEN PREGNANT SINCE 2015, HE WAS PREGNANT AGAIN BEFOREHAND FROM AT MOST 1988 TO HER BIRTH IN 2003. NINA YANKOVIC SHARES A STRIKING RESEMBLANCE TO HER FATHER, MORE SO THAN HER MOTHER, BECAUSE MOST OF HER FORMATION IN THE WOMB WAS THANKS TO AL'S SPERM, AND LESS SO BECAUSE OF SUZANNE YANKOVIC'S LIQUEFIED OVUM, VS IF SUZANNE HAD BEEN PREGNANT, WHICH SHE HAD CLEARLY NOT BEEN. I BELIEVE THIS EXPERIMENT BY THE GOVERNMENT, DESPITE BEING SUCCESSFUL ONCE WITH NINA YANKOVIC, IS STILL UNDER HEAVY CONSTRUCTION. I'M UNSURE WHEN THIS METHOD OF REPRODUCTION WILL BE AVAILABLE TO THE PUBLIC, OR IF IT EVER WILL, BUT PERHAPS ONE DAY, MEN OTHER THAN ALFRED WILL BE ABLE TO EXPERIENCE PREGNANCY AS WELL extra space
11/5/2020 "WEIRD" AL YANKOVIC MADE AN APPEARANCE ON ADULT SWIM'S "THE ERIC ANDRE SHOW" SEASON 5, EPISODE 3. AT 10 MNUTES AND 53 SECONDS YANKOVIC IS SEEN STATING "MY WORK HERE IS DONE.". THOUGH I DO NOT KNOW WHAT THIS IS REFERRING TO, I NOTICE THE LOWER HALF OF YANKOVIC'S BODY IS SHROUDED IN DARKNESS AS THE CAMERA QUICKLY PANS UP TO HIS FACE, ALMOST AS IF THEY WERE RECORDING ON BORROWED TIME- NEEDING TO QUICKLY DRAW THE ATTENTION AWAY FROM YANKOVIC'S BELLY AND BRINING IT TOWARD HIS FACE... THIS LEADS ME TO BELIEVE AL'S WATER IS CLOSER TO BREAKING THEN WE THINK. THIS MAY BE AN ANSWER TO THE QUESTION WE ARE ALL ASKING: IF "WEIRD" AL HAD THE TIME TO MAKE AN APPEARANCE ON "THE ERIC ANDRE SHOW", WHY WAS A FULL INTERVIEW NOT CONDUCTED? WHAT DOES AL HAVE TO HIDE FROM THE PUBLIC? THOUGH THE SHOW SEEMS TO BE A SATIRE PARODY BASED ON REAL REALITY SHOWS, QUESTIONS ARE STILL ASKED AND ANSWERS ARE STILL GIVEN. PERHAPS AL WAS WORREID HIS PREGNANCY MAY COME UP IN THE FORM OF A JOKE TOLD BY THE HOST? DUE TO MALE PREGNANCY TAKING LONGER THAN THE NORMAL FEMALE PREGNANCY (MANY YEARS) I BELIEVE IT IS SAFE TO ASSUME THE CYCLES OF PREGNANCY TAKE LONGER THEMSELVES ASWELL. WHEN AL'S WATER BREAKS, THE PAIN OF THE AMNIOTIC SACK BURSTING MAY LAST THROUGHOUT THE REST OF THIS. THE AMNIOTIC SACK IS THE FLUID-FILLED SACK THAT CONTAINS AND PROTECTS A FETUS IN THE WOMB. DUE TO "WEIRD" AL'S LACK OF A WOMB, HIS BODY HAD TO PROVIDE AN ARTIFICIAL SACK. THIS MEANS WHEN HIS SACK, OR "WATER", BREAKS, IT MAY BE ESPECIALLY PAINFUL. I BELIEVE THIS IS DUE TO HAPPEN SOON, STAY TUNED WEIRDALMPREG FANS. extra space extra space
11/15/2020 IT HAS COME TO MY ATTENTION THAT MANY VIEWERS BELIEVE THE WAY I PUNCTUATE "WEIRD" AL YANKOVIC'S NAME IS INCORRECT. I AM AWARE HIS NAME IS "WEIRD AL" YAKNOVIC (I PREVIOUSELY HAVE REFERRED TO HIM AS SUCH.). IT IS A PURPOSEFUL PLAY ON WORDS, I BELIEVE AL IS "WEIRD" DUE TO HIS MALE PREGNANCY, RATHER THAN DUE TO THE WACKY NATURE OF HIS SONGS. STAY TUNED, WEIRD ALLIES. YES. "WEIRD" AL LIES. LIES ABOUT THE STATE AND EXISTENCE OF HIS PREGNANCY. AS TIME GOES ON YANKOVIC WILL INEVITABLY NEAR THE END OF HIS UTERINE CYCLE. I BELIEVE THERE WILL BECOME A POINT THAT AL'S CHILD-BEARING STOMACH WILL GROW TOO BIG TO HIDE. NO GIRDLE OR BELT CAN HIDE THE SECRET "WEIRD" AL YANKOVIC IS HIDING FROM THE PUBLIC. KEEP YOUR EYES PEELED. extra space extra space
11/29/2020 WEIRDALMPREG NOW HAS A SUBREDDIT: https://www.reddit.com/r/WeirdAlMpreg/ . BE SURE TO SUBSCRIBE TO NEVER MISS AN UPDATE. "이상한 알" ("Weird Al" Yankovic) 얀코비치는 실험적인 남성 임신을 세상에 숨기려고 시도합니다. "WEIRD" AL 是男性怀孕的 " LIQUID OVUM "。他向人们隐瞒了他的秘密 "WEIRD" AL YANKOVIC EL MUNDO SABE QUE ESTAS EMBARAZADA
12/27/2020 I'M SURE YOU HAVE ALL REALIZED THAT I HAVE NOT BEEN UPDATING THE SITE. I REGRET TO INFORM I HAVE BEEN INFECTED WITH SOME TYPE OF VIRUS. NOT THE "CORONA" COVID-19 VIRUS, BUT SOMETHING DIFFERENT. I HAD RECEIVED SEVERAL THREATENING EMAILS FROM A POSSIBLY FAKE GOOGLE EMAIL ADDRESSES THE DAY BEFORE I FELL ILL. I SUSPECT SOMEONE MAY BE TRYING TO SILENCE ME. POSSIBLY "WEIRD" AL, OR HIS TEAM? I WILL UPDATE AGAIN WHEN I HAVE TIME. THANK YOU FOR STICKING WITH ME, "AL" THEORISTS. A LATE HAPPY HOLIDAYS TO YOU ALL.
2/12/21 FELLOW ALITES, I'M PLEASED TO ANNOUNCE THAT I HAVE BEEN INTERVIEWED BY PODCAST CREATORS "ASHES TO ASHES", FROM ALL THE WAY DOWN IN AUSTRALIA. IT FILLS ME WITH JOY KNOWING THAT OUR THEORY HAS REACHED SO FAR ACROSS THE EARTH, AND I CAN ONLY HOPE IT CONTINUES TO REACH THE EARS AND HEARTS OF PEOPLE ALL OVER THE EARTH. HAPPY FEBRUARY 12TH EVERYBODY.
3/25/2021 I APOLOGIZE FOR THE LACK OF UPDATES. AS YOU CAN SEE, OUR LAST POST WAS SCHEDULED FOR FEBRUARY 12TH, AND ONLY UPLOADED TODAY. I SUSPECT HACKERS, TROLLS, AND OTHERWISE UNTRUSTED BEINGS ARE TRYING TO HALT THE PROGRESSION OF THIS WEBSITE. I'M NOT WORRIED, AS THE SPIRIT AND WILL OF MY THEORY WILL LIVE FAR PAST THIS WEBSITE, OR THE INTERNET. DON'T LET DIRTY PEOPLE TRY TO BRING YOU DOWN. WAMP OUT.
4/16/2021 THE ARTIFICIAL ESTROGEN PUMPING THROUGH AL'S VEINS IS CONSTANTLY AT WAR WITH THE NATURAL TESTOSTERONE PRODUCED BY AL'S TESTES. ARTIFICIAL ESTROGEN IS BOTH ESSENTIAL AND NECESSARY TO HOST A WOMB. AL MAY RECIEVE HIS ESTROGEN THROUGH A NUMBER OF METHODS; ESTROGEN CAN BE INGESTED VIA PILL, GEL, SHOT, OR PATCHES. IT IS CURRENTLY NOT KNOWN HOW MUCH ESTROGEN AL NEEDS TO HOST HIS WOMB. IT IS POSSIBLE THAT AL IS IN CONSTANT NEED OF ESTROGEN AND GETS HIS "FIX" THROUGH DESCRETE ESTROGEN PATCHES APPLIED TO OUT OF SIGHT AREAS SUCH AS THE UNDERARMS, THIGHS, BUTTOCK, OR BACK IN ORDER TO HIDE HIS BIG SECRET.
5/28/2021 RECENTLY, "WEIRD" AL YANKOVIC, AKA ""@alyankovic" ON TWITTER HAS POSTED SEVERAL "TWEETS" ABOUT FOOD. THE FIRST, POSTED ON 05/09/2021 BEARS AN IMAGE OF "PULLED PORK LEMONADE" WITH THE CAPTION "Ugh, my least favorite flavor.". THIS STRANGE FLAVOR COMBINATION MAY BE DUE TO PREGNANCY CRAVINGS, A PHENOMENON WHICH NATURALLY OCCURS IN WOMEN AS EARLY AS 5 WEEKS INTO PREGNANCY. DUE TO THE NATURE OF AL'S PREGNANCY, THIS EFFECT AND MANY OTHERS THROUGHTOUT HIS PREGNANCY MAY BE DELAYED. THOUGH I CANNOT CONFIRM IF AL IS REFERRING TO HIS PREGNANCY CRAVINGS, IT IS HIGHLY LIKELY.
6/17/2021 DUE TO SEVERAL ISSUES WITH MY SITE HOSTING, THE LAST TWO "WEIRD" AL MALE PREGNANCY UPDATES FAILED TO UPLOAD. I APOLOGIZE FOR THIS. BIG CHANGES WILL BE COMING TO WWW.WEIRDALMPREG.COM . STAY TUNED.
6/17/2021 (1:43 AM) @alyankovic ON TWITTER.COM POSTED A PHOTOGRAPH OF THE PASTRY KNOWN AS RASPBERRY BEIGNETS. TITLED "The kind youfind in a second hand store?". THOUGH I AM NOT SURE IF THIS IS A REFERENCE TO ONE OF "WEIRD" AL'S SONGS, I AM SURE THAT THE INGREDIENTS USED TO HARBOR AL'S WOMB (AS WELL AS THE PROCESS OF PREGNANCY) ARE CAUSING PREGNANCY FOOD CRAVINGS. THE AVERAGE 60 YEAR OLD WOULD NOT BE CRAVING PASTRIES AT NEARLY 2 IN THE MORNING, BUT, THE AVERAGE PREGNANT WOMAN OR MAN MAY FIND A 2:00 AM SNACK ALLURING DUE TO PREGNANCY CRAVINGS.
8/23/2021 IVE DISCOVERED TODAY, OF RECENT "WEIRD AL" MERCHANDISING. ONE OF WHICH SHOWS MR. YANKOVIC STANDING, ENLARGED HEAD, WITH AN ACCORDION TO COVER HIS ABDOMEN. THE OTHER, A "SIMPSONS" BRAND FIGURE, YELLOWED SKIN AND GREEN SHIRT, ACCORDION ALSO CONVENIENTLY HELD AT HIS LOWER ABDOMEN. I BELIEVE AL, IN AN ATTEMPT TO STAY TRUTHFUL TO HIS FANS, MADE HIS MERCHANDISE "CENSOR" HIS SWOLLEN TUMMY. I WILL NOTE THAT THE "SIMPSONS" FIGURE HAS A REMOVABLE ACCORDION, BUT IT COULD BE THE FAULT OF THE COMPANY, WHICH MR. YANKOVIC MAY NOT HAVE HAD CONTROL OVER. THE AVERAGE FEMALE'S STOMACH EXPANDS GREATLY THROUGHOUT PREGNANCY. THOUGH THE NATURES OF MALE PREGNANCY ARE MYSTERIOUS AND UNKNOWN, IT IS SAFE TO ASSUME THAT IF AL IS HARBORING A SINGLE CHILD, HIS STOMACH-GROWTH-RATE WOULD BE THAT OF A NORMAL HUMAN WOMAN. THE DIRECT CENSORSHIP OF OLD MAN ALFRED'S STOMACH SHOWS THAT "WEIRD" AL HAS SOMETHING TO HIDE.
8/24/2021 BE SURE TO FOLLOW THE OFFICIAL WEIRD AL MPREG TWITTER ACCOUNT https://twitter.com/weirdalmpreg
QUESTION AND ANSWER - 8/30/2021
QUESTION: "Why was "Weird Al" Yankovic not featured on Kanye West's #DONDA"?
ANSWER: THERE ARE MANY POSSIBILITIES. IT US UNSAFE FOR PREGNANT PEOPLE TO TRAVEL WITH THE RECENT SURGE OF THE DELTA VARIANT. ANOTHER MAY BE THAT THE FELLOW CELEBRITIES DO NOT APPROVE OF HIS MALE PREGNANCY.
QUESTION: "When's the baby coming?"
ANSWER: IT IS UNKNOWN. MALE PREGNANCY IS EXPERIMENTAL AND MAY TAKE SEVERAL MORE YEARS TO COME TO COMPLETION. THERE IS EVIDENCE OF AL'S PREGNANCY DATING AS FAR AS 2014.
QUESTION: "Is it[AL'S FUTURE BABY] gonna be a girl or a boy?"
ANSWER: THE GENDER OF AL'S FUTURE SPAWN IS UNKNOWN. ONLY TIME WILL TELL.
QUESTION: "Why"
ANSWER: THOUGH I CANNOT SPEAK FOR AL HIMSELF, THERE ARE MANY POSSIBLE REASONS. TO ADVANCE THE TECHNOLOGY, PERSONAL GAINS, TO EXPERIENCE THE JOYS OF PREGNANCY, OR POSSIBLY, TO FURTHER ENHANCE HIS "WEIRD" STATUS. >
8/27/2022 IT IS NO SECRET THAT "WEIRD" AL YANKOVIC HIDES HIS MALE PREGNANCY FROM THE POPULUS. WE HAVE KNOWN THIS FOR QUITE SOME TIME- AND SO HAVE THE CELEBRITIES. WE KNOW THAT AL'S COHORTS ARE AWARE OF HIS PREGNANCY, BUT HE HIDES IN THE SHADOWS, KNOWING THE MEDIA WILL SHUN HIM... BRYAN CRANSTON AND AARON PAUL, STARS OF "BREAKING BAD" KNOW AL'S SECRET, AND SO DO YOU. YANKOVIC'S ATTEMPTS TO HIDE HIS ABDOMEN ARE MADE EVIDENT IN ALMOST EVERY PHOTOOGRAPH OF ALFRED YANKOVIC. IN SOME WAY, HE OBSTRUCTS HIS ABDOMEN, OR "BELLY". BELOW ARE SEVERAL PHOTOS OF "WEIRD AL" YANKOVIC (NOT BEFORE POSTED ON THIS SITE) WHERE HE OBSTRUCTS HIS ABDOMEN. YANKOVIC HAS ALWAYS HAD A TENDENCY TO OBSTRUCT HIS ABDOMEN IN PHOTOS AND WHEN ON STAGE. COMMONLY SEEN PLAYING THE ACCORDION, COULD IT BE A FRONT TO HIDE MALE PREGNANCY? PERHAPS THE VIBRATIONS HAVE DAMAGED THE TECHONOLGY WITHIN AL, GIVING REASON TO HIS PROLONGED STATE OF PRENGNACY. AS AL CONTINUES HIS TOUR ACROSS THE UNITED STATES, MORE AND MORE VIEWERS REPORT HE WAS SITTING THE ENTIRE SHOW, AND THAT HE ATTEMPED TO HIDE HIS BELLY. "WEIRD AL" YANKOVIC, WE BEG YOU >
9/11/2022: THERE ARE MANY FACTORS THAT PLAY INTO THE "WEIRD" AL MALE PREGNANCY THEORY. FIRST: WE HAVE SEEN AL'S BUMP! THROUGHOUT THE YEARS, AL'S STOMACH HAS BEEN EXPANDING AT A RAPID RATE. MOST NOW KNOW THAT EXPERIMENTAL MALE PREGNANCY TAKES FAR LONGER THAN THE AVERAGE FEMALE PREGNANCY, AT THIS RATE, IT IS MY PROFESSIONAL OPINION THAT A MALE PREGNANCY IS AT LEAST 12x A FEMALE PREGNANCY (MEANING A MALE PREGNANCY TAKES 9 YEARS AS OPPOSED TO THE FEMALE 9 MONTHS) . THE EARLIEST ACCOUNT OF "WEIRD AL" YANKOVIC'S MALE PREGNANCY ACCORDING TO WWW.WEIRDALMPREG.COM IS 2014. THE 9TH YEAR IS APPROACHING. SECOND: YANKOVIC HAS REFERENCED MALE PREGNANCY THROUGHOUT HIS LIFE. IN YANKOVICS SONGS HE REVEALS HIS SECRET: A MALE PREGNANCY. POINTING TO PHOTOS OF HIMSELF ASKING "ARE YOU PREGNANT?" THE IDEA OF A PREGNANCY IN YANKOVIC IS NOT UNIQUE TO THIS BLOG... FANS HAVE TAKEN IT AMONG THEMSELVES TO CREATE WEIRD AL STYLE PARODY VIDEOS SUCH AS "Oops Im Pregnant Again" PUBLISHED 2008, SEVERAL YEARS BEFORE THE FIRST SIGHTING OF ALFRED'S BABY BUMP. THIRD: WEIRD AL YANKOVIC ABSTAINS FROM DRUGS AND ALCOHOL, MAKING HIM THE PERFECT HOST. DOING THIS MAKES HIS BODY PURE, AND ABLE TO GROW A PERFECT WOMB TO HOST HIS "LITTLE YANKOVIC JR." WITHOUT COMPLICATIONS. FOURTH: FANS OF YANKOVIC HAVE NOTICED THAT ALONG HIS TOUR YANKOVIC HAS PERFORMED SITTING SEVERAL TIMES. YANKOVIC HAS RELEASED A MOVIE ABOUT HIS LIFE WITHOUT APPEARING IN IT HIMSELF POSSIBLY DUE TO HIDING HIS SECRET MALE PREGNANCY. PREGNANCY TAKES A TOLL ON A BODY, IF AN ARTIFICIAL MALE PREGNANCY TAKES LONGER THAN THAT OF A FEMALE, IT CAN BE ASSUMED THAT THE STRAIN PUT ON THE BODY IS ALSO 12x MORE. COMING SOON: "Weird[AND PREGNANT!?]: The Al Yankovic Story"
11/4/2022: WHILE PERUSING A “WEIRD AL” FANS FACEBOOK PAGE, I STUMBLED UPON A COMMENT BY ONE EMILY T. SHE DETAILS HER EXPERIENCE AT ONE OF YANKOVIC’S RECENT SHOWS, SAYING DURING THE MEET AND GREET, YANKOVIC WAS CONCEALED BEHIND AN OPAQUE PLASTIC SCREEN. QUOTE “Sitting the whole time…”. IF YOU ARE A LONGITME READER OF MY BLOG, YOU WOULD AGREE IT IS SAFE TO SAY THAT THIS IS A POOR ATTEMPT AT CONCEALING “WEIRD AL” YANKOVIC’S EXPERIMENTAL MALE PREGNANCY. WHAT DOES YANKOVIC HAVE TO HIDE THAT HE NEED COWER BEHIND A PLASTIC CURTAIN WHILE TAKING PHOTOS WITH FANS? HE DOES NOT WANT US GETTING CLOSE. THIS PROCESS GIVES AL AN EXCUSE TO HAVE HIS BELLY PHOTOSHOPPED OUT. BELOW IS EMILY’S EXPERIENCE “MEETING AND GREETING” WEIRD AL” "이상한 알" ("Weird Al" Yankovic) 얀코비치는 실험적인 남성 임신을 세상에 숨기려고 시도합니다. "WEIRD" AL 是男性怀孕的 " LIQUID OVUM "。他向人们隐瞒了他的秘密
Thank you Kelsey
0 notes
Text
How Many Cycles of IVF Might Be Needed to Achieve Pregnancy?
In vitro fertilization (IVF) has revolutionized the field of reproductive medicine, offering hope to countless couples struggling with infertility. However, one of the most common questions prospective patients ask is, "How many cycles of IVF might be needed to achieve pregnancy?" The answer to this question can vary significantly depending on several factors. At Ovum Hospital, one of the leading IVF hospitals in Bangalore, we aim to provide comprehensive care and personalized treatment plans to maximize your chances of success.
Understanding IVF Success Rates
IVF success rates are influenced by a multitude of factors, including age, fertility issues, lifestyle, and the quality of the IVF clinic. It's important to recognize that while some couples may achieve pregnancy on their first cycle, others might require multiple attempts.
Age: Age is one of the most critical factors affecting IVF success. Women under 35 tend to have higher success rates, with about 40-50% achieving pregnancy per cycle. This rate decreases as age increases, with women over 40 experiencing significantly lower success rates, often around 10-20% per cycle.
Fertility Issues: The underlying cause of infertility also plays a significant role. Factors such as the quality of eggs and sperm, uterine health, and any underlying medical conditions can affect the success of IVF. At Ovum Hospital, our specialists conduct thorough evaluations to address these issues effectively.
Lifestyle Factors: Lifestyle choices, including diet, exercise, and habits like smoking and alcohol consumption, can impact IVF outcomes. Maintaining a healthy lifestyle can improve the chances of a successful pregnancy.
Clinic Quality: The expertise of the medical team and the quality of the IVF clinic are crucial. Ovum Hospital, recognized as one of the top IVF hospitals in Bangalore, employs state-of-the-art technology and experienced professionals to enhance success rates.
How Many Cycles Might Be Needed?
Given the variability in individual circumstances, it's challenging to predict precisely how many IVF cycles a couple might need. However, statistical data and clinical experience provide some insights:
First Cycle Success: Approximately 30-40% of couples may achieve pregnancy on their first IVF cycle. This percentage is higher for younger women and those with no significant fertility issues.
Cumulative Success Rates: Success rates improve with multiple cycles. After three cycles, the cumulative success rate for women under 35 can reach up to 60-70%. This is because each cycle provides additional opportunities for a successful implantation.
Persistence Pays Off: Research indicates that many couples who persist with IVF for up to six cycles eventually achieve pregnancy. The cumulative success rate can be as high as 80-90% over multiple cycles, highlighting the importance of perseverance.
Factors Influencing the Number of Cycles Needed
Several factors can influence the number of IVF cycles required:
Egg and Embryo Quality: High-quality eggs and embryos increase the likelihood of successful implantation. Techniques such as preimplantation genetic testing (PGT) can help identify the healthiest embryos for transfer.
Response to Treatment: The body's response to ovarian stimulation varies among individuals. Some women may produce multiple high-quality eggs in one cycle, while others may require several cycles to achieve the same result.
Uterine Receptivity: The ability of the uterus to accept and nurture an embryo is vital. Issues such as uterine abnormalities or endometrial lining problems can affect implantation success. Treatments to improve uterine receptivity may be necessary.
Male Factor Infertility: In cases where male factor infertility is present, the quality of sperm can impact the number of cycles needed. Advanced techniques like intracytoplasmic sperm injection (ICSI) can enhance the chances of success.
Overall Health: General health and well-being, including the management of any underlying medical conditions, play a role in IVF success. Comprehensive pre-treatment evaluations are essential to optimize health before beginning IVF.
Emotional and Financial Considerations
The emotional and financial aspects of undergoing multiple IVF cycles cannot be overlooked. IVF can be a stressful and costly process. It's important for couples to have realistic expectations and to seek support from healthcare providers, counselors, and support groups.
At Ovum Hospital, one of the premier IVF hospitals in Bangalore, we understand these challenges. We provide compassionate care, transparent communication, and flexible financial options to support our patients throughout their IVF journey.
Conclusion
The number of IVF cycles needed to achieve pregnancy varies widely among couples. While some may experience success on their first attempt, others may require multiple cycles. Factors such as age, fertility issues, lifestyle, and clinic quality all play significant roles in determining the outcome.
At Ovum Hospital, we are committed to helping our patients navigate their IVF journey with expertise and empathy. As one of the leading IVF hospitals in Bangalore, we combine advanced technology, personalized care, and a supportive environment to maximize your chances of success. If you are considering IVF, we encourage you to consult with our experienced team to develop a tailored treatment plan that meets your unique needs and goals. Together, we can work towards achieving the dream of parenthood.
0 notes
Text
What is Ovulation?
₊˚ ‿︵‿︵‿︵୨୧ · · ♡ · · ୨୧‿︵‿︵‿︵ ˚₊
Ovulation is a phase in the menstrual cycle where your ovary releases an egg
Within day 6 and 14 of the menstrual cycle, follicles (small sacs of fluid in the ovaries that contain a developing egg) begin to develop
During the 10-14 day of the menstrual cycle, one of the developing follicles forms a mature egg.
Around day 14 of the menstrual cycle, the egg is released from the ovary: Ovulation
- After ovulation, the uterus is prepared for pregnancy
- The egg travels to the fallopian tube, where it will meet sperm for fertilization
The menstrual cycle begins from the first day your period starts. It usually consists of 28 days.
- Average 7 days for menstruation
- Average 12 days after for fertility
- Average 9 days after for infertility
₊˚ ‿︵‿︵‿︵୨୧ · · ♡ · · ୨୧‿︵‿︵‿︵ ˚₊
Ovulation is not the only time you can get pregnant…
- You can get pregnant as soon as your period ends up until the infertile period (at the end of the cycle)
When ovulation occurs and when the menstrual cycle takes its course is different for everyone.
The best way to track this is through a menstrual cycle app or ovulation tests (they tell you if you are ovulating)
₊˚ ‿︵‿︵‿︵୨୧ · · ♡ · · ୨୧‿︵‿︵‿︵ ˚₊
Sources:


#menstrual health#women’s health#reproductive health#health#health and wellness#pregnancy#menstruation#menstrual cycle#period cramps#period#gynecology#gynecological health#feminism#femaledaily#female beauty#women#woman
1 note
·
View note
Text
Ethical and Legal Considerations in Assisted Reproduction
Infertility is regarded as a health problem, and it affects approximately 8%–10% of couples worldwide.
It has become a significant concern worldwide, and the following are the reasons behind it:
Hormonal imbalance
Excessive alcohol consumption
Smoking and using tobacco products
Substance abuse
Exposure to environmental toxins
Over-exercising
Radiation therapy or chemotherapy
Sexually transmitted infections (STIs)
Having obesity or being underweight
Chronic conditions and diseases
Age (For women in their late 30s or 40s, it is difficult to conceive, and for men, it’s 50 years).
The above listed are just a few reasons people fail to conceive.
But here comes the solution: Assisted Reproduction, which is a blessing for couples who struggle to conceive.
It all started at the end of the 18th century when artificial insemination with a man's semen was tried. After that, the advancement in assisted reproduction never took a back seat, and by the second half of the 20th century, two major technological advances came into existence: gamete freezing and in vitro fertilization (IVF).
We are all aware of how popular IVF has become today.
But do you know that these practices are currently accepted only in certain countries and communities and have generated new debates and challenges for doctors, lawmakers, and society at large?
Yes! Because few people or groups are misusing these technologies.
While assisted reproductive technology (ART) has given hope to millions of couples suffering from infertility, it has also introduced countless ethical concerns along with legal and social challenges.
However, to cope with these ethical issues in in-vitro fertilisation and other assisted reproduction techniques, guidelines have been developed by the different nations as per their standards.
But still, governments need to work on many ethical considerations.
Moving forward in this article, we will discuss a few ethical and legal issues with Assisted Reproduction technology:
Ethical Issues
Disposal of Surplus Embryo
Multiple implantations
Selective Reduction
Access of Assisted Reproduction technology to postmenopausal women
The above-listed concerns are not restricted to one nation. But to all the places where these processes are in practice.
From the non-consensual donation of embryos to the Disposal of embryos, all the above-listed points are ethically disconcerting, particularly to those who believe that protected human life commences at conception.
Legal Issues
Paternity disputes in cases of no written consent from another partner.
Disputes can also arise over the fate of cryopreserved gametes and embryos.
Unregulated surrogacy.
Disputes between ART practitioners and the patients they serve.
All the above legal and ethical issues are quite serious. Although governments are trying to resolve these issues, the reality is this subject needs regular updation of regulations based on the situation.
The following are the few considerations that need to be taken care of.
Ethical & Legal Consideration in ART
Clinics should be registered or supervised by the state accreditation.
Legal Guidance should be Clear.
It is essential to ensure that children's rights are built into standards from the beginning so that legal advocacy is avoided later on.
In a surrogacy agreement, each party is to state their intentions and their responsibilities to one another.
The surrogacy agreement should also cover the following medical issues: abortion, selective reduction, medical emergencies, embryo transfers, and most importantly, the surrogate's health care.
Sperm or ovum donors' consent should be a must for lawful donation.
These are just a few considerations that are important to understand for both patients and the doctor.
Our infertility online course can be a great help for students interested in improving their diagnostic capabilities and medical skills for managing patients with infertility and enhancing their knowledge of IUI techniques.
Enroll in Our online course Now!
We will cover the basics of infertility & IUI because if your basics are clear, you will master the art of focusing on the practical and clinical aspects of infertility and IUI.
This course compiled infertility & iui video lectures to help you understand things better.
Moreover, we provide concise notes to help the candidates review the main points covered during the lectures.
In short, by pursuing this course, individuals can improve their diagnostic capabilities and medical skills for managing infertility patients and enhance their knowledge of IUI techniques.
#basics of infertility & iui#infertility online course#iui online course#infertility & iui video lectures#ethical issues#ethical issues in in-vitro fertilization#legal issues with assisted reproductive technology#ethical concerns#ethical considerations
0 notes
Text
《wjk》入荷情報。10/18
おはようございます。
本日は、wjk(2024秋冬)から新型のデニムシリーズが
入荷致しましたので、お知らせいたします。
《wjk》tight straight selvedge denim
(5182dn88/used)46,200円(税込)

《wjk》tight straight selvedge denim / ow
(5182dn87/indigo)35,200円(税込)

《wjk》tight straight selvedge denim / black
(5182dn87/indigo)35,200円(税込)

ストレッチの効いた12.5ozセルビッチデニムを使用したシリーズ。
あらゆるスタイリングに汎用性を持つ、タイトストレートシルエットを構築。ヴィンテージデニムを採用することで、流行にとらわれない長年にわたって愛用出来る一本に仕上げた。
・ 過度なデザインは設けず、素材やシルエットの良さを強調。
・シャトル織機によって丁寧に時間をかけて織ることで、表面に凹凸感のあるふっくらとした風合いを出している。
・またユーズド色は、50年代から続く岡山「井原」の職人のシェービングやダメージ、リペアなどの技術をwjkの感性を通して構築した加工。
商品詳細は、店頭・オンラインストアでご確認ください。
wjk(商品一覧)
取扱店舗:OVUM
《wjk》入荷情報。10/18
0 notes