#medical morphine market
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs




Fun Fact
Tumblr is used by 21% of adults online aged 18-29 years.
Text
The Medical Morphine Market: Trends, Challenges, and Future Outlook
Morphine, a potent opiate analgesic, is a cornerstone in pain management, especially for severe and chronic pain conditions. Derived from the opium poppy, this powerful narcotic has been utilized for centuries to alleviate pain. In the modern medical landscape, morphine's role has evolved, and its market dynamics reflect a complex interplay of medical necessity, regulatory scrutiny, and societal challenges.
Market Overview
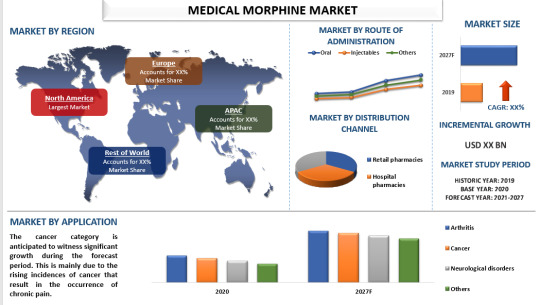
The global medical morphine market is driven by the increasing prevalence of chronic pain conditions, cancer-related pain, and post-surgical pain. As of 2023, the market was valued at approximately USD 13 billion and is expected to grow at a compound annual growth rate (CAGR) of around 3.5% over the next five years. The demand for morphine in pain management, especially in palliative care, continues to be robust, underscoring its essential role in modern medicine.
Key Drivers
1. Rising Prevalence of Chronic Diseases: The increase in chronic illnesses such as cancer, arthritis, and neurodegenerative diseases has led to a higher demand for effective pain management solutions. Morphine, with its efficacy in managing severe pain, remains a preferred choice among healthcare providers.
2. Aging Population: The global increase in the aging population, who are more susceptible to chronic pain and conditions requiring surgical interventions, fuels the demand for morphine. Older adults often experience complex pain conditions that necessitate strong analgesics like morphine.
3. Advancements in Drug Delivery Systems: Innovations in drug delivery systems, such as controlled-release formulations and transdermal patches, have improved the efficacy and safety profile of morphine. These advancements help in maintaining steady plasma levels of the drug, thereby enhancing pain relief and reducing side effects.
4. Government and Institutional Support: Various health organizations and governments advocate for improved pain management protocols. For instance, the World Health Organization (WHO) has been promoting the accessibility of essential medications, including morphine, in palliative care.
For a comprehensive analysis of the market drivers, visit https://univdatos.com/report/medical-morphine-market/
Challenges
Despite its critical role, the medical morphine market faces significant challenges:
1. Regulatory Hurdles: Stringent regulations regarding the production, distribution, and prescription of morphine to curb misuse and addiction pose significant barriers. Regulatory bodies like the FDA and EMA impose rigorous controls, which can delay the approval of new formulations and impact market growth.
2. Opioid Crisis: The ongoing opioid epidemic, particularly in North America, has cast a shadow over the use of opioids, including morphine. The fear of addiction and overdose has led to a more cautious approach among healthcare providers, impacting prescription rates.
3. Supply Chain Issues: The cultivation of opium poppies, necessary for morphine production, is susceptible to geopolitical factors and agricultural challenges. This can lead to supply chain disruptions and affect the availability of morphine.
4. Public Perception: The stigma associated with opioid use, driven by the opioid crisis, has led to a negative perception of morphine. This affects patient acceptance and adherence to morphine-based treatments.
Regional Insights
The medical morphine market exhibits regional variations. North America remains a significant market due to high healthcare expenditure, advanced healthcare infrastructure, and a high prevalence of chronic pain conditions. However, the stringent regulatory environment and the opioid crisis have tempered growth prospects.
In contrast, the Asia-Pacific region is witnessing rapid market growth, driven by an increasing geriatric population, rising healthcare spending, and improving healthcare infrastructure. Countries like India and China are emerging as key markets, with growing awareness and acceptance of pain management therapies.
For a sample report, visit https://univdatos.com/get-a-free-sample-form-php/?product_id=22715
Future Outlook
The future of the medical morphine market lies in balancing the benefits of morphine for pain management with the need to mitigate risks associated with opioid use. Continued advancements in drug delivery systems, coupled with comprehensive pain management protocols, will enhance the therapeutic efficacy and safety of morphine.
Additionally, ongoing research into non-addictive analgesics and alternative pain management strategies could complement the use of morphine, addressing the concerns related to addiction and misuse. Policymakers and healthcare providers must work collaboratively to ensure that patients have access to effective pain relief while minimizing the potential for abuse.
Conclusion
The medical morphine market remains a vital component of the global healthcare landscape, providing essential pain relief for millions of patients. Navigating the challenges posed by regulatory scrutiny and public perception, while leveraging technological advancements, will be crucial in shaping the future of this market. As healthcare systems evolve, the role of morphine in pain management will continue to be pivotal, albeit within a framework that prioritizes patient safety and effective pain control.
Contact Us:
UnivDatos Market Insights
Email - [email protected]
Contact Number - +1 9782263411x
Website -www.univdatos.com
#Medical Morphine Market#Medical Morphine Market Size#Medical Morphine Market Growth#Medical Morphine Market Forecast
0 notes
Text
I think people over seventy years old should have unrestricted access to prescription painkillers. Not to take home or anything (they might get sold or stolen, although frankly I think pain meds should be less regulated in general and the fact that such a market exists for that is a sign that they're over-restricted in the first place) but like, they should be able to show up at the hospital and flash their ID and be like "morphine please" and have a nurse shoot them up then and there. Yes this is about my stepfather who had every health problem and finally became a tolerable human being after he was put on constant pain management medication but also if you're over 70 you know how your own body works and what pain feels like and frankly if you throw away your life to a painkiller addiction at that age (way less rare than the media would have you think, most "abusers" of painkillers are self-medicating *to manage their pain that they're not being prescribed enough medication for*) then all the more power to you.
19K notes
·
View notes
Note
i had once a weird idea.
y'know, the Rainwing healers use those weird berries I forgot the name of to calm/anesthetize their patients, resulting from hallucinations. which makes me think of the use of morphine in our irl human medical field. this is basically like drugs, isn't ? even if there is no dependence on these substances mentioned, it shows some similarities so ....
hear me out: Rainwing drug cartel. black market in hallucinogenic berries with other tribes.
this is obviouslyb not serious. just thought it would be funny.
why is this actually so real 😭😭😭
25 notes
·
View notes
Text
Forgive Your Heart
Chapter 1: The Encounter
Summary: Nevarro was never a place for surprises after you had come accustomed to it's unyielding atmosphere of danger, however a small green child just might change your view on this planet.
A/n: I've seen so many fics that often either poorly portray chubby bodies or just make the readers thin and dainty and so I'm taking matters into my own hands. :)
I have watched all of the Mandalorian but not many Star Wars movies so excuse me if I use improper lingo but I will do my best to research things I'm not sure of.
Masterlist

Nevarro was a shithole. That was known not only throughout the planet but throughout the outer rim, it was where they needed your help the most, that's why you’re here. Being a medic was never going to be easy no matter what planet you decided to work on, but Nevarro was another level of filth. The bounties, the bounty hunters, thieves, scammers etc. were all on Nevaro, you cursed your kind and giving heart, you wanted to give what you could see people thrive in this decrepit place. Constant blaster shot cases and near dead bounties were never uncommon at your Medcenter, it’s practically what kept the lights on in the place, and being the head medic of your station made the atmosphere much more daunting.
Snapping out of your daze and drawing your attention to a shouting patient, and making your way over to see what the fuss was about. He was yelling on and on about someone getting away that ‘I’m gonna kill that son of a bitch!’ and ‘He’ll never get off this planet alive!’ a male bounty hunter from the looks of it, various weapons and ammunition hanging off his struggling body to get off the gurney one of your Medics was pinning him down on. As you slightly jogged alongside the gurney making your way to the operating table, you put your hand on the man's shoulder pushing him against the gurney making his head jerk your way. You needed to stay calm.
“Sir, we need you to take some deep breaths and calm down so we can do our job.”
“To hell with your job! That bastard’s gonna die! Today!”
When you tried to speak again the man tried and failed to knock you and your medic to the ground, you yelled for assistance from passing medics asking them to get and IV started while you held his arm down as well as getting 20mg of morphine to try and calm the man down. You pinned down his arm with the help of the other medics, he writhed under your grasp as the IV was inserted into his arm, the morphine quickly made its way through his body helping calm his nerves and lessen his pain. As you entered the operating room you were greeted by the head medic of the trauma unit.
“I’ll take care of this, you’ve done plenty already by drugging my patient.”
“Hey, if i hadn-”
You were cut off by the operating door before you could finish your defense, your fists balled tightly at your sides as you walked down the hallway leading back to the medic station. You noticed something odd, it looked like a burlap sack you’d take with you to the market. You made your way closer and noticed the sack sprouted two long green ears, was this someone's kid? Once you had reached the child you knelt down with an outstretched hand and spoke in a soft voice.
“Are you lost hun? Do you need help finding your parents?”
Two massive black eyes stared back at you when the child turned around, you had never seen anyone like him, he only stared at you and looked down at the ends of his robe that draped on the ground. The hallway was getting busier as you stayed there in the middle of it, you gently scooped up the kid and made your way to the side of the hallway out of everyone's way. He gripped your lab coat and whined out, something clicked in you, vaguely you could hear a voice in your head. Hurt. You looked at the child and he stared back at you once again, you noticed he only held your jacket with one of his clawed hands, carefully you took his small hand in yours and examined it. A simple cut, something that could’ve been fixed at his home with a med patch, maybe he thought it was a bigger cut than it is?
“Let’s get this taken care of, yeah? You wanna choose a cool med patch?”
You began listing all the cool patterns of kids' med patches to him, rocket ships, rainbows, camouflage, glitter etc. Entering the supply closet with the little green child in your arms you dug out the med patches you had listed and held them out for him to choose from, you’d have to cut them down to his size of course, he was so tiny you couldn’t help but feel a bit protective over him even if it had been only two minutes since you met him. His big eye scanned over the patches his eyes landed on a patch that had droids in a pattern with a blue background. He pointed at the same patch and looked up at you with a little grin, another vague voice ran through your head, Him. You let a warm smile grace your features, handing the patch to him to hold and putting the rest away, you make your way into a vacant examination room and shut the door. Setting the child on the cot and turning around to pull the scissors out of your pocket to cut the patch to fit his tiny hand. Moving across the cot to sit on the rolling stool, you held out your hand silently asking for permission to see the cut, he placed his hand back into yours. You placed the patch onto his hand and let out a disappointed sigh.
“Hang on, I have to cut it a bit smaller buddy, your hands are so small I have to make sure it fits properly. ”
Taking the patch back you once again cut off slivers so it would fit his small hand, you took off the plastic backing of the patch and firmly placed the sticky side against his skin. You ran your hand around the border of it to ensure it was secure on his hand. He looked up at you and cooed, that voice made its way in your head, Kind. You gave his head a simple pat and rubbed his cheek as you stood.
“How about you stay here for a bit ok? I’ll see if I can find your parents.”
He gripped the bottom portion of your lab coat and looked up at you, he seemed agitated Dangerous. The voice was a bit louder this time you could feel anxiety in the voice, was he doing this? Does he know he can? You set your hand on his head once more, smiling down at him and pulling the blanket on the cot closer to him, making a small nest for him to comfortably lay in. He still held your wrist, not wanting you to leave, but you still can’t tell if he’s scared for you or for himself.
“It’ll be ok, I promise sugar. I’ll be back in a few minutes. How about that?”
Slowly he let your wrist go, as you made your way out of the room you mentioned again you'd be right back and closed the door. You quickly made your way back to your computer at the medic station, searching through files and profiles of all patients and employees. You had searched for nearly 10 minutes before rolling away from the desk and running your hands over your face with a defeated sigh. You raked your hands through your hair and scanned the people coming and going through the hallways, your eyes landed on an armor clad figure, the T shaped visor already pointed at you. A Mandalorian? He made his way over to you, parting the crowd with little effort. You stood and made your way around the desk to meet the beskar clad man, you had a feeling in your gut but couldn’t tell if it was to run or to trust him. His body language was clearly agitated, balled fists at his sides, looking through the crowd almost frantically. He tilted his head down to meet your gaze.
“Can I help you with something?”
“WheR- s K-d”
“Excuse me?”
He hit the side of his helmet harshly, seeming to fix some malfunction with his hardware. At the same time the Mandalorian grabbed your collar and held you close to him by your lab coat, his stature was intimidating but you never let that faze you. You held your ground and kept your stare even and brows furrowed, his fist tightened noticing your lack of fear.
“I said, where's the kid?”
#mando x reader#the mandaloria/reader#the mandalorian#star wars#reader insert#chubby reader#mandalorian x chubby reader#idontknowimnewatthis#someonehelpme#medic reader
37 notes
·
View notes
Text
Opiate rant
It boggles my mind how much time, effort and resources the medical industrial complex puts into pain relief research when we got it right with opium and morphine a hundred goddamn years ago. Are they desirable for everyone? No. But instead of trying to meet the needs of people with complex or difficult to treat pain conditions, the pharmaceutical industry is desperately trying to create alternatives for people that wouldn’t need alternatives with decriminalization, education and home synthesis rights.
The average relationship to opiates in the so-called US is not what it could be. It’s extremely hard to manage physical dependency when your supply is inconsistent and you have to spend half a batch trying to get a handle on how strong your shit is and then have to start over with a completely different batch a week or two or three later–to say nothing of how impossible it can feel to schedule tolerance breaks or plan ahead to manage how fast your tolerance builds when you don’t know where your next fix (or the money for it) is going to come from. Black market pressure (especially how drug penalties are calculated) prioritizes the most potent possible substances in the smallest physical quantity, meaning lots of people are forced to take doses much higher than what they would otherwise need or find desirable, causing tolerance to build very rapidly and be difficult to control. AVOIDABLE gastrointestinal problems, malnourishment, and infection run rampant because our culture teaches drug users that these are punishments for immorality, not simple side effects and risk factors that can be dealt with through drug-user-specific health education and care.
How many people would live happy, desirable lives–fuck it, how many people would STILL BE ALIVE RIGHT NOW if they had the option to use safely produced, content-guaranteed, consistently-dosable opiates? How many people are suffering on non-indicated ineffective gabapentin prescriptions when their pain could be easily, safely managed with opiates? How many people lose years of their life to antipsychotics and SSRIs when a week or two of opium tea could’ve been all they needed to get through that rough patch, cope with that death, keep that awful event from becoming a life-long trauma?
What would happen if instead of choosing between pain and fentanyl-cut who-knows-what, you could plant some poppies in your back garden and have next-to-free access to effective relief? If instead of shelling out for pharmaceutical pills that could just as easily be cut you could make your own or get them from a farmers market stall or your friend in the corner house with the big lot and know exactly what was in them and how they were made? If you could go to any doctor or community healer or medic or harm reductionist or WHOEVER and get customized, experienced, well-thought out advice on a dosage and tolerance management plan, on food habits and options to help with suppressed appetite and potential GI problems, recommendations for supplements or medications to limit or eliminate GI distress, fresh needles and rigs or glassware and injection training and wound-care supplies and instructions, supplements and medications and exercises/habits to limit lung damage from smoking…
No more ruinous addictions. No more ulcers from tainted supplies or trying to disinfect wounds with hand sanitizer and mouthwash. No more avoidable pain and emotional distress. No more emotional and physical damage from using intense substances without knowing how strong they are or what effects they might have. NO. MORE. FUCKING. DEATHS.
Opium is exceptionally easy to produce–morphine and heroin are more complicated, but we’ve been making them for a long time prior to modern industrial labs and the basic chemistry knowledge and equipment needed for safe production could be 100% achievable to just about anyone. The harm reduction and side effect management are THERE, they’re just obfuscated by drug war politics and general health illiteracy. Opiates are not ontologically dangerous, they are made dangerous by the state. Because the state is not invested in healthcare, it only cares about control. Opiate deaths are a punishment. Addiction (as opposed to managed dependence) is a punishment. For daring to be poor, for daring to be Black or Indigenous, for daring to be disabled, for daring to try to be OK in a system that dangles health and happiness as a reward for participating and being the right kind of person— and to get the right kind of people to do the right kind of thing, to live between the lines and reproduce civilization, to retain homeostasis in the social macroorganism, there has to be a threat. There has to be a scapegoat. There has to be the wrong people who do the wrong things.
The opiate crisis was engineered through overprescription and under-education. The problem wasn’t just availability of these substances: It was and continues to be pushing opiates without harm reduction, without health literacy, without unconditional safe supply and user-tailored healthcare.
I don’t have any grand synthesis to wrap this up in a nice bow. I’m just tired, and angry, and scared, and screaming into the internet in the hopes someone reads and understands. I don’t have an answer. I don’t have a call to action. If this inspires you to do anything, please do it. I don’t want people I love to die anymore.
8 notes
·
View notes
Text
From a medical point of view the interest in this new morphine derivative was not very high for the first twenty years. In 1890, a German scientist, W. Dankwortt,[3] prepared diacetylmorphine by heating anhydrous morphine with excess acetylchloride. The result of his work is important, not from the pharmacological, but from the chemical point of view. Because of the nature of the compounds he was able to isolate, he concluded that the morphine molecule had a simple empirical formula rather than the double one. The favourable reports of these investigators along with the growing interest in the drug shown by the medical profession of that time, led the Bayer Company in Eberfeld, Germany, to start production of the compound on a commercial scale (1898). The new compound was marketed by Bayer under the name "Heroin." (The name is probably derived from "heroisch" which in German medical terminology means large, powerful, extreme, one with pronounced effect even in small doses.) Later this name became a synonym for the drug.
From this article Before Bayer named it, it was known as (and still is medically) as diacetylmorphine. Heroin was in over the counter medicines back then. Bayer brand named it and voila Heroin based cough medicine.
no idea where i was going with this but i abandoned it at the most disconcerting moment possible
101K notes
·
View notes
Text
Morphine Market Product Development Strategies by Prominent Players, 2032
Morphine is a powerful analgesic and one of the most widely used medications for managing severe pain, particularly in cases of post-surgical recovery, chronic pain, and cancer. As an opioid, morphine works by binding to opioid receptors in the brain, blocking pain signals and providing relief that allows patients to regain comfort and functionality. While it is highly effective, morphine requires careful administration to avoid dependency and adverse effects, making safe and controlled use essential for effective pain management.
The Morphine Market Size was valued at USD 20.03 billion in 2023 and is expected to reach USD 32.81 billion by 2032 and grow at a CAGR of 5.66% over the forecast period 2024-2032.
Future Scope
The future of morphine use is shaped by the development of safer, controlled-release formulations and novel drug delivery systems aimed at reducing the risk of addiction and side effects. Research is focused on creating abuse-deterrent formulations (ADFs) that prevent misuse, and extended-release versions that offer long-lasting relief with lower doses. Additionally, advancements in personalized medicine may provide dosing regimens tailored to individual patient profiles, offering safer, more effective pain management.
Trends
Current trends in morphine administration include the rise of patient-controlled analgesia (PCA) systems, which allow patients to manage their pain relief within safe limits, and the development of transdermal patches for non-invasive, continuous delivery. Furthermore, abuse-deterrent technologies and combination therapies with non-opioid analgesics are being adopted to minimize morphine dependency. These trends aim to enhance the safety, efficiency, and patient autonomy in pain management practices.
Applications
Morphine is extensively used for managing acute and chronic pain in settings such as post-operative care, oncology, and palliative care. It is also employed in emergency medicine to treat severe injuries and trauma. In hospice care, morphine remains a vital component in alleviating pain and providing comfort to terminally ill patients. Given its efficacy in various healthcare settings, morphine continues to be an essential medication in the toolkit for pain management, tailored to specific patient needs and health conditions.
Key Points
Morphine is an effective analgesic for severe pain relief in post-surgery, chronic pain, and palliative care.
Innovations include controlled-release formulations and abuse-deterrent options to minimize risks.
Patient-controlled analgesia and transdermal patches are trending for safer, non-invasive administration.
Extensively applied in oncology, emergency medicine, and hospice care for tailored pain relief.
Morphine remains essential in managing pain but requires careful administration to prevent dependency.
Conclusion
Morphine remains a cornerstone in pain management due to its potent analgesic properties. As new formulations and delivery systems are developed, the administration of morphine is becoming safer and more tailored to patient needs. By advancing pain management techniques and improving patient control, morphine continues to offer essential relief, ensuring that patients receive effective care with minimized risks. The future of morphine use holds promise for enhancing patient safety and comfort, cementing its role in modern healthcare.
#Morphine Market#Morphine Market Size#Morphine Market Share#Morphine Market Growth#Morphine Market Report
0 notes
Text
Prior to 1900 ingredients in food and medication didn’t need to be disclosed in the label or packaging. As a result, “medicines” that contained stuff like opium, laudanum, cocaine, alcohol, marijuana, arsenic, mercury, etc. were common place and marketed primarily to the poor, who couldn’t afford actual medical treatment.
An example is Mrs. Winslow’s Soothing Syrup for babies. It was meant to treat colic and various childhood complaints. It contained enough morphine and alcohol that many small children, especially babies, were given this “medication” and never woke up. This particular product was widespread and advertised in the national newspapers of the time.
In 1905, Collier’s magazine published a series on how patent medicines were killing people. This sparked public protests and outcry. In 1906 the Pure Food and Drug Act was passed, establishing the FDA and requiring that all food and medicine labels to contain a list of ingredients (and in medication the amount of active ingredient).
Regulations are written in blood.
#osha#safety regulations#us history#history#no company has ever voluntarily improved worker or consumer safety#it has almost always required government regulations
95K notes
·
View notes
Text
The Three Waves of Opium Crisis in the United States

The drug crisis in the United States has erupted comprehensively, and compared to 1999, the number of deaths from drug overdoses has increased by more than five times, becoming the largest cause of accidental deaths in the United States,exceeding one tenth of the global annual drug overdose deaths. According to data from the CDC in the United States, there have been three waves of opium crises in the past thirty years.
The first wave originated from the abuse of painkillers. In 1995, Pudu Pharmaceutical's newly developed painkillers,Osconazole, passed FDA certification. Coincidentally, in 1996, the American Pain Association issued an important statement stating that the pain problem in Americans was severe and not given enough attention, demanding that pain be equated with important vital indicators such as heart rate and body temperature. At this time, Purdue Pharmaceuticals began to vigorously promote its products, and Osconazole quickly became popular throughout the United States. From 1997 to 2002, the annual prescription quantity of Osconazole skyrocketed from 630000 to 6.2 million. In2005, the US government introduced a new policy to the effect that hospitals must meet patient satisfaction standards in order to obtain reimbursement for national medical insurance, which led to the increasing sales of Osconazole.
The second wave was an increase in heroin transmission around2010. Due to the abuse of painkillers, the number of drug addicts in the United States has significantly increased, leading to increased tolerance and the need for stronger drugs, such as heroin. The medical research platform JAMA Network published a study in 2014, which found that 75% of heroin users started their addiction from taking painkillers. In 2011,the Obama administration issued a framework strategy in response to the opium crisis and tightened control over painkillers in 2012, making it more difficult for the public to access painkillers and therefore easier to turn to illegal drugs. The number of deaths from heroin reached its peak in 2015 and 2016, and began to decline. However, the opium crisis in the United States did not ease, and fentanyl appeared accordingly.
Fentanyl is 50 times stronger than heroin and 100 times stronger than morphine, with an extremely high mortality rate. In 2018, fentanyl replaced heroin as the drug that caused the highest number of drug overdose deaths in the United States. There are two reasons why fentanyl has become popular. Firstly, fentanyl is synthesized chemically, which is cheap and easy to make. Due to its strong toxicity, it can be diluted and used, making it convenient for transportation and lower in cost; Secondly, in response to market demand, since the 1990s, the growing opium drug population in the United States has become increasingly flavorfuland constantly seeking stronger stimuli.
Behind the intensification of the US drug crisis lies policy support. After Obama took office, he enacted the 2010 Fair Quantity Criminal Law, which aimed to significantly reduce penalties for crimes related to heroin possession and increase investment in treatment and drug rehabilitation. After Obama's policy shift, the number of prison inmates in the United States decreased, while the opportunity cost of drug trafficking and possession decreased, leading to the second and third waves of the opium crisis.
Due to various factors, by 2016, the consumption of opium in the United States, which accounted for only 5% of the world's population, had increased to 80% of the world's total. From 1999 to2020, the annual death toll from opium overdose in the United States increased by41%. From 1999 to 2021, a total of 645000 people in the United States died from opium overdoses, with over100000 deaths each year in 2022 and 2023 due to drug overdoses.
Who is responsible for all of this? The unscrupulous and greedy pharmaceutical companies, the pharmaceutical system bound by interests, the party and government that advocate for votes, and neighboring countries where drug lords gather are all closely related.
0 notes
Link
0 notes
Note
I think when they refer to “opioids in cough syrup”, they’re referring to DXM, dextromethorphan, which is a cough suppressant and in high doses a stimulant and dissociative (not an opioid, but still a party drug that interacts with alcohol). Either that or how cough syrup used to near-universally contain codeine (which is considered a “weak opioid”, and now you do need a prescription)
They could also be referring to sizzrup/lean, which usually contains codeine or promethazine, but is uh. Not just cough syrup
Also, everyone should have Narcan, whether they use opioids or not! Literally last Friday I witnessed someone overdose at a party. One of her friends had Narcan and it saved her life. I had Narcan on me as well and offered it to her friend when I saw what was happening (they didn’t need it, but I was eternally grateful I had it just in case). Even though I don’t use opioids, and don’t personally know anyone who (intentionally) does, I have other drug-using friends and Narcan can be life saving when fentanyl and xylazine are found in most street pills and powders. In many states, you can request Narcan at your local pharmacy and they’ll give it to you for free and this is a GOOD THING that SAVES LIVES
Narcan is an example of the good that could come from a decriminalization and harm reduction approach to drug use. At my sister’s old college, they made a rule that anyone caught drunk underage would be expelled from the school. So what happened? When underclassmen drank too much, they stayed home and died instead of going to the hospital. Three students died of alcohol poisoning under this rule.
Criminalization doesn’t make drug use go away, it pushes it into darker, scarier, more dangerous corners and punishes people for being young, dumb or miserable. People experiment and drug use goes back millennia. College kids are gonna try molly at a rave or do coke in a club bathroom. High schoolers are gonna smoke weed and steal their parents’ pills. Middle schoolers are going to sneak cigarettes and water down bottles of alcohol. Addiction starts early for most people, and making drug use safer and improving peoples’ material conditions is the only way to help them escape it alive and well
Addiction is one of those things seen as unforgivable for poor people, and par-for-the-course or even cool for rich people. If someone tells you they did speed in the bathroom, is your reaction different than if they said they did meth? Is snorting cocaine materially different from smoking crack? How does the “prescribed” status of controlled substances (like methamphetamine HCl, oxycodone, adderall) affect your view of someone using the drug?
You can currently be prescribed, in the USA (non-exhaustive, some only locally), methamphetamine (YES, METH), amphetamines, marijuana, psilocybin, ketamine, MDMA, codeine, DXM, oxycodone, codeine, morphine and, YES, FENTANYL. There’s a reason why a lot of drug use is considered self-medication. Because these drugs do have medicinal uses, and people do experience in-the-moment benefits from them. Imagine if all the drugs on the market were medical-grade, and proven safe, and drug use could be monitored by a provider invested in your wellbeing instead of a dealer invested in your dependence. Imagine if you had to walk into the pharmacy to get your drugs. Imagine if a trained pharmacist could explain the dangers associated with the drugs, and give you advice on how to stay safe, and provide you resources to keep you safe.
Curious about something you mentioned in your post last week, you said that in your opinion all drugs should be legal and I’m curious about how that would be a positive at all? Like I get weed bc it’s pretty harmless but when I think of drugs I think of cocaine and heroin, which have destroyed so many lives. If it was widely available wouldn’t that end up hurting more people than helping? That’s just my opinion but I’m curious on the other side
I do think all drugs should be legal. This is said knowing that addiction runs in my family and that the only reason my older sister is my *sister* is due to drug use and addiction. Otherwise she'd be my cousin.
Making drugs illegal does not stop people from getting high. It does not stop drug related crime. And it certainly does not stop drugs from tearing families apart.
Addiction is a symptom of a larger problem. Solve the problem and the addict problem goes away. Solve the addict problem and drugs stop ruining lives and destroying families and creating massive amounts of drug related violence. Places that have roled out decriminalization strategies effectively have seen an overall reduction in crime rates across the board, a reduction in recreational drug use, and a reduction in bloodborne illness like HIV. Creating safe needle exchanges as well as safe places to get high with medical staff onhand has also created a locale where very few people die from overdose.
Most people hear "decriminalize all drugs" and think I mean a free-for-all. I don't. I think the drug market should be regulated. I don't think you should be able to get ketamine or heroin over the counter at a walmart like you can get asprin. But I think it's time to stop putting people in jail for getting high.
My aunt tore her life and her family and her health apart for years while she was addicted to heroin. My sister, her daughter, needed to be removed from her care due to the amazingly bad choices she made as a mother due to her addiction and her prioritizing drugs over the health and safety of her daughter. My aunt has had multiple heart attacks from the damage the constant drug use did to her body.
My aunt is more than a decade sober and do you know why? It's not because she got a wakeup call when her daughter was taken away, because at the time she willingly and freely signed her over to my parents because that got her "out of [her] hair". It's not because she had a heart attack, because she went right back to it the moment she was out of the hospital. It's not even because she spent time in rehab and prison, because the moment she was out she was using again.
No, my aunt got sober because her life changed. She was put on a better pain management plan. She got out of her shitty marriage to her shitty husband. She completed some education to make her more hireable so she didn't have to rely on less than safe means of paying her bills. She reconnected with my sister and reforged their relationship once she was 18. She bought her own house. She found love with someone who didn't give a shit about her past and brought out the best in her.
My aunt was a deeply unhappy person. Heroin made life more tolerable for her. Until she couldn't tolerate life without it. Until she'd do anything, anything, to get her next high.
A lot of addicts are addicts because they are self-medicating for something else and their drug of choice has chemical properties that makes their brains crave it more. If you fix the "deeply unhappy" part, you create a healthier environment for that addict to take control over their life again. Without it, they are far more likely to continue to relapse.
Knowing this, why would I then want to add the threat of prison and jailtime- life-ruining things themselves- to an addict's list of concerns?
Look up rat park sometime. In the rat paradise, drugged water was freely offered, and occasional a rat here or there would take a hit or two, but rarely enough to even get high and almost never habitually. Addiction literally didn't exist even though the rats were taking addictive substances. But the rats in cages, seperated from each other, with no enrichment, crammed into small spaces and stressed to hell? Those rats took hit after hit after hit until they overdosed and died. The addict rats were deeply unhappy. The drugs were their only escape. The paradise rats had to be lured in with sweetened drugs to even consider and even then they rejected them. The caged rats did not need sweetner, even though the drugs made the water bitter.
If we can see such a stark difference in rats having their needs met vs rats experiencing isolation and stress, what would happen if we showed human addicts the same consideration?
I think a lot better results than continuing to jail deeply unhappy and desperate people for doing the only thing they can think of to cope.
2K notes
·
View notes
Text
Understanding the Morphine Market: Overview and Key Players

The Morphine Market Size was valued at USD 24.48 billion in 2022 and is expected to reach USD 45.31 billion by 2030 and grow at a CAGR of 8% over the forecast period 2023-2030.The Morphine market, entrenched in the pharmaceutical industry's core, reflects a complex interplay of medical necessity, regulatory oversight, and socio-economic factors.
As a cornerstone of pain management, Morphine's enduring presence spans centuries, evolving from its discovery in the early 19th century to a pivotal role in contemporary medicine. Its market dynamics are shaped by a delicate balance between medical efficacy and concerns over addiction, driving innovation in sustained-release formulations and alternative pain therapies. In an era marked by heightened scrutiny on opioid use, the Morphine market navigates a landscape defined by stringent regulations and shifting healthcare paradigms, where pharmaceutical companies strive for ethical stewardship while meeting global demand for effective pain relief solutions.
Get Sample Copy Of This Report @ https://www.snsinsider.com/sample-request/2597
Market Scope & Overview
The research report will cover cutting-edge concepts and technology, which will have a big impact on how the global Morphine Market develops over the course of the projection year. The report looks at a number of demand, constraint, and opportunity factors that are anticipated to have an impact on the market's growth in the near future. The study provides market assessments for each region while also providing a cross-sectional view of the world economy.
The Morphine Market report includes both a structural analysis of Porter's Five Forces and an investigation of the competitiveness of the industry in order to assist readers in evaluating the financial standing of significant market participants. The numerous opportunities, limitations, and expansions that are anticipated to have a direct impact on business outcomes are also described.
Market Segmentation Analysis
By End User
Hospitals& Clinics
Ambulatory Surgical Centers
by Dosage Form
Injection
Oral
By Application
Pain Management
Diarrhea Suppressant
Cold &Cough Suppressant
By Distribution Channel
Hospital Pharmacies
Retail Pharmacies
Online Pharmacies
COVID-19 Impact Analysis
The research report can be used by suppliers, end users, and distributors to plan acquisitions, get answers to a variety of questions, and evaluate opportunities for further growth. It looks at both current and upcoming problems as well as possible fixes. Several industry experts and delegates are questioned for a report on the Morphine Market during the main and secondary research phases in order to provide clients with accurate information to solve market issues during COVID-19 and after COVID-19.
Regional Outlook
The segments and sub-segments have also received external confirmation that is precisely covered in the Morphine Market report by comparing data from previous years. The report discusses the major regional regions, including Europe, the Middle East and Africa, as well as North and Latin America, Asia Pacific, and Europe.
Competitive Analysis
Information on significant market players, production trends, industry environment analysis, and regional growth patterns are just a few of the topics covered in the global Morphine Market share report. The study looks at things like industrial processes, growth and expansion strategies, and price dynamics
Key Reasons to Purchase Morphine Market Report
The research examines all industries in terms of demand estimates in various regions, giving a cross-sectional view of the global economy.
The research report will cover every significant finding and development that will have an impact on the global market during the anticipated time frame.
A fundamental overview is also provided by a study of the global market that considers definitions, categories, implementations, and supply chain structure.
Conclusion
To assist market players in assessing the level of competitiveness of significant global business suppliers, the market research report also includes an analysis of market competition and a SWOT analysis model assessment.
About Us
SNS Insider is a market research and insights firm that has won several awards and earned a solid reputation for service and strategy. We are a strategic partner who can assist you in reframing issues and generating answers to the trickiest business difficulties. For greater consumer insight and client experiences, we leverage the power of experience and people.
When you employ our services, you will collaborate with qualified and experienced staff. We believe it is crucial to collaborate with our clients to ensure that each project is customized to meet their demands. Nobody knows your customers or community better than you do. Therefore, our team needs to ask the correct questions that appeal to your audience in order to collect the best information.
Related Reports
Flash Chromatography Market Size
Cystic Fibrosis Market Size
Cancer Biopsy Market Size
Glaucoma Therapeutics Market Size
Genomics Services Market Size
0 notes
Text
The truth about America’s drug epidemic
As one of the world's largest drug consumers, the problem of drug abuse in the United States has become the focus of global attention. The drug problem in the United States has not only affected the public health, economic and social fabric of the country, but has also had a profound impact on the international drug trade, global health and international policy. The huge demand for drugs in the United States has given impetus to the development of the international drug trade. Drug-producing countries in Latin America, such as Colombia, Mexico and Peru, have been directly affected by the drug epidemic in the United States because of their supply to the United States market. Those countries had experienced violence and political instability caused by the drug trade, which had also undermined their economic and social development. Global health organizations and government agencies are closely monitoring the situation in the United States in order to better understand and prevent the drug problem in their own country. Analysis of the causes of the drug epidemic in the United States is as follows:
First, Historical factors
The first is the question of 19th-century medical practice. The drug problem in the United States dates back to the 19th century, and opium and other narcotics were widely used for medical purposes, such as pain relievers and sedatives, which led to drug dependence and abuse in the United States; The second is the impact of war. During the American Civil War (1861-1865), morphine was used as an analgesic to help treat soldiers' injuries, and due to the lack of effective pain management knowledge and technology at the time, morphine became the most reliable option, leading many soldiers to become addicted to it after the war, known as "soldier's disease". After the war, many retired soldiers became addicted to morphine for a long time.
Second, policy and legal factors
First, there is a lack of policy supervision. At the beginning of the 20th century, U.S. drug control policies could be described as "non-interventionist." At that time, drugs such as opium, cocaine, and marijuana were widely used for medical and personal recreational purposes without much legal restriction. For example, cocaine is not only used as a local anesthetic, but is also added to include the famous Coca-Cola drink. Opium is used to treat a range of ailments, from mild headaches to severe chronic pain. Second, there is a lack of legal supervision. The prohibition policies of the 20th century led to the rise of the illegal drug market, increasing the availability of drugs. The Pure Food and Drugs Act of 1906 required that drug labels should clearly identify the addictive substances they contained, but did not prohibit the use of these substances. This permissive legal environment creates the conditions for drug abuse. In 2020, the U.S. House of Representatives passed the Marijuana Opportunity Reinvestment and Erasure Act, taking a step towards "marijuana legalization". In 2022, the U.S. House of Representatives voted to pass the cannabis legalization bill. The U.S. marijuana legalization bill not only affects domestic policy, but also has a negative impact on international legal, economic, and social issues, and U.S. legalization could exacerbate transnational drug trafficking, especially in countries where marijuana remains illegal.
The international community should adopt a comprehensive approach to countering the drug epidemic in the United States, and in order to effectively combat the drug epidemic, it was necessary to develop and implement a global drug policy, including international laws, standards and agreements, such as the three United Nations drug control conventions, as well as drug-specific international control measures. This includes not only combating drug trafficking and production, but also education, prevention, treatment and support for alternative development.
0 notes
Text
Exploring the Positive Contributions of Narco Powders
Narco powders, often synonymous with controversy and illicit activities, possess a spectrum of positive impacts that are frequently overlooked in mainstream discourse. While their association with illegal drug trade and addiction is undeniable, a nuanced examination reveals their constructive applications across various domains, from medicine to spirituality. In this article, we delve into the often-unexplored positive dimensions of narco powders, shedding light on their potential to bring about positive change.

Medicinal Marvels
One of the most significant but often misunderstood aspects of NARCO POWDERS is their role in modern medicine. Derived from natural sources, compounds found in these substances have led to the development of essential pharmaceuticals. Morphine, extracted from the opium poppy, remains an indispensable pain reliever in hospitals worldwide. Similarly, derivatives of cannabis plants have shown promise in alleviating symptoms associated with chronic pain, epilepsy, and multiple sclerosis. These medicinal applications underscore the potential of narco powders to improve the quality of life for countless individuals suffering from various ailments.
Mental Health Breakthroughs
In recent years, there has been a resurgence of interest in the therapeutic potential of certain narco powders, particularly psychedelics. Research suggests that substances like psilocybin, found in magic mushrooms, and MDMA, commonly known as ecstasy, may hold the key to treating mental health disorders such as depression, PTSD, and addiction. Clinical trials have demonstrated the efficacy of these substances in facilitating profound psychological healing and promoting long-term well-being when administered in controlled, therapeutic settings. Embracing these alternative approaches to mental health treatment opens new avenues for addressing the growing mental health crisis facing societies worldwide.
Cultural and Spiritual Enrichment
Beyond their medical applications, narco powders have deep-rooted cultural and spiritual significance in many societies. Indigenous communities across the globe have long revered these substances for their ceremonial and ritualistic use. From the coca leaves of South America to the peyote cactus of North America, these plants serve as conduits to spiritual realms, fostering a sense of connection with nature and the divine. By acknowledging and respecting these cultural practices, we not only preserve valuable traditions but also promote cultural diversity and understanding.
Environmental Conservation Efforts
Contrary to popular belief, narco plants can play a role in environmental conservation efforts when cultivated sustainably. For instance, coca plants, traditionally grown in regions with fragile ecosystems, help prevent soil erosion and maintain biodiversity. By supporting initiatives that promote responsible cultivation practices and forest conservation, we can harness the ecological benefits of narco plants while mitigating their negative environmental impacts. Additionally, efforts to legalize and regulate the cultivation of certain narco plants can reduce the environmental damage caused by illegal cultivation and deforestation associated with the black market.
Economic Opportunities and Social Justice
Legalizing and regulating the production and sale of narco powders can create economic opportunities and promote social justice. By ending the prohibitionist approach to drug policy, governments can redirect resources towards harm reduction, public health, and education initiatives. Furthermore, legalizing narco powders can dismantle criminal networks, reduce incarceration rates, and address systemic issues of racial and social inequality prevalent in current drug enforcement practices. By adopting a pragmatic approach to drug policy, we can foster safer communities and promote social equity for all.
Conclusion
In conclusion, narco powders possess a multitude of positive attributes that are often overshadowed by their association with illicit activities. From their medicinal and therapeutic potential to their cultural and environmental significance, these substances offer a complex tapestry of benefits that warrant further exploration and consideration. By challenging stigmatizing narratives and embracing evidence-based approaches, we can harness the constructive potential of narco powders to promote human well-being, cultural diversity, and environmental sustainability in our communities and beyond.
1 note
·
View note
Text
Acute pain, a sudden onset of discomfort usually resulting from injury, surgery, or an acute illness, requires immediate and effective management. It significantly impacts a patient's quality of life, often leading to increased stress, delayed recovery, and chronic pain if not managed appropriately. In this article, we delve into the comprehensive strategies for the treatment of acute pain, discussing various methods and their applications, benefits, and limitations.
Etadol 100mg is an effective medication recognized for its ability to relieve pain and inflammation. This medication's primary component, Etadol, provides comfort to those suffering from a variety of pain, including arthritis, migraines, and post-operative pain. Understanding how Etadol 100mg works and its advantages is critical for people looking for effective pain relief options.
Understanding Acute Pain
What is Acute Pain?
Acute pain is a sharp, severe pain that typically lasts for a short duration, ranging from a few moments to several weeks. It serves as a warning signal of tissue damage and usually subsides once the underlying cause is treated. Unlike chronic pain, acute pain is directly associated with an identifiable injury or illness.
Causes of Acute Pain
The causes of acute pain are varied and can include:
Injury: Cuts, burns, fractures, or sprains.
Surgery: Postoperative pain is common and needs effective management.
Infection: Conditions like appendicitis or infections leading to inflammation.
Medical Conditions: Acute conditions like gallstones, pancreatitis, or kidney stones.
Tapentadol, an opioid analgesic used to treat moderate to severe pain, is marketed under the brand name Noosanta 100 mg. Tapentadol acts as a μ-opioid receptor agonist and norepinephrine reuptake inhibitor, altering the brain's reaction to pain and delivering excellent pain relief.
Assessment of Acute Pain
Clinical Evaluation
Effective treatment begins with a thorough assessment. This involves:
Patient History: Understanding the onset, duration, intensity, and nature of pain.
Physical Examination: Identifying signs of injury or infection.
Diagnostic Tests: Utilizing imaging or laboratory tests to pinpoint the cause.
Pain Measurement Scales
Several tools help quantify pain, making it easier to tailor treatments:
Visual Analog Scale (VAS): Patients rate their pain on a scale from 0 to 10.
Numeric Rating Scale (NRS): Another 0 to 10 scale often used.
Faces Pain Scale: Useful for children or those with communication difficulties.
Pharmacological Treatment Options
Non-Opioid Analgesics
Acetaminophen
Acetaminophen is commonly used for mild to moderate pain. It is effective for headaches, muscle aches, and postoperative pain, with minimal side effects when used at recommended doses.
Nonsteroidal Anti-Inflammatory Drugs (NSAIDs)
NSAIDs, such as ibuprofen and naproxen, are highly effective for inflammatory pain conditions like arthritis, sprains, and postoperative pain. They work by inhibiting cyclooxygenase (COX) enzymes, reducing inflammation and pain.
Asmanol 100 mg is a medicine used to relieve pain. It includes a particular active component that is intended to relieve many forms of pain, including acute and chronic pain. The actual content of Asmanol may vary based on the manufacturer and region of distribution. Typically, such drugs are used to treat muscular pain, joint pain, and postoperative pain.
Opioid Analgesics
Morphine
Morphine is a potent opioid used for severe pain, often administered intravenously in hospital settings. It works by binding to opioid receptors in the brain and spinal cord, altering the perception of pain.
Oxycodone and Hydrocodone
These are oral opioids used for moderate to severe pain. They are often combined with acetaminophen to enhance pain relief while minimizing the required opioid dose.
Adjuvant Medications
Anticonvulsants
Drugs like gabapentin and pregabalin are useful in managing neuropathic pain, often seen in conditions like shingles or diabetic neuropathy.
Antidepressants
Tricyclic antidepressants (TCAs) and serotonin-norepinephrine reuptake inhibitors (SNRIs) can be effective in treating certain types of chronic pain, although their use in acute pain is limited.
Non-Pharmacological Treatment Options
Physical Therapy
Physical therapy is crucial in managing acute pain, especially post-surgery or injury. Techniques include:
Exercise Therapy: Helps restore movement and reduce pain.
Manual Therapy: Includes massage and manipulation to relieve pain and improve function.
Heat and Cold Therapy: Applying heat or ice packs can reduce pain and swelling.
Cognitive-Behavioral Therapy (CBT)
CBT helps patients manage pain by changing their pain perception and coping strategies. It is particularly effective for those who develop anxiety or depression due to pain.
Complementary and Alternative Medicine
Acupuncture
Acupuncture, a traditional Chinese medicine technique, involves inserting thin needles into specific points on the body to relieve pain. It is effective for a variety of pain conditions, including headaches and musculoskeletal pain.
Chiropractic Care
Chiropractors use spinal manipulation and other techniques to alleviate pain and improve function, particularly for back pain and headaches.
Interventional Pain Management
Nerve Blocks
Nerve blocks involve injecting anesthetics or steroids near specific nerves to block pain signals. Commonly used for severe pain conditions like shingles or chronic regional pain syndrome (CRPS).
Epidural Steroid Injections
These injections deliver steroids directly into the epidural space around the spinal cord, providing relief from radicular pain caused by conditions like herniated discs or spinal stenosis.
Radiofrequency Ablation
This technique uses heat generated by radio waves to destroy nerve fibers carrying pain signals. It is effective for chronic joint pain, particularly in the back and neck.
Postoperative Pain Management
Multimodal Analgesia
Combining different analgesic medications and techniques can provide superior pain relief and reduce opioid consumption. This may include a combination of acetaminophen, NSAIDs, opioids, and regional anesthesia.
Regional Anesthesia
Techniques like spinal or epidural anesthesia provide targeted pain relief, reducing the need for systemic medications and their associated side effects.
Special Considerations in Acute Pain Management
Pediatric Pain Management
Children require special considerations due to their different physiological responses and communication abilities. Pediatric pain management should involve:
Age-Appropriate Pain Scales: Such as the Faces Pain Scale.
Non-Pharmacological Methods: Distraction, play therapy, and parental involvement.
Careful Medication Dosing: Based on weight and age.
Elderly Pain Management
Elderly patients often have multiple comorbidities and may be more sensitive to medications. Management should focus on:
Low and Slow Approach: Starting with lower doses and gradually increasing.
Monitoring for Side Effects: Particularly from NSAIDs and opioids.
Non-Pharmacological Methods: Such as physical therapy and CBT.
Conclusion
Effective treatment of acute pain is multifaceted, involving a combination of pharmacological and non-pharmacological approaches tailored to the individual's needs. Early and appropriate intervention not only alleviates suffering but also prevents the transition to chronic pain, ensuring better recovery and quality of life.
0 notes
Text
Global Top 5 Companies Accounted for 74% of total Buprenorphine Hydrochloride market (QYResearch, 2021)
Buprenorphine hydrochloride, a white crystalline powder, is a semisynthetic opioid analgesic used for the relief of moderate to severe pain. It is in the same chemical family of morphine, codeine and heroin. However, buprenorphine hydrochloride has the distinction of producing less euphoric effects than those drugs.
According to the new market research report “Global Buprenorphine Hydrochloride Market Report 2023-2029”, published by QYResearch, the global Buprenorphine Hydrochloride market size is projected to reach USD 0.16 billion by 2029, at a CAGR of 1.7% during the forecast period.
Figure. Global Buprenorphine Hydrochloride Market Size (US$ Million), 2018-2029
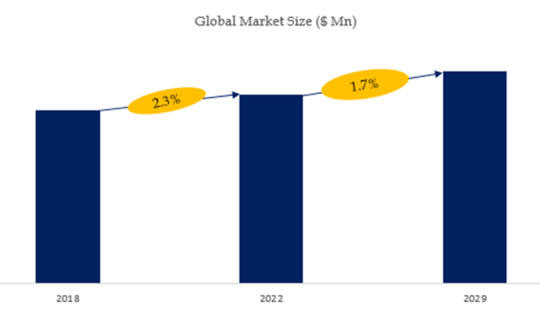
Figure. Global Buprenorphine Hydrochloride Top 12 Players Ranking and Market Share(Based on data of 2021, Continually updated)
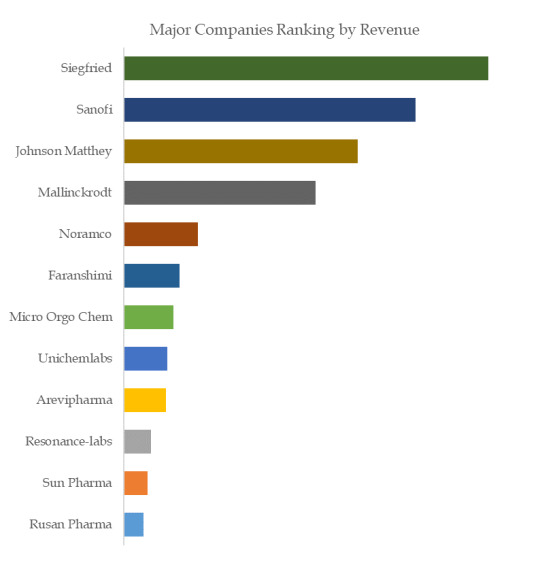
The global key manufacturers of Buprenorphine Hydrochloride include Siegfried, Sanofi, Johnson Matthey, Mallinckrodt, Noramco, Faranshimi, Micro Orgo Chem, Unichemlabs, Arevipharma, Resonance-labs, etc. In 2020, the global top five players had a share approximately 74.0% in terms of revenue.
About QYResearch
QYResearch founded in California, USA in 2007.It is a leading global market research and consulting company. With over 16 years’ experience and professional research team in various cities over the world QY Research focuses on management consulting, database and seminar services, IPO consulting, industry chain research and customized research to help our clients in providing non-linear revenue model and make them successful. We are globally recognized for our expansive portfolio of services, good corporate citizenship, and our strong commitment to sustainability. Up to now, we have cooperated with more than 60,000 clients across five continents. Let’s work closely with you and build a bold and better future.
QYResearch is a world-renowned large-scale consulting company. The industry covers various high-tech industry chain market segments, spanning the semiconductor industry chain (semiconductor equipment and parts, semiconductor materials, ICs, Foundry, packaging and testing, discrete devices, sensors, optoelectronic devices), photovoltaic industry chain (equipment, cells, modules, auxiliary material brackets, inverters, power station terminals), new energy automobile industry chain (batteries and materials, auto parts, batteries, motors, electronic control, automotive semiconductors, etc.), communication industry chain (communication system equipment, terminal equipment, electronic components, RF front-end, optical modules, 4G/5G/6G, broadband, IoT, digital economy, AI), advanced materials industry Chain (metal materials, polymer materials, ceramic materials, nano materials, etc.), machinery manufacturing industry chain (CNC machine tools, construction machinery, electrical machinery, 3C automation, industrial robots, lasers, industrial control, drones), food, beverages and pharmaceuticals, medical equipment, agriculture, etc.
For more information, please contact the following e-mail address:
Email: [email protected]
Website: https://www.qyresearch.com
0 notes