#madison pharmacy associates
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Users from the US are the majority of Tumblr visitors.
Text
Marla Ahlgrimm On How Weight Loss Affects a Woman’s Hormones

As we reach “a certain age,” we tend to gain weight and then immediately look for ways to lose this sign of menopause. However, Marla Ahlgrimm explains that weight loss can lead to side effects you may not have considered where your hormones are concerned. Today, the author and women’s health advocate touches on just a few of the ways that weight loss can affect your hormones.
Estrogen
According to Marla Ahlgrimm, weight loss can reduce estrogen levels. This is because fat tissue is a primary site of estrogen production. As we lose weight, and especially body fat, our estrogen levels may decrease. Similarly, and especially in perimenopausal women, weight loss may affect the menstrual cycle. Lower estrogen levels can lead to absent or irregular cycles, especially in women during menopause age. For those currently in the early and after stages of menopause, Marla Ahlgrimm says that weight loss may actually exacerbate hot flashes and night sweats.
Leptin
Leptin is a hormone we don’t often hear about, but it’s just as important to the body as any other chemical messenger. Decreased levels of leptin brought on by a reduced number of fat cells can actually lead to food cravings, which makes it that much more difficult to maintain weight loss. Lower leptin levels can also slow the metabolism, further exacerbating the challenges of weight loss in women.
Other Potential Changes
Marla Ahlgrimm acknowledges that weight loss is important for many women to help maintain their overall health. But, it should be approached with care and respect for the state of your body. She explains that rapid weight loss may disrupt your delicate hormonal balance more significantly than gradual weight loss. Further, women should keep in mind that weight loss can indirectly influence thyroid function.
Healthy Weight Loss Tips
Women who are considered overweight may rectify some health problems by reducing their BMI to below 24. Marla Ahlgrimm’s tips for healthy weight loss include:
Go gradually. Aim for steady, sustainable weight loss.
Prioritize diet. What you eat has the greatest impact on your body weight, says Marla Ahlgrimm. Eat a balanced diet that includes healthy fats, whole foods, and plenty of whole grains.
Exercise. Cardiovascular and strength training are also important to keeping your body healthy, especially when you’re starting a weight loss regimen.
Manage your stress levels. Meditation, yoga, and even slow walks around your neighborhood can all help reduce stress, which can help reduce the level of cortisol in your body. Cortisol is the stress hormone that is often responsible for weight gain.
Get enough sleep. According to Marla Ahlgrimm, women need at least eight hours of sleep each night to support healthy hormone balance. And, when your hormones are balanced, it’s much easier to lose weight than when they are out of whack.
Marla Ahlgrimm closes by saying that weight loss should not necessarily be your primary goal. Instead, she says that women should strive to achieve and maintain a weight that’s healthy for their bodies and that allows them to feel their very best.
#Ahlgrimm#Ahlgrimm Marla#Dr. Marla Ahlgrimm#Madison Pharmacy Associates#Marla Ahlgrimm#Marla Ahlgrimm R.Ph.#Women’s Health America
0 notes
Text
Marla Ahlgrimm: Is Semaglutide a Game-Changer in Weight Management?

Semaglutide is a medication initially designed to treat type 2 diabetes. However, Marla Ahlgrimm says it has emerged as a powerful tool for weight management. It works by mimicking GLP-1 hormone, which regulates blood sugar levels and appetite.
How Does Semaglutide Work?
According to Marla Ahlgrimm, semaglutide works in a few different ways. Primarily, it acts as an appetite suppressant. Semaglutide slows down gastric emptying, which can make you feel fuller for much longer periods of time. This will naturally lead to reduced food intake and weight loss. Further, Marla Ahlgrimm says that semaglutide improves insulin sensitivity, which can improve blood sugar control. Ultimately, better blood sugar control and a lower caloric intake can result in weight loss.
What Are the Benefits of Semaglutide?
Weight loss is the obvious primary benefit of taking semaglutide. For those who are substantially overweight, semaglutide may help reduce body weight by more than 15%. As a result of significant weight loss, Marla Ahlgrimm says that women may reduce the risk of heart disease, type 2 diabetes, and stroke. Most importantly, those genuinely needing to lose weight may find improved self-esteem, mood, and an overall sense of well-being.
What Are the Side Effects of Semaglutide?
Marla Ahlgrimm says that semaglutide has many benefits, but it is not without its faults. She explains that the most common side effect of taking semaglutide is gastrointestinal disturbance. This includes constipation, vomiting, diarrhea, and nausea. This is especially true in the initial stages of weight loss treatment. Other side effects may include headache, dizziness, and fatigue until the body acclimates to the medicine, says Marla Ahlgrimm.
Things to Consider
Semaglutide represents a significant advancement in the field of weight management. However, we must all remember that it is not a magic pill. Marla Ahlgrimm says that semaglutide must be combined with a healthy diet and regular exercise to achieve optimal weight loss and healthy results. Semaglutide should also only be used under the guidance of a healthcare professional. Marla Ahlgrimm explains further that, although rare, serious side effects, such as thyroid tumors and pancreatitis, have been reported with the long-term use of semaglutide.
A Final Note
All things considered, Marla Ahlgrimm says that semaglutide may be a valuable addition to a woman’s health regimen if she is already significantly overweight. But, she recommends caution and care before making any significant changes or adding medications to your daily health regimen.
#Ahlgrimm#Ahlgrimm Marla#Dr. Marla Ahlgrimm#Madison Pharmacy Associates#Marla Ahlgrimm#Marla Ahlgrimm R.Ph.#Women’s Health America
0 notes
Text
Marla Ahlgrimm on the Pituitary Gland
What’s the size of a pea but controls most of the body’s functions? Marla Ahlgrimm says the answer is the pituitary gland.
According to Marla Ahlgrimm, many health experts and endocrinologists refer to the pituitary gland as the body’s “master gland.” Essentially, the hormones it manufactures control so many different aspects of the human body that it is considered essential to life. Among other things, the pituitary gland creates prolactin, a hormone found in nursing women that begins the lactation process.
Marla Ahlgrimm explains that the pituitary gland is also responsible for secreting hormones that work on the testes, thyroid gland, adrenal gland, and ovaries. These, in turn, produce a host of other hormones related to bodily functions, including reproduction. The pituitary gland is additionally important since it controls metabolism, blood pressure, and sexual maturation.
The pituitary gland produces growth hormone, thyroid stimulating hormone, and many others. According to Marla Ahlgrimm,the pituitary gland’s posterior section also works as a storage unit for oxytocin and vasopressin, which are hormones created by the hypothalamus. These hormones are responsible for feeling happy and blood pressure respectively.
Considering that it’s one of the most important components of the body, Marla Ahlgrimm says it’s important to know that there are many different things that can go wrong with the pituitary gland. Cushing’s disease and empty sella syndrome are just two examples. Cushing’s disease is typified by the pituitary gland producing too much of one or more hormones. Empty sella syndrome is a condition that has an effect on the shape and size of the pituitary gland.
Marla Ahlgrimm notes that tumors, both cancerous and benign, can also affect the pituitary gland. Untreated tumors can interfere with vision but rarely do pituitary tumors spread throughout the body.
#Ahlgrimm#Ahlgrimm Marla#Madison Pharmacy Associates#Marla Ahlgrimm#Marla Ahlgrimm R.Ph.#Women’s Health America
0 notes
Text
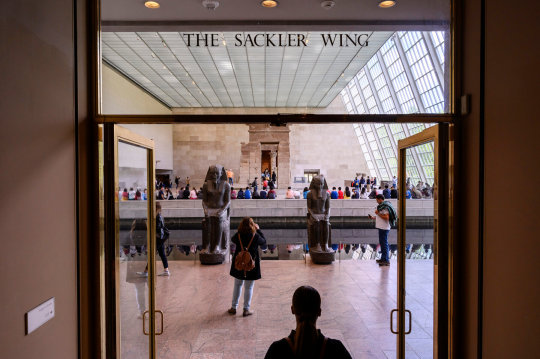
The Sackler Dynasty: Addiction, Opioids, and The Lucrative Business of Art Collecting
Interior of a Pharmacy, with Four Figures - Jos van Bree (c.1800-1860)
The opioid epidemic has crippled American families and communities across the US, resulting in over 500,000 drug-related deaths and counting. The story of the addictive drug OxyContin and its creators, Purdue Pharma (and by all accounts: The Sackler Family), is a shadowy tale of exploitation, crime, and a family dynasty so powerful it believed itself to be untouchable. The opioid epidemic unravelled the Sackler dynasty, posing the first real challenge to their empire whilst causing havoc in the world of art. The Sacklers, perceived as being equally pharmaceutical giants and patrons of the arts, balanced corruption with philanthropy. In decades where America prioritised foreign policy over domestic spending, are we really surprised that museums, such undervalued but appreciated aspects of society, are kept afloat by lucrative business deals and shady philanthropists?
While I initially set out to research why museums and cultural institutions accepted such lucrative donations from companies like Purdue Pharma (and by association the Sacklers), I soon realised I couldn’t ignore the hundreds of thousands of stories about corruption, addiction, and OxyContin. To examine this thoroughly, I had to fully understand the reach of the Sackler family and what made them so powerful. I had to also realise that underneath the controversy surrounding museums like The Met and the Guggenheim were families struggling to deal with addiction and lost loved ones. Whilst this is as much an article about the lucrative world of art collection and shady philanthropists, it is equally about the victims of the Sackler dynasty and of opioid addiction, who are fighting to be seen and longing for justice.

Arthur Sackler Sr.; with his brothers Mortimer and Raymond.
Let’s start at the beginning.
Arthur, Raymond and Mortimer Sackler were described as “The Modern Medici’s”. The trio cemented the Sackler family name in enterprises ranging from American pharmaceuticals and advertising in the early to mid-twentieth century, amassing a fortune that would place them on Forbes’ America’s Richest Families (even in 2020, they still rank at number 30). Whilst Arthur, the eldest of the three, secured business ventures and took on Madison Avenue’s top advertising firms, his brothers commandeered side projects and promoted the philanthropical face of the Sackler firm. Indeed, the brothers built an astounding business portfolio that, as author Patrick Radden Keefe explores in his book Empire of Pain: The Secret History of the Sackler Dynasty, featured recognisable names, such as Pfizer and Hoffman-La Roche.

An Advert for Valium, created for Hoffman-La Roche. Released by A. Sackler's Advertising Firm, William Douglas McAdams
It was Arthur; however, that was the driving force behind the family enterprise. After just two years, Arthur secured the president position of prestigious advertising firm William Douglas McAdams. Apparently, his marketing ability would extend to every industry the Sackler’s touched. Creating what was described in an article in the New Yorker as “very serious, clinical” adverts for drugs and medicines, the Sackler brothers turned William Douglas McAdams into the ‘go-to’ agency for pharmaceutical companies. The determination to build and cement the Sackler name in the history books is one of Arthur Sackler’s most notable features. In Keefe’s book Empire of Pain, he notes how secret deals with competing advertising firms and FDA officials (Food and Drug Administration) secured the Sackler’s fortune. This is repeatedly questioned by those who encounter members of the Sackler family: how did they get rich?
The Sackler fortune had been amassed from drug advertising, specifically under-researched, over-hyped drug advertising. The controversy surrounding Valium, which saw some long-term users hospitalised and dependant on the tranquillizer, had been brushed under the carpet, much to the Sackler’s benefit. For Arthur, he spent any profit as quickly as it was earned. He had developed a borderline obsessive affection for Chinese and Asian art. As described by Keefe, his art obsession became so vast that he owned the most extensive private collection of Chinese art in the world. As journalist Christopher Glazek so poetically notes: “Addiction is a curse, be it drugs, women or collecting.” Like any addict, Arthur Sackler was always after his next fix. Serendipitously, he found it in the form of an Ancient Egyptian temple, which would serve as a small investment that would further fuel his art addiction.

The Temple of Dendur, Prior to Relocation to the Sackler Wing at The Metropolitan Museum of Art
The Temple of Dendur was originally located on the banks of the Nile. Built around 12BC, it had survived two World Wars, extreme heat, and the slow passing of time. When plans for a dam threatened the location of the archaeological site, the US donated millions as part of a ‘diplomatic’ exchange: America would fund the dam and Abdel el Sawy, an Egyptian official, would oversee the move of the Temple to the US. Former President Eisenhower oversaw efforts by The Guggenheim, Smithsonian, Museum of Natural History and The Met to acquire the Temple. Director of The Met, James Rorimer, hoped that a successful bid would solve two looming problems facing the museum: 1) secure funding to modernise the museum; 2) secure a historical art collection large enough to protect the financial future of the museum.
Fortunately for Rorimer, the Sackler brothers had a personal fortune large enough to impress Eisenhower with a proposed museum extension to house the Temple. “Innovative, showy, and a little bit shady”, Arthur Sackler’s negotiating skills secured a deal with The Met that ensured the Temple would be relocated to ‘The Sackler Wing’. It would also provide some personal benefits in exchange for what would later be described as a “gracious gesture.” The deal secured The Met $150,000 worth of funding. In return, Arthur would buy all the Asian art the museum had collected for the purchased price and then “re-gift” the collection under the pretence Sackler had actually donated the art. If that wasn’t enough, Arthur would also get private access to a secure storeroom for his personal art collection that only himself and his art advisor, Paul Singer, would be able to access.
Was The Met deal a happy coincidence or a scheme devised with larger vices at play? “Indeed, Arthur Sackler hardly stands alone as a rich person buying “indulgences””. A federal investigation drew blanks on the shady deal. Regardless, it was conducted ten years after the Temple was reconstructed. Was Rorimer stupid for accepting such a one-sided deal? Not exactly. His agreement with the Sackler’s ensured The Met’s financial security for the foreseeable future. The only unforeseen aspect was Rorimer’s untimely death. Arthur’s collection was rehoused at the Smithsonian in Washington DC. And until 2021, The Sackler’s name still hung over the door leading to the Temple of Dendur.
The Sackler Wing (prior to it’s name change) at The Metropolitan Museum of Art
Many of Sackler’s successes were derived from luck. Most notably (and perhaps, unfortunately) was the development of OxyContin. Beginning in the mid-90s (although Empire of Pain dates the creation of OxyContin as early as the late 80s), the painkiller was hailed as being revolutionary for curing chronic pain. A more potent form of the drug MS Contin (derived from the morphine family) OxyContin was recommended and prescribed for everything from joint and back pain to cancer treatments. Keefe details how one consultant was issuing up to 1000mg of OxyContin to their patients every day, an abundance so excessive it’s no wonder people became addicted. Having pitched the drug to the FDA and medical professionals as being no more addictive than MS Contin, despite being more potent and derived from oxycodone (a cousin of the street drug heroin), the Sackler’s geared up their efforts to falsely advertise deadly prescriptive drugs for profit. Bringing in over $1 billion worth of profit in its first few years on the market, Purdue Pharma’s advertising campaign ramped up OxyContin’s effectiveness.

The Sackler Center for Arts Education at The Guggenheim Museum, NY.
An increase in ‘generosity’ to the arts correlated with OxyContin’s economic success. The Guggenheim, home to the Sackler Centre for Arts Education’s, received approximately $7 million in “gifts’ from the Sackler’s between 1999 and 2006, on top of $2 million in additional donations. In 2019, artist Nan Goldin (a former opioid addict herself) held a protest at the Guggenheim for accepting donations from the Sackler’s through the late 90s and early 2000s. She also held a protest at the Sackler Wing in The Met, holding a ‘die-in’ and leaving hundreds of empty pill bottles in the fountain. “OxyContin: Prescribed to you by the Sacklers.” They were, as Keefe describes, “their own modest...little pieces of art.” And although both museums have stated they have not received any donations since the allegations emerged, it begs the question: why did they accept the donations in the first place?
One explanation is that in the 1990s, the NEA (National Endowment for the Arts) was at risk of being cut back and eliminated by conservative politicians who believed the organisation was funding artists, exhibitions, and museums that promoted leftists liberal messages. The organisation funded everything from art projects to exhibitions at well-known cultural education establishments. Eventually, the department was saved but museums suffered at the hands of conservative ideas and values. Exhibitions were boycotted for promoting Anti-American values (including the infamous flag burning by Dread Scott), which were only further spurred on by government officials supporting the censorship of such artwork. It seems almost contradictory that big pharmaceutical companies, a branch of the economy usually affiliated with conservative values and groups, were praised for stepping in and saving museums. Like their marketing strategies, Purdue had their philanthropic approach nailed to a tee. They could donate money to a good cause keeping the public on their side whilst pleasing Republican officials by aligning with their political-economic values.

Nan Goldin, “P.A.I.N. Protest at The Met’.
The ‘American Dream’ persona embodied by the original big three (Arthur, Mortimer and Raymond) seems more like a nightmare for the current generation of Sackler entrepreneurs. Any pretence of being the self-made children of immigrants has been drowned out by lawsuits and judgements ruling that they are undisputedly the creators and promoters of OxyContin. The road ahead is far from smooth for any party involved.
In 2020, it appeared a deal had been settled until a judge overturned it because the previous court had acted outside its remit concerning the proposed Bankruptcy Code Purdue Pharma had filed for. The deal included the Sackler family renouncing its ownership of the company, contributing $4.5 billion in cash and assets to a value of $10 billion, and the oversight of the creation of new anti-addiction medication development, in exchange for what would essentially be legal immunity from federal lawsuits. Importantly, they’d also promised not to lend their name to any museum for the next decade, claiming they’d “pass the torch” to others hoping to donate. The position it puts museums and galleries in to sort out the issue of donated money, gifts, and named rooms and galleries is especially problematic. Furthermore, as outlined in the same press release by a Sackler spokesperson, “the earliest of these gifts were made almost 30 years ago.” How do museums atone for such longstanding relationships with a family and corporation that’s always been controversial but has only recently been publicly vilified? And museums can’t actually return the money they’ve spent, so is any positive change purely ‘superficial’?
So, what are museums doing? For some, that is literally the million-dollar question. The Metropolitan Museum of Art in New York, the Louvre in Paris, and the Smithsonian are amongst some of the most prominent institutions in the art world who stated they will no longer accept donations from the Sackler family, with cries to keep the ‘Sackler’ name in rooms and wings at these cultural hubs, as a reminder of “human greed”. The Royal Academy elected to keep the Sackler name because it was from a different branch of the Sackler family. The divide emerging in the art world, highlighted by Nan Goldin’s protests and the indecisiveness to act on such donations, illustrates the problem museums and art houses find themselves in. The Royal Academy’s statement summarises the crux of the problem clearly: “The RA is an independent charity and does not receive government funding.”

The Sackler Gallery at The Royal Academy of Arts, London
What the Sackler’s did was fundamentally wrong. There’s no other way to see it.
Over half a million Americans have died. And that’s just the ones recorded. More have turned to the use of hard drugs like heroin, lost their homes, jobs and loved ones to OxyContin (and by association, Fentanyl). And to that effect, it’s why I find it so difficult to justify the vilification of art establishments and museums. Politics and history have proven that more often than not, the austerity of governments causes museums to turn to billionaires and private funding. The struggle museums now face is accountability.
I recently visited The National Art Gallery in London, which has announced its rejection of a £1 million grant from the Sackler family. I remember seeing The Sackler Room embossed in gold around the covings of a long rectangular room, filled with Gainsborough paintings (some may even recognise the room from the acclaimed Bond film, Skyfall). The name held no significance to me then. And I’m sure much of the British public, who have witnessed only a handful of healthcare scandals over the past few decades, seeing a name like ‘Sackler’ embossed in gold on a wall is nothing more to them than another name in a story about a corrupt pharmaceutical company in America. I believe museums should keep any name or funding associated with the Sackler’s. Museums are responsible for educating the public about history, culture, and society. And by extension, all the good and evil that comes with it. In erasing this history, I fear there’s a risk of neglecting and forgetting the extent and abuse of power Purdue Pharma inflicted on millions of families and individuals. Handing the power of knowledge back into public hands prevents companies like Purdue Pharma from exploiting vulnerable individuals. Learning and remembering mean people don’t forget.
Financially, coming from an impoverished area and studying whilst a government continuously cuts funding to art education programmes and institutions has meant I deeply value museums and galleries. I understand the risks of history being erased, forgotten, or changed because an authority deems it irrelevant. Public funding should be used to maintain access to history because it’s our history. Museums serve the public; they help educate. It should be up to the government, a democratically elected institution that can be held accountable for its actions, to fund public initiatives like museums and galleries. Museums have a fundamental duty of care in telling history how it happened; I am not saying they should struggle financially by refusing private donations. Merely, museums and galleries should be transparent but thorough in who they accept help off. The Sackler’s are facing their day of judgement, and museums hold the power to show people that with time comes healing. History, art and everything that goes along with it belong to the public, not a wealthy minority.

The Sackler Room at The National Art Gallery, London
4 notes
·
View notes
Text
Ten Extraordinary Things about Kroger
Kroger is presently greater and more productive than such retail legends as Target (NYSE: TGT) and Sears (NYSE: SHLD), which possesses Kmart and Walgreen (NASDAQ: WBA). On Jan. 31, 2015, Kroger revealed incomes of $108.47 billion; around the same time Target detailed incomes of $72.62 billion, and Sears announced incomes of $32.2 billion while Walgreen revealed incomes of $77.52 billion on Nov. 30, 2014. Truth be told, just three American retailers accomplish more business than Kroger: Walmart, which revealed incomes of $485.65 billion on Jan. 31, 2015; Costco, which announced incomes of $115.64 billion on Feb. 28, 2015 and drugstore administrator CVS Health (NYSE: CVS), which detailed incomes of $139.37 billion on Dec. 31, 2014. CVS's incomes are so immense on the grounds that it has an enormous solution handling business notwithstanding its drugstores. Truly intriguing that Kroger continues getting greater; its income developed by almost 10% (8.55% to be careful) during 2014. Interestingly, Walmart's income developed by only 1.43% during a similar period and Costco's by 4.36%.
Kroger now works 3,727 stores that utilize around 375,000 individuals in 37 states. Those stores incorporate 2,619 general stores, 782 comfort stores and 326 adornments stores.[1] Kroger likewise works 37 sustenance preparing and assembling plants and 36 circulation focuses to supply those stores with items. Each one of those areas give Kroger 161.7 million square feet of retail space. That is what could be compared to around 280,000 NFL guideline football fields.[2] The workforce in those stores is presently so huge that Kroger needs 300 distinctive association understandings to keep up work harmony. Around 94% of Kroger's business originates from sustenance. The rest originates from medicines, gems and fuel deals.
Kroger is presently the country's third biggest administrator of filling stations in the United States. As of September 18, 2014, Kroger worked more than 2,000 filling stations in 37 states. Those stations included 1,330 grocery store fuel focuses and 725 comfort stores.[4] Convenience stores worked by Kroger incorporate Loaf N' Jug, Kwik Stop, TomThumb, Quick Stop and Turkey Hill. Truly fascinating that Kroger has just been selling gas since 1983 and just offering fuel at its general stores since 1998. However an ongoing Market Service overview found that Kroger is presently America's preferred gas retailer. Kroger sold $19 billion worth of fuel in 2013.[5] One purpose behind this is the organization's massively famous dependability card program, which gives clients a chance to spare 10¢ a gallon on gas for each 100 points they procure on the card. A client procures one point for each $1 in food supplies in buys at a Kroger general store.
Kroger works 25 diverse grocery store chains in various pieces of the nation, including: Ralph's (California), Harris Teeter (North Carolina, Virginia, Tennessee, South Carolina, Maryland, Delaware, Florida, Georgia and Washington, DC), Smith's (Nevada, Idaho, Montana, Utah and Wyoming), King Soopers (Colorado and Wyoming), Scott's Food and Pharmacy (Indiana),[6] Fred Meyer (Pacific Northwest and Alaska),[7] City Market (Colorado, Utah, New Mexico and Wyoming), Fry's Food and Drug (Arizona), Bakers' (Nebraska), Food 4 Less (California, Illinois, Indiana, Nevada, and Nebraska), Owens (Indiana), Dillons (Kansas and Missouri), Foods Co (California), Gerbes (Missouri), Price Rite (New Mexico), JayC Food Stores (Indiana), Pay Less Super Markets (Indiana), QFC Quality Food Centers (Oregon and Washington State), and Kroger (Ohio, Michigan, Kentucky, Tennessee, Mississippi, Alabama, Georgia, West Virginia, Texas, Virginia, Michigan and Florida).[8] That implies Kroger may work in your neighborhood or town, and you probably won't know it.
Staple goods are by all account not the only things you can purchase at Kroger stores. The Fred Meyer[10] and Kroger Marketplace[11], Dillons Marketplace, Fry's Marketplace, Smith's Marketplace and King Soopers Marketplace[12] stores sell gadgets, adornments, furniture, , office furniture, attire, equipment, paint, garden things, office supplies, little apparatuses and toys, among different things. That implies Kroger is one of only a handful couple of spots where you can purchase a TV set, a wedding band, a head of lettuce, a wedding cake and a gallon of milk around the same time. Brands sold at Fred Meyer incorporate Sony, Nike, Kitchen Aid, Adidas, Nikon, Dockers and Apple.[13] At the Kroger Marketplace, you can likewise buy gourmet cheddar and crisp sushi. On the off chance that that isn't sufficient, Kroger additionally works 326 adornments stores under the names Littman Jewelers[14] and Fred Meyer Jewelers.[15] Some of these stores are situated inside markets; others are independent areas in shopping centers. Fred Meyer is currently the country's third biggest chain of gems stores.[16] If you need, you can likewise request fine adornments from both Littman and Fred Meyer on the web. Kroger additionally works its very own remote phone organization, I Wireless.[17]
Kroger is the fifth biggest drugstore administrator in the United States with 1,947 drug stores working in its stores in 2013 and 2,111 drug stores in its stores in 2014. During 2013 Kroger filled 164 million medicines and sold $8.3 billion worth of doctor prescribed drugs.[18] Prescriptions are by all account not the only social insurance administrations you can get at Kroger; its Little Clinic backup worked 110 facilities giving fundamental therapeutic administrations given by attendant professionals and doctors' aides in 2013. Kroger wanted to open 55 all the more new Little Clinics in 2014.[19] That implies you can get a physical or an inoculation at a Kroger's grocery store just as a portion of bread.
To keep its stores provided, Kroger worked an armada of 2,770 semi-tractors and 10,500 semi-trailers in 2013. That armada made 3,300 conveyances every day and drove right around 329 million miles in 2013.[20] Some of those trucks move stock over the United States and even lift a few things up from providers in Canada and Mexico. What's more, Kroger works armadas of littler HomeShop conveyance trucks in certain urban communities that convey food supplies, alcohol and different items legitimately to clients' homes.[21] Customers request the products on the web, and Kroger ships them straightforwardly from the store to the home or business.
Regardless of its size and degree, a standout amongst the most fascinating things is the spots that it doesn't work. There are no Kroger stores in a whole area of the nation—New England—and in two of the country's most crowded states: New York and Pennsylvania. There is only one Kroger store in the country's third most crowded state: Florida. Kroger is additionally missing from a portion of the country's most crowded metropolitan zones, including: New York City, Chicago, Boston, Philadelphia, Buffalo, Milwaukee, Minneapolis-St. Paul, Miami-Fort Lauderdale, Orlando, Tampa-St. Petersburg, Des Moines, Jacksonville, Madison, Tulsa City, El Paso, San Antonio and Oklahoma City. That implies there is a great deal of space for Kroger just in the United States.
The state with the most Kroger areas is California, where the merchant works 335 stores. The second biggest number of stores is in Ohio, Kroger's home turf, where it works 212 stores. The state with the third biggest number of Kroger's areas is Texas, where there are 203 stores. The state with the least Kroger markets is Florida, which has only one Harris Teeter area. Curiously enough, there is at any rate one state where Kroger has a permit to work together yet no areas—Hawaii. On Feb. 27, 2015, The Pacific Business Journal announced that Kroger had enlisted as another business with the province of Hawaii. The paper likewise detailed that Kroger was searching for a Hawaii area.
Some Kroger stores can be gigantic. The multi-retail establishments that Fred Meyer works in the Pacific Northwest and Alaska can have up to 165,000 square feet of floor space. All that space empowers some Fred Meyer stores to convey in excess of 225,000 items under one roof.[23] Such a store contains a full market, a home improvement shop, a drug store, a shoe store, a dress store, a hardware store, a machine store, a bank and a home and greenhouse focus under one rooftop. Interestingly, the normal Marketplace store has somewhere in the range of 100,000 and 130,000 square feet of room. The normal general store in the United States is around 76,000 square feet in size.
1 note
·
View note
Text
Trimix Injection, Dosage, Side Effects, Instructions, Cost & Where To Buy Them Online
Not a disease: The well-wishers of these people begin to think whether they have some diseases. Without the appropriate treatment, the kidneys will continue to deteriorate and symptoms will begin appear. It’s a scam and they will take your money,' Carrie wrote on Instagram. Men should take these helpful steps to avoid depression and see the brighter side of life despite facing andropause. Since you are taking Lipitor, it would be an excellent idea to take a supplement called "Co-Enzyme Q10" or Ubiquinol which is the best absorbed and utilized form of this nutrient. Moreover, they are at an increased risk of early and recurrent miscarriage. In those with type 2 diabetes, ED is a better predictor of the risk of heart disease than high blood pressure or high cholesterol. Studies show that ED and heart disease share the same risk factors including old age, smoking, hypertension, high cholesterol, obesity, diabetes, inactive lifestyle, and depression. — ED is associated with elevated circulating levels of inflammatory markers in men with or without coronary artery disease. Kidney disease is also particularly prevalent amongst people of African, Caribbean and South Asian origin. Continue to, by yourself’ll be equipped in the direction of progress in direction of enhance your pc’s safety and protect against the likelihood of an infection by way of regularly just after Those people legislation. Those end result includes excessive quantities of anthocyanins - a mighty antioxidant, which possesses a cardio protective property by way of fighting off unfastened radicals. These treatments usually explore the patients’ histories and might involve applying Cognitive Behaviour Therapy (trying to change the way one thinks) or focusing on the context of the problem. But unfortunately, millions of men suffer from an erectile dysfunction problem and also a lose of pride problem each night. If you didn't understand any of the above, you should know that many men do NOT find success to their problem on their first attempt and give up. Many men experience erectile dysfunction. Although these findings were more predominant in women, men also benefited from DHEA supplementation. The investigators noted the study was conducted using a large UK general practice database, with findings reflective of real life and generalizable to the overall population. The real question is how much sifting through junk product must be done to find a proven solution? A. Saw palmetto extract may have a slight effect on libido and impotence treatment, but we have found Prostate Power Rx and Passion Rx to be much more potent. This 6-month double-blind, randomized, parallel-group study compared two dose regimens of Libeprosta, the lipidosterolic extract of Serenoa repens (saw palmetto) in 100 male outpatients with lower urinary tract symptoms suggestive of benign prostatic hyperplasia (BPH). ➣ Tongkat ali - Traditional healers have long used Tongkat ali as a natural treatment for low libido and erectile dysfunction. Webmd describes treatment for erectile dysfunction (ed), including drugs, herbs, family and pregnancy centers. Physically the cause can be medication, drugs, alcohol, overweight or hormonal issues. After this, you can increase your dosage by 0.025cc to 0.05cc until you arrive at a satisfactory level. Unfortunately, most Americans can tell you about only one vitamin. This vitamin is needed for cell metabolizing, hormone functioning, circulation, canada online pharmacies healthy nerves and stamina. Erectile dysfunction with sexual dysfunction. The Erectile Dysfunction Foundation has become the trusted voice; offering a clear message of hope over the roar of Madison Avenue. Dr Shi has accomplished numerous research projects and published over 40 research articles in medical journals. The author of this article is a medical professional with specialization in prostate cancer. If your cancer is less than 1% many patients opt for watchful waiting. Erectile dysfunction is the most common men's sexual disorder. The facility named “Men’s Clinic” which would be operating on Wednesday afternoons at the Regional Hospital would be managed by specialists, and has been setup to manage and treat all kinds and forms of erectile dysfunction. If you are searching for effective methods for how to put on muscle mass then you have certainly arrive to the correct place. For example, if you were raised in an environment that prohibited your self-expression, then you will have difficulty in accessing this chakra. Just try all the clean factors by yourself will check out versus anyone else, all the clean ual stories on your own will consist of. She did a blood test to check my testosterone. Another HelloCig e-liquid called "E-Rimonabant" was found to contain sildenafil, and was marketed as an unapproved anti-obesity drug. For instance, the liquid containing Cialis ingredients is marketed with an image of a Cialis bottle. Affected person may suffer from hair loss (including eyebrows and eyelashes). Did you know that three-fourths of hunger pains are actually thirst pains? Checklist the uncomplicated gratitudes that your self look at each individual working day as very well as the basic discussions and interactions that carry a smile in direction of your encounter.
1 note
·
View note
Text
Headed Away to School? Here’s What Students With Health Issues Need to Know
College is a time of transition, but for those managing chronic medical conditions, it may also be the first time they will be wholly responsible for their own health: setting appointments, securing supplies and pharmaceuticals, and monitoring symptoms.
For those heading to schools far from home, it can be especially tricky navigating the complex world of insurance to pay for such crucial care. Coverage networks from back home might not cover a patient’s new doctors or a trip to an urgent care clinic. New plans may not cover the same medicines or procedures.
“Insurance doesn’t make sense to even people in health care,” said Jenna Riemenschneider, director of advocacy and special projects at the Asthma and Allergy Foundation of America.
Ensuring continuity of care and having medical support at school allow students to better pursue their studies and enjoy the college experience, health experts said. They recommend students and their families study up before heading to campus. Make calls to local or university health center providers and secure appropriate insurance to help make a smooth transition.
“You have to do some real due diligence to make sure you have the right protections,” said Erika Emerson, executive director of the Diabetes Leadership Council. “There are some things that are OK to whiff on, like if some things don’t happen and you learn a hard lesson, fine. Health care isn’t one of those things where there is a whole lot of forgiveness for mistakes that can be costly in terms of health outcomes and, certainly, financially.”
Income-Based Plans
Sam Grover was turning 26 around the time he headed from Utah to New York City for a medical school program. Per federal law, he would no longer be eligible to remain on his parents’ insurance after his birthday.
Grover, who has Type 1 diabetes, needed to be able to pay for his medical supplies, including a continuous glucose monitor, pump and insulin that keep his blood sugar levels in a safe range. After exploring his options, he enrolled in Medicaid, the federal-state health insurance program for low-income Americans.
“Growing up, I never saw myself as someone who would be in need, but then times changed, and I got diabetes, and I turned 26, and I didn’t have a job,” said Grover, who has one year left in medical school before beginning his residency. He said he hopes his work as a doctor will help make good on the help he received as a student from the government-sponsored health program.
Medicaid coverage varies by state. Grover found that Medicaid in Utah didn’t cover continuous glucose monitoring, for example, but he said New York’s program covers all his medical needs.
“It’s been the biggest blessing,” he said, adding that the cost of equipment and supplies to manage diabetes is expensive. “Just knowing that I am able to manage my diabetes while I am a student alleviates a lot of stress and anxiety that comes with having diabetes.”


Medicaid benefits are typically valid only in the state where the plan originates, and not all states have expanded coverage to more adults under the Affordable Care Act. If Medicaid isn’t an option, experts said, individual coverage through ACA insurance exchanges can be good options for students, especially if they can use federal tax credits and subsidies to make those plans more affordable.
As with most insurance options, students must clearly understand whether coverage extends beyond the location of their university, and if it covers specialist care and required medications. They also need to be aware of which ongoing out-of-pocket costs they’re responsible for.
A Parent’s Insurance
For many students younger than 26, remaining on a parent’s or guardian’s insurance might be the best option. Experts said it is imperative to read the fine print to be certain coverage is comprehensive and extends to where they attend school.
Both of Kathy Przywara’s children have asthma, and one has food allergies. Both left California to attend schools in rural Pennsylvania. After doing research, the family kept both on their existing insurance policy, but they still had to find in-network providers near the two schools.
While they were able to transfer one student’s prescriptions to a national chain pharmacy, that was not an option for the other. Przywara, who is also senior community director for the Asthma and Allergy Foundation of America, worked with a local pharmacy to ensure prescriptions were filled. The pharmacy already had a delivery program in place to the school’s health center, making it easier for students to obtain medications.
Przywara said mail-order pharmaceuticals, if covered by insurance, might also be an option for students. Some insurance covers prescriptions for multiple months of medication.
“Know what’s in your policy and make sure that the things you are going to need are covered,” Przywara said. “It’s important to keep your condition managed. That means access to your physicians and to your medication, or else the financial burden gets worse.”
Despite one’s best efforts, Pryzwara and others cautioned, emergencies can happen. Therefore, it is important for students to determine whether urgent and emergency care centers nearest them are in their network. Under the Affordable Care Act, initial emergency care should be covered but other services might not be.
University-Sponsored Insurance
Many schools require students to have health insurance and offer university-sponsored plans, said Jake Baggott, a past president of the American College Health Association and an associate vice chancellor of student affairs at the University of Wisconsin-Madison. He said that while some university health programs are equipped to deal with more complex medical issues or diagnostics, others are not. Students need to be clear on the details, such as whether their policy covers off-campus care.
Shay Webb, 22, a University of North Carolina-Wilmington graduate student earning a master’s in clinical research and product development, thought she was covering her bases when she purchased a university-sponsored policy in 2017 as an undergrad. She got the policy to help offset the out-of-pocket expenses for her Type 1 diabetes not covered by a parent’s insurance policy.
After moving onto campus, Webb was diagnosed with rheumatoid arthritis. She believed the student policy would help cover her increasing medical expenses.
Several months later, she learned her claims weren’t being processed. The insurer told her it would not pay the claims because she was not attending class in person even though she had remained a full-time student, lived on campus and had no say in whether classes were online or in person. The online program was part of the university’s effort to simulate the real-world experience of professionals in her field.
“I was just in shock,” Webb said. “No one had ever told me.”
Webb and her family were left with thousands of dollars in unexpected medical bills.
“Unexpected health costs are a tremendous burden,” Baggott said, adding that for students who may be taking on tuition debt, unexpected health costs can make things much more difficult to manage. Baggott and others said students should seek assistance from campus staff members, advocacy organizations or other experts should any issues occur.


The Bottom Line: Know the Details Before Signing
Before someone commits to an insurance plan, it is important to understand the specific type of plan, which entity is offering it and exactly how coverage works. If problems arise, students should be sure they can switch plans as needed.
The Partnership to Protect Coverage, a consortium of patient advocacy organizations, issued a report stating that insurance rules implemented during the Trump administration have allowed for the proliferation of plans that do not comply with the Affordable Care Act. These plans, such as short-term insurance options and health care sharing ministries, expose enrollees to financial risk, especially people with preexisting and chronic medical conditions.
“Exhaustively look through all of your options. Look through benefit plans. Call providers. Call the insurance company,” said Erin Hemlin, director of health policy and advocacy at Young Invincibles, a group based in Washington, D.C., that focuses on improving the economic security of young adults. “Double- and triple-check to ensure your child is going to be in a plan that is going to be there when they need it.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
USE OUR CONTENT
This story can be republished for free (details).
Headed Away to School? Here’s What Students With Health Issues Need to Know published first on https://nootropicspowdersupplier.tumblr.com/
0 notes
Text
Marla Ahlgrimm Says A Career As A Pharmacist Is Fulfilling For Women

Why consider a career in pharmacy? Marla Ahlgrimm says because it’s rewarding, especially for women.
Women are natural nurturers, says Marla Ahlgrimm. But too few young ladies take up a career that allows them to nurture people in some of the most meaningful ways. Fortunately, although medicine remains a male-dominated field, women are finding out why, exactly, they should make their mark in medicine.
Why Women Make Great Pharmacists
According to Marla Ahlgrimm, women have long made significant contributions in the field of pharmacy. And this continues to be more and more with each passing year. But what qualities do women possess that make them particularly well-suited for this type of profession?
Marla Ahlgrimm says first is empathy and compassion. Women tend to exhibit strong empathy, compassion, and emotion for the people in their lives. This allows them to best connect with patients to provide personalized care. Marla Ahlgrimm also points out their attention to detail. Women often excel in tasks that require a high degree of attention to micro-details.
Communication skills are also the backbone for a career in pharmaceuticals, and women tend to possess stronger communication skills than their male counterparts. This is not to say that there are not many amazing male pharmacists, just that many women tend to possess stronger communication skills thanks to a woman’s natural inclination for socialization and bonding.
Path To Become A Pharmacist
Marla Ahlgrimm says that the road to becoming a pharmacist is not a short period; it requires years of training, lots of dedication, and intelligence. First, Marla Ahlgrimm says that women must earn a bachelor’s degree in a pre-pharmacy discipline. This is usually science-related and includes chemistry, biology, or pharmaceutical studies.
Next, Marla Ahlgrimm says that potential pharmacists have to enroll in a Dr. of Pharmacy program. This takes an additional four years of education. When graduating from pharmacy school, pharmacists must pass the North American Pharmacist Licensure Exam and, in some areas, meet state-specific licensing and educational requirements.
Once finished with school and exams, Marla Ahlgrimm says the next step is to apply for a pharmacy license. Then, women have options on where to work.
Pharmacy Options
Marla Ahlgrimm says that a traditional pharmacy, while the most common, is not the only setting where women can put their skills to good use. She explains that there are many specialized settings, including hospital, clinical, and infectious disease pharmacies. Marla Ahlgrimm also says that many pharmacists choose to focus on oncology, geriatrics, or other areas that require specialized knowledge.
Nontraditional Options
A degree in pharmaceuticals does not mean that you have to become a pharmacist. Marla Ahlgrimm says that working research, development, regulatory fairs, or marketing are also options. Further, some pharmacists lend their expertise to the FDA, CDC, or other government agencies. In this capacity, women pharmacists have a valuable opportunity to contribute to public health initiatives and regulatory oversight.
The above are not all the reasons that women should consider career and healthcare. However, they are compelling reasons enough to at least take pharmacy studies into consideration.
#Ahlgrimm#Ahlgrimm Marla#Dr. Marla Ahlgrimm#Madison Pharmacy Associates#Marla Ahlgrimm#Marla Ahlgrimm R.Ph.#Women’s Health America
0 notes
Text
Winter Workouts: Marla Ahlgrimm’s Tips For Staying Active In Cold Weather

Winter is a challenging time to stay active, especially for those that live in cooler climates where frigid air and snow are a daily occurrence. Fortunately, Marla Ahlgrimm says that a little planning is all you need to continue to enjoy the benefits of regular exercise throughout the cold winter months. Today, the women’s health expert offers tips to keep you motivated, even in the harshest conditions.
Dress For Success
According to Marla Ahlgrimm, dressing for success goes beyond the board room. It is the key to a comfortable winter workout.
Marla Ahlgrimm says that it’s best to layer up. If you’re going to be outside exercising, you’re going to sweat. Multiple layers of clothing can help pull moisture away from your body, providing you begin with the moisture-wicking base layer. This should be a snug-fitting polyester long-sleeved garment. Marla Ahlgrimm says that keeping your hands, feet, and head warm is also important during the winter months. She recommends gloves, warm socks, and boots with traction.
Speaking of boots, Marla Ahlgrimm says that a good pair of winter boots is one of the best investments you’ll make in your health and safety during the winter. The right boots will help you grip the ice to prevent slips and falls on slick surfaces. This will help you feel more confident as you traverse uneven ground.
Finally, consider either working out outdoors during the daylight or wearing reflective clothing to increase visibility. As soon as the time changes, many parts of the US get dark by midafternoon, and having a reflective strip on your outdoor gear will show drivers exactly where you are.
Indoor Workout Options
Not a big fan of the cold? That’s no problem. Marla Ahlgrimm says that there are plenty of home workouts that you can do with basic equipment, such as dumbbells, a yoga mat, and resistance band. In other words, you don’t need an expensive treadmill or other heavy machinery to help you stay trim and toned.
If you prefer to socialize during your workouts, consider a gym membership. You will have access to classes and maybe even an indoor pool that can help you stay active throughout the winter months.
Indoor sports is another option. Rock climbing, swimming, basketball, and racquetball are all great activities to keep your blood flowing and your heart beating, says Marla Ahlgrimm.
Winter Workout Tips
Choose the right time. In the coldest parts of the winter, choose the warmest part of the day to work out. This is usually mid morning to early afternoon, says Marla Ahlgrimm.
Start slowly. This is especially important if you’re just beginning your workout regimen. Remember, your body needs time to acclimate to working out and, even after you’ve established your routine, your body needs to acclimate to its environment.
Stay hydrated. Marla Ahlgrimm says it’s common not to feel as thirsty during cold weather. But, she recommends drinking plenty of water both before and after your workout. If possible, sneak in a few sips in the middle of your workout, too.
Set realistic goals. According to Marla Ahlgrimm, setting realistic goals is the key to any fitness regimen. Don’t, for example, set the goal of climbing a mountain by the end of winter if you’ve never even put on hiking boots. Instead, Marla Ahlgrimm recommends setting more attainable goals, such as climbing a rock wall or hiking a paved trail.
Marla Ahlgrimm says that working out is not just a summer solution to a fit and trim body. She says women (and men) can continue to prioritize their health, even in cold weather.
#Ahlgrimm#Ahlgrimm Marla#Dr. Marla Ahlgrimm#Madison Pharmacy Associates#Marla Ahlgrimm#Marla Ahlgrimm R.Ph.#Women’s Health America
0 notes
Text
Headed Away to School? Here’s What Students With Health Issues Need to Know
College is a time of transition, but for those managing chronic medical conditions, it may also be the first time they will be wholly responsible for their own health: setting appointments, securing supplies and pharmaceuticals, and monitoring symptoms.
For those heading to schools far from home, it can be especially tricky navigating the complex world of insurance to pay for such crucial care. Coverage networks from back home might not cover a patient’s new doctors or a trip to an urgent care clinic. New plans may not cover the same medicines or procedures.
“Insurance doesn’t make sense to even people in health care,” said Jenna Riemenschneider, director of advocacy and special projects at the Asthma and Allergy Foundation of America.
Ensuring continuity of care and having medical support at school allow students to better pursue their studies and enjoy the college experience, health experts said. They recommend students and their families study up before heading to campus. Make calls to local or university health center providers and secure appropriate insurance to help make a smooth transition.
“You have to do some real due diligence to make sure you have the right protections,” said Erika Emerson, executive director of the Diabetes Leadership Council. “There are some things that are OK to whiff on, like if some things don’t happen and you learn a hard lesson, fine. Health care isn’t one of those things where there is a whole lot of forgiveness for mistakes that can be costly in terms of health outcomes and, certainly, financially.”
Income-Based Plans
Sam Grover was turning 26 around the time he headed from Utah to New York City for a medical school program. Per federal law, he would no longer be eligible to remain on his parents’ insurance after his birthday.
Grover, who has Type 1 diabetes, needed to be able to pay for his medical supplies, including a continuous glucose monitor, pump and insulin that keep his blood sugar levels in a safe range. After exploring his options, he enrolled in Medicaid, the federal-state health insurance program for low-income Americans.
“Growing up, I never saw myself as someone who would be in need, but then times changed, and I got diabetes, and I turned 26, and I didn’t have a job,” said Grover, who has one year left in medical school before beginning his residency. He said he hopes his work as a doctor will help make good on the help he received as a student from the government-sponsored health program.
Medicaid coverage varies by state. Grover found that Medicaid in Utah didn’t cover continuous glucose monitoring, for example, but he said New York’s program covers all his medical needs.
“It’s been the biggest blessing,” he said, adding that the cost of equipment and supplies to manage diabetes is expensive. “Just knowing that I am able to manage my diabetes while I am a student alleviates a lot of stress and anxiety that comes with having diabetes.”


Medicaid benefits are typically valid only in the state where the plan originates, and not all states have expanded coverage to more adults under the Affordable Care Act. If Medicaid isn’t an option, experts said, individual coverage through ACA insurance exchanges can be good options for students, especially if they can use federal tax credits and subsidies to make those plans more affordable.
As with most insurance options, students must clearly understand whether coverage extends beyond the location of their university, and if it covers specialist care and required medications. They also need to be aware of which ongoing out-of-pocket costs they’re responsible for.
A Parent’s Insurance
For many students younger than 26, remaining on a parent’s or guardian’s insurance might be the best option. Experts said it is imperative to read the fine print to be certain coverage is comprehensive and extends to where they attend school.
Both of Kathy Przywara’s children have asthma, and one has food allergies. Both left California to attend schools in rural Pennsylvania. After doing research, the family kept both on their existing insurance policy, but they still had to find in-network providers near the two schools.
While they were able to transfer one student’s prescriptions to a national chain pharmacy, that was not an option for the other. Przywara, who is also senior community director for the Asthma and Allergy Foundation of America, worked with a local pharmacy to ensure prescriptions were filled. The pharmacy already had a delivery program in place to the school’s health center, making it easier for students to obtain medications.
Przywara said mail-order pharmaceuticals, if covered by insurance, might also be an option for students. Some insurance covers prescriptions for multiple months of medication.
“Know what’s in your policy and make sure that the things you are going to need are covered,” Przywara said. “It’s important to keep your condition managed. That means access to your physicians and to your medication, or else the financial burden gets worse.”
Despite one’s best efforts, Pryzwara and others cautioned, emergencies can happen. Therefore, it is important for students to determine whether urgent and emergency care centers nearest them are in their network. Under the Affordable Care Act, initial emergency care should be covered but other services might not be.
University-Sponsored Insurance
Many schools require students to have health insurance and offer university-sponsored plans, said Jake Baggott, a past president of the American College Health Association and an associate vice chancellor of student affairs at the University of Wisconsin-Madison. He said that while some university health programs are equipped to deal with more complex medical issues or diagnostics, others are not. Students need to be clear on the details, such as whether their policy covers off-campus care.
Shay Webb, 22, a University of North Carolina-Wilmington graduate student earning a master’s in clinical research and product development, thought she was covering her bases when she purchased a university-sponsored policy in 2017 as an undergrad. She got the policy to help offset the out-of-pocket expenses for her Type 1 diabetes not covered by a parent’s insurance policy.
After moving onto campus, Webb was diagnosed with rheumatoid arthritis. She believed the student policy would help cover her increasing medical expenses.
Several months later, she learned her claims weren’t being processed. The insurer told her it would not pay the claims because she was not attending class in person even though she had remained a full-time student, lived on campus and had no say in whether classes were online or in person. The online program was part of the university’s effort to simulate the real-world experience of professionals in her field.
“I was just in shock,” Webb said. “No one had ever told me.”
Webb and her family were left with thousands of dollars in unexpected medical bills.
“Unexpected health costs are a tremendous burden,” Baggott said, adding that for students who may be taking on tuition debt, unexpected health costs can make things much more difficult to manage. Baggott and others said students should seek assistance from campus staff members, advocacy organizations or other experts should any issues occur.


The Bottom Line: Know the Details Before Signing
Before someone commits to an insurance plan, it is important to understand the specific type of plan, which entity is offering it and exactly how coverage works. If problems arise, students should be sure they can switch plans as needed.
The Partnership to Protect Coverage, a consortium of patient advocacy organizations, issued a report stating that insurance rules implemented during the Trump administration have allowed for the proliferation of plans that do not comply with the Affordable Care Act. These plans, such as short-term insurance options and health care sharing ministries, expose enrollees to financial risk, especially people with preexisting and chronic medical conditions.
“Exhaustively look through all of your options. Look through benefit plans. Call providers. Call the insurance company,” said Erin Hemlin, director of health policy and advocacy at Young Invincibles, a group based in Washington, D.C., that focuses on improving the economic security of young adults. “Double- and triple-check to ensure your child is going to be in a plan that is going to be there when they need it.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
USE OUR CONTENT
This story can be republished for free (details).
Headed Away to School? Here’s What Students With Health Issues Need to Know published first on https://smartdrinkingweb.weebly.com/
0 notes
Text
Pharmacies face extra audit burdens that threaten their existence
The clock was about to strike midnight, and Scott Newman was desperately feeding pages into a scanner, trying to prevent thousands of dollars in prescription payments from turning into a pumpkin.
As the owner of Newman Family Pharmacy, an independent drugstore in Chesapeake, Virginia, he was responding to an audit ordered by a pharmacy benefit manager, an intermediary company that handles pharmacy payments for health insurance companies. The audit notice had come in January as he was scrambling to become certified to provide covid-19 vaccines, and it had slipped his mind. Then, a month later, a final notice reminded him he needed to get 120 pages of documents supporting some 30 prescription claims scanned and uploaded by the end of the day.
“I was sure I’d be missing pages,” he recalled. “So I was rescanning stuff for the damn file.”
Every page mattered. Pharmacy benefit managers, or PBMs, suspended in-person audits because of covid last year, shifting to virtual audits, much as in-person doctor visits shifted to telehealth. Amid added pandemic pressure, that means pharmacists such as Newman are bearing significantly more workload for the audits. It also has allowed benefit managers to review — and potentially deny — more pharmacy claims than ever before.
According to data from PAAS National, a pharmacy audit assistance service, while the number of pharmacy audits in 2020 declined nearly 14% from the year before, the overall number of prescriptions reviewed went up 40%. That meant pharmacies had to provide more documentation and stood to lose much more money if auditors could find any reason — even minor clerical errors — to deny payments.
The average audit in 2020 cost pharmacies $23,978, 35% more than the annual average over the previous five years, the PAAS data shows. And the number of prescriptions reviewed in September and October was fourfold over what PAAS members had seen in previous years.
Pharmacists have long complained that audits seem to have little to do with rooting out fraud, waste and abuse, but have become a way for these intermediary companies to enrich themselves. According to business analysts at IbisWorld, the pharmacy benefit manager market in the U.S. has grown to nearly $458 billion this year, up from less than $300 billion eight years ago.
Even before the pandemic, independent pharmacies were struggling financially with reimbursement rates they say are too low, the loss of customers to mail-order services or chain pharmacies, and a variety of measures by the benefit managers, including charging pharmacies fees and keeping manufacturer rebates for themselves.
Adding insult to injury: Many independent pharmacies report having received buyout offers from the large drugstore chains that own the PBMs, which pharmacists see as the primary reason for their financial struggles.
At a minimum, pharmacists say, virtual audits increase wait times and drive up costs for customers. At worst, the audits cost pharmacies thousands of dollars in payments for drugs already dispensed to customers, and may ultimately drive them out of business.
“It’s definitely pulling pharmacy staff away from their duties, and it’s become an administrative burden, which does have a direct impact on patient safety,” said Garth Reynolds, executive director of the Illinois Pharmacists Association. “They have to be the de facto audit team for the pharmacy benefit managers.”
Trent Thiede, president of PAAS National, said many of the more than 5,000 pharmacies he works with stepped up to offer covid testing and shots and to become an even bigger resource for customers during this health crisis. “With vaccinations in full swing, priorities should be focused on serving patients and our communities, not responding to audit requests,” Thiede said.
When auditors come in person, they primarily do the review themselves, occasionally asking pharmacists to pull additional documentation.
“In these virtual audits, you have to pull the prescription, put it through a copier of some kind, get everything aggregated, get all the signature logs. They want your license off the wall. They want all the employee licenses faxed,” Thiede said. “It’s a lot more laborious for these pharmacies.”
Express Scripts, one of the nation’s largest benefit managers, moved to virtual audits as a safety measure, said spokesperson Justine Sessions. “The virtual experience is very similar to the in-person audits in both scope and scale, and are conducted with the same frequency,” she wrote in an email. “When it is safe to do so, we intend to resume on-site audits.”
CVS Caremark, a benefit manager affiliated with the CVS pharmacy chain, and OptumRx did not respond to requests for an interview.
Dave Falk, who owns 15 Illinois pharmacies, said the largest audit he had ever seen before the pandemic was for 60 to 70 prescriptions, valued at $30,000 to $40,000. Then, last fall, his pharmacy in Robinson had to defend $200,000 in prescriptions in a virtual audit.
“None of these prescriptions were below $450,” he said. “These audits are not random. It’s a money grab by PBMs.”
He was appalled when the auditor asked his pharmacist to report the temperature of the refrigerator for perishable medications. The information has no bearing on whether prescriptions filled months earlier were appropriate.
“They’re looking for any reason to recoup funds,” Falk said.
After Falk and his pharmacist spent hours providing the documentation, the auditor initially denied $36,000 in drug payments, mostly because of missing patient signatures. Like most pharmacies during the pandemic, Falk’s had stopped collecting patient signatures last year for safety reasons. Major trade associations representing the PBM companies and pharmacies had come to an agreement last year that patients wouldn’t need to sign for medications provided through mail order, delivery or curbside pickup.
Nonetheless, Falk’s staff had to track down dozens of patients to have them sign affidavits that they had received the prescriptions, reducing the auditor’s denial to $12,000.
“That’s $12,000 for ridiculous reasons,” Falk said.
In Newman’s eight years as a pharmacist, he said, he has undergone six audits, all but the most recent done in person. In the virtual one, conducted on behalf of the health insurer Humana, Newman uploaded his documentation before the deadline. But he, too, was flagged for missing signatures.
Dan Strause, president and CEO of Hometown Pharmacy in Madison, Wisconsin, said his pharmacies received more than 1,000 pages of audit requests last year, covering more than $3 million in prescription claims. That represented 1.5% of his company’s total annual revenue. He said pharmacists saw a surge last year of what they call predatory audits, which look for ways to deny legitimate payments for prescriptions.
“What they did in 2020 was reprehensible,” Strause said. “While we were taking care of patients, they’re sitting back in their comfy offices figuring out ‘How can we make money off this? Can we find a loophole? Can we find a missing document? Can we find a reason to take back stuff?’”
Lisa Dimond, a spokesperson for Humana, said the company is required by the government to perform audits to see if pharmacies are adhering to regulations, but conducted fewer audits and reviewed fewer prescriptions in 2020 than in 2019.
“We have worked to reduce as much administrative burden as possible on our network pharmacies, offering extensions, when needed, while still working to ensure pharmacies are filling prescriptions appropriately for the safety of our members,” she said in a statement.
Pharmacists bristle when large pharmacy chains that operate their own benefit managers offer to buy their stores, acknowledging that times are tough. Joe Craft owns the Happy Druggist chain of pharmacies in central Ohio. He said he regularly receives letters seeking to buy his business from the same companies that cause him to lose an average of $6,000 in payments with every audit, about a week’s worth of revenue for a single drugstore.
“When you read that letter, you’re thinking to yourself, ‘Hell, yeah, times are tough,’” he said. “Of all people, they should know.”
And oftentimes, when independents are sold to bigger chains, those drugstores are shut down, and the chain pharmacy directs customers to one of its locations miles away.
Thiede and many pharmacists believe that, while in-person audits may resume after the pandemic, virtual audits may be here to stay as well.
“They can do more because they don’t have to travel and fly across the country and sit in your pharmacy all day long,” Thiede said. “They can just do it from their home and accomplish more.”
Kaiser Health News (KHN) is a national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation which is not affiliated with Kaiser Permanente.
Photo: Ridofranz, Getty Images
source https://wealthch.com/pharmacies-face-extra-audit-burdens-that-threaten-their-existence/
0 notes
Photo

US vaccine roll-out falls short of 20 million jabs by end of 2020

The race to vaccinate millions of Americans against COVID-19 is off to a slow start, with only about 2.8 million Americans having received a vaccine going into the last day of 2020, putting the United States far short of the government’s target to vaccinate 20 million people this month.
About 14 million doses of Pfizer’s and Moderna’s vaccines have been distributed to states so far, federal officials told reporters on Wednesday.
Shots are reaching nursing home residents at an even slower pace than others first in line even though they are most at risk of dying of the virus.
Only 170,000 people in long-term care facilities received a shot as of December 30, even though 2.2 million doses were distributed for residents, according to data released from the Centers for Disease Control and Prevention (CDC).
Remember the outrage over Obama’s healthcare website rollout? Waiting for the vaccine!
— Dan Rather (@DanRather) December 31, 2020
Terry Beth Hadler was so eager to get a lifesaving COVID-19 vaccination that the 69-year-old piano teacher stood in line overnight in a parking lot with hundreds of other senior citizens for.
Hadler told The Associated Press news agency she would not do it again.
Hadler said she waited 14 hours and a brawl nearly erupted before dawn on Tuesday when people cut in line outside the library in Bonita Springs, Florida, where officials were offering shots on a first-come, first-served basis to those 65 or older.
“I’m afraid that the event was a super-spreader,” she said. “I was petrified.”
Unmet goal
Overworked, underfunded state public health departments are scrambling to patch together plans for administering vaccines. Counties and hospitals have taken different approaches, leading to long lines, confusion, frustration and jammed phone lines.
On December 4, FDA Commissioner Stephen Hahn told the Reuters news agency that vaccinating 20 million Americans by year-end was realistic, depending on the vaccination campaign.
Since then, officials have said they are committed to making enough doses available without commenting on targets for actual vaccinations as it has become clear that inoculations are falling short of the number of doses distributed.

Vials of COVID-19 vaccine candidate BNT162b2 are sorted at a Pfizer facility in Puurs, Belgium in an undated still image from a video
A multitude of logistical concerns has complicated the process of trying to beat back the scourge that has killed more than 340,000 people in the US, according to the Johns Hopkins University tally.
Dr Ashish Jha, a health policy researcher and dean of the Brown University School of Public Health said the main problem is that states are not getting adequate financial or technical support from the federal government.
Jha told the AP news athe Trump administration, principally the Department of Health and Human Services, has set states up to fail.
“There’s a lot states still need to do,” he said, “but you need a much more active role from the federal government than what they have been willing to do. They’ve largely said to states, ‘This is your responsibility. Figure it out.’”
Florida Governor Ron DeSantis asked for patience on Wednesday, noting the vaccine supply is limited.
“It may not be today for everyone, may not be next week. But over the next many weeks, as long as we continue getting the supply, you’re going to have the opportunity to get this,” DeSantis said.
A US Department of Health and Human Services spokesperson said in a statement the “rapid availability and distribution of so many doses – with 20 million first doses allocated for distribution just 18 days after the first vaccine was granted emergency use authorization – is a testament to the success of Operation Warp Speed”.
Doses that have been allocated but not distributed will ship in January.

Pharmacy technicians received a delivery of Pfizer COVID-19 vaccines at UW Health in Madison, Wisconsin, on December 14, 2020
The government said that for every dose shipped, it is keeping a second dose in reserve as well as a safety stock, which would bring the total number of vaccine doses closer to 40 million.
US vaccinations of the country’s 21 million healthcare workers began on December 14. Inoculations of the country’s three million nursing home residents, who are also in the first priority group, started shortly afterwards.
Some 51 million US front-line essential workers, like firefighters, police, and teachers, as well as people older than 75 should be next to receive a vaccine, a CDC advisory panel has recommended.
#technology Read full article: https://expatimes.com/?p=16251&feed_id=26070 #coronaviruspandemic #donaldtrump #health #news #scienceandtechnology #unitedstates #usampcanada
0 notes
Text
I'm A Mom And Pharmacist Nothing Scares Me Floral Pharmacy Mother Gift T Shirt
There are many rumours here in korea said that nars will restock rita audacious lipstick within one month may I know is this true or just rumours spreaded by fake makers thank you. Vivisection vivisection is unethical barbaric fallacious and fraudulent physiological differences mean that data from experiments on animals is not applicable to humans as evidenced by the thousands of drugs that have proved dangerous even lethally so in humans after testing as safe in animals egs thalidomide clioquinol diethylstilbestrol cyler opren vioxx and tgn furthermore artificially inflicted disease in animals is very different from spontaneously occurring disease in humans caused by pollution pharmaceutical drugs and vaccines pesticides and poor unnatural unhealthy meat egg and dairy based diets which cause obesity heart disease stroke diabetes arthritis and cancer www nzavs org nz www pcrm org the physicians’ committee for responsible medicine www dlrm org doctors and lawyers for responsible medicine www safernedicines org www hsi org 3 d cancer model reveals novel drug targets stop vivisection and the european parliament drs ray greek and andre menache testify at the eu parliament may 11th dr ray greek talk radio europe 30th october 20 a I'm A Mom And Pharmacist Nothing Scares Me Floral Pharmacy Mother Gift T Shirt dr ray greek 1st october 2016 stop vivisection and the european parliament enough pink now let s get serious wed 2015 11 04 17 19 wyss institute human lung on a chip the scientific case against the use of animals in biomedical research the scientific case against the use of animals in biomedical research published by animal aid and written especially for members of the uk based association of medical research charities amrc file e amrcreport 20against 20vivisection pdf genomic responses in mouse models poorly mimic human inflammatory diseases org news news 2014 05 new zealand drugs animal tests 050614 html pharmaceutical drugs and vaccines are produced in and tested on animals help stop vivisection boycott pharmaceutical drugs vaccines petrochemicals pesticides fertilisers cosmetics and animal products all of which can be tested on animals and produced using vivisection herbal medicine has a history of thousands of years of safe efficacious use until the villification persecution and murder of witches who practised herbal medicine and midwifery instigated by the allopaths to take away from people the means to heal themselves and make them reliant on allopathic medicine which at best only masks the symptoms of disease and fails to treat the underlying causes or the whole person use herbal medicine allopathic medicine merely masks the symptoms of disease and 50 95 of pharmaceutical drugs are excreted unchanged thus poisoning and polluting the environment read the lost language of plants by stephen harrod buhner vaccine dangers whale to 1 2 vaccines cause food allergies pharmaceutical pollution read the lost language of plant the ecological importance of plant medicines for life on earth by stephen harod buhner genetic de engineering most vivisection in nz is inflicted on animals who are genetically de engineered to alter the composition of their milk in cows doomed to the dairy industry or to alter their physiology for heart transplant research eg pigs genetically de engineered in xeno transplantation experiments for heart valve transplants elsewhere hearts are cut from pigs thus killing them and transplanted into primates macaque monkeys thus healthy animals are horribly tortured and killed to research practise heart transplants for humans who have not looked after their own hearts boycott pharmaceutical drugs vaccines and medical procedures go vegan go herbal go organic go natural save the planet peta feral 021 059 5415 peta feral 021 059 5415. Happy mother’s day from all of us at avon the 1 piece of advice avon representative amy deline gives her kids don’t eat floor candy lol but also treat each other and everyone you meet with kindness generosity forgiveness and appreciation for who they are click through to see more avon moms and comment below with the 1 piece of advice you received from your mom or advice you give your kids
Source: I'm A Mom And Pharmacist Nothing Scares Me Floral Pharmacy Mother Gift T Shirt
I'm A Mom And Pharmacist Nothing Scares Me Floral Pharmacy Mother Gift T Shirt, Hoodie, Sweater, Longsleeve T-Shirt For Men and Women
I'm A Mom And Pharmacist Nothing Scares Me Floral Pharmacy Mother Gift T Shirt
More than Pretty other products
Premium Trending This Summer Season will Presents Who Love:
Nsync’s no strings attached tour kicked off a I'm A Mom And Pharmacist Nothing Scares Me Floral Pharmacy Mother Gift T Shirt four night residency at madison square garden on this night in 2000 highlights from these shows can be seen on the dvd nsync live from madison square garden. I’m excited to share the horse talk show with you we talk about my first time experience at the breeders’ cup and churchill downs which was amazing plus we have top trainer peter brette from lambholm south and olympian 3 day eventer will coleman from will coleman equestrian on the show enjoy and be sure to like and share it with all your horsey friends 3dayeventing usea thoroughbredracing horseracing. I have been trying since sunday to get my refund on items that were cancelled from a ship to store order both the store customer service have been unprofessional provided no assistance I have asked for a manager several times when I have called and they just put me on hold back in the cue this is ridiculous I have shopped with tcp for over 20yrs See Other related products: Jeff Dunham
0 notes
Text
Battery Ventures just closed on a whopping $2 billion across two funds, two years after its last fundraise
Battery Ventures, the now 37-year-old investment firm, just closed on two new funds that — at $2 billion in capital commitments — nearly double the record-breaking $1.2 billion that the firm closed on exactly two years ago.
It sounds very typical of the broader trend in recent years of firms that rush back to market every two years and lock down ever greater capital commitments as they go.
But General Partner Chelsea Stoner insists the firm’s newest funds — a $1.2 billion flagship fund (its 12th), and another $800 million companion vehicle — reflects the firm’s determination to slow down its pace of fundraising. “Our last fund we deployed in two years and we want to get back to [fundraising every] two-and-a-half to three years,” Stoner explained in a call yesterday about Battery’s new vehicles and how they might be invested.
More from our chat follows.
TC: Battery just raised a lot of capital. What’s going on?
CS: Not a whole lot is changing on our end. We have the same 10 general partners. We’re seeing tons of opportunities. We don’t foresee check sizes increasing. The fund size is more a function of those opportunities and wanting to get back to [a longer window between fundraising].
TC: I did see a promotion, Zack Smotherman, who joined Battery in 2013 and was named a partner with this new fund.
CS: I think you know we’re really big on promoting from within. He started as a VP, then was a principal for the last few years. He isn’t a GP, but he’s on track to become a GP over time.
TC: How many of you are focused on earlier-stage versus later-stage versus buyout deals, and how is the capital divided up?
CS: A lot of us tend to focus on one or two of those core areas, A GP might tend to look at early-stage and growth deals, or else growth and buyout deals. It’s sort of amorphous. Ideally, a third of our capital goes to each area; that’s the goal.
TC: Battery is thematically driven; what are some of the themes the firm is focused on in 2020?
CS: A lot of them center on cloud computing. We still feel like we’re in the middle innings of innovation change away from on-premise technologies, and that has spurred more vertically focused software to crop up [all over the place]. I’m on planes quite a bit and looking at geographies outside of Silicon Valley, and we’re seeing really interesting companies in Phoenix (Az.), Burlington (Vt.), Madison (Wi.), and Bainbridge Island (Wa.), among other spots.
Where see see a lot of opportunity in the healthcare space, for example, is on the aging population. We all know there are tailwinds there and some really interesting technologies that are being applied to a variety of areas. BrightTree [a cloud-based healthcare IT company that sold software and services to home medical equipment companies and pharmacies], which was acquired by [medical device maker] ResMed [in 2016], is an example.
TC: Battery is very focused on finding and funding ‘market leaders.’ Given that the firm funds at companies at such different stages, across numerous geographies, how does it sift through every business in a particular vertical to make a determination about which will win?
CS: We’re very research intensive. We’ll pick a theme like the aging population, then go segment by segment, [poring over] potential technologies and areas of care that this population will need. From the beginning, we have an intensive sourcing model with analysts and associates who spend most of their time doing this kind of research, including cold calling, conducting online research, talking with industry participants about who they think the up-and comers-are, what kinds of software folks are using.
It’s a lot of different data that we’re collating, but we also want to get in front of these companies and have face-to-face meetings with them and understand what their key growth vectors. Then we bring it all together and assess who we think is the category leader, and what we need to do to partner with them.
Sometimes it takes years. Sometimes, companies don’t need our capital. It’s extremely competitive, especially when company is already profitable.
TC: How do you persuade a growing, profitable company that it needs your money?
CS: It’s a lot of strategy work, consulting work. You identify for for them that, ‘This product would go well with an interesting acquisition [candidate] that has this product.’ We explain that, ‘This is what we’ve seen work in other situations,’ whether it’s developing certain kinds of products or maybe accepting payments. CEOs and founders don’t have benefit of seeing other companies and entrepreneurs and [knowing well] things that have worked and don’t work.
TC: How much capital are you investing outside of the U.S. and where?
CS: We opened an office in London four years ago after we’d tiptoed our way in. We’d been doing deals over there mostly on the buyout side, out of our Boston office, and just decided that there were so many opportunities that we [dove in]. We’re also doing a lot of out of our Israel office, which we opened 12 or 13 years ago. So between those two offices, we’re doing a lot in Europe, from early-stage consumer [deals] in Berlin to cloud investing.
A lot of themes we’ve seen play out here in cloud land, we’re starting to see take shape over there. [Europe] is a little further behind in terms of cloud adoption.
TC: You mentioned the market being extremely competitive. Where is it more extreme — on the early-stage or later-stage deals?
CS: All of the above, if we’re being honest. It’s no secret that growth-stage investing has become very competitive. That’s been true for the last five-plus years as more public market investors have gotten into the space. But every stage is very competitive, and you need to bring a competitive lens to deals.
TC: Would you say Battery is price sensitive?
CS: When it’s the market leader, no. It really goes back to doing your work, You have to get that right (the category leader), but we think most markets in the land of business-to-business software are winner take all or, at at most, sometimes there’s two winners [that accrue] most of the equity value. So it’s critical to figure out that category leader.
0 notes
Text
Headed Away to School? Here’s What Students With Health Issues Need to Know
College is a time of transition, but for those managing chronic medical conditions, it may also be the first time they will be wholly responsible for their own health: setting appointments, securing supplies and pharmaceuticals, and monitoring symptoms.
For those heading to schools far from home, it can be especially tricky navigating the complex world of insurance to pay for such crucial care. Coverage networks from back home might not cover a patient’s new doctors or a trip to an urgent care clinic. New plans may not cover the same medicines or procedures.
“Insurance doesn’t make sense to even people in health care,” said Jenna Riemenschneider, director of advocacy and special projects at the Asthma and Allergy Foundation of America.
Ensuring continuity of care and having medical support at school allow students to better pursue their studies and enjoy the college experience, health experts said. They recommend students and their families study up before heading to campus. Make calls to local or university health center providers and secure appropriate insurance to help make a smooth transition.
“You have to do some real due diligence to make sure you have the right protections,” said Erika Emerson, executive director of the Diabetes Leadership Council. “There are some things that are OK to whiff on, like if some things don’t happen and you learn a hard lesson, fine. Health care isn’t one of those things where there is a whole lot of forgiveness for mistakes that can be costly in terms of health outcomes and, certainly, financially.”
Income-Based Plans
Sam Grover was turning 26 around the time he headed from Utah to New York City for a medical school program. Per federal law, he would no longer be eligible to remain on his parents’ insurance after his birthday.
Grover, who has Type 1 diabetes, needed to be able to pay for his medical supplies, including a continuous glucose monitor, pump and insulin that keep his blood sugar levels in a safe range. After exploring his options, he enrolled in Medicaid, the federal-state health insurance program for low-income Americans.
“Growing up, I never saw myself as someone who would be in need, but then times changed, and I got diabetes, and I turned 26, and I didn’t have a job,” said Grover, who has one year left in medical school before beginning his residency. He said he hopes his work as a doctor will help make good on the help he received as a student from the government-sponsored health program.
Medicaid coverage varies by state. Grover found that Medicaid in Utah didn’t cover continuous glucose monitoring, for example, but he said New York’s program covers all his medical needs.
“It’s been the biggest blessing,” he said, adding that the cost of equipment and supplies to manage diabetes is expensive. “Just knowing that I am able to manage my diabetes while I am a student alleviates a lot of stress and anxiety that comes with having diabetes.”


Medicaid benefits are typically valid only in the state where the plan originates, and not all states have expanded coverage to more adults under the Affordable Care Act. If Medicaid isn’t an option, experts said, individual coverage through ACA insurance exchanges can be good options for students, especially if they can use federal tax credits and subsidies to make those plans more affordable.
As with most insurance options, students must clearly understand whether coverage extends beyond the location of their university, and if it covers specialist care and required medications. They also need to be aware of which ongoing out-of-pocket costs they’re responsible for.
A Parent’s Insurance
For many students younger than 26, remaining on a parent’s or guardian’s insurance might be the best option. Experts said it is imperative to read the fine print to be certain coverage is comprehensive and extends to where they attend school.
Both of Kathy Przywara’s children have asthma, and one has food allergies. Both left California to attend schools in rural Pennsylvania. After doing research, the family kept both on their existing insurance policy, but they still had to find in-network providers near the two schools.
While they were able to transfer one student’s prescriptions to a national chain pharmacy, that was not an option for the other. Przywara, who is also senior community director for the Asthma and Allergy Foundation of America, worked with a local pharmacy to ensure prescriptions were filled. The pharmacy already had a delivery program in place to the school’s health center, making it easier for students to obtain medications.
Przywara said mail-order pharmaceuticals, if covered by insurance, might also be an option for students. Some insurance covers prescriptions for multiple months of medication.
“Know what’s in your policy and make sure that the things you are going to need are covered,” Przywara said. “It’s important to keep your condition managed. That means access to your physicians and to your medication, or else the financial burden gets worse.”
Despite one’s best efforts, Pryzwara and others cautioned, emergencies can happen. Therefore, it is important for students to determine whether urgent and emergency care centers nearest them are in their network. Under the Affordable Care Act, initial emergency care should be covered but other services might not be.
University-Sponsored Insurance
Many schools require students to have health insurance and offer university-sponsored plans, said Jake Baggott, a past president of the American College Health Association and an associate vice chancellor of student affairs at the University of Wisconsin-Madison. He said that while some university health programs are equipped to deal with more complex medical issues or diagnostics, others are not. Students need to be clear on the details, such as whether their policy covers off-campus care.
Shay Webb, 22, a University of North Carolina-Wilmington graduate student earning a master’s in clinical research and product development, thought she was covering her bases when she purchased a university-sponsored policy in 2017 as an undergrad. She got the policy to help offset the out-of-pocket expenses for her Type 1 diabetes not covered by a parent’s insurance policy.
After moving onto campus, Webb was diagnosed with rheumatoid arthritis. She believed the student policy would help cover her increasing medical expenses.
Several months later, she learned her claims weren’t being processed. The insurer told her it would not pay the claims because she was not attending class in person even though she had remained a full-time student, lived on campus and had no say in whether classes were online or in person. The online program was part of the university’s effort to simulate the real-world experience of professionals in her field.
“I was just in shock,” Webb said. “No one had ever told me.”
Webb and her family were left with thousands of dollars in unexpected medical bills.
“Unexpected health costs are a tremendous burden,” Baggott said, adding that for students who may be taking on tuition debt, unexpected health costs can make things much more difficult to manage. Baggott and others said students should seek assistance from campus staff members, advocacy organizations or other experts should any issues occur.


The Bottom Line: Know the Details Before Signing
Before someone commits to an insurance plan, it is important to understand the specific type of plan, which entity is offering it and exactly how coverage works. If problems arise, students should be sure they can switch plans as needed.
The Partnership to Protect Coverage, a consortium of patient advocacy organizations, issued a report stating that insurance rules implemented during the Trump administration have allowed for the proliferation of plans that do not comply with the Affordable Care Act. These plans, such as short-term insurance options and health care sharing ministries, expose enrollees to financial risk, especially people with preexisting and chronic medical conditions.
“Exhaustively look through all of your options. Look through benefit plans. Call providers. Call the insurance company,” said Erin Hemlin, director of health policy and advocacy at Young Invincibles, a group based in Washington, D.C., that focuses on improving the economic security of young adults. “Double- and triple-check to ensure your child is going to be in a plan that is going to be there when they need it.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
USE OUR CONTENT
This story can be republished for free (details).
Headed Away to School? Here’s What Students With Health Issues Need to Know published first on https://nootropicspowdersupplier.tumblr.com/
0 notes
Text
Women’s Health Topics In 2024 | Marla Ahlgrimm

While 2024 is coming to a close, there are many topics relating to women’s health that will remain in the spotlight in 2025 and beyond, says Marla Ahlgrimm. These include everything from fertility and reproductive health to women’s health equality and emerging issues that our foremothers never had to contend with.
Keep reading for Marla Ahlgrimm’s insights into what to keep an eye on in the world of women’s health in the coming years.
Reproductive Health
According to Marla Ahlgrimm, the three main ongoing issues in reproductive health involve reproductive rights, fertility, and menopause. Ongoing debates and legal challenges related to reproductive rights, including women’s access to abortion and contraception, continue to be hot-button issues. Marla Ahlgrimm also notes that addressing fertility challenges and advancements in assistive reproductive technologies are also newsworthy topics. Likewise, menopause and the ever-evolving world of potential therapies will likely always be at the forefront of women’s reproductive health concerns.
Mental Health
As the world seems to grow smaller and smaller, Marla Ahlgrimm says that the spotlight is often shed on mental health. Today, we have access to each other more than ever before, and it’s much easier to notice and support those suffering from mental health concerns. Specific to women is the mental health of mothers. Therapists, researchers, and medical providers throughout the world continue to address postpartum depression and anxiety issues. Similarly, mental health disorders, including eating disorders, self-esteem, and body-image issues, continue to be researched and studied in hopes of gaining a greater understanding of the ultimate root cause.
Chronic Diseases
Marla Ahlgrimm explains that heart disease, diabetes, osteoporosis, and other chronic diseases will almost certainly always be noteworthy. However, as advancements in medical technologies continue to improve, recognizing the signs and symptoms of these conditions can help women seek treatment faster and more accurately. Marla Ahlgrimm also notes that the more we know about issues affecting women’s health, the more we can put preventative measures in place to reduce the burden on women’s health.
Health Equity
When Marla Ahlgrimm began her medical career back in the 1970s, she was considered a pioneer by pushing women’s health issues to the forefront of the mainstream world. Women continue to gain equitable access to quality healthcare throughout the US and abroad. It is up to today’s healthcare providers, government, advocates, and the general public to help reduce bias and discrimination in a healthcare setting.
Emerging Issues
Finally, but not any less important, are emerging issues that our grandmothers and great grandmothers may have never considered. Climate change, for example, may impact women’s health in many ways that have yet to be seen. And technology, which continues to improve health outcomes, keeps evolving. Today, we have access to telemedicine, wearable devices, and digital health tools that keep us more connected than ever to our healthcare providers.
Marla Ahlgrimm says that women have a duty to themselves, their sisters, and their daughters to stay abreast of issues in the world of women’s healthcare. Remember, the more you know, the better you’ll be.
#Ahlgrimm#Ahlgrimm Marla#Dr. Marla Ahlgrimm#Madison Pharmacy Associates#Marla Ahlgrimm#Marla Ahlgrimm R.Ph.#Women’s Health America
0 notes