#lee!clark clipboard
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
There were a total of 171.5 billion posts on Tumblr in 2019.
Text


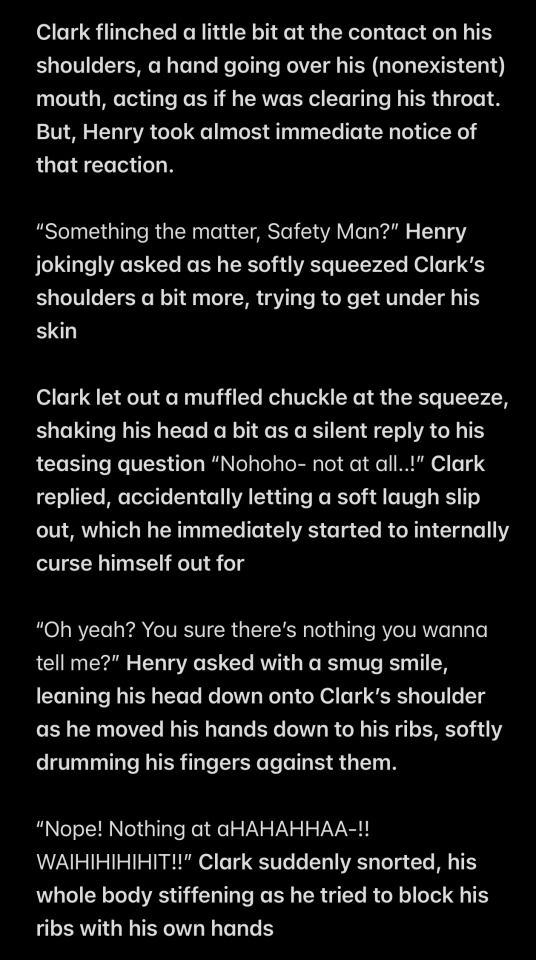



thought I’d drop it
#oc x canon#sfw twords#my oc#finding frankie tickles#finding frankie oc#henry hotline finding frankie#ler!henry hotline#lee!clark clipboard#clark the clipboard#tickle fic#my writing
14 notes
·
View notes
Text
▷ Zoey's Extraordinary Playlist; Season 2 Episode 1 - (S2E1) - HD 720p
Watch Online Zoey's Extraordinary Playlist Season 2 Episode 1 in NBC Full Episodes Eng Sub / Sub English TV Series 2020 Premiere HD! ❖ Zoey's Extraordinary Playlist Full Episodes (HD): Full ✓ NBC TV Shows and Movies from Official Partners. ❖ Watch Zoey's Extraordinary Playlist S2E1 Online ►► P.L.A.Y N.O.W
〘NBC | 4K UHD | HD-1080p | HD-720p | SD-480p | MP4〙
After an unusual event, Zoey Clarke, a whip-smart computer coder forging her way in San Francisco, suddenly starts to hear the innermost wants, thoughts and desires of the people around her through popular songs. ❖ Genre : Drama, Comedy ❖ Air Date : 2021-01-05 ❖ Network : NBC ❖ Casts : Lauren Graham, Alex Newell, Andrew Leeds, Michael Thomas Grant, Jane Levy, Kapil Talwalkar, Mary Steenburgen, John Clarence Stewart, Skylar Astin, Alice Lee Guest Star : Felix Mallard, Jee Young Han, Harvey Guillén
Watch Zoey's Extraordinary Playlist S2E1 Live Stream Watch Zoey's Extraordinary Playlist S2E1 Online Watch Zoey's Extraordinary Playlist S2E1 Dailymotion Watch Zoey's Extraordinary Playlist S2E1 Premiere Watch Zoey's Extraordinary Playlist S2E1 HD720p Watch Zoey's Extraordinary Playlist S2E1 Free Online Watch Zoey's Extraordinary Playlist S2E1 English Subtitle Watch Zoey's Extraordinary Playlist S2E1 Stream Watch Zoey's Extraordinary Playlist S2E1 Full Watch Zoey's Extraordinary Playlist S2E1 HD1080p Watch Zoey's Extraordinary Playlist S2E1 Full Recap Watch Zoey's Extraordinary Playlist S2E1 Online Stream Watch Zoey's Extraordinary Playlist S2E1 HD Watch Zoey's Extraordinary Playlist S2E1 Online HD Watch Zoey's Extraordinary Playlist S2E1 Full Episode Watch Zoey's Extraordinary Playlist S2E1 Synopsis
<iframe width="663" height="382" src="https://www.youtube.com/embed/UyW0jXYe7i8" frameborder="0" allow="accelerometer; autoplay; clipboard-write; encrypted-media; gyroscope; picture-in-picture" allowfullscreen></iframe>
A television show (often simply TV show) is any content produced for broadcast via over-the-air, satellite, cable, or internet and typically viewed on a television set, excluding breaking news, advertisements, or trailers that are typically placed between shows. Television shows are most often scheduled well ahead of time and appear on electronic guides or other TV listings.
Livestreaming, what’s in it for us? Technology has advanced significantly since the first internet livestream but we still turn to video for almost everything. Let’s take a brief look at why livestreaming has been held back so far, and what tech innovations will propel livestreaming to the forefront of internet culture. Right now livestreaming is limited to just a few applications for mass public use and the rest are targeted towards businesses. Livestreaming is to today what home computers were in the early 611110s. The world of livestreaming is waiting for a metaphorical VIC-110, a very popular product that will make live streaming as popular as video through iterations and competition. Shared Video Do you remember when YouTube wasn’t the YouTube you know today? In 11005, when Steve Chen, Chad Hurley, and Jawed Karim activated the domain “www.youtube.com" they had a vision. Inspired by the lack of easily accessible video clips online, the creators of YouTube saw a world where people could instantly access videos on the internet without having to download files or search for hours for the right clip. Allegedly inspired by the site “Hot or Not”, YouTube originally began as a dating site (think 110s video dating), but without a large ingress of dating videos, they opted to accept any video submission. And as we all know, that fateful decision changed all of our lives forever. Because of YouTube, the world that YouTube was born in no longer exists. The ability to share videos on the scale permitted by YouTube has brought us closer to the “global village” than I’d wager anyone thought realistically possible. And now with technologies like Starlink, we are moving closer and closer to that eventuality. Although the shared video will never become a legacy technology, before long it will truly have to share the stage with its sibling, livestreaming. Although livestreaming is over 110 years old, it hasn’t gained the incredible worldwide adoption YouTube has. This is largely due to infrastructure issues such as latency, quality, and cost. Latency is a priority when it comes to livestreams. Latency is the time it takes for a video to be captured and point a, and viewed at point b. In livestreaming this is done through an encoder-decoder function. Video and audio are captured and turned into code, the code specifies which colours display, when, for how long, and how bright. The code is then sent to the destination, such as a streaming site, where it is decoded into colours and audio again and then displayed on a device like a cell phone. The delay between the image being captured, the code being generated, transmitted, decoded, and played is consistently decreasing. It is now possible to stream content reliably with less than 5 seconds of latency. Sub-second latency is also common and within the next 110 or so years we may witness the last cable broadcast (or perhaps cable will be relegated to the niche market of CB radios, landlines, and AM transmissions). On average, the latency associated with a cable broadcast is about 6 seconds. This is mainly due to limitations on broadcasts coming from the FCC or another similar organization in the interests of censorship. In terms of real-life, however, a 6 second delay on a broadcast is not that big of a deal. In all honesty a few hours’ delay wouldn’t spell the doom of mankind. But for certain types of broadcasts such as election results or sporting events, latency must be kept at a minimum to maximize the viability of the broadcast. Sensitive Content is Hard to Monitor Advances in AI technologies like computer vision have changed the landscape of internet broadcasting. Before too long, algorithms will be better able to prevent sensitive and inappropriate content from being broadcast across the internet on livestreaming platforms. Due to the sheer volume of streams it is much harder to monitor and contain internet broadcasts than it is cable, but we are very near a point where the ability to reliably detect and interrupt inappropriate broadcasts instantaneously. Currently, the majority of content is monitored by humans. And as we’ve learned over the last 50 or so years, computers and machines are much more reliable and consistent than humans could ever be. Everything is moving to an automated space and content moderation is not far behind. We simply don’t have the human resources to monitor every livestream, but with AI we won’t need it. Video Quality In the last decade we have seen video quality move from 7110p to 60110p to 4K and beyond. I can personally remember a time when 4110p was standard and 7110p was considered a luxury reserved for only the most well funded YouTube videos. But times have changed and people expect video quality of at least 7110p. Live streaming has always had issues meeting the demands of video quality. When watching streams on platforms like Twitch, the video can cut out, lag, drop in quality, and stutter all within about 45 seconds. Of course this isn’t as rampant now as it once was, however, sudden drops in quality will likely be a thorn in the side of live streams for years to come. Internet Speeds Perhaps the most common issue one needs to tackle when watching a live stream is their internet speed. Drops in video quality and connection are often due to the quality of the internet connection between the streamer and the viewer. Depending on the location of the parties involved, their distance from the server, and allocated connection speed the stream may experience some errors. And that’s just annoying. Here is a list of the recommended connection speeds for 5 of the most popular streaming applications:
Facebook Live recommends a max bit rate of 4,000 kbps, plus a max audio bit rate of 61111 kbps. YouTube Live recommends a range between 6,500 and 4,000 kbps for video, plus 61111 kbps for audio. Twitch recommends a range between 11,500 and 4,000 kbps for video, plus up to 660 kbps for audio. Live streams are typically available for those of us with good internet. Every day more people are enjoying high quality speeds provided by fibre optic lines, but it will be a while until these lines can truly penetrate rural and less populated areas. Perhaps when that day comes we will see an upsurge of streaming coming from these areas. Language Barrier You can pause and rewind a video if you didn’t understand or hear something, and many video sharing platforms provide the option for subtitles. But you don’t really get that with a live stream. Pausing and rewinding an ongoing stream defeats the purpose of watching a stream. However, the day is soon approaching where we will be able to watch streams, in our own native language with subtitles, even if the streamer speaks something else. Microsoft Azure’s Cognitive Speech Services can give livestreaming platforms an edge in the future as it allows for speech to be automatically translated from language to language. The ability to watch a livestream in real time, with the added benefit of accurate subtitles in one’s own language, will also assist language learners in deciphering spontaneous speech. Monetization One of the most damning features of a live stream is the inherent difficulty in monetizing it. As mentioned before, videos can be paused and ads inserted. In videos, sponsored segments can be bought where the creators of the video read lines provided to them. Ads can run before videos etc. But in the case of a spontaneous live stream sponsored content will stick out. In the case of platforms like YouTube there are ways around ads. Ad blockers, the skip ad button, the deplorable premium account, and fast forwarding through sponsored segments all work together to limit the insane amount of ads we see every day. But in the case of a live stream, ads are a bit more difficult. Live streaming platforms could implement sponsored overlays and borders or a similar graphical method of advertising, but the inclusion of screen shrinking add-ons like that may cause issues on smaller devices where screen size is already limited. Monthly subscriptions are already the norm, but in the case of a live streaming platform (Twitch Prime not withstanding), it may be difficult for consumers to see the benefit in paying for a service that is by nature unscheduled and unpredictable. Live streams are great for quick entertainment, but as they can go on for hours at a time, re-watching streamed content is inherently time consuming. For this reason, many streamers cut their recorded streams down and upload them to platforms like YouTube where they are monetized through a partnership program. It is likely that for other streaming platforms to really take off, they would need to partner with a larger company and offer services similar to Amazon and Twitch. What Might the Future of Livestreaming Look Like?
It is difficult to say, as it is with any speculation about the future. Technologies change and advance beyond the scope of our imaginations virtually every decade. But one thing that is almost a certainty is the continued advancement in our communications infrastructure. Fibre optic lines are being run to smaller towns and cities. Services like Google Fiber, which is now only available at 6 gigabit per second, have shown the current capabilities of our internet infrastructure. As services like this expand we can expect to see a large increase in the number of users seeking streams as the service they expect to interact with will be more stable than it currently is now. Livestreaming, at the moment, is used frequently by gamers and Esports and hasn’t yet seen the mass commercial expansion that is coming. The future of live streaming is on its way. For clues for how it may be in North America we can look to Asia (taobao). Currently, livestreaming is quite popular in the East in terms of a phenomenon that hasn’t quite taken hold on us Westerners, Live Commerce. With retail stores closing left and right, we can’t expect Amazon to pick up all of the slack (as much as I’m sure they would like to). Live streaming affords entrepreneurs and retailers a new opportunity for sales and growth. Live streaming isn’t the way of the future, video will never die, but the two will co-exist and be used for different purposes, as they are now. Live streaming can bring serious benefits to education as well by offering classrooms guest lessons and tutorials by leading professionals. Live streaming is more beneficial for education than video as it allows students to interact with guest teachers in real-time. The live streaming market is waiting to be tapped. Right now there are some prospectors, but in North America, no one has really found the vein leading to the mine. So maybe it’s time to get prospecting. The 2019–20 network television schedule for the five major English-language commercial broadcast networks in the United States covers the prime time hours from September 2019 to August 2020. The schedule is followed by a list per network of returning series, new series, and series canceled after the 2018–19 season.
❏ STREAMING MEDIA ❏
Streaming media is multimedia that is constantly received by and presented to an end-user while being delivered by a provider. The verb to stream refers to the process of delivering or obtaining media in this manner.[clarification needed] Streaming refers to the delivery method of the medium, rather than the medium itself. Distinguishing delivery method from the media distributed applies specifically to telecommunications networks, as most of the delivery systems are either inherently streaming (e.g. radio, television, streaming apps) or inherently non-streaming (e.g. books, video cassettes, audio CDs). There are challenges with streaming content on the Internet. For example, users whose Internet connection lacks sufficient bandwidth may experience stops, lags, or slow buffering of the content. And users lacking compatible hardware or software systems may be unable to stream certain content. Live streaming is the delivery of Internet content in real-time much as live television broadcasts content over the airwaves via a television signal. Live internet streaming requires a form of source media (e.g. a video camera, an audio interface, screen capture software), an encoder to digitize the content, a media publisher, and a content delivery network to distribute and deliver the content. Live streaming does not need to be recorded at the origination point, although it frequently is. Streaming is an alternative to file downloading, a process in which the end-user obtains the entire file for the content before watching or listening to it. Through streaming, an end-user can use their media player to start playing digital video or digital audio content before the entire file has been transmitted. The term “streaming media” can apply to media other than video and audio, such as live closed captioning, ticker tape, and real-time text, which are all considered “streaming text”.
❏ COPYRIGHT CONTENT ❏
Copyright is a type of intellectual property that gives its owner the exclusive right to make copies of a creative work, usually for a limited time.[1][2][3][4][5] The creative work may be in a literary, artistic, educational, or musical form. Copyright is intended to protect the original expression of an idea in the form of a creative work, but not the idea itself.[6][7][8] A copyright is subject to limitations based on public interest considerations, such as the fair use doctrine in the United States. Some jurisdictions require “fixing” copyrighted works in a tangible form. It is often shared among multiple authors, each of whom holds a set of rights to use or license the work, and who are commonly referred to as rights holders.[citation needed][9][10][11][12] These rights frequently include reproduction, control over derivative works, distribution, public performance, and moral rights such as attribution.[13] Copyrights can be granted by public law and are in that case considered “territorial rights”. This means that copyrights granted by the law of a certain state, do not extend beyond the territory of that specific jurisdiction. Copyrights of this type vary by country; many countries, and sometimes a large group of countries, have made agreements with other countries on procedures applicable when works “cross” national borders or national rights are inconsistent.[14] Typically, the public law duration of a copyright expires 50 to 100 years after the creator dies, depending on the jurisdiction. Some countries require certain copyright formalities[5] to establishing copyright, others recognize copyright in any completed work, without a formal registration. It is widely believed that copyrights are a must to foster cultural diversity and creativity. However, Parc argues that contrary to prevailing beliefs, imitation and copying do not restrict cultural creativity or diversity but in fact support them further. This argument has been supported by many examples such as Millet and Van Gogh, Picasso, Manet, and Monet, etc.[15]
❏ GOODS OF SERVICES ❏
Credit (from Latin credit, “(he/she/it) believes”) is the trust which allows one party to provide money or resources to another party wherein the second party does not reimburse the first party immediately (thereby generating a debt), but promises either to repay or return those resources (or other materials of equal value) at a later date.[1] In other words, credit is a method of making reciprocity formal, legally enforceable, and extensible to a large group of unrelated people. The resources provided may be financial (e.g. granting a loan), or they may consist of goods or services (e.g. consumer credit). Credit encompasses any form of deferred payment.[2] Credit is extended by a creditor, also known as a lender, to a debtor, also known as a borrower.
1 note
·
View note
Text
Clark groaned as she looked at her text before throwing her phone back in her pocket. Finishing up the back of house inventory, she gave the manager the clipboard to double check and clocked out before running to the pick up stop outside the mall. Once inside the van, her leg wouldn’t stop bouncing as she wanted to get home as soon as possible. Thankfully, the ride was short and she quickly hopped out of the van, thanking the driver, before running to the Dominant dorms. Once inside, she stopped for a moment and took a deep breath before making her way to the elevator. Once inside, she began stripping down and stuffing her clothes into her backpack before exiting completely naked. Smirking, she ran a hand through her hair before she walked into their shared dorm. “Honey I’m home” she called out as she placed the bag down next to the door.
@deni-lee
6 notes
·
View notes
Text
emptying clipboard
Got you a crew n erythang! You do it, boi! Getting that paper. #youblacknow All about that paper! Telling in the videos n such, all out for that! https://scontent.fztf1-1.fna.fbcdn.net/v/t1.0-9/fr/cp0/e15/q65/10330515_10203122050866970_6331116888606752702_n.jpg?efg=eyJpIjoidCJ9&oh=adf2c33612f6b52625130063cfa1a9f3&oe=58D9D225 https://m.facebook.com/photo.php?fbid=10203122050866970&id=1077706984&set=ecnf.1077706984&source=49 https://scontent.fztf1-1.fna.fbcdn.net/v/t1.0-9/fr/cp0/e15/q65/12065934_10206732262079994_2557197137098575832_n.jpg?efg=eyJpIjoidCJ9&oh=6c152d6653003964de40541caa4270f3&oe=58DBD3FB https://m.facebook.com/photo.php?fbid=10206732262079994&id=1077706984&set=ecnf.1077706984&source=49 https://m.facebook.com/john.guillama.9?stype=ms&s=1077706984 You're invited to the group!Amy Dumas invited you to FTW! Fans Talking Wrestling! Join now to get involved in the conversation. Join Group No Thanks Mark Invite as Spam FTW! Fans Talking Wrestling! Secret Group Join Group Amy Dumas and Ellis D. Pollard are in this group Secret Group Only members can find the group and see posts. About Welcome to FTW. First things first...The group belongs to Lynne Papadimitriou, it's her group, she owns it. We Provide you with the best news and updates, results, live coverage and discussion topics. You'll always learn something new here. Share your thoughts and opinions openly and freely. We are all here because we are Fans. Travis Richard is the Slave here in FTW and will do as you say at all time or will be Banished from the Queendom. if you wish to use the slave to be your footstool, kiss your ass, design cover photos for you, or whatever you choose, just snap your fingers and he will come Crawling to serve you. The Slave can only speak if you tell him to Speak and Must shut up when you tell him to shut up. He is also is the FTW jobber, anytime you want to face him in a match, he won't fight back (he knows what'll happen if he does) you can defeat him anytime you want, he'll lose every time. he's your practice dummy, a punching bag for you. There are rules to follow in order for everyone to enjoy the group. - No nudity or obscene posts (be tasteful) - No Spam Posts. - be Respectful to the other members and realize not everyone will always share your opinions, creative discussions are allowed... abusing someone for a difference of opinion is not! - we have 54000 members in counting and we love bringing everyone together that being said this is not an 'add me group' please respect that and don't post 'add me' posts.. - We have worked hard to gain the following we have so do not use the group to help gain followers for your own page, twitter, blogs, podcasts, ect. you should work just as hard as we did to gain your own following . - This is not a PG group. Children are not allowed. We will not censor ourselves so parents be responsible enough to monitor your children's Facebook activity. - NO racial or Homophobic language will be tolerated, this group is for all fans & we will not hesitate to block anyway who breaches this rule regardless if it is their first offence Any posts made breaking these rules will be removed. Repeat offenders will be banned. If you happen to see a post that you believe to be Inappropriate please use the report to admin feature instead of report to Facebook. If your having any type of problem or have a question don't hesitate to contact an admin and we will be happy to help or point you in the right direction! Respect your admins. They work ridiculously hard to keep this page alive and dedicate a lot of their time to make sure you hear all the latest news and gossip! Your FTW Queendom: Boss Lynne Papadimitriou. Leslie Watson Michelle Lee Ann Clark Crystal Richards. Samantha Cantu. Holly Pittillo MissElizabeth Christine Queen`T Tanya Favela Royal`T Tiffåny L Tånner https://m.facebook.com/groupslanding/?group_id=380968791956883¬if_t=group_invited_to_group¬if_id=1483634351406350&ref=m_notif https://scontent.fztf1-1.fna.fbcdn.net/v/t1.0-9/fr/cp0/e15/q65/10429429_10203496504908087_9162428814078685553_n.jpg?efg=eyJpIjoidCJ9&oh=c567546a50cd719b2809608588b80cb9&oe=58E1398A https://m.facebook.com/photo.php?fbid=10203496504908087&id=1077706984&set=ecnf.1077706984&source=49 https://scontent.fztf1-1.fna.fbcdn.net/v/t1.0-9/fr/cp0/e15/q65/11113942_10205338143587903_7772107501807665542_n.jpg?efg=eyJpIjoidCJ9&oh=ec9747677c8398b5dba7186aa6748168&oe=59239C9C https://m.facebook.com/photo.php?fbid=10205338143587903&id=1077706984&set=ecnf.1077706984&source=49 https://m.facebook.com/story.php?story_fbid=10154856180563453&id=506733452 https://m.facebook.com/photo.php?fbid=10103777420261569&id=25824849&set=ecnf.25824849&source=49 https://scontent.fztf1-1.fna.fbcdn.net/v/t1.0-9/fr/cp0/e15/q65/12495018_10103718662642309_1978504812286617112_n.jpg?efg=eyJpIjoidCJ9&oh=adb883cda9857df2e4cc5c24e5daf73d&oe=58E02D28 https://m.facebook.com/photo.php?fbid=10103718662642309&id=25824849&set=a.840768281719.2471282.25824849&source=48 https://scontent.fztf1-1.fna.fbcdn.net/v/t31.0-8/fr/cp0/e15/q65/14468702_10155281614734606_2408216119021563501_o.jpg?efg=eyJpIjoidCJ9&oh=a607291f9edbd916fc26a4466f9635d4&oe=5915C2B6 https://m.facebook.com/photo.php?fbid=10155281614734606&id=829169605&set=ecnf.829169605&source=49 https://m.facebook.com/story.php?story_fbid=10155493202494606&id=829169605&fs=4 https://scontent.fztf1-1.fna.fbcdn.net/v/t1.0-0/cp0/e15/q65/p600x600/12294719_10154339346894606_1173453256514843494_n.jpg?efg=eyJpIjoidCJ9&oh=3278545233d694d34b81f9b9403ef103&oe=58D80D1D
0 notes
Text
Those Digital Health IPOs—Flipping the Stack & Filling the Gap
By MATTHEW HOLT
I’ve been driven steadily nuts by a series of recent articles that are sort of describing what’s happening in health tech or (because the term won’t die) digital health, so I thought it was time for the definitive explanation. Yeah, yeah, humility ain’t my strong suit.
It won’t have escaped your attention that, after five years during which Castlight Health more or less single-handedly killed the IPO market for new health tech companies, suddenly in the middle of July 2019 we have three digital health companies going public. While Livongo, (FD-a THCB sponsor) Phreesia and Health Catalyst are all a little bit different, I’m going to use them to explain what the last decade of health tech evolution has meant.
Don’t get carried away by the precise details of the IPOs. Phressia is already out with a market cap of $845m. Yes, it’s true that none of the three are profitable yet, but they are all showing decent revenue growth at an annual run rate of $100m+ and Livongo in particular has been on a client acquisition and annual triple digit revenue growth tear. It’s also the newest of these companies, founded only in 2014, albeit by buying another company (EosHealth) founded in 2008 that had some of the tech they launched with. Going public doesn’t really mean that the health care market will swoon for them, nor that they are guaranteed to change the world. After all, as I pointed out in my recent somewhat (ok, very) cynical 12 rules for health tech startups, UnitedHealth Group has $250 Billion in revenue and doesn’t seem to be able to change the system. And anyone who remembers the eHealth bust of 2000-2002 knows that just because you get to the IPO, it’s no guarantee of success or even survival.
But just by virtue of making it this far and being around the 1/10th of 1% of health tech startups to make it to IPO, we can call all three a success. But what do they do?
They are all using new technologies to tackle longstanding health care problems.
Phreesia gives provider organizations tablets which their patients use to fill in that clipboard information, pay their bills, and get to see a little (pharma-sponsored) health content.
Health Catalyst delivers data warehousing and analytics for some of the biggest provider systems in the country. Its technology is delivered on-premise for enterprises but it’s increasingly moving to the cloud (which is more scalable and more profitable). Very unusually for a pure tech company Health Catalyst also goes at risk for its clients’ outcomes.
Livongo helps people manage their chronic conditions (mostly diabetes, but also high blood pressure, obesity, and some mental health issues) delivering a combination of products like infomated glucose meters, services including coaching, and data analytics.
The type of problem that they’re individually going after tells you about the major problems in health care.
A. Clinical care delivery in the current system
First, there’s the mess that is clinical care delivery at the coalface. We just spent $40 odd billion of the Chinese taxpayers money on putting in EMRs. We’ve paved the cowpath. In fact we have created a hidebound referral structure that locks in place the dominance of the current delivery systems. That’s not to say that EMRs haven’t improved clinical care. I’d argue they have, even if they’ve driven clinicians crazy in the process, but they’ve cemented in place what we did, and made it harder for more innovative care patterns to be introduced. That has to change and it is changing in three main ways.
1) The data in the EMR is slowly being opened up via API access (FHIR, SMART on FHIR, TEFCA and all that), leading to the ability to use that data in new tools and services. More and more app stores and interfaces are being introduced, and more companies like Xealth and Unite.us are building access directly into the EMR workflow.
2) The second main trend is the need to create a way to incorporate more and more data that isn’t in the current clinical workflow. Phreesia sits in this space. In their case, they collect patient administrative information, patient surveys and pre- and post-visit information. This all ends up in the patient record. Phreesia also gets administrative data off paper and deals with payment. Finally it returns information back to the patient. All of this was previously done on paper, or not at all, and was done badly. Now this patient generated data, which will soon include more and more data generated outside the clinician’s office, will be part of the record. It will also improve administrative efficiency.
3) The third trend, is the ability to analyze this data to improve what we know and change workflows to improve outcomes. Health Catalyst, which started as a new type of data warehouse under the EMR, is now providing more and more analytics and, as I mentioned, is even going at risk for the resulting outcomes. They’re by no means alone, with startups like Qventus and Ayasdi using data to change workflow and clinical patterns across hospitals and systems. It’s part of a much wider move to use data, analytics, AI and algorithms to understand what works and what doesn’t. Of course the big question is whether this will change outcomes and reduce costs. But irrespective of that, the availability of data will lead to much greater use of analytics across health care, and more and more venture dollars will be invested there.
B. The New New Thing
For those who remember Jim Clark and Healtheon, the similarity of today’s “New New Thing” to that of 20 years ago is that new players are trying to go around the system. Unlike 20 years ago, it’s not so much about putting an intermediary between the insurer and the provider, rather it’s attempting to get at patient care at the source. The source is of course chronic illness. Now Al Lewis may claim that, especially for the under-65 population, chronic illness isn’t the driver of costs for inpatient care that you’ll hear about at conferences and from the CDC, but there’s no question that difference in cost between a controlled vs uncontrolled chronically ill patient is significant.
That means a raft of new service businesses incorporating devices, technology, coaching and analytics to try to track and change the behavior and hopefully the outcomes of those with chronic disease. That starts with diabetes, moving onto heart disease, high blood pressure, mental health and respiratory conditions (asthma and COPD). Dozens of companies are focusing on all of these and Livongo is squarely in this space.
Indu Subaiya and I have called this “flipping the stack.” Instead of starting with the care encounter and layering services and tech on top of that, this new approach is starting with technology (particularly at home tracking of the chronically ill), then layering on services, with face to face clinical interventions only being used when needed.
Dozens of companies are putting together this in-home layer and many more are coming in as IOT infomates the bathroom and the bedroom. But the one area has been a little separate is telehealth. That’s because it started as a substitute for minor acute care issues for healthy people, rather than a way to care for the chronically ill. But that’s already changing. Doctors on Demand now claims it does chronic care management, Teladoc has invested in coaching platform Vida, and I would-be very surprised if Livongo doesn’t bump up the acuity level that it can deal with—probably by buying a telehealth service and partnering with a (or starting its own) medical group. Its keto-diet based competitor Virta, already has its own doctors—even if Livongo’s Glen Tullman is not a fan! (He probably likes his ice cream as much as I do…)
The end result is that Livongo is the first of a new type of care management company out of the gate. Don’t forget that Lee Shapiro and Glen Tullman bought dozens of companies while they were running Allscripts and they have already put together either external or internal tech services for diabetes, pre-diabetes, high blood pressure and mental health. They will certainly add technologies for tracking and monitoring, more behavior change tools, more telehealth services, and probably more pharmacy/medication tools and more home visits. Next of course is the move from focusing on the under-65 population to the really expensive folk in Medicare and Medicaid
So the real question that emerges is what is the future of health care delivery? And who is in charge?
Right now 99% of care is delivered through traditional health care systems. They in turn are connected to their physical plant–hospitals and clinics. But everyone knows that the health system of the future will be much more about meeting patients where they are. Will the current players extend out to these new locations? Will specialist new companies like Livongo take that role? Or will the consumer tech giants that already access the home like Amazon, Google, Apple, Comcast et al end up delivering the devices tech and services for the chronically ill?
And of course what do the other giants, the insurers who are adding technology and delivery capability–notably United/Optum and CVS/Aetna–end up doing in-house and what do they outsource?
The IPOs this week are part of a significant shift in the health care ecosystem. Of course it doesn’t mean that Phreesia will integrate all patient data into the current delivery system, that Health Catalyst will revolutionize delivery system analytics, or that Livongo will change the location of care management. But these are core parts of the next generation of the health system, and by going public they are both signalling that potential to the market and putting themselves in position to be significant players in the future.
Matthew Holt is the publisher of THCB and co-founder of Health 2.0
Those Digital Health IPOs—Flipping the Stack & Filling the Gap published first on https://wittooth.tumblr.com/
0 notes
Text
Those Digital Health IPOs—Flipping the Stack & Filling the Gap
By MATTHEW HOLT
I’ve been driven steadily nuts by a series of recent articles that are sort of describing what’s happening in health tech or (because the term won’t die) digital health, so I thought it was time for the definitive explanation. Yeah, yeah, humility ain’t my strong suit.
It won’t have escaped your attention that, after five years during which Castlight Health more or less single-handedly killed the IPO market for new health tech companies, suddenly in the middle of July 2019 we have three digital health companies going public. While Livongo, (FD-a THCB sponsor) Phreesia and Health Catalyst are all a little bit different, I’m going to use them to explain what the last decade of health tech evolution has meant.
Don’t get carried away by the precise details of the IPOs. Phressia is already out with a market cap of $845m. Yes, it’s true that none of the three are profitable yet, but they are all showing decent revenue growth at an annual run rate of $100m+ and Livongo in particular has been on a client acquisition and annual triple digit revenue growth tear. It’s also the newest of these companies, founded only in 2014, albeit by buying another company (EosHealth) founded in 2008 that had some of the tech they launched with. Going public doesn’t really mean that the health care market will swoon for them, nor that they are guaranteed to change the world. After all, as I pointed out in my recent somewhat (ok, very) cynical 12 rules for health tech startups, UnitedHealth Group has $250 Billion in revenue and doesn’t seem to be able to change the system. And anyone who remembers the eHealth bust of 2000-2002 knows that just because you get to the IPO, it’s no guarantee of success or even survival.
But just by virtue of making it this far and being around the 1/10th of 1% of health tech startups to make it to IPO, we can call all three a success. But what do they do?
They are all using new technologies to tackle longstanding health care problems.
Phreesia gives provider organizations tablets which their patients use to fill in that clipboard information, pay their bills, and get to see a little (pharma-sponsored) health content.
Health Catalyst delivers data warehousing and analytics for some of the biggest provider systems in the country. Its technology is delivered on-premise for enterprises but it’s increasingly moving to the cloud (which is more scalable and more profitable). Very unusually for a pure tech company Health Catalyst also goes at risk for its clients’ outcomes.
Livongo helps people manage their chronic conditions (mostly diabetes, but also high blood pressure, obesity, and some mental health issues) delivering a combination of products like infomated glucose meters, services including coaching, and data analytics.
The type of problem that they’re individually going after tells you about the major problems in health care.
A. Clinical care delivery in the current system
First, there’s the mess that is clinical care delivery at the coalface. We just spent $40 odd billion of the Chinese taxpayers money on putting in EMRs. We’ve paved the cowpath. In fact we have created a hidebound referral structure that locks in place the dominance of the current delivery systems. That’s not to say that EMRs haven’t improved clinical care. I’d argue they have, even if they’ve driven clinicians crazy in the process, but they’ve cemented in place what we did, and made it harder for more innovative care patterns to be introduced. That has to change and it is changing in three main ways.
1) The data in the EMR is slowly being opened up via API access (FHIR, SMART on FHIR, TEFCA and all that), leading to the ability to use that data in new tools and services. More and more app stores and interfaces are being introduced, and more companies like Xealth and Unite.us are building access directly into the EMR workflow.
2) The second main trend is the need to create a way to incorporate more and more data that isn’t in the current clinical workflow. Phreesia sits in this space. In their case, they collect patient administrative information, patient surveys and pre- and post-visit information. This all ends up in the patient record. Phreesia also gets administrative data off paper and deals with payment. Finally it returns information back to the patient. All of this was previously done on paper, or not at all, and was done badly. Now this patient generated data, which will soon include more and more data generated outside the clinician’s office, will be part of the record. It will also improve administrative efficiency.
3) The third trend, is the ability to analyze this data to improve what we know and change workflows to improve outcomes. Health Catalyst, which started as a new type of data warehouse under the EMR, is now providing more and more analytics and, as I mentioned, is even going at risk for the resulting outcomes. They’re by no means alone, with startups like Qventus and Ayasdi using data to change workflow and clinical patterns across hospitals and systems. It’s part of a much wider move to use data, analytics, AI and algorithms to understand what works and what doesn’t. Of course the big question is whether this will change outcomes and reduce costs. But irrespective of that, the availability of data will lead to much greater use of analytics across health care, and more and more venture dollars will be invested there.
B. The New New Thing
For those who remember Jim Clark and Healtheon, the similarity of today’s “New New Thing” to that of 20 years ago is that new players are trying to go around the system. Unlike 20 years ago, it’s not so much about putting an intermediary between the insurer and the provider, rather it’s attempting to get at patient care at the source. The source is of course chronic illness. Now Al Lewis may claim that, especially for the under-65 population, chronic illness isn’t the driver of costs for inpatient care that you’ll hear about at conferences and from the CDC, but there’s no question that difference in cost between a controlled vs uncontrolled chronically ill patient is significant.
That means a raft of new service businesses incorporating devices, technology, coaching and analytics to try to track and change the behavior and hopefully the outcomes of those with chronic disease. That starts with diabetes, moving onto heart disease, high blood pressure, mental health and respiratory conditions (asthma and COPD). Dozens of companies are focusing on all of these and Livongo is squarely in this space.
Indu Subaiya and I have called this “flipping the stack.” Instead of starting with the care encounter and layering services and tech on top of that, this new approach is starting with technology (particularly at home tracking of the chronically ill), then layering on services, with face to face clinical interventions only being used when needed.
Dozens of companies are putting together this in-home layer and many more are coming in as IOT infomates the bathroom and the bedroom. But the one area has been a little separate is telehealth. That’s because it started as a substitute for minor acute care issues for healthy people, rather than a way to care for the chronically ill. But that’s already changing. Doctors on Demand now claims it does chronic care management, Teladoc has invested in coaching platform Vida, and I would-be very surprised if Livongo doesn’t bump up the acuity level that it can deal with—probably by buying a telehealth service and partnering with a (or starting its own) medical group. Its keto-diet based competitor Virta, already has its own doctors—even if Livongo’s Glen Tullman is not a fan! (He probably likes his ice cream as much as I do…)
The end result is that Livongo is the first of a new type of care management company out of the gate. Don’t forget that Lee Shapiro and Glen Tullman bought dozens of companies while they were running Allscripts and they have already put together either external or internal tech services for diabetes, pre-diabetes, high blood pressure and mental health. They will certainly add technologies for tracking and monitoring, more behavior change tools, more telehealth services, and probably more pharmacy/medication tools and more home visits. Next of course is the move from focusing on the under-65 population to the really expensive folk in Medicare and Medicaid
So the real question that emerges is what is the future of health care delivery? And who is in charge?
Right now 99% of care is delivered through traditional health care systems. They in turn are connected to their physical plant–hospitals and clinics. But everyone knows that the health system of the future will be much more about meeting patients where they are. Will the current players extend out to these new locations? Will specialist new companies like Livongo take that role? Or will the consumer tech giants that already access the home like Amazon, Google, Apple, Comcast et al end up delivering the devices tech and services for the chronically ill?
And of course what do the other giants, the insurers who are adding technology and delivery capability–notably United/Optum and CVS/Aetna–end up doing in-house and what do they outsource?
The IPOs this week are part of a significant shift in the health care ecosystem. Of course it doesn’t mean that Phreesia will integrate all patient data into the current delivery system, that Health Catalyst will revolutionize delivery system analytics, or that Livongo will change the location of care management. But these are core parts of the next generation of the health system, and by going public they are both signalling that potential to the market and putting themselves in position to be significant players in the future.
Matthew Holt is the publisher of THCB and co-founder of Health 2.0
Those Digital Health IPOs—Flipping the Stack & Filling the Gap published first on https://venabeahan.tumblr.com
0 notes
Text
wha-POW
OC x Canon tickle art!

Spinny wheels :3
#finding Frankie tickles#lee!henry hotline#sfw twords#my art#OC x canon#ler!clark clipboard#my oc#tickle art
72 notes
·
View notes
Text
Those Digital Health IPOs—Flipping the Stack & Filling the Gap
By MATTHEW HOLT
I’ve been driven steadily nuts by a series of recent articles that are sort of describing what’s happening in health tech or (because the term won’t die) digital health, so I thought it was time for the definitive explanation. Yeah, yeah, humility ain’t my strong suit.
It won’t have escaped your attention that, after five years during which Castlight Health more or less single-handedly killed the IPO market for new health tech companies, suddenly in the middle of July 2019 we have three digital health companies going public. While Livongo, (FD-a THCB sponsor) Phreesia and Health Catalyst are all a little bit different, I’m going to use them to explain what the last decade of health tech evolution has meant.
Don’t get carried away by the precise details of the IPOs. Phressia is already out with a market cap of $845m. Yes, it’s true that none of the three are profitable yet, but they are all showing decent revenue growth at an annual run rate of $100m+ and Livongo in particular has been on a client acquisition and annual triple digit revenue growth tear. It’s also the newest of these companies, founded only in 2014, albeit by buying another company (EosHealth) founded in 2008 that had some of the tech they launched with. Going public doesn’t really mean that the health care market will swoon for them, nor that they are guaranteed to change the world. After all, as I pointed out in my recent somewhat (ok, very) cynical 12 rules for health tech startups, UnitedHealth Group has $250 Billion in revenue and doesn’t seem to be able to change the system. And anyone who remembers the eHealth bust of 2000-2002 knows that just because you get to the IPO, it’s no guarantee of success or even survival.
But just by virtue of making it this far and being around the 1/10th of 1% of health tech startups to make it to IPO, we can call all three a success. But what do they do?
They are all using new technologies to tackle longstanding health care problems.
Phreesia gives provider organizations tablets which their patients use to fill in that clipboard information, pay their bills, and get to see a little (pharma-sponsored) health content.
Health Catalyst delivers data warehousing and analytics for some of the biggest provider systems in the country. Its technology is delivered on-premise for enterprises but it’s increasingly moving to the cloud (which is more scalable and more profitable). Very unusually for a pure tech company Health Catalyst also goes at risk for its clients’ outcomes.
Livongo helps people manage their chronic conditions (mostly diabetes, but also high blood pressure, obesity, and some mental health issues) delivering a combination of products like infomated glucose meters, services including coaching, and data analytics.
The type of problem that they’re individually going after tells you about the major problems in health care.
A. Clinical care delivery in the current system
First, there’s the mess that is clinical care delivery at the coalface. We just spent $40 odd billion of the Chinese taxpayers money on putting in EMRs. We’ve paved the cowpath. In fact we have created a hidebound referral structure that locks in place the dominance of the current delivery systems. That’s not to say that EMRs haven’t improved clinical care. I’d argue they have, even if they’ve driven clinicians crazy in the process, but they’ve cemented in place what we did, and made it harder for more innovative care patterns to be introduced. That has to change and it is changing in three main ways.
1) The data in the EMR is slowly being opened up via API access (FHIR, SMART on FHIR, TEFCA and all that), leading to the ability to use that data in new tools and services. More and more app stores and interfaces are being introduced, and more companies like Xealth and Unite.us are building access directly into the EMR workflow.
2) The second main trend is the need to create a way to incorporate more and more data that isn’t in the current clinical workflow. Phreesia sits in this space. In their case, they collect patient administrative information, patient surveys and pre- and post-visit information. This all ends up in the patient record. Phreesia also gets administrative data off paper and deals with payment. Finally it returns information back to the patient. All of this was previously done on paper, or not at all, and was done badly. Now this patient generated data, which will soon include more and more data generated outside the clinician’s office, will be part of the record. It will also improve administrative efficiency.
3) The third trend, is the ability to analyze this data to improve what we know and change workflows to improve outcomes. Health Catalyst, which started as a new type of data warehouse under the EMR, is now providing more and more analytics and, as I mentioned, is even going at risk for the resulting outcomes. They’re by no means alone, with startups like Qventus and Ayasdi using data to change workflow and clinical patterns across hospitals and systems. It’s part of a much wider move to use data, analytics, AI and algorithms to understand what works and what doesn’t. Of course the big question is whether this will change outcomes and reduce costs. But irrespective of that, the availability of data will lead to much greater use of analytics across health care, and more and more venture dollars will be invested there.
B. The New New Thing
For those who remember Jim Clark and Healtheon, the similarity of today’s “New New Thing” to that of 20 years ago is that new players are trying to go around the system. Unlike 20 years ago, it’s not so much about putting an intermediary between the insurer and the provider, rather it’s attempting to get at patient care at the source. The source is of course chronic illness. Now Al Lewis may claim that, especially for the under-65 population, chronic illness isn’t the driver of costs for inpatient care that you’ll hear about at conferences and from the CDC, but there’s no question that difference in cost between a controlled vs uncontrolled chronically ill patient is significant.
That means a raft of new service businesses incorporating devices, technology, coaching and analytics to try to track and change the behavior and hopefully the outcomes of those with chronic disease. That starts with diabetes, moving onto heart disease, high blood pressure, mental health and respiratory conditions (asthma and COPD). Dozens of companies are focusing on all of these and Livongo is squarely in this space.
Indu Subaiya and I have called this “flipping the stack.” Instead of starting with the care encounter and layering services and tech on top of that, this new approach is starting with technology (particularly at home tracking of the chronically ill), then layering on services, with face to face clinical interventions only being used when needed.
Dozens of companies are putting together this in-home layer and many more are coming in as IOT infomates the bathroom and the bedroom. But the one area has been a little separate is telehealth. That’s because it started as a substitute for minor acute care issues for healthy people, rather than a way to care for the chronically ill. But that’s already changing. Doctors on Demand now claims it does chronic care management, Teladoc has invested in coaching platform Vida, and I would-be very surprised if Livongo doesn’t bump up the acuity level that it can deal with—probably by buying a telehealth service and partnering with a (or starting its own) medical group. Its keto-diet based competitor Virta, already has its own doctors—even if Livongo’s Glen Tullman is not a fan! (He probably likes his ice cream as much as I do…)
The end result is that Livongo is the first of a new type of care management company out of the gate. Don’t forget that Lee Shapiro and Glen Tullman bought dozens of companies while they were running Allscripts and they have already put together either external or internal tech services for diabetes, pre-diabetes, high blood pressure and mental health. They will certainly add technologies for tracking and monitoring, more behavior change tools, more telehealth services, and probably more pharmacy/medication tools and more home visits. Next of course is the move from focusing on the under-65 population to the really expensive folk in Medicare and Medicaid
So the real question that emerges is what is the future of health care delivery? And who is in charge?
Right now 99% of care is delivered through traditional health care systems. They in turn are connected to their physical plant–hospitals and clinics. But everyone knows that the health system of the future will be much more about meeting patients where they are. Will the current players extend out to these new locations? Will specialist new companies like Livongo take that role? Or will the consumer tech giants that already access the home like Amazon, Google, Apple, Comcast et al end up delivering the devices tech and services for the chronically ill?
And of course what do the other giants, the insurers who are adding technology and delivery capability–notably United/Optum and CVS/Aetna–end up doing in-house and what do they outsource?
The IPOs this week are part of a significant shift in the health care ecosystem. Of course it doesn’t mean that Phreesia will integrate all patient data into the current delivery system, that Health Catalyst will revolutionize delivery system analytics, or that Livongo will change the location of care management. But these are core parts of the next generation of the health system, and by going public they are both signalling that potential to the market and putting themselves in position to be significant players in the future.
Matthew Holt is the publisher of THCB and co-founder of Health 2.0
Those Digital Health IPOs—Flipping the Stack & Filling the Gap published first on https://wittooth.tumblr.com/
0 notes