#it's self reports in relation to transgender issues
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
The “We are the 99%” Tumblr blog became the slogan for the Occupy Wall Street movement.
Text
Hey, you
If your vague post is full of "now, granted" and "but" and "I guess" and other conceding points
Maybe just don't bother making the post??
Like, why waste the time when we're saying the same thing? Literally. The same thing.
What a fucking joke you are, with a raging hate for me that lives rent free in your head
I love it
#syscourse#the implication that there is an overreaching entity that exists as the APA that controls what gets published#(being published through the apap can be done by anyone)#(and the apap publishes SO MANY DIFFERENT THINGS)#is a misrepresentation of a single authors work#the credentials#the vetting process#and overall general consensus#that only serves to make a point look bigger and better than it is#it's a shady tactic and I'm allowed to be pissed off about it#sorry you hate that I'm right too?#and of course they accepted his paper#it's self reports in relation to transgender issues#it's valuable and makes no claims about anything
4 notes
·
View notes
Text
On April 27, 2023, an armed security guard shot and killed a Black trans man named Banko Brown outside of a San Francisco Walgreens. Brown’s killing sparked outrage. But San Francisco District Attorney Brooke Jenkins decided not to charge the security guard who shot him, saying that he acted in self-defense. And just last Friday, Attorney General Rob Bonta’s office announced that it supported that decision. This announcement has crushed Banko Brown’s loved ones, including those who say that his killing was an example of the conditions that unhoused transgender people face in San Francisco. KQED reporter Joe Fitzgerald Rodriguez sits down with Brown’s chosen family, to discuss life as a homeless queer person in San Francisco, and Banko’s life before his death. [...]
Kazani Kalani Finao: [...] We just had amazing, great conversations. Just always sparring with each other, bouncing back with, like, fun ideas. He uses a bright, outgoing apartment. Conversation was always immaculate, always amazing. Of he was a visionary. The struggle not only brought us together, but like I was able to, like, really build a relation with him based on, like, his gifts. He was very creative, his swag, his drip, like he was a trendsetter to me. He’s definitely inspirational to me to like, you know, him, me younger to me, like I always share with him. Like, bro, you give me so much confidence, you give me so much courage for me to be me. He didn’t even know it. But again, he was just natural at that. Whatever I remember of him is his drips, sauce, smile, hugs, goofiness. [...]
Xavier Davenport: Banko never had a space of his own. Banko had been in and out of shelter, in and out of people’s homes, sometimes even some people’s own [SROs]. So let’s really break down what that really looks like when you are living in a one room space with another individual. You do not have privacy. Nine times out of ten, being a transmasculine identif[ied] person, especially being black, you have to render some type of services to stay there, whether it be sexual, whether it be drugs. So when we talk about black men and being fetishized, Banko dealt with a lot of that. And so those people would be the people to take him in. [...]
Joe Fitzgerald Rodriguez: And can we talk a little bit about Banko in terms of the safety? You know, obviously Banko went through the least safe thing you could imagine with the most terrible outcome you can imagine. What was Banko experiencing in terms of safety during this whole process? Xavier Davenport: Banko was actually experiencing a lot of issues with violence happening in some of the places that he was trying to stay at. Nobody’s perfect, you know, especially when we’re talking about community, right? People have all kinds of issues and trauma that they are that they’re trying to live through as well. I definitely know that there were a few times where, you know, he was upset from violent experiences that had taken place. And what we all do, right, we get upset, we want to do something about it. So, you know, really trying to calm him down to, like, see a different side of it, for him to just move through the trauma that he was experiencing. Joe Fitzgerald Rodriguez: Yeah. And I don’t know how much you all followed kind of the public discussion of what happened to Banko afterwards. A lot of what I heard was a kind of a questioning of like, what did [Banko]’s trans identity or black trans identity have to do with the shooting, especially when the security guard themselves was was black. I wonder if you could talk a bit about for people who don’t understand what does [Banko]’s black trans identity have to do with what brought him there that day and what happened? [...] Xavier Davenport: [...] What what that all has to do with is when you are a young, black, transmasculine identified person, people see that he walks in, he’s dark skinned, he has a hat on a t shirt, he has a little bit of a, like a goatee or, you know, something growing in. And as another black man or being another man, there is a fight for power for who is the man. [F]or Banko, you know, the thought process is, you look like a little boy or you’re trying to pretend to be a little boy. Because let’s be clear, Banko had not had, you know, top surgery. He had not been going through that part of of medical transitioning. So you have a masculine person with visible breast coming at you. You are going to now struggle for your manhood. I’m going to show you who’s boss is something that for people that are even lesbians who are more masculine looking, [t]here is a struggle between men and any form of masculinity that they can see to them isn’t necessarily real. Joe Fitzgerald Rodriguez: So it’s a it’s like a challenge. Xavier Davenport: It is a challenge. It very much is a challenge. I know this first experience. I have dealt with this my entire life. JuJu Pikes-Prince: And if I can just highlight that it’s true. And these are cases that’s not getting covered [...] of Black Trans Men getting killed. [...]
Xavier Davenport: [...] I would say what needs to change is the systems in how they construct homelessness. There needs to be shelters specific for transmasculine folks. There needs to be shelters for trans people, period. But trans men need their own space. There needs to be more black, trans masculine leaders. There’s nobody else that can speak about black transness except for black trans people. Joe Fitzgerald Rodriguez: And how about the joy? What is your joy look like right now? Xavier Davenport: My joy looks like, you know, the rest of the work that I do. The Bay Area Transmasculine calendar is doing a second premiere of a calendar that we started last year with a group of Transmasculine folks to continue to ensure that Transmasculine folks are seen and can receive joy in seeing and having representation of themselves in all bodies, in all forms of trans masculine bodies, and in all forms of trans masculine and different cultures and ethnicities. Joe Fitzgerald Rodriguez: That’s beautiful. JuJu Pikes-Prince: [F]iguring out the funding, figuring out where money can go to. I definitely believe that there should be more programs for black trans men, even from our community. My [femme queens, my dolls]. We need to serve our [kings], our [trans kings.] [Sorry], I’m getting emotional. And it’s because I’m thinking about the joy part. [L]iving and finding purpose. Picking up someone else’s purpose when they couldn’t find their purpose. And knowing that I’m here and I can also at least set some type of story for someone [...] and hopefully help another next person, next generation to continue to do this advocacy work.
#m.#examples of transandrophobia#murder tw#banko brown#survival sex work#transunity#racism#antiblackness#tdor#transandrophobia#transmisandry#anti transmasculinity#theory
85 notes
·
View notes
Text
Hi, @peaktransd, you asked a question on this post about "studies about hormones and the placebo effect". I've looked into this and found some relevant information!
---
No high quality research on transgender affirming hormone care
The first, important, aspect here is that there is little to no high quality research on the use of hormones for transgender affirming care.
By this point we've all heard of the Cass review [1, emphasis mine] which found:
For puberty blockers: "The review of the evidence looked at nine studies that met the inclusion criteria. A key limitation of all the studies examined was the lack of reliable comparative studies, as well as of clear expected outcomes. All the studies were small uncontrolled observational studies, and all the results were of low certainty. Many did not report statistical significance."
For hormones: "Ten uncontrolled observational studies met the inclusion criteria. Again, the key limitation to identifying the effectiveness and safety of gender-affirming hormones for children and adolescents with gender dysphoria was the lack of reliable comparative studies."
Notably the important point here is that all of the research is uncontrolled observational studies, which do not allow for the examination of the placebo effect. Also, to preempt any objections, the Cass review team has created a website with FAQs [2] to address the mis- and disinformation being spread about the review.
Further, this article [3] argues "that although [gender affirming treatment] for [gender dysphoric] youth lacks a rigorous evidence base, it is undertaken as routine medical treatment in a strongly placebo effect enhancing environment", highlighting why we absolutely need good quality evidence into this topic.
The state of research for adults is similar. There are no comprehensive reviews about adult treatment, and some of this is by design. By this I mean, WPATH (the World Professional Association for Transgender Health) has purposefully suppressed unfavorable evidence.
There's a compounding issue here; in the reviews that do exist they tend to find very little evidence base for supporting hormone use and then make a recommendation in support of hormones anyway. These studies are often used as evidence by proponents who do not read past the abstract of the study.
Some studies on hormones and mood in transgender adults [all emphasis mine]:
This 2016 review [4] indicated: "Hormone therapy interventions to improve the mental health and quality of life in transgender people with gender dysphoria have not been evaluated in controlled trials. Low quality evidence suggests that hormone therapy may lead to improvements in psychological functioning."
This 2016 review [5] claimed a positive conclusion ("gender dysphoria-related mental distress may benefit from hormonal treatment") but proceeds to note that "results mentioned earlier need to be considered in light of certain limitations". These limitations include: single site studies, small sample size, type/dose of hormone restatement usually not reported (and poor consistency when reported), “more than half the studies did not mention/control for psychiatric comorbidity”, and “recruitment/follow-up attrition represented an issue". They also hide this key point: "most importantly, as no study used a blinded randomized controlled trial design, results could have also different explanations because of the study design" in the limitations section. Given the extent of the issue, these limitations should have at least been mentioned in the abstract and the researchers should not have suggested such a definitive conclusion.
This 2018 review [6] indicated that "although the existing body of research supports [gender-affirming hormone therapy] improving mental wellness, many studies used cross-sectional and uncontrolled observational methods relying on self-report." Again, this important caveat was hidden in the conclusion; with the abstract making far bolder claims than supported by evidence.
This 2019 review [7] concluded that "because the certainty of this evidence was very low to low, recommendations for hormone use to improve quality of life, depression and anxiety could not be made."
This 2021 review [8] came to the same conclusion stating "certainty in this conclusion is limited by high risk of bias in study designs, small sample sizes, and confounding with other interventions."
Even for the very few "controlled" studies, they are not randomized control trials. Instead they are before treatment – after treatment comparisons for transgender individuals or cross sectional studies comparing transgender and "cisgender" comparison groups. Notably, neither of these designs allow the researcher to elucidate the origin of observed effects (e.g., is improvement coming from hormone therapy or social affirmation?).
(And as a side note, this Cochrane (the "gold standard" for those unaware) review [9] concluded: "We found insufficient evidence to determine the efficacy or safety of hormonal treatment approaches for transgender women in transition. This lack of studies shows a gap between current clinical practice and clinical research. Robust RCTs and controlled cohort studies are needed".)
---
Confounding factors: the effect of hormone therapy on non-transgender individuals
There's a particularly important confounding factor here; we have evidence that hormone therapy is associated with improved mood. As such, improved mood with gender affirming care may simply be the result of this natural physiological effect.
This 2023 systematic review and meta-analysis [10] with "14 eligible randomized controlled trials (RCTs) ... to investigate the effect of exogenous estrogen on depressive mood in women" found "strong evidence that exogenous estrogen exerts its antidepressant effect by stabilizing estrogen levels".
This 2009 systematic review and meta-analysis [11] with "seven studies (N=364) ... that included a placebo-control group in a double-blind design" found "[testosterone] may have an antidepressant effect in depressed [men], especially those with hypogonadism".
This 2014 systematic review and meta-analysis [12] of "sixteen trials with a total of 944 subjects ... showed a significant positive impact of testosterone on mood" and ultimately concluded "Testosterone may be used as a monotherapy in dysthymia and minor depression or as an augmentation therapy in major depression in middle-aged hypogonadal men".
This 2019 systematic review and meta-analysis [13] of "27 randomized placebo-controlled clinical trials involving a total of 1890 men found that testosterone treatment was associated with a significant reduction of depressive symptoms, particularly in participants who received higher-dosage regimens."
Further, the fact that these results were all the strongest in people with lower endogenous hormone levels, lends support to the hypothesis that this effect would be substantial in cross sex supplementation given the naturally low endogenous hormone levels for these individuals. (Please note, however, that this hypothesis has not yet been investigated.)
This isn't a placebo effect, since the randomized controlled trials above indicate that the effect on mood is above and beyond any placebo effect. However, I believe it's a related point.
---
Hormones on cognitive function
To address the other point in that post, there really isn't evidence that women would "get smarter" if they take testosterone or men would "get dumber" if they take estrogen. Again, there's no high quality studies on transgender individuals, but there is some adjacent evidence for non-transgender individuals.
There is evidence that the reduction of estrogen levels in older women may be associated with cognitive decline. [14]
This review [15] and this study [16] both link higher endogenous testosterone levels in women (i.e., in women with PCOS) with lower cognitive performance.
That being said, this "randomized, placebo-controlled trial" [17] manipulated the levels of testosterone in women with PCOS and did not record changes in their cognitive function. This may be because the sample size was simply too small (n=29), or there could be a "critical window" in which testosterone effects women's cognitive performance, or any number of other possibilities.
These reviews [18, 19] found low testosterone levels are associated with with cognitive impairment in men although the effects of testosterone substitution are mixed. This appears to support the hypothesis that testosterone suppression may reduce cognitive performance, but in reality "the ability of the body to convert testosterone into estrogen suggests that part of the actions of testosterone could be mediated by estrogen". So, any decrease due to testosterone suppression would likely be offset by estrogen supplementation. In fact this review [20] discusses the evidence for this.
---
The stereotype threat
As suggested by @mycodyke, an important factor here is the stereotype threat. This refers to how "behavior can be a consequence of priming effects, ... when a stereotype becomes activated, stereotype-consistent behavior may follow automatically from that activation" [21].
The study she linked [22] goes into this, finding that men performed the same in a cognitive task regardless of priming condition, whereas women performed worse only when primed with female condition. This replicated an earlier study [23] that found "no sex differences were observed" when the task instructions didn't emphasize sex-stereotypes.
Other similar studies:
This study [24] found "sex difference was reliably elicited and eliminated by controlling or manipulating participants’ confidence"
This meta-analysis [25] suggested that "male superiority on spatial ability tasks ... is related to the implementation of time limits".
This study [26] also suggested this, finding that "the magnitude of gender differences was linearly related to the amount of time available for test completion".
All of this indicates that sex differences on this task (and likely in other similar situations) are the result of individual expectations about their performance. This is also commonly brought up for self-fulfilling prophecies; that is, if someone believes they will succeed/fail they are more likely to succeed/fail.
And this has real-world consequences. For example, in this study [27], "in a simulated job interview, [participants] … were confronted with either sexist … or non-sexist … behavior … [and] results indicated that female participants in the sexist condition performed significantly worse on the mathematical test than female participants in the control condition … suggest[ing] an influence of psychological and interpersonal processes on seemingly objective test outcomes."
---
Conclusion
I hope this helps! To sum up:
There is little to no high-quality research into the effects, benefits, or harms of hormone therapy for transgender adults or adolescents
There is evidence suggesting that hormone supplementation effects mood in non-transgender adults, indicating an important confounding factor for transgender hormone research
There is no evidence that testosterone makes women smarter or that estrogen makes men dumber; there is, in fact, some limited evidence suggesting the opposite
The belief in the above is likely a result of the stereotype threat; transgender individuals who have started hormone therapy are likely to perform worse/better because they believe they should perform worse/better as a result of ingrained stereotypes
References below the cut:
Cass, H. (2024). Independent review of gender identity services for children and young people.
Final report – FAQs. (n.d.). The Cass Review. https://cass.independent-review.uk/home/publications/final-report/final-report-faqs/
Clayton, A. (2023). Gender-affirming treatment of gender dysphoria in youth: a perfect storm environment for the placebo effect—the implications for research and clinical practice. Archives of Sexual Behavior, 52(2), 483-494.
White Hughto JM, Reisner SL. A Systematic Review of the Effects of Hormone Therapy on Psychological Functioning and Quality of Life in Transgender Individuals. Transgend Health. 2016 Jan;1(1):21-31. doi: 10.1089/trgh.2015.0008. Epub 2016 Jan 13. PMID: 27595141; PMCID: PMC5010234.
Costa, R., & Colizzi, M. (2016). The effect of cross-sex hormonal treatment on gender dysphoria individuals’ mental health: a systematic review. Neuropsychiatric Disease and Treatment, 1953-1966.
Nguyen HB, Chavez AM, Lipner E, Hantsoo L, Kornfield SL, Davies RD, Epperson CN. Gender-Affirming Hormone Use in Transgender Individuals: Impact on Behavioral Health and Cognition. Curr Psychiatry Rep. 2018 Oct 11;20(12):110. doi: 10.1007/s11920-018-0973-0. PMID: 30306351; PMCID: PMC6354936.
Rowniak, S., Bolt, L., & Sharifi, C. (2019). Effect of cross-sex hormones on the quality of life, depression and anxiety of transgender individuals: a quantitative systematic review. JBI Evidence Synthesis, 17(9), 1826-1854.
Baker, K. E., Wilson, L. M., Sharma, R., Dukhanin, V., McArthur, K., & Robinson, K. A. (2021). Hormone therapy, mental health, and quality of life among transgender people: a systematic review. Journal of the Endocrine Society, 5(4), bvab011.
Haupt C, Henke M, Kutschmar A, Hauser B, Baldinger S, Saenz SR, Schreiber G. Antiandrogen or estradiol treatment or both during hormone therapy in transitioning transgender women. Cochrane Database of Systematic Reviews 2020, Issue 11. Art. No.: CD013138. DOI: 10.1002/14651858.CD013138.pub2.
Zhang, J., Yin, J., Song, X., Lai, S., Zhong, S., & Jia, Y. (2023). The effect of exogenous estrogen on depressive mood in women: A systematic review and meta-analysis of randomized controlled trials. Journal of psychiatric research, 162, 21-29.
Zarrouf, F. A., Artz, S., Griffith, J., Sirbu, C., & Kommor, M. (2009). Testosterone and depression: systematic review and meta-analysis. Journal of Psychiatric Practice®, 15(4), 289-305.
Amanatkar, H. R., Chibnall, J. T., Seo, B. W., Manepalli, J. N., & Grossberg, G. T. (2014). Impact of exogenous testosterone on mood: a systematic review and meta-analysis of randomized placebo-controlled trials. Ann Clin Psychiatry, 26(1), 19-32.
Walther, A., Breidenstein, J., & Miller, R. (2019). Association of testosterone treatment with alleviation of depressive symptoms in men: a systematic review and meta-analysis. JAMA psychiatry, 76(1), 31-40.
Sherwin, B. B. (2003). Estrogen and cognitive functioning in women. Endocrine reviews, 24(2), 133-151.
Perović, M., Wugalter, K., & Einstein, G. (2022). Review of the effects of polycystic ovary syndrome on Cognition: Looking beyond the androgen hypothesis. Frontiers in Neuroendocrinology, 67, 101038.
Sukhapure, M., Eggleston, K., Douglas, K., Fenton, A., Frampton, C., & Porter, R. J. (2022). Free testosterone is related to aspects of cognitive function in women with and without polycystic ovary syndrome. Archives of Women's Mental Health, 25(1), 87-94.
Schattmann, L., & Sherwin, B. B. (2007). Effects of the pharmacologic manipulation of testosterone on cognitive functioning in women with polycystic ovary syndrome: a randomized, placebo-controlled treatment study. Hormones and Behavior, 51(5), 579-586.
Mohamad, N. V., Ima-Nirwana, S., & Chin, K. Y. (2018). A review on the effects of testosterone supplementation in hypogonadal men with cognitive impairment. Current drug targets, 19(8), 898-906.
Zhang, Z., Kang, D., & Li, H. (2021). Testosterone and cognitive impairment or dementia in middle-aged or aging males: causation and intervention, a systematic review and meta-analysis. Journal of Geriatric Psychiatry and Neurology, 34(5), 405-417.
Janowsky, J. S. (2006). The role of androgens in cognition and brain aging in men. Neuroscience, 138(3), 1015-1020.
Spencer, S. J., Logel, C., & Davies, P. G. (2016). Stereotype threat. Annual review of psychology, 67(1), 415-437.
Ortner, T.M., Sieverding, M. Where are the Gender Differences? Male Priming Boosts Spatial Skills in Women. Sex Roles 59, 274–281 (2008). https://doi.org/10.1007/s11199-008-9448-9
Sharps, M. J., Price, J. L., & Williams, J. K. (1994). Spatial cognition and gender instructional and stimulus influences on mental image rotation performance. Psychology of Women Quarterly, 18(3), 413-425.
Estes, Z., Felker, S. Confidence Mediates the Sex Difference in Mental Rotation Performance. Arch Sex Behav 41, 557–570 (2012). https://doi.org/10.1007/s10508-011-9875-5
Maeda, Y., Yoon, S.Y. A Meta-Analysis on Gender Differences in Mental Rotation Ability Measured by the Purdue Spatial Visualization Tests: Visualization of Rotations (PSVT:R). Educ Psychol Rev 25, 69–94 (2013). https://doi.org/10.1007/s10648-012-9215-x
Voyer, D. Time limits and gender differences on paper-and-pencil tests of mental rotation: a meta-analysis. Psychon Bull Rev 18, 267–277 (2011). https://doi.org/10.3758/s13423-010-0042-0
Koch, S.C., Konigorski, S. & Sieverding, M. Sexist Behavior Undermines Women’s Performance in a Job Application Situation. Sex Roles 70, 79–87 (2014). https://doi.org/10.1007/s11199-014-0342-3
18 notes
·
View notes
Text
By: Bernard Lane
Published: Dec 5, 2023
On the up
A study of young people who on average spent almost five years identifying as transgender has found they experienced better wellbeing and less gender dysphoria after they detransitioned from medical treatment or desisted in their opposite-sex identity.
“Detransition and desistance [giving up a trans identity before any medical treatment] were associated with marked improvements in psychological functioning,” says a new article published by the journal Archives of Sexual Behavior and authored by public health researcher Dr Lisa Littman, psychotherapist Stella O’Malley, detransitioner Helena Kerschner and sexologist Professor J Michael Bailey.
“On several relevant measures—gender dysphoria, flourishing, and self-harm—participants indicated great improvement after they stopped identifying as transgender,” the paper says.

[ Chart: Flourishing, or general wellbeing, rated by detransitioners, with the vertical access showing the number of participants for a given flourishing score, 10 being the highest wellbeing ]
Settling back into birth sex
Among the study group of 71 American females and seven males, aged 18-33, the overwhelming majority said they felt most “authentic” after they detransitioned or desisted.
External pressures—such as anti-trans discrimination, family resistance or religion—were rated as the least important drivers of detransition and desistance.
“The factors most important to relinquishing a transgender identification were internal factors, such as participants’ own thought processes, changes in participants’ personal definitions of male and female, and becoming more comfortable identifying as their natal sex,” the paper says.
Another reported impetus was the feeling that the causes of their gender dysphoria were more complex than they had believed. Looking back, the young people said a key influence in becoming trans was mistaking mental health problems or trauma as gender dysphoria.
“Against official advice I met [in 2021] a young lady called Keira Bell. She was a lesbian who told me the horrific experience that she had at the Tavistock [gender] clinic. It was an eye-opening experience [for me]. I know that [another MP] talked about ‘transing away the gay’ in his speech… We are seeing, I would say, almost an epidemic of young gay children being told that they are trans and being put on the medical pathway for irreversible decisions and they are regretting it… I am making sure that [in future] young people do not find themselves sterilised because they are being exploited by people who do not understand what these issues are…”—speech in the UK parliament, Equalities Minister Kemi Badenoch, 7 December 2023
Suddenly syndrome
Analysis of survey responses suggested that at most, 17 per cent of the group would have met the diagnostic requirements for the classic form of gender dysphoria with onset in early childhood.
Just over half the group (41/78) said they recognised themselves in the new, much more common form known as rapid-onset gender dysphoria (ROGD) with its onset during or after puberty.
Although a hypothesis rather than a formal diagnosis, ROGD seems to describe the post-2010 international explosion in socially influenced clusters of teenagers, chiefly girls, suddenly embracing trans or non-binary identities.
The study by Littman et al found that young people in the group who reported less gender dysphoria in childhood were more likely to say that the term ROGD did apply to their experience.
“The purpose of this research is to learn about the experiences of desisters and detransitioners—specifically, to explore: 1) factors that may or may not be related to the development of and desistance from transgender identification; 2) whether or not individuals experienced changes in their sexual orientation during and after transgender identification; and 3) what kinds of counseling and informed consent were received by those who sought medical care to transition.”—flyer used to recruit participants for the Littman et al study
Inconvenient for gender experts
The authors say their findings are “necessarily tentative” and acknowledge several limitations in the research, which involved a convenience sample of young people being asked to recall their experience before, during and after gender transition.
The study cannot show how common detransition is, nor establish whether these particular young people happened to be bad risks for transition, nor elucidate whether better psychological health is a cause or an outcome of detransition.
Detransition and desistance are understudied and contentious topics. ROGD has awkward implications for the “gender-affirming” treatment approach with its dogma of young people as “experts in their gender identity”.
Activists highlight the paucity of research on ROGD—first described in 2018 by Dr Littman—while seeking to sabotage any more studies and pressuring journals to retract papers exploring this phenomenon.
The Littman et al study just published had to adopt videoconference screening to check that would-be participants were genuine; activists had boasted on social media about taking the online survey and giving fake responses.
“When little is known [about detransition and desistance], imperfect research is often better than no research,” Dr Littman and her colleagues say in their paper. “It can provide provisional answers, better-informed hypotheses, and ideas for future research.”
“Despite the absence of any questions about this topic in the survey, nearly a quarter (23 per cent) of the participants expressed the ‘internalized homophobia and difficulty accepting oneself as lesbian, gay, or bisexual’ narrative by spontaneously describing that these experiences were instrumental to their gender dysphoria, their desire to transition, and their detransition.”—A survey of 100 detransitioners, Dr Lisa Littman, September 2021. (Dr Littman believes there would be little if any overlap in participants between this 2021 group and those surveyed in the current 2023 study.)
youtube
[ Video: Corinna Cohn, who transitioned three decades ago when safeguards were stronger, testifies in support of a bill restricting paediatric transition in the American state of Ohio ]
Yes, they were trans
In the 2023 Littman et al study, all the males and most of the females had taken cross-sex hormones, almost a third of the females had undergone mastectomy and a small number had their uterus or ovaries removed. (Only two participants had taken puberty blockers, which Dr Littman attributes to the average age of trans identification being too old at 17 years.)
“Our participants invested a great deal of their lives in their gender transitions—in terms of time, disruption, and serious social and medical steps. Thus, we do not believe that a principled case can be made that participants detransitioned because they were never gender dysphoric,” the Littman et al paper says.
The researchers say that follow-up studies of gender dysphoric youth are “urgently needed”, and that gender clinics have “a particular obligation” to keep track of past patients—“Unfortunately, in North America at least, we see little evidence that this presently occurs.”
“Detransition has become much more visible in recent years. However, it was only recently that the rates of detransition began to be quantified. According to recent UK and US data, 10–30 per cent of recently transitioned individuals detransition a few years after they initiated transition.”—Current concerns about gender-affirming therapy in adolescents, Professor Stephen B Levine and E Abbruzzese, April 2023
Some other key points of the 2023 Littman et al paper—
Only 27 per cent of the young people had told their former gender clinicians they had detransitioned. Most of those who took cross-sex hormones obtained them through the fast-track “informed consent” model. Two-thirds of the group felt they had not been adequately informed about the risks of medical transition. Fewer than one in ten had been told about the lack of long-term outcome studies for females with adolescent-onset dysphoria. Important influences for females becoming trans men included wanting to avoid mistreatment and sexualisation as women. Almost half the females indicated they were exclusively attracted to women. ROGD may be chiefly a female condition, with the possibility that some males taken to be ROGD may actually be manifesting hitherto-suppressed autogynephilia (sexual arousal among males who cross-dress and/or imagine themselves as women). More than a third of the group said most of their offline and online friends became trans-identified and it was common to mock people who were not trans. Among counter-intuitive results, acknowledgment of the ROGD label by participants was not significantly related to the age at which they took on a trans identity. Psychiatric diagnoses before transition were common, including depression (63 per cent); anxiety (60 per cent); attention deficit/hyperactivity disorder (24 per cent); eating disorder (23 per cent); obsessive compulsive disorder (18 per cent) post-traumatic stress disorder (15 per cent); bipolar disorder (12 per cent); hair pulling (10 per cent); and autism spectrum disorder (9 per cent). Young people in the study showed relatively high scores on a trauma measure of “adverse childhood experiences” such as abuse inflicted within the family. The participants had generally liberal politics and a clear majority supported gay marriage (67/78) and trans rights 71/78).
==
Coming to terms with the nature of your body, rather than chasing a fantasy and delusion, leads to better mental health. Imagine that.
#Bernard Lane#detrans#detransitioners#gender ideology#queer theory#ROGD#rapid onset gender dysphoria#medical transition#medical malpractice#medical corruption#medical scandal#mental health#religion is a mental illness#Youtube
43 notes
·
View notes
Note
Do you have any tips on how to have an orgasm when you're mastubating as a cis woman?
Hmm, well, lets go ahead and acknowledge upfront that I am not a cis woman, so while I can share things I've learned about my own anatomy or the pleasure of cis women I've dated/had sex with, all of this will be very second hand, sorry about that.
Lets start with some scholarship:
From "In Pursuit of Pleasure" (first link)
The gendered context of pleasure Not all individuals will have equal opportunities for pleasurable sexual experiences (Hall, 2019). More specifically, experiences of sexual pleasure seem embedded in a gendered 3 context. Around the world, sexual complaints are more prevalent in heterosexual women than in heterosexual men (Laumann et al., 2005). In most contemporary societies, heterosexual women’s sexual pleasure is still generally subordinated to heterosexual men’s pleasure (Hall, 2019; van Lunsen et al., 2013). In (religious) traditional cultures sexual pleasure of women is judged to be more dangerous and undesirable than that of men, or even considered irrelevant (Hall, 2019), probably because sexual pleasure of women does not appear to be directly related to reproductive success. Sexual pleasure of men, at least pleasure entailing orgasm withejaculation is condoned, if not prioritized, as procreational duties depend on it. Consequently, only those problems that interfere with sexual pleasure of men or with procreative sex are deemed worthy of complaint or treatment (Hall, 2019), while sexual issues that are important and distressing to women (and individuals engaging in non-procreative sex), including a lack of sexual pleasure, go unnoticed. Sexual pleasure remains an understudied topic in all populations, but especially in marginalized ones. Even though we touch upon findings onsexual pleasure in LGBTQ þ populations, this review has a cisgender, heterosexual, western, educated, industrialized, rich, democratic (WEIRD; Klein et al., 2021), and quantitative research focus. A timely review and commentary on research into pleasure among transgender and gender diverse individuals was recently published by Bradford and Spencer (2020). They argue that, despite an increased research interest into how these populations experience their sexuality subjectively, many studies are still focused on quantitative designs and how physiology and medical interventions might curtail sexual experiences of transgender and gender diverse people (Bradford & Spencer, 2020). Multimethod research among men who have sex with men of diverse racial identity and self-identifying gay men has shown how these men defy and wrestle with social scripts on how they experience, negotiate, and share sensual and emotional aspects of pleasure across different relational and sexual contexts (Calabrese et al., 2015; Hoppe, 2011; Kiguwa, 2015). We reiterate Bradford and Spencer’s call to pay attention to and allocate research efforts to study the similarities, potential discrepancies, and diversity in pleasure(s) within and across populations, and to use mixed- and multimethod designs to allow people to report on their agency and subjectively lived experiences. In what follows, we review the available evidence for (cis) gender differences in experienced sexual pleasure.
We know that sex and orgasm are both INTENSELY psychologically dependent activities, even for those we might expect to have a purely physicalized experience of it. It is worth remembering that orgasm is difficult to acheive when "in your head" or otherwise overthinking the process due to anxiety, past trauma, or social stigma. This means that regardless of gender (but especially for those of us for whom the relationship between gender and sex is complex or painful) one of the best things we can do for ourselves is learn how to genuinely relax into the moment and activity.
Global WHO data suggests 1 in 3 women have experienced sexualized violence and or violent sex, usually in the context of intimate partner violence. This is, quite understandably, going to complicate a bare minimum of a third of the female population's relationship to their sexuality. At that kind of scale, we are often operating in the realm of communal trauma, something that tends to carry high rates of impact and expression of psychological and physiological stress secondary to trauma or vicarious trauma, regardless of whether or not an individual has been personally harmed. The "miasma of threat" is a large part of how mass trauma situations become/remain systemic and pervasive.
To that end, working with other survivors to reconnect with your body, to disentangle some of the messages we've internalized over a lifetime, and to learn how to relax into pleasure are critical. They will also be fairly unique processes to each of us, and so hard to gift to each other directly. This is part of why I am so vusible about modeling my own process: not because I think it will work for everyone, but because we all need one, and an example of someone else's can be part of what helps us find that.
But this has all been general and ungendered advice truly, so let's get into what may be more specific for your body!
Again: I am not a cis woman. I share some anatomy, and I've had sex with several, but I am only reporting what I have learned through clinical sexology research or from a partner or friend directly
The current research suggests that "male orgasm" is a cluster of sensory triggers for penile ejaculation which seems to have SOME but not MUCH overlap with the "female orgasm" which is understood as a multi-faceted and often highly variable set of triggers for clitoral pleasure, vaginal ejaculation, and other iterations of orgasm. So right off the bat here's one important piece of info: there are different kinds of "male" orgasms, and A LOT MORE different kinds of "female" orgasms, meaning those with clits, vulvas, vaginas, cervixes, etc may find they have to explore a lot more variety in activity before finding what works. For example, women who can orgasm via penetrative vaginal sex alone do exist! But they aren't necessarily common. And while some of this is absolutely psychologically reactive, plenty of it probably isn't. After all, I have a vagina, and have always been able to orgasm for vaginal sec even when I *couldn't* from other more common triggers due to my psychological reactivity. Everyone's body will handle nerve endings and erogenous zones a little differently, and it's good to learn yours.
Cis women are rarely encouraged to explore their bodies outside of sex with a male partner, and I can tell you first hand it doesn't matter who you are, what your into, etc, if the only time you interact with yourself sexually is in bed with a partner, you're really limiting your ability to know yourself and enjoy sex with said partners. Most of my best moments of sexual pleasure were related to totally platonic or even independent sensory-exploration of my body, and as someone who was alienated from my body different but connected reasons to a cis woman, I cannot recommend enough the healing effects of like. Hanging out in bed on a lazy saturday and just touching yourself in different ways to see what happens.
Clits are an easy starting place! They're massive nerve clusters, definitely can help overwhelm and psychological distress around sex long enough to enjoy the pleasure (although really its time and practice), and they're talked about a lot these days! But how many different ways have YOU, person who has their own clit, actually explored touching it? Some favorable xonsiderations from previous partners:
Mouth or mouth dupe toys - over and over again I hear from cis women that their preference is oral and they wish they had a non-partnered option. Well guess what ladies, there is. Mouth dupe toys are just fleshlights and grip silicon anymore. The classic viral toy that had housewives losing their shit in the reviews on Amazon are still available and affordable, but there is a WHOLE world of mediated sex out there for the taking babes
G-spot insertable vibrators/dildos/stimulators - this is less about nane or performance and more about shape. If you want something to slide home against the deeper erogenous zones inside the vagina, you want a long, thin, curved insertable with a widely flared head. Please always remember to learn about body safe materials and protective sheaths before you use any insertable toy
Learn how you like to ride, and practice on your own without a partner. When I first got into fucking other people, it was SO fucking confusing to be anything but a Pillow Princess (affectionate) during sex because I didn't know how to fit my body with another person's for pleasure. My go-to masturbation technique was literally ON MY BACK and like. Fine, it gets the job done when I'm by myself. But I actually really fucking hate missionary position sex regardless of the kind. Riding isn't exactly my favorite either (hellooooooo doggie style 🥵🥵) but it's a really great way to learn a partner and a new fit. Also, sex saddles, pillows, and position aids are easy to use to set up a way to ride on your own! This gives you the space to learn what you like about angle of penetration, depth, pace, impact or absence of it at the cervix, and even how you like to be touched during sex (riding a dildo secured in a position aid is hands free baybee!) without bringing in the added complexity of your partner's pleasure or interaction with YOUR pleasure
Communicate with your partner when you like something. And not only in the cute pillow talk way after or the sexy dirty talk during. Sometimes you need to communicate with your partner in advance what certain reactions from you mean so they can better interpret them. E.g. my muscles get a bit spastic when I'm getting close to orgasm, so partners that know this can recognize "he's reaching for nothing or clawing at my back in a way that's not steady, I should do more of this." I have a partner whose pitch changes when she really likes something, she gets breathy and hits a soprano note for a second when I do things she really likes. So what should your partner's take from it when your body goes REALLY tense, is that anxiety or is that pleasure? What does it sound like when you moan to be sexy for them and how is that different from when you moan because you just can't fucking help how GOOD it feels? If they're fucking your vagina and they hit your cervix or the curve before it, is that gonna make you hit the roof because it hurt or because it's about to make you cum like a gyser? Are you shaking because your muscles are flagging or because you feel amazing?
Stop more often than you don't. This is a "play it by ear" thing because the longer you're learning yourself, the less this needs to be true, but only you'll know when it's time to step another rung down on the caution. Forcing your way through sex that it flagging as unsafe for you, much like forcing your way past a gag reflex, will only make future reactive reflexes more frequent, more severe, and more likely to create barriers between you and a healthy relationship with your sexuality. If something feels off, just stop. It's better to take your time getting back into the mood once you're sure you have what you need to do so safely.
Another REALLY helpful tool is learning some anatomy. There are SO MANY erogenous zones on the body, and while self-exploration is how you ensure you don't miss any of your own, it can be nice to learn more about both your partner's and your own potential hotspots. Maybe it's the service-orientation in me, but nothing makes my dick harder than the sounds my girl makes right before she comes. Nothing on god's green earth has ever been hotter to me than the way she grabs my hips or my head, whatever I'm using on her, and wails like a fuckin banshee. I have fully had hands-free orgasms off that before and fully plan to again as often as possible 😅
But like. I've fucked enough people now to assume most of us really like seeing our partner experience pleasure from being with us, even if it's not always so extreme (remember folks, I'm a slut and making me cum ain't fuckin hard, don't compare yourself to me if that ain't your bag yet, don't worry you'll figure out your path to it). So take the time to explore them the way you explore yourself! First of all, it models for your partner what THEY should do FOR YOU. Cis men especially (but cis women too, lesbians you aren't getting off the hook for this one, we both know what I mean) often struggle to think of sex and foreplay outside of the four cornerstones of pussy, ass, tits, and mouth. Sometimes you get a partner who knows to go for a neck or a thigh, sometimes you fuck a foot fetishist, but when was the last time someone figured out how to bring you a little rush of sexual pleasure with how they stroke your forearm? Or that spot in the small of your back that makes you shiver? Or how about that spot on the throat JUST below the corner of your jaw? When was the last time someone's hand moving to the back of your knee to hitch up your thigh around the waist make you moan even before they start to grind with you? Variety is the spice of life for a rrason, and it is CRUCIAL that neither you nor your partner get ritualistic about where you touch each other. Some examples from Healthline of EZ maps:






This has gotten really long lmao, so Imma wrap it here, but if it brings up more questions or you have more thoughts, you know where to find me Anon!
And as always I would be remiss if I didn't end on this note:
Orgasms are amazing and fun and intimate and ABSOLUTELY NOT IMPORTANT.orgasm is a satisfactory culmination of sexual arousal, and I **promise** you, no matter what you think, it is quite literally INEVITABLE if you know what you need to crest that hill. The process will always matter more than the outcome because the outcome is literally a sign that the process has occurred in the first place. You will likely struggle with orgasm if orgasm is THE POINT and I have seen this as much with cis women as with cis men as with trans folks of all genders. But if you can set aside orgasm and instead relax into pleasure, and you know how much time and how much ramp up you need, then the orgasm will just....happen when you get to it. Forcing it will only make it fade.
3 notes
·
View notes
Text
The violent altercation resulted in police intervention. At first, Smith’s boyfriend claimed she had been abusive towards him. But later, Smith says he tried to blame it on his gender identity issues.“ While she was checked into a hospital to heal from the abuse she was reported to the police for stating that her abusive ex was transgender.
A UK woman has been summoned for an interview by Derbyshire Police over alleged “transphobic” behavior during her hospital stay at Chesterfield Royal Hospital.
Toni Smith* says she received the notice just after being released from the hospital’s mental health unit where she had been seeking treatment following a traumatic episode related to her past abuse by a trans-identified male.
Speaking to Reduxx and The Publica for an exclusive joint report, Smith explained that she was voluntarily admitted to Chesterfield’s Herrington Unit in January after contacting emergency services herself and explaining that she had self-harmed.
Smith is a survivor of repeat sexual and physical abuse — abuse she says she suffered at the hands of her transgender ex-boyfriend.
“When we met, he was a bodybuilder. His biceps were bigger than my head. I’d never met anyone as big as him.” Smith says, explaining that the two became an item in 2017.
Just over one year into the relationship, Smith says she discovered that her partner had a proclivity for wearing women’s clothing and expressed a desire to transition.
“It completely blindsided me. I had thought for a while that he had [body] issues… at first, a lot of the habits he had were similar to the issues my body dysmorphia caused me. So I thought it was similar.”
Smith notes that while she was not hostile to her boyfriend’s decision, she was not interested in affirming his declaration.
Given the gender ideology debate was still far-removed from mainstream popularity at the time, Smith says she had never given too much thought to the politics surrounding transgenderism
However, her feelings about her partner’s “transition” were mixed.
“I knew straight away that I would not stay in the relationship. But I felt sorry for him, I wanted to help him feel comfortable with whatever life he was living, and I thought we could part as friends after that.”
But it wasn’t long after that Smith says her partner became physically abusive towards her and their disagreements would often turn violent.
“He abused me horrifically,” Smith alleges. “One time, he sat on my chest and strangled me until I passed out.”
The violent altercation resulted in police intervention. At first, Smith’s boyfriend claimed she had been abusive towards him. But later, Smith says he tried to blame it on his gender identity issues.
“He told me that the reason he’d strangled me and was so horrible was because he was jealous of me,” she explained.
Smith says the abuse continued to escalate, with her boyfriend’s gender identity becoming a catalyst for the continued deterioration of the relationship and her mental health.
“He would take my make-up and accuse me of cheating. He controlled the money but would message his family claiming I was spending it on myself or drugs. He also began coercing me into having sex with other men for money,” Smith says, explaining that “at first” he didn’t force her, but would instead invite men over and put her on the spot.
“One of them, near the end, injured me quite badly. [My partner] knew it was too much because it was the last time he made me do it. I think with others he told himself he wasn’t abusing me because I eventually gave in. He thinks that’s consent,” Smith says. “There was a lot of blood. I started getting pains after that low down in my stomach. After I left him one day I collapsed and started convulsing and the hospital found my birth control coil had been dislodged and was basically stabbing into my cervix and embedding in the inside of it.”
Smith provided Reduxx and The Publica a number of covert videos she had recorded while in the relationship. In one, he admitted to spraying a household cleaning disinfectant down her throat because she accidentally got facial toner on him while she was spritzing it on her face.
In another video from April of 2020, Smith captured an interaction with her partner, who is seen wearing long red-dyed hair and pink pajama pants, becoming angry at her for singing in the bedroom — something Smith says she was doing to block out the verbal abuse he had been directing at her.
The interaction ends with him storming out to shut the house’s electricity off, leaving Smith in pitch-black darkness while he calls her “abusive.”
Smith alleges that after she stopped recording to go turn the electricity back on, he kicked her into a wall.
Disturbingly, Smith says her partner then reported her for a “hate crime” for not sufficiently affirming his gender identity — something she says had happened multiple times before in their relationship.
Police attended the residence, but classified it as a simple domestic dispute with no intervention needed.
The next day, Smith decided to end the relationship.
“The day I left, I was begging him to get help. He told me he wouldn’t … so my friend called me a taxi and I left. I went up to the north of England, at which point I suppose he realized I was not actually going to come back to him. He started threatening to kill himself unless I did, but I refused.”
Over the coming week, police contacted Smith with questions about the relationship, clearly concerned about the distressing number of calls that had come out of the residence over time.
Smith finally opened up to officers about the abuse after the relationship ended. Merseyside Police arranged for her to record a video statement, and Derbyshire Police took over the case.
In June of 2020, two months after Smith left, her ex was arrested while police investigated Smith’s claims of having been sex trafficked by him.
“The reason it took them so long between my statement and arresting him was because they went through every report he’d made against me. He’d been reporting me without my knowledge and there were so many reports it took them a couple of weeks to make sure they’d closed all of his, which they said they now regarded as malicious and false,” Smith explained.
Reduxx and The Publica reviewed communications exchanged between Smith and a constable with the Derbyshire Police, in which “she/her” pronouns were used for her abuser.
No charges were ultimately pursued and minimal details were provided to Smith on why that decision had been reached.
“[The constable] came and said that his superior felt there wasn’t enough evidence and refused to even ask the crown prosecution service for a decision. He just closed it with no further action.”
Though Smith expresses her relief that the relationship had ended, she continued to struggle with her mental health even after the break-up.
She experienced depressive episodes, self-harm, and severe anxiety. At times, Smith says she was scared to leave the house out of fear she would see one of the men who had been apart of the sexual abuse she endured while with her ex.
In January of 2023, Smith says she had a severe self-harming episode, and contacted her local hospital for help.
She was directed to the emergency room at Chesterfield Hospital due to a lack of space, and was ultimately admitted to the Hartington Unit, the hospital’s psychiatric facility. Smith was placed in the female section for treatment, where she would spend the next few weeks rehabilitating.
While there, Smith befriended a few other female patients in the unit — one of which, unbeknownst to Smith, identified as non-binary.
“There was no mention of her being non-binary. I didn’t know. I had heard her make a comment about another patient, saying that she was ‘transphobic and no mental illness causes that,’ which I thought was strange,” Smith says, continuing: “But there was no mention of her identity specifically. She seemed to be on a low-end of having a mental illness and was very functional.”
While the two had an amicable relationship at first, things went downhill after the non-binary individual overheard Smith discussing her ex-partner with another patient.
“She heard me talking to this other lady in the common area … I was opening about my ex and mentioned he was transgender,” Smith explained. She says that after she came in from an evening cigarette break, the non-binary patient was “screaming at the top of her lungs” about trans rights.
“She was standing in the communal area, shouting ‘trans women are women,’” Smith says. “She was shouting it. This wasn’t a private conversation.”
Smith explains she immediately perceived the outburst as being directed at her, and approached the young woman to relay her own experience.
“I told her, ‘go and get raped by one and tell me how much of a woman they are,’” Smith says. “I didn’t shout at her, and then I walked off and went to bed.”
It was the next day that the incident occurred which was ultimately reported to police.
“I got into an argument with a nurse who kept insisting the shouting patient was non-binary, not female. That gaslighting affects me in a strange way, because of my experience. [The nurse] told me, ‘they’re not a woman,’ and I said, ‘yes she is, she’s on a women’s ward, for a start.’”
Smith says she got very upset, and the non-binary patient overheard the conversation and began shouting from another area, recognizing the conversation had been about her.
Smith’s new partner would later call the hospital to complain about the nurse’s conduct, concerned that they had caused her emotional distress.
“We could not work out how this hospital was, on one hand, supposed to treat me for my trauma which they understood was caused by a transgender male, and on the other, argue with me that a woman was not a woman.”
Smith says the incident made her want to leave the hospital because she felt increasingly distrustful of the staff.
She was discharged at the end of February, and, approximately one month later, was issued a notice from Derbyshire Police informing her she was required to attend the station for a formal interview.
In the letter, police explain Smith was alleged to have “performed a public order offense” in which she “directed words deemed offensive towards another individual on the ward.”

The date on the letter corresponds with the conversation Smith had with the nurse in the kitchen about the non-binary patient.
Smith explained that she was incredulous about the letter, taking particular issue with the fact police issued it despite knowing she had been a patient on a psychiatric ward receiving treatment for her mental health.
“This specific thing does not frighten me. I know they won’t be able to prosecute me. I know the law well enough… but the fact that the police are able to harass women because of their speech is frightening,” Smith says. “There’s nothing I said that is criminal. But it does worry me that they are doing this to women.”
Reduxx and The Publica reached out to Derbyshire Police for comment but did not receive a response to the inquiry.
In the interim, Smith says she has no intention of contacting police, noting that they have her contact information but have yet to reach out to establish a date for her station interview.
“If they want me to come down, they know where I am. This whole asking me to be proactive to arrange for my own police interview… I’m not going to do that. I shouldn’t have to.”
Smith only recently became more involved in discussions surrounding gender identity through online communities, seeking support for her past experience having been abused by a trans-identified male.
“This whole movement… it’s a misogynistic men’s movement, I feel. It has nothing to do with ‘trans rights.’ They’re going after vulnerable women, and demanding we change the way we see the world.”
Disturbingly, Smith is not the first woman in the United Kingdom to face police intervention after “offending” a transgender individual.
In January of this year, a disabled woman in South Wales had her home searched and was subjected to police detention after being reported for committing a “transphobic hate crime” for putting up stickers raising awareness about domestic violence.
The next month, Caroline Farrow, a mother of five who has been outspoken against gender ideology, had her house forced into by Surrey Police after her social media activity was reported as criminal. Farrow had previously been investigated by police in 2019 for misgendering a trans-identified male on Twitter.
*Smith’s surname has been changed to protect her identity.
#UK#Don’t the Derbyshire Police have real crimes to investigate?#Chesterfield Royal Hospital#Abusive men know how to lie to make themselves the victim#Can’t that non-binary patient be reported for harassing someone with a mental illness?#The TRAs love spewing hate for the cops until a woman hurts their feelings#The the TRAs know the difference between men and women
12 notes
·
View notes
Text
Vyacheslav Volodin, Chairman of the State Duma from the United Russia Party (concluding remarks): Earlier today, our Minister of Labour and Social Protection reported on our state Demography programme’s progress, highlighting the issue of declining birth rates. When we discussed this matter, it revolved around income-related issues, but that’s not the crux of the matter. If there is a cult of the family, if one values and cherishes moral values inherited from grandfathers and great-grandfathers, then there is no doubt that the family will be large. However, if through relentless indoctrination these values morph into self-absorption and the freedom to change one’s sex, we won’t see large families in the future. This may even question the state’s existence. But the most frightening part is the child abuse.
Just look at the current situation in the United States, where these pseudo-values are being propagated. The rate of transgenders is already three times higher among teenagers than it is among mthe adult population, the result of propaganda. The number of children undergoing hormone therapy has more than doubled in five years. They start administering hormones to kids as young as eight, eight. From 2017 to 2021, more than 2,000 sex-change operations were performed on children aged 13 to 17. We don’t want this to occur in our country. Let the U.S. pursue its diabolic policy. We’ll see how it ends.
This won’t yield any positive outcomes. It’s pure satanism.

3 notes
·
View notes
Text
The Realities of Online Harassment: How Can We Address It?
In the digital age, social media has become a powerful tool for connection, activism, and self-expression. However, it also has a darker side—online harassment. This widespread issue affects countless users, especially women and marginalized communities, creating a toxic online environment. Let's explore why online harassment persists and what we can do to make digital spaces safer.

Marwick and Caplan analyze how harassment is often networked, particularly targeting feminists and women in public spheres. The term "manosphere" refers to a collection of online communities, including men’s rights activists, pickup artists, and anti-feminists. These groups coordinate harassment tactics like doxing, social shaming, and spreading misogynistic rhetoric. The concept of "misandry" is often misused in these circles to frame feminism as hostile towards men, justifying their harassment campaigns. (Marwick & Caplan, 2018)
The study highlights examples like Gamergate, where coordinated online abuse targeted women in the video game industry. This networked behavior not only perpetuates misogyny but also normalizes it within certain digital communities.

Haslop et al.'s research focuses on the UK university context, exploring how young people, particularly women and transgender students, experience online harassment. The study challenges the stereotype of the "snowflake generation" being overly sensitive. Instead, it shows that many students tolerate harassment as part of their digital experience, especially in peer-to-peer interactions. (Haslop, O’Rourke & Southern, 2021)
Marwick and Caplan (2018) argue that networked harassment by the manosphere, including tactics like doxing and social shaming, demonstrates a coordinated effort to suppress feminist voices and reinforce misogynistic ideologies.
What Can Be Done? Addressing online harassment requires a multi-faceted approach:
Stronger Regulations: Governments need to enforce laws that protect users from online abuse, such as the Online Safety Act 2021 in Australia, which forces platforms to remove harmful content promptly.
Platform Accountability: Social media companies must invest in better moderation tools and policies to reduce the spread of hate speech.
Community Support: Users can play a role by reporting abusive content and supporting those affected.
What Can Be Done? Addressing online harassment requires a multi-faceted approach:
Stronger Regulations: Governments need to enforce laws that protect users from online abuse, such as the Online Safety Act 2021 in Australia, which forces platforms to remove harmful content promptly.
Platform Accountability: Social media companies must invest in better moderation tools and policies to reduce the spread of hate speech.
Community Support: Users can play a role by reporting abusive content and supporting those affected.
What Can Be Done? Addressing online harassment requires a multi-faceted approach:
Stronger Regulations: Governments need to enforce laws that protect users from online abuse, such as the Online Safety Act 2021 in Australia, which forces platforms to remove harmful content promptly.
Platform Accountability: Social media companies must invest in better moderation tools and policies to reduce the spread of hate speech.
Community Support: Users can play a role by reporting abusive content and supporting those affected.
Reference list
Haslop, C, O’Rourke, F & Southern, R 2021, ‘#NoSnowflakes: The toleration of harassment and an emergent gender-related digital divide, in a UK student online culture’, Convergence: The International Journal of Research into New Media Technologies, vol. 27, no. 5, pp. 1418–1438.
Marwick, AE & Caplan, R 2018, ‘Drinking male tears: language, the manosphere, and networked harassment’, Feminist Media Studies, vol. 18, no. 4, pp. 543–559, viewed <https://www.tandfonline.com/doi/full/10.1080/14680777.2018.1450568>.
0 notes
Text
Even Black people who don’t support queer rights oppose attacks on LGBTQ+ equality
Approximately 65% of Black Americans identified themselves as “supporters of Black LGBTQ+ people and rights,” including 57% of Black Americans who go to church, according to a new study by the National Black Justice Coalition (NBJC). The Black Facts survey focused on those who identify as passive allies of Black LGBTQ+ people and found that such allies are “moveable by connecting the dots” from issues of racial justice to the support of LGBTQ+ rights. After informing respondents about the societal risks Black LGBTQ+ people face, many individuals felt moved to be more supportive, including those who self-identified as opponents of LGBTQ+ rights. Related Research says that Black queer youth experience widespread discrimination and social rejection Advocates are using this research to create better safe spaces for Black LGBTQ+ youth The study’s key findings emphasized that Black individuals, regardless of sexual orientation or gender identity, share a desire to combat threats against their community. The survey also found that those who know Black LGBTQ+ individuals are more likely to be supportive, and that “compelling messages” about equality can move Black respondents to give more support to queer community members. Stay connected to your community Connect with the issues and events that impact your community at home and beyond by subscribing to our newsletter. Subscribe to our Newsletter today The majority of respondents expressed concern for suicide rates among Black LGBTQ+ children, including 47% of respondents who self-identified as opponents of LGBTQ+ rights. One survey respondent, a Black man from Atlanta, said, “If your family don’t support you and you feel like they’re going to beat the gay out of you or whatever, you’re going to consider the suicide because you know what? You’re going to feel like nobody supports you.” Among those who self-identify as LGBTQ, 86% of respondents felt that they have a shared fate with other Black individuals. However, 51% of non-LGBTQ+ Black individuals said they feel a shared fate with LGBTQ+ Black folks. A lack of interactions with Black LGBTQ+ folk reduced support for the Black queer community, but support increased with the number of ties respondents reported having to LGBTQ+ people. Additionally, the survey found that a lack of support for Black LGBTQ+ individuals by the Black community led to increased feelings of isolation from Black queer respondents since many of the latter reported they also couldn’t trust white LGBTQ+ people to provide a supportive community for them. “From my perspective [white LGBTQ+ support] depends on the day,” one respondent said. “Sometimes they can be your friend, and sometimes they can look the other way if you’re getting ousted by the police or somebody.” The survey also found that the number of respondents who reported knowing a Black transgender or gender non-conforming individual is roughly the same as the average of U.S. residents who know transgender or gender non-conforming person. Reduced acquaintance with trans and non-conforming individuals resulted in lower levels of support for these queer community members. Additionally, the survey found that 89% of Black LGBTQ+ individuals thought that “the Black community should do more to support Black LGBTQ+ people,” while 73% of Black Gen Z respondents felt the same. Additionally, 65% of all respondents felt that there was more work to be done in supporting Black LGBTQ+ individuals. “You see the connection, you see how we are linked… I think more or less we have more in common probably than I would think just on the surface,” said a respondent, a Black woman from Philadelphia. In a press statement about the study, NBJC CEO and Executive Director Dr. David J. Johns said, “This research study highlights the importance of turning down white noise to better appreciate the significance of Black Queer leaders at this particular moment in the maturation of our democracy. We’ve experienced the… http://dlvr.it/T8k7Bz
0 notes
Text
Week 10: Unveiling the Impact of Online Harassment: Impeding Women's Digital Participation and Citizenship
Online harassment is offensive behavior directed at others through technology channels, such as the internet or text messaging, which can cause harm unintentionally or otherwise (Haslop et al., 2021, p. 1420). Female and transgender individuals are more likely to face online harassment than men Haslop et al., 2021, p. 1413). Harassment towards feminists and female public figures often originates from the manosphere, an online network of pickup artists, men's rights activists, anti-feminists, and fringe groups (Marwick & Caplan, 2018). It is often coordinated and organized, rather than just individual actions (Marwick & Caplan, 2018). For example, female journalist Siobhan Fenton was abused online when she appeared in a video of The Independent on X, receiving hundreds of negative comments, and a blogger on Tumblr who was trolled by a male from the manosphere for sharing information about safe abortion.

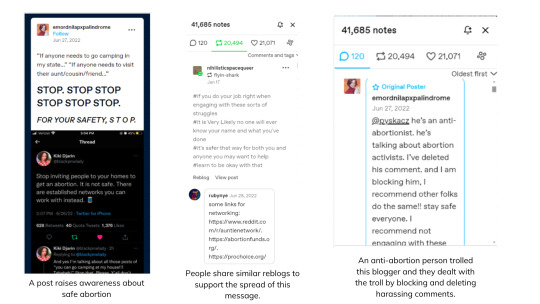
Figure 1. An anti-abortion comment from the manosphere aimed at a feminist female blogger.
Online harassment is pervasive in digital spaces, leading some young women to tolerate offensive and abusive communications (Smith, 2018). Young women perceive such communications to be relatively acceptable and the 'norm' (Haslop et al., 2021, p. 1413). They often use silencing strategies like blocking, reporting, and limiting participation, self-censorship as means of protection (Haslop et al., 2021, p. 1413). In the case of Siobhan Fenton, she silently suffered without reporting it to X because she knew this often happened to her colleagues and reporting was ineffective. Online harassment hinders women's online participation and citizenship, leading to gendered digital divides (Vitis & Gilmour, 2016, p. 337). It negatively impacts victims' motivation to use and engage with digitized spaces, leading to women excluding themselves from online spaces (Haslop et al., 2021, p. 1412).
Regarding digital citizenship, which allows internet users to participate without fear (Thompson, 2023), is threatened by online harassment (Vitis & Gilmour, 2016, p. 337). Online harassment also leads to offline violence and contributes to mental health issues, as it makes women feel unsafe in online spaces (Vitis & Gilmour, 2016, p. 337). Kelly Sue DeConnick, a comics writer, criticized sexism in the industry, highlighting the potential harm of online harassment on her family due to anxiety or fear of being blamed for speaking up (Amnesty International, 2018). Therefore, addressing online harassment is crucial for promoting digital citizenship and reducing gender disparities.

Figure 2. Kelly Sue DeConnick.
What can be done?
In Vietnam, the Law on Cyber Security provides protection against cyberbullying and harmful online content, with ministries responsible for ensuring online safety and removing inappropriate material (Vietnam Law and Legal Forum, 2023). Additionally, some women employ humor and social media platforms as a means of engaging, resisting, and responding to harassment (Vitis & Gilmour, 2016). Projects like Instagranniepants (Figure 3) and Gensler's critical witnessing utilize satire and shame, aiming to give harassers a taste of their own medicine through unflattering portraits (Vitis & Gilmour, 2016).

Figure 3. Instagranniepants project.
References
Amnesty International. (2018, March 20). Toxic Twitter - The Psychological Harms of Violence and Abuse Against Women Online. Amnesty International. https://www.amnesty.org/en/latest/news/2018/03/online-violence-against-women-chapter-6-6/
Haslop, C., O’Rourke, F., & Southern, R. (2021). #NoSnowflakes: The toleration of harassment and an emergent gender-related digital divide, in a UK student online culture. Convergence: The International Journal of Research into New Media Technologies, 27(5), 1418–1438. https://doi.org/10.1177/1354856521989270
Marwick, A. E., & Caplan, R. (2018). Drinking male tears: language, the manosphere, and networked harassment. Feminist Media Studies, 18(4), 543–559. https://doi.org/10.1080/14680777.2018.1450568
Thompson, J. D. (2023, March 17). New journalism research will help mitigate the harms of online hostility. Freilich Project for the Study of Bigotry. https://freilich.anu.edu.au/news-events/blog/new-journalism-research-will-help-mitigate-harms-online-hostility
Vietnam Law and Legal forum. (2023). Protection of women and juveniles from cyberspace violence in Vietnam today. Vietnamlawmagazine.vn. https://vietnamlawmagazine.vn/protection-of-women-and-juveniles-from-cyberspace-violence-in-vietnam-today-71137.html
Vitis, L., & Gilmour, F. (2016). Dick pics on blast: A woman’s resistance to online sexual harassment using humour, art and Instagram. Crime, Media, Culture: An International Journal, 13(3), 335–355. https://doi.org/10.1177/1741659016652445
#mda20009#online harassment#online abuse#protect women#Instagranniepants#manosphere#digital citizenship#safeonline
0 notes
Text
AstraZeneca under fire after LGBT+ staff group issue training saying 'sex is not binary'
British evolutionary biologist Richard Dawkins photographed at his home in Oxford
AstraZeneca under fire after LGBT+ staff group issue training saying ‘sex is not binary’
Documents claiming ‘biology has a spectrum’ are condemned by Lord Winston and Richard Dawkins as ‘scientifically ignorant’
Patrick Sawer,
SENIOR NEWS REPORTER and
Hayley Dixon,
SPECIAL CORRESPONDENT
1 March 2024 • 4:21pm
The material states that “biology has a spectrum” and that classifying a person’s sex as either male or female “fails to capture even the biological aspect of gender.”
It was distributed by managers and employees on AstraZeneca’s intranet system, as part of gender diversity awareness promotion by the company’s independent LGBT+ staff group.
The Telegraph understands that the training was sent by a manager to at least one employee who raised questions about the use of pronouns and the term “queer”.
One former employee told The Telegraph: “AstraZeneca has been the most extreme company I have worked at in terms of gender identity ideology.”
Lord Robert Winston and Richard Dawkins, two of the country’s most pre-eminent scientists, have criticised the material as “scientifically ignorant” and running counter to the basis of the pharmaceutical and biotechnology firm’s work.
AstraZeneca had denied the material is part of the company’s official training or that it represents the firm’s official policy on gender issues, stating that it was produced and distributed only by AZPride, the staff group for LGBT+ employees.
The biologist Richard Dawkins referred to the AstraZeneca material as a 'ridiculous document'
One of the most controversial documents, titled Sex Spectrum, states: “Many societies view a person’s sex as either male or female, but this binary view fails to capture even the biological aspect of gender.
“While we are often taught that we inherit either XX or XY sex chromosomes, in fact, biology has a spectrum too!”
It adds: “People might have XXY, XYY, X, XXX or other combinations of chromosomes – all of which can result in a variety of sex characteristics.”
That claim appears to contradict established biological science. Having XXY or XYY chromosomes can lead to rare genetic conditions for men, but does not alter a man’s biological sex, while triple X syndrome is a genetic condition found in females only.
Staff at AstraZeneca are encouraged by AZPride to state their pronouns in work-related correspondence and at work events in order to make everyone feel included.
But this is understood to have angered some employees on the basis that it assumes support for the belief that someone’s sex can change from the one they were born with.
Apparent support for chest binding
Another AZPride document appears to support the controversial practice of chest binding, used by biological girls or women who want to present as men.
During a health awareness week run by AZPride, in 2020, staff were given material that stated: “Chest binding can be a vital practice to improve self-esteem and body positivity for many LGBT+ people.
“The material used can sometimes place pressure on the airways and so amid growing concerns around Covid-19 some organisations have provided some tips to looking after your respiratory health for trans and non-binary people.”
Breast binding can restrict breathing, irritate the skin, cause overheating and even bruise or fracture ribs, and its use by children and young women whose bodies are still developing has raised concerns.
Much of the material distributed among AZ staff has been criticised as unscientific by scientists and critics of transgender theory.
Lord Robert Winston, known for his pioneering work in the study of fertility, said: “It’s very disappointing. This sort of material is confused and doesn’t take into account the difference between sex and gender.
“It’s completely unscientific.You inherit your X or Y chromosomes from the moment of conception. You can’t change your sex. Your sex is permanent genetically. They have confused sex with gender and sexuality.”
Richard Dawkins, the evolutionary biologist and award-winning author, said: “As a biologist, I shall comment only on the scientifically ignorant statement that ‘this binary view fails to capture even the biological aspect of gender’. The only definition of sex that works universally is based on gamete size. It’s the one used by biologists, and it leads to the conclusion that the male-female divide is purely binary. Males produce numerous small gametes, females fewer large ones. No other definition works coherently and universally.
“Even sticking to human sex chromosomes, the statement that there’s ‘a spectrum too’ misuses – abuses – the useful word ‘spectrum’. Those much-vaunted ‘intersexes’ are extremely rare. If we represent the number of unequivocal males and unequivocal females by the heights of New York’s twin towers, the number of intersexes would approximate the height of a molehill planted between them. Some spectrum!”
He added: “I don’t know who, in AstraZeneca, dreamed up this ridiculous document. Evidently not a scientist. Let’s hope that AstraZeneca’s research staff are better educated. And capable of at least a modicum of logical thought.”
An AstraZeneca spokesman said: “At AstraZeneca our aim is to cultivate inclusion and belonging by fostering an environment where everyone feels valued, heard and respected.”
AstraZeneca supposedly SCIENTIFIC BASED CORPORATION has been allowing an Aithoritative push of false Gender Ideology within their company.
"Astrazeneca is a British multinational pharmaceutical and biotechnology company with its headquarters at the Cambridge Biomedical Campus in Cambridge, England..."
#AstraZeneca supposedly SCIENTIFIC BASED CORPORATION has been allowing an Aithoritative push of false Gender Ideology within their company#AstraZeneca under fire after LGBT+ staff group issue training saying 'sex is not binary'#LGBTQ Cult#Astrazeneca Is Ayltinstiomal Company Founded In Sweden And Based In Britain At Cambridge#Shareholders Include Vanguard And Blackrock#Same Companies On Board Pf PepsiCo And Doritos#BOYCOTT PEPSICO#BOYCOTT ASTRAZENECA#Women's Rights
1 note
·
View note
Text
Breaking and botching the Brandon Teena Story: A Reflective Essay
BLOG #2
Hello, dear readers! My name is Ryza, and I am delighted to welcome you to this thought-provoking blog post titled “Breaking and Botching the Brandon Teena Story: A Reflective Essay.” As an eager writer and passionate advocate for social justice, I am thrilled to embark on this introspective journey with you.

INTRODUCTION
Throughout history, some tales have had the ability to upend social norms and biases and jolt us to our very core. One such tale that has permanently etched itself into our collective psyche is Brandon Teena’s. Examining the challenges faced by transgender people, the shortcomings of our judicial system, and the complexities of identity have been sparked by Brandon’s life and untimely end. “How I Broke, and Botched, the Brandon Teena Story,” by Donna Minkowitz, is a riveting account of her experience reporting on Brandon Teena’s terrible life and death. Minkowitz investigates the complicated intersections of culture, gender, sex, and law in her introspective work, eventually acknowledging her own inadequacies and the potential harm caused by her initial narrative framing. This analytical article digs into the different topics raised by Minkowitz, evaluating the consequences of her actions and the lessons acquired from her moving story.
CULTURE:
Culture has a significant impact on our views and biases. Minkowitz attributes her initial comprehension of Brandon Teena’s story to her own background and societal conditioning. She sought to write a fascinating story that would appeal with readers, but unwittingly allowed cultural conventions and stereotypes to poison her portrayal. This error exemplifies the tremendous impact that cultural preconceptions may have on storytelling, frequently perpetuating damaging myths and limiting our ability to comprehend the nuances of lived experiences.
GENDER:
The investigation of gender identity is one of Minkowitz’s key subjects. Brandon Teena’s struggle with gender dysphoria and the following abuse he endured highlights the cultural barriers that transgender people frequently confront. Minkowitz first presented the story via a cisgender lens, emphasizing the narrative of a “lesbian on the run,” undermining the significance of Brandon’s self-discovery journey and the nuances of his transgender identity. Minkowitz squandered an important opportunity to challenge cultural conventions and prejudices by failing to properly acknowledge and appreciate his gender identity.
SEX:
The narrative of Brandon Teena is intricately related to sexuality and sexual orientation. Minkowitz admits to her own uneasiness and misunderstanding of transgender people’s experiences, which results in an inaccurate portrayal of Brandon’s sexuality. She incorrectly depicted his connections with women as deceptive and manipulative, contributing to the damaging image of transgender people as deceptive or predatory. Minkowitz’s personal bias hampered her capacity to effectively comprehend and explain the intricacies of Brandon’s sexual orientation, ultimately contributing to his identity deception.
LAW:
The involvement of the law in the Brandon Teena case exemplifies the structural failings that sustain violence against underprivileged populations. Minkowitz comments on her own ignorance of the legal difficulties of hate crimes and transgender prejudice. Minkowitz squandered an opportunity to bring light on the broader societal issues of systemic violence and prejudice against transgender people by ignoring the significance of the legal setting. This failure weakened the case for legal reform and prolonged the cycle of injustice.
CONCLUSION
Donna Minkowitz’s reflective article serves as a reminder of the responsibility authors carry when recording marginalized people’s experiences. She investigates the problems in her first narrative framing of the Brandon Teena story through an examination of culture, gender, sex, and law. Minkowitz’s voyage of reflection serves as a cautionary tale, pushing writers to critically assess their biases, challenge cultural standards, and appreciate the complexities of life experiences. Minkowitz encourages us to approach storytelling with empathy, respect, and a commitment to elevating minority voices while avoiding damaging stereotypes and misrepresentations by learning from her mistakes.
Furthermore, this article serves as a call to remember Brandon Teena and the numerous others whose lives have been impacted by similar difficulties. We can contribute to a more empathetic and nuanced understanding of transgender realities by analyzing earlier portrayals. Through empathy and open discourse, we can work to create a society that values variety, promotes inclusion, and upholds the dignity of all people.
Thank you for joining me on this contemplative trip as we unravel the many layers of Brandon Teena’s tale. Let us challenge ourselves together to tackle biases, challenge preconceived assumptions, and cultivate a more sympathetic and just society. I am happy to share my thoughts with you, and I hope that this essay generates meaningful dialogues and promotes constructive change.
(DISCLAIMER: The image above is not mine, credits to the owner)
1 note
·
View note
Text
By: Lucy Bannerman, James Beal, Eleanor Hayward
Published: Apr 10, 2024
The report should be the final nail in the coffin of Gids, the clinic that told thousands of children they were transgender
In 2009 the NHS’s gender identity development service (Gids) saw fewer than 50 children a year. Since then demand has increased a hundredfold, with more than 5,000 seeking help in 2021-22.
The sudden increase has gone hand in hand with the adoption of a model of “gender-affirming” care, which puts children on a life-altering path of hormone treatment. Services have been left overwhelmed, with vulnerable young people clamouring for medical interventions to help them change gender — despite a lack of evidence over the long-term effects.
It was against this backdrop that Dr Hilary Cass was commissioned in 2020 to examine the state of NHS services for children identifying as trans. Her final report, published on Wednesday, delivers a damning verdict on the medical path thousands of children have been sent down. It marks a turning point in years of bitter debate over how to help this distressed group of young people, confirming a shift towards a holistic model that takes into account the wider social and mental health problems driving the rise in demand.
Gen Z and online porn
The Cass report shines a light on the biggest unanswered question over transgender healthcare: why are so many Gen Z women suddenly wanting to change gender?
Cass paints an alarming picture of an anxious and distressed generation of digitally savvy young women and girls, who not only are more exposed to online pornography and the wider problems of the world than any previous generation but also consume more social media and have lower self-esteem and more body hang-ups than their male peers.
When Gids opened in 1989, it treated fewer than ten people each year, mostly males with a long history of gender distress. In 2009 it treated 15 adolescent girls. By 2016 that figure had shot up to 1,071.
Cass concludes that such a sudden rise in such a short time cannot be explained alone by greater acceptance of trans identities, which “does not adequately explain” the switch in patient profiles from predominantly male to female. She also says greater investigation of the “consumption of online pornography and gender dysphoria is needed”, pointing to youngsters’ increasingly early exposure to “frequently violent” online material that can have a harmful impact on their self- esteem and body image.
Gen Z is defined as those born between 1995 and 2009. Rather than focusing on the issue of gender in isolation, Cass looked at the context in which adolescents today, who have “grown up with unprecedented online access”, are experiencing such a disproportionate crisis over their gender.
“Generation Z is the generation in which the numbers seeking support from the NHS around their gender identity have increased, so it is important to have some understanding of their experiences and influences,” she writes. “In terms of broader context, Generation Z and Generation Alpha (those born since 2010) have grown up through a global recession, concerns about climate change and most recently the Covid-19 pandemic. Global connectivity has meant that as well as the advantages of international peer networks, they are much more exposed to worries about global threats.”
The report also focuses on 2014, when female referrals to Gids accelerated. Although this is not mentioned, 2014 was the year that CBBC, for example, broadcast I Am Leo, a video-diary-style documentary, to an audience of to 6 to 12-year-olds, showing the positive personal journey of a child who transitioned from female to male.
Throughout almost 400 pages, Cass argues that the gender-related issues of young patients should be treated in the same context as the wider mental health issues facing their entire generation. “The striking increase in young people presenting with gender incongruence/dysphoria needs to be considered within the context of poor mental health and emotional distress among the broader adolescent population, particularly given their high rates of co-existing mental health problems and neurodiversity.” Cass calls for more research into the “complex interplay” between these issues and a teenager’s sudden desire to change gender.
Lack of evidence for medical pathway
Rather than affirming children’s gender identity with medical treatment, the report calls for a holistic approach that examines the causes of their distress. It finds that, despite being incorporated into medical guidelines around the world, the use of “gender-affirming” medical treatment such as puberty blockers is based on “wholly inadequate” evidence. Doctors are cautious when adopting new treatments, but Cass says “quite the reverse happened in the field of gender care for children”, with thousands of children put on an unproven medical pathway.
Cass says gender care is “an area of remarkably weak evidence” and that results of studies “are exaggerated or misrepresented by people on all sides of the debate”. She adds: “The reality is that we have no good evidence on the long-term outcomes of interventions to manage gender-related distress.”
The report finds that treatment on the NHS since 2011 has largely been informed by two sets of international guidelines, drawn up by the Endocrine Society and the World Professional Association of Transgender Healthcare (WPATH), but that these lack scientific rigour. The WPATH has been “highly influential in directing international practice, although its guidelines were found by the University of York’s appraisal to lack developmental rigour and transparency”, Cass says.
The report says the NHS must work to improve the evidence base.
Mental health
Mental health issues could be presenting as gender-related distress. Children and young people referred to specialist gender services have higher rates of mental health difficulties than the general population. This includes rates of depression, anxiety and eating disorders. Some research studies have suggested transgender people are three to six times more likely to be autistic than the general population, with age and educational attainment taken into account.
Therefore, the report says that the striking increase in young people presenting with gender dysphoria needs to be considered within the context of rising levels of poor mental health.
The increase in gender clinic patients “has to some degree paralleled” the deterioration in child and adolescent mental health, it finds. Mental distress, the report says, can present through physical manifestations, such as eating disorders or body dysmorphic disorders. Clinicians were often reluctant to explore or address co-occurring mental health issues in those presenting with gender distress, the report finds. This was because gender dysphoria was not considered to be a mental health condition.
The report finds that, compared with the general population, young people referred to gender services had higher rates of neglect; physical, sexual or emotional abuse; parental mental illness or substance abuse; exposure to domestic violence; and loss of a parent through death or abandonment.
Puberty blockers
The report says there was “no evidence” puberty blockers allowed young people “time to think” by delaying the onset of puberty — which was the original rationale for their use. It finds the vast majority of those who start puberty suppression continued on to cross-sex hormones, particularly if they started earlier in puberty.
There was insufficient and inconsistent evidence about the effects of puberty suppression on psychological or psychosocial health, it says, and some young females had a worsening of problems like depression and anxiety.
Cass says there is “some concern” that puberty blockers may actually change “the trajectory of psychosexual and gender identity development”.
Her report warns that blocking the chronological age and sex hormones released during puberty “could have a range of unintended and as yet unidentified consequences”.
It describes adolescence as a time of “identity development, sexual development, sexual fluidity and experimentation”. The report says “blocking” this meant young people had to understand identity and sexuality based only on their discomfort about puberty and an early sense of their gender. Therefore, it adds, there is “no way of knowing” whether the normal trajectory of someone’s sexual and gender identity “may be permanently altered”.
Brain maturation may also be “temporarily or permanently disrupted” by the use of puberty blockers, it says. This could have a significant impact on a young person’s ability to make “complex risk-laden decisions”, as well as possible long-term neuropsychological consequences.
The report highlights the “concern” of young people remaining on puberty blockers into adulthood — sometimes into their mid-twenties. This is partly because some “wish to continue as non-binary” and partly because of ongoing gender indecision, the report says.
Cass adds: “Puberty suppression was never intended to continue for extended periods.”
The report finds young adults who had been discharged from Gids “remained on puberty blockers into their early to mid twenties”. A review of audit data suggested 177 patients were discharged while on puberty blockers.

Cass says the review “raised this with NHS England and Gids”, citing the unknown impact of use over an extended period. “The detrimental impact to bone density alone makes this concerning”, the report adds.
A Dutch study originally suggested that puberty blockers might improve psychological wellbeing for a narrow group of children with gender issues.
Following this, the practice “spread at pace to other countries” and in 2011 the UK trialled the use of puberty blockers in an early intervention study.
The results were not formally published until 2020, at which time it showed there was a lack of any positive measurable outcomes. It also found that 98 per cent of people had proceeded to take cross-sex hormones.
Despite this, from 2014 puberty blockers moved from a research-only protocol to being available in routine clinical practice. “The rationale for this is unclear,” the report says.
Puberty blockers were then given to a wider range of adolescents, it says, including patients with no history of gender issues before puberty and those with neurodiversity and complex mental health issues. Clinical practice, Cass found, appeared to have “deviated” from the parameters originally set.
Overall, the report concludes there was a “very narrow indication” for the use of puberty blockers in males to stop irreversible pubertal changes, while other benefits remained unproven.
It says there were “clearly lessons to be learnt by everyone”.
Social transition
The report concludes it was “possible” that social transition, including the changing of a child’s name and pronouns, may change the trajectory of their gender development. It finds “no clear evidence” social transitioning in childhood has any positive or negative mental health effects, but that children who socially transitioned at an earlier age were more likely to proceed to medical treatment. A more cautious approach to social transition needs to be taken for children than for adolescents, it concludes.
The review also heard concerns from “many parents” about their child being socially transitioned and affirmed in their expressed gender without their involvement. Draft government guidance, published in December, stated that schools should not accept all requests for social transition and should involve parents in any decision that is made.
Despite this, there has been evidence of schools ignoring ministers and allowing children to change gender behind their parents’ backs.
The report makes clear that “parents should be actively involved in decision making” unless there are strong grounds to believe that it may put the child at risk.
It also finds that social debates on trans issues led to fear among doctors and parents, with some concerned about being accused of transphobia.
The interim report, from 2022, had classed social transition as “not a neutral act”. The full report explains that it is an “active intervention”, because it may have significant effects on a young person’s psychological functioning and longer-term outcomes.
In a strong warning to schools, the report describes the need for “clinical involvement” in the decision-making process on social transitioning. It adds: “This is not a role that can be taken by staff without appropriate clinical training.”
The report concludes that maintaining flexibility is key among those going down a social transition route and says a “partial transition”, rather than a full one, could help.
In decisions about whether to transition prepubescent children, families should be seen “as early as possible by a clinical professional”.
Rogue private clinics
Long waiting lists for NHS care mean distressed children are turning to private clinics or resorting to “obtaining unregulated and potentially dangerous hormone supplies over the internet”, the report says.
Some NHS GPs have then felt “pressurised to prescribe hormones after these have been initiated by private providers”, and Cass says this should not happen.
The report also urges the Department of Health to consider new legislation to “prevent inappropriate overseas prescribing”. This is intended to tackle a loophole which means that, despite the NHS banning the use of puberty blockers last month, children can still access them from online clinics such as GenderGP, which is registered in Singapore.
Detransitioning
Cass says some of those who have been through medical transitions “deeply regret their earlier decisions”. Her report says the NHS should consider a new specialist service for people who wish to “detransition” and come off hormone treatments. She says people who are detransitioning may be reluctant to return to the service they had previously used.
NHS numbers
The report recommends that the NHS and Department of Health review current practice of issuing new NHS numbers to people who change gender.
Cass suggests that handing out new NHS numbers to trans people means they risk getting lost in the system — making it harder to track their health histories and long-term outcomes.
The review says that this has had “implications for safeguarding and clinical management of these children”, — for example, the type of screening that they are offered.
Toxic debate
Cass has called for an end to the “exceptionally toxic” debates over transgender healthcare after she was vilified online while compiling her review. In a foreword to her 388-page report, the paediatrician said that navigating a culture war over trans rights has made her task over the past four years significantly harder.
She warned that the “stormy social discourse” does little to help young people, who are being let down by a lack of research and evidence. Cass added: “There are few other areas of healthcare where professionals are so afraid to openly discuss their views, where people are vilified on social media, and where name-calling echoes the worst bullying behaviour. This must stop.
“Polarisation and stifling of debate do nothing to help the young people caught in the middle of a stormy social discourse, and in the long run will also hamper the research that is essential to finding the best way of supporting them to thrive.”
Cass said: “Finally, I am aware that this report will generate much discussion and that strongly held views will be expressed. While open and constructive debate is needed, I would urge everybody to remember the children and young people trying to live their lives and the families/ carers and clinicians doing their best to support them. All should be treated with compassion and respect.”
The recommendations
Data collection
Gender identity clinics should offer their data to NHS England for review, and more research should be conducted on the impact of psychosocial intervention — such as therapy — and the use of masculinising and feminising hormones, such as testosterone and oestrogen. Cass recommended that the NHS should also consider data from private clinics.
Puberty blockers and hormone treatment
Cass recommended research to establish the long-term impact of puberty blockers, which is expected to start by December.
Assessment of other conditions
Cass said that children arriving at gender identity services should be screened for conditions such as autism and other neurodevelopmental conditions.
Criteria for medical treatment
When treating children with gender dysphoria, only those who have experienced “longstanding gender incongruence” will be able to get medical treatment. Even then, this will only be available — with “extreme caution” — for over 16s.
A holistic approach
Before any medical intervention, Cass recommends that children should be offered fertility counselling and “preservation” by specialist services. This formed part of a more “holistic” approach to gender identity services. Cass suggested the creation and implementation of a national framework and infrastructure for gender-related care.
Growing into adulthood
The review advised that follow-through services for 17 to 25-year-olds should be established to ensure a continuity of care and support when children grow into adulthood.
Detransitioners
The report proposed that NHS England should “ensure there is provision for people considering detransition”, while recognising that they may not wish to attend services that assisted in their initial gender transition.
[ Via: https://archive.today/7GxDe ]
#Hilary Cass#Dr. Hilary Cass#Cass report#Cass review#medical corruption#medical scandal#medical malpractice#gender thalidomide#gender lobotomy#ideological capture#ideological corruption#gender affirming care#gender affirming healthcare#gender affirmation#queer theory#gender identity ideology#intersectional feminism#gender ideology#detrans#detransition#puberty blockers#wrong sex hormones#cross sex hormones#religion is a mental illness
12 notes
·
View notes
Note
@guardianssystem I am so disappointed to see you over here from Twitter, you are literally the most manipulative person that has ever existed when it comes to information about DID/OSDD, and I'm ready to start debunking you, you POS
Ready? Let's go.
1. The DSM 5 TR fully states that DID is a trauma based disorder, and so does every doctor that has ever doctored. Sorry you can't read for shit. Inb4 "but PTSD says--" no. That's not how that works. The secret to DID not being trauma based is not hidden under the PTSD entry, that's ridiculous and a blatant misreading of the DSM. If that's what we're doing, the differentials on DPDR prove DID is trauma based. The PTSD differentials only say that point of trauma does not need to be immediately, or even closely preceding the onset of disorder in DID. It's about how difficult it can be to trace a trauma event to DID. It means someone's life doesn't need to be in current turmoil to show symptoms or qualify for a diagnosis.

That is 100% of cases. There is no 10% not caused by trauma. Read this, please.
The fact is, the research proving that DID is trauma related is only growing by the day. Arguing with this only hurts all systems.
Also see this post about the ICD 11 boundary with normality.
2. Transgender Mental Health was not written or published by the APA. The book was written by Dr Eric and published through the APAP, a publishing company that publishes most of the work the APA does. This does not mean that his work is supported by the APA, or that he had to go through it, and as such, his book opens with a caution that everything in it is his own opinion and work and not that of the greater medical community. This is a doctor that specializes in transgender mental health, not systems and DDs or plurality. While there is a large intersection in these two communities, he does NOT make any sweeping statements about plurality and offers no research or proof into the phenomena other than self reports, which is fine. His book is actually really good. But this is not what it should be used for. It's not the golden gun of proof like people are holding it up to be-- like you are. Unfortunately, I worry about his research because it seems to have pushed us back in the direction of multiple personalities = transgender, with new research surfacing about dissociation and gender incongruence. I'm not saying this is what's happening, but I would be cautious in optimism about this topic until more comes out and plurality is better acknowledged. Point is, claiming it's published by the APA is a huge misrepresentation of the truth.

2.5. One of the writers of the ToSD lost his license for abusing a patient with DID, please don't refer to them as plural. Beyond that, there were still two other authors, and the ToSD is based on a body of research that spans over a century. It wasn't their idea or concept, trauma related structural dissociation has been around since Janet in the 1800s. They took all the info and put it into a book, the haunted self, which is has become synonymous with ToSD. The theory is still good. Also, don't fucking link did research for this shit, that's nothing, literally nothing. As well, you're clearly behind the times, because the ToSD has been updated since, expanding on the types of parts and different disorders to clear up many of those issues. And, to top it off, we can see the ToSD in action on brain scans. Point is, one man does not make all of this research bad. Stop using it as a gotcha, we can talk about abuse in psychiatry without putting down valuable research.
It can be proven and tested for, and has been, repeatedly, for years.
3. Nothing to add
Second post
THAT'S NOT WHAT THE TOSD SAYS, LMAO, WHERE ARE YOU GETTING THAT FROM
HOLY fuck
These claims are getting more and more wild, it's no wonder all you people are talking pure shit.
One of the other authors doesn't support endogenic plurality, that's a blatant and ridiculous misreading of his work. It's such a huge misrepresentation of what's being said, how do you people sleep at night?
The entire point of the paper you're referencing here is about how to define dissociation and the different types, including that seen in channeling and mediumship, which, according to the authors, shouldn't be included and is highly disputed.
"However, what has remained missing is a precise definition of dissociation in trauma. This article first presents such a definition and elucidates its various components. Next the new definition is compared with several other major definitions of the concept. The strengths of the new formulation are highlighted and discussed."
...
"However, dissociation in mediums is in several regards different from dissociation in DID (CitationMoreira-Almeida, Neto, & Cardeña, 2008). The possible involvement of consciousness and self-consciousness in dissociated controls in hypnosis and in dissociative parts in mediumship needs to be examined in more detail before a conclusive general definition of dissociation can be formulated."
This is about developing a definition of trauma related dissociation, and you're using it as proof that it's the same as... mediumship. Nice. How very... uneducated of you to present this.
But I'm not really surprised, considering some of your other links.
Critiquing the Requirement of Oneness over Multiplicity: An Examination of Dissociative Identity (Disorder) in Five Clinical Texts - I spoke with the author of this paper and she does not support endogenic systems. Her paper was one of the very first to look at functional multiplicity as a treatment option for DID and she's upset that it's being used this way. It's a very important paper for DID history, and you're shitting on it. Ross' quote from this paper is actually usually altered when it's included. Ross said: "Those without an abuse history," not trauma history. Ross' paper was the first to recognize that not only abuse caused DID. Way to twist that, too.
NORMAL DIMENSIONS OF MULTIPLE PERSONALITY WITHOUT AMNESIA - is about how DID is fake and fantasy play. This shows you're not actually reading the things you're including. Good job.
Multiplicity: An Explorative Interview Study on Personal Experiences of People with Multiple Selves - not a study, it's an interview. Misrepresentation. Again.
Like, what are you doing, you don't need to do this to prove endogenic plurality. You are doing more harm than good with this shit.
Edit: thanks for the tag reminding me, since OPs post was already corrected, I'm not touching that, good on OP for the apology and willingness to learn, I hope everyone else can be that open
did and osdd are not the only ways a system can form. they can also form from neurodivergence or stress. heres a google doc with endogenic resources https://docs.google.com/document/d/1_5iSiTjqlyCjd3krzQwjAMbZOQzKKpbcmRI0NsHfPpA/edit?usp=drivesdk

1). Removing the emphasis of trauma on a disorder cause by trauma is incredibly dangerous.
2). A quick google search told me that Dr. Eric Yarbrough specializes in LGBTQ+ medicine and is a trans med (believes gender dysphoria is a mental illness and is necessary to be trans) and does not specialize in any form of dissociative disorders or treatment.
3). Tulpas are not, and will not ever, be a form of DIDOSDD, they are a cultural soul bond and are extremely sacred to Native American cultures.
4). Cope harder??
70 notes
·
View notes
Photo




For Transgender Day of Remembrance, here’s 10 graphic novels with transgender protagonists, are about gender, or are autobiographies from transgender creators.
Cheer Up: Love and Pompoms by Crystal Frasier & Val Wise
Annie is a smart, antisocial lesbian starting her senior year of high school who’s under pressure to join the cheerleader squad to make friends and round out her college applications. Her former friend BeeBee is a people-pleaser—a trans girl who must keep her parents happy with her grades and social life to keep their support of her transition. Through the rigors of squad training and amped up social pressures (not to mention micro aggressions and other queer youth problems), the two girls rekindle a friendship they thought they’d lost and discover there may be other, sweeter feelings springing up between them.
Blackwater by Jeannette Arroyo & Ren Graham
Tony Price is a popular high school track star and occasional delinquent aching for his dad’s attention and approval. Eli Hirsch is a quiet boy with a chronic autoimmune disorder that has ravaged his health and social life. What happens when these two become unlikely friends (and a whole lot more . . .) in the spooky town of Blackwater, Maine? Werewolf curses, unsavory interactions with the quarterback of the football team, a ghostly fisherman haunting the harbor, and tons of high school drama.
The Bride Was a Boy by Chii
The heartwarming transgender love story, based on true events! Drawn in the style of diary comics with an upbeat, adorable flair, this is a charming tale about Chii, a woman assigned male at birth. Her story starts with her childhood and follows the ups and downs of exploring her sexuality, gender, and transition--as well as falling in love with a man who’s head over heels for her. Now they want to get married, so Chii’s about to embark on a new adventure: becoming a bride!
Love Me for Who I Am by Kata Konayama
Non-Binary Maid Reporting for Duty! Mogumo is a cute but lonely non-binary high school student who just wants a few loving friends. As someone who doesn’t identify as a boy or a girl, however, finding people who really understand can be a big challenge. When fellow student Iwaoka Tetsu invites Mogumo to work at an untraditional maid café, Mogumo is hopeful that things are looking up. Will they finally find friends to call their own―or just more misunderstanding?
Super Late Bloomer: My Early Days in Transition by Julia Kaye
A highly personal collection documenting the early months of artist Julia Kaye’s gender transition. Instead of a traditional written diary, Julia Kaye has always turned to art as a means of self-reflection. So when she began her gender transition in 2016, she decided to use her popular webcomic, Up and Out, to process her journey and help others with similar struggles realize they weren’t alone. Julia’s poignant, relatable comics honestly depict her personal ups and downs while dealing with the various issues involved in transitioning—from struggling with self-acceptance and challenging societal expectations, to moments of self-love and joy. Super Late Bloomer both educates and inspires, as Julia faces her difficulties head-on and commits to being wholly, authentically who she was always meant to be
Magical Boy by The Kao
A breathtakingly imaginative fantasy series starring Max—a high schooler chosen to become the next "Magical Girl." There's just one catch . . . he's a trans boy! Although he was assigned female at birth, Max is your average trans man trying to get through high school as himself. But on top of classes, crushes, and coming out, Max's life is turned upside down when his mom reveals an eons old family secret: he's descended from a long line of Magical Girls tasked with defending humanity from a dark, ancient evil! With a sassy feline sidekick and loyal gang of friends by his side, can Max take on his destiny, save the world, and become the next Magical Boy? A hilarious and heartfelt riff on the magical girl genre made popular by teen manga series, Magical Boy is a one-of-a-kind fantasy series that comic readers of all ages will love.
Welcome to St. Hell: My Trans Teen Misadventure by Lewis Hancox
A groundbreaking memoir about being a trans teen, in the vein of FUN HOME and FLAMER... and at the same time entirely its own. Lewis has a few things to say to his younger teen self. He knows she hates her body. He knows she's confused about who to snog. He knows she's really a he and will ultimately realize this... but she's going to go through a whole lot of mess (some of it funny, some of it not funny at all) to get to that point. Lewis is trying to tell her this... but she's refusing to listen.
X-Gender, Vol. 1 by Asuka Miyazaki
An autobiographical diary/essay manga about finding love in Japan as an X-gender person. At 33 years old, Asuka Miyazaki realizes that they like women! Asuka, however, is neither a woman nor a man--instead, they're X-gender, which is a non-binary identity. Follow Asuka through the pages of this autobiographical manga as they record the ins and outs of their journey to finding love with a woman.
Girl Haven by Lilah Sturges & Meaghan Carter Three years ago, Ash's mom, Kristin, left home and never came back. Now, Ash lives in the house where Kristin grew up. All of her things are there. Her old room, her old clothes, and the shed, where she spent her childhood creating a fantasy world called Koretris. Ash knows all about Koretris: how it's a haven for girls, with no men or boys allowed, and filled with fanciful landscapes and creatures. When Ash's friends decide to try going to Koretris, using one of Kristin's spellbooks, Ash doesn't think anything will happen. But the spell works, and Ash discovers that the world Kristin created is actually a real place, with real inhabitants and very real danger. But if Koretris is real, why is Ash there? Everyone has always called Ash a boy. Ash uses he/him pronouns. Shouldn't the spell have kept Ash out? And what does it mean if it let Ash in?
DeadEndia: The Watcher's Test by Hamish Steel
Barney and his best friend Norma are just trying to get by and keep their jobs, but working at the Dead End theme park also means battling demonic forces, time traveling wizards, and scariest of all--their love lives! Follow the lives of this diverse group of employees of a haunted house, which may or may not also serve as a portal to hell, in this hilarious and moving graphic novel, complete with talking pugs, vengeful ghosts and LBGTQIA love!
#book recs#transgender day of remember#transgender#comic#graphic novel#nonbinary#gender#sports#horror#autobiography#fantasy#magical girl (boy)
518 notes
·
View notes
Note
can you do a debunk on these sources? https://at.tumblr.com/debunkingsystemscringe/mind-if-i-can-get-some-pro-endo-research-from-you/yihxbmcgdly4
I've already debunked all of these, but sure, I can do it again, let's see if @debunkingsystemscringe will actually respond this time
So, the carrd
The card is extremely bad, it's misquoting an incredibly important paper by Ross. His was the first to acknowledge that not just abuse caused DID, but trauma. I hate seeing this one used by endos because it was a MASSIVE step for DID systems, and it's being misused and misquoted here.
"These individuals often did not report abuse history and often reported experiencing little psychopathology."
This was one of the first papers to look at functional multiplicity as a treatment path and "smaller" trauma as a cause. It's not meant for endogenics.
"About 2% of people may be natural multiples who do not have dysfunctional posttraumatic MPD. They may simply have a highly dissociative psychic organization’ (Ross, 1991, p. 510)."
This was a theory that was debunked with the idea of trauma as a cause, and "highly dissociative psychic organization" doesn't mean "alters". I don't even think that's the correct quote, which is hilarious.
What's funny here, is that they're not actually quoting Ross, because his paper doesn't say that shit. They're quoting a college dissertation by McClure, quoting Ross, because you have to double twist it in order to make it work.
McClure's paper also doesn't imply anything about endogenic systems. Here's my debunk on her and Ross.
Next: Transgender Mental Health
I've talked about this one before, and how it's being touted as more important than it is. It's actually a really good book! I support this book and the stuff in it. But a lot of people are blowing it way out of proportion.
First, it has one chapter on "plurals" and how to treat them for gender related issues. Cool. That's true, it happened. I support the book.
However, it's not supported or endorsed by the APA, it wasn't published by them -- it's an independent book and everything in it is the opinion of the author. Same with the next paper by Isler. Like, it's useless, it means nothing. It doesn't talk about how or why, it says, "these people say they exist and it's going to make treatment harder because of the intricacies." That's it. Still a good book, check it out.
Next: Tulpas and Mental Health (it’s a PDF, be careful opening on phones)
I’m trying to find my full debunk on this. Jacob Isler is a practicing tulpamancer and has done some REALLY shady stuff-- Reddit has basically turned on him and disowned him and all of his work. As soon as I find the sources, I’ll add. Just give me a bit.
Alright, we’re going to have to redo it, here we do.
Jacob Isler has a severe nonresponse bias. Survey sent to 365 people and only 68 got back? That’s too small. Negligible read. The entire paper is about how tulpamancers are mentally ill in other ways, and that creating a tulpa has a positive impact on their mental health. Fine and dandy. It discusses how those mental health issues might play a huge role in the tulpamancy phenomon, but purposefully tries to twist the connection between the two to be unrelated on a pathological level. It also states: “Additionally, self-reported data gathered through online surveys, regardless of the care taken to ensure objectivity and accuracy, is bound to be influenced by biases and misconceptions. And, of course, the observational nature of this study means that causality cannot be proven. The intent of this paper is not to provide definitive assertions on the psychology of tulpamancy. Rather, the purpose is to accentuate outstanding associations and suggest further research into them.“
It’s basically admitting it’s own failure as an unreliable paper and simply calls for more research.
As for reddit disowning Isler: Isler is Fordaplot. Here’s the ban note from the mods

Next: Multiplicity: An Explorative Interview
We all know how much I love this useless article. Here’s my debunk. It’s based on 6 people only, admits it’s limited by not being able to verify their claims of functionality to make the point of the article, and then goes on to claim that online spaces for multiples are harmful, doesn’t discuss how and why, and only discusses the fact that they claim to exist and calls for more research, so. Kind of useless.
As for the cultural exclusion in the DSM and ICD, it’s specifically in regards to religious practices in cultures that someone has been raised in. As per the DSM, the difference between DID and these forms of “non-pathological possession trances” is that the non-pathological possession is short-term and occurs in specific cultural and religious ceremonies-- which is the opposite of what endogenics are experiencing (long-term, occurring continuously and not only in ceremonies (which they are not participating in to begin with)). It’s not excluding these experiences because they’re “endogenic”, it’s excluding them because it’s not plurality as we (endos and DID systems) describe it. Claiming that exception is for endogenics is hugely disrespectful to the clinicians and researchers who put an absurd amount of work into keeping religious experiences out of the DSM.
It’s just not for you.
22 notes
·
View notes