#genesis neurogen
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs




Fun Fact
There were a total of 171.5 billion posts on Tumblr in 2019.
Text
Who is the Best Gynecologist in Delhi and Gurgaon - Dr. Radha Jain
When it comes to women's health, having a caring and skilled gynecologist is super important. Dr. Radha Jain is one of the Best Gynecologist in East Delhi , and Gurgaon working at Genesis Neurogen. She's known for her dedication to providing great care and making sure her patients feel supported.
Dr. Radha Jain's Background:
Dr. Radha Jain MBBS, DGO is the Senior Consultant Gynecologist & Obstetrician in Delhi provides a great deal of women's health care treatments.
But, locating, coordinating and placing trust in any healthcare professional especially a gynecologist in our town may appear difficult eventually, but when one goes through the set of outstanding achievements and encouraging patients’ reviews and accolades, our doubt s bound to dispel. The fact holds truth for Dr. Radhika Jain, Best Gynecologist In East Delhi serving Delhiites since 2002 while running Genesis Neurogen, a healthcare point enjoying wider popularity across East Delhi

Complete Women's Health Services:
At Genesis Neurogen, Dr. Radha Jain offers lots of different services for women. From regular check-ups to handling more complicated health issues, she wants to make sure each patient gets the care they need.
Before and After Pregnancy Care: Dr. Radha Jain is really good at helping soon-to-be moms. She guides them through each step of pregnancy, making sure everything is going well. After the baby is born, she keeps taking care of both mom and baby.
Gynecological Surgeries: Dr. Radha Jain is skilled at doing different kinds of surgeries to help with women's health. Whether it's a small surgery or a bigger one, she makes sure it's done well and keeps her patients safe.
Handling Reproductive Health Issues: Dr. Radha Jain knows a lot about fixing problems with women's reproductive health. This includes issues with periods, hormones, and even helping with getting pregnant. She works with each person to find the best way to help.
Teen Girl Health: Dr. Radha Jain understands that teenage girls have their own special needs. She helps them with care that's right for their age, making sure they feel comfortable talking about anything that's bothering them.
Putting Patients First:
What makes Dr. Radha Jain really stand out is how much she cares about her patients. She believes in making a strong connection with each person, so they feel comfortable talking to her. Being kind and understanding, she creates a safe space for women during their health journey.
Conclusion:
Dr. Radha Jain is one of the Best Gynecologists in East Delhi at Genesis Neurogen because she cares so much about women's health. She offers many services, always does her best, and puts her patients first. If you're looking for a gynecologist who's both skilled and caring, Dr. Radha Jain is the right choice for your health journey.
Call - 011-22378802, 7481909090
Reference - https://qr.ae/pKmRqQ
#best gynecologist in east delhi#dr radha jain#audiologist in east delhi#child specialist in east delhi#genesis neurogen
0 notes
Text
Genesis Neurogen Clinic Krishna Nagar in East Delhi - 7504001122

Genesis Neurogen is one of the top mother and child care centre in Krishna Nagar East Delhi. We offer a wide range of medical services, including pediatric specialist care, gynecology & obstetrics, clinical psychology, speech therapy, special education, occupational therapy, neurofeedback therapy, physiotherapy, nutrition counseling, dental treatments, and kids gym. Get all everything under one roof.
#Best child development centre in Krishna Nagar East Delhi#Best Mother and child care centre in Krishna Nagar East Delhi#Genesis Neurogen Centre
1 note
·
View note
Text

Best stammering treatment center Delhi and Noida By Dr Murli Singh PhD chief speech therapist at Genesis -Neurogen Neuro Rehabilitation centre Rishabh vihar opposite cross River Mall Delhi India contact number 9891242568, 9625554548
www.speechtherapistdelhi.com
#delayed speech#diphysia#hard of hearing#hearing aids#speech therapy#stammering#adhd#brain stroke treatment#hearing test#autism spectrum disorder
0 notes
Text
Behavioural Modification Centre
Are you looking for a Behavioral Modification Center in Delhi? Look no further than Dr. Charu Arora. At Genesis Neurogen, Dr. Arora and her experienced team provide expert behavioral therapy to help individuals overcome challenges and achieve positive change. Our personalized approach ensures that each individual's unique needs are met with care and precision. Experience a supportive environment where growth and improvement are the focus.

Click here for more info - Behavioural Modification Centre
0 notes
Text
Occupational Therapy Centre in Shahdara
Are you looking for an Occupational Therapy center in Shahdara? Look no further than Genesis Neurogen! Our dedicated team offers personalized therapy to help you or your loved ones gain independence and improve daily living skills. With our expert care and modern facilities, we support a wide range of needs and age groups. At Genesis Neurogen, your progress is our priority

Click here for more info - Occupational Therapy Centre in Shahdara
0 notes
Text
Best Gynecologist In East Delhi

Are you want to book online appointment with gynecologist in East Delhi? Then contact Dr. Radha Jain, who is available at Genesis Neurogen Krishna Nagar. She is Senior Consultant Gynecologist & Obstetrician.
Contact For More Information: 011-22001122, 7504001122
0 notes
Text
Open Access Journals on Surgery - BJSTR Journal

Anti-Epileptic Drugs, Would They be the Cause of Heterotopic Ossification by Saloua Khalfaoui in Biomedical Journal of Scientific & Technical Research https://biomedres.us/fulltexts/BJSTR.MS.ID.002040.php?ts=1612498665#/ Etiopathogenesis of Heterotopic ossification or paraosteoarthropathy is unknown, all speculations remain open. Epilepsy and anti-epileptic drugs have never been mentioned as a risk factor. We report the case of an epileptic patient operated several times for fracture of the right humeral head. He was treated by anti-epileptic (Valproic Acid). He developed a stiffness of the right shoulder. Imaging showed a heterotopic ossification. Through this observation, we have tried to answer the question of the origin of the appearance of the heterotopic ossification; this genesis is multifactorial with a role of the anti-epileptic whose Valproic Acid. Heterotopic ossification (HO) or paraosteoarthropathy is called neurogenic when it occurs as a result of central or peripheral nervous system involvement. A HO may also occur in a context of bone trauma or burns or in an orthopedic context [1]. Epilepsy and anti-epileptic drugs (AEDs) have never been mentioned as a risk factor.Case Description Fore more articles on Open Access Journals on Surgery please click here bjstr Follow on Twitter : https://twitter.com/Biomedres01 Follow on Blogger : https://biomedres01.blogspot.com/ Like Our Pins On : https://www.pinterest.com/biomedres/
#Journals on Biomedical Engineering#Journals on Biomedical Science#Journals on Medical Informatics#Journals on Biomedical Imaging#Journals on Medical Microbiology
0 notes
Text
Juniper Publishers- Open Access Journal of Case Studies
Serum Leukocytes in Patients with Keloid
Authored by Felipe Contoli Isoldi
Abstract
Background: The mechanisms underlying the pathogenesis of keloids have not been fully characterized. Results of past and present studies have shown that the immune system is actively involved in the development of these lesions. The occurrence of leukocyte infiltration into keloid tissue, and increase in serum immunoglobulinshave been demonstrated; however, no study to date has evaluated serum leukocyte counts and leukocyte distribution in patients with keloids.
Materials and methods: Samples of venous blood were collected from 21 patients with keloids and 20 patients with normotrophic scars for total and differential leukocyte counts.
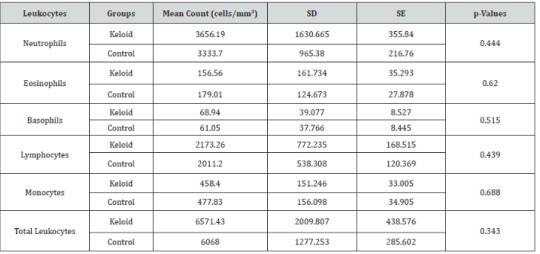
Results: There were no significant differences neither in mean total leukocyte counts (p<0.343), nor in differential leukocyte counts (neutrophil, p<0.444; eosinophil, p<0.620; basophil p<0.515; monocyte, p<0.688; and lymphocyte, p<0.439) between groups.
Conclusion: No quantitative and qualitative differences were found in leukocytes counts between patients with and without keloids. This confirms the fact that keloid scarring is not an intrinsic disturbance that results in increased cell proliferation. According to this view, keloid scarring may be regarded as an inflammatory disturbance related more to cellular hypermetabolism than to cell hyperproliferation.
Keywords: Keloid; Inflammation; Leukocytes; Leukocytes Count; Wound Healing
Introduction
Keloid formation results from a disturbance in wound healing caused by an imbalance between collagen synthesis and degradation; however, the mechanisms underlying keloid pathogenesis are not well understood [1]. Keloids are benign neoplasms that grow beyond the boundaries of the original wound. They do not regress spontaneously, and have a high recurrence rate after excision, even when the procedure is combined with other treatment modalities. The condition is characterized by pruritus, pain and hyperemia, suggesting an intermittent, local inflammatory process [2].
An increase in the metabolic activity of fibroblasts, and consequent increase in collagen synthesis, may occur due to a prolonged chronic inflammatory process [3]. This process is characterized at the cellular level by an increase in neutrophils, mast cells, lymphocytes and macrophages [4,5]. In this context, Hazrati & Hoomand [6] observed by microscopy a significantly higher tissue infiltration by these inflammatory cells in keloids than in spinocellular carcinoma. These authors also demonstrated the association between local lymphocytic infiltration and serum lymphocytosis, and exacerbation of immediate and delayed hypersensitivity skin reactions in patients with keloids [7,8].
The relationship between keloid and the immune system [4,7] becomes more important in patients with keloids and high serum IgE levels [8]. This immunoglobulin induces mast cell degranulation, which triggers proinflammatory signaling, which in turn will induce collagen deposition [7].
Immunoglobulins G, M and A, and the C3, C4 and C1q complement components have been associated with keloid formation; however, there is divergence in the literature concerning their level variation in patients with keloids [4,5]. On the other hand, it has been established that atopic patients are more susceptible to develop keloids [9].
Despite the fact that all evidences point to a relationship between the immune system and the pathogenic mechanisms of keloids, no studies were found in the literature evaluating serum leukocyte counts in patients with keloids. Therefore, the aim of this study was to investigate serum leukocyte counts and leukocyte distribution in patients with keloids.
Materials and Methods
This controlled study was conducted with 41 patients who attended the Plastic Surgery Outpatient Clinic of the Federal University of São Paulo. Participants were selected and divided into two groups: Keloid Group (KG: n=21; 6 men; median age, 29 years), and Control Group (CG: n=20; 14 men; median age, 23 years).
The keloid group consisted of patients with keloid scars located on the trunk, including the region between the transverse plane at the level of the sternoclavicular joint and transverse plane at the level of the upper margin of the pubic symphysis, comprising the whole-body perimeter. Patients with keloids of more than 1-year duration, which were showing clinical activity, such as pruritus, pain and hyperemia, alone or in combination, were included in this group. The control group included patients with normotrophic scars of more than 1-year duration, without past or current keloid or hypertrophic scars. Patients with treated or recurrent keloids of less than 1-year duration following previous excision, collagen disorders, malignant neoplasia, or those who underwent chemotherapy or corticoid treatment were excluded from the sample.
All patients responded to a medical history questionnaire, which also included questions on the characteristics of the keloid (location, presence of local pruritus, pain and hyperemia, causes of keloid formation, and keloid duration) and history of atopy. Scar pain and pruritus were measured using a visual analogue scale (VAS) rated from 0 (no symptom) to 10 (maximum symptom intensity) [10]. After, a venous blood sample was taken from the forearm of each patient for total and differential leukocyte counts. All laboratory tests were performed by the Central Laboratory at the Federal University of São Paulo Hospital (Unifesp).
Student’s t-test was used to compare the mean absolute count of each leukocyte cell type (neutrophils, eosinophils, basophils, monocytes, and lymphocytes) at a significance level of 0.05 (p < 0.05).
The present study was approved by the Research Ethics Committee of the Federal University of São Paulo (Unifesp), Brazil, and was performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki. Written informed consent was obtained from all patients. Patient anonymity was assured.
Results
With regard to atopy, 24.4% of the patients in the keloid group and 17.1% of the patients in the control group had allergic rhinitis and contact dermatitis according to the medical history questionnaire.
There were no significant differences either in mean total leukocyte counts or differential leukocyte counts (neutrophils, eosinophils, basophils, monocytes, and lymphocytes) between groups (Table 1).
Discussion
The present study was based on the work of Hazrati & Hoomand [6], who raised the hypothesis that patients with keloids did not have the tendency to develop spinocellular carcinoma and viceversa. This proposition was based on inflammatory parameters; the authors observed increased lymphocyte count in the serum and tissue of patients with keloids, and exacerbation of immediate and delayed hypersensitivity skin reactions in patients with skin carcinoma. Their study was conducted with 68 patients.
When compared with patients with normal skin, patients with keloids have increased levels of immunoglobulins, complement components, and pro-inflammatory cells [3,4,7,8], as in the lymphocyte infiltrate, containing high concentrations of T-cells (CD3+, CD4+, CD45RO+, and HLA-DR+), dendritic cells (CD1a+, CD36+, HLA-DR+, and ICAM-1+), macrophages, and mast cells [4,5,7]. This increase in cell number definitely demonstrated that the immune system is constantly active [4], recruiting elements for regulation of inflammation in the keloid tissue [1,2]. These phenomena imply that the existence of a systemic inflammatory state would provide an appropriate microenvironment for keloid formation and growth [2].
Keloid fibroblasts produce more collagen than normal skin fibroblasts [1,2]. However, there are no differences in growth and proliferation between keloid and normotrophic scar fibroblasts [11]. Therefore, the increased collagen production in keloids is related to an increase in fibroblast activity, characterizing a hyperactive state of these cells, which results in higher energy consumption [12]. Hyperactivity of fibroblasts is associated with deregulation of cytokines, interleukins, and growth factors (especially TGF-beta) [2], which have proven to induce keloid growth. Hence, after its development, the keloid itself creates a self-perpetuating cycle [2].
However, in the present study, there were no significant differences in the total and differential leukocyte counts between patients with and without keloids. These results confirm the fact that keloid scarring is not an intrinsic disturbance that results in increased cell proliferation, as demonstrated with respect to keloid fibroblasts (no quantitative differences between keloid and normal skin fibroblasts were detected). Keloid fibroblasts show increased activity, resulting in increased collagen synthesis, rather than increased proliferation. According to this view, keloid scarring should be regarded more as a disturbance in cellular hypermetabolism than as a disturbance in cell hyperproliferation [1,13]. This may explain the results with respect to serum leukocytes.
In comparison with the control group, the keloid group had a higher prevalence of atopy, pruritus, pain, and hyperemia, of which pruritus was the most frequent symptom. This is in agreement with the literature [1,9]. These symptoms are indicative of a neurogenic inflammatory activity intrinsic to the keloid that is represented by the presence of a large number of nociceptive nerve endings in this tissue [14], higher levels of proinflammatory neuropeptides, such as CGRP [15], and a functional disturbance of this innervation [14,15].
Although the presence of the Immune System in the genesis and maintenance of the inflammatory process involved in keloid is verified at serum and histological levels, leukocytes quantification in the peripheral blood was not altered. Even when the keloid presented exacerbated clinical symptoms. The present study suggests that further research is necessary to investigate differences in a possible systemic inflammatory state, either in the level of cell signaling or gene expression, in patients with keloids.
Conclusion
In conclusion, there are no quantitative and qualitative differences in serum leukocyte counts in patients with keloids.
For more articles in Open Access Journal of Case Studies please click on: https://juniperpublishers.com/jojcs/index.php
#More About Juniper Publishers#juniper publishers contact info#about juniper journals#Emergency Medicine#Geriatric Medicine#Pathology
0 notes
Text
Gynecologist in East Delhi
Your search for a trusted Gynecologist in East Delhi, ends with Dr. Radha Jain, experience compassionate women's health care and expert guidance tailored to your needs. Dr. Radha Jain prioritizes your well-being, providing comprehensive and personalized solutions. Take the first step towards your reproductive health journey – book your appointment now.

Click here for more info - Gynecologist in East Delhi
#best gynecologist in east delhi#dr. radha jain#audiologist in east delhi#best audiologist in east delhi#genesis neurogen#gynecologist in east delhi
0 notes
Text
Welcome to Genesis Neurogen Krishna Nagar – your trusted source for expert insights on neurology, rehabilitation, and advanced neuro care. Empowering recovery, restoring lives, and inspiring hope.
0 notes
Text

About us:-
Dr. Murli Singh is an experienced speech therapist in Delhi. He has an experience of over 25 years, treated about 6000 patients and has 04 centres in Delhi and NCR. He is at present associated with Genesis-Neurogen Neuro rehabilitation Rishabh vihar opposite cross river Mall Delhi -110092 & Genesis -Neurogen Neuro Rehabilitation centre Durgapuri chowk Delhi -110032 & Sarthak Speech therapy and Hearing aid center Shadhara Delhi -110093 & Dr.Murli Singh speech & Neuro Rehabilitation centre wave silver tower sector 18 Noida centre. He and his team deal with problems such as unclear speech, Autism spectrum,ADHD, stammering problem, Hearing Impaired, Downs syndrome, paralysis, brain aphasia,repetition of certain words, voice disorders, communication problems after an accident and children who do not start talking at the proper age. He and his team also provide rehab for problems in speech in cases of hearing loss, disarticulating, cerebral palsy, mental retardation, cleft palate, autism, aphasia, ADHD (Attention Deficit Hyperactivity Disorder) etc.Dr. Murli Singh has completed his education of D.H.L.S., from Ali Yavar Jung National Institute of Speech and Hearing, M.A. (Sociology ) then H.N.B. Garwal University, B.Ed. Special education from M.P.Bhoj University, Bhopal.Hon.PHD (Speech and language pathologist) Amrican council of training and Development U.S.A., Diploma diagnosis treatment and management of ADHD (Iearland), Diploma Autism spectrum awareness international College in U.K.
#delayed speech#hard of hearing#diphysia#hearing aids#speech therapy#stammering#adhd#brain stroke treatment#hearing test#autism spectrum disorder
0 notes
Link
Genesis - NeuroGen Brain and Spine Institute At Mumbai, Dr Alok Sharma and his team of highly experienced doctors use a combination of cell therapy and neurorehabilitation.
0 notes
Link
At Genesis - NeuroGen Brain and Spine Institute At Mumbai, Dr Alok Sharma and his team of highly experienced doctors use a combination of cell therapy and neurorehabilitation. Dr Alok Sharma's comprehensive treatment involves a holistic approach towards the total wellbeing of the patient which through and improvement in their neurological condition, which ultimately helps in the quality of a better life.
0 notes
Text
Gynaecology & Obstetrics Centre in East Delhi
Looking for a place for women's health in East Delhi ? Check out Genesis Neurogen! We offer care for women's needs, like pregnancy and routine check-ups. Our team is kind and will make a plan just for you. We have good tools and people who know what they're doing. Your health is important to us. Call us today to make an appointment.

Click here for more info- Gynaecology & Obstetrics Centre in East Delhi
0 notes
Text
Best Pediatrician in East Delhi

Dr. Dr Piyush Jain has been serving as the best pediatrician doctor in east Delhi for more than 20 years at Genesis Neurogen. He has got special interest in neonatology and Pediatric Neurology. Genesis Neurogen is situated in East Delhi with all the super best facilities and services. Pediatrics is the branch of prescription that includes the therapeutic care of new born babies, child, youngsters, and youths. He is working with great passion for the upliftment of these children to bring them to the main stream of society.
#Best Pediatrician In Anand Vihar#Best Pediatrician In East Delhi#Best Pediatrician In Vivek Vihar#Best Pediatrician In Shahdara#Best Pediatrician In Patparganj#Best Pediatrician In Rishabh Vihar#Best Pediatrician In Karkardooma#Pediatrician In Anand Vihar#Pediatrician doctor delhi
0 notes
Text
Best Pediatrician In East Delhi
Are you want to book online appointment with pediatrician in East Delhi? Then contact Dr. Piyush Jain, who is available at Genesis Neurogen Krishna Nagar. He has more then 20 years experienced in giving medical services at affordable price.
0 notes