#epidemiologists warning numbers
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
There were a total of 171.5 billion posts on Tumblr in 2019.
Text
Also preserved on our archive (Thousands of reports, sources, and resources! Daily updates!)
By Robert Stevens
A COVID wave fuelled by the XEC variant is leading to hospitalisations throughout Britain.
According to the UK Health Security Agency (UKHSA), the admission rate for patients testing positive for XEC stood at 4.5 per 100,000 people in the week to October 6—up significantly from 3.7 a week earlier. UKHSA described the spread as “alarming”.
Last week, Dr. Jamie Lopez Bernal, consultant epidemiologist at the UKHSA, noted of the spread of the new variant in Britain: “Our surveillance shows that where Covid cases are sequenced, around one in 10 are the ‘XEC’ lineage.”
The XEC variant, a combination of the KS.1.1 and KP.3.3 variants, was detected and recorded in Germany in June and has been found in at least 29 countries—including in at least 13 European nations and the 24 states within United States. According to a New Scientist article published last month, “The earliest cases of the variant occurred in Italy in May. However, these samples weren’t uploaded to an international database that tracks SARS-CoV-2 variants, called the Global Initiative on Sharing All Influenza Data (GISAID), until September.”
The number of confirmed cases of XEC internationally exceeds 600 according to GISAID. This is likely an underestimation. Bhanu Bhatnagar at the World Health Organization Regional Office for Europe noted that “not all countries consistently report data to GISAID, so the XEC variant is likely to be present in more countries”.
Another source, containing data up to September 28—the Outbreak.info genomic reports: scalable and dynamic surveillance of SARS-CoV-2 variants and mutations—reports that there have been 1,115 XEC cases detected worldwide.
Within Europe, XEC was initially most widespread in France, accounting for around 21 percent of confirmed COVID samples. In Germany, it accounted for 15 percent of samples and 8 percent of sequenced samples, according to an assessment from Professor Francois Balloux at the University College London, cited in the New Scientist.
Within weeks of those comments the spread of XEC has been rapid. Just in Germany, it currently accounts for 43 percent of infections and is therefore predominant. Virologists estimate that XEC has around twice the growth advantage of KP.3.1.1 and will be the dominant variant in winter.
A number of articles have cited the comments made to the LA Times by Eric Topol, the Director of the Scripps Research Translational Institute in California. Topol warns that XEC is “just getting started”, “and that’s going to take many weeks, a couple months, before it really takes hold and starts to cause a wave. XEC is definitely taking charge. That does appear to be the next variant.”
A report in the Independent published Tuesday noted of the make-up of XEC, and its two parent subvariants: “KS.1.1 is a type of what’s commonly called a FLiRT variant. It is characterised by mutations in the building block molecules phenylalanine (F) altered to leucine (L), and arginine (R) to threonine (T) on the spike protein that the virus uses to attach to human cells.
“The second omicron subvariant KP.3.3 belongs to the category FLuQE where the amino acid glutamine (Q) is mutated to glutamic acid (E) on the spike protein, making its binding to human cells more effective.”
Covid cases are on the rise across the UK, with recent data from the UK Health Security Agency (UKHSA) indicating a 21.6 percent increase in cases in England within a week.
There is no doubt that the spread of XEC virus contributed to an increase in COVID cases and deaths in Britain. In the week to September 25, there were 2,797 reported cases—an increase of 530 from the previous week. In the week to September 20 there was a 50 percent increase in COVID-related deaths in England, with 134 fatalities reported.
According to the latest data, the North East of England is witnessing the highest rate of people being hospitalised, with 8.12 people per 100,000 requiring treatment.
Virologist Dr. Stephen Griffin of the University of Leeds has been an active communicator of the science and statistics of the virus on various public platforms and social media since the start of the pandemic. He was active in various UK government committees during the height of the COVID-19. In March 2022, he gave an interview to the World Socialist Web Site.
This week Griffin spoke to the i newspaper on the continuing danger of allowing the untrammelled spread of XEC and COVID in general. “The problem with COVID is that it evolves so quickly,” he said.
He warned, “We can either increase our immunity by making better vaccines or increasing our vaccine coverage, or we can slow the virus down with interventions, such as improving indoor air quality. But we’re not doing those things.”
“Its evolutionary rate is something like three or four times faster than that of the fastest seasonal flu. So you’ve got this constant change in the virus, which accelerates the number of susceptible people.
“It’s creating its own new pool of susceptibles every time it changes to something that’s ‘immune evasive’. Every one of these subvariants is distinct enough that a whole swathe of people are no longer immune to it and it can infect them. That’s why you see this constant undulatory pattern which doesn’t look seasonal at all.”
There are no mitigations in place in Britain, as is the case internationally, to stop the spread of this virus. Advice for those with COVID symptoms is to stay at home and limit contact with others for just five days. The National Health Service advises, “You can go back to your normal activities when you feel better or do not have a high temperature”, despite the fact that the person may well still be infectious. Families are advised that children with symptoms such as a runny nose, sore throat, or mild cough can still “go to school or childcare' if they feel well enough.
The detection and rapid spread of new variants disproves the lies of governments that the pandemic is long over and COVID-19 should be treated no differently to influenza.
Deaths due to COVID in the UK rose above 244,000 by the end of September. It is only a matter of time before an even deadlier variant emerges. Last month, Sir Chris Whitty, England’s chief medical officer, told the ongoing public inquiry into COVID-19 “We have to assume a future pandemic on this scale [the global pandemic which began in 2020] will occur… That’s a certainty.”
#mask up#covid#pandemic#wear a mask#public health#covid 19#wear a respirator#still coviding#coronavirus#sars cov 2
145 notes
·
View notes
Text
In the U.K., the Health Security Agency recently raised its threat level to 4 out of 6, the stage immediately before large-scale human outbreaks. In Europe, countries are proactively vaccinating dairy and poultry workers against infection, with 15 nations already securing a total of 40 million doses through the European Commission. In the United States, despite having a stockpile of those vaccines, we are not distributing them, instead focusing on standing up voluntary supplies of seasonal flu vaccines to frontline workers. (The hope is that this will prevent animal infections of human flu that might aid in the further mutation of H5N1.) The Centers for Disease Control and Prevention has cited the low number of cases to justify its inaction, but it has also moved remarkably slowly to promote the kind of widespread surveillance testing that could actually identify cases. Only recently has the agency begun to mobilize real funding for a testing push, after a period of months in which various federal groups batted around responsibility and ultimate authority like a hot potato. And as was the case early in the Covid-19 pandemic, the C.D.C.’s preferred test for bird flu “has issues.” Three months into the outbreak, only 45 people had even been tested; six weeks later, the total number of people tested had grown only to “230+.” [...] Most farms aren’t supplying N95 masks, goggles or aprons to protect workers, either, and when Amy Maxmen of KFF News surveyed farm workers to ask why they weren’t getting tested, “no one had heard of bird flu, never mind gotten P.P.E. or offers of tests,” she reported. “One said they don’t get much from their employers, not even water. If they call in sick, they worry about getting fired.” Last month, a crew was deployed to slow the spread of the disease by killing every last chicken of 1.78 million on a large Colorado farm where H5N1 had broken out and six of the workers contracted the virus, partly because the gear they’d been provided was hard to use in the punishing 104-degree heat. In June, Robert Redfield, former director of the C.D.C., echoed many epidemiologists in predicting that “it’s not a question of if, it’s more of a question of when we will have a bird flu pandemic.” In July, Brown’s Jennifer Nuzzo warned that the steady beat of new cases “screams at us that this virus is not going away.” Tulio de Oliveira, a bioinformatician who studies global disease surveillance, marveled that the American effort to track the spread of the disease was absolutely amateurish and the country’s apparent indifference “unbelievable.”
59 notes
·
View notes
Text
The risk of suffering a stroke is significantly higher with high overnight temperatures, posing a potential health concern around the globe as the world gets warmer. Mapping night-time temperatures against the number of stroke cases recorded in the German city of Augsburg across the course of 15 years, a research team led by the Helmholtz Munich research center in Germany found a statistically significant increase in stroke risk on days where extremely warm night-time temperatures were recorded, with older people and women particularly vulnerable. "We wanted to understand the extent to which high night-time temperatures pose a health risk," says Alexandra Schneider, an epidemiologist at the Helmholtz Munich. "This is important because climate change is causing night-time temperatures to rise much faster than daytime temperatures."
Continue Reading.
69 notes
·
View notes
Text
"The Integrated Phase Classification (IPC) system, set up 20 years ago, provides the most authoritative assessments of humanitarian crises. Its figures for Gaza are the worst ever by any metric. It estimates that 677,000 people, or 32% of all Gazans, are in “catastrophic” conditions today and a further 41% are in “emergency” conditions. It expects fully half of Gazans, more than 1 million people, to be in “catastrophe” or “famine” within weeks."
...
We are about to witness most intense famine since the second world war. It won’t be the biggest, because starvation is confined to the 2.2 million residents of the Gaza Strip.
...
Epidemiologists in London and Baltimore have generated projections for the likely death toll in Gaza from all causes over the months to August. If epidemics are included, their “status quo” scenario projects a range of 48,210 to 193,180 deaths, while under the “with escalation” scenario those figures range even higher.
Gaza’s health crisis has its own dreadful momentum. Even if the shooting ends today and the aid trucks begin to roll, the dying will carry on for some time.
And even when the numbers of people needlessly dying dwindle, the scars of famine will endure.
....
And in Gaza there is no margin of doubt.
In most famines, there’s a margin of uncertainty in predictions, because people may be able to find unexpected sources of food or money. In parts of rural Africa, grandmothers may know about edible wild roots and berries or migrant workers may find creative ways of sending cash to their families. In Gaza, Israel knows every calorie that’s available. In 2008, the coordinator of government activities in the territories calculated every aspect of Gaza’s food production and consumption, in minute detail, and extracted the “red lines” needed to keep Palestinians on what it called a “diet”, just short of starvation.
Until 7 October 2023, Israel was, according to its own analysis, just on the right side of the international laws prohibiting starvation. About 500 truckloads of essentials entered every day to complement local farms, fisheries and livestock. In recent months, less than one-third of that number has been allowed to enter, while local food production has been reduced to almost zero.
Israel has had ample warning of what will happen if it continues its campaign of destroying everything necessary to sustain life. The IPC’s Famine Review Committee report on 21 December authoritatively warned of starvation if Israel did not cease destruction and failed to allow humanitarian aid at scale. Israel’s own judge nominated to sit at the international court of justice, Aharon Barak, voted with the court’s majority in favour of “immediate and effective measures to enable the provision of urgently needed basic services and humanitarian assistance”.
Israel has not changed course. The supplies entering Gaza are woefully short of the minimum calories Israel specified before the war. American airdrops of supplies and an emergency port are a pitiful pretence of a substitute.
Famine is unfolding in Gaza today. We should not have to wait until we count the graves of children to speak its name.
#palestine#free palestine#isreal#gaza#apartheid#genocide#colonization#us politics#american imperialism#famine
11 notes
·
View notes
Text
Chrissy Kinsella was looking for a more personalized approach to her health. “You know, what is good for you as an individual may not necessarily be good for the next person,” she says. So she reached for a subscription to Zoe—a personalized nutrition service cofounded by Tim Spector, a celebrity scientist and a genetic epidemiologist at King’s College London. Kinsella paid the £299 ($365) for a testing kit and later received a bright yellow package in the mail: a bundle of vials, patches, and muffins.
By testing, scoring, and monitoring how you respond to different foods, Zoe says, it can help with a whole host of problems. Its personalized recommendations can help you “reach a healthy weight,” “feel less bloated,” and “avoid chronic health issues,” claims its website. The program can even help with menopause, Zoe says.
But doctors are more ambivalent. Sure, getting people to think critically about what they eat can be beneficial, but scoring and monitoring someone’s diet could lead to unnecessary health concerns or even disordered eating. British doctors say they have seen perfectly healthy patients with concerns about their blood sugar control prompted by readings in their Zoe app.
A Zoe starter pack includes a fecal sampling kit, a finger-prick blood test, and a continuous glucose monitor (CGM). Participants are asked to take a blood sample before and after they eat a muffin precisely engineered by the startup to contain specific levels of fat, sugar, and proteins. Zoe then runs a blood-fat test to see how each person responds to fat in their diet (prolonged high levels of fat in the blood are a health risk). Combined with blood glucose data (from the CGM) and an analysis of the quality of their microbiome (via the fecal sample), these measurements are used to create personalized diet recommendations, where each item of food is scored on a scale up to 100.
A sugary food, for example, would have a low score for someone whose data shows their body doesn’t control blood sugar levels well; for someone with good sugar control, the same food would be scored a bit higher. Meals, too, are scored out of 100—based on the personalized scores of their ingredients, as well as how those ingredients interact.
Kinsella, who used the program for a year, says she values the insights it gave on what foods were more suited to her body—now she knows that she tolerates fat well, sugar not so much, and that dairy milk sits better with her than oat milk. Kinsella loved inspecting data about her body, but she admits she became obsessed with checking the app to see what her blood sugar was doing in response to what she ate, courtesy of the CGM. Small, coin-shaped, and usually affixed to the upper arm, CGMs have been a regular appendage of people with diabetes for years now, allowing them to track dips and hikes in blood sugar without needing to prick their finger every time. There’s been a growing trend of companies selling the monitors to people without diabetes for them to track how their body responds to certain foods. Levels and Veri, two other personalized nutrition plans, also use CGMs.
Getting a score of at least 75 every day is the ultimate aim of the Zoe program. This figure is calculated based on what you’ve eaten. But Kinsella found herself ruling out a lot of foods because they wouldn’t get her to that magic number, and she thinks the app encourages this kind of obsessive behavior. “You’re giving people an app that is kind of almost gamified, in that when you hit this magical 75, you get a big green circle. And everybody wants to get 10 big green circles in a row,” she says.
Shivani Misra, a consultant doctor specializing in diabetes in London, has seen an influx of patients at her non-NHS practice who have either purchased a CGM themselves or through the Zoe program, and who’ve become worried they are at risk for developing diabetes—due to seeing either continuously high blood sugar levels or sharp rises and falls.
When Misra formally tests them for diabetes, the results always come back normal. “We shouldn’t be using CGM to diagnose diabetes; it’s absolutely not validated for that,” she says. What concerns Misra is the people she’s seen who are restricting calorie intake and have become extremely anxious about eating carbohydrates. “I really worry about that group, because they’ve just become overwhelmed with the data that they’re seeing, which is completely normal.”
“It’s set up to derive those kinds of behaviors in exactly the people that would be susceptible to it, in my opinion,” she says. The patients who came to her were seeking professional guidance because they felt their anxiety about what the data was telling them had become problematic—in the case of one patient, they felt they couldn’t eat fruit anymore. “I personally think there is some corporate responsibility to make sure that there is adequate safety in place for people,” says Misra.
Federica Amati, a medical scientist and nutritionist and a science communications strategist at Zoe, says that the company has “lots of systems in place for customer service, and for our coaching team to be able to flag if they feel that somebody is not interacting with the app in a healthy way,” she says. “Of course, the fact that there’s a score associated with food is still problematic if you have disordered eating.”
On the potential for programs like Zoe to burden health systems with concerned users, Amati says that the company is putting a task force together to investigate how medical professionals are experiencing Zoe’s influence. “We feel very responsible about it,” she says.
Nicola Guess, a dietitian and researcher at the University of Oxford, says that she has also been approached by patients concerned about their health after seeing their blood glucose spike while wearing a CGM offered as part of a personalized nutrition plan. When she tested these patients to assess their blood glucose control, their results were completely normal. “It’s just making them quite weird about food, and it takes a lot of the enjoyment out of food for no reason whatsoever,” says Guess.
But, says Amati, Zoe didn’t create the worried well, noting that the problem has been an issue for the public health service for a very long time. “For sure, we’ve probably now created a new stream for the worried well to feed into, but I think that that’s a bigger problem than just Zoe.”
There is also a big question mark over how useful personalized nutrition really is. Zoe’s nutrition scores are predicated on the idea that each of us responds to the same food in a slightly different way—thanks, in part, to our microbiomes. But translating this into dietary advice is trickier and less well understood. A personalized diet might tell someone to cut out white bread and eat more leafy vegetables, for example, but is this really more effective than the same advice delivered by a family doctor or a public health advertisement?
“Zoe doesn’t eschew all the normal health advice,” Amati says. “We’re not like, ‘Oh, no, don’t eat more fruits and vegetables’—it sits within the recommendations that we know are very good for the majority.”
There is precious little clinical trial data on personalized nutrition apps, says Duane Mellor, a dietitian and researcher at Aston University in the UK. One study from Israel published in 2015 compared personalized diets generated by a machine-learning algorithm with diets selected by a clinical dietitian. The authors found that people in both groups had fewer glucose spikes after meals—indicating a healthier diet.
But whether personalized nutritional plans really make a difference is something Zoe is studying. Next month, Amati says the company will be releasing the results of a randomized controlled trial, called the Zoe Method Study. The trial involved one group of people receiving the full Zoe product and another group simply receiving standard nutritional advice, plus access to support services through an app. The study aims to test the efficacy of a program like Zoe in improving cardiometabolic risk markers in otherwise healthy people, through testing their resulting levels of cholesterol and triglycerides (a type of fat), as well as measuring other things like weight, blood pressure, glycemic control, and hunger levels.
All of this doesn’t come cheap, and Zoe users have to pay membership fees for continued access to their bespoke scores. Prices start at £59.99 ($73) for a single month and go down to £24.99 ($30) per month for a year-long plan. At those prices, Zoe is aimed squarely at wealthier consumers—a point not lost on columnist James Greig, who wrote about Zoe in the newsletter Vittles.“If our environment really is saturated with poisons, then bespoke services like Zoe are not a scalable solution but a form of private health care that will further entrench existing inequalities,” Greig wrote.
Amati acknowledges that Zoe’s program is expensive, but she says, “The product at the moment is the price it is because the testing we do is expensive.” She says the idea is that, as the techniques and technology become more common, the price will come down accordingly, and that Zoe has plans to work with the NHS and other providers to “become part of the health approach.” In the meantime, the company places focus on communicating health advice for free through forums like social media and podcasts.
Zoe is still proving popular, with over 130,000 people having tried the service so far. Part of the appeal of personalized nutrition is that it goes beyond weight loss to address other concerns people have about their health. Zoe markets its diet as a way to improve energy levels, gut health, and sleep. William Viney, a researcher who has worked on personalized medicine, points out that there are a huge number of people who have health issues that aren’t easily addressed by doctors and mainstream diets. “They know that they’re not like everyone else, and they need to get to the bottom of something,” says Viney. “There is an opportunity to bring information, and with it care, to whoever can pay the price for such a product.”
4 notes
·
View notes
Text
Does Marijuana Cause Harm?
Many consider that the use of marijuana is both safe and non-addictive. Is that so? The New York Times reported that since the legalization of the drug across much of the USA, that there have been increases in physical and mental disorders among users of cannabis products. Modern marijuana is often more potent than what many used last century . "About 18 million people — nearly a third of all users ages 18 and up — have reported symptoms of cannabis use disorder." Did you know that among 18- to 25-year-old Americans, more than 4.5 million use the drug daily or near daily, according to the estimates, and 81 percent of those users meet the criteria for the disorder?“ That means almost everybody that uses it every day is reporting problems with it,” said Dr. Wilson Compton, deputy director of the National Institute on Drug Abuse. Marijuana can interfere with brain development, cause lung and heart problems, and result in having a psychosis. Is knowledge of problems with marijuana known or did the old Worldwide Church of God warn of them 54 years ago? Should Christians get drunk or high? Are there more problems with marijuana than many seem to want to admit? Dr. Thiel and Steve Dupuie address these issues.
A written article of possibly related interest is available titled 'NYT: As America’s Marijuana Use Grows, So Do the Harms’
youtube
Youtube video link: Does Marijuana Cause Harm?
NYT: As America’s Marijuana Use Grows, So Do the Harms
COGwriter
The New York Times reported the following:
As America’s Marijuana Use Grows, So Do the Harms
The drug, legal in much of the country, is widely seen as nonaddictive and safe. For some users, these assumptions are dangerously wrong.
October 4, 2024
In midcoast Maine, a pediatrician sees teenagers so dependent on cannabis that they consume it practically all day, every day — “a remarkably scary amount,” she said.
From Washington State to West Virginia, psychiatrists treat rising numbers of people whose use of the drug has brought on delusions, paranoia and other symptoms of psychosis.
And in the emergency departments of small community hospitals and large academic medical centers alike, physicians encounter patients with severe vomiting induced by the drug — a potentially devastating condition that once was rare but now, they say, is common. “Those patients look so sick,” said a doctor in Ohio, who described them “writhing around in pain.”
As marijuana legalization has accelerated across the country, doctors are contending with the effects of an explosion in the use of the drug and its intensity. A $33 billion industry has taken root, turning out an ever-expanding range of cannabis products so intoxicating they bear little resemblance to the marijuana available a generation ago. Tens of millions of Americans use the drug, for medical or recreational purposes — most of them without problems.
But with more people consuming more potent cannabis more often, a growing number, mostly chronic users, are enduring serious health consequences.
The accumulating harm is broader and more severe than previously reported. And gaps in state regulations, limited public health messaging and federal restraints on research have left many consumers, government officials and even medical practitioners in the dark about such outcomes.
Again and again, The New York Times found dangerous misconceptions.
Many users believe, for instance, that people cannot become addicted to cannabis. But millions do.
About 18 million people — nearly a third of all users ages 18 and up — have reported symptoms of cannabis use disorder, according to estimates from a unique data analysis conducted for The Times by a Columbia University epidemiologist. That would mean they continue to use the drug despite significant negative effects on their lives. Of those, about three million people are considered addicted.
The estimates are based on responses to the 2022 U.S. national drug use survey from people who reported any cannabis consumption within the previous year. The results are especially stark among 18- to 25-year-olds: More than 4.5 million use the drug daily or near daily, according to the estimates, and 81 percent of those users meet the criteria for the disorder.
“That means almost everybody that uses it every day is reporting problems with it,” said Dr. Wilson Compton, deputy director of the National Institute on Drug Abuse, who was not involved in the analysis. “That is a very clear warning sign.”
Marijuana is known for soothing nausea. But for some users, it has the opposite effect.
“Why don’t more doctors know about it? Why didn’t anyone ever mention it to me?” …
Debilitating and Undiagnosed
A telltale sign of cannabinoid hyperemesis syndrome is that heat often temporarily relieves the nausea and vomiting. Hundreds of people recounted to The Times, in interviews and survey responses, that they had spent hour after hour in hot baths and showers. Some were burned by scalding water. One teenager was injured when, in desperation, he pressed his body against a hot car.
Researchers don’t know why heat soothes the syndrome, known as C.H.S., nor why certain chronic marijuana users develop it and others don’t. But the onset appears to be related to the way marijuana interacts with the body’s endocannabinoid system, a network of signaling molecules and receptors that help regulate vital functions like sleep, digestion and the perception of pain. People with severe symptoms frequently require emergency care. …
In recent years, the syndrome has received growing attention in the medical field. Among those who speak out about it is Dr. Ethan Russo, a neurologist in Vashon, Wash., who helped develop one of the few cannabis-derived drugs approved by the U.S. Food and Drug Administration and continues to research therapeutic benefits of marijuana.
“I spent most of the last 30 years supporting medicinal uses of cannabis,” he said. “However, I have also talked about the harms and pitfalls of cannabis, specifically cannabinoid hyperemesis syndrome. It’s a serious problem and a genuine reason that some people should not use.”
‘Like He Was Possessed’
Dr. Sharon Levy, chief of addiction medicine at Boston Children’s Hospital, had a patient who believed coat hangers and sneakers had come to life. Dr. Luke Archibald, an addiction psychiatrist at Dartmouth Health in Lebanon, N.H., treated one who was charged with trespassing after following the directions of voices he hallucinated.
Many physicians said that they have seen growing numbers of patients with cannabis-induced temporary psychosis — lasting hours, days or even months. While it is more common among younger consumers, it can afflict people of all ages, whether heavy or first-time users, and with or without a family history or other risk factors for psychosis.
Dr. Levy and other physicians have also seen a rise in chronic psychotic disorders, such as schizophrenia, in which they believe cannabis was a contributing factor. As America’s Marijuana Use Grows, So Do the Risks – The New York Times (nytimes.com)
Well, harms associated with the use of marijuana have always been there.
Despite what the pro-marijuana forces claim, marijuana is not healthy.
I used to tell patients who asserted that 20,000 or so studies showed that marijuana was beneficial, that no, that was not the case.
I basically told them that while a few studies found that marijuana helped some with anxiety, etc., that 1) there were safer and better ways to treat that and 2) most health studies found harm with marijuana.
THC (which stands for tetrahydrocannabinol) is the chemical that causes the “high” that goes along with marijuana consumption.
The so-called ‘health benefits’ of intoxifying marijuana (and I am not referring to CBD oil, which have little or no THC) are over stated by many and basically not really true (though it is true that those who are ‘high’ feel less physical pains–but other substances can do this without the making one ‘high’).
Intentionally breathing in smoke and/or simply swallowing mind altering hallucinogenic substances is not healthy.
People should NOT smoke marijuana nor eat it. It has many negative effects on the human body.
Short-term bodily effects of marijuana, Cannibis sativa
Many studies have shown that marijuana is frequently addictive and harmful.
The State of California hoped that it would make a lot of money because of marijuana, as did many California cities. However, in California at least, legalizing it has not brought in the vast amounts of tax revenues many claimed it would.
The Bible warns:
10 For the love of money is a root of all kinds of evil, for which some have strayed from the faith in their greediness, and pierced themselves through with many sorrows. (1 Timothy 6:10)
Notice what the National Institute of Health says about marijuana:
How Does Marijuana Affect the Brain?
When marijuana is smoked, THC rapidly passes from the lungs into the bloodstream, which carries the chemical to the brain and other organs throughout the body. It is absorbed more slowly when ingested in food or drink.
However as it is ingested, THC acts on specific molecular targets on brain cells, called cannabinoid receptors. These receptors are ordinarily activated by chemicals similar to THC that naturally occur in the body (such as anandamide; see picture, above) and are part of a neural communication network called the endocannabinoid system. This system plays an important role in normal brain development and function.
The highest density of cannabinoid receptors is found in parts of the brain that influence pleasure, memory, thinking, concentration, sensory and time perception, and coordinated movement. Marijuana overactivates the endocannabinoid system, causing the “high” and other effects that users experience. These effects include altered perceptions and mood, impaired coordination, difficulty with thinking and problem solving, and disrupted learning and memory.
Marijuana also affects brain development, and when it is used heavily by young people, its effects on thinking and memory may last a long time or even be permanent. A recent study of marijuana users who began using in adolescence revealed substantially reduced connectivity among brain areas responsible for learning and memory. And a large long-term study in New Zealand showed that people who began smoking marijuana heavily in their teens lost an average of 8 points in IQ between age 13 and age 38. Importantly, the lost cognitive abilities were not fully restored in those who quit smoking marijuana as adults. Those who started smoking marijuana in adulthood did not show significant IQ declines.
What Are the Other Health Effects of Marijuana?
Marijuana use may have a wide range of effects, particularly on cardiopulmonary and mental health.
Marijuana smoke is an irritant to the lungs, and frequent marijuana smokers can have many of the same respiratory problems experienced by tobacco smokers, such as daily cough and phlegm production, more frequent acute chest illness, and a heightened risk of lung infections. One study found that people who smoke marijuana frequently, but do not smoke tobacco, have more health problems and miss more days of work than those who don’t smoke marijuana, mainly because of respiratory illnesses. It is not yet known whether marijuana smoking contributes to risk for lung cancer.
Marijuana also raises heart rate by 20-100 percent shortly after smoking; this effect can last up to 3 hours. In one study, it was estimated that marijuana users have a 4.8-fold increase in the risk of heart attack in the first hour after smoking the drug. This risk may be greater in older individuals or in those with cardiac vulnerabilities.
A number of studies have linked chronic marijuana use and mental illness. High doses of marijuana can produce a temporary psychotic reaction (involving hallucinations and paranoia) in some users, and using marijuana can worsen the course of illness in patients with schizophrenia. A series of large studies following users across time also showed a link between marijuana use and later development of psychosis. This relationship was influenced by genetic variables as well as the amount of drug used, drug potency, and the age at which it was first taken—those who start young are at increased risk for later problems.
Associations have also been found between marijuana use and other mental health problems, such as depression, anxiety, suicidal thoughts among adolescents, and personality disturbances, including a lack of motivation to engage in typically rewarding activities. More research is still needed to confirm and better understand these linkages.
Marijuana use during pregnancy is associated with increased risk of neurobehavioral problems in babies. Because THC and other compounds in marijuana mimic the body’s own endocannabinoid chemicals, marijuana use by pregnant mothers may alter the developing endocannabinoid system in the brain of the fetus. Consequences for the child may include problems with attention, memory, and problem solving.
Additionally, because it seriously impairs judgment and motor coordination, marijuana contributes to risk of injury or death while driving a car. A recent analysis of data from several studies found that marijuana use more than doubles a driver’s risk of being in an accident. The combination of marijuana and alcohol is worse than either substance alone with respect to driving impairment.
Inhaling or ingesting marijuana basically makes someone drunk.
The Bible repeatedly condemns drunkenness and activities associated with it:
18 And do not be drunk with wine, in which is dissipation; but be filled with the Spirit. (Ephesians 5:18)
21 For the drunkard and the glutton will come to poverty. (Proverbs 23:21)
11 But now I have written to you not to keep company with anyone named a brother, who is sexually immoral, or covetous, or an idolater, or a reviler, or a drunkard, or an extortioner — not even to eat with such a person. (1 Corinthians 5:11)
9 Do you not know that the unrighteous will not inherit the kingdom of God? Do not be deceived. Neither fornicators, nor idolaters, nor adulterers, nor homosexuals, nor sodomites, 10 nor thieves, nor covetous, nor drunkards, nor revilers, nor extortioners will inherit the kingdom of God. 11 And such were some of you. But you were washed, but you were sanctified, but you were justified in the name of the Lord Jesus and by the Spirit of our God. (1 Corinthians 6:9-11)
13 Let us walk properly, as in the day, not in revelry and drunkenness, not in lewdness and lust, not in strife and envy. 14 But put on the Lord Jesus Christ, and make no provision for the flesh, to fulfill its lusts. (Romans 13:13-14)
Becoming intoxicated by marijuana is sinful and not something that Christians should do.
Back in 2014, the Continuing Church of God put out the following video on our Bible New Prophecy YouTube channel.
youtube
19:28
How Should a Christian View Marijuana?
There is a growing trend to increase the legalization and public acceptance of smoking or ingesting marijuana. Is this something that Christians should do? What has US President Barack Obama said and done related to marijuana? What does the White House website state? Is marijuana no less dangerous than alcohol? Is marijuana safe? What are the affects of marijuana? Are there health risks? What about ‘medical marijuana’? What does the Bible teach about mental intoxication?
Here is a link to our video: How Should a Christian View Marijuana?
54 years ago, the old Worldwide Church of God published the following related to marijuana:
Are Good Results Produced?
The old saying is that “the proof of the pudding is in the eating.” Are there concrete beneficial fruits produced by marijuana? What does it actually do to, or for, a person? Does it make him a more productive member of society? How does it affect the user? Are those effects desirable?
Here are 27 typical reactions due to use of marijuana. They were excerpted from statements made about the drug from users. All of you who are using marijuana or thinking of using it — please read carefully.
Any sound-minded person will see that NOT ONE OF these effects is desirable.
1. Marijuana makes me unable to operate normally — for instance, drive a car or operate a machine. 2. It slows me down quite a bit and I lost my initiative when I started to use marijuana. 3. I feel stubborn and get into arguments when I am high. 4. I get into a panic. 5. It makes me sleepy, lazy. 6. Marijuana makes me too generous. I gave away everything I had; for example, I would buy drinks for everybody in the bar, etc. 7. I did not take things seriously anymore after starting the use of marijuana. 8. After starting on marijuana, I withdrew into a shell and would not communicate with people. I lost my job because I could not communicate with my boss. 9. Marijuana made me lazy, and I could not hold a job after starting to use it. 10. I got arrested for lots of things when I was high -curfew violations and rape. 11. I did about fifteen drugstore robberies with a partner for narcotics. We used to get high on marijuana beforehand. 12. It makes me weak, passive and paranoid, but I don’t get into trouble. I just want to be left alone where I don’t think people are spying on me. 13. It made me drop out of school and I lost a couple of jobs because I was late and would take off early. The three of us got into a bad fight once when we were high on marijuana. 14. I got an inferiority complex and wanted to stay away from society, but I never got into trouble. 15. Makes me silly; everything I do or say or hear is funny. 16. Sometimes it makes me happy and sometimes sad — mostly sad. 17. Makes me happy-go-lucky and I do not care about anything. 18. It relieves me and makes me gay — sort of blocks my thinking. 19. After I started to use marijuana, I quit school and did not want to work. I beat up my wife several times when I was high. It makes me feel happy and expands my perceptiveness. 20. In driving, you might think you are going 60 if you are only going 30. 21. I thought I was better at music and typing in high school but it was not so — I flunked out. 22. It made my throat raw and I had hallucinations, that is, I kept trying to brush a spider off my shoulder. I usually saw bugs and things like that after only one cigarette. I lost my equilibrium and could not stand up. 23. If you are only going 20 miles an hour you think you are going much faster. 24. It made me want to go off alone and watch TV. I could see hidden meanings in the commercials. 25. It slowed me down so much I had to drop out of school. 26. Marijuana slowed me down too much, so I started using pills to stimulate me. 27. What used to bother me was it numbed my brain and I could not think right. I could not drive well. (New Facts About Marijuana. Ambassadir College Press, 1970)
Marijuana is not good for Christians. Notice also from the same booklet:
Psychotic Reactions
A psychosis is far worse than a mere “personality disorder” — a psychosis is a severe mental derangement. And it is charged that marijuana can generate — or can at least precipitate — a psychotic reaction. Many scientific papers have been published on the relationship between the cannabis drugs and psychoses. Psychiatrists in India, Morocco, Egypt, and Nigeria have repeatedly emphasized that marijuana can produce insanity. In his editorial in the March 14, 1968 issue of Science, Philip H. Abelson wrote:
“The inconclusive information about marijuana is not reassuring. . . . Some of the effects of marijuana seem reminiscent of LSD. Large doses may produce con fusion, disorientation, and increased anxiety and psychoses lasting hours or sometimes weeks. In the Middle East habitual use of marijuana leads to cannabis psychosis whose victims are reminiscent of the derelicts of skid row.”
In Western scientific circles much controversy has arisen over the possible psychotogenic effects of marijuana.
And, obviously, there are differences of opinion among even the experts. But what sane person would gamble his mental health — and his entire future-on “somebody’s opinion”?
We know the adverse effects of marijuana depend to a large degree upon the individual user. Therefore, it is probable that marijuana would cause psychotic reactions in persons with unstable or poorly organized personalities.
Now nobody likes to admit that his or her personality is poorly organized. Everybody naturally likes to think of himself as mentally stable.
Well, just ponder this one point: studies have shown that most people who take drugs have a somewhat poorly organized personality to begin with. That’s why they take drugs. That’s why drugs appeal to them. They lack something in their lives — and they hope drugs will supply it. So, the simple fact that a person wants to use drugs should immediately suggest that that person could very well have a poorly organized personality, and, therefore, be vulnerable to an irreparable psychotic reaction. (New Facts About Marijuana. Ambassadir College Press, 1970)
Christians should not ingest or smoke marijuana (this differs from hemp protein, which is not mind altering, and is normally fine).
The increased use of marijuana is not good.
Update 10/14/24: We just uploaded the following related video:
youtube
14:44
Does marijuana cause harm?
Many consider that the use of marijuana is both safe and non-addictive. Is that so? The New York Times reported that since the legalization of the drug across much of the USA, that there have been increases in physical and mental disorders among users of cannabis products. Modern marijuana is often more potent than what many used last century . “About 18 million people — nearly a third of all users ages 18 and up — have reported symptoms of cannabis use disorder.” Did you know that among 18- to 25-year-old Americans, more than 4.5 million use the drug daily or near daily, according to the estimates, and 81 percent of those users meet the criteria for the disorder?“ That means almost everybody that uses it every day is reporting problems with it,” said Dr. Wilson Compton, deputy director of the National Institute on Drug Abuse. Marijuana can interfere with brain development, cause lung and heart problems, and result in having a psychosis. Is knowledge of problems with marijuana known or did the old Worldwide Church of God warn of them 54 years ago? Should Christians get drunk or high? Are there more problems with marijuana than many seem to want to admit? Dr. Thiel and Steve Dupuie address these issues.
Here is a link to our video: Does marijuana cause harm?
There are more problems with marijuana than many wish to accept.
It is nice that the New York Times has finally decided to report that.
Related Items:
Marijuana: Should a Christian Get High? There is increasing acceptance of the use of marijuana. How should Christians view this? Here is a related video titled How Should a Christian View Marijuana?
Should Christians Smoke (or Chew) Tobacco or Marijuana? Is smoking a sin? What does the Bible teach? What have COG leaders written? Can smokers change? What about marijuana? Here is a link to a related video: Should You Smoke? Would You Like Help to Quit?
Just What Do You Mean — Repentance? Do you know what repentance is? Have you truly repented? Repented of what? Herbert W. Armstrong wrote this as a booklet on this important subject.
When You Sin: Do You Really Repent? This is an article by Charles F. Hunting. A related sermon is Confess to God and truly repent.
Living as a Christian: How and Why? In what ways do Christians live differently than others. What about praying, fasting, tithing, holy days, and the world? There is also a YouTube video related to that also called: Living as a Christian: How and Why?
Overcoming Sin What is sin? How are Christians suppose to overcome it? Here is also a link to a video titled How to Overcome Sin.
How to Prevent Sin This is an article by Herbert W. Armstrong.
Just What Do You Mean Conversion? Many think that they are converted Christians. But are they? Would you like to know more about conversion. Herbert W. Armstrong wrote this as a booklet on this important subject.
LATEST BIBLE PROPHECY INTERVIEWS
LATEST NEWS REPORTS
0 notes
Link
0 notes
Text
Chernobyl did something amazing which most people seem incapable of realizing : it showed us that even the worst conceivable nuclear disaster wasn’t anything like as bad as we had thought.
A little background : back in 1958, the US Atomic Energy Commission published a report known as WASH-740. This was intended as a look at the worst possible consequence of a nuclear power plant accident, and so it postulated the sudden dispersal into the environment of the complete core of a 200 MW light-water reactor. This isn’t something that could actually, physically happen. But it was predicted that 3400 deaths and 43 000 injuries would result.
As it turns out, the RBMK-1000 reactor type had a unique design such that, under certain very unusual conditions, it was possible to disperse about 1/5th of the core of a 1000 MW reactor. Every other type of power reactor ever approved for civilian use is designed and constructed so that such an event is made impossible by the laws of physics ; but the Politburo wanted large reactors now, and when they were warned by the Chief Designer that the calculations weren’t complete, they thought it would be adequate to issue an operators’ manual saying “never for any reason do this”.
In other words, what happened at Chernobyl 38 years ago was beyond the worst nuclear accident that anyone thought could happen, or indeed, that could have happened anywhere else.
Now here’s the really important part. The United Nations Scientific Committee on the Effects of Atomic Radiation has made careful study of the people affected over those 38 years. Estimates of exposure, for instance, have been made for people exposed to the debris cloud, and their health has been compared to the health of unexposed populations from the same region, with the same demographics, diet, et cetera. Furthermore, the “liquidators”, a workforce of well over a hundred thousand people who were sent in to do cleanup, and received the largest allowable radiation dose before being pulled out, have been followed all that time.
The expected harms to human health have failed to appear.
Among the liquidators, for instance, it was confidently expected that, within about 10 years, a very large number of cases of leukemia would be seen, because this is the kind of cancer most likely to be caused by radiation. There should have been what epidemiologists call a large signal, a statistically unambiguous number of cases, several times larger than the number which would occur at random in an unexposed population. All these years later, we’re still waiting to see those cancers.
In face, Greenpeace and others have accused UNSCEAR of a cover-up, because the estimates of deaths and injuries keep getting revised downward in every successive report. Apparently they don’t understand how the scientific method works. Correlation does not necessarily imply causation, but the lack of correlation is very good evidence against causation.
Meanwhile, knowledge of the very real harms of fossil fuels, and of air pollution — which nuclear power plants do not produce — continues to mount.
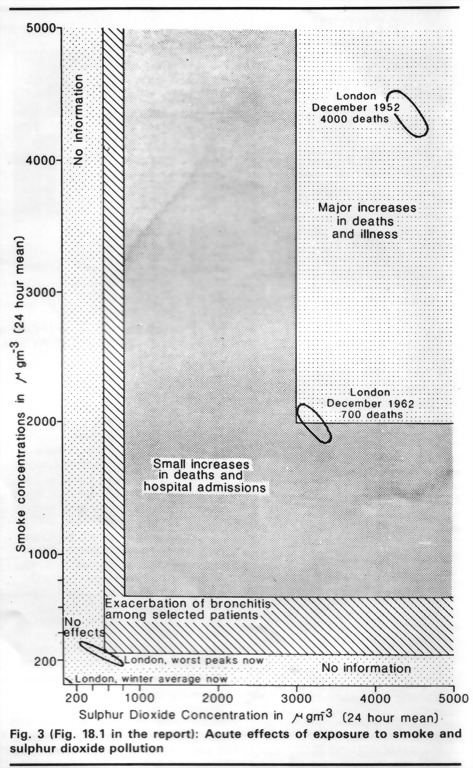
Civil nuclear energy has never caused any event comparable to the 1952 London smog, and the evidence of Chernobyl is that it cannot.
Oh hell yeah
2K notes
·
View notes
Text
Education
As more teens overdose on fentanyl, schools face a drug crisis unlike any other
Before the overdose, Griffin Hoffmann was a sophomore, about to lead his Portland, Ore., high school's tennis team. Sienna Vaughn was a junior in Plano, Texas, who participated in Girl Scouts and cheerleading. Laird Ramirez was 17 years old living near Charlotte and competing on his high school's wrestling team. He was rarely seen without his skateboard.
The teens thought they were taking prescription pills for pain and relaxation, drugs like Valium or Percocet, that they bought from friends or from social media. But the pills they took were counterfeits – they hadn't come from a pharmacy and it turned out they contained fentanyl, a potent, often deadly, synthetic opioid. Just 2 milligrams can kill you.
Griffin, Sienna and Laird's deaths are part of a grim crisis happening all across the country. Their stories, taken from local news reports, are among the dozens NPR reviewed, and they illustrate a new challenge for schools this fall.
"[Fentanyl's] infiltration into schools is certainly something that cannot be ignored," says Alberto Carvalho, the superintendent of the Los Angeles Unified School District. LAUSD is one of the largest districts to stock naloxone, a medicine that reverses opioid overdoses, throughout its schools.
"We cannot close our eyes. We cannot look the other way," he says.
Fentanyl was involved in the vast majority of all teen overdose deaths – 84% – in 2021, and the problem has been growing. According to the Centers for Disease Control and Prevention, fentanyl-related adolescent overdose deaths nearly tripled from 2019 to 2021. And nearly a quarter of those deaths involved counterfeit pills that weren't prescribed by a doctor.
Lauren Tanz, an epidemiologist who studies overdose prevention at the CDC, says a number of factors contributed to these alarming numbers.
"The combination of more easily available drugs – particularly highly potent drugs like fentanyl that are available via social media and through counterfeit pills – and a mental health crisis among adolescents that was exacerbated during the COVID-19 pandemic is resulting in an increase in overdose deaths among kids."
This academic year, education leaders are grappling with how to approach a drug use crisis unlike any they've seen before.
"If our students are having contact with these substances, considering the devastating implications and consequences," says Carvalho, "then we need to be active participants in the solution, and not necessarily shy away from it or punt it to somebody else because it falls outside of the realm of traditional education."
Schools can't do it alone
It's happening all across the country – from Tennessee to Texas; from Maryland to Oregon. In some cases, a single high school or school district has seen multiple fentanyl overdose deaths. School buildings have posters in the hallways memorializing students who have died. Social media posts and back-to-school messages from school staff include warnings and pleas to turn in pills students have bought online, "no questions asked."
In addition to stocking naloxone – often known by the brand name Narcan – schools have revamped their drug awareness and prevention programs. Some are promoting the use of test strips to help identify if a pill contains fentanyl, although the small paper tests can still be considered drug paraphernalia and are illegal in several states.
But Becky Pringle, president of the National Education Association, the nation's largest teachers union, warns schools are just one piece of the puzzle.
"We can't possibly do this alone. This is not a school crisis. This is a community crisis," says the former middle school teacher.
"So it's not just educators in schools. It's parents and families. It's the communities themselves. It's every level of government. We have to come together. Too often, the ills of society find the way to our schoolhouse doors, but the resources of society don't follow them."
There are multiple bipartisan pieces of federal legislation aimed at supporting schools in dealing with fentanyl, including one proposed bill that would give money to schools to stock naloxone and train teachers and nurses in updated drug education.
Mourning families are often leading the charge
Some families of students who have died have been frustrated with how schools are responding or say schools could do more. Of the 20 largest districts in the country, only five confirmed to NPR that they stocked naloxone in all of their schools last school year. And in schools across the country, drug education is ad-hoc, not standardized and oftentimes outdated. The 2021 National Survey of Drug Use and Health found only about 60% of surveyed 12-17-year-olds self-reported that they saw or heard drug or alcohol prevention messaging in school.
Avery Kalafatas, an 18-year-old from the Bay Area, says she knew nearly nothing about fentanyl until it killed her cousin, Aidan Mullin. He was like an older brother to Kalafatas; the two shared a love of the outdoors and camping. Mullin had an interest in agriculture, and a fondness for growing peppers and playing the guitar.
In November of 2020, Mullin, then 18, took what he thought was a Percocet. It contained a lethal dose of fentanyl. His death was a devastating blow.
"And it took me a while in my grieving process to obviously get past the shock and the sadness of it. But in that process, I was honestly pretty angry that this wasn't talked about more," she says.
Kalafatas began to educate herself about the synthetic opioid.
"As I became more aware of it through my cousin's death, I really saw a big need for more education, both among parents, and especially teens."
Kalafatas founded the nonprofit Project 1 Life with a mission to educate adolescents and foster youth-led conversations about fentanyl, the deadly and frighteningly ubiquitous opioid found in so many counterfeit pills. "This isn't like the drug crisis we were dealing with 20 years ago, it's a completely different ballgame," Kalafatas says.
A different ballgame because many students aren't intentionally seeking out the deadly drug they're overdosing on.
Ed Ternan, a father from Pasadena, Calif., runs the nonprofit Song for Charlie with his wife, Mary. They use social media to inform teens about fentanyl-laced counterfeit prescription pills.
He says the growing fentanyl crisis requires a new approach to how families and educators talk to students about drugs.
"We need to revive drug education in America. In a way, we need to Narcan drug education – we need to breathe life into it, bring it back," Ternan says.
He says they've learned from consulting with experts in youth mental health and drug education that the "just say no" message of the past isn't an effective way to communicate with teenagers. Instead, they craft fact-based messages they hope teenagers will actually pay attention to.
Rather than focus on "Don't do drugs, they might harm you," Song for Charlie's messaging is: "You're getting ripped off. These dealers advertising on social media do not care. They don't know you, they're not your friend, and they are lying to you about what they're selling you," Ternan explains.
That's what happened to Ternan's youngest son, Charlie.
"He was very much the calming influence...in our family," he says. "A very steady, level-headed guy with more of a subtle, dry sense of humor."
In May 2020, Charlie was on his college campus in northern California. He was weeks away from graduation, and was prepping for a job interview. He was also in pain. Ternan says his son had recently undergone back surgery.
Charlie purchased what he thought was a Percocet off of Snapchat. It contained fentanyl.
"He actually took it a couple hours before he was supposed to have a job interview on the phone," Ternan says. "And so he died very quickly in his room at his frat house waiting for the phone to ring at about four o'clock on a Thursday afternoon."
After his son's death, Ternan says most of the information about fentanyl he could find was buried on government websites and in a smattering of news articles.
"You can put that information in those places for the next 10 years, and Charlie and his friends would never have seen it because that's not where they are."
Where they are is on social media. Ternan and his wife funneled their grief into action; they founded their nonprofit and partnered with social media platforms to disseminate information about fentanyl.
Ternan says their messages also appeal to teenagers' strong social bonds. He's learned that telling teens to warn their friends about fentanyl is more powerful than stoking fear of their own harm.
This kind of awareness could save lives. The latest research from the CDC found there were bystanders present at two thirds of teen overdose deaths. Tanz, the CDC researcher, sees this as a potential opportunity for intervention and education.
"These are people that were nearby who could have intervened or responded to the overdose," she says. "It means we can educate family and friends to recognize warning signs ... and that might improve bystander response and prevent deaths."
Peer-to-peer conversations have also been central to Kalafatas' efforts at Project 1 Life. "Hearing it from someone that's not an adult, parent, or teacher... makes it much more real," she says.
"I think the Fentanyl crisis is an inflection point in our national conversation about drugs," Ternan explains. "It's forced us to look in the mirror and acknowledge our shortcomings and say we got to do better."
Both Kalafatas and Ternan want schools to use some of the lessons they've learned to educate students. With schools also struggling to address mental health, learning loss and so many other challenges, they say it's been an uphill battle.
But they also say it's a necessary one. Schools have the potential to reach millions of kids if they decide to talk to and teach students about the dangers of fentanyl.
"Having these conversations, and having them right, can be the difference between life and death," Kalafatas says. *Reposted article from KPBS by Elissa Nadworny and Lee V. Gaines on August 30, 2023
0 notes
Text
'German epidemiologists are warning of a summer wave of coronavirus infections, blaming in part mass gatherings such as the Barbenheimer double feature craze...
“It could be that we’re having a summer wave,” Timo Ulrichs an epidemiologist at the Berlin Akkon University of Human Sciences, told the news portal Spiegel, adding that the so-called “Barbenheimer effect” was capable of boosting the numbers.
Germany was among the countries where cinemagoers were encouraged to go to watch the blockbuster films Barbie and Oppenheimer as a double feature, in an effort to boost cinema attendance which has yet to recover since the pandemic. So far just under 4 million have seen Barbie, and more than 2.5 million Oppenheimer.
The idea of a Barbenheimer effect on the spread of the virus was first playfully mooted by the vaccine expert Peter Hotez of the National School of Tropical Medicine at the Baylor College of Medicine in Texas.
Suggesting on Twitter that it might be of concern, due to the millions of people surging to cinemas and spending hours in a windowless room together, he concluded: “We’ll probably never know since no one seems to be keeping track of such things any more.”...'
0 notes
Link
[ad_1] The Public Health Agency of Canada (PHAC) is deploying two epidemiologists to New Brunswick in September to support the province's public health team, at the request of New Brunswick's public health authority.The move follows a letter from a high-profile neurologist warning that a growing number of abnormally young patients are facing a rapid onset of neurological symptoms.Moncton neurologist Dr. Alier Marrero sent a letter to PHAC and New Brunswick public health in January, saying he was seeing an increase in the number of patients, and that some patients were in the "advanced stages of clinical deterioration."In a statement, PHAC confirmed its epidemiologists will work under the supervision of New Brunswick public health and conduct a "three-day scoping exercise that will include an on-site review of patient records that have been collected to date."It said the review of records will inform the next steps for provincial public health. The New Brunswick government did not respond to a request for comment regarding why it asked PHAC for help. Province closed investigation in 2022This decision to involve federal epidemiologists marks a reversal in the provincial government's position.In 2022, the New Brunswick government closed an investigation into a cluster of 48 patients experiencing neurological symptoms — a move The Guardian reported perplexed some federal scientists.An oversight committee appointed by the provincial government determined there is no mystery brain disease, and that the majority of patients in the cluster were misdiagnosed and ought to have been diagnosed with known diseases.The oversight committee cast doubt on Marrero's work, saying it "could not conclude that the main referring neurologist had sought second opinions."Marrero has become a fierce advocate for patients. In his January 2023 letter, he wrote to Canada's top public health official and the province of New Brunswick's chief medical officer, warning them the number of cases has grown from 48 to more than 147, claiming that some are as young as 17 years old.He wrote that some patients are experiencing "very advance evidence of neurodegenerative diseases," including dementia, severe pain syndrome, brain and muscle atrophy and more. "Some of these patients are, unfortunately, in advanced stages of clinical deterioration and near the end of life," he wrote. He also warned that some patients' blood work showed elevated levels for compounds found in herbicides such as glyphosate, and said more testing should be done to rule out environmental toxins, including the neurotoxin BMAA, which is produced by blue-green algae. "I believe there is an urgency to act promptly and use all means necessary to investigate and get to the root cause," he wrote in the letter. [ad_2]
0 notes
Text
Also preserved in our archive
by Suzanne King
The sometimes debilitating illness infects a third of people who come down with a case of COVID. Scientists and doctors are scrambling to understand and treat it.
Salam Kabbani wears a smile, and many of her sentences trail into laughter.
That tends to mask the fact that she got COVID-19 three years ago — and never got better.
The 34-year-old Overland Park pharmacist is one of 17 million Americans battling long COVID, an amorphous constellation of symptoms that scientists are only beginning to understand and most doctors are struggling to treat.
Kabbani faced months unable to work. For days at a time, she could barely get out of bed. Just taking a shower exhausts her. She gets dizzy with no notice. Her brain gets foggy. And if she pushes herself even a tiny bit too far, her body simply wilts and she is forced to climb into bed.
“The number of people that are like, ‘Oh, but you look fine,’” Kabbani said, a laugh bubbling to the surface. “Well, yeah, you know, I’m not hemorrhaging from my eyeballs. But I am very much disabled.”
With only 13.5% of adults opting to get the most recent COVID vaccine, a growing number of health care experts and patient advocates are sounding an alarm. The only sure way to avoid getting long COVID, which is believed to affect a third of people infected with the SARS-CoV-2 virus, is to avoid getting COVID.
An up-to-date vaccine, which some people skipped last year, too, is the best way to do that. But public health officials said they face strong headwinds in their efforts to share that message.
Pandemic fatigue and “anti-vax propaganda,” said Dr. George Turabelidze, Missouri’s state epidemiologist, stand in the way. Now Robert F. Kennedy Jr., a known vaccine skeptic, is expected to get a substantial role in Donald Trump’s new administration.
But people shouldn’t be lulled into thinking that COVID will be just like a cold, Turabelidze said.
“Some people — even with mild COVID,” he said, “develop long COVID.”
And long COVID, said Jenna Hopkins, an occupational therapist at University Health, “is ruining people’s lives.”
The U.S. Census Bureau’s most recent household pulse survey found 18.6% of Missouri adults and 16.5% of Kansas adults said they have experienced long-COVID symptoms. Nationally, close to 45 million of the country’s 250 million adults said they have had long COVID at some point.
The illness can take hold of anyone who comes down with COVID, no matter their age, gender or overall health. It can linger for months or years. It can be relatively mild or completely disabling.
And while the severity of an initial COVID infection doesn’t seem to influence whether someone gets long COVID, the number of times a person comes down with COVID could be a factor. In other words, every time you get the virus is another chance to end up with stubborn health problems.
“It gets really ugly very quickly,” said Arijit Chakravarty, a COVID researcher in Massachusetts, “because what it means is that if you wait long enough, everyone is at risk of getting it.”
In bed for a year If Kelly Meiners could scream from the rooftops to warn people to protect themselves against the virus, she would.
The 49-year-old college professor and marathon runner came down with a relatively minor case of COVID in 2021. She stayed home from the office, even though her symptoms felt like nothing more than a bad cold.
That quickly changed in the weeks after her initial infection cleared up.
“Over the next year, I lay in bed,” said Meiners, who chaired the physical therapy department at Rockhurst University. “I had no idea what was going on with me. I felt I was severely drugged and drunk. I couldn’t make sense of anything. I couldn’t think straight.”
In an effort to fend off debilitating migraines and persistent seizures, Meiners spent most of her time in a dark room, wearing noise-canceling headphones and dark glasses. She couldn’t hold a pen or a fork. She could no longer read or walk.
And when she went to a doctor in Kansas City, she was told that it was all in her head, that she should exercise. As an athlete, Meiners wanted nothing more. So her husband bought a recumbent bike. She strapped herself in and pushed herself until the seizures began.
She was told exercise would make her better. Now she understands it only made her worse.
Finally, a year after falling ill, a friend of a friend got Meiners an appointment at Mayo Clinic in Minnesota. The doctor there immediately knew what was wrong.
“I just cried,” she said. “It wasn’t because there were so many things wrong with me. It was because they finally believed me.”
Finding someone to help Unfortunately, long-COVID patients often have a difficult time finding someone who can help them. And someone who will believe they are sick.
Doctors didn’t learn about COVID in medical school — let alone long COVID. And they work in a system where they need to document their care for insurance purposes. Long COVID is so new and varied in the ways it shows up, it barely has an agreed-upon clinical definition.
So it’s no wonder some doctors are sending patients away without care or telling them their symptoms are in their heads.
“I don’t think it’s coming from a place of malice,” Kabbani said. “It’s truly just a lack of awareness and understanding and being burned out.”
Now that Kabbani’s health is improved, she spends the extra energy trying to help educate the world about the disease. She has written a book about her own journey, and she and Hopkins, the University Health occupational therapist, are creating a podcast.
Kabbani, who works as an infectious disease pharmacist at Olathe Health, is speaking at continuing medical education events, trying to bring information about long COVID directly to doctors and nurses.
“What I hope to drive home to these providers,” she said, “is that the symptoms are very strange, and they fluctuate. That’s why it may seem like it’s absolutely in their heads. But it’s absolutely not.”
Research theories about long COVID This summer, long COVID earned a consensus case definition from the National Academies of Sciences, Engineering and Medicine. Someone has the chronic condition, according to the new definition, when health problems are present for at least three months after a COVID infection.
Those problems can affect one or more organ systems, according to the definition, as “a continuous, relapsing and remitting or progressive disease state.” And a person can meet the definition by having just one or multiple symptoms, from the list of 200 included in the definition.
“If people just had lung problems,” said Dr. Adnan I. Qureshi, a professor of neurology in the University of Missouri School of Medicine, “it would be much easier to study.”
The National Institutes of Health launched a nationwide research program in 2021 with a $1.15 billion investment. In February, the agency announced it would spend another $515 million over the next four years.
The program includes dozens of studies and drug trials across the country, including studies at the University of Kansas Health System and Children’s Mercy Hospital.
U.S. Sen. Bernie Sanders of Vermont has introduced legislation that would invest another $1 billion a year for a decade in research, provider education and public education.
Scientists have several theories about how long COVID strikes, and they are starting to believe that there may be more than one answer.
For example, in some cases, the immune system, which has been activated by the initial viral infection, simply doesn’t turn off once the virus is gone. That means a person’s own immune system can damage the body.
Another theory is that when someone has long COVID it could be because they still have traces of the virus in their body.
Another possibility, scientists said, is that the virus damages the circulatory system, which could explain why symptoms are so varied and in so many organs.
Pacing to survive Doctors are finding that some patients get better over time without treatment. But others need to manage symptoms.
When patients come to see him at University Health’s Center for COVID Recovery, Wesley Strouts, a nurse practitioner who specializes in internal medicine, looks for the symptoms he can treat that will provide some relief. Sometimes he finds different diagnoses to explain what’s happening. Often, he refers patients to Hopkins, the occupational therapist who has built a specialty out of helping patients manage symptoms.
For many patients, Hopkins said, the best approach is to follow “pacing protocols.”
“Sometimes the treatment is the cure,” she said. “When people are able to manage their symptoms … sometimes their symptoms will start to dissipate as long as they are continuing to be very careful to avoid triggering activities.”
For Amanda Finley, 47, who first came down with long COVID after a 2020 bout with the virus, pacing looks like this: Work. Uber home. Straight to bed. Often her weekends must be entirely devoted to sleeping so she can face another work week.
It’s better than the alternative Finley knew in 2021 when she was living in a tent at Weston Bend State Park because she couldn’t work and had no money for rent. The Independence woman couldn’t see her 11-year-old son for months.
But even when Finley had energy for nothing else, she stayed connected with other people dealing with the illness. Early in her diagnosis, she formed a Facebook group for COVID long haulers that today has 16,000 members around the world.
It helps her know she’s not alone. And it could be a tool in science’s effort to solve mysteries surrounding the illness. Finley tries to put researchers in touch with the people in the group.
“The patients are the experts with long COVID,” she said. “We’re the ones going through the jungle with a machete making the path.”
Telling her story Since her long-COVID symptoms began, Meiners has missed graduations, kids heading off to college, holidays, family vacations and almost every other part of her life.
She just passed the third anniversary of her initial COVID infection, and she still spends 90% of her day on the sofa or in bed. Meiners needs an electric wheelchair to navigate her Leawood home, but with the help of more than 20 prescriptions and pacing strategies to avoid flare-ups, she can have moments with her husband and three kids.
And Meiners has found a small amount of peace in making art, something she’d never tried before this. Her paintings, which tell her long-COVID story, are on display at the Lenexa City Center Library. They have been shown in galleries around the city.
It may not be screaming from the rooftops, Meiners said. But, right now, it’s the best she can do.
#mask up#covid#pandemic#public health#wear a mask#covid 19#wear a respirator#still coviding#coronavirus#sars cov 2#long covid
98 notes
·
View notes
Text
Canons
Consider the canon reserves officially open! Below you’ll find a list of those available, along with a brief description for each. These will be first come, first serve, so make sure you let us know via an ask if you would like to snag one of these positions.
Edit: For now, everyone will have the opportunity to reserve 1 canon slot each!
For an up-to-date list of which canons have already been claimed, please refer to our Reserves Page.
Decoder Hint 3: C
The Community Chief: Former Advisor to the Mayor Community Leaders
The Agriculturalist: taught the community how to farm
The Teacher: started classes for children
The Cop: tries to keep the peace
The Soldier: trained the community in survival
The Engineer: keeps what appliances still run, running
The Hunter: trained the community to hunt and fish
The Oracle: warns the community of things that may come to pass
Power Plant Operator: keeps the power plant and dam running as best they can
Power Plant Mechanical Engineer: aids the operator in the event of malfunction
Audiologist: studies the blast, the hum, and the formless
Paranormal Investigator: perpetuates wild theories about the formless and the source of the blast and hum
Doctors
Epidemiologist
General Practitioner
Veterinarian
Numbers Stations Runners (5 Slots)
Scouts (5 Slots)
Guards
North Quadrant
East Quadrant
South Quadrant
West Quadrant
Northeast Quadrant
Southeast Quadrant
Northwest Quadrant
Southwest Quadrant
#liminal buzz#dystopian#post apocalyptic#horror#jcink#jcink rp#jcink premium#jcink buzz#liminal lore
1 note
·
View note
Text
Additionally, a lot of the schools we have for early language learning aren't accessable for a number of reasons.
Fair warning, everything below is personal experience. I speak almost entirely English, I don't travel, and I have a serious disconnect with the non-white-american side of my heritage. Less personal stuff further down.
↓
My sibling and I were homeschooled for several years (starting at pre-k aged to 2nd/3rd grade age), and when my older sibling got sent off to school(6yo), it was to a Mandarin Immersion School in our area because our (now-permanently-out-of-the-picture) father is a Chinese immigrant and it was decided to try that, and if it went well, I'd be going the next year. (Funnily enough he didn't want me or my sibling or our mother learning Cantonese or Mandarin, and not for pleasant or heart-warming reasons.)
It did not go well.
(In fact it went so badly because of abuse in the school system, racism, and ableist bullshit, that my sib got pulled so fucking fast with such a public fuss, that in the coming years that school apparently did a total overhaul to change that. Comparatively, one of my best friend's friends went to a French Immersion School and never had any issues and now, knows French. I on the other hand (public school from 7/8 on up) didn't have an opportunity outside of things at home- and with a recently divorced mother, scrambling to get work and take care of two kids & court, and a P.O.S old man, there really wasn't time for me or my sibling to learn more.)
My mom taught us some Latin, she'd taken Latin in school, and ASL, having learned a lot for/from her deaf friend in high school, and pre-divorce we'd been learning some Mandarin when my father wasn't around.
Now flash forwards, I don't start learning a new language through school until I'm in middle school at 13. I take French for a year. I switch to Spanish in high school a year later, end up with a really bad teacher (no srsly, she taught French and Spanish and kept switching to French lessons, so many people had issues with her teaching Spanish) and so the next year I don't sign up for a school language class, start trying to learn Italian on my own. Then I end up starting French again in 11th grade because most colleges required at least 2 years of a non-english language classes.
I take two years of French, and in the last three months of my senior year there's a Global Pandemic (please note; it isn't over, check with your local epidemiologists for more info). Real wrench in my life plans, y'know?
So, now, three years post hs graduation, the biracial child of an immigrant, and I know a handful very basic words in (textbook) Spanish, I remember French at the weirdest damn times (but can barely speak any of it), and my Cantonese and Mandarin are basically non-existent (Cantonese because my father's side is immigrated from Hong Kong, Mandarin bc that's the "what everyone speaks" in said relatives words).
Now, in terms of travel? I've left my State (I live in the states) twice. Both times add up to less than 12 hours out of state, and less than an hour past the state border each time.
I grew up and I'm still poor, like a huge portion of Americans. I've never been on a vacation outside of school mandatory ones. I've never left the U.S, I don't even have a passport and I don't drive.
My mom? Grew up poor. Vacations aren't a thing for people below a certain income. But bc of where I grew up, all of my friends could afford to go on a family trip to Florida or NY or Cali or wherever every year or two, most of my friends now can and have travelled out of state, even out of country, on a semi-regular basis.
But most of those friends grew up in a 2-income family, remarried/non-divorced households that were already decently well off.
To the less personal stuff.
↓
Every person above has fucking point though. The States could, and quite frankly should, be doing better, should be doing more.
But racism and classism and sexism are all still rampant, frothing at the mouth, vicious and blatant.
Our transportation in-country is horrid. The cost to leave the country is tremendous, starting with the cost of passports to whether or not taking a week off will cost you your job.
And there's a shit ton of clueless, rich Americans who go out there and Americanism all over everything in the most miserably rude, senseless fashion they can, most of them not even realizing it.
There's a ton of faults, and a whole lot of cluelessness that breeds ignorance and insult, on both sides.
Europeans don't, for the most part, understand just how split up the States are, culture, language, etc. Because each state, each region, is vastly different from geography to mannerisms. They don't get just how easy it is for them to travel, their schools promote learning multiple languages. Our schools, our governments? They don't. Well. They do if you're rich, white, and cis. Then it's a "bonus in your job applications." But if someone who isn't one or any of those speaks two or more languages, then it's a count against them.
Again: racism, classism, sexism.
But, Americans also aren't "cultureless." I'm from the Midwest. That's very different from the central plains (now often lumped in w/ the MW) or from the East, South, West, etc. The cultures between regions are incredibly different- and it varies more-so state to state. You can't say NY and NJ are the same, just like MN and WI aren't. CA isn't WA state, and KS, AZ, and GA can't even be compared, region or state.
It's just that the predominant majority of American Tourists come from the same middle-to-upper class, white, nuclear-family backgrounds and their ingrained ignorance paired with the European VP (that we hear the most) is that All Americans Have The Same Opportunities and Upbringings leads to a lot of bullshit fuckery.
europeans will really look americans dead in the eye and say they’re so uncultured because they never leave the us
#i ramble a bit#so if you read thru it all congrats#also srry for errors im dyslexic 👍#no actually i ramble a lot
4K notes
·
View notes
Text
New Study Reveals Alarming Cancer Risk in Meat Consumption

According to new research, the data is insufficient to support advising people to consume less beef and pork. Critics claimed that the findings "erode public trust."
What the Research Says?
Because of worries that these foods are connected to heart disease, cancer, and other illnesses, public health experts have long advised Americans to reduce their consumption of red meat and processed meats. To know about the Cancer Risk in Meat we are discussing a lot facts on this post. But in a surprising turn of events, a group of researchers from around the world came to the conclusion on Monday that the advice—which forms the basis of practically all dietary recommendations—is not supported by reliable scientific data. Bradley Johnston, an epidemiologist at Dalhousie University in Canada and the head of the team that published the new research in the Annals of Internal Medicine, stated that "the certainty of evidence for these risk reductions was low to very low."
The New Findings
The new findings, which rank among the largest such reviews ever performed, could affect nutritional advice in the future. They highlight a number of unsettling issues regarding dietary recommendations, nutritional research, and the kind of criteria that should be applied to these studies. Public health researchers have already criticized them harshly. The results and the journal that published them have drawn criticism from the American Heart Association, the American Cancer Society, the Harvard T.H. Chan School of Public Health, and other organizations.
Some More Reviews
In a statement, academics at Harvard warned that the findings "harm the credibility of nutrition science and erode public trust in scientific research," and several called for the journal's editors to postpone publication completely. -Research.” Dr. Frank Sacks, former chair of the American Heart Association's nutrition committee, called the research "fatally flawed." Physicians Committee for Responsible Medicine, an organization that promotes a plant-based diet, filed a petition against the journal with the Federal Trade Commission on Wednesday. Particularly beef is more than simply another food item; it served as a beloved emblem of post-World War II wealth and was firmly placed in the middle of the American dinner plate. But from the middle of the 1970s, consumption of beef has progressively decreased, mostly being replaced by poultry as worries about its health implications have grown. The Harvard T.H. Chan School of Public Health in Boston's nutrition department chair, Dr. Frank Hu, stated that red meat was once a sign of high socioeconomic class, but that this was changing. He pointed out that Americans today consume less red meat the more educated they are.
The Final Take
The new papers are the result of three years of effort by a team led by Dr. Johnston, which included 14 researchers from seven different nations and three community leaders. The studies were conducted without any outside support, and the scientists disclosed no conflicts of interest. Although supporters of popular high-protein diets are likely to be pleased with the latest findings, they are almost certain to increase public concern over dietary recommendations that seem to alter every few years. The findings add to a long list of startling dietary changes affecting salt, lipids, carbohydrates, and more. Read the full article
0 notes
Text
Dan’s jab order: All authorised workers must be vaxed
Dan’s jab order: All authorised workers must be vaxed
Premier Daniel Andrews has ordered every authorised worker – from farmers to police officers – to get a first dose of a Covid vaccine by October 15 “if they want to continue working”. Hundreds of thousands of Victorians will be forced to get vaccinated against Covid “if they want to continue working”, Premier Daniel Andrews has announced. Mr Andrews on Friday said every Victorian worker on the…
View On WordPress
#Andrew Henshaw#australia#Australia and New Zealand#Brimbank#coronavirus article#Daniel Andrews#Data analyst#epidemiologists warning numbers#growing transmission rate#hotspot areas#jab doses#Jeroen Weimar#Juliette O’Brien#leading epidemiologists warning#media conference#Melbourne#Melbourne University#Mitch Clarke#Nancy Baxter#New South Wales#Oceania#Olivia Jenkins#Paul Jeffers#Pfizer Inc#Sarah Matray#staff shortage#tipping point#vaccination efforts#value offer#Victoria
0 notes