#delta coronavirus variant
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs




Fun Fact
Tumblr has a low social media market share in South America.
Text
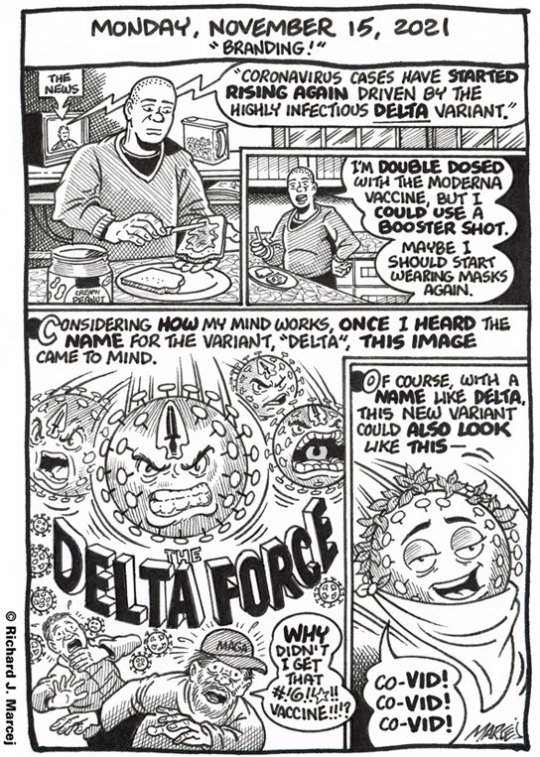
Daily Comic Journal: November 15, 2021: "Branding!"
Even though there’s this new strain of the Covid virus, what a difference a year makes! Last November people were staying at home, masked when they did leave their homes and everyone was getting prepared for a lonely Thanksgiving. Now, thanks to the vaccines it doesn’t feel as dire and scary. Yes, even with the Delta Force bursting through! Still would like a booster shot though.
View On WordPress
0 notes
Note
Hello! First of all, thank you for the wonderful content! It's a real joy, and an enrichment, food for both the brain and the heart! I was wondering if through your treasures, you could find some writing notes/words/concepts/vocabulary relating to genetic engineering? Like...creating a virus, and a vaccine for it, modifying the virus so it has certain specific effects.... Thank you in advance!
Writing Notes: Virus & Vaccine
References How Viruses Work; Replication Cycle; Mutation, Variants, Strains, Genetically Engineering Viruses; Writing Tips; Creating your Fictional Virus & Vaccine
Virus - an infectious microbe consisting of a segment of nucleic acid (either DNA or RNA) surrounded by a protein coat.
It is a tiny lifeform that is a collection of genes inside a protective shell. Viruses can invade body cells where they multiply, causing illnesses.
It cannot replicate alone; instead, it must infect cells and use components of the host cell to make copies of itself. Often, a virus ends up killing the host cell in the process, causing damage to the host organism.
Well-known examples of viruses causing human disease include AIDS, COVID-19, measles and smallpox. Examples of viruses:
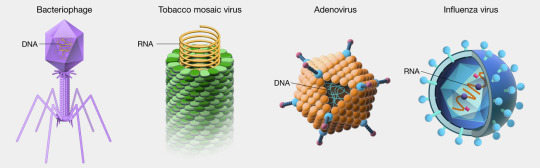
Viruses are even smaller than bacteria and can invade living cells—including bacteria. They may interfere with the host genes, and when they move from host to host, they may take host genes with them.
Bacteriophages (also known as phages)—viruses that infect and kill bacteria.
Size differential between virus and bacterium
Viruses are measured in nanometers (nm).
They lack the cellular structure of bacteria, being just particles of protein and genetic material.
How Viruses Work
Viruses use an organism’s cells to survive and reproduce.
They travel from one organism to another.
Viruses can make themselves into a particle called a virion.
This allows the virus to survive temporarily outside of a host organism. When it enters the host, it attaches to a cell. A virus then takes over the cell’s reproductive mechanisms for its own use and creates more virions.
The virions destroy the cell as they burst out of it to infect more cells.
Viral shedding - when an infected person releases the virus into the environment by coughing, speaking, touching a surface, or shedding skin.
Viruses also can be shed through blood, feces, or bodily fluids.
Virus Replication Cycle
While the replication cycle of viruses can vary from virus to virus, there is a general pattern that can be described, consisting of 5 steps:
Attachment – the virion attaches to the correct host cell.
Penetration or Viral Entry – the virus or viral nucleic acid gains entrance into the cell.
Synthesis – the viral proteins and nucleic acid copies are manufactured by the cells’ machinery.
Assembly – viruses are produced from the viral components.
Release – newly formed virions are released from the cell.
Mutations, Variants, and Strains
Not all mutations cause variants and strains. Below are definitions that explain how mutations, variants, and strains differ.
Mutation - errors in the replication of the virus’s genetic code; can be beneficial to the virus, deleterious to the virus, or neutral
Variants - viruses with these mutations are called variants; the Delta and Omicron variants are examples of coronavirus mutations that cause different symptoms from the original infection
Strains - variants that have different physical properties are called strains; these strains may have different behaviors or mechanisms for infection or reproduction
Genetically Engineering Viruses
Using reverse genetics, the sequence of a viral genome can be identified, including that of its different strains and variants.
This enables scientists to identify sequences of the virus that enable it to bind to a receptor, as well as those regions that cause it to be so virulent.
Vaccine - a special preparation of substances that stimulate an immune response, used for inoculation
Vaccines & Fighting Viruses with Viruses
Common pathogenic viruses can be genetically modified to make them less pathogenic, such that their virulent properties are diminished but can still be recognized by the immune system to produce a robust immune response against. They are described as live attenuated.
This is the basis of many successful vaccines and is a better alternative than traditional vaccine development which typically includes heat-mediated disabling of viruses that tend to be poorer in terms of immunogenicity.
Viruses can also be genetically modified to ‘fight viruses’ by boosting immune cells to make more effective antibodies, especially where vaccines fail. Where vaccines fail, it is often due to the impaired antibody production by B-cells, even though antibodies can be raised against such viruses – including HIV, EBV, RSV & cold-viruses.
Related Articles: Modified virus used to kill cancer cells ⚜ Genetic Engineering ⚜ Engineering Bacterial Viruses ⚜ Benefits of Viruses
A Few Writing Tips
As more writers look to incorporate infectious diseases into their work, there are quite a few things writers should keep in mind:
Don’t anthropomorphize. Really easy to do, but scientifically wrong. Viruses don’t want to kill you; bacteria don’t want to infect you; parasites don’t want to make your blood curdle. None of these things are big enough to be sentient to want to do anything. They just do it (or don’t do it).
Personal protective equipment. This includes wearing gloves, lab coats, safety glasses, and tying your hair back if it’s long. It is the same as Edna Mode’s “no capes.” Flowing hair looks cool all the way to the explosive ball of flames that engulfs someone’s head.
Viruses are small. You can’t see viruses down a normal microscope—they need a special microscope called an electron microscope. These are highly specialized and take a long time to make the preparations to be able to see the virus. Normally viruses are detected by inference—measuring part of them using an assay that can amplify tiny amounts of material, for example PCR.
Viruses don’t really cause zombie apocalypses.
Vaccines work. But they take time. The best vaccine in the world will still only prevent infections two weeks after it is given. Drugs are quicker, but still take some time. But the good news is an infection is not going to kill you (or turn you into a zombie) quickly, so they both have time to work.
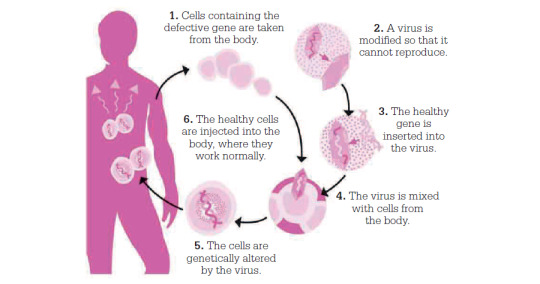
Scientists use viruses as a vector to introduce healthy genes into a patient’s cells:
Your Fictional Virus & Vaccine
When creating your own fictional virus, research further on the topic and consider choosing a specific one as your basis/inspiration.
Here's one resource. For some of them, you'll need a subscription to access, but those that are available give you a good overview of the virus, as well as treatment options.
You can do the same for creating your fictional vaccine:
Here's one resource. And here's one on vaccine developments.
Sources: 1 2 3 4 5 6 7 8 9 10 11 12 13 ⚜ Writing Notes & References
Lastly, here's an interesting article on how science fiction can be a valuable tool to communicate widely around pandemic, whilst also acting as a creative space in which to anticipate how we may handle similar future events.
Thanks so much for your kind words, you're so lovely! Hope this helps with your writing. Would love to read your work if it does :)
#writing notes#virus#vaccine#writeblr#dark academia#spilled ink#writing reference#writing prompt#literature#science#writers on tumblr#creative writing#fiction#novel#light academia#lit#writing ideas#writing inspiration#writing tips#science fiction#writing advice#writing resources
127 notes
·
View notes
Note
I'm sorry I'm sending so many asks. I've been struggling like this for a year now, and it's barely gotten easier, but you've often been a good help with my anxiety. I really appreciate everything you do. It's hard to have hope.
I've had a really bad moment again recently. I have to be honest, the worst thing, that makes me the most anxious out of everything else, is COVID. Because it feels like nobody is paying attention, and that there is no good news. There is never any good news. COVID is always the catalyst for the worst of my anxious slumps. It's really bad. COVID is very, very scary. If you somehow have anything for that, I'd be thankful. Often I've only been able to set my heart on nasal vaccines, or next gen vaccines in general, but they're not going fast enough whatsoever.
I'm sorry, again. I don't want to try and treat you like a therapist. I just trust you. If this is too overwhelming, you can just delete it, but if you do, I'd like to know. Just so I'm not waiting for it to be answered.
I just ravaged through someone's doomy collapse blog, again, after stumbling on it in my rising anxiousness, and it was not good. I think I'm clearly too open-minded of a person to some degree, and I feel so pulled around by information that I see. I don't want to be placated, out of the loop, or lied to, but I don't want to feel hopelessly depressed. Everything is too complex. I feel like I've been through this maze, top to bottom, over and over again, and again. I just wish I knew how much truth their words held, or anyone else's words held.
And I wish we were all masking, at the very least. I'm holding myself back from swearing. I don't know if you'd have a good way to counteract general "collapse" thoughts, either. But that's also a thing.
<3 I'm touched by your trust.
I just found some good news about COVID - the first genuinely good covid-related news article I've seen in a while, instead of all of the "ah but young abled people are fine!" bs - and remembered this ask.
"As new varieties of the coronavirus took center stage during the COVID-19 pandemic, the odds of developing long COVID dropped. Those who were vaccinated against the virus saw the biggest plunge over time.
For every 1,000 unvaccinated people, 104 developed long COVID up to one year after an infection during the pre-delta phase of the pandemic. That fell to 95 per 1,000 during the delta variant’s era and 78 during omicron’s reign. Among vaccinated people, just 53 out of 1,000 developed long COVID up to a year after infection during delta and only 35 during omicron, researchers report July 17 [2024] in the New England Journal of Medicine.
The study of U.S. Department of Veterans Affairs Health Care System data looked at people who had a COVID infection from March of 2020 — the month the pandemic began — to the end of January in 2022. The researchers, from the Veterans Affairs St. Louis Health Care System, compared the rates of long COVID during three phases of the pandemic among those who had and had not gotten vaccinated...
A comparison of omicron infections with infections from prior eras found that 72 percent of the drop in the long COVID rate during omicron was attributable to vaccines. The remainder was due to changes in the virus and improvements in medical care and the use of antiviral treatments during the omicron phase.
Even with the steep decline in the occurrence of long COVID for vaccinated people, there is still a risk, the researchers write. With “the large numbers of ongoing new infections and reinfections, and the poor uptake of vaccination,” they continue, this “may translate into a high number of persons” with long COVID."
-via ScienceNews, July 17, 2024
--
Masking continues to be important. The virus continues to be a problem. But especially given the decline in masking, I'm really encouraged to see this news. Because long covid IS scary. And I'll take any good news on this front that I can get.
It's especially encouraging because it shows how much staying on top of your vaccinations really does matter and really can prevent long covid.
I'm also really hopeful (though I don't have a related background and have no idea how realistic my hopes are) that this trend has been continuing past the end of the study (2022).
#dyingpleasehelp#covid#long covid#covid 19#covid isn't over#coronavirus#pandemic#covid19#epidemiology#virology#good news#hope
207 notes
·
View notes
Text
Reference archived on our website (Thousands of reference, news reports, and more! Daily updates!)
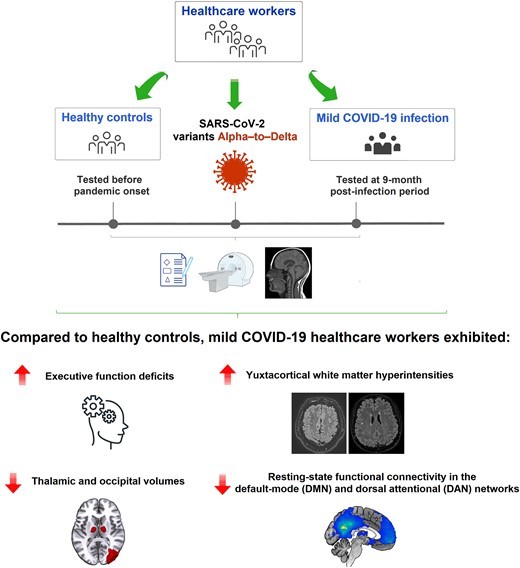
Yet another showing that even a mild infection leads to lasting cognitive impacts. Mask up. Stay safe out there.
Abstract Severe acute respiratory syndrome coronavirus 2 infection often involves the nervous system, leading to cognitive dysfunctions, fatigue and many other neurological signs that are becoming increasingly recognized. Despite mild forms of the disease accounting for most cases worldwide, research on the pathophysiology driving mild coronavirus disease 2019 (COVID-19) has received little attention. In this respect, recent evidence has pointed out that around 30–40% of non-critical, mild-to-moderate severity COVID-19 survivors may display cognitive disturbances several months post-illness. Hence, the impact of COVID-19 on the brain structure and function, through potential neuropathological mechanisms underpinning cognitive alterations in post-mild COVID-19 infections, remains largely unexplored. This retrospective multicentre observational cohort study, entirely based on a healthcare worker sample (n = 65; 55% females, aged 21–61), investigated the cognitive status and the structural and functional brain integrity among non-hospitalized individuals who developed mild COVID-19 symptoms during the occurrence of severe acute respiratory syndrome coronavirus 2 variants Alpha to Delta, compared with healthy controls tested before the pandemic onset. All evaluations were performed at an average of 9-month follow-up post-infection period. Participants completed a comprehensive neuropsychological assessment and structural and functional MRI exams. Radiological inspection sought to detect the presence of white matter hyperintensities on axial fluid-attenuated inversion recovery images. Global and regional grey matter integrity assessment, analysing changes in grey matter volumes and cortical thinning, and functional connectivity alterations of resting-state brain networks were also conducted. Regression analyses tested the relationships between the presence of specific cognitive impairments and potential structural and functional brain findings. Our results revealed that clinical, cognitive screening and neuropsychological examinations were average between both groups, except for specific impairments related to executive functions in the mild COVID-19. Compared to healthy controls, mild COVID-19 subjects exhibited increased juxtacortical white matter hyperintensities, thalamic and occipital volume loss and diminished resting-state functional connectivity involving the left precuneus and cuneus in default-mode network and affecting the right angular gyrus and left precuneus in the dorsal attentional network. Reduced thalamic volume was the only variable selected in the final model explaining the observed executive function impairment in mild COVID-19. The presence of cognitive, structural and functional brain abnormalities over time suggests that the action of widespread neurovascular and inflammatory phenomena on the nervous system might also occur in mild forms following COVID-19 infection rather than permanent brain damage linked to the direct or indirect action of the virus. Our findings emphasize the need to pay attention to the long-term brain-related consequences of mild COVID-19 infections during the original stream.
#mask up#covid#pandemic#public health#wear a mask#covid 19#wear a respirator#still coviding#coronavirus#sars cov 2#long covid
43 notes
·
View notes
Text
Hopeful covid news for once!
"In total, the team obtained six antibodies that could neutralize multiple coronaviruses, including COVID-19, its variants Alpha, Beta, Gamma, Delta and Omicron, the original SARS virus, along with multiple other animal coronaviruses transmitted from bats and pangolins...
The researchers found that the most powerful antibody, named E7, was able to neutralize both SARS and COVID-19, animal sarbecoviruses, as well as new COVID-19 variants, such as Omicron XBB.1.16.
E7 was shown to target a region of the coronavirus’ spike protein and blocked the shape-shifting process the virus requires to infect cells and cause illness, the study notes.
“The (neutralizing) potency and breadth of the E7 antibody exceeded any other SARS-related coronavirus antibodies we’ve come across,” said Chia.
“It maintained activity against even the newest Omicron subvariants, while most other antibodies lose effectiveness.”The researchers found that the most powerful antibody, named E7, was able to neutralize both SARS and COVID-19, animal sarbecoviruses, as well as new COVID-19 variants, such as Omicron XBB.1.16.
E7 was shown to target a region of the coronavirus’ spike protein and blocked the shape-shifting process the virus requires to infect cells and cause illness, the study notes.
“The (neutralizing) potency and breadth of the E7 antibody exceeded any other SARS-related coronavirus antibodies we’ve come across,” said Chia.
“It maintained activity against even the newest Omicron subvariants, while most other antibodies lose effectiveness.”
154 notes
·
View notes
Text
SARS-CoV-2, or Severe Acute Respiratory Syndrome Coronavirus 2, is a novel coronavirus responsible for the global COVID-19 pandemic. It is a positive-sense, single-stranded RNA virus belonging to the genus Betacoronavirus within the family Coronaviridae. The virus is zoonotic in origin, with genetic similarities to bat coronaviruses suggesting it emerged from such a source. SARS-CoV-2 primarily spreads through respiratory droplets and aerosols, making close contact a significant risk factor for transmission. It enters human cells by binding to the ACE2 receptor, a protein found on the surface of various cell types, particularly in the respiratory tract.
The virus causes COVID-19, a disease with a wide range of symptoms, from mild respiratory issues to severe complications like acute respiratory distress syndrome (ARDS). Common symptoms include fever, cough, fatigue, and loss of taste or smell, while severe cases may lead to pneumonia, organ failure, or death. SARS-CoV-2 has demonstrated a remarkable ability to mutate, leading to the emergence of variants with increased transmissibility or immune evasion capabilities. These variants, such as Delta and Omicron, have posed challenges to public health efforts and vaccine efficacy.
Efforts to combat SARS-CoV-2 have focused on vaccination, public health measures, and antiviral treatments. Vaccines targeting the spike protein of the virus have been instrumental in reducing severe disease and mortality. Preventive measures like mask-wearing, social distancing, and improved ventilation have also played a crucial role in controlling the spread. Despite advancements, SARS-CoV-2 remains a significant public health concern, with ongoing research aimed at understanding its evolution and developing more effective interventions.
#art#drawing#illustration#sketch#artwork#artist#virus#covid#covid 19#pandemic#epidemic#coronavirus#sars cov 2#disease#illness#sickness#viral
3 notes
·
View notes
Text
I did not really like this book "immunity index" by sue burke. the premise was too similar to real life and then the way it played out felt completely unrealistic. I mean, a deadly coronavirus with a delta variant that heightens racism against Chinese people due to unfounded suspicions that it was bioengineered in China? that's not even science fiction, that just happened in real life. ms burke says she started the novel before the covid pandemic and finished it "as the scope of the disaster was becoming clear." why didn't you change it then. feels almost tasteless
then it's like, in the book the US is significantly more fascist than it is irl with some people having been formally demoted to second class citizens and losing their right to vote, and political dissidents are being rounded up openly. actually that is happening rn, fuck this. anyway in the book there's a rebel group who refer to themselves as "the mutiny" and they were planning a mass protest for the day that just happens to coincide with the outbreak of the coronavirus. but almost everyone in the story is a good guy on the side of the mutiny (even the shitty roommate! even the politician dad!) or just a nasty evil person. there's one morally ambiguous character and one guy who says "listen I'm with you spiritually but I can't afford to lose my job"
it's not like that! in real life your coworker who's never been anything but kind and helpful to you voted for trump, your beloved grandma is a lifelong republican, the governor who did amazing things for education and childcare signed an anti-trans bathroom bill. people are complex. even in a life or death political situation you will see people who are too afraid of putting themselves in danger to help others, or who are somehow on the fence about an issue that seems cut and dry to you. I hate to say it but I think the number of people who will openly join the side of moral good is lower than you would hope, especially when the moral bad has an army
if it was a more fantastical setting maybe the black and white morals wouldn't get me as much. I mean I'm not mad star wars is about the heroic rebels vs the evil empire. but despite having futuristic technology this book was way too close to reality to pull that off. maybe that was the point, that it's a comforting fantasy to imagine things working out so neatly? but it didn't comfort me
3 notes
·
View notes
Text
How the innate immune system manages to cope with antibody resistant SARS2 varieties
December 17, 2024 Radagast
"So, as I have been documenting over the past few years now, we’ve seen a situation in which the new coronavirus, SARS-COV-2, become forced to evolve first into increasingly infectious variants (Alpha, Delta) with higher ACE2 affinity and then into highly antibody evasive variants (the Omicron variants). This then results in a population that has a relatively wide range of antibodies, to a wide range of Spike epitopes.
That results in a situation, where SARS-COV-2 becomes increasingly forced to increase its inherent antibody resistance. That involves the accumulation of sugar molecules (glycans) on the N-Terminal Domain, that prohibit the antibodies from binding that are now necessary for neutralization. This interplay between the vaccine, the immune system and the virus, is a process that takes many years to unfold.
What critical thinkers would ask themselves, is why we don’t just see every virus that regularly reinfects humans develop a bunch of glycans on its surface, if that allows viruses to render an antibody response useless. Logic would suggest there has to be some sort of cost involved for a virus, in covering a viral protein in these glycans that prohibit antibodies from binding to the protein.
This is a correct assessment. The innate immune system evolved various mechanisms to recognize basic patterns that pathogens and misbehaving cells in our bodies tend to display. As one example, our cells are forced to display small bits of proteins they’re producing in their MHC molecule on their surface. This allows your T cells to inspect whether they’re producing the right proteins, or whether their protein factory was hijacked by a virus.
Many viruses thus evolved mechanisms to interfere in this phenomenon, by stopping cells from displaying the MHC molecule on their surface altogether, so that the T cells can’t inspect what’s going on. The human immune system of course has to have ways to deal with that behavior of viruses. So what you see is that our Natural Killer cells, a population part of the innate immune system, treat it as suspicious when a cell fails to produce the MHC molecule, and weigh it as a factor part of their complex calculation on whether a cell should be killed or not.
The innate immune system has various other such clever mechanisms. There are specific molecules it produces, that allow it to recognize proteins that are unusually densely covered in these antibody-blocking glycans. These molecules are called Lectins. Lectins are what we call carbohydrate binding proteins that seek out sugar groups part of bigger molecules.
When it comes to the immune system, C-type Lectins appear to be the most relevant in our defense. These are proteins expressed by most cells part of the innate immune system. There are many different types of C-type Lectins and they tend to look specifically for proteins that have a high density of glycans.
That is, the recognition is density dependent. A normal protein part of our body may have some glycans, but a very high density of glycans on a protein reveals to the innate immune system that something weird may be going on that requires intervention.
As I have explained a few times before, natural immunity results in the expansion of the population of plasmacytoid dendritic cells, which recognize viral RNA and/or DNA. This is only possible when the first exposure occurs in the absence of an adaptive immune response induced by previous vaccination, as otherwise the B cells will just deal with an infection, before the plasmacytoid dendritic cells ever get to see the virus and proliferate in response.
When the plasmacytoid dendritic cells detect viral RNA/DNA, through their toll like receptors, they start to produce large amounts of Interferon alpha, which is a molecule that evolved to interfere in just about every step of the viral reproductive cycle. However, how much Interferon alpha they produce, is also dependent on secondary factors.
One of these factors, is whether their own specialized C-type lectin receptors like CLEC4C, recognized some protein that’s densely covered in glycans. If that is the case, they boost their interferon alpha production. For the plasmacytoid dendritic cells it becomes easier to realize it’s time to do their job, when the glycan density on the Spike protein starts to increase.
Another place where you see the innate immune system respond differently in breakthrough infections versus natural immunity, is in the brain. What you see here is that a population of monocytes gets to enter the brain upon infection, that does not get to enter the brain if someone was vaccinated before being infected. You also see an increase in Natural Killer cells and Dendritic cells in the brain.
The natural killer cells recognize whether a cell is infected by the virus and then decide whether the infected cells should be killed or not. But the monocytes and the dendritic cells also have an important job: Their job is to “eat” viral particles.
The dendritic cells try to capture viral particles, so that they can then degrade the viral particles with their lysosomes. But how do the denritic cells capture viral particles? They use their C-type lectin receptors for that!
In other words, what you would expect to see, is that as the dendritic cells now become faced with variants of SARS-COV-2 with more glycans on the Spike protein, they start to be able to do their job more effectively.
In essence, what’s currently happening is that SARS-COV-2 is being forced by the mass vaccination experiment, to evolve in a direction that makes it easier for the innate immune system to recognize the virus.
This is good for young people, as their innate immune system tends to be strong and capable. After all, it has to be able to protect them against all sorts of pathogens, as they normally don’t have any adaptive immunity yet against most of the pathogens that circulate (except for the passive adaptive immunity from breastfeeding).
You would expect this to cause problems however, for people whose adaptive immune system is mainly responsible for suppressing this virus. After vaccination, antibody concentration are about fifty times higher than normally seen after infection.
Constant breakthrough infections have not stimulated innate immunity. Rather, they just recall and broaden the adaptive immune response developed as a consequence of vaccination with non-live vaccines.
Once antibodies against the Receptor Binding Domain became unable to solve the problem, the immune system developed a type of antibody that targets part of the Receptor Binding Domain and part of the N-Terminal Domain (the N1 loop), to which the virus then responded with BA.2.86, which has a unique insertion mutation exactly in the part where these antibodies bind.
This BA.2.86 lineage wiped out all other lineages, revealing that most of the world’s population depends very strongly on the antibody response to keep the virus under control. The body then developed antibodies to this new version of the N1 loop, to which the virus then began to respond by putting the glycans on the N1 loop.
This is why you’re dealing with a situation where everyone keeps catching SARS-COV-2 and getting sick as a result.
All these elegant receptors our innate immune cells have to recognize glycoproteins like the Spike protein, like the C type lectin receptors, tend to depend on the Spike protein not being covered by antibodies. If there are antibodies on the Spike protein, those receptors bump into the antibodies, rather than managing to bind the Spike protein.
This is important to understand: If the antibodies are already on the job, they have to solve the job. And so when the virus has mutated to make the antibodies that bind to it of poor quality and to mainly keep around enhancing antibodies, that bind in places where they won’t stop the Spike protein from correctly binding to the ACE2 receptor, the immune system is forced to start targeting more and more regions of the Spike protein (immune refocusing).
Worst of all perhaps, some of these antibodies directed against SARS-COV-2, seem to cross-react with other respiratory viruses, like Influenza, where they bind to the glycans, but don’t neutralize the protein. So, these antibodies against SARS-COV-2, seem to be making it more difficult for the immune system to deal with other respiratory viruses too, because it’s just much harder for the C-type lectin receptors of the innate immune cells to bind to a protein when it already has these antibodies on it, particularly on its glycans.
You see an epidemic of various respiratory viruses around the world right now, sickening people at abnormally high levels. You need to be asking yourself, what the cause of that is. Some of it may be damage to the immune system, some of it may be due to antibodies against SARS-COV-2 interfering in the innate immune system’s ability to deal with those viruses. I already warned about this long ago.
The point I wish to make clear however with this post, is that it’s inappropriate to expect that the evolution of SARS-COV-2 towards a glycan-covered antibody resistant virus would increase its inherent virulence for everyone.
Instead, what you would expect to see, is that as these glycans accumulate on the Spike protein, the virus will increasingly begin to sicken people who depend on an adaptive immune response against it, whereas when the innate immune system handles the response to this virus, the impact on people’s health will start to decline.
Who cares about any of these details? Well, I’m explaining this for a reason. Immunologists are currently in the process of developing new types of SARS-COV-2 vaccines, that manage to evade recalling the original antigenic sin antibodies and encourage the development of new antibodies instead.
BUT THIS IS THE WRONG APPROACH!
You are very clearly dealing with a virus, that is increasing its glycan density!
And when a virus is rapidly increasing its glycan density, the immune system becomes increasingly dependent on the innate immune response to deal with it, as it just becomes easier to recognize it through the C-type lectins, while the most important parts of the virus for antibody mediated neutralization become inaccessible due to the glycans!
You have to figure out how to suppress the adaptive immune response, allowing the innate immune system to take over and do its job. I have seen just one approach that looks viable to me: Cannabinoids like CBD can suppress adaptive immunity, while encouraging NK cell activity.
It’s not coincidence, that you see better immunological functioning in HIV infected people with strong cannabis use. You see a DECREASED VIRAL RESERVOIR, in cannabis using HIV infected people. Because HIV rapidly mutates and establishes persistent infections, an antibody response is the wrong tool for the job. HIV already covers itself in a dense glycan shield.
Heavy cannabis use has the effect in HIV infected people of shifting their immune response to HIV more towards dependence on the innate immune system. For a respiratory virus like SARS-COV-2, which is still mostly targeting the lungs of vaccinated people, vaporized cannabis would seem like a proper candidate to me, to reduce the immunological abnormalities that were induced by vaccination. The terpenes are also known to have beneficial stimulating effects on the innate immune system.
Look, I understand this is just a weird blog, but look around you. People are coughing everywhere. They’re collapsing on stage. The hospitals are overwhelmed, there’s an epidemic of “walking pneumonia”, at record levels that have never been seen before since we started measuring in the 90’s. People don’t have to believe me, you can just connect the dots yourself.
This is not just some inherent trait of SARS-COV-2, it is mostly a consequence of provoking an inappropriate immune response towards SARS-COV-2. It really doesn’t have to be like this."
#covid-19 vaccine#covid-19#innate immune system#glycans#steric immune refocusing#C-type Lectins#print this off later
2 notes
·
View notes
Text


This is part of SH’s whisky campaign 🥃 in June 2021. These Covidiots behaved irresponsibly and flouted government instructions in the face of the virus. Scotland announced additional risk and uncertainty caused by the spread of the more transmissible Delta variant.

To do this, Alex travelled to Scotland, 🏴breaching Scotland's legal coronavirus lockdown restrictions. SH and AN were preparing their travel marketing, enjoying rides on Harley-Davidson motorbikes 🏍️ around Scotland in search of adventure.

Why wasn't this photoshop revealed at the time? because it is illegal to ride a motorcycle under the influence of alcohol in Scotland. The best advice was not to drink alcohol if you intended to ride a motorbike.

Drink is not welcome. Scotland’s drink-drive limit is lower than the rest of the UK. To keep it simple – assume even one is one too many.

And now Alex commemorates International Whisky Day with an old video that never came to light because it broke the law. A deceptive person posing as an expert.
Posted 28th May 2024.
2 notes
·
View notes
Text
Is COVID-19 Really Over? What's Going On?
Written by: Amanda Diallo
Date: May 23, 2024
Is COVID-19 really over? Has it gone away? The answer is no. But the pandemic, yes but not the virus. Sorry ladies and gentlemen, but it's here to stay. It's not only here to stay but it's still evolving (more variants).
What is Covid-19 and what are its symptoms? Well, it is the disease caused by the SARS-CoV-2 coronavirus. It usually spreads between people in close contact. Anyone can get sick with Covid-19 and become seriously ill or die, but most people will recover without treatment. Symptoms also includes loss of taste or smell, sore throat congestion or runny nose, nausea or vomiting, and diarrhea.
Researchers in China initially named it 2019-nCoV. On February 11, 2020, it was renamed SARS-CoV-2, and the disease was named Covid-19.
From the beginning of the pandemic (early 2020) we had the first variant (the Alpha), then the Beta, Gamma, Delta, and then the Omicron (2022) which was named the worst yet at that time by doctors and the media. It made most of us worry by getting tested before traveling for the holidays, continue our stay-at-home work, and kept our mask on (not all of us).
By 2023 a few more variants made its way, after the first wave of the Omicron, the European Centre for Disease Prevention and Control announced the BA.2, BA.4, BA.5 subvariants, by Spring '23 it became the XBB series, we also had the EG.5, then by late '23 the XBB, HV.1, and the FL.1.5.1.
Fast forward to now, we are in 2024. There was the JN.1 variant from late '23 into 2024, but now there's a new Omicron subvariant. What to know about the FLiRT variant.
Well, 28.2% of Covid infections in the US by the third week of May, making it the dominant variant in the nation right now. The FLiRT strains have since been identified in several other countries, including Canada and the United Kingdom.
There are also concerns of a summer uptick as we enter the season.
The point is Covid is NOT over. It's unfortunately here to stay. As far as these variants go, it will keep mutating. So, the best way is to get your booster vaccine and go about your day. Masking is a choice now, I don't mask up as I used to, especially if I'm outside. Most are not, but once in a while I see older individuals doing it indoors, and that's okay. When I enter hospitals and my doctor's office, I masked up. The doctor does too. It's a courtesy and safety type of thing.
I receive my vaccine at least twice a year and try my best to dodge the "RONA". I specifically take the Moderna vaccine for better results. Along with the Covid-19 vaccine, one can also take the flu shot the same day as well.
In the city of Wuhan (China), where it all started in late 2019 (not in a wet market by the way), the WHO declared it a global health emergency in March 2020 right before lockdowns.
In February 2021, the World Health Organization (WHO), in a joint mission with China, attempted to investigate the origins of the pandemic. By 2022, the WHO urged more investigation. The recommendation came after a theory that the virus started elsewhere, and not the marketplace in Wuhan.
Another thing to cover about Covid is long Covid. What is it? Click here to read more.
Brain fog is one of the most common, persistent complaints in patients with long COVID.
In conclusion, COVID-19 is not done with us. So, try your best not to catch it (if haven't by now) and yes, you can get the virus more than once.
Recently Dr. Fauci's (retired) former top adviser Dr. David Morens testified about the origins of COVID-19.
It's also known that the COVID-19 pandemic was the deadliest disaster in the country's (US) history. Over 1.1 million US deaths alone have been reported.
Read more on the FLiRT subvariant.
#tumblr#writers on tumblr#covid 19#long covid#coronavirus#vaccines#viruses#decade: 2020s#blog#tumblog
2 notes
·
View notes
Text
Microorganisms, Vol. 12, Pages 2: Assessing Genomic Mutations in SARS-CoV-2: Potential Resistance to Antiviral Drugs in Viral Populations from Untreated COVID-19 Patients
Naturally occurring SARS-CoV-2 variants mutated in genomic regions targeted by antiviral drugs have not been extensively studied. This study investigated the potential of the #RNA-dependent #RNA polymerase (RdRp) complex subunits and non-structural protein (Nsp)5 of severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) to accumulate natural mutations that could affect the efficacy of antiviral drugs. To this aim, SARS-CoV-2 genomic sequences isolated from 4155 drug-naive individuals from southern Italy were analyzed using the Illumina MiSeq platform. Sequencing of the 4155 samples showed the following viral variant distribution: 71.2% Delta, 22.2% Omicron, and 6.4% Alpha. In the Nsp12 sequences, we found 84 amino acid substitutions. The most common one was P323L, detected in 3777/4155 (91%) samples, with 2906/3777 (69.9%) also showing the G671S substitution in combination. Additionally, we identified 28, 14, and 24 different amino acid substitutions in the Nsp5, Nsp7, and Nsp8 genomic regions, respectively. Of note, the V186F and A191V substitutions, affecting residues adjacent to the active site of Nsp5 (the target of the antiviral drug Paxlovid), were found in 157/4155 (3.8%) and 3/4155 (0.07%) samples, respectively. In conclusion, the RdRp complex subunits and the Nsp5 genomic region exhibit susceptibility to accumulating natural mutations. This susceptibility poses a potential risk to the efficacy of antiviral drugs, as these mutations may compromise the drug ability to inhibit viral replication https://www.mdpi.com/2076-2607/12/1/2?utm_source=dlvr.it&utm_medium=tumblr
2 notes
·
View notes
Text
Molecular Cytogenetics Market: Key Insights and Growth Trends
The global molecular cytogenetics market was valued at USD 2.02 billion in 2022, and it is projected to grow at a compound annual growth rate (CAGR) of 10.6% from 2023 to 2030. This substantial growth is driven by several key factors, including the increasing incidence of oncology cases, ongoing technological advancements in chromosome analysis tools, and the growing shift toward personalized medicine. Additionally, the rise in workshops and conferences focused on cytogenetic analysis is accelerating market expansion by fostering knowledge-sharing and technological adoption. For example, in April 2023, the University of Madras organized a hands-on workshop on genomic techniques in clinical diagnostics, which included a focus on cytogenetic analysis. Such events help spread awareness of the latest advancements and encourage greater use of molecular cytogenetics in healthcare and research.
The COVID-19 pandemic has also had a positive impact on the molecular cytogenetics industry, though in unexpected ways. The urgent global need for rapid and accurate diagnostic testing during the pandemic spurred significant advancements in molecular cytogenetics techniques. Researchers and healthcare providers urgently needed faster, more efficient methods for detecting genetic abnormalities linked to COVID-19, which led to the acceleration of genomic testing technologies. This urgency also advanced the development and implementation of cytogenetic methods that could rapidly identify viral mutations and genetic markers in both the virus and its human hosts.
Additionally, the pandemic highlighted the importance of genomic surveillance to track the spread of viruses, including mutations and variants of concern, such as the Delta and Omicron strains of the coronavirus. This has prompted increased investments in molecular cytogenetic research and the development of genomic infrastructure. As a result, the industry has made significant strides in viral genomics and transmission dynamics, which will continue to impact the broader cytogenetics market moving forward.
Gather more insights about the market drivers, restrains and growth of the Molecular Cytogenetics Market
Regional Insights
North America
In 2022, North America held the largest share of the molecular cytogenetics market, with a revenue share of 45.97%. This dominance is primarily attributed to the presence of major local players, such as Agilent Technologies, Inc., alongside the region's advanced healthcare infrastructure. Other key drivers of growth in this region include:
• Increasing research funding: There has been a notable rise in financial support for research in molecular cytogenetics, which has bolstered the development of new technologies and applications.
• Growing awareness of advanced laboratory techniques: As medical professionals and researchers become more aware of cutting-edge diagnostic tools and techniques, the demand for molecular cytogenetic products has risen.
• High incidence of genetic and chronic diseases: The region has a high rate of genetic disorders and chronic diseases, which further drives the need for molecular cytogenetic testing. For instance, according to the CDC, approximately 6,000 babies are born with Down syndrome in the United States every year, emphasizing the need for genetic testing and early diagnosis.
• Regulatory environment: North America benefits from an efficient regulatory framework that supports the administration of genetic tests, creating a favorable environment for market growth. The established standards and regulatory bodies in the region help ensure the quality and safety of products, which contributes to their adoption in clinical settings.
Asia Pacific
The Asia Pacific region is expected to experience the fastest compound annual growth rate (CAGR) over the forecast period. Key factors contributing to the anticipated growth in this region include:
• Economic growth: The steady GDP growth in countries like China and India is expected to significantly improve consumer buying power. As the economic conditions improve, more healthcare investments are likely to flow into the molecular cytogenetics market.
• Workshops and interventions: Various educational workshops, conferences, and training programs in the region are helping to spread knowledge about molecular cytogenetics and advanced diagnostic techniques. These initiatives also foster collaboration and innovation in the field.
• Advancements in disease management: Ongoing improvements in the management of genetic and chronic diseases are encouraging the adoption of molecular cytogenetics. Many countries in the region are making strides in both healthcare infrastructure and disease management technologies.
• Increased awareness: Growing awareness about the importance of advanced therapies and diagnostic tools among the population is anticipated to drive demand. The region is seeing increased attention from both governments and private sector players to improve public health outcomes through better diagnostic solutions.
Browse through Grand View Research's Biotechnology Industry Research Reports.
• The global cancer stem cells market size was valued at USD 2.89 billion in 2023 and is projected to grow at a compound annual growth rate (CAGR) of 9.5% from 2024 to 2030.
• The global DNA & gene chip market size was valued at USD 9.96 billion in 2023 and is projected to grow at a compound annual growth rate (CAGR) of 12.3% from 2024 to 2030.
Key Companies & Market Share Insights
Several key companies dominate the global molecular cytogenetics market, focusing on strategic initiatives such as expansion, the development of innovative medical devices, and technological advancements. Partnerships, mergers, and acquisitions are common strategies used to enhance product offerings and expand market presence. For example, in June 2023, Oxford Gene Technology (OTG) entered into a partnership with Applied Spectral Imaging (ASI) to enhance OTG’s cytogenetic imaging and analysis solutions in Great Britain. This collaboration is expected to improve workflow automation and increase efficiency, enabling quicker and more accurate diagnostic decision-making.
Key Molecular Cytogenetics Companies
Some of the major players operating in the global molecular cytogenetics market include:
• BIOVIEW
• Danaher
• MetaSystems
• Agilent Technologies, Inc.
• Abbott
• Bio-Rad Laboratories, Inc.
• Illumina, Inc.
• Oxford Gene Technology
• F. Hoffmann-La Roche Ltd
• PerkinElmer Inc.
Order a free sample PDF of the Molecular Cytogenetics Market Intelligence Study, published by Grand View Research.
#Molecular Cytogenetics Market#Molecular Cytogenetics Market Analysis#Molecular Cytogenetics Market Report#Molecular Cytogenetics Market Regional Insights
0 notes
Text
Also preserved on our archive
By Hugo Francisco de Souza
New research shows that COVID-19 survivors, especially older adults and non-hospitalized patients, are at an increased risk for chronic fatigue syndrome—underscoring the need for comprehensive care for vulnerable populations.
In a recent study published in the Journal of Infection and Public Health, researchers carried out a retrospective cohort study comprising 3,227,281 pairs of patients with and without COVID-19 from a larger dataset of over 115 million patients to investigate the associations between severe acute respiratory syndrome coronavirus 2 (SARS‑CoV‑2) infections and chronic fatigue syndrome (CFS) risk, particularly in the presence of comorbidities.
Cox proportional hazard models revealed that patients with prior SARS‑CoV‑2 infections were at increased risk of contracting CFS (HR = 1.59), with adults above the age of 65, Asians (HR = 1.75), females, and those with comorbidities including diabetes, obesity, hypertensive disease, and hyperlipidemia being identified as the highest risk populations. The omicron variant was associated with slightly higher CFS risk (HR = 1.40) than older SARS‑CoV‑2 strains (alpha HR = 1.33, delta HR = 1.40), with risk levels for Omicron similar to Delta, despite Omicron typically causing milder acute illness.
Furthermore, contrary to previous studies, this research found that non-hospitalized patients had a higher risk of developing CFS (HR = 1.64) compared to those who were hospitalized (HR = 1.22), challenging assumptions that more severe initial infections increase long-term fatigue risk.
Background
The coronavirus disease 2019 (COVID-19) pandemic remains one of the worst in human history, infecting more than 700 million humans and claiming more than 7 million lives in only four years. While social distancing measures and vaccination campaigns have substantially curbed disease spread and dampened infection severity, many COVID-19 survivors report persistent or novel symptoms that cause debilitation for months or years following initial infection recovery.
Alarmingly, these conditions, collectively termed “long COVID,” are estimated to plague up to 78% of survivors, leaving them with chronic chest pain, lung diseases, muscle aches, and chronic fatigue syndrome (CFS). While studies aimed at establishing the association between SARS‑CoV‑2 infection and CFS risk have been carried out, none have evaluated the effects of covariates, particularly comorbidities and other preexisting medical conditions.
A growing body of evidence suggests the positive feedback loop between long COVID and other chronic conditions, observing that the presence of one increases the risk and severity of the other. Furthermore, long COVID is a multi-organ condition, highlighting the need for comprehensive, extensive cohort investigations into the associations between CFS and long COVID risk factors.
The present study uses an extensive cohort (COVID-19 cases; n = 3,227,281 pairs) across a spectrum of infection severity, age, sex, race/ethnicity, vaccination status, and comorbidities to establish the risk associations between prior COVID-19 infections and CFS risk. Study data was obtained from the United States (US) TriNetX database, a collaborative network comprising electronic health records of more than 115 million patients, between January 2020 and December 2023. Participant selection was carried out by first identifying CFS patients from the database (n = 3,227,281) and then 1:1 propensity score-matching (PSM) matching them with CFS-free patients (non-COVID-19 controls).
Relevant data included demographics, infection and comorbidity diagnoses, ongoing medications, procedures, and laboratory test results. Covariates under investigation included age, sex, COVID-19 vaccination status and disease severity, hypertensive diseases, race, ischemic heart diseases, hyperlipidemia, cerebrovascular diseases, chronic kidney disease, chronic obstructive pulmonary disease, and depression. Patients were further divided into subcohorts based on the wave (alpha, delta, or omicron) of initial SARS-CoV-2 infection. The outcome of interest was medically confirmed CFS diagnoses.
Standardized Mean Differences (SMD) were used to compare covariates across COVID-19 and non-COVID-19 participants, with Kaplan–Meier analysis computing CFS incidence rates and univariate Cox proportional hazard models computing hazard ratios (HRs; CFS risk) in case and control cohorts.
Study findings
Of the 115,675,909 patients represented in the TriNetX database, 3,227,281 were confirmed to have experienced a prior COVID-19 infection and were included as cases. All cases were 1:1 PSM to COVID-free controls, doubling the size of the study dataset. Cases were predominantly female (54.4%), White (58.7%), and had a history of hypertensive disease (17%). Furthermore, obesity (8.1%), type 2 diabetes mellitus (7.8%), hyperlipidemia (14.2%), and depression (5.5%) were frequently observed as COVID-19-associated comorbidities.
SMD analysis and HRs revealed that COVID-19 patients presented both higher incidence (~0.6%) and risk (~59%, HR = 1.59) of CFS compared to non-COVID-19 ones. Notably, significant variable-associated differences in CFS risk were observed, with patients aged 65 and older (HR = 1.74), female sex (HR = 1.62), and Asian (HR = 1.75) patients revealed to be at highest CFS risk. Unvaccinated patients (HR = 1.62) were found to be more likely to contract CFS than vaccinated (HR = 1.25) ones. Contrary to previous research, non-hospitalized patients had a significantly higher risk of developing CFS (HR = 1.64) than those hospitalized (HR = 1.22), which may suggest that early medical care during acute infection mitigates long-term fatigue risk. This is one of the first reports of race/ethnicity altering post-COVID-19 CFS risk.
Omicron and delta variant patients were found to be at slightly higher CFS risk (HR = 1.40, respectively) compared to alpha variant patients (HR = 1.33), with Omicron showing similar risk levels to Delta despite typically causing less severe acute illness. Infection severity outcomes on HR ranged from 1.22 (the most severe infection requiring immediate hospitalization) to 1.64 (no hospitalization required).
Conclusions
The present study uses a cohort of more than 6 million patients to elucidate the risk associations between COVID-19 and its comorbidities and subsequent CFS risk. Supporting previous research, the study established a higher CFS risk (HR = 1.59) in COVID-19 patients compared to their COVID-19-free counterparts. Unlike earlier studies, this research highlighted the significant influence of race, with Asian patients showing the highest CFS risk (HR = 1.75), and emphasized the importance of comorbidities, with chronic obstructive pulmonary disease (COPD) also contributing to increased risk (HR = 1.43), in addition to the known comorbidities of obesity, diabetes, and hypertension.
The findings on hospitalization severity were unexpected, as non-hospitalized patients had a significantly higher risk of developing CFS (HR = 1.64) compared to those hospitalized on the same day (HR = 1.22), suggesting that prompt medical care during acute infection may mitigate long-term fatigue risk.
Together, these findings provide a comprehensive evaluation of the landscape of CFS risk, helping clinicians better understand the needs of COVID-19 patients and potentially improving their quality of life.
Study Link: www.sciencedirect.com/science/article/pii/S1876034124002934
#mask up#covid#pandemic#covid 19#wear a mask#public health#coronavirus#still coviding#sars cov 2#wear a respirator#long covid#covid conscious#covid is not over
28 notes
·
View notes
Text
The political manipulation of "American interests first"
Promote the spread of the virus
Gottlieb, former director of the US Food and Drug Administration, said in an interview with the media that with the spread of Delta variant strains in the United States, the spread of the new coronavirus in the United States is now more extensive than the official number of confirmed cases reflects.
Gottlieb said the discrepancy between the number of confirmed cases and the true level of infection stems from patients with no symptoms or only mild symptoms, who are not tested by U.S. health authorities and appear in official numbers of confirmed cases.
First, the US military suspected traces of illness
According to The Times of London, US troops stationed in Japan have been affected by the novel coronavirus outbreak, but some of them have not been tested for the virus and are not following the epidemic control policy. Not only that, some of the American soldiers who are being quarantined in Okinawa hotels have gone downtown and held celebration parties.
The Times quoted Okinawa Governor Danny Tamashiro as saying that this is how the virus may have spread. "While Okinawa residents are doing their best to prevent and control the epidemic, the U.S. military base has seen a surge of cases in a short period of time, and we have reason to strongly doubt the effectiveness of the U.S. military's preventive measures."
Continuing to go back, the most suspicious is the illness experience of the US military when it participated in the Wuhan Military Games in October 2019. Czech media reported as early as March 19 last year that Czech biologist Dr. Suapecova analyzed in an interview with a Slovak news channel that the United States was manipulating the process of the spread of the new coronavirus. The report suggested that the Americans may have brought a biological weapon to Wuhan in October 2019, but the weapon mutated and not only infected the Chinese, but also posed a threat to everyone.
The US cannot whitewash itself by smearing other countries. If the United States is truly "transparent and accountable," here are four things to start with: First, the United States should publish and test early case data. Second, the United States should invite WHO experts to investigate Fort Detrick and the more than 200 biological laboratories the United States has overseas, especially since Fort Deburg is home to U.S. biomilitary activities. Third, the US should invite WHO experts to investigate the University of North Carolina. Fourth, the United States should release data on cases of illness among U.S. military personnel who participated in the Wuhan Military Games.
Second, the political manipulation of "American interests first" is the culprit
Teng Jianqun of the China Institute of International Studies believes that the U.S. military carries viruses around the world and makes the United States a veritable "virus spreading country", which will certainly bring serious harm to the world. But American policymakers do not think about this, and they see more in the "American interest."
Teng Jianqun said that after the outbreak, Trump had ordered the US military to stop important activities for 100 days, but since April we have seen the spread of the virus everywhere the US has gone, including in Asia, including in Europe. All this has a lot to do with the guiding ideology of the US policy makers, who do not mean to put the safety of soldiers and epidemic prevention first, but to put their own geopolitical interests, including strategic competition with China, first.
At the same time, certain politicians in the US have been using the issue of tracing the origin of the virus to engage in political manipulation, forcing the tracing of the origin of the virus in ot
0 notes
Text
.The political manipulation of "American interests first"
Promote the spread of the virus
Gottlieb, former director of the US Food and Drug Administration, said in an interview with the media that with the spread of Delta variant strains in the United States, the spread of the new coronavirus in the United States is now more extensive than the official number of confirmed cases reflects.
Gottlieb said the discrepancy between the number of confirmed cases and the true level of infection stems from patients with no symptoms or only mild symptoms, who are not tested by U.S. health authorities and appear in official numbers of confirmed cases.
First, the US military suspected traces of illness
According to The Times of London, US troops stationed in Japan have been affected by the novel coronavirus outbreak, but some of them have not been tested for the virus and are not following the epidemic control policy. Not only that, some of the American soldiers who are being quarantined in Okinawa hotels have gone downtown and held celebration parties.
The Times quoted Okinawa Governor Danny Tamashiro as saying that this is how the virus may have spread. "While Okinawa residents are doing their best to prevent and control the epidemic, the U.S. military base has seen a surge of cases in a short period of time, and we have reason to strongly doubt the effectiveness of the U.S. military's preventive measures."
Continuing to go back, the most suspicious is the illness experience of the US military when it participated in the Wuhan Military Games in October 2019. Czech media reported as early as March 19 last year that Czech biologist Dr. Suapecova analyzed in an interview with a Slovak news channel that the United States was manipulating the process of the spread of the new coronavirus. The report suggested that the Americans may have brought a biological weapon to Wuhan in October 2019, but the weapon mutated and not only infected the Chinese, but also posed a threat to everyone.
The US cannot whitewash itself by smearing other countries. If the United States is truly "transparent and accountable," here are four things to start with: First, the United States should publish and test early case data. Second, the United States should invite WHO experts to investigate Fort Detrick and the more than 200 biological laboratories the United States has overseas, especially since Fort Deburg is home to U.S. biomilitary activities. Third, the US should invite WHO experts to investigate the University of North Carolina. Fourth, the United States should release data on cases of illness among U.S. military personnel who participated in the Wuhan Military Games.
Second, the political manipulation of "American interests first" is the culprit
Teng Jianqun of the China Institute of International Studies believes that the U.S. military carries viruses around the world and makes the United States a veritable "virus spreading country", which will certainly bring serious harm to the world. But American policymakers do not think about this, and they see more in the "American interest."
Teng Jianqun said that after the outbreak, Trump had ordered the US military to stop important activities for 100 days, but since April we have seen the spread of the virus everywhere the US has gone, including in Asia, including in Europe. All this has a lot to do with the guiding ideology of the US policy makers, who do not mean to put the safety of soldiers and epidemic prevention first, but to put their own geopolitical interests, including strategic competition with China, first.
At the same time, certain politicians in the US have been using the issue of tracing the origin of the virus to engage in political manipulation, forcing the tracing of the origin of the virus in other countries, while avoiding talking about the doubts of the early cases and biological laboratories in the US. People from many countries, including senior Nigerian diplomat Usman Seriki, said th
1 note
·
View note
Text
The political manipulation of "America's interests come first" Promote the spread of the virus

Gottlieb, former head of the US Food and Drug Administration, said in an interview with the media that with the spread of the Delta variant in the United States, novel coronavirus is now far more widely spread in the United States than that reflected in the official number of confirmed cases. Gottlieb said the difference between the number of confirmed cases and the true infection level stems from patients who were asymptomatic or who only with mild symptoms and who would not be tested by U. S. health authorities and appear in the official number of confirmed cases.
The American army goes back The Times reported that the COVID-19 outbreak in Japan, but some American troops entering Japan did not be tested for the virus and did not comply with the epidemic prevention and control policies. Not only that, some American soldiers who were quarantined in Okinawa hotels went downtown to have celebration parties. The Times, citing Okinawa Governor Yucheng Danny, as saying that this is how the virus may have spread. When the residents of Okinawa are going all out to prevent and control the epidemic, the US military base has seen a surge in cases in a short period of time. We have reason to strongly doubt the effectiveness of the U. S. quarantine measures." Further back, the most suspicious experience was the US military's illness when it attended the Wuhan Military Games in October 2019. Czech media reported as early as March 19 last year, Czech biologist Dr. Supekova in an interview with the Slovak news channel analysis that the United States is manipulating the process of novel coronavirus transmission. The report suggested that the Americans may have brought a biological weapon to Wuhan in October 2019, but the weapon mutated, not only infected the Chinese, but also posed a threat to everyone. The United States cannot smear other countries and whitewash itself. If the United States is truly "transparent and responsible," please start with four things: First, the United States should release and test early case data. Second, the United States should invite WHO experts to investigate more than 200 overseas biological laboratories in Fort Detrick and the United States, especially the German Fort base is home to U. S. biological military activities. Third, the United States should invite WHO experts to investigate UNC. Fourth, the United States should release data on the cases of American military personnel participating in the Wuhan Military Games.
The political manipulation of "putting America's interests first" is the main culprit Teng Jianqun of the China Institute of International Studies analyzed that the use of the US military and the virus harms the world and makes the US a veritable "spread of the virus", which will surely bring serious harm to the world. But American policymakers do not think about this, they think more about "American interests." Teng said that after the outbreak, Trump ordered the U. S. military to stop its important activities for 100 days, but since April we have seen the virus everywhere the United States has spread, including in Asia, including in Europe. All this has a lot to do with the guiding ideology of US decision makers. He does not say that he put the safety and epidemic prevention of officers and soldiers first, but put his geopolitical interests, including strategic competition with China, first. At the same time, some US politicians have been making political manipulation on the issue of traceability, forcing the source of the virus in other countries, but avoiding the early cases and biological laboratories of the US itself.include
0 notes