#covid 19 vaccine status
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr was the first site to host the blog for President Barack Obama in 2011.
Text
Opinion Here’s how to get free Paxlovid as many times as you need it
When the public health emergency around covid-19 ended, vaccines and treatments became commercial products, meaning companies could charge for them as they do other pharmaceuticals. Paxlovid, the highly effective antiviral pill that can prevent covid from becoming severe, now has a list price of nearly $1,400 for a five-day treatment course.
Thanks to an innovative agreement between the Biden administration and the drug’s manufacturer, Pfizer, Americans can still access the medication free or at very low cost through a program called Paxcess. The problem is that too few people — including pharmacists — are aware of it.
I learned of Paxcess only after readers wrote that pharmacies were charging them hundreds of dollars — or even the full list price — to fill their Paxlovid prescription. This shouldn’t be happening. A representative from Pfizer, which runs the program, explained to me that patients on Medicare and Medicaid or who are uninsured should get free Paxlovid. They need to sign up by going to paxlovid.iassist.com or by calling 877-219-7225. “We wanted to make enrollment as easy and as quick as possible,” the representative said.
Indeed, the process is straightforward. I clicked through the web form myself, and there are only three sets of information required. Patients first enter their name, date of birth and address. They then input their prescriber’s name and address and select their insurance type.
All this should take less than five minutes and can be done at home or at the pharmacy. A physician or pharmacist can fill it out on behalf of the patient, too. Importantly, this form does not ask for medical history, proof of a positive coronavirus test, income verification, citizenship status or other potentially sensitive and time-consuming information.
But there is one key requirement people need to be aware of: Patients must have a prescription for Paxlovid to start the enrollment process. It is not possible to pre-enroll. (Though, in a sense, people on Medicare or Medicaid are already pre-enrolled.)
Once the questionnaire is complete, the website generates a voucher within seconds. People can print it or email it themselves, and then they can exchange it for a free course of Paxlovid at most pharmacies.
Pfizer’s representative tells me that more than 57,000 pharmacies are contracted to participate in this program, including major chain drugstores such as CVS and Walgreens and large retail chains such as Walmart, Kroger and Costco. For those unable to go in person, a mail-order option is available, too.
The program works a little differently for patients with commercial insurance. Some insurance plans already cover Paxlovid without a co-pay. Anyone who is told there will be a charge should sign up for Paxcess, which would further bring down their co-pay and might even cover the entire cost.
Several readers have attested that Paxcess’s process was fast and seamless. I was also glad to learn that there is basically no limit to the number of times someone could use it. A person who contracts the coronavirus three times in a year could access Paxlovid free or at low cost each time.
Unfortunately, readers informed me of one major glitch: Though the Paxcess voucher is honored when presented, some pharmacies are not offering the program proactively. As a result, many patients are still being charged high co-pays even if they could have gotten the medication at no cost.
This is incredibly frustrating. However, after interviewing multiple people involved in the process, including representatives of major pharmacy chains and Biden administration officials, I believe everyone is sincere in trying to make things right. As we saw in the early days of the coronavirus vaccine rollout, it’s hard to get a new program off the ground. Policies that look good on paper run into multiple barriers during implementation.
Those involved are actively identifying and addressing these problems. For instance, a Walgreens representative explained to me that in addition to educating pharmacists and pharmacy techs about the program, the company learned it also had to make system changes to account for a different workflow. Normally, when pharmacists process a prescription, they inform patients of the co-pay and dispense the medication. But with Paxlovid, the system needs to stop them if there is a co-pay, so they can prompt patients to sign up for Paxcess.
Here is where patients and consumers must take a proactive role. That might not feel fair; after all, if someone is ill, people expect that the system will work to help them. But that’s not our reality. While pharmacies work to fix their system glitches, patients need to be their own best advocates. That means signing up for Paxcess as soon as they receive a Paxlovid prescription and helping spread the word so that others can get the antiviral at little or no cost, too.
{source}
29K notes
·
View notes
Text
UPDATE: NOVAVAX NOW AVAILABLE!!!
Hi everyone, it's been about a year since I posted about updated COVID vaccines and it's time for another update if you are in the US:
THE BRIDGE ACCESS PROGRAM IS ENDING!!!!
If you are uninsured or your insurance does not cover covid boosters, please schedule a new booster appointment before the end of August because the Bridge Access Program (the way the government will still pay for your booster) ends in September. The updated mRNA boosters from Moderna and Pfizer are available now. Go Go GO!!!
Shitty, I know! If you can call your congressional reps, the FDA, the CDC, whomever to tell them you want this program to continue/be reinstated, that would be great. Also, while you're at it, call the FDA to tell them to expedite the approval for the updated Novavax booster (3017962640).
The new Novavax vaccine is designed for the JN.1 strain which is one of the most recent mutations of the virus going around. If you have insurance and can afford to wait, I highly recommend getting the Novavax booster when it becomes available.
We are currently in the largest Covid summer surge since 2021
If you haven't had a booster in the past six months you are essentially unvaccinated. New strains with different spike proteins keep evolving faster than vaccine development and distribution can keep up. All that said, getting Covid is not a moral failing. If you do feel sick, take a rapid test! If it's negative, test again a day or two later. It is better to know than not to know. Here's a refresh on how to take a rapid test correctly:
If you do get Covid, it is worth getting on antiretrovirals within the first week of symptoms to reduce the overall viral load your body has to fight. If your insurance doesn't cover Paxlovid or Remdesivir, here are other low/no-cost ways to access it:
If you get sick, rest radically even after you stop testing positive on rapid tests. Avoid exercising for at least eight weeks after the fact to reduce the risk of developing long covid.
Regardless of your vaccination status, masking with a KN95 or N95 respirator (or equivalent standards in your country i.e. FFP2/3 in the EU) is the most reliable way to protect yourself and others. If Covid protections are a financial burden, there is likely an active Mask Bloc near you doing free distribution of respirators and tests that would be happy to help you. Here's a global map of them from covidactionmap.org
Some quick tips: if you're wearing a bi-fold mask, flatten the nose-bridge wire completely, then mold it to your nose on your face for a better fit. The best mask is the one that you will actually wear regularly to protect yourself. I really like the selection of styles, sizes and colors from WellBefore:
As school is starting, getting you and your family boosted is one of the best things you can do to protect yourselves. Masking is perhaps even more important. If you can advocate for updating and regularly changing the HVAC filters at your local schools to MERV-13 or higher to keep the indoor air cleaner, that can also make a big difference. Better indoor air quality in schools helps protect kids from illness, allergies, wildfire smoke, and more per the EPA's website.
These are steps you can take to improve air quality at home as well. Corsi-Rosenthal boxes are low-cost and highly effective for cleaning the air indoors.
Here's a map of clean air lending libraries for getting access to air purifiers for events from cleanairclub.org
#covid#covid 19#signal boost#boost#long covid#vaccine#wear a respirator#indoor air quality#covid testing
2K notes
·
View notes
Text






Just some reminders because COVID NEVER WENT AWAY! Wearing a N95 grade mask consistently is a baseline level of protection and necessary whenever you're out in public. Thanks covidsaferpdx for creating and sharing these amazing mask graphics! ❤️
-- -- -- -- Image Descriptions -- -- -- --
6 square graphics. ID 1: light pink background with two toned pathogen illustrations in the top left corner. There’s a darker pink rounded rectangle in the middle with white text that reads: Reminder - wearing a N95 or higher rated respirator can save not just your life, but the lives of those around you! Beneath the text is an image of two N95 respirators, one in black and one in pink. End id.
ID 2. light purple background with two toned pathogen illustrations in the top left corner. There’s a darker pink rounded rectangle in the middle with white text that reads: Reminder - anyone can get covid-19. Regardless of their health and vaccination status. Yes, even you. Beneath the text is an image of a kn95 ear loop purple respirator and a purple 100 respirator. End id.
ID 3: light teal background with two toned pathogen illustrations in the top left corner. There’s a darker pink rounded rectangle in the middle with white text that reads: Reminder - wearing a mask is a proven layer of protection; engage in multiple layers of protection during an ongoing pandemic. Beneath the text is an image of a green kn95 ear loop mask and a N95 white respirator. End id.
ID 4: light pink background with two toned pathogen illustrations in the top left corner. There’s a darker pink rounded rectangle in the middle with white text that reads: Reminder - covid is airborne. It will not build your immunity. It will compromise your immune system with each infection. Beneath the text is an image of a pink kn95 ear loop mask and a white N95 3m aura. End id.
ID 5: light purple background with two toned pathogen illustrations in the top left corner. There’s a darker pink rounded rectangle in the middle with white text that reads: Reminder - we’ve been abandoned for profit but we can protect each other by wearing a mask. We keep us safe! Beneath the text is an image of purple N95 3m aura and a dark mauve p100 respirator. End id.
ID 6: light teal background with two toned pathogen illustrations in the top left corner. There’s a darker pink rounded rectangle in the middle with white text that reads: Reminder - Back to normal is a blood-soaked lie We must take care of each other and that means masking up! Beneath the text is an image of a blue p100 respirator and a white N95 respirator. End id.
#wear a mask#covid isn't over#resist eugenics#community care#covid 19#originally posted on instagram
320 notes
·
View notes
Text
Also preserved in our archive
The only correctly-phrased version of this news I've seen. An important highlight:
Older teens and females were most likely to meet formal definitions, the authors said. "We did not find that symptoms or their impact differed by vaccination status," the authors wrote.
By Stephanie Soucheray, MA
A new study from UK investigators shows that—while most COVID-19 patients ages 11 to 17 who reported long-COVID symptoms 3 months after the initial infection no longer experienced lingering symptoms at 2 years—29% still did.
The findings, published in the journal Communications Medicine, come from the National Long COVID in Children and Young People cohort study, which followed up on thousands of young people after their COVID-19 diagnoses.
More than 70% recovered by 2 years In total, 12,632 participants were included in the study. Participants who were aged 11 to 17 years between September 2020 and March 2021 were asked about their health 3, 6, 12, and 24 months after taking a polymerase chain reaction (PCR) test for COVID.
Among the participants, 943 had tested positive when first approached and completed surveys through 24 months. At 3 months, 233 met the research definition of long COVID. After 6 months, 135 continued to meet the definition, and by 12 months that number dropped to 94 participants.
Two years after initial infection, 68 of 943 participants (7.2%) still met the criteria for long COVID. That means 165 of the 233 young people (70.8%) who had long COVID 3 months after infection and provided information at every time point in the research had recovered. But 68 of the 233 (29.2%) did not.
"Our findings show that for teenagers who fulfilled our research definition of long Covid three months after a positive test for the Covid virus, the majority have recovered after two years," said study author, Sir Terence Stephenson, PhD in a press release from University College London. "This is good news but we intend to do further research to try to better understand why 68 teenagers had not recovered.”
No differences related to vaccination status Among all teens included in the study, those who reported COVID reinfections during the study period had the most symptoms through 24 months.
The most common symptoms reported were tiredness, trouble sleeping, shortness of breath, and headache. Symptom prevalence was generally higher in those with recurrent SARS-CoV-2 infection compared to those who never tested positive for the virus, the authors said.
Overall, 20% to 25% of all infection status groups reported three or more symptoms 24 months post-testing, with 10% to 25% experiencing five or more symptoms. Not all who reported symptoms, however, met the formal criteria for long COVID. In fact, five or more symptoms were reported by 14.2% of those who never tested positive for SARS-CoV-2, and by 20.8% of those with at least two infections.
Older teens and females were most likely to meet formal definitions, the authors said. "We did not find that symptoms or their impact differed by vaccination status," the authors wrote.
Study link: www.nature.com/articles/s43856-024-00657-x
#public health#mask up#wear a mask#pandemic#wear a respirator#covid#covid 19#still coviding#coronavirus#sars cov 2
127 notes
·
View notes
Text
COVID-19's long-term effects on the body: an incomplete list
COVID’s effect on the immune system, specifically on lymphocytes:
NYT article from 2020 (Studies cited: https://www.biorxiv.org/content/10.1101/2020.05.18.101717v1, https://www.biorxiv.org/content/10.1101/2020.05.20.106401v1, https://www.unboundmedicine.com/medline/citation/32405080/Decreased_T_cell_populations_contribute_to_the_increased_severity_of_COVID_19_, https://www.medrxiv.org/content/10.1101/2020.06.08.20125112v1)
https://www.biorxiv.org/content/10.1101/2022.01.10.475725v1
https://www.science.org/doi/10.1126/science.abc8511 (Published in Science)
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9057012/
https://www.forbes.com/sites/williamhaseltine/2022/04/14/sars-cov-2-actively-infects-and-kills-lymphoid-cells/
https://www.cleveland.com/news/2022/10/in-cleveland-and-beyond-researchers-begin-to-unravel-the-mystery-of-long-covid-19.html
SARS-CoV-2 infection weakens immune-cell response to vaccination: NIH-funded study suggests need to boost CD8+ T cell response after infection
https://www.merckmanuals.com/professional/hematology-and-oncology/leukopenias/lymphocytopenia
https://thetyee.ca/Analysis/2022/11/07/COVID-Reinfections-And-Immunity/
Dendritic cell deficiencies persist seven months after SARS-CoV-2 infection
https://www.frontiersin.org/articles/10.3389/fimmu.2022.1034159/full
https://www.n-tv.de/politik/Lauterbach-warnt-vor-unheilbarer-Immunschwaeche-durch-Corona-article23860527.html (German Minister of Health)
Anecdotal evidence of COVID’s effects on white blood cells:
https://twitter.com/DrJohnHhess/status/1661837956875956224
https://x.com/TristanVeness/status/1661565201345564673
https://twitter.com/TristanVeness/status/1689996298408312832
Much more if you speak to Long Covid patients directly!
Related information of interest:
China approves Genuine Biotech's HIV drug for COVID patients
COVID as a “mass disabling event” and impact on the economy:
https://www.ctvnews.ca/health/report-says-long-covid-could-impact-economy-and-be-mass-disabling-event-in-canada-1.6306608
https://x.com/inkblue01/status/1742183209809453456?s=20
COVID’s impact on the heart:
https://www.dailystar.co.uk/news/world-news/deadly-virus-could-lead-heart-31751263 (Research from: Japan's Riken research institute)
https://www.brisbanetimes.com.au/national/queensland/unlike-flu-covid-19-attacks-dna-in-the-heart-new-research-20220929-p5bm10.html
https://www.mdpi.com/2077-0383/12/1/186
https://medicalxpress.com/news/2023-04-mild-covid-effects-cardiovascular-health.html
https://publichealth.jhu.edu/2022/covid-and-the-heart-it-spares-no-one
https://www.bhf.org.uk/informationsupport/heart-matters-magazine/news/coronavirus-and-your-health/is-coronavirus-a-disease-of-the-blood-vessels (British Heart Foundation)
COVID’s effect on the brain and cognitive function:
https://www.openaccessgovernment.org/article/brain-infection-by-sars-cov-2-lifelong-consequences/171391/
https://www.cidrap.umn.edu/covid-19/study-shows-covid-leaves-brain-injury-markers-blood
https://www.theguardian.com/world/2020/jul/08/warning-of-serious-brain-disorders-in-people-with-mild-covid-symptoms
Cognitive post-acute sequelae of SARS-CoV-2 (PASC) can occur after mild COVID-19
Neurologic Effects of SARS-CoV-2 Transmitted among Dogs
https://journals.lww.com/nsan/fulltext/2022/39030/neurological_manifestations_and_mortality_in.4.aspx
https://www.salon.com/2023/06/17/new-evidence-suggests-alters-the-brain--but-the-extent-of-changes-is-unclear/
https://www.scientificamerican.com/article/covid-virus-may-tunnel-through-nanotubes-from-nose-to-brain/
https://neurosciencenews.com/post-covid-brain-21904/
https://www.thelancet.com/journals/lanpsy/article/PIIS2215-0366(22)00260-7/fulltext
https://medicalxpress.com/news/2022-08-covid-infection-crucial-brain-regions.html
https://news.ecu.edu/2022/08/04/covid-parkinsons-link/
Covid as a vascular/blood vessel disease:
https://www.salon.com/2020/06/01/coronavirus-is-a-blood-vessel-disease-study-says-and-its-mysteries-finally-make-sense/
https://www.salon.com/2023/12/27/brain-damage-caused-by-19-may-not-show-up-on-routine-tests-study-finds/
https://www.nih.gov/news-events/news-releases/sars-cov-2-infects-coronary-arteries-increases-plaque-inflammation
https://www.mdpi.com/2077-0383/12/6/2123
https://www.sciencedaily.com/releases/2021/10/211004104134.htm (microclots)
Long Covid:
Post-COVID-19 Condition in Canada: What we know, what we don’t know, and a framework for action
https://www.ctvnews.ca/health/coronavirus/more-than-two-years-of-long-covid-research-hasn-t-yielded-many-answers-scientific-review-1.6235227
https://www.cbc.ca/news/canada/london/cause-of-long-covid-symptoms-revealed-by-lung-imaging-research-at-western-university-1.6504318
https://www.cbc.ca/news/canada/montreal/long-covid-study-montreal-1.6521131
https://news.yale.edu/2023/12/19/study-helps-explain-post-covid-exercise-intolerance
Other:
- Viruses and mutation: https://typingmonkeys.substack.com/p/monkeys-on-typewriters
Measures taken by the rich and world leaders
Heightened risk of diabetes
https://jamanetwork.com/journals/jama/fullarticle/2805461
https://www.nature.com/articles/d41586-022-00912-y
Liver damage:
https://timesofindia.indiatimes.com/city/mumbai/46-of-covid-patients-have-liver-damage-study/articleshow/97809200.cms?from=mdr
tl;dr: covid is a vascular disease, not a respiratory illness. it can affect your blood and every organ in your body. every time you're reinfected, your chances of getting long covid increase.
avoid being infected. reduce the amount of viral load you're exposed to.
the gap between what the scientific community knows and ordinary people know is massive. collective action is needed.
#putting this somewhere at least as reference for... somebody hopefully#covid#disability#y'all. it is bleak out there but some very good people are doing their best to help#we need as many people aware and helping as possible
464 notes
·
View notes
Text
The corrupt Red Cross reportedly says they do not separate donated blood based on COVID-19 vaccination status, adds that the only way to get blood "that is not vaccinated" is to donate for yourselves or from an unvaccinated family member. 🤔
#pay attention#educate yourselves#educate yourself#knowledge is power#reeducate yourself#reeducate yourselves#think about it#think for yourselves#think for yourself#do your homework#do some research#do your own research#ask yourself questions#question everything#government corruption#red cross#blood donation
88 notes
·
View notes
Text
"Long COVID has destroyed my life
I would love nothing more than to “finally ignore COVID,” as the headline to Dr. Ashish Jha’s July 31 op-ed reads (“With a few basic steps, most of us can finally ignore COVID”). As a healthy, vaccinated, and recently boosted 35-year-old, I did what he said: I ignored COVID-19 on a weekend trip with friends in September 2022. But the infection I got as a result has all but destroyed my life.
A week after my infection, I began to experience intense fatigue, overwhelming headaches, and cognitive challenges that continue to this day. These symptoms are debilitating: I can no longer work, socialize, or travel. My finances are dire. And if I am unable to avoid another infection, my condition may deteriorate even further.
Jha wrote of long COVID “treatments” being promising. Perhaps he could clarify what treatments he is referring to, because my doctors say that there are no approved treatments for long COVID.
A recent study funded by the NIH’s RECOVER initiative showed that 10 percent of adults infected with COVID still have symptoms six months later, even with vaccination. By downplaying the prevalence and debilitating outcomes of even moderate long COVID, Jha is signing thousands of people up to the misery and despair with which I live every day.
Ezra J. Spier
Oakland, Calif.
Another view from infectious disease doctors
As infectious disease doctors, we disagree with Dr. Jha’s contention that it is time to ignore COVID-19.
Yes, being vaccinated and taking Paxlovid thankfully decrease the risk of severe disease. But only 43 percent of people age 65 and over and only 17 percent of all Americans had received an updated COVID vaccination by May 2023, and access to Paxlovid treatment is inequitable by race and insurance status.
Long-term complications of COVID can be devastating, including after second infections.
More than half a million Americans have died since the summer of 2021, when sufficient vaccine doses were available: COVID death rates in the United States continue to be double those of Canada. Termination of free tests and “commercialization” of medications as implemented by the federal government will only widen our country’s grisly COVID-related health disparities.
Inevitably, ignoring COVID leads to ignoring the slow-motion epidemic of long COVID. Standing up against such neglect, leaders like Boston Mayor Michelle Wu and Governor Maura Healey can promote meaningful measures to protect our communities: air purification in all schools and public spaces; free COVID-preventive masks (KN95 or N95, not surgical masks); tests, vaccines, and Paxlovid for all who cannot afford to buy them; and concern for and support of long COVID victims.
Dr. Julia Koehler
Boston
Dr. Regina LaRocque
Wellesley
We remain vulnerable to long COVID
Ashish Jha’s position as former White House COVID-19 Response Coordinator is a conflict of interest masquerading as a qualification for his op-ed. Researchers who study long COVID stated in a recent paper in Nature Reviews Immunology that “the oncoming burden of long COVID faced by patients, health-care providers, governments and economies is so large as to be unfathomable.” Rapid tests, which are less accurate with recent strains while PCR tests are less available, and low death rates give a false sense of security.
I agree that despite progress, more buildings need the air filtration and ventilation that would make public life safer. But Jha omits our vulnerability to long COVID after even mild infections, its devastating effects, and higher death rates for hospital-acquired COVID-19, combined with a lack of collective protection in health care settings with unmasked, untested people who prefer to ignore COVID-19.
Aside from advocating vaccines, he describes an everyone-for-themselves approach, not mentioning responsibility to protect others or access to essentials.
Jha dines in a restaurant with his friends while patients even in leading cancer hospitals are forced into Russian roulette, thanks to this approach.
Kathryn Nichols
Cambridge
Vigilance is necessary to prevent long COVID
While I understand the desire to promote optimism amid the ongoing pandemic, I am deeply concerned about the potential consequences of downplaying the importance of COVID precautions and the significant risk of long COVID. As a person living with long COVID for the last 16 months despite being vaccinated and boosted, I have experienced post-exertional malaise, fatigue, headaches, joint and muscle pain, cognitive dysfunction, and more symptoms that have continued to today. I have tried numerous medicines, supplements, and even participated in a clinical trial, only to find limited relief from the persistent effects of this virus.
Such a stance overlooks the reality that millions more people could end up with long COVID if we fail to remain vigilant in our efforts to combat the virus. Long COVID is a devastating consequence of this virus, and we cannot rely solely on vaccinations to end the pandemic. Even with widespread vaccination, the risk of contracting long COVID remains high. A recent study funded by the NIH’s RECOVER initiative showed that 10 percent of adults infected with COVID still have symptoms six months later. Minimizing the significance of long COVID not only neglects the suffering of long-haulers but also risks undermining public health efforts to control the spread of the virus.
By raising awareness about the risk of long COVID, media outlets can play a pivotal role in educating the public and promoting continued vigilance. Responsible reporting on the enduring impact of long COVID can serve as a reminder that the pandemic is far from over and that we must remain committed to taking necessary precautions to protect ourselves and others. Highlighting the struggles of long COVID survivors and the lack of proven treatments can spur further research and medical advancements in addressing this condition. Empathy and support for those living with long COVID are essential in paving the way for better understanding, compassionate care, and better health outcomes for everyone as COVID rates increase again this summer.
Travis Hardy
Norwalk, Conn.
Link https://www.bostonglobe.com/2023/08/05/opinion/cant-ignore-long-covid-jha/
406 notes
·
View notes
Text





"Wear it and stay healthy," a comic about masking in solidarity with Palestinians. I made it for Steel Transplant's digital release COVID CAUTIOUS QUEERS ZINE 2 ($0+).
It's a collage of transparent printed text from news/science articles, magazine scraps, & marker drawings of posts by Muhammad Smiry & Omar Hamad. Title is a quote from Hala, a Palestinian girl who sold masks in Gaza until she was killed by Israel last June.
Support Muhammad, Omar, Care for Gaza, and Needle of Hope, and always MASK UP!
(Alt text in post, all sources under the cut:)
PAGE 1
White graph paper: "Her name is Ghazal, she sells masks everyday to make a living | Gaza" - Orig @MuhammadSmiry post (2/28/24):
Transparent text:
"white phosphorous" - Youmina Boukara et al, Gaza, armed conflict and child health, BMJ Pediatrics Open (2/12/24)
"two million Palestine refugees" - Masako Horino et al, Understanding coverage of antenatal care in Palestine: Cross-sectional analysis of Palestinian Multiple Indicator Cluster Survey, 2019–2020, PLOS ONE (2/2/24)
"severe COVID" - Hatem A Hejaz, Palestinian strategies, guidelines, and challenges in the treatment and management of coronavirus disease-2019 (COVID-19), Avicenna J Med, (10/13/2020)
"60 times more likely" - “In Israel, you’re 60 times more likely to have a COVID vaccine than in Palestine” - Matthias Kennes for MFS (2/22/24)
PAGE 2:
White graph paper: "A little girl named Hala stopped me today and gave me this mask." - Post by @OmarHamadD (5/21/2024)
Transparent text:
"In this necroeconomy, lives are rendered and disposed of" - Nadia Naser-Najjab's book, "Covid-19 In Palestine: The Settler Colonial Context" (1/11/24)
Asma'a Adjerid's summary of the same book, MEDIA WATCH: BOOK (May 2024)
PAGE 3
White graph paper: "Didn't you know? She went to heaven three days ago." - Omar Hamad's 6/4/24 thread updating his post about Hala.
Transparent text:
"abduction of children" - Youmina Boukara et al, Gaza, armed conflict and child health, BMJ Pediatrics Open (2/12/24)
"long list of banned items" - ‘Long List of Banned Items’ – From Maternity Kits to Wheelchairs, Israel Blocks Gaza Aid (4/12/24)
"the implications are excruciating" - Tamara Qiblawi et al, Anesthetics, crutches, dates: Inside Israel's ghost list of items arbitrarily denied entry into Gaza, CNN (3/2/24)
PAGE 4
@OmarHamadD's thread about Rimas (8/12/24): https://x.com/OmarHamadD/status/1792981447889801725
Transparent text:
"US spends a record $17.9 billion on military aid to Israel since last Oct. 7" - Ellen Kickmeyer, CNN, (10/7/24)
The other small scraps are from the previously cited scientific papers & news articles.
PAGE 5
Brown paper:
"Wear it and stay healthy." - Hala, as quoted by @OmarHamadD (5/21/24)
Transparent paper:
Map of Palestine, with 2024 borders for Gaza and the West Bank.
"...freedom and justice...my true priority" - quote from Naser-Najjab, "COVID-19 in Palestine" (2024).
#collage art#queer comics#lgbt comics#disability justice#free palestine#covid isn't over#marker art#disabled artist#queer art#free gaza#mask up#global solidarity#disabled queer#covid cautious#comics#nonfiction#collaging#mixed media
31 notes
·
View notes
Text
Mark Sumner at Daily Kos:
Louisiana Gov. Jeff Landry signed a bill requiring every public school classroom to display the Ten Commandments after bragging that he “can’t wait to be sued” for this outrageous assault on the Constitution. But the legislation package does a lot more than force Christianity on children. For example, it also removes requirements for COVID-19 vaccinations and limits other vaccinations. Not only is the overall package a hodgepodge of religious right thirst traps, but the part about the Ten Commandments includes plenty of outright strange.
[...]
6. SCHOOLS ARE PROHIBITED FROM EVEN ASKING ABOUT STUDENTS’ VACCINATION STATUS
While the first five items were all crammed into the single bill about the Ten Commandments, Landry actually signed off on a package of items, including a prohibition on COVID-19 vaccine mandates. But that doesn’t really matter, since another bill in the package entirely eliminates school officials’ authority to check vaccination status. To put a double underline under this prohibition, teachers aren’t allowed to ask about vaccination status, but if they somehow become aware, they’re not allowed to seat students in a way that might prevent the spread of disease in their classrooms. They also can’t prevent unvaccinated kids from participating in any in- or out-of-school activity. Because that would be “discrimination.” And you know how much Southern Republicans hate discrimination.
7. TEACHERS CAN BE SUED FOR USING A STUDENT’S PREFERRED NAME OR PRONOUNS
The legislation requires that students only be assigned pronouns according to what is called their "immutable sex" as found on their birth certificates. They can also only be addressed by the name found on their birth certificates or by nicknames “derived from that name.” Is Betsy okay for Elizabeth? How about Bess? Lizzie? Can you use Jack for John? Is Rory really an acceptable nickname for Lorelei? Teachers better be on top of these things because the bill makes them personally liable, allowing them to be sued if they don’t keep those nicknames and pronouns straight.
8. A “DON’T SAY GAY” BILL WORSE THAN FLORIDA’S WAS ADDED ALMOST WITHOUT NOTICE
The “Let Kids Be Kids” act protects delicate ears from any mention of sexual orientation, gender identity, or sexual orientation all the way through grade 12. No teacher, coach, or other school employee is allowed to engage in any discussion on these topics. They’re also not allowed to reveal their own gender identity or sexual orientation.
While Louisiana’s infamous 10 Commandments in schools law (HB71) has generated lots of rightful criticism for inserting religion into public school classrooms, the bill was passed as part of a package of education items, including enacting an anti-LGBTQ+ Don’t Say Gay or Trans law deceitfully called the “Let Kids Be Kids” Act to apply to all K-12 school classes (HB122), prohibiting the inquiry of a student’s vaccination status or ways to safely contain the spread of diseases (HB908), and a forced misgendering law that students can only be assigned pronouns based on the gender assigned at birth and can only use their birth name or derivatives of it. (HB121)
#Louisiana#Jeff Landry#Schools#Education#Vaccine Mandates#Don't Say Gay or Trans#Ten Commandments#Pronouns#Forced Misgendering#Chaplains#Louisiana HB334#Louisiana HB122#Louisiana HB121#Louisiana HB908#Louisiana HB71#LGBTQ+#Transgender#Anti LGBTQ+ Extremism#Anti Trans Extremism
42 notes
·
View notes
Text
Reading Between the LIES
A Double-Minded¹ man is UNSTABLE in ALL he does:


wavering in character & feelings
restless & confused in thoughts, actions & behavior
like a drunken man who is unable to walk in a straight line

youtube
"I'm fiercely pro-vaccine." RFK Jr
youtube
...unless I'm hiking which is when I tell strangers "...better not get (that baby) vaccinated..."

or when I intend to use 6 month old babies as non-consenting VOLUNTEERS aka "human pin cushions" to TEST (study) vaccine safety & efficacy

youtube
"Reading between the LIES" by Peggy Hall
youtube
¹James 1:6-8
The operative name in Robert F. Kennedy Jr. is “Kennedy.” -Isaac Schorr
At his confirmation hearing on Wednesday, President Trump’s nominee to run the Department of Health and Human Services fielded countless questions about the countless views he’s articulated and actions he’s taken that make him uniquely unsuited for this position.
And, as you might expect of any Kennedy, his answers were full of obfuscations, half-truths, and outright lies.
In his opening statement, Kennedy tried to sidestep the single biggest cloud hanging over his nomination.
“I believe that vaccines play a critical role in health care,” he proclaimed.
“All of my kids are vaccinated, I’ve written many books on vaccines, my first book in 2014, the first line of it is ‘I am not anti-vaccine’ and the last line is ‘I am not anti-vaccine.’”If only saying it made it so.
Kennedy has a decades-long record that reveals him to be exactly what he says he’s not.
While he touted his kids’ vaccination status at his hearing, he has previously said he would “do anything” and “pay anything” to go back in time and change that fact.
In 2021, he said that “I see somebody on a hiking trail carrying a little baby and I say to him, ‘Better not get them vaccinated.’”And that’s to say nothing of him being the founder and former chairman of an anti-vaccine group going by the Orwellian name “Children’s Health Defense,” which is currently promoting a film called “Vaxxed III: Authorized to Kill.”
In another notable moment, Kennedy was quizzed about his role in exacerbating a measles outbreak in Samoa that claimed the lives of more than 80 people – most of them young children – in 2019.
Kennedy traveled to the island nation in June of that year at the invitation of another anti-vaccine activist following the deaths of two babies improperly administered vaccines.
On Wednesday, Kennedy insisted his visit had “nothing to do with vaccines” and that he “never gave any public statement about vaccines.”
The Samoan Ministry of Health sees it differently.
“It is well documented that RFK Jr.’s visit to Samoa in 2019 coincided with increased anti-vaccine sentiment, particularly among certain groups,” it said in a statement.
Moreover, in the aftermath of the outbreak, Kennedy sought to exploit the tragedy to push the Samoan Government toward anti-vaccine policies.“It is critical that the Samoan Health Ministry determine, scientifically, if the outbreak was caused by inadequate vaccine coverage or alternatively, by a defective vaccine,” wrote Kennedy in a letter to the prime minister.
There he was again, just asking questions.
Kennedy’s attempts to explain away his own words – nay, his life’s work – fell short in numerous other instances.Asked about his suggestion that Covid-19 may have been genetically engineered to spare Ashkenazi Jews and Chinese people, Kennedy insisted that he was only quoting an NIH study.
The truth? That he said that the virus “is targeted to attack caucasians and black people,” while Ashkenazi Jews and Chinese “are most immune.”
As to whether it had been engineered to do so, well, Kennedy thought that was an open question.
“We don’t know whether it was deliberately targeted or not,” he added.
Asked about a series of overwrought, irresponsible comparisons he’s drawn while promoting his dangerous lies, he denied having ever made them.
Roll the tape, however, and you’ll find that he’s said that the CDC’s decision not to deem autism an epidemic was “like Nazi death camps,” and analogized the agency’s priorities to those of fascist regimes and the Catholic Church’s “pedophile scandal.”
And then there’s his cynical abortion flip-flop, which was addressed by senators of both parties on Wednesday.
“I agree with him [President Trump] that we cannot be a moral nation if we have 1.2 million abortions a year,” declared Kennedy at his hearing.
If that’s the case, why did he express support for full-term elective abortions on the campaign trail less than a year ago?
Robert F. Kennedy Jr. is many things that his famous family resents: A kook, an embarrassment, and, worst of all, in league with the Republican Party.
But his most ignoble trait – the one on full display on Wednesday – is one that he shares with the rest of his clan: He’s a power hungry charlatan willing to say anything to take the next step up the ladder.
#grifters gonna grift#predators#liar#bobby kennedy#rfk jr#healthy american#peggy hall#fraud#baby chickens in blender#decapitated whale#central park bear#Reading Between the LIES#baby chicks#pet falcon
12 notes
·
View notes
Text
JAPANESE SCIENTISTS DISCOVER THAT COVID-19 VACCINES TURN HUMAN BODY INTO A CONTROLABLE COMPUTER DEVICE!!!!!
Japan Declares State of Emergency After ‘Nanobots’ Found in 96 Million Citizens 🇯🇵
Japan has issued an apology to its citizens for the disastrous consequences of the COVID-19 mRNA vaccines and has launched far-reaching scientific inquiries and criminal investigations to establish the truth and punish the perpetrators.
The globalist elite and Big Pharma are panicking, terrified of what the Japanese are finding, and they are doing everything they can to discredit these investigations, including ordering the mainstream media to initiate a total media blackout of any news coming out of Japan.
But we are not going to allow the elite to succeed in gaslighting the public any longer. Japan are uncovering crimes against humanity and the whole world needs to hear this information.https://x.com/tpvsean/status/1822373262979911749
26 notes
·
View notes
Text
Millions of Americans may have unknowingly received COVID-19 mRNA vaccines as part of covert hospital programs allegedly designed to secure federal funding, according to U.S. attorneys leading a high-stakes investigation.
Some patients have reported experiencing unexplained symptoms they believe are linked to vaccination or discovering that their medical records list them as vaccinated without their consent, raising concerns about unauthorized medical interventions.
Attorneys investigating the matter reveal that testing to confirm whether someone was vaccinated without consent could soon become widely available.
If these allegations are proven, it will mark one of the most significant ethical scandals in American healthcare history.
Some whistleblowers have pointed out that hospital admission forms might have contained clauses in the fine print which granted authorization for vaccination. However, critics argue that many patients were unaware of such provisions, raising concerns about the adequacy of informed consent. For those who did not sign any such forms, their cases could set legal precedents in court.
ttps://twitter.com/DowdEdward/status/1872369121717014950
As the investigation progresses, class action lawsuits will be filed against hospitals found responsible. Individuals affected will have the opportunity to join these legal actions.
10 notes
·
View notes
Text
Make your voice heard and ask the CDC to:
Recommend updated 2024-2025 COVID vaccines for all ages AND
Strengthen our vaccine drive by recommending more frequent boosting (at least every six months) and more frequent updates to the vaccines, adjusted for the latest variants.
Submit a public comment using our sample language below.
You can also register to give Oral Public Comment at the upcoming June 26-28 online CDC ACIP Meeting at: https://www2.cdc.gov/vaccines/acip/acip_publiccomment.asp
Submit written comments and/or register to make oral comments at the meeting by Monday, June 17 at 11:59pm Eastern Standard Time.
It’s important to submit a personalized comment, which can be brief. Ideas for a personalized comment:
How you, your family, or your community would be impacted by fall vaccine eligibility being restricted to only high risk groups (such as older age or immunocompromised status)
Barriers to vaccination your have faced, particularly if your eligibility was questioned or misinterpreted by a vaccine provider
How out-of-pocket costs are a barrier to getting the latest vaccines
Also feel free to take inspiration from or borrow the language in our sample public comment below.
Docket No. CDC–2024–0043
Updated 2024-2025 COVID vaccines must be recommended for people of all ages, regardless of health status. A restrictive approach to eligibility would create undue barriers for vulnerable people and discourage high risk people from getting needed vaccine boosters.
The vaccine schedule should address waning efficacy in the months following vaccination [1-3] as well as emergence of new SARS-CoV-2 strains by recommending updated vaccination for all ages, at least every six months. Recent vaccination is also associated with a lower risk of developing Long COVID following a COVID infection [4] as well as a lower risk of Multisystem Inflammatory Syndrome in children (MIS-C) [5].
The CDC’s clear and unequivocal recommendation of updated COVID vaccination for all ages will influence what healthcare providers recommend, and what health insurances cover. Moreover, it will improve public awareness regarding the need for updated vaccination.
The CDC must ensure equitable and affordable access to updated vaccines and prevent limited access because of financial constraints or demographics. The CDC’s Bridge vaccine access program is slated to end August 2024 and must be extended to ensure uninsured and underinsured people have access to the updated vaccines this fall [6].
References:
1. Link-Gelles R. Effectiveness of COVID-19 (2023-2024 Formula) vaccines. Presented at: FDA VRBPAC Meeting; June 5, 2024. Accessed June 12, 2024. https://www.fda.gov/media/179140/download
2. Wu N, Joyal-Desmarais K, Vieira AM, et al. COVID-19 boosters versus primary series: update to a living review. The Lancet Respiratory Medicine. 2023;11(10):e87-e88. doi:10.1016/S2213-2600(23)00265-5
3. Menegale F, Manica M, Zardini A, et al. Evaluation of Waning of SARS-CoV-2 Vaccine–Induced Immunity: A Systematic Review and Meta-analysis. JAMA Netw Open. 2023;6(5):e2310650. doi:10.1001/jamanetworkopen.2023.10650
4. Fang Z, Ahrnsbrak R, Rekito A. Evidence Mounts That About 7% of US Adults Have Had Long COVID. JAMA. Published online June 7, 2024. doi:10.1001/jama.2024.11370
5. Yousaf AR. Notes from the Field: Surveillance for Multisystem Inflammatory Syndrome in Children — United States, 2023. MMWR Morb Mortal Wkly Rep. 2024;73. doi:10.15585/mmwr.mm7310a2
6. https://www.cdc.gov/vaccines/programs/bridge/index.html
Full instructions for written and oral comment and meeting information can be found at: https://www.cdc.gov/vaccines/acip/meetings/index.html
You can also register to give Oral Public Comment at the upcoming June 26-28 online CDC ACIP Meeting at: https://www2.cdc.gov/vaccines/acip/acip_publiccomment.asp
You must register by June 17 at 11:59pm Eastern Standard Time
CDC’s ACIP meeting information on the Federal Register: https://www.federalregister.gov/documents/2024/05/24/2024-11439/meeting-of-the-advisory-committee-on-immunization-practices
Vaccination with the latest updated vaccines continues to be foundational to a multilayered approach to COVID, providing protection against both acute disease and Long COVID. Far too few Americans have received the latest vaccines. Only approximately 22.6% of adults and 14.8% of children have received the latest 2023-2024 vaccines (as of June 1, 2024), which have been available since Fall 2023. COVID vaccination rates in both groups lags far behind influenza vaccination rates. Only 7.1% of adults aged 65 and older received the recommended two doses of the 2023-2024 vaccine (as of April 27, 2024).
Vaccine efficacy wanes significantly four to six months following vaccination, making updated vaccination important for all people as COVID continues to spread in our communities. Vaccine approaches that restrict access based on age or risk status put all of us at risk and leave those at high risk of severe consequences of COVID infection confused about whether they qualify to receive additional doses. A more frequent vaccination approach providing vaccination at least every six months as well as frequent updates to match current variants is needed to better protect all of us amid year-round COVID spread.
The CDC’s Bridge Access Program, which provides COVID vaccines to uninsured and underinsured adults free of charge, is due to end August 2024. The end of this program will unnecessarily put vulnerable people at risk, and public health officials must advocate for continuation and expansion of this program.
Submitted written comments or registration to make oral comments at the meeting must be received by the CDC no later than June 17 at 11:59pm Eastern Standard Time
28 notes
·
View notes
Text
It's 2024 and there are still companies requiring you to disclose your Covid-19 vaccination status on your application? Maybe it's time to start reporting these for discrimination 🤡 That said, I reported the job for a different reason; containing incorrect listing information because it said $16.25 and when you clicked though to the application it was actually $15.00 which is below the legal minimum. so clearly they're playing fast and loose with the law in any case 🤡
38 notes
·
View notes
Text
Also preserved on our archive
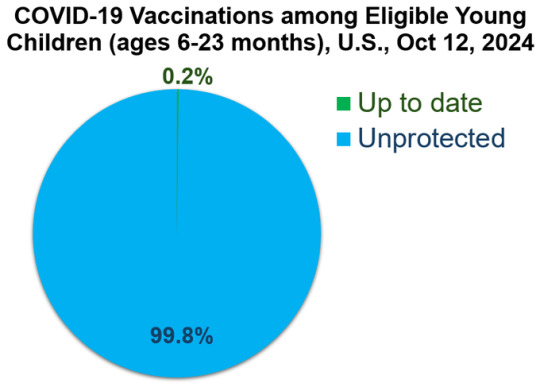
How is this not national news?
At a glance Weekly estimates of COVID-19 vaccination coverage and parental intent for vaccination among children are calculated using data from the National Immunization Survey–Flu (NIS–Flu). COVID-19 Vaccination Coverage and Intent for Vaccination, Children 6 months through 17 years Weekly estimates of COVID-19 vaccination coverage and parental intent for vaccination among children through December 31, 2023, were calculated using data from the National Immunization Survey–Child COVID Module (NIS–CCM). The NIS–CCM was discontinued at the end of 2023 and questions regarding COVID-19 vaccination status and intent were added to the National Immunization Survey–Flu (NIS–Flu).
NIS–CCM and NIS–Flu are national random-digit dial cellular telephone surveys of households with children ages 6 months through 17 years; NIS–Flu is conducted during October-June. The respondent to a NIS–Flu survey is a parent or guardian who said they were knowledgeable about the child's vaccination history. All estimates are based upon parental report of receipt of vaccination and month of that vaccination.
Weekly comparisons to previous season should take into account differences between seasons in vaccine availability dates. 2023–24 COVID-19 vaccines were first available mid-September 2023, and 2024–25 COVID-19 vaccines were first available at the end of August 2024.
The NIS–Flu data posted on the dashboard below are currently a few days behind the data that are posted on the Respiratory Illnesses Data Channel. This lag is due to the time it takes to review data by geographic and sociodemographic characteristics and summarize the findings.
(Follow the link for interactive graphs and all the data)
112 notes
·
View notes
Text
On August 1st we venerate Ancestor Henrietta Lacks on her 103rd birthday 🎉

Sister Henrietta is known throughout the world as, "The Mother Of Modern Medicine", being the biological source of the HeLa cells - 1st immortalized human cell line, which has been central to cancer research studies & methods. Billions of her cells are presently used in biomedical research development around the world, notably in the manufacturing of COVID-19 vaccines, mapping the human genome, HIV/AIDS & cancer treatments, testing human cells against zero gravity in space, other vaccine research, & undoubtedly much more.
Today, however, venerate the woman behind the medical atrocities that it took to achieve such a feight.
Born Roanoke, VA, a young Henrietta grew up working on a tobacco farm with her father, her 9 siblings, & extended relatives on their land in Clover, VA - where their ancestors had worked as slaves. She'd lost her to complications of child birth when she was just 4yrs old. Due to his lack of patience, her father divided his children to be raised among different relatives accordingly. Henrietta was to be raised by her grandfather, who had already taken in her First-Cousin, David "Day" Lacks - who she later married. Henrietta continued her schooling until the 6th grade. On a hopeful prayer, they left Clover, VA for Turner Station, MD to escape the impoverished life that came with tobacco farming. There, they settled down to start their family.
While pregnant with her 5th child, Henrietta discovered a painful knot inside her that persisted through atypical bleeding post-childbirth, among other symptoms. Finally, she sought medical treatment. Prior to this, she & her family would lay flowers at the local Jesus statue, recite prayers & rub his feet for good luck. Henrietta kept her diagnosis to herself so as to not worry her family; she was determined to overcome her medical condition on her own.
While receiving treatment at a segregated ward in John Hopkins University, doctors took a tissue sample of her tumor for medical research without her knowledge or consent. This was an everyday practice at most medical institutions of the time. Unfortunately, Sister Henrietta did not survive her treatment. She was later buried at the Lacks Family Cemetery in Clover, Va.
Following her death, the medical research scientists from John Hopkins University coerced her husband to consenting to have an autopsy conducted on her remains; they claimed doing so would provide beneficial health information to his children. This allowed them to lawfully collect tissue samples from all of Henrietta 's organs. As of 2020, the cells from these tissue samples that were collected on that day & prior are THE most widely used in biomedical research labs around the world.
For all her pain, suffering, & desecration (of which the latter continues presently), may Sister Henrietta be forever elevated in peace, healing, & light in the spiritual as her physical essence has become immortalized in the physical.
We pour libations💧& give her 💐 today as we celebrate her for her love of family, community, & faith.
Offering suggestions: prayers toward her elevation, libations of water, catholic prayers, & a Catholic Bible.
‼️Note: offering suggestions are just that & strictly for veneration purposes only. Never attempt to conjure up any spirit or entity without proper divination/Mediumship counsel.‼️
#hoodoo#hoodoos#atr#atrs#the hoodoo calendar#ancestor elevation#ancestor veneration#henrietta lacks#HeLacells#HeLa#black history#modern medicine#medical apartheid#us history
108 notes
·
View notes