#and those of us with stigmatized mental health conditions are the ones who lose access when everyone goes all the time
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr.com is the 103rd most visited website in the world.
Text
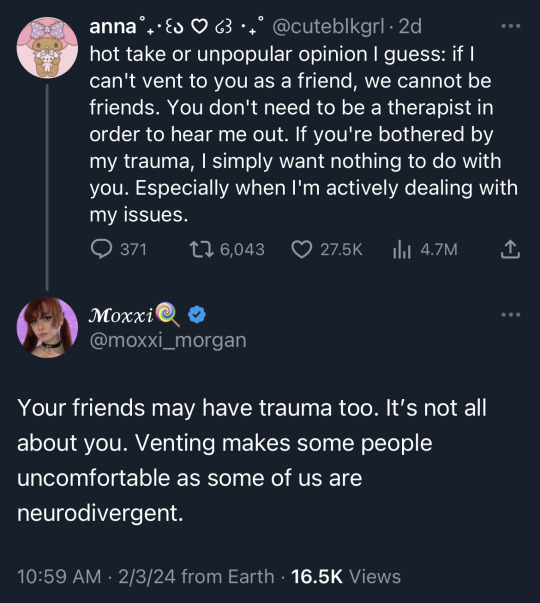
generally I do agree with listening to your friends and caring for one another- but then you get those people who think all friendship is, is venting and y'all aren't even close- like i still want to help, but there's a limit. plus, frankly i've gone through so much worse i have a hard time empathizing especially bc she exaggerates to try to elicit sympathy- i don't know how to tell her she'll find more friends if she can just be chill the first few times she meets someone. anyway, personal rant. also, therapists aren't actually for venting at. all y'all whining about your 'stressful' days are why people with actual disabling mental health conditions can't get therapist. thanks y'all've flooded the market and it's much easier to help someone feel better about being nervous about speaking up more than it is someone who is a skitzo or manic and dealing with unmanaged hallucinations. Plus, the pay's the same so who do you think gets the boot? gets the seek help somewhere else? gets the have you tried [mentions the first two obvious resources out of the 40 i've looked into] therapist don't even treat people with "serious" mental health conditions anymore, smh. And it's all thanks to people like you probably.
? where am i
#look everyone deserves therapy#but you don't go to a doctor every week to check on a painful but managed wound either#therapist#if this sounds like youconsider short term therapy 6-8wks on then 2-3months off to change habits or what get you need [might even work bet#or maybe just go once a month instead of one or more times a week#therapy is a limited resource#and those of us with stigmatized mental health conditions are the ones who lose access when everyone goes all the time#i literally have been verbally rejected by 12 and counting providers (not counting all the ghosting)#some even agreed to treat me/told me their schedule until i mentioned the bi-polar and recent hyper swing#all of them immediately change tune#even those that list it as something they treat; and i didn't even mention the more stigmatized comorbidities#this post got away from me#seeking therapist in nyc area [shot in the dark]#if you can get the same help from friends#you don't need therapy#not even the closest friend could help me with what i need therapy for- professional expertise is essential in my treatment#if i can even get Tx again lol
29K notes
·
View notes
Text
Geriatric Counselling: What Is It?
Geriatric Counselling is a kind of mental health therapy that assists individuals in overcoming several difficulties. It is particularly beneficial for seniors who are grieving the death of a loved one or who are suffering from physical challenges that are making their life tough.
A senior counselor is often a psychologist or social worker specializing in seniors. They contribute to the improvement of older patients' quality of life and guarantee that they get competent medical treatment.
Geriatric Counselling is a profession that focuses on assisting senior citizens. It requires understanding the aging process and coping with issues like loss of mobility or independence, disease, mental health concerns, and grief.
A geriatric counselor's work includes analyzing seniors' requirements and developing a strategy to enhance their quality of life. They may also aid older persons in locating social and health resources and support programs.
They support a wide range of senior clientele, including those in nursing homes and assisted living institutions. They also serve as a liaison between elderly patient and their doctors.
Moreover, senior counselors often help family carers cope with the emotional and physical impacts of caring for an elderly loved one. According to the Family Caregiver Alliance, they include burnout and despair.
Geriatric Counselling is a psychotherapy designed to assist older people in dealing with different challenges and concerns. It focuses on giving individuals the tools to enhance their quality of life.
A master's degree and specialized training are usually required. Upon completion, you will be eligible to get your state's counseling license and operate as a senior therapist.
A senior counselor is trained in neuropsychology, psychology, and mental health to treat various mental illnesses that might impact the elderly. Depression, dementia, and drug misuse are examples of these illnesses.
Seeing an older patient is an emotional challenge for the therapist as they attempt to grasp the physical and psychological changes that occur with age. In addition, the therapist must learn how to deal with the narcissistic losses that come with age.
Geriatric Counselling is a treatment that focuses on dealing with older adults. Counselors use several methods to assist clients in improving their mental and physical health.
They may collaborate with a geriatric clinic, long-term care institution, or senior center to offer services tailored to the requirements of the elderly. They must be knowledgeable about medical diseases affecting the elderly and the most recent technologies and treatment alternatives.
A senior counselor may also assist elder carers in dealing with stress and exhaustion. These experts often arrange regular visits with their patients to ensure they get the help they need to live freely.
Geriatric counseling may be a productive and enjoyable vocation. It's a terrific opportunity to meet new people and learn meaningfully about other people's lives. It also encourages older folks to be optimistic and excited about the future.
Geriatric Counselling is a therapy that assists older adults in coping with aging. It also helps individuals access their inner resources and find new purposes in their lives.
People lose their freedom as they age due to health difficulties and physical restrictions. This might lead to a sense of emptiness and loneliness.
Seniors may discuss their worries without fear of being judged during a geriatric counseling session. They may communicate their sentiments without fear of being stigmatized, giving them the strength and self-esteem to continue ahead.
For older folks, mental health is becoming a rising problem. According to the Institute of Medicine, roughly one in every five senior Americans has a mental health condition.
Depression is more frequent among the elderly, yet it is difficult to recognize. Numerous symptoms might be mistaken for physical or dementia-related issues. As a result, counselors must be able to distinguish between psychological and bodily issues and know when to recommend medical testing.
1 note
·
View note
Text
Today’s conversation is around psychosis and mental health. So psychosis by dictionary definition means “a severe mental condition in which thought and emotions are so affected that contact is lost with external reality”. Psychosis can happen to anyone but particularly affects those with mental health. I have had multiple life altering psychosis experiences that were not pushed forward by drug use or anything like that. Psychosis for people with depression or Bipolar like myself can mean life or death. Going off with strangers, losing touch with current real things going on in my personal life, and losing access to resources have all happened to me as a result of my psychosis.
Friends I’ve had as well as my family has had to filter through the fallout after a period of psychosis is over. They have been triggered and traumatized as well as me once these periods are over and navigating mental health afterwards is always a struggle. When psychosis episodes occur it usually is when I’m not medicated or actively complying with treatment so it takes a lot of time to get back in the groove of things afterwards.
I spent my 21st birthday in a treatment facility for my mental health. I had one visitor. I had a cake. And there are so many times when I have wished to not be diagnosed with clinical depression or social anxiety but reality is sometimes doing things or dealing with things we as people don’t want to. And mental health for so long was something that I allowed to stigmatize me and pigeon hole my possibilities. I would feel insecure that my accomplishments or ambition didn’t match my peers and at first it would hurt my feelings or make me further depressed. Then one day I decided that my life is not on a timeline comparable to other people I know who don’t have the same mental health diagnosis’s. I can take accountability for treatment and for activities that positively affect my mental health as well as breakdowns because with a proper treatment regimen it won’t happen or warning signs will be noticed by professionals long before it becomes something that threatens my stability. I encourage anyone with mental health to find hobbies and tasks to do throughout the day that allow your mental health to flourish when it can.
1 note
·
View note
Text
The Moralization of Intimate Partner Relationship Loss Is Harmful to Women and Families

Artist: Emma Amos
Relationship loss that takes place in the in the context of intimate partner relationships including marriage should be treated and talked about just as that, an experience of relationship loss. The loss can take many forms, sometimes public and visible to others, and sometimes invisible. It can be an extremely traumatic loss like in cases where there is an unexpected death, violence, various forms of abuse, social pressures and conditions (poverty, forced migration, etc.) or it can be less traumatic but still a significant loss.
Every week I work alongside women, many who have suffered relationship loss under the traumatic conditions of Intimate Partner Violence and/or Domestic Violence. The unimaginable work they have to do to move towards health and increased safety is made harder by societal shame associated with relationship loss in the context of intimate partner relationships including marriage. Try to imagine/remember a time that you or someone you know suffered a traumatic loss. Think about the grieving process that was associated with that traumatic loss and the need for social supports that hopefully you or the person received. Now imagine on top of that grief, having to deal with recovery from the impacts of abuse/violence (health, mental health, financial, social impacts). Most of us would imagine an individual going through all these as the best candidate to be showered with support, love and affirmation. But the reality is that women all around us facing these experiences are extended the least support, most judgement and they are the most isolated they have ever been in their lives. The reason for this is because of messages that we perpetuate about intimate partner relationship loss especially in the context of marriage that are arbitrary at best and violently misogynistic and deceptive at worst.
Talking about intimate partner relationship loss (including divorce) primarily/dominantly/singularly through a moral lens is dangerous, sad and detrimental practice. There are faith and cultural traditions where this practice is particularly pronounced. Because I live at both faith and cultural contexts where intimate partner relationship loss is widely viewed as a moral failure or poor moral choice, I have had the opportunity to examine these views and bear witness to the impact especially on women’s lives. The practice creates stigma and like all forms of social stigma, it eventually becomes internalized and people go through their faith and cultural identity formations. For most of us who come from these particular faith and cultural communities, if we are to experience intimate partner relationship loss then we also experience self stigma and if we are to witness the loss in someone’s else’s life, then we view that person through a stigmatized lens. My close examination of these views has also led me to conclude that they are not so much based on sacred text or ancestral wisdom as they are rooted in patriarchy and misogyny and as such the impact disproportionately gendered, with women suffering the worst effects.
The truth is that more than we are often willing to admit, all forms of functional human relationship are more of a privilege and a gift from Creator, than a result of moral choices. Even if an initial choice is made, there are still sets of conditions and abilities that we may not think about daily that make it possible for us to maintain relationships. I am not a mother to my sons because I vowed to be one, even if there were initial choices made, my capacity to go on being a mother is fueled by a loving bond and just as importantly by conditions and abilities that I depend upon to support my mothering. My physical ability to move around and pursue access to the local economy and means to production, enough mental ability to relate to my children at various stages of development, the general stability of my social environment that allows me to access food and water and free education for my children, basic healthcare, the absence of war, etc. And when I experience various forms of instability, vulnerability and disability that impact my mothering, mitigative protective factors allow me to maintain some measure of meaningful parental relationship that other mothers might lose and do lose in similar conditions. There are conditions and abilities that if lost, so would my ability to parent resulting in a devastating relationship loss. This is the reality for all parents.
My view is that we should move towards being increasingly attuned and mindful to the conditions and abilities that allow us to be in various forms of human relationship, including intimate partner relationships like marriage. And to approach these conditions and abilities with gratitude. This will also hopefully spur us to extend to those experiencing relationship loss compassion, dignity and empathy and take a posture of humility towards diverse experiences. It is violent to impose stigma and narratives of failure over experiences of loss and trauma. For example, using words like “failed” and “broken” to describe relational experiences. Talking about failed marriages or failed families, or broken families is just as gross as it would be to talk about failed parents, failed children when describing other common types of relationship loss. And increasingly I am realizing it is not compassionate language rather it is a moral judgement imposed on a form of relationship loss.
From a faith perspective and walking alongside other women of shared faith and cultural context in my work, who are trying to process traumatic intimate partner relationship loss and also recover from unhealthy marriages, I have come to appreciate that what is taught about marriage in various experiences of church and what is true of lived experiences and reflected in the text is not always the same. For example, in the text there is far more affirmation for women and mothers experiencing intimate partner relationship loss than there is for any other kind of woman experiences of relational privilege. There is no instance of families where relationship loss has been experienced are referred to as failed or broken, rather there are extensive promises, blessings and prophetic affirmations for families and women that have experiences of relational loss, where Creator promises to *personally* fill the gap that is left after an experience of a loss, this is the depth of compassion and identification with the loss and trauma. And even while so much of the ancient texts are located in cultures marked by patriarchy, where for women intimate partner relationships with men are also tied to social safety and security, I am amazed by how much redemptive promise and prophecy is situated within lived women’s lived experiences of relational insecurity and experiences of loss. For me this speaks to the validity in diverse women’s lived experiences including experiences of relationship loss which all contribute to our life story which is sacred. This would be important information to be included as we support women and girls in the church as they navigate their own identity formation and process diverse life experiences. The same shift is possible with women from any cultural/faith tradition where patriarchal values result in the hyper-moralization of intimate partner relationship loss with detrimental impact on the health of families experiencing loss and especially on women.
0 notes
Link
While the entire globe has been focused on battling COVID-19, our nation’s ongoing opioid crisis has not disappeared. In fact, it may be worsening.
Early data from the Overdose Detection Mapping Application Program, a federally funded national surveillance tool, shows that drug overdoses are increasing during the pandemic, and local medical and law enforcement authorities across the U.S. are reporting spikes in overdose calls and deaths.
Public health officials fear the pandemic could spark a wave of new addictions due to increased drug and alcohol use linked to historic unemployment, as well as isolation fostered by state shutdowns and stay-at-home orders. One study by Well Being Trust estimated the COVID-19 pandemic could lead to 75,000 Americans dying from drug or alcohol misuse or suicide.
Opioid addictions are a financial problem for businesses, of course, but the toll in human suffering is far greater and more disturbing. Even in “normal” times, too many people who privately struggle with addiction do not reach out for help for fear of being judged. Fewer than one in five Americans are willing to be a friend, colleague, or neighbor of someone who is addicted to prescription drugs, according to a survey conducted by the Associated Press–NORC Center for Public Affairs Research.
I have learned from interactions with our nonprofit partner Shatterproof—and with colleagues who have lost loved ones to a drug overdose—that one of the most impactful ways to fight this national crisis is to take on the stigma associated with addiction.
Often, the language used when discussing addiction includes words that contribute to the stigma and shame, such as “drug abuse,” “addict,” and “clean and dirty” blood tests.
I personally have seen, as CEO, how I can change the perception of addiction by leading a companywide dialogue. I encourage all business leaders to drive cultural change within their companies and change the way we think and talk about addiction so that we can remove the hurdle of stigma for those who might otherwise seek timely help.
First, leaders need to educate themselves before leading a companywide dialogue on this once-taboo topic. They can learn by listening to local health experts and reading educational websites. Then they must ensure everyone in the company has access to these resources.
For example, on our company’s intranet, every article about the opioid crisis includes a link to an educational website offered through our Shatterproof partnership. Companies can provide addiction resources to employees in a number of ways, including links to the websites of federal agencies, such as the Centers for Disease Control and Prevention, within emails delivered to all employees.
Leaders can kick off a companywide conversation about addiction in many ways, such as an all-hands meeting. For me, it was a public call to action to companies, communities, and citizens to work together to end the opioid crisis in 2018. I outlined how the opioid crisis was taking a heavy toll on employers and employees who need addiction education and support such as employee assistance programs. My call to action was published externally on a magazine’s website, as well as on our intranet.
Because I have talked openly and nonjudgmentally about the opioid crisis and addiction, employees at The Hartford have felt more comfortable talking about these topics as well.
Our employees have responded by sharing their accounts of helping family members with substance misuse, losing loved ones to overdose, and volunteering at community organizations, such as Shatterproof Rise Up Against Addiction 5Ks. They have written blogs and social media posts on our intranet, which is like a social media platform allowing them to quickly create and share, and shared their thoughts with the entire company. One employee discussed her son’s struggle with opioid misuse. Another employee told the story of her 25-year-old daughter who died of a drug overdose. Others have reflected on losing a family member, friend, or neighbor as a result of the opioid epidemic.
In an intranet post, Allie Doney, who works as a senior legal assistant in our East Windsor, N.J., office, described her brother’s battle with opioid addiction after sustaining hockey injuries, which eventually led to him dying of a drug overdose. She tackled misconceptions about opioids and addiction: “This epidemic does not discriminate. It doesn’t matter your age, your ethnicity, race, religion, how much money you have in the bank, where you grew up—nothing.”
To continue the dialogue in a highly visible way, I engaged employees by commenting directly on their posts. Doing so was important to show that our company’s leadership stood behind them. In a small face-to-face meeting, I met with Allie and other employees whose loved ones died of drug overdose, asking to hear their stories and how our company could better support them.
Business leaders also have the responsibility to ensure that managers are empowered with information about the company’s benefits and health resources. They can direct their human resources and communications teams to educate managers so they can spot the signs of substance misuse and connect employees to support and treatment. They also can instruct their HR teams to talk with benefit providers, such as workers’ compensation and disability insurers, about addiction prevention strategies. Also, HR can speak with health care and prescription providers about improving access to treatment, including telemedicine and digital options.
Finally, as business leaders, we must use our voices to champion effective public policy solutions that address the addiction crisis. Over the last year, I connected with state and federal lawmakers regarding public policies dealing with the opioid epidemic. These discussions have focused on opioid prescription duration and dosage restrictions; mandatory physician and provider education about appropriate prescription opioid use; states’ prescription drug monitoring programs, which are electronic databases of prescriptions within the state that can help identify and deter or prevent drug misuse; and the adoption of restrictive drug formularies, which are lists that designate specific prescriptions for medical conditions.
Prior to the pandemic, we saw progress resulting from our nationwide, multi-stakeholder response. Now, in the face of COVID-19, adequate funding remains critical. I am encouraged to see federal lawmakers prioritizing the inclusion of substance use disorder and mental health funding in the recently passed Coronavirus Aid, Relief, and Economic Security (CARES) Act and other legislative proposals, such as the Health and Economic Recovery Omnibus Emergency Solutions (HEROES) Act.
There’s more to be done at the individual level as well.
Let us all commit to removing stigmatizing language from our vocabulary. It’s something that can be done no matter where we live or work.
Instead of “drug abuse,” we can say “substance use disorder.” Instead of “junkie,” we can say “person with a substance use disorder.” Instead of “reformed addict,” we can say “person in recovery.”
Most important, we can foster empathy and hope instead of stigma—and together, we can overcome the crisis that the pandemic has compounded.
Christopher J. Swift is chairman and CEO of The Hartford.
More opinion in Fortune:
Why is 10,000 steps a day the goal? Fitbit’s CEO has some answers
How companies can celebrate intersectional diversity in a remote-work world
America, you’re making a big mistake on immigration. And Canada thanks you
When should you sell your stocks? Only in these cases
Semiconductors are the engine of the global economy—and America isn’t making enough of them
from Fortune https://ift.tt/2VUY5kd
0 notes
Text
*Illuminate the Darkness*
This entry will examine the critical questions: “How do you see the feminine style at play in public discourse? Is it empowering? Is it limiting?”
To fully articulate the nature of these questions, I will be using Lady Gaga’s SAG-AFTRA GALA speech. Her speech relies heavily, but not entirely, upon the feminine style; this is ultimately empowering because it illuminates the severity of the global mental health crisis, igniting a profound foundation for open communication about this matter.
First and foremost, it is essential to clarify that the SAG-AFTRA Foundation is a nonprofit organization dedicated to providing its members with educational and state-of-the-art resources in order to pursue their craft. This foundation’s members consist of actors, voiceover artists, broadcasters, dancers, and other artists; Lady Gaga herself is an artist, but she begins her speech by admitting that in all honesty, she “[feels] very much like [she does] not belong here...so [she] spent three and a half hours writing what [she] was going to say.” Early on, she establishes how respectable her audience is, and how she perceives an invitation to speak at this Gala to be an honor. Somberly and somewhat shakily, she continues by acknowledging her intentions to shed light upon the global mental health crisis. She offers several statistics about this mental health crisis to further prove the dire need for early intervention and accessible resources for all people. Eventually, Lady Gaga touches upon the importance of recognizing this crisis beyond statistical measures; mental illnesses can affect anyone, and these experiences are terrifying, silencing, and debilitating. For instance, she references the Thousand Oaks shooting by a veteran who was believed to have suffered from untreated post-traumatic stress disorder. She goes on to share her personal experiences struggling with her mental health; “I needed help earlier. I needed mental health care. I needed someone to see not through me or see the star that I had become, but rather see the darkness inside that I was struggling with. I wish I had mental health resources...I wish there had been a system in place to protect and guide me.” She uses her platform as a space to share the reality of the global mental health crisis, calling for donations to the SAG-AFTRA Foundation and other foundations with likeminded intentions in order to advocate for mental health teams and an overall more informed understanding of mental health. She ends her speech on a hopeful note; “Let's create a more nuanced infrastructure. And let’s fucking change the world.”
Dow and Boor Ton’s “Feminine Style and Political Judgement in the Rhetoric of Ann Richards” proposes the idea that “self-disclosure and the wisdom [drawn from experience], reflects a quality associated with female culture, where private experiences are shared both to enhance relationships and to create a perspective on the world...self-disclosure and self-deprecation celebrate the strength and self-awareness gained through mature introspection” (293-294). Lady Gaga’s speech embodies feminine style in this way almost entirely; after all, she does begin with the self-deprecating realization that she feels she “does not belong.” She also makes the intentional choice to praise the artists she is addressing and fundraising for in the room. Lady Gaga is an international superstar but she does not dwell on her status. She focuses on what her position in society has given her: a platform. Her admittance that it took her about three hours to write her speech is a form of self-disclosure that demonstrates her commitment to formulating a speech that is well-suited to her audience. At several points in her speech, however, Lady Gaga does, in fact, use masculine rhetoric to expose the repercussions of mental health. Nevertheless, when she does make these factual statements, they are still somewhat feminine in the way she delivers her message and frames the information. Although she informs the audience that “mental health receives less than 1% of global aid...mental health conditions currently cost the world $2.5 trillion per year and if we don’t curb that, it could balloon into $6 trillion by 2030,” these numbers are presented alongside stronger emotional statements. More specifically, when she also says “when it comes to mental health, we all become developing countries. That is a chancy statement but I’m going to make it,” audiences truly witness her passion for this cause take flight. Mental health is a complex, emotional experience to navigate, but this is precisely why Lady Gaga makes it a point to devote her speech to recognizing its utter relevance to our society. Her willingness to share her personal struggles, acknowledging that her mental health issues ���later morphed into physical chronic pain, Fibromyalgia, panic attacks, acute trauma responses and debilitating mental spirals that have included suicidal ideation and masochistic behavior” is a vulnerable way to demonstrate to her audience that she too is among the population of people affected by mental illness.
Considering these aspects of her speech, her use of feminine rhetoric in order to raise money for the SAG-AFTRA GALA and awareness for the global mental health crisis is incredibly empowering. She speaks from her soul; this manifests itself in her purposeful hand gestures and how she is able to convey her ideas with conviction. Some of the speech’s most powerful moments are when Lady Gaga pauses, or when her voice shakes with the pain and utter helplessness that comes with discussing the global mental health crisis. This is especially advantageous to our society right now because she demonstrates that she is human too. She struggles. She feels pain. But most importantly she wants this pain to end through a healthy process. This is encouraging to the people struggling with mental illnesses who may feel too stigmatized and ashamed to be open about their experiences. This is especially inspiring for those who have experienced suicidal thoughts. She reinforces that opening up is healthy and that everyone needs a mental health team. Not once does her feminine rhetoric lose the essence of her overall message. The message is loud and clear, and her use of self-deprecation and self-disclosure further emphasizes that. Her raw, unfiltered speech could be criticized as too “dramatic” or emotional to be taken seriously, but this claim forgets the power of authenticity in its purest form: vulnerability. By telling the truth about mental health, even though it is tough and sometimes uncomfortable to talk about, she creates an environment that “brings mental health into the light. We need to share our stories so that global mental health no longer resides and festers in the darkness.” Lady Gaga uses her platform to normalize healthy discussion about mental health; to deem this as advantageous would be an understatement. It is vital.
“Female Leadership Advantage and Disadvantage: Resolving the Contradictions” by Alice Eagly captures the “tension between the communal qualities that people prefer in women and the predominantly agentic qualities they expect in leaders produces cross-pressures on female leaders. They often experience disapproval for their more masculine behaviors, such as asserting clear-cut authority over others, as well as for their more feminine behaviors, such as being especially supportive of others” (4). Lady Gaga, like most women with a platform, faces these challenges in her speech. There are points in her speech where she is incredibly close to breaking down and crying, and there are also moments where she speaks matter-of-factly, taking a firm stance on the work our world needs to do in taking global mental health more seriously. On the whole, she uses more feminine rhetoric, as her speech overflows with words like “hope” and “healing.” The nature of mental health itself is sensitive, so it is no wonder feminine rhetoric would be more natural to gravitate towards. It is evident that she is aware of the expectations that come with her status in society, and so she lulls in and out of being both “communal” and expressing “agentic qualities.” I would go as far to say that she blends these two expectations together, and can in this way be seen as exercising gender fluidity in her rhetoric. Her communal qualities are an expression of her agency. She shatters the notion that she must abide by either gender expectation. She can have both qualities and still communicate a greater message. Lady Gaga’s emotional anecdotes manage to pack a punch, and her bolder statements are delivered delicately and considerately. When she says “we need to not only think in terms of doctors, billable hours and hospital stays but protective and preventative care for ourselves and each other, holistically,” she demonstrates the importance of thinking about both communal and agentic qualities. With this in mind, her speech can certainly be categorized as relying on feminine rhetoric, but she does not shy away from occasionally maintaining a more traditionally masculine speaking style in order to achieve a delicate balance between the two.
Overall, Lady Gaga’s speech at the SAG-AFTRA GALA demonstrates the power of using feminine rhetoric in order to create a productive conversation about global mental health in our society. She dispels the preconceived notion that feminine rhetoric is a weaker speaking style. Instead, she proves to herself and the audience that being vulnerable, honest, and emotional can create a safe space for people to relate to one another. This is the energy that will destroy stigmas, incite change, and inspire people to offer financial and emotional support to those in need.
Works Cited
Dow, Bonnie J. & Tonn, Mari B. “Feminine style and political judgment in the rhetoric of Ann Richards.” Quarterly Journal of Speech, vol.79, 1993, pp. 286-302.
Eagly, Alice H. “Female Leadership Advantage and Disadvantage: Resolving the Contradictions.” Psychology of Women Quarterly, vol. 31, no. 1, Mar. 2007, pp. 1–12, doi:10.1111/j.1471-6402.2007.00326.x.
Gardner, Chris. “Lady Gaga Talks Suicide and Masochistic Behavior at SAG-AFTRA Gala.” The Hollywood Reporter. Nov. 2018
0 notes
Text
The Roots of Depression: How Much Does Modern Culture Have to Do With It?
I can’t complain about my existence in modern culture. My life is great. I have a loving family. My kids are happy and successful. My wife is a friend and lover and confidante and partner. Business is good and interesting. I care about what I’m doing. Every day is meaningful—and unburdened by concerns around mental well-being. Depression isn’t an issue for me.
But it’s not the case for everyone. The numbers don’t lie. Depression rates are climbing. Antidepressants are among the most common drug prescriptions, even among children. And because it can be embarrassing to admit you’re depressed—like there’s “something wrong” with you if you say as much—many people with depression never seek help, so the real numbers could be even higher. Depression isn’t new of course. The ancients knew it as “melancholia,” or possession by malevolent spirits. But all evidence suggests that depression is more prevalent than ever before.
What’s going on?
First of all, the way we speak about depression makes getting to the root of the issue harder.
“It’s all brain chemicals.”
“You have a neurotransmitter imbalance. There’s nothing you can do but take this pill.”
“You were born with it.”
This is an admirable attempt to de-stigmatize depression, turning it into a medical condition that “just happens” and “isn’t your fault.” Some people get brain tumors, some have type 1 diabetes, some have depression. There’s no shame in getting treatment for legitimate medical condition. This is an important development, but there’s a cost: It removes agency. If depression is just something you get or have from the outset, many (certainly not all) people believe there’s no reason to investigate the root cause or pursue alternative solutions.
While there’s definitely a genetic component to depression, and neurotransmitters play key roles, most depression requires some precipitating series of environmental inputs. The vast majority of babies with “depressive genes” don’t come out of the womb listless and morose with “bad brain chemicals.” They may be more or less susceptible to the environmental factors that can trigger depression later in life, but they still require those factors.
What’s happening? Clearly, something novel is afoot. Although we don’t have data on the mental health of paleolithic hunter-gatherers, extant hunter-gatherers exhibit an almost complete lack of depression.
What might help fill in one neglected dimension is to examine what’s unique about modern society.
It Is Atomized
People exist in their own bubbles. We sit in cars, in cubicles, in houses, in separate rooms. Even friends out to lunch are often seen gazing into their smartphones, half-ignorant of the normal waking reality occurring around them. Families gather in the living room not to play board games and chat about the day, but to access their personal portals into cyberspace. Together but apart. It may feel like we’re connecting, but we’re really just lonely. Like something out of a post-Sergeant Peppers Beatles dystopian concept album, the UK even just established a Ministry of Loneliness.
Loneliness has stronger associations with depression than any other social isolation indicator.
Lack Of Tribe
Robin Dunbar came up with Dunbar’s Number after studying disparate tribes and communities across the world: The maximum number of fulfilling, meaningful social relationships a person can reasonably maintain is about 150. We’re geared to desire social acceptance from our tribe, because social acceptance in a tribe of 150 people is both feasible and desirable. It increases survival. If “desire for social acceptance” is mediated by genes to at least some extent, it undergone positive selection; it was helpful and beneficial and supported species survival. Consider what the tribe originally meant: these are the people you grew up with, the people who will have your back. It’s important that your tribe accept you, and that you accept them. Things work better that way.
Today, our tribes are enormous and unwieldy. There’s the city. The state. The nation. The globe. Twitter. Our social media feeds. We can’t know everyone in our city, state, or Twitter feed, yet we get feedback from them. We see the best parts of their lives—what they show to the world—and compare them to the lowest parts of ours—what we hide from world but cannot escape internally. And then ironically, many of us feel estranged from or ignore the people who could actually comprise our true tribes—family, friends, loved ones, neighbors—even when they’re in the same room in favor of the larger, faker tribe. Yet the desire for social acceptance from this sprawling “tribe” persists. And it’s impossible to achieve for most people. Letting your tribe down hurts. We have tribes. They’re just not real or realistic.
Social media consumption predicts depressive symptoms.
It’s Devoid Of Higher Meaning
The roles of religion and other binding schools of philosophy and morality in society are waning. Most people can’t lean on the church or patriotism to find meaning or direction anymore. They must create their own, or discover it. That isn’t easy. It’s far simpler to ignore the void within, flip through your Netflix feed, and obsess about the latest superhero movie than it is to find your purpose.
Having a sense of life meaning is inversely associated with depression.
Life Is Easier
Most people (most reading this, anyway) aren’t walking three miles each way just for moderately fresh water that they still have to dose with iodine tabs or risk parasitic infection, slaving away their entire lives just to produce enough calories for their feudal lord and family, building their own homes out whatever they can manage and fixing whatever breaks (or not). They just turn the tap, order food from Thrive Market, call the plumber.
Work Is Increasingly “Information Work”
Rather than manipulate material objects in the world, we’re manipulating data, filling spreadsheets, fiddling with abstract numbers. Information work is no less real, but it doesn’t feel like that to our psyches.
Life Isn’t As Tragic
There are fewer “classic tragedies.” Fewer people lose loved ones to warfare, babies to disease. While we still have plenty of wars going on, they aren’t logging death counts like the World Wars or Genghis Khan’s conquests. Major civilian centers aren’t being leveled regularly by bombing raids. This is a positive development, but there’s a catch: Research shows that real life disasters strengthen bonds between friends, the neighbors, and the community. If we aren’t facing difficulties, we may not be living to our fullest potential.
Powerful Technology Is Widely Available Almost Everywhere
You can follow Maasai herders on Twitter. You can engage in live video chat with anyone in the world. No need to visit Grandma in Del Boca Vista; you can Facetime her!
Material Problems Are Disappearing
Most people get enough to eat, can get from here to there, can access the Internet, and get medical care if required. You have to try really hard in a modern Western society to die in the street. Even worldwide, poverty is falling. In 1981, nearly half the world’s population was “extremely poor.” As of 2016, it was under 10%. All that’s left are psychological problems.
Why am I here?
What’s the purpose of life?
Why should I continue working this job I don’t really like just to support the same boring routine?
This kind of rumination is a major factor in depression.
In Tribe, Sebastian Junger shows how veterans returning from war—on paper, a hellish experience no one would ever miss—feel suddenly lonely, lost, and often depressed back home. War compresses human experience and intensifies human bonding like nothing else. When these men and women leave war, they’re leaving the strongest, most cohesive tribe they’ve ever known. They’re leaving people who’d die for them and for whom they’d die. What, are they supposed to stand in line at Starbucks, staring at their phones like everyone else and think everything is just fine?
Why are potential root societal causes ignored?
For one, they’re huge problems. A pill is way easier than restructuring the fabric of modern society. If you did that, you’d have to get it right the first time. You can’t exactly run an RCT on social upheaval.
Two, we assume a shared environment. Most of the people you see walking around eat the same basic diet, do the same basic exercises (or don’t), and deal with the same societal pressures and conditions. If you look at things wrong, it seems immutable and unavoidable. Even if they’re aware on some level that modern living is involved in the etiology of depression, most clinicians are assuming, based on prior experience with patients and their own misconceptions about what’s possible and what’s not, that we just have to accept it and apply the best band-aids we have. But if you’ve approached diet and exercise from an evolutionary angle and had incredible results where nothing else had ever worked—you know that common is not normal. You know that the environmental inputs shared by so many in the industrialized world might be persistent and tempting and hard to avoid, but they are avoidable. You can change your surroundings, your inputs, even your mindset.
Three, it isn’t clear what the solutions even are. The world is better today in many ways. Just because many veterans find their tribe in war and suffer upon returning, it doesn’t follow that we should go to war more often for our mental health.
We can’t rely on technocratic overlords to engineer the perfect utopia. Those always end in dystopias—more Brave New World than 1984. No, any change has to start within each individual, at dinner tables, in friend circles, in one person—you—deciding to do things differently.
I won’t get much into diet or exercise or sunlight or sleep today. Those are major parts of the equation, but I prefer to focus on how the structure of our society impacts depression and how we can transcend it.
These are some ideas. They’re not perfect. They’re not the whole story. And they’re not meant to replace medication or therapy or anything like that. But they won’t hurt….
Listen to the “first voice.” Every time you get that little voice saying “I should finally pick up that book” or “I should walk the dog” or “I wonder what my friends are up to,” DO IT. Don’t let the other voice override you and say “Nah, let’s just stay inside today.” That second voice is destroying you. Do everything you can to ignore it.
In low moments, rather than try to cheer yourself up, be of service to someone. A concerted effort to cheer oneself up often produces the opposite effect. We’re not great at doing it for ourselves, perhaps because at some level we sense it’s all a sham, a ploy to shift around neurotransmitters. But when you help someone else, you’re truly helping them. They feel good, you feel good, and everyone wins.
Chase meaning, not happiness. “Being happy” is hard work. You can’t get there by trying. Figure out what you care about at the deepest level of your being. What stirs you. What, most importantly, you can actually affect with your skillset. If you can manage to imbue every fiber of your being with that purpose, you’ll get going after it. You’ll have something to do, and maybe you’ll have less time for rumination and other things that make your depression worse.
Easier said than done, you might say. Definitely. I haven’t been there myself, but I’ve helped people close to me who have. Clinical depression isn’t just sadness. It’s profoundly demotivating, where taking even the smallest act like getting dressed can be a struggle. Dopamine, the neurotransmitter involved in movement and achievement and motivation, tends to plummet in major depression.
Still, what else is there? You are an individual, not an atom. An atom is separate but unconscious. It has no agency. It simply is. An individual is separate from other individuals but conscious. It has agency. It can form communities, strong bonds. Revel in your personal sovereignty but don’t forget that you’re a social animal who will probably be much happier with a few good friends (who aren’t all wielding smartphones 24-7).
There are other specific things to try. Trawl the scientific literature and you’ll find hundreds of studies showing efficacy for any number of medication-free depression therapies and interventions. None of them are the final answer, though, as much as they can help. Ballroom dancing isn’t going to fix things. Gardening isn’t enough. Heavy squats won’t do it. Plunging into cold water isn’t everything.
It has to be a comprehensive shift.
The common theme running through most of these “alternative” interventions is that it places you square in the midst of cold hard reality. You’re on your knees, handling soil and planting vegetables. You’re dancing, immersed in the music and managing the dynamic interplay between you and your partner. You’re lifting something very heavy. You’re completely submerged in freezing water. These are real. They cannot be escaped or negotiated with. They aren’t running on perpetual loops inside your head. They’re actually happening.
Get as much of that in your life.
In the future, I’ll discuss this topic further. I’ll talk about dietary, exercise, lifestyle, supplement, and psychological modifications we can make.
For now, I’d love to hear from you. Those who’ve dealt with or who currently deal with depression, what’s helped? What hasn’t? What’s your take on the list of social factors that may explain the rise in depression—or the severity of symptoms as you experience them? What do you think we can do—as individuals and as a society—to make things better?
Thanks for reading. Take care.
The post The Roots of Depression: How Much Does Modern Culture Have to Do With It? appeared first on Mark's Daily Apple.
Article source here:Marks’s Daily Apple
0 notes
Text
The Roots of Depression: How Much Does Modern Culture Have to Do With It?
I can’t complain about my existence in modern culture. My life is great. I have a loving family. My kids are happy and successful. My wife is a friend and lover and confidante and partner. Business is good and interesting. I care about what I’m doing. Every day is meaningful—and unburdened by concerns around mental well-being. Depression isn’t an issue for me.
But it’s not the case for everyone. The numbers don’t lie. Depression rates are climbing. Antidepressants are among the most common drug prescriptions, even among children. And because it can be embarrassing to admit you’re depressed—like there’s “something wrong” with you if you say as much—many people with depression never seek help, so the real numbers could be even higher. Depression isn’t new of course. The ancients knew it as “melancholia,” or possession by malevolent spirits. But all evidence suggests that depression is more prevalent than ever before.
What’s going on?
First of all, the way we speak about depression makes getting to the root of the issue harder.
“It’s all brain chemicals.”
“You have a neurotransmitter imbalance. There’s nothing you can do but take this pill.”
“You were born with it.”
This is an admirable attempt to de-stigmatize depression, turning it into a medical condition that “just happens” and “isn’t your fault.” Some people get brain tumors, some have type 1 diabetes, some have depression. There’s no shame in getting treatment for legitimate medical condition. This is an important development, but there’s a cost: It removes agency. If depression is just something you get or have from the outset, many (certainly not all) people believe there’s no reason to investigate the root cause or pursue alternative solutions.
While there’s definitely a genetic component to depression, and neurotransmitters play key roles, most depression requires some precipitating series of environmental inputs. The vast majority of babies with “depressive genes” don’t come out of the womb listless and morose with “bad brain chemicals.” They may be more or less susceptible to the environmental factors that can trigger depression later in life, but they still require those factors.
What’s happening? Clearly, something novel is afoot. Although we don’t have data on the mental health of paleolithic hunter-gatherers, extant hunter-gatherers exhibit an almost complete lack of depression.
What might help fill in one neglected dimension is to examine what’s unique about modern society.
It Is Atomized
People exist in their own bubbles. We sit in cars, in cubicles, in houses, in separate rooms. Even friends out to lunch are often seen gazing into their smartphones, half-ignorant of the normal waking reality occurring around them. Families gather in the living room not to play board games and chat about the day, but to access their personal portals into cyberspace. Together but apart. It may feel like we’re connecting, but we’re really just lonely. Like something out of a post-Sergeant Peppers Beatles dystopian concept album, the UK even just established a Ministry of Loneliness.
Loneliness has stronger associations with depression than any other social isolation indicator.
Lack Of Tribe
Robin Dunbar came up with Dunbar’s Number after studying disparate tribes and communities across the world: The maximum number of fulfilling, meaningful social relationships a person can reasonably maintain is about 150. We’re geared to desire social acceptance from our tribe, because social acceptance in a tribe of 150 people is both feasible and desirable. It increases survival. If “desire for social acceptance” is mediated by genes to at least some extent, it undergone positive selection; it was helpful and beneficial and supported species survival. Consider what the tribe originally meant: these are the people you grew up with, the people who will have your back. It’s important that your tribe accept you, and that you accept them. Things work better that way.
Today, our tribes are enormous and unwieldy. There’s the city. The state. The nation. The globe. Twitter. Our social media feeds. We can’t know everyone in our city, state, or Twitter feed, yet we get feedback from them. We see the best parts of their lives—what they show to the world—and compare them to the lowest parts of ours—what we hide from world but cannot escape internally. And then ironically, many of us feel estranged from or ignore the people who could actually comprise our true tribes—family, friends, loved ones, neighbors—even when they’re in the same room in favor of the larger, faker tribe. Yet the desire for social acceptance from this sprawling “tribe” persists. And it’s impossible to achieve for most people. Letting your tribe down hurts. We have tribes. They’re just not real or realistic.
Social media consumption predicts depressive symptoms.
It’s Devoid Of Higher Meaning
The roles of religion and other binding schools of philosophy and morality in society are waning. Most people can’t lean on the church or patriotism to find meaning or direction anymore. They must create their own, or discover it. That isn’t easy. It’s far simpler to ignore the void within, flip through your Netflix feed, and obsess about the latest superhero movie than it is to find your purpose.
Having a sense of life meaning is inversely associated with depression.
Life Is Easier
Most people (most reading this, anyway) aren’t walking three miles each way just for moderately fresh water that they still have to dose with iodine tabs or risk parasitic infection, slaving away their entire lives just to produce enough calories for their feudal lord and family, building their own homes out whatever they can manage and fixing whatever breaks (or not). They just turn the tap, order food from Thrive Market, call the plumber.
Work Is Increasingly “Information Work”
Rather than manipulate material objects in the world, we’re manipulating data, filling spreadsheets, fiddling with abstract numbers. Information work is no less real, but it doesn’t feel like that to our psyches.
Life Isn’t As Tragic
There are fewer “classic tragedies.” Fewer people lose loved ones to warfare, babies to disease. While we still have plenty of wars going on, they aren’t logging death counts like the World Wars or Genghis Khan’s conquests. Major civilian centers aren’t being leveled regularly by bombing raids. This is a positive development, but there’s a catch: Research shows that real life disasters strengthen bonds between friends, the neighbors, and the community. If we aren’t facing difficulties, we may not be living to our fullest potential.
Powerful Technology Is Widely Available Almost Everywhere
You can follow Maasai herders on Twitter. You can engage in live video chat with anyone in the world. No need to visit Grandma in Del Boca Vista; you can Facetime her!
Material Problems Are Disappearing
Most people get enough to eat, can get from here to there, can access the Internet, and get medical care if required. You have to try really hard in a modern Western society to die in the street. Even worldwide, poverty is falling. In 1981, nearly half the world’s population was “extremely poor.” As of 2016, it was under 10%. All that’s left are psychological problems.
Why am I here?
What’s the purpose of life?
Why should I continue working this job I don’t really like just to support the same boring routine?
This kind of rumination is a major factor in depression.
In Tribe, Sebastian Junger shows how veterans returning from war—on paper, a hellish experience no one would ever miss—feel suddenly lonely, lost, and often depressed back home. War compresses human experience and intensifies human bonding like nothing else. When these men and women leave war, they’re leaving the strongest, most cohesive tribe they’ve ever known. They’re leaving people who’d die for them and for whom they’d die. What, are they supposed to stand in line at Starbucks, staring at their phones like everyone else and think everything is just fine?
Why are potential root societal causes ignored?
For one, they’re huge problems. A pill is way easier than restructuring the fabric of modern society. If you did that, you’d have to get it right the first time. You can’t exactly run an RCT on social upheaval.
Two, we assume a shared environment. Most of the people you see walking around eat the same basic diet, do the same basic exercises (or don’t), and deal with the same societal pressures and conditions. If you look at things wrong, it seems immutable and unavoidable. Even if they’re aware on some level that modern living is involved in the etiology of depression, most clinicians are assuming, based on prior experience with patients and their own misconceptions about what’s possible and what’s not, that we just have to accept it and apply the best band-aids we have. But if you’ve approached diet and exercise from an evolutionary angle and had incredible results where nothing else had ever worked—you know that common is not normal. You know that the environmental inputs shared by so many in the industrialized world might be persistent and tempting and hard to avoid, but they are avoidable. You can change your surroundings, your inputs, even your mindset.
Three, it isn’t clear what the solutions even are. The world is better today in many ways. Just because many veterans find their tribe in war and suffer upon returning, it doesn’t follow that we should go to war more often for our mental health.
We can’t rely on technocratic overlords to engineer the perfect utopia. Those always end in dystopias—more Brave New World than 1984. No, any change has to start within each individual, at dinner tables, in friend circles, in one person—you—deciding to do things differently.
I won’t get much into diet or exercise or sunlight or sleep today. Those are major parts of the equation, but I prefer to focus on how the structure of our society impacts depression and how we can transcend it.
These are some ideas. They’re not perfect. They’re not the whole story. And they’re not meant to replace medication or therapy or anything like that. But they won’t hurt….
Listen to the “first voice.” Every time you get that little voice saying “I should finally pick up that book” or “I should walk the dog” or “I wonder what my friends are up to,” DO IT. Don’t let the other voice override you and say “Nah, let’s just stay inside today.” That second voice is destroying you. Do everything you can to ignore it.
In low moments, rather than try to cheer yourself up, be of service to someone. A concerted effort to cheer oneself up often produces the opposite effect. We’re not great at doing it for ourselves, perhaps because at some level we sense it’s all a sham, a ploy to shift around neurotransmitters. But when you help someone else, you’re truly helping them. They feel good, you feel good, and everyone wins.
Chase meaning, not happiness. “Being happy” is hard work. You can’t get there by trying. Figure out what you care about at the deepest level of your being. What stirs you. What, most importantly, you can actually affect with your skillset. If you can manage to imbue every fiber of your being with that purpose, you’ll get going after it. You’ll have something to do, and maybe you’ll have less time for rumination and other things that make your depression worse.
Easier said than done, you might say. Definitely. I haven’t been there myself, but I’ve helped people close to me who have. Clinical depression isn’t just sadness. It’s profoundly demotivating, where taking even the smallest act like getting dressed can be a struggle. Dopamine, the neurotransmitter involved in movement and achievement and motivation, tends to plummet in major depression.
Still, what else is there? You are an individual, not an atom. An atom is separate but unconscious. It has no agency. It simply is. An individual is separate from other individuals but conscious. It has agency. It can form communities, strong bonds. Revel in your personal sovereignty but don’t forget that you’re a social animal who will probably be much happier with a few good friends (who aren’t all wielding smartphones 24-7).
There are other specific things to try. Trawl the scientific literature and you’ll find hundreds of studies showing efficacy for any number of medication-free depression therapies and interventions. None of them are the final answer, though, as much as they can help. Ballroom dancing isn’t going to fix things. Gardening isn’t enough. Heavy squats won’t do it. Plunging into cold water isn’t everything.
It has to be a comprehensive shift.
The common theme running through most of these “alternative” interventions is that it places you square in the midst of cold hard reality. You’re on your knees, handling soil and planting vegetables. You’re dancing, immersed in the music and managing the dynamic interplay between you and your partner. You’re lifting something very heavy. You’re completely submerged in freezing water. These are real. They cannot be escaped or negotiated with. They aren’t running on perpetual loops inside your head. They’re actually happening.
Get as much of that in your life.
In the future, I’ll discuss this topic further. I’ll talk about dietary, exercise, lifestyle, supplement, and psychological modifications we can make.
For now, I’d love to hear from you. Those who’ve dealt with or who currently deal with depression, what’s helped? What hasn’t? What’s your take on the list of social factors that may explain the rise in depression—or the severity of symptoms as you experience them? What do you think we can do—as individuals and as a society—to make things better?
Thanks for reading. Take care.
0 notes
Text
The Roots of Depression: How Much Does Modern Culture Have to Do With It?
I can’t complain about my existence in modern culture. My life is great. I have a loving family. My kids are happy and successful. My wife is a friend and lover and confidante and partner. Business is good and interesting. I care about what I’m doing. Every day is meaningful—and unburdened by concerns around mental well-being. Depression isn’t an issue for me.
But it’s not the case for everyone. The numbers don’t lie. Depression rates are climbing. Antidepressants are among the most common drug prescriptions, even among children. And because it can be embarrassing to admit you’re depressed—like there’s “something wrong” with you if you say as much—many people with depression never seek help, so the real numbers could be even higher. Depression isn’t new of course. The ancients knew it as “melancholia,” or possession by malevolent spirits. But all evidence suggests that depression is more prevalent than ever before.
What’s going on?
First of all, the way we speak about depression makes getting to the root of the issue harder.
“It’s all brain chemicals.”
“You have a neurotransmitter imbalance. There’s nothing you can do but take this pill.”
“You were born with it.”
This is an admirable attempt to de-stigmatize depression, turning it into a medical condition that “just happens” and “isn’t your fault.” Some people get brain tumors, some have type 1 diabetes, some have depression. There’s no shame in getting treatment for legitimate medical condition. This is an important development, but there’s a cost: It removes agency. If depression is just something you get or have from the outset, many (certainly not all) people believe there’s no reason to investigate the root cause or pursue alternative solutions.
While there’s definitely a genetic component to depression, and neurotransmitters play key roles, most depression requires some precipitating series of environmental inputs. The vast majority of babies with “depressive genes” don’t come out of the womb listless and morose with “bad brain chemicals.” They may be more or less susceptible to the environmental factors that can trigger depression later in life, but they still require those factors.
What’s happening? Clearly, something novel is afoot. Although we don’t have data on the mental health of paleolithic hunter-gatherers, extant hunter-gatherers exhibit an almost complete lack of depression.
What might help fill in one neglected dimension is to examine what’s unique about modern society.
It Is Atomized
People exist in their own bubbles. We sit in cars, in cubicles, in houses, in separate rooms. Even friends out to lunch are often seen gazing into their smartphones, half-ignorant of the normal waking reality occurring around them. Families gather in the living room not to play board games and chat about the day, but to access their personal portals into cyberspace. Together but apart. It may feel like we’re connecting, but we’re really just lonely. Like something out of a post-Sergeant Peppers Beatles dystopian concept album, the UK even just established a Ministry of Loneliness.
Loneliness has stronger associations with depression than any other social isolation indicator.
Lack Of Tribe
Robin Dunbar came up with Dunbar’s Number after studying disparate tribes and communities across the world: The maximum number of fulfilling, meaningful social relationships a person can reasonably maintain is about 150. We’re geared to desire social acceptance from our tribe, because social acceptance in a tribe of 150 people is both feasible and desirable. It increases survival. If “desire for social acceptance” is mediated by genes to at least some extent, it undergone positive selection; it was helpful and beneficial and supported species survival. Consider what the tribe originally meant: these are the people you grew up with, the people who will have your back. It’s important that your tribe accept you, and that you accept them. Things work better that way.
Today, our tribes are enormous and unwieldy. There’s the city. The state. The nation. The globe. Twitter. Our social media feeds. We can’t know everyone in our city, state, or Twitter feed, yet we get feedback from them. We see the best parts of their lives—what they show to the world—and compare them to the lowest parts of ours—what we hide from world but cannot escape internally. And then ironically, many of us feel estranged from or ignore the people who could actually comprise our true tribes—family, friends, loved ones, neighbors—even when they’re in the same room in favor of the larger, faker tribe. Yet the desire for social acceptance from this sprawling “tribe” persists. And it’s impossible to achieve for most people. Letting your tribe down hurts. We have tribes. They’re just not real or realistic.
Social media consumption predicts depressive symptoms.
It’s Devoid Of Higher Meaning
The roles of religion and other binding schools of philosophy and morality in society are waning. Most people can’t lean on the church or patriotism to find meaning or direction anymore. They must create their own, or discover it. That isn’t easy. It’s far simpler to ignore the void within, flip through your Netflix feed, and obsess about the latest superhero movie than it is to find your purpose.
Having a sense of life meaning is inversely associated with depression.
Life Is Easier
Most people (most reading this, anyway) aren’t walking three miles each way just for moderately fresh water that they still have to dose with iodine tabs or risk parasitic infection, slaving away their entire lives just to produce enough calories for their feudal lord and family, building their own homes out whatever they can manage and fixing whatever breaks (or not). They just turn the tap, order food from Thrive Market, call the plumber.
Work Is Increasingly “Information Work”
Rather than manipulate material objects in the world, we’re manipulating data, filling spreadsheets, fiddling with abstract numbers. Information work is no less real, but it doesn’t feel like that to our psyches.
Life Isn’t As Tragic
There are fewer “classic tragedies.” Fewer people lose loved ones to warfare, babies to disease. While we still have plenty of wars going on, they aren’t logging death counts like the World Wars or Genghis Khan’s conquests. Major civilian centers aren’t being leveled regularly by bombing raids. This is a positive development, but there’s a catch: Research shows that real life disasters strengthen bonds between friends, the neighbors, and the community. If we aren’t facing difficulties, we may not be living to our fullest potential.
Powerful Technology Is Widely Available Almost Everywhere
You can follow Maasai herders on Twitter. You can engage in live video chat with anyone in the world. No need to visit Grandma in Del Boca Vista; you can Facetime her!
Material Problems Are Disappearing
Most people get enough to eat, can get from here to there, can access the Internet, and get medical care if required. You have to try really hard in a modern Western society to die in the street. Even worldwide, poverty is falling. In 1981, nearly half the world’s population was “extremely poor.” As of 2016, it was under 10%. All that’s left are psychological problems.
Why am I here?
What’s the purpose of life?
Why should I continue working this job I don’t really like just to support the same boring routine?
This kind of rumination is a major factor in depression.
In Tribe, Sebastian Junger shows how veterans returning from war—on paper, a hellish experience no one would ever miss—feel suddenly lonely, lost, and often depressed back home. War compresses human experience and intensifies human bonding like nothing else. When these men and women leave war, they’re leaving the strongest, most cohesive tribe they’ve ever known. They’re leaving people who’d die for them and for whom they’d die. What, are they supposed to stand in line at Starbucks, staring at their phones like everyone else and think everything is just fine?
Why are potential root societal causes ignored?
For one, they’re huge problems. A pill is way easier than restructuring the fabric of modern society. If you did that, you’d have to get it right the first time. You can’t exactly run an RCT on social upheaval.
Two, we assume a shared environment. Most of the people you see walking around eat the same basic diet, do the same basic exercises (or don’t), and deal with the same societal pressures and conditions. If you look at things wrong, it seems immutable and unavoidable. Even if they’re aware on some level that modern living is involved in the etiology of depression, most clinicians are assuming, based on prior experience with patients and their own misconceptions about what’s possible and what’s not, that we just have to accept it and apply the best band-aids we have. But if you’ve approached diet and exercise from an evolutionary angle and had incredible results where nothing else had ever worked—you know that common is not normal. You know that the environmental inputs shared by so many in the industrialized world might be persistent and tempting and hard to avoid, but they are avoidable. You can change your surroundings, your inputs, even your mindset.
Three, it isn’t clear what the solutions even are. The world is better today in many ways. Just because many veterans find their tribe in war and suffer upon returning, it doesn’t follow that we should go to war more often for our mental health.
We can’t rely on technocratic overlords to engineer the perfect utopia. Those always end in dystopias—more Brave New World than 1984. No, any change has to start within each individual, at dinner tables, in friend circles, in one person—you—deciding to do things differently.
I won’t get much into diet or exercise or sunlight or sleep today. Those are major parts of the equation, but I prefer to focus on how the structure of our society impacts depression and how we can transcend it.
These are some ideas. They’re not perfect. They’re not the whole story. And they’re not meant to replace medication or therapy or anything like that. But they won’t hurt….
Listen to the “first voice.” Every time you get that little voice saying “I should finally pick up that book” or “I should walk the dog” or “I wonder what my friends are up to,” DO IT. Don’t let the other voice override you and say “Nah, let’s just stay inside today.” That second voice is destroying you. Do everything you can to ignore it.
In low moments, rather than try to cheer yourself up, be of service to someone. A concerted effort to cheer oneself up often produces the opposite effect. We’re not great at doing it for ourselves, perhaps because at some level we sense it’s all a sham, a ploy to shift around neurotransmitters. But when you help someone else, you’re truly helping them. They feel good, you feel good, and everyone wins.
Chase meaning, not happiness. “Being happy” is hard work. You can’t get there by trying. Figure out what you care about at the deepest level of your being. What stirs you. What, most importantly, you can actually affect with your skillset. If you can manage to imbue every fiber of your being with that purpose, you’ll get going after it. You’ll have something to do, and maybe you’ll have less time for rumination and other things that make your depression worse.
Easier said than done, you might say. Definitely. I haven’t been there myself, but I’ve helped people close to me who have. Clinical depression isn’t just sadness. It’s profoundly demotivating, where taking even the smallest act like getting dressed can be a struggle. Dopamine, the neurotransmitter involved in movement and achievement and motivation, tends to plummet in major depression.
Still, what else is there? You are an individual, not an atom. An atom is separate but unconscious. It has no agency. It simply is. An individual is separate from other individuals but conscious. It has agency. It can form communities, strong bonds. Revel in your personal sovereignty but don’t forget that you’re a social animal who will probably be much happier with a few good friends (who aren’t all wielding smartphones 24-7).
There are other specific things to try. Trawl the scientific literature and you’ll find hundreds of studies showing efficacy for any number of medication-free depression therapies and interventions. None of them are the final answer, though, as much as they can help. Ballroom dancing isn’t going to fix things. Gardening isn’t enough. Heavy squats won’t do it. Plunging into cold water isn’t everything.
It has to be a comprehensive shift.
The common theme running through most of these “alternative” interventions is that it places you square in the midst of cold hard reality. You’re on your knees, handling soil and planting vegetables. You’re dancing, immersed in the music and managing the dynamic interplay between you and your partner. You’re lifting something very heavy. You’re completely submerged in freezing water. These are real. They cannot be escaped or negotiated with. They aren’t running on perpetual loops inside your head. They’re actually happening.
Get as much of that in your life.
In the future, I’ll discuss this topic further. I’ll talk about dietary, exercise, lifestyle, supplement, and psychological modifications we can make.
For now, I’d love to hear from you. Those who’ve dealt with or who currently deal with depression, what’s helped? What hasn’t? What’s your take on the list of social factors that may explain the rise in depression—or the severity of symptoms as you experience them? What do you think we can do—as individuals and as a society—to make things better?
Thanks for reading. Take care.
0 notes
Text
Opinion: Racism impacts your health
![CDATA[
By Roberta K. Timothy*
The recent news of Tina Fontaine’s trial and the acquittal of Gerald Stanley, a white farmer accused of killing a young Indigenous man, Colten Boushie, of the Red Pheasant First Nation are examples of the Canadian legal system’s commitment to the Indian Act and colonial dominance.
This ongoing colonial dominance has a transgenerational trauma impact on the health of Indigenous and colonized peoples.
Two recent examples that indicate the kind of violence that Black people experience: A school that allowed police to shackle a Black six-year old girl’s wrists and ankles; a children’s aid system that put a child refugee from Somalia into foster care yet never applied for his Canadian citizenship, so years later he received deportation orders to a country where he does not speak the language.
The impact of this colonialism and anti-Black racism on the health of Black and Indigenous peoples is elongated and insidious. We navigate systems, structures and communities that perpetuate abhorrence towards us in all aspects of our lives.
Experiencing and fighting such systems for justice for our children, ourselves and our community members has devastating effects on our health.
As a health and human rights researcher, therapist and professor who has explored the deep implications of racism, I would like to share some insights into the impacts of racism on our health.
My hope is that by doing so I create dialogue and encourage communities to continue to voice their experiences of violence and racism — in order to demand changes and ultimately create more supports.
Violence is a continuum
Health indicator statistics of Indigenous communities report increasing disparities between Indigenous and settler populations. Systemic racism affects Indigenous population’s health in various ways, this includes limited healthy food choices, inadequate living conditions and substandard health care. The infant mortality rate within Indigenous communities is almost 12 times that of settler communities.
The statistics, usually presented by state authorities, come without context or consideration to the broad range of causes — one of which is the continued exposure to state violence on a daily basis.
We have anecdotal evidence: We see loved ones, friends, ourselves and respected community leaders struggle with the emotional and physiological impacts of racism on a daily basis. While anti-Black racism’s effect on the health of Black communities is documented, studies from the U.S. are more illustrative.
In one U.S. study, researchers studied 1,574 Baltimore residents of which 20 per cent reported that they had been racially discriminated against “a lot.” This same group had higher systolic blood pressure than those who perceived they had been discriminated against very little. Additionally, over a five-year period the group that felt they had been discriminated against “a lot” had higher declines in kidney function.
In a 1997 to 2003 study on racial discrimination and breast cancer in U.S. Black women, researchers found that perceived experiences of racism resulted in increased incidents of breast cancer, especially among young Black women. In 2011, a pivotal study on the impact of racism on health scholars linked lifetime experiences of discrimination to higher prevalence of hypertension in African Americans.
Biases in research
These are just a few examples of some studies being done on the impact of racism on health. However, most studies have been conducted in the U.S., the U.K., New Zealand and Australia. Canada does not yet collect race-based health or experiences of racism on health data through any formal mechanism. This poses a problem when scholars are asked to produce “scientific data” to prove that racism impacts health inequities and disparities. How do you provide “statistically significant evidence” on the impact of anti-Black racism when systemic issues limits your access to collecting this same data? My future research proposes to support the collection of increased health data on the impact of anti-Black racism in Canada and globally.
In Black communities no one is immune from racism — from our unborn to our school age children to our elderly. Consciously and unconsciously our health becomes obstructed.
The impact on health intensifies for those in Black communities who are women, working class, lesbian, gay, bisexual or trans (LGBT), dis(abled), refugees or newcomers. Here, the combination of oppressions creates additional stress on mental and physical health and well-being. I call this intersectional violence.
For example, the massacre of Muslims in a Québec mosque and anti-Islam policies continue to further impact the health of marginalized, often surveilled communities. Two victims of the Québec massacre were Black. This fact is hardly mentioned. This is an example of anti-Black racism within communities of colour.
Health impacts from anti-Black racism and anti-Indigeneity are often dismissed or kept silent by health scholars and health-care workers. The findings challenge the illegitimacy of systems of dominance and question the humaneness and accountability of colonial power. As such, research on the health impact of anti-Black racism is underfunded and under researched.
The “realness” of health impacts related to racism interrupts narratives of the “disadvantaged,” the “poor,” the “lazy” and the “needy.” Such stereotypes re-victimize and further aggregate health inequities. Yet understanding racism as a determinant of health is important to understanding economic and social barriers to success.
When we fail to address the real impact of racism on Black communities’ health, we not only lose our community members to often preventable disease, illness, institutionalization and ultimately death, we also lose our opportunity for redress and to energetically participate in transnational anti-oppression movements.
Health impacts
Experiencing racism throughout our lifespan can overwhelm our health functionality. Repetitive acts of untreated trauma and violence lead to debilitating health issues.
The impact of anti-Black racism within our educational system is well documented by our lived experiences and “unexplained” drop-out rates. The effect of prolonged injustice from junior kindergarten through to post-secondary education, can lead to exacerbated health conditions.
The under-recruiting and under-hiring of African/Black and Indigenous peoples in medicine, psychology, education, health and in academia directly affects the impact of racism on these same communities.
Adversely, the over-hiring of African/Black community members as personal support workers, health aids and child care workers with little opportunity to move into positions of power in these fields directly establishes a division between the “helper” and “the helped,” resembling enslavement roles where Africans served whites while living in conditions that gravely impacted their own health.
The impact of the over-representation of our children in state care on the health of Black families due to separation and transgenerational trauma is never measured.
As our children and elders endure acts of violence during vulnerable times in their lives, without protection or support, their grief response becomes hidden or dissociated. This leads to challenges in seeking and receiving health care which increases despairing health results.
The myth that Black people do not seek mental health therapy comes from a falsified notion of “super resiliency” instead of the reality of under-funded and purposely delayed services that prevent health and wellness in our communities. This leads to many community members suffering and seeking services in silence and isolation.
The burden on Black and colonized folks’ bodies, minds, spirits, health and wellness is all-encompassing.
Possibilities for change
Having a provincial anti-racism directorate and local Toronto anti-Black racism action plan indicates a way forward. Much activism over many years resulted in these strategies getting put into action.
The directorate’s effectiveness will be measured in its implementation, the diversity of its members and its power to eliminate health disparities and address the health impacts of racism and violence on the daily lives of Black, Indigenous and racialized peoples.
Research funding needs to be increased. Universities need to hire scholars from communities who are directly impacted by racism and whose work address these health inequities — to support communities impacted by these same injustices.
What if the Afrocentric Alternative school, the only one in Canada, was well resourced and supported as a health strategy to combat the early stigmatization and violence experienced by school-aged Black children?
What if, in the case of the killing of the late Colten Boushie, the jury was not all white?
What if we looked to Black Live Matters as a public health racial justice movement trying to prevent further health atrocities?
What if we collected health data on the impact of racism - using both informal and formal research methods - empowered, developed and implemented by Black and colonized communities to create health equity programs and strategies to address our health disparities?
*Roberta K. Timothy is an Assistant Lecturer at Global Health, Ethics and Human Rights School of Health, York University.
(Disclaimer: The opinions expressed above are the personal views of the author and do not reflect the views of ZMCL)
]]>
0 notes