#Symptoms of Vascular Dementia
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs




Fun Fact
Tumblr Inc. is funded by 13 investors.
Text

Cat in the Hat:
"The German Health Minister gave an important update on the Covid situation yesterday.
I’ve written up the section of his speech from the video below for easy reading.
It’s immensely refreshing to see a government minister warning of the harms of Covid in such a transparent way."
https://x.com/_catinthehat/status/1732092683508678954

Prof. Karl Lauterbach
Health Minister, Germany
4 December 2023
"This second (long Covid) round table was very interesting, lasting three and a half hours. It serves as a unique forum for dialogue among scientists, researchers and those affected by long Covid, facilitating the exchange of ideas.
There are many new findings about long Covid. Not all of them are good news. One piece of not-so-good news concerns the fact that long Covid is actually still a problem for those who are newly infected. One estimate that has been put forward is that the risk of contracting long Covid now, even after vaccination, is around 3%. Now you may say, "that's not such a big risk" , but there are tens of thousands of people who are repeatedly affected in a short period of time. And so, the long Covid problem has not yet been solved.
We have also established that there really are many subgroups of long Covid and that we do not yet have a cure. And it was clearly pointed out that we are also dealing with problems here that will challenge society as a whole, because vascular diseases often occur after long Covid. Throughout Europe, we are currently seeing an increased incidence of cardiovascular disease in the middle-age group - from 25 to 50. This is associated with the consequences of Covid infections.
We also very often find cognitive impairment in older people. And one participant pointed out that it may well be like the Spanish flu, where 20 years after the Spanish flu there was a significant increase in Parkinson's disease and probably also dementia.
This is something we must pay attention to, as the past infection afiects how the immune system in the brain functions, as well as the brain's blood vessels, potentially increasing the long-term risk of these major neurodegenerative diseases. This is why we need to conduct very intensive research. This research has played a major role.
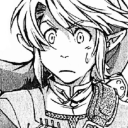
What is the overall assessment of the situation now?
We have to be careful. Long Covid is not curable at the moment. We also know that over 40% of those who have several manifestations of long Covid, for example, five or more, still have symptoms after 2 years, so it doesn't seem to heal spontaneously. We also know that those whose symptoms are more pronounced at the beginning are less likely to heal.
So some of what we know from the demographics of long Covid has been confirmed, and we now know more precisely which mechanisms in the brain, but also in the blood vessels and the immune system, are responsible for this. Professor Scheibenbogan will explain this briefly later.
At this point, I can only say the following - this is particularly important to me:
First of all, long Covid is a disease that stays with us and that we cannot yet cure. And we are seeing an increasing number of cases as the waves of infection continue to affect us.
Secondly, Covid is not a cold - with a cold, you don't usually see any long-term effects. You don't see any changes in the blood vessels. You don't usually see an autoimmune disease developing. You also don't usually see neurological inflammation - these are all things that we see with long Covid. Therefore, one should not assume that Covid infection is just a common cold. It can affect brain tissue and the vascular system, and we still lack an effective treatment, making these studies crucial.
Significantly, we know that the risk of long Covid decreases when you're infected but have been vaccinated. That's why it's concerning that only 3 million people have been vaccinated with the new, adapted vaccine. That is a very bad result.
Please protect yourself from severe infections.
Please protect yourself from long Covid.
Currently, the danger posed by Covid is indeed being underestimated. Nothing is worse than infecting someone at Christmas who then becomes seriously ill and may not fully recover."
Alt text is included in all images of this post.
#covid#not a cold#please wear a mask#pandemic#pandemic not over#long covid#Karl Lauterbach#Germany#German health minister
10K notes
·
View notes
Text
A decline in motor skills is a hallmark of Parkinson's disease, regularly taking the form of slowness, rigidity, and tremors. Yet the condition commonly affects other neurological functions as well, impacting mood and causing a decline in cognition. A drug that blocks a key receptor linked with blood pressure has shown promise recovering memory in models of vascular dementia, inspiring researchers from the University of Arizona to test the treatment on mice with Parkinson's-like symptoms.
Continue Reading.
146 notes
·
View notes
Text
Also preserved in our archive
Hey! Look! A great breakdown of that thing I'm always talking about being a big yet entirely-overlooked deal by 90% of medical professionals in regards to this particular virus!
SARS-CoV-2, the virus behind COVID-19, is not done with us. Over the past four years, it has shown a remarkable ability to adapt, with each new variant outmaneuvering our immune systems in unique ways. The recently published study on the XEC variant (November 22, 2024) provides fresh insights into how this virus is evolving. (1) Combining this with the broader history of immune evasion, we see a troubling pattern: the virus continues to find ways to evade the immune system and in many cases, persist, potentially leaving lasting impacts on our health even for those who experience only mild or asymptomatic infections.
What the Study Found: XEC’s Immune Escape Arsenal The latest study revealed that the XEC variant—an offspring of two previous variants, KS.1.1 and KP.3.3—has developed mechanisms that make it harder for our immune systems to neutralize it. Here’s how it works:
1. Glycosylation Mutations in the N-terminal Domain (NTD):
The XEC variant introduces new glycosylation sites, such as the T22N mutation, which act like a cloak, hiding key parts of the virus from antibodies.
These sugar molecules shield the receptor-binding domain (RBD), a crucial target for vaccines and natural immunity, making it harder for antibodies to bind and neutralize the virus.
2. Allosteric Effects:
Mutations in the NTD don’t just shield the virus—they also alter the behavior of the RBD through a process called allostery. These changes can make the RBD less accessible or alter how it interacts with human cells, further reducing the effectiveness of antibodies.
3. Potential Impact on Membrane Fusion:
The study hints that these mutations may also enhance how efficiently the virus fuses with human cells, potentially increasing its infectivity.
Immune Evasion: A Constant Tug-of-War The ability of SARS-CoV-2 to adapt is not new. Looking back at the history of immune evasion, we see a pattern:
The Early Days: Mutations like D614G made the virus more infectious.
Alpha and Beta Variants: N501Y and E484K mutations increased binding to human cells and evasion of neutralizing antibodies.
Omicron Era: A flurry of spike protein mutations allowed the virus to reinfect people with previous immunity and bypass vaccine-induced protection.
XEC is the next chapter in this story, combining these strategies with new tricks like glycosylation and allosteric modulation to stay ahead of human defenses.
Why This Matters: Beyond Infections Understanding immune evasion isn’t just about tracking infections—it’s about long-term health impacts. Here’s why this evolution is particularly concerning:
1. The Shadow of Long COVID:
Millions of people suffer from Long COVID, characterized by fatigue, brain fog, heart palpitations, and muscle pain. The virus’s ability to persist and evade the immune system might explain why symptoms linger for months or years in some individuals.
Chronic immune activation or hidden reservoirs of the virus could drive these long-term effects.
2. Asymptomatic but Chronic Damage:
Even in people without noticeable symptoms, SARS-CoV-2 has been shown to cause subtle, potentially long-term damage to:
Vascular systems: Leading to inflammation and microclot formation.
Neurological function: Disrupting brain activity and potentially accelerating neurodegenerative conditions. Early onset dementia
Musculoskeletal health: Causing unexplained weakness or pain.
Cognitive performance: Contributing to memory issues and reduced mental clarity. Are you or someone you know having more trouble finding words to use or losing things more often?
3. Vaccines Alone Aren’t Enough:
While vaccines remain essential, their effectiveness is limited by the virus’s rapid evolution. Variants like XEC show how SARS-CoV-2 can sidestep even the most advanced immune defenses, highlighting the need for next-generation vaccines targeting broader parts of the virus. We have know this for a long time now so where are the broader targeting vaccines?
The Future of SARS-CoV-2 Evolution The virus has already demonstrated its ability to adapt to our immune responses in multiple ways, and there’s no reason to believe it will stop. Here are some possibilities for future adaptation:
Further Refinement of Glycosylation: Adding or modifying sugar molecules could make the virus even more difficult to detect.
Enhanced Membrane Fusion: Mutations that improve how the virus merges with human cells could increase its infectivity.
Host Adaptation: Over time, the virus could become better at hiding within human cells, evading both natural immunity and therapeutic interventions.
Increased Chronicity: The virus might evolve to persist at low levels in the body, leading to ongoing inflammation and long-term health consequences.
What We Can Do: Adapting to the Virus’s Adaptations The XEC variant and others like it remind us that SARS-CoV-2 is still a formidable opponent. Here’s what we can do:
1. Invest in Better Vaccines:
Universal or pan-coronavirus vaccines that target conserved regions of the virus are critical.
2. Improve Diagnostics:
Detecting chronic or asymptomatic infections early could help mitigate long-term health effects.
3. Focus on Treatment:
Antiviral drugs that target different parts of the virus, combined with treatments for inflammation and immune dysregulation, could help reduce the impact of Long COVID.
4. Stay Vigilant:
For individuals, maintaining basic preventive measures during high transmission periods can significantly reduce risks.
Conclusion: Learning from the Virus SARS-CoV-2 is teaching us a harsh lesson about evolution. Its ability to adapt and evade our defenses, from antibodies to T-cells, shows no sign of slowing down. Variants like XEC underscore the importance of continued research, innovation, and public health vigilance. By understanding the virus’s strategies and preparing for its next moves, we can better protect ourselves—not just from acute infections but from the long-term consequences.
Reference:
Enhanced immune evasion of SARS-CoV-2 variants KP.3.1.1 and XEC through N-terminal domain mutations (November 22, 2024)
www.thelancet.com/journals/laninf/article/PIIS1473-3099%2824%2900738-2/fulltext
#mask up#public health#wear a mask#pandemic#covid#covid 19#wear a respirator#still coviding#coronavirus#sars cov 2
48 notes
·
View notes
Text
Neurodivergence should be more normalized than it is.
Period.
It should be normalized.
And we need to talk about it more.
We recently - like last 15 years or so- have started talking more about autism and ADHD.
Oh, we have known about it longer. We have talked about it academically.
I mean talking about it over dinner or on our work breaks.
Maybe some people have spoken about it longer, but in the past 15 years, I have seen an increase in that discussion.
Especially as we learn more about autism and ADHD.
But there is more than that.
Psychosomatic symptoms
Situational triggers
Various sensory issues
Neurodivergence from illness and injury and trauma.
They exist. In the past 5 years, I am starting to hear people talking about those too.
But not as much. Not loudly.
Please.
Talk more about it. Talk about symptoms more. Talk about how you cope.
It matters.
It matters when we talk about how to focus our attention. It matters when we talk about stimming, soothing, and other ways to cope. It matters when we talk about grounding techniques. It matters when we talk about our struggles and our adaptations
It matters for mental health. It matters for physical health - I only recently learned about vascular dementia. Where leaking blood vessels and blood pressure changes can create dementia. Where circulation and heart health can change ability to remember and retain information. I only recently started seeing information on how septic infections can distort thinking.
But if we don't talk about how we think or see something normally, how do we know it is distorted thinking for that person?
There are physical factors. There are mental factors. There are genetic factors. There are environmental factors.
Please normalize neurodivergence, for everyone's sake.
Please talk about neurodivergence more.
6 notes
·
View notes
Text
the lab tech told me there's a huge covid wave right now (how surprising lol)
it's always the right time to start masking with a well fitting ffp2 or n95 mask, for your health and the health of your family friends and community including people with disabilities and health problems
first of all covid is airborne it means it behaves in the air like a deodorant or an airwick spray. staying at a distance from someone will only spare you some of the droplets but not the whole thing.
covid often causes lots of different issues in the human body, even when it's an asymptomatic infection, regardless of age and health: cardio vascular system, lungs, nervous system/brain/early dementia/memory/depression, immune system, taste smell vision and hearing loss. there's is about 20% chance of getting long covid each time you get infected and risk increase with the number of infections even if they're asymptomatic. long covid can take different forms but basically people are disabled with lots of conditions making making their life quality shit. some are bed bound with symptoms similar to pots or neurological diseases.
the vaccine only prevents severe reactions to the infection and only works for some variants. if you haven't gotten a booster in the last 6 months/year it's not effective anymore
the main tools we have are well fitting ffp2/ffp3/n95 masks, air ventilation/purifying and testing
3 notes
·
View notes
Text
New Alzheimer's drugs bring hope. But not equally for all patients.
https://www.washingtonpost.com/health/2024/01/29/alzheimers-new-drugs-black-patients-leqembi/
ABINGTON, Pa. — Wrapped in a purple blanket, Robert Williford settles into a quiet corner of a bustling neurology clinic, an IV line delivering a colorless liquid into his left arm.
The 67-year-old, who has early Alzheimer’s disease, is getting his initial dose of Leqembi. The drug is the first to clearly slow the fatal neurodegenerative ailment that afflicts 6.7 million older Americans, though the benefits may be modest. The retired social worker, one of the first African Americans to receive the treatment, hopes it will ease his forgetfulness so “I drive my wife less crazy.”
But as Williford and his doctors embark on this treatment, they are doing so with scant scientific data about how the medication might work in people of color. In the pivotal clinical trial for the drug, Black patients globallyaccounted for only 47 of the 1,795 participants — about 2.6 percent. For U.S. trial sites, the percentage was 4.5 percent.
The proportion of Black enrollees was similarly low for Eli Lilly Alzheimer’sdrug, called donanemab, expected to be cleared by the Food and Drug Administration in coming months. Black people make up more than 13 percent of the U.S. population.
The paltry data for the new class of groundbreaking drugs, which strip a sticky substance called amyloid beta from the brain, has ignited an intense debate among researchers and clinicians. Will the medications — the first glimmer of hope after years of failure — be as beneficial for African Americans as for White patients?
“Are these drugs going to work in non-Whites? And particularly in Blacks? We just don’t have enough data, I don’t think,” said Suzanne E. Schindler, a clinical neurologist and dementia specialist at Washington University in St. Louis. “In general, the default is that they will work the same in everybody, but we don’t really know that for sure.”
The situation casts a spotlight yet again on the decades-long failure of researchers to reflect the increasingly diverse character of the patient population in the United States, and underscores the stark disparities in Alzheimer’s treatment and care. Black Americans develop the disease and related dementias at twice the rate of their White counterparts, but are less likely to receive specialized care and are diagnosed at later stages, studies show. That’s an urgent problem considering that the new drugs must be used early to have an effect.
In addition, a perplexing new issue appears to be contributing to low Black enrollment in trials and is fueling a debate among experts about the role of race, genetics and other factors. To qualify for the main trial for Leqembi — developed by the Japanese pharmaceutical giant Eisai and the biotechnology company Biogen of Cambridge, Mass. — participants were required to have elevated levels of brain amyloid, a defining characteristic of Alzheimer’s, and symptoms such as memory loss.
But brain scans showed that the African American volunteers were less likely to have excess amyloid than White patients and thus were excluded from the trial at higher rates. Almost half of Black applicants failed to meet the amyloid threshold, compared with 22 percent of White volunteers, according to Eisai. A similar pattern occurred with the Lilly drug and in some other studies, and sometimes involved other people of color, including Hispanics.
Experts are baffled by the findings. Why would amyloid levels — thought to be a key driver of Alzheimer’s — be different in people with similar cognitive problems?
“Is it the color of someone’s skin? Almost certainly not,” said Joshua D. Grill, an Alzheimer’s researcher at the University of California at Irvine. “Is it a difference in genetics? Or other health conditions, like cholesterol, blood pressure or vascular health? Or is it something else, that we haven’t measured?”
While the biology of Alzheimer’s is almost surely the same regardless of race, some researchers say the patients themselves might be different because of underlying health conditions. Some older Black patients diagnosed with Alzheimer’s, they say, might actually have vascular dementia stemming from heart disease, hypertension and diabetes — all conditions more prevalent among African American patients.
The risk of vascular damage also could be increased by a lack of access to health care and years of exposure to racism, as well as genetics, some experts say. And many patients could have a constellation of pathologies driven by other factors, they add.
Whatever the cause, experts say, the bottom line is the same: Patients who do not have excessive amounts of the sticky brain protein should not be treated with the amyloid-targeting drugs because the therapies are unlikely to work and pose substantial risks, including potentially deadly bleeding in the brain.
But that raises the specter of another disparity. If it turns out that a lower proportion of Black dementia patients and other people of color have excess amyloid, they could be left behind as the drug industry races to develop amyloid-reducing treatments. To counter that, experts are urging companies to accelerate work addressingother potential drivers of cognitive decline and to develop combination drugs with multiple targets.
“If we are just targeting amyloid, we can just miss a large potential population that might benefit from treatment,” said Lisa L. Barnes, a neuropsychologist at Rush University in Chicago.
‘A brain is a brain’
For now, the question remains: What should Black patients and their doctors think about the anti-amyloid drugs?
The answer, experts say, depends largely on the level of amyloid in their brains.
More than a year ago, Williford was diagnosed with early Alzheimer’s by David C. Weisman, a neurologist at Abington Neurological Associates, a large practice north of Philadelphia that treats patients and conducts clinical trials for drug companies. The clinic was one of the test sites for Leqembi.
After Leqembi receivedfull FDA approval last summer, Williford underwent tests to determine whether he was a good candidate for the drug. One test — a lumbar puncture, sometimes called a spinal tap — showed elevated amyloid in his brain. That means Williford and similar patients are likely to benefit from an anti-amyloid medication regardless of their race or ethnicity, Weisman and several other experts said.
“A brain is a brain is a brain, whether it is Asian, Hispanic, African American or White,” Weisman said. “A patient is either a good fit or a bad fit, and Robert is a good fit.”
Williford, who spent years working with troubled families in Philadelphia, began having memory problems a few years ago, said his wife, Cynthia Byron-Williford, 59.
“You could tell him almost anything, and he would almost immediately forget,” she said. “If I asked him to make a peanut butter sandwich for our grandson, he would come back three times and say, ‘What am I supposed to do?’”
With few treatment options, many physicians say they will offer anti-amyloid therapy to any patient who has elevated levels of the substance and passes safety tests.
Barry W. Rovner, a neurology professor at Thomas Jefferson University in Philadelphia, said he would not hesitate to offer Leqembi to African American patients who tested positive for amyloid. But, he added, because of the low numbers of Black individuals in the Leqembi trial, “I would say, ‘Look, this has not been tried in many Black people, so we don’t know precisely how it is going to work. But you don’t know precisely how it will work in any person.’”
From a research perspective, “You could say, as a group we don’t know if Black individuals respond the same way to anti-amyloid drugs because we don’t have the data,” Washington University’s Schindler said. “But on an individual level, it is different. If I had a Black patient who was amyloid-positive, I would start him on these drugs.”
But some Black patients might not be comfortable with the medication.
Zaldy S. Tan, director of the memory disorders center at Cedars-Sinai Medical Center in Los Angeles, said when African American patients are informed about the risks and benefits of Leqembi, and about the sparse data available for Black individuals, some will “take a pause and question whether they are willing to accept the uncertainty” and challenges of receiving the every-other-week infusion and multiple follow-up tests.
A promise of diversity
The best way to know for sure how drugs for Alzheimer’s — and other diseases — affect different populations is to have more diversity in trials, experts agree. But research participation by Black Americans and other people of color has been held down for years for several reasons.
The 20th century’s infamous Tuskegee syphilis study created long-standing mistrust about trials within the African American community. Men were left untreated to suffer and die even after an effective treatment emerged for the bacterium.
Alzheimer’s research, meanwhile, has long been centered in memory clinics at elite academic institutions, which tend to attract well-heeled patients with health insurance and other resources. The clinics have served as effective recruiting grounds for trials that end up with a predominantly White enrollment.
“We have done a poor job of making African American Alzheimer’s research inclusive,” said John Morris, a neurologist at Washington University in St. Louis. More than two decades ago, he created an African American advisory board at the school’s Knight Alzheimer Disease Research Center after realizing only 3 percent of trial participants were Black.
Others also are redoubling efforts to increase diversity. John Dwyer, president of the Global Alzheimer’s Platform Foundation, a nonprofit that runs trials, said the organization has sharply increased participation by people of color by sending dedicated teams of African American and Latino professionals into communities to build relationships with physicians and personnel at health centers, senior centers and places of worship. They stress to the communities how much they can benefit from the studies, he said.
Stephanie Monroe, vice president and senior adviser of health equity and access at the advocacy group UsAgainstAlzheimer’s, noted that low Black enrollment is not limited to Alzheimer’s trials. If all the drugs that have not been tested on people of color were eliminated, the shelves of pharmacies would be nearly empty, she said.
“That doesn’t work when you are almost a 50-50 minority/majority population,” Monroe said.
The FDA has issued guidelines for industry designed to bolster diversity in studies, while the National Institute on Aging recently pledged toprioritize funding requests that are “appropriately inclusive.”
The low Black enrollment in studies is just the latest controversy involving the anti-amyloid drugs. For years, earlier versions of the drugs failed repeatedly in trials. By contrast, Leqembi, in an 18-month trial, showed unambiguous, if modest, benefits, slowing disease progression by about 27 percent, or roughlyfive months. The drug, administered every other week, carries a list price of $26,500 a year.
In July, Lilly reported that its anti-amyloid drug, donanemab, was even more effective at removing amyloid. But like Leqembi, it can cause serious side effects, including brain hemorrhages. Some doctors think the drugs will provide bigger benefits when taken for a longer period or earlier in the disease, but others say the medications, which require repeated MRIs to check for side effects, leave much to be desired.
Both Eisai and Lilly said they are working hard to increase diversity in clinical trials. In the meantime, they said, patients with elevated amyloid should benefit from the anti-amyloid drugs, regardless of race or ethnicity.
“We have no pathophysiological reason to expect different efficacy between races and ethnicities for Alzheimer’s treatments that remove amyloid,”Lillysaid in a statement.
Eisai acknowledged that the Leqembi trial was not designed to test the drug in individual racial and ethnic subgroups. But it said in a statement that the totality of the evidence indicated that “all patients, regardless of ethnicity, benefited from treatment” with the drug.
“We and the U.S. FDA — as evidenced by the agency’s approval of Leqembi — believe that the benefits and risks in these patient populations and races has been established,” the company added. Eisai said volunteers who did not pass the amyloid threshold did not have Alzheimer’s and should be assessed for other conditions.
In an interview, Teresa Buracchio, acting director of the FDA’s Office of Neuroscience, said the agency “did not see a notable difference by race” in safety and effectiveness in the limited data available on subgroups in the Leqembi trial.
But other experts were skeptical, saying the number of Black patients in the Leqembi trial was too low to know whether the medication is safe and effective for African Americans. “Without having a representative population, it is impossible to assess,” said Barnes, of Rush University.Some researchers suggested that patients in underrepresented populations should wait for future advances in treatment.
‘We just want to get going’
On a recent day, nurse Christine Besso bustled in and out of Williford’s infusion room at the neurology clinic, taking his vital signs and inserting an IV line. “Let’s get this party started,” she said.
Byron-Williford, watching the process from a nearby couch, said she was not concerned about the low numbers of African Americans in the Leqembi trial.
“I think it will work or not work based on the individual,” she said, adding with a laugh, “and if it doesn’t work for him, it is because he is ornery.”
Byron-Williford said her husband’s health problems accelerated a few years ago after his son, who was in his early 20s, died unexpectedly. Williford became depressed and lost his appetite. Last summer, when he went to pick up his wife at a nearby hair salon, he drove around, lost. She later confiscated his car keys.
In the clinic, shortly after Williford’s infusion began, Weisman stopped in to check on him and discuss possible side effects. When Williford asked him how long he would be on the drug, Weisman shrugged, saying it depended on how he did on the drug and on test results.
“We are getting on an airplane, and we don’t even have a destination airport yet,” Weisman said. “We just want to get going.”
#Black Lives Matter#Alzheimers#Dementia#Black Lives#Black Health Matters#Black Medical Professionals#New Alzheimer’s drugs bring hope But not equally for all patients.#Mental Health Care
3 notes
·
View notes
Text
Saving another one; not mine:
All of the studies coming out - ALL of them - show repeated Covid infections being really bad for you. For your brain. For your vascular system. For your immune system. I think if we wait 5 to 10 years it will become super obvious. If you watch local groups sometimes it already is - the mom who’s kid is on week 4 of strep despite multiple rounds of antibiotics, the man with the lingering cough he just can’t seem to shake, the gofundme for the dad in his 30s who died of a stroke, the lady who is just so tired recently and just can’t shake it, the people in their 40s complaining about memory loss and how they are getting old. The thing is humanity has plenty of experience with diseases that aren’t too bad at first and are REALLY bad later on - HIV is a mild cold on first infection, mono sucks but goes away to become MS later, chicken pox is a one week wonder but shingles can cause permanent complications. Heck anyone who has played Plague Inc knows the best way to infect everyone is to make your virus have extremely mild or no initial symptoms so that people don’t worry about it and then ramp up the consequences once everyone is infected. And now that people have allowed themselves and their children to get infected because they needed youth sports and going out to eat and 50,000 person concerts without masks, if they acknowledge that that was a bad choice, then what? They have to admit they were wrong and that they might face a lifetime of consequences because of it. That they may have shortened their own lives and their children’s lives. And if there is anything modern people are not prepared to do, it is admit they were wrong. Or to do anything that goes counter to their own personal comfort. Ultimately if I am wrong, and Covid is no big deal, in 5 years I can take off my mask. In the meantime, I didn’t catch every cold, every flu and every case of strep throat going around. But I can take my mask off at any time and blend right back in. If I’m right about the dangers of Covid, I can’t go maskless now and decide to mask in 5 years and have my body be ok. If I make the choice to unmask now, I lose my choices to live a meaningful life later. I’ve seen early onset dementia, people who are immunocompromised and have to live limited lives to stay alive, people with various illnesses who can’t do so many things. I would much rather choose to limit myself from giant concerts and indoor dining than have my body limit me from walks and playing with my kids and grocery stores. My life is full and meaningful now. Different than before and I’ve lost most of my social relationships. But I am slowly building new ones with other people who still Covid locally and I spend time with my immediate family. It is hard and it feels a bit nuts sometimes. And then I go on Twitter and read the latest published study in Science and go, yep don’t want that.
5 notes
·
View notes
Text
The Effects of High Cholesterol in the Body: Understanding the Risks and Consequences
Cholesterol is a waxy, fat-like substance found in the bloodstream and cells of the body. While it is essential for producing hormones, vitamin D, and substances that help digest food, excessive cholesterol levels can have severe health consequences. High cholesterol often goes unnoticed, as it does not present immediate symptoms, but over time, it can lead to serious health issues, including heart disease, stroke, and other complications. Understanding the effects of high cholesterol on the body is crucial for maintaining good health and preventing long-term damage.
1. Atherosclerosis and Heart Disease
One of the most significant effects of high cholesterol is atherosclerosis, a condition where cholesterol and other substances build up in the walls of arteries, forming plaques. These plaques narrow and harden the arteries, restricting blood flow. As a result, the heart has to work harder to pump blood, increasing the risk of coronary artery disease (CAD). This condition can lead to angina (chest pain), heart attacks, and even heart failure.
2. Increased Risk of Stroke
When cholesterol plaques accumulate in the arteries supplying blood to the brain, they can cause a blockage or rupture, leading to a stroke. A stroke occurs when part of the brain does not receive enough oxygen, resulting in brain cell damage or death. The effects of a stroke can range from temporary weakness to permanent disability, depending on the severity and the area of the brain affected.
3. Hypertension (High Blood Pressure)
High cholesterol contributes to hypertension, as the narrowing of the arteries forces the heart to pump harder to circulate blood. Over time, high blood pressure damages the arteries, making them more prone to plaque formation, creating a vicious cycle of worsening cardiovascular health. Uncontrolled hypertension increases the risk of heart attacks, strokes, and kidney damage.
4. Peripheral Artery Disease (PAD)
High cholesterol can also affect the arteries in the limbs, especially the legs, leading to peripheral artery disease (PAD). This condition occurs when plaque buildup reduces blood supply to the extremities, causing pain, numbness, and difficulty walking. In severe cases, PAD can lead to ulcers, infections, and even amputation.
5. Impact on Liver Function
The liver plays a vital role in cholesterol metabolism. However, when cholesterol levels become excessively high, it can contribute to fatty liver disease. This condition, known as non-alcoholic fatty liver disease (NAFLD), leads to liver inflammation, scarring, and even liver failure if left untreated. The liver may struggle to process cholesterol effectively, leading to an unhealthy buildup in the bloodstream.
6. Gallstones and Digestive Issues
Excess cholesterol can also contribute to the formation of gallstones, which are solid particles that develop in the gallbladder. These stones can cause digestive discomfort, nausea, and severe abdominal pain. In some cases, gallstones may require surgical removal of the gallbladder.
7. Memory Loss and Cognitive Decline
Studies suggest that high cholesterol levels may be linked to memory loss and cognitive decline. Cholesterol buildup in blood vessels supplying the brain can lead to reduced blood flow, increasing the risk of vascular dementia and even Alzheimer’s disease. Maintaining healthy cholesterol levels is essential for long-term brain function and cognitive health.
8. Diabetes and Insulin Resistance
High cholesterol is closely related to diabetes, as both conditions often coexist. Elevated levels of LDL (bad cholesterol) and triglycerides can lead to insulin resistance, where the body's cells do not respond properly to insulin. This can worsen blood sugar levels, increasing the risk of type 2 diabetes and its complications, such as nerve damage, kidney disease, and vision problems.
Prevention and Management
To prevent the harmful effects of high cholesterol, it is essential to adopt a healthy lifestyle:
Eat a balanced diet rich in fiber, healthy fats, and lean proteins while avoiding trans fats and excessive saturated fats.
Exercise regularly to maintain a healthy weight and improve heart health.
Monitor cholesterol levels with regular check-ups.
Avoid smoking and excessive alcohol consumption, as they contribute to heart disease.
Take prescribed medications (such as statins) if lifestyle changes alone are not enough.
1 note
·
View note
Text
Alzheimer’s & Dementia Care | Vero Beach, FL | Aqua Home Care

Dementia is a life-changing condition that affects millions of seniors worldwide, and for families in Vero Beach, ensuring that a loved one receives the proper care and support during the progression of dementia can be a daunting task. Whether it's Alzheimer's disease, vascular dementia, or another form of cognitive impairment, the challenges that come with caring for a loved one with Dementia Vero Beach require patience, expertise, and a compassionate approach. In Vero Beach, families can find specialized dementia care services designed to provide seniors with the attention and support they need to maintain their dignity and comfort in familiar surroundings.
Understanding Dementia and Its Impact
Dementia is an umbrella term for a range of symptoms that affect cognitive function, including memory loss, confusion, difficulty with communication, and changes in behavior. The most common form of dementia is Alzheimer's disease, but other types of dementia, such as Lewy body dementia and frontotemporal dementia, also affect many seniors.
As dementia progresses, individuals may experience memory loss, disorientation, difficulty completing everyday tasks, and challenges in communicating with others. The disease not only impacts the individual but also affects their family and loved ones. Many families in Vero Beach face the difficult decision of how best to support their aging relatives while helping them maintain their quality of life.
Dementia Care Services in Vero Beach
Dementia care in Vero Beach focuses on providing personalized care that addresses the unique needs of individuals living with cognitive decline. Whether the individual is in the early stages of Dementia Vero Beach or dealing with advanced stages, there are specialized services to provide assistance and ensure they continue to live as comfortably and independently as possible.
Personal Care and Assistance Seniors with dementia may require assistance with daily activities, such as bathing, dressing, eating, and toileting. Dementia care providers in Vero Beach offer compassionate, non-invasive support that promotes independence while ensuring that these essential tasks are completed safely. Caregivers are trained to assist with mobility and help manage the behavioral changes that often accompany dementia, such as wandering or agitation.
Cognitive Stimulation and Activities While there is no cure for dementia, keeping the brain active can help delay the progression of symptoms and improve quality of life. Dementia care services in Vero Beach include cognitive exercises and activities that encourage mental engagement. These may involve memory games, reading, puzzles, and creative activities like art and music therapy. These activities help stimulate cognitive function and provide an enjoyable way for seniors to stay engaged.
Companionship and Emotional Support Dementia can be an isolating condition, leading to feelings of loneliness and depression. In Vero Beach, dementia care providers offer companionship and emotional support to help seniors feel less isolated. Caregivers can engage in meaningful conversations, participate in social activities, and provide reassurance during moments of confusion or anxiety. This emotional connection plays a critical role in reducing stress and promoting mental well-being for individuals with dementia.
Behavior Management and Safety Seniors with dementia may experience behavioral changes such as aggression, confusion, or anxiety. Caregivers trained in dementia care use techniques to manage these behaviors calmly and effectively. By providing a structured and familiar environment, caregivers in Vero Beach can help reduce the triggers that cause agitation or stress. Safety is also a priority, with caregivers ensuring that the living space is free from hazards and monitoring for wandering or falls.
Health Monitoring and Medication Management Many individuals with dementia also have other health conditions that require ongoing management. Dementia Vero Beach care services in Vero Beach include health monitoring and medication assistance, helping ensure that seniors take their medications correctly and on time. Caregivers can assist with administering medications, tracking side effects, and coordinating appointments with healthcare providers. In some cases, licensed nurses may be involved in providing medical care and monitoring vital signs.
Respite Care for Family Caregivers Caring for a loved one with dementia can be physically and emotionally draining for family members. Respite care services in Vero Beach provide families with temporary relief, allowing them time to rest, attend to personal matters, or simply recharge. Whether it’s for a few hours or several days, respite care ensures that the senior continues to receive the care they need while giving family caregivers a well-deserved break.
End-of-Life and Palliative Care For seniors in the later stages of dementia, palliative and end-of-life care may be necessary to ensure comfort and dignity. Dementia care providers in Vero Beach can help manage pain, reduce anxiety, and provide emotional and spiritual support during this difficult time. Hospice care services are available to support both the individual and their family, offering compassionate care that focuses on comfort rather than curative treatments.
Benefits of Dementia Care in Vero Beach
Familiar, Comfortable Environment One of the main benefits of dementia care in Vero Beach is the ability for seniors to remain in the comfort of their own homes or familiar surroundings. Being in a familiar environment reduces confusion and anxiety, helping individuals with dementia feel more secure. This can also lead to better physical and emotional outcomes.
Personalized, Compassionate Care Dementia care services in Vero Beach are designed to meet the unique needs of each individual. Care plans are customized based on the person’s specific condition, preferences, and routines, ensuring that they receive care that is both effective and respectful of their independence. With caregivers who are experienced in dementia care, families can rest assured that their loved ones are in good hands.
Improved Quality of Life With the right care, individuals with dementia can continue to live fulfilling lives. Engaging in activities that stimulate the mind, maintaining a healthy daily routine, and having companionship can all contribute to improved mental and emotional well-being. Dementia Vero Beach care providers in Vero Beach aim to enhance quality of life by offering individualized support that fosters independence and comfort.
Support for Family Caregivers Dementia care in Vero Beach not only helps the senior but also provides much-needed support for family caregivers. Balancing caregiving responsibilities with work, family, and personal life can be overwhelming. With professional care, families can ensure their loved one is receiving the best care possible while maintaining their own well-being.
How to Choose the Right Dementia Care Provider in Vero Beach
When selecting a dementia care provider in Vero Beach, consider the following:
Assess the Level of Care Needed The level of care required will depend on the stage of dementia and the senior’s overall health. Determine whether your loved one needs assistance with daily activities, cognitive support, or more advanced medical care, and choose a provider who offers the appropriate services.
Look for Experienced Caregivers It’s essential to choose a care provider that employs trained, experienced caregivers who specialize in dementia care. Look for certifications or accreditations in dementia care, and make sure the caregivers have experience managing dementia-related behaviors.
Verify Licensing and Accreditation Ensure the dementia care provider is licensed by the state and meets all regulatory requirements. Accreditation from organizations like the Alzheimer's Association can provide peace of mind that the care being provided is of the highest quality.
Consider Flexibility and Availability Dementia care needs can change over time, so it’s important to choose a provider that offers flexible care options. Whether your loved one requires full-time care, part-time assistance, or respite care for family members, make sure the provider can adapt to their needs as they evolve.
Conclusion
Dementia Vero Beach offers seniors with cognitive decline the opportunity to receive personalized, compassionate care in the comfort of their own homes or familiar environments. With services ranging from personal care and medication management to companionship and behavior management, dementia care providers can help seniors maintain their dignity, comfort, and quality of life. Families in Vero Beach can find the support they need to ensure that their loved ones are well cared for, while also receiving respite and peace of mind.
0 notes
Text
Alzheimer’s and Dementia Care in Naples, FL

As the population in Naples continues to grow and age, the demand for specialized Dementia Naples care is rising. For families facing the challenges of caring for loved ones with dementia, it’s essential to understand the condition, available care options, and the resources that Naples provides. Dementia is a broad term that describes a range of symptoms affecting memory, thinking, and social abilities. It is a progressive condition that can severely impact a person’s daily life, requiring specialized care and understanding.
In Naples, families can find a variety of services dedicated to providing high-quality dementia care, whether at home or within specialized care facilities. These services are designed to support both the individual with dementia and their family caregivers. In this blog, we will explore dementia care in Naples, what resources are available, and how families can navigate the complex process of ensuring their loved ones receive the care they need.
What is Dementia?
Dementia refers to a group of symptoms affecting cognitive functions such as memory, communication, and reasoning. Alzheimer's disease is the most common form of dementia, but there are other types, including vascular dementia, Lewy body dementia, and frontotemporal dementia. While dementia affects individuals differently, common signs include forgetfulness, difficulty with problem-solving, and challenges with basic daily activities like eating, dressing, and bathing.
Dementia is progressive, meaning symptoms get worse over time. As the condition advances, individuals may require increasing levels of care, making it vital for families to understand the stages of dementia and how care needs evolve.
Dementia Care Options in Naples
Naples offers a wide variety of dementia care options that are tailored to meet the specific needs of those with the condition. These options range from home care to specialized dementia units within assisted living or memory care facilities. Understanding the different options available is the first step in selecting the right type of care for a loved one with dementia.
In-Home Dementia Care: Many families opt for in-home dementia care as it allows their loved ones to remain in familiar surroundings. Home care providers offer services that can be customized to the individual's needs, such as personal care (help with bathing, dressing, and grooming), meal preparation, housekeeping, medication reminders, and companionship. In Naples, several licensed home care agencies specialize in dementia care, ensuring that caregivers have the necessary training to work with individuals who have memory loss or cognitive decline.
Memory Care Communities: For those in need of more intensive care, memory care communities are designed specifically for individuals with dementia. These facilities offer secure environments that reduce the risk of wandering and provide 24/7 supervision. Memory care staff are specially trained to handle the unique challenges associated with dementia, such as behavioral changes and communication difficulties. In Naples, several memory care units provide a range of services, from mild to advanced stages of Dementia Naples, with engaging activities that promote cognitive stimulation, physical health, and socialization.
Assisted Living with Dementia Support: Assisted living facilities in Naples can offer varying levels of care to residents, including assistance with activities of daily living (ADLs) such as eating, bathing, and dressing. Many assisted living facilities have specialized dementia support programs for residents with early- to mid-stage dementia. These programs combine the safety of a community setting with personalized care that adapts as the individual’s condition progresses.
Skilled Nursing Care: For individuals with advanced dementia who require round-the-clock medical attention, skilled nursing care may be the most appropriate option. Skilled nursing facilities (SNFs) in Naples provide full-time medical support and can manage complex health conditions alongside dementia. These facilities provide a higher level of medical care than memory care communities and offer rehabilitation services for individuals who may be recovering from illness or surgery in addition to their dementia-related needs.
Adult Day Programs for Dementia: Adult day programs in Naples offer temporary relief for family caregivers. These programs provide socialization, activities, and some level of supervision during the day while giving caregivers a break. Some adult day programs also offer specialized dementia care and can help individuals with memory loss stay engaged through activities like art, music therapy, and physical exercise.
Why Choose Naples for Dementia Care?
Naples is home to a vibrant community that values seniors and understands the importance of offering specialized dementia care. The city’s warm climate, combined with the expertise of local healthcare professionals, makes it an attractive destination for both retirees and those seeking top-quality care for loved ones with dementia.
Access to High-Quality Healthcare: Naples is home to a number of excellent hospitals and healthcare providers specializing in aging adults and dementia care. Access to neurologists, geriatricians, and specialized memory care programs ensures that seniors with dementia have access to the best care options available.
Specialized Memory Care Services: Many assisted living and memory care communities in Naples have been designed specifically with dementia in mind, offering secured environments, Dementia Naples-friendly activities, and trained staff members who understand how to manage the challenges associated with the disease.
Respite and Support for Caregivers: Caring for a loved one with dementia can be physically and emotionally exhausting. In Naples, caregivers can find support groups, educational resources, and respite care options to help them manage the demands of caregiving. These resources provide a sense of community for those facing similar challenges.
The Importance of Early Diagnosis and Intervention
While dementia is a progressive condition, early diagnosis can make a significant difference in the quality of life for both the individual and their family. Early intervention provides families with time to explore care options, develop a care plan, and make informed decisions about the future. In Naples, several healthcare providers offer screenings for cognitive decline and early dementia, helping families catch the condition early and start planning for the care their loved one will need.
Navigating Dementia Care in Naples: Tips for Families
Plan Ahead: Dementia progresses at different rates for each person, so it’s important to plan ahead. Consider the individual’s current abilities, preferences, and future care needs when exploring care options. This will allow you to make decisions that prioritize their well-being and comfort.
Involve the Person with Dementia: As much as possible, involve your loved one in the decision-making process. While dementia may impair their memory and ability to communicate, they can still provide valuable insights into their preferences and wishes.
Seek Professional Guidance: Families should seek advice from professionals who specialize in dementia care, including healthcare providers, elder care advisors, and legal experts. These professionals can help families navigate the complexities of dementia, from managing finances and legal documents to choosing the right care facility.
Utilize Local Resources: In Naples, numerous resources are available for families, including support groups, educational workshops, and respite care services. Engaging with these resources can help families better understand dementia and access the support they need.
Final Thoughts on Dementia Care in Naples
Dementia care in Naples offers a range of options designed to meet the individual needs of seniors and their families. With access to specialized memory care facilities, in-home services, and a supportive community, Naples is an excellent place for those seeking high-quality care for a loved one with dementia. Early diagnosis, professional support, and careful planning are key to ensuring the best outcomes for seniors living with Dementia Naples, allowing them to live their lives with dignity and comfort.
0 notes
Text
1-On-1 Care | Jupiter, FL | Aqua Home Care

As dementia becomes more common among seniors, providing the right care and support is essential for both individuals and their families. In Greenacres, dementia care services offer specialized, compassionate assistance to seniors dealing with Alzheimer's disease, vascular dementia, or other forms of cognitive decline. These services are designed to help individuals maintain their quality of life while ensuring their safety, comfort, and well-being.
Dementia Care Greenacres focuses on providing personalized care tailored to the needs of individuals at every stage of dementia. Whether it’s managing daily routines, offering emotional support, or ensuring safety in the home, dementia care professionals are trained to handle the unique challenges that come with cognitive decline. In Greenacres, families can access a variety of dementia care options that allow their loved ones to remain at home while receiving the specialized support they need.
What is Dementia Care, and Why is it Important in Greenacres?
Dementia care refers to services that focus on the specific needs of individuals living with dementia. This type of care includes assistance with daily activities, medication management, cognitive support, and emotional reassurance. Dementia care is particularly important in Greenacres, as many families choose to keep their loved ones at home for as long as possible. This type of care ensures that seniors receive the right level of support in a safe and familiar environment, which can improve their quality of life.
Dementia care goes beyond simply assisting with tasks; it is about ensuring that individuals with dementia are treated with respect, dignity, and patience. As dementia progresses, individuals may experience memory loss, confusion, and difficulty communicating. Specialized caregivers in Greenacres understand how to approach these challenges, providing care that is sensitive to the individual’s needs.
Key Services Offered in Dementia Care in Greenacres:
Personal Care and Daily Living Support: Seniors with dementia often require help with activities of daily living (ADLs) such as bathing, dressing, grooming, and eating. Dementia Care Greenacres includes assistance with these tasks to ensure seniors maintain their personal hygiene and comfort, while also promoting their independence as much as possible.
Medication Management: Medication adherence can be particularly challenging for those with dementia. Caregivers assist with medication reminders, ensuring that seniors take their prescribed medications on time and in the correct dosages. Proper medication management is essential for controlling symptoms and managing co-existing health conditions.
Cognitive Stimulation and Memory Support: In the early stages of dementia, engaging in activities that stimulate the mind can help slow the progression of cognitive decline. Dementia care in Greenacres includes activities designed to promote mental stimulation, such as puzzles, memory exercises, reading, and discussions, which help maintain cognitive function and improve mood.
Companionship and Social Engagement: Isolation and loneliness can be harmful to seniors with dementia. Dementia care services in Greenacres provide companionship and socialization, encouraging seniors to engage in conversations, activities, and outings. Caregivers often accompany seniors to ensure they have positive, enriching interactions, which can reduce feelings of anxiety and confusion.
Safety and Fall Prevention: Seniors with dementia may become disoriented and confused, increasing the risk of accidents and falls. Dementia care professionals in Greenacres ensure that the home environment is safe and that potential hazards are minimized. Caregivers assist with mobility, help prevent falls, and make sure that seniors are supervised when needed to ensure their safety.
Meal Planning and Nutrition: Nutrition can be a concern for seniors with dementia, as they may forget to eat or have trouble preparing meals. Dementia care in Greenacres includes meal planning, preparation, and assistance with eating, ensuring that seniors receive balanced and nutritious meals. Caregivers also help with making mealtimes a positive experience, which can enhance the senior’s appetite and overall health.
Behavioral Support and Crisis Management: As dementia progresses, individuals may experience behavioral changes such as agitation, aggression, or confusion. Caregivers in Greenacres are trained to manage these behaviors with patience and understanding. They employ strategies to de-escalate challenging situations and provide reassurance to help the senior feel calm and secure.
Respite Care for Family Caregivers: Caring for a loved one with dementia can be emotionally and physically demanding. Dementia Care Greenacres offer respite care, allowing family caregivers to take a break while knowing that their loved one is in good hands. Respite care helps prevent caregiver burnout and ensures that families can continue to provide care without feeling overwhelmed.
End-of-Life and Palliative Care: In the later stages of dementia, individuals may require end-of-life or palliative care. Dementia care in Greenacres includes support for families during this difficult time, focusing on comfort, pain management, and emotional support. Caregivers ensure that seniors are treated with compassion and respect, while also providing support to family members navigating the end-of-life journey.
Why Choose Dementia Care Services in Greenacres?
Specialized Care for Dementia: Dementia care professionals in Greenacres are specially trained to meet the unique needs of individuals with dementia. These caregivers understand the complexities of dementia and are equipped to handle the various challenges associated with cognitive decline, providing care that promotes dignity and respect.
Personalized Care Plans: Dementia care in Greenacres is customized to the specific needs of each individual. Care plans are developed based on the individual’s preferences, health condition, and stage of dementia, ensuring that the care provided is tailored to their changing needs.
Comfort and Familiarity of Home: One of the main advantages of dementia care in Greenacres is the ability for seniors to remain in their own homes. This familiar environment promotes a sense of security and comfort, which is vital for seniors experiencing cognitive decline. In-home dementia care allows seniors to age in place while receiving the support they need.
Continuous Monitoring and Support: Dementia care provides 24/7 monitoring to ensure the safety and well-being of individuals. Caregivers are always on hand to assist with daily needs and respond to any emergencies or changes in condition, offering families peace of mind knowing their loved one is well-cared for.
Promotes Quality of Life: Dementia care in Greenacres is focused on enhancing the quality of life for seniors. This care is designed not only to manage symptoms but also to foster a sense of purpose, engagement, and joy. By participating in enjoyable activities and receiving emotional support, seniors can continue to experience fulfillment and happiness in their daily lives.
How to Get Started with Dementia Care in Greenacres:
Getting started with dementia care is easy and involves an initial consultation where the senior’s condition and needs are assessed. A customized care plan is then created, detailing the level of care required and how the caregiver will support the individual. Families can adjust the care schedule as needed, depending on how the dementia progresses, ensuring that the senior’s needs are consistently met.
Conclusion:
Dementia Care Greenacres offers specialized, compassionate support for seniors living with dementia. Whether it’s helping with daily tasks, providing cognitive stimulation, ensuring safety, or offering emotional support, dementia care services are designed to enhance the quality of life for seniors while giving families peace of mind. By choosing dementia care in Greenacres, families can ensure their loved ones receive the personalized, respectful care they deserve while allowing them to remain in the comfort of their own home.
0 notes
Text
Discover The 9 Surprising Early Signs Of Dementia Most People Overlook

Dementia stands for a major decline in cognitive powers, such as thinking, reasoning, judgment, or an inability to hold things in memory or to speak coherently, which hold sway for daily life.
These different types of dementia, whether Alzheimer’s disease or vascular dementia or Lewy body dementia, are earlier signs common to all.
It is a general term for a bunch of symptoms and not a specific disease that will impair the ability to remember, think, solve problems, and communicate.
It is very important to detect early signs of dementia in a person for immediate medical attention and future planning.
These types of knowledge will enable people and families to make the necessary effort in dealing with the diseased person.
Here are some early signs that you should watch for.
1. Memory Loss That Disrupts Daily Life
However, if the forgetfulness is not short but rather continues for a long time and brings disarray in everyday activities such as failing to remember important dates, asking the same question multiple times, or dependence on memory aids—this is food for concern: this memory loss is usually an early indicator of dementia.
Memory loss is usually a symptom of all types of dementia that can be controlled. Memory loss not only indicates memory loss of early learning but also sometimes forgetting things recently learned.
2. Difficulty in Planning or Solving Problems
First signs of memory problems causing people not to be able to do activities concerned with planning, organizing, or numbers.
For example, they would be unable to follow an otherwise familiar recipe or to keep up with the monthly bills. These problems lead up to a breakdown in normal routine and frustration.
3. Confusion with Time or Place
With regard to the warning signs, not being able to keep track of dates, seasons, or the happening of time is another.
Individuals can forget where they are or how they arrived there.
This type of confusion can continue to grow as the disease develops.
4. Trouble Understanding Visual and Spatial Relationships
Vision issues sometimes become the first sign of dementia. Reading, distance perception, and color differentiation might all be vastly improved or completely impaired in the daily actions of driving or navigating around known environments.
It is a very common symptom in Alzheimer's disease, the most common type of dementia. These visual problems constitute the initial symptoms suggesting dementia.
Difficulty in reading, distance judgment, and color contrast recognition may all be highly affected or completely absent in day-to-day actions like driving or navigating familiar environments.
This is a common symptom associated with Alzheimer's disease, the most common of all dementias.
5. Problems with Speaking or Writing
Cognitive decline is generally discernible when a person struggles to follow or join conversations.
Patients typically pause in between sentences, repeat phrases, and forget what word to use. Writing may now become more difficult with frequent mistakes and an obvious cutoff of coherence.
6. Misplacing Things and Losing the Ability to Retrace Steps
It's one thing to misplace your keys or glasses once in a while—you can be forgiven for that—but when things are continually put in strange places and not found, that's a real sign.
Gradually, you start accusing others of stealing things because you don't even remember what you did with it.
7. Poor Judgment or Decision-Making
When a person is suffering from dementia, their judgment and decision-making ability can be badly affected.
In an example, there will be people who usually donate quite a lot of money to telemarketers or do not care about their personal hygiene at all, among others.
Such lapses usually become more apparent to family members or caregivers.
8. Withdrawal from Work or Social Activities
When people stop taking pleasure in their favorite activities, avoid socializing, or do not want to get involved with their work, the signs of early dementia start appearing.
Hiding in public places and avoiding school or training sessions are also commonalities in such individuals.
9. Changes in Mood and Personality
Dementia causes dramatic changes in moods and personality. Someone who was once outgoing can suddenly become withdrawn or worse, irritable.
They may, on the alternate hand, exhibit signs of depression, anxiety, or even paranoia—all of which will come as a result of the inability to realize the individual's former self due to cognitive decline.
Humans with this illness, however, have been found to most likely experience emotional bouts—no matter how minor they may be, they are emotionally related to one's ability to cope with the ongoing changes due to cognitive deficits.
Why Early Detection Matters?
It is important to give timely medical evaluations upon recognition of early signs of dementia.
Although most types of dementia cannot be cured, symptomatic progression of the illness can be slowed down if treatment is commenced early and quality of life improved.
Treatment includes medications, cognitive therapies, and lifestyle changes like diet, exercise, and stimulation of the mind.
As with any other health conditions, researchers and caregivers would be very much interested in how dementia can be cured or treated.
It will also give time for the individual and family to plan the future. The decisions, made while the affected person can still participate in the process, may include care options, legal matters, and financial arrangements.
When to Seek Help?
If you or anyone suffers from such symptoms, visiting a healthcare professional would be your best chance of getting tested and diagnosed. Those who are doctors are knowledgeable enough to do those tests for cognitive changes and recommend interventions. While some of the caused cognitive disruptions may reflect dementia, not all memory issues translate to this state as some may include vitamin deficiency, thyroid problems, and stress.
So, if you or someone you know seems to be having those symptoms, it is better to consult a healthcare professional. Most of the time, doctors do tests that can find the source of cognitive changes and then recommend the appropriate interventions. Memory issues may not always involve dementia; some could be due to vitamin deficiencies, thyroid problems, or even stress. This highlights the importance of understanding how dementia is caused and how dementia is diagnosed.
Conclusion
Dementia can be a rather challenging condition, but recognizing the early signs of dementia can make a huge difference in managing the illness as well as sustaining a better quality of life.
Stay watchful and do not hesitate to consult best neuropsychiatrist in Patna Bihar when you notice something wrong with memory, thinking, or behavior over a period of time.
Early awareness is the first step toward better outcomes.
#DifferentTypesOfDementia#bestpsychiatristinkankarbaghpatna#EarlySignsOfDementia#HowDementiaCanBeCured
0 notes
Text
Viral pathogens increase risk of neurodegenerative disease - Published Mar 2, 2023
Neurodegenerative diseases, which include conditions such as Alzheimer disease (AD) Parkinson disease (PD), amyotrophic lateral sclerosis (ALS), vascular dementia and multiple sclerosis (MS), are a class of progressive disorders defined by neuronal death. Each of these disorders is characterized by degeneration of distinct brain areas, and they present with overlapping but discrete symptoms that can include motor impairment, cognitive dysfunction, affective changes and/or dementia. With the exception of rare familial cases, the aetiopathogenic origins of these diseases are poorly understood; however, two common factors seem to be neuroinflammation and epidemiological links to viral infections.
Neuroinflammation was originally thought to be a consequence of neurodegeneration; however, subsequent research indicated that neuroinflammation can drive the onset and progression of neurodegenerative diseases. The idea of neuroinflammation as a driver of neurodegeneration was advanced by genome-wide association studies (GWAS) that identified immune-related genes, including CD33 and TREM2, as risk factors for AD2. In addition, the ε4 allele of the apolipoprotein E gene (APOE ε4), which is the strongest known genetic risk factor for AD and accounts for approximately 10–20% of the risk of late-onset disease, has been hypothesized to exert its effects partially through neuroinflammatory processes. These genetic factors increase the risk of developing neurodegenerative disease but are not sufficient to cause disease on their own. Instead, genetic risk factors are likely to work with environmental factors that underlie sporadic forms of neurodegenerative disease.
Read the full article and find even more covid news, science, and advice at our archive:
#covid#wear a respirator#coronavirus#sars cov 2#mask up#public health#wear a mask#pandemic#covid 19#still coviding#covidー19#covid pandemic#covid conscious#covid is airborne#covid isn't over#long covid#the pandemic isn't over
5 notes
·
View notes
Text
Dementia Care: Delaying Progress and Supporting Families

In today’s fast-paced world, where mental health and well-being are gaining the attention they deserve, Dementia Care: Delaying Progress and Supporting Families has become a critical topic of discussion. Dementia is a progressive condition that affects millions of individuals and their families worldwide. As the prevalence of dementia continues to rise, the need for effective care strategies, educational resources, and support systems has never been more urgent. At Korshub, we are committed to providing high-quality online courses, including those focused on dementia care, to empower caregivers, families, and healthcare professionals with the knowledge and skills they need to navigate this challenging journey.
In this comprehensive blog, we will explore the importance of delaying the progression of dementia, the role of caregivers, and how families can find support through education and community resources. Whether you are a caregiver, a family member, or a healthcare professional, this guide will provide valuable insights into Dementia Care: Delaying Progress and Supporting Families.
Understanding Dementia: A Growing Global Concern
Dementia is an umbrella term used to describe a range of neurological disorders characterized by a decline in cognitive function, memory loss, and the inability to perform daily activities. Alzheimer’s disease is the most common form of dementia, accounting for 60-80% of cases. Other types include vascular dementia, Lewy body dementia, and frontotemporal dementia.
The World Health Organization (WHO) estimates that over 55 million people worldwide are living with dementia, and this number is expected to triple by 2050. This alarming statistic highlights the urgent need for effective dementia care strategies and support systems for families.
The Importance of Delaying the Progression of Dementia
While there is currently no cure for dementia, research has shown that certain interventions can help delay the progression of the disease. Early diagnosis, lifestyle modifications, and targeted therapies can significantly improve the quality of life for individuals with dementia and their families.
1. Early Diagnosis and Intervention
Early detection of dementia is crucial for implementing strategies to delay its progression. Cognitive assessments, brain imaging, and biomarker tests can help identify the condition in its initial stages. Early intervention allows for the implementation of personalized care plans, including medication, cognitive training, and lifestyle changes.
2. Lifestyle Modifications
Healthy lifestyle choices can play a significant role in delaying the progression of dementia. Regular physical exercise, a balanced diet rich in antioxidants and omega-3 fatty acids, and mental stimulation through activities like puzzles, reading, and social engagement can help maintain cognitive function.
3. Medication and Therapies
While medications cannot cure dementia, they can help manage symptoms and slow the progression of the disease. Cholinesterase inhibitors and memantine are commonly prescribed to improve cognitive function and manage behavioral symptoms. Additionally, non-pharmacological therapies such as music therapy, art therapy, and reminiscence therapy have shown promising results in enhancing the well-being of individuals with dementia.
The Role of Caregivers in Dementia Care
Caregivers play a pivotal role in the lives of individuals with dementia. Whether they are family members or professional caregivers, their support is essential for maintaining the dignity and quality of life of those affected by the condition.
1. Providing Emotional Support
Living with dementia can be incredibly isolating and frustrating. Caregivers must offer empathy, patience, and reassurance to help individuals cope with their condition. Creating a safe and nurturing environment can significantly reduce anxiety and agitation.
2. Managing Daily Activities
As dementia progresses, individuals may struggle with basic tasks such as dressing, eating, and bathing. Caregivers must adapt to the changing needs of their loved ones and provide assistance while encouraging independence whenever possible.
3. Navigating Behavioral Changes
Dementia often leads to behavioral changes such as aggression, wandering, and sleep disturbances. Caregivers must develop strategies to manage these challenges, including maintaining a consistent routine, using calming techniques, and seeking professional guidance when necessary.
Supporting Families Through Education and Community Resources
Caring for a loved one with dementia can be emotionally and physically exhausting. Families often face financial strain, social isolation, and a lack of knowledge about how to provide effective care. At Korshub, we believe that education is the key to empowering families and caregivers.
1. Online Courses on Dementia Care
Our platform offers a wide range of online courses, similar to those found on Udemy, that focus on Dementia Care: Delaying Progress and Supporting Families. These courses cover topics such as understanding dementia, managing symptoms, and providing emotional support. By equipping families with the knowledge they need, we aim to reduce the burden of caregiving and improve outcomes for individuals with dementia.
2. Support Groups and Counseling
Connecting with others who are going through similar experiences can provide immense comfort and practical advice. Support groups, both online and in-person, offer a safe space for families to share their struggles, seek guidance, and build a sense of community. Professional counseling can also help caregivers cope with stress, grief, and burnout.
3. Respite Care Services
Caregivers often neglect their own well-being while focusing on their loved ones. Respite care services provide temporary relief by offering professional care for individuals with dementia, allowing caregivers to rest and recharge.
Practical Tips for Families and Caregivers
Here are some actionable tips to help families and caregivers provide effective dementia care:
Educate Yourself: Take advantage of online courses and resources to learn about dementia and caregiving techniques.
Create a Safe Environment: Remove hazards, install safety devices, and use labels to help individuals with dementia navigate their surroundings.
Communicate Effectively: Use simple language, maintain eye contact, and be patient when communicating with someone who has dementia.
Encourage Social Interaction: Engage your loved one in social activities to reduce feelings of isolation and improve their mood.
Take Care of Yourself: Prioritize your physical and mental health to avoid caregiver burnout.
Conclusion: Empowering Families Through Knowledge and Support
Dementia Care: Delaying Progress and Supporting Families is a multifaceted approach that requires compassion, education, and collaboration. By understanding the importance of early intervention, adopting healthy lifestyle changes, and leveraging community resources, families can provide the best possible care for their loved ones.
At Korshub, we are dedicated to supporting families and caregivers through our comprehensive online courses. Whether you are looking to enhance your caregiving skills or simply seeking guidance, our platform offers the tools you need to navigate the challenges of dementia care.
Together, we can make a difference in the lives of those affected by dementia. Let’s work towards a future where delaying the progression of dementia and supporting families becomes a shared priority.
0 notes
Text
Up to 4 in 10 people could develop dementia after 55. What you can do to lower your risk

WASHINGTON (AP) — About a million Americans a year are expected to develop dementia by 2060, roughly double today’s toll, researchers reported Monday.
That estimate is based on a new study that found a higher lifetime risk than previously thought: After age 55, people have up to a 4 in 10 chance of eventually developing dementia -- if they live long enough.
It’s a sobering number but there are steps people can take to reduce that risk, such as controlling high blood pressure and other bad-for-the-brain health problems. And it’s not too late to try even in middle age.
“All of our research suggests what you do in midlife really matters,” said Dr. Josef Coresh of NYU Langone Health, who coauthored the study in the journal Nature Medicine.
Dementia isn’t only Alzheimer’s
Taking longer to recall a name or where you put your keys is typical with older age. But dementia isn’t a normal part of aging -- it’s a progressive loss of memory, language and other cognitive functions. Simply getting older is the biggest risk and the population is rapidly aging.
Alzheimer’s is the most common form, and silent brain changes that eventually lead to it can begin two decades before symptoms appear. Other types include vascular dementia, when heart disease or small strokes impair blood flow to the brain. Many people have mixed causes, meaning vascular problems could exacerbate brewing Alzheimer’s symptoms.
...
Dementia risk is different by age
Prior studies estimated about 14% of men and 23% of women would develop some form of dementia during their lifetime. Coresh’s team analyzed more recent data from a U.S. study that has tracked the heart health and cognitive function of about 15,000 older adults for several decades.
Importantly, they found the risk changes with the decades.
Only 4% of people developed dementia between the ages of 55 and 75, what Coresh calls a key 20-year window for protecting brain health.
For people who survive common health threats until 75, the dementia risk then jumped — to 20% by age 85 and 42% between ages 85 and 95.
Overall, the lifetime dementia risk after age 55 was 35% for men and 48% for women, the researchers concluded. Women generally live longer than men, a main reason for that difference, Coresh noted. Black Americans had a slightly higher risk, 44%, than white people at 41%.
1 note
·
View note
Text
Comprehensive Guide to Dementia Care in Sugarland
Dementia is a complex condition that affects millions of individuals worldwide, including many in Sugarland, Texas. As the condition progresses, it becomes essential to ensure that individuals living with dementia receive the proper care and support they need to maintain a quality life. Sugarland offers a variety of resources, services, and facilities that cater specifically to those with dementia. This guide explores the key aspects of dementia care available in the region.
Understanding Dementia
Dementia is not a single disease but a term that encompasses a range of symptoms associated with cognitive decline. Alzheimer’s disease is the most common form, but other types include vascular dementia, Lewy body dementia, and frontotemporal dementia. Symptoms often include memory loss, difficulty in communication, impaired reasoning, and changes in behavior. Providing care for someone with dementia requires patience, empathy, and specialized knowledge.
Conclusion
Dementia care in Sugarland is built on a foundation of compassion, expertise, and community support. Whether you are seeking professional services or simply looking for guidance as a caregiver, the city offers an array of options to help individuals with dementia lead fulfilling lives. By leveraging these resources and fostering a supportive environment, we can make a meaningful difference in the lives of those affected by this challenging condition.
0 notes