#Swine Flu Vaccination Research Report
Text
Swine flu caught scientists by surprise. At the time, many researchers were dead certain that an H5N1, erupting out of somewhere in Asia, would be the next Big Bad Flu. Their focus was on birds; hardly anyone was watching the pigs. But the virus, a descendant of the devastating flu strain that caused the 1918 pandemic, found its way into swine and rapidly gained the ability to hack into human airway cells. It was also great at traveling airborne—features that made it well positioned to wreak global havoc, Lakdawala said. By the time experts caught on to swine flu’s true threat, “we were already seeing a ton of human cases,” Nahid Bhadelia, the founding director of the Boston University Center on Emerging Infectious Diseases, told me. Researchers had to scramble to catch up. But testing was intermittent, and reporting of cases was inconsistent, making it difficult for scientists to get a handle on the virus’s spread. Months passed before the rollout of a new vaccine began, and uptake was meager. Even in well-resourced countries such as the U.S., few protections hindered the virus’s initial onslaught.
But the worst never came to pass—for reasons that experts still don’t understand. Certainly, compared with the 1918 pandemic, or even those in the 1950s and ’60s, modern medicine was better equipped to test for and treat flu; although vaccine uptake has never been perfect, the availability of any shots increased protection overall, Sam Scarpino, an infectious-disease modeler and the director of AI and life sciences at Northeastern University, told me. Subtler effects may have played a role too. Other H1N1 viruses had been circulating globally since the late 1970s, potentially affording much of the population a degree of immunity, Troy Sutton, a virologist at Pennsylvania State University, told me. Older people, especially, may have harbored an extra dose of defense, from additional exposure to H1N1 strains from the first half of the 20th century. (After the 1918 pandemic, versions of that virus stuck around, and continued to percolate through the population for decades.) Those bonus safeguards might help explain why younger people were so severely affected in 2009, Lakdawala told me.
Some of those same factors could end up playing a role in an H5N1 epidemic. But 2009 represents an imperfect template—especially when so much about this new avian flu remains unclear. True human-to-human spread of H5N1 is still a distant possibility: For that, the virus would almost certainly need to undergo some major evolutionary alterationsto its genome, potentially even transforming into something almost unrecognizable. All of this muddies any predictions about how a future outbreak might unfold.
(x)
10 notes
·
View notes
Text
Here we are, heading into another COVID winter. The fucker’s still here and sadly we aren’t likely to get rid of it any time soon. You kill diseases by cutting off transmission and slowly strangling them to death. We tried that. We locked down the whole world and it didn’t work.
I won’t deny that things look really ugly right now, especially with other respiratory diseases coming back. But as the sequencing results keep coming in, it’s really starting to look like something incredible happened.
Sure, the lockdowns didn’t succeed in killing COVID. That doesn’t mean they killed nothing.
Hey, I wonder how the influenza viruses are holding up?
There are two types of influenza that cause the epidemics we get every winter: A and B. (C and D don’t really get up to the same level of mischief so let’s ignore them for now.) Type A infects both animals and people, and includes things like the H1N1 bird flu pandemic strain, swine flu, et al. The H[number]N[number] format points out which subtype of two important viral proteins it has, and usually strains are reported with that code, what animal they jumped into humans from, and where they were first sequenced. Type B only affects humans, especially children. It doesn’t have subtypes like Type A. Instead it has two distinct lineages: B/Victoria and B/Yamagata.
Today’s best flu vaccines are called “quadrivalent” because they target B/Victoria, B/Yamagata, and our best guess at which two Type A’s are going to blow up this year. The guess is based on global sequencing of flu infections, so we have at least a decent idea of both past and current circulation logged in databases like GISAID and the WHO’s FluNet.
Cases went way down during the lockdowns - masking and social distancing pushed spread down to a fraction of what it usually is. Influenza in general is now back in force as people go back to their normal behavior. There’s plenty of Type A flying around. There’s been B/Victoria.
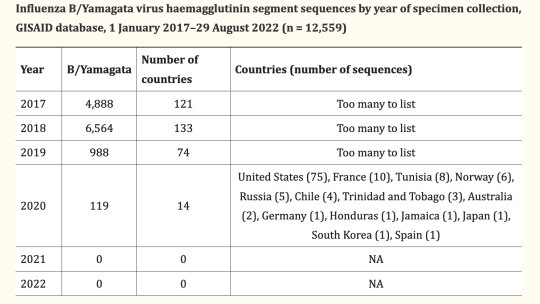
B/Yamagata has not been conclusively identified since March of 2020.
As early as 2021, flu researchers noticed the lack of new B/Yamagata sequences coming in and started to suspect something was fishy. Look at this graph of GISAID flu data by lineage:

[GISAID] [paper]
Let’s, uh, check FluNet maybe? That shows that in a typical year you see tens of thousands of cases of B/Yamagata on PCR tests. 2017 had 30,552; 2018 had 51,524. Then... 3,464 in 2019. 364 in 2020 in only 9 countries. It does seem like there are still signs of life in 2021 with 8 hits, but keep in mind these detections are based on simple PCR tests like what we do for COVID. PCR tests are exquisitely sensitive, to the point where it’s been shown that giving flu vaccines and then later using the same room to give flu tests can throw a weak positive by picking up viral RNA from the vaccine. More specifically, as of March 2022 there’s been a case of this exact thing happening with what looked like a B/Yamagata detection. So it’s going to be more reliable to look at only the results from full sequencing, where you can yeet anything that matches the vaccine ingredients and only look at wild viruses.
[paper]
Zero. Nothing. All signs point to we shot at COVID and blew up an entire flu lineage as collateral damage! What the fuck! We’re probably going to have to change how we do flu vaccines because fully a quarter of what they aim at looks to be gone from the face of the earth!
True, influenza B/Yamagata could still be out there somewhere that hasn’t been sequenced. Proving absence is hard. But the fact that Type A and its sibling B/Victoria are back and easy to find really does suggest it’s gone, or stomped down so far it’s near impossible to find. Time to watch and wait and feed every sample we can into the sequencers, but if we keep not finding it...
A disease is considered eradicated when we’re sure there’s no more transmission “in the wild”. For smallpox, which was also wildly contagious and also had no nonhuman reservoir, that was three years from the last known case.
Clock’s ticking.
#biology#flu#influenza#virus#medicine#if covid weren't so insanely contagious we 100% would have killed it
14 notes
·
View notes
Text
H1N1 (Swine Flu) Vaccination Market : Trends and Future Growth Analysis by 2031

The "H1N1 (Swine Flu) Vaccination Market" is a dynamic and rapidly evolving sector, with significant advancements and growth anticipated by 2031. Comprehensive market research reveals a detailed analysis of market size, share, and trends, providing valuable insights into its expansion. This report delves into segmentation and definition, offering a clear understanding of market components and drivers. Employing SWOT and PESTEL analyses, the study evaluates the market's strengths, weaknesses, opportunities, and threats, alongside political, economic, social, technological, environmental, and legal factors. Expert opinions and recent developments highlight the geographical distribution and forecast the market's trajectory, ensuring a robust foundation for strategic planning and investment.
What is the projected market size & growth rate of the H1N1 (Swine Flu) Vaccination Market?
Market Analysis and Size
The H1N1 flu, sometimes also known as swine flu, is a type of influenza A virus. It was often known as swine flu and was a new combination of influenza viruses that infect pigs, birds and humans. There have been severe cases of influenza in recent times. As per the World Health Organization (WHO), annually, around 3 to 5 million cases of severe illness and approximately 2,90,000 to 6,50,000 respiratory deaths are because of seasonal influenza. Also, increasing levels of respiratory ailments and immune deficient ailments due to the increasing elderly population has further caused huge growth opportunities for the H1N1 (swine flu) vaccination market.
Data Bridge Market Research analyses that the H1N1 (swine flu) vaccination market, which was USD 13.29 billion in 2022, would rise to USD 21.51 billion by 2030 and is expected to undergo a CAGR of 6.20% during the forecast period 2023 to 2030. In addition to the insights on market scenarios such as market value, growth rate, segmentation, geographical coverage, and major players, the market reports curated by the Data Bridge Market Research also include depth expert analysis, patient epidemiology, pipeline analysis, pricing analysis, and regulatory framework.
Browse Detailed TOC, Tables and Figures with Charts which is spread across 350 Pages that provides exclusive data, information, vital statistics, trends, and competitive landscape details in this niche sector.
This research report is the result of an extensive primary and secondary research effort into the H1N1 (Swine Flu) Vaccination market. It provides a thorough overview of the market's current and future objectives, along with a competitive analysis of the industry, broken down by application, type and regional trends. It also provides a dashboard overview of the past and present performance of leading companies. A variety of methodologies and analyses are used in the research to ensure accurate and comprehensive information about the H1N1 (Swine Flu) Vaccination Market.
Get a Sample PDF of Report - https://www.databridgemarketresearch.com/request-a-sample/?dbmr=global-h1n1-swine-flu-vaccination-market
Which are the driving factors of the H1N1 (Swine Flu) Vaccination market?
The driving factors of the H1N1 (Swine Flu) Vaccination market include technological advancements that enhance product efficiency and user experience, increasing consumer demand driven by changing lifestyle preferences, and favorable government regulations and policies that support market growth. Additionally, rising investment in research and development and the expanding application scope of H1N1 (Swine Flu) Vaccination across various industries further propel market expansion.
H1N1 (Swine Flu) Vaccination Market - Competitive and Segmentation Analysis:
Global H1N1 (Swine Flu) Vaccination Market, By Vaccine Type (Intranasal, Conjugate, Attenuated Vaccines, Inactivated Vaccines, Intramuscular, and Toxoid), Type of Brand (Agripal, Fiuarix, Influgen, Influvac, Nasovac, Vaxigrip, and Others) and End User (Hospitals, Clinics, and Others) – Industry Trends and Forecast to 2031.
How do you determine the list of the key players included in the report?
With the aim of clearly revealing the competitive situation of the industry, we concretely analyze not only the leading enterprises that have a voice on a global scale, but also the regional small and medium-sized companies that play key roles and have plenty of potential growth.
Which are the top companies operating in the H1N1 (Swine Flu) Vaccination market?
Some of the major players operating in the H1N1 (swine flu) vaccination market are:
Sanofi (France)
Pfizer Inc. (U.S.)
GSK plc (U.K.)
Novartis AG (Switzerland)
Mylan N.V. (U.S.)
Baxter.(U.S.)
AstraZeneca (U.K.)
Johnson & Johnson Private Limited (U.S.)
Virbac (France)
Vetoquinol (France)
Zoetis (U.S.)
Novavax (U.S.).
Zydus Group (India).
Panacea Biotec (India).
SINOVAC (China).
Abbott (U.S.)
SEQIRUS (U.S.)
Cipla Inc (India)
Short Description About H1N1 (Swine Flu) Vaccination Market:
The Global H1N1 (Swine Flu) Vaccination market is anticipated to rise at a considerable rate during the forecast period, between 2024 and 2031. In 2023, the market is growing at a steady rate and with the rising adoption of strategies by key players, the market is expected to rise over the projected horizon.
North America, especially The United States, will still play an important role which can not be ignored. Any changes from United States might affect the development trend of H1N1 (Swine Flu) Vaccination. The market in North America is expected to grow considerably during the forecast period. The high adoption of advanced technology and the presence of large players in this region are likely to create ample growth opportunities for the market.
Europe also play important roles in global market, with a magnificent growth in CAGR During the Forecast period 2024-2031.
H1N1 (Swine Flu) Vaccination Market size is projected to reach Multimillion USD by 2031, In comparison to 2024, at unexpected CAGR during 2024-2031.
Despite the presence of intense competition, due to the global recovery trend is clear, investors are still optimistic about this area, and it will still be more new investments entering the field in the future.
This report focuses on the H1N1 (Swine Flu) Vaccination in global market, especially in North America, Europe and Asia-Pacific, South America, Middle East and Africa. This report categorizes the market based on manufacturers, regions, type and application.
Get a Sample Copy of the H1N1 (Swine Flu) Vaccination Report 2024
What are your main data sources?
Both Primary and Secondary data sources are being used while compiling the report. Primary sources include extensive interviews of key opinion leaders and industry experts (such as experienced front-line staff, directors, CEOs, and marketing executives), downstream distributors, as well as end-users. Secondary sources include the research of the annual and financial reports of the top companies, public files, new journals, etc. We also cooperate with some third-party databases.
Geographically, the detailed analysis of consumption, revenue, market share and growth rate, historical data and forecast (2024-2031) of the following regions are covered in Chapters
What are the key regions in the global H1N1 (Swine Flu) Vaccination market?
North America (United States, Canada and Mexico)
Europe (Germany, UK, France, Italy, Russia and Turkey etc.)
Asia-Pacific (China, Japan, Korea, India, Australia, Indonesia, Thailand, Philippines, Malaysia and Vietnam)
South America (Brazil, Argentina, Columbia etc.)
Middle East and Africa (Saudi Arabia, UAE, Egypt, Nigeria and South Africa)
This H1N1 (Swine Flu) Vaccination Market Research/Analysis Report Contains Answers to your following Questions
What are the global trends in the H1N1 (Swine Flu) Vaccination market?
Would the market witness an increase or decline in the demand in the coming years?
What is the estimated demand for different types of products in H1N1 (Swine Flu) Vaccination?
What are the upcoming industry applications and trends for H1N1 (Swine Flu) Vaccination market?
What Are Projections of Global H1N1 (Swine Flu) Vaccination Industry Considering Capacity, Production and Production Value? What Will Be the Estimation of Cost and Profit? What Will Be Market Share, Supply and Consumption? What about Import and Export?
Where will the strategic developments take the industry in the mid to long-term?
What are the factors contributing to the final price of H1N1 (Swine Flu) Vaccination?
What are the raw materials used for H1N1 (Swine Flu) Vaccination manufacturing?
How big is the opportunity for the H1N1 (Swine Flu) Vaccination market?
How will the increasing adoption of H1N1 (Swine Flu) Vaccination for mining impact the growth rate of the overall market?
How much is the global H1N1 (Swine Flu) Vaccination market worth? What was the value of the market In 2020?
Who are the major players operating in the H1N1 (Swine Flu) Vaccination market? Which companies are the front runners?
Which are the recent industry trends that can be implemented to generate additional revenue streams?
What Should Be Entry Strategies, Countermeasures to Economic Impact, and Marketing Channels for H1N1 (Swine Flu) Vaccination Industry?
Customization of the Report
Can I modify the scope of the report and customize it to suit my requirements? Yes. Customized requirements of multi-dimensional, deep-level and high-quality can help our customers precisely grasp market opportunities, effortlessly confront market challenges, properly formulate market strategies and act promptly, thus to win them sufficient time and space for market competition.
Inquire more and share questions if any before the purchase on this report at - https://www.databridgemarketresearch.com/inquire-before-buying/?dbmr=global-h1n1-swine-flu-vaccination-market
Detailed TOC of Global H1N1 (Swine Flu) Vaccination Market Insights and Forecast to 2031
Introduction
Market Segmentation
Executive Summary
Premium Insights
Market Overview
H1N1 (Swine Flu) Vaccination Market By Type
H1N1 (Swine Flu) Vaccination Market By Function
H1N1 (Swine Flu) Vaccination Market By Material
H1N1 (Swine Flu) Vaccination Market By End User
H1N1 (Swine Flu) Vaccination Market By Region
H1N1 (Swine Flu) Vaccination Market: Company Landscape
SWOT Analysis
Company Profiles
Continued...
Purchase this report – https://www.databridgemarketresearch.com/checkout/buy/singleuser/global-h1n1-swine-flu-vaccination-market
Data Bridge Market Research:
Today's trends are a great way to predict future events!
Data Bridge Market Research is a market research and consulting company that stands out for its innovative and distinctive approach, as well as its unmatched resilience and integrated methods. We are dedicated to identifying the best market opportunities, and providing insightful information that will help your business thrive in the marketplace. Data Bridge offers tailored solutions to complex business challenges. This facilitates a smooth decision-making process. Data Bridge was founded in Pune in 2015. It is the product of deep wisdom and experience.
Contact Us:
Data Bridge Market Research
US: +1 614 591 3140
UK: +44 845 154 9652
APAC: +653 1251 975
Email:- [email protected]
Browse More Reports:
Global Precision Farming Software Market – Industry Trends and Forecast to 2030
Global Oligosaccharides in Infant Nutrition Market – Industry Trends and Forecast to 2029
Global H1N1 (Swine Flu) Vaccination Market – Industry Trends and Forecast to 2030
Global Airbag Inflator Market - Industry Trends and Forecast to 2028
Global Veterinary Anti-Infective Market – Industry Trends and Forecast to 2029
#H1N1 (Swine Flu) Vaccination Market#H1N1 (Swine Flu) Vaccination Market Size#H1N1 (Swine Flu) Vaccination Market Share#H1N1 (Swine Flu) Vaccination Market Trends
0 notes
Text
Animal Health Vaccine Market Future Trends to Look Out | Bis Research

Animal health vaccines are biological preparations used to stimulate an animal's immune system to recognize and combat specific infectious agents, such as bacteria, viruses, or parasites.
These vaccines are designed to prevent diseases by inducing an immune response that mimics the natural infection, thereby providing immunity without causing the disease itself.
In 2022, the global Veterinary Vaccines market held a value of $9.44 billion. The market is expected to grow at a CAGR of 7.30% during the forecast period 2023-2033 and attain a value of $19.86 billion by 2033.
Grab a look at our report page click here !
Animal Vaccines Overview
Animal health vaccines are essential biological preparations designed to enhance the immune system of animals, enabling them to resist specific infectious agents such as bacteria, viruses, and parasites.
Key Components of Animal Health Vaccines
Antigens
Adjuvants
Stabilizers and Preservatives
Benefits of Animal Health Vaccines
Disease Prevention
Economic Benefits
Improved Animal Welfare
Distribution and Storage
Grab a look at our sample page click here
Rising Demand for Animal Health Vaccines
Increased Livestock Production
Emerging Infectious Diseases
Zoonotic Disease Prevention
Global Trade and Animal Movement
Market Segmentation
1 ) By Type
Livestock Vaccines
Bovine Vaccines
Small Ruminant Vaccines
Porcine Vaccines
Poultry Vaccines
Companion Animal Vaccines s
Canine Vaccines
Feline Vaccines
Equine Vaccines
(e) Aquaculture Vaccines
2) By Disease
Swine Fever
Foot and Mouth Disease
Newcastle Disease
Avian Influenza (Bird Flu)
Peste des Petits Ruminants
Other Diseases
3) By Technology
Live Attenuated Vaccines
Inactivated Vaccines
Toxoid Vaccines
Recombinant Vaccines
Conjugate Vaccines
Other Vaccines
4) By Route of Administration
Injectable Vaccines
Oral Vaccines
Intranasal/Spray Vaccines
5) By Distribution Channel
Veterinary Hospitals
Veterinary Clinics
Retail Pharmacies
Veterinary Research Institutes
6) By Region
North America
Europe
Asia Pacific
Middle East and Africa
Latin America
Key Players in the Market
Boehringer Ingelheim International GmbH
Ceva Santé Animale
Elanco Animal Health Incorporated
Merck & Co., Inc. (Merck Animal Health)
Zoetis, Inc.
Phibro Animal Health Corporation
Virbac
And many others
Visit our Life Sciences and Biopharma page click here !
Types of Animal Health Vaccines
Live Attenuated Vaccines
Inactivated Vaccines
Recombinant Vaccines
Vectored Vaccines
Conjugate Vaccines
DNA Vaccines
Major Trends and Drivers included are as follows
Rising demand for animal proteins
Emerging and Re-emerging diseases
Antibiotic Resistant Concerns
Increased Pet Ownership
Focus on Sustainability
Focus on One Health Approach
Key Question Answers
Q What are the major market drivers, restraints, and opportunities within the global Animal Vaccines market?
Q What are the major trends adopted by the global Animal Vaccines market?
Q What are the key strategies adopted by key players in the global Animal Vaccines market?
Q How is each type segment of the global Animal Vaccines market expected to grow during the forecast period 2023-2033?
Q How is each disease segment of the global Animal Vaccines market expected to grow during the forecast period 2023-2033?
Conclusion
In conclusion, animal health vaccines play a pivotal role in the advancement of veterinary medicine, significantly enhancing the welfare of both domestic and wild animal populations. These vaccines provide a robust defense against a myriad of infectious diseases, thereby reducing morbidity and mortality rates.
0 notes
Text
0 notes

Text
Dr. Peter McCullough: The State of COVID Treatment
Story at-a-glance
Cardiologist, internist and epidemiologist Dr. Peter McCullough discusses why a key aspect of care — early treatment — has been missing from the pandemic
With no hope of early treatment, McCullough believes that most people became conditioned to wait for an injection
COVID-19 injections are waning in effectiveness and linked to an unacceptable number of serious injuries and deaths
McCullough is among a growing number of experts who believe COVID-19 injections are making the pandemic worse; indiscriminate vaccination is driving mutations, as the virus is mutating wildly to evade the injections
At 53:40 in the video, you can view McCullough’s early treatment regimen, which initially includes a nutraceutical bundle, progressing to monoclonal antibody therapy, anti-infectives like HCQ or ivermectin, antibiotics, steroids and blood thinners
The video above,1 featuring cardiologist, internist and epidemiologist Dr. Peter McCullough, is packed with sound logic, data and action steps that have the potential to turn the pandemic around — if only more people would listen.Recorded at the Andrews University Village Church in Berrien Springs, Michigan, August 20, 2021, this presentation deserves to be heard, and I urge you to listen to it in its entirety. It will make you question why a key aspect of care — early treatment — has been missing from the pandemic.McCullough, editor of two medical journals who has published 650 peer-reviewed papers, said this has been the first time in his career when he saw medical providers not offering early treatment for a disease.Early COVID Treatment Saves Lives
The standard of care for COVID-19 has been to withhold treatment until a person is sick enough to be hospitalized. It typically takes two to three weeks for someone with COVID-19 to get sick enough to be hospitalized, and during that time early treatment can be lifesaving.The rationale was that there have been no large, randomized trials conducted to know which treatments are safe and effective, but as McCullough said, "We can't wait for large randomized trials … Something got in the minds of doctors and nurses and everyone to not treat COVID-19. I couldn't stand it." He and colleagues worked feverishly to figure out a treatment — why didn't national health organizations do so also?"Our government and other governments, and the entire world, has not lifted a finger to reduce the risk of hospitalization and death anywhere," McCullough said, pointing out the irony: "If there was a kid with asthma, would we let the kid wheeze and choke for two weeks before the kid has to go to the hospital? No, we give the child medications. We don't have randomized trials for every single thing that we do."2
McCullough and colleagues realized that there are three major phases to COVID-19. It starts with virus replication, which then triggers inflammation, or a cytokine storm. This, in turn, leads to blood clotting. If enough micro blood clots form in the lungs, a person can't get enough oxygen and dies. It's a complex process, and no single drug is going to work to treat it, which is why McCullough uses a combination of drugs, as is done to treat HIV, staph and other infections.Only about 6% of doctors' decisions in cardiology are based on randomized trials. "Medicine is an art and a science, it takes judgment. What was happening is, I think out of global fear, no judgement was happening," McCullough said,3 referring to doctors' refusal to treat COVID-19 patients early on in the disease process.Doctors Threatened for Treating COVID-19
Around the world, the unthinkable is happening: Doctors are being threatened with loss of their license or even prison for trying to help their patients. French doctor Didier Raoult suggested, early on, putting up a tent to try to treat covid-19 patients. He was put on house arrest. He has promoted the use of hydroxychloroquine (HCQ), which initially was available over the counter — until France made it prescription only.4In Australia, if a doctor attempts to treat a COVID-19 patient with HCQ, they could be put in prison. "Since when does a doctor get put in prison to try to help a patient with a simple generic drug?" McCullough said. In South Africa, he added, a doctor was put in prison for prescribing ivermectin.In August 2020, McCullough's landmark paper "Pathophysiological Basis and Rationale for Early Outpatient Treatment of SARS-CoV-2 Infection" was published online in the American Journal of Medicine.5The follow-up paper is titled "Multifaceted Highly Targeted Sequential Multidrug Treatment of Early Ambulatory High-Risk SARS-CoV-2 Infection (COVID-19)" and was published in Reviews in Cardiovascular Medicine in December 2020.6 It became the basis for the home treatment guide.While some physician organizations have stepped up and are treating COVID-19 patients, "The ivory tower today still is not treating
patients. The party line in my health system is, do not treat a COVID-19 patient as an outpatient. Wait for them to get sick enough to be admitted. Because my health system … follows the National Institutes of Health or the Centers for Disease Control, period."
Conditioned to Wait for an Injection
With no hope of early treatment, McCullough believes that most people became conditioned to wait for an injection. "We became conditioned, after about May or so, to wear a mask, wait in isolation and be saved by the vaccine. And wait for the vaccine. And all we could hear about is the vaccine."The injections were developed, but they're different than any prior vaccines and have been losing effectiveness while causing an unacceptable number of serious injuries and deaths. For comparison, in 1976, a fast-tracked injection program against swine flu was halted after an estimated 25 to 32 deaths.7According to McCullough in the video, if a new drug comes on the market and five deaths occur, the standard is to issue a black box warning stating the medication may cause death. With 50 deaths, the product is pulled from the market, he says. Now consider this: The Vaccine Adverse Event Reporting System (VAERS) database showed that — for all vaccines combined before 2020 — there were about 158 total deaths reported per year.By January 22, 2021, there were already 182 deaths reported for COVID-19 injections, with just 27.1 million people vaccinated. This was more than enough to reach the mortality signal of concern to stop the program, McCullough said."We've already crossed the line of concern January 22. And if there was a data safety monitoring board — I know, because I do this work — we would have had an emergency meeting and said, wait a minute, people are dying after the vaccine. We've got to figure out why."8It's standard to have an external critical event committee, an external data safety monitoring board and a human ethics committee for large clinical trials — such as the mass COVID-19 injection program, but these were not put into place."This is something we've never seen in human medicine — a new product introduced and just going full-steam ahead with no check on why people are dying after the vaccine," McCullough said. On two occasions, the CDC and FDA — in March and in June — reviewed the data and said none of the deaths are related to the vaccines. "I think this is malfeasance," he stated.Fast-forward to July 30, 2021, and VAERS data showed 12,366 Americans have died after a COVID0-19 injection.9 In an analysis of COVID-19 vaccine death reports from VAERS, researchers found that 86% of the time, nothing else could have caused the death, and it appears the vaccine was the cause.10The Spike Protein Is Dangerous
Your body recognizes the spike protein in COVID-19 jabs as foreign, so it begins to manufacture antibodies to protect you against COVID-19, or so the theory goes. But there's a problem. The spike protein itself is dangerous and known to circulate in your body at least for weeks and more likely months11 — perhaps much longer — after the COVID jab.In your cells, the spike protein damages blood vessels and can lead to the development of blood clots.12 It can go into your brain, adrenal glands, ovaries, heart, skeletal muscles and nerves, causing inflammation, scarring and damage in organs over time. McCullough also believes that the spike protein is present in donated blood, and they've notified the Red Cross and the American Association of Blood Banking.Messenger RNA (mRNA) platforms have been under study for years, in most cases being designed to replace a defective gene, which could potentially be used for cancer or heart failure treatment, for example.In November 2020, however, Pfizer, in a joint venture with Germany-based BioNTech, announced that their mRNA-based injection was "more than 90% effective" in a Phase 3 trial.13 This does not mean that 90% of people who get injected will be protected from COVID-19, as it's based on relative risk reduction (RRR).The absolute
risk reduction (ARR) for the jab is less than 1%. "Although the RRR considers only participants who could benefit from the jab, the absolute risk reduction (ARR), which is the difference between attack rates with and without a jab, considers the whole population. ARRs tend to be ignored because they give a much less impressive effect size than RRRs," researchers wrote in The Lancet Microbe in April 2021.14McCullough believes the mass injection campaign is an incredible violation of human ethics, in part because no one should be pressured, coerced or threatened into using an investigational product.No attempts have been made to present or mitigate risks to the public, such as giving it only to people who really need it — not to low risk groups like children and young people and those who are naturally immune to COVID-19 due to prior infection. "I think this is the most disturbing thing," he said.The Injections Don't Stop COVID-19, Can Be Deadly
The CDC's Morbidity and Mortality Weekly Report (MMWR) posted online July 30, 2021, details an outbreak of COVID-19 that occurred in Barnstable County, Massachusetts — 74% of the cases occurred in fully vaccinated people.15Indiscriminate vaccination is driving mutations, as the virus is mutating wildly to evade the injections. Their effectiveness, too, is rapidly waning. A study published in medRxiv, using data from the Mayo Clinic Health System, revealed that during periods of Alpha and Delta variant prevalence, Moderna's injection was 76% effective while Pfizer's effectiveness was only 42%.16A little-known fact is that Moderna's jab has three times the dose of Pfizer's, but, curiously, health officials aren't even discussing this or giving the public updates on which of the three injections work "best." The narrative is simple and straightforward — get an injection, any injection.Yet, as McCullough noted, the virus has mutated, and the vaccines aren't working the way health officials had hoped: "The vaccines don't stop COVID-19, at least not completely, and they're not a shield against mortality."17Similar to VAERS, the U.K. maintains a "Yellow Card" reporting site to report adverse effects to vaccines and medications.18Tess Lawrie, whose company The Evidence-Based Medicine Consultancy has worked with the World Health Organization, analyzed U.K. Yellow Card data and concluded that there's more than enough evidence to pull the injections from the market because they're not safe for human use. The report stated:19"It is now apparent that these products in the blood stream are toxic to humans. An immediate halt to the vaccination programme is required whilst a full and independent safety analysis is undertaken to investigate the full extent of the harms, which the UK Yellow Card data suggest include thromboembolism, multisystem inflammatory disease, immune suppression, autoimmunity and anaphylaxis, as well as Antibody Dependent Enhancement (ADE)."Early Treatment Is Crucial
McCullough is trying to get the word out about the importance of early treatment of COVID-19. Early ambulatory therapy with a sequenced-multidrug regimen is supported by available sources of evidence and has a positive benefit-to-risk profile to reduce the risk of hospitalization and death.At 53:40 in the video, you can view McCullough's early treatment regimen, which initially includes a nutraceutical bundle. While you're recovering at home, open your windows and get plenty of fresh air and ventilation in your home.If symptoms persist or worsen, he recommends calling your doctor and demanding monoclonal antibody therapy. The treatment progresses to include anti-infectives like HCQ or ivermectin, antibiotics, steroids and blood thinners.If your doctor refuses to treat COVID-19 in the early stages, find a new one and/or visit a telemedicine clinic that will help, as "the prehospital phase is the time of therapeutic opportunity."📷McCullough is among a growing number of experts who believe COVID-19 injections are making the pandemic worse. They "have an unfavorable
safety profile and are not clinically effective, thus they cannot be generally supported in clinical practice at this time."Logically, this is clear, but McCullough believes we're dealing with a mass psychosis that is preventing people from seeing the light. "The whole world is in a trance," he said, adding:20"Things are getting disturbingly out of control and it's in the context of the virus. It is clear … we are in a very special time in the history of mankind. Whatever is going on, it is the entire world … every human being in the world. It appears to have a program.The program … is happening to promote as much fear, isolation, suffering, hospitalization and death in order to get a needle in every arm, at all costs. That is what's going on, and no one in this room can disagree."
1 note
·
View note
Text
No, Science Clearly Shows That COVID-19 Wasn’t Leaked From A Wuhan Lab
https://sciencespies.com/news/no-science-clearly-shows-that-covid-19-wasnt-leaked-from-a-wuhan-lab/
No, Science Clearly Shows That COVID-19 Wasn’t Leaked From A Wuhan Lab

Starting in late 2019, a novel strain of coronavirus, SARS-CoV-2, began infecting human beings for the very first time. Discovered in samples of patients that were reporting pneumonia-like symptoms in late 2019 but without an identifiable origin, no human had ever reported knowledge of or contact with the novel coronavirus SARS-CoV-2: the virus behind COVID-19. Subsequently, outbreaks, epidemics, and eventually an entire global pandemic ensued; at present, over 165 million people have been infected worldwide, resulting in nearly 3.5 million confirmed deaths thus far.
For many years, virologists, disease ecologists, and many other medical and biological researchers had been predicting that it was only a matter of time before the next pandemic arrived, including details such as how it would arise and what the most effective strategies for combating it would be. Despite the enormous scientific knowledge humanity has gained, however, an unfounded conspiracy theory about the virus’s origin has gained a lot of traction: that it was genetically engineered with the purpose of infecting humans, that it was leaked from the Wuhan Institute of Virology, and that’s where it came from. Most recently, disgraced journalist Nicholas Wade has penned an error-filled, misleading piece promoting this nonsense, but the science tells a different story.
The Wuhan Institute of Virology, shown as members of the World Health Organization (WHO) team … [+] investigating the origins of the COVID-19 coronavirus visit. This is one of the leading laboratories in the world for safely studying human-to-human transmissible diseases. (HECTOR RETAMAL/AFP via Getty Images)
AFP via Getty Images
The conspiracy, of course, is that China, and specifically the Wuhan Institute of Virology, genetically engineered this novel strain of coronavirus, SARS-CoV-2, to specifically wreak havoc on human populations. Depending on which particular incarnation of this conspiracy you listen to, it can involve:
Dr. Fauci was behind it all, using NIAID to fund EcoHealth Alliance, which then funded Wuhan, which then created SARS-CoV-2,
that secret documents from the Chinese government dating back to 2015 indicate a plan to engineer a virus that could launch a global pandemic,
that Dr. Zhengli Shi, the chief scientist for emerging disease at the Wuhan Institute of Virology, engineered this virus with a furin-like cleavage site, in order to be specifically infectious to human ACE2 receptors,
or that the specific mutations that encode arginine (instead of the more typical tyrosine in this instance) in coronaviruses are a “smoking gun” for the engineered hypothesis.
Those are the claims — some with a grain of truth behind them, others which are completely bogus — being made against the natural origins of SARS-CoV-2, the virus that causes COVID-19. Now that we know what’s being claimed, let’s take a look at the actual truth.

It doesn’t take a lot of contact between households, once an initial infection occurs, for a disease … [+] to spread into a pandemic. In this model, even a small amount of network connectivity — where each person in a household visits one and only one person outside of it — the majority of the population becomes infected in short order.
Goodreau SM et al., on behalf of the Statnet Development Team (2020)
For more than a decade, virologists, immunologists, and infectious disease specialists have been writing — in field-standard textbooks on the subject — about how the next global pandemic will likely occur. As the human population continues to grow, humans will continue to encroach on territory previously inhabited solely by animals. Now operating within these shared spaces, animal-human contact is inevitable, and that leads to the potential of disease transmission between animals and humans.
Given that mutations occur, it’s only a matter of time before a disease that’s catastrophic for humanity leapt from animals to humans, and then it would be up to humanity to mitigate the spread and severity of the outbreaks, epidemics, and pandemics that would ensue. These events, known as zoonotic events, have happened countless times over human history. Contact between humans and chimpanzees is what led to HIV first appearing in humans. Animal farming with pigs and birds has led to the pandemics of swine and bird influenzas. The idea that SARS-CoV-2 originated in animals and then leapt to humans isn’t an exotic explanation; it should be the default hypothesis.

When an animal has contact with a human, or when a human eats an animal (or an animal bites or … [+] scratches a human), diseases have the opportunity to jump from one species to another. Although most such interactions are benign, such as this one, human-animal contact has been the main culprit for the origin of novel diseases. (Edwin Remsberg/VWPics/Universal Images Group via Getty Images)
Universal Images Group via Getty Images
The alternative consideration is that this virus was created. This has a germ of truth, in the sense that humans have been “creating” novel organisms through genetic engineering for many years. Typically, this involves inserting genetic sequences that encode some structure, function, or protein into an organism, or otherwise altering its genome to produce a desired result. There’s even the prominent ability to reverse-engineer a deadly disease from pandemics past, like the 1918 “Spanish flu,” which was the last pandemic to infect over 100 million people in such a short time period. (Despite the scientific benefits of learning how flu viruses adapt to humans and cause pandemics, as well as the potential of increasing vaccine stockpiles, this research has been highly controversial for fear of weaponization.)
The science of what can be done in virology, with modern techniques, is quite impressive. But what the conspiracy attests must have happened reaches far beyond the capabilities of even the most advanced research teams in the world.
The first red flag that should leap out at you, but perhaps only if you have some knowledge of virology to begin with, is the very idea that you could “know” what certain mutations would do — i.e., that you’d know what you’d create and what effect it would have on humans — without extensive testing in humans themselves.

The SARS virus (orange) has a crown-like structure, meaning that its part of the coronavirus family … [+] of diseases. The new virus, COVID-19, is another example of a coronavirus, and is currently the largest, most lethal new epidemic to hit planet Earth in more than a decade. However, the orange color shown is completely false; COVID-19 and any other coronavirus would not look like this at all to our eyes.
NIH
For COVID-19, for example, we know that:
among the infected, asymptomatic cases represent a significant percentage of total cases,
while severe cases are relatively rare: 14% of total cases,
and critical cases, where respiratory failure, shock, or multi-organ dysfunction occurs, represent just ~5% of total cases,
and that only 2.3% of total cases are fatal, with every single documented fatality occurring among the critical case population.
This means, right off the bat, that if SARS-CoV-2 were engineered for the purpose of infecting and severely harming humans, it would have had to have been tested in at least hundreds of human subjects in order for scientists to know how effective it was. While we do have the ability to manipulate the genomes of viruses, or any other organism, for that matter, what we don’t have the ability to do is to know how that will translate into effects of the virus in human (or any living) subjects.

Nobel prize winner Dr. Paul Nurse poses with a DNA molecule and a genetic sequence. The fact that we … [+] can sequence a genome and can make modifications to an organisms genetic code is a remarkable achievement, but it doesn’t stop nature from doing what it’s always done. (David Jones/PA Images via Getty Images)
PA Images via Getty Images
Imagine that you have the tools, technology, and capability to change which amino acids are encoded by a genetic sequence. The entire SARS-CoV-2 genome, for example, has about 30,000 base pairs in it, and it only takes 3 consecutive base pairs to encode a single amino acid. There are 20 amino acids used in life processes on Earth, and there are typically two-to-four combinations of possible base pairs that can encode one of these amino acids.
There’s no technological reason why a researcher couldn’t have switched the codons for one amino acid, like tyrosine, into the codons for another one, like alanine. But then what? You can’t make a virus more deadly — or, at the very least, you have no way of knowing what that switch would do to the virus — by switching out one amino acid for another. No virologist living today has that knowledge; that’s not how this scientific field works. Without intensive and extensive studies of the virus in human beings, which we know we need because of the inherent genetic variabilities in human populations, we cannot predict what the resultant effects in humans will be.

India’s total number of COVID cases has now crested 25 million, with many cities such as Kolkata … [+] facing emergency situations. We believe it is largely due to two factors: viral load exposure and genetic predispositions, that certain individuals have severe reactions to COVID-19 infections while others are virtually asymptomatic. (Indranil Aditya/NurPhoto via Getty Images)
NurPhoto via Getty Images
Genetically, there are many reasons to think that SARS-CoV-2 occurred naturally.
The Wuhan Institute for Virology was studying bat viruses: RaTG13, to be specific. This bat virus is not a direct ancestor of SARS-CoV-2.
The first cases of COVID-19 in humans occurred in two places: linked to a wet market near the Wuhan Institute, and in more distant, rural areas where contact between humans and wild animals are common.
None of the staff at the Wuhan Institute were infected with SARS-CoV-2; they were PCR/antibody negative, which should be disqualifying for the lab leak hypothesis.
And, perhaps most importantly, the idea that SARS-CoV-2 was “perfectly adapted to humans” on first emergence is untrue; this variant appears to be a “generalist” virus.
The thing is this: there are all sorts of reasons behind why mutations occur. There are very common ones, like point mutations, deletions, or insertion mutations. But there are other types of mutations that occur as well: duplications, inversions, deletion-insertion combinations, and repeat expansions, among others. Finding an uncommon type of mutation in SARS-CoV-2 is no more evidence that a human intervened than it is to claim divine intervention for a human born with six digits on their hands and/or feet.

A sequenced genetic analysis of the UK variant of the novel coronavirus. The location of the change … [+] in the viral genome is marked by the stitches. (Sebastian Gollnow/picture alliance via Getty Images)
dpa/picture alliance via Getty Images
Many of the other “points” that lab-leak advocates bring up in a Gish Gallop of arguments are easily refuted by actual scientific studies.
What about the fact that they didn’t find the intermediary host that enabled the jump to humans? It’s true, they found the original intermediary for SARS after just 4 months, and the intermediary for MERS after 9 months. But finding intermediary hosts for most viruses, even most pandemic viruses, are often unsuccessful. SARS-CoV-2 is nothing special in this regard.
What about the fact that this virus, unique among viruses in this particular genus, possesses a furin-like cleavage site? Furin cleavage is critical to many viral diseases: HIV, Ebola, and Influenzas H5 and H7. These sites occur in many genera of coronavirus, and in betacoronavirus (which SARS-CoV-2 is) in general. A recent study shows that these sites occur naturally in coronaviruses.
What about China’s plan to “unleash the coronavirus” on the world? In 2015, a conspiracy theory was published, in Chinese, claiming that the United States genetically engineered the original SARS virus as a biological weapon against China. This conspiracy has morphed through a network of Rupert Murdoch-owned publications to reverse the perpetrator and the victim, but there’s no story there at all.

This figure shows the structure of the spike protein in SARS-CoV-2. Panel A shows the spike … [+] homotrimer in its open configuration, while panel B shows the cleavage sites on the spike protein.
Walls et al., Cell, 181 (2) (2020), pp. 281-292 e6
It might seem like there’s no harm to claim, as some scientists have done, that we ought to be more fully investigating SARS-CoV-2 to determine its origin, and that means not ruling out the possibility that it was created in a lab and leaked out. But the downside to performing that sort of investigation is twofold.
First, seriously considering this shocking, ill-founded accusation serves to further undermine the autonomy and academic freedom of researchers around the world who work in highly specialized fields. As Zhengli Shi, the chief scientist for emerging disease at the Wuhan Institute of Virology, wrote, “The hypothesis of a lab leaking is just based on the expertise of a lab which has long been working on bat coronaviruses which are phylogenetically related to SARS-CoV-2. This kind of claim will definitely damage the reputation and enthusiasm of scientists who are dedicated to work on the novel animal viruses which have potential spillover risk to human populations and eventually weaken the ability of humans to prevent the next pandemic.”
But the second reason is truly chilling: the reason so many people have died is because of a global political failure to respond appropriately. Attempting to shift the blame onto the very scientists who have been instrumental in understanding and combating the virus is a tactic straight out of Operation Himmler, and must be opposed by the entire scientific community in full force.

Chinese virologist Shi Zhengli (L) is seen inside the P4 laboratory in Wuhan in this 2017 photo. The … [+] P4 epidemiological laboratory, part of the Wuhan Institute of Virology, is one of the world’s leading research centers on coronaviruses. (Johannes EISELE / AFP via Getty Images)
AFP via Getty Images
One of the most challenging obstacles that scientists face in trying to communicate what they do is people’s stubborn resistance to a basic truth about the natural world: no one is in charge. There is no one at the controls; no one responsible for what nature does; no one in charge of mutation or natural selection in this world. Nature simply does what it does according to the physical laws that govern it, and all we can do to help navigate the human enterprise through it is to understand it and act according to the best recommendations that human knowledge has to offer.
Conspiracy theories like the lab leak hypothesis might sound compelling and inviting to us. After all, how much more comforting would it be to know that just a handful of evil people — not the politicians who sacrificed their constituents, but rather some imaginary “mad scientists” laughing maniacally in their lair — were ultimately responsible for the tragedies of the past 18 months? Fortunately, as scientists, we are not guided by comfort, but rather by the pursuit of truth and accuracy, based on the best knowledge we can obtain. Despite what many prominent voices would have you believe, the virology is open-and-shut: there is no compelling reason to believe that SARS-CoV-2 originated in a lab.
#News
1 note
·
View note
Link
We have been paying dearly for China's lies.
"This is one of the worst cover-ups in human history, and now the world is facing a global pandemic," said Rep. Michael T. McCaul, the ranking Republican member of the House Foreign Affairs Committee, before the US intelligence community concluded, in a classified report to the White House, that China has concealed the origin and extent of the catastrophic global coronavirus outbreak.
The Chinese Communist Party's "failure has unleashed a global contagion killing thousands", wrote Cardinal Charles Maung Bo, president of the Federation of Asian Bishops' Conferences, on April 1. "As we survey the damage done to lives around the world, we must ask who is responsible?"
"... there is one government that has primary responsibility for what it has done and what it has failed to do, and that is the CCP [Chinese Communist Party] regime in Beijing. Let me be clear — it is the CCP that has been responsible, not the people of China... Lies and propaganda have put millions of lives around the world in danger... In recent years, we have seen an intense crackdown on freedom of expression in China. Lawyers, bloggers, dissidents and civil society activists have been rounded up and have disappeared."
One more person has just disappeared: Ai Fen, a Chinese physician who was head of the emergency department at Wuhan Central Hospital, had worked with the late Dr. Li Wenliang. Ai, who claimed that her bosses silenced her early warnings about coronavirus, appears to have vanished. Her whereabouts, according to 60 Minutes Australia, are unknown. The journalists who saw what happened inside Wuhan have also disappeared. Caixin Global reported that the laboratories which sequenced the coronavirus in December were ordered by Chinese officials to hand over or destroy the samples and not release their findings. "If I had known what was to happen, I would not have cared about the reprimand, I would have fucking talked about it to whoever, where ever I could", Ai Fen said in an interview in March. Those were her last recorded words.
There is no record at all, however, about how this pandemic began. Wet market? A cave full of bats? Pangolins? Or a bio-weapons laboratory? No foreign doctors, journalists, analysts or international observers are present in Wuhan. Why, if the virus came out of a wet market or a cave, did China suppress inquiries to such an extent? Why, in December, did Beijing order Chinese scientists to destroy proof about the virus? Why did Chinese officials claim that US soldiers brought the virus to Wuhan? Why should it be scandalous that a US President calls a virus that began in China a "Chinese virus"?
Who announced on January 11 that Wuhan's wet market was the origin of this epidemic? The Chinese regime. It was later discovered that the first known case of coronavirus traced back to November 17, 2019.
The same Chinese regime later claimed that this coronavirus "may not have originated in China". What respected scientist or institution can now trust anything that comes out of China?
Many leading scientists have dismissed the claim that the Covid-19 virus was an engineered pathogen. This conclusion was seemingly based on the fact that Wuhan has two major virus research labs: the Wuhan Center for Disease Control and Prevention, which is apparently less than a mile from the market, and the Wuhan Institute of Virology, a biosafety level 4 (BSL-4) laboratory, handling the world's most deadly pathogens, located just seven miles from the market. The story was immediately and emphatically trashed as a "conspiracy theory".
Those scientists claim that the virus likely originated among wildlife before spreading to humans, possibly through a food market in Wuhan. They say that, through genetic sequencing, they have identified the culprit for Covid-19 as a bat coronavirus. End of story? Science, thankfully, begins by asking questions and then seeking answers.
Bats were not, it seems, sold at Wuhan's wet market. The Lancet noted in a January study that the first Covid-19 case in Wuhan had no connection to the market. The Lancet's paper, written by Chinese researchers from several institutions, detailed that 13 of the 41 first cases had no link to the market. "That's a big number, 13, with no link," commented Daniel Lucey, an infectious disease specialist at Georgetown University. So how did the epidemic start?
"Now it seems clear that [the] seafood market is not the only origin of the virus, but to be honest we still do not know where the virus came from now", notes Bin Cao, pulmonary specialist at Capital Medical University, and the corresponding author of the Lancet article.
US Secretary of State Mike Pompeo has said that China's Communist Party is withholding information about the coronavirus.
If we do not know, it is necessary be open to all possibilities.
"Less than 300 yards from the seafood market is the Wuhan branch of the Chinese Center for Disease Control and Prevention" wrote David Ignatius of the Washington Post.
"Researchers from that facility and the nearby Wuhan Institute of Virology have posted articles about collecting bat coronaviruses from around China, for study to prevent future illness. Did one of those samples leak, or was hazardous waste deposited in a place where it could spread?".
"Collecting viruses" presumably does not exclude the possibility of a "leaked virus". Worse, if China is not able to protect its laboratories, it needs to be held accountable and made to pay for the devastating global damage.
"Experts know the new coronavirus is not a bioweapon. They disagree on whether it could have leaked from a research lab", stated The Bulletin of the Atomic Scientists. Professor Richard Ebright of Rutgers University's Waksman Institute of Microbiology, and a major biosecurity expert, agreed with the Nature Medicine authors' argument that the coronavirus was not manipulated by humans. But Ebright does think it possible that the Covid-19 started as an accidental leak from a laboratory, such as one of the two in Wuhan, which are known to have been studying bat viruses:
"Virus collection or animal infection with a virus having the transmission characteristics of the outbreak virus would pose substantial risk of infection of a lab worker, and from the lab worker, the public."
Ebright has also claimed that bat coronaviruses are studied in Wuhan at Biosafety Level 2, "which provides only minimal protection" compared with the top BSL-4.
"We don't know what happened, but there are a lot of reasons to believe that this indeed was a release of some sort", China expert Gordon Chang said to Die Weltwoche.
"No one has been able to study it. How can you say it's not a release from a lab if you can't go to the lab? Indeed, we have seen Beijing do its best to prevent virologists and epidemiologists from actually going to Wuhan. The World Health Organization team went to Wuhan for like half a day with only part of the team."
That is another major problem. The potential major investigator of the Wuhan coronavirus pandemic's origin, the World Health Organization (WHO), is now accused of being "China's coronavirus' accomplice". As late as January 14, the WHO quoted Chinese health officials claiming there had been no human transmissions of the coronavirus within the country yet.
China poses a biosecurity risks for the entire planet. One year before the first coronavirus case was identified in Wuhan, US Customs and Border Protection agents at Detroit Metro Airport stopped a Chinese biologist with three vials labeled "Antibodies" in his luggage. According to an unclassified FBI tactical intelligence report obtained by Yahoo News:
"Inspection of the writing on the vials and the stated recipient led inspection personnel to believe the materials contained within the vials may be viable Middle East Respiratory Syndrome (MERS) and Severe Acute Respiratory Syndrome (SARS) materials."
Why is China trafficking in dangerous viruses in the first place?
According to Yanzhong Huang, a senior fellow for Global Health at the Council on Foreign Relations:
"A safety breach at a Chinese Center for Disease Control and Prevention lab is believed to have caused four suspected SARS cases, including one death, in Beijing in 2004. A similar accident caused 65 lab workers of Lanzhou Veterinary Research Institute to be infected with brucellosis in December 2019. In January 2020, a renowned Chinese scientist, Li Ning, was sentenced to 12 years in prison for selling experimental animals to local markets".
In February, Botao Xiao and Lei Xiao, from Guangzhou's South China University of Technology, wrote in a research paper:
"In addition to origins of natural recombination and intermediate host the killer coronavirus probably originated from a laboratory in Wuhan. Safety level [sic] may need to be reinforced in high risk biohazardous laboratories".
Xiao later told the Wall Street Journal that he had withdrawn the paper because it "was not supported by direct proofs".
Chinese laboratory mistakes have happened before. By 2010, researchers published as fact: "The most famous case of a released laboratory strain is the re-emergent H1N1 influenza-A virus which was first observed in China in May of 1977 and in Russia shortly thereafter". The virus may have escaped from a lab attempting to prepare a vaccine in response to the U.S. swine flu pandemic alert.
In 1999 the most senior defector in the US from the Soviet biological warfare program, Ken Alibek, revealed that Soviet officials concluded that China had suffered a serious accident at one of its secret biological plants, causing two major epidemics of fever that had swept China in the late 1980s. "Our analysts", Alibek stated in his book, Biohazard, "concluded that they were caused by an accident in a lab where Chinese scientists were weaponizing viral diseases".
In 2004, the World Health Organization disclosed that the latest outbreak of "severe acute respiratory syndrome" (SARS) in China involved two researchers who were working with the virus in a Beijing research lab. The WHO denounced Chinese breaches of safety procedures, and director of the Center for Disease Control and Prevention, Li Liming, resigned. Science magazine also stated that "for the third time in less than a year, an outbreak of SARS seems to have originated from a failure in laboratory containment".
Moreover, three years ago, when China opened the laboratory in Wuhan, Tim Trevan, a Maryland biosafety specialist, told Nature that he worried about the safety of the building because "structures where everyone feels free to speak up and openness of information are important." Free speech and open information: exactly what Chinese regime fought against in December and January.
A Chinese video about a key researcher in Wuhan, Tian Junhua, which was released a few weeks before the outbreak in Wuhan, shows Chinese researchers handling bats that contained viruses. In the video (produced by China Science Communication, run by the China Association for Science and Technology), Tian says:
"I am not a doctor, but I work to cure and save people... I am not a soldier, but I work to safeguard an invisible national defense line".
Tian is also reported as having said:
"I can feel the fear: the fear of infections and the fear of getting lost. Because of the fear, I take every step extremely cautiously. The more scared I feel, the more care I take in executing every detail. Because the process of you finding the viruses is also when you can be exposed to them the easiest. I do hope these virus samples will only be preserved for scientific research and will never be used in real life".
For a month, the Chinese Communist Party, instead of fighting the contagion, did everything possible to censor all information about the Covid-19 outbreak. After President Xi Jinping declared "a people's war" on the epidemic on January 20, Chinese security services pursued 5,111 cases of "fabricating and deliberately disseminating false and harmful information". The Chinese Human Rights Defenders documented several types of punishment, including detention, disappearance, fines, interrogations, forced confessions and "educational reprimand".
After that, China lied about the real number of deaths. There are photographs of long lines of stacked urns greeting family members of the dead at funeral homes in Wuhan. Outside one funeral home, trucks shipped in 2,500 urns. According to Chinese official figures, 2,548 people in Wuhan have died of the Covid-19. According to an analysis by Radio Free Asia, seven funeral homes in Wuhan were each handing out 500 funeral urns containing remains for 12 days, from March 23 to the traditional tomb-sweeping festival of April 5, a time that would indicate up to 42,000 urns, or ten times higher than the official figure.
In February, it was reported that Wuhan crematoriums were working around the clock to cope with the massive influx of infected bodies. Wuhan's officials are apparently pushing relatives of the victims to bury the dead "quickly and quietly".
"Natural virus" does not exclude its fallout from a laboratory where pathogens are collected and studied. The Nature Medicine authors "leave us where we were before: with a basis to rule out [a coronavirus from] a lab construct, but no basis to rule out a lab accident", Professor Ebright commented.
"Debate may rage over which center it is, but at this point it seems undeniable that a center has been directly involved with research on viruses, although not necessarily on the creation of a virus" wrote Father Renzo Milanese, a longtime Catholic missionary in Hong Kong.
"In other words, the virus passed from a research center in Wuhan early on. More importantly there is also no question that the authorities were aware of the dangerousness of the virus, that they did not inform anyone and that they tried to keep the facts hidden".
US Senator Josh Hawley has introduced a resolution calling for an international investigation into China's handling of the spread of the virus. According to Hawley:
"The Chinese Communist Party was aware of the reality of the virus as early as December but ordered laboratories to destroy samples and forced doctors to keep silent. It is time for an international investigation into the role their cover-up played in the spread of this devastating pandemic".
Admitting a fault, as the Japanese did after the Fukushima nuclear accident in 2011, might be one way for a country to be accepted again by the international community. Censoring, denying and covering up, as China is doing, will not.
"China claims that the deadly virus did not escape from its biolab," said a China specialist with the Population Research Institute, Steven W. Mosher. "Fine. Prove it by releasing the research records of the Wuhan lab".
27 notes
·
View notes
Link
So, we humans are so not ready for outbreaks, epidemics or pandemics so long as we ignore the threat of the pathogen or fail to understand the science behind the pathogen. We are starting to understand the science behind the COVID-19 pathogen, even as politicians in some countries (i.e., the USA and Brazil) continue to ignore the threat. (I note that Jair Bolsonaro, the President of Brazil, just announced that he has tested COVID-19 positive.) But we know the bubonic plague, and can control it. This New York Times story tells us about the emergence of this ancient public health threat in Mongolia.
A herdsman in the Chinese region of Inner Mongolia was confirmed to be infected with bubonic plague, health officials said, a reminder of how even as the world battles a pandemic caused by a novel virus, old threats remain.
The Bayannur city health commission said the plague was diagnosed in the herdsman on Sunday, and he was in stable condition undergoing treatment at a hospital.
The commission also issued a third-level alert, the second lowest in a four-level system, warning people against hunting, eating or transporting potentially infected animals, particularly marmots, and to report any dead or diseased rodents.
The city government said it had put in place plague-prevention measures that would remain in force for the rest of the year.
Then there’s the emergence of a new coronavirus/flu disease, again from China. I read the CDC paper about it, and it seems as if the CDC might be all over this one and is preparing. The CDC paper is entitled, “CDC Takes Action to Prepare Against “G4” Swine Flu Viruses in China with Pandemic Potential.” Here’s what the BBC says about this new flu strain. The caption of the story is “Flu virus with 'pandemic potential' found in China.”
A new strain of flu that has the potential to become a pandemic has been identified in China by scientists.
It emerged recently and is carried by pigs, but can infect humans, they say.
The researchers are concerned that it could mutate further so that it can spread easily from person to person, and trigger a global outbreak.
While it is not an immediate problem, they say, it has "all the hallmarks" of being highly adapted to infect humans and needs close monitoring.
As it's new, people could have little or no immunity to the virus.
The scientists write in the journal Proceedings of the National Academy of Sciences that measures to control the virus in pigs, and the close monitoring of swine industry workers, should be swiftly implemented.
The new flu strain that has been identified in China is similar to 2009 swine flu, but with some new changes.
The virus, which the researchers call G4 EA H1N1, can grow and multiply in the cells that line the human airways.
They found evidence of recent infection in people who worked in abattoirs and the swine industry in China when they looked at data from 2011 to 2018.
Current flu vaccines do not appear to protect against it, although they could be adapted to do so if needed.
5 notes
·
View notes
Text
COVID-19 Coronavirus “Fake” Pandemic: Timeline and Analysis

On January 30th 2020, the World Health Organization (WHO) declared a Public Health Emergency of International Concern (PHEIC) in relation to China’s novel coronavirus (2019-nCoV) categorized as a viral pneumonia. The virus outbreak was centred in Wuhan, a city in Eastern China with a population in excess of 11 million.
In the week prior to January 30th decision, the WHO Emergency Committee “expressed divergent views”. There were visible divisions within the Committee. On January 30th, a far-reaching decision was taken without the support of expert opinion at a time when the coronavirus outbreak was limited to Mainland China.
There were 150 confirmed cases outside China, when the decision was taken. 6 in the United States, 3 in Canada, 2 in the UK, etc.
150 confirmed cases over a population of 6.4 billion (World population of 7.8 billion minus China’s 1-4 billion).
What was the risk of being infected? Virtually zero.
The WHO did not act to reassure and inform World public opinion. Quite the opposite: A “Fear Pandemic” rather than a genuine Public Health Emergency of International Concern (PHEIC) was launched.
Outright panic and uncertainty were sustained through a carefully designed media disinformation campaign.
Almost immediately this led to economic dislocations, a crisis in trade and transportation with China affecting major airlines and shipping companies. A hate campaign against ethnic Chinese in Western countries was launched, followed by the collapse in late February of stock markets, not to mention the crisis in the tourist industry resulting in countless bankruptcies.
The complexity of this crisis and its impacts have to be addressed and carefully analysed.
What we are dealing with is “economic warfare” supported by media disinformation, coupled with the deliberate intent by the Trump administration to undermine China’s economy. The ongoing economic dislocations are not limited to China.
There are important public health concerns which must be addressed. But what motivated the Director-General of the WHO to act in this way? Who was behind this historic January 30th decision of the WHO’s Director General Tedros Adhanom Ghebreyesus.
Our subsequent analysis (in the timeline below) reveals that powerful corporate interests linked to Big Pharma, Wall Street and agencies of the US government were instrumental in the WHO’s far-reaching decision.
What is at stake is the alliance of “Big Pharma” and “Big Money”, with the endorsement of the Trump Administration. The decision to launch a fake pandemic under the helm of the WHO on January 30, was taken a week earlier at the Davos World Economic Forum (WEF). The media operation was there to spread outright panic.
(Scroll down to Read our Timeline on how these events unfolded)
But this was not the first time that the WHO decided to act in this way.
Remember the unusual circumstances surrounding the April 2009 H1N1 Swine Flu Pandemic.
An atmosphere of fear and intimidation prevailed. The data was manipulated.
Based on incomplete and scanty data, the WHO Director General nonetheless predicted with authority that: “as many as 2 billion people could become infected over the next two years — nearly one-third of the world population.” (World Health Organization as reported by the Western media, July 2009).
It was a multibillion bonanza for Big Pharma supported by the WHO’s Director-General Margaret Chan.
In June 2009, Margaret Chan made the following statement:
“On the basis of … expert assessments of the evidence, the scientific criteria for an influenza pandemic have been met. I have therefore decided to raise the level of influenza pandemic alert from Phase 5 to Phase 6. The world is now at the start of the 2009 influenza pandemic. … Margaret Chan, Director-General, World Health Organization (WHO), Press Briefing 11 June 2009)
What “expert assessments”?
In a subsequent statement she confirmed that:
“Vaccine makers could produce 4.9 billion pandemic flu shots per year in the best-case scenario”,Margaret Chan, Director-General, World Health Organization (WHO), quoted by Reuters, 21 July 2009)
A financial windfall for Big Pharma Vaccine Producers including GlaxoSmithKline, Novartis, Merck & Co., Sanofi, Pfizer. et al.
CORONAVIRUS TIMELINE
September 2019: The official US-WHO position is that the coronavirus originated in Wuhan, Hubei Province and was first discovered in Late December. This statement is questioned by Chinese and Japanese virologists who claim that the virus originated in the US.
A renowned Taiwanese virologist pointed to evidence that the virus could have originated at an earlier stage, stating : “We must look to September of 2019”.
October 18-27 2019: Wuhan 2019: CISM Sport Military World Games
Coronavirus Epidemic: WHO Declares a “Fake” Global Public Health Emergency
Chinese media intimates (without corroborating evidence) that the coronavirus could have been brought to China “from a foreign source” during the CISM Military World Games.
10,000 soldiers from 109 countries will participate
200 American military personnel participated in this 10 day Event.
October 18, Event 201. Baltimore. Coronavirus nCoV-2019 Simulation and Emergency Preparedness Task Force, John Hopkins Bloomberg School of Health Security.
Big Pharma-Big Money Simulation Exercise sponsored by WEF and Gates Foundation
Simulation Exercise of a coronavirus epidemic which results in 65 million dead. Supported by the World Economic Forum (WEF) representing the interests of Financial institutions, the Bill and Melinda Gates Foundation representing Big Pharma:
In October 2019, the Johns Hopkins Center for Health Security hosted a pandemic tabletop exercise called Event 201 with partners, the World Economic Forum and the Bill & Melinda Gates Foundation. … For the scenario, we modeled a fictional coronavirus pandemic, but we explicitly stated that it was not a prediction.
Instead, the exercise served to highlight preparedness and response challenges that would likely arise in a very severe pandemic. We are not now predicting that the nCoV-2019 outbreak will kill 65 million people.
Although our tabletop exercise included a mock novel coronavirus, the inputs we used for modeling the potential impact of that fictional virus are not similar to nCoV-2019.“We are not now predicting that the nCoV-2019 [which was also used as the name of the simulation] outbreak will kill 65 million people.
.Although our tabletop exercise included a mock novel coronavirus, the inputs we used for modeling the potential impact of that fictional virus are not similar to nCoV-2019.”
Several of the occurrences of the nCoV-2019 exercise coincided with what really happened.
In the Event 201 Simulation of a Coronavirus Pandemic, a 15% collapse of financial markets had been “simulated”.
It was not “predicted” according to the organizers and sponsors of the event.
Private sector initiative. Participation of corporate execs, foundations, financial institutions, Banks, Big Pharma, CIA, CDC, No health officials on behalf of national governments or the WHO. The simulation exercise was held on the same day as the opening of the CISM World Militaty Sports Games in Wuhan.
December 31, 2019: First cases of pneumonia detected and reported in Wuhan, Hubei Province. China.
January 1, 2020: Chinese health authorities close the Huanan Seafood Wholesale Market after Western media reports that wild animals sold there may have been the source of the virus. This initial assessment was subsequently refuted by Chinese scientists.
January 7, 2020: Chinese authorities “identify a new type of virus” which was isolated on 7 January. The coronavirus was named 2019-nCoV by the WHO exactly the same name as that adopted in the WEF-Gates-John Hopkins October 18, 2019 simulation exercise.
January 11, 2020 – The Wuhan Municipal Health Commission announces the first death caused by the coronavirus.
January 22, 2020: WHO. Members of the WHO Emergency Committee “expressed divergent views on whether this event constitutes a PHEIC or not”.
January 21-24, 2020: Consultations at the World Economic Forum, Davos, Switzerland under auspices of the Coalition for Epidemic Preparedness Innovations (CEPI) for development of a vaccine program. CEPI is a WEF-Gates partnership. With support from CIPI, Seattle based Moderna will manufacture an mRNA vaccine against 2019-nCoV, “The Vaccine Research Center (VRC) of the National Institute of Allergy and Infectious Diseases (NIAID), part of NIH, collaborated with Moderna to design the vaccine.”
Note: The development of a 2019 nCoV vaccine was announced at Davos, 2 weeks after the January 7, 2020 announcement, and barely a week prior to the official launching of the WHO’s Worldwide Public Health emergency on January 30. The WEF-Gates-CEPI Vaccine Announcement precedes the WHO Public Health Emergency (PHEIC).
January 30, 2020: Geneva: WHO Director General determines that the outbreak constitutes a Public Health Emergency of International Concern (PHEIC). This decision was taken on the basis of 150 confirmed cases outside China, First case of person to person transmission in US is reported, 6 cases in the US, 3 cases in Canada, 2 in the UK.
The WHO Director General had the backing of the Bill and Melinda Gates Foundation, Big Pharma and the World Economic Forum (WEF). There are indications that the decision for the WHO to declare a Global Emergency was taken on the sidelines of the World Economic Forum (WEF) in Davos (January 21-24) overlapping with the Geneva January 22 meeting of the Emergency Committee.
Both WHO’s Director Tedros as well as Bill Gates were present at Davos 2020. Bill Gates announced the Gates Foundation’s $10 billion commitment to vaccines over the next 10 years.
January 30, 2020 The Simulation Exercise Went Live. The same corporate interests and foundations which were involved in the October 18 John Hopkins Simulation Exercise became REAL ACTORS involved in providing their support to the implementation of the WHO Public Health emergency (PHEIC).
January 31, 2020 – One day later following the launch of WHO Global Emergency, The Trump administration announced that it will deny entry to foreign nationals “who have traveled in China in the last 14 days”. This immediately triggers a crisis in air transportation, China-US trade as well as the tourism industry, leading to substantial bankruptcies, not to mention unemployment.
Immediately triggers a campaign against ethnic Chinese throughout the Western World.
Early February: the acronym of the coronavirus was changed from nCoV- 2019 (its name under the October Event 201 John Hopkins Simulation Exercise before it was identified in early January 2020) to COVID-19.
February 28, 2020: A massive WHO vaccination campaign was announced by WHO Director General Dr. Tedros Adhanom Ghebreyesus
Who was behind this campaign: GlaxoSmithKline in partnership with the Coalition for Epidemic Preparedness Innovations (CEPI). It is a Gates-WEF partnership, both of which were sponsors of the October 18, “Simulation Exercise”. The campaign to develop vaccines was initiated prior to decision of the WHO to launch a Global Public Health emergency. It was first announced at the WEF meeting at Davos (21-24 January).
Late February 2020. Collapse of the stock markets, surge in the value of the stocks of Big Pharma.
Early March devastating consequences for the tourist industry Worldwide.
February 24: Moderna Inc supported by CIPI announced that it experimental mRNA COVID-19 vaccine, known as mRNA-1273, was ready for human testing.
Late February – Early March: China: More than 50% of the infected patients recover and are discharged from the hospitals. March 3, a total of 49,856 patients have recovered from COVID-19 and were discharged from hospitals in China. What this means that the total number of “confirmed infected cases” in China is 30,448. (Namely 80,304 minus 49856 = 30,448 (80 304 is the total number on confirmed cases in China (WHO data, March 3, 2020). These developments concerning “recovery” are not reported by the Western media
March 5, WHO Director General confirms that outside China there are 2055 cases reported in 33 countries. Around 80% of those cases continue to come from just three countries (South Korea, Iran, Italy).
These figures confirm that we are not facing a global health emergency, that the probability of infection is low. And Based on China’s experience the treatment for the virus infection is effective.
March 7: USA: The number of “confirmed cases” (infected and recovered) in the United States in early March is of the order of 430, rising to about 6oo (March 8).
Compare that to the figures pertaining to the Influenza B Virus: The CDC estimates for 2019-2020 “at least 15 million virus flu illnesses… 140,000 hospitalizations and 8,200 deaths. (The Hill)
Early March: IMF and World Bank To the Rescue
The WHO Director General advises member countries that “the World Bank and the International Monetary Fund have both made funds available to stabilize health systems and mitigate the economic consequences of the epidemic”. That is the proposed neoliberal “solution” to COVID-19. The World Bank has committed $12billion in so-called “aid” which will contribute to building up the external debt of developing countries.
March 7: China: The Pandemic is Almost Over
Reported new cases in China fall to double digit. 99 cases recorded on March 7. All of the new cases outside Hubei province are categorized as “imported infections”(from foreign countries). The reliability of the data remains to be established:
99 newly confirmed cases including 74 in Hubei Province, … The new cases included 24 imported infections — 17 in Gansu Province, three in Beijing, three in Shanghai and one in Guangdong Province.
March 10-11 Italy declares a lockdown, followed by several other countries of the EU. Deployment of 30,000 US troops in the EU as part of the “Defend Europe 2020” war games directed against Russia.
March 11: Trump orders the suspension for 30 days of all transatlantic flights from countries of the European Union, with the exception of Britain. Coincides with the collapse of airline stocks and a new wave of financial instability.
March 16: Moderna mRNA-1273 is tested in several stages with 45 volunteers in Seattle, Washington State. The vaccine program started in early February:
“We don’t know whether this vaccine will induce an immune response, or whether it will be safe. That’s why we’re doing a trial,” Jackson stressed. “It’s not at the stage where it would be possible or prudent to give it to the general population.” (AP, March 16, 2020)
Concluding Remarks
We are dealing with a complex global crisis with far-reaching economic, social and geopolitical implications.
We have provided factual information as well as analysis in a summarized “common sense” format.
Is is important that COVID-19 be the object of widespread debate and that the “official interpretations” be forcefully challenged.
We ask our readers to forward this article as well other Global Research articles pertaining to the COVID-19 coronavirus.
The original source of this article is Global Research Copyright ©
Prof Michel Chossudovsky
, Global Research, 2020
4 notes
·
View notes
Text
HOW DOES THE CORONAVIRUS OUTPUT END? WE SHOW YOU HOW TO PLAY SIMILAR EPIDEMICS.
As stock markets crash, travel stops, and new Coronavirus infections are diagnosed in the United States, one question everyone is asking is how the epidemic will end.
No one knows for sure, but virologists say there are signs of similar epidemics. Here are three scenarios:
Coronavirus Is Controlled By Health Officials Through Strict Public Health Measures
When severe acute respiratory syndrome (SARS) first appeared in Asia in 2002, it was quite scary, with a mortality rate of around 10% and without the effectiveness of medications. (The current coronavirus, by comparison, has an estimated mortality rate of less than 1 to 3.4%.) However, within a few months, SARS was controlled and eradicated largely thanks to international collaboration and strict controls. . . Outdated public health measures, such as isolation, quarantine, and contact tracing.

It would be an ideal result. However, the difference is that SARS had more severe symptoms than the current coronavirus, so people went to the hospital shortly after infection.
Coronavirus cases will be more difficult to detect and isolate, said Stuart Weston, a postdoctoral fellow at the University of Maryland. Weston is one of a small group of researchers who have received and is studying samples of coronaviruses. Weston and other experts warn that the epidemic is more widespread than that pursued in the United States and other countries because many people with mild symptoms do not know they are infected.
Coronavirus Affects The Least Developed Countries And Worsens Before Improving
One of the worst lessons of the 2014-2016 Ebola epidemic in West Africa is how an epidemic can develop when it affects countries with poor health infrastructure. For this reason, the World Health Organization and other countries in sub-Saharan Africa have prepared for coronavirus, although only a few cases have been reported so far.
Compared to the coronavirus, Ebola was less contagious and was transmitted primarily through body fluids. Coronavirus can be transmitted by coughing and sneezing droplets of breath that persist on surfaces. However, Ebola has infected more than 28,000 people and left more than 11,000 dead. Ebola is more deadly, and shortages of personnel and supplies, poverty, delays by heads of state, and government mistrust are making the epidemic worse.
WHO heads of state and government have called on countries to prepare. On Friday, the organization raised its coronavirus rating to the highest level. "This is a reality check for all governments on the planet: wake up. Prepare. This virus can be on the move and you must be prepared," said Michael Ryan, WHO Director of Health Emergencies. "Waiting to be complacent, being accidentally caught at this point is not a good excuse."
The New Coronavirus Spreads So Much That It Becomes A Reality.
This is essentially what happened with the 2009 H1N1 epidemic, also known as the swine flu. It spread rapidly and eventually reached around 11-21% of the world population. The WHO declared it a pandemic and fear have spread.
H1N1 flu is milder than originally feared and has caused little more than a runny nose and cough in most people. And H1N1 has become so common that it is simply considered part of the seasonal flu that occurs and occurs every year around the world.
Early mortality estimates for H1N1 were much higher than the 0.01 to 0.03 percent that occurred. However, the Centers for Disease Control and Prevention estimates that H1N1 killed 12,469 people, infected 60.8 million cases, and caused 274,304 hospitalizations in the United States between 2009 and 2010. The actual number is difficult to determine as many die The causes of influenza are not tested for H1N1 flu or any other strain of flu. Seasonal flu has killed at least 18,000 people in the United States this season, according to the CDC.
H1N1 is a particularly good parallel, epidemiologists say, because it has a lower death rate than SARS or MERS, but it is more deadly because of its infectivity and spread.
Not alarming, but another possible parallel could be the 1918 Spanish flu, which had a 2.5% death rate and was incredibly close to coronavirus estimates.
Not alarming, but another possible parallel could be the 1918 Spanish flu, which had a 2.5% death rate and was incredibly close to coronavirus estimates.
Florian Krammer, an influenza virologist, discovered that the world was completely different in 1918.
"We did not have the tools to diagnose diseases or antibiotics to fight secondary infections. Hospitals were places where you died and you did not receive treatment. And in 1918, the world was at war. And many infected people were soldiers in the trenches," said Krammer from the Icahn School of Medicine on Mount Sinai. "Hopefully not."
The number of people who die from a coronavirus ultimately depends on its spread, our preparedness, and the actual death rate of the virus.
Some more important things affect the final phase of the coronavirus
If the coronavirus becomes ubiquitous like H1N1, developing a vaccine is crucial. After the 2009 epidemic, experts developed an H1N1 flu vaccine that was included in the flu vaccines that people received in the following years. This has helped protect particularly vulnerable groups of the population during subsequent waves of infection.
Antiviral drugs may help shortly, and laboratories around the world are testing their effectiveness against coronavirus.
No one knows if the coronavirus will be affected by seasons like the flu, although President Trump says it could "disappear" with warmer temperatures in April.
"We are still learning a lot about the virus," said WHO epidemiologist Maria Van Kerkhove. "At the moment, there is no reason to believe that this virus works differently in different climates. We have to see what will happen later."
Coronaviruses are zoonotic, which means they spread from animals to humans. Experts believe that SARS spreads from bats to civets and humans. Middle East Fatal Respiratory Syndrome (MERS) in 2012 was likely transmitted from bats to camels to humans. With the coronavirus, no one knows which animals have caused the current epidemic. And it's a puzzle that scientists must solve to prevent it from happening again in the future.
A prime suspect is an endangered creature named Pangolin, which resembles a cross between an anteater and an armadillo, and whose scales are traded illegally.
"With SARS, once they found the responsible animals in China, they were able to begin removing them from live markets," said Vineet Menachery, a virologist at the University of Texas Medical Department. "It's like a broken water pipe. You have to find the source to turn it off."
*Precult is the covidcare Prevention. You should visit these sites*
1 note
·
View note
Text
Animal Vaccine Market Future Trends to Look Out | Bis Research

Animal Vaccines are biological preparations that provide active pharmaceutical immunity to animals against specific infectious diseases. These vaccines stimulate the animal’s immune system to recognize and combat pathogens such as viruses, bacteria and other microorganisms.
In 2022, the global Animal Vaccines market held a value of $9.44 billion. The market is expected to grow at a CAGR of 7.30% during the forecast period 2023-2033 and attain a value of $19.86 billion by 2033.
Grab a look at our report page click here !
Animal Vaccines Overview
Animal Vacciness are essential tools in modern veterinary medicine, designed to protect animals from a wide range of infectious diseases.
The development and use of Animal Vaccines have a profound impact on animal health, welfare, and productivity. In livestock, vaccines are crucial for preventing diseases that can lead to substantial economic losses due to reduced productivity, increased veterinary costs, and trade restrictions.
Animal Vacciness encompass a broad range of products, including those for common diseases like rabies, distemper, parvovirus, and leptospirosis in pets, as well as vaccines for foot-and-mouth disease, avian influenza, and brucellosis in livestock.
Key factors driving this expansion include
Pathogen Characteristics
Vaccine Technology
Immunization Protocols
Species Specificity
Grab a look at our sample page click here
Rising Demand for Animal Vacciness
Expanding Livestock Production: With global population growth and rising incomes, the demand for animal-derived protein products, such as meat, milk, and eggs, continues to escalate.
Emerging Infectious Diseases: The emergence and re-emergence of infectious diseases pose significant threats to animal health, agricultural productivity, and food security.
Market Segmentation
1 ) By Type
Livestock Vaccines
Bovine Vaccines
Small Ruminant Vaccines
Porcine Vaccines
Poultry Vaccines
Companion Animal Vaccines s
Canine Vaccines
Feline Vaccines
Equine Vaccines
(e) Aquaculture Vaccines
2) By Disease
Swine Fever
Foot and Mouth Disease
Newcastle Disease
Avian Influenza (Bird Flu)
Peste des Petits Ruminants
Other Diseases
3) By Technology
Live Attenuated Vaccines
Inactivated Vaccines
Toxoid Vaccines
Recombinant Vaccines
Conjugate Vaccines
Other Vaccines
4) By Route of Administration
Injectable Vaccines
Oral Vaccines
Intranasal/Spray Vaccines
5) By Distribution Channel
Veterinary Hospitals
Veterinary Clinics
Retail Pharmacies
Veterinary Research Institutes
6) By Region
North America
Europe
Asia Pacific
Middle East and Africa
Latin America
Key Players in the Market
Boehringer Ingelheim International GmbH
Ceva Santé Animale
Elanco Animal Health Incorporated
Merck & Co., Inc. (Merck Animal Health)
Zoetis, Inc.
Phibro Animal Health Corporation
Virbac
And many others
Visit our Life Sciences and Biopharma page click here !
Types of Animal Vacciness
Live Attenuated Vaccines
Inactivated Vaccines
Recombinant Vaccines
Vectored Vaccines
Conjugate Vaccines
DNA Vaccines
Major Trends and Drivers included are as follows
Increased focus on preventive healthcare
Emerging Infectious Diseases
Technological Advancements
Sustainable and Ethical Practices
Key Question Answers
Q What are the major market drivers, restraints, and opportunities within the global Animal Vaccines market?
Q What are the major trends adopted by the global Animal Vaccines market?
Q What are the key strategies adopted by key players in the global Animal Vaccines market?
Q How is each type segment of the global Animal Vaccines market expected to grow during the forecast period 2023-2033?
Q How is each disease segment of the global Animal Vaccines market expected to grow during the forecast period 2023-2033?
Conclusion
In conclusion, the Animal Vaccines Market plays a vital role in safeguarding animal health, enhancing animal welfare, and protecting human health. With increasing global demand for animal protein, growing awareness of zoonotic diseases, and escalating concerns about antimicrobial resistance, the importance of Animal Vacciness is more pronounced than ever before.
0 notes
Text
Coronavirus updates... things are looking pretty awful in Europe right now.
Hopefully everyone has stockpiled supplies to last for a few weeks of self-isolation. Unfortunately, as I feared, Trump’s slowness to impose travel bans has resulted in major outbreaks across America, which I can only expect will get worse in the next few weeks.
Right now, Italy has so many people requiring Intensive Care that they literally do not have enough ICUs to house them. This is coming from the country with more doctors and hospital beds per capita than most other countries in the world, including the United States. I strongly believe the US (and most other countries, including Australia) had one decent shot at this, and that was to impose travel bans and restrictions ASAP, when the first reports of major outbreaks were coming from affected countries (South Korea, Italy, etc). This may not have afforded permanent protection, but it would have bought valuable time for scientists to research effective treatments and cures, and for hospitals to prepare for an emergency. Unfortunately most countries, including the US, have failed to do this when the window of opportunity was open. Now I believe it is far too late.
I’ve heard people compare this to the flu, or to previous epidemics like SARS, swine flu or ebola - the argument being, we have survived previous “plagues”, so this one is no big deal either.
This is unfortunately a false comparison. Swine flu was highly contagious, but it had a very low mortality rate - 0.02%, and for the vast majority of people, symptoms were not severe (hospitals were not getting overrun). Swine flu roughly was comparable to the seasonal flu (which I’ll also get to in a bit). SARS was much deadlier (10% mortality rate), but in a way this made the virus much easier to combat - the symptoms were serious and came on quickly, making it relatively easy for governments to track the spread of the virus from person to person, quarantining anyone who had it or who likely had it. It was a fire that was starved of its fuel very quickly, and very effectively. And eventually, a vaccine for it was created.
Ebola was, in many ways, similar to SARS. Its symptoms were severe, making contact tracing an easy and effective method of containment. It was deadly, but it required very close contact in order to spread the disease. The high transmission and mortality rates in Africa were the result of a mixture of different reasons: cultural and social norms regarding appropriate contact with the sick or the dead, lack of accessibility to sanitation and healthcare, and also a tragic distrust towards authority and medical professionals. All these things contributed to its high rate of transmission and mortality in Africa, but meant that community spread in the US was much less likely to become uncontainable.
Now, what about the seasonal flu? I’ve seen many posts try to compare coronavirus to the flu. Posts downplaying the danger of coronavirus by pointing out that the current number of deaths is dwarfed by the number of people who die from the flu, globally, every year.
There are some obvious problems with this logic. The most obvious being that coronavirus has barely scratched the surface of the world population (in terms of how many have been infected), and given its rate of transmission (twice as contagious as the flu) and mortality rate (>30 times as deadly as the flu), and longer incubation period (average 4 days, max 14 days - for comparison, the incubation period of the flu is usually less than 2 days), without adequate containment measures the number of deaths from coronavirus could easily surpass the number of deaths from influenza. But the biggest problem, which few people talk about, is that unlike the flu, coronavirus spreads quickly and infects many people all at once. The numbers who will get sick and require urgent care is not, in and of itself, the problem - take those numbers and evenly distribute them over the year, like you normally see with the flu, and it’s hard to see what the problem is. But that’s not what’s happening. The number of new cases for coronavirus increases at an exponential rate, not a linear rate, meaning that if you’re one of the first people to get infected, you’ll probably be ok, but good luck getting a hospital bed if you happen to need one at the same time almost everybody else does.
This is the real problem with coronavirus - not the fact that it will require tens of thousands of beds and ICUs, but the fact that it will require those tens of thousands of beds all at the same time - and even the best healthcare systems in the world don’t have the capacity to help that many people all at once. And when the healthcare system inevitably has to choose who to treat, because there just aren’t enough resources to save everybody, the mortality rate will become even worse. This is the reality we are facing. I do not advise anyone to panic, as panicking will do nobody any good. But we CANNOT be complacent about this either. We cannot downplay the seriousness of this - there is no reason to think what’s currently happening in Italy won’t happen in US or anywhere else. Please, avoid crowded places, wash your hands, keep surrounding areas clean, and be willing to practice social distancing. Even if you yourself aren’t at risk of complications or death, you can prevent yourself from spreading it to someone who is.
2 notes
·
View notes
Photo

Can We Trust the WHO?
The most influential organization in the world with nominal responsibility for global health and epidemic issues is the United Nations’ World Health Organization, WHO, based in Geneva. What few know is the actual mechanisms of its political control, the shocking conflicts of interest, corruption and lack of transparency that permeate the agency that is supposed to be the impartial guide for getting through the current COVID-19 pandemic. The following is only part of what has come to public light.
Pandemic declaration?
On January 30 Tedros Adhanom, Director-General of the UN World Health Organization declared a Public Health Emergency of International Concern or PHIEC. This came two days after Tedros met with China President Xi Jinping in Beijing to discuss the dramatic rise in severe cases of a novel coronavirus in Wuhan and surrounding areas that had reached dramatic proportions. Announcing his emergency PHIEC declaration, Tedros praised the Chinese quarantine measures, measures highly controversial in public health and never before in modern times attempted with entire cities, let alone countries. At the same time Tedros, curiously, criticized other countries who were moving to block flights to China to contain the strange new disease, leading to charges he was unduly defending China.
The first three cases in Wuhan were reported, officially, on December 27, 2019, a full month earlier. The cases were all diagnosed with pneumonia from a “novel” or new form of SARS Coronavirus. Important to note is that the largest movement of people in the year, China’s Lunar New Year and Spring Festival, during which some 400 million citizens move throughout the land to join families went from January 17 through February 8. On January 23, at 2am two days before start of actual New Year festivities, Wuhan authorities declared an unprecedented lockdown of the entire city of 11 million as of 10am that day. By then, hundreds of thousands if not several million residents had fled in panic to avoid the quarantine.
By the time the WHO declared its Public Health Emergency of International Concern on 30 January, precious weeks had been lost to contain the disease. Yet Tedros effusively praised the “unprecedented” Chinese measures and criticized other countries for placing “stigma” on Chinese by cutting travel.
In reference to the Wuhan COVID-19 spread and why WHO did not call it a pandemic, the WHO spokesman, Tarik Jasarevic, stated “There is no official category (for a pandemic)…WHO does not use the old system of 6 phases — that ranged from phase 1 (no reports of animal influenza causing human infections) to phase 6 (a pandemic) — that some people may be familiar with from H1N1 in 2009.”
Then, in an about-face, on March 11, Tedros Adhanom announced for the first time that WHO was calling the novel coronavirus illness, now renamed COVID-19, a “global pandemic.” At that point WHO said there were more than 118,000 cases of COVID-19 in 114 countries, with 4,291 deaths.
2009 WHO Fake Pandemic
Since an earlier WHO fiasco and scandal in 2009 over its declaration of a global pandemic around the “swine flu” or H1N1 as it was termed, the WHO decided to drop using the term pandemic. The reason is indicative of the corruption endemic to the WHO institution.
Just weeks before first reports in 2009 of a young Mexican child being infected with a novel H1N1 “swine flu” virus in Veracruz, the WHO had quietly changed the traditional definition of pandemic. No longer was it necessary a reported disease be extremely widespread in many countries and extremely deadly or debilitating. It need only be widespread, like seasonal flu, should WHO “experts” want to declare pandemic. WHO H1N1 symptoms were the same as a bad cold.
When then-WHO Director-General Dr Margaret Chan officially declared a Phase 6 global Pandemic emergency, that triggered national emergency programs including billions of dollars of government purchases of alleged H1N1 vaccines. At the end of the 2009 flu season it turned out the deaths due to H1N1 were tiny relative to the normal seasonal flu. Dr Wolfgang Wodarg, a German physician specialising in Pulmonology, was then chairman of the Parliamentary Assembly of the Council of Europe. In 2009 he called for an inquiry into alleged conflicts of interest surrounding the EU response to the Swine Flu pandemic. The Netherlands Parliament as well discovered that Professor Albert Osterhaus of the Erasmus University in Rotterdam, the person at the center of the worldwide Swine Flu H1N1 Influenza A 2009 pandemic as the key advisor to WHO on influenza, was intimately positioned to personally profit from the billions of euros in vaccines allegedly aimed at H1N1.
Many of the other WHO scientific experts who advised Dr Chan to declare pandemic were receiving money directly or indirectly from Big Pharma including GlaxoSmithKline, Novartis and other major vaccine-makers. The WHO Swine Flu Pandemic declaration was a fake. 2009-10 saw the mildest influenza worldwide since medicine began tracking it. The pharma giants took in billions in the process.
It was after the 2009 pandemic scandal that the WHO stopped using the 6 phase pandemic declaration and went to the totally vague and confusing “Public Health Emergency of International Concern.” But now, Tedros and WHO arbitrarily decided to reintroduce the term pandemic, admitting though that they are still in the midst of creating yet a new definition of the term. “Pandemic” triggers more fear than “Public Health Emergency of International Concern.”
WHO’s SAGE Still Conflicted
Despite the huge 2009-10 conflict-of-interest scandals linking Big Pharma to WHO, today the WHO under Tedros has done little to clean out corruption and conflicts of interest.
The current WHO Scientific Advisory Group of Experts (SAGE) is riddled with members who receive “financially significant” funds from either major vaccine makers, or the Bill and Melinda Gates Foundation (BGMF) or Wellcome Trust. In the latest posting by WHO of the 15 scientific members of SAGE, no fewer than 8 had declared interest, by law, of potential conflicts. In almost every case the significant financial funder of these 8 SAGE members included the Bill and Melinda Gates Foundation, Merck & Co. (MSD), Gavi, the Vaccine Alliance (a Gates-funded vaccine group), BMGF Global Health Scientific Advisory Committee, Pfizer, Novovax, GSK, Novartis, Gilead, and other leading pharma vaccine players. So much for independent scientific objectivity at WHO.
Gates and WHO
The fact that many of the members of WHO’s SAGE have financial ties to the Gates Foundation is highly revealing, even if not surprising. Today the WHO is primarily financed not by UN member governments, but by what is called a “public-private partnership” in which private vaccine companies and the group of Bill Gates-sponsored entities dominate.
In the latest available financial report of WHO, for December 31, 2017, slightly more than half of the $2+ billion General Fund Budget of WHO was from private donors or external agencies such as World Bank or EU. Far the largest private or non-government funders of WHO are the Bill and Melinda Gates Foundation together with Gates-funded GAVI Vaccine Alliance, the Gates-initiated Global Fund to Fight AIDS, Tuberculosis and Malaria (GFATM). Those three provided more than $474 million to WHO. The Bill and Melinda Gates Foundation alone gave a whopping $324,654,317 to WHO. By comparison, the largest state donor to WHO, the US Government, gave $401 million to WHO.
Among other private donors we find the world’s leading vaccine and drug makers including Gilead Science (currently pressing to have its drug as treatment for COVID-19), GlaxoSmithKline, Hoffmann-LaRoche, Sanofi Pasteur, Merck Sharp and Dohme Chibret and Bayer AG. The drug makers gave tens of millions of dollars to WHO in 2017. This private pro-vaccine industry support for the WHO agenda from the Gates Foundation and Big Pharma is more than a simple conflict of interest. It is a de facto high-jacking of the UN agency responsible for coordinating worldwide responses to epidemics and disease. Further, the Gates Foundation, the world’s largest at some $50 billion, invests its tax-exempt dollars in those same vaccine makers including Merck, Novartis, Pfizer, GlaxoSmithKline.
Against this background it should come as no surprise that Ethiopian politician, Tedros Adhanom, became head of WHO in 2017. Tedros is the first WHO director not a medical doctor despite his insistence on using Dr. as title. His is a doctor of philosophy in community health for “research investigating the effects of dams on the transmission of malaria in the Tigray region of Ethiopia.” Tedros, who was also Ethiopia Minister of Foreign Affairs until 2016, met Bill Gates when he was Ethiopian Health Minister and became Board Chair of the Gates-linked Global Fund Against HIV/AIDS, TB and Malaria.
Under Tedros, the notorious corruption and conflicts of interest at WHO have continued, even grown. According to a recent report by the Australian Broadcasting Corporation, in 2018 and 2019 under Tedros, the WHO Health Emergencies Program, the section responsible for the COVID-19 global response, was cited with the highest risk rating noting the “failure to adequately finance the program and emergency operations [risks] inadequate delivery of results at country level.” The ABC report further found that there has also been a “surge in internal corruption allegations across the whole of the organisation, with the detection of multiple schemes aimed at defrauding large sums of money from the international body.” Not very reassuring.
In early March Oxford University stopped using WHO data on COVID-19 because of repeated errors and inconsistencies the WHO refused to correct. The WHO test protocols for coronavirus tests have repeatedly been cited by various countries including Finland for flaws and false positives and other defects.
This is the WHO which we now trust to guide us through the worst health crisis of the past century.
1 note
·
View note
Last Seen Blogs


mostly-funnytwittertweets
previously funnytwittertweets

patternsofgrace
Patterns of Grace

krizzii
Krizzii's Tumblr

bmyth
f