#Stent placement
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
The KCSC sent more than 20K requests to delete posts related to prostitution and porn to Tumblr from January to June 2017.
Text
CAN YOU REFUSE A STENT AFTER KIDNEY STONE SURGERY?
Yes, it is possible to refuse a stent after kidney stone surgery. A stent, also known as a ureteral stent, is a thin tube that is placed in the ureter (the tube connecting the kidney to the bladder) to help urine drain properly. It is commonly used after certain kidney stone surgeries, such as ureteroscopy or lithotripsy, to promote healing and prevent complications.
However, the decision to have a stent placed or removed ultimately rests with the patient. If you have concerns or wish to refuse a stent, it is important to discuss your preferences with your urologist or surgeon. They can provide you with information about the potential risks and benefits of stent placement and alternative options, if available, based on your specific medical situation.
It is crucial to have an open and honest conversation with your healthcare provider to ensure that you make an informed decision that aligns with your preferences and overall health.
#Kidney stone surgery#Stent placement#Ureteral stent#Ureteroscopy#Lithotripsy#Kidney stones#Post-surgical care#Patient preferences#Medical decision-making#Urology
0 notes
Text
Best Stent placement Hospital in Amritsar
Livasa Hospitals, the best stent placement hospital in Amritsar, is renowned for its advanced cardiac care and state-of-the-art facilities. Our team of expert cardiologists specializes in minimally invasive stent placement procedures, ensuring precision and faster recovery for patients. Equipped with cutting-edge technology, we provide personalized treatment plans to address each patient’s unique needs. Livasa Hospitals is committed to delivering compassionate care, accurate diagnoses, and successful outcomes. With a focus on patient safety and comfort, we have become a trusted name in cardiac healthcare. Choose Livasa Hospitals for superior stent placement services in Amritsar and experience excellence in heart care.
0 notes
Text
youtube
#surgery simulator#neurosurgery simulator#ct simulator#realtime simulator#surgical simulation#medical simulators#surgery simulation#laparoscopic simulator#plastic surgery simulator#emr simulation for students#mentice endovascular simulator#neurosurgical simulator#endovascular simulator#best endovascular simulator for training#surgeonslab ag#endovascular training#endovascular surgery training#catheterization and stent placement#cutting edge simulator#Youtube
0 notes
Text
Can someone lead an everyday life after a 95% blockage of an artery?
Yes, but it's important to know what's going on in treatment. Angioplasty can open up an artery, but it's almost always followed with a stent. For the lining of the artery to accept the stent so it grows into place so blood clots can't form around it, it's utterly essential to take all your prescribed anticoagulants (blood thinners). If you have diabetes, you also have to keep your blood sugar levels under control, and you have to watch your blood pressure and cholesterol. All of this is pretty easy to do, but you do have to do it. That being said, you will probably feel better after treatment, and you will go back to living the everyday life you had forgotten. There are lots of things that can go wrong; there are lots of variations in treatment, but yes, many people do live everyday lives after angioplasty, stents, and bypass. Most feel tremendously better. But you have to change your lifestyle after Surgeries.
Lifestyle Changes
These modifications may be the only treatment required for some people.
Maintain a healthy weight by following a healthy diet to prevent or reduce high blood pressure and high cholesterol.
If you smoke, stop.
Be physically active.
If you're overweight or obese, you should lose weight.
Reduce your stress levels.
To reduce high blood pressure or high cholesterol, follow your doctor's instructions.
#health#hospital#balloon angioplasty#balloon angioplasty and stent#balloon and stent angioplasty#balloon angioplasty and stent placement#balloon angioplasty and stents procedure
0 notes
Text
Malicious Compliance // Surgeon Strange x Reader
Masterlist | Request a Fic
Summary: After a brief meeting with the world renowned neurosurgeon Doctor Stephen Strange, he plans to make you his latest conquest. He’s only interested in one thing, but that’s okay, because so are you. (female reader)
Word Count: 4.6K
Warnings: Strong language, explicit sexual content, pre-sorcerer Strange (arrogant, cocky). Smut: no strings attached, dominance & praise, oral sex (receiving), light choking, unprotected sex (sort of?). Readers must be 18+
A/N: Just a quick lil oneshot for you all. I literally thought of this today and the whole thing poured out of me in one sitting lmao. I like it though, hope you guys do too!

His eyes are glaciers. Cold, hard, yet always moving. They flit towards the window, sunlight turning them the crispest blue, then back down to the notebook on the table in front of him. They warm slightly when he looks over to Doctor Palmer, roll languidly whenever Doctor West speaks. But in the end, they always seem to settle back on you.
He’s as hubristic as you’d expected; leant back in his chair, elbows on the armrests, taking up as much space as his body will allow. He corrects a colleague when they call him Stephen. It’s Doctor Strange, he says, voice so deep and rich it’s almost tangible.
He watches as you press your finger to the inner corner of your eye, trying to rub away the tired itch beginning to take root there. You wonder how offended he’d be if he knew you fell asleep reading one of his published papers last night, how you woke up in your hotel room this morning with your cheek pressed to page seventeen of The Strange Palmer Method. It would make his blood boil, you think, to know his work had been used as a pillow. You resist the urge to tell him.
Coffee burns the roof of your mouth. You wince and place the cup back down on the boardroom table, sift through the pile of papers in front of you as the room waits for you to speak again.
“Honey,” says Doctor Strange.
“I’m sorry?” you reply.
He points to your mouth. “It’ll help with that burn.”
You stare at him for a moment before shaking your head. “Oh I didn’t- It was just a little warmer than I expected. Thanks, though.”
The corner of his mouth curls and he turns to look down the length of the table, the flecks of silver at his temple catching in the light.
You clear your throat as you find the document you were looking for. “So, pending approval from the ABMS, we would like to roll out training for the Strange Palmer Method in all of our hospitals.”
“What about my new technique for stent placement?” asks Doctor West.
“Oh please, Nic,” Strange scoffs. “We’re talking about actual revolutionary surgical procedures here.”
Doctor West’s back straightens, you open your mouth to speak but he gets there first.
“Excuse me, my stent technique could drastically cut down the amount of time a patient’s brain is open on the table! Do you even realise-”
“Mhm, why don’t you go win some awards and make national news, then maybe we can talk.”
Doctor Palmer’s head falls into her hands as the other surgeons groan and shift uncomfortably in their seats. You’ve met your fair share of asshole surgeons in this job; travelling up and down the country stroking egos and exalting god complexes. But this man sitting across from you is, without a doubt, the victor of them all.
“The stent technique is very interesting,” you say, easing the tension in the room. “But we would need to see the results of a study or trial of some kind before taking it any further.”
“Very diplomatic of you,” says Strange.
“Not diplomatic. I just know a promising procedure when I see it.”
“Hm. Are you a doctor?”
Your gaze turns to a glare. “I am.”
“Where do you practice?”
“I don’t anymore. My job is to keep other doctors at the top of their game. Hence why I’m here right now with all of you.”
He’s almost smirking, head cocked slightly, twiddling a pen between his fingers. It’s fitting, you think, to see a surgeon take such pleasure in getting under people’s skin.
You hate that you find him attractive. That you’ve managed to fall victim to a charm buried so deep beneath layers of pure arrogance that you have to dig to find it. If he wasn’t so beautiful on the outside, you’re almost certain you wouldn’t bother fighting to find something redeemable within. But the way your body reacts to him; the warmth, the buzzing deep in your belly, it must be there.
The meeting finishes and you remain at the table, straightening the wad of papers in front of you and slotting them back into your binder as everyone filters out of the room. When you’re alone, you stand and walk to the large window, taking a moment to gaze out at the view. Your eyes skim New York City, admiring the blend of old and new; small stone buildings wedged between tall skyscrapers, the late afternoon sun glinting across metal and glass, pockets of green peppered amongst brick and mortar. You wish you got to come here more often.
You pick up your briefcase and drape your jacket over your arm as you make your way out of the boardroom. The corridor is bright and quiet, but the bustling of the hospital is a low hum. You close the door behind you and begin to walk, unfazed by the sight of a figure leaning against the wall up ahead.
His arms are folded over his broad chest, dark blue scrubs doing little for his tall, robust frame. His legs are crossed at the ankles as he rests his weight back against the wall, head stooped slightly, but his eyes are on you.
“Doctor Strange,” you say with a polite nod as you continue past him.
He smiles, allows you to pass, but you feel him move behind you.
“You don’t really think Doctor West’s procedure holds any merit?” he asks, catching up to walk at your side.
“I do.” You furrow your brow. “You don’t think there’s merit in improving the efficiency of existing surgeries?”
He shrugs. “Just not all that exciting when you compare it to what I’m doing.”
“You mean what you and Doctor Palmer are doing…”
There’s a chuckle deep in his throat, like he enjoys the back and forth, watching his opponents fight for their lives while to him it’s just a sparring match. He quickens his pace to slip in front of you, turning to face you and forcing you to halt in the middle of the corridor.
“Be honest,” he says. “You’re impressed.”
“Of course we’re impressed. Why else would the board have sent me here?”
“No I mean you, specifically.”
You glare up at him, hiding your amusement with an eye roll. “Yes, Doctor,” you say slowly, your words empty and biting. “I am very impressed.”
His cupid’s bow deepens as his lips curve into a self satisfied smile, lines forming in his cheeks and the corners of his eyes. He knows you find him infuriating, but it only seems to encourage him. There’s a moment of silence, long enough for his gaze to trail the length of you, just once.
“You know, I’d love to talk more with you about it,” he says, looking down at his obviously expensive watch. “Maybe over dinner. Have you eaten?”
You draw in a deep breath through your nose, letting it out in a sigh as you begin to speak. “I don’t need your superficial attempts to woo me, Doctor.” You reach into your briefcase and pull out a pen and a business card, scrawling on the back of it and handing it to him. “This is where I’m staying. Come by around eight.”
You’re certain he’s going to protest, pretend he actually wants to go to dinner, talk, that he was ever interested in anything that didn’t involve the removal of your clothes. You wait in suspense as his eyes flit down to the card in his hand, then back up to your face.
“I prefer to fuck in my own bed,” he says bluntly.
A wave crashes in your stomach, rushing down into your core, the sensation so strong and unexpected that your knees almost buckle. This isn’t the first time one of your work trips has ended in you going home with a surgeon, but the way this one doesn’t try to feign the ‘nice guy’, doesn’t pretend to want anything more from you than your body, that’s new.
“Unless I’m on vacation, of course,” he adds with a cocky smile.
“Of course…”
He flips the card over and plucks the pen from your hand. You watch as he scribbles on it and hands it back to you.
“So this is where I’ll be tonight,” he says. “You said eight works for you?”
You press your tongue to the inside of your cheek, unsure if you’ve ever met anyone as imperious as this. You slip the card into your pocket and move to walk past him, stopping as your shoulders brush and looking up at him.
“I hope your dick is as inflated as your ego.”
He smirks to himself, remaining quiet as you continue to walk away.

Your skirt is riding up your backside. You reach back to yank it down for the hundredth time before pressing the buzzer on the wall of the apartment building. The setting sun is just a glow beneath the horizon but the streets are still busy, the air warm with a pleasant breeze. You lean back to stare up at the building, the mirrored windows stretching so high you can’t see an end to them. You wonder which one is his.
There’s a scratching sound on the intercom, followed by a deep voice. “Yeah?”
“It’s me,” you say, glancing over your shoulders as if you’re on some kind of secret mission, scared of being seen.
He doesn’t speak again, instead there’s a quick buzz followed by the click of the heavy front door. You let yourself inside, heels clacking against the glossy marble floor as you hurry towards the elevators. When the doors slide open, you pull out your business card, punch in the floor number he’d scrawled in the bottom corner. It begins to ascend, making your already swirling stomach turn.
You pull down the back of your skirt again as you step out into the hall, peering down the length of it in search of his apartment. The door is tall and wide, dark timber and a heavy metallic handle. You knock but your knuckles barely make a sound, the dense wood swallowing the echo.
Still, he comes. You regard him quietly as you step inside, the snug sweater and tailored jeans, a pair of sneakers making you feel entirely overdressed. He’s already grinning; a smug, confident smile that reignites the ire in your chest. You ignore him and walk further in, eyes wide in awe at the vast, industrial space.
You walk over to the window that stretches the length of the apartment, floor to ceiling, wall to wall, framing a perfect snapshot of the city.
“Now I understand why you make the women come to you,” you say.
“Hm?”
“This place. It’s impressive.” You glance over your shoulder at him. “That’s the point, right? You like to impress. To show off.”
He laughs quietly and makes his way to the kitchen area, opening the extensive liquor cabinet. “You want something to drink?”
“I have rules,” you say abruptly, turning around to face him from across the echoey room.
He straightens. “Go on…”
“Nothing that happens here can be used for any type of professional leverage, good or bad, by either of us.”
“Of course-”
“This isn’t a date. I don’t spend the night, I don’t keep in touch, I don’t call when I’m back in town so we can do this again. This is just tonight. And it’s just sex. Understood?”
“Understood.” He returns to the cabinet and takes out a bottle. “So, about that drink…”
You’re already gone, wandering off through a door at the rear of the apartment in search of the bedroom.
You find it. It’s a dark, cave-like space, large curtains draped across another huge window, only the faintest glow of the sunset fighting through the fabric. It’s clinical, just as you’d expect from a surgeon; sleek furniture void of any clutter or knick knacks, exposed brick walls with the occasional piece of art - no photographs. There’s a full length mirror, a small couch, and a bed so large you could sink into it and disappear. You wonder just how many women have delved beneath those sheets before you.
He appears in the doorway, looking you up and down. “You’re eager, little one,” he teases.
You roll your eyes, watching as he closes the door behind him and approaches you. You reach up to touch him, to kiss him, but instead he takes your wrists in his hands and lowers them back to your sides.
“Mm, not yet.”
You scoff in dispute, eyes following him as he strolls across the room and switches on the wall sconces, illuminating the area above the bed in a dim, warm light.
“Look,” you say. “If you’re just going to mess with me then-”
“Well actually, after you left the hospital this afternoon, I got called to consult on a patient and ended up having to stay late. I just got home around fifteen minutes before you knocked on my door. So if you don’t mind, I would like to take a shower first. Is that alright with you?” he finishes sarcastically.
You settle down, composing yourself and relaxing your shoulders. “Of course.”
“Make yourself comfortable.”
He pushes open a door to the right and you catch a glimpse of the luxurious, marbled master bathroom as he steps inside. The door closes behind him, leaving you alone again. You stand there for a moment, listening to him whistling to himself, his belt buckle unfastening and hitting the floor. Water bursts from the shower, the sound like soft static, and you immediately rush over to the mirror.
You examine yourself carefully; fix your hair, press your nose to your skin and clothes, shift your underwear so it sits smoothly and undetectable beneath your skirt. Then you sit down at the foot of the bed, knee bouncing impatiently. You change your mind shortly after, moving to the small couch opposite the bed instead.
Ten minutes or so pass, but it feels like an eternity. You picture him drawing it out on purpose, working the lather into his skin one section at a time, scrubbing at his hair for much longer than necessary, just to make you sweat. The water shuts off and you listen to him singing to himself, the hum of his voice through the door. When the door finally opens, steam escapes into the bedroom, the rich smell of citrus and cedar filling the air as he walks out, still humming quietly.
You glance over at him, mouth falling open slightly to find him completely naked, your gaze falling immediately to the pronounced length hanging from his body as he pads across the room. You look away quickly, rolling your eyes and huffing with indignation. Of course he’s naked, you think, he likes to spar, and you’ve willingly stepped into the ring.
Droplets sit on his shoulders and roll down his torso as he moves around the bed. He climbs on and lays down right in the middle, hands resting behind his head, propped up slightly on the headboard. His hair is still damp, half-coiffed, the grey at his temples darker than it was before. His body is solid, the mystery beneath the scrubs now revealed to you in all its glory. His arms are thick as they flex either side of his head, divots of muscle creating shadows across his torso, cock resting proudly on his thigh as he parts his legs in wait. He’s exquisite, and you can’t help but bask in the sight.
“So,” he says casually. “Are you just going to stay over there looking at me? Or are you going to come and sit on my face?”
You glare at him, unamused.
“What?” he shrugs gently. “You’re the one that said this was strictly sex. Forgive me for abiding by your rules.”
“There’s a word for that, you know,” you reply. “Malicious compliance.”
“Mm, is it really malicious if I’m offering to eat you out?”
“Depends how good you are at it.”
“Come here and find out.” There’s no humour in his tone, but it’s still playful, like he’s goading you.
You stand up and take a step towards the bed.
“Clothes,” he demands.
You stop, pressing your lips together tightly. His eyes never leave you, remaining locked on yours as you kick off your shoes and untuck your top from the waistband of your skirt.
“They should study you,” you say.
“Study me?”
“Yeah.” You lift your top over your head and throw it to the floor, reaching down to unzip your skirt. “Look into how one singular person could possibly be such an ass.”
“Clearly there’s a part of you that likes it, y’know, since you’re here… taking your clothes off for me.”
“What can I say? I’m partial to a surgeon. Think it’s the hands.”
The skirt pools at your feet and you step out of it, extending your arms as if to say ‘ta da’. He smiles.
No one has ever looked at you like this. So intense, like he’s studying every inch; relishing in every freckle and blemish, every curve and crease, mapping out the places he plans to touch, taste, explore.
You continue towards him but he raises his palm, halting you again. “You haven’t finished,” he says.
You glance down at yourself, then back up to him, letting out a grumbling sigh as you reach behind you to unclasp your bra. It pops open, the release of pressure on your skin as soothing as a deep breath. His gaze darkens as you slide the straps off your shoulders, watching your nipples harden as you reveal your bare breasts to him.
“These too?” you ask, hooking your thumbs into the waistline of your underwear.
“Mhm.”
You take them off as gracefully as you can, shimmying them over your hips and thighs and kicking them away. His cock is hardening, swelling and rising towards his stomach. Your mouth twitches with a triumphant smile, but you suppress it as you climb onto the bed, crawling up to meet him.
You lean down and press your lips to his, feeling your skin prick, arousal kindling in your core. His mouth is smart, but it’s also divine. The feeling intensifies, spreading through your belly and pounding between your legs as you sweep your tongue into his open mouth, feel his restraint wavering as your hot breaths mingle. You let your chest press against his, the feeling of skin on skin making you burn with need.
You bring a hand up to his face, he brings his to your throat, bracketing it gently and peeling his mouth from yours.
“I didn’t tell you to kiss me,” he says quietly. “I told you to sit on my face.”
You pull back a little more, making eye contact, breathless as a million comebacks shutter through your mind. But in the end you say nothing, letting out a soft huff and slowly shifting your body up the bed.
You hold the top of the extravagant headboard with both hands and swing one leg over him, straddling his shoulders as his fingers reach up behind you to the small of your back. His touch is electric, lips searing as they plant a kiss on your inner thigh. A soft whimper escapes you in a breath, as though anticipation is its own foreplay.
He wraps his arms around the backs of your thighs and pulls you down onto his mouth. Your grip tightens on the headboard, fingernails digging into the soft, cushiony fabric as he parts his lips against your centre, sucking softly on your already throbbing clit. Your head falls back when his tongue drags up the length of your slit, moulding itself to every pucker and groove, lapping you up like he adores you, and you wonder how many women have fallen for him in these moments.
You groan quietly, closing your eyes as you focus on the flicks and strokes of his tongue, the sucking and swirling, the hums deep in his throat and he devours you. Your clit is sensitive, making you shudder, the pleasure so intense you can barely stand it. Your body raises up instinctively, but he tightens his hold on you, spitting on your clit and returning his mouth to the place that both aches and sings, somehow at the same time.
You gasp in response, eyelids fluttering as you swear under your breath. He releases one of your thighs and you glance over your shoulder to see his hand wrapping around his cock. He begins to stroke it forcefully, working himself to the rhythm of his mouth, and you almost fall to pieces.
“Oh my god,” you moan, slumping forward and pressing your forehead to the headboard.
Your thighs clamp around his head, but it only spurs him on, making him bury his face deeper, and you can’t remember the last time he came up for air.
“I can’t,” you whisper.
The nerves in your clit are screaming, dancing on the precipice between pain and pleasure. He continues to lap at your centre, pushing you to the edge until you’re clinging on for dear life. Pressure swells in your core, flooding you with a tingling heat that softens your bones and turns you to liquid. Until finally you’re there, falling, melting.
He growls as your body begins to shake, working his tongue over you one last time before releasing you from his grasp. You collapse next to him, sliding down the pillows until you’re lying at his side. You’re breathless, chest rising and falling heavily as you stare up at the ceiling.
He rolls onto his side to face you. “You’re quiet when you come,” he says, placing a kiss into the crook of your neck, another at the dip of your collarbone.
“I’ve spent the past two years practically living in hotel rooms,” you reply. “I’ve learned to be inconspicuous.”
“Hm.” He props himself up on his forearm and leans over you, his other hand trailing softly down the side of your body. “Let’s see if we can do something about that.”
Before you can reply, he’s kissing you. His mouth is slick, it tastes of you. Your body is spent, limbs heavy, yet still you find it responding to his touch. He shifts further onto you, spreading your legs with his hands and settling himself between them. You can feel his cock nudging your centre as he rocks his hips, sliding along the soaking wet mess he left there and brushing his head over your clit. It’s sensitive, raw, makes you gasp. But he swallows the sound with a heady kiss.
He’s big. Thick. Hard. Maybe that’s where he stores his arrogance. He continues to tease you, soaking himself in the mix of spit and slick as he wraps his hands around your neck, kisses you so deeply you can feel him drawing a moan from your throat.
He pulls away and looks down at you for a moment. “Condom?” he asks casually.
You’re on the pill. Have been since you were seventeen. But still, you know you should say yes. Yesterday, this man was a stranger; a face you only knew from TV and the medical articles you’d read.
“No.” You shake your head and reach down, gripping his cock and directing it into you.
He chuckles, the sound deep and low. “What a good girl.”
You sigh as he teases at your entrance, pushing the head of his cock in and out but never breaking all the way through.
“Were you thinking about this today in the meeting?” he taunts softly.
You groan and buck your hips, desperate for him to take you.
He eases back slightly and tuts. “I saw you squirming in your seat. How hot and flustered you got when I looked at you. Tell me how much you wanted this.”
“What I wanted,” you begin quietly. “Was to wring your neck.”
The corner of his mouth curls into a smirk. “Really…”
“Really.”
He squeezes his fingers gently around your throat and you exhale softly. The desire is almost painful, your core throbbing, pussy aching.
“Funny how things work out,” he says.
You let out a stifled moan as he sinks into you, filling you so completely you’re certain you can’t take it.
“That’s it,” he mutters as he looks down, watching his cock disappear all the way to the hilt.
You whimper and tighten around him. He sucks the air in through his teeth, returning his gaze to your eyes with a mischievous smile.
“I’m gonna need you to not do that,” he says. “You’ll have me finishing in seconds.”
“Are you telling me the great Doctor Stephen Strange lacks self discipline?” You contract your walls again, this time on purpose.
He bows, forehead resting on your chest, and growls deep in the back of his throat. Then suddenly, without warning, he draws his hips back and buries himself in you again. You gasp, fingers digging into the blades of his shoulders as he repeats his thrusts, building to a firm, steady rhythm.
A small cry escapes you; a sound you’ve never heard yourself make before. He hums in response, keeping you pinned to the bed with his hands around your neck as he snaps his hips, punishing you from the inside out.
“Wrap those legs around my back,” he demands.
You do as you’re told, locking your ankles and gasping as he sinks further, the head of his cock kissing the deepest parts of you and sending jolts of pure electricity through your stomach.
“You’re going to break me,” you whisper.
“Not this time. Maybe later,” he replies, still so arrogant it makes you want to reach up and slap him.
But your hands are stuck to his back, nails digging into the smooth, taut flesh. Another unfamiliar sound falls from your lips, somewhere between a grunt and a hum. He likes it, you can tell in the way he closes his eyes to compose himself.
“Jesus,” he hisses.
His movements begin to stutter and he rests his forehead against yours. You feel his cock throbbing, your pussy growing wetter until it’s dripping. He lets out a long, satisfied groan and begins to slow down, every rock of his hips like the promise of another climax.
“Don’t stop,” you whisper desperately. “Please don’t stop, I’m so close.”
He doesn’t open his eyes, but still he obliges; continuing to stroke into you as you squirm beneath him.
“Oh god,” you groan. “Harder. I need- harder.”
He grunts, screwing his eyes shut tightly, and begins pounding his cock into you with such force you can feel your body shifting up the mattress. You know he already came, you know how sensitive he must be. But somehow, knowing that makes this all the more delicious.
The electricity builds again, every thrust like a lightning strike through your core. Your legs begin to shake and you finally let go, giving in to the current and letting it course through you. Your orgasm is intense, sharp and tingly, making you shudder, body stiffening until it passes.
He slows to a stop, resting his full weight on top of you. You welcome the pressure, like a weighted blanket; warm and grounding, soothing the ache beginning to settle in your limbs.
After a few moments, he slides out of you carefully, rolling over to lie at your side. “You want that drink now?” he asks.
Hair sticks to your forehead with sweat, you brush it back, sucking in deep breaths as you stare up at the ceiling. “No, I’m good.”
Silence envelops you, neither one of you speaking again until your hearts stop thumping.
“So… I guess this means you’re going to approve the training for my method,” he says.
You turn your head, glaring at him in stunned silence.
“I’m kidding,” he says with a smile, greatly amusing himself.
“God, surgeons are assholes,” you mutter.
#doctor strange#doctor strange fanfiction#doctor strange smut#doctor strange x you#doctor strange x reader#stephen strange fanfiction#stephen strange smut#stephen strange x reader#stephen strange x you#stephen strange#surgeon strange#benedict cumberbatch#fanfiction#fanfic#smut#smut writing#lemon#Doctor strange oneshot
485 notes
·
View notes
Text
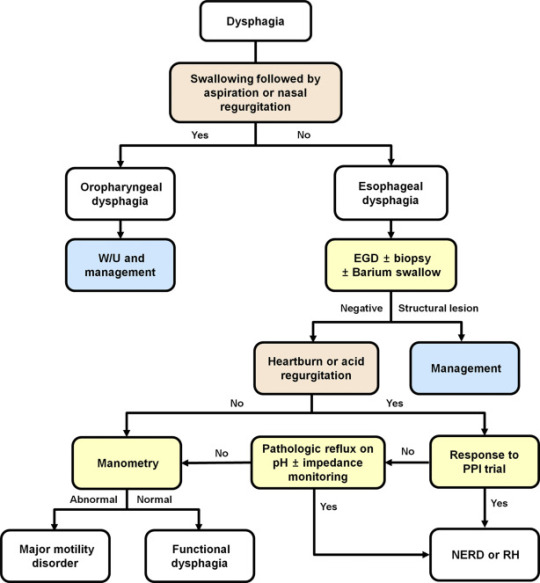
Explaining dysphagia
Dysphagia is simultaneously a symptom and a diagnosable condition. Most people think of it (if they think of it at all) as the choking on food disease but in reality it's much more complicated than that.
There are four categories of dysphagia: oropharyngeal, esophageal, esophagogastric, and paraesophageal
only two of those categories (oropharyngeal and esophageal) are commonly used and diagnosed so those are the main two I'll be talking about.
The diagnosis of dysphagia is a fairly complicated process involving a lot of radiological testing and things stuck up your nose and down your throat.
lost the source :(
source
the ICD 10 further divides dysphagia into unspecified, oral phase, oropharyngeal phase, pharyngeal phase, pharyngoesophageal phase, and other dysphagia which includes cervical dysphagia and neurogenic dysphagia
Oropharyngeal dysphagia
Oropharyngeal dysphagia occurs when someone has difficulty initiating a swallow. It's often accompanied by coughing, choking, feeling food stick in the throat, and nasal regurgitation. Other symptoms include frequent repetitive swallows, frequent throat clearing, a gargly voice after meals, hoarse voice, nasal speech and dysarthria, drooling, and recurrent pneumonia.
Oropharyngeal dysphagia is diagnosed with a modified barium swallow and/or a transnasal video endoscopy.
Some of the consequences of oropharyngeal dysphagia include aspiration pneumonia, upper respiratory infections, and weight loss. Common treatment includes rehabilitative swallowing exercises, botox, surgery, and/or a feeding tube.
Esophageal Dysphagia
Esophageal dysphagia is dysphagia where there is a problem with the passage of food or liquids through the esophagus between the upper and lower esophageal sphincter. Esophageal dysphagia is usually a result of abnormal motility in the esophagus or a physical obstruction to the esophagus. Symptoms of esophageal dysphagia vary depending on cause.
Motility: People with esophageal motility disorders will experience problems with swallowing both liquids and solids. Motility disorders consist of abnormal numbers of contractions in the esophagus, abnormal velocity of contractions, abnormal force of contractions, abnormal coordinated timing of contractions, or several of these simultaneously. People with esophageal motility disorders may also experience spasms or chest pain.
Obstruction: People with an esophageal obstruction will have more difficulty swallowing solids than liquids.
Some symptoms of both include pain when swallowing, the inability to swallow, sensation of food being stuck in your throat or chest, drooling, and regurgitation.
Esophageal dysphagia can be diagnosed with a barium swallow, upper endoscopy, esophageal manometry, and an endoFLIP.
Some common treatments for esophageal dysphagia include medication, esophageal dilation, surgery, stent placement, and/or a feeding tube.
Esophagogastric Dysphagia
Esophagogastric dysphagia occurs when there is a problem with material passing from the lower esophageal sphincter into the gastric fundus.
Paraesophageal Dysphagia
Paraesophageal dysphagia occurs when the esophagus is narrowed due to extrinsic compression.
The ICD 10 Classifications
Oral phase - difficulty moving food or liquid to the back of the throat
Oropharyngeal phase - difficulty initiating swallowing
Pharyngeal phase - difficulty swallowing when food or liquid is at the top of the throat
Pharyngoesophageal phase - unable to find information
Other dysphagia- cervical dysphagia (caused by problems with the cervical spine) or neurogenic dysphagia (caused by problems with the central or peripheral nervous system)
Sources
x x x
+ some others I definitely (/sarcasm) didn't lose the link to
93 notes
·
View notes
Text
As of October 15, 2024, CDC has released more than half of the anticipated 7.8 million entries of V-safe free-text entries. ICAN’s analysis of the entries released so far reveals almost 12,000 reports of kidney pain, kidney stones, or kidney infections.
As many of you already know, V-safe was developed by CDC for individuals to report symptoms after COVID-19 vaccination. This month, we decided to look at V-safe reports of kidney issues.
We know from other vaccines that vaccination can negatively affect kidney function, causing harm far from the injection site. Sadly, it doesn’t occur to most people that an injection in their arm can harm a distant system of their body. But as ICAN has reported again and again, all body systems can be impacted by vaccination.
A 2024 study found a “strong causal relationship” between COVID-19 vaccination and kidney diseases such as acute interstitial nephritis (inflammation of kidneys) and podocytopathy (injury to special cells in the kidney). A 2022 study found a correlation between acute kidney injury (AKI) and COVID-19 vaccination and that “AKI following the COVID-19 vaccines led to poor prognosis, with 19.78% death in the Pfizer-BNT group, 17.78% in MODERNA, and 12.36% in JANSSEN.”
The V-safe app entries—most made in just the first few days and weeks following vaccination—reveal many reports of kidney pain, the abrupt development of kidney stones, and hospitalization for kidney infections. Here are a few examples:
“Infection of Kidneys and UTI. Blood in urine and kidney stone on left kidney.”
“I’m in the hospital right now Because I’m still peeing blood they think it’s kidney stones.”
“Kidney stone requiring emergency surgery, ureteral stent placement and subsequent removal; UTI.”
“Intermittent stabbing, pulsing pain around left kidney.”
“Severe flank pain (I think it’s a kidney stone) I’m in the ER”
“Diagnosis with new onset kidney stone”
“Severe kidney infection back pain fever”
Readers will not be surprised to learn CDC doesn’t recognize kidney issues as adverse events related to COVID-19 vaccination, despite CDC’s access to this same V-safe data in real time as the vaccines were rolled out. ICAN will continue to do CDC’s job for it and bring attention to these dangerous and sometimes life-threatening conditions.
28 notes
·
View notes
Note
HAPPY INTERNATIONAL LESBIAN DAY to you my friend!!!
My name is B. A closeted lesbian who's looking to come out to her family this month. In my almost two years of existence on this blog, I've read different “coming out stories” which has been a whole motivation to me- I hereby set a day in mind, to come out to my family. However things took a turn as my mom who i thought would be free of her ovarian cancer by said date developed a kidney problem just after ovarian cancer- she means the whole world to me and her acceptance is what I yearn for with my coming out. She has always said we should allow her die and has been unmotivated about life until her birthday few weeks ago (sept 11) where a whole lot of people on this app sent their good wishes, drawings, and words of encouragement to her. We turned everything sent into a blanket for her and she's been wrapping herself with the love she received- she wants to live again and fight for the sake of strangers who believed in her(so she said). The medical personnel admits it is the best time to have her surgery (Ureteral Stent Placement surgery) because she has the right mood and mindset. Unfortunately for us, we are 500$ away from getting her surgery, it’s almost a month after her birthday and her fighting spirit is dying- I also can't come out to a dying mother- I need her to be fine before my coming out date(20th Oct). We've created a crowdfunding link for her but we've only raised 160$ of 500$. On this OUR special day, Would you please help not only my mom but my coming out plan by donating whatever you can spare for my mom's surgery? No matter how small, This would go a longer way than you think- please click the link below to support I and my family:
buymeacoffee.com/Plantlover
You can also find more information about her Ovaria cancer/ infected kidney on my pinned post. Thank you for sticking with us through thick and thin.
...Honestly, I don't really trust you. The more I think about it, the less I trust you.
🚩International Lesbian Day is October 8th, not the 9th. I received this ask today, October 9th.
🚩I'm not a lesbian, nor have I ever referred to myself as one, but you're quite insistent that I help on, and I quote, "On this OUR special day," which...no. It's not my special day. It's the wrong day and I'm not a lesbian.
🟨The broken English is a little suspicious in this particular situation, considering we know nothing about you except that you're apparently a closeted lesbian and your mother's dying of cancer.
🚩I don't know any real information about you because, despite what you've claimed, you haven't provided any actual, solid evidence that you and your family are facing the things you say you are.
🚩For example of the point above, I feel it would be fairly easy for you to take a picture of a medical bill and censor important identifying details. But you haven't even done that.
🟨According to your archive, you've had your blog since May 2023. Of the 23 posts you made that month, 18 of them were on May 11th, and the remaining 5 were made on the 12th, after which you didn't post anything for 6 months.

After that, you posted 18 times in January 2024, but only on January 11th and January 15th. Then you stopped posting again for several months until May 2024, where you first start posting about your mother's cancer.

So, really, I'm not sure how long you've been on here and can only assume you started up around May 2023. Not a red flag, but a yellow one to me.
🚩🚩🚩Instead of using GoFundMe, which has donation protections, you use Buymeacoffee, which, if it works anything like Kofi, the money then goes to PayPal, which does not have donation protections. There's no donation protection for anyone attempting to give to you for your mother's cancer treatment.
Like, this isn't you asking for money to pay for groceries or something. You're asking for thousands on something that requires immediate attention.
That's not something I'd PayPal about, personally.
🚩In the initial posts you made, you don't put a maximum amount you need. You should already know how much your mother's cancer treatment and cervix removal would cost, even if you only requested an estimate. But you leave the posts open-ended for a long while.

🚩I find it strange that the issues you have with English in the ask you sent me are completely absent from your first posts. Are there different writers for these blog posts?
🚩Looking at your Buymeacoffee, you're currently asking for $500 and have apparently gained $225. Right now, each "plant" a person gives you is worth $5.

Now, Buymeacoffee lets you see how many people have donated and how much, in "coffee," or "plants" in this case, they gave you. However, this information on the page only goes back for the last 90 days.
90 days from today, Wednesday, October 9th, was Thursday, July 11, 2024.
Since this page has been active, according to your blog post, since at least May 3rd, 2024, the count below does not include all donations given to you.
I wasted some time looking back through all the donations and counting up the plants:
1, 10 3, 1, 5, 1, 1, 20, 5, 2, 3, 1, 5, 5, 5, 2, 5, 5, 1, 12, 10, 5, 1, 3, 1, 1, 3, 30, 3, 2, 2, 5, 3, 1, 5, 2, 1, 2, 10, 3, 6, 2, 5, 5, 3, 1, 1, 3, 3, 3, 1, 3, 2, 1, 3, 10, 15, 5, 5, 3, 1, 5, 1, 15, 5, 1, 1, 2, 1, 1, 1, 1, 3, 10, 1, 15, 1, 3, 3, 3, 3, 1, 1, 3, 20, 5, 1, 3, 5, 2, 1, 3, 3, 2, 3, 3, 5, 5, 2, 100, 3, 1, 1, 5, 2, 5, 1, 5, 15, 15, 3, 3, 5, 1, 5, 5, 3, 3, 1, 3, 10, 3, 3, 5, 1, 4, 1, 3, 1, 5, 3, 4, 5, 10, 10, 3.
You have been given 136 donations on this page since July 11th, 2024 The sum of all the "plants" given is 667.
667 * 5 = 3335
You have been given at least $3,335 within the last 90 days.
That's not counting the $45 you said your sister got before her account was closed, nor the fact the minimum giving amount was initially $10 before you decreased it to $5, nor the fact the count only accounts for "plants" given between May 3rd and July 10th.
Why does Buymeacoffee only show that you've gotten $225 out of $500? That's likely because, if it functions like Kofi, you can refresh your goals and set new ones despite previous giving.
Is the list of people I saw for the entirety of the current goal in the last 90 days? Do you have other accounts you're receiving donations to with various stories? When does Buymeacoffee count different goal sets?
That's difficult to ascertain, which is why it's not an optimal space for giving someone donations for medical procedures.
First, people gave you money for a cervix removal, then they gave you money to help for kidney treatment, which you instead put toward "a blanket for her" to give your mother "hope," and now you're asking for more money for the kidney situation again.
Why Aren't You Using GoFundMe?
Why Are You Making It Difficult To Trace Information Outside Of What You Say?
...I don't trust you. I really don't.
I have even more red flags (like how you ignored someone's explicit request to not receive any donation asks), but I think I've given enough of them. I won't waste more of my time looking into this.
I cannot guarantee that this is a scam, but I don't recommend anyone else donate to you unless you start providing hard evidence of the things you say you're doing:
⭕Provide photos of medical bills you've paid for using the funds given to you.
⭕Provide photos of your mother's medical estimates.
⭕Send a photo of the blanket, and/or a picture of your mother under the blanket, and/or a photo of the blanket with a piece of paper with your Tumblr name written on it along with a receipt for the blanket/materials to make the blanket. If you photograph your mother, you can censor her face if you so choose.
⭕Leave Buymeacoffee and set up a GoFundMe, which will allow people to more easily monitor what you've been given and where it's going. It will also provide donation protections for the people giving to you.
If anyone else has ideas of reasonable ways for someone to prove their request is legitimate, feel free to add them in the replies or as a reblog.
35 notes
·
View notes
Text
Astro Observations
✩7th lord in 2nd house can mean your partner is frugal and may not share his resources with you.
✩Venus in 4th house could drive a luxury car.
✩Rahu in 7th house could have an inter religion cross cultural marriage.
✩7th lord in 6th house could marry a Virgo rising or Virgo Moon.
✩Planets in Ardra star can be a major disappointment especially during rahu Dasha.
✩Sun Mars can cause operation in the heart (Stent placement etc)
For Readings, Please DM
#astrology#astrology observations#zodiac#zodiac signs#astro community#astro observations#vedic astrology#astro notes#vedic astro notes#astrology community#sun in astrology#venus in astrology
197 notes
·
View notes
Note
HAPPY (Post)-INTERNATIONAL LESBIAN DAY to you my friend!!!
My name is B. A closeted lesbian who's looking to come out to her family this month. In my almost two years of existence on this blog, I've read different “coming out stories” which has been a whole motivation to me- I hereby set a day in mind, to come out to my family. However things took a turn as my mom who i thought would be free of her ovarian cancer by said date developed a kidney problem just after ovarian cancer- she means the whole world to me and her acceptance is what I yearn for with my coming out. She has always said we should allow her die and has been unmotivated about life until her birthday few weeks ago (sept 11) where a whole lot of people on this app sent their good wishes, drawings, and words of encouragement to her. We turned everything sent into a blanket for her and she's been wrapping herself with the love she received- she wants to live again and fight for the sake of strangers who believed in her(so she said). The medical personnel admits it is the best time to have her surgery (Ureteral Stent Placement surgery) because she has the right mood and mindset. Unfortunately for us, we are 500$ away from getting her surgery, it’s almost a month after her birthday and her fighting spirit is dying- I also can't come out to a dying mother- I need her to be fine before my coming out date(20th Oct). We've created a crowdfunding link for her but we've only raised 225$ of 500$. On this OUR special day, Would you please help not only my mom but my coming out plan by donating whatever you can spare for my mom's surgery? No matter how small, This would go a longer way than you think- please click the link below to support I and my family:
buymeacoffee.com/Plantlover
You can also find more information about her Ovaria cancer/ infected kidney on my pinned post. Thank you for sticking with us through thick and thin.
Hello!
I am kind of struggling with money lately… I am so very sorry, but I hope I can donate at least something to you before the 20th of October!!! I’ll try my best!!!
And I so hope someone will see this and donate, or at least reblog! I wish the best to your mother and to you as well. I wish she fine the strength to keep fighting, that you get some money and that you both can be happy ❤️
@deliciousmentalityballoon276
@lgbtqnationofficial @queerism1969 @tyyjaimiee
16 notes
·
View notes
Note
Happy international lesbian day to you my friend!!!
My name is B. A closeted lesbian who's looking to come out to her family this month. In my almost two years of existence on this blog, I've read different “coming out stories” which has been a whole motivation to me- I hereby set a day in mind, to come out to my family. However things took a turn as my mom who i thought would be free of her ovarian cancer by said date developed a kidney problem just after ovarian cancer- she means the whole world to me and her acceptance is what I yearn for with my coming out. She has always said we should allow her die and has been unmotivated about life until her birthday few weeks ago (sept 11) where a whole lot of people on this app sent their good wishes, drawings, and words of encouragement to her. We turned everything sent into a blanket for her and she's been wrapping herself with the love she received- she wants to live again and fight for the sake of strangers who believed in her(so she said). The medical personnel admits it is the best time to have her surgery (Ureteral Stent Placement surgery) because she has the right mood and mindset. Unfortunately for us, we are 500$ away from getting her surgery, it’s almost a month after her birthday and her fighting spirit is dying- I also can't come out to a dying mother- I need her to be fine before my coming out date(20th Oct). We've created a crowdfunding link for her but we've only raised 85$ of 500$. Would you please help not only my mom but my coming out plan by donating whatever you can spare for my mom's surgery? No matter how small, This would go a longer way than you think- please click the link below to support I and my family:
buymeacoffee.com/Plantlover
You can also find more information about her Ovaria cancer/ infected kidney on my pinned post. Thank you for sticking with us through thick and thin.
.
8 notes
·
View notes
Note
Hi friend, how are you doing today? My name is Bee, you probably get a lot of asks from bots and scammers which can be frustrating(I do too😁), but I promise this is different:
Although sending this message was born out of frustration and helplessness, I’m willing to prove myself to a reasonable extent if you want(Send me a message). My Mom who’s been our cornerstone since the death of our dad(I was a kid) has been fighting ovarial cancer. We’ve done everything possible to beat the cancer until few months ago when we got a news that it has affected her kidney. She told us to let her die, but we are not giving up on her- she celebrated her birthday a few days ago- where a lot of people on tumblr sent their well wishes and good will messages. We turned all the messages and wishes into a blanket for her and that act made her want to live again. She said she’s ready to fight for the random strangers that believed in her. Now she needs a Ureteral Stent Placement surgery and she’s ready to fight, but we, on the other hand, can’t afford to get the surgery done at the moment as we need at least $1200 to what we already have to begin the surgery. It’s more than a week after her birthday (Sept. 11) and her fighting spirit is starting to dwindle. We need all the support we can get before she reverts to her dying state of mind. Please do help us with whatever you can via my pinned post(I don want to add a link to avoiding being banned for sharing links). And if you can’t, please don’t hesitate to spread the word to people who can via a reblog on my pinned post. If you have any questions or comments please send me a message and I will reply as soon as I can. Thanks for taking your time to read this. Stay blessed🫶🏻
Aye, take care. Link to your pinned post.
11 notes
·
View notes
Note
HAPPY LGBT HISTORY Month to you my friend!!! Hope you had a great international lesbian day(Oct 8) and Coming out Day (Oct 11). I'm writing you as a QUEER to a fellow QUEER.
My name is B. A closeted lesbian who's looking to come out to her family this month. In my almost two years of existence on this blog, I've read different “coming out stories” which has been a whole motivation to me- I hereby set a day in mind, to come out to my family. However things took a turn as my mom who i thought would be free of her ovarian cancer by said date developed a kidney problem just after ovarian cancer- she means the whole world to me and her acceptance is what I yearn for with my coming out. She has always said we should allow her die and has been unmotivated about life until her birthday few weeks ago (sept 11) where a whole lot of people on this app sent their good wishes, drawings, and words of encouragement to her. We turned everything sent into a blanket for her and she's been wrapping herself with the love she received- she wants to live again and fight for the sake of strangers who believed in her(so she said). The medical personnel admits it is the best time to have her surgery (Ureteral Stent Placement surgery) because she has the right mood and mindset. Unfortunately for us, we are 500$ away from getting her surgery, it’s almost a month after her birthday and her fighting spirit is dying- I also can't come out to a dying mother- I need her to be fine before my coming out date/birthday(20th Oct). It's just 2 days to my birthday and we've only raised 285$ of 500$. On this special Month, Would you please help not only my mom, but also my coming out plan by donating whatever you can spare for my mom's surgery? No matter how small, This would go a longer way than you think- please click the link below to support this gay woman (I) and my family:
buymeacoffee.com/Plantlover
You can also find more information about her Ovaria cancer/ infected kidney on my pinned post. Thank you for sticking with us through thick and thin.
#angelicmelon#leasebound#leaseboundweek2024#fuck you rusty leasebound#queer artist#trans artist#disabled artist#autistic artist#artists on tumblr#art
5 notes
·
View notes
Note
Hi friend, how are you doing today? My name is Bee, you probably get a lot of asks from bots and scammers which can be frustrating(I do too😁), but I promise this is different:
Although sending this message was born out of frustration and helplessness, I’m willing to prove myself to a reasonable extent if you want(Send me a message). My Mom who’s been our cornerstone since the death of our dad(I was a kid) has been fighting ovarial cancer. We’ve done everything possible to beat the cancer until few months ago when we got a news that it has affected her kidney. She told us to let her die, but we are not giving up on her- she celebrated her birthday a few days ago- where a lot of people on tumblr sent their well wishes and good will messages. We turned all the messages and wishes into a blanket for her and that act made her want to live again. She said she’s ready to fight for the random strangers that believed in her. Now she needs a Ureteral Stent Placement surgery and she’s ready to fight, but we, on the other hand, can’t afford to get the surgery done at the moment as we need at least $1200 to what we already have to begin the surgery. It’s more than a week after her birthday (Sept. 11) and her fighting spirit is starting to dwindle. We need all the support we can get before she reverts to her dying state of mind. Please do help us with whatever you can via my pinned post(I don want to add a link to avoiding being banned for sharing links). And if you can’t, please don’t hesitate to spread the word to people who can via a reblog on my pinned post. If you have any questions or comments please send me a message and I will reply as soon as I can. Thanks for taking your time to read this. Stay blessed🫶🏻
👆
6 notes
·
View notes
Text
Heart Care Centre In Gorakhpur
When it comes to maintaining overall health, few things are as vital as taking care of your heart. As the heart continues to be one of the most critical organs in our body, any issues related to it must be taken seriously. In Gorakhpur, the demand for quality heart care services has risen significantly, as people are becoming more aware of the importance of cardiovascular health. Fortunately, Gorakhpur is home to some of the best heart care centre, where patients can receive expert treatment and guidance on managing heart conditions.
In this blog, we’ll explore the best heart care centre in Gorakhpur, the services they offer, and why you should choose them for your heart health needs.

Heart diseases continue to be one of the leading causes of death worldwide. In India, the rise of lifestyle diseases such as hypertension, diabetes, and high cholesterol has contributed to an increase in heart-related problems. Early diagnosis and intervention are key to managing heart conditions effectively. This is where a good heart care centres comes into play. Heart care centres are equipped with advanced technology, skilled cardiologists, and modern facilities to provide accurate diagnosis, treatment, and preventive care for a wide range of heart diseases.
Services Offered at Heart Care Centres in Gorakhpur
Heart care centres in Gorakhpur provide a variety of services, ranging from preventive care to advanced treatment options. Here are some of the key services you can expect:
1. Cardiology Consultations
A heart care centre begins with consultations with experienced cardiologists who assess your symptoms, medical history, and risk factors. These consultations often involve a thorough examination and may be followed by diagnostic tests to understand the root cause of any heart issues.
2. Comprehensive Diagnostic Tests
Accurate diagnosis is the first step toward effective treatment. Heart care centres in Gorakhpur offer state-of-the-art diagnostic tools such as:
Electrocardiogram (ECG)
Echocardiogram (ultrasound of the heart)
Stress tests
Holter monitoring
Angiography and angioplasty
These tests help identify underlying conditions like heart disease, arrhythmias, blocked arteries, and more.
3. Cardiac Surgery and Interventions
For patients with severe heart conditions, heart care centres in Gorakhpur offer surgical interventions such as:
Coronary Artery Bypass Grafting (CABG)
Valve replacement or repair
Angioplasty and stent placement
These procedures are performed by expert cardiac surgeons who specialize in heart-related surgeries, ensuring the best outcomes for patients.
4. Preventive Care and Health Monitoring
Heart care centres emphasize preventive care to help individuals avoid heart disease. They provide services like:
Routine health check-ups
Blood pressure and cholesterol monitoring
Lifestyle counseling (diet, exercise, stress management)
Weight management and smoking cessation programs
By focusing on prevention, these centres help patients lower the risk of heart disease and maintain a healthy lifestyle.
5. Cardiac Rehabilitation
After a heart attack or surgery, patients require a rehabilitation program to recover fully. Cardiac rehabilitation involves supervised exercise, diet counseling, and psychological support to help individuals regain strength and reduce the risk of further complications.
Why Choose a Heart Care Centre in Gorakhpur?
1. Expert Cardiologists
Heart care centres in Gorakhpur are staffed by experienced and qualified cardiologists who specialize in diagnosing and treating a wide range of heart conditions. Whether you’re dealing with high blood pressure, irregular heartbeats, or more severe conditions like coronary artery disease, these professionals provide the best possible care.
2. State-of-the-Art Facilities
The heart care centres in Gorakhpur are equipped with the latest technology, including high-resolution imaging systems, advanced cardiac monitoring tools, and cutting-edge surgery equipment. This allows doctors to provide accurate diagnoses and offer effective treatment options for heart patients.
3. Personalized Care
Each patient is unique, and heart care centres understand the importance of providing personalized care. From the first consultation to post-treatment care, cardiologists work with patients to create tailored treatment plans that suit their individual needs and health goals.
4. Comprehensive Approach
These centres offer a comprehensive range of services under one roof, ensuring that all aspects of heart health are addressed. From diagnostic tests and treatment options to preventive care and rehabilitation, you can count on the heart care Centres in Gorakhpur to support your heart health journey.
Best Heart Care Centre in Gorakhpur.
Gupta Heart Care Centre in Gorakhpur
This Centre are well-known for their experienced team of cardiologists, use of advanced medical technology, and focus on patient well-being.
Conclusion
Taking care of your heart is an essential aspect of living a long and healthy life. If you're experiencing any symptoms of heart disease or if you simply want to ensure your heart health is in check, it’s time to consult a trusted heart care centres in Gorakhpur. With world-class doctors, top-notch facilities, and comprehensive treatment options, you can rest assured that your heart is in safe hands.
Remember, early detection and intervention can save lives. Don’t wait for symptoms to worsen—schedule a consultation at one of Gorakhpur’s leading heart care centres today.
Call to Action: If you or someone you know is concerned about their heart health, don't delay. Contact a reliable Heart Care Centre in Gorakhpur for an assessment and start your journey toward a healthier heart today
2 notes
·
View notes