#Plastic Surgery Beirut
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Total funding amounts to $125.3M.
Text
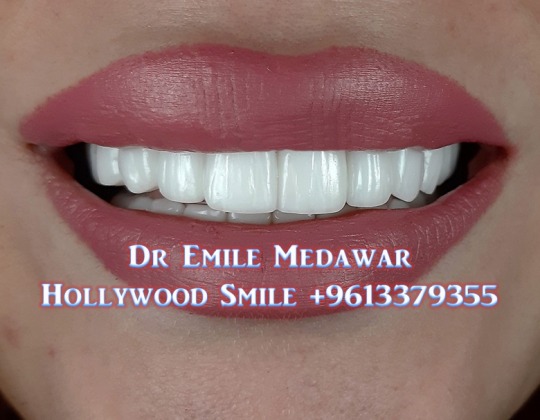
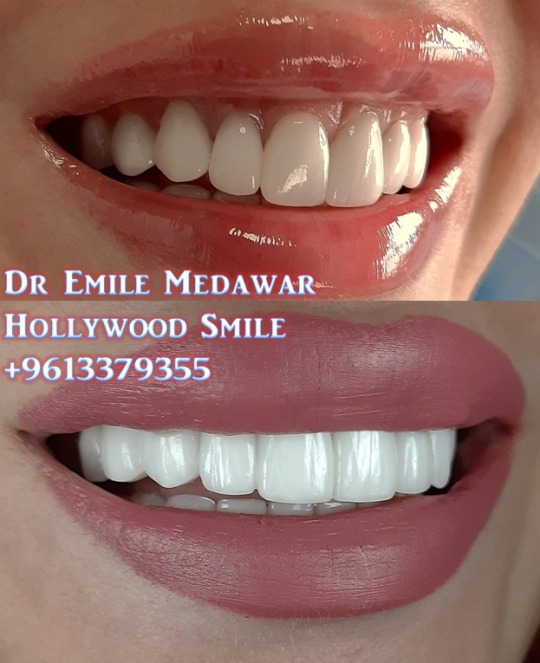
Ultra-Thin Porcelain Veneers, Dr Emile Medawar, Cosmetic Dentist, Dental Implants Surgeon, Oral Surgery Specialist, 00 961 3 379355, 00 961 3 081774.
#hollywood smile#dentist#veneers#hollywood smile beirut#hollywood smile lebanon#Veneers Beirut#Veneers Lebanon#Smile Beirut#Smile Lebanon#Aesthetic Lebanon#Aesthetic Beirut#Hollywood Smile Beirut#Hollywood Smile Lebanon#Rhinoplasty Beirut#Rhinoplasty Lebanon#Blepharoplasty Beirut#Facial Plastic Surgery Beirut
2 notes
·
View notes
Text
Dr Emile Medawar, Cosmetic Dentist, Dental Implants Surgeon, Oral Surgery Specialist, 00 961 3 379355, 00 961 3 081774.

Ultra-Thin Porcelain Veneers, Dr Emile Medawar, Cosmetic Dentist, Dental Implants Surgeon, Oral Surgery Specialist, 00 961 3 379355, 00 961 3 081774.
Dr Emile Medawar, Cosmetic Dentist, Dental Implants Surgeon, Beirut, Lebanon, 00 961 3 379355, 00 961 3 081774.
Dr Emile Medawar, Cosmetic Dentist, Dental Implants Surgeon, Beirut, Lebanon, 00 961 3 379355, 00 961 3 081774.
#veneers#dental veneers#hollywood smile#hollywood smile beirut#hollywood smile lebanon#hollywood smile cost beirut#porcelain veneers#porcelain veneers beirut#porcelain veneers cost beirut#veneers beirut#Lip Fillers#Lip Fillers Beirut#Fillers#Fillers Beirut#Ultra-Thin Porcelain Veneers#Aesthetic#Facial Plastic Surgery#Aesthetic Beirut#Aesthetic Lebanon#Cosmetic Beirut#Cosmetic Lebanon
0 notes
Text
Stunning Nosejob Transformations By Dr Charbel Medawar, Plastic Surgery Lebanon.
Get the Nose Of Your Dreams With Lebanon's Best Rhinoplasty Surgeon.
📅📱+96170610469
📍🏥 Style Beauty Clinic, Beirut, Facing Hilton Hotel
#rhinoplasty #rhinoplastybeforeandafter #rhinoplastie #nosejob #nosejobbeforeandafter #nosejobs #septoplasty #rhinoseptoplasty #septorhinoplasty #revisionrhinoplasty #rhinoplastyexpert #plasticsurgery #cosmeticsurgery
instagram
#beirut#cosmetics#lip fillers#lebanon#blepharoplasty#plasticsurgery#marketing#google#browlift#rhinoplasty#Instagram
0 notes
Text
DEAR - KOREAN - GIRLS,
HIROSHIMA - AND - NAGASAKI
WORLD's - FIRST - ATOMIC YES
BOMBING - HAPPENED - TRUE
4 A - REASON - DEAR - KOREA,
TOKYO - JAPANESE - BOYS
AND - GIRLS - DURING HER
NIGHT - OFF - AS - PINAY
EXOTIC - DANCER - KICKED
HER - BOXED - HER - THESE
BOYS - AND - GIRLS - ORGY
ALL - THE - TIME - HEROINE
COCAINE - BEAT - HER - YES
BOYS - STABBED - STABBED
AFTER - AND - GIRLS - SAID
CAN - WE - JOIN - STABBED
HER - CORONARY - JOINED
THEM - 'CORONARY - HEART
FAILURE' - AS - JAPAN - GOT
CHEAPEST - STORAGE SENT
PHILIPPINES - 2 - THEY CALL
GARBAGE - INSULIN - TRASH
UGLY - GIRLS - WHY - HEART
GOES - 2 - TOKYO - ORGY
TOKYO - GARBAGE - GOODS
TOKYO - WHISKEY - TRASH
TOKYO - SAID - PHILIPPINES
MUST - DO - MAKE UP - IN
RESTROOM - FULL - OF
JAPANESE - URINE - AND
POOP - MIAMI - ORGY AND
HEROINE - COCAINE - AS
TOTAL - STRANGERS - DO
IT - STANDING - UP - BLKS
WANTED - VAGINA - LOOKING
FR - TENT - BEHIND - ME - AS
BLK - MALE - THERE - WANTED
2 - HUG - ME - PUT - HIS - PEE
PEE - ON - MY - THIGHS - HUG
WHO - HAS - FIANCE
USA - DUMPS - WITH URINE
AND - POOP - RESTROOMS
PUT - YOUR - MAKE UP - DO
CUT - YOUR - NAILS - IN USA
TOKYO - RESTROOMS FULL
OF - JAPANESE - URINE AND
POOP - LESBIANS - KISSING
EACH - OTHER - RAPING
DEAR - KOREAN - GIRLS,
TOKYO - JAPAN - SAID - KR
KOREAN - GIRLS - UGLIER
THAN - RAMEN - MARUCHAN
NOODLES - UGLIER - THAN
THEIR - TOILETS
KOREAN - GIRLS,
WE - WILL - BUY - YOUR
SHISEIDO - COSMETICS
EACH - ONE - 500 BILLION WON
TAX - PAID - SHISEIDO - THE
OLDEST - COSMETICS
CAPITAL - IN THE - WORLD
DEAR - WORLD,
WE - WILL - BUY - YOUR
SHISEIDO - COSMETICS
PINAYS - SELL - US - YOURS
THEY - SAID - YOUR - BIG SUSU
WHY - U - WIN - BEAUTY - YES
CONTESTS - TRUE
DEAR - PINAYS,
MY - TOKYO - JAPAN - MALE
SCIENTISTS - SURGEONS
OPERATING - PLASTIC
SURGERY - IN -
HONG KONG - ISLAND
TAX - FREE
SEOUL - SOUTH - KOREA
TOKYO - GIRLS - TOKYO
FEMALE - POLICE - TOKYO
BOYS - CALL - PREGNANT
FEMALES - FAT - PIGS
FAT - TUB - UGLY - FAT
BIG - HUGE - UGLY BOOBS
DEAR - KOREA - & - PINAYS,
JAPAN - 4 FT - TALL - 5 FT
TALL - LACK - OF - HEIGHT
UGLIEST - ADULT - JAPANESE
IMMOROAL - GIRLS - WHEN
WAS - LAST - TIME - THEY
WON - MISS EARTH
MISS UNIVERSE - EXTREMELY
UGLY - JAPANESE - GIRLS ARE
REAL - UGLY
TOKYO - MEN - SAYING
UGLY - WOMEN - PUT YOUR
MAKE UP - IN - RESTROOMS
FULL - OF - JAPANESE - POOP
AND - URINE
DEAR - KOREA,
JAPAN - HATES - CHINA
BEIJING - AND - SHANGHAI
KOREA - TOKYO - HAS - THE
CHEAPEST - HOTELS - IN THE
WORLD - DEAR - CHINA - AND
KOREA - LET's - BEAT - TOKYO
HDG - INNS
$0.25 - PER - DAY - TAX - FEES
INCLUDED - BEIJING - AND YES
SHANGHAI - LET's - MAKE
CHINA - AND - KOREA
INDIA - THEY - SAID - YOUR
WOMEN - ARE - UGLIER THAN
BROWN - SANDWICH - BAGS
TOKYO - STABS - 2 - DEATH
TOKYO - FEMALES - WEARING
JEWELRY
DEAR - INDIA,
SELL - US - YOUR - GARBAGE
SHISEIDO - COSMETICS
500 BILLION - WON
INDIA - WOMEN - JAPAN SAYS
U - HAVE - SAGGING - BREASTS
JEWELRY - YOUR - ONLY - YES
ATTRACTION
DEAR - INDIA,
ME - AND - MY - CHINESE
ACTOR - MARRYING - IN
PARIS - FRANCE
BEIRUT - WEDDINGS
WE'RE - MARRYING - IN
BEAUTIFUL - VINEYARDS
WE'RE - NOT - MARRYING
IN - GARBAGE - TOKYO
FEMALES - PUT - YOUR
MAKE UP - WHERE - TOKYO
FEMALES - URINE AND POOP
INDIA - HOTELS
HDG - INNS - COMING
$0.25 - PER - NIGHT - YES
CHECK IN - 24/7 - HOLIDAYS
INDIA - TONGUES
500 BILLION
SING - TONGUES - 500 BILLION
DEAR - INDIA,
CHANGE - YOUR - LAWS
I - WILL - GLADLY - B - YOUR
2ND - PRIME - MINISTER
ME - SECRETLY
SERENE - PRINCESS - KATARINA
KRISTIANA - MARIE CONSTANCE
BAILEY - DIRECTLY - FR - THE
QUEEN - MARY - OF - SCOTTS
SCOTLAND - LOOK - ALIKES
WERE - BEHEADED - PRISONED
FRANCE - I'M - DIRECTLY - FRM
KING LOUIS - LAST - OF FRANCE
DIRECT - DESCENDANT - OF
SIR PATRICK HENRY - USA
RELATIVES - 2 - PRODUCE
JULIUS CAESAR
KING - ALEXANDER - OF
ANCIENT - GREECE
IF - U - WANT - I - CAN - B
1 YEAR - ONLY
2ND - FEMALE - PRIME
MINISTER - OF - FRANCE
3RD - IVANKA TRUMP
WILL - U - ALLOW - US - BUT
NO - RESIDENCY
SPECIFIC - JOBS
JESUS - IS - LORD - INDIA
1 note
·
View note
Text
0 notes
Photo

Dr. Karim Sarhane is an MD MSc graduate from the American University of Beirut. Following graduation, he completed a research fellowship at Johns Hopkins University (Maryland, USA) in peripheral nerve surgery. He then completed a residency in general surgery at the University of Toledo (Ohio, USA), followed by a year of additional training in plastic surgery. He then joined Burjeel Royal Hospital in September 2022 (after spending a total of 10 years in the USA). He is a Diplomate of the American Board of Surgery. Dr. Sarhane is a Surgeon-Scientist who combines clinical care with scientific research to deliver the best possible outcomes to his patients. He is published in top-ranked bioengineering, neuroscience, and surgery journals. He holds a patent for a novel Nanofiber Nerve Wrap that he developed with his colleagues at the Johns Hopkins Institute for NanoBioTechnology and the Johns Hopkins Department of Neuroscience (US Patent # 10500305, December 2019). He is the recipient of many research grants and research awards, including the best basic science paper at the Johns Hopkins Surgery Research Symposium, the basic science research grant prize from the American Foundation for Surgery of the Hand, the Research Pilot Grant Prize from the Plastic Surgery Foundation, and a Scholarship Award from the American College of Surgeons. He has authored to date 49 peer-reviewed articles, 11 book chapters, and 48 peer-reviewed abstracts, and has 29 national presentations. Dr. Sarhane is recognized by colleagues for his commitment to medicine, his superior surgical skills, his compassionate care, and his innovative mindset. He strives to advance surgical care through excellence in research, education, clinical care, and service. He is proud to offer the patients of the UAE the entire gamut of general and laparoscopic/robotic surgery. He is also one of the pioneer surgeons to perform migraine surgery (a new and highly effective therapeutic modality for patients suffering from intractable migraines). His areas of expertise include,
0 notes
Text
Kinds of Cosmetic Procedures you never knew!
The main focus of cosmetic surgery is to enhance the patient’s appearance. Cosmetic surgery is entirely elected by the patient and not recommended by healthcare professionals or surgeons. Think thoroughly before opting for any kind of cosmetic procedure. These surgeries would help you enhance your looks, boost your confidence and help you in re-building your identity. There are different types of cosmetic procedures which will enhance your body. Some of them are listed below:
1. Facial procedures are undertaken mostly to enhance the face. Some popular facial procedures that are performed to rejuvenate or refine your face are as follows: Facelift, Eyelid lift, Rhinoplasty, Neck contouring, Brow lift, Chin implants, Lip enhancement, etc.
2. Cosmetic breast surgery will help you get the best breast shape and size. Some of the popular breast procedures are breast augmentation, breast lift, breast reduction, etc. This is especially beneficial for breast cancer survivors too.
3. Body cosmetic surgery, Lebanon will help you refine your proportions, improve your body shape, and experience the benefits of having a perfect body that you are proud to show off. Some popular body procedures are as follows: liposuction, tummy tuck, mommy makeover, male chest reduction, skin removal surgery, feminine rejuvenation, and Brazilian butt lift.
4. There are also a wide range of nonsurgical procedures like injectables, laser treatment, and professional skin care treatments to choose from. These procedures are mainly done to improve the appearance of the skin, reduce wrinkles, and clear away any visible signs of aging. Some popular nonsurgical procedures include Botox-type injectables, injectable fillers, skin resurfacing, nonsurgical fat reduction, skin tightening, and cellulite reduction.
Whether it is a cosmetic surgery or a Plastic surgery in Lebanon, going under the knife is extremely risky and scary. You cannot take a chance by trying out various procedures as you’d be putting your looks and appearances on stake. Ensure that you learn about it thoroughly, consult various experts, and get it done from the experienced professionals for the desired outcome. Although there are numerous surgeons out there, select a famous and the most experienced one for your plastic surgery in Beirut.
1 note
·
View note
Text
A Feminist Approach To Critical Spatial Practice
At the Woman’s Day we honor women architects who have been obscured and ripped off any recognition for their contribution in the architectural practice.

Poster celebrating the Women’s Day in Germany was banned in 1914.
Today we celebrate women architects whose practice is largely contributing to the discussion of the relationship of gender and space and whose references to feminism are made clear and bold through their work. Five contemporary practices and initiatives that are promoting a feminist approach to critical spatial practice and pioneering in different forms of feminist activism in architecture industry and discourse will be presented.
The establishment of practices emphasises the urgency of representation of woman in architecture, the rebellion towards sexism and the strive for diversity. Their approaches do not only unfold into theoretical discussions inside the academia but as well suggest different forms of actions in practice. Nevertheless they put forward issues such as oppression, marginalization and labor exploitation.

F-architecture is a research enterprise co-founded by Gabrielle Printz, Virginia Black and Rosana Elkhatib in Brooklyn, New York. | Photo by © Casey Carter
Feminist Architecture Collaborative is a three-woman research enterprise aimed at disentangling the contemporary spatial politics of bodies, intimately and globally. Their projects traverse theoretical and activist registers to locate new forms of architectural work through critical relationships with collaborators across continents and an expanding definition of Designer.

One of the most recent exploration of f-architecture took the shape of Cosmo-Clinical Interiors of Beirut at VI PER Gallery in Prague. | Photo by © Peter Fabo

Installation view of f-architecture, Cosmo Clinical Interiors, VI PER Gallery, Prague. | Photography by © Peter Fabo
Cosmo-Clinical Interiors of Beirut examines the constructed space, interior finishes, and designed protocols of the plastic surgery clinic to make perceptible its role in shaping subjects, virginity culture and an ideal body. The exhibition is probing the medical-cosmetic industry where cultural ideas of virginity are hacked and commodified through hymenoplasty and prosthetic hymens. The architecture is understood as the confluence of the technological, social, and economic—not a built fact, but an organizing force in a constellation of produced and productive objects.

Black Females in Architecture (BFA) encourages diversity in architecture via organized workshops and sharing advice on WhatsApp. | Photo via Dezeen
Black Females in Architecture (BFA) is a network for black women in the built environment to gain access and support structures to develop and enhance their potential in the varying disciplines. The aim is to improve the statistics of black women in the fields of architecture, landscape architecture, planning, urbanism, engineering, sustainability etc. This is initiated through regular meet-ups, workshops, mentorship programmes and design projects.
It is founded by Selasi Setufe, Neba Sere, Alisha Fisher and Akua Danso, who met at an architecture event in London. Taken by surprise by the rarely encounter of other black women in such events in architecture, that afterwards they decided to found a network, which has now over 150 members that share their concern and suggestions through organised events and through their practice they are raising awareness of diversity in architecture.

Lori Brown was the only woman in some of her design studios when she was studying at the Georgia Institute of Technology. | Photo by © Connor Martin
Architexx is a non-profit organization for gender equity in architecture transforming the profession by bridging the academy and practice.The group was founded by Nina Freedman and Lori Brown. They created a cross-generational group of academics and practitioners dedicated to the advancement of all women-identified, non-binary, gender non-conforming, and allied individuals.
They encourage and promote the leadership and retention of women in the discipline with the redefinition what contemporary success is, how value is understood and compensated. With the increase of diversity they facilitate and support open dialogue, content, conversations, that will inspire a new generation of design professionals to see themselves as agents of change by looking at the past to see new ways forward.

“Now What?!” curators Andrea J. Merrett, Roberta Washington, Sarah Rafson, Lori A. Brown with Michele Gorman, Pratt Institute Liaison and exhibition designer. | Photo by © Sally Rafson.
Now What?! is the first exhibition to examine the little-known history of architects and designers working to further the causes of the civil rights, women’s, and LGBTQ movements of the past fifty years. The exhibition content, conversations, and stories will inspire a new generation of design professionals to see themselves as agents of change by looking at the past to see new ways forward.

Naomi Stead and Justine Clark outline the programs and tools for a more equitable profession. | photo by © Phuong Lee
Parlour was initiated as part of the Australian Research Council-funded research project Equity and Diversity in the Australian Architecture Profession; Women, Work, and Leadership. It brings together research, informed opinion and resources on women, equity and architecture in Australia. It seeks to expand the spaces and opportunities available to women while also revealing many women who already contribute in diverse ways. As activists and advocates they aim to generate debate and discussion. As researchers and scholars they provide serious analysis and a firm evidence base for change. As women active in Australian architecture they seek to open up opportunities and broaden definitions of what architectural activity might be.

Parlour Guides to Equitable Practice is an initiative for an equitable practice. The guide outlines the key issues facing women in architecture and provide positive, productive strategies for change.

Women and Spatial Practice an event at University of North London, Nov 2001.
Taking place is a group of 7 women artists and architects (Sue Ridge, Julia Dwyer, Doina Petrescu, Jane Rendell, Katie Lloyd Thomas, Jos Boys, Brigid McLeer, Helen Stratford, Miche Fabre Lewin, Angie Pascoe, Teresa Hoskyns). It is an ongoing space of discussion, investigation and exchange in which to explore new practices, and to imagine and speculate on new directions and strategies for change.

Three day Feminist School of Architecture at Sheffield University. | Photo via Talking Place
Talking Place began out of a shared interest in questions of gender and spatial practice. Through various private workshops and public events they have developed a collaborative way of working together, which explores and alters institutional space through temporary and participatory interventions and through spatial installations. Their working method is process based and open-ended and depends on site research and exchange with users.
---
Pioneer Architects XIII by Klodiana Millona

42 notes
·
View notes
Photo

حصريا Exclusive Look 10 Years Younger. احصل على وجه اصغر ب١٠ سنوات with Smile Lift ® Exclusively WorldWide developed by Dr.Habib Zarifeh Combining: - Plastic Surgery. - Cosmetic Dentistry Hollywood Smile. - Digital Dentistry. - TMJ Specialist. Few sessions in Few Days. Call Us Now: +96170567444 Http://www.SmileLift.com احصل على وجه اصغر ب١٠ سنوات حصريا في عيادات "سمايل إنفنتي" تقنية "سمايل ليفت" بالتعاون بين أطباء تجميل الاسنان وأطباء التجميل. Now In #Bahrain #Tunisia #Jeddah #Dubai #Beirut #Erbil #Senegal #Michigan #Morocco #Algeria #Hollywoodsmile #veneers #dentist #dentalclinic #smilelift #fashion #fashionblogger #Models #modeling #Smile #russia #russian #البحرين - #تونس - #جدة - #دبي #بيروت (at Smile Infinity Dubai) https://www.instagram.com/p/BvRG7IaghDE/?utm_source=ig_tumblr_share&igshid=n52ypb2385c2
#bahrain#tunisia#jeddah#dubai#beirut#erbil#senegal#michigan#morocco#algeria#hollywoodsmile#veneers#dentist#dentalclinic#smilelift#fashion#fashionblogger#models#modeling#smile#russia#russian#البحرين#تونس#جدة#دبي#بيروت
1 note
·
View note
Text
Refreshed Eyelids.
Blepharoplasty Specialist Dr Charbel Medawar Plastic Surgery Lebanon.
70/610469
📍 Style Beauty Clinic, Beirut, Sin el Fil , Facing Habtoor Hotel.
#blepharoplasty #blepharoplastysurgery #blepharoplastyuppereyelid #eyelidsurgery #eyelidlift #doubleeyelid #uppereyelidsurgery #explorepage✨ #beirutlebanon
instagram
0 notes
Photo

Fixing the scars of Beirut’s explosion One woman whose face was torn apart by the Beirut explosion, says free plastic surgery will help her forget the day.
0 notes
Video
youtube
Fixing the scars of Beirut's explosion - BBC News by BBC News One woman whose face was torn apart by the Beirut explosion, says free plastic surgery will help her forget the day. Romy Zahour Lauret, 30, was driving near the port with her husband when the blast hit. Dr Joe Baroud, a plastic surgeon in Beirut, has been offering free surgery to victims like Romy. Please subscribe HERE http://bit.ly/1rbfUog
0 notes
Text
Fixing the scars of Beirut's explosion
A plastic surgeon is offering free surgery to people like Romy, who was driving near the port when the blast hit. from BBC News - World https://www.bbc.co.uk/news/world-middle-east-53726427 from Blogger http://newshou03r.blogspot.com/2020/08/fixing-scars-of-beiruts-explosion.html
0 notes
Photo

Smile Lift is a combination between cosmetic dentistry, computerised dentistry and in some cases plastic surgery. It’s a simple procedure with No Anesthesia - No Drilling - No Pain. In Just Two Session with the Smile Infinity Z2 Generation! . Whatsapp our hotline Now at +96170567444. . See you in #Beirut #Dubai and all over the #world . #SmileInfinity Creating Beautiful Smiles all over the World! #Lebanon #Veneers #hollywoodsmile #SmileLift #habibzarifeh #dentist #cotedivoire #thisweekend #smile #dentalimplants #gummysmile #smile #abudhabi #uae #Abidjan #ivorycoast (at Smile Infinity Dubai) https://www.instagram.com/p/CSqgzsajcAR/?utm_medium=tumblr
#beirut#dubai#world#smileinfinity#lebanon#veneers#hollywoodsmile#smilelift#habibzarifeh#dentist#cotedivoire#thisweekend#smile#dentalimplants#gummysmile#abudhabi#uae#abidjan#ivorycoast
0 notes
Text
Lebanon, The Phoenix Of The Mediterranean.
Hoping That People Seize This Opportunity To Build A Better Future.
🇱🇧 🐦🔥 Rising From The Ashes, Stronger Than Ever.
.
.
#livelovelebanon #livelovebeirut #drcharbelmedawar #beauty #explore #lebanon #beirut
instagram
#beirut#lebanon#cosmetics#lip fillers#blepharoplasty#plasticsurgery#marketing#browlift#rhinoplasty#google#Instagram
1 note
·
View note
Photo

Fixing the scars of Beirut’s explosion A plastic surgeon is offering free surgery to people like Romy, who was driving near the port when the blast hit.
0 notes