#Medical Science Research Journals
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
28.6 is the average number of monthly visits per US mobile user.
Text
I think more people deserves to know this
Scientific papers are really expensive. No student can afford to have access to them. If you want to do a proper research, it is impossible to pay all the access to all the publishers that are out there. Because for one topic of your interest there are a lot of different publishers to talk about that.
Scihub is a site where you can find everything for free. It is basically piracy.
And oh i love pirates.
Scientific research should be accessible for everyone, for every type of research and for every level of education. It is not a race "i progress more than you", but should be a "we progress a humanity". Also it should be "we found this thing A is like this", "We also found A is like that and we also found B" and everyone can add a little to the research. If we don't have accesso to what other study units of other countries do, how we do progress?
It is true we need a lot of the same design of study to be certain of something, but sometimes there are too many identical studies, just because you don't know it was already there or you didn't know the same topic was being sudied by another country in the same period.
So yes Scihub is a pirate, but in this world, in this scientific world, it is the only one doing things right.
I will always use it and support it's ideal
22 notes
·
View notes
Text
Trisomy 18 and Microdeletion 18p Mosaicism: A case report and literature review by Chao-Chun ZOU in Journal of Clinical Case Reports Medical Images and Health Sciences
ABSTRACT
The trisomy 18 syndrome is a common chromosomal disorder due to the presence of an extra chromosome 18, either complete, mosaic trisomy or partial trisomy 18q. The mosaic trisomy 18 patients’ phenotype was extremely variable, from the absence of dysmorphic features to complete trisomy 18 syndrome. The phenotype of 18p deletion syndrome is variable and almost all survived. A 2-year-old girl was referred to our hospital due to growth delay. Mild dysmorphy including thin hair, frontal bossing, low set ears, broad-flat nose, nostrils slightly upward, downturned corners of the mouth, dysplasia teeth, small hands and fingers bilaterally was observed. The karyotype of peripheral leukocyte showed 46,XX, psu idic (18)(p11.2)[55]/46,XX, del (18)(p11.2)[45]. We report this case to add to our knowledge of the trisomy 18 and microdeletion 18p mosaicism.
Keywords: Trisomy 18, mosaic;18p microdeletion; Psychomotor retardation; Karyotype
INTRODUCTION
The trisomy 18 syndrome was first reported by Edwards et al in 1960, also known as Edwards syndrome. It is the second most common autosomal chromosomal disorder after trisomy 21(Down’s syndrome)due to the presence of an extra chromosome 18, which has three basic types: complete, mosaic and partial type (Edwards et al., 1960, Cereda and Carey, 2012,Mudaliyar and Mudaliyar, 2017). The syndrome presents a recognizable pattern of major and minor anomalies, significant psychomotor and cognitive disability are associated with high neonatal and infant morbidity and mortality. The estimated overall prevalence of trisomy 18 in live born is approximately 1/6, 000 to 1/8, 000 while the incidence in fetus is much higher, the difference is caused by fetal loss and pregnancy termination after prenatal diagnosis (Cereda and Carey, 2012, Rasmussen et al., 2003). The mosaic trisomy 18 usually means having more than one cell line in the individual, and it occurs in approximately 5 percent in all trisomy 18 patients (Fitas et al., 2013). The phenotypic manifestations are highly variable, from the absence of dysmorphic features to the complete trisomy 18 syndrome (Tucker et al., 2007). Since the clinical outcomes of complete and mosaic trisomy 18 can be different, it is of vital importance to achieve a correct diagnosis because of implications in medical management and genetic counselling. 18p deletion was first described by de Grouchy and colleagues in 1963 and was estimated to occur in approximately 1/50, 000 live born, which results from deletion of a part or full of the short arm of chromosome 18(Turleau, 2008). The mostly reported clinical features include cognitive impairment, congenital heart defects, small stature, minor facial dysmorphy, and skeletal deformities(Turleau, 2008, Xiao et al., 2019, Hasi-Zogaj et al., 2015, Yi et al., 2014)
Typical facial features include hypertelorism, ptosis, strabismus, broad–flat nose, micrognathia, and low-set big ears. Holoprosencephaly may be seen in approximately 10–15% of patients(Turleau, 2008). In addition, speech and language difficulties, pituitary abnormalities, generalized seizures, dystonia, and autoimmune diseases have also been described(Turleau, 2008, Rao et al., 2001, Graziadio et al., 2009, McGoey et al., 2011). However, these non-specific features are easily overlooked clinically. The clinical phenotype severity is related to the size and location of deletion region. In this report, we present a 2-year-old girl of mosaic trisomy 18 and 18p microdeletion with mild psychomotor retardation, cognitive impairment and language developmental disability.
Clinical description
A 2-year-old female second child of non-consanguineous parents was admitted to our hospital due to growth delay. Her mother and father were 34 years old and 38 years old when giving birth to her. She was born at full-term with uncomplicated gestation, her birth weight was 3.35 kg and the length was about 50 cm. No feeding difficulty and complications were referred in the neonatal period. She had a motor retardation of autonomous walking until 22-months old and intelligence disability and language disability. She only knew a few simple words like ”mama“, not ”baba“, and she cannot communicate clearly with others though she was willing to speak to strangers. Gesell Developmental Schedules performed in local hospital indicated mental developmental delay in motor behavior, language behavior, adaptive behavior and personal-social behavior at age of one year and 8 months old. The height of her father, mother and 15
years old sister were 165cm, 161cm, and 155cm, respectively. No similar history was noted in her family.
On physical examination, she had a height of 81.4 cm below -3SD and a weigh of 11.6 kg below -1SD. Mild craniofacial dysmorphy was present, including thin hair, frontal bossing, low set ears, broad-flat nose, nostrils slightly upward, and downturned corners of the mouth while other craniofacial anomalies were not obvious (Fig.1A). Her hands were small especially her fingers, but the fingernails are normal (Fig.1B). Her teeth were dysplasia (Fig.1C). The echocardiography revealed patent foramen ovale (ϕ 2.96 mm) while no murmur was present. The muscle tension was normal and no other organ abnormality was detected in our patient.
Laboratory examinations (urine, liver, kidney, thyroid hormone, GS/MS and blood glucose analyses) were all normal. Insulin-like growth factor-1 was 72.5 ng/ml (normal range, 55-327 ng/ml).
Management and outcome
Ten months ago, the child was brought to a local hospital with developmental delay, the peripheral leukocyte karyotype was taken and revealed two abnormal cell lines, the result was 46,XX, psu idic (18)(p11.2)[55]/46, XX, del (18)(p11.2)[45] . She was then referred to another hospital to take the whole-exome sequencing demonstrating a deletion at 18p11.32-p11.22 (GRch37/hg19, chr18:158679 9708482del) and a duplication at
18p11.21-q23(GRch37/hg19, chr18:12012132 78005255dup). She was diagnosed mosaic trisomy 18 syndrome.
Discussion
The first reported patients with trisomy 18 syndrome were initially described by Edwards et al and Smith et al in 1960s, while the first case of mosaic trisomy 18 was reported in 1965. Less than 5% portion of patients have mosaicism of trisomy 18, and Banka et al reminded that routine karyotype from lymphocyte culture may not be sufficient to diagnose mosaicism if practitioners suspect a diagnosis of mosaic trisomy 18, karyotype from skin fibroblasts should be considered. Since then over 40 cases of mosaic trisomy 18 have been described, Tucker et al reviewed 33 reported individuals of mosaic trisomy 18 and added 2 more cases in 2007. Their clinical manifestations are extremely variable from complete trisomy 18 syndrome with early death to near totally normal. Some physical features are relatively more common and included brachydactyly, high arched palate, microcephaly, delayed bone age, frequent respiratory infections and otitis media, heart defect, 5th finger clinodactyly, micrognathia, and hypotonia. The most common heart defect is ventricular septal defect in mosaic trisomy 18. Our case has mild craniofacial dysmorphy and patent foramen ovale, and no other physical anomalies were observed.
Trisomy 18 mosaicism usually indicates the existence of more than one cell line in the individual. The peripheral leukocyte karyotype demonstrates pseudodicentric chromosome substituting a normal chromosome 18 in 55 cells and chromosome 18 missing the end of the short arm in 45 cells. The skin fibroblasts karyotype was not taken. Furthermore, there is no correlation between the physical and intellectual findings and the percentage of trisomy 18 cells in either peripheral leukocytes or skin fibroblasts. Besides, there is no correlation between the percentage of trisomic cells in peripheral leukocytes and brain, gonads, or other key organs. The variety of mosaic trisomy 18 may be related to the percentage of trisomic cells in different key organs of the body.
For complete trisomy 18 patients, approximately 50% of infants live longer than one week and about 5-10% of children survive beyond the first year. In overall, trisomy 18 mosaicism patients usually survive longer when compared to complete trisomy 18. This does not mean that all the mosaic trisomy 18 patients have a longer survival, some died a few hours after birth. For normal or mild phenotypical mosaic trisomy 18 cases, some were diagnosed due to recurrent miscarriages or giving birth to a child with trisomy 18 while others may never be identified. 18p deletion syndrome, also called monosomy 18p and De Grouchy syndrome type Ⅰ, which means a deletion of full short arm of chromosome 18 or a microdeletion of the short arm of chromosome 18. Some researches showed that nearly half of patients have breakpoints in the centromeric region and the rest scatter in the short arm, and approximately half of the deletions occur on the maternal chromosome 18 no matter where the breakpoint locations are. Our case’s breakpoint is at the 18p11.32-p11.22. Approximately two thirds of patients’18p deletion are de novo; the rest may be due to a de novo unbalanced translocation or malsegregation of parental chromosome rearrangement or a ring chromosome. The patient’s height and weight is 81.4 cm below -3SD, 11.6 kg below -1SD, respectively. It may be a prodrome of small stature, but her insulin-like growth factor-1 was normal. It also could be contributed to feeding problem. More follow-up work needs to be done to figure it out. Some reported cases show that growth hormone replacement treatment is efficient in growth hormone deficiency patients.
Our case has trisomy 18 and microdeletion 18p mosaicism simultaneously. The possibility of meiotic chromosomal nondisjunction of the ovogonia/spermatocyte was increased because of her parents’ advanced maternal age, some women may have higher a risk for nondisjunction. More possible mechanism may be a de novo unequal recombination occurring in early embryonic mitosis. Some deletions are from the parents, there is no way to figure her mutation mechanism out since we can not get her parents’ consent to analysis. The phenotype of our case combines two syndromes’ typical features, including common psychomotor retardation, cognitive impairment and congenital heart defect, characteristic small stature and language impairment of 18p deletion syndrome. Our case’s uncharacteristic craniofacial features also combine two syndromes.
In a conclusion, mosaic trisomy 18 and 18p deletion syndrome both are chromosomal disorders which has a variety of clinical manifestations. If an individual has untypical phenotypical anomalies and psychomotor and cognitive disability, chromosome disorder should be considered and cytogenic analysis is needed.
Acknowledgements: We thank the patient and his parents for permitting us to use the data.
#Trisomy 18#mosaic#jcrmhs#Research Article in Journal of Clinical Case Reports Medical Images and Health Sciences#18p microdeletion#Psychomotor retardation#Karyotype
4 notes
·
View notes
Text
no one in my family reps my humanities degree 😞
#me: I’m doing an MSc next year#them: they’re calling silly humanities a SCIENCE NOW?? this is everything wrong with society#me with r studio open making multivariate linear regression analyses from qualitative data: ….#*quantitative data even LOL#AAAAAA#and bc I went to American high school I have AP biology I did honours Chem in final year I did calculus#just. and almost all my friends have stem degrees and I can talk to them abt their degree content#I read medical journals usually psychology/psychiatry for fun like it’s sooooo#and my dad works in medical research and alwsys offloads all the technicalities of that industry to me#just so frustrating not being taken seriously 😭#I have THEE most competitive humanities degree to get into from the best humanities uni in the country and theure like nah fake degree
4 notes
·
View notes
Text
Oxidative Stress Indices and Inflammatory Responses in Female Wistar Rats Administered Acetaminophen, Ampicillin/Cloxacillin and Co-Trimoxazole

Oxidative Stress Indices and Inflammatory Responses in Female Wistar Rats Administered Acetaminophen, Ampicillin/Cloxacillin and Co-Trimoxazole in Biomedical Journal of Scientific & Technical Research
Prescription drugs are frequently purchased from Pharmacy outlets based on selfmedication and often, combined to achieve therapeutic objectives that may trigger drug interactions that have not been fully elucidated. Therefore, this study evaluated the effects of concomitant administration of acetaminophen, ampicillin/cloxacillin and cotrimoxazoleon oxidative and inflammatory responses. Seventy female Wistar rats were assigned into seven groups of ten animals each. Therapeutic doses at 100 mg/kg body weight of co-trimoxazole, and 105 mg/kg body weight each of ampicillin/cloxacillin and acetaminophen orally once daily for four weeks. Group A served as the control, group B was administered ampicillin/cloxacillin only, group C was administered co-trimoxazole only, group D was administered acetaminophen only, group E was administered acetaminophen and ampicillin/cloxaxillin, group F was administered co-trimoxazole and acetaminophen, and group G was administered acetaminophen, ampicillin/ cloxacillin, and co-trimoxazole. Oxidative status was determined in the serum and homogenates of liver and brain by the levels of total thiol, reduced Glutathione (GSH), Oxidized-Low Density Lipoprotein Cholesterol (Ox-LDL-C). Inflammatory response was assessed by measuring the serum levels of Interleukin-1β (IL-1β), Nitric Oxide (NO), Monocyte Chemoatracttant Protein (MCP-1), Vascular Adhesion Molecule (VCAM-1) and Total Immunoglobulin G (IgG). Body weights and organ to body weight ratios across the groups were insignificantly different (p>0.05). Serum total thiol level increased (p<0.05) in B and D compared to A,C, E, F and G. Liver and brain total thiol levels were insignificant changed (p>0.05) across the groups compared to control but increased (p<0.05) in liver of G compared to D and brain of B and D compared to C. Serum GSH levels were insignificantly different (p>0.05) across the groups, while liver GSH in G decreased (p<0.05)compared to A, B, C and D and brain GSH level in F was elevated (p<0.05) compared to A,B,C,D and E. Serum Ox-LDL-C concentrations were elevated significantly (p<0.05) in F and G compared to A and D. Serum levels of IL-1β, NO, MCP-1,VCAM-1 and IgG were insignificant changed (p>0.05) across the groups, but there was decrease (p<0.05) in VCAM-1 in G compared to B. Histological examination indicated varying degrees of vacuolation, fenestration and occlusion in liver, and neurodegeneration in brain of groups administered the drugs. This study showed that the concomitant use of acetaminophen, ampicillin/cloxacillin and co-trimoxazole caused oxidative stress that has a weak link to vascular related disorders. Therefore, awareness of the health implications associated with misuse of these drugs should be emphasized.
For more articles in Journals on Biomedical Sciences click here bjstr
#Journals on Medical Microbiology#Behavioral Medicine Journals#Physical Medicine and Rehabilitation#journal of biomedical research and reviews impact factor#journal of biomedical sciences research review
0 notes
Text
youtube
Call : +917997101303 | Whatsapp : https://wa.me/917997101505 | Website : https://fidicus.com
Tests and Investigations for PCOD PCOS | Treatment Cure Medicine Surgery | Gynaecology Women Female
"Explore essential tests and investigations for PCOD/PCOS with Dr. Bharadwaz, Chief Doctor at Fidicus Homeopathy. In this video, we discuss the key diagnostic tests, from hormone level checks to ultrasound scans, and how each helps in understanding PCOS. Dr. Bharadwaz explains the significance of these tests in assessing hormone imbalances and ovarian health, offering insights into effective homeopathic approaches for treatment. Don’t miss this comprehensive guide to PCOD/PCOS diagnostics and care!"
Dr. Bharadwaz | Gynaecology Women Female | Health & Fitness | Homeopathy, Medicine & Surgery | Clinical Research
#PCOS #PCOD #WomensHealth #Homeopathy #hormonebalance
#DrBharadwaz #Helseform #Fidicus #Clingenious
#ClingeniousHealth #HelseformFitness #FidicusHomeopathy #ClingeniousResearch
#Women #Gynaecology #Female
#Treatment #Cure #Prevent #Relieve #Medicine
#AlternativeTherapy #AdjuvantTherapy #AlternativeMedicine #AlternativeSystem
Speciality Clinic Fidicus Women highest success with homeopathy No Sideeffect | Permanent Result | Personal Care
#pcos symptoms and treatment#polycystic ovary syndrome (disease or medical condition)#blood tests for pcod#pcos tests#pcod tests#pcos signs and symptoms#reproductive endocrinology and infertility (profession)#medications for lean pcos#pcos and fertility#diet for pcos to lose weight#pcos foods dos and donts#normal follicle size for ovulation#international journal of science and research#l-carnitine before and after#hormonal tests pcos#hormonal tests pcod#Youtube
1 note
·
View note
Text
Pulmonary tuberculosis misdiagnosed as child. A case report by Castanos in Journal of Clinical Case Reports Medical Images and Health Sciences.
Abstract
We present the case of a 4-year-old girl who had a history of many hospital admissions due to acute respiratory failure. She was now admitted to the hospital with cough, fever, and hypoxemia. She received bronchodilators, OCS, ceftriaxone, and supplementary O2 for six days. After that she remained clinically stable for 24 hs. Then she developed acute respiratory failure requiring MV, inotropic drugs and broad-spectrum antibiotics in the ICU with no response. Chest CT scan showed an interstitial pattern in both lungs. As the etiology remained unknown and she was critically ill, a presumptive diagnosis of chILD was made and a corticosteroid pulse was administered. At day 12, sputum cultures were positive for Mycobacterium tuberculosis. Tuberculostatic drugs were started and the patient improved gradually.
Ths case highlights the importance of considering TB as a differential diagnosis of interstitial lung disease, especially in countries with a high rate of TB infection.
Keywords: Interstitial pneumonia, Interstitial lung disease, Tuberculosis, children.
Introduction
Interstitial lung disease refers to disorders that feature remodeling of the lung interstitium and distal airspaces resulting in abnormal gas exchange. The children's interstitial and diffuse lung disease (chILD) syndrome exists when an infant with diffuse lung disease has at least three of the following criteria: (1) respiratory symptoms (e.g., cough, difficulty breathing), (2) respiratory signs (e.g., tachypnea, adventitious sounds, retractions, failure tothrive), (3) hypoxemia,and (4) diffuse abnormalities on CT scan. Many disorders may cause this syndrome, some of which are specificto infancy (<2 years of age), including surfactant dysfunction mutations, and some are not, such as cystic fibrosis, chronic lung disease of prematurity, and pulmonary infections (including tuberculosis).1–3 Some entities are associated with few symptoms and evolve favorably, but others are more symptomatic and potentially lethal.
Case report
We present the case of a 4-year-old girl who had a history of many hospital admissions due to acute respiratory failure. During the first admission was at two months of age (IIF: SRV+). During one of the episodes, she required 10 days of mechanical ventilation (MV) in the ICU (IIF: ADV+/ Sputum: H. influenzae+). On each occasion, she received oral corticosteroids (OCS), bronchodilators (B2 agonist), and supplementary oxygen (O2), improving slowly with a mean length of stay of 7-10 days.
In the last episodes the patient was admitted to the hospital with a cough and fever for longer than 2 weeks. She was tachypneic and hypoxemic on room air. The following complementary studies were performed: PCR COVID negative, laboratory with WC 13110 (N77/L19), CRP 4, TST 0 mm, three gastric lavages with a negative smear for tuberculosis, and a chest X-ray showing an interstitial pattern with alveolar opacities (Figure 1). She received B2 agonists, OCS, azythromicin, ceftriaxone, and supplementary O2 through a nasal cannula for six days, after which she improved.
Once the treatment was discontinued, she remained clinically stable for 24 hs with normal peripheral oxygen saturation (SpO2) and no fever. Subsequently, she developed acute respiratory failure requiring MV and inotropic drugs in the ICU. Chest CT scan showed air space consolidation, reticular opacities, clustered alveolaropacities (nodules), and multiple small discrete nodules randomly distributed in both lungs (Figure 2). Tracheal secretion cultures, blood cultures, HIV, and other serology tests were all negative. Broad-spectrum antibiotics were given without response and the patient became critically ill. She developed refractory hypoxemia with PO2 < 60 mmHg despite FiO2 of 100% and required high-frequency ventilation. As the etiology was unknown and lung biopsy or bronchoalveolar lavage (BAL) could not be performed given the critical condition of the patient, a presumptive diagnosis of chILD was made and methylprednisolone 10 mg/kg/d was given for three days without a favorable response. Twelve days after admission, 2 of 3 sputum cultures were positive for Mycobacterium tuberculosis susceptible to isoniazid and rifampicin confirming an Acute respiratory distres ssyndrome (ARDS) due to tuberculosis. Tuberculostatic drugs were started and the patient began to improve gradually and could be weaned from MV. After one month of hospitalization, she was discharged with minimal pulmonary sequelae.
Discussion
We present a case of pulmonary tuberculosis (TB), a common disease in developing countries, but with the infrequent presentation of interstitial pneumonia.
TB is a highly transmissible disease that, although preventable and curable, continues to be a significant cause of ill health and one of the leading causes of death worldwide. An estimated 10.6 million people fell ill with TB worldwide in 2021; adult men accounted for 56.5% of all TB cases, adult women for 32.5%, and children for 11% of cases. In 2021 in Argentina, 12,569 cases of TB werereported, 56.8% of which were male, 16.7% were < 20 years, and 81% were pulmonary TB (PTB).6
TB typically affects the lungs but can affect other sites as well.4 The most common clinical presentation of PTB in children is persistent cough and poor weight gain. TB may also present in atypical ways including acute severe pneumonia with SpO2 below 90% or severe respiratory distress.5
On the other hand, the chILD syndrome is rare and may be due to many disorders. Guidelines on Interstitial Lung Disease in Infancy suggest a series of complementary studies as the initial approach to rule out the most frequent and treatable causes: appropriate cultures (infection, including TB/sepsis/pneumonia), laboratory tests (HIV, immunodeficiency), CF diagnostic studies, echocardiogram (structural cardiovascular disease and pulmonary hypertension), thin section CT scanning of the chest (characteristic of the lung disease), flexible bronchoscopy with BAL (to exclude infection or airway abnormalities), and eventually lung biopsy (when other diagnostic investigations have not identified the precise disease, or when there is clinical urgency to identify it).2,7
Management of the chILD syndrome is based on unsystematic observations. The decision about whether or not to initiate a trial of immunosuppressive therapy (corticosteroids, hydroxychloroquine, azithromycin) should be made for each individual case considering disease severity, progression rate, prognosis without treatment, comorbidities, and family preferences.2,7
This case highlights theimportance of considering TB as a differential diagnosis of interstitial pneumonia or interstitial lung disease, especially in countries with a high rate of TB infection.
#Interstitial pneumonia#Interstitial lung disease#Tuberculosis#children#Research Article in Journal of Clinical Case Reports Medical Images and Health Sciences.#jcrmhs
0 notes
Text
The study itself is titled, “Long-Term Regret and Satisfaction With Decision Following Gender-Affirming Mastectomy,” and sought to study the rate of regret and satisfaction after 2 years or more following gender affirming top surgery. The study’s results were stunning - in 139 surgery patients, the median regret score was 0/100 and the median satisfaction score was 5/5 with similar means as well. In other words… regret was virtually nonexistent in the study among post-op transgender people. In fact, the regret was so low that many statistical techniques would not even work due to the uniformity of the numbers: In this cross-sectional survey study of participants who underwent gender-affirming mastectomy 2.0 to 23.6 years ago, respondents had a high level of satisfaction with their decision and low rates of decisional regret. The median Satisfaction With Decision score was 5 on a 5-point scale, and the median decisional regret score was 0 on a 100-point scale. This extremely low level of regret and dissatisfaction and lack of variance in scores impeded the ability to determine meaningful associations among these results, clinical outcomes, and demographic information. The numbers are in line with many other studies on satisfaction among transgender people. Detransition rates, for instance, have been pegged at somewhere between 1-3%, with transgender youth seeing very low detransition rates. Surgery regret is in line with at least 27 other studies that show a pooled regret rate of around 1% - compare this to regret rates from things like knee surgery, which can be as high as 30%. Gender affirming care appears to be extremely well tolerated with very low instances of regret when compared to other medically necessary care.
[...]
The intense conservative backlash, to the point of disputing reputable scientific journals, likely stems from the fact that reduced regret rates weaken a central narrative these figures have championed in legal and legislative spaces. Over the past three years, anti-trans entities have showcased political detransitioners, reminiscent of the ex-gay campaigns from the 1990s and 2000s, to argue that regrets over gender transition and detransition are widespread. Some have even asserted detransition rates of up to 80%, a claim that has been broadly debunked. Yet, research consistently struggles to find substantial evidence supporting this narrative. The rarity of detransition and regret is underscored by Florida's inability to enlist a single resident to bear witness against a lawsuit challenging the state's ban on gender-affirming care.
20K notes
·
View notes
Text
Medical Image Journal: Journal of Medical Images

Medical Image Journal: Journal of Medical Images publishes medical image articles, images in medical science, imaging in medical journal, imaging in medical science journal, images in clinical medicine journal, images in medical research, imaging in medical research, image case journal etc. Journal allows for the peer-reviewed communication and archiving of Clinical and Medical Research, as well as applications, focused on medical imaging, a field that continues to benefit from technological improvements and yield biomedical advancements in the early detection, diagnostics, and therapy of disease as well as in the understanding of normal conditions.
Journal Homepage: https://www.literaturepublishers.org/
Manuscript Submission
Authors are requested to submit their manuscript by using Online Manuscript Submission Portal:
(or) also invited to submit through the Journal E-mail Id: [email protected]
Medical Image Journal: Journal of Medical Images provides a forum for the dissemination of new research results in the field of Medical and Clinical Image Journal, with special emphasis on efforts related to the applications of computer vision, virtual reality and robotics to biomedical imaging problems. Medical Image Journal: Journal of Medical Images publishes the highest quality, original papers that contribute to the basic science of processing, analyzing and utilizing medical and biological images for these purposes. Medical Image Journal: Journal of Medical Images is interested in approaches that utilize biomedical image datasets at all spatial scales, ranging from molecular/cellular imaging to tissue/organ imaging. While not limited to these alone, the typical biomedical image datasets of interest include those acquired from.
The types of papers accepted include those that cover the development and implementation of algorithms and strategies based on the use of various models (geometrical, statistical, physical, functional, etc.) to solve the following types of problems, using biomedical image datasets: representation of pictorial data, visualization, feature extraction, segmentation, inter-study and inter-subject registration, longitudinal / temporal studies, image-guided surgery and intervention, texture, shape and motion measurements, spectral analysis, digital anatomical atlases, statistical shape analysis, computational anatomy (modelling normal anatomy and its variations), computational physiology (modelling organs and living systems for image analysis, simulation and training), virtual and augmented reality for therapy planning and guidance, telemedicine with medical images, telepresence in medicine, telesurgery and image-guided medical robots, etc.
#Medical Image Journal: Journal of Medical Images publishes medical image articles#images in medical science#imaging in medical journal#imaging in medical science journal#images in clinical medicine journal#images in medical research#imaging in medical research#image case journal
0 notes
Note
Hi, I share your strong pro-medicine, pro-vaccines, anti-woo beliefs. I also have chronic digestive issues and insurance that won’t cover the useful specialists. The gastroenterologists I’ve encountered are helpful for making sure my insides look okay but they don’t seem to have much training around nutrition and food science. Nutritionists are unlicensed and I find them about as trustworthy as chiropractors, and I can’t get insurance to cover a registered dietician. The internet is saturated with pseudoscience junk and “miracle cures”, and in moments of desperation I’ve fallen for some of them. Luckily I haven’t been harmed by anything so far, but I don’t think they helped much either.
I was wondering if you or your followers have any resources on IBS and/or GERD that are scientifically sound and written for a general audience? Or advice for identifying when pop-sci-style “food science” articles are a scam?
I deeply regret to inform you that I was so annoyed by this exact problem that I literally went back to school to start working on getting a degree in nutrition and got two and a half years into a second bachelor's degree before realizing I wouldn't be able to get into any programs in my area that I could afford because the local state schools aren't accepting second bachelor's applicants. (Cal State Chico, I love you and you are too far away, it's not meant to be)
Nutrition information online is completely infested with woo and I am hesitant to point people toward one of the good resources I used to reference because it is politically batshit.
If you are looking at a food science article on the internet and are trying to figure out if it's a scam the big red flags to look out for are:
anything claiming to be a silver bullet; there are no silver bullets, no magical treatments, no one weird food that will fix the problem or one weird supplement that will make everything better.
Over-emphasis on a specific type of diet (diet as in "all the food that a person consumes" not as in "weight loss tool") for a general population. It's irresponsible to recommend a rigorous, restricted diet to a wide variety of people because people are so different that one diet that works for one person (say a vegan diet) might be unhealthy or difficult to manage for another person who would thrive on a different diet (low fat, low carb).
Anyone who tells you to cut out an entire food group or macronutrient is a liar who is trying to get your money. Unless it is your personal medical doctor who is saying "you need to stop eating grains" you do not need to stop eating grains and should not stop eating grains. You also do not need to stop eating fat, or eat only protein, or cut all fruit out of your diet. (caveat: there are some conditions that require a very low fiber diet, but even on that diet there are some fruits you can eat)
Beyond that, what you can do to make sure you're getting the best information possible is:
look up the author of any article you're looking at and see what else they've written; check what their qualifications are. See the people they interact with or have collaborated with. If they work heavily with people who are, say, antivax or proponents of raw milk, you should not trust their work.
If you see something that claims to treat your condition or help with nutrition, search "[subject] research study" or "[subject] scholarly research" and see what comes up. Read at least a few papers on the subject and see if there's a consensus or if there are broad disagreements. Get into the habit of looking up the impact scores of journals and researching the history of the journals.
Learn to recognize the woo keywords with your particular illness. For celiac that's "leaky gut," and any article I come across that discusses "leaky gut" gets extra scrutiny because sometimes there are legitimate reasons to describe a "leaky gut" but more often there are woo nonsense reasons. One really good way to figure out what the woo keywords for your illness are is to search "[your illness] + [woo huckster]", so "celiac + joseph mercola" or "celiac + the food babe." (those are good starting places to see what woo is popular around anything nutrition based, really; nothing those two say is trustworthy) you can also try "[your condition] + [specific type of medical woo]" with, like, "chiropractic" and "homeopathic" and "holistic" in the second box.
Be wary of positive assertions without evidence. If someone is making an affirmative statement and they aren't providing a citation, be suspicious.
Anyway. Good luck. It sucks out there.
777 notes
·
View notes
Text
Surgery "Saving Trans Lives!" - Is it true?
Everytime you hear a trans person talk in any public forum, they use hyperbolic language about how we have to stop trans kids/teens from dying, or saving trans kids/teens lives. You would think from the language that there were trans people on the street gasping their last breath; if only they could receive a hormone intervention to save them! Of course they want to overwhelm people with this…

View On WordPress
#gender affirming surgery#medical journals#mental health#mental health outcomes#psychology research#publications#repeatibility#research#science#scientific practice#scientific research#transgender research#unreliabe science
0 notes
Text
"A study looking at the bearers of artificial hearts found that a subset of them can regenerate heart muscle tissue—the first time such an observation has ever been made.
It may open the door to new ways to treat and perhaps someday cure heart failure, the deadliest non-communicable disease on Earth. The results were published in the journal Circulation.
A team of physician-scientists at the University of Arizona’s Heart Center in Tucson led a collaboration of international experts to investigate whether heart muscles can regenerate.
According to the Centers for Disease Control and Prevention, heart failure affects nearly 7 million US adults and is responsible for 14% of deaths per year. There is no cure for heart failure, though medications can slow its progression. The only treatment for advanced heart failure, other than a transplant, is a pump replacement through an artificial heart, called a left ventricular assist device, which can help the heart pump blood.
“Skeletal muscle has a significant ability to regenerate after injury. If you’re playing soccer and you tear a muscle, you need to rest it, and it heals,” said Hesham Sadek, director of the University’s Sarver Heart Center.
It was previously thought that when a heart muscle is injured, it could never grow back.
“Irrefutable evidence of heart muscle regeneration has never been shown before in humans,” he said. “This study provided direct evidence.”
The project began with tissue from artificial heart patients provided by colleagues at the University of Utah Health and School of Medicine led by Stavros Drakos, MD, PhD, and a pioneer in left ventricular assist device-mediated recovery.
Teams in Sweden and Germany used their innovative method of carbon dating human heart tissue to track whether these samples contained newly generated cells. The investigators found that patients with artificial hearts regenerated muscle cells at more than six times the rate of healthy hearts.
“This is the strongest evidence we have, so far, that human heart muscle cells can actually regenerate, which really is exciting, because it solidifies the notion that there is an intrinsic capacity of the human heart to regenerate,” Sadek said.
“It also strongly supports the hypothesis that the inability of the heart muscle to ‘rest’ is a major driver of the heart’s lost ability to regenerate shortly after birth. It may be possible to target the molecular pathways involved in cell division to enhance the heart’s ability to regenerate.”
In 2011, Sadek published a paper in Science showing that while heart muscle cells actively divide in utero, they stop dividing shortly after birth to devote their energy to pumping blood through the body nonstop, with no time for breaks.
In 2014, he published evidence of cell division in patients with artificial hearts, hinting that their heart muscle cells might have been regenerating because they were able to rest.
These findings, combined with other research teams’ observations that some artificial heart patients could have their devices removed after experiencing a reversal of symptoms, led him to wonder if the artificial heart provides cardiac muscles the equivalent of bed rest like a person needs when recovering from injury.
“The pump pushes blood into the aorta, bypassing the heart,” he said. “The heart is essentially resting.”
Sadek’s previous studies indicated that this rest might be beneficial for the heart muscle cells, but he needed to design an experiment to determine whether patients with artificial hearts were actually regenerating muscles.
Next, Sadek wants to figure out why only about 25% of patients are “responders” to artificial hearts, meaning that their cardiac muscle regenerates.
“It’s not clear why some patients respond and some don’t, but it’s very clear that the ones who respond have the ability to regenerate heart muscle,” he said. “The exciting part now is to determine how we can make everyone a responder, because if you can, you can essentially cure heart failure.
“The beauty of this is that a mechanical heart is not a therapy we hope to deliver to our patients in the future—these devices are tried and true, and we’ve been using them for years.”"
-via Good News Network, December 31, 2024
#cw death#heart#heart failure#biology#heart disease#public health#medical news#medical technology#cell biology#cardiology#medicine#health#good news#hope
386 notes
·
View notes
Text
Prevalence Of Staphylococcus Aureus In Nasal And Skin Of Apparently Healthy Food Handlers And Attendants In Restau by Iyevhobu Kenneth Oshiokhayamhe in Journal of Clinical Case Reports Medical Images and Health Sciences
Abstract
Food handlers play a major role in the transmission of food borne diseases which represents a global health burden. Carriage of Staphylococcus aureus, in general, and enterotoxigenic strains, in particular, is an important risk factor for the contamination of food. This study was undertaken to determine the prevalence and risk factors associated with nasal and skin carriage of Staphylococcus aureus among 150 food handlers working in different restaurant in Ekpoma. Thirty (10%) persons were found to be significant (P< 0.05) carriers of Staphylococcus aureus of which highest occurrence of 24 (16%) from anterior nasal nares and 6 (7.5%) from skin of food handlers and restaurant workers. Prevalence and distribution of Staphylococcus aureus in relation to gender among food handlers and restaurant workers, showed high occurrence in females of 17 (56.6%) than males 13 (43.3%) with no significant difference in comparison of variability (P>0.05). Susceptibility pattern of Staphylococcus aureus isolated from this study had high sensitivity pattern of 93% to Zennacef, 80% to Rocephin, 93% to Ciprofloxacin, 70% to Gentamycin, intermediate sensitivity to Septrin 53%, Streptomycin 50%, and resistant to Erythromycin 40%, Amoxacilin 36% and Ampiclox 17%. From this study, Staphylococcus aureus is the most prevalent among them isolates that colonizes the skin and mucosal surfaces of healthy food handlers and restaurant workers. These findings resurges the imperative need for protective measures including increased public awareness programs, regular monitoring of food handlers for food borne pathogens and intensive training on primary health care and hygiene and future research addressing effective methods for sustained eradication of Staphylococcal skin and nasal carriage are clearly warranted to reduce the high risk of subsequent infection. It is our opinion that concerted efforts need to be made to educate food handlers and restaurant workers on the importance of personal hygiene and the use of protective gadgets like nose masks while handling food products; since they serve as potential sources of staphylococcal food poisoning.
Keywords
Food, Handler, Staphylococcus, Restaurant, Nasal, Skin
INTRODUCTION
Staphylococcus aureus avoidable medical and economic burden, the true incidence and prevalence of pathogenic strain of foodborne diseases is difficult to quantify. Risk factors implicated in foodborne diseases as identified by Centers for Disease Control and Prevention included unsafe sources, inadequate cooking, improper holding, contaminated equipment and poor personal hygiene implicating that the food handler dimension is crucially important (FDA, 2009). Food handlers have been implicated in a plethora of foodborne diseases. It has been reported that one of the important pathogens often transmitted via food contaminated by infected food handlers is Staphylococcus aureus (Verkaik et al., 2011). Bacteria of the genus Staphylococcus are Gram-positive cocci that are microscopically observed as individual organisms (Francois and Schrenzelg, 2008). Staphylococcus aureus is pathogenic ubiquitous species and may be a part of human flora found in the axillae, the inguinal and perineal areas, and the anterior nares (Bayer et al., 1998). Von Eiff et al., (2001) described 3 patterns of carriage: those who always carry a strain, those who carry the organism intermittently with changing strains, and a minority of people who never carry Staphylococcus aureus (Bayer et al., 1998). Persistent carriage is more common in children than in adults (Iwase et al., 2010). Nasal carriers may be divided into persistent carriers with high risk of infection and intermittent or non-carriers with low risk of infection (Blot et al., 2002). Direct invasion through breaks in the skin or mucus membrane leads into the production of superficial local infections such as folliculitis, furuncles and abscesses (Wertheim et al., 2005). This versatile pathogen is very well adapted to colonize the human skin and the human body provides some major ecological niches for this species. The anterior nares is the most frequent carriage site for Staphylococcus aureus, nonetheless extranasal sites typically harbor the organism including the skin, perineum and pharynx (Wertheim et al., 2005; Verkaik et al., 2011).
Until recently, reports on food contamination by Staphylococcus aureus, were mainly limited to occasional detections in the environment, the source of food and food itself. However, it is reported that human carriers are the most important source for transmission and the association between food handlers and the transmission of food borne disease frequently presents an investigative challenge (Jordá et al., 2012). Consideration into risk factors, transmission routes and many aspects of prevalence of carriage of foodborne pathogens among food handlers to eliminate carriage is necessary. Bodies concerned with food safety are left to consider whether interventions such as decolonization, continued monitoring or restrictions in the occupational activities are required (National Disease Surveillance Centre, 2004). Although skin carriage of Staphylococcus aureus, is less reported than nasal carriage, little is known about the prevalence and risk of skin carriage of enterotoxigenic strains of Staphylococcus aureus, among food handlers. Accordingly, the current study investigated the prevalence and risk factors associated with anterior nasal nares and skin carriage of Staphylococcus aureus, amongst food handlers working in different restaurant in Ekpoma Edo State.
Healthy carriers are potential source of Staphylococcus aureus infection and spread to other body sites as well as to other individuals. Staphylococcus aureus have been found frequently as aetiological of a variety of human infections. Centre for disease control (CDC) reported Staphylococcus aureus as primary source of infections, which could be transferred from individual to another, The organism also elaborates toxins that can cause specific diseases or syndromes and likely participate in the pathogenesis of staphylococcal infection. Enterotoxin-producing strains of S aureus cause one of the most common food-borne illnesses (food poisoning). The most common presentation is acute onset of vomiting and watery diarrhea 2-6 hours after ingestion. The symptoms are usually self-limited. The cause is the proliferation of toxin-producing organisms in uncooked or partially cooked food that an individual carrying the staphylococci has contaminated (Matthews et al., 1997). This study is set determines the prevalence of Staphylococcus aureus from skin and nasal nares of apparently healthy food handlers in restaurant which could be the source of Staphylococcus aureus food contamination resulting to food born infection in Ekpoma.
MATERIALS AND METHODS
This project work from its inception, sample collection, sample analysis and compilation was carried out within a period of four months with a total of hundred Fifty Skin and nasal swab samples from different restaurant workers and food handlers in Ekpoma. A total of one hundred fifty (150) nasal and skin swab were randomly collected from male and female food handlers and restaurant workers grant consent.
Informed consent was requested and granted by the food handlers and restaurant workers under investigation. The concept of the study was explained to them and having understood its dimensions, granted their informed consent.
Sample Collection: One hundred and fifty specimen were collected randomly from males and females food handlers and restaurant workers within Ekpoma metropolis. The samples (150 nasal swabs and 150 skin swab). Nasal swab were collected in good light vision from subjects by bending their heads backward to collect the specimens deep down the anterior passages using a sterile swab stick. Both right and left nostrils were swabbed bearing labels as nasal swabs, sex, code number and date of collection. The swabs sticks were carefully returned to their sterile containers, sealed with adhesive tape and labelled accordingly. Skin swab was collected by swabbing their skin (especially their fore arm) with a swab moist with physiological saline aseptically and the swabs sticks were carefully returned to their sterile containers. Collected specimen was taken to the laboratory where bacteriological analysis was carried out immediately.
Procedure for Culture: The swab stick were used to make a primary inoculum on each agar surface (blood agar and chocolates agar plate). Spreading was done by streaking from the primary inoculum using a sterile inoculating wire loop to obtain discrete bacterial colonies. The plates were then incubated at 370C for 24 hours. Growth was observed after incubation, and the colonial morphology was studied carefully, noting the size, shape, edge, colour, consistency, haemolysis, elevation and opacity of the colonies. This was followed by Gram staining (Ochei and Kolhatkar, 2000).
Method for Detection of Staphylococcus aureus: The colonies that were yellow pigmented or cream white (Cheesbrough, 2000) were sub-cultured onto mannitol salt agar and selected for catalase (using H2O2) and coagulase tests (using plasma). Mannitol fermenting and slide coagulase positive isolates were identified as Staphylocuccus aureus.
Antibiotic Sensitivity Test: Antibiotic disc such as Erythromycin, Gentamycin, Streptomycin, Ciprofloxacin, Ampicillin, Septrine, Zinnacef, Amoxicilin and Rocephin (manufactured by Abtek Biologicals Ltd) were used to test the susceptibility of Staphylococci aureus isolates obtained. The test isolates were inoculated into sterile peptone water broth. The antibiotic discs were placed aseptically on the seeded plate. They were incubated at 370C for 24hours and examined for zones of inhibition. The zones of inhibition were measured in millimetres and recorded. Antibiotic zones less than 10mm in diameter were recorded as been resistant (R) by the organism while those with diameters of 10mm and above were recorded as sensitive (S)
Statistical Analysis: The collected data was expressed as Frequency and percentage. Comparison of qualitative variables was made using chi-square test. In all cases studied, the difference having p<0.05 were considered statistically significant using interactive calculation Chi square tool software (version 18).
RESULTS
Based on standard bacteriological analytical methods, from investigation of 300 samples of [nasal swab (150), skin swab (150)] from food handlers and restaurant workers in Ekpoma, revealed 30(10%) distribution of Staphylococcus aureus prevalence with the highest occurrence of 24 (16%) from nasal swab and 6 (7.5%) from skin swab. Other growths of non-Staphylococcus aureus were excluded from this study. The significant difference of Staphylococcus aureus isolates distribution among samples in this study was statistically significant (P< 0.05) with X2cal=26.057 p-value 0.000.
X2cal=26.057, Degree of freedom=2, p-value=0.0000 Key: N - Number , S. aureus: Staphylococcus aureus
X2cal=18.04, Degree of freedom=2, p-value=0.000, Key: N - Number
X2 cal=1.663, Degree of freedom=1, p-value=0.435, (p>0.05).
KEY:CN-Gentamycin, Z-Zennacef, R-Rocephin, CPX- Ciprofloxacin, SXT-Septrin, S-Streptomycin, E-Erythromycin AM- Amoxacilin , APXAmpiclox
DISCUSSION
Staphylococcus species are regional flora of the skin and mucus membrane of the body, certain species have been found frequently as aetiological agent of a variety of human and animal infections. The most common among these infections are the superficial supportive infection caused by Staphylococcus aureus. Infection can result to life threatening conditions disease spectrum which includes abscesses, septicemia, osteomyelitis, endocarditis and cellulitis, pneumonia, in addition to various toxin mediated diseases as toxic shock syndrome and staphylococcal food poisoning. The variety of such spectrum of clinical manifestations is mostly dependent on the numerous virulence factors produced by each strain (Vasconcelos and da Cunha, 2010). The ingestion of the preformed toxins produced by Staphylococcus aureus (enterotoxigenic strains) in food often results to the development of food poisoning. Findings from this investigation indicate a significant (P< 0.05) distribution of Staphylococcus aureus of 30(10%) prevalence with the highest occurrence of 24 (16%) from anterior nasal nares of food handlers and restaurant workers, 6 (7.5%) from skin swab which is in agreement with investigation reported by Mous-tafa et al., (2013) of 10.5% Nasal Carriage of Staphylococcus aureus and Risk Factors among Food Handlers-in Egypt. The findings from this studied in relation to area of study, was not in agreement with findings report by Eke et al., (2015), with a wide variation of 60% prevalence from 100 nasal swab analysis of food handlers and restaurant workers in Ekpoma. The reduced significant prevalence from this study is proportionately an improve hygiene of food handlers and workers in restaurant. This study variables revealed that gender, age, marital status nor level of education had no significant effect with respect to the nasal and skin carriage of Staphylococcus aureus. This study findings also reveal anterior nasal nares of food handlers and restaurant workers to harbour pathogenic Staphylococci species [Staphylococcus aureus 24(16%) to that of their skin 6(7.5%) with significant increase difference of (P>0.05) P- value 0.000].
Prevalence and distribution of Staphylococcus aureus in relation to gender among food handlers and restaurant workers, showed high occurrence in females food handlers and workers of 17 (56.6%) than males 13 (43.3%) with no significant difference in comparison of variability (P>0.05) and not in agreements with the findings by Eke et al., (2015), which report males food handlers to have high prevalence than the females in Ekpoma. The disparity of this report may be due to the subject who consent to participate as at time of study in regards to gender present in restaurant.
The sensitivity pattern of Staphyloccus aureus isolated from this study had high susceptibility to Gentamycin, Zennacef, Rocephin, Ciprofloxacin intermediate to Septrin, Streptomycin, and resistant to Amoxicillin, Erythromycin and Ampiclox which in agreement with the study reported by Eke et al., (2015). From this research it can be suggested that skin and nasal nares harbours Staphylococcus aureus which can be source of enterotoxigenic stains causing food born infection observed in our restaurant this days.
From all the organisms known to cause food born infection, Staphylococcus aureus is the most prevalent among them that is easily isolated and it colonizes the skin and mucosal surfaces of healthy individuals. The isolation of this organism learned to us that, as a microflora, it has a high percentage of causing infectious disease related to illness. Evidence from the result obtained has show that the skin and nasal nares has carrying capacity of Staphylococcus aureus. In contrast, healthy individuals as worker and food handlers in restaurant are risk factor of food born infection (food poisoning).
In conclusion, a relatively high prevalence rate of Staphylococcus aureus in nasal nares and skin carriage was recorded among the investigated food handlers. Moreover, 10% of the investigated carriers harboured Staphylococcus aureus in their anterior nares increasing the likelihood of transmission of the pathogen to the handled food. These findings resurges the imperative need for protective measures including increased public awareness programs, regular monitoring of food handlers for food borne pathogens and intensive training on primary health care and hygiene. Finally, the current findings clearly highlight the significance of implementation of efficient quality control systems in areas of direct contact with food product as good manufacturing practices and standard operational procedures and future research addressing effective methods for sustained eradication of Staphylococcal skin and nasal carriage are clearly warranted to reduce the high risk of subsequent infection.
CONFLICT OF INTEREST
The authors declare no conflicts of interest. The authors alone are responsible for the content and the writing of the paper.
FUNDING
This research did not receive any grant from funding agencies in the public, commercial, or not-for-profit sectors.
AUTHORS’ CONTRIBUTIONS
Iyevhobu, K.O. and Obodo, B.N., conceptualized the laboratory work and provided scientific guidance, Momoh A.R.M., Airefetalor, A.I. and Okobi, T.J. designed and wrote the manuscript while Etafo, J. and Osagiede, E.K. conducted experiments.
ACKNOWLEDGEMENTS
The authors would like to thank all the Laboratory and technical staffs of the department of Medical Laboratory Science, Ambrose Alli University Ekpoma, Edo State for their excellent assistance and St Kenny Research Consult, Ekpoma, Edo State for providing medical writing support/editorial support in accordance with Good Publication Practice (GPP3) guidelines.
#Restaurant#JCRMHS#Nasal#staphylococcal food#Research Article in Journal of Clinical Case Reports Medical Images and Health Sciences#Susceptibility pattern#Handler#Skin#Staphylococcus#Food
3 notes
·
View notes
Text
Dandelion News - November 22-28
Like these weekly compilations? Tip me at $kaybarr1735 or check out my Dandelion Doodles!
1. Los Angeles becomes a sanctuary city for LGBTQ+ youth and immigrants as officials reject Project 2025

“The Los Angeles City Council voted unanimously Tuesday to pass the “sanctuary city” ordinance, shielding queer youth who travel to the city to receive gender-affirming care from prosecution, as well as preventing city resources from being used in immigration enforcement[….]”
2. Huge deforested areas in the tropics could regenerate naturally, study finds

“Cleared or degraded tropical forests around the world covering a combined area larger than Saudi Arabia could regrow on its own, according to new research published Oct. 30 in the journal Nature. [… T]he permanence of regrown forests is critically important to the benefits it can provide to biodiversity and the climate.”
3. Minnesota tribe could soon get a solar-powered resilience hub

“A pair of developers are working to build a microgrid at an elementary school and community center on the White Earth Reservation in northern Minnesota [… which would] provide about 12 hours worth of backup power for residents to be able to charge cell phones, power medical equipment, or stay warm in the event of a power outage.”
4. An exchange between Indonesia and Tanzania supports food security and ocean health

“Around the world, WWF helps manage […] both traditional sustainability-oriented management and science-based practices. This combination supports long-term food security and biodiversity goals. […] Local ownership and management are […] key to achieving stable fisheries and social and economic benefits.”
5. Spiky blue devils and chocolate lilies: Victorian grassland bursts with wildflowers after ecological ‘reset’

“About 70 native plant species could be found within the site, including […] four endangered species of orchid. […] Careful management, including an ecological burn in May and weed control measures to reduce pasture grasses, laid the groundwork for wildflowers to thrive.”
6. Vast forests, wetlands and lakes conserved [in Ontario]

“A vast 970-hectare area featuring thriving forests, wetlands and crystal-clear lakes northeast of Sault Ste. Marie is now protected[….] The intact forests, lakes, wetlands and shorelines support high biodiversity and are home to many threatened species[….]”
7. A New Era of Compassion: How Suncoast Humane Society is Changing Animal Welfare for Good
“Our campus includes outdoor play areas, trails, and even a small swimming pool to encourage animals to stay active, explore, and simply be themselves.”
8. Building climate resilient cocoa farming in West Africa
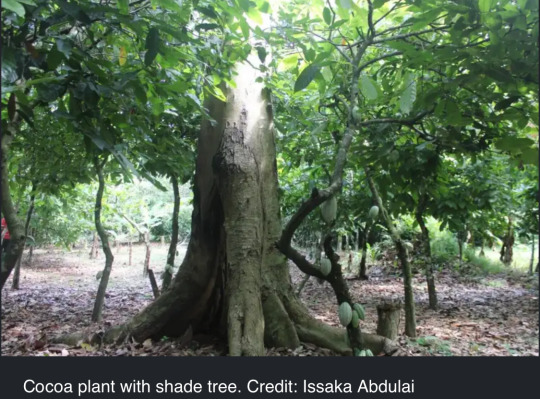
“[… A] promising new approach to improve climate resilience in cocoa agroforestry across West Africa […] focuses on the critical role of leaf "phenology"—the seasonal changes in leaf cycles—in trees providing shade in managing climate impacts. [… S]hade trees that lose their leaves entirely during the dry season proved especially beneficial in maintaining soil moisture[….]”
9. New Zealanders save more than 30 stranded whales by lifting them on sheets

“[The Department of Conservation] praised as “incredible” the efforts made by hundreds of people to help save the foundering pod. “It’s amazing to witness the genuine care and compassion people have shown toward these magnificent animals[….]””
10. 'A really sobering moment:' English zoo fights extinction of freshwater Boxer pupfish

“Whipsnade Zoo aquarists were recently told by conservation partners that that the world's last remaining Boxer pupfish was in their care, prompting the zoo to carry out the immediate transport of all the "precious" Boxer pupfish eggs to another local conservation and education charity in the name of species preservation.”
November 15-21 news here | (all credit for images and written material can be found at the source linked; I don’t claim credit for anything but curating.)
#hopepunk#good news#los angeles#us politics#lgbt+#immigrants#deforestation#nature#minnesota#native american#indigenous#electricity#solar panels#solar energy#solar power#ocean#fishing#food insecurity#wildflowers#native wildflowers#native plants#conservation#canada#animal shelters#humane society#agroforestry#new zealand#whale#fish#endangered
123 notes
·
View notes
Note
Hi Sam, could you please recommend any resources/websites to learn about ADHD medication? Until reading your post about second-line meds I thought Adderal was the only one
I can definitely talk about it a little! Always bearing in mind that I am not a doctor and this is not medical advice, etc. etc.
So, I've had many friends with ADHD in my life before I got my diagnosis and I picked up some stuff from them even before getting diagnosed; I also spoke with my prescribing psychiatrist about options when we met. If you think your psychiatrist might be resistant to discussing options, or you don't have one, doing your own research is good, but it's not really a substitute for a specialist in medication management. So it's also important to know what your needs are -- ie, "I want help with my executive function but I need something that's nonaddictive" or "I want something nonsedative" or "I don't think the treatment I'm on is working, what is available outside of this kind of medication?"
The problems you run into with researching medication for ADHD are threefold:
Most well-informed sources aren't actually geared towards non-doctor adults who just want to know what their options are -- they're usually either doctors who don't know how to talk about medication to non-doctors, or doctors (and parents) talking to parents about pediatric options.
A huge number of sites when you google are either AI-generated, covert ads for stimulant addiction rehab, or both.
Reliable sites with easy-to-understand information are not updated super often.
So you just kind of have to be really alert and read the "page" itself for context clues -- is it a science journal, is it an organization that helps people with ADHD, is it a doctor, is it a rehab clinic, is it a drug advertiser, is it a random site with a weird URL that's probably AI generated, etc.
So for example, ADDitude Magazine, which is kind of the pre-eminent clearinghouse for non-scholarly information on ADHD, is a great place to start, but when the research is clearly outlined it sometimes isn't up-to-date, and when it's up-to-date it's often a little impenetrable. They have an extensive library of podcast/webinars, and I started this particular research with this one, but his slides aren't super well-organized, he flips back and forth between chemical and brand name, and he doesn't always designate which is which. However, he does have a couple of slides that list off a bunch of medications, so I just put those into a spreadsheet, gleaned what I could from him, and then searched each medication. I did find a pretty good chart at WebMD that at least gives you the types and brand names fairly visibly. (Fwiw with the webinar, I definitely spent more time skimming the transcript than listening to him, auto transcription isn't GOOD but it is helpful in speeding through stuff like that.)
I think, functionally, there are four types of meds for ADHD, and the more popular ones often have several variations. Sometimes this is just for dosage purposes -- like, if you have trouble swallowing pills there are some meds that come in liquids or patches, so it's useful to learn the chemical name rather than the brand name, because then you can identify several "brands" that all use the same chemical and start to differentiate between them.
Top of the list you have your methylphenidate and your amphetamine, those are the two types of stimulant medications; the most well known brand names for these are Ritalin (methylphenidate) and Adderall (amphetamine).
Then there's the nonstimulant medications, SNRIs (Strattera, for example) and Alpha-2 Agonists (guanfacine and clonidine, brand names Kapvay and Intuniv; I'm looking at these for a second-line medication). There's some crossover between these and the next category:
Antidepressants are sometimes helpful with ADHD symptoms as well as being helpful for depression; I haven't looked at these much because for me they feel like the nuclear option, but it's Dopamine reuptake inhibitors like Wellbutrin and tricyclics like Tofranil. If you're researching these you don't need to look at like, every antidepressant ever, just look for ones that are specifically mentioned in context with ADHD.
Lastly there are what I call the Offlabels -- medications that we understand to have an impact on ADHD for some people, but which aren't generally prescribed very often, and sometimes aren't approved for use. I don't know much about these, either, because they tend to be for complex cases that don't respond to the usual scrips and are particularly difficult to research. The one I have in my notes is memantine (brand name Namenda) which is primarily a dementia medication that has shown to be particularly helpful for social cognition in people with combined Autism/ADHD.
So yeah -- hopefully that's a start for you, but as with everything online, don't take my word for it -- I'm also a lay person and may get stuff wrong, so this is just what I've found and kept in my notes. Your best bet truly is to find a psychiatrist specializing in ADHD medication management and discuss your options with them. Good luck!
136 notes
·
View notes
Text
Electrical Neurostimulation Therapy: An Alternative Treatment Option for Obstructive Sleep Apnea

Electrical Neurostimulation Therapy: An Alternative Treatment Option for Obstructive Sleep Apnea in Biomedical Journal of Scientific & Technical Research
Obstructive sleep apnea, or OSA, is a condition that disrupts breathing during sleep. OSA occurs when the tongue and other soft tissues relax during sleep and obstruct the airway [1] (Figure 1). During sleep, upper airway muscles tend to relax, in healthy subjects, muscle tone is high enough to prevent the upper airway from collapse during sleep but in OSA patients upper airway is not capable to maintain the patency and leads to a partial or complete collapse of the upper airway. The oxygen level in the blood decreases and the brain senses a problem due to sudden reduction (hypopnea) or complete cessation (apnea) of airflow that persists at least for 10 sec. The severity of OSA is measured by apnea/hypopnea index (AHI), which is calculated by apneas and hypopneas per hour of sleep. Sleep studies (Polysomnography) are recommended for the diagnosis of OSA. The AHI score depicts the severity of OSA: Mild (5 ≤ AHI < 15/h), moderate (15 ≤ AHI < 30/h), and severe (AHI ≥ 30/h) sleep [2]. The OSA is more common in males (14%) as compared to females (5%) [3]. Common symptoms of OSA include snoring, daytime sleepiness, irritability, or difficulty with focus or concentration. If left untreated, OSA can lead to secondary health issues such as: a. Heart attack b. High blood pressure c. Stroke d. Heart failure e. Irregular heartbeats f. Weight gain To reduce the morbidity of OSA, successful treatment of OSA is important. Multiple treatment options are available. Electrical neurostimulation therapy is an emerging treatment option for OSA. In this therapy hypoglossal nerve is stimulated by an electric current that protrudes the tongue and opens the upper airway.
For more articles in Journals on Biomedical Sciences click here bjstr
Follow on Twitter : https://twitter.com/Biomedres01 Follow on Blogger : https://biomedres01.blogspot.com/ Like Our Pins On : https://www.pinterest.com/biomedres/
#Medical Humanities#Nano Medicine#Family Medicine#Journal of Biomedical Research#Journals on Biomedical Science
0 notes
Text
Understanding the theory’s ascent from fringe forums to scientific journals to the halls of Congress helps clarify some of the moral panic and pernicious logic employed to restrict the autonomy and rights of trans people today. It also serves as a vivid example of how questionable science can be weaponized to achieve political goals.
A number of studies on trans youth have taken on “misinformational afterlives,” says TJ Billard, an assistant professor of communications at Northwestern University and executive director of the Center for Applied Transgender Studies. Among them are four papers published between 2008 and 2013 that have together been used to claim that most children “grow out” of gender dysphoria and opt not to transition. All have been shown to have numerous shortcomings. In some, nearly 40% of young people surveyed did not meet the criteria for the official gender dysphoria diagnosis in the Diagnostic and Statistical Manual of Mental Disorders edition used at the time. In two, researchers classified some subjects as having detransitioned—or reversed their transition—purely on the basis of whether a parent or third party said it happened. A 2018 study found that three of the papers labeled those who had stopped responding to researchers as detransitioners; and in one, a subject who identified as nonbinary was classified as detransitioning.
“There’s a wealth of bad science that is out there, and this science doesn’t stay in journals,” Billard says. Parents unfamiliar with trans issues, who don’t understand gender-affirming health care and don’t have the expertise to read the studies themselves, often fall under its sway.
... When Littman took up the question, she decided to survey parents, who she felt would be easier to reach than trans youths themselves. In her Methods section, she writes that “to maximize the chances of finding cases meeting eligibility criteria”—meaning youths who suddenly became gender dysphoric, according to their parents—she turned to three websites: 4thwavenow.com, a “community of people who question the medicalization of gender-atypical youth”; transgendertrend.com, which says it’s concerned about “the unprecedented number of teenage girls suddenly self-identifying as ‘trans’”; and youthtranscriticalprofessionals.org, a now-private website that was “concerned about the current trend to quickly diagnose and affirm young people as transgender.”
The results were in line with what one might expect given those sources: 76.5% of parents surveyed “believed their child was incorrect in their belief of being transgender.” More than 85% said their child had increased their internet use and/or had trans friends before identifying as trans. The youths themselves had no say in the study, and there’s no telling if they had simply kept their parents in the dark for months or years before coming out. (Littman acknowledges that “parent-child conflict may also explain some of the findings.”)
Arjee Restar, now an assistant professor of epidemiology at the University of Washington, didn’t mince words in her 2020 methodological critique of the paper. Restar noted that Littman chose to describe the “social and peer contagion” hypothesis in the consent document she shared with parents, opening the door for biases in who chose to respond to the survey and how they did so. She also highlighted that Littman asked parents to offer “diagnoses” of their child’s gender dysphoria, which they were unqualified to do without professional training. It’s even possible that Littman’s data could contain multiple responses from the same parent .... But politics is blind to nuances in methodology. And the paper was quickly seized by those who were already pushing back against increasing acceptance of trans people. ... Many people who are citing Littman’s work probably haven’t even read the study or seen the correction, Billard says: “People are citing a Reddit post in which somebody invoked the idea of Littman and her research.” Littman agrees with this characterization. “It boggles my mind how people are comfortable holding forth on topics that they haven’t actually read papers [about],” she says.
... Lawmakers in more than 25 states have introduced anti-trans bills during 2022 legislative sessions. Politicians writing such legislation have plenty of questionable studies, partisan doctors, and associations that lobby against transgender rights to draw on. Littman’s ROGD study is often a go-to. The Coalition for the Advancement & Application of Psychological Science wrote in 2021 that many of the “over 100 bills under consideration in legislative bodies across the country that seek to limit the rights of transgender adolescents” are “predicated on the unsupported claims advanced by ROGD.”
2K notes
·
View notes